
Submitted:
17 August 2024
Posted:
19 August 2024
You are already at the latest version
Abstract
Venous and arterial thromboembolism (VTE/ATE) often coexist with onco-hematologic diagnosis. The study aimed to assess the time relationship between the diagnosis of VTE/ATE and blood cancers. The second aim was to identify VTE/ATE risk factors related to the type of hematology disease and cardiac history. 1283 patients underwent cardio-oncology evaluation at the Institute of Hematology and Transfusion Medicine in Warsaw from March 2021 through March 2023 (2 years), and 101 (7.8%) cases were identified with VTE/ATE. ATE compared to VTE significantly more often occurred before the diagnosis and treatment of hematologic malignancy: 33/47 (70.2%) vs. 15/54 (27.8%), p<0.0001. The risk of a VTE episode is exceptionally high in the first months after the diagnosis of an onco-hematological disease. The higher frequency of VTE was associated with acute myeloid leukemia (17 cases/270 patients/6.30%/p = 0.055), acute lymphocytic leukemia (7 cases/76 patients/9.21%/p = 0.025) and chronic myeloproliferative disease (7 cases/48 patients/14.58%/p=0.0003). Only the risk of VTE was significantly increased before (OR=6.79; 95%CI: 1.85-24.95; p=0.004) and after diagnosis of myeloproliferative disease (OR=3.12; 95%CI: 1.06-9.16; p=0.04). ATEs occur more often than VTE before a diagnosis of blood cancer. The risk of VTE is exceptionally high before and after diagnosis of chronic myeloproliferative disease.
Keywords:
cardio-oncology
; hemato-oncology
; thromboembolism
Introduction
A thromboembolic event may be the first symptom of cancer.[1,2] The first data on such a relationship concerned pulmonary embolism and deep vein thrombosis.[3] Another correlation was found for stroke.[4,5,6] The effects of cancer screening programs in patients after pulmonary embolism have been analyzed.[7] Cancer screening programs for stroke patients have also been planned.[8] We need data on the importance of myocardium infarction as the first symptom of cancer.[9]
It seems that there is a high risk of thromboembolism in the group of blood cancers, where coagulation disorders may be particularly turbulent.[10] However, initiating anticancer therapy may be associated with increased activation of prothrombotic factors or damage to the vascular endothelium, consequently leading to coagulopathy. An exceptionally high risk of venous and arterial thromboembolic events (VTE/ATE) is associated with the use of antiangiogenic drugs, second- and third-generation BCR-ABL inhibitors and immune checkpoint inhibitors.[11,12,13,14] These observations allowed us to define a separate group of complications related to oncological treatment called vascular toxicity.[15] It includes symptomatic and asymptomatic venous and arterial thrombosis, myocardial infarction, stroke, peripheral artery diseases, and coronary artery spasms.
Both venous and arterial thromboembolic events are associated with worse prognosis in cancer patients.[16,17] It seems clinically essential to assess to what extent a given event is related to the cancer and to what extent it is related to its treatment. Identification of factors predisposing to the occurrence of venous and arterial thromboembolic events and the time relationship to the moment of cancer diagnosis seems to be crucial to optimize recommendations for primary and secondary prevention. This is especially important because these patients are at an exceptionally high risk of bleeding, which results from thrombocytopenia, platelet dysfunction, and bone marrow suppression.[18,19] Moreover, knowing such a temporal relationship may help plan optimal oncological screening. This is particularly important in patients with blood cancers because we have the most minor epidemiological data.
The aim of the study was to assess the time relationship between the moment of diagnosis of hematological cancer and the moment of occurrence of venous or arterial thromboembolism. The second aim was to identify VTE/ATE risk factors related to the type of cancer and cardiac characteristics of the patients.
Materials and Methods
The retrospective analysis included patients evaluated by cardio-oncologists certified by the International Cardio-Oncology Society at the reference Polish hematology center - the Institute of Hematology and Transfusion Medicine in Warsaw. Clinical data were collected from March 2021 through March 2023 (2 years).
During cardio-oncology evaluation the moment of de novo diagnosis of venous or arterial thromboembolism (VTE/ATE) was analyzed relative to the date of diagnosis of blood cancer. The second step was to assess odds ratio for VTE/ATE depending on the type of hematologic malignancy and cardiac history data.
Statistical analyses were performed by using the Statistica software. Patient characteristics were presented as frequency of diagnoses and their percentages in population for hematologic malignancies, comorbid cardiovascular diseases, including diagnoses of venous and arterial thromboembolisms. The following were considered thromboembolic (TE) diseases: pulmonary embolism and/or thrombosis of the veins of the limbs, and arterial TE: myocardial infarction and/or ischemic stroke. The chi-square test was used to compare the difference in the incidence of arterial and venous thromboembolism (ATE vs. VTE) before the diagnosis of hematologic malignancy. Then, the chi-square test with the possible Yates correction was used to determine the relationship between the more frequent occurrence of venous or arterial thromboembolism in correlation with the diagnosis of a specific type of blood cancer. Finally, logistic regression analyzes were used and the odds ratio for the occurrence of ATE and VTE was calculated depending on the type of cancer and comorbid cardiovascular diseases. Statistically significant results were considered those for which p was less than 0.05
Results
At the Institute of Hematology and Transfusion Medicine in Warsaw, from March 2021 through March 2023 (two years), 1283 hemato-oncology patients underwent cardio-oncology evaluation. The majority were men (673/52.5%), the median age was 63 years (IQ: 47 - 71) (Table 1, Figure 1)
The dominant hematological diagnoses were acute myeloid leukemia (n= 270, 21%), non-Hodgkin's lymphoma (NHL) (n= 250, 19.5%), and multiple myeloma (n= 223, 17.4%), chronic lymphocytic leukemia (CLL) (n=101, 7.88%), acute lymphocytic leukemia (ALL) (n=76, 5.92%). Nearly half of the patients had at least one comorbid cardiovascular disease, of which arterial hypertension (40%) and cardiac arrhythmias (15.8%) were predominant.
The group of 101 (7.8%) patients with a history of thromboembolism (TE) were identified in the analyzed population. Venous thromboembolic events (VTE) accounted for 53%. It was shown that VTE episodes occurred significantly more often after the initiation of anticancer treatment (p< 0.0001) compared to arterial thromboembolism (ATE), most of which were observed before (70.2%) the hematological malignancy was revealed.
