
Submitted:
21 October 2024
Posted:
23 October 2024
Read the latest preprint version here
Abstract
The application of three-dimensional (3D) printing/bioprinting technologies and cell therapies has garnered significant attention due to their potential in the field of regen-erative medicine. This paper aims to provide a comprehensive overview of 3D print-ing/bioprinting technology and cell therapies, highlighting their results in diverse medical applications, while also discussing the capabilities and limitations of their com-bined use. The synergistic combination of 3D printing and cellular therapies has been recognised as a promising and innovative approach, and it is expected that these tech-nologies will progressively assume a crucial role in the treatment of various diseases and conditions in the foreseeable future. This review concludes with a forward-looking perspective on the future impact of these technologies, highlighting their potential to revolutionize regenerative medicine through enhanced tissue repair and organ re-placement strategies.
Keywords:
3D printing
; additive manufacturing
; biomaterials
; biomedical applications
; bioprint-ing
; cellular therapies
; tissue regeneration
1. Introduction
Nowadays, regenerative medicine is considered an emerging field of research worldwide with the potential to revolutionise healthcare (improving patient outcomes and quality of life) in the 21st century [1]. This field is focused on the replacement, engineering and regeneration of human cells, tissues and organs. Its aim is to repair, restore, supplement or replace the normal function of a biological system following treatment with autologous, allogeneic stem and stromal cells [2,3,4].
In recent years, two promising approaches that have gained attention, namely three-dimensional (3D) printing and cellular therapies. 3D printing has revolutionized tissue engineering through the manufacture of complex, patient-specific, whilst providing precise control over the spatial distribution of cells and biomaterials. On the other hand, cellular therapies encompass the use of living cells to replace, repair, or regenerate injured tissues. The integration of 3D printing with cell therapies provides personalised, cell-laden constructs that mimic the complex architecture and function of native tissues. This approach stimulates cell-cell interactions, cell-matrix interactions and the creation of functional tissue-like constructs [5,6].
This review presented an overview of current advances in the combination of 3D printing/ bioprinting and cell therapies in the field of regenerative medicine. Firstly, the principles and applications of 3D printing/bioprinting and cell therapies were addressed individually. Subsequently, we explored recent advances in the integration of these technologies to create 3D-printed cellular structures. The limitations and challenges associated with these approaches were also mentioned, and the current state was analysed. Finally, we presented a future perspective on the potential impact of these technologies in the field of regenerative medicine and concluded with a summary of the main findings.
By providing a detailed understanding of the current state and future directions, this review seeks to contribute to the growing body of knowledge in this challenging and rapidly evolving field.
2. Three-Dimensional Printing
Three-dimensional (3D) printing (alternatively termed as additive manufacturing (AM) or biofabrication) is a burgeoning technique for rapid prototyping of structures in diverse fields, encompassing regenerative medicine [7,8,9,10,11]. In the past two decades, 3D printing has been widely researched due to its simplicity and its highly flexible manufacture provides unlimited possibilities for creating complex structures [12,13]. Several examples of 3D printed medical devices include: instrumentation, including guides to facilitate the correct surgical placement of devices; implants, such as hip joints; and external prostheses, such as bionic hands [14].
This advanced manufacturing technology, pioneered by Charles Hull in the early 1980s, enables the creation of customized and intricate structures with high precision and accuracy [15]. The technology operates by using computer-aided design (CAD) software to create a virtual model of the structure, which is subsequently converted into a physical object through the use of various 3D printing techniques [16]. The International Standard Organization (ISO) and the American Society for Testing and Materials (ASTM) [17] have established a classification system comprising seven overarching categories to categorize 3D printing methods based on part manufacturing approaches, as outlined in Figure 1. The subsequent sections provide a succinct overview of 3D printing processes.
2.1. Vat Photopolymerization
This method is characterized by principle of selectively solidifying a liquid photopolymer resin by exposing it to specific light sources or patterns. In the procedure, a vat contains the liquid resin, which is selectively cured layer by layer in the desired regions, gradually constructing the intended object. The laser, guided by predetermined digital coordinates, provides the necessary information to cure the resin at precise locations within each layer. To facilitate this curing process, a photoinitiator is introduced into the resin material. The photoinitiator absorbs the incident ultraviolet (UV) radiation and generates active species that initiate the photopolymerization reaction [18,19].
The vat photopolymerization technique includes various commonly utilized processes, such as stereolithography (SLA), continuous light interface production (CLIP), digital light processing (DLP) and two-photon polymerization (2PP) [20]. These methods involve SLA, which uses a laser or digital light projector to cure the resin layer by layer, whereas DLP employs a digital light projector to cure an entire layer at once. CLIP employs a continuous liquid interface production approach, where a continuous liquid interface is established between the resin and a transparent window, enabling continuous printing. Lastly, 2PP utilizes a focused laser beam and a photosensitive resin to achieve high-resolution printing via a nonlinear optical process [21]. These vat photopolymerization techniques offer versatile and AM capabilities for fabricating complex and detailed structures.
2.2. Material Extrusion
Materials extrusion is a widely adopted AM technique due to its fast manufacturing, cost efficiency, simplicity, user-friendly nature and the potential to produce complex components [22,23,24]. This technique involves extruding the material through an orifice and depositing it on a construction platform [25,26,27].
The most common technique is the fused filament fabrication (FFF), which is also reffered to as fused deposition modeling (FDM) [28]. In this method, the filament is heated to a temperature typically between 150–250°C until it melts, and the molten material is extruded through a nozzle [25]. The extruded material is then placed onto a build plate, which can be adjusted in the z direction. This technique usually uses more polymers, although it is also used to print metal and ceramic components. FDM uses a support to create overhang features, which can be removed either mechanically by detaching it from the printed part or chemically by dissolving it in a solvent [29].
2.3. Powder Bed Fusion
The powder bed fusion (PBF) technique uses a laser or an electron beam to melt and fuse the material into powder [30]. The principle used in this technique is to produce the product layer by layer and melt it. A heat source concentrates its heat on a powdered base material and heats the cross-sectional area [31].
PBD is mainly used due to the low cost of producing the object and the powder can be recycled to produce another piece from it [32]. This method encompasses several commonly utilized processes, including direct metal laser sintering (DMLS), selective laser sintering (SLS), electron beam melting (EBM), and selective laser melting (SLM). PBF utilizes a laser source (as DMLS, SLM and SLS) or an electron beam (EBM) to selectively melt or sinter layers of material, thereby fabricating a solid component. This technique is applicable to a range of powder-based materials, with metals and polymers being the most commonly processed [29].
2.4. Material Jetting
The material jetting (MJ) deposits the liquid in droplets to bind powder material [33]. In the MJ, the material is injected into the surface/building platform, where it so-lidifies, and the model is assembled layer by layer. The layers are subsequently cured or toughened with ultraviolet light. In this method, the material must be deposited in droplets, and therefore the materials used are limited. Generally, polymers and waxes are used, considering their viscous nature and ability to produce droplets [34]. This is a fast and proficient method and offers greater freedom when designing and printing complex models [24].
2.5. Binder Jetting
In the binder jetting (BJ), a liquid bonding compound is applied selectively to bind powder materials. A relevant feature of this technique today is the possibility of using color inkjet technology to create colored objects in the binders [35].
Binders are used to ensure adhesion between the powdered material particles. These binders contribute to obtaining the strength of the part and the desired form of the final product [31,36]. The materials commonly used in this method are metals (e.g., stainless steel), ceramics (e.g., glass) and polymers (e.g., acrylonitrile butadiene styrene, polyamide and polycarbonate) [32].
2.6. Directed Energy Deposition
The directed energy deposition (DEP) is an AM technique that utilizes focused thermal energy to melt materials, which are fused as they are deposited. In this method, an energy source - such as an electron beam, a laser and a plasma - is used to melt the materials which are then deposited [35].
The DED involves a nozzle assembled on a multi-hub arm that deposits the dissolved material at a surface layer where it solidifies A significant advantage of this method is its ability to precisely control the grain structure of the deposited material [32,37,38].
This process is analogous to material extrusion; however, the nozzle in DED has the capacity to transverse multiple directions rather than being being restricted to a single axis. While the process is applicable to polymers and ceramics, it is predominantly utilized for metals, which are provided in either powder or wire form [39].
2.7. Sheet Lamination
Sheet lamination involves the sequential bonding of thin sheets of material, normally fed through a set rollers [40]. This technique can employ various materials, including paper, polymer and metal [28]. Although this is a less precise method, it offers advantages in terms of speed and cost-effectiveness [40].
The predominant sheet lamination techniques are laminated object manufacturing (LOM) and ultrasonic additive manufacturing (UAM). LOM employs a layer-by-layer method similar to other additive manufacturing processes, utilizing paper as the primary material and adhesive for bonding, rather than welding. Conversely, UAM involves metals such as aluminum, stainless steel, and titanium, and operates at relatively low temperatures, enabling the production of complex internal geometries [41].
3. Bioprinting
Considering the incorporation of active substances such as biomaterials, living cells and active biomolecules, three-dimensional printing can be progressed to bioprinting, thus providing the manufactured structures with biological functions [12].
Bioprinting technology allows for the manufacture of complex, functional structures that promote cell growth and tissue formation. The prospect of manufacturing complete tissues or organs using 3D printing is very promising and has the potential to revolutionise regenerative medicine [42].
In the recent decades, significant advancements have been made in the field of 3D bioprinting (Figure 2) [43,44,45,46]. The evolution of this technology began with the invention of SLA by Charles Hull in 1984, which marked the beginning of 3D bioprinting [44]. Subsequently, in 2002, Landers et al. introduced extrusion-based bioprinting technology, which was later commercialized under the name “3D-Bioplotter” [47,48]. In 2003, Thomas and Boland's research team adapted a conventional inkjet printer to develop the first inkjet bioprinter capable of printing living cells [47,48]. Later, the engineering of scaffold-free vascular tissue via bioprinting was achieved by Norotte et al. [49]. The subsequent years witnessed the development and introduction of various bioprinted constructs, including an artificial liver in 2012, full human skin in 2014, a heart valve in 2016, and a lung-mimicking air sac with surrounding blood vessels in 2019, among other innovations [43,44,45,46].
3.1. Techniques
Among the diverse AM techniques, the most employed in bioprinting are laser-based printing (SLA and SLS), extrusion printing and inkjet printing [50,51,52].
SLA is a vat photopolymerization process and consists of photocurable bioinks that are subjected to UV, infrared or visible light to produce 3D pieces using the layer-by-layer procedure [53,54]. Among the advantages of SLA is its capacity to rapidly cure at physiological temperatures, which facilitates the production of constructs suitable for regenerative medicine applications. This technique has been widely employed to fabricate micro-needles designed for transdermal drug delivery, hearing aids, surgical guides for placing dental implants, temporary crowns and bridges, and supports for tissue engineering with/ without encapsulated cells [53,55].
During SLS printing, fine particles of the entire substance are fused by the heat of a high-powered laser to fabricate a 3D structure [56,57]. In this technique, several categories of powders, including polymers, ceramics ande metals, must be processed into powder. SLS is a PBF process and is used in numerous applications in the medical field, namely the fabrication of prototypes for medical devices, physical models used in surgery and scaffolds for tissue engineering. The popularity of SLS printers is attributed to their affordability, high productivity and material versatility [57,58].
Extrusion printing is considered the most popular bioprinting technology [59]. In this method, material is melted and extruded, through a nozzle, orifice or needle, using a screw, piston, or high-pressure pneumatic force, to form successive layers of the part [60,61,62,63,64]. This technique has been used extensively in the medical field, enabling the biofabrication of tissues, organs, implants and personalised drug delivery systems. Extrusion is also highly applicable in the field of disease modelling. Models made by extrusion can provide a baseline for the comprehension of the underlying biological mechanisms behind disease progression, thus contributing to the identification of effective treatments [65].
Inkjet bioprinting is considered as the pioneering technology in the field of bioprinting. The printing process utilizing this technique comprises two phases: first, the generation of discrete droplets that are precisely directed to specific locations on a substrate, and second, the subsequent interaction between these droplets and the substrate [44,66]. It is employed in various medical applications, including the creation of patient-specific or project-specific implants for static load-bearing purposes (such as dental crowns and prosthetic structures), joint applications (such as osteochondral cartilage implants), and for facilitating in vivo blood vessel formation and tissue regeneration. [67].
Table 1 presents the aforementioned techniques, as well as the advantages and drawbacks of each.
3.2. Materials Used in 3D Bioprinting
Nowadays, a diverse range of biomaterials are being used in 3D bioprinting [72]. The interaction between biomaterials and cells is fundamental for cell viability, proliferation, and differentiation. Hence, it is fundamental to consider the characteristics of biomaterials, such as non-toxicity, biocompatibility, and the absence of immune reactions and foreign body responses [73].
Bioprinting materials are categorized into two types: natural and synthetic biomaterials. Natural biomaterials are particularly attractive due to their bioactivity, being similar to the extracellular matrix (ECM) and biocompatible. The following are some examples of natural materials used in this field: collagen, xanthan gum (XG), silk fibroin (SF), gelatine, pectin, gellan gum, albumin, chitosan, sodium alginate, agarose, fibrin, keratin and hyaluronic acid (HA). However, these types of materials generally exhibit poor mechanical properties [74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95]. Conversely, synthetic materials provide disntinct advantages compared to natural materials, including the ability to be customized with specific physical properties and greater uniformity. The following are some examples of synthetic materials used in this field: poly (ℇ-caprolactone) (PCL), poly(lactic-co-glycolic) acid (PLGA), poly(l-lactic) acid (PLA), poly (glycolic acid) (PGA), polyurethane (PU), polyethylene glycol (PEG), polyether ether ketone (PEEK), polyvinylpyrrolidone (PVP) and pluronic. Nevertheless, synthetic materials for 3D bioprinting have some disadvantages, such as poor biocompatibility, the potential release of toxic degradation byproducts, and the absence of bioactive ligands [96,97,98,99,100,101,102,103,104,105,106,107,108,109].
To address the drawbacks, a more comprehensive knowledge of the physiological characteristics of the ECM and a higher ability to replicate the complex 3D structures mimetic of the ECM would represent a significant advance in 3D bioprinting. Advances in composite and hybrid bioprinting materials, as well as multimaterial bioprinting technologies, have emerged in the field of tissue regeneration [110,111]. Nonetheless, human tissues and organs operate within a highly dynamic biochemical environment, and conventional bioprinted materials often fail to adapt to the evolving spatial and temporal requirements of tissue and organ development. Consequently, there is increasing interest in developing sophisticated stimuli-responsive biomaterials for 3D bioprinting, which would facilitate the adaptation of artificial constructs to the intricate and dynamic physiological conditions [111,112,113].
4. Cellular Therapies
Cellular therapies, also known as cell therapy, cell transplantation, or cytotherapy involve the injection, grafting or implantation of cells into a patient autologous or allogeneic to achieve a medicinal effect [114,115]. Cell therapies are frequently applied in combination with biomaterial supports, which are designed to support and guide the cells both during and after transplantation [116].
Advances in 3D printing technology allow for the precise spatial arrangement of multiple cells and biomaterials, thereby enhancing the efficiency of cell delivery and integration onto scaffolds. There are two primary methods to delivering cells via 3D printed scaffolds: post-printing cell seeding and embedding cells within bioinks during the 3D bioprinting process [117,118,119,120]. The approach of seeding the cells after printing provides more flexible requirements for both the conditions and 3D printing process, though it is hindered by low cell adhesion rates on the scaffolds. To address this challenge, one approach involves encapsulating cells in hydrogels prior to combining them with 3D printed scaffolds. Alternatively, the bioprinting method enhances cell loading efficiency and allows for precise control over the spatial distribution of various cell types. However, this method demands stringent conditions and precise parameters during printing, as cells are sensitive to suboptimal environmental conditions. This necessitates requires detailed knowledge of the parameters of the bioinks and printing conditions beforehand [70,121,122,123,124].
The selection of a specific type of cell therapy is highly important, since it affects the function and design of the tissue engineering model [125,126]. There are three categories of cell therapies that can be applied to printed scaffolds, namely stem cell-based, non-stem cell-based and multicellular therapies [114].
4.1. Stem Cell-Based Therapies
Stem cells are among the most frequently utilized cell types due to their unspecialized nature, which allows them to self-renew and differentiate into various cell lineages. [11,125,127,128]. Their ability to differentiate into specific cell types while continuously dividing and self-renewing makes them interesting prospects for medicine regenerative. They have successfully been used to create functional tissues that replicate the properties of natural organs. These stem cells can be sourced from several origins [129]. In the field of bioengineering, the three most frequently employed types are mesenchymal stem/stromal cells (MSCs), embryonic stem cells (ESCs) and induced pluripotent stem cells (iPSCs) [130].
Also known as multipotent cells, MSCs can be sourced from various tissues, including bone marrow, muscle, lung, teeth, adipose tissue, liver, and perinatal/extra-embryonic tissues. They exhibit the capacity to proliferate and differentiate into a broad range of cell types, such as osteoblasts, chondrocytes and adipocytes [131]. Additionally, MSCs can differentiate into other mesenchymal and non-mesenchymal cells, including myocytes, tendocytes, neural cells, ligament cells, smooth muscle cells, endothelial cells, cardiomyocytes and hepatocytes [131,132]. In regenerative medicine, these cells offer numerous advantages, including ease of expansion in culture and the capacity to differentiate into desired cell lines. They also possess specific immunological properties, such as being immunoprivileged and immunomodulatory, and have tropisms for injury sites. Additionally, they can stimulate trophic responses and modulate tissue functions and inflammation through the secretion of essential bioactive molecules [133]. However, MSCs present some possible challenges, such as poor-quality control and inconsistency regarding heterogeneity, stability, differentiation, immunocompatibility, and migratory capacity [134,135] .
In turn, ESCs are pluripotent cells originating from the inner cell mass of blastocytes (an early embryo). They possess the capability to differentiate into nearly all cell types originating from the three germ layers, with the exception of trophoblastic cells [136]. However, ESCs raise ethical concerns, exhibit challenges in controlling differentiation, and have the potential to form teratomas and provoke immune responses [130,137,138,139,140].
Finally, iPSCs are pluripotent stem cells generated by reprogramming adult somatic cells through the introduction of specific genes and factors, thereby mimicking the pluripotent state of ESCs [141]. While iPSCs share many characteristics with ESCs, they do not carry the same ethical issues or immunogenicity concerns. Nonetheless, iPSCs, such as ESCs, are also associated with the risk of teratoma formation in vivo [130].
4.2. Non-Stem Cell-Based Therapies
Non-stem cell therapies commonly use somatic cells isolated that are isolated from humans, subsequently cultured and expanded in vitro, and then applied to patients for therapeutic, preventive, or diagnostic treatment [142]. These can be categorized into immune cells and non-immune cells. Immune cells, including natural killer cells, dendritic cells and macrophages can be engineered to target specific antigens. This approach is used in therapeutic strategies, including cancer, infections, autoimmune diseases, and allogeneic transplantation. On the other hand, non-immune cells, such as chondrocytes, fibroblasts, hepatocytes, keratinocytes, and pancreatic islet cells, normally are involved in the host’s defense response, as structural architectures, regulators and effectors of its protective immune reaction [114,142,143,144,145,146].
These somatic cell-based therapies serve as in vivo resource of cytokines, enzymes and growth factors. Additionally, they are frequently used in adoptive cell therapy for cancer treatment and as transplanted cells (e.g., hepatocytes or pancreatic islet cells) to address genetic metabolic disorders. They also find applications as cell-based or scaffold-free systems in the treatment of burns, ulcers, and cartilage injuries [114,143,147].
4.3. Multicellular Therapies
Multicellular therapies comprise at least two types of cultured stem and/or non-stem cells. This emerging approach considers that using a combination of cell types is more effective for promoting long-term tissue repair compared to single-cell therapy. This effectiveness is attributed to cell-cell interactions that extend beyond embryogenesis and play a crucial role in regenerative procedures [114,145,148].
5. Advancements in 3D Printed/ Bioprinting and Cellular Therapies for Regenerative Medicine
The advancements in combining 3D printing/bioprinting and cellular therapies holds considerable promise for advancing regenerative medicine. This synergy has the potential to enhance tissue engineering capabilities and introduce novel therapeutic approaches for a range of diseases and conditions. Such advancements could substantially improve patient outcomes and have the potential to significantly impact survival rates. [13,152,153].
This approach has been successful in printing the structures of different tissues, including cardiovascular, bone, liver, skin and neural tissues (Figure 3). The following sections analyze the advancements in the integration of 3D printing/bioprinting and cellular therapies in several regenerative medicine applications.
5.1. Cardiovascular Tissue Engineering
Cardiovascular diseases, which include pathologies affecting the myocardium, heart valves, and body’s vasculature, are highly prevalent worldwide. These diseases are a leading cause of morbidity and mortality, especially in developed countries [154,155,156,157]. Current therapeutic approaches include cellular therapies, bypass grafting, implantation of medical devices, cardiac tissue patches, and organ transplantation [154,158,159,160,161]. Organ transplantation is often not the optimal solution due to the imbalance between the availability of donor organs and the high demand. Additionally, the success of organ transplants is frequently compromised by complications related to immune rejection [155,162]. Among the various therapeutic approaches, cell therapy has demonstrated success in regenerating cardiovascular tissue. Nevertheless, the absence of ECM limits cell survival following injection, resulting in reduced long-term viability [162].
To address these concerns, 3D printing and bioprinting have emerged as effective approaches for developing scaffolds that incorporate ECM components and enhance cell viability [163]. These structures can more accurately the spatial and mechanical properties of native tissues, which is relevant for their functionality and integration in vivo [157]. Currently, scaffolds for cardiovascular tissue engineering have been fabricated using various 3D printing technologies, such as inkjet printing, SLA and extrusion-based techniques.
The scaffolds commonly incorporate biocompatible materials of natural origin, including fibrin, alginate, gelatin, collagen, HA, and fibrinogen [164]. However, to achieve complex structures with optimal physical, chemical, and mechanical properties, synthetic materials, including poly (glycerol sebacate) (PGS), PCL, and poly (ethylene glycol) methacrylate (PEGMA) are also employed. Additionally, some studies utilize a combination of natural and synthetic materials or semi-synthetic derivatives, such as gelatin methacrylate (GelMA) and hyaluronic acid-gelatin methacrylate (HAGM), to optimize scaffold properties while maintaining cell viability [13]. Furthermore, decellularized matrices are extensively utilized due to their provision of a porous, interconnected polymeric network that facilitates cell migration, proliferation, and the delivery of essential nutrients for cell survival [165] .
Maiullari et al. developed a technique for fabricating 3D cardiac tissue models that include a vascular network (Figure 4-A). They created multi-cellular constructs using human umbilical vein endothelial cells (hUVECs) and induced pluripotent stem cell-derived cardiomyocytes (iPSC-CMs), encapsulated in alginate and PEG-Fibrinogen (PF). These constructs were extruded through a custom-designed microfluidic printing head. Their research demonstrated that bioprinted endothelial cells are capable of forming functional vascular structures within the transplanted tissues and interacting with the host's existing vascular network [166].
To address myocardium damaged, Beijleri et al., produced a 3D-printed cardiac patch consisting of a decellularized cardiac extracellular matrix (cECM) hydrogel combined with GelMA. This patch was designed for the delivery of pediatric human cardiac progenitor cells (hCPC) (Figure 4-B). The GelMA-cECM bioinks ensure uniform distribution of cECM and hCPCs, with the hCPCs maintaining over 75% viability. Additionally, conditioned media from GelMA-cECM patches demonstrate more than a 2-fold increase in angiogenic potential. The patches also remain adhered to rat hearts and show vascularization over a 14-day period in vivo [167]. Also, in the development of tissue patches, Melhem et al. proposed a hydrogel patch embedded with multiple microchannels to enhance cell retention and factor delivery at the target tissue (Figure 4-C). They integrated bone marrow-derived MSCs (BMSCs) into a hydrogel by cross-linking a poly (ethylene glycol) dimethacrylate (PEGDMA) solution containing the cells. Microchannels with precise diameters were created within the cell-loaded hydrogel using an SLA unit for in situ cross-linking. This 3D-printed, microchanneled hydrogel, was designed as an advanced therapeutic tool for sustained delivery of multiple therapeutics, aiming to improve outcomes in ischemic heart injury [168].
Noor et al. established a technique to 3D print thick, vascularized cardiac patches tailored to a patient's specific properties. They used patient-derived cells, reprogrammed into cardiomyocytes and endothelial cells, and a personalized hydrogel made from the patient's extracellular matrix. These components were combined to create bioinks for printing cardiac tissue and blood vessels. The patches, optimized for oxygen transfer, demonstrated proper structure and function in vitro, and the approach was further validated by successfully printing cellularized human hearts presenting natural architecture (Figure 4-D) [169].
In turn, to mimic human microvasculature, Cui et al. developed a bioink combining human microvascular endothelial cells (hMVECs) and fibrin, used to fabricate micron-sized fibrin channels via drop-on-demand polymerization (Figure 4-E). This aqueous-based printing method reduces cellular damage. The hMVECs printed with fibrin aligned within the channels and proliferated to form continuous linings, resulting in a three-dimensional tubular structure. The study concludes that the concurrent printing of cells and scaffolds enhances the proliferation of hMVECs and supports the formation of microvascular networks [170].
