
Submitted:
21 August 2024
Posted:
22 August 2024
You are already at the latest version
Abstract
Cleft lip and palate are the most common congenital craniofacial anomalies. The etiology of this condition is unclear. The overall incidence of cleft lip and palate is 1/700. Prenatal diagnosis of cleft lip by 3D ultrasound is possible in more than 70% of cases, while it is less effective for cleft palate. There are several classifications of cleft lip and palate that were proposed over the years, however, only few have found clinical application, with none of them generally accepted as most effective and understandable. Allori et al. presented classification of a cleft lip and palate which is comprehensive and uniform, and it can precisely define the vast majority of the clefts, thus enabling easier communication between the health workers during their everyday practice. In this paper, we compared the accuracy of preoperative diagnoses compared to intraoperative diagnoses according to Kernahan and Stark classification from 1958, and these diagnoses were converted according to the Allori et al. classification of cleft lip and palate. Classification of cleft lip and palate presented by Allori et al. is clear, easy to understand, and it can be successful tool in studying the epidemiology of clefts.
Keywords:
cleft
; classification
; cleft lip and palate
1. Introduction
Clefts of the lip and palate (CL/P) are the most common congenital craniofacial anomalies, and the second most frequent birth defect, that constitute a heterogenous group of birth defects with multifactorial origin and various incidence among different races (1:600-1:1000) [1,2,3,4,5,6,7]. Isolated cleft palate (CP) occurs in 1:2000 -1:2500 live births [4,5]. CL/P is the most common diagnosis, predominant in males, followed by isolated CP which is predominant in females [2,4,5]. Unilateral clefts, involving left side are most common types of clefts, and majority of cleft lip (CL) (unilateral or bilateral) are associated with a CP [1,2,4,5,6].
The causes of orofacial clefts remain largely unknown [1,5,6,7,8,9,10]. Multiple environmental and genetic factors are involved in the genesis of CL/P [1,2,3,4,5,6,11]. Clefts can be classified as non-genetic, and genetic, which are classified as non-syndromic (70% of all clefts) and syndromic [1,4,5]. They also can be classified as nonisolated (at least one unrelated defect is present), isolated (no major defects are present) and syndromic [5,6]. There are more than 350 Mendelian disorders associated with CLP (200 with CL and 400 with CP) [1,4,5,6,11]. Genetic evaluation is recommended for individuals and families affected with orofacial clefts [4,5,6,7].
Prenatal diagnosis of CL by ultrasound (US) is possible in more than 70% of cases, with mean gestational age at detection of 25.5 weeks, and incorporation of 3D US and magnetic resonance imaging (MRI) could significantly enhance the diagnosis of CL/P [1,5,8,9]. After birth and cleft evaluation, complete examination of the oral cavity and entire body has to be performed [1,4,5,8].
1.1. Treatment
Clefts represent a great burden for the patient, his family and society [6]. Multidisciplinary approach in treatment of these patients is very important [1,5,6,7]. There is a significant difference in services and treatment protocols for children with CL/P between developed countries resulting the paucity of published randomized trials of cleft care [4,5,6].
Feeding difficulties among cleft patients is well known, especially in cases with CP [4,5,6]. Several cleft specific bottles (assisted-delivery-squeeze and rigid bottles) are available for cleft patients and families should use the one which works best for their child [4,5].
Presurgical infant orthopedics (PSIO) implies different techniques which facilitates the surgical treatment of children with clefts. [1,2,5,12,13,14]. The external taping is the simplest technique for presurgical molding used in combination with dental plate [1,5,12,13,14]. Objectives of presurgical nasal and alveolar molding (PNAM) which (in most cases) is applied during 6 weeks after birth are active molding and repositioning of the nasal cartilages and alveolar processes, and lengthening of the deficient columella [1,5,12,13]. Presurgical infant orthopedics is classified as passive (by using of alveolar molding plate known as Liu’s and Grayson’s method) and active (which requires a surgical procedure to introduce the device and to remove it - Latham pinned coaxial screw appliance) [1,5]. Gingivoperiostoplasty (GPP) is a procedure used for correction of the cleft alveolar segments at the time of cleft lip repair [1,2,5]. If the alveolar segments are appropriately aligned and <2 mm apart, then the infant is candidate for GPP, if this is not a case, then alveolar bone grafting should be performed [1,2,5,13].
The goal of any operative technique for CL is to restore normal appearance including lip and nasal deformity [1,2,3,5,13,14,15]. The two most common techniques for unilateral CL repair are straight-line (Tennison) and rotation-advancement (Millard) repairs [14,15]. There are several other operative techniques such as: Noordhoff (Chang Gung), Mohler, Fisher etc. [1,2,5,14,15]. The CL repair is scheduled when the patient is approximately 3 months of age and it’s performed in general anesthesia [1,14]. There are several techniques for bilateral cleft lip and nose repair (Mulliken, Chen-Noordhoff, McComb, Cutting,) with the similar goals of operative techniques as for the unilateral clefts [1,3,5,13,14,15,16].
Currently two common approaches to the timing of cleft palate repair exists: one-stage repair, and two-stage repair [1,2,6]. According to Woo, 88% of surgeons in the United States use one stage cleft palate repair between 6 and 14 months [7,14,15].
The most common techniques used for hard palate repair are Bardach two-flap palatoplasty, von Langenbeck bipedicle flaps, Veau-Wardill-Kilner pushback technique, with several other techniques such as buccal myomucosal flap or buccal fat pad flaps [1,2,7,13,14]. In case of wide clefts vomerine flaps are used for closing nasal mucosa [7].
For soft palate repair intravelar veloplasty, radical intravelar veloplasty, or Furlow double opposing “Z” plasty are most commonly used techniques [1,2,5,7,15]. Sommerlad et al. promote the use of the operating microscope for cleft palate repair [7,15].
The primary goal of palatoplasty is normal speech, based on the ability of complete closing of the velopharyngeal sphincter [2,5,13,14,15]. Velopharyngeal insufficiency presents the inability of closing the velopharyngeal sphincter and this is presented by hypernasality, nasal emission, and imprecise consonant production [1,2,5,15]. The diagnosis of VPI is made by subjective and objective means and treatment includes posterior pharyngeal wall augmentation, palatal lengthening, sphincter and pharyngeal flap pharyngoplasty etc. [2,5,15]. Furlow technique can be also used to treat velopharyngeal insufficiency (VPI) [1,2,5,7].
Hearing loss is a well-known complication of CP, and these patients need ear, nose and throat (ENT) specialist and audiological surveillance [1,2,5,13]. Cleft palate closure significantly reduces the prevalence of audiological problems [13]. Cleft lip and palate include various abnormal dental conditions [10].
