
Submitted:
19 August 2024
Posted:
20 August 2024
You are already at the latest version
Abstract
Background: Lower limb length discrepancy (LLD) in children and adolescents, often due to congenital or acquired conditions, is treated to achieve limb equality and alignment, optimizing function and minimizing cosmetic concerns for an active adulthood. This study evaluated the Health-Related Quality of Life (HRQoL) and physical functioning of adults who underwent unilateral limb lengthening with circular external fixators (EFs) in childhood. Methods: Fifty patients treated at a median age of 14.9 years completed the Short Form 36 (SF-36) and Stanmore Limb Reconstruction Score (SLRS) questionnaires in adulthood, with a median follow-up of 8.9 years. Results: Among the 50 patients, 38 underwent a single limb lengthening (21 tibia, 12 femur, 5 both), while 12 required multiple cycles. The median residual LLD was 0.4 cm, with 12 patients (24%) having over 2 cm. Complications occurred in 67% of procedures, mainly due to prolonged healing. Physical and mental health scores were significantly lower than normative data. The mean Physical Component Summary was 52.2 ± 7.2 (p = 0.20). The mean Mental Component Summary was 43.9 ± 8.6 (p = 0.001), notably lower in congenital LLD cases. Many SLRS items (Pain, Social, Physical Function, Work, and Emotions) strongly correlated with SF-36 items. Conclusions: The study highlights the challenges in treating LLD, emphasizing the significant mental health impact, especially in congenital cases, and the necessity for comprehensive long-term care strategies. These findings suggest that future therapeutic strategies should focus on both physical and psychological outcomes to improve overall recovery in LLD treatment.
Keywords:
limb lengthening
; Ilizarov
; external fixation
; congenital
; pediatric
; Patient-Reported Outcomes
; Short Form 36
; Stanmore Limb Reconstruction Score
1. Introduction
Lower limb length discrepancy (LLD) and associated deformities are common concerns during childhood and adolescence, resulting from congenital conditions or acquired factors like sepsis sequelae, trauma involving growth plates, tumors, or rare genetic disorders [1]. The overarching goal in treating children with LLD is to enable an active adult lifestyle with optimal function, minimal musculoskeletal pain, and minimal cosmetic concerns [2]. Decisions about LLD treatment in children are typically made collaboratively by parents and healthcare professionals during childhood, encompassing both operative and non-operative approaches [3]. Traditionally, orthopedic surgeons strive for nearly normal alignment, equal limb length, and a typical gait pattern through surgical interventions. This objective commonly entails preserving the foot and salvaging the limb through lengthening procedures, a preference typically shared by both patients and parents when compared to the alternative of amputation and fitting a prosthesis [4,5]. However, limb salvage may entail repeated interventions, prolonged treatments, and a high risk of complications or failure, with the added challenge of an occasionally uncertain final functional outcome. These challenges can profoundly impact the child or adolescent [3].
Typically, the results of these multimodal treatments are quantitatively assessed in terms of body functions, activity performance, and societal participation. Patient-reported outcome measures (PROMs) are universally recognized as a crucial element in evaluating surgical outcomes, providing valuable insights into the impact on health, well-being, and quality of life, irrespective of the procedure's type or quality [6]. They facilitate the quantification of improvement achieved or desired from a therapeutic intervention, allowing comparisons of diverse therapeutic approaches and evaluation against general or target population standards. Investigating PROMs streamlines informed decision-making among therapeutic strategies and reveals aspects of health and well-being most affected by a pathological condition—some (such as loss of self-esteem, feelings of inadequacy, anxiety or depression, social impact) challenging to clinically detect but crucial to address in treating a pathology.
Limited information currently exists on the quality of life for patients who underwent limb lengthening procedures due to congenital or acquired deformities in childhood or adolescence. Our study investigates Health-Related Quality of Life (HRQoL) and physical functioning in patients who underwent unilateral limb lengthening with circular external fixation (EF) during childhood, comparing their outcomes with age- and gender-matched normative data from the general population.
2. Materials and Methods
This was a retrospective study that included pediatric and adolescent patients who underwent one or more lower limb lengthening procedures using circular EF at a single institution between January 2009 and December 2021 (NCT06519175). The surgical technique used in this study have been comprehensively detailed in a prior publication [7]. Patients with LLD who underwent unilateral lengthening of the lower limb with circular EF before the age of 18 were invited to complete two specific questionnaires to evaluate their quality of life upon reaching legal adulthood (>18 years). Exclusion criteria comprised: age > 18 years at the time of the lengthening procedure, and age <18 when responding to the questionnaires, bilateral lengthening procedures (e.g., achondroplasia) or conditions other than LLD (e.g., acute fractures), patients treated with intramedullary lengthening nail, patients with incomplete or absent radiographic data, patients with incomplete or partially answered questionnaires. From medical records were extracted the following patient data: sex, affected side, family history, underlying pathologies, comorbidities, and LLD etiology. Any previous surgeries performed outside our Institution were documented (e.g., hemiepiphysiodesis, corrective osteotomies, etc.). Specifics of the surgical lengthening procedures were assessed, and the Total Treatment Time (TTT) and the Healing Index (HI) were calculated for each intervention [7]. All data were recorded blindly by two independent authors (A.D. and A.C.). Complications were assessed according to Lascombes’ classification [8], with HI > 45 days/cm defined as major complication (grade IIIa) but considered separately from the other complications [7]. The requirement for orthoses, or assistive devices was also recorded. The presence of painful symptoms or functional limitations, along with the assessment of quality of life, was assessed with the following Patient-Reported Outcome Measures (PROMs): the Italian version of the Short Form 36 (SF-36) and the Stanmore Limb Reconstruction Score (SLRS) [6,9,10,11]. While the SF-36 is a generic, widely used, multidimensional tool divided into 8 scales, designed to assess overall health status and capture the impact of a disease on various dimensions of quality of life, the SLRS has recently specifically designed for patients undergoing limb reconstruction surgery. Telephonic and email communication was established with all patients by a single author (A.C.), who proposed the questionnaires. Call details were recorded and divided into three primary groups: patients who did not respond to the phone call or email, patients who declined to recount their experience or voice concerns, and patients who expressed willingness to complete the questionnaires. Those who consented to participate in the questionnaires received a form containing the SF-36 and the SLRS. A section for additional comments was included at the end of each form.