The time-dependence analysis showed that the highest risk of diagnosing acute VTE occurs in the first months after anticancer treatment is started (Figure 2). A similarly strong correlation was not demonstrated in the case of arterial events, which were observed mainly before the diagnosis of hematologic cancer and thus before the initiation of anticancer treatment - 33 cases, representing 70.2% of all diagnoses of arterial thromboembolic complications (Figure 3).
Through an analysis of the distribution of thromboembolic events in relation to histopathological diagnoses of hematological malignancies, it was shown that VTE was most often diagnosed in patients with AML (17 cases/6.30%/p=0.055), ALL (7 cases/9.21%/p=0.025) and chronic myeloproliferative disease (7 cases/14.58%/p=0.0003). However, there was no increased incidence of ATE depending on the diagnosis of hematologic cancer (Table 2).
For the occurrence of ATE events before the diagnosis of hematologic cancer, the cardiac history was important, both in terms of the presence of classic risk factors for atherosclerosis, i.e., older age and hypertension and as co-occurring heart failure, coronary artery disease, or arrhythmia (Table 3). Interestingly, all these factors were significant only before the diagnosis of cancer; their significance disappeared after the diagnosis of cancer and the initiation of hematological treatment. Only coronary artery disease retained its importance for the risk of ATE after a cancer diagnosis.
Cardiological history was of no significance in the context of VTE. (Table 4). Only diabetes melittus had the significant correlation with the diagnosis of VTE especially after diagnosis of hematological malignancy (OR=2.42, p=0.03). Some histopathological diagnoses were also important for VTE. Diagnosis of acute lymphocytic leukemia correlated with later with increased probability of VTE (OR=3.05, p=0.015). In the case of myeloproliferative disease, the risk of VTE was increased both before and after diagnosis (OR=6.79, p=0.004 and OR=3.12, p=0.04.
Discussion
Venous and arterial thromboembolic events (VTE/ATE) occur with quite significant frequency in hematological patients. The latest data indicate that the pathogenesis and clinical picture may differ from solid tumors.[20] Regardless of the cause or type of tumor, the prognosis of patients with a thrombotic event is always poorer.[16,21] The mortality risk is particularly high when cancer is diagnosed at the same time as a thromboembolic event. The benefits of anticoagulant therapy using anticoagulants that are not vitamin K antagonists may also differ in hemato-oncology, and there is undoubtedly less evidence for its effectiveness.[22] There may be a greater risk of complications such as bleeding, which may be caused by thrombocytopenia and platelet dysfunction.[23] The risk of late complications such as thromboembolic pulmonary hypertension may also be higher.[24] Myeloproliferative diseases are a known risk factor for the development of pulmonary hypertension.[25] Risk factors for the development of pulmonary hypertension in the course of myeloproliferative diseases are constantly discussed.[26] Our publication shows an increased risk of venous thromboembolic complications, adding a new aspect related to thromboembolic changes. Currently, pulmonary hypertension due to myeloproliferative diseases is classified in group 5, i.e. with unknown or multifactorial pathogenesis.[27]
Multiple myeloma has well-defined indications for primary thromboprophylaxis.[28,29] This is due to the high risk of thromboembolic events associated with the use of immunomodulatory drugs, steroids, or the presence of fractures and immobilization.[30] Lymphoma patients also usually receive primary antithrombotic prophylaxis because, according to the thromboembolic risk stratification proposed by Khorana, lymphoma receives one point.[31] Such prophylaxis can be considered from two points of view, according to the latest research.[32,33] For this reason, perhaps in our population, patients with myeloma and non-Hodgkin's lymphoma did not experience VTE very often.
Our data, however, confirm other reports indicating that patients with AML and ALL are at risk of VTE.[14]Our analysis shows that patients with AML and ALL are at exceptionally high risk of VTE events. In the literature, the incidence of VTE in AML is estimated to range from 2% to nearly 15%; in our population 6.3% of patients with AML experience an acute episode of VTE.[34] The pathogenesis of these events is complex, but considering the correlation with the initiation of chemotherapy, it should be assumed that the dominant mechanism is the massive release of procoagulants due to the lysis of cancer cells.[35] This mechanism is strengthened by hemodynamic changes and vascular damage. Another factor of thrombotic events in AML is DIC (disseminated intravascular coagulation), which occurs in about 30% of patients at diagnosis.[36] The coexistence of increased risk of thrombosis and bleeding, such as thrombocytopenia typical of AML, makes it challenging to choose the optimal antithrombotic therapy. It should be emphasized that, unlike patients with lymphoma and ALL, a VTE episode in patients with AML is not associated with an increased risk of death within one year.[37,38]. Our study confirmed the problem of VTE in AML is noticeable, although the result of the correlation between VTE and AML was on the verge of statistical significance.
Another group of our patients at a clear significant risk of VTE is patients with ALL, with an incidence of 9.2%. In a large meta-analysis of 72 prospective studies, including 9061 patients, the VTE incidence rate (IR) in ALL was determined to be 5% (95% CI: 4–6%).[32] The authors emphasize that antithrombotic prophylaxis using LMWH significantly reduces the risk of VTE events in this group. One of the main factors associated with a higher rate of thrombotic events is the use of chemotherapy.[39] There are no similar observations in the case of targeted treatment with TKIs (tyrosine kinase inhibitors), and reports regarding the use of steroids are unclear.[39,40,41]. Our study clearly shows that after the diagnosis of ALL, and therefore during active treatment of ALL, we had a problem with a significantly higher incidence of VTE. Therefore, future studies should be conducted to identify risk factors for VTE in ALL related not so much to the patients' characteristics but to the drugs used for ALL treatment and the possible degree of aggressiveness of the ALL course.
It should be added that it is surprising that patients with AML and ALL were not included in large clinical trials with new anticoagulants.[42,43] The latest guidelines of the European Society of Cardiology emphasize this fact.[44] This may be surprising in the context of the results of our observation and the cited studies. These patients are disqualified from large clinical trials due to thrombocytopenia and a high baseline risk of bleeding. Therefore, personalized trials should be planned for AML and ALL patients in terms of both primary and secondary prevention of VTE.
A lot of data show that the risk of both venous and arterial thromboembolic events is the highest during the period of diagnosis of cancer.[45,46] The disease in the metastatic phase poses a significantly higher risk of both venous and arterial complications, but this applies to solid tumors.[14,47] Also, recurrence of venous thromboembolism is more common in metastatic disease.[48] Additionally, the molecular type of cancer increases the risk of thromboembolism.[49] The type of anticancer therapy or supportive care is also important.[50,51].