Additional surgery includes previously mentioned bone grafting, pharyngoplasty, fistuloraphy, rhinoplasty, and LeForte osteotomies (middle face retraction) and they are performed in different age of patients [5,16,17]. Secondary deformities mostly depend of the severity of primary defect, effectiveness of orthodontic treatment, and the method of repair and there are several different techniques for treatment of secondary cleft deformities [16,17].
1.2. Classification
There are several classification systems of CL/P developed and implemented from the beginning of the last century [1,2,5,8,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32]. Despite numerous attempts, there is still need for a universal and simple classification which would find clinical application [8,18,30]. Houkes at al. stated that classifying clefts in a clear, easy to understand and concise manner is a key element of cleft care [30].
Ritchie and Davis suggested the classification of CL/P at 1922 which gained wide acceptance [2,18,20,22,25]. They have used the alveolar process as a line of division between lip and palate anomalies [18].
Kernahan and Stark presented new classification for CL/P in 1958 (on embryological basis), and they proposed that instead of alveolus, incisive foramen become dividing point between different groups of clefts including: cleft of primary palate (lip and premaxilla), cleft of secondary palate only, and clefts of primary and secondary palate [1,2,8,18]. After 15 years Kernahan stated that the size of charts of cleft patients is a problem especially that they don’t show the exact degree of clefts [18]. At 1973 he proposed a “Y” shaped diagram where the upper limbs represent primary palate and lower limb represent hard and soft palate [1,2,8,11,19,20,21,22]. This was followed by several modifications of Kernahan “Y” classification by different authors. Elsahry at 1973 offered modified stripped “Y” classification [22]. Sandham in 1985 modified Kernahan and Stark classification of CL/P by adding the group of rarer types of facial clefts [20]. Friedman et al. in 1991 proposed a modification of Kernahan “Y” classification assigning the scale depending on the severity of clefts [2,26]. Smith at 1998 revised the Kernahan “Y” classification and proposed the system that allows a compact alphanumeric description of any cleft [2,25]. At 2013 Khan et al. revised Smiths modification of Kernahan striped “Y” classification by incorporating different subclasses of submucous cleft palate [29].
Despite numerous modifications of Kernahan “Y” classification, there was still no classification that would satisfy all the necessary criteria for a universally accepted classification [22]. Otto Kriens in 1989 proposed a system that used letters to present components and by this system every possible cleft form can be typed [2,21]. The acronym LAHSHAL denotes the bilateral anatomy of lip (L), alveolus (A), hard (H) and soft (S) palates [2,21,22]. Capital letters indicate complete clefts, small one’s partial clefts, asterisks (*) noted the minimal clefting, the dot (.) means that anatomic feature is unaffected, and (+) sign can be placed for Simonart band in the L column [1,2,8,22,30]. The right side is the left side of the patients and vice versa (like an x-ray formula) [22]. According to Houkes et al. LAHSHAL could be the most suited universal classification system [30].
Schwartz et al. in 1993 have reviewed existing classifications presented by Davis and Ritchie, Brophy, Veau, Fogh-Andersen, Pruzanski, Kernahan and Stark Harkins et al., Vilar-Sancho and Kernahan [1,2,23,30]. They conclude that 63 possible combinations of clefting may occur and by comparing description of the type of cleft by anatomic components and its modification presented by Kernahan, they developed their three-digit numerical system where the three limbs of “Y” present three-digit (RPL) [23,26].
Mortier et al. analyzed patients with partial unilateral incomplete clefts and they proposed the rating scheme which permits the comparison of postoperative results with the severity of the cleft [24,31]. Ortiz-Posadas et al. proposed a more precise modification of Mortier binary method by assigning a value to each one of the clefts [2,26].
According to Liu et al. an ideal system of classification would be easy to understand and to document, with the detailed information of the exact location and the extent of the deformities [27]. They criticized Kernahan's classification stating that, among other things, it did not adequately describe asymmetric bilateral clefts and that the data from this classification could not be adequately computerized, and also analyzed Smith et al. and Schwartz et al. modification of Kernahan classification. Liu et al. stated that their LAPAL system (L-right lip, A-left alveolus and primary palate, P-secondary palate, A-left alveolus and primary palate, L- left lip, with the extent of cleft deformity presented by Arabic numerals 0 to 4) allows a numerical description of all kinds of clefts [27].
Koul et al. analyzed following symbolic classifications: striped “Y” classification of Kernahan, RPL system of Schwartz, and the LAHSHAL system of Royal College of Surgeons and criticized them mainly for not defining the extent of the cleft in a particular unit. They stated that their classification of CL/P named “Expression System” that comprises two components: (1) anatomical nomenclature (text) and (2) symbols based on the phrase ‘‘lip and palate’’ is accurate and flexible to record the degree and variations of clefting of the lip and palate [28].
Singh stated that classification scheme of the American Cleft Palate Association (ACPA) which is more complex compare to Kernahan and Stark classifications represent probably the best variable system based on embryological theory about the development of the face [31].
At 2017 Allori et al. summarized the experience related to cleft classification systems and according to criteria for an “ideal classification scheme” offered their own classification that includes the laterality and severity of labial defect, description of an alveolar defect and a morphological characterization of the palatal defect, with exclusion of facial clefts.
Authors stated that: a. Incisive foramen is surgically useful dividing point; b. Integrity of alveolar process is critical detail; c. Morphologic features of labial and palatal cleft should be described to degree relevant to treatment planning; and d. High-level morphological details should be excluded from the classification, and by that complete description of CL/P should include the laterality and severity of the labial defect, acknowledgment of alveolar defect, and a morphological characterization of the palatal defect [30,32].
In order to avoid longhand notations authors developed complementary shorthand notation which is strictly structured according to a few rules and definition [32]. Uppercase letters summarize anatomical involvement (C stands for the word cleft, L for lip, A for alveolus, and P for palate, while lowercase prefix describes of the preforaminal and postforaminal component: the laterality (u, unilateral; b, bilateral; med, median;) and severity (c, complete; i, incomplete; m, lesser form [minor-form, microform, or mini-microform]; and a, asymmetric (only for bilateral case) [32]. For unilateral cases the terms right and left are not abbreviated. Morphology of the cleft palate is described as follows: bu (bifid uvula), sm (submucous cleft palate with/without bifid uvula, v1, v2, v3, v4 according to Veau classification of cleft palate The plus sign (+) means “and”, that is combination of two features, the plus or minus sign (±) mean “with/without” and the virgule / mean and/or [32]. The author suggested that initial encounter describe the CL/P using longhand structured form and all the notes at subsequent encounters may simply reference the shorthand notation.
The primary aim of this study is to perform a review of the accuracy of the preoperative diagnoses for the patients with CL/P. Furthermore, we aimed to point out errors that occur when applying standard classifications, and to demonstrate the simplicity and comprehensiveness of the Allori et al. classification.