Statistical analyses were performed using STATA (version 17.0) based on the data collected in Excel 2021 (Microsoft Corporation, CA, USA). Normality of distribution of continuous variables was tested using the Shapiro-Wilk test and comparisons were made with Mann–Whitney U tests or Student’s t tests depending on the data distribution. Results were expressed as mean (± standard deviation - SD) for continuous variables with normal distribution, median with first and third quartile (Q1-Q3) and/or complete range for non-normally distributed variables and as numbers with associated percentages for categorical variables. Univariable and multivariable analysis with linear and logistic regression were performed to assess the influence of baseline variables (e.g., age at surgery, sex, preoperative LLD, etiology, age at survey) and surgical variables (e.g., bone healing, complications, residual LLD) on the outcomes (SF-36 and SLRS). For SF-36, Physical Component Summary (PCS) and Mental Component Summary (MCS) were calculated according to the method by Ware et al. [10,12]. Most recent normative data by age and sex available on a European population were used for comparison, using t-test for comparison of means and grouping the patients by number of SD from normative data (above – 1, between – 1 and – 2 and below – 2) [13]. The relationship strength among variables was assessed using the correlation coefficient (absolute adjusted R-squared value): R-squared < 0.3: None or very weak effect size; 0.3 ≤ R-squared < 0.5: Weak or low effect size; 0.5 ≤ R-squared < 0.7: Moderate effect size; R-squared ≥ 0.7: Strong effect size [14]. A difference was considered statistically significant for a p-value less than 0.05.
3. Results
3.1. Patients Included and Demographics
Based on clinical records, a cohort of 178 eligible patients was initially identified for inclusion in this study. Unfortunately, 67 of these patients were unreachable due to various issues, such as missing contact information, non-functioning numbers, or unresponsive calls. Of the 111 patients successfully contacted by telephone and invited to participate by completing questionnaires, four declined to participate in a rather impolite manner, 50 patients (28% of the entire series) completed the questionnaires and were included in the final analysis (see flowchart in Figure 1). The remaining 57 patients, who initially agreed to participate, ultimately did not return their completed questionnaires, despite the follow-up reminders. No statistically significant differences were observed in primary outcomes between these groups (see details in Table S1 in Supplementary Materials).
In the responders’ cohort, 38 patients underwent a single limb lengthening procedure. Among them, 21 patients received lengthening in the tibial segment, 12 patients in the femoral segment, and 5 patients in both segments simultaneously. Additionally, 12 patients required two or more lengthening cycles, and in 6 of these cases, a single limb segment was treated multiple times. Overall, 70 segments were treated, 29 femurs and 41 tibiae, at a median patient age of 14.9 years (range 7.0 – 17.3, see details in Table 1). The median preoperative LLD at the first lengthening procedure was 6.0 cm (range 3 – 20 cm), corresponding to a median 3.6% of height (range 2 – 13%).
3.2. Surgical Parameters and Outcomes
Most lengthening procedures (93%) were performed with the traditional Ilizarov circular frame, while 5 procedures (7%) with hexapod EFs. Median follow-up was 8.9 years since the last EF removal (range 2.0 – 13.5 years). Overall, median HI was 51 days/cm (range 24 – 151 days/cm) and median TTT was 247 days (range 135 – 604 days). There were no statistically significant differences observed in both the HI and the TTT when comparing congenital and acquired etiologies (p-value > 0.42). Likewise, no significant differences were found between the femur and tibia for both HI and TTT (p-value > 0.36).
Residual LLD had a median value of 0.4 cm (range 0.0 – 9.0 cm). 38 patients (76%) had a residual LLD up to 2 cm, while 12 patients (24%) had a residual LLD exceeding 2 cm. Preoperative LLD showed a correlation with residual LLD after all lengthening procedures (Spearman’s rho = 0.60, p-value = 0.001). In particular, patients with preoperative LLD of more than 4.5% of height had a significantly higher prevalence of a residual LLD of more than 2 cm, raising from 7% to 41% (p-value = 0.006).
3.3. Complications
Twenty-three lengthening procedures (33%) had no complications, while, among the remaining forty-seven procedures, seventy-one complications were observed, which were all major ones except for sixteen cases of minor complications. HI was higher than 45 days/cm in thirty-eight procedures (54%) and among nineteen of them (27% of total procedures) high HI was the only complication observed. Details about complications are reported in Table 2.
Revision surgery was required during or after eight lengthening procedures. One case of pin infection required surgical debridement and revision of local pins. One case of fracture of femoral regenerate after EF removal was treated with cast immobilization and healed with severe procurvatum deformity, which then required corrective osteotomy. One case of early consolidation required revision of the osteotomy site to complete lengthening. A patient, after simultaneous lengthening of femur and tibia, developed severe stiffness of knee and ankle, which were treated with femoral and tibial osteotomies and contralateral epiphysiodesis. A case of non-union was treated with open fixation with plate and an autograft from iliac crest eight months after EF removal. In one case of femoral lengthening, EF was removed during the lengthening phase for an infection and the patient was then treated with an opening-wedge osteotomy to treat the residual shortening and valgus deformity. In one case of femoral lengthening, residual valgus deformity required corrective osteotomy.
3.4. PROMs
The median age at survey was 23.1 (range 18.5 – 29.3). Among SF-36 items, physical function (PF), general health (GH), social function (SF), role-emotional (RE) and mental health (MH) were significantly lower than normative data (p-value = 0.001). Conversely, results in role-physical (RP), bodily pain (BP) and vitality (VT) were comparable with normative data (p-value > 0.130). The mean Physical Component Summary (PCS) was 52.2 ± 7.2 (range 28.6 – 61.1), with no significant difference from normative data for age (p-value = 0.20). Mental Component Summary (MCS) had a mean value of 43.9 ± 8.6 (range 24.4 – 58.5), significantly lower than normative data for age (p-value = 0.001, see Figure 2a). Sixteen percent of patients had a PCS score more than 1 standard deviation (SD) below the normative data, and 6% had a score more than 2 SD below. For the MCS, 42% of patients scored more than 1 SD below the normative data, while 10% scored more than 2 SD below (see details in Figure S1 in Supplementary Material). This difference was even more evident in patients affected by congenital LLD, in which 51% had MCS results below – 1 SD, and 12% below – 2 SD (see Figure 2b).
Preoperative LLD showed a very weak impact on BP and PCS (adjusted R-squared 0.07 with p = 0.038), while residual LLD showed a weak influence on PF item and on PCS (adjusted R-squared 0.11 with p = 0.025). Age at questionnaire showed a weak influence on GH item (adjusted R-squared 0.07 with p = 0.034). None of the pre- and postoperative variables considered showed influence on MCS results (see Table 3 for details).