Several researchers have employed 3D printing or bioprinting, with or without cell therapies, to advance cardiovascular tissue engineering. Table 2 provides a summary of these studies.
5.2. Bone Tissue Engineering
Severe bone defects resulting from aging, trauma, osteoporosis, degenerative diseases, autoimmune diseases (such as rheumatoid arthritis), or tumor removal are a leading cause of disability globally, affecting an estimated 1.71 billion people [182,183]. Current therapeutic strategies for addressing these defects include autografting, allografting, xenografting, and bone transplantation. Despite their application, these methods present significant risks, including the potential for infectious disease transmission and immune rejection [184,185]. To address the limitations of traditional bone defect treatments, 3D printing and bioprinting techniques, with or without cellular therapies, have been developed for bone tissue engineering. These methods enable the large-scale fabrication of custom-tailored bone tissues, meeting the growing demand for functionalized bone implants [186]. The 3D-printed scaffolds serve as a support for cell growth and differentiation, forming a hierarchical bone microvascular architecture [187]. For optimal performance, a scaffold should possess several critical attributes: biocompatibility, sterility, osteoconductivity, biodegradability, and a porous, interconnected structure that supports cellular infiltration and nutrient transport. Additionally, it should effectively repair bone defects while closely mimicking the characteristics of native bone tissue [188,189,190].
The most commonly employed printing techniques in bone tissue engineering are laser powder bed fusion, vat photopolymerization, and extrusion-based methods.
Various biomaterials are utilized for printing scaffolds: ceramics (e.g., beta-tricalcium phosphate (β-TCP), hydroxyapatite (HAp), and amorphous calcium phosphate (ACP)); natural polymers (e.g., matrigel, alginate, HA, and dextran emulsion); synthetic polymers (e.g., GelMA, PLGA, PCL, and polyethylene glycol diacrylate (PEGDA); metals (e.g., titanium alloy (Ti6Al4V), tantalum (Ta), and titanium (Ti)) and the combinations of these materials.
Lei et al. developed Ti6Al4V-based porous tantalum (Ta) scaffolds with high interfacial strength using laser powder bed fusion. In this process, porous Ta was directly deposited onto a solid Ti6Al4V substrate (Figure 5-A). In vitro biocompatibility assessments conducted with rat bone marrow mesenchymal stem cells (r-BMSCs) confirmed the scaffolds' biocompatibility. The findings demonstrated strong mechanical compatibility and osteointegration properties of the Ti6Al4V-based porous Ta scaffold, underscoring its considerable potential for orthopedic applications [191].
For mandibular bone defect reconstruction, Yu et al. encapsulated BMSCs in matrigel and infiltrated this mixture into porous Ti6Al4V scaffolds. The study demonstrated that rats with critical full-thickness mandibular defects treated with Matrigel-infused Ti6Al4V scaffolds exhibited significantly greater new bone formation compared to those treated with either local BMSC injections or Matrigel alone (Figure 5-B). These results indicate that Matrigel enhances the 3D microenvironment for BMSCs, positioning Matrigel-infused scaffolds as a promising method for improving bone regeneration in 3D-printed Ti6Al4V scaffolds [192].
Wu et al. produced a 3D-bioprintable scaffold combining alginate and β-TCP, for the treatment of bone defects (Figure 5-C). MG-63 cells were seeded onto these scaffolds. The 3D-printed scaffolds using a 10% alginate/β-TCP bioink exhibited enhanced physical characteristics and significantly improved cell viability and alkaline phosphatase activity. These findings suggest that the scaffolds have considerable potential for application in personalized bone regeneration therapies [193].
To produce a scaffold that replicates bone microstructure, Ressler et al. developed trabecular-like porous scaffolds using ceramic vat photopolymerization with HAp powders doped with magnesium (Mg2+), strontium (Sr2+) and zinc (Zn2+). Scaffolds sintered at 1100-1300°C exhibited mechanical properties similar to trabecular bone, with optimal performance at 1300 °C. The microstructure resembled cancellous bone, and the incorporation of trace elements resulted in a biphasic calcium phosphate system (HAp/β-TCP), potentially enhancing bioactivity.
Numerous studies have utilized 3D printing or bioprinting, either with or without cellular therapies, to advance bone tissue engineering. An overview of these studies is provided in Table 3.
5.3. Liver Tissue Engineering
The liver plays a vital role in blood protein synthesis, glucose metabolism, and the detoxification of metabolites [205]. It is also the only organ in the human body capable of efficient regeneration. However, this regenerative capacity can be compromised by excessive drug use or viral infections, which can cause irreversible damage to hepatocytes and lead to liver failure [206,207]. Chronic liver diseases, including fibrosis, cirrhosis, chronic viral hepatitis, and fatty liver disease, significantly contribute to global morbidity and mortality. Unfortunately, advancements in treatment options for these conditions remain limited [208,209].
The primary medical intervention for liver failure is partial or total liver transplantation. Nevertheless, this approach faces challenges, including limited donor availability, immune rejection, and variable graft success rates. Alternative approaches in tissue engineering encompass bioartificial liver systems, which involve the in vitro creation of liver tissue to repair or replace damaged liver segments, as well as hepatocyte transplantation and cellular therapy methods [206]. There has been a continuous search for a reliable and reproducible source of hepatocytes, whether for liver regeneration therapy, seeding liver support devices, or in vitro screening applications [207].
Numerous studies have investigated 3D bioprinting of liver tissue utilizing either stem cells or immortalized hepatic cell lines [210,211]. Stem cells are particularly promising due to their ability to express hepatocyte-like phenotypes. In contrast, adult hepatocytes are scarce, challenging to isolate, exhibit poor propagation, and experience rapid functional deterioration in vitro [212].
In liver tissue engineering, a variety of biomaterials are employed, categorized intonatural and synthetic polymers [213]. Natural polymers, such as alginate, HA, collagen, cellulose nanocrystal (CNC), and gelatin, present the advantages of enhanced cell compatibility and ease of manipulation. Nevertheless, they are constrained by relatively weaker mechanical properties, limited availability, and variable degradation rates. Consequently, synthetic polymers, such as PCL, have been developed to provide superior mechanical strength, flexibility, processability, and adjustable degradability. Despite these advantages, synthetic polymers generally lack cell recognition and adhesion sites, resulting in reduced biocompatibility compared to natural polymers [214]. To mitigate these issues, a strategy of combining natural and synthetic polymers is employed to create effective bioinks for 3D bioprinting. Additionally, liver decellularized extracellular matrix (dECM), sourced from animals, is frequently used to establish microenvironments for liver cells, offering cross-species tolerance and minimizing the risk of immune rejection [215,216,217].
Yang et al. developed a liver tissue model through 3D bioprinting using HepaRG cells, a widely utilized hepatic progenitor cell line. This 3D bioprinted model, termed hepatorganoids, exhibited essential liver functions, including albumin production, drug metabolism, and glycogen accumulation, after a 7-day differentiation period (Figure 6-A). In vivo studies showed that the 3D bioprinted hepatorganoids further matured, exhibiting enhanced synthesis of liver-specific proteins and more human-like drug metabolism. Notably, transplantation of 3D bioprinted hepatorganoids significantly increased survival rates in recipient mice. These finfings suggest that 3D bioprinted hepatorganoids can effectively undergo hepatic differentiation and ameliorate liver failure in vivo [218].
In the study conducted by Xie et al a 3D bioprinted model of hepatocellular carcinoma, derived from patient cells, was created using isolated primary hepatocellular carcinoma cells mixed with gelatin and sodium alginate to form a bioink (Figure 6-B). The resulting models were successfully generated and exhibited substantial growth over prolonged culture durations. They preserved key characteristics of the original hepatocellular carcinoma tumors, including consistent biomarker expression, stable genetic alterations, and expression profiles. Thus, 3D bioprinted hepatocellular carcinoma models prove to be reliable in vitro systems, suitable for long-term culture, and capable of predicting patient-specific drug responses for tailored therapeutic approaches [219].
Lewis et al. studied a technique for 3D printing gelatin into precisely defined geometries, which exhibit distinct biological effects on seeded hepatocytes (Figure 6-C). Their research reveals that the structural configuration of gelatin can markedly impact biological processes. An undifferentiated hepatocyte cell line demonstrated high viability and proliferation on 3D-printed scaffolds with two distinct geometries. Notably, hepatocyte-specific functions—such as albumin secretion, cytochrome P450 activity, and bile transport—were enhanced in more interconnected 3D-printed gelatin structures compared to those with less interconnectivity and traditional two-dimensional (2D) cultures. This study underscores the gap between gene expression and protein functionality in simplistic 2D cultures, highlighting the importance of a physiologically relevant 3D environment for optimizing hepatocyte expression and functionality [220].
Jeon et al. employed 3D bioprinting technology to reconstruct liver tissues and organs using human hepatocellular carcinoma (HepG2) cells, a liver cancer-derived cell line. They created multi-layered 3D structures by integrating alginate with HepG2 cells (Figure 6-D). The study demonstrated that replicating the 3D hepatic architecture using this technology enhances the stability and gene expression profiles of HepG2 cells. Cells cultured on these 3D alginate scaffolds for three weeks were analyzed via fluorescence microscopy, histology, and immunohistochemistry. Results indicated that HepG2 cells exhibited improved growth and liver-specific gene expression in 3D cultures compared to 2D cultures, highlighting the effectiveness of 3D bioprinting in mimicking liver architecture and enhancing cellular function [221].
Using the same 3D bioprinting technique, Wu et al, produced a novel bioink containing alginate, CNC and GelMA (namely 135ACG hybrid ink), aimed at fabricating both cell-laden and acellular structures (Figure 6-E). The bioink presented good shear-thinning behavior and solid-like characteristics, ensuring high printability and minimal cell damage. Following crosslinking, it formed a rigid ECM conducive to stromal cell growth. The team engineered a GelMA bioink with suitable mechanical properties to mimic human liver tissue, enabling the printing of liver lobule-mimetic constructs with precise cell placement (fibroblasts and hepG2) in different ECMs (135ACG and GelMA). These constructs were used to study the impact of mechanical stimuli and cellular interactions on cell behavior. These findings demonstrated that fibroblasts proliferated effectively within the rigid 135ACG matrix, whereas HepG2 cells developed into spheroid structures in the more compliant GelMA matrix. Co-cultures of hepG2 and fibroblasts cells showed increased albumin production, highlighting the role of soluble factors in enhancing hepatic function. The study demonstrated that the developed bioinks and printing methods are effective for creating complex, multi-cellular constructs with varied ECMs, advancing both fundamental research and tissue engineering applications [222].
Several studies have employed 3D printing/bioprinting with or without the incorporation of cellular therapies, to advance liver tissue engineering. A summary of these studies is presented in Table 4.
5.4. Skin Tissue Engineering
The skin, regarded as the largest organ in the human body, plays essential roles including serving as a protective barrier, regulating body temperature, and preventing dehydration [232]. Extensive full-thickness skin wounds, which damage underlying blood vessels, pose serious risks due to induced cellular hypoxia and nutrient deprivation [233]. While autografts are considered the "gold standard" for treating severe skin injuries, their use is limited by issues such as donor site availability and associated morbidity [234]. Furthermore, existing commercial skin substitutes lack sufficient vascular networks necessary for effective nutrient delivery in full-thickness wounds. Consequently, skin substitutes are seen as promising alternatives, offering the potential for vascularized skin reconstruction with customized cell compositions and controlled geometrical structures [233,235].
3D printing/ bioprinting have arisen as an innovative technological approach, in skin tissue engineering, for engineering structures by depositing cell-embedded bioinks layer by layer [236,237]. This approach includes several techniques, including, DLP, extrusion bioprinting, inkjet printing and electrospinning. The materials commonly used in this field are natural polymers (e.g., collagen, alginate, HA, gelatin, and fibroin) and synthetic polymers (e.g., PCL, PLGA, polyglycolic acid, polyurethanes, polycarbonates, and PEGDA). These materials, often referred to as biopolymers, are biocompatible and biodegradable. In applications related to wound healing, bioinks can be integrated with antibiotic agents or antimicrobial peptides, as well as growth factors such as epidermal growth factor (EGF), fibroblast growth factor (FGF), or vascular endothelial growth factor (VEGF), to enhance cell stimulation, growth, proliferation, and migration throughout the healing process [236,238]. Latest developments in wound care and skin regeneration involve embedding various cell types, including fibroblasts, hUVECs, keratinocytes, and human umbilical cord mesenchymal stem cells (hUCMSCs), directly into bioinks. Liu et al. fabricated vascularized full-thickness skin substitute by printing an alginate-gelatin hydrogel to simulate the epidermis, and a phosphosilicate calcium bioglass (PSC)-alginate-GelMA hydrogel containing hUVECs and hUCMSCs to replicate the dermis (Figure 7-A). They showed a marked enhancement in blood vessel formation and collagen deposition, demonstrating the effectiveness of these skin substitutes in reconstructing full-thickness skin injuries in rat models [233]. Also, with a view to developing a full-thickness skin substitute, Admane et al. employed extrusion-based 3D bioprinting to create a silk fibroin-gelatin construct containing fibroblasts to mimic the dermis, and a silk fibroin-gelatin layer with keratinocytes to replicate the epidermis (Figure 7-B). The 3D bioprinted full-thickness skin model showed extensive keratinocyte migration and differentiation, mimicking reepithelialization. Analysis revealed similarities to native human skin, involving pathways related to skin development, extracellular matrix organization, and keratinization [239]. Also, Jin et al. developed an advanced 3D bioprinted structure designed to mimic natural full-thickness skin, incorporating the epidermis, dermis, and a vascular network. This model utilized GelMA with HaCaTs for the epidermal layer, an acellular dermal matrix (ADM) with fibroblasts for the dermis, and a GelMA mesh with hUVECs for the vascular network (Figure 7-C). They demonstrated that this functional skin model not only enhanced cell viability and proliferation but also supported epidermal reconstruction in vitro. In vivo, the functional skin model-maintained cell viability for at least one week and promoted wound healing, re-epithelization, dermal ECM secretion, and angiogenesis, thereby improving wound healing quality [240].
Song et al. developed a bilayer skin scaffold incorporating drug delivery for the repair of full-thickness skin defects. The scaffold features an outer layer of amoxicillin (AMX)-loaded PCL nanofibers, fabricated through electrospinning, which functions as an antibacterial membrane mimicking the epidermis (Figure 7-D). The inner layer, designed to replicate the dermis, is a hydrogel composed of sodium alginate and gelatin, infused with recombinant human epidermal growth factor (rhEGF) to maintain wound moisture and promote healing. The successful incorporation of AMX and rhEGF into the scaffold was demonstrated, with the scaffold exhibiting excellent physicochemical properties, effective drug release, and antibacterial activity. Both in vitro and in vivo evaluations revealed enhanced cell adhesion, proliferation, and accelerated skin wound healing, alongside favorable biocompatibility. These results suggest that the scaffold holds considerable potential for skin regeneration applications [241].
Numerous studies have utilized 3D printing and bioprinting techniques, both with and without the integration of cellular therapies, to advance skin tissue engineering. A comprehensive overview of these studies is provided in Table 5.
5.5. Neural Tissue Engineering
The nervous system represents one of the most intricate and complex biological systems formed during development [253]. The human nervous system is divided into two primary components: the central nervous system, consisting of the brain and spinal cord, and the peripheral nervous system, which includes cranial and spinal nerves along with associated ganglia [254]. Traumatic injuries, including traumatic brain injury and spinal cord injury, as well as neurodegenerative diseases such as Alzheimer's, Parkinson's, Huntington’s and multiple sclerosis, pose major public health challenges, with limited treatment options that mainly offer symptomatic relief. Autologous nerve graft transplantation is widely regarded as the optimal approach for addressing severe nerve injuries. Nonetheless, its clinical utility is constrained by several substantial issues, such as the restricted availability of suitable donor nerves and the risk of incompatibilities between the donor and recipient nerves [255,256,257]. Despite ongoing clinical advancements, fully effective therapies for neural regeneration are still in early stages, driving interest in neural tissue engineering [258]. Neural tissue engineering focuses on developing biological substitutes that integrate biomimetic 3D scaffolds with cells to improve neural tissue functionality. Advances in 3D printing technology have significantly impacted neural autograft engineering, enabling precise fabrication of tissue-engineered neural implants. Various 3D printing methods, such as extrusion-based printing, laser-assisted bioprinting, SLA and 4D printing, are increasingly employed to create accurately structured implants for nerve injury repair and to develop models and devices for in vitro neural tissue engineering.
The materials chosen for printing of neural structures encompass biocompatible polymers (e.g. PCL and PU), composites (e.g. reduced graphene oxide (rGO)), and hydrogels (e.g. GelMa, HA, collagen and fibrin). These materials must meet specific requirements for printability and biocompatibility, as well as possess suitable physicochemical properties and mechanical strength [257].
Researchers have combined 3D printing/bioprinting with cellular therapies for neural tissue engineering. Lee et al. created a photocrosslinkable methacrylated silk fibroin-pectin bioinks (Figure 8-A) and they exhibited tunable mechanical properties, favorable biocompatibility, and an environment highly supportive of neural induction in 3D bioprinted constructs containing neural stem/progenitor cell spheroids [259].
For spinal cord injury treatment, Song et al. engineered scaffolds composed of PCL microfiber-reinforced spinal cord ECM hydrogels incorporating oxymatrine (OMT), using electrospinning techniques (Figure 8-B). These scaffolds promoted neuronal differentiation of neural stem cells (NSCs) and suppressed astrocyte proliferation in vitro. In vivo, they promoted the recruitment of NSCs, stimulated neuronal growth, diminished glial scar formation, and enhanced motor function recovery in rats with spinal cord injuries [260].
In turn, Lin et al. developed a model designed to forecast cell growth and distribution, aimed at reducing the need for empirical adjustments. They established a multiphysics model that integrates oxygen diffusion and substrate consumption dynamics within a rat adrenal medullary pheochromocytoma (pc-12) cell-laden nerve scaffold (Figure 8-C). This model was used to simulate and forecast oxygen levels and cellular growth patterns. The scaffold was produced using SLA, and the distribution of cells was assessed through fluorescence staining to confirm the model. The findings demonstrated that the model effectively forecast cellular growth patterns [261].
Numerous studies have utilized 3D printing and bioprinting technologies, both with and without the integration of cellular therapies, to develop the area of neural tissue engineering. Table 6 provides a comprehensive overview of these investigations.
6. Limitations and Challenges
Despite the benefits of 3D printing/bioprinting and cellular therapies for regenerative medicine, there are several challenges that need to be addressed. Despite extensive research efforts in recent years, the clinical application of these technologies has been constrained. The lack of sufficient animal studies and the absence of viable 3D models in clinical trials underscore the need for further focus and development in these critical areas [272,273,274].
One of the current challenges is the advancement of functional vascular networks within bioprinted tissues and organs. Specifically, creating a vascular system that can seamlessly connect with the host's native blood vessels is complicated by the complex structural architecture and the variability of tissue componentes [275,276,277]. Vascularization is crucial for providing nutrients and oxygen, which are vital for maintaining cell viability and ensuring tissue functionality. A robust, multi-level vascular network is necessary to support the long-term survival and growth of bioprinted organs, incorporating smooth muscle cells and hUVECs into the blood vessels [278]. To overcome challenges related to nutrient and oxygen transport, researchers have utilized proangiogenic factors such as vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (BFGF) to promote the development of microvessels. Additionally, incorporating endothelial cells into the culture medium has been shown to promote micro vessel formation and the development of angiogenic sprouts in engineered constructs [279]. However, endothelial cells and angiogenic factors generally do not produce perfusable constructs in a fast way [280]. Bioreactors offer a solution by continuously supplying media to porous constructs, reducing the reliance on arterial scaffolds and large tissue samples. Despite this, these constructs often lack micro vessels and are stored outside of bioreactors, which can compromise cell survival. Microfluidic systems represent a potential alternative for vascular network fabrication, though scaling these systems to larger physiological sizes remains a significant challenge [275].
The selection and sourcing of cells is another challenge in regenerative medicine. Cells used in bioinks must possess some key characteristic: high proliferative capacity, printability, functionality, safety, and economic viability [278]. The choice of cells encapsulated in bioinks critically influences their differentiation potential and ability to develop into various lineages. Although live cells, such as stem cells, are very promising, their practical application is limited by issues related to availability and ethical concerns. Researchers have reported successful integration of stem cells with bioprinting technologies [272]. An additional challenge is the mass production of cells, which needs substantial quantities of cells and increases the demand on in vitro expansion cultures. Addressing the cost-effectiveness of large-scale cell production is a crucial challenge [278]. Extended processing times and mechanical forces experienced during 3D printing can adversely affect cell viability by altering cell geometry and disrupting signaling pathways [281]. To address these issues, it is essential to enhance existing bioprinting techniques to minimize processing duration and to develop specialized buffers that can protect cells throughout the printing process.
In 3D bioprinting, choosing the most appropriate biomaterials is critical for the effective fabrication of tissues with clinical relevance [281,282]. Biomaterials are essential for providing structural support, maintaining cellular viability, and ensuring long-term tissue integration. While numerous polymers traditionally utilized in 3D printing and tissue engineering have been explored for bioprinting due to their availability and previous applications, they may not always provide the optimal biological compatibility required for successful bioprinting outcomes [283]. These materials might display excessive biological reactivity, which can result in undesirable cellular interactions and premature or inappropriate differentiation of stem cells. For a bioink to be suitable for clinical applications, it must have specific characteristics, such as structural stability, the ability to support cell proliferation, and a degradation rate that matches the needs of tissue regeneration. Additionally, bioinks must be compatible with bioprinting technologies to facilitate rapid prototyping [13]. A major challenge is ensuring that printed structures are biocompatible and provide an appropriate environment for cell growth. Current research is focused on developing novel biopolymers and hydrogels that more accurately replicate the nanoscale features and responsive characteristics of the ECM and native tissue microenvironment [284]. However, these advanced materials often encounter compatibility issues with traditional bioprinting techniques. Many of these materials may lack the necessary structural integrity, leading to collapse if they are too soft [285]. One potential solution is to combine various materials to harness their individual strengths, such as merging the mechanical properties of more rigid materials with the cell-supportive and biocompatible features of softer ones [130,286].
Furthermore, the development and implementation of 3D printing and cell therapies in regenerative medicine pose significant financial challenges, which could prevent the widespread adoption of these technologies. The costs associated with research, development, and clinical trials are substantial, and securing funding for these endeavors can be difficult. Moreover, the cost-efficiency of these technologies needs careful consideration, particularly in relation to the high expenses of 3D printers, cellular materials, and associated computer software [287]. Generally, the costs of maintaining and scaling bioprinting technologies limit the rapid integration of 3D printing capabilities into clinical settings [284]. Another challenge is the size of bioprinted tissues. Currently, bioprinted constructs are typically small and consist of a limited number of cell types, which restricts their functionality and scalability [284,287,288,289]. Moreover, 3D printers are often constrained by their build volume, which limits the maximum size of bioprinted tissues and complicates the creation of entire 3D-printed organs [284].
Lastly, the application of 3D printing/bioprinting and cellular therapies in regenerative medicine is subject to regulatory approval processes. Despite their complexity and time demands, valuable guidelines for these processes can be obtained from regulatory agencies such as the Food and Drug Administration (FDA) in the United States and the European Medicines Agency (EMA) in the European Union, especially with regard to 3D-printed medical devices. For tissue bioprinting to achieve clinical translation, it is essential to establish a clear and defined regulatory pathway [290]. Additionally, ethical challenges and concerns related to biosafety and liability arise when fabricating internal tissues and organs. The clinical translation of bioprinting techniques will depend on regulatory bodies' thorough evaluation of safety, efficacy, and risk. Globally, regulatory authorities face challenges in addressing the potential and uncertain risks associated with 3D bioprinting, such as immune responses to bioinks or materials [284]. In the absence of specific regulations, the FDA is currently relying on the Center for Biologics Evaluation and Research (CBER) guidelines for 3D bioprinting products. These products require FDA approval, and adherence to regulatory guidelines is mandatory from the initial stages of product development. As the field advances, more 3D bioprinting products are likely to emerge, highlighting the need for more specific regulatory guidelines. Currently, only South Korea’s Ministry of Food and Drug Safety (MFDS) and Japan’s Pharmaceuticals and Medical Devices Agency (PMDA) have developed specific guidelines for 3D bioprinting. Thus, the global development of comprehensive regulations for 3D bioprinting techniques, bioinks, and printers is of increasing importance [13].
These limitations and challenges highlight the complexity of integrating 3D printing with cellular therapies in regenerative medicine, emphasizing the need for continuous research and development in this field. Overcoming these obstacles requires transdisciplinary collaboration among cell biologists, engineers, physiologists and pharmaceutical industry partners, to advance and expand the potential of this technology [291]. Despite existing challenges, advancements persist, and it is anticipated that these technologies will increasingly impact the treatment of various diseases and conditions in the future. Ongoing research is progressively making the goal of creating safe and fully functional bioprinted tissues more achievable [278].