2. Material and Methods
2.1. Study Group
Five hundred and twenty-one consecutive patients who underwent their primary surgical procedure for CL/P deformities at the Department of the Plastic and Reconstructive Surgery and Burns at the Institute for Mother and Child Health Care were reviewed. This was a prospective study that started from 1. January of 2014. The clefts were analyzed from chart records, operating records and pictures. Clefts of palate were analyzed in details at the operative procedures.
2.2. Patient’s Characteristics
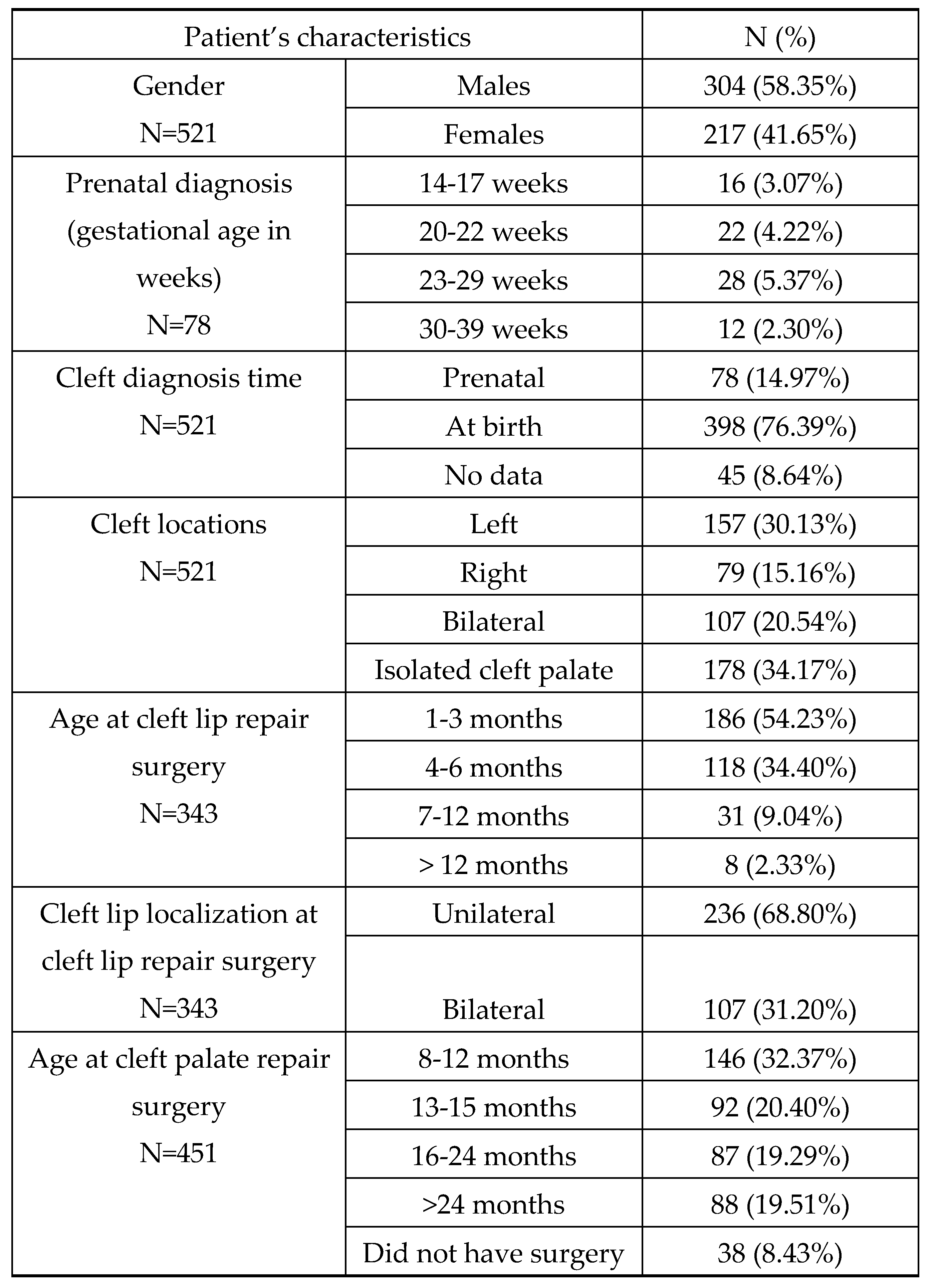
Further characteristics were evaluated: gender (males and females), prenatal diagnosis expressed in gestational age in weeks (14-17 weeks, 20-22 weeks, 23-29 weeks and 30-39 weeks), time of cleft diagnosis (prenatal, at birth, and no data), cleft locations (left, right, bilateral, and isolated CP), age at surgical intervention for CL (1-3 months, 4-6 months, 7-12 months, and >12 months), laterality of CL group (unilateral and bilateral), and type of surgical intervention and age at surgical intervention for CP (8-12 months, 13-15 months, 16-24 months, and >24 months). Furthermore, distribution of cleft types as well as associated anomalies with a CL/P were evaluated.
2.3. Surgical Techniques
Surgical techniques for CL and for CP were analyzed. For CL we analyzed Millard, Onizuka, Tennison, Chang Gung, Mohler, and Fisher technique, for bilateral clefts we analyzed combination of Noordhoff-Mulliken technique and Mulliken technique, and for CP we analyzed Veau-Wardil-Kliner with intravelar veloplasty technique and Furlow double-opposing Z-plasty.
2.4. Statistical Interpretation
Results are presented as categorical variables as whole numbers (N) and frequencies (%) with in table and figures.
3. Results
In Table 1 we presented patients characteristics. A total of 343 cleft lip surgeries and 413 palatoplasty surgeries were performed on 521 patients. Out of the total number, prenatal diagnostic by US was obtained in 303 patients and it was correct in 78 patients (14.97%).
Distribution of cleft types in our study according to Kernahan and Stark classification from 1958 is presented at Figure 1 [18].
Associated anomalies in our group of patients with cleft lip and palate is presented in Figure 2.
Surgical techniques for unilateral and bilateral cleft lip are presented in Figure 3.
A total of 413 children with cleft palate were operated on and the distribution of the surgical techniques is presented at Figure 4.
4. Discussion
Cleft lip and palate represent a broad phenotypic group of congenital anomalies and it has been described in different ways for many centuries [1,2,3,4,5,6,7,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32]. The terms “harelip”, “split lip”, “hare teeth”, and “beak of the hare” have been used a long time period, until meeting in St Louis in 1922, where Davis and Ritchie proposed a term “congenital cleft lip” instead of above-mentioned terms, and they also advocate for a standard system of classification [32].