Results of SLRS for entire cohort are reported in Table 4. Many items of SLRS (Pain, Social, Physical Function, Work and Emotions) showed a strong correlation with one or more items combined of SF36 (adjusted R-squared > 0.72, p = 0.001, see details in Table S3 in Supplementary Material). Hygiene in SLRS showed a medium correlation with SF36 Physical Function (adjusted R-squared = 0.53, p = 0.001). Sleep, Leisure, Future and Cosmetic showed no more than weak correlations with all SF36 items, including PCS and MCS (adjusted R-squared < 0.30). Conversely, PF, BP, SF and RE showed strong correlation with other items of SLRS (adjusted R-squared > 0.77, p = 0.001), while RP, GH, VT and MH showed medium correlation with other items of SLRS (adjusted R-squared 0.41 – 0.55, p = 0.001). PCS showed strong correlation with SLRS Physical Function and Work (adjusted R-squared 0.63, p = 0.001), while MCS showed strong correlation with SLRS Social and Emotions (adjusted R-squared 0.73, p = 0.001).
4. Discussion
Our study explores the HRQoL and physical functioning of young adults who underwent unilateral correction and lengthening procedures using a circular external fixator for various reasons during childhood. The main finding that emerges is the high prevalence of residual psychological distress despite achieving clinical-functional milestones, a result that was found almost only among patients affected by congenital LLD. Patients with acquired LLD had both PCS and MCS scores comparable to healthy population, similarly to data on treatment of post-traumatic LLD reported by Schep et al., who reported normal quality of life in adults that underwent distraction osteogenesis [15]. On the other hand, most patients affected by congenital etiologies of LLD had scores of MCS below – 1 SD from normative data. This means that their results were at least 8.9 below the mean value for age and sex. For comparison, the effect of depression is a reduction of MCS between 9.3 and 12.7 [10].
Several studies highlighted the psychosocial distress in individuals with skeletal deformities or LLD due to self-perception of physical appearance [16]. However, the achieved correction may not always enhance the patient's perceived well-being as expected [17]. In our series, 82% reached normal values in PCS, while only 46% did so in MCS. Residual disfiguring scars, joint stiffness, residual LLD or deformities, along with syndromic associations highlighting the disparity between expected and actual outcomes, partially contribute to this psychological distress. Coping with rare and disfiguring skeletal conditions during childhood and adolescence, along with a prolonged and challenging clinical journey involving repeated hospitalizations, multiple surgeries, and the need to undergo intense procedures like circular external fixation, can weigh heavily and leave lasting psychological distress into adulthood. The family and social context present another challenge, especially in cases of dysfunctional family dynamics and inadequate parental guidance during the child's treatment journey or absence of psychosocial support avenues like summer camps or group activities with peers facing deformities [18]. Moreover, future uncertainty and feelings of inadequacy in work and social life contribute to this overall state of psychological distress.
The importance of a psychological support in distraction osteogenesis for LLD was already reported by several authors in the last decades. Ghoonem et al. observed overall normal psychological scores in 45 patients treated between 3 and 18 years of age who were given a thorough psychological preparation during lengthening procedure [19]. Similarly, Ramaker et al. found no psychological issues caused by the Ilizarov lengthening procedure if patients and parents were given preoperative assessment for depression and anxiety and a support during the months of the procedure [20]. As consequence, lower scores in MCS may have been the consequence of an insufficient support to children and adolescents to cope with their condition. Niemelä et al. observed a higher prevalence of behavior problems in patients with LLD of various etiologies compared to healthy children of the same age [21]. They also clearly demonstrated that strong support in coping with the condition can significantly enhance the Ilizarov lengthening procedure's effectiveness in improving children's behavior [21]. In summary, growing patients with LLD, especially those with congenital causes, are often vulnerable both psychologically and socially. As such, treatment should focus not only on correcting the length discrepancy but also on helping the child build confidence and a positive body image. Martin et al. recommended to put a lot of effort in helping the patients during the first month of lengthening, in which they found the highest level of distress for the patients [22].
Preoperative and residual LLD had a weak effect on PCS, and with the available data, they did not significantly impact the MCS. Our findings partially contrast with the study by Moraal et al., where seven years post Ilizarov limb lengthening, patients showed normal psychosocial functioning, self-esteem, and perceived competence, exhibiting quality of life scores similar to norm groups, with exceptions of reduced gross motor function, lower vitality, and increased pain [23]. Notably, a residual LLD greater than 2 cm remained a significant factor in long-term follow-up, leading to a reported decline in quality of life. Other studies have confirmed this impact, emphasizing that both the initial limb length inequality—whether congenital or acquired—and contributing factors such as obesity can significantly affect overall quality of life, including mental and social aspects [17]. Ramaker et al. observed in a cohort of 26 patients that 87% of them would undergo again the lengthening procedure, but the authors could not identify a precise complication and/or residual issue associated with bad experience in the remaining 13% [20]. One patient from our case series wrote: I hope the doctors who put their hands on me suffer as much as I did. An important takeaway from this study is that any young patient undergoing a lengthening procedure may express a similar dissatisfaction, but it is impossible to predict who will feel this way. Even with a flawless technique, minimal time in the frame, and no complications, this dissatisfaction may still arise. The difference among families and/or other type of social support may explain this unpredictability.
The SF-36 was used in this study due to its widespread use in assessing quality of life, including in patients undergoing limb reconstruction with circular EF [24]. Its results can also be compared with normative data from large, up-to-date global cohort studies [25]. With its incorporation of eight domains, it offers a comprehensive assessment of the patient's overall well-being. Moreover, the method of evaluating outcomes derived from SF36 questionnaires through comparison with normative data from the general population has become an established approach in various analogous studies. This method proves particularly valuable when dealing with scenarios where a pre-operative SF36 score is unavailable. This comparative analysis enhances the interpretability of the SF36 outcomes, providing a contextually meaningful understanding of the impact of interventions in the absence of pre-operative baseline measurements. Kaastad et al. compared the HRQoL, assessed using SF-36, among limb-deficient individuals with normative data from the general health population. They observed diminished physical functioning, heightened bodily pain, and decreased general health and emotional role. These outcomes align with our study, suggesting an enduringly low quality of life into adulthood for children who underwent limb lengthening [25]. Other multidimensional questionnaires have been used to evaluate patients with lower limb discrepancies requiring lengthening with external fixation, including the EuroQol, PedsQL, PODCI, and WHOQoL-BREF [17,25,26,27].