7. Current State and Future Outlook
The current state of clinical trials combining 3D printing/bioprinting and cellular therapies is promising, though still in its early stages. Numerous research groups are actively developing and testing new treatments utilizing these technologies, and several clinical trials have been initiated in recent years to assess their safety and efficacy.
Tissue engineering currently has broad applications, including the development of various tissues, cardiac, vascular, bone, skin, neural, cartilage, retinal tissues, among others. Conventionally, this method entails seeding cells onto a porous scaffold to promote their growth and, subsequently, promote tissue development. [292]. The approach presents several advantages, including providing strong structural support with suitable degradation timing, regulating the cellular environment, and allowing for effective nutrient and waste exchange between the scaffold and cells [293,294].
Bioprinting has opened up a whole new era in tissue regeneration allowing the production of patient-specific autologous organs and tissues [18,295,296,297,298]. This rapid prototyping technique the fabrication of intricate tissue and organ structures by precisely depositing living cells and biomaterials layer by layer, based on a CAD model. Using this approach, 3D constructs can be produced with high accuracy in terms of positioning and architecture, including shape, pore geometry, and interconnectivity. This allows for the development of tissue and organ models that closely resemble the human body with high reproducibility [299,300,301]. By simultaneously printing multiple cell types and biomaterials, bioprinting can replicate the structural and biochemical complexity of living tissues, creating a heterogeneous microenvironment at specified locations [214,302,303].
Although in vitro models have advanced significantly for developing new therapies, their application in surgical settings is still not fully realized. However, significant progress is being made in hydrogel design and the development of advanced technological tools. These advancements are bringing us closer to meeting the fidelity and safety standards required for bioprinted constructs to be consistently and personalized used in patients in the near future [304].
The future of tissue biomaterials is expected to replicate not only the structural design and characteristics of organs and tissues but also their dynamic, functional behaviors [159,160]. The concept of time as the fourth dimension (4D) has gained prominence, in the context of bioprinting, introducing two key aspects: materials capable of deformation and structures that mature after printing [305,306]. This new approach to bioprinting addresses the complexity of the system, which is very important for fully understanding the behaviour of functional living materials during the post-processing stage [304].
8. Conclusion
The combination of 3D printing/bioprinting technologies with cellular therapies represents a significant advancement in regenerative medicine. Advances in this area are leading to the development of new functional tissues that closely resemble native tissues. This review has detailed the fundamental principles and applications of each technology individually and has elucidated how their convergence is pushing the boundaries of tissue engineering
This study underlines that the latest developments have markedly enhanced the capacity to produce complex 3D cellular structures presenting high precision. Innovations in bioprinting techniques, coupled with improvements in biomaterials and cellular engineering, have enabled more sophisticated control over tissue architecture and cellular organization. These advancements facilitate the creation of more accurate and functional tissue models, which hold promise for personalized regenerative therapies.
Nevertheless, there are still several critical barriers that need to be addressed, such as the development of functional vascular networks, regulatory and ethical issues, and the advancement of suitable biomaterials.
The potential impact of these integrated technologies in regenerative medicine is expected to be high in the future. As the field progresses, solving these issues will be essential to realizing the full potential of 3D printing/bioprinting and cell therapies. Ongoing research and innovation in these areas is therefore expected to produce transformative advances in personalized medicine and tissue regeneration, ultimately improving outcomes for patients and advancing therapeutic options.
Author Contributions
Conceptualization, Ana Catarina Sousa, José Domingos Santos, Luís Atayde, Nuno Alves and Ana Colette Maurício; methodology, Ana Catarina Sousa, Rui Alvites, Bruna Lopes, Patrícia Sousa, Alícia Moreira and André Coelho; investigation, Ana Catarina Sousa; writing—original draft preparation, Ana Catarina Sousa; writing—review and editing, Nuno Alves, Rui Alvites, Ana Colette Maurício, José Domingos Santos and Luís Atayde; visualization, Ana Catarina Sousa; supervision, José Domingos Santos, Luís Atayde, Nuno Alves, and Ana Colette Maurício; project administration, Ana Colette Maurício; funding acquisition, Nuno Alves, and Ana Colette Maurício. All authors have read and agreed to the published version of the manuscript.
Funding
Ana Catarina Sousa (SFRH/BD/146689/2019), Bruna Lopes (2021.05265.BD), Patrícia Sousa (2023.00246.BD), André Coelho (2023.00428.BD), Alícia Moreira (2023.00544.BD) and acknowledge Fundação para a Ciência e Tecnologia (FCT), for financial support. Rui Alvites acknowledges the CECA, UP, and FCT for the funding and accessibility of all technical, structural, and human resources necessary for the development of this work. The work was supported through the project UIDB/00211/2020 funded by FCT/MCTES, national funds. This research was funded by Projects PEst-OE/AGR/UI0211/2011 from FCT, and COM-PETE 2020, from ANI–Projetos ID&T Empresas em Copromoção, by the project “InnovaBIOMAS - Optimized Additive Biofabrication System for the Production of Hierarchical Multi-Tissue Scaffolds Applied in the Treatment of Joint Diseases” with the reference 2022.10564.PTDC, by the project “Bone2Move- Development of “in vivo” experimental techniques and modelling methodologies for the evaluation of 4D scaffolds for bone defect in sheep model: an integrative research approach” with the reference POCI-01-0145-FEDER-031146.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author on request.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| 2D | Two-dimensional |
| 132ACG | Bioink with alginate (1%), cellulose nanocrystal (3%), and gelatin methacryloyl (5%) |
| 2PP | Two-photon polymerization |
| 3D | Three-dimensional |
| 3DP-HOs | Three-dimensional bioprinted hepatorganoids |
| 4D | Four-dimensional |
| ACP | Amorphous calcium phosphate |
| AD | Additive manufacturing |
| ADM | Acellular dermal matrix |
| aHSC | Primary fetal activated hepatic stellate cells |
| ALP | Alkaline phosphatase |
| AMX | Amoxicillin |
| ASTM | American Society for Testing and Materials |
| BFGF | Basic fibroblast growth factor |
| BJ | Binder jetting |
| BL | Bi-layer |
| BMP-2 | Bone morphogenetic protein 2 |
| BMSCs | bone marrow-derived mesenchymal stem/stromal cells |
| C17.2 | Murine neural stem cells |
| Ca | Calcium |
| CAD | Computer-aided design |
| CBER | Center for Biologics Evaluation and Research |
| cECM | decellularized cardiac extracellular |
| CFs | Human cardiac fibroblasts |
| CLIP | Continuous light interface production |
| CNC | Cellulose nanocrystal |
| CSMA | Chondroitin sulfate methacrylate |
| dECM | Decellularized extracellular matrix |
| DEP | Directed energy deposition |
| Dex | Dextran |
| DFs | Dermal fibroblasts |
| DLP | Digital light processing |
| DMLS | Direct metal laser sintering |
| DO | Diamond |
| DPSCs | Dental Pulp stem/stromal cells |
| EBM | Electron beam melting |
| ECM | Extracellular matrix |
| EMA | European medicines agency |
| EPCs | Endothelial progenitor cells |
| ESCs | Embryonic stem cells |
| ESCs | Epidermal stem cells |
| EVCs | Early vascular cells |
| FDA | Food and Drug Administration |
| FDM | Fused deposition modeling |
| Fe | Iron |
| FFF | Fused filament fabrication |
| GAM | Matrix hydrogel with 2.8% of gellan gum, 1.6% of alginate, and 2.8% of methyl cellulose |
| Gel | Gelatin |
| GelMA | Gelatin methacrylate |
| H9c2 | Cardiomyocytes |
| HA | Hyaluronic acid |
| HAGM | Hyaluronic acid-gelatin methacrylate |
| HAp | Hydroxyapatite |
| Hap/β-TCP | Biphasic calcium phosphate system |
| hCAECs | Human coronary artery endothelial cells |
| HCC | Hepatocellular carcinoma |
| hCMPCs | Human cardiac-derived cardiomyocyte progenitor cells |
| hCPCs | Human cardiac progenitor cells |
| hdECM | Heart tissue-derived extracellular matrix |
| hDFs | Human dermal fibroblasts |
| hECM | Human extracellular matrix |
| hECs | Human endothelial cells |
| hepG2 | Human hepatocellular carcinoma |
| hESCs | Human embryonic stem cells |
| hiHep | Human-induced hepatocyte |
| hiPSCs | Human induced pluripotent stem cells |
| hKCs | Human keratinocytes |
| hLFs | Human lung fibroblasts |
| hMVECs | Human microvascular endothelial cells |
| hnDFs | Human neonatal dermal fibroblasts |
| hPCs | Human placental pericytes |
| hPSCs | Human pluripotent stem cells |
| hSFs | Human skin fibroblasts |
| hUCMSCs | Human umbilical cord mesenchymal stem cells |
| HUH7 | Undifferentiated hepatocyte cell line |
| hUVECs | Human umbilical vein/vascular endothelial cells |
| iCMs | Induced pluripotent stem cell-derived cardiomyocytes |
| IFN-γ | Interferon-gamma |
| iPSC-CMs | Induced pluripotent stem cell-derived cardiomyocytes |
| iPSCs | Induced pluripotent stem cells |
| ISO | International Standard Organization |
| Kr | Keratin |
| L x 2 | Human hepatic stellate cell line |
| LAP | Lithium phenyl-2,4,6-trimethylbenzoylphosphinate |
| LOM | Laminated object manufacturing |
| mEFs | Mouse embryonic fibroblasts |
| MFDS | Ministry of Food and Drug Safety |
| Mg | Magnesium |
| MJ | Material jetting |
| Mn | Manganese |
| MSCs | Mesenchymal stem/stromal cells |
| MUVECs | Murine umbilical vein endothelial cells |
| n/a | Not applicable |
| Nb | Niobium |
| NB | N-(2-aminoethyl)-4-(4-(hydroxymethyl)-2-methoxy-5-nitrosophenoxy) butanamide |
| NPCs | Neural progenitor cells |
| NRCMs | Neonatal rat cardiomyocytes |
| NSCs | Neural stem cells |
| NSPCs | Neural stem/progenitor cells |
| OMT | Oxymatrine |
| PBF | Powder bed fusion |
| pc-12 | Rat adrenal medullary pheochromocytoma |
| PCL | Poly (ℇ-caprolactone) |
| PecMA | Pectin methacrylate |
| PEDOT | Poly(3,4-ethylenedioxythiophene) |
| PEEK | Polyether ether ketone |
| PEG | Polyethylene glycol |
| PEG4A | 4-arm polyethylene glycol acrylate |
| PEGDA | Diacrylate poly (ethylene glycol) |
| PEGDMA | Poly (ethylene glycol) dimethacrylate |
| PEGMA | Poly (ethylene glycol) methacrylate |
| PF | PEG-Fibrinogen |
| PF | Poly (ethylene glycol)-fibrinogen |
| PGA | Poly (glycolic acid) |
| PGS | Poly (glycerol sebacate) |
| phDFs | Primary human dermal fibroblasts |
| PLA | Poly(l-lactic) acid |
| PLGA | Poly (lactic-co-glycolic) acid |
| PMDA | Pharmaceuticals and Medical Devices Agency |
| PMHs | Primary mouse hepatocytes |
| PrHCs | Primary rat hepatocytes cells |
| PRP | Platelet-rich plasma |
| PSC | Phosphosilicate calcium bioglass |
| PSCs | Phosphosilicate calcium bioglasses |
| PU | Polyurethane |
| PVP | Polyvinylpyrrolidone |
| r-BMSCs | Rat bone marrow mesenchymal stem cells |
| RD | Rhombic dodecahedron |
| rGO | Reduced graphene oxide |
| rhEGF | External human epidermal growth factor |
| SCAPs | Stromal cells from apical papilla |
| SF | Silk fibroin |
| SilMA | Methacrylated silk fibroin |
| SLA | Stereolithography |
| SLM | Selective laser melting |
| SLS | Selective laser sintering |
| Sr-CSH | Xonotlite |
| SR2+ | Strontium |
| SS | Strontium silicate |
| Ta | Tantalum |
| Ti | Titanium |
| Ti6AI4V | Titanium alloy |
| UAM | Ultrasonic additive manufacturing |
| UV | Ultraviolet |
| VEGF | Vascular endothelial |
| XG | Xanthan gum |
| Zn2+ | Zinc |
| Zr | Zirconium |
| β-TCP | Beta-tricalcium phosphate |
References
- Jessop, Z.M. et al. Transforming healthcare through regenerative medicine. BMC Medicine 2016, 14, 115. [Google Scholar] [CrossRef] [PubMed]
- Damaser, M.S. and K.D. Sievert, Tissue engineering and regenerative medicine: bench to bedside in urology. Preface. Adv Drug Deliv Rev 2015, 82-83, v. [Google Scholar] [CrossRef] [PubMed]
- Jacques, E. and E.J. Suuronen, The Progression of Regenerative Medicine and its Impact on Therapy Translation. Clinical and Translational Science 2020, 13, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J., R. Thomas, and R. Guilliatt, Regenerative medicine: from the laboratory looking out. Palgrave Communications 2017, 3, 27. [Google Scholar] [CrossRef]
- Pathak, K. et al. 3D printing in biomedicine: advancing personalized care through additive manufacturing. Exploration of Medicine 2023, 4, 1135–1167. [Google Scholar] [CrossRef]
- Huang, G. et al. Applications, advancements, and challenges of 3D bioprinting in organ transplantation. Biomaterials science 2024, 12. [Google Scholar] [CrossRef]
- Bakhtiar, S.M., et al., Chapter 10 - 3D Printing Technologies and Their Applications in Biomedical Science, in Omics Technologies and Bio-Engineering, D. Barh and V. Azevedo, Editors. 2018, Academic Press. p. 167-189. [CrossRef]
- dos Santos, J. et al. 3D Printing and Nanotechnology: A Multiscale Alliance in Personalized Medicine. Advanced Functional Materials 2021, 31, 2009691. [Google Scholar] [CrossRef]
- Li, J. et al. 3D printing for regenerative medicine: From bench to bedside. Mrs Bulletin 2015, 40, 145–153. [Google Scholar] [CrossRef]
- Amoyav, B. et al. 3D Printed Microfluidic Devices for Drug Release Assays. Pharmaceutics 2021, 13, 13. [Google Scholar] [CrossRef]
- Ong, C.S. et al. 3D bioprinting using stem cells. Pediatric Research 2018, 83, 223–231. [Google Scholar] [CrossRef]
- Liu, K. et al. 3D printing and bioprinting in urology. IJB 2023, 9. [Google Scholar] [CrossRef]
- Jain, P., H. Kathuria, and N. Dubey, Advances in 3D bioprinting of tissues/organs for regenerative medicine and in-vitro models. Biomaterials 2022, 287, 121639. [Google Scholar] [CrossRef] [PubMed]
- Administration, U.S.F.D. Medical Applications of 3D Printing. Available online: https://www.fda.gov/medical-devices/3d-printing-medical-devices/medical-applications-3d-printing.
- Martins, J.P., et al., Chapter 4 - 3D printing: prospects and challenges, in Nanotechnologies in Preventive and Regenerative Medicine, V. Uskoković and D.P. Uskoković, Editors. 2018, Elsevier. p. 299-379. [CrossRef]
- Chung, J.J. et al. Toward Biomimetic Scaffolds for Tissue Engineering: 3D Printing Techniques in Regenerative Medicine. Frontiers in Bioengineering and Biotechnology 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- ASTM, ASTM International Committee F42 on Additive Manufacturing Technologies ASTM F2792–10, in Standard Terminology for Additive Manufacturing Technologies. 2009.
- Ng, W.L. et al. Vat polymerization-based bioprinting-process, materials, applications and regulatory challenges. Biofabrication 2020, 12, 022001. [Google Scholar] [CrossRef]
- Robles Martinez, P. W. Basit, and S. Gaisford, The History, Developments and Opportunities of Stereolithography, in 3D Printing of Pharmaceuticals, A.W. Basit and S. Gaisford, Editors. 2018, Springer International Publishing: Cham. p. 55-79. [CrossRef]
- Xu, X. et al. Vat photopolymerization 3D printing for advanced drug delivery and medical device applications. Journal of Controlled Release 2021, 329, 743–757. [Google Scholar] [CrossRef]
- Al Rashid, A. et al. Vat photopolymerization of polymers and polymer composites: Processes and applications. Additive Manufacturing 2021, 47, 102279. [Google Scholar] [CrossRef]
- Rajan, K. et al. Fused deposition modeling: process, materials, parameters, properties, and applications. The International Journal of Advanced Manufacturing Technology 2022, 120, 1531–1570. [Google Scholar] [CrossRef]
- Marwah, O.M.F. et al. Direct Investment Casting For Pattern Developed By Desktop 3D Printer. MATEC Web of Conferences 2017, 135, 00036. [Google Scholar] [CrossRef]
- Siddique, S.H. et al. Lessons from nature: 3D printed bio-inspired porous structures for impact energy absorption – A review. Additive Manufacturing 2022, 58, 103051. [Google Scholar] [CrossRef]
- Chartrain, N.A. et al. 3D bioprinting for the repair of articular cartilage and osteochondral tissue. Bioprinting 2022, 28, e00239. [Google Scholar] [CrossRef]
- Gibson, I. Additive manufacturing technologies; Springer, 2021; Volume 17. [Google Scholar]
- Ligon, S.C. et al. Polymers for 3D Printing and Customized Additive Manufacturing. Chemical Reviews 2017, 117, 10212–10290. [Google Scholar] [CrossRef] [PubMed]
- Alami, A.H. et al. Additive manufacturing in the aerospace and automotive industries: Recent trends and role in achieving sustainable development goals. Ain Shams Engineering Journal 2023, 14, 102516. [Google Scholar] [CrossRef]
- Zhang, X. and F. Liou, Chapter 1 - Introduction to additive manufacturing, in Additive Manufacturing, J. Pou, A. Riveiro, and J.P. Davim, Editors. 2021, Elsevier. p. 1-31. [CrossRef]
- University, L. About Additive Manufacturing: Powder Bed Fusion. 2024. Available online: https://www.lboro.ac.uk/research/amrg/about/the7categoriesofadditivemanufacturing/powderbedfusion/.
- Singh, R. et al. Powder bed fusion process in additive manufacturing: An overview. Materials Today: Proceedings 2020, 26, 3058–3070. [Google Scholar] [CrossRef]
- Thakur, V. Singh, and R. Kumar, Chapter Two - Materials for additive manufacturing in clinical podiatry, in 3D Printing in Podiatric Medicine, K. Sandhu, et al., Editors. 2023, Academic Press. p. 35-50. [CrossRef]
- Bourell, D. et al. Materials for additive manufacturing. CIRP Annals 2017, 66, 659–681. [Google Scholar] [CrossRef]
- University, L. About Additive Manufacturing: Material Jetting 2024. Available online: https://www.lboro.ac.uk/research/amrg/about/the7categoriesofadditivemanufacturing/materialjetting/.
- Bourell, D.L. Perspectives on Additive Manufacturing. Annual Review of Materials Research 2016, 46, 1–18. [Google Scholar] [CrossRef]
- Mostafaei, A. et al. Binder jet 3D printing—Process parameters, materials, properties, modeling, and challenges. Progress in Materials Science 2021, 119, 100707. [Google Scholar] [CrossRef]
- Naghieh, S. and X. Chen, Printability–A key issue in extrusion-based bioprinting. Journal of Pharmaceutical Analysis 2021, 11, 564–579. [Google Scholar] [CrossRef]
- Tuominen, J. Directed energy deposition–Review of materials, properties and applications. in conference seminar, 3D Boosti ja Invest, Tampere, Finland. 2017. [Google Scholar]
- University, L. About Additive Manufacturing: Directed Energy Deposition. 2024. Available online: https://www.lboro.ac.uk/research/amrg/about/the7categoriesofadditivemanufacturing/directedenergydeposition/.
- Gibson, I. et al. Sheet lamination. Additive manufacturing technologies. 2021; 253–283. [Google Scholar]
- University, L. About Additive Manufacturing: Sheet Lamination. 2024. Available online: https://www.lboro.ac.uk/research/amrg/about/the7categoriesofadditivemanufacturing/sheetlamination/.
- Pantermehl, S. et al. 3D Printing for Soft Tissue Regeneration and Applications in Medicine. Biomedicines 2021, 9. [Google Scholar] [CrossRef]
- Xing, F. et al. Recent advances in biofabrication strategies based on bioprinting for vascularized tissue repair and regeneration. Materials & Design 2023, 229, 111885. [Google Scholar] [CrossRef]
- Gu, Z. et al. Development of 3D bioprinting: From printing methods to biomedical applications. Asian Journal of Pharmaceutical Sciences 2020, 15, 529–557. [Google Scholar] [CrossRef]
- Sufaru, I.-G. et al. 3D Printed and Bioprinted Membranes and Scaffolds for the Periodontal Tissue Regeneration: A Narrative Review. Membranes 2022, 12, 902. [Google Scholar] [CrossRef] [PubMed]
- Ayran, M., B. Bulut, and S. Ulag, Bioprinting, in Biomaterials and Tissue Engineering, O. Gunduz, et al., Editors. 2023, Springer International Publishing: Cham. p. 357-384. [CrossRef]
- Mironov, V. et al. Organ printing: computer-aided jet-based 3D tissue engineering. TRENDS in Biotechnology 2003, 21, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Roth, E.A. et al. Inkjet printing for high-throughput cell patterning. Biomaterials 2004, 25, 3707–3715. [Google Scholar] [CrossRef] [PubMed]
- Norotte, C. et al. Scaffold-free vascular tissue engineering using bioprinting. Biomaterials 2009, 30, 5910–5917. [Google Scholar] [CrossRef]
- Roque, R., G. F. Barbosa, and A.C. Guastaldi, Design and 3D bioprinting of interconnected porous scaffolds for bone regeneration. An additive manufacturing approach. Journal of Manufacturing Processes 2021, 64, 655–663. [Google Scholar] [CrossRef]
- Dababneh, A.B. and I.T. Ozbolat, Bioprinting technology: a current state-of-the-art review. Journal of Manufacturing Science and Engineering 2014, 136, 061016. [Google Scholar] [CrossRef]
- Rider, P. et al. Additive Manufacturing for Guided Bone Regeneration: A Perspective for Alveolar Ridge Augmentation. International Journal of Molecular Sciences 2018, 19, 3308. [Google Scholar] [CrossRef]
- Bartolo, P. et al. Biomedical production of implants by additive electro-chemical and physical processes. CIRP Annals 2012, 61, 635–655. [Google Scholar] [CrossRef]
- Yi, H.-G. et al. Application of 3D bioprinting in the prevention and the therapy for human diseases. Signal Transduction and Targeted Therapy 2021, 6, 177. [Google Scholar] [CrossRef]
- Ovsianikov, A., M. Farsari, and B.N. Chichkov, Photonic and Biomedical Applications of the Two-Photon Polymerization Technique, in Stereolithography: Materials, Processes and Applications, P.J. Bártolo, Editor. 2011, Springer US: Boston, MA. p. 257-297. [CrossRef]
- Gu, B.K. et al. 3-dimensional bioprinting for tissue engineering applications. Biomater Res 2016, 20, 12. [Google Scholar] [CrossRef]
- Song, Y. et al. An overview of selective laser sintering 3D printing technology for biomedical and sports device applications: Processes, materials, and applications. Optics & Laser Technology 2024, 171, 110459. [Google Scholar] [CrossRef]
- Xie, Z. et al. 3D Bioprinting in Tissue Engineering for Medical Applications: The Classic and the Hybrid. Polymers 2020, 12, 1717. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, S. et al. Extrusion bioprinting: Recent progress, challenges, and future opportunities. Bioprinting 2021, 21, e00116. [Google Scholar] [CrossRef]
- Arefin, A.M.E. et al. Polymer 3D Printing Review: Materials, Process, and Design Strategies for Medical Applications. Polymers 2021, 13, 1499. [Google Scholar] [CrossRef]
- Dong, G. et al. Optimizing process parameters of fused deposition modeling by Taguchi method for the fabrication of lattice structures. Additive Manufacturing 2018, 19, 62–72. [Google Scholar] [CrossRef]
- Carneiro, O.S., A. F. Silva, and R. Gomes, Fused deposition modeling with polypropylene. Materials & Design 2015, 83, 768–776. [Google Scholar] [CrossRef]
- Dong, C., M. Petrovic, and I.J. Davies, Applications of 3D printing in medicine: A review. Annals of 3D Printed Medicine 2024, 14, 100149. [Google Scholar] [CrossRef]
- Barbeck, M., et al., Biomaterial-Supported Tissue Reconstruction or Regeneration. 2019: BoD–Books on Demand.