In hematology, of course, we cannot talk about metastatic disease, but we can use other criteria to assess the advancement or aggressive course of a hematological cancer. It is worth checking to what extent VTE diagnosed, especially in ALL and myeloproliferative diseases, is associated with a negative cardiological and oncological prognosis. Our observation shows one more problem. ATE may be a clinical indicator preceding the diagnosis of hematologic cancer by up to several months. This correlation shown in Figure 3 should attract the attention of interventional cardiologists, who should monitor especially older patients after an ATE episode for a possible subsequent diagnosis of hematologic malignancy.
Our publication is the first to comprehensively analyze the problem of venous and arterial thromboembolic events in patients with hematological malignancies. We have proven that the type of histopathological diagnosis is essential for the risk of venous thromboembolic events (VTE). Many guideline documents indicate that one should remember patient-related factors among the risk factors for thromboembolic complications and those related to cancer and cancer treatment. This, of course, includes the issue of comorbidities that may additionally increase the risk of thromboembolism. Our study shows that coexisting cardiac diseases are not crucial for the occurrence of VTE. This suggests that the main predictors of a VTE are the onco-hematological disease and/or its treatment.[17,52] Still, they are decisive for the occurrence of arterial complications, especially before the diagnosis of cancer. Only coronary artery disease remains a significant risk factor for ATE if hematological cancer is already diagnosed and treated. Moreover, in the aspect of hematological malignancies, only ATEs may precede the diagnosis of cancer. Some studies have shown an increased risk of ATE in the period preceding the diagnosis of cancer, suggesting that cancer is associated with a risk of ATE that goes beyond conventional cardiovascular risk factors. Further population studies are needed to determine whether patients with a history of ATE should be screened for hematological malignancies.
To some extent, our study constitutes another step in the discussion about the importance of the so-called "reverse cardio-oncology".[53,54] This is a relatively new hypothesis claiming that cardiovascular diseases contribute to the development and progression of cancer.[55] Of course, the common denominator may be common risk factors, chronic inflammation, and tissue hypoxia in patients with atherosclerosis.[56,57] Several preclinical studies are being conducted to elucidate possible pathomechanisms.[58] Our study may complement the current discussion on the co-occurrence of heart diseases and cancer.[59] We have proven that ATEs occur quite frequently before the diagnosis of a hematologic malignancy. We do not know whether this is just an early effect of clotting disorders caused by developing blood cancer.
Our study is limited in that it is not a large population study but only an observational study based on cardio-oncologists' activities at the main hematology Polish center. However, given that the current guidelines on cardio-oncology published in 2022 by the European Society of Cardiology in cooperation with the European Hematology Association, recommend risk stratification according to Heart Failure Association -International Cardio-Oncology Society (HFA-ICOS) tool in patients before anticancer treatment, it can be assumed that we analyzed a representative population of patients with hematologic malignancies in the reference Polish hematology center.[60] Undoubtedly, large population studies are necessary to confirm our observations.
Conclusions
ATEs occur significantly more often than VTE before the diagnosis of hematological malignancies, especially in patients with a significant cardiac history.
The occurrence of VTE is most frequently observed in the first months after the diagnosis of onco-hematological disease andis most closely associated with the diagnosis of acute lymphocytic leukemia and myeloproliferative disease.
Funding
The study has been supported by the Centre of Postgraduate Medical Education: Program number: 501-1-142-21-24.
Conflicts of Interest
The authors have no conflict of interest to declare regarding this study.
Ethical Approval: The study was approved by the Bioethical Committee of the Centre of Postgraduate Medical Education, Warsaw, Poland, opinion number 74/2022, date 08 June 2022.
Availability of data and materials: All data of the study will be available upon reasonable request and
with permission of the Directors of the Institute of Hematology and Transfusion Medicine in Warsaw, Poland.
References
- Delluc, A.; Ianotto, J.-C.; Tromeur, C.; De Moreuil, C.; Couturaud, F.; Lacut, K. , et al. Real-world incidence of cancer following a first unprovoked venous thrombosis: Results from the EPIGETBO study. Thrombosis Research. 2018, 164, 79–84. [Google Scholar] [CrossRef]
- White RH, Chew HK, Zhou H, Parikh-Patel A, Harris D, Harvey D, et al. Incidence of Venous Thromboembolism in the Year Before the Diagnosis of Cancer in 528 693 Adults. Archives of Internal Medicine. 2005, 165, 1782. [CrossRef]
- Douketis, J.D.; Gu, C.; Piccioli, A.; Ghirarduzzi, A.; Pengo, V.; Prandoni, P. The long-term risk of cancer in patients with a first episode of venous thromboembolism. J Thromb Haemost. 2009, 7, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Taccone, F.S.; Jeangette, S.M.; Blecic, S.A. First-ever stroke as initial presentation of systemic cancer. J Stroke Cerebrovasc Dis. 2008, 17, 169–174. [Google Scholar] [CrossRef]
- Selvik, H.A.; Bjerkreim, A.T.; Thomassen, L.; Waje-Andreassen, U.; Naess, H.; Kvistad, C.E. When to Screen Ischaemic Stroke Patients for Cancer. Cerebrovasc Dis. 2018, 45, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Quintas S, Rogado J, Gullón P, Pacheco-Barcia V, Dotor García-Soto J, Reig-Roselló G, et al. Predictors of unknown cancer in patients with ischemic stroke. J Neurooncol. 2018, 137, 551–557. [CrossRef]