The main criticism of these questionnaires is that they are not specific to any particular condition or treatment, which may result in some aspects of well-being, emotional impact, and the psychosocial effects of circular external fixation going underexplored. Recent systematic reviews found that existing PROMs for patients undergoing limb reconstruction with circular external fixation do not fully capture the specific health outcomes relevant to this group, underscoring the need for a tailored PROMs [28,29]. There is a clear need to develop new PROMs specifically for patients with congenital limb length discrepancies who require lengthening with external fixation. The SLRS was developed for this purpose, and we tested it against the SF-36, finding a strong correlation between the two questionnaires. However, the SLRS, recently introduced in a pilot study, has only undergone face validity testing. Its reliability, responsiveness, precision, and criterion validity have yet to be tested, and it has not been applied to large populations undergoing limb reconstruction surgery [6].
More recently the LIMB-Q and the LIMB-Q Kids questionnaires have been validated in multiple languages and shows promise as the most specific tool for assessing LLD [30,31,32,33]. Also the PROLLIT (Patient-Reported Outcome Measure for Lower Limb Reconstruction) study group developed a conceptual framework outlining six key domains important to patients undergoing limb lengthening with circular external fixation: pain, self-perception, work and finances, daily lifestyle and functioning, emotional well-being, and support. Some of these domains, particularly “support,” are poorly represented in current PROMs, prompting the development of new, condition-specific tools [34]. However, further research is needed to gather more data for accurate interpretation. Monitoring changes in quality of life throughout the entire lifespan, from childhood to adulthood, is undoubtedly challenging, particularly for these patients. The decision to undergo such a stressful treatment is often made by caregivers, adding another layer of complexity to the process.
Limitations
Several limitations should be noted. The retrospective design of the study introduces the potential for recall bias, which may have influenced the results. Additionally, the comparison with a preoperative assessment and/or a control group of healthy adults of the same age is only partially addressed by using normative data adjusted for age and sex. However, the SF-36 is not validated for children under 15 years of age, making it impossible to compare results for more than 50% of the patient cohort. Furthermore, the heterogeneity of LLD etiologies with varying levels of severity may serve as a confounding factor. However, many of these conditions are exceedingly rare, even in a large pediatric orthopedic center, making it challenging to assemble a consistent case series. Another significant source of bias was the low patient adherence to PROMs, with only 28% of the initial case series (and just 45% of reachable patients) returning completed forms.
Low adherence to completing PROMs via phone or email has been reported, with response rates dropping below 30% in some studies, particularly for complex and painful treatments that patients may prefer to mentally distance themselves from [35].
5. Conclusions
Adults treated for congenital limb length discrepancy (LLD) during infancy or adolescence exhibit lower mental health scores compared to age- and sex-matched normative data. The specifics of the lengthening procedures did not significantly impact mental health outcomes. Therefore, we recommend routine assessment of psychological and social factors before, during, and after the lengthening procedure using age-appropriate, validated questionnaires.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Table S1: Heterogeneity analysis among the groups of patients observed after the inclusion process. Table S2: Results of Short Form 36 (SF-36) items reporting mean, median, normality test, normative data and comparison. Figure S1: Visual representation of Short Form 36 (SF-36) results comparison with normative data by age and sex. Table S3: Spearman’s correlations among Short Form 36 (SF-36) items and Stanmore Limb Reconstruction Score (SLRS) results.
Author Contributions
Conceptualization, M.M., G.T. and A.D.; methodology, G.T. and G.G.; software, G.C.M..; validation, M.M. and G.T.; formal analysis, A.D. and A.C.; investigation, A.C. and M.R.; resources, G.R.; data curation, A.D. and A.C.; writing—original draft preparation, A.D.; writing—review and editing, M.V. and G.C.M.; visualization, G.G.; supervision, G.R.; project administration, G.T.; funding acquisition, G.T. and G.R. All authors have read and agreed to the published version of the manuscript.
Funding
The work reported in this publication was funded by the Italian Ministry of Health, RCR-2022-23682299 project, under the Italian Musculoskeletal Apparatus Network RAMS and “Donazione ASD Cernobbio 2010”, 2022/730827. These projects have also been partly used to fund scholarships for AD and GCM.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and is part of a study approved by the Ethics Committee of “Comitato Etico di Area VastaEmilia Centro” CE-AVEC 786/2023/Sper/IOR) on 08 April 2024 also registered on ClinicalTrials.gov (Identifier: NCT06519175)
Informed Consent Statement
Informed consent was obtained from all the subjects involved in the study. Written informed consent was obtained from the patient(s) and their families to publish this paper.
Data Availability Statement
Data are available from the corresponding authors upon reasonable request.
Acknowledgements
We sincerely thank Laura Di Maio and Martina Piccinni, the entire Clinical Trial Center, and the Scientific Leadership of the Rizzoli Orthopedic Institute for their support in the drafting and submission of the study protocol.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sabharwal, S. Pediatric Lower Limb Deformities: Principles and Techniques of Management. Pediatric Lower Limb Deformities: Principles and Techniques of Management 2016, 1–635, doi:10.1007/978-3-319-17097-8/COVER. [CrossRef]
- Hosny, G.A. Limb Lengthening History, Evolution, Complications and Current Concepts. J Orthop Traumatol 2020, 21, 3, doi:10.1186/S10195-019-0541-3. [CrossRef]
- Hootnick, D.; Ellingsworth, L.; Mauchin, R.; Brown, A.C. ⇜it Occupied Her Entire Childhood⇝: Looking Back on Limb-Lengthening. Pediatrics 2021, 147, doi:10.1542/PEDS.2020-1055/36363. [CrossRef]
- Tang, C.H.; Addar, A.; Fernandes, J.A. Amputation vs Reconstruction in Type IV Tibial Hemimelia: Functional Outcomes and Description of a Novel Surgical Technique. Strategies Trauma Limb Reconstr 2023, 18, 32, doi:10.5005/JP-JOURNALS-10080-1576. [CrossRef]
- Elmherig, A.; Ahmed, A.F.; Hegazy, A.; Herzenberg, J.E.; Ibrahim, T.; Ibrahim, T. Amputation Versus Limb Reconstruction for Fibula Hemimelia: A Meta-Analysis. J Pediatr Orthop 2020, 40, 425–430, doi:10.1097/BPO.0000000000001510. [CrossRef]
- Wright, J.; Timms, A.; Fugazzotto, S.; Goodier, D.; Calder, P. Development of a Patient-Reported Outcome Measure in Limb Reconstruction: A Pilot Study Assessing Face Validity. Bone Jt Open 2021, 2, 705, doi:10.1302/2633-1462.29.BJO-2021-0105.R1. [CrossRef]
- Depaoli, A.; Magnani, M.; Casamenti, A.; Cerasoli, T.; Ramella, M.; Menozzi, G.C.; Mordenti, M.; Rocca, G.; Trisolino, G. Is the High Healing Index a Complication of Progressive Long Bone Lengthening? Observations from a Cohort of 178 Children Treated with Circular External Fixation for Lower Limb Length Discrepancy. Children (Basel) 2023, 10, doi:10.3390/CHILDREN10101586. [CrossRef]
- Lascombes, P.; Popkov, D.; Huber, H.; Haumont, T.; Journeau, P. Classification of Complications after Progressive Long Bone Lengthening: Proposal for a New Classification. Orthop Traumatol Surg Res 2012, 98, 629–637, doi:10.1016/j.otsr.2012.05.010. [CrossRef]
- Ware, J.E.J.; Sherbourne, C.D. The MOS 36-Item Short-Form Health Survey (SF-36). I. Conceptual Framework and Item Selection. Med Care 1992, 30, 473–483.