- Rossi, A. et al. Biomaterials for extrusion-based bioprinting and biomedical applications. Frontiers in Bioengineering and Biotechnology 2024, 12. [Google Scholar] [CrossRef]
- Saunders, R.E. and B. Derby, Inkjet printing biomaterials for tissue engineering: bioprinting. International Materials Reviews 2014, 59, 430–448. [Google Scholar] [CrossRef]
- Barui, S. 3D inkjet printing of biomaterials: Principles and applications. MEDICAL DEVICES & SENSORS 2021, 4, e10143. [Google Scholar] [CrossRef]
- Saygili, E. et al. 3D bioprinting: A powerful tool to leverage tissue engineering and microbial systems. Bioprinting 2020, 18, e00071. [Google Scholar] [CrossRef]
- Derakhshanfar, S. et al. 3D bioprinting for biomedical devices and tissue engineering: A review of recent trends and advances. Bioactive Materials 2018, 3, 144–156. [Google Scholar] [CrossRef]
- Li, J. et al. Recent advances in bioprinting techniques: approaches, applications and future prospects. Journal of Translational Medicine 2016, 14, 271. [Google Scholar] [CrossRef]
- Ng, W.L. et al. Microvalve-based bioprinting – process, bio-inks and applications. Biomater. Sci. 2017, 5. [Google Scholar] [CrossRef]
- Vanaei, S. et al. An Overview on Materials and Techniques in 3D Bioprinting Toward Biomedical Application. Engineered Regeneration 2021, 2, 1–18. [Google Scholar] [CrossRef]
- Ouyang, L. et al. Effect of bioink properties on printability and cell viability for 3D bioplotting of embryonic stem cells. Biofabrication 2016, 8, 035020. [Google Scholar] [CrossRef]
- Lozano, R. et al. 3D printing of layered brain-like structures using peptide modified gellan gum substrates. Biomaterials 2015, 67, 264–273. [Google Scholar] [CrossRef]
- Su, C. et al. Natural Materials for 3D Printing and Their Applications. Gels 2022, 8. [Google Scholar] [CrossRef]
- Marques, C.F. et al. Collagen-based bioinks for hard tissue engineering applications: a comprehensive review. J Mater Sci Mater Med 2019, 30, 32. [Google Scholar] [CrossRef]
- Suo, H. et al. Low-temperature 3D printing of collagen and chitosan composite for tissue engineering. Mater Sci Eng C Mater Biol Appl 2021, 123, 111963. [Google Scholar] [CrossRef]
- Dai, M. et al. Elastin-like Polypeptide-Based Bioink: A Promising Alternative for 3D Bioprinting. Biomacromolecules 2021, 22, 4956–4966. [Google Scholar] [CrossRef] [PubMed]
- Aiyelabegan, H.T. et al. Albumin-based biomaterial for lung tissue engineering applications. International Journal of Polymeric Materials and Polymeric Biomaterials 2016, 65, 853–861. [Google Scholar] [CrossRef]
- Placone, J.K. et al. Development and Characterization of a 3D Printed, Keratin-Based Hydrogel. Ann Biomed Eng 2017, 45, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, B. et al. Porous keratin scaffold-promising biomaterial for tissue engineering and drug delivery. J Biomed Mater Res B Appl Biomater 2010, 92, 5–12. [Google Scholar] [CrossRef]
- Khanarian, N.T. et al. A functional agarose-hydroxyapatite scaffold for osteochondral interface regeneration. Biomaterials 2012, 33, 5247–5258. [Google Scholar] [CrossRef]
- Axpe, E. and M.L. Oyen, Applications of Alginate-Based Bioinks in 3D Bioprinting. Int J Mol Sci 2016, 17. [Google Scholar] [CrossRef]
- Petta, D. et al. Hyaluronic acid as a bioink for extrusion-based 3D printing. Biofabrication 2020, 12, 032001. [Google Scholar] [CrossRef]
- Dutta, P., K. Rinki, and J. Dutta, Chitosan: A promising biomaterial for tissue engineering scaffolds. Chitosan for biomaterials II, 2011: p. 45-79.
- Kumar, A., K. M. Rao, and S.S. Han, Application of xanthan gum as polysaccharide in tissue engineering: A review. Carbohydr Polym 2018, 180, 128–144. [Google Scholar] [CrossRef]
- Jena, S.R. et al. Harnessing the potential of dialdehyde alginate-xanthan gum hydrogels as niche bioscaffolds for tissue engineering. Int J Biol Macromol 2022, 207, 493–506. [Google Scholar] [CrossRef]
- Kumar, P.T. et al. Drug delivery and tissue engineering applications of biocompatible pectin-chitin/nano CaCO3 composite scaffolds. Colloids Surf B Biointerfaces 2013, 106, 109–116. [Google Scholar] [CrossRef]
- Akkineni, A.R. et al. Addition of High Acyl Gellan Gum to Low Acyl Gellan Gum Enables the Blends 3D Bioprintable. Gels 2022, 8. [Google Scholar] [CrossRef] [PubMed]
- Li, S. et al. Chitosans for tissue repair and organ three-dimensional (3D) bioprinting. Micromachines 2019, 10, 765. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q., D. Therriault, and M.-C. Heuzey, Processing and properties of chitosan inks for 3D printing of hydrogel microstructures. ACS Biomaterials Science & Engineering 2018, 4, 2643–2652. [Google Scholar]
- Rastogi, P. and B. Kandasubramanian, Review of alginate-based hydrogel bioprinting for application in tissue engineering. Biofabrication 2019, 11, 042001. [Google Scholar] [CrossRef]
- Gaetani, R. et al. Epicardial application of cardiac progenitor cells in a 3D-printed gelatin/hyaluronic acid patch preserves cardiac function after myocardial infarction. Biomaterials 2015, 61, 339–348. [Google Scholar] [CrossRef]
- Negrini, N.C. et al. Three-dimensional printing of chemically crosslinked gelatin hydrogels for adipose tissue engineering. Biofabrication 2020, 12, 025001. [Google Scholar]
- Abelseth, E. et al. 3D printing of neural tissues derived from human induced pluripotent stem cells using a fibrin-based bioink. ACS Biomaterials Science & Engineering 2018, 5, 234–243. [Google Scholar]
- Khoeini, R. et al. Natural and Synthetic Bioinks for 3D Bioprinting. Advanced NanoBiomed Research 2021, 1, 2000097. [Google Scholar] [CrossRef]
- Xin, S. et al. Clickable PEG hydrogel microspheres as building blocks for 3D bioprinting. Biomater Sci 2019, 7, 1179–1187. [Google Scholar] [CrossRef]
- Izgordu, M.S. et al. Investigation of 3D-printed polycaprolactone-/polyvinylpyrrolidone-based constructs. Cartilage 2021, 13, 626S–635S. [Google Scholar] [CrossRef]
- Hospodiuk, M. et al. The bioink: A comprehensive review on bioprintable materials. Biotechnology advances 2017, 35, 217–239. [Google Scholar] [CrossRef] [PubMed]
- Diomede, F. et al. Three-dimensional printed PLA scaffold and human gingival stem cell-derived extracellular vesicles: a new tool for bone defect repair. Stem Cell Research & Therapy 2018, 9, 1–21. [Google Scholar]
- Wang, P. et al. Effects of printing parameters of fused deposition modeling on mechanical properties, surface quality, and microstructure of PEEK. Journal of Materials Processing Technology 2019, 271, 62–74. [Google Scholar] [CrossRef]
- Lee, J. Lee, J., et al., A 3D printing strategy for fabricating in situ topographical scaffolds using pluronic F-127. Additive Manufacturing 2020, 32, 101023. [Google Scholar] [CrossRef]
- Liu, F. and X. Wang, Synthetic Polymers for Organ 3D Printing. Polymers (Basel) 2020, 12. [Google Scholar] [CrossRef]
- Clapper, J.D. et al. Development and characterization of photopolymerizable biodegradable materials from PEG–PLA–PEG block macromonomers. Polymer 2007, 48, 6554–6564. [Google Scholar] [CrossRef]
- Shan Wong, Y. et al. Engineered polymeric biomaterials for tissue engineering. Current Tissue Engineering (Discontinued) 2012, 1, 41–53. [Google Scholar] [CrossRef]
- S, S. et al. A review on the recent applications of synthetic biopolymers in 3D printing for biomedical applications. Journal of Materials Science: Materials in Medicine 2023, 34, 62. [Google Scholar] [CrossRef]
- Im, S.H. et al. Stereocomplex Polylactide for Drug Delivery and Biomedical Applications: A Review. Molecules 2021, 26, 2846. [Google Scholar] [CrossRef]
- Alqurashi, H. et al. Polyetherketoneketone (PEKK): An emerging biomaterial for oral implants and dental prostheses. Journal of Advanced Research 2021, 28, 87–95. [Google Scholar] [CrossRef]
- Elmowafy, E.M., M. Tiboni, and M.E. Soliman, Biocompatibility, biodegradation and biomedical applications of poly(lactic acid)/poly(lactic-co-glycolic acid) micro and nanoparticles. Journal of Pharmaceutical Investigation 2019, 49, 347–380. [Google Scholar] [CrossRef]
- Rutz, A.L. et al. A multi-material bioink method for 3D printing tunable, cell-compatible hydrogels. Advanced materials (Deerfield Beach, Fla.) 2015, 27, 1607. [Google Scholar] [CrossRef] [PubMed]
- Mao, H. et al. Recent advances and challenges in materials for 3D bioprinting. Progress in Natural Science: Materials International 2020, 30, 618–634. [Google Scholar] [CrossRef]
- Lui, Y.S. et al. 4D printing and stimuli-responsive materials in biomedical aspects. Acta biomaterialia 2019, 92, 19–36. [Google Scholar] [CrossRef]
- Li, Y.-C. et al. 4D bioprinting: the next-generation technology for biofabrication enabled by stimuli-responsive materials. Biofabrication 2016, 9, 012001. [Google Scholar] [CrossRef]
- El-Kadiry, A.E., M. Rafei, and R. Shammaa, Cell Therapy: Types, Regulation, and Clinical Benefits. Front Med (Lausanne) 2021, 8, 756029. [Google Scholar] [CrossRef]
- Kim, I. A brief overview of cell therapy and its product. J Korean Assoc Oral Maxillofac Surg 2013, 39, 201–202. [Google Scholar] [CrossRef]
- Facklam, A.L., L. R. Volpatti, and D.G. Anderson, Biomaterials for Personalized Cell Therapy. Advanced Materials 2020, 32, 1902005. [Google Scholar] [CrossRef]
- Xue, J., C. Qin, and C. Wu, 3D printing of cell-delivery scaffolds for tissue regeneration. Regenerative Biomaterials 2023, 10, rbad032. [Google Scholar] [CrossRef]
- Urciuolo, A. et al. Intravital three-dimensional bioprinting. Nat Biomed Eng 2020, 4, 901–915. [Google Scholar] [CrossRef]
- Matai, I. et al. Progress in 3D bioprinting technology for tissue/organ regenerative engineering. Biomaterials 2020, 226, 119536. [Google Scholar] [CrossRef] [PubMed]
- Mandrycky, C. et al. 3D bioprinting for engineering complex tissues. Biotechnol Adv 2016, 34, 422–434. [Google Scholar] [CrossRef] [PubMed]
- Gungor-Ozkerim, P.S. et al. Bioinks for 3D bioprinting: an overview. Biomater Sci 2018, 6, 915–946. [Google Scholar] [CrossRef] [PubMed]
- Ventura, R.D. An Overview of Laser-assisted Bioprinting (LAB) in Tissue Engineering Applications. Medical Lasers 2021, 10, 76–81. [Google Scholar] [CrossRef]
- Fahimipour, F. et al. Enhancing cell seeding and osteogenesis of MSCs on 3D printed scaffolds through injectable BMP2 immobilized ECM-Mimetic gel. Dent Mater 2019, 35, 990–1006. [Google Scholar] [CrossRef]
- Jang, C.H., Y. Koo, and G. Kim, ASC/chondrocyte-laden alginate hydrogel/PCL hybrid scaffold fabricated using 3D printing for auricle regeneration. Carbohydr Polym 2020, 248, 116776. [Google Scholar] [CrossRef]
- Polak, J.M. and S. Mantalaris, Stem cells bioprocessing: an important milestone to move regenerative medicine research into the clinical arena. Pediatr Res 2008, 63, 461–466. [Google Scholar] [CrossRef]
- Saini, G. et al. Applications of 3D Bioprinting in Tissue Engineering and Regenerative Medicine. J Clin Med 2021, 10. [Google Scholar] [CrossRef]
- Jaenisch, R. and R. Young, Stem cells, the molecular circuitry of pluripotency and nuclear reprogramming. Cell 2008, 132, 567–582. [Google Scholar] [CrossRef]
- Poliwoda, S. et al. Stem cells: a comprehensive review of origins and emerging clinical roles in medical practice. Orthop Rev (Pavia) 2022, 14, 37498. [Google Scholar] [CrossRef]
- Caddeo, S., M. Boffito, and S. Sartori, Tissue Engineering Approaches in the Design of Healthy and Pathological In Vitro Tissue Models. Front Bioeng Biotechnol 2017, 5, 40. [Google Scholar] [CrossRef] [PubMed]
- Irvine, S.A. and S.S. Venkatraman, Bioprinting and Differentiation of Stem Cells. Molecules 2016, 21, 1188. [Google Scholar] [CrossRef] [PubMed]
- Kariminekoo, S. et al. Implications of mesenchymal stem cells in regenerative medicine. Artif Cells Nanomed Biotechnol 2016, 44, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Huang, N.F. and S. Li, Mesenchymal stem cells for vascular regeneration. Regen Med 2008, 3, 877–892. [Google Scholar] [CrossRef]
- Alvites, R.D. et al. Rat Olfactory Mucosa Mesenchymal Stem/Stromal Cells (OM-MSCs): A Characterization Study. International Journal of Cell Biology 2020, 2020, 2938258. [Google Scholar] [CrossRef]
- Zhou, T. et al. Challenges and advances in clinical applications of mesenchymal stromal cells. Journal of Hematology & Oncology 2021, 14, 24. [Google Scholar] [CrossRef]
- Conrad, C. et al. Multipotent mesenchymal stem cells acquire a lymphendothelial phenotype and enhance lymphatic regeneration in vivo. Circulation 2009, 119, 281–289. [Google Scholar] [CrossRef]
- Paulo Zambon, J., A. Atala, and J.J. Yoo, Methods to generate tissue-derived constructs for regenerative medicine applications. Methods 2020, 171, 3–10. [Google Scholar] [CrossRef]
- Kaebisch, C. et al. The role of purinergic receptors in stem cell differentiation. Computational and Structural Biotechnology Journal 2015, 13, 75–84. [Google Scholar] [CrossRef]
- Ntege, E.H., H. Sunami, and Y. Shimizu, Advances in regenerative therapy: A review of the literature and future directions. Regenerative Therapy 2020, 14, 136–153. [Google Scholar] [CrossRef]
- Feyen, D.A.M. et al. Stem cell-based therapy: Improving myocardial cell delivery. Advanced Drug Delivery Reviews 2016, 106, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Cui, H. et al. 3D bioprinting for cardiovascular regeneration and pharmacology. Advanced Drug Delivery Reviews 2018, 132, 252–269. [Google Scholar] [CrossRef] [PubMed]
- Ye, L., C. Swingen, and J. Zhang, Induced pluripotent stem cells and their potential for basic and clinical sciences. Curr Cardiol Rev 2013, 9, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Golchin, A. and T.Z. Farahany, Biological Products: Cellular Therapy and FDA Approved Products. Stem Cell Rev Rep 2019, 15, 166–175. [Google Scholar] [CrossRef] [PubMed]
- De Pieri, A., Y. Rochev, and D.I. Zeugolis, Scaffold-free cell-based tissue engineering therapies: advances, shortfalls and forecast. NPJ Regen Med 2021, 6, 18. [Google Scholar] [CrossRef]
- Sánchez, A., T. Schimmang, and J. García-Sancho, Cell and tissue therapy in regenerative medicine. Adv Exp Med Biol 2012, 741, 89–102. [Google Scholar] [CrossRef]
- Gyorgypal, A. An Introduction to Cell Therapy. 2023. Available online: https://www.technologynetworks.com/biopharma/webinars/strategies-for-error-free-chromatographic-analyses-388826 (accessed on 28 July 2024).
- Dainichi, T. et al. Editorial: Regulation of Immunity by Non-Immune Cells. Frontiers in Immunology 2021, 12. [Google Scholar] [CrossRef]
- Guidance for human somatic cell therapy and gene therapy. Hum Gene Ther 2001, 12, 303–314. [CrossRef]
- Bartel, R.L. et al. The Aastrom experience. Stem Cell Research & Therapy 2012, 3, 26. [Google Scholar] [CrossRef]
- Wolff, M. et al. Injections of concentrated bone marrow aspirate as treatment for Discogenic pain: a retrospective analysis. BMC Musculoskelet Disord 2020, 21, 135. [Google Scholar] [CrossRef]
- Buisseret, L. et al. Tumor-infiltrating lymphocyte composition, organization and PD-1/ PD-L1 expression are linked in breast cancer. Oncoimmunology 2017, 6, e1257452. [Google Scholar] [CrossRef] [PubMed]
- Guo, J. et al. Stromal vascular fraction: A regenerative reality? Part 2: Mechanisms of regenerative action. J Plast Reconstr Aesthet Surg 2016, 69, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Heo, D.N. et al. 3D bioprinting of carbohydrazide-modified gelatin into microparticle-suspended oxidized alginate for the fabrication of complex-shaped tissue constructs. ACS applied materials & interfaces 2020, 12, 20295–20306. [Google Scholar]
- Dey, M. and I.T. Ozbolat, 3D bioprinting of cells, tissues and organs. Scientific Reports 2020, 10, 14023. [Google Scholar] [CrossRef]
- Alonzo, M. et al. 3D Bioprinting of cardiac tissue and cardiac stem cell therapy. Transl Res 2019, 211, 64–83. [Google Scholar] [CrossRef]
- Qasim, M. et al. 3D printing approaches for cardiac tissue engineering and role of immune modulation in tissue regeneration. Int J Nanomedicine 2019, 14, 1311–1333. [Google Scholar] [CrossRef]
- Roth, G.A. et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J Am Coll Cardiol 2017, 70, 1–25. [Google Scholar] [CrossRef]
- Bhandari, S. et al. Trends and Challenges in the Development of 3D-Printed Heart Valves and Other Cardiac Implants: A Review of Current Advances. Cureus 2023, 15, e43204. [Google Scholar] [CrossRef]
- Itier, R. and J. Roncalli, New therapies for acute myocardial infarction: current state of research and future promise. Future Cardiology 2018, 14, 329–342. [Google Scholar] [CrossRef]
- Shi, W.Y., et al., Role of coronary artery bypass surgery in acute myocardial infarction. Primary Angioplasty: A Practical Guide, 2018; p. 211-221.
- Kwon, Y.-W., H. -M. Yang, and H.-J. Cho, Cell therapy for myocardial infarction. International journal of stem cells 2010, 3, 8–15. [Google Scholar] [CrossRef]
- Das, S., H. Nam, and J. Jang, 3D bioprinting of stem cell-laden cardiac patch: A promising alternative for myocardial repair. APL bioengineering, 2021. 5.
- Fernandes, S. et al. Synthetic matrices to serve as niches for muscle cell transplantation. Cells Tissues Organs 2011, 195, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Vukicevic, M. et al. Cardiac 3D printing and its future directions. JACC: Cardiovascular Imaging 2017, 10, 171–184. [Google Scholar] [PubMed]
- Hinderer, S., E. Brauchle, and K. Schenke-Layland, Generation and assessment of functional biomaterial scaffolds for applications in cardiovascular tissue engineering and regenerative medicine. Advanced healthcare materials 2015, 4, 2326–2341. [Google Scholar] [CrossRef]
- Zhu, J. and R.E. Marchant, Design properties of hydrogel tissue-engineering scaffolds. Expert review of medical devices 2011, 8, 607–626. [Google Scholar] [CrossRef]
- Maiullari, F. et al. A multi-cellular 3D bioprinting approach for vascularized heart tissue engineering based on HUVECs and iPSC-derived cardiomyocytes. Scientific Reports 2018, 8, 13532. [Google Scholar] [CrossRef]
- Bejleri, D. et al. A Bioprinted Cardiac Patch Composed of Cardiac-Specific Extracellular Matrix and Progenitor Cells for Heart Repair. Advanced Healthcare Materials 2018, 7, 1800672. [Google Scholar] [CrossRef]
- Melhem, M.R. et al. 3D Printed Stem-Cell-Laden, Microchanneled Hydrogel Patch for the Enhanced Release of Cell-Secreting Factors and Treatment of Myocardial Infarctions. ACS Biomaterials Science & Engineering 2017, 3, 1980–1987. [Google Scholar] [CrossRef]
- Noor, N. et al. 3D Printing of Personalized Thick and Perfusable Cardiac Patches and Hearts. Advanced Science 2019, 6, 1900344. [Google Scholar] [CrossRef]
- Cui, X. and T. Boland, Human microvasculature fabrication using thermal inkjet printing technology. Biomaterials 2009, 30, 6221–6227. [Google Scholar] [CrossRef]
- Kucukgul, C. et al. 3D bioprinting of biomimetic aortic vascular constructs with self-supporting cells. Biotechnology and Bioengineering 2015, 112, 811–821. [Google Scholar] [CrossRef]
- Gaetani, R. et al. Cardiac tissue engineering using tissue printing technology and human cardiac progenitor cells. Biomaterials 2012, 33, 1782–1790. [Google Scholar] [CrossRef] [PubMed]
- Ketabat, F. et al. Optimization of 3D printing and in vitro characterization of alginate/gelatin lattice and angular scaffolds for potential cardiac tissue engineering. Frontiers in Bioengineering and Biotechnology 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Roche, C.D. et al. 3D bioprinted alginate-gelatin hydrogel patches containing cardiac spheroids recover heart function in a mouse model of myocardial infarction. Bioprinting 2023, 30, e00263. [Google Scholar] [CrossRef]
- Zhang, Y.S. et al. Bioprinting 3D microfibrous scaffolds for engineering endothelialized myocardium and heart-on-a-chip. Biomaterials 2016, 110, 45–59. [Google Scholar] [CrossRef]
- Das, S. et al. Decellularized extracellular matrix bioinks and the external stimuli to enhance cardiac tissue development in vitro. Acta Biomaterialia 2019, 95, 188–200. [Google Scholar] [CrossRef]
- Atari, M., S. Labbaf, and S.H. Javanmard, Fabrication and characterization of a 3D scaffold based on elastomeric poly-glycerol Sebacate polymer for heart valve applications. Journal of Manufacturing Processes 2023, 102, 350–364. [Google Scholar] [CrossRef]
- Yang, Y. et al. Elastic 3D-Printed Hybrid Polymeric Scaffold Improves Cardiac Remodeling after Myocardial Infarction. Advanced Healthcare Materials 2019, 8, 1900065. [Google Scholar] [CrossRef]
- Liu, Y. et al. hESCs-Derived Early Vascular Cell Spheroids for Cardiac Tissue Vascular Engineering and Myocardial Infarction Treatment. Adv Sci (Weinh) 2022, 9, e2104299. [Google Scholar] [CrossRef]
- Miller, K.L. et al. Rapid 3D BioPrinting of a human iPSC-derived cardiac micro-tissue for high-throughput drug testing. Organs-on-a-Chip 2021, 3, 100007. [Google Scholar] [CrossRef]
- Wang, Z. et al. 3D bioprinted functional and contractile cardiac tissue constructs. Acta Biomaterialia 2018, 70, 48–56. [Google Scholar] [CrossRef]
- Cieza, A. et al. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet 2020, 396, 2006–2017. [Google Scholar] [CrossRef] [PubMed]
- Bauso, L.V. et al. Bone Tissue Engineering and Nanotechnology: A Promising Combination for Bone Regeneration. Biology 2024, 13, 237. [Google Scholar] [CrossRef] [PubMed]
- Smrke, D., et al., Treatment of bone defects—allogenic platelet gel and autologous bone technique, in Regenerative medicine and tissue engineering. 2013, IntechOpen.