Since then, there have been numerous attempts to classify these anomalies in the simplest and most precise way that would facilitate the work of both medical and non-medical professionals participating in the treatment of these patients [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32]. All the classifications offered so far did not meet the basic requirement, and that is a common language understandable to all [25,28].
Blair criticized Davis and Ritchie classification system because it was based only on contemporary surgical perspectives [32]. Brophy presented classification system that was not widely accepted because it was complex and impractical [18,30,32]. It was used later by Veau to promote his simplified classification [2,18,30,32].
Fogh and Anderson offered their classification system [2,18,30,32]. They pointed out the importance of the incisive foramen and stated that cleft lip and alveolus are possibly etiologically related [2,30,32].
Kernahan and Stark followed Fogh and Anderson work, adopted incisive foramen as the embryologically sound dividing line, presenting their classification in 1958, based on developmental anatomy (adding modifiers to describe laterality and severity) [1,2,18,32]. Kernahan translated in 1971 his ow classification presented earlier in cooperation with Stark with the diagram in form of letter “Y”, where the incisive foramen was a reference, in order to simplify the record keeping [2,8,32].
Since the need for standardized terminology was becoming increasingly important, in 1962 Nomenclature Committee appointed by American Association for Cleft Palate Rehabilitation published criteria for an ideal classification scheme, encouraging use of Greek and Latin terms, and advocating for a system that would respect embryology and surgical anatomy [31,32].
American Cleft Palate-Craniofacial Association (ACPA) used the previously given instructions of Nomenclature Committee's and divided the clefts into prepalatal (cleft of the lip and embryologic primary palate) and palatal clefts (cleft of the embryologic secondary palate) [32].
In 1967, the Subcommittee on Nomenclature and Classification chaired by T. Ray Broadbent at International Confederation for Plastic and Reconstructive Surgery devised a two-tier classification of the lip, alveolus, and palate based on the embryologic principles, and this was published in 1969 [32].
In 1981 ACPA Reclassification Committee criticize the International Classification of 1969, and determined that Kernahan and Stark classification (1955) and ACPA Classification (1962) were better systems [32].
Almost all further classifications attempt to show anomalies numerically or in letters as briefly and simply as possible, but only the LAHSHAL classification of Kriens and associates has gained significant acceptance [2,8].
There is also another system introduced recently which is actually a registration process for coding and categorization of the disease named International Statistical Classification of Diseases and Related Health Problems (ICD) promoted by World Health Organization and its broadly implemented in Europe and North America [30].
In our study, boys were most frequently affected, similar to the reports of other authors [1,2,5,6].
Cleft was prenatally diagnosed by US in 78 out of 303 patients. This points to the fact that other authors stated that orofacial region is not part of ultrasound screening in pregnancy, especially in the developing and under developing countries [2,6,8]. Incorporation of 3D US and magnetic resonance imaging (MRI) as routine practices could enhance the diagnosis of CL/P [8]. The majority of clefts are diagnosed at birth since the anomaly is visible and accessible.
According to literature the most common type of cleft is unilateral complete CL/P [1,2,3,4,5,6]. Isolated CP (different variations) was most common type of cleft in our group of patients, followed by unilateral complete CL/P, and bilateral complete CL/P (Table 1). According to Ezzeldin et al. isolated CP account for approximately 44%, and unilateral complete CL/P accounts for 22% of all clefts [10]. Clefts are most often localized on the left side, and that was a case in our group of patients [1,7].
Associated anomalies occurred in 16% of patients with CL/P. In our group of patients, the incidence of single and several additional diagnoses was almost the same. The urinary tract was most commonly single organic system involved. According to Woo associated anomalies are found in one quarter of patients with CL/P and in one half of the patents with CP alone [7]. Other authors reported around 30%-36% total incidence of additional diagnosis [3,11].
In case of CL, in our study, the most commonly applied techniques were by Millard, Onizuka and Tennison. Chang Gung and Mohler technique were also used, and during the last several years we introduced in our practice Fisher anatomic subunit approach for cleft lip reconstruction (similar to several studies), since it offers better results compare to other techniques [1,7,14].
The combination Noordhoff-Mulliken technique for bilateral cleft lip was used in more than 80% of patients, while Mulliken technique for bilateral CL in past several years became a standard procedure in in our hospital as in the most of cleft centers [3].
More than half of patients with cleft lip surgery have been treated at the age of 1-3 months and one third of patients was treated at the age of 4 to 6 months, and that is in accordance with other cleft center protocols [1,3,4,5,6]. In case of cleft palate, one stage technique according to Veau-Wardil-Kliner (pushback technique) with intravelar veloplasty was most commonly used. Some authors advocate a two-stage repair trying to avoid limitation in facial growth [2,7,14,15]. We have used Furlow double-opposing Z-plasty for soft palate or submucous clefts. These two techniques are cited in the literature as the most frequently applied techniques for cleft palate surgery [2,4,5,6,7,15]. Cleft palate surgery was performed in more than half of the patients until 15 months of life which the most optional time for cleft palate surgery when the best speech outcomes are obtained [7,14].