- Robertson, L.; Yeoh, S.E.; Stansby, G.; Agarwal, R. Effect of testing for cancer on cancer- and venous thromboembolism (VTE)-related mortality and morbidity in people with unprovoked VTE. Cochrane Database Syst Rev. 2017, 8, CD010837. [Google Scholar] [CrossRef]
- Fang J, Wu J, Hong G, Zheng L, Yu L, Liu X, et al. Cancer screening in hospitalized ischemic stroke patients: a multicenter study focused on multiparametric analysis to improve management of occult cancers. EPMA J. 2024, 15, 53–66. [CrossRef]
- Pernod G, Cohen A, Mismetti P, Sanchez O, Mahé I, INNOVTE CAT Working Group. Cancer-related arterial thromboembolic events. Arch Cardiovasc Dis. 2024, 117, 101–113. [CrossRef] [PubMed]
- Martens KL, Li A, La J, May SB, Swinnerton KN, Tosi H, et al. Epidemiology of Cancer-Associated Venous Thromboembolism in Patients With Solid and Hematologic Neoplasms in the Veterans Affairs Health Care System. JAMA Netw Open. 2023, 6, e2317945. [CrossRef]
- Miroddi M, Sterrantino C, Simmonds M, Caridi L, Calapai G, Phillips RS, et al. Systematic review and meta-analysis of the risk of severe and life-threatening thromboembolism in cancer patients receiving anti-EGFR monoclonal antibodies (cetuximab or panitumumab). Intl Journal of Cancer. 2016, 139, 2370–2380. [CrossRef] [PubMed]
- Arnold D, Fuchs CS, Tabernero J, Ohtsu A, Zhu AX, Garon EB, et al. Meta-analysis of individual patient safety data from six randomized, placebo-controlled trials with the antiangiogenic VEGFR2-binding monoclonal antibody ramucirumab. Annals of Oncology. 2017, 28, 2932–2942. [CrossRef]
- Haguet, H.; Douxfils, J.; Mullier, F.; Chatelain, C.; Graux, C.; Dogné, J.-M. Risk of arterial and venous occlusive events in chronic myeloid leukemia patients treated with new generation BCR-ABL tyrosine kinase inhibitors: a systematic review and meta-analysis. Expert Opinion on Drug Safety. 2017, 16, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.P.; Hisada, Y.M.; Kasthuri, R.S.; Reeves, B.N.; Mackman, N. Cancer Therapy–Associated Thrombosis. ATVB. 2021, 41, 1291–1305. [Google Scholar] [CrossRef]
- Herrmann J, Lenihan D, Armenian S, Barac A, Blaes A, Cardinale D, et al. Defining cardiovascular toxicities of cancer therapies: an International Cardio-Oncology Society (IC-OS) consensus statement. European Heart Journal. 2021, ehab674.
- Sørensen, H.T.; Pedersen, L.; van Es, N.; Büller, H.R.; Horváth-Puhó, E. Impact of venous thromboembolism on the mortality in patients with cancer: a population-based cohort study. Lancet Reg Health Eur. 2023, 34, 100739. [Google Scholar] [CrossRef]
- Mulder FI, Horváth-Puhó E, van Es N, Pedersen L, Büller HR, Bøtker HE, et al. Arterial Thromboembolism in Cancer Patients: A Danish Population-Based Cohort Study. JACC CardioOncol. 2021, 3, 205–218.
- Hsu, C.; Patell, R.; Zwicker, J.I. The prevalence of thrombocytopenia in patients with acute cancer-associated thrombosis. Blood Adv. 2023, 7, 4721–4727. [Google Scholar] [CrossRef]
- Wang, T.-F.; Leader, A.; Sanfilippo, K.M. Thrombosis and bleeding in hematological malignancy. Best Practice & Research Clinical Haematology. 2022, 35, 101353. [Google Scholar]
- Giustozzi M, Connors JM, Ruperez Blanco AB, Szmit S, Falvo N, Cohen AT, et al. Clinical characteristics and outcomes of incidental venous thromboembolism in cancer patients: Insights from the Caravaggio study. Journal of Thrombosis and Haemostasis. 2021, 19, 2751–2759. [CrossRef]
- Navi BB, Reiner AS, Kamel H, Iadecola C, Okin PM, Elkind MSV, et al. Risk of Arterial Thromboembolism in Patients With Cancer. Journal of the American College of Cardiology. 2017, 70, 926–938. [CrossRef]
- Giustozzi M, Agnelli G, del Toro-Cervera J, Klok FA, Rosovsky RP, Martin A-C, et al. Direct Oral Anticoagulants for the Treatment of Acute Venous Thromboembolism Associated with Cancer: A Systematic Review and Meta-Analysis. Thromb Haemost. 2020, 120, 1128–1136. [CrossRef] [PubMed]
- Falanga A, Leader A, Ambaglio C, Bagoly Z, Castaman G, Elalamy I, et al. EHA Guidelines on Management of Antithrombotic Treatments in Thrombocytopenic Patients With Cancer. HemaSphere. 2022, 6, e750. [CrossRef] [PubMed]
- Bohacekova, M.; Kaldararova, M.; Valkovicova, T.; Remkova, A.; Vesely, J.; Simkova, I. Risk factors detection in chronic thromboembolic pulmonary hypertension, a tool for risk quantification? Bratisl Lek Listy. 2016, 117, 577–582. [Google Scholar] [CrossRef]
- Montani D, Thoré P, Mignard X, Jaïs X, Boucly A, Jevnikar M, et al. Clinical Phenotype and Outcomes of Pulmonary Hypertension Associated with Myeloproliferative Neoplasms: A Population-based Study. Am J Respir Crit Care Med. 2023, 208, 600–612. [CrossRef]
- Ferrari, A.; Scandura, J.; Masciulli, A.; Krichevsky, S.; Gavazzi, A.; Barbui, T. Prevalence and risk factors for Pulmonary Hypertension associated with chronic Myeloproliferative Neoplasms. Eur J Haematol. 2021, 106, 250–259. [Google Scholar] [CrossRef]
- Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. European Heart Journal. 2022, 43, 3618–3731. [CrossRef]
- Falanga A, Ay C, Di Nisio M, Gerotziafas G, Jara-Palomares L, Langer F, et al. Venous thromboembolism in cancer patients: ESMO Clinical Practice Guideline. Ann Oncol. 2023, 34, 452–467. [CrossRef] [PubMed]
- Key NS, Khorana AA, Kuderer NM, Bohlke K, Lee AYY, Arcelus JI, et al. Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Guideline Update. J Clin Oncol. 2023, 41, 3063–3071. [CrossRef]
- Sanfilippo KM, Luo S, Wang T, Fiala M, Schoen M, Wildes TM, et al. Predicting venous thromboembolism in multiple myeloma: development and validation of the IMPEDE VTE score. American J Hematol. 2019, 94, 1176–1184. [CrossRef]
- Khorana, A.A.; Kuderer, N.M.; Culakova, E.; Lyman, G.H.; Francis, C.W. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood. 2008, 111, 4902–4907. [Google Scholar] [CrossRef]
- Khorana AA, Soff GA, Kakkar AK, Vadhan-Raj S, Riess H, Wun T, et al. Rivaroxaban for Thromboprophylaxis in High-Risk Ambulatory Patients with Cancer. N Engl J Med. 2019, 380, 720–728. [CrossRef] [PubMed]