- Schlickewei, C.W. et al. Current and future concepts for the treatment of impaired fracture healing. International journal of molecular sciences 2019, 20, 5805. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y. et al. 3D printing of chemical-empowered tendon stem/progenitor cells for functional tissue repair. Biomaterials 2021, 271, 120722. [Google Scholar] [CrossRef] [PubMed]
- Aytac, Z. et al. Innovations in craniofacial bone and periodontal tissue engineering–from electrospinning to converged biofabrication. International materials reviews 2022, 67, 347–384. [Google Scholar] [CrossRef]
- Sousa, A.C. et al. Assessment of 3D-Printed Polycaprolactone, Hydroxyapatite Nanoparticles and Diacrylate Poly(ethylene glycol) Scaffolds for Bone Regeneration. Pharmaceutics 2022, 14. [Google Scholar] [CrossRef]
- Dubey, N. et al. Highly tunable bioactive fiber-reinforced hydrogel for guided bone regeneration. Acta biomaterialia 2020, 113, 164–176. [Google Scholar] [CrossRef]
- Chung, J.J. et al. Toward biomimetic scaffolds for tissue engineering: 3D printing techniques in regenerative medicine. Frontiers in Bioengineering and Biotechnology 2020, 8, 586406. [Google Scholar] [CrossRef]
- Lei, P. et al. Porous tantalum structure integrated on Ti6Al4V base by Laser Powder Bed Fusion for enhanced bony-ingrowth implants: In vitro and in vivo validation. Bioactive Materials 2022, 7, 3–13. [Google Scholar] [CrossRef]
- Yu, L. et al. 3D Culture of Bone Marrow-Derived Mesenchymal Stem Cells (BMSCs) Could Improve Bone Regeneration in 3D-Printed Porous Ti6Al4V Scaffolds. Stem Cells International 2018, 2018, 2074021. [Google Scholar] [CrossRef]
- Wu, Y.-F. et al. 3D-bioprinted alginate-based bioink scaffolds with β-tricalcium phosphate for bone regeneration applications. Journal of Dental Sciences 2024, 19, 1116–1125. [Google Scholar] [CrossRef] [PubMed]
- Ressler, A. et al. Vat photopolymerization of biomimetic bone scaffolds based on Mg, Sr, Zn-substituted hydroxyapatite: Effect of sintering temperature. Ceramics International 2024, 50, 27403–27415. [Google Scholar] [CrossRef]
- Yu, X. et al. Osteoimmunomodulatory bioinks for 3D bioprinting achieve complete regeneration of critical-sized bone defects. Composites Part B: Engineering 2024, 273, 111256. [Google Scholar] [CrossRef]
- Choe, G. et al. Three-dimensional bioprinting of mesenchymal stem cells using an osteoinductive bioink containing alginate and BMP-2-loaded PLGA nanoparticles for bone tissue engineering. Biomaterials Advances 2022, 136, 212789. [Google Scholar] [CrossRef]
- Wang, W. et al. 3D bioprinting of DPSCs with GelMA hydrogel of various concentrations for bone regeneration. Tissue and Cell 2024, 88, 102418. [Google Scholar] [CrossRef]
- Tao, J. et al. DLP-based bioprinting of void-forming hydrogels for enhanced stem-cell-mediated bone regeneration. Materials Today Bio 2022, 17, 100487. [Google Scholar] [CrossRef]
- Gatto, M.L. et al. Biomechanical performances of PCL/HA micro- and macro-porous lattice scaffolds fabricated via laser powder bed fusion for bone tissue engineering. Materials Science and Engineering: C 2021, 128, 112300. [Google Scholar] [CrossRef]
- Hong, D. et al. Binder-jetting 3D printing and alloy development of new biodegradable Fe-Mn-Ca/Mg alloys. Acta Biomaterialia 2016, 45, 375–386. [Google Scholar] [CrossRef]
- Barro, Ó. et al. Improved Commercially Pure Titanium Obtained by Laser Directed Energy Deposition for Dental Prosthetic Applications. Metals 2021, 11. [Google Scholar] [CrossRef]
- Arias-González, F. et al. In-Situ Laser Directed Energy Deposition of Biomedical Ti-Nb and Ti-Zr-Nb Alloys from Elemental Powders. Metals 2021, 11. [Google Scholar] [CrossRef]
- Cedeño-Viveros, L.D. et al. Influence of process parameters for sheet lamination based on laser micro-spot welding of austenitic stainless steel sheets for bone tissue applications. The International Journal of Advanced Manufacturing Technology 2021, 115, 247–262. [Google Scholar] [CrossRef]
- Touya, N. et al. In vitro and in vivo characterization of a novel tricalcium silicate-based ink for bone regeneration using laser-assisted bioprinting. Biofabrication 2022, 14, 024104. [Google Scholar] [CrossRef] [PubMed]
- Li, W. et al. Application of 3D Bioprinting in Liver Diseases. Micromachines (Basel) 2023, 14. [Google Scholar] [CrossRef]
- Kasturi, M. et al. Three Dimensional Bioprinting for Hepatic Tissue Engineering: From In Vitro Models to Clinical Applications. Tissue Eng Regen Med 2024, 21, 21–52. [Google Scholar] [CrossRef]
- Palakkan, A.A. et al. Liver tissue engineering and cell sources: issues and challenges. Liver Int 2013, 33, 666–676. [Google Scholar] [CrossRef]
- Asrani, S.K. et al. Burden of liver diseases in the world. Journal of hepatology 2019, 70, 151–171. [Google Scholar] [CrossRef]
- Singh, S., N. A. Osna, and K.K. Kharbanda, Treatment options for alcoholic and non-alcoholic fatty liver disease: A review. World journal of gastroenterology 2017, 23, 6549. [Google Scholar] [CrossRef]
- Robbins, J.B. et al. A novel in vitro three-dimensional bioprinted liver tissue system for drug development. The FASEB Journal 2013, 27, 872.12. [Google Scholar] [CrossRef]
- Chang, R. et al. Biofabrication of a three-dimensional liver micro-organ as an in vitro drug metabolism model. Biofabrication 2010, 2, 045004. [Google Scholar] [CrossRef]
- Lee, S.Y., H. J. Kim, and D. Choi, Cell sources, liver support systems and liver tissue engineering: alternatives to liver transplantation. International journal of stem cells 2015, 8, 36–47. [Google Scholar] [CrossRef]
- Iqbal, S. et al. Biomaterials evolution: from inert to instructive. Biomaterials Science 2023, 11, 6109–6115. [Google Scholar] [CrossRef] [PubMed]
- Gungor-Ozkerim, P.S. et al. Bioinks for 3D bioprinting: an overview. Biomaterials science 2018, 6, 915–946. [Google Scholar] [CrossRef] [PubMed]
- Allu, I. et al. Decellularization techniques for tissue engineering: towards replicating native extracellular matrix architecture in liver regeneration. Journal of Functional Biomaterials 2023, 14, 518. [Google Scholar] [CrossRef] [PubMed]
- Khati, V. et al. Indirect 3D bioprinting of a robust trilobular hepatic construct with decellularized liver matrix hydrogel. Bioengineering 2022, 9, 603. [Google Scholar] [CrossRef]
- Wang, Q. et al. Innovations in 3D bioprinting and biomaterials for liver tissue engineering: Paving the way for tissue-engineered liver. iLIVER 2024, 3, 100080. [Google Scholar] [CrossRef]
- Yang, H. et al. Three-dimensional bioprinted hepatorganoids prolong survival of mice with liver failure. Gut 2021, 70, 567. [Google Scholar] [CrossRef]
- Xie, F. et al. Three-dimensional bio-printing of primary human hepatocellular carcinoma for personalized medicine. Biomaterials 2021, 265, 120416. [Google Scholar] [CrossRef]
- Lewis, P.L., R. M. Green, and R.N. Shah, 3D-printed gelatin scaffolds of differing pore geometry modulate hepatocyte function and gene expression. Acta Biomaterialia 2018, 69, 63–70. [Google Scholar] [CrossRef]
- Jeon, H. et al. Generation of Multilayered 3D Structures of HepG2 Cells Using a Bio-printing Technique. Gut Liver 2017, 11, 121–128. [Google Scholar] [CrossRef]
- Wu, Y. et al. 3D bioprinting of bicellular liver lobule-mimetic structures via microextrusion of cellulose nanocrystal-incorporated shear-thinning bioink. Sci Rep 2020, 10, 20648. [Google Scholar] [CrossRef]
- Mao, Q. et al. Fabrication of liver microtissue with liver decellularized extracellular matrix (dECM) bioink by digital light processing (DLP) bioprinting. Mater Sci Eng C Mater Biol Appl 2020, 109, 110625. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K. et al. 3D bioprinting of dECM-incorporated hepatocyte spheroid for simultaneous promotion of cell-cell and -ECM interactions. Frontiers in Bioengineering and Biotechnology 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Faulkner-Jones, A. et al. Bioprinting of human pluripotent stem cells and their directed differentiation into hepatocyte-like cells for the generation of mini-livers in 3D. Biofabrication 2015, 7, 044102. [Google Scholar] [CrossRef] [PubMed]
- Lee, H. et al. Development of Liver Decellularized Extracellular Matrix Bioink for Three-Dimensional Cell Printing-Based Liver Tissue Engineering. Biomacromolecules 2017, 18, 1229–1237. [Google Scholar] [CrossRef]
- Lee, J.W. et al. Development of a 3D cell printed construct considering angiogenesis for liver tissue engineering. Biofabrication 2016, 8, 015007. [Google Scholar] [CrossRef]
- Hiller, T. et al. Generation of a 3D Liver Model Comprising Human Extracellular Matrix in an Alginate/Gelatin-Based Bioink by Extrusion Bioprinting for Infection and Transduction Studies. International Journal of Molecular Sciences 2018, 19, 3129. [Google Scholar] [CrossRef]
- Kang, D. et al. Bioprinting of Multiscaled Hepatic Lobules within a Highly Vascularized Construct. Small 2020, 16, 1905505. [Google Scholar] [CrossRef]
- Mazzocchi, A. et al. Optimization of collagen type I-hyaluronan hybrid bioink for 3D bioprinted liver microenvironments. Biofabrication 2018, 11, 015003. [Google Scholar] [CrossRef]
- Wu, Y. et al. 3D bioprinting of liver-mimetic construct with alginate/cellulose nanocrystal hybrid bioink. Bioprinting 2018, 9, 1–6. [Google Scholar] [CrossRef]
- Calonje, J.E., et al., McKee's Pathology of the Skin, 2 Volume Set E-Book. 2018: Elsevier Health Sciences.
- Liu, Y. et al. 3D bioprinting bioglass to construct vascularized full-thickness skin substitutes for wound healing. Materials Today Bio 2024, 24, 100899. [Google Scholar] [CrossRef]
- Zöller, N. et al. Clinical application of a tissue-cultured skin autograft: an alternative for the treatment of non-healing or slowly healing wounds? Dermatology 2014, 229, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.V. and A. Atala, 3D bioprinting of tissues and organs. Nature biotechnology 2014, 32, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Tabriz, A.G. and D. Douroumis, Recent advances in 3D printing for wound healing: A systematic review. Journal of Drug Delivery Science and Technology 2022, 74, 103564. [Google Scholar] [CrossRef]
- Hong, N. et al. 3D bioprinting and its in vivo applications. Journal of Biomedical Materials Research Part B: Applied Biomaterials 2018, 106, 444–459. [Google Scholar] [CrossRef]
- Vijayavenkataraman, S., W. Lu, and J. Fuh, 3D bioprinting of skin: a state-of-the-art review on modelling, materials, and processes. Biofabrication 2016, 8, 032001. [Google Scholar] [CrossRef]
- Admane, P. et al. Direct 3D bioprinted full-thickness skin constructs recapitulate regulatory signaling pathways and physiology of human skin. Bioprinting 2019, 15, e00051. [Google Scholar] [CrossRef]
- Jin, R. et al. Three-dimensional bioprinting of a full-thickness functional skin model using acellular dermal matrix and gelatin methacrylamide bioink. Acta Biomaterialia 2021, 131, 248–261. [Google Scholar] [CrossRef]
- Song, Y. et al. Electrospinning/3D printing drug-loaded antibacterial polycaprolactone nanofiber/sodium alginate-gelatin hydrogel bilayer scaffold for skin wound repair. International Journal of Biological Macromolecules 2024, 129705. [Google Scholar] [CrossRef]
- Ma, J. et al. 3D Printing of Strontium Silicate Microcylinder-Containing Multicellular Biomaterial Inks for Vascularized Skin Regeneration. Advanced Healthcare Materials 2021, 10, 2100523. [Google Scholar] [CrossRef]
- Pajooh, A.M.D. et al. Biomimetic VEGF-loaded bilayer scaffold fabricated by 3D printing and electrospinning techniques for skin regeneration. Materials & Design 2024, 238, 112714. [Google Scholar] [CrossRef]
- Zhou, F. et al. Rapid printing of bio-inspired 3D tissue constructs for skin regeneration. Biomaterials 2020, 258, 120287. [Google Scholar] [CrossRef] [PubMed]
- Kwak, H. et al. Formation of a keratin layer with silk fibroin-polyethylene glycol composite hydrogel fabricated by digital light processing 3D printing. Journal of Industrial and Engineering Chemistry 2019, 72, 232–240. [Google Scholar] [CrossRef]
- Zhao, M. et al. Functionalizing multi-component bioink with platelet-rich plasma for customized in-situ bilayer bioprinting for wound healing. Materials Today Bio 2022, 16, 100334. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-D. et al. Planar-/Curvilinear-Bioprinted Tri-Cell-Laden Hydrogel for Healing Irregular Chronic Wounds. Advanced Healthcare Materials 2022, 11, 2201021. [Google Scholar] [CrossRef]
- Datta, S. et al. Alginate-honey bioinks with improved cell responses for applications as bioprinted tissue engineered constructs. Journal of Materials Research 2018, 33, 2029–2039. [Google Scholar] [CrossRef]
- Pereira, R.F. et al. A single-component hydrogel bioink for bioprinting of bioengineered 3D constructs for dermal tissue engineering. Materials Horizons 2018, 5, 1100–1111. [Google Scholar] [CrossRef]
- Baltazar, T. et al. Three Dimensional Bioprinting of a Vascularized and Perfusable Skin Graft Using Human Keratinocytes, Fibroblasts, Pericytes, and Endothelial Cells. Tissue Eng Part A 2020, 26, 227–238. [Google Scholar] [CrossRef]
- Shi, L. et al. Three-dimensional printing alginate/gelatin scaffolds as dermal substitutes for skin tissue engineering. Polymer Engineering & Science 2018, 58, 1782–1790. [Google Scholar] [CrossRef]
- Fligge, M. et al. Personalized dermal patches – Inkjet printing of prednisolone nanosuspensions for individualized treatment of skin diseases. International Journal of Pharmaceutics 2023, 630, 122382. [Google Scholar] [CrossRef]
- Cadena, M. et al. 3D Bioprinting of Neural Tissues. Adv Healthc Mater 2021, 10, e2001600. [Google Scholar] [CrossRef]
- Joung, D. et al. 3D Printed Neural Regeneration Devices. Adv Funct Mater 2020, 30. [Google Scholar] [CrossRef]
- Yi, S. et al. Application of stem cells in peripheral nerve regeneration. Burns & trauma 2020, 8, tkaa002. [Google Scholar]
- Han, Y. and J. Yin, Industry news: the additive manufacturing of nerve conduits for the treatment of peripheral nerve injury. 2022, Springer. p. 1-3.
- Zhu, H. et al. 3D printing of functional bioengineered constructs for neural regeneration: a review. International Journal of Extreme Manufacturing 2023, 5, 042004. [Google Scholar] [CrossRef]
- Hsieh, F.-Y. and S.-h. Hsu, 3D bioprinting: A new insight into the therapeutic strategy of neural tissue regeneration. Organogenesis 2015, 11, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-W. et al. Dual crosslinking silk fibroin/pectin-based bioink development and the application on neural stem/progenitor cells spheroid laden 3D bioprinting. International Journal of Biological Macromolecules 2024, 269, 131720. [Google Scholar] [CrossRef]
- Song, S. et al. Three-dimensional printing of microfiber- reinforced hydrogel loaded with oxymatrine for treating spinal cord injury. Int J Bioprint 2023, 9, 692. [Google Scholar] [CrossRef]
- Li, J. et al. The development of the multi-physical model for cell-laden nerve scaffolds and its bioprinting by stereolithography. Materials Today: Proceedings 2022, 70, 388–394. [Google Scholar] [CrossRef]
- Hsieh, F.-Y., H. -H. Lin, and S.-h. Hsu, 3D bioprinting of neural stem cell-laden thermoresponsive biodegradable polyurethane hydrogel and potential in central nervous system repair. Biomaterials 2015, 71, 48–57. [Google Scholar] [CrossRef]
- Yan, Y. et al. 3D bioprinting of human neural tissues with functional connectivity. Cell Stem Cell 2024, 31, 260–274. [Google Scholar] [CrossRef]
- Tortorella, S. et al. Laser Assisted Bioprinting of laminin on biodegradable PLGA substrates: Effect on neural stem cell adhesion and differentiation. Bioprinting 2022, 26, e00194. [Google Scholar] [CrossRef]
- Ho, L. and S.-h. Hsu, Cell reprogramming by 3D bioprinting of human fibroblasts in polyurethane hydrogel for fabrication of neural-like constructs. Acta Biomaterialia 2018, 70, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-B. et al. Bio-printing of collagen and VEGF-releasing fibrin gel scaffolds for neural stem cell culture. Experimental Neurology 2010, 223, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Chen, C. et al. 3D printing of interferon γ-preconditioned NSC-derived exosomes/collagen/chitosan biological scaffolds for neurological recovery after TBI. Bioactive Materials 2024, 39, 375–391. [Google Scholar] [CrossRef]
- Han, Y. et al. A 3D printable gelatin methacryloyl/chitosan hydrogel assembled with conductive PEDOT for neural tissue engineering. Composites Part B: Engineering 2024, 273, 111241. [Google Scholar] [CrossRef]
- Song, S. et al. Neural stem cell-laden 3D bioprinting of polyphenol-doped electroconductive hydrogel scaffolds for enhanced neuronal differentiation. Biomaterials Advances 2022, 133, 112639. [Google Scholar] [CrossRef]
- Liu, J. et al. Additive-lathe 3D bioprinting of bilayered nerve conduits incorporated with supportive cells. Bioactive Materials 2021, 6, 219–229. [Google Scholar] [CrossRef]
- Vijayavenkataraman, S. et al. 3D-Printed PCL/rGO Conductive Scaffolds for Peripheral Nerve Injury Repair. Artificial Organs 2019, 43, 515–523. [Google Scholar] [CrossRef]
- Heinrich, M.A. et al. 3D bioprinting: from benches to translational applications. Small 2019, 15, 1805510. [Google Scholar] [CrossRef]
- Stanco, D. et al. 3D bioprinting for orthopaedic applications: Current advances, challenges and regulatory considerations. Bioprinting 2020, 20, e00103. [Google Scholar] [CrossRef]
- Agarwal, K. et al. Insights of 3D bioprinting and focusing the paradigm shift towards 4D printing for biomedical applications. Journal of Materials Research 2023, 38, 112–141. [Google Scholar] [CrossRef]
- Jafarkhani, M. et al. Bioprinting in Vascularization Strategies. Iran Biomed J 2019, 23, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.K. et al. Engineering vascularized tissue. Nat Biotechnol 2005, 23, 821–823. [Google Scholar] [CrossRef] [PubMed]
- Zheng, K. et al. Recent progress of 3D printed vascularized tissues and organs. Smart Materials in Medicine 2024, 5, 183–195. [Google Scholar] [CrossRef]
- Ma, Y. et al. Advancements of 3D bioprinting in regenerative medicine: Exploring cell sources for organ fabrication. Heliyon 2024, 10, e24593. [Google Scholar] [CrossRef]
- Inglis, S. et al. Human endothelial and foetal femur-derived stem cell co-cultures modulate osteogenesis and angiogenesis. Stem cell research & therapy 2016, 7, 1–16. [Google Scholar]
- Lovett, M. et al. Vascularization strategies for tissue engineering. Tissue Eng Part B Rev 2009, 15, 353–370. [Google Scholar] [CrossRef]
- Bishop, E.S. et al. 3-D bioprinting technologies in tissue engineering and regenerative medicine: Current and future trends. Genes & diseases 2017, 4, 185–195. [Google Scholar]
- Persaud, A. et al. 3D Bioprinting with Live Cells. Engineered Regeneration 2022, 3, 292–309. [Google Scholar] [CrossRef]
- Martin, I., P. J. Simmons, and D.F. Williams, Manufacturing challenges in regenerative medicine. Science translational medicine 2014, 6, 232fs16. [Google Scholar] [CrossRef]
- Jin, Z. et al. 3D Printing of Physical Organ Models: Recent Developments and Challenges. Advanced Science 2021, 8, 2101394. [Google Scholar] [CrossRef]
- Hinton, T.J. et al. Three-dimensional printing of complex biological structures by freeform reversible embedding of suspended hydrogels. Science advances 2015, 1, e1500758. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.-W. et al. A 3D bioprinting system to produce human-scale tissue constructs with structural integrity. Nature biotechnology 2016, 34, 312–319. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.V., P. De Coppi, and A. Atala, Opportunities and challenges of translational 3D bioprinting. Nature Biomedical Engineering 2020, 4, 370–380. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.S. et al. Three-Dimensional Bioprinting Strategies for Tissue Engineering. Cold Spring Harb Perspect Med 2018, 8. [Google Scholar] [CrossRef]
- Jones, N. Science in three dimensions: The print revolution. Nature 2012, 487, 22–23. [Google Scholar] [CrossRef]
- Liang, K. Tissue Bioprinting: Promise and Challenges. Bioengineering (Basel) 2023, 10. [Google Scholar] [CrossRef]
- Ramadan, Q. and M. Zourob, 3D Bioprinting at the Frontier of Regenerative Medicine, Pharmaceutical, and Food Industries. Frontiers in Medical Technology 2021, 2. [Google Scholar] [CrossRef]
- Muskan, D. Gupta, and N.P. Negi, 3D bioprinting: Printing the future and recent advances. Bioprinting 2022, 27, e00211. [Google Scholar] [CrossRef]
- Cui, H. et al. 3D bioprinting for organ regeneration. Advanced healthcare materials 2017, 6, 1601118. [Google Scholar] [CrossRef]
- Ghosh, R. et al. Micro/nanofiber-based noninvasive devices for health monitoring diagnosis and rehabilitation. Applied Physics Reviews 2020, 7. [Google Scholar]
- Yilmaz, B. et al. Bioprinting: A review of processes, materials and applications. Bioprinting 2021, 23, e00148. [Google Scholar] [CrossRef]
- Koons, G.L. and A.G. Mikos, Progress in three-dimensional printing with growth factors. J Control Release 2019, 295, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.S. et al. 3D extrusion bioprinting. Nature Reviews Methods Primers 2021, 1, 75. [Google Scholar] [CrossRef]
- Abbadessa, A., A. Ronca, and A. Salerno, Integrating bioprinting, cell therapies and drug delivery towards in vivo regeneration of cartilage, bone and osteochondral tissue. Drug Deliv Transl Res 2024, 14, 858–894. [Google Scholar] [CrossRef]
- Reddy, V.S. et al. A review on electrospun nanofibers based advanced applications: From health care to energy devices. Polymers 2021, 13, 3746. [Google Scholar] [CrossRef]
- Bejoy, A.M. et al. An insight on advances and applications of 3d bioprinting: A review. Bioprinting 2021, 24, e00176. [Google Scholar] [CrossRef]
- Ozbolat, I.T., W. Peng, and V. Ozbolat, Application areas of 3D bioprinting. Drug discovery today 2016, 21, 1257–1271. [Google Scholar] [CrossRef]
- De Santis, M.M. et al. Extracellular-matrix-reinforced bioinks for 3D bioprinting human tissue. Advanced materials 2021, 33, 2005476. [Google Scholar] [CrossRef]
- Reddy, V.S. et al. Contemporary standpoint and future of 3D bioprinting in tissue/organs printing. Current Opinion in Biomedical Engineering 2023, 27, 100461. [Google Scholar] [CrossRef]
- Veiga, A. et al. Current Trends on Protein Driven Bioinks for 3D Printing. Pharmaceutics 2021, 13, 1444. [Google Scholar] [CrossRef]
- Gao, B. et al. 4D Bioprinting for Biomedical Applications. Trends in Biotechnology 2016, 34, 746–756. [Google Scholar] [CrossRef]
- An, J., C.K. Chua, and V. Mironov, A perspective on 4D bioprinting. IJB 2016, 2. [CrossRef]
Figure 1.
Schematic representation of the various AM processes.
