
Submitted:
23 August 2024
Posted:
24 August 2024
You are already at the latest version
Abstract
Objectives: In recent years, ear endoscopy has gradually become an important tool in ear surgery. This study further explored its application in ear surgery, to establish a surgical approach for semicircular canal obstruction (SOC) via the ear canal to control vertigo in Meniere's disease. Methods: With the approval of the ethics committee, recruitment started in June 2019. Four patients with Meniere's disease who had been treated conservatively for more than six months received SCO via an external ear canal approach under otoendoscopy and were followed for two years after surgery to assess the safety and efficacy of the procedure. Results The control of vertigo after the operation was satisfactory (100%), and the frequency and degree of vertigo were significantly improved. Tinnitus improved in 1 case (25%) and did not progress in the other 3 cases. Hearing loss did not progress in all patients. Postoperative walking instability occurred in 1 patient (25%), and there were no obvious complications. All patients reported significant improvements in their quality of life. Conclusions: SCO via the external auditory canal approach is safe, effective, easy to accept, and an alternative to conservative treatment of Meniere's disease with no actual hearing for more than 6 months.
Keywords:
Endoscopic ear surgery
; Refractory Meniere disease
; Semicircular canal occlusion
; Vertigo
1. Introduction
Meniere’s disease is characterized by recurrent rotatory vertigo, undulating sensorineural hearing loss, and tinnitus with or without a feeling of fullness in the ears [1], which can seriously affect the quality of life. The management of Meniere’s disease primarily focuses on reducing the frequency of attacks, alleviating the severity of symptoms such as vertigo and tinnitus, and minimizing hearing loss. In cases where conservative treatment fails to address persistent and intractable Meniere’s disease, surgical intervention should be considered. The central compensatory mechanism can take effect by surgically modifying the fluctuating excitation differences (bilateral asymmetry) in the bilateral vestibular system to a fixed asymmetry, leading to the resolution of vertigo symptoms. Semicircular canal occlusion (SCO) is a surgical procedure involving the creation of a window in the bony canal of the semicircular canal to obstruct or interrupt the flow of endolymphatic fluid and otolithic stimulation to the cupula using materials such as bone wax, bone chips, peritoneum, biological glue, or laser [2]. In 1990, Parnes et al. [3] first described using a transmastoid approach for lateral semicircular canal occlusion in treating refractory benign paroxysmal positional vertigo (BPPV), and subsequent research has confirmed its efficacy. Given that both Meniere’s disease and BPPV involve vertigo attacks that are partially or fully caused by endolymphatic fluid flow, SCO has been increasingly used in clinical practice for patients with refractory Meniere’s disease in recent years [4]. Endoscopic surgery is a minimally invasive procedure that patients have widely welcomed due to its advantages of reaching the middle ear through the natural entrance of the ear canal and without a noticeable incision [5,6]. This study is the first to perform a horizontal semicircular canal occlusion procedure through the external ear canal approach for the treatment of Meniere’s disease, intending to expand the use of endoscopic techniques in the surgical treatment of vertigo.
2. Materials and Methods
2.1. Clinical Data
The case data were from 4 patients with intractable Ménière’s disease admitted to our hospital from November 2019 to December 2023, including 1 male and 3 female patients, with an average age of (61.75±10.01) years and a disease duration of 2-4 years.
Inclusion criteria: Diagnosis meets the criteria set out in the “Guidelines for Diagnosis and Treatment of Meniere’s Disease (2017)” [7]; Standardized conservative treatment of Meniere’s disease for at least 6 months with frequent episodes of vertigo; Patients have a strong desire for surgical treatment and fully understand and consent to treatment plans and possible risks.
Exclusion criteria: Bilateral Meniere’s disease; Central nervous system disorders or other disorders of the inner ear; Other underlying conditions require long-term use of diuretics, glucocorticoids, etc. This study adheres to the principles of the Helsinki Declaration and has been approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology (Ethics approval number: [2023]0602-01).