- Carrier M, Abou-Nassar K, Mallick R, Tagalakis V, Shivakumar S, Schattner A, et al. Apixaban to Prevent Venous Thromboembolism in Patients with Cancer. N Engl J Med. 2019, 380, 711–719. [CrossRef]
- Paterno G, Palmieri R, Forte V, Del Prete V, Gurnari C, Guarnera L, et al. Predictors of Early Thrombotic Events in Adult Patients with Acute Myeloid Leukemia: A Real-World Experience. Cancers. 2022, 14, 5640. [CrossRef]
- Lyman, G.H.; Eckert, L.; Wang, Y.; Wang, H.; Cohen, A. Venous Thromboembolism Risk in Patients With Cancer Receiving Chemotherapy: A Real-World Analysis. The Oncologist. 2013, 18, 1321–1329. [Google Scholar] [CrossRef]
- Libourel EJ, Klerk CPW, van Norden Y, de Maat MPM, Kruip MJ, Sonneveld P, et al. Disseminated intravascular coagulation at diagnosis is a strong predictor for thrombosis in acute myeloid leukemia. Blood. 2016, 128, 1854–1861. [CrossRef]
- Khorana, A.A. Venous thromboembolism and prognosis in cancer. Thrombosis Research. 2010, 125, 490–493. [Google Scholar] [CrossRef]
- Ku, G.H.; White, R.H.; Chew, H.K.; Harvey, D.J.; Zhou, H.; Wun, T. Venous thromboembolism in patients with acute leukemia: incidence, risk factors, and effect on survival. Blood. 2009, 113, 3911–3917. [Google Scholar] [CrossRef]
- Faiz, A.S.; Sridharan, A.; Guo, S.; Lin, Y.; Philipp, C.S. Risk factors and mortality associated with venous thromboembolism in the elderly US population with acute lymphocytic leukemia. Thrombosis Update. 2024, 14, 100155. [Google Scholar] [CrossRef]
- Johannesdottir SA, Horváth-Puhó E, Dekkers OM, Cannegieter SC, Jørgensen JOL, Ehrenstein V, et al. Use of Glucocorticoids and Risk of Venous Thromboembolism: A Nationwide Population-Based Case-Control Study. JAMA Intern Med. 2013, 173, 743. [CrossRef]
- Orsi FA, Lijfering WM, Geersing G, Rosendaal FR, Dekkers OM, Le Cessie S, et al. Glucocorticoid use and risk of first and recurrent venous thromboembolism: self-controlled case-series and cohort study. Br J Haematol. 2021, 193, 1194–1202. [CrossRef] [PubMed]
- Raskob GE, van Es N, Verhamme P, Carrier M, Di Nisio M, Garcia D, et al. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism. New England Journal of Medicine. 2018, 378, 615–624. [CrossRef]
- Agnelli G, Becattini C, Meyer G, Muñoz A, Huisman MV, Connors JM, et al. Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer. N Engl J Med. 2020, 382, 1599–1607. [CrossRef] [PubMed]
- Lyon AR, López-Fernández T, Couch LS, Asteggiano R, Aznar MC, Bergler-Klein J, et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). European Heart Journal. 2022, ehac244.
- Giustozzi M, Curcio A, Weijs B, Field TS, Sudikas S, Katholing A, et al. Variation in the Association between Antineoplastic Therapies and Venous Thromboembolism in Patients with Active Cancer. Thromb Haemost. 2020, 120, 847–856. [CrossRef]
- Herrmann, J. Vascular toxic effects of cancer therapies. Nature Reviews Cardiology. 2020, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Navi BB, Reiner AS, Kamel H, Iadecola C, Okin PM, Elkind MSV, et al. Risk of Arterial Thromboembolism in Patients With Cancer. Journal of the American College of Cardiology. 2017, 70, 926–938.
- Verso M, Agnelli G, Munoz A, Connors JM, Sanchez O, Huisman M, et al. Recurrent venous thromboembolism and major bleeding in patients with localised, locally advanced or metastatic cancer: an analysis of the Caravaggio study. Eur J Cancer. 2022, 165, 136–145. [CrossRef] [PubMed]
- Feldman S, Gupta D, Navi BB, Grace Ho K-W, Willeit P, Devlin S, et al. Tumor Genomic Profile Is Associated With Arterial Thromboembolism Risk in Patients With Solid Cancer. JACC CardioOncol. 2023, 5, 246–255. [CrossRef]
- Moik F, Chan W-SE, Wiedemann S, Hoeller C, Tuchmann F, Aretin M-B, et al. Incidence, risk factors, and outcomes of venous and arterial thromboembolism in immune checkpoint inhibitor therapy. Blood. 2021, 137, 1669–1678. [CrossRef]
- Mulder FI, Horváth-Puhó E, van Es N, van Laarhoven HWM, Pedersen L, Moik F, et al. Venous thromboembolism in cancer patients: a population-based cohort study. Blood. 2021, 137, 1959–1969. [CrossRef]
- Wang, J.; Kim, Y.D.; Kim, C.H. Incidence and Risk of Various Types of Arterial Thromboembolism in Patients With Cancer. Mayo Clinic Proceedings. 2021, 96, 592–600. [Google Scholar] [CrossRef]
- Aboumsallem, J.P.; Moslehi, J.; de Boer, R.A. Reverse Cardio-Oncology: Cancer Development in Patients With Cardiovascular Disease. J Am Heart Assoc. 2020, 9, e013754. [Google Scholar] [CrossRef] [PubMed]
- Imran S, Rao MS, Shah MH, Gaur A, Guernaoui AE, Roy S, et al. Evolving perspectives in reverse cardio-oncology: A review of current status, pathophysiological insights, and future directives. Curr Probl Cardiol. 2024, 49, 102389. [CrossRef]
- Liang, Z.; He, Y.; Hu, X. Cardio-Oncology: Mechanisms, Drug Combinations, and Reverse Cardio-Oncology. Int J Mol Sci. 2022, 23, 10617. [Google Scholar] [CrossRef]
- Sinha A, Bavishi A, Hibler EA, Yang EH, Parashar S, Okwuosa T, et al. Interconnected Clinical and Social Risk Factors in Breast Cancer and Heart Failure. Front Cardiovasc Med. 2022, 9, 847975. [CrossRef] [PubMed]
- Di Fusco SA, Cianfrocca C, Bisceglia I, Spinelli A, Alonzo A, Mocini E, et al. Potential pathophysiologic mechanisms underlying the inherent risk of cancer in patients with atherosclerotic cardiovascular disease. Int J Cardiol. 2022, 363, 190–195. [CrossRef]
- Koelwyn, G.J.; Aboumsallem, J.P.; Moore, K.J.; de Boer, R.A. Reverse cardio-oncology: Exploring the effects of cardiovascular disease on cancer pathogenesis. J Mol Cell Cardiol. 2022, 163, 1–8. [Google Scholar] [CrossRef] [PubMed]
- de Wit S, de Boer RA. From Studying Heart Disease and Cancer Simultaneously to Reverse Cardio-Oncology. Circulation. 2021, 144, 93–95. [CrossRef] [PubMed]
- Lyon AR, Dent S, Stanway S, Earl H, Brezden-Masley C, Cohen-Solal A, et al. Baseline cardiovascular risk assessment in cancer patients scheduled to receive cardiotoxic cancer therapies: a position statement and new risk assessment tools from the C ardio- O ncology S tudy G roup of the H eart F ailure A ssociation of the E uropean S ociety of C ardiology in collaboration with the I nternational C ardio- O ncology S ociety. Eur J Heart Fail. 2020, 22, 1945–1960.