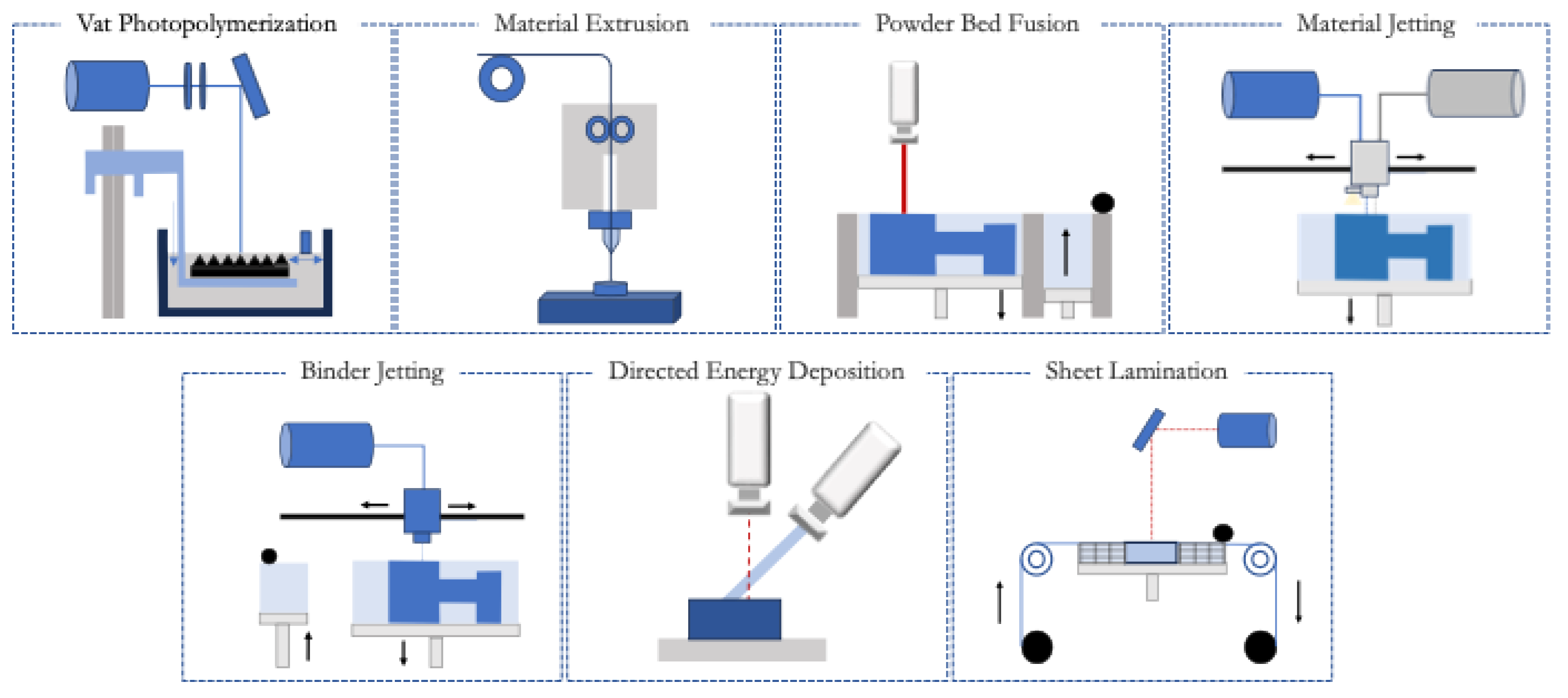
Figure 2.
Major milestones in the history of 3D bioprinting.
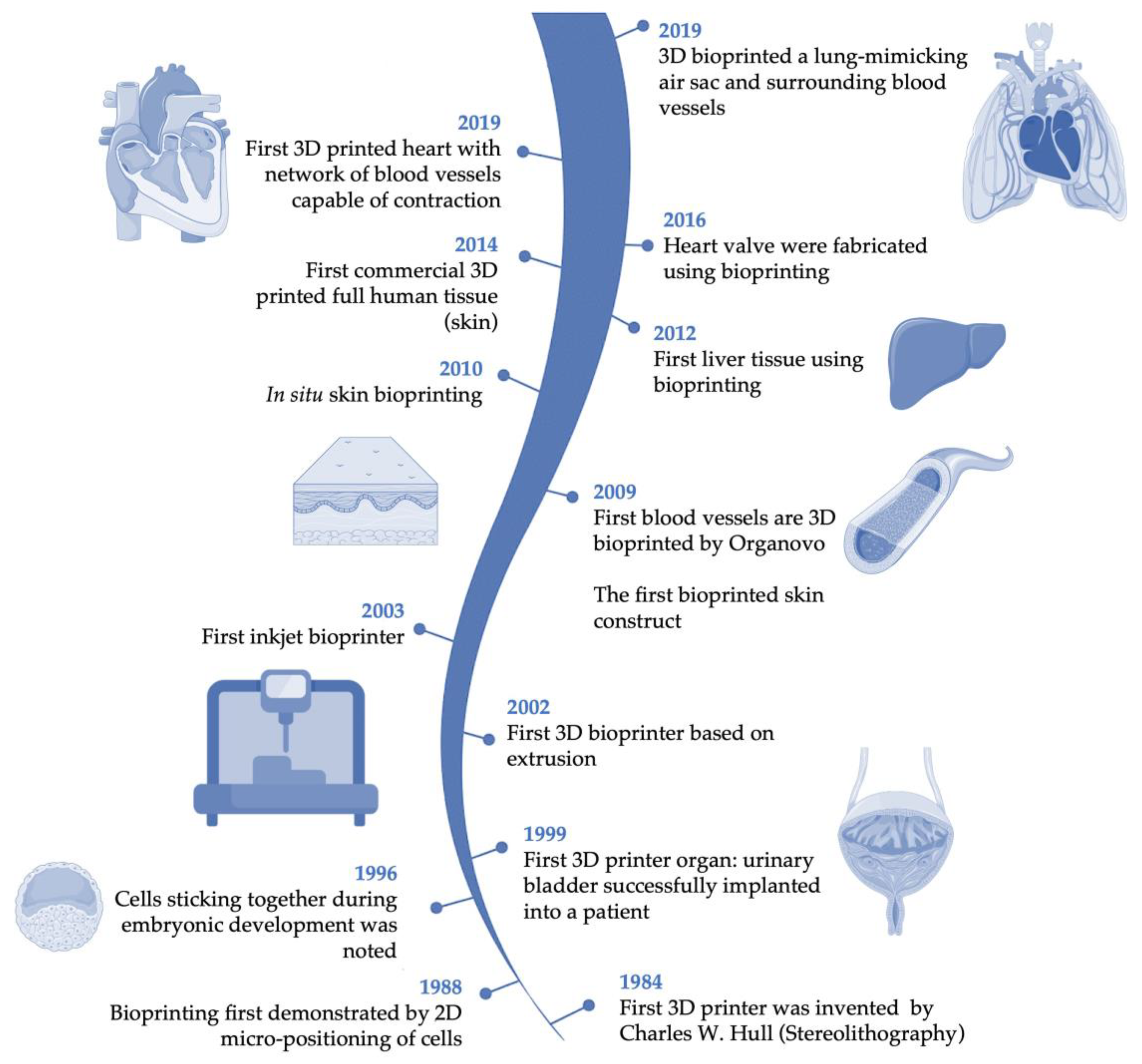
Figure 3.
Advances in cell therapies, 3D printing, and bioprinting are addressing the challenges in engineering cardiovascular, bone, liver, skin, and neural tissues.
Figure 3.
Advances in cell therapies, 3D printing, and bioprinting are addressing the challenges in engineering cardiovascular, bone, liver, skin, and neural tissues.
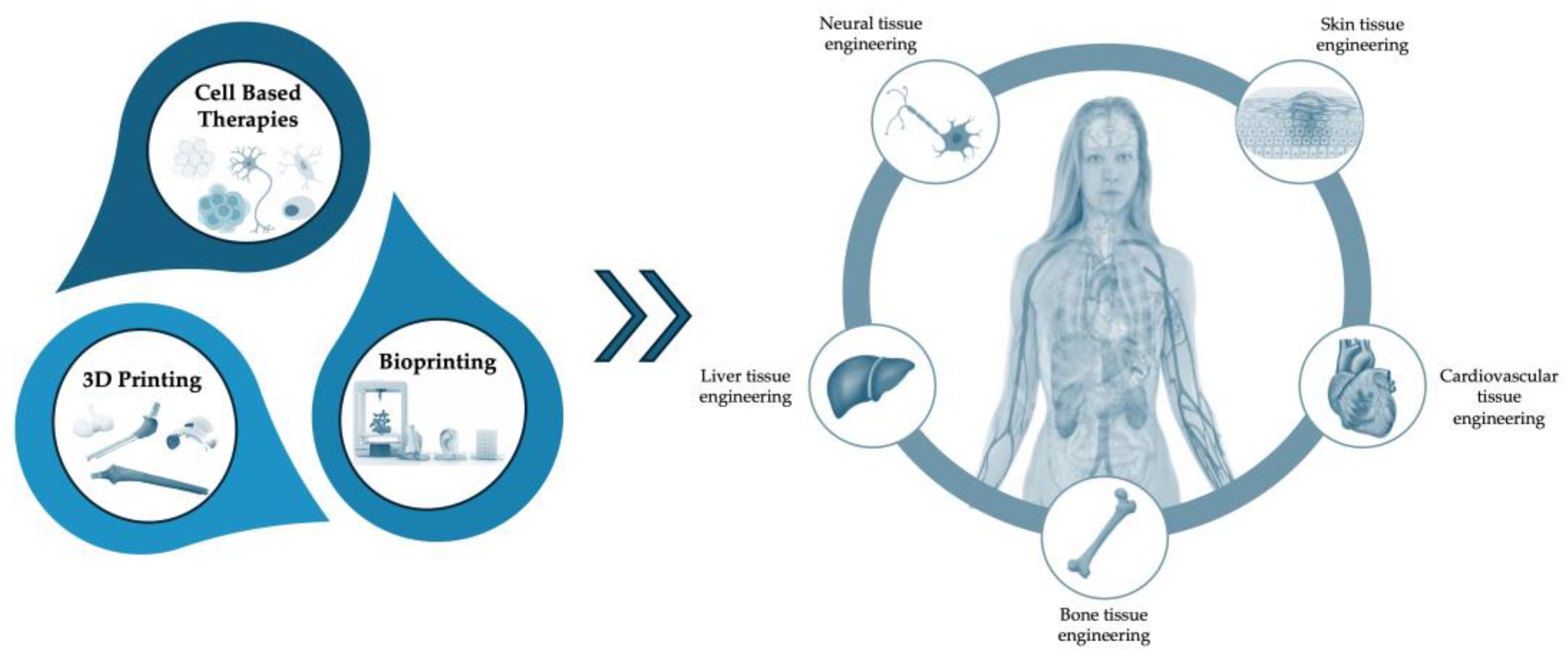
Figure 4.
Advances 3D printing/ bioprinting and cell therapies in engineering cardiovascular: A: Bioprinted cellularized construct incorporating human Umbilical Vein Endothelial Cells (hUVECs) and induced pluripotent stem cell-derived cardiomyocytes (iPSC-CMs), embedded in alginate and PEG-Fibrinogen (PF) (adapted from [166]); B: Printed patches composed of decellularized cardiac extracellular (cECM) matrix hydrogel and GelMA, for delivery of pediatric human cardiac progenitor cell (hCPC) (adapted from [167]); C: MSC-loaded gel patches with microchannels of controlled diameters. Three models tested: one without microchannels and two with nine evenly spaced microchannels, maintained at diameters of 500 μm and 1000 μm (adapted from [168]); D: A 3D-printed cellularized human heart is shown. (Left: CAD model of the human heart; Middle and right: The printed cardiac structure immersed in a supportive bath) (adapted from [169]); E: Printed fibrin scaffold using modified thermal inkjet printer (adapted from [170], Copyright (5839410409139) with permission from Elsevier).
Figure 4.
Advances 3D printing/ bioprinting and cell therapies in engineering cardiovascular: A: Bioprinted cellularized construct incorporating human Umbilical Vein Endothelial Cells (hUVECs) and induced pluripotent stem cell-derived cardiomyocytes (iPSC-CMs), embedded in alginate and PEG-Fibrinogen (PF) (adapted from [166]); B: Printed patches composed of decellularized cardiac extracellular (cECM) matrix hydrogel and GelMA, for delivery of pediatric human cardiac progenitor cell (hCPC) (adapted from [167]); C: MSC-loaded gel patches with microchannels of controlled diameters. Three models tested: one without microchannels and two with nine evenly spaced microchannels, maintained at diameters of 500 μm and 1000 μm (adapted from [168]); D: A 3D-printed cellularized human heart is shown. (Left: CAD model of the human heart; Middle and right: The printed cardiac structure immersed in a supportive bath) (adapted from [169]); E: Printed fibrin scaffold using modified thermal inkjet printer (adapted from [170], Copyright (5839410409139) with permission from Elsevier).
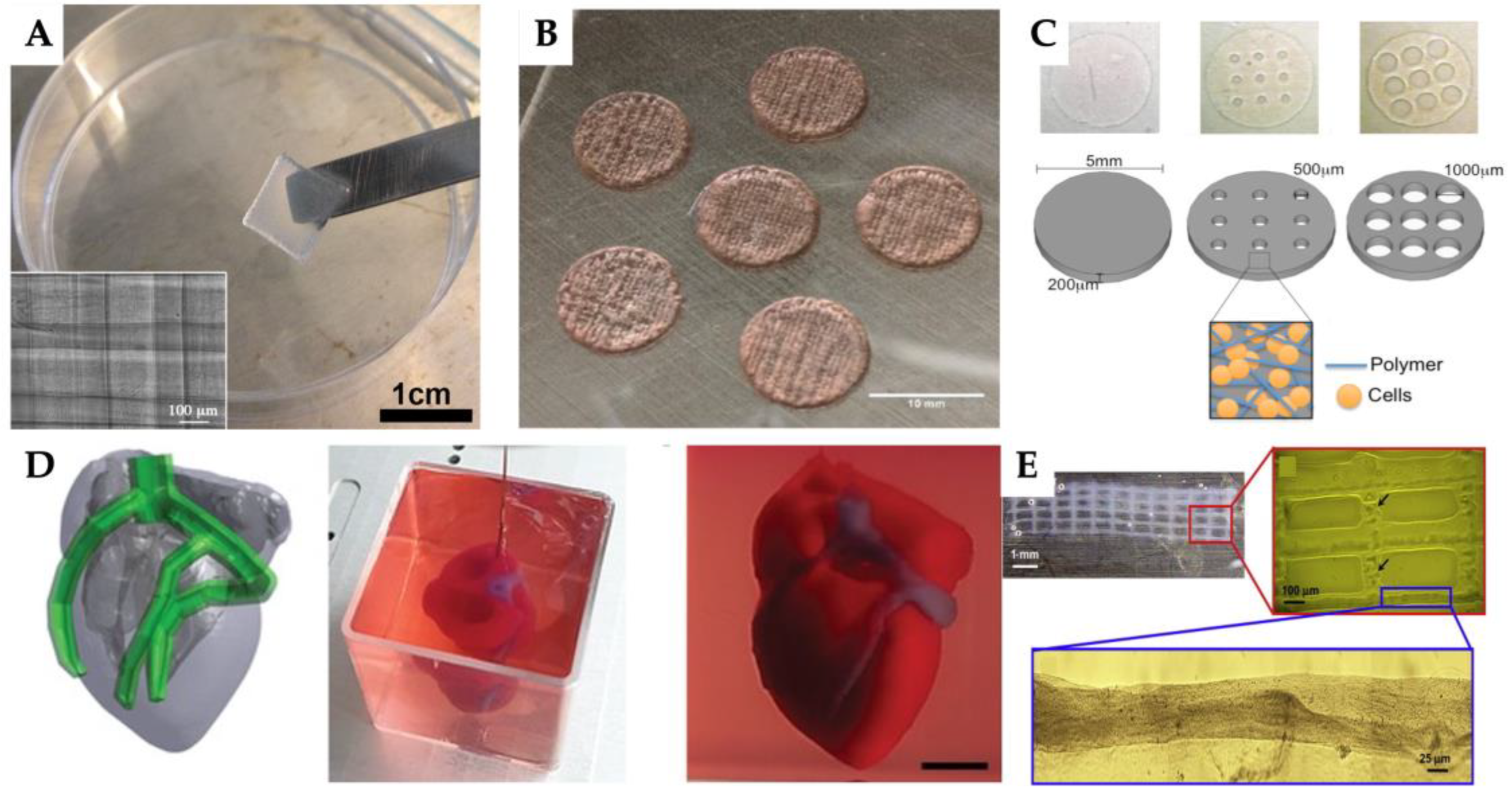
Figure 5.
Advances 3D printing/ bioprinting and cell therapies in bone tissue engineering: A: Ti6Al4V-based porous tantalum (Ta) scaffolds and scanning electron microscopy images (adapted from [191]); B: Newly formed bone within the scaffold was assesses through ex vivo micro-computed tomography(micro-CT) scans at 6 and 12 weeks (adapted from [192]); C: Visual representations of 3D-printed samples at different alginate concentrations, alginate alone or alginate with beta-tricalcium phosphate (β-TCP) (adapted from [193], Copyright (5841970729622) with permission from Elsevier); D: Bone scaffolds based on magnesium (Mg2+), strontium (Sr2+) and zinc (Zn2+)-substituted hydroxyapatite, as represented in the CAD model [194]).
Figure 5.
Advances 3D printing/ bioprinting and cell therapies in bone tissue engineering: A: Ti6Al4V-based porous tantalum (Ta) scaffolds and scanning electron microscopy images (adapted from [191]); B: Newly formed bone within the scaffold was assesses through ex vivo micro-computed tomography(micro-CT) scans at 6 and 12 weeks (adapted from [192]); C: Visual representations of 3D-printed samples at different alginate concentrations, alginate alone or alginate with beta-tricalcium phosphate (β-TCP) (adapted from [193], Copyright (5841970729622) with permission from Elsevier); D: Bone scaffolds based on magnesium (Mg2+), strontium (Sr2+) and zinc (Zn2+)-substituted hydroxyapatite, as represented in the CAD model [194]).
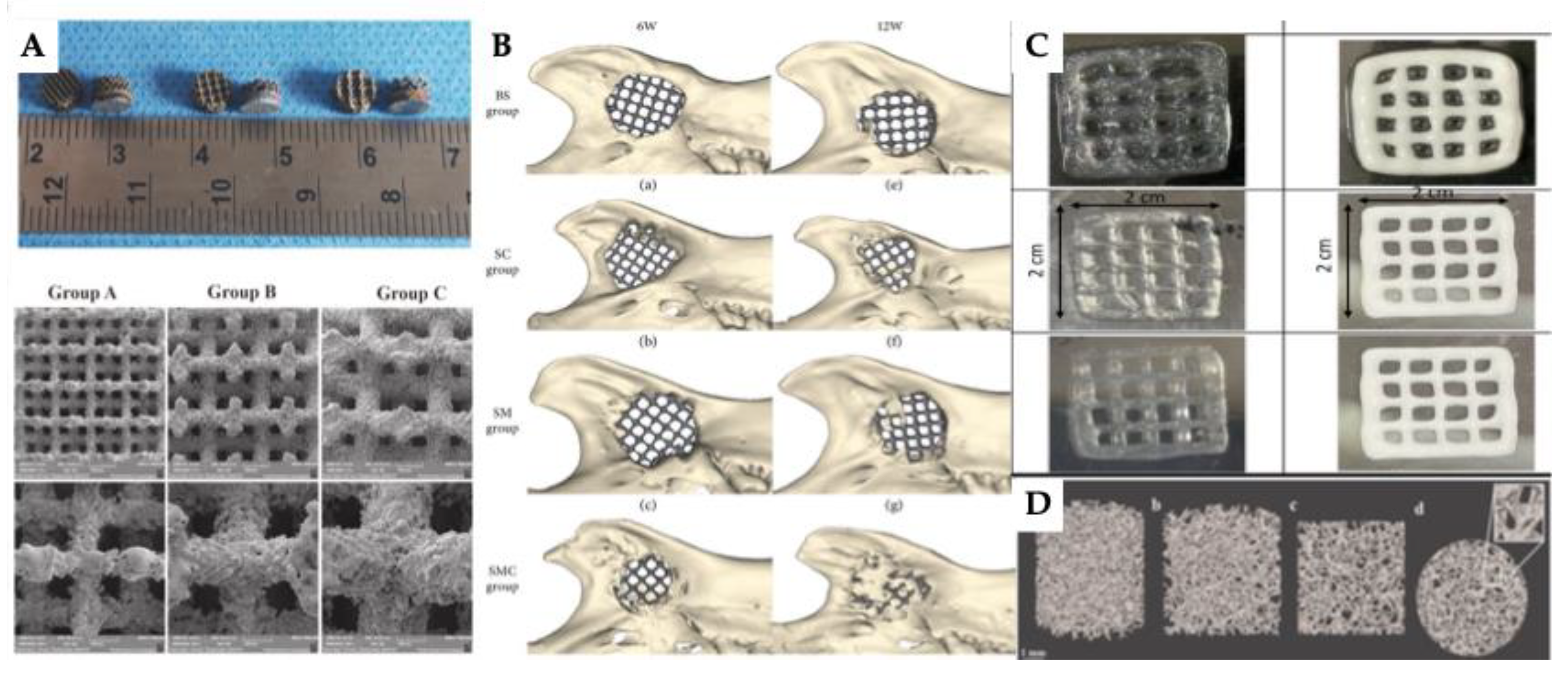
Figure 6.
Advances 3D printing/ bioprinting and cell therapies in liver tissue engineering: A: Human liver functions of 3D bioprinted hepatorganoids in mice. First column: Macroscopic observation of transplanted 3D bioprinted hepatorganoids. The vascular system is illustrated following the infusion of dextran. Secund and third column: The figure shows the dextran infusion with the formation of functional vessels and the red fluorescence showing the expression of human ALB at 4 weeks (adapted from [218]); B: The study details the production of patient-derived 3D bioprinted hepatocellular carcinoma models. Initially, HCC samples were obtained following post-surgical resection and subsequently processed into cell suspensions. These suspensions were then combined with sodium alginate and gelatin to create the bioink used for bioprinting. The images provided in the second line include: (1) the general appearance of the 3D bioprinted hepatocellular carcinoma model, (2) a light microscopy image showing the distribution of cells within the model, and (3) an in vitro view of the model, where live cells are marked in green and dead cells are marked in red (adapted from [219], Copyright (5842091348696) with permission from Elsevier); C: First line: schematic representation of the 3D printed scaffold, including strut spacing, nozzle diameter and angle between adjacent layers (90 or 60 degrees). Second line: large-scale 3D printed gelatin structure. Third line: cross-linked scaffolds and biopsy-punched samples (adapted from [220], Copyright (5842111318276) with permission from Elsevier); D: Construction of 3D-printed mCherry-HepG2 hepatic structures: (A) 3D bioprinting machine; (B) extrusion of alginate combined with mCherry-HepG2 cells through nozzle pressure; (C) layer-by-layer deposition of cross-linked structures in square arrays; (D) phase contrast microscopy showing a confluent monolayer of HepG2 cells; (E) fluorescence microscopy image of mCherry-HepG2 cells within the alginate scaffold; (F) multilayered mCherry-HepG2 cells solidified and stacked repetitively (adapted from [221]); E: Schematic representation of the liver lobule-mimetic honeycomb structure, including top and side views of the embedded-printed scaffolds (adapted from [222]).
Figure 6.
Advances 3D printing/ bioprinting and cell therapies in liver tissue engineering: A: Human liver functions of 3D bioprinted hepatorganoids in mice. First column: Macroscopic observation of transplanted 3D bioprinted hepatorganoids. The vascular system is illustrated following the infusion of dextran. Secund and third column: The figure shows the dextran infusion with the formation of functional vessels and the red fluorescence showing the expression of human ALB at 4 weeks (adapted from [218]); B: The study details the production of patient-derived 3D bioprinted hepatocellular carcinoma models. Initially, HCC samples were obtained following post-surgical resection and subsequently processed into cell suspensions. These suspensions were then combined with sodium alginate and gelatin to create the bioink used for bioprinting. The images provided in the second line include: (1) the general appearance of the 3D bioprinted hepatocellular carcinoma model, (2) a light microscopy image showing the distribution of cells within the model, and (3) an in vitro view of the model, where live cells are marked in green and dead cells are marked in red (adapted from [219], Copyright (5842091348696) with permission from Elsevier); C: First line: schematic representation of the 3D printed scaffold, including strut spacing, nozzle diameter and angle between adjacent layers (90 or 60 degrees). Second line: large-scale 3D printed gelatin structure. Third line: cross-linked scaffolds and biopsy-punched samples (adapted from [220], Copyright (5842111318276) with permission from Elsevier); D: Construction of 3D-printed mCherry-HepG2 hepatic structures: (A) 3D bioprinting machine; (B) extrusion of alginate combined with mCherry-HepG2 cells through nozzle pressure; (C) layer-by-layer deposition of cross-linked structures in square arrays; (D) phase contrast microscopy showing a confluent monolayer of HepG2 cells; (E) fluorescence microscopy image of mCherry-HepG2 cells within the alginate scaffold; (F) multilayered mCherry-HepG2 cells solidified and stacked repetitively (adapted from [221]); E: Schematic representation of the liver lobule-mimetic honeycomb structure, including top and side views of the embedded-printed scaffolds (adapted from [222]).
