
Submitted:
20 August 2024
Posted:
22 August 2024
You are already at the latest version
Abstract
Ovarian torsion (OT) is a rare gynaecological emergency that requires a prompt diagnosis for optimal patient management. To determine whether there were any biomarkers suitable for the non-invasive detection of OT, two independent reviewers performed systematic searches of five literature databases following Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. Full-texts of 24 selected articles were assessed for risk of bias and quality assurance using a modified Newcastle-Ottawa Scale (NOS). 15 articles described studies on animals and all described serum biomarkers comparing results between OT versus a sham operation, a control group or readings before and after OT. Ischaemia modified albumin (IMA), serum D-dimer (s-DD), heat shock protein-70 (hsp-70), Pentraxin-3 (PTX-3) and c-reactive protein (CRP) showed the most promise, each with p-values for the difference between groups achieving ≤0.001. In studies of humans, the biomarkers ranged from 16.4-92.3% sensitivity and 77-100% specificity. The most promising biomarkers for the early prediction of OT in patients included s-DD, interleukin-6 (IL-6), IMA and tumour necrosis factor-alpha (TNF-. IL-6 had the highest sensitivity of any biomarker identified in this review and was raised in all 13 patients with proven OT, with values of ≥10.2pg/ml, indicative of a 16 times higher risk of having OT. Signal peptide, CUB domain and EGF like domain containing 1 (SCUBE1) had a high specificity at 93.3%, second only to s-DD and a positive likelihood ratio (LR)>10. IMA was the only other biomarker that also had a positive LR>10, making it a promising diagnostic biomarker. The studies identified by this systematic literature review each analysed small patient groups but IMA, DD and SCUBE1 nevertheless showed promise as serum biomarkers with a pooled LR>10. However, further well-designed studies are needed to identify and evaluate individual markers, or diagnostic panels to help clinicians manage this important, organ-threatening condition.
Keywords:
ovarian torsion
; biomarker
; non-invasive
; blood
; IL-6
; systematic review
1. Introduction
Ovarian torsion (OT) is a rare gynaecological emergency that requires prompt surgical intervention to prevent ovarian ischaemia, necrosis and loss of function. OT affects approximately 9.9/100,000 women of reproductive age each year [1]. OT arises when the ovary twists over its supporting ligaments in the adnexa [2], and in combination with the fallopian tube is termed an adnexal torsion (AT). OT is most commonly associated with benign cysts greater than 5cm [3], but 20% occur in pre-pubescent girls, 50% of whom have normal sized ovaries but may have elongated infundibulopelvic ligaments [4]. People who are pregnant or undergoing fertility treatments are at particular risk of OT due to enlarged follicles on the ovary [5].
OT frequently presents with symptoms such as acute onset pain, nausea and vomiting [6] making differentiating OT from acute abdomen difficult. Ultrasound (US) is reported to have a sensitivity of 84% and common findings include large oedematous ovaries, free pelvic fluid and the “whirlpool” sign (WS) arising from twisted vascular pedicles [4]. Surgical intervention, normally in the form of diagnostic laparoscopy, is the gold standard for the diagnosis of OT; furthermore, it enables concurrent treatment. In premenopausal women, this is now routinely undertaken based on clinical findings even when the US is normal, to preserve ovarian function [7]. Novoa et al. [8] reported that only one in five necrotic appearing ovaries were confirmed histopathologically [7]. Where there is a significant diagnostic delay, or in the presence of other complicating factors, an oophorectomy may still need to be performed. The consequences of this remain uncertain [9], although the impact on quantity but not quality of the ovarian reserve can adversely affect women seeking assisted reproductive techniques [10].
The risk of a serious complication from a gynaecological laparoscopy [11] is approximately 2 per 1000, but can include organ damage or major vessel injury both associated with significant morbidity and mortality [12]. The long-term consequences of bilateral oophorectomy is increasingly understood and may increase the risk of all-cause mortality, coronary artery diseases and non-gynaecological cancers [13,14,15,16,17]. The need to preserve ovaries should therefore be considered for reasons more than just maintaining reproductive function.
Although potential diagnostic biomarkers for OT have been identified few have evidence to support their use in clinical practice. This study aims to compare non-invasive biomarkers for the detection of OT, identified in animal models and human studies, and to determine their potential to provide an early non-invasive indication of OT.
2. Results
2.1. Screened Studies Selected for Systematic Review
This study was registered with the International prospective register of systematic reviews (PROSPERO) 2022 CRD42022370628 (Table S1). The search amassed 335 articles on blood biomarkers for OT (Figure 1). For the purpose of the literature searches we used prespecified inclusion/exclusion criteria (Table 1) to screen articles on title and abstract resulting. At the stage of abstract reading our search excluded books, systematic reviews, meta-analyses and conference papers. The articles were then screened by full text, with 24 meeting the eligibility criteria to be included in further analysis (Table S2).
2.2. Quality Assurance
The full-text versions of the 24 articles were assessed for eligibility and quality assurance using a modified Newcastle Ottawa Scale (NOS) [18](Table 2). None of them were excluded at this step (Table S3) and all met the requirements for data extraction. All had a good rating except Karatas Gurgun et al., 2017 [19] was deemed fair.
2.3. b Comparability between Studies
The extracted data was entered into the RevMan 5 tool [43](Figure 2). Each of the human trial articles reported the sensitivity and specificity of each biomarker (Figure 3A) while the animal model papers used serum biomarker concentrations (Table 3) or absorbance units (AU) [19,20,28]. The authors did not respond to requests to provide individual or pre-operative biomarker levels, or median and interquartile range of the results. Thus, the varied study designs and different units utilised for measuring each biomarker prevented meta-analysis on the animal studies.
2.3. c Biomarkers Studied Only in Animal Models
Plasma heat shock protein 70 (plasma HSP70; [22]) and pentraxin-3 (PTX3), were examined in animal models only. Plasma HSP70 belongs to a family of proteins that are released in response to cellular stress [44]. The authors randomised 21 Winstar albino rats into three groups: a torsion group, a sham operation group and no operation, and blood was sampled after 12h. There was an increase in HSP70 in the torsion group (1.75ng/ml) compared to both laparotomy (1.16ng/ml) and control groups (1.19ng/ml). Akman et al. [11] examined PTX3, which is a protein involved in the innate immune response [45]. The authors used 16 Sprague-Dawley rats and induced ischaemia for 3h. They found that mean PTX3 was significantly higher in the torsion group (2.13ng/ml) versus the control (1.07ng/ml). CRP was also examined in one mouse model study (33), where the authors also found higher concentrations of CRP in the torsion group.
2.3. d Biomarkers of OT Studied in Human Subjects
Of the articles that focussed solely on human studies, seven potential biomarkers were identified. These were IL-6, serum D-dimer (s-DD), neutrophil to lymphocyte ratio (NLR), Ferric Reducing Ability of Plasma (FRAP), GSH, ischaemia modified albumin (IMA) and malondialdehyde (MDA)(Table 3). Four articles explored the use of inflammatory ratios to diagnose OT [29,31,34,38]. Each assessed NLR while Nissen et al. [38] also analysed platelet to lymphocyte ratio (PLR). Ratios may give a more accurate indication of an acute inflammatory state [38] and while the cause of these ratios in patients experiencing OT has not been extensively studied, there is a possibility that they could aid with diagnosing and monitoring treatment response.