Figure 1.
General diagram of frequency of thromboembolic events (TE): arterial thromboembolic events (ATE) were more frequent before malignancy diagnosis than venous thromboembolic events (VTE): 33/47 (70.2 %) vs. 15/54 (27.8 %), p<0.0001.
Figure 1.
General diagram of frequency of thromboembolic events (TE): arterial thromboembolic events (ATE) were more frequent before malignancy diagnosis than venous thromboembolic events (VTE): 33/47 (70.2 %) vs. 15/54 (27.8 %), p<0.0001.
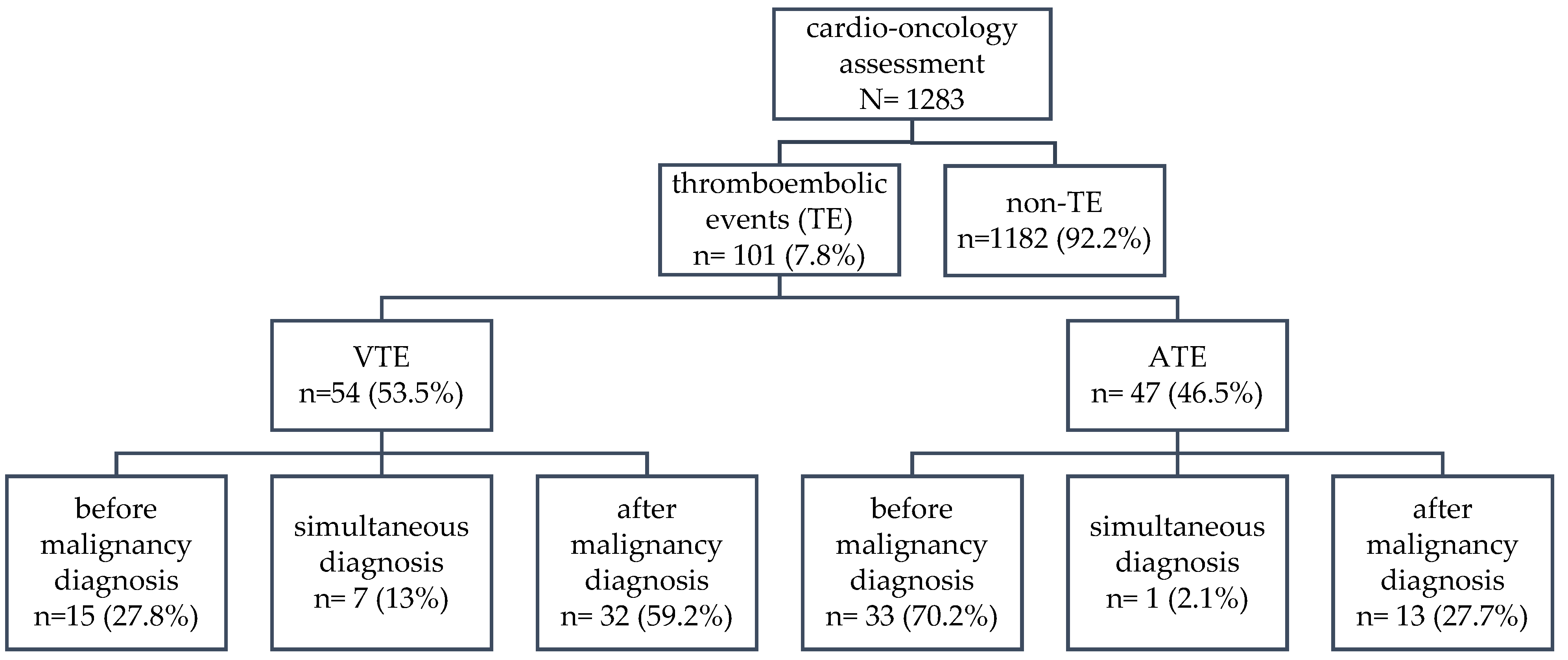
Figure 2.
Incidence of acute VTE before and after diagnosis of hematologic malignancy.