- Ware, J.E.; Ware, J. SF-36 Physical and Mental Health Summary Scales: A User’s Manual. 1993.
- Apolone, G.; Mosconi, P. The Italian SF-36 Health Survey: Translation, Validation and Norming. J Clin Epidemiol 1998, 51, 1025–1036, doi:10.1016/S0895-4356(98)00094-8. [CrossRef]
- Laucis, N.C.; Hays, R.D.; Bhattacharyya, T. Scoring the SF-36 in Orthopaedics: A Brief Guide. J Bone Joint Surg Am 2015, 97, 1628–1634, doi:10.2106/JBJS.O.00030. [CrossRef]
- Garratt, A.M.; Stavem, K. Measurement Properties and Normative Data for the Norwegian SF-36: Results from a General Population Survey. Health Qual Life Outcomes 2017, 15, 1–10, doi:10.1186/S12955-017-0625-9/TABLES/4. [CrossRef]
- Moore, D.S..; Notz, William.; Fligner, M.A.. The Basic Practice of Statistics : David S. Moore, William I. Notz, Michael A. Fligner. 2013, 745.
- Schep, N.W.L.; van Lieshout, E.M.M.; Patka, P.; Vogels, L.M.M. Long-Term Functional and Quality of Live Assessment Following Post-Traumatic Distraction Osteogenesis of the Lower Limb. Strategies Trauma Limb Reconstr 2009, 4, 107, doi:10.1007/S11751-009-0070-3. [CrossRef]
- Heath, M.R.; Shin, T.J.; Mehta, R.; Principe, P.S.; MacKie, A.T.; Fragomen, A.; Rozbruch, S.R.; Fabricant, P.D. Patients With Lower Limb Deformity Report Worse Quality of Life Than Control Subjects Regardless of Degree of Deformity. JAAOS Global Research & Reviews 2021, 5, doi:10.5435/JAAOSGLOBAL-D-21-00182. [CrossRef]
- Pawik, Ł.; Pawik, M.; Wrzosek, Z.; Fink-Lwow, F.; Morasiewicz, P. Assessment of the Quality of Life in Patients with Varying Degrees of Equalization of Lower Limb Length Discrepancy Treated with Ilizarov Method. J Orthop Surg Res 2021, 16, 1–9, doi:10.1186/S13018-021-02202-1/TABLES/3. [CrossRef]
- Sjöberg, L.; Hermansson, L.; Lindner, H.; Fredriksson, C. Adolescents with Congenital Limb Reduction Deficiency: Perceptions of Treatment during Childhood and Its Meaning for Their Current and Future Situation. Child Care Health Dev 2022, 48, 613–622, doi:10.1111/CCH.12967. [CrossRef]
- Ghoneem, H.F.; Wright, J.G.; Cole, W.G.; Rang, M. The Ilizarov Method for Correction of Complex Deformities. Psychological and Functional Outcomes. J Bone Joint Surg Am 1996, 78, 1480–1485, doi:10.2106/00004623-199610000-00004. [CrossRef]
- Ramaker, R.R.; Lagro, S.W.J.; Van Roermund, P.M.; Sinnema, G. The Psychological and Social Functioning of 14 Children and 12 Adolescents after Ilizarov Leg Lengthening. Acta Orthop Scand 2000, 71, 55–59, doi:10.1080/00016470052943900. [CrossRef]
- Niemelä, B.J.; Tjernström, B.; Andersson, G.; Wahlsten, V.S. Does Leg Lengthening Pose a Threat to a Child’s Mental Health?: An Interim Report One Year after Surgery. J Pediatr Orthop 2007, 27, 611–617, doi:10.1097/BPO.0B013E31814256C6. [CrossRef]
- Martin, L.; Farrell, M.; Lambrenos, K.; Nayagam, D. Living with the Ilizarov Frame: Adolescent Perceptions. J Adv Nurs 2003, 43, 478–487, doi:10.1046/J.1365-2648.2003.02745.X. [CrossRef]
- Moraal, J.M.; Elzinga-Plomp, A.; Jongmans, M.J.; Van Roermund, P.M.; Flikweert, P.E.; Castelein, R.M.; Sinnema, G. Long-Term Psychosocial Functioning after Ilizarov Limb Lengthening during Childhood: 37 Patients Followed for 2–14 Years. Acta Orthop 2009, 80, 704, doi:10.3109/17453670903473024. [CrossRef]