NLR was found to increase in OT compared to the controls [29,31,38] but there was a broad range of results (16-92% sensitivity [31,38]; 70.7-91% specificity [29,34])(Figure 3A) which may be explained by study design. Aiob et al. [31] combined NLR with sonographic findings while all other studies assessed NLR alone. In addition, Nissen et al. [38] focused on paediatric OT only (3 days old to 17 years 8 months old) whereas all other studies included both adult and paediatric populations.
Aiob et al. had a far larger sample size (n=278; [31]) compared to Yilmaz et al. (n=136; [29]), Ghimire et al. (n=125; [34]) and Nissen et al. (n=92; [38]). Only Yilmaz et al. [29] reported a cut-off value (2.44 NLR) which limited our capacity to perform comparative analysis. Nissen et al. [38] also found that PLR had a lower specificity (82%) but higher sensitivity (90%), the “strongest discriminatory accuracy” and was independently predictive of OT. Again, the focus on paediatric participants may limit the applicability of these findings to the wider population.
2.3. c Biomarkers Studied in Humans and Animal Models
Certain biomarkers were studied in both animal models and patients, including s-DD, IMA, IL-6 and signal peptide, CUB domain and EGF like domain containing 1 (SCUBE1). S-DD is a well-established biomarker used to assess the presence of blood clot formation and fibrinolysis [46] and could be useful due to their association with OT [47]. The potential of s-DD was assessed in animal models [19,25] and humans [35,37,40]. Kart et al. [25] and Karatas Gurgun et al. [19] had similar study designs, and both found that DD increased in the torsion group although Karatas Gurgun et al. used 24 Wistar Albino rats and Kart et al. used 16 Sprague Dawley rats. However, Karatas Gurgun et al. [19] found a far higher concentration of DD in rats 4h after bilateral ovarian rotation compared to sham controls (p=0.001) that may be accounted for by the fact Kart et al. used a unilateral OT model. In addition, Karatas Gurgun et al. induced ischaemia for longer (4h) than Kart et al. who used 2h.
Gu et al. [35] and Incebiyik et al. [37] had a similiar number of human participants (n=28 and n=34, respectively) compared to Topçu et al. [40](n=17). Topçu et al. [40] studied pregnant women with ovarian cysts who suffered from pelvic pain and found elevated s-DD levels in patients with surgically proven AT (77% versus 21%, p<0.01). They noted that elevated s-DD and a cyst diameter >5cm yielded the highest sensitivity (82%) while the presence of nausea and vomiting alongside elevated c-reactive protein (CRP) had the highest specificity (>85%). Plasma D-dimer (pls-DD) was significantly higher in women who were found to have an adnexal mass compared to those with benign ovarian cysts (p=0.002). When a cut-off value of 0.65µg/ml was used, the sensitivity and specificity for detecting AT was 71.4% and 85%, respectively [37](Figure 3A). Gu et al. [35] described the use of sonographic markers (WS and pls-DD) and a laboratory index for AT in women presenting with a benign ovarian mass, abdominal pain and clinically suspected AT. They observed an increase in WS and pls-DD levels in women with AT (cut-off level 248ng/ml), compared to those without (p<0.01).
Oxidative stress markers were examined in five studies. IMA is a biomarker used to assess ischemic conditions and measures alterations in the structure of albumin which occur in response to tissue ischaemia. Four studies assessed IMA only in animal models [19,20,28,48] and examined induced ischaemia for 3-4h, although Karatas Gurgun et al. [19] and Lazăr et al. [48] took additional measurements over 24h. Aside from Aran et al. [20], the papers took post-operative samples only. Results were overall promising, with three of the studies [20,28,48] finding a statistically significant increase in the IMA value. However, no statistically significant difference was identified by Karatas Gurgun et al. [19]. Guven et al. [36] showed that the oxidative stress marker, MDA, total oxidant status (TOS) and total antioxidant status (TAS) were all significantly higher in the torsion (n=14) compared to the control group (n=20). The authors also found IMA had a relatively high sensitivity (90%), specificity (92.31%) and an LR = +11.7 (Figure 3B). Surprisingly, TAS, TOS and Oxidative Stress Index (OSI) were highest in the control group that did not have OT.
IL-6 is a cytokine that contributes to the local inflammatory response in OT [49] and was the most observed biomarker in human [30,32,33,39] but not animal studies [24]. It has several roles in OT, such as the recruitment of immune cells [50] and angiogenesis to restore blood flow in the torsed ovary [51]. A study by Reed et al. [39] found that IL-6 was elevated in patients with OT compared to non-surgical controls; however, there was no difference in IL-6 levels between patients with OT and appendicitis. In contrast, Cohen et al. [32] did find higher IL-6 levels in the torsion group. There was a substantial difference between the sensitivity reported by Zangene et al. (41.79%; n=284 [30]) and Daponte et al. (92.3%; n=37 [33]) although the specificity was closer (82.49% and 78.1%, respectively). This variation could be due to the larger sample size in Zangene et al. as well as the slight difference in cut-off values used in each study - 9.9pg/ml in Zangene et al. [30] versus 10.2pg/ml in Daponte et al. [33].
Uzun et al. 2018 [27] found a statistically significant increase in mean SCUBE1 levels (p<0.01) in rats that were subjected to bilateral OT and ischaemia lasting 24h compared to rats that experienced bilateral OT and ovarian ischaemia for 8h or the sham group that were only given a laparotomy procedure; however, Gunaydin et al. 2019 [23] found no difference between SCUBE1 levels after 4h of unilateral torsion suggesting this is not an early indicator of OT. Uyanikoglu et al. [41] noted a statistically significant increase in SCUBE1 (1.40ng/ml versus 1.22ng/ml) in patients with OT versus the control group, with a positive LR >10. Reported sensitivity was 80% and specificity 93.3%.
3. Discussion
The reasons behind the delayed diagnosis of OT are complex; however, it is apparent that poor diagnostic tools are a key contributing factor to its impact on human health. The accuracy of a US diagnosis is highly dependent on operator skill and experience. It has been reported to be as low as 23%-66% [52] which is exacerbated by the time-critical nature of an OT diagnosis and reliance on access to a skilled gynaecological sonography, which is often limited out-of-hours. There is no consensus of opinion as to whether immediate surgical intervention has consistently better outcomes than awaiting investigations [53]. This is due in part to the limitations of currently available diagnostic techniques, avoidance of unnecessary surgical intervention and uncertainty about the window prior to irreversible adnexal ischaemia. However, an accurate diagnostic test would aid clinicians in managing this rare, but serious gynaecological emergency.
Eight biomarkers were identified in this review; and overall, the sensitivity of the biomarkers across the eligible studies on humans ranged from 22% to 100% and the specificity ranged from 60% to 100%. Promising biomarkers for the early prediction of OT included SCUBE1, s-DD, IL-6, IMA, and tumour necrosis factor-alpha (TNF-α). However, none thus far have been identified as clinically useful.
DD was widely used in clinical practise as a screening tool for venous thromboembolism (VTE) and to guide therapeutic anti-coagulation in unprovoked VTE [54]. Although the sensitivity reported in each paper was unremarkable; the specificity showed more promise. Notably, DD was the only biomarker that had a specificity of 100% [35], although this was not replicated in the two other articles assessing DD which reported specificities of 78% and 84% (range 78-100%)[37,40]. The limitations of DD testing in current clinical practice are caused by variations due to age, pregnancy, VTE, malignancy and testing method that have been widely discussed [54]. It should be noted that Gu et al. [35] excluded 26/94 participants due to this. Malignancy and pregnancy are both significant risk factors for OT and excluding these will elevate specificity of DD but limit its clinical application. All of these factors would need to be addressed prior to DDs integration into clinical practise, however, it is plausible that DD could be used as a tool to rule-out OT.