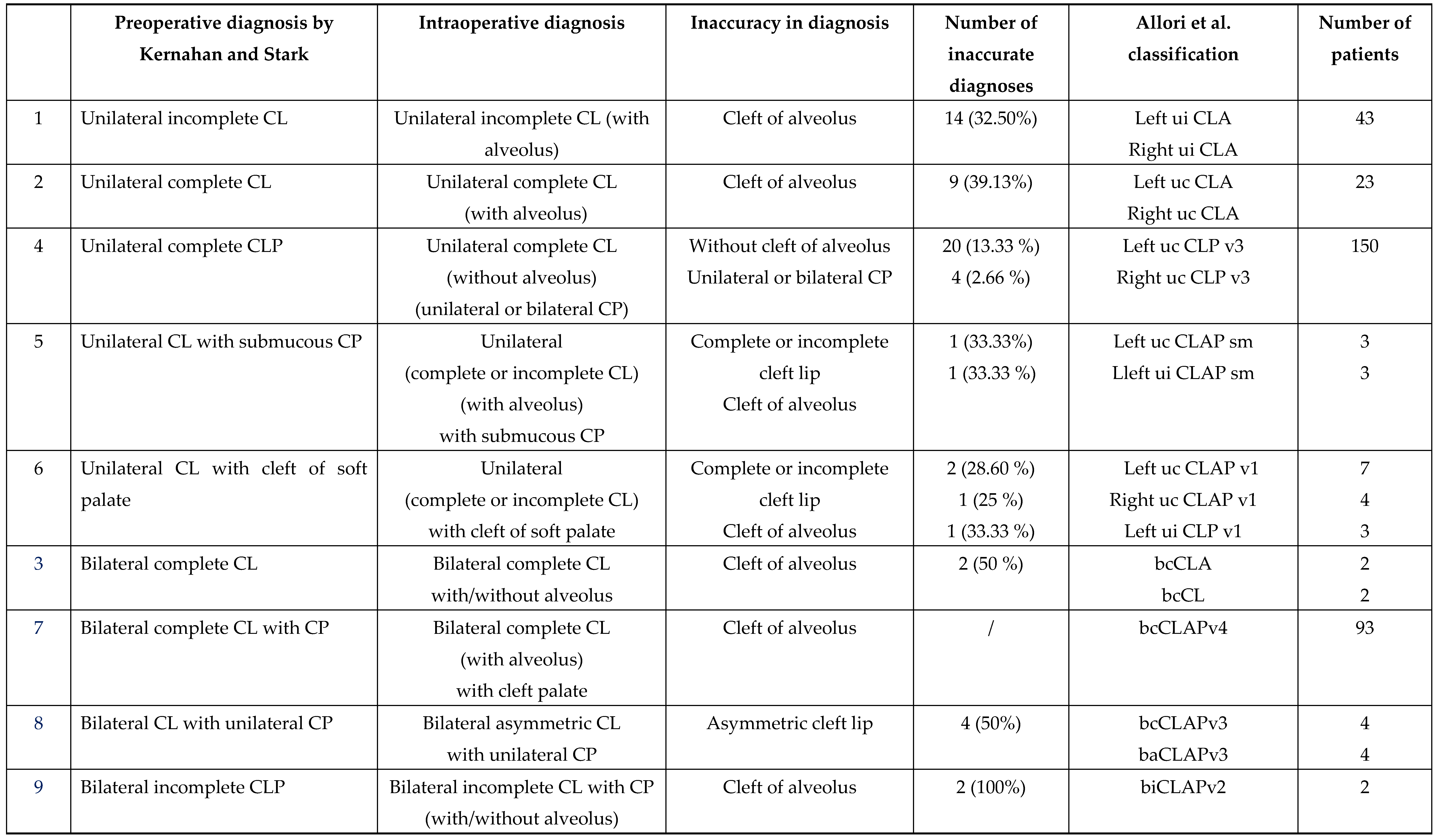
Our patients were analyzed through preoperative and intraoperative diagnoses, photographs, and operative findings. Similar to other cleft centers, classification of the anomalies in our patients was done multiple times during cleft management [30]. In most of the cases cleft was classified at the preoperative visit, and it was re-evaluated during the surgery. The diagnosis was made mainly by a specific specialist during the preoperative visit. Classification was done both for clinical and research purposes. In our country there is no national registration for clefts and the classification was mainly performed for reimbursement purposes.
The main classification system was Kernahan and Stark classification of CL/P. We compared the diversity and complexity of the preoperative diagnoses, their inaccuracy in relation to the intraoperative findings, and we translate them into a uniform classification system according to Allori et al. In our study, 17.78% of patients had an inaccurate preoperative diagnosis. The intraoperative diagnoses were more accurate, especially in cases of the severity of CL, presence or absence of alveolar cleft, symmetry of bilateral clefts and laterality of CP (unilateral or bilateral), and they showed us anatomical and morphological shortcomings of preoperative diagnoses. These intraoperative diagnose were translated into abbreviated diagnoses based on the classification of Allori and associates (Table 2).

5. Conclusions
Our findings demonstrated the importance and role of CL/P classification according to the Allori et al., with special attention to the anatomical and morphological characteristics of CL/P. Implementation of this classification into routine healthcare practice would have positive impact on clinical and non-clinical decision making in treatment and follow-up of patients with cleft pathology.
Author Contributions
Conceptualization, A.V., D.N.; methodology, A.V., D.N., T.M., O.S.; validation A.V., D.N., T.M., O.S.; formal analysis A.V., D.N., T.M., O.S., K.M., M.V.; investigation A.V., D.N., T.M., O.S., K.M., M.V., S.S., S.D., F.M., N.Z.; resources A.V., D.N., T.M., O.S.; data curation A.V., D.N.; writing-original draft preparation A.V., D.N., O.S., M.V., K.M., F.M., N.Z; writing-review and editing A.V., D.N., O.S., K.M.; visualization, A.V., D.N., O.S., K.M.; supervision A.V., S.S., S.D.; All authors have read and agreed to the published version of the manuscript.
Funding
The research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the institutional Ethics Committee of the Institute for Mother and Child Health Care (protocol code 8/191, date 14.08.2024).
Informed Consent Statement
Not applicable.
Acknowledgments
We appreciate the support of the Faculty of Medicine, University of Belgrade, Project Contract Number 451-03-66/2024-03/200110, for this research.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chen Kuo-Ting P, M. Noordhoff S, Kane A. Repair of unilateral cleft lip. In: Neligan PC, ed. Plastic surgery, 3rd ed. Saunders, London, United Kingdom;2013. p. 517-549e3.
- Punjabi AP, Hardesty RA. Classification and anatomy of cleft palate. In: Mathes SJ Hentz VR, editors. Plastic surgery, 2nd ed. Saunders, London, United Kingdom; Volume 4.p.69-87.
- Xue AS, Buchanan EP, Hollier LH Jr. Bilateral cleft lip repair: lessons from history. Plast Reconstr Surg. 2022;150(1):201e-210e.
- Vyas T, Gupta P, Kumar S, Gupta R, Gupta T, Singh HP. Cleft of lip and palate: A review. J Family Med Prim Care. 2020;9(6):2621-2625.
- Worley ML, Patel KG, Kilpatrick LA. Cleft lip and palate. Clin Perinatol. 2018;45(4):661-78.
- Mossey PA, Little J, Munger RG, Dixon MJ, Shaw WC. Cleft lip and palate. Lancet. 2009;374(9703):1773-85.
- Woo AS. Evidence-based medicine: cleft palate. Plast Reconstr Surg. 2017;139(1):191e-203e.
- Smarius B, Loozen C, Manten W, Bekker M, Pistorius L, Breugem C. Accurate diagnosis of prenatal cleft lip/palate by understanding the embryology. World J Methodol. 2017;7(3):93-100.
- Baeza-Pagador A, Tejero-Martínez A, Salom-Alonso L, Camañes-Gonzalvo S, García-Sanz V, Paredes-Gallardo V. Diagnostic methods for the prenatal detection of cleft lip and palate: a systematic review. J Clin Med. 2024;13(7):2090.
- Ezzeldin M, Gee S, Curtis J, Clark VJ, Smallridge J, Collard M. Dental anomalies in cleft lip and/or palate children at age 10 - a retrospective review across three cleft centres: Part 1. Br Dent J. 2023;234(12):926-930.