- McKee, M.D.; Yoo, D.; Schemitsch, E.H. Health Status after Ilizarov Reconstruction of Post-Traumatic Lower-Limb Deformity. J Bone Joint Surg Br 1998, 80, 360–364, doi:10.1302/0301-620X.80B2.8192. [CrossRef]
- Kaastad, T.S.; Tveter, A.T.; Steen, H.; Holm, I. Physical Function and Health-Related Quality of Life in Young Adults with Unilateral Congenital Lower-Limb Deficiencies. J Child Orthop 2017, 11, 348–357, doi:10.1302/1863-2548.11.170026. [CrossRef]
- Montpetit, K.; Hamdy, R.C.; Dahan-Oliel, N.; Zhang, X.; Narayanan, U.G. Measurement of Health-Related Quality of Life in Children Undergoing External Fixator Treatment for Lower Limb Deformities. J Pediatr Orthop 2009, 29, 920–926, doi:10.1097/BPO.0B013E3181C1E2E2. [CrossRef]
- Lee, K.M.; Chung, C.Y.; Gwon, D.K.; Sung, K.H.; Cho, J.H.; Kim, T.W.; Choi, I.H.; Cho, T.J.; Yoo, W.J.; Park, M.S. Parental Perspectives on Leg Length Discrepancy. Journal of Pediatric Orthopaedics Part B 2012, 21, 146–149, doi:10.1097/BPB.0B013E32834C67B2. [CrossRef]
- Antonios, T.; Barker, A.; Ibrahim, I.; Scarsbrook, C.; Smitham, P.J.; David Goodier, W.; Calder, P.R. A Systematic Review of Patient-Reported Outcome Measures Used in Circular Frame Fixation. Strategies Trauma Limb Reconstr 2019, 14, 34, doi:10.5005/JP-JOURNALS-10080-1413. [CrossRef]
- Leggett, H.; Scantlebury, A.; Byrne, A.; Harden, M.; Hewitt, C.; O’Carroll, G.; Sharma, H.; McDaid, C.; Adamson, J.; Cocks, K.; et al. Exploring What Is Important to Patients with Regards to Quality of Life after Experiencing a Lower Limb Reconstructive Procedure: A Qualitative Evidence Synthesis. Health Qual Life Outcomes 2021, 19, 1–16, doi:10.1186/S12955-021-01795-9/FIGURES/3. [CrossRef]
- Chhina, H.; Klassen, A.; Bade, D.; Kopec, J.; Cooper, A. Establishing Content Validity of LIMB-Q Kids: A New Patient-Reported Outcome Measure for Lower Limb Deformities. Qual Life Res 2022, 31, 2805–2818, doi:10.1007/S11136-022-03140-Z. [CrossRef]
- Mundy, L.R.; Klassen, A.F.; Pusic, A.L.; deJong, T.; Hollenbeck, S.T.; Gage, M.J. The LIMB-Q: Reliability and Validity of a Novel Patient-Reported Outcome Measure for Lower Extremity Trauma Patients. Plast Reconstr Surg 2024, doi:10.1097/PRS.0000000000011293. [CrossRef]
- Vogt, B.; Fresen, J.; Gosheger, G.; Chhina, H.; Brune, C.S.; Toporowski, G.; Frommer, A.; Laufer, A.; Cooper, A.; Roedl, R.; et al. LIMB-Q Kids—German Translation and Cultural Adaptation. Children 2022, 9, doi:10.3390/CHILDREN9091405. [CrossRef]
- Jønsson, C.E.; Poulsen, L.; Rölfing, J.D.; Chhina, H.; Cooper, A.; Sørensen, J.A. Danish Linguistic Validation and Cultural Adaptation of the LIMB-Q Kids. Children 2023, 10, doi:10.3390/CHILDREN10071107. [CrossRef]
- Leggett, H.; Scantlebury, A.; Hewitt, C.; Sharma, H.; McDaid, C.; Adamson, J.; Cocks, K.; Harwood, P.; Ferguson, D.; Hamdy, R.; et al. What Is Important to Adults after Lower Limb Reconstruction Surgery: A Conceptual Framework. Quality of Life Research 2023, 32, 1671–1682, doi:10.1007/S11136-022-03340-7/TABLES/3. [CrossRef]
- Benson, T. Why It Is Hard to Use PROMs and PREMs in Routine Health and Care. BMJ Open Qual 2023, 12, 2516, doi:10.1136/BMJOQ-2023-002516. [CrossRef]
Figure 1.
Flowchart of inclusion of patients.
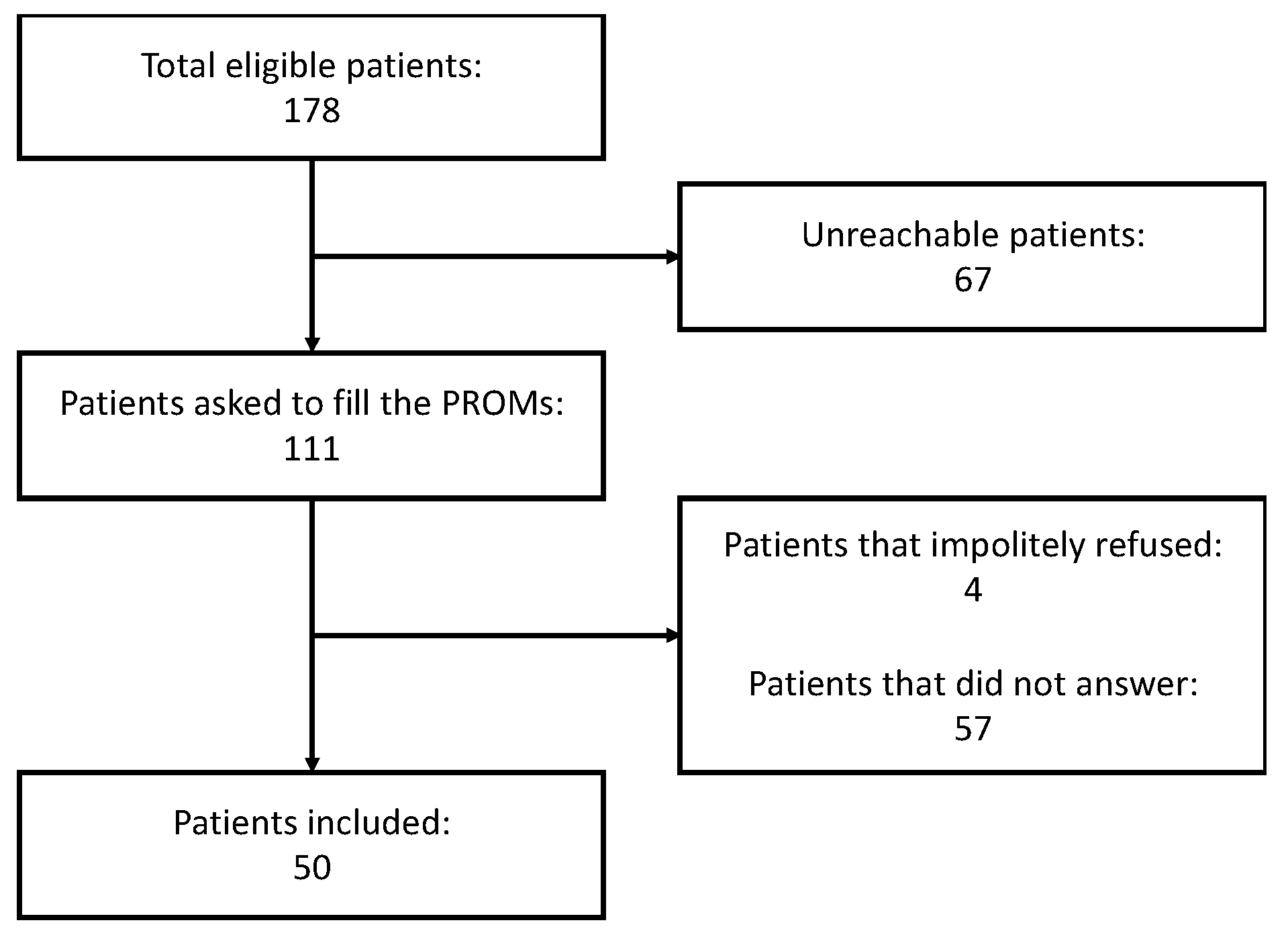
Figure 2.