SCUBE1, IL-6 and IMA also showed significant potential in human trials, although a larger sample size would be needed to confirm this. IL-6 had the highest sensitivity of any biomarker assessed in this review [33] and was raised in all 13 patients with proven OT, with values of ≥10.2pg/ml, indicative of a 16 times higher risk of having OT. SCUBE1 had a high specificity at 93.3%, second only to DD. Most importantly, SCUBE1 had a positive LR>10. IMA was the only other biomarker that also had a positive LR>10, making it a promising diagnostic biomarker. However, SCUBE1, IL-6 and IMA can be raised in other pathologies, especially chronic inflammatory and autoimmune diseases. Therefore, the use of these biomarkers alone may not be specific enough to identify OT.
Animal model results mirrored those seen in humans. Almost all the animal model papers found statistically significant increases in the biomarkers they were assessing. The exception to this was Gunaydin et al. [23] who assessed IMA. Plasma HSP70 and PTX3 were the only two biomarkers that were assessed in animal model papers alone [11,22]. Both studies found an increase in the torsion group, however it was notable that there was only one paper on each biomarker, thus further investigation is needed before human trials could be considered. In addition, it is important to consider that these biomarkers are not commonly used in healthcare. Therefore, it may be difficult to introduce them into clinical practice.
Preliminary research should continue to help identify more specific biomarkers. However, given the nature of the pathology and similarity of underlying mechanisms such as ischaemia and inflammation being present in many of the differential diagnoses, this may not be possible. At this stage, it seems unlikely that a non-invasive biomarker could be a gold-standard diagnostic tool. Therefore, a combination of biomarkers, or biomarkers and clinical findings may be a better way of identifying OT. This question was explored by Gu et al. [35], who found a sensitivity of 96.43% and a specificity of 100% when DD was combined with US. Further work could determine whether US can improve the sensitivity and specificity of other biomarkers.
A notable finding from this literature search was the focus on venous blood biomarkers. This leaves urine and vaginal fluid as unexplored areas that could be used as a source for more sensitive and specific biomarker(s). It was also noteworthy that the studies amassed from this systematic literature review each had small sample sizes. This may reflect the infrequency by which OT occurs; however larger studies will be needed for a fuller interpretation of sensitivity and specificity of the biomarkers.
Limitations of this study included the heterogeneity of the objectives, inclusion criteria, participant recruitment and methodology of the human studies selected by this systematic review. In addition, the methodology and study design varied notably amongst the animal model studies. The absence of pre-operative measurements in six studies [19,23,24,27,28,48] made it difficult to assess the extent of the increase of each biomarker. Another problem was the lack of standardisation between the methods used ie there was variation between the degree of adnexal twisting, whether it was unilateral or bilateral, and the length of time that ischaemia was induced for.
4. Materials and Methods
4.1. Systematic review
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were adhered to [55,56] including the development of a Protocol (Table S1) and prospective registration. In accordance with Population Intervention Comparator Outcome (PICO) framework to formulate our research question, which was ‘Are there non-invasive biomarker(s) that would facilitate the detection of ovarian torsion?’ In the animal studies, population were rats with surgically induced OT, intervention were non-invasive biomarkers that predict OT, comparators were rats without torsion, and outcome was whether the biomarker level was raised. In human studies, population were adults with OT, interventions were non-invasive biomarkers that predicted OT, comparators were patients with OT symptoms which were not confirmed and the outcome was timely treatment saving the ovary and indications of no negative impact on fertility.
The search strategy was developed based on index terms that were found in three to six sentinel articles that were identified following an initial screen of the literature using PubMed. Published manuscripts focusing on OT and non-invasive biomarkers were identified using MeSH search terms as follows biomarker* OR “biological marker*” OR “metabolic process” OR “disease diagnosis” OR “molecular marker*” OR “signature molecule*” OR “bio* indicator*” OR “blood indicator*” Blood OR “blood sample*” OR “blood analysis” AND “Ovar* torsion” OR “Adnexal torsion”.
We identified articles in five online databases (PubMed, Medline, Scopus, Cochrane and CINAHL) from inception until October 1st, 2023. Excel was used to exclude duplicated studies (Table S2), then the articles were screened by title and abstract. The studies remaining were assessed against the inclusion criteria to determine their appropriateness for this review.
Studies assessed were not limited by language, and included patients with OT that had quantified biomarker expression; with no age, geographical location, publication date, or setting restrictions (Table 1). Articles were excluded if OT was found incidentally or were based on qualitative analyses.
Review articles were only removed once the cited articles in all selected manuscripts had been screened against the inclusion/exclusion criteria as detailed above. This ‘backward snowballing’ step helped to ensure that all relevant literature was successfully found as part of this systematic review [57].
4.2. Bias Quality Assessment
A modified NOS for Assessing the Quality of Nonrandomized Studies in Meta-Analysis [18] was used to perform a quality assurance assessment of the selected studies. The studies were assessed based on selection, comparability and outcome, and were ranked from zero to four stars. Zero stars signified a lack of the information required, and four stars signified that nothing else could be added and that the information perfectly matched the criteria. An adapted version was used for animal studies (Table S3A).
4.3. Data Extraction
For standardisation, a data extraction form was piloted in Excel using several selected studies with input from all reviewers. This included fields for study methodology, type of specimen (ie blood), sample size, outcomes as well as the sensitivity and specificity of the biomarker. Both G.D. and M.N. performed the data extraction and any queries were resolved through discussions between them or where an agreement could not be reached a third reviewer (B.G.) was consulted.
4.4. Meta-Analysis
Data analysis was performed using RevMan (©2022 The Cochrane Collaboration). Data imported into RevMan consisted of the total number of OT cases in the control group compared to the intervention group. RevMan was then used to create box plots representing the pooled data for each biomarker. The likelihood ratios (LR) were calculated for all the studies that presented their sensitivity and specificity. To enable this where specificity was presented as 100%, a small constant (0.01) was subtracted from all values for specificity. Values above 10 were considered strong evidence to rule in OT.
5. Conclusions
Standardization of study methodology would enable more reliable identification of potential biomarkers for the early detection of OT. This review sought to identify the most promising biomarkers for the early detection of OT and this is the first systematic review to evaluate the state-of-the-art in non-invasive biomarkers for diagnosing OT as examined in animal models and patients. IMA, DD and SCUBE1 show promise as markers with a pooled LR>10 in humans with OT. However, further well-designed trials are needed to identify and evaluate individual markers, or diagnostic panels to help clinicians manage this important, organ-threatening condition.
Supplementary Materials
Supplementary Data can be found at https://zenodo.org/records/10072094 as follows - Table S1: Protocol; Table S2A and S2B SLR; Table S3A: Adapted NOS for animal studies; Table S3B: Adapted NOS scoring.
Author Contributions
The following statements should be used Conceptualization, T.A.; methodology, M.N. and G.D.; validation, M.N., and G.D.; formal analysis, M.N., G.D., H.D. and A.R.; data curation, M.N., G.D., H.D. and A.R.; writing—original draft preparation, G.D. and M.N.; writing—review and editing, B.G.; supervision, B.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by an INSPIRE grant awarded to the Hull York Medical School by the Academy of Medical Sciences through the Wellcome Trust [Ref: IR5\1018](MN). HD was funded by a Hull University Teaching Hospitals NHS Trust Clinical Fellowship and a British Society for Gynaecological Endoscopy grant. DF by a HIKE-MRC Impact Accelerator grant.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
The original data presented in the study are openly available in zenodo.org at https://zenodo.org/records/10072094.