- Aspelin E, Cornefjord M, Klintö K, Becker M. Additional diagnoses in children with cleft lip and palate up to five years of age. J Plast Surg Hand Surg. 2023;57(1-6):476-82.
- Kapadia H, Olson D, Tse R, Susarla SM. Nasoalveolar molding for unilateral and bilateral cleft lip repair. Oral Maxillofac Surg Clin North Am. 2020;32(2):197-204.
- Paradowska-Stolarz A, Mikulewicz M, Duś-Ilnicka I. Current concepts and challenges in the treatment of cleft lip and palate patients-a comprehensive review. J Pers Med. 2022;12(12):2089.
- Aycart MA, Caterson EJ. Advances in cleft lip and palate surgery. Medicina (Kaunas). 2023;59(11):1932.
- Fisher DM, Sommerlad BC. Cleft lip, cleft palate, and velopharyngeal insufficiency. Plast Reconstr Surg. 2011;128(4):342e-60e.
- Sarrami SM, Skochdopole AJ, Ferry AM, Buchanan EP, Hollier LH Jr, Dempsey RF. Revisional techniques for secondary cleft lip deformities. Semin Plast Surg. 2021;35(2):65-71.
- Allori AC, Mulliken JB. Evidence-based medicine: secondary correction of cleft lip nasal deformity. Plast Reconstr Surg. 2017;140(1):166e-176e.
- Kernahan DA, Stark RB. A new classification for cleft lip and cleft palate. Plast Reconstr Surg Transplant Bull. 1958;22(5):435-41.
- Kernahan DA. The striped Y-a symbolic classification for cleft lip and palate. Plast Reconstr Surg. 1971;47(5):469-70.
- Sandham A. Classification of clefting deformity. E Hum Develop 1985; 12: 81-5.
- Kriens O. LAHSHAL: a concise documentation system for cleft lip, alveolus and palate diagnosis in what is a cleft lip and palate?: A multidisciplinary update. New York: Thieme MedicalPublishers; 1989: 30-34.
- Härtel J, Kriens O, Kundt G. Incidence of cleft lip, alveolus and palate forms. Journal of Cranio-Maxillofacial Surgery. 19(4):1991, 144-46.
- Schwartz S, Kapala JT, Rajchgot H, Roberts GL. Accurate and systematic numerical recording system for the identification of various types of lip and maxillary clefts (RPL system). Cleft Palate Craniofac J. 1993;30(3):330-2.
- Mortier PB, Martinot VL, Anastassov Y, Kulik JF, Duhamel A, Pellerin PN. Evaluation of the results of cleft lip and palate surgical treatment: preliminary report. Cleft Palate Craniofac J. 1997;34(3):247-55.
- Smith AW, Khoo AK, Jackson IT. A modification of the Kernahan "Y" classification in cleft lip and palate deformities. Plast Reconstr Surg 1998;102(6):1842-7.
- Ortiz-Posadas MR, Vega-Alvarado L, Maya-Behar J. A new approach to classify cleft lip and palate. Cleft Palate Craniofac J. 2001;38(6):545-50.
- Liu Q, Yang ML, Li ZJ, Bai XF, Wang XK, Lu L, Wang YX. A simple and precise classification for cleft lip and palate: a five-digit numerical recording system. Cleft Palate Craniofac J. 2007;44(5):465-8.
- Koul R. Describing cleft lip and palate using a new expression system. Cleft Palate Craniofac J. 2007;44(6):585-9.
- Khan M, Ullah H, Naz S, Igbal T, Ullah T, Tahir M, Ullah O. A revised classification of the cleft lip and palate. Can J Plast Surg 2013; 21: 48-50.
- Houkes R, Smit J, Mossey P, Don Griot P, Persson M, Neville A, Ongkosuwito E, Sitzman T, Breugem C. Classification systems of cleft lip, alveolus and palate: results of an international survey. Cleft Palate Craniofac J. 2023;60(2):189-96.
- Singh D, Bastain TS, Kudva S, Singh MK, Sharma P. Classification systems for orofacial clefts. Or Max Path J 2015;6:556-60.
- Allori AC, Mulliken JB, Meara JG, Shusterman S, Marcus JR. Classification of cleft lip/palate: then and now. Cleft Palate Craniofac J. 2017;54(2):175-88.
Figure 1.
Types of clefts in our study.
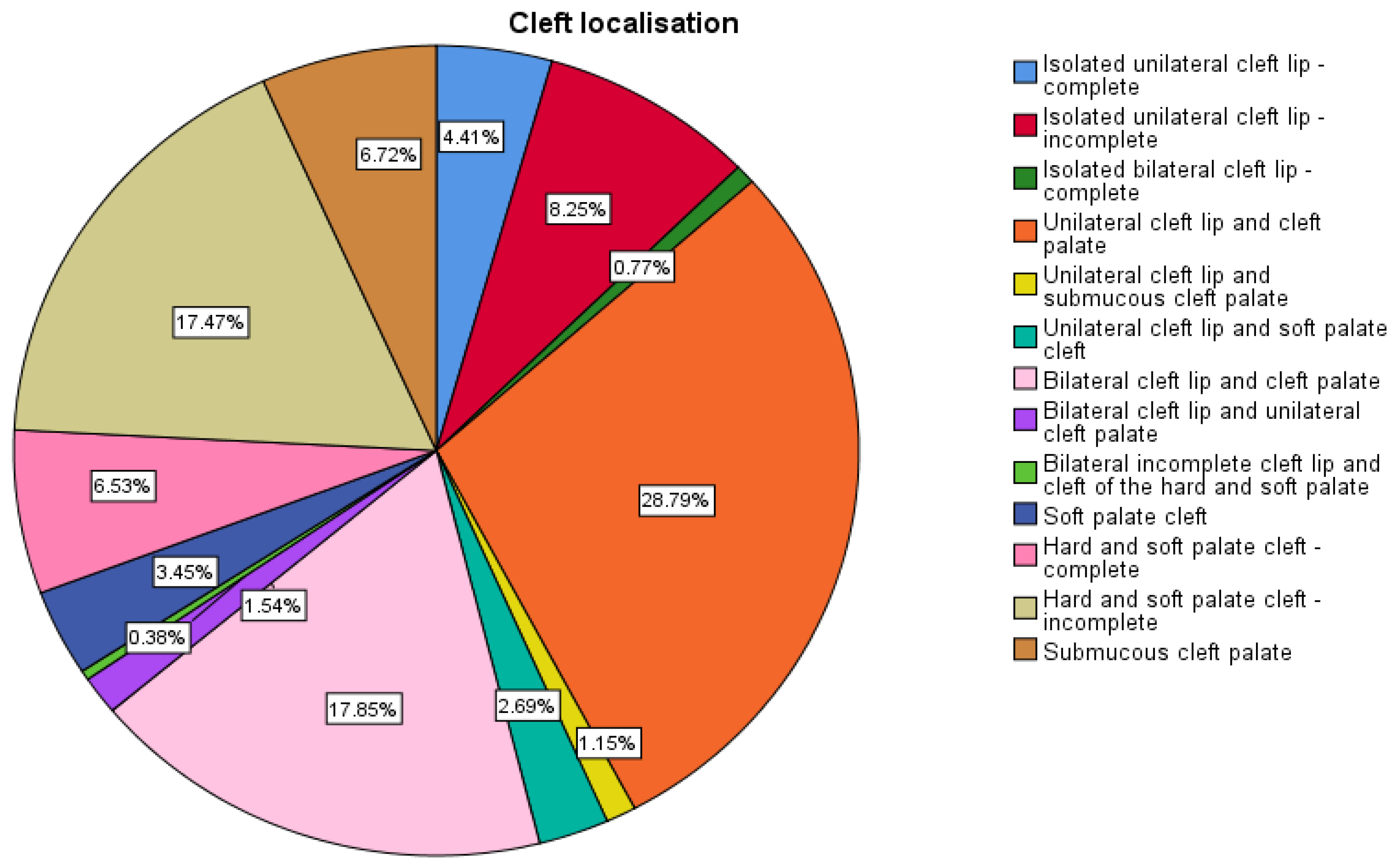
Figure 2.