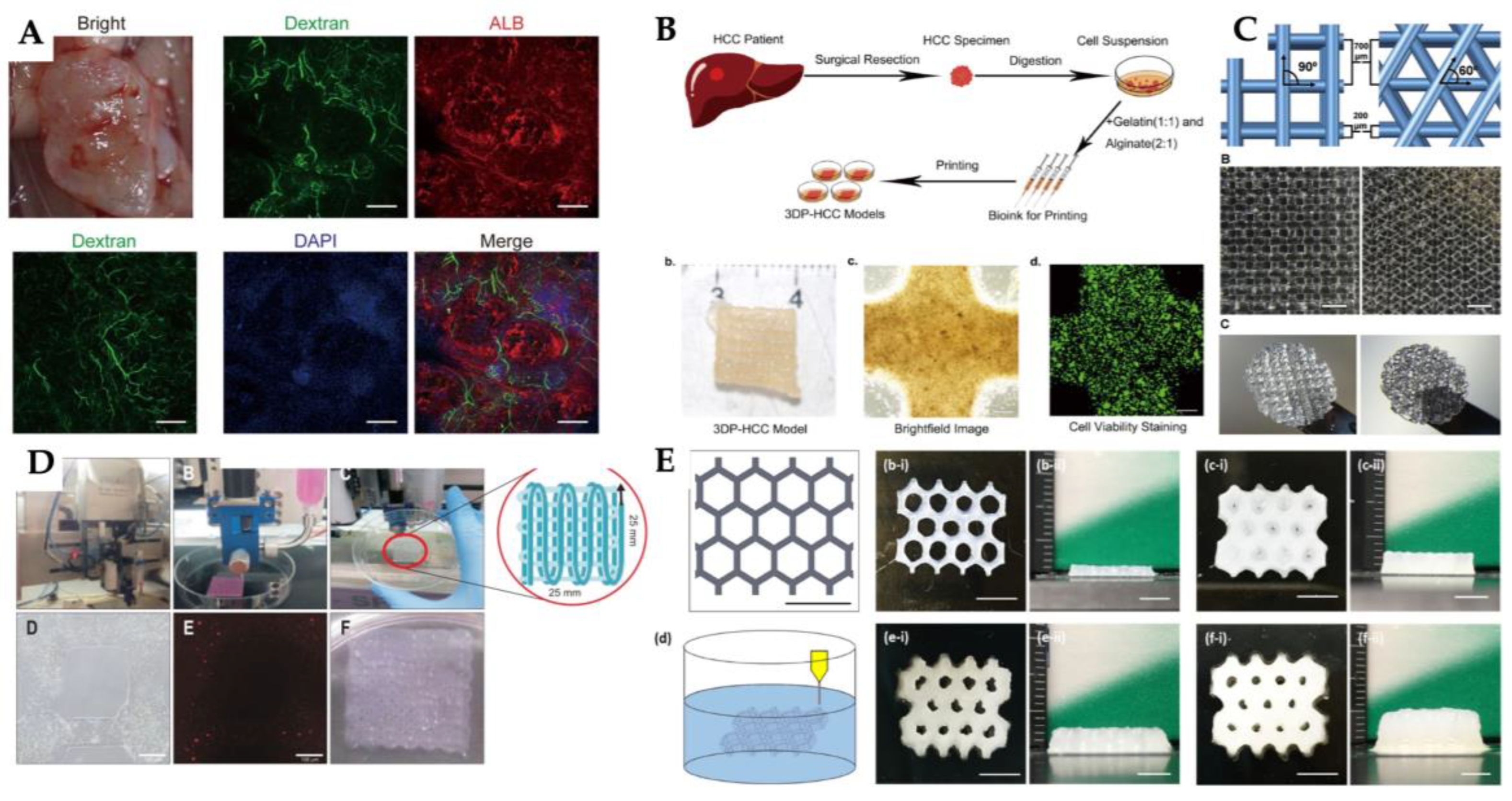
Figure 7.
Advances 3D printing/ bioprinting and cell therapies in skin tissue engineering: A: The image shows the printed epidermal layer (red) composed of alginate-gelatin hydrogel, and the dermal layer (green) made of phosphosilicate calcium bioglass (PSC)-alginate-GelMA hydrogel embedded with hUVECs and hUCMSCs (adapted from [233], Copyright (5842131198782) with permission from Elsevier); B: Diagram overview of the produced structure design: diagram illustration of the CAD model; illustration of human skin anatomy, with the dermis and epidermis; approach for designing the dual-layered 3D printed structure; dimensions of the layers: the dermal layer consists of 10 layers, while the epidermal layer has 8 filaments, oriented perpendicularly with an interfilament spacing of 0.75 mm and a Z-axis increment of 0.08 mm per layer; microscopic view of the printed structure; dual-layered 10 × 10 mm 3D printed structure in culture; and the mechanically printed structure is noted for its optimal handling properties, which facilitate thorough characterization and assessment (adapted from [239], Copyright (5842131492259) with permission from Elsevier); C: Assessment of the printability of acellular dermal matrix and GelMA hydrogels by fabricating identical structural patterns using these materials (adapted from [240], Copyright (5842140280407) with permission from Elsevier); D: Macrographs and scanning electron microscopy (SEM) images of PCL-AMX, SG-rhEGF, and PCL-AMX-SG-rhEGF structures (adapted from [241], Copyright (5842140587126) with permission from Elsevier).
Figure 7.
Advances 3D printing/ bioprinting and cell therapies in skin tissue engineering: A: The image shows the printed epidermal layer (red) composed of alginate-gelatin hydrogel, and the dermal layer (green) made of phosphosilicate calcium bioglass (PSC)-alginate-GelMA hydrogel embedded with hUVECs and hUCMSCs (adapted from [233], Copyright (5842131198782) with permission from Elsevier); B: Diagram overview of the produced structure design: diagram illustration of the CAD model; illustration of human skin anatomy, with the dermis and epidermis; approach for designing the dual-layered 3D printed structure; dimensions of the layers: the dermal layer consists of 10 layers, while the epidermal layer has 8 filaments, oriented perpendicularly with an interfilament spacing of 0.75 mm and a Z-axis increment of 0.08 mm per layer; microscopic view of the printed structure; dual-layered 10 × 10 mm 3D printed structure in culture; and the mechanically printed structure is noted for its optimal handling properties, which facilitate thorough characterization and assessment (adapted from [239], Copyright (5842131492259) with permission from Elsevier); C: Assessment of the printability of acellular dermal matrix and GelMA hydrogels by fabricating identical structural patterns using these materials (adapted from [240], Copyright (5842140280407) with permission from Elsevier); D: Macrographs and scanning electron microscopy (SEM) images of PCL-AMX, SG-rhEGF, and PCL-AMX-SG-rhEGF structures (adapted from [241], Copyright (5842140587126) with permission from Elsevier).
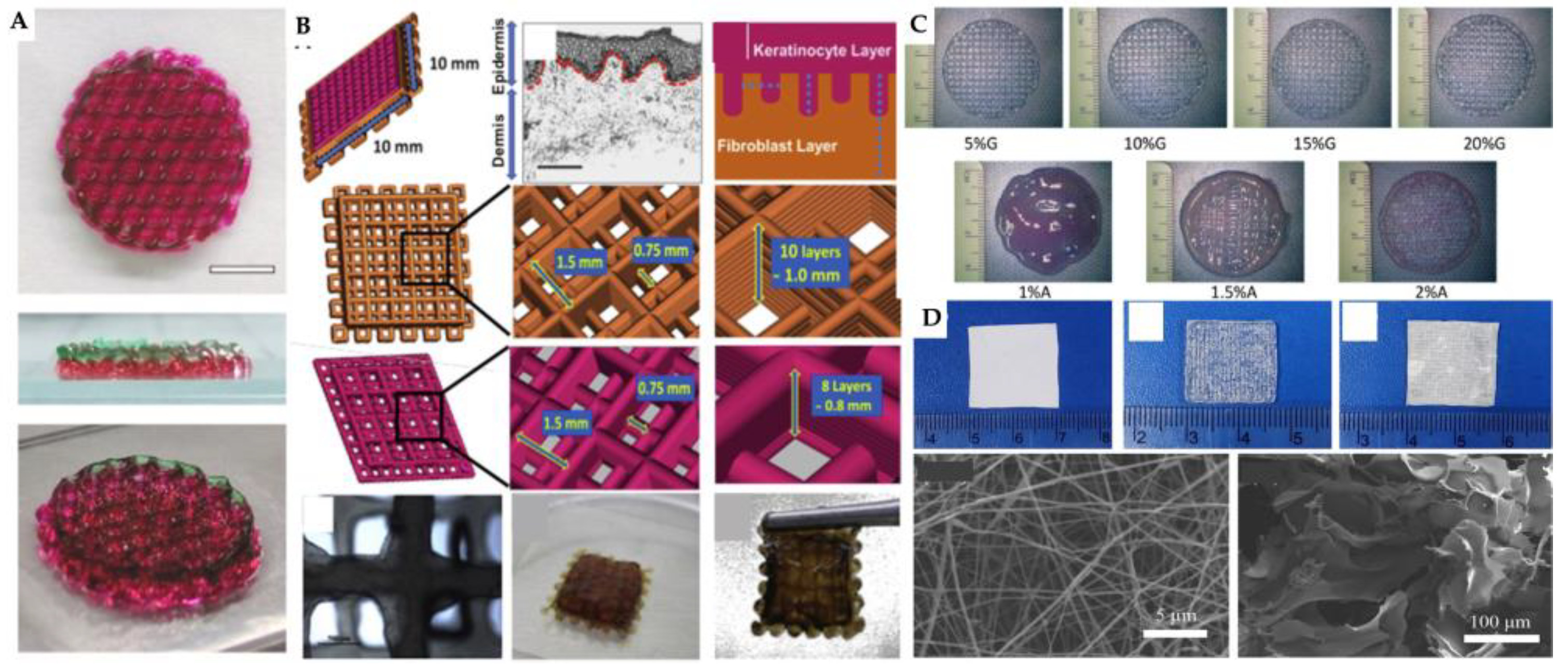
Figure 8.
Advances 3D printing/ bioprinting and cell therapies in neural tissue engineering: A: Evaluation of bioink printability was conducted for various compositions of methacrylated silk fibroin and methacrylated silk fibroin/pectin hydrogels. Optical microscopy images were captured to examine the morphology, while a live/dead assay was performed on L929 cells embedded within 3D bioprinted constructs using bioinks composed of 10% methacrylated silk fibroin/0.5% pectin and 15% methacrylated silk fibroin/0.5% pectin (adapted from [259], Copyright (5842151229827) with permission from Elsevier); B: Characterization of the scaffolds was conducted as follows: (A) Normal spinal cord tissue; (B) Decellularized spinal cord scaffold; (C) Polycaprolactone (PCL) microfiber structure; (D) Overall morphology of the 3D-bioprinted composite scaffold; (E–H) Microstructure of scaffolds visualized through scanning electron microscopy (SEM). The SEM images of both the scaffold alone and the scaffold combined with OMT reveal parallel microfibers of consistent thickness, with hydrogels adhering to the fibers. The interior of the scaffold exhibited uniform and densely packed pores, which are conducive to neural stem cell (NSC) growth and efficient nutrient exchange (adapted from [260]); C: Schematic representation of the experimental procedure for spinal cord injury repair utilizing stereolithography apparatus (SLA) to create neural scaffolds. (a) Computer-aided design (CAD) to develop the scaffold model corresponding to the injured region for bioprinting; (b) Construction of neural scaffolds employing the SLA technique; (c) Utilization of the fabricated scaffolds for in vitro cell culture; (d) Assessment of the functionality of scaffolds following a period of in vitro cultivation (adapted from [261], Copyright (5842160814781) with permission from Elsevier). .
Figure 8.
Advances 3D printing/ bioprinting and cell therapies in neural tissue engineering: A: Evaluation of bioink printability was conducted for various compositions of methacrylated silk fibroin and methacrylated silk fibroin/pectin hydrogels. Optical microscopy images were captured to examine the morphology, while a live/dead assay was performed on L929 cells embedded within 3D bioprinted constructs using bioinks composed of 10% methacrylated silk fibroin/0.5% pectin and 15% methacrylated silk fibroin/0.5% pectin (adapted from [259], Copyright (5842151229827) with permission from Elsevier); B: Characterization of the scaffolds was conducted as follows: (A) Normal spinal cord tissue; (B) Decellularized spinal cord scaffold; (C) Polycaprolactone (PCL) microfiber structure; (D) Overall morphology of the 3D-bioprinted composite scaffold; (E–H) Microstructure of scaffolds visualized through scanning electron microscopy (SEM). The SEM images of both the scaffold alone and the scaffold combined with OMT reveal parallel microfibers of consistent thickness, with hydrogels adhering to the fibers. The interior of the scaffold exhibited uniform and densely packed pores, which are conducive to neural stem cell (NSC) growth and efficient nutrient exchange (adapted from [260]); C: Schematic representation of the experimental procedure for spinal cord injury repair utilizing stereolithography apparatus (SLA) to create neural scaffolds. (a) Computer-aided design (CAD) to develop the scaffold model corresponding to the injured region for bioprinting; (b) Construction of neural scaffolds employing the SLA technique; (c) Utilization of the fabricated scaffolds for in vitro cell culture; (d) Assessment of the functionality of scaffolds following a period of in vitro cultivation (adapted from [261], Copyright (5842160814781) with permission from Elsevier). .
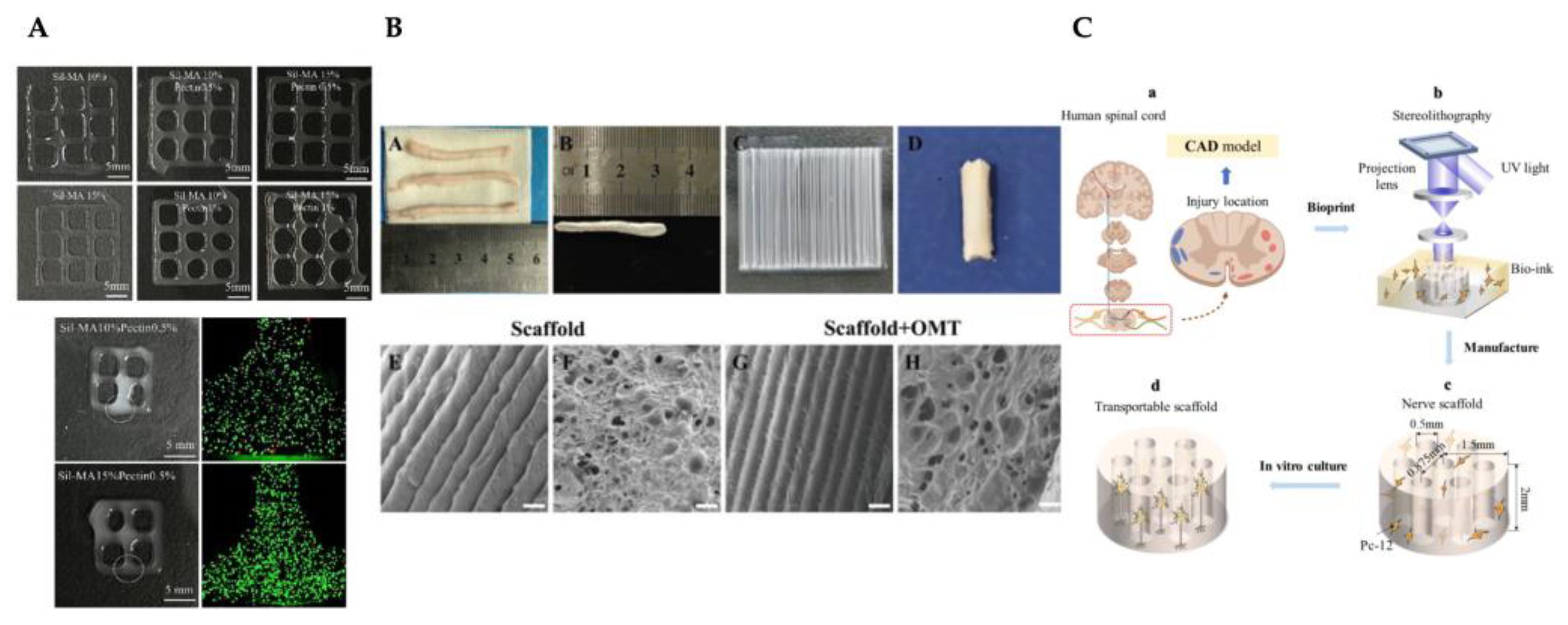

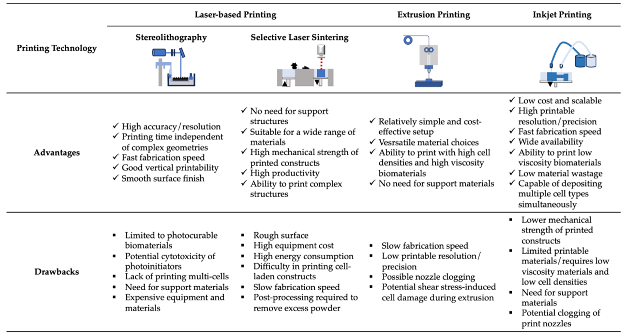
Table 2.
Recent advances in 3D printing/bioprinting and cellular therapies for cardiovascular tissue engineering. Abbreviations: human microvascular endothelial cells (hMVECs); mouse embryonic fibroblasts (mEFs); human cardiac-derived cardiomyocyte progenitor cells (hCMPCs); human umbilical vein endothelial cells (hUVECs); cardiomyocytes (H9c2 cells); induced pluripotent stem cell-derived cardiomyocytes (iCMs); human cardiac fibroblasts (CFs); human coronary artery endothelial cells (hCAECs); gelatin methacrylate (GelMA); decellularized cardiac extracellular matrix hydrogel (cECM); human cardiac progenitor cells (hCPCs); heart tissue-derived extracellular matrix (hdECM); neonatal rat cardiomyocytes (NRCMs); poly(ethylene glycol)-fibrinogen (PF); induced pluripotent stem cell-derived cardiomyocytes (iPSC-CMs); digital light processing (DLP); poly (glycerol sebacate) (PGS); poly (ℇ-caprolactone) (PCL); fused deposition modeling (FDM); not applicable (n/a); stereolithographic assembly (SLA); poly(ethylene glycol) dimethacrylate (PEGDMA); bone marrow-derived mesenchymal stem cells (BMSCs); mesenchymal stem/stromal cell (MSC); hyaluronic acid (HA); human embryonic stem cells (hESCs); early vascular cells (EVCs); hyaluronic acid glycidyl methacrylate (HAGM); neonatal rat cardiomyocytes (NRCMs).
Table 2.
Recent advances in 3D printing/bioprinting and cellular therapies for cardiovascular tissue engineering. Abbreviations: human microvascular endothelial cells (hMVECs); mouse embryonic fibroblasts (mEFs); human cardiac-derived cardiomyocyte progenitor cells (hCMPCs); human umbilical vein endothelial cells (hUVECs); cardiomyocytes (H9c2 cells); induced pluripotent stem cell-derived cardiomyocytes (iCMs); human cardiac fibroblasts (CFs); human coronary artery endothelial cells (hCAECs); gelatin methacrylate (GelMA); decellularized cardiac extracellular matrix hydrogel (cECM); human cardiac progenitor cells (hCPCs); heart tissue-derived extracellular matrix (hdECM); neonatal rat cardiomyocytes (NRCMs); poly(ethylene glycol)-fibrinogen (PF); induced pluripotent stem cell-derived cardiomyocytes (iPSC-CMs); digital light processing (DLP); poly (glycerol sebacate) (PGS); poly (ℇ-caprolactone) (PCL); fused deposition modeling (FDM); not applicable (n/a); stereolithographic assembly (SLA); poly(ethylene glycol) dimethacrylate (PEGDMA); bone marrow-derived mesenchymal stem cells (BMSCs); mesenchymal stem/stromal cell (MSC); hyaluronic acid (HA); human embryonic stem cells (hESCs); early vascular cells (EVCs); hyaluronic acid glycidyl methacrylate (HAGM); neonatal rat cardiomyocytes (NRCMs).
| 3D printing technology | Biomaterials | Cellular Therapies | Application | Outcomes | Reference |
|---|---|---|---|---|---|
| Inkjet Printing | Fibrin gel | hMVECs | Microvasculature construction | The construction promoted hMVEC proliferation and microvasculature formation. | [170] |
| Extrusion 3D Bioprinting | NovoGel | mEFs | Aortic tissue construct | Support structure and mEF were successfully printed with the self-supporting approach. | [171] |
| Alginate | hCMPCs | Construction with cardiogenic potential for use in vitro and in vivo | The printed hCMPCs were able to migrate in the alginate matrix while maintaining their functional properties. | [172] | |
| Alginate/ Gelatin | hUVECs, H9c2 cells | Cardiac tissue engineering | A new angular structure that replicates the alignment of cardiac fibers demonstrates excellent cell viability for both hUVECs and H9c2 cells, substantial mechanical strength, and appropriate characteristics for dilation and degradation. | [173] | |
| Alginate/Gelatin | iCMs, CFs, hCAECs | Cardiac tissue patches | Epicardial transplantation using 3D bioprinted patches based on AlgGel resulted in improved cardiac function. | [174] | |
| GelMA, Alginate | hUVECs | Endothelialized myocardial tissues | New method for generating endothelialised fabricated organoids. | [175] | |
| GelMA | cECM, hCPCs | Cardiac tissue patches | Cardiac patches printed with cECM and GelMA demonstrated significantly higher viability of hCPCs and exhibited a 30-fold increase in the gene expression of cardiogenic genes related to patches made exclusively of GelMA. In vivo studies on rats revealed vascularization over a period of 14 days. | [167] | |
| Collagen | hdECM, NRCMs | Cardiac tissue model | It promoted early differentiation and improved the maturation of cardiomyocytes in hdECM. | [176] | |
| 3D bioprinting with microfluidic printing head | Alginate, PF | iPSC-CMs, hUVECs | Vascularized cardiac tissue | The 3D cardiac tissue composed of iPSC-CMs presents a high orientation index due to the distinct geometries and vascular-like formations generated by hUVECs. | [166] |
| DLP-based 3D printing | PGS/PCL/Gelatin | hUVECs | Heart valve substitute | A crosslinked 3D valve analog with elastomeric characteristics. | [177] |
| FDM 3D printing | PGS/PCL | n/a | Myocardial remodeling | It improved and preserved heart function. |
[178] |
| SLA | PEGDMA | BMSCs | Gel patch to damaged cardiac tissue | Application of the MSC-laden microchanneled gel patch resulted in enhanced ejection fraction, fractional shortening, and stroke volume. | [168] |
| Pneumatic-extrusion | Fibrinogen, gelatin, aprotinin, HA | hESCs-derived EVCs | Cardiac tissues | Spheroids derived from hESC-derived endothelial and EVCs offer greater potential for engineering complex vascular structures compared to single cells. | [179] |
| Micro-continuous optical printing | GelMA, HAGM | hiPSC-CMs | Cardiac micro-tissue (for drug testing) | The micro-tissue exhibited a well-organized sarcomere structure and a marked upregulation in the expression of maturity markers. | [180] |
| Pneumatic 3D printing | Fibrinogen, gelatin, aprotinin, glycerol, HA | NRCMs | Functional and contractile cardiac tissue constructs | They fabricated a structured construct exhibiting physiological and biomechanical properties comparable to those of native cardiac tissue. | [181] |
Table 3.
Recent developments in 3D printing/bioprinting and cellular therapies for bone tissue engineering. Abbreviations: selective laser melting (SLM); bone marrow-derived mesenchymal stem cells (BMSCs); beta-tricalcium phosphate (β-TCP); gelatin methacrylate (GelMA); Xonotlite (Sr-CSH); poly(lactic-co-glycolic acid) (PLGA); bone morphogenetic protein 2 (BMP-2); human umbilical cord mesenchymal stem cells (hUCMSCs); alkaline phosphatase (ALP); hydroxyapatite (HAp); Magnesium (Mg2+); Strontium (Sr2+); Zinc (Zn2+); not applicable (n/a); polycaprolactone (PLC); amorphous calcium phosphate (ACP); dental pulp stem cells (DPSCs); diacrylate poly(ethylene glycol) (PEGDA); digital light processing (DLP); tantalum (Ta); rat bone marrow mesenchymal stem cells (r-BMSCs); diamond (DO); rhombic dodecahedron (RD); iron (Fe) ; manganese (Mn); calcium (Ca); magnesium (Mg); titanium (Ti); niobium (Nb); zirconium (Zr); stromal cells from apical papilla (SCAPs); human umbilical vein endothelial cells (hUVECs).
Table 3.