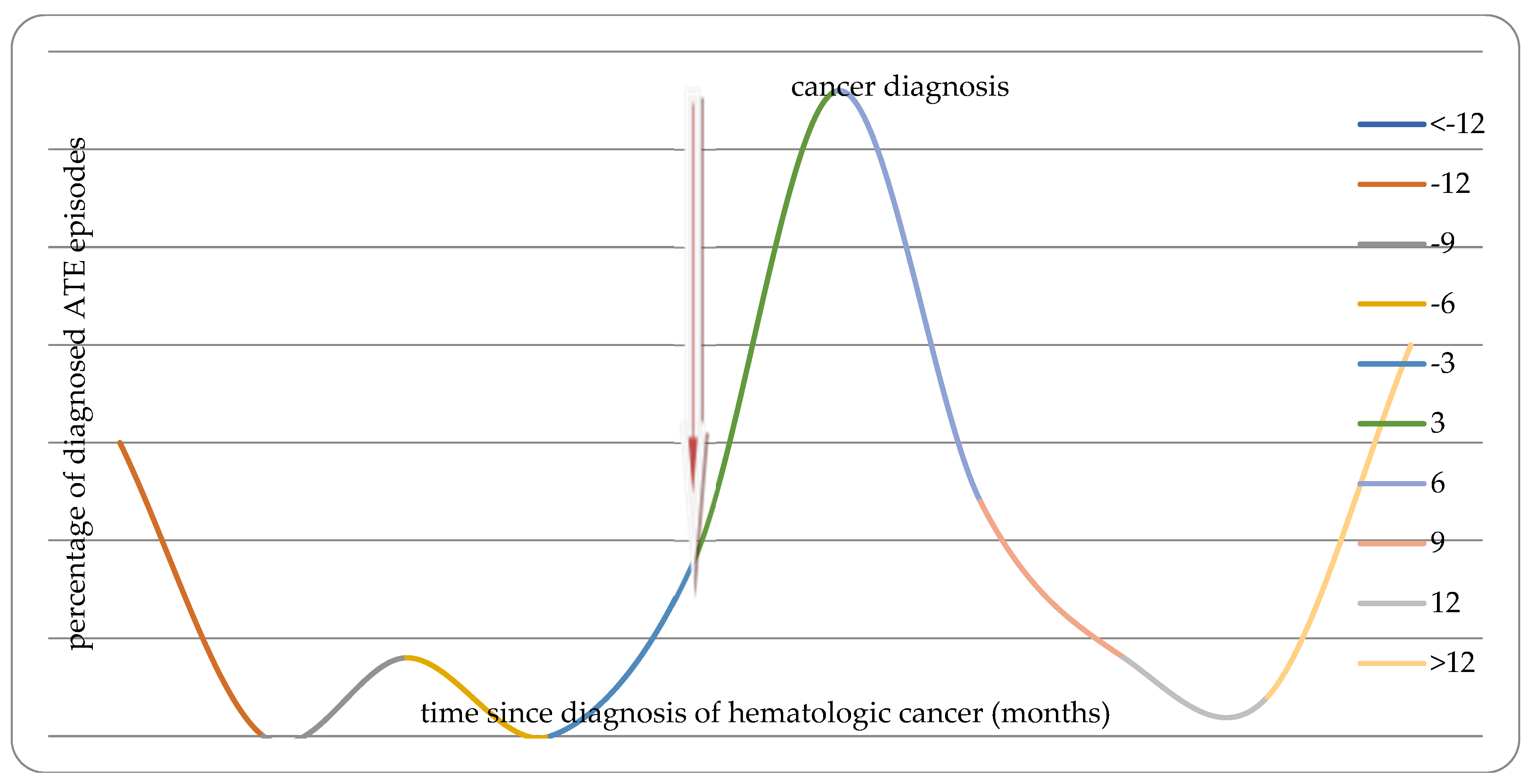
Figure 3.
Incidence of acute ATE before and after diagnosis of hematologic malignancy.
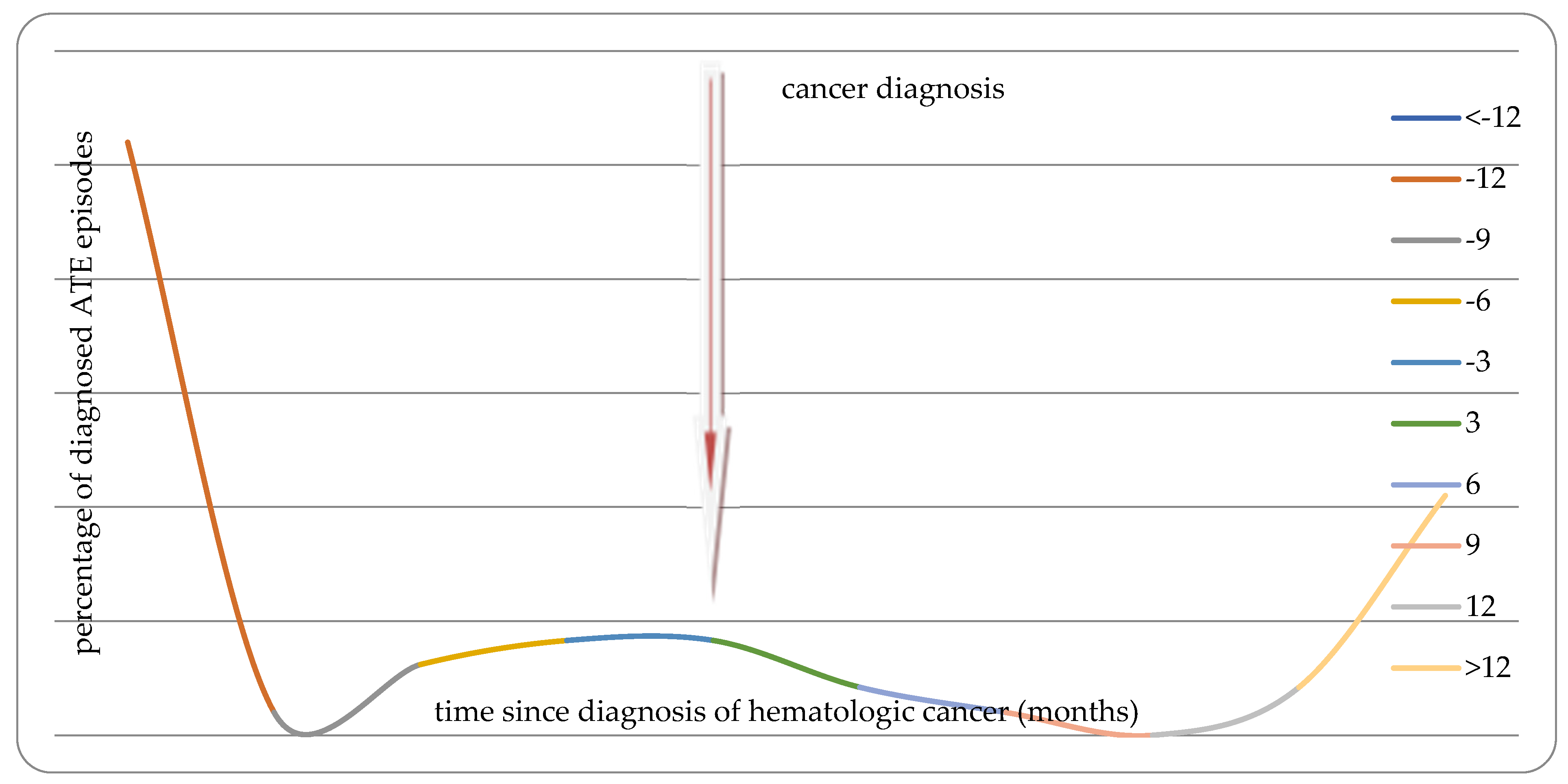

Table 1.