Acknowledgments
We would like to thank Dr Heidi Baseler who runs the INSPIRE program at the Hull York Medical School and all patients whose data contributed to this work.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
Abbreviations
| AT | adnexal torsion | HSP70 | Heat Shock Protein 70 |
| AU | Absorbance Units | s- or pls-DD | Serum or plasma D-dimer |
| CRP | c-reactive protein | PLR | platelet to lymphocyte ratio |
| FRAP | Ferric Reducing Ability of Plasma | PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| GSH | Glutathione | PROSPERO | International prospective register of systematic reviews |
| IL-6 | interleukin-6 | PTX3 | pentraxin-3 |
| IMA | Ischaemia Modified Albumin | SCUBE 1 | Signal peptide, CUB domain and EGF like domain containing 1 |
| LR | likelihood ratio | SOD | superoxide dismutase |
| MDA | Malondialdehyde | TAS | Total Antioxidant Status |
| NLR | neutrophil to lymphocyte ratio | TOS | Total Oxidant Status |
| NOS | Newcastle Ottawa Scale | US | ultrasound |
| OSI | Oxidative Stress Index | VTE | venous thromboembolism |
| OT | ovarian torsion | WS | Whirlpool sign |
| PICO | Population Intervention Comparator Outcome |
References
- ACOG Committee Opinion No. Adnexal Torsion in Adolescents. Obstetrics and Gynecology 2019, 134, 435–436. [CrossRef]
- Guile, S.M., J. . Ovarian Torsion. StatPearls Publishing 2022.
- White, M.; Stella, J. Ovarian torsion: 10-year perspective. Emerg Med Australas 2005, 17, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Shetty, M. Acute Pelvic Pain: Role of Imaging in the Diagnosis and Management. Semin Ultrasound CT MR 2023. [CrossRef]
- Mahonski, S.; Hu, K.M. Female Nonobstetric Genitourinary Emergencies. Emerg Med Clin North Am 2019, 37, 771–784. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Hong, M.K.; Ding, D.C. A review of ovary torsion. Ci Ji Yi Xue Za Zhi 2017, 29, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Balachandren, N., Yasmin, E., Mavrelos, D., Saridogan, E. Does ovarian cystectomy pose a risk to ovarian reserve and fertility? The Obstetrician and Gynaecologist 2020, 23, 28–37.
- Novoa, M.; Friedman, J.; Mayrink, M. Ovarian torsion: can we save the ovary? Arch Gynecol Obstet 2021, 304, 191–195. [Google Scholar] [CrossRef]
- Gasparri, M.L.; Ruscito, I.; Braicu, E.I.; Sehouli, J.; Tramontano, L.; Costanzi, F.; De Marco, M.P.; Mueller, M.D.; Papadia, A.; Caserta, D.; et al. Biological Impact of Unilateral Oophorectomy: Does the Number of Ovaries Really Matter? Geburtshilfe Frauenheilkd 2021, 81, 331–338. [Google Scholar] [CrossRef]
- Younis, J.S.; Naoum, I.; Salem, N.; Perlitz, Y.; Izhaki, I. The impact of unilateral oophorectomy on ovarian reserve in assisted reproduction: a systematic review and meta-analysis. BJOG 2018, 125, 26–35. [Google Scholar] [CrossRef]
- Akman, L.; Erbas, O.; Terek, M.C.; Aktug, H.; Taskiran, D.; Askar, N. The long pentraxin-3 is a useful marker for diagnosis of ovarian torsion: An experimental rat model. J Obstet Gynaecol 2016, 36, 399–402. [Google Scholar] [CrossRef]
- Brierley, G.; Arshad, I.; Shakir, F.; Visvathanan, D.; Aramabage, K. Vascular injury during laparoscopic gynaecological surgery: a methodological approach for prevention and management. The Obstetrician and Gynaecologist 2020, 22, 191–198. [Google Scholar] [CrossRef]
- Parker, W.H.; Broder, M.S.; Chang, E.; Feskanich, D.; Farquhar, C.; Liu, Z.; Shoupe, D.; Berek, J.S.; Hankinson, S.; Manson, J.E. Ovarian conservation at the time of hysterectomy and long-term health outcomes in the nurses’ health study. Obstet Gynecol 2009, 113, 1027–1037. [Google Scholar] [CrossRef] [PubMed]
- Jett, S.; Schelbaum, E.; Jang, G.; Boneu Yepez, C.; Dyke, J.P.; Pahlajani, S.; Diaz Brinton, R.; Mosconi, L. Ovarian steroid hormones: A long overlooked but critical contributor to brain aging and Alzheimer’s disease. Front Aging Neurosci 2022, 14, 948219. [Google Scholar] [CrossRef] [PubMed]
- Manolagas, S.C.; Kousteni, S. Perspective: nonreproductive sites of action of reproductive hormones. Endocrinology 2001, 142, 2200–2204. [Google Scholar] [CrossRef]
- Farland, L.V.; Rice, M.S.; Degnan, W.J., 3rd; Rexrode, K.M.; Manson, J.E.; Rimm, E.B.; Rich-Edwards, J.; Stewart, E.A.; Cohen Rassier, S.L.; Robinson, W.R.; et al. Hysterectomy With and Without Oophorectomy, Tubal Ligation, and Risk of Cardiovascular Disease in the Nurses’ Health Study II. J Womens Health (Larchmt) 2023, 32, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Hassan, H.; Allen, I.; Sofianopoulou, E.; Walburga, Y.; Turnbull, C.; Eccles, D.M.; Tischkowitz, M.; Pharoah, P.; Antoniou, A.C. Long-term outcomes of hysterectomy with bilateral salpingo-oophorectomy: a systematic review and meta-analysis. Am J Obstet Gynecol 2023. [CrossRef]
- Wells, G., Shea, B., O’Connell, D., Peterson, J., Welch, V., Losos, M., Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analysis. https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp 2021.