Recent developments in 3D printing/bioprinting and cellular therapies for bone tissue engineering. Abbreviations: selective laser melting (SLM); bone marrow-derived mesenchymal stem cells (BMSCs); beta-tricalcium phosphate (β-TCP); gelatin methacrylate (GelMA); Xonotlite (Sr-CSH); poly(lactic-co-glycolic acid) (PLGA); bone morphogenetic protein 2 (BMP-2); human umbilical cord mesenchymal stem cells (hUCMSCs); alkaline phosphatase (ALP); hydroxyapatite (HAp); Magnesium (Mg2+); Strontium (Sr2+); Zinc (Zn2+); not applicable (n/a); polycaprolactone (PLC); amorphous calcium phosphate (ACP); dental pulp stem cells (DPSCs); diacrylate poly(ethylene glycol) (PEGDA); digital light processing (DLP); tantalum (Ta); rat bone marrow mesenchymal stem cells (r-BMSCs); diamond (DO); rhombic dodecahedron (RD); iron (Fe) ; manganese (Mn); calcium (Ca); magnesium (Mg); titanium (Ti); niobium (Nb); zirconium (Zr); stromal cells from apical papilla (SCAPs); human umbilical vein endothelial cells (hUVECs).
| 3D printing technology | Biomaterials | Cellular Therapies | Application | Outcomes | Reference |
|---|---|---|---|---|---|
| SLM | Ti6Al4V, Matrigel | BMSCs | Mandibular bone defect reconstruction | Scaffold-Matrigel-BMSCs with enhanced bioactivity and mechanical properties for bone repair. | [192] |
| 3D bioprinting | Alginate, β-TCP | MG-63 fibroblasts | Bone defects | 10 % alginate/β-TCP improved cells proliferation and alkaline phosphatase activity | [193] |
| GelMA, Sr-CSH | BMSCs | Critical-size bone defects | GelMA-Sr–CSH scaffolds indicated complete regeneration of critical-size bone defects. | [195] | |
| Alginate, PLGA | BMP-2, hUCMSCs | Bone tissue engineering | hUCMSCs printing with Alginate/ BMP-2 loaded into PLGA improved osteogenesis of the printed cells as demonstrated by higher rates of ALP activity, calcium deposition, expression of genes associated with osteogenesis, and mineralization when compared with controls. | [196] | |
| Vat photopolymerization | HA multi-substituted with Mg2+, Sr2+, and Zn2+ ions | n/a | Cancellous bone defects | It is a suitable technique for manufacturing highly complex trabecular structures for bone regeneration. | [194] |
| Extrusion 3D Bioprinting | PCL, ACP | n/a | Bone defects | It presented suitable properties, such as compressive strength, pore size, rigidity and repeatability (related to the interconnectivity between the pores). | [50] |
| GelMA | DPSCs | Bone regeneration | DPSCs in GelMA bioprinted presented better osteogenic differentiation potential | [197] | |
| PCL, HAp, PEGDA | DPSCs | Bone regeneration | PCL/HANp/PEGDA revealed hydrophilic properties, suitable mechanical performance and significantly higher cell viability than the other groups. | [188] | |
| DLP-based bioprinting | GelMA, dextran emulsion | BMSCs | Bone regeneration | It promoted the proliferation, migration, dissemination and differentiation of encapsulated BMSCs. | [198] |
| Laser Powder Bed Fusion | Ti6Al4V, Ta | r-BMSCs | Orthopedic clinical applications | It works well with the mechanics, supports the adhesion, growth, and development of r-BMSCs into osteoblasts. | [191] |
| PCL, HAp | BMSCs | Human mandibular trabecular bone regeneration | The biodegradable structures (with DO and RD elementary unit cell geometry) demonstrated their suitability as supports for bone regeneration. | [199] | |
| Binder-jetting | Fe-Mn-Ca, Mg | n/a | Cranio-maxillofacial bone defects | The Fe-Mn and Fe-Mn-1Ca structures confirmed higher degradation from the addition of Ca to the 3D printed structures and good cytocompatibility. | [200] |
| Laser Directed Energy Deposition | Commercially pure Ti | n/a | Dental restoration | Commercially pure grade 4 titanium produced by Laser Directed Energy Deposition has a higher mechanical response than other techniques, which can be attributed to the modification of the microstructure inherent in the process. | [201] |
| Ti-Nb, Ti-Zr-Nb | n/a | Orthopedic and dental applications | Ti-35Zr-25Nb presented a lower modulus of elasticity, higher hardness, good corrosion resistance and in vitro biocompatibility. | [202] | |
| Sheet lamination | AISI 302 | n/a | Bone regeneration | The scaffold prototype was designed and fabricated with the parameters selected through experimental tests and using the mathematical model. | [203] |
| Laser-assisted bioprinting | BioRoot RCS® | SCAPs, hUVECs | Bone regeneration | The application of laser-assisted bioprinting techniques with this ink failed to provide complete bone repair, whether the SCAPs were printed in direct proximity or not. | [204] |
Table 4.
Recent advances in 3D printing/bioprinting and cellular therapies for liver tissue engineering. Abbreviations: digital light processing (DLP); methacrylated gelatin (GelMA); decellularized extracellular matrix (dECM); human-induced hepatocyte (hiHep cells); hyaluronic acid (HA); primary mouse hepatocytes (PMHs); human induced pluripotent stem cells (hiPSCs); human embryonic stem cells (hESCs); human pluripotent stem cells (hPSCs); induced pluripotent stem cells (iPSC); 3D bioprinted hepatorganoids (3DP-HOs); hepatocellular carcinoma (HCC); poly (ℇ-caprolactone) (PCL); human bone marrow-derived mesenchymal stem cells (BMMSCs); human hepatocellular carcinoma (hepG2); cellulose nanocrystals (CNCs); bioink with alginate (1%), cellulose nanocrystal (3%), and gelatin methacryloyl (5%) (135ACG); undifferentiated hepatocyte cell line (HUH7); primary rat hepatocytes cells (PrHCs); human umbilical vein endothelial cells (hUVECs); human lung fibroblasts (hLFs); human extracellular matrix (hECM); human hepatic stellate cell line (L × 2); primary fetal activated hepatic stellate cells (aHSC).
Table 4.
Recent advances in 3D printing/bioprinting and cellular therapies for liver tissue engineering. Abbreviations: digital light processing (DLP); methacrylated gelatin (GelMA); decellularized extracellular matrix (dECM); human-induced hepatocyte (hiHep cells); hyaluronic acid (HA); primary mouse hepatocytes (PMHs); human induced pluripotent stem cells (hiPSCs); human embryonic stem cells (hESCs); human pluripotent stem cells (hPSCs); induced pluripotent stem cells (iPSC); 3D bioprinted hepatorganoids (3DP-HOs); hepatocellular carcinoma (HCC); poly (ℇ-caprolactone) (PCL); human bone marrow-derived mesenchymal stem cells (BMMSCs); human hepatocellular carcinoma (hepG2); cellulose nanocrystals (CNCs); bioink with alginate (1%), cellulose nanocrystal (3%), and gelatin methacryloyl (5%) (135ACG); undifferentiated hepatocyte cell line (HUH7); primary rat hepatocytes cells (PrHCs); human umbilical vein endothelial cells (hUVECs); human lung fibroblasts (hLFs); human extracellular matrix (hECM); human hepatic stellate cell line (L × 2); primary fetal activated hepatic stellate cells (aHSC).
| 3D printing technology | Biomaterials | Cellular Therapies | Application | Outcomes | Reference |
|---|---|---|---|---|---|
| DLP bioprinting | GelMA | dECM, hiHep cells | Hepatic functional restoration | It was found that the addition of hepatic dECM to the biotints improved printing capacity and cell viability. Furthermore, hiHep cells exhibited increased spreading and enhanced functional performance within the liver microtissue. | [223] |
| 3D bioprinting | HA, alginate, gelatin | dECM, PMHs | Functional in vitro liver tissue models | The inclusion of dECM enhanced the hepatic function of hepatocyte spheroids. | [224] |
| Alginate | hiPSCs, hESCs | Mini-liver tissue structures | Using this approach, researchers have been successfully bioprinting hPSCs whilst preserving their pluripotency or directing their differentiation towards specific cell types. | [225] | |
| NovoGel 2.0 | iPSC-derived hepatocyte | Functional in vitro liver tissue models | It demonstrated a method for rapidly fabricating multicellular 3D liver constructs in a multi-well format, displaying critical liver functions including albumin synthesis, cholesterol biosynthesis, production of fibrinogen and transferrin, and inducible activities of CYP 1A2 and CYP 3A4. | [210] | |
| Alginate | HepaRG cells | Hepatorganoids: Liver tissue model | The implantation of 3DP-HOs markedly enhanced the survival rates of mice experiencing liver failure. | [218] | |
| Gelatin, Alginate | Primary HCC cell lines | In vitro models for patient-specific drug screening for HCC | The generated models preserved the key characteristics of the original HCCs, including consistent biomarker expression, stable genetic alterations, and maintained expression profiles. | [219] | |
| PCL | dECM, BMMSCs, HepG2 | 3D cell printing-based liver tissue engineering | The liver dECM bioink proved to have excellent printing capacity without significant cell death during the process. It also improved stem cell differentiation and HepG2 cell function. | [226] | |
| Alginate | HepG2 | Reconstruction of liver tissues or organs | The cells proliferated well in the scaffold and the expression of liver-specific genes increased. | [221] | |
| GelMA, alginate, CNC | NIH/3T3 fibroblasts, hepG2 | Bicellular liver lobule-mimetic structures | NIH/3T3 cells proliferated effectively within the rigid 135ACG matrix and aligned along the boundary between 135ACG and GelMA, demonstrating durotaxis. In contrast, HepG2 cells formed spheroids exclusively within the softer GelMA matrix. The 3D co-culture of HepG2 and NIH/3T3 cells exhibited increased albumin secretion, indicating that the enhancement in liver cell functionality may be due to soluble factors in the environment. | [222] | |
| Pneumatic extrusion | Gelatin | HUH7 | Model hepatocyte system | It has been proved that the scaffold geometry, using well-defined gelatine constructs, modulates hepatocyte function. | [220] |
| PCL, collagen | PrHCs, hUVECs, hLFs | Liver tissue engineering | The 3D cell printed construct comprising a capillary-like network enhanced the protein secretion and metabolism of PrHCs. It demonstrated a great potential for functional liver tissue regeneration. | [227] | |
| Alginate, gelatin | hECM, human HepaRG liver cells | 3D liver model for infection and transduction studies | It was demonstrated that supplementing an alginate/gelatin bioink with hECM enhanced cell viability and hepatic metabolic function in a 3D-printed humanized liver model. | [228] | |
| Extrusion bioprinting | Alginate | HepG2/C3A, EA.hy926 | Hepatic lobules within a highly vascularized construct | The successful bioprinting of hepatic lobules with a complex, highly vascularized architecture resulted in enhanced albumin secretion, urea production, and elevated levels of albumin, MRP2, and CD31 proteins. Additionally, cytochrome P450 enzyme activity was significantly greater in these constructs compared to other groups. | [229] |
| HA, Collagen I | L × 2, aHSC | 3D bioprinted liver model | The formulations seemed to facilitate cell viability, in line with the biomatrices used. The bioinks incorporating primary human hepatocytes were evaluated over two weeks, demonstrating sustained production of urea and albumin while showing a responsive reaction to acetaminophen. | [230] | |
| Alginate, CNCs | Fibroblasts, Human hepatoma cells | Liver-mimetic structures | This bioink showed excellent shear-thinning property, extrudability, and shape fidelity after the deposition. The bioprinting caused minimal cell damage. | [231] |
Table 5.
Recent advances in 3D printing/bioprinting and cellular therapies for skin tissue engineering. Abbreviations: strontium silicate (SS); matrix hydrogel with 2.8% of gellan gum, 1.6% of alginate, and 2.8% of methyl cellulose (GAM); human dermal fibroblasts (hDFs); human umbilical vascular endothelial cells (hUVECs); murine umbilical vein endothelial cells (MUVECs); dextran (Dex); vascular endothelial (VEGF); gelatin (Gel); keratin (Kr); not applicable (n/a); bi-layer (BL); poly (ℇ-caprolactone) (PCL); amoxicillin (AMX); external human epidermal growth factor (rhEGF); Digital light processing (DLP); gelatin methacrylate (GelMA), hyaluronic acid (HA); N-(2-aminoethyl)-4-(4-(hydroxymethyl)-2-methoxy-5-nitrosophenoxy) butanamide (NB); lithium phenyl-2,4,6-trimethylbenzoylphosphinate (LAP); human skin fibroblasts (hSFs); silk fibroin (SF); 4-arm polyethylene glycol acrylate (PEG4A); platelet-rich plasma (PRP); dermal fibroblasts (DFs); epidermal stem cells (ESCs); acellular dermal matrix (ADM); polyurethane (PU); endothelial progenitor cells (EPCs); human keratinocytes (hKCs); pectin methacrylate (PecMA); human neonatal dermal fibroblasts (hNDFs); extracellular matrix (ECM); human endothelial cells (hECs); human placental pericytes (hPCs); phosphosilicate calcium bioglasses (PSCs); human umbilical cord mesenchymal stem cells (hUCMSCs); poly-(lactic-co-glycolic acid) (PLGA).
Table 5.
Recent advances in 3D printing/bioprinting and cellular therapies for skin tissue engineering. Abbreviations: strontium silicate (SS); matrix hydrogel with 2.8% of gellan gum, 1.6% of alginate, and 2.8% of methyl cellulose (GAM); human dermal fibroblasts (hDFs); human umbilical vascular endothelial cells (hUVECs); murine umbilical vein endothelial cells (MUVECs); dextran (Dex); vascular endothelial (VEGF); gelatin (Gel); keratin (Kr); not applicable (n/a); bi-layer (BL); poly (ℇ-caprolactone) (PCL); amoxicillin (AMX); external human epidermal growth factor (rhEGF); Digital light processing (DLP); gelatin methacrylate (GelMA), hyaluronic acid (HA); N-(2-aminoethyl)-4-(4-(hydroxymethyl)-2-methoxy-5-nitrosophenoxy) butanamide (NB); lithium phenyl-2,4,6-trimethylbenzoylphosphinate (LAP); human skin fibroblasts (hSFs); silk fibroin (SF); 4-arm polyethylene glycol acrylate (PEG4A); platelet-rich plasma (PRP); dermal fibroblasts (DFs); epidermal stem cells (ESCs); acellular dermal matrix (ADM); polyurethane (PU); endothelial progenitor cells (EPCs); human keratinocytes (hKCs); pectin methacrylate (PecMA); human neonatal dermal fibroblasts (hNDFs); extracellular matrix (ECM); human endothelial cells (hECs); human placental pericytes (hPCs); phosphosilicate calcium bioglasses (PSCs); human umbilical cord mesenchymal stem cells (hUCMSCs); poly-(lactic-co-glycolic acid) (PLGA).
| 3D printing technology | Biomaterials | Cellular Therapies | Application | Outcomes | Reference |
|---|---|---|---|---|---|
| 3D bioprinting | Collagen, SS, GAM | hDFs, hU-VECs, MUVECs, BALB/3T3 fibroblast | Vascularized Skin substitute | Collagen-2SS-GAM demonstrated significant capabilities in promoting angiogenesis, integrating with host tissue and facilitating wound repair in vivo. | [242] |
| Extrusion-based 3D printer and electrospinning | Dex-VEGF, Gel-Kr | n/a | Construct to accelerate wound healing | The BL-VEGF construct is identified as an optimal candidate for enhancing the healing process of full-thickness skin wounds. | [243] |
| PCL, AMX, alginate, gelatin | rhEGF | Repair defective skin tissue and wound healing | The PCL-AMX@SG-rhEGF scaffold demonstrated superior drug release capabilities and significant antibacterial properties. Both in vitro and in vivo analyses indicated that the scaffold facilitates cell adhesion and proliferation, accelerates skin wound healing, and exhibits favorable biocompatibility. | [241] | |
| DLP-based 3D printing | GelMA/HA, NB/LAP | hSFs, hUVECs | Functional living skin | The bioink exhibited rapid gelation, customizable mechanical properties, high biocompatibility, and effective tissue adhesion. In vivo studies in large animal models showed that the bioink elicited an immediate defense response and was particularly effective in enhancing dermal regeneration, including the development of skin appendages. | [244] |
| SF, PEG4A | NIH 3T3 fibroblas, keratinocytes | Artificial skin model | SF-polyethylene glycol hydrogels presented higher cell proliferation, and the thickest keratin layer was produced with SF-PEG4A hydrogels when compared to PEG4A alone. | [245] | |
| Extrusion-based bioprinting (in situ) | Alginate, gelatin, PRP | DFs, ESCs | Wound repair | The addition of PRP enhanced the cellular behaviour of the cells, regulated vascular endothelial cell tube formation and macrophage polarisation in a paracrine manner. In in-situ bioprinting, incorporating PRP accelerated high-quality wound closure, regulated inflammation, and stareted angiogenesis more effectively than using alginate-gelatin bioink. | [246] |
| Extrusion-based bioprinting | GelMA | ADM, HaCaTs, hUVECs, fibroblasts | Functional skin model | The in vivo results showed that the functional skin model stimulated wound healing and re-epithelialisation, enhanced the production of dermal extracellular matrix, stimulated angiogenesis, and overall improved the quality of wound repair. | [240] |
| PU, gelatin | Fibroblasts, keratinocytes, EPCs | Skin tissue engineering. | Curvilinear-bioprinted hydrogel showed superior structural integrity over planar-bioprinted hydrogel. In the treatment of large and irregular rat skin wounds, the curvilinear-bioprinted tri-cell-laden hydrogel achieved complete repair within 28 days. | [247] | |
| Alginate, honey | 3T3 fibroblast | Skin tissue engineering | The incorporation of honey resulted in bioprinted scaffolds with enhanced cell proliferation, without any visible decrease in printability. | [248] | |
| SF, gelatin | hDFs, hKCs | Full-thickness skin constructs | A silk and gelatine bioink have been printed that can be used to recapitulate a series of biological and design parameters comparable to human skin. | [239] | |
| 3D Bioprinting | PecMA | hNDFs | Biomimetic skin constructs | The hydrogels exhibited significant versatility, enabling precise adjustment of their rheological and viscoelastic properties. Additionally, they created an optimal microenvironment that supported the deposition of endogenous ECM by the entrapped hNDFs, which is rich in collagen and fibronectin. | [249] |
| Rat tail type I collagen | hDFs, hKCs, hECs, hPCs, | Multilayered vascularized human skin grafts | In in vitro studies, hKCs grow and develop into a multi-layered barrier, while hECs and hPCs form interconnected microvascular networks. In vivo, the presence of hPCs in the printed dermal tissue increased the integration of the graft with the host's microvessels and supports the generation of an epidermal network. | [250] | |
| PSCs, alginate, gelMA, gelatin | hUVECS, hUCMSCs | Skin tissue grafts | The incorporation of PSCs revealed enhanced cell proliferation and elevated expression of angiogenesis-related genes in vitro. In vivo experiments showed an improved wound healing effect, characterized by an increase in angiogenesis and collagen deposition. | [233] | |
| Pneumatic-assisted extrusion freeforming | Alginate, gelatin | hSFs | Bioactive dermal substitute scaffold | The three-phase crosslinking technique can produce dermal substitute supports with physicochemical and biological properties suitable to be used in skin tissue engineering. | [251] |
| Inkjet printing | PLGA, prednisolone | n/a | Personalized dermal patches for treatment of skin diseases | The first steps have been made towards the concept of manufacturing personalized patches by inkjet printing that can be made for poorly soluble pharmaceuticals. The model drug prednisolone was successfully processed and printed in the format of a nanosuspension. The PLGA nanoparticles and the patches produced demonstrated a prolonged release of the pharmaceutical. | [252] |
Table 6.
Recent advances in 3D printing/bioprinting and cellular therapies for neural tissue engineering. Abbreviations: methacrylated silk fibroin (SilMA); pectin methacryloyl (PecMA); silk fibroin (SF); neural stem/progenitor cells (NSPCs); polyurethane (PU); neural stem cells (NSCs); hyaluronic acid (HA); neural progenitor cells (NPCs); poly(lactic-co-glycolic acid) (PLGA); primary human dermal fibroblasts (phDFs); vascular endothelial growth factor (VEGF); murine neural stem cells (C17.2); interferon-gamma (IFN-γ); poly (ℇ-caprolactone) (PCL); oxymatrine (OMT); polyethylene glycol diacrylate (PEGDA); digital light processing (DLP); gelatin methacrylate (GelMA); Poly(3,4-ethylenedioxythiophene) (PEDOT); not applicable (n/a); chondroitin sulfate methacrylate (CSMA); bone marrow-derived mesenchymal stem cells (BMSCs); stereolithography (SLA); rat adrenal medullary pheochromocytoma (pc-12); reduced graphene oxide (rGO).
Table 6.
Recent advances in 3D printing/bioprinting and cellular therapies for neural tissue engineering. Abbreviations: methacrylated silk fibroin (SilMA); pectin methacryloyl (PecMA); silk fibroin (SF); neural stem/progenitor cells (NSPCs); polyurethane (PU); neural stem cells (NSCs); hyaluronic acid (HA); neural progenitor cells (NPCs); poly(lactic-co-glycolic acid) (PLGA); primary human dermal fibroblasts (phDFs); vascular endothelial growth factor (VEGF); murine neural stem cells (C17.2); interferon-gamma (IFN-γ); poly (ℇ-caprolactone) (PCL); oxymatrine (OMT); polyethylene glycol diacrylate (PEGDA); digital light processing (DLP); gelatin methacrylate (GelMA); Poly(3,4-ethylenedioxythiophene) (PEDOT); not applicable (n/a); chondroitin sulfate methacrylate (CSMA); bone marrow-derived mesenchymal stem cells (BMSCs); stereolithography (SLA); rat adrenal medullary pheochromocytoma (pc-12); reduced graphene oxide (rGO).
| 3D printing technology | Biomaterials | Cellular Therapies | Application | Outcomes | Reference |
|---|---|---|---|---|---|
| Extrusion-based 3D Bioprinting | SilMA, Pectin, PecMA, SF | NSPCs | Neural tissue engineering applications or in vitro brain models | The SilMA/pectin biotints showed adjustable mechanical properties, biocompatibility and a highly propitious environment for neural induction. | [259] |
| PU | NSCs | Neural tissue engineering | NSCs proliferated and differentiated favourably in PU2 bioprinted hydrogels. In the in vivo model of neural injury in the zebrafish embryo, the injection of hydrogels loaded with NSCs facilitated the repair of the damaged central nervous system. Additionally, the functionality of adult zebrafish with traumatic brain injury was recovered following the injection of constructs with NSCs. | [262] | |
| Gelatin, alginate, fibrinogen, nanofibrillate cellulose, matrigel, HA | NPCs, astrocytes | Study the connection between human neuronal networks, model pathological processes and provide a platform for drug testing. | Imprinted neuronal progenitors differentiate into neurons and form functional neuronal circuits within and among tissue layers with specificity within weeks. | [263] | |
| Laser Assisted Bioprinting | PLGA | NE-4C | Artificial neural tissue constructs | The findings of the work showed that the topological clue presents a relevant role in the development of clusters on the support, but the bioprinted laminin dots appeared to regulate the strength of the bond between them, paving the way for controlling the functional morphology of artificial neural tissue constructions. | [264] |
| 3D Bioprinting | PU | FoxD3 plasmids, phDFs | Personalized drug screening or neuroregeneration. | The phDFs embedded with FoxD3 in the thermo-responsive PU hydrogel exhibited the capacity to undergo reprogramming and develop into a neural tissue-like structure within 14 days post-induction. | [265] |
| Collagen, fibrin gel | VEGF, C17.2 | Neural tissue regeneration | The bioprinting of fibrin gel containing VEGF facilitated the prolonged release of growth factors on the collagen scaffold. | [266] | |
| 3D printing technology based on low-temperature extrusion | Collagen, chitosan | IFN-γ, NSC-derived exosomes | Neurological recovery after traumatic brain injury | The 3D printed collagen/chitosan structure exhibited favorable biological and mechanical characteristics, creating an optimal microenvironment for NSC differentiation and exosome secretion. Additionally, this scaffold played a role in various pathological processes following traumatic brain injury in rats, significantly improving neurofunctional recovery. | [267] |
| Electrospinning | PCL, OMT, gelatin, PEGDA, β-cyclodextrin | Spinal cord extracellular matrix | Treatment of spinal cord injuries | The manufactured scaffolds led to the differentiation of NSCs into neurons while suppressing their conversion into astrocytes. They established an optimal microenvironment for spinal cord tissue regeneration in vivo and directed axonal growth. Additionally, the transplantation of these scaffolds, combined with OMT, improved motor function recovery in rats with spinal cord injuries. | [260] |
| DLP printing | GelMA, chitosan, PEDOT | n/a | Neural tissue repair | The GelMA/Chitosan-PEDOT hydrogel showed good and stable electrical conductivity, enhanced mechanical strength and noticeable biocompatibility. In vivo tests showed that the hydrogels promoted nerve regeneration and helped muscle recovery in the repair of sciatic nerve defects. | [268] |
| Microextrusion-based 3D bioprinting | GelMA, PEGDA, PEDOT, CSMA | NSCs | Nerve injury repair | 3D bioprinted electroconductive hydrogel showed biocompatibility, suitable mechanical strength and good conductivity, thus promoting the adhesion, growth and proliferation of NSCs. | [269] |
| Additive-lathe 3D bioprinting | GelMA, PEGDA | BMSCs | Peripheral nerve injury repair | An integrated two-layer nerve conduit was developed, in which the BSMCs within the printed nerve conduits demonstrated excellent cell viability and extended cellular morphology. In vitro studies with PC12 cells revealed that the growth of neurons is significantly enhanced in nerve conduits embedded with BMSCs. | [270] |
| SLA | GelMA, PEGDA | Pc-12 | Multi-physical model for cell-laden nerve scaffolds | This model enables the prediction of key regions for cell growth within neural scaffolds during in vitro culture experiments. By identifying these primary growth areas, the model allows for targeted increases in oxygen concentration in these regions, thereby enhancing cell density and distribution. | [261] |
| Electrohydrodynamic jet | PCL, rGO | PC-12 | Peripheral nerve injury repair | The addition of rGO to scaffolds results in softer materials that enhance neural differentiation. In vitro studies with PC12 cells show increased cell proliferation and improved support for neural differentiation in PCL/rGO scaffolds compared to PCL-only scaffolds, as confirmed by RT-PCR and immunocytochemistry analyses. | [271] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