Demographic characteristics of the study group of 1283 patients with hematological malignancies who underwent cardio-oncology assessment between March 2021 and March 2023).
Table 1.
Demographic characteristics of the study group of 1283 patients with hematological malignancies who underwent cardio-oncology assessment between March 2021 and March 2023).
| Number | Percentage | ||
|---|---|---|---|
| Sex | men | 673 | 52.46 |
| Older age | ≥ 70 years | 390 | 30.4 |
| Hematological malignancies | AML - acute myeloid leukemia | 270 | 21.04 |
| NHL - non-Hodgkin's lymphoma | 250 | 19.49 | |
| MM - multiple myeloma | 223 | 17,38 | |
| CLL - chronic lymphocytic leukemia | 101 | 7.87 | |
| ALL - acute lymphocytic leukemia | 76 | 5.92 | |
| MDS - myelodysplastic syndrome | 70 | 5.46 | |
| HL - Hodgkin lymphoma | 56 | 4.36 | |
| CML - chronic myeloid leukemia | 51 | 3.98 | |
| Chronic myeloproliferative disease | 48 | 3.74 | |
| Other rarer (together) | 138 | ||
| Thromboembolism | All | 101 | 7.87 |
| VTE - venous thromboembolism | 54 | 4.21 | |
| ATE - arterial thromboembolism | 47 | 3.66 | |
| Coexisting diseases | Hypertension | 521 | 40.61 |
| Arrhythmia | 203 | 15.82 | |
| AF - atrial fibrillation | 105 | 8.18 | |
| HF - heart failure | 142 | 11.07 | |
| IHD - ischemic heart disease | 107 | 8.34 | |
| DM - diabetes melitus | 128 | 9.98 |
Table 2.
Analysis of association between thromboembolism occurrence and different diagnoses of hematological malignancies.
Table 2.
Analysis of association between thromboembolism occurrence and different diagnoses of hematological malignancies.
| VTE | ATE | |||
|---|---|---|---|---|
| frequency | p-value | frequency | p-value | |
| All | 54 of 1283 4.21% |
- | 47 of 1283 3.66% |
- |
| AML- acute myeloid leukemia | 17 of 270 6.30% |
0.055 | 8 of 270 2.96% |
0.491 |
| NHL- non-Hodgkin's lymphoma | 7 of 250 2.80% |
0.216 | 6 of 250 2.40% |
0.236 |
| MM- multiple myeloma | 10 of 223 4.48% |
0.822 | 11 of 223 4.93% |
0.267 |
| CLL- chronic lymphocytic leukemia | 3 of 101 2.97% |
0.698* | 6 of 101 5.94% |
0.204 |
| ALL- acute lymphocytic leukemia | 7 of 76 9.21% |
0.025 | 2 of 76 2.63% |
0.858* |
| MDS- myelodysplastic syndrome | 1 of 70 1.43% |
0.376* | 3 of 70 4.29% |
0.966* |
| HL- Hodgkin lymphoma | 0 of 56 0% |
0.206* | 1 of 56 1.79% |
0.688* |
| CML- chronic myeloid leukemia | 0 of 51 0% |
0.241* | 4 of 51 7.84% |
0.215* |
| Chronic myeloproliferative disease | 7 of 48 14.58% |
0.0003 | 4 of 48 8.33% |
0.173* |
*Yates corrected Chi-square.
Table 3.
Odds ratio for the occurrence of ATE in relation to cardiac history.
| All ATE | ATE before diagnosis of malignancy | ATE after diagnosis of malignancy | |
|---|---|---|---|
| Older age (≥70 y) | OR=3.55 (1.96-6.44) p=0.00003 |
OR=4.17 (2.03-8.57) p=0.0001 |
NS |
| Hypertension | OR=4.5 (2.31-8.76) p<0.00001 |
OR=5.67 (2.44-13.16) p=0.00005 |
NS |
| Arrhythmia | OR=2.61 (1.39-4.92) p=0.003 |
OR=3.17 (1.53-6.55) p=0.002 |
NS |
| Atrial Fibrillation | NS | NS | NS |
| Heart Failure | OR=3.28 (1.69-6.38) p=0.0004 |
OR=4.92 (2.37-10.24) p=0.00002 |
NS |
| Ischemic Heart Disease | OR=83.74 (37.63-186.32) p<0.00001 |
OR=108.94 (37.32-317.98) p<0.00001 |
OR=30.21 (9.29-98.2) p<0.00001 |
| Diabetes Mellitus | NS | NS | NS |
Legend: NS- non significant.
Table 4.
Odds ratio for VTE in time relation of diagnoses of hematological malignancies.
| All VTE | VTE before diagnosis of malignancy | VTE after diagnosis of malignancy | |
|---|---|---|---|
| AML- acute myeloid leukemia | NS | NS | NS |
| ALL- acute lymphocytic leukemia | OR=2.5 (1.09-5.75) p=0.03 |
NS | OR=3.05 (1.24-7.53) p=0.015 |
| Chronic myeloproliferative disease | OR=4.32 (1.84-10.13) p=0.0008 |
OR=6.79 (1.85-24.95) p=0.004 |
OR=3.12 (1.06-9.16) p=0.04 |
| Older age (≥70 y) | NS | NS | NS |
| Hypertension | NS | NS | NS |
| Arrhythmia | NS | NS | NS |
| Atrial Fibrillation | NS | NS | NS |
| Heart Failure | NS | NS | NS |
| Ischemic Heart Disease | NS | NS | NS |
| Diabetes Mellitus | OR=2.43 (1.22-4.85) p=0.01 |
NS | OR=2.42 (1.09-5.38) p=0.03 |
Legend: NS- non significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