- Karatas Gurgun, A.; Kaban, I.; Aka, N.; Mentese, A.; Aker, F.; Uras, A.R. The Role of Ischemia Modified Albumin and D-dimer as Early or Late Biochemical Markers in Ovarian Torsion. J Obstet Gynaecol Res 2017, 43, 895–901. [Google Scholar] [CrossRef]
- Aran, T.; Guven, S.; Unsal, M.A.; Alver, A.; Mentese, A.; Yulug, E. Serum ischemia-modified albumin as a novel marker of ovarian torsion: an experimental study. Eur J Obstet Gynecol Reprod Biol 2010, 150, 72–75. [Google Scholar] [CrossRef]
- Bakacak, M.; Kostu, B.; Ercan, O.; Bostanci, M.S.; Kiran, G.; Aral, M.; Ciralik, H.; Serin, S. High-sensitivity C-reactive protein as a novel marker in early diagnosis of ovarian torsion: an experimental study. Arch Gynecol Obstet 2015, 291, 99–104. [Google Scholar] [CrossRef]
- Cilgin, H.; Simsek, M.; Bal, R. Can adnexal torsion be predicted by measuring plasma heat shock protein 70 level? An experimental study. Arch Gynecol Obstet 2017, 296, 941–946. [Google Scholar] [CrossRef]
- Gunaydin, M.; Sipahi, M.; Kesicioglu, T.; Usta, M.; Tezcan, B.; Tokgoz, V.Y. The value of plasma SCUBE1 and oxidative stress parameters in the early diagnosis of acute ovarian torsion. Bratisl Lek Listy 2019, 120, 456–461. [Google Scholar] [CrossRef]
- Karakoc-Sokmensuer, L.; Hacivelioglu, S.; Demir, A.; Kose, M.; Kaymaz, F.F.; Cakir, D.U.; Bozdag, G. Histopathology of ipsilateral and contralateral ovaries and plasma interleukin 6 levels after unilateral ovarian torsion. Clin Exp Obstet Gynecol 2016, 43, 82–87. [Google Scholar] [CrossRef]
- Kart, C.; Aran, T.; Guven, S.; Karahan, S.C.; Yulug, E. Acute increase in plasma D-dimer level in ovarian torsion: an experimental study. Hum Reprod 2011, 26, 564–568. [Google Scholar] [CrossRef]
- Lazăr, C., , Vozian, M., Pantea, V., Mișina, A., Tagadiuc, O. . Ischemia modified albumin in experimental ovarian torsion with and without controlled reperfusion. Revista Romana de Medicina de Laborator 2019, 27, 43–50. [CrossRef]
- Uzun, O.; Kaban, I.; Midi, A.; Uysal, H.; Boran, A.B.; Bacanakgil, B.H.; Tarbaghia, M. Diagnostic value of signal peptide-CUB-EGF domain-containing protein 1 as an early and late biochemical marker in the ovarian torsion rat model. J Obstet Gynaecol Res 2018, 44, 1092–1099. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, A.; Yildirim, S.; Topaloglu, N.; Tekin, M.; Kucuk, A.; Erdem, H.; Erbas, M.; Cakir, D.U. Correlation of ischemia-modified albumin levels and histopathologic findings in experimental ovarian torsion. Turk J Emerg Med 2016, 16, 8–11. [Google Scholar] [CrossRef]
- Yilmaz, M.; Cimilli, G.; Saritemur, M.; Demircan, F.; Isaoglu, U.; Kisaoglu, A.; Emet, M. Diagnostic Accuracy of Neutrophil/Lymphocyte Ratio, Red Cell Distribution Width and Platelet Distribution Width in Ovarian Torsion. J Obstet Gynaecol 2016, 36, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Zangene, M.; Ashoori Barmchi, A.; Rezaei, M.; Veisi, F. The comparison between the serum level of interleukin-6 in women with acute ovarian torsion and other causes of lower abdominal pain. J Obstet Gynaecol 2017, 37, 223–227. [Google Scholar] [CrossRef]
- Aiob, A.; Lowenstein, L.; Borik, I.; Naskovica, K.; Mikhail, S.M.; Odeh, M. The value of clinical symptoms, the neutrophil-to-lymphocyte ratio, and ultrasonographic features in predicting adnexal torsion: A case-control study. J Obstet Gynaecol Res 2023, 49, 289–295. [Google Scholar] [CrossRef]
- Cohen, S.B.; Wattiez, A.; Stockheim, D.; Seidman, D.S.; Lidor, A.L.; Mashiach, S.; Goldenberg, M. The accuracy of serum interleukin-6 and tumour necrosis factor as markers for ovarian torsion. Hum Reprod 2001, 16, 2195–2197. [Google Scholar] [CrossRef]
- Daponte, A.; Pournaras, S.; Hadjichristodoulou, C.; Lialios, G.; Kallitsaris, A.; Maniatis, A.N.; Messinis, I.E. Novel serum inflammatory markers in patients with adnexal mass who had surgery for ovarian torsion. Fertil Steril 2006, 85, 1469–1472. [Google Scholar] [CrossRef]
- Ghimire, A.; Ghimire, S.; Shrestha, A.; Pant, S.R.; Subedi, N.; Pant, P.R. Preoperative Neutrophil Lymphocyte Ratio in Prediction of Adnexal Mass Torsion. Obstet Gynecol Int 2023, 2023, 3585189. [Google Scholar] [CrossRef]
- Gu, X.; Yang, M.; Liu, Y.; Liu, F.; Liu, D.; Shi, F. The ultrasonic whirlpool sign combined with plasma d-dimer level in adnexal torsion. Eur J Radiol 2018, 109, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Guven, S.; Kart, C.; Guvendag Guven, E.S.; Cetin, E.C.; Mentese, A. Is the measurement of serum ischemia-modified albumin the best test to diagnose ovarian torsion? Gynecol Obstet Invest 2015, 79, 269–275. [Google Scholar] [CrossRef]
- Incebiyik, A.; Camuzcuoglu, A.; Hilali, N.G.; Vural, M.; Camuzcuoglu, H. Plasma D-dimer level in the diagnosis of adnexal torsion. J Matern Fetal Neonatal Med 2015, 28, 1073–1076. [Google Scholar] [CrossRef] [PubMed]
- Nissen, M.; Sander, V.; Rogge, P.; Alrefai, M.; Trobs, R.B. Neutrophil to Lymphocyte Ratio and Platelet to Lymphocyte Ratio Might Predict Pediatric Ovarian Torsion: A Single-Institution Experience and Review of the Literature. J Pediatr Adolesc Gynecol 2021, 34, 334–340. [Google Scholar] [CrossRef]