Distribution of Physical Component Summary (PCS, in blue) and Mental Component Summary results (MCS, in red) compared with normative data by age and sex, in which the thick gray line represents the mean score and the dashed gray lines the ± 1 SD values. Results of MCS were significantly lower (a), especially among patients treated for congenital etiologies of LLD (b).
Figure 2.
Distribution of Physical Component Summary (PCS, in blue) and Mental Component Summary results (MCS, in red) compared with normative data by age and sex, in which the thick gray line represents the mean score and the dashed gray lines the ± 1 SD values. Results of MCS were significantly lower (a), especially among patients treated for congenital etiologies of LLD (b).
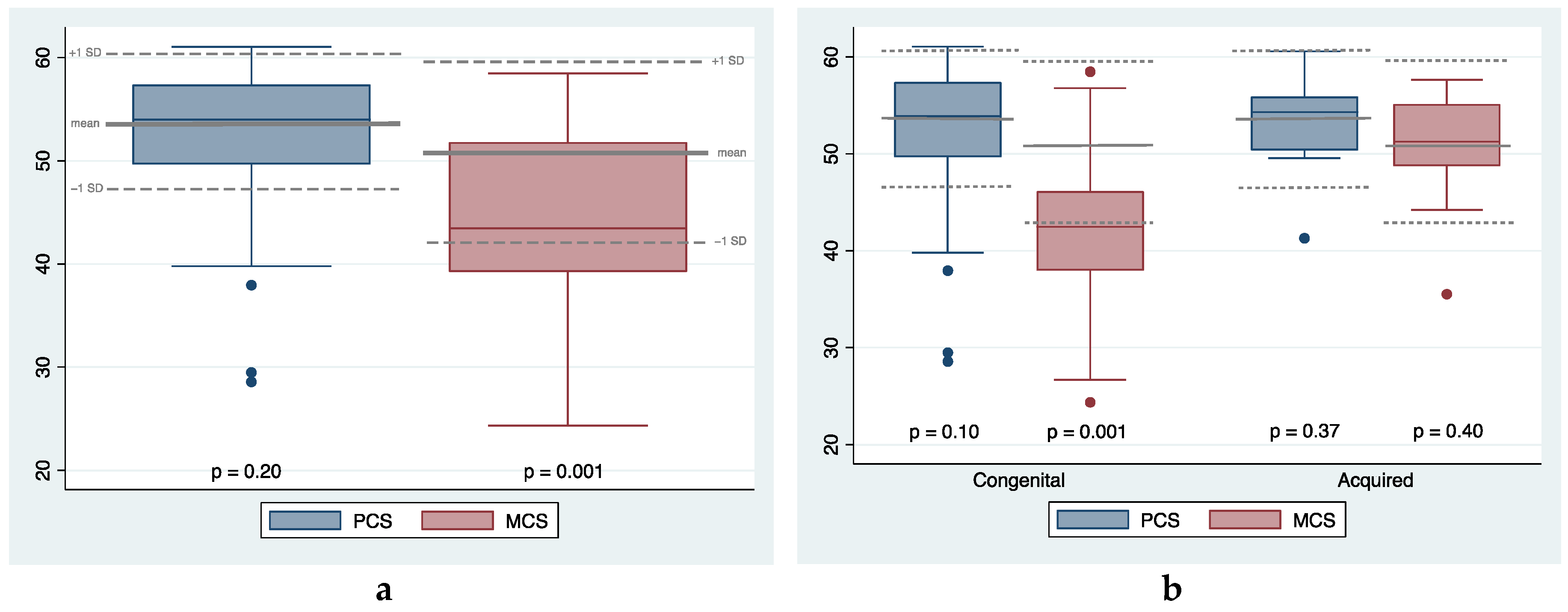

Table 1.
Patients’ descriptives and surgical outcomes by etiology. N = number; LPs = lengthening procedures; Q1-Q3 = first and third quartile values; LLD = lower limb length discrepancy; HI = healing index; TTT = total time of treatment; CFD = congenital femoral deficiency; DDH = developmental dysplasia of the hip; CPMBT = congenital posteromedial tibial bowing; NF1 = neurofibromatosis type 1; CPT = congenital pseudoarthrosis of tibia; MHE = multiple hereditary exostoses.
Table 1.
Patients’ descriptives and surgical outcomes by etiology. N = number; LPs = lengthening procedures; Q1-Q3 = first and third quartile values; LLD = lower limb length discrepancy; HI = healing index; TTT = total time of treatment; CFD = congenital femoral deficiency; DDH = developmental dysplasia of the hip; CPMBT = congenital posteromedial tibial bowing; NF1 = neurofibromatosis type 1; CPT = congenital pseudoarthrosis of tibia; MHE = multiple hereditary exostoses.