Associated anomalies in patients with cleft lip and palate.
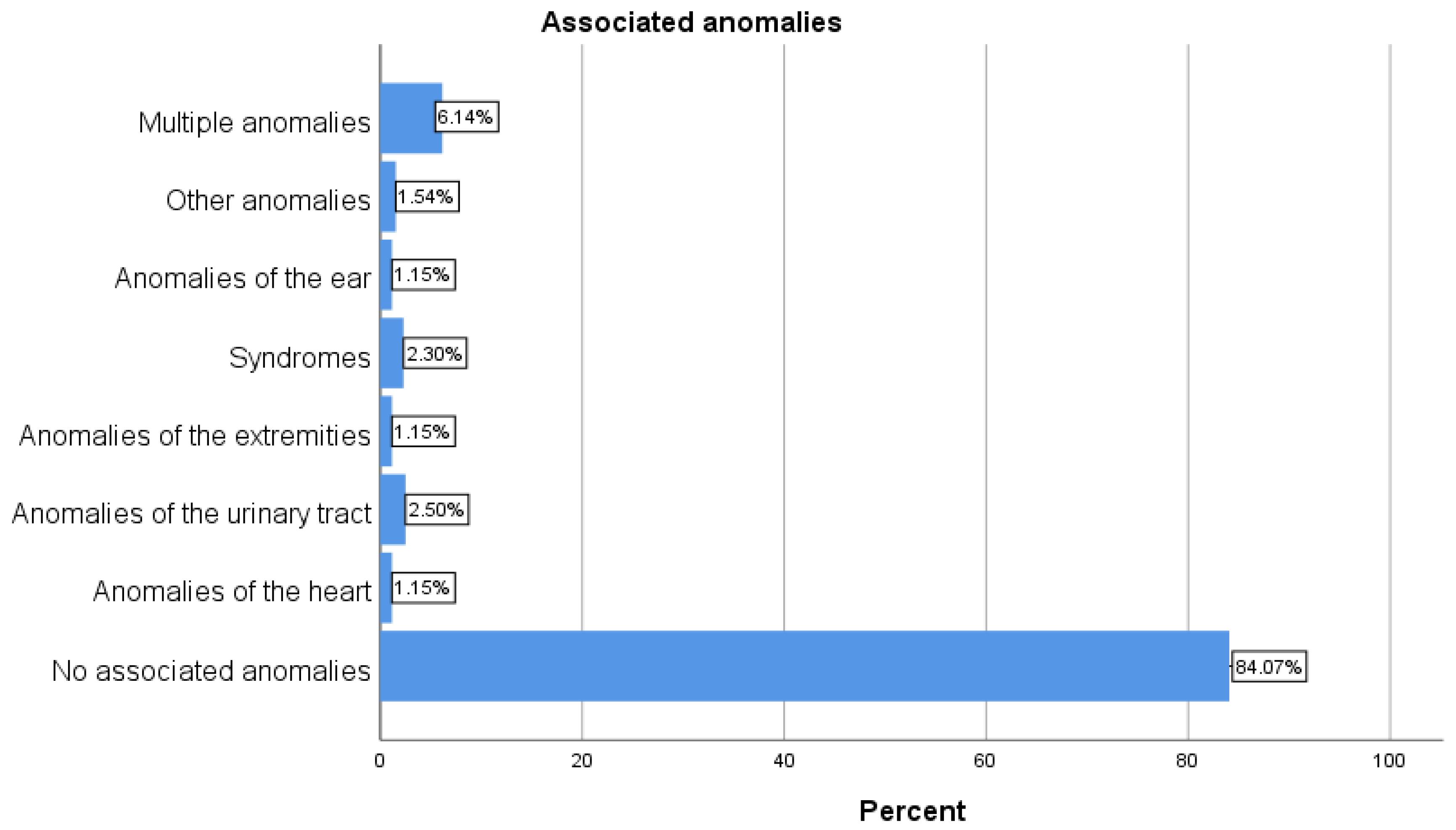
Figure 3.
Types of surgical techniques for unilateral and bilateral cleft lip.