- Reed, J.L.; Strait, R.T.; Kachelmeyer, A.M.; Byczkowski, T.L.; Ho, M.L.; Huppert, J.S. Biomarkers to distinguish surgical etiologies in females with lower quadrant abdominal pain. Acad Emerg Med 2011, 18, 686–691. [Google Scholar] [CrossRef]
- Topcu, H.O.; Iskender, C.T.; Ceran, U.; Kaymak, O.; Timur, H.; Uygur, D.; Danisman, N. Evaluation of the Diagnostic Accuracy of Serum D-Dimer Levels in Pregnant Women with Adnexal Torsion. Diagnostics (Basel) 2015, 5, 1–9. [Google Scholar] [CrossRef]
- Uyanikoglu, H.; Hilali, N.G.; Yardimciel, M.; Koyuncu, I. A new biomarker for the early diagnosis of ovarian torsion: SCUBE-1. Clin Exp Reprod Med 2018, 45, 94–99. [Google Scholar] [CrossRef]
- Shamsrizi, P.; Gladstone, B.P.; Carrara, E.; Luise, D.; Cona, A.; Bovo, C.; Tacconelli, E. Variation of effect estimates in the analysis of mortality and length of hospital stay in patients with infections caused by bacteria-producing extended-spectrum beta-lactamases: a systematic review and meta-analysis. BMJ Open 2020, 10, e030266. [Google Scholar] [CrossRef]
- Lee-Robichaud, H.; Thomas, K.; Morgan, J.; Nelson, R.L. Lactulose versus Polyethylene Glycol for Chronic Constipation. Cochrane Database Syst Rev 2010. [CrossRef]
- Rylander, M.N.; Feng, Y.; Bass, J.; Diller, K.R. Thermally induced injury and heat-shock protein expression in cells and tissues. Ann N Y Acad Sci 2005, 1066, 222–242. [Google Scholar] [CrossRef]
- Porte, R.; Davoudian, S.; Asgari, F.; Parente, R.; Mantovani, A.; Garlanda, C.; Bottazzi, B. The Long Pentraxin PTX3 as a Humoral Innate Immunity Functional Player and Biomarker of Infections and Sepsis. Front Immunol 2019, 10, 794. [Google Scholar] [CrossRef]
- Ohara, T.; Farhoudi, M.; Bang, O.Y.; Koga, M.; Demchuk, A.M. The emerging value of serum D-dimer measurement in the work-up and management of ischemic stroke. Int J Stroke 2020, 15, 122–131. [Google Scholar] [CrossRef]
- Favresse, J.; Lippi, G.; Roy, P.M.; Chatelain, B.; Jacqmin, H.; Ten Cate, H.; Mullier, F. D-dimer: Preanalytical, analytical, postanalytical variables, and clinical applications. Crit Rev Clin Lab Sci 2018, 55, 548–577. [Google Scholar] [CrossRef] [PubMed]
- Lazăr, C., Vozian, M, Pantea, V, Mishina, A, Tagadiuc, O. . Ischemia modified albumin in experimental ovarian torsion with and without controlled reperfusion. In: Russian Open Medical Journal. 2019, 8. [CrossRef]
- Dugue, B.; Leppanen, E. Short-term variability in the concentration of serum interleukin-6 and its soluble receptor in subjectively healthy persons. Clin Chem Lab Med 1998, 36, 323–325. [Google Scholar] [CrossRef]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb Perspect Biol 2014, 6, a016295. [Google Scholar] [CrossRef] [PubMed]
- Kumari, N.; Dwarakanath, B.S.; Das, A.; Bhatt, A.N. Role of interleukin-6 in cancer progression and therapeutic resistance. Tumour Biol 2016, 37, 11553–11572. [Google Scholar] [CrossRef]
- Grunau, G.L.; Harris, A.; Buckley, J.; Todd, N.J. Diagnosis of Ovarian Torsion: Is It Time to Forget About Doppler? J Obstet Gynaecol Can 2018, 40, 871–875. [Google Scholar] [CrossRef] [PubMed]
- Yaakov, O.; Ashwal, E.; Gemer, O.; Peled, Y.; Kapustian, V.; Namazov, A.; Eitan, R.; Krissi, H. Acute Adnexal Torsion: Is Immediate Surgical Intervention Associated with a Better Outcome? Gynecol Obstet Invest 2022, 87, 100–104. [Google Scholar] [CrossRef]
- Linkins, L.A.; Takach Lapner, S. Review of D-dimer testing: Good, Bad, and Ugly. Int J Lab Hematol 2017, 39 Suppl 1, 98–103. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 2015, 4, 1. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef]
- Wohlin, C. Guidelines for snowballing in systematic literature studies and a replication in software engineering. EASE ‘14: Proceedings of the 18th International Conference on Evaluation and Assessment in Software Engineering 2014, 38, 1-10.
Figure 1.
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram. Searches of the databases PubMed, Medline, Scopus, Cochrane and CINAHL identified 335 articles that appeared to relate to the project title. The removal of any duplicated articles was followed by the selection of articles based on their title and/or abstract. Articles were then screened against the inclusion and exclusion criteria, and papers excluded due to the lack of quantified biomarkers for OT or assessing biomarkers for conditions that were not OT. After the final full text screening, the 24 articles remained were deemed to meet the inclusion criteria and fit the eligibility screening.
Figure 1.
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram. Searches of the databases PubMed, Medline, Scopus, Cochrane and CINAHL identified 335 articles that appeared to relate to the project title. The removal of any duplicated articles was followed by the selection of articles based on their title and/or abstract. Articles were then screened against the inclusion and exclusion criteria, and papers excluded due to the lack of quantified biomarkers for OT or assessing biomarkers for conditions that were not OT. After the final full text screening, the 24 articles remained were deemed to meet the inclusion criteria and fit the eligibility screening.
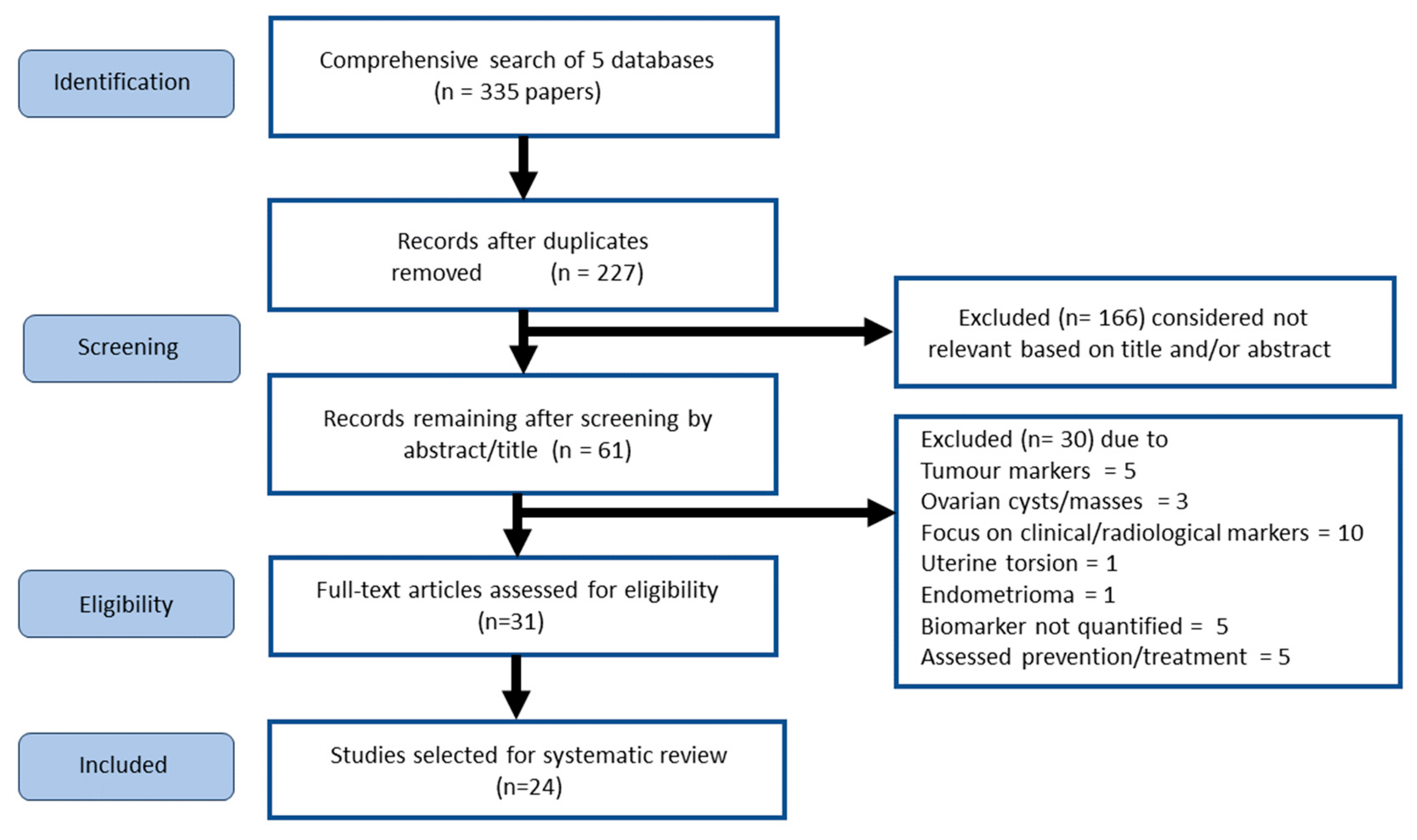
Figure 2.