| N patients (%) | N LPs (%) |
Median (Q1-Q3) age at surgery (years) | Median (Q1-Q3) preoperative LLD (cm) | Median (Q1-Q3) HI (days/cm) | Median (Q1-Q3) TTT (days) | Median (Q1-Q3) postoperative LLD (cm) | % LPs with one or more complications | % LPs with one or more complications (HI > 45 included) | |
|---|---|---|---|---|---|---|---|---|---|
| Congenital causes | 41 (82%) | 59 (84%) | 14.8 | 7.0 | 50 | 248 | 1.0 | 42% | 68% |
| (11.7-16.0) | (5.0-9.0) | (40-59) | (214-300) | (0.0-2.5) | |||||
| Idiopathic | 8 (16%) | 9 (13%) | 15.2 | 4.0 | 62 | 302 | 0.0 | 22% | 100% |
| (13.5-16.2) | (4.0-7.0) | (52-67) | (232-318) | (0.0-1.3) | |||||
| Proximal limb hypoplasia CFD |
12 (24%) 11 |
19 (27%) 18 |
15.1 (10.3-15.4) |
7.5 (6.0-9.0) |
51 (42-78) |
223 (209-251) |
1.5 (0.0-3.0) |
44% |
50% |
| Hypoplasia in DDH | 1 | 1 |
11.7 (-) |
9.0 (-) |
63 (-) |
316 (-) |
1.5 (-) |
0% | 100% |
| Distal limb hypoplasia Fibular hemimelia |
17 (34%) 9 |
26 (37%) 18 |
13.4 (8.6-15.9) |
8.0 (6.0-11.0) |
46 (39-54) |
274 (217-283) |
1.5 (1.0-2.0) |
56% |
78% |
| Tibial hemimelia | 5 | 5 |
14.8 (14.5-15.9) |
6.0 (5.5-6.0) |
39 (37-45) |
271 (224-278) |
0.0 (0.0-1.0) |
60% | 60% |
| CPMBT | 3 | 3 |
15.0 (13.7-15.1) |
4.5 (4.0-5.0) |
42 (36-43) |
211 (182-239) |
0.0 (0.0-0.0) |
0% | 0% |
| Skeletal dysplasias | 4 (8%) | 5 (7%) | 16.0 | 5.0 | 47 | 256 | 1.8 | 40% | 80% |
| Ollier’s disease | 1 | 2 | (14.0-16.1) | (4.5-9.0) | (37-55) | (192-279) | (0.5-3.8) | ||
| CPT without NF1 | 1 | 1 | |||||||
| CPT in NF1 | 1 | 1 | |||||||
| MHE | 1 | 1 | |||||||
| Acquired causes | 9 (18%) | 11 (16%) | 15.6 | 6.0 | 56 | 245 | 0.0 | 27% | 64% |
| (14.8-16.4) | (5.0-9.0) | (44-64) | (194-299) | (0.0-0.0) | |||||
| Infections | 3 (6%) | 4 (6%) | 14.8 (13.4-15.7) |
9.5 (6.5-10.0) |
67 (50-77) |
376 (270-453) |
1.8 (0.0-3.0) |
25% | 75% |
| Trauma | 6 (12%) | 7 (10%) | 16.0 | 5.2 | 52 | 225 | 0.0 | 29% | 57% |
| (14.8-16.4) | (5.0-6.0) | (30-60) | (186-265) | (0.0-0.0) | |||||
| TOTAL |
50 (100%) |
70 (100%) |
14.9 (12.0-16.0) |
6.3 (5.0-9.0) |
51 (40-60) |
247 (211-299) |
0.4 (0.0-2.0) |
40% | 67% |
Table 2.
Complications classified according to the classification of Lascombes’ et al. N = number; EF = external fixator; GA = general anesthesia.
Table 2.
Complications classified according to the classification of Lascombes’ et al. N = number; EF = external fixator; GA = general anesthesia.
| Grade according to Lascombes’ classification | Type of complication | N |
|---|---|---|
| Grade I | Superficial infection requiring antibiotics Superficial thrombophlebitis Temporary nerve palsy |
14 1 1 |
| Grade IIa | Early union of regenerate Revision of EF under GA |
1 1 |
| Grade IIb | - | 0 |
| Grade IIIa | HI > 45 days/cm Joint stiffness Fracture after EF removal Non-union Residual angular deformity requiring osteotomy |
38 9 1 1 2 |
| Grade IIIb | Lengthening procedure interrupted and EF removed | 2 |
| Grade IVa | - | 0 |
| Grade IVb | - | 0 |
| TOTAL | 71 |
Table 3.
Spearman’s rank correlations among SF-36 items and preoperative and postoperative variables. Rho coefficient is reported, (*) indicates coefficient with a p-value < 0.10. PF = physical function; RP = role-physical; BP = bodily pain; GH = general health; VT = vitality; SF = social function; RE = role-emotional; MH = mental health; PCS = Physical Component Summary; MCS = Mental Component Summary; LLD = lower limb length discrepancy.
Table 3.
Spearman’s rank correlations among SF-36 items and preoperative and postoperative variables. Rho coefficient is reported, (*) indicates coefficient with a p-value < 0.10. PF = physical function; RP = role-physical; BP = bodily pain; GH = general health; VT = vitality; SF = social function; RE = role-emotional; MH = mental health; PCS = Physical Component Summary; MCS = Mental Component Summary; LLD = lower limb length discrepancy.
| PF | RP | BP | GH | VT | SF | RE | MH | PCS | MCS | |
|---|---|---|---|---|---|---|---|---|---|---|
| Lengthening cycles | 0.14 | -0.07 | 0.04 | -0.07 | 0.09 | 0.01 | -0.04 | -0.10 | 0.06 | -0.09 |
| Age at first surgery | -0.05 | -0.09 | 0.06 | -0.12 | 0.05 | -0.10 | -0.10 | -0.10 | -0.03 | -0.06 |
| Age at questionnaire | -0.21 | -0.07 | -0.11 | -0.37* | -0.29 | -0.17 | -0.14 | -0.15 | -0.21 | -0.18 |
| Preoperative LLD | -0.14 | -0.09 | -0.31* | -0.26 | -0.04 | -0.16 | -0.10 | -0.06 | -0.33* | -0.09 |
| Total lengthening | 0.15 | -0.07 | 0.05 | -0.08 | 0.09 | 0.01 | -0.04 | -0.10 | 0.01 | -0.09 |
| Complications | 0.05 | -0.15 | 0.08 | -0.05 | -0.01 | 0.13 | -0.06 | -0.25 | 0.08 | -0.19 |
| Minor complications | 0.02 | -0.01 | 0.14 | -0.05 | -0.04 | 0.05 | 0.04 | -0.15 | 0.08 | -0.09 |
| Major complications | -0.04 | -0.25 | -0.04 | -0.10 | 0.05 | 0.06 | -0.14 | -0.27 | -0.03 | -0.22 |
| Total treatment time | -0.08 | -0.21 | -0.23 | -0.23 | -0.01 | -0.18 | -0.28 | -0.19 | -0.14 | -0.27 |
| Healing index | -0.22 | -0.13 | -0.25 | -0.17 | -0.12 | -0.21 | -0.27 | -0.18 | -0.23 | -0.27 |
| Residual LLD | -0.31* | -0.20 | -0.28 | -0.28 | -0.15 | -0.23 | -0.20 | -0.17 | -0.34* | -0.19 |
| Follow-up | 0.01 | 0.02 | 0.02 | 0.08 | -0.05 | 0.02 | 0.02 | 0.01 | 0.07 | -0.01 |
Table 4.
Results of single items of Stanmore Limb Reconstruction Score (SLRS).
| Pain | Sleep | Social | PF | Hygiene | Leisure | Work | Future | Emotions | Consmetic | |
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | 84 | 73 | 81 | 87 | 96 | 70 | 89 | 73 | 61 | 54 |
| Median | 87 | 75 | 88 | 95 | 100 | 75 | 100 | 75 | 60 | 50 |
| Range | 46-100 | 13-100 | 25-100 | 8-100 | 25-100 | 0-100 | 13-100 | 25-100 | 15-100 | 10-100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