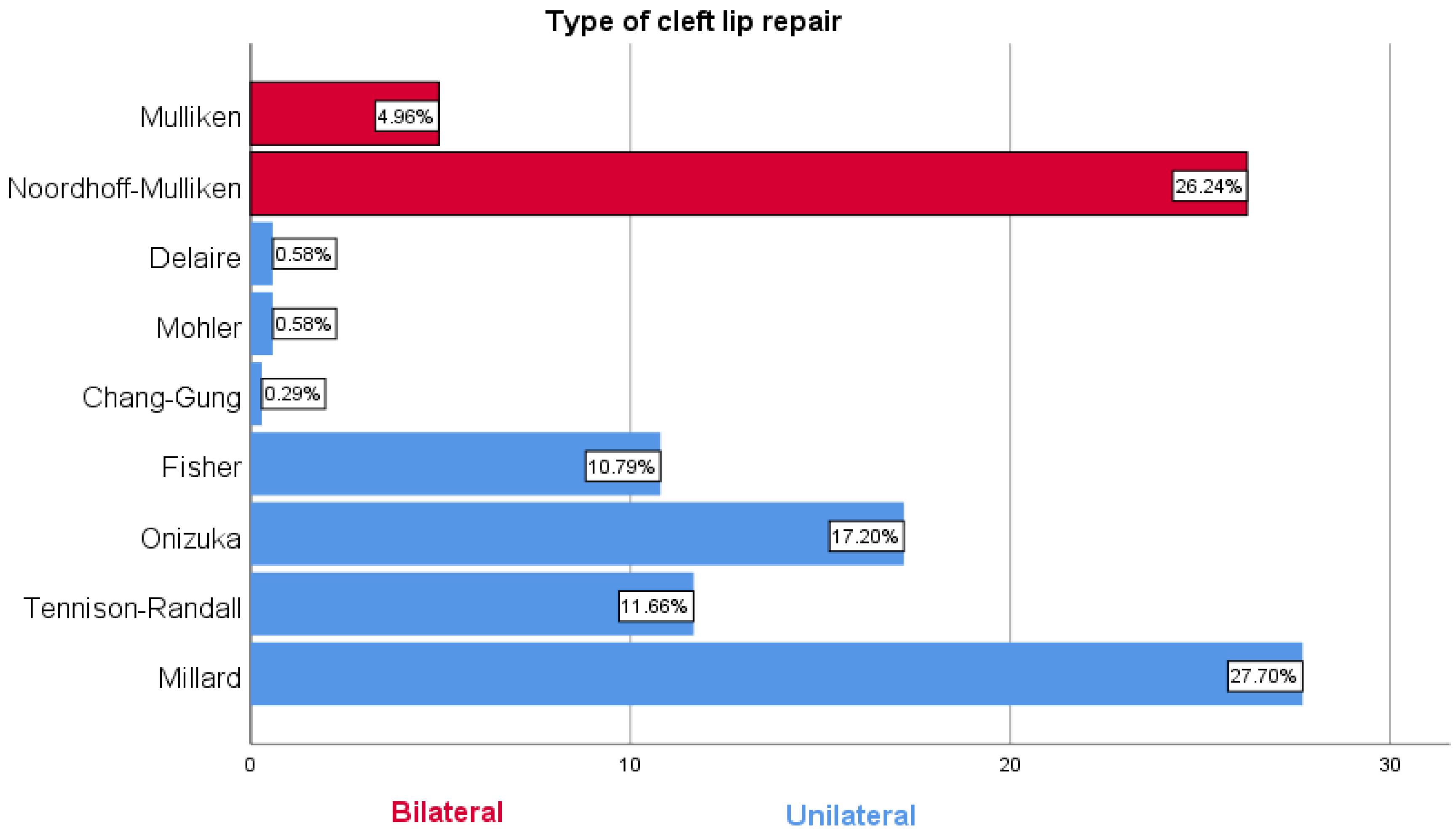
Figure 4.
Types of surgical techniques for cleft palate.
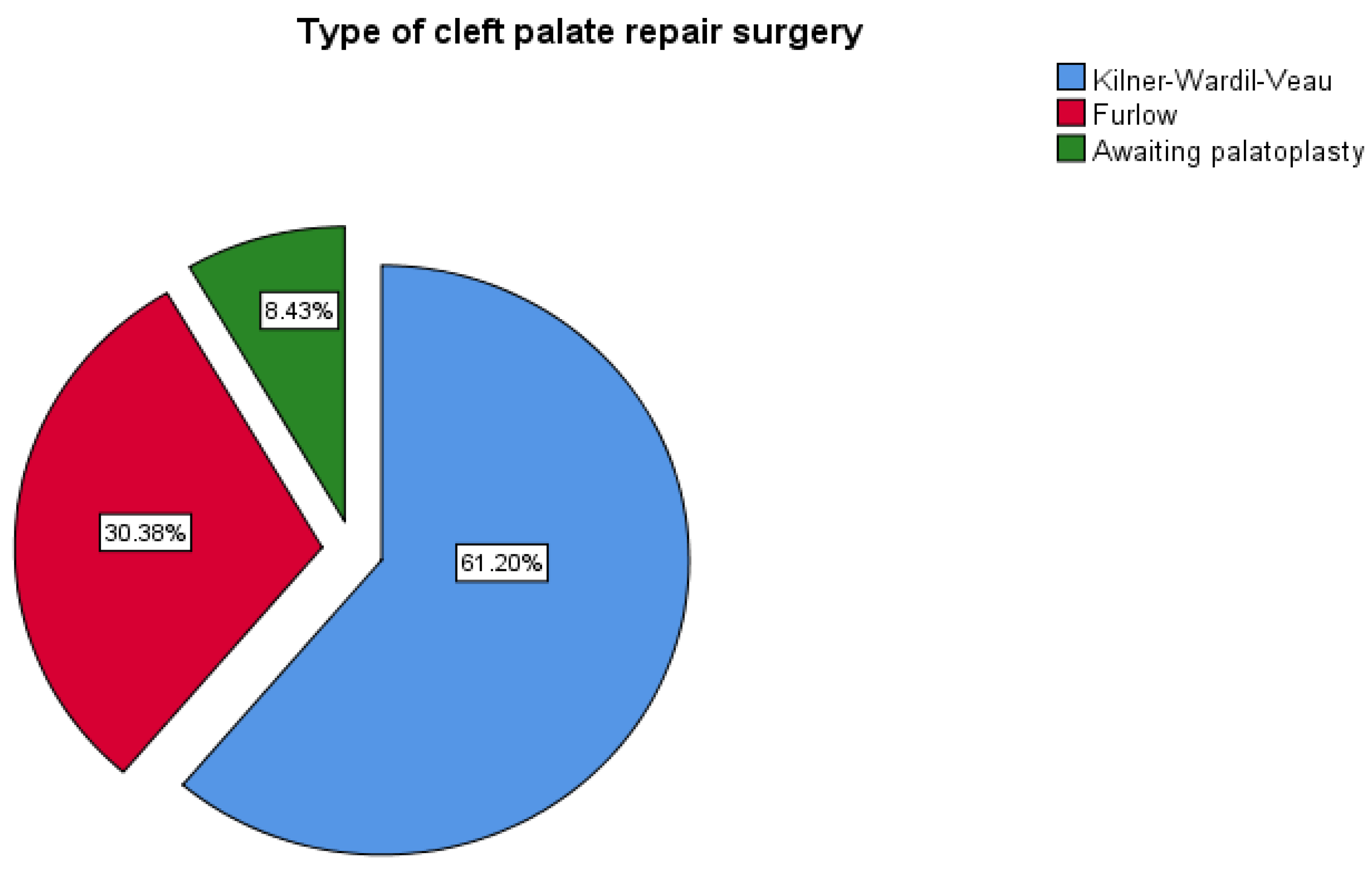

Table 1.
Patient’s characteristics.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