Biomarker analysis of samples from human subjects with OT. (A) Interleukin-6 (IL-6) showed a significant heterogeneity P value of (p<0.00001), a highly varied I2 value of 100%, and an insignificant overall effect. Chi2 value was not statistically significant as 871.56 > 0.05. There was no significant difference in the favour of OT as indicated by IL-6 levels; (B) serum D-dimer (s-DD) showed an insignificant heterogeneity P value of (p<0.97), a I2 value of 0%, and a significant overall effect P value of (p<0.00001). The Chi2 value was not statistically significant; (C) NLR showed a significant heterogeneity (p<0.00001), a very varied I2 value of 96%, and an insignificant overall effect P value of (p=0.16). The Chi2 value was not significant, there was no significance that favoured NLR levels in OT compared with the control group; (D) There was no available data for the heterogeneity P or I2 value for glutathione (GSH), as only one paper had quantified data for analysis. The overall effect P value was significant (p=0.008); (E) IMA also had no available data for the heterogeneity P or I2 value, as only one paper had quantified data for analysis no comparison can be drawn. The overall effect P value was just significant (p=0.02).
Figure 2.
Biomarker analysis of samples from human subjects with OT. (A) Interleukin-6 (IL-6) showed a significant heterogeneity P value of (p<0.00001), a highly varied I2 value of 100%, and an insignificant overall effect. Chi2 value was not statistically significant as 871.56 > 0.05. There was no significant difference in the favour of OT as indicated by IL-6 levels; (B) serum D-dimer (s-DD) showed an insignificant heterogeneity P value of (p<0.97), a I2 value of 0%, and a significant overall effect P value of (p<0.00001). The Chi2 value was not statistically significant; (C) NLR showed a significant heterogeneity (p<0.00001), a very varied I2 value of 96%, and an insignificant overall effect P value of (p=0.16). The Chi2 value was not significant, there was no significance that favoured NLR levels in OT compared with the control group; (D) There was no available data for the heterogeneity P or I2 value for glutathione (GSH), as only one paper had quantified data for analysis. The overall effect P value was significant (p=0.008); (E) IMA also had no available data for the heterogeneity P or I2 value, as only one paper had quantified data for analysis no comparison can be drawn. The overall effect P value was just significant (p=0.02).

Figure 3.
Sensitivity, specificity and likelihood ratio of each biomarker as an indicator of OT or AT in studies of samples from human subjects. (A) Signal peptide, CUB domain and EGF like domain containing 1 (SCUBE1) had the highest sensitivity, while IMA had the highest specificity. The interquartile (box), range (whisker), sensitivities (blue) and specificities (green) for pooled data on each biomarker are shown; (B) Likelihood ratios (LR) with standard error of the mean calculated for each biomarker on studies that allowed it. Numerical marker points indicate article reference.
Figure 3.
Sensitivity, specificity and likelihood ratio of each biomarker as an indicator of OT or AT in studies of samples from human subjects. (A) Signal peptide, CUB domain and EGF like domain containing 1 (SCUBE1) had the highest sensitivity, while IMA had the highest specificity. The interquartile (box), range (whisker), sensitivities (blue) and specificities (green) for pooled data on each biomarker are shown; (B) Likelihood ratios (LR) with standard error of the mean calculated for each biomarker on studies that allowed it. Numerical marker points indicate article reference.
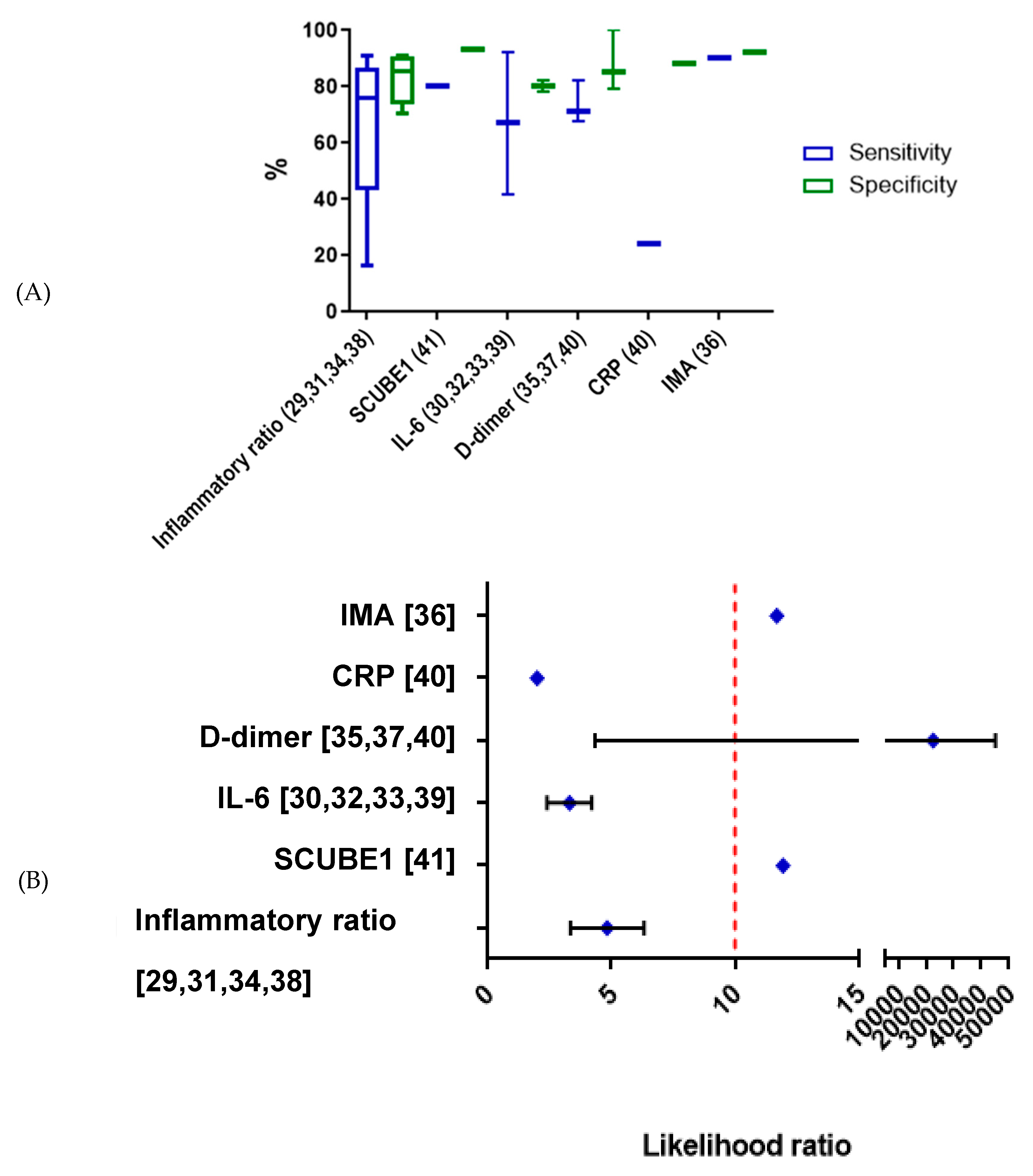

Table 1.
Exclusion/inclusion criteria.
| Inclusion | Exclusion |
|---|---|
| Primary literature sources: with reviews kept in until screening is completed to facilitate the benefits of reverse snowballing | Biomarkers are not directly quantified (qualitative biomarkers) |
| Humans and animal models | Cell lines |
| Patients diagnosed with OT | Disease other than OT |
| Quantitative biomarkers | Biomarkers for ovarian cancer |
| Have a quantified non-invasive blood biomarker expression which predicts OT | |
| All ages | |
| All geographical locations | |
| All publication dates |
Table 2.
A modified NOS criteria of Selection, Comparability and Outcome was applied to the selected studies. Studies that had zero stars would have been excluded, as these would have been deemed to not contain the depth of information required to be included in this review.
Table 2.
A modified NOS criteria of Selection, Comparability and Outcome was applied to the selected studies. Studies that had zero stars would have been excluded, as these would have been deemed to not contain the depth of information required to be included in this review.
| Paper | Selection | Comparability | Outcome | |
| Animal models | Akman et al., 2016 [11] |

|
|
|
| Aran et al., 2010 [20] |
|
|
|
|
| Bakacak et al., 2015 [21] |
|
|
|
|
| Çılgın et al., 2017 [22] |
|
|
|
|
| Gunaydin et al., 2019 [23] |
|
|
|
|
| Karakoc-Sokmenseur et al., 2016 [24] |
|
|
|
|
| Karatas Gurgun et al., 2017 [19] |
|
|
|
|
| Kart et al., 2011 [25] |
|
|
|
|
| Lazăr et al., 2019 [26] |
|
|
|
|
| Uzun et al., 2018 [27] |
|
|
|
|
| Yildirim et al., 2016 [28] |
|
|
|
|
| Yilmaz et al., 2015 [29] |
|
|
|
|
| Zangene et al., 2017 [30] |
|
|
|
|
| Clinical studies | Aiob et al., 2023 [31] |
|
|
|
| Cohen et al., 2001 [32] |
|
|
|
|
| Daponte et al., 2006 [33] |
|
|
|
|
| Ghimire et al., 2023 [34] |
|
|
|
|
| Gu et al., 2018 [35] |
|
|
|
|
| Guven et al., 2015 [36] |
|
|
|
|
| Incebiyik et al., 2015 [37] |
|
|
|
|
| Nissen et al., 2019 [38] |
|
|
|
|
| Reed et al., 2011 [39] |
|
|
|
|
| Topçu et al., 2015 [40] |
|
|
|
|
| Uyanikoglu et al., 2018 [41] |
|
|
|
The thresholds for converting the NOS to the Agency for Healthcare Research and Quality (AHRQ) standards [42] of good, fair or poor were applied as follows: good quality—three-to-four stars in the selection domain AND one-to-two stars in the comparability domain AND two-to-three stars in outcome domain; fair quality—two stars in selection domain AND one-to-two stars in comparability domain AND two-to-three stars in outcome domain; poor quality—zero-to-one star in selection domain OR zero star in comparability domain OR 0/1 star in outcome domain.
Table 3.
Animal studies of OT and AT.
| Article | Primary Data | P-value | Secondary Data | |||
| Aran et al., 2010 [20] |
Pre-operative IMA (AU) | Similar in both groups | Group 2 had increased follicular degeneration | |||
| Post-operative IMA (AU) | 0.05 | |||||
| Sham operation: 0.191 ± 0.034 | Torsion model: 0.277 ± 0.089 | |||||
| Akman et al., 2016 [11] |
Pentraxin-3 (PTX3) | Sham operation (ng/ml) | Torsion model (ng/ml) | |||
| Pre-operative levels (ng/ml) | 1.05 ± 0.20 | 1.09 ± 0.28 | >0.05 | Higher follicular degeneration in group | ||
| Post-operative levels (ng/ml) | 1.07 ± 0.22 | 2.13 ± 0.49 | 0.001 | |||
| Bakacak et al., 2015 [21] |
Sham operation | Torsion model | Higher follicular cell degeneration in group 2 | |||
| CRP levels | Pre-operative | 0.36±0.04 | 0.36±0.04 | 0.214 | ||
| (mg/l) | Post-operative | 0.39±0.06 | 0.91±0.18 | <0.001 | ||
| Çilgin et al., 2017 [22] |
Heat shock protein 70 (hsp-70; ng/ml) | No statistical difference between pre-operative levels (p= 0.966); P=0.001 for post-operative levels | ||||
| Torsion model (Group 1) |
Sham operation (Group 2) |
No operation (Group 3) |
||||
| Pre-operative | 1.19 (±0.13) | 1.18 (±0.78) | 1.15 (±0.49) | / | ||
| Post-operative |
1.75 (±0.25) | 1.16 (±0.99) |
1.19 (±0.11) |
Statistically significant difference between Group 1 and 2 (p=0.002), 1 and 3 p=0.002) but not 2 and 3 (p=0.561) | ||
| Gunaydin et al., 2019 [23] |
Control | Torsion | Increased vascular congestion and haemorrhage in the torsion group | |||
| SCUBE1 (ng/ml) | 1.83+0.16 | 1.82+0.18 | 0.987 | |||
| Superoxide dismutase (SOD)(U/ml) | 5.33+0.44 | 5.98+0.45 | 0.33 | |||
| malondialdehyde (MDA)(mmol/l) | 25.81+2.16 | 33.83+2.78 | 0.039 | |||
| Total antioxidant status (TAS; mmmol Trolox Evuiv/l) | 0.92+0.01 | 1.04+0.08 | 0.244 | |||
| Karakoc-Sokmensuer et al., 2016 [24] |
No change to mean plasma IL-6 (pg/ml) |
0.584 | Total tissue damage was similar across groups | |||
| Karatas Gurgun et al., 2017 [19] |
Sham operation | 4-hr torsion | 24-hr torsion | Increased follicular cell degeneration in the torsion groups | ||
| IMA (ng/ml) | 0.59+0.06 | 0.58 +0.1 | 0.71 +0.14 | 0.064 | ||
| DD (ng/ml) | 250.71+ 71.95 | 1740.20+913.94 | 474.36+222.4 | 0.001 | ||
| Kart et al., 2011 [25] |
DD (mg/l) | Sham operation | Torsion model | Greater follicular cell degeneration in group 2 | ||
| Pre-operative plasma levels | 0.5963+0.2047 | 0.6344+ 0.1348 | 0.815 | |||
| 2h after OT | 1.2267+0.3099 | 0.6213+0.2346 | 0.001 | |||
| Mean difference | +0.0250+0.2660 | +0.5922+0.3001 | 0.001 | |||
| IMA levels (μmol/l) | ||||||
| Lazăr et al., 2019 [26] |
Control | 402.370 ± 2.732 | 0.003 | |||
| Sham operation | 418.472 ± 1.854 | |||||
| 3h torsion | 478.359 ± 5.218 | <0.001 |
||||
| 3h torsion, 1hr simple reperfusion | 490.024 ± 3.376 | |||||
| 3h ischaemia, 1hr controlled reperfusion | 452.564 ± 3.096 | |||||
| 3h ischaemia, 24h simple reperfusion | 483.370 ± 1.550 | |||||
| 3h ischaemia, 24h-controlled reperfusion | 454.207 ± 0.878 | |||||
| Uzun et al., 2018 [27] |
Post-operative | Group 1. Sham operation | Group 2. Torsion model + ischaemia >8h | Group 3. Torsion model + ischaemia >24h | Group 1: 0.004 Group 2: 0.150 Group 3: 0.016 |
Increased follicular degeneration in the ischemic groups |
| SCUBE1 (ng/ml) | 51.12+17.04 | 71.83+20.53 | 132.85+51.18 | |||
| Yildirim et al., 2016 [28] |
Median post-operative IMA levels (ABSU) | Torsion group | Control group | 0.001 for the difference between groups |
No pathological change in the control group, but pathological change present in the OT group | |
| 921 (870.0-966.00) | 853 (783-869) | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