2.2. Surgical Methods
Preoperative preparation is standardized and surgical procedures are standardized according to the endoscopic ear surgery [8]: a. Clean the external ear canal and subcutaneously inject a solution of freshly prepared lidocaine epinephrine in to the external ear canal to reduce bleeding that may occur during the preparation of the tympanic membrane flap; b. Make a U-shaped tympanic membrane flap from the 3 o’clock position in the external auditory canal, with the flap being larger than 180°. (Too small an angle may cause excessive tearing of the external auditory canal tissue when the flap is raised); c. Enter the middle ear cavity and dissect the malleus-incus joint. This step emphasizes the protection of the chorda tympani nerve and the stipe of the malleus; d. Use a curette to scrape off a portion of the lateral wall of the superior drum; e. A U-shaped bone chisel was used to enlarge the depression created by the curette on the lateral wall of the superior eardrum, exposing a sufficient view of the middle ear; f. Expose and dissect the incus-stapes joint; g. Remove the incus; h. Continue scraping off a portion of the inferior wall of the superior drum so that the endoscope view covers the middle and lower part of the superior and posterior drum; i. To expose the semicircular canal, a portion of the canal bone is bored out with a drill to form a window hole, taking care to avoid damage to the membranous semicircular canal; j. The bony semicircular canal window-hole is enlarged by the tip of a hook, and the membranous semicircular canal is exposed; k. After identification of the membranous semicircular canal, subcutaneous tissue from the external auditory canal is used to fill the membranous semicircular canal, pressing it firmly against the opposite bone wall, thus providing complete and permanent occlusion of the semicircular canal; l. Sufficient hemostasis and drying with cotton, sealing the bony semicircular canal with bone wax. It can be covered with absorbent hemostatic material; m. Use small bone chips or bone powder to repair defects in the lateral wall of the mastoid; n. Reset the mastoid process skin flap.
2.3. Postoperative Evaluation
To observe the healing of the ear wound in the patient 2 weeks after the surgery, an MRI of the inner ear membrane labyrinth was performed to observe the degree of occlusion of the horizontal semicircular canal in the operated ear and to assess the success rate of the surgery. The number and severity of vertigo attacks, tinnitus, and ear fullness were queried at 6 months to 2 years post-operative, and the quality of life and efficacy of the treatment were assessed.
3. Results
As of June 2024, the follow-up period is 6 months to 2 years, as shown in Table 1. Two weeks postoperatively, the rate of the obstructed horizontal semicircular canal was 100%, as confirmed by imaging studies (Figure 2, Figure 3). No patients experienced local infection, bleeding, severe pain, facial paralysis, or loss of taste in the short-term postoperative complications. Long-term follow-up showed no recurrence of vertigo in all four patients, a control rate of 100%; None of the patients reported progressive hearing loss; postoperative tinnitus improved in 1 case (25%), and the other 3 patients did not report progressive tinnitus; 1 case (25%) of postoperative unsteady walking was observed, and no patient experienced ear discharge, tympanic membrane non-healing, or pain. All patients reported significant improvements in their quality of life and were able to perform daily tasks.
4. Discussion
The SCO is an important advance in the treatment of the vertigo symptoms of Meniere’s disease by partially destroying the semicircular canal, while retaining to a certain extent the functions of the elliptical canal, the spherical canal, and the cochlea. This approach preserves the functions of hearing and otolaryngology. SCO has a smaller incision and a lower risk of hearing loss compared to other procedures [9]. The procedure was relatively simple and the post-operative response was light, significantly better than labyrinthitis and vestibular dissection. The conventional surgical procedure for SCO [10] involves making a skin incision behind the ear to expose and open the mastoid, followed by shaping and opening the mastoid. The horizontal semicircular canal was then located, and its outline was drilled using an electric drill before a micro-diamond drill was used to create a bone window. Subsequently, after opening the window, the peri-venous semicircular canal is identified, and a mixture of bone or tissue mass with fibrin glue is filled into the posterior semicircular canal through the window, compressing the membranous semicircular canal against the opposite bone wall. This leads to the ossification of bone or tissue masses, resulting in permanent complete occlusion of the posterior semicircular canal. Omitting this canal results in the formation of blind ends in the membranous labyrinth, preventing compression or expansion of the periosteum, and thereby controlling vertigo by reducing sensitivity to angular acceleration of the head due to the elimination of vestibular stimulation [11,12]. Several researchers have attempted to modify this surgical approach; Anthony [13] utilized an argon laser for cauterizing bony semicircular canals followed by local fibrosis induced by thermal effect for occluding membranous canals. However, complete occlusion is not guaranteed with this method and there is potential for post-surgery recurrence. In addition, sensorineural hearing loss may result from thermal effects due to laser usage. Similarly, Kartush et al. [14] performed CO2 laser carbonization on membranous semicircular canals via a bone window created on their bony walls using a posterior approach following an incision behind the ear. This led directly to the contraction and obscuration of these canals. While quick and thorough compared to the argon laser method, and safer at the same time, the mastoid approach to horizontal semicircular occlusion often necessitates the significant removal of the mastoid bone during the incision behind the ear, resulting in heightened post-operative reactions including pain and prolonged numbness. Surgery using an ear endoscope eliminates the need for incisions behind the ear or extensive mastoid bone removal. Thus, it offers greater patient acceptance along with the absence of postoperative head wrapping/pain requirements as well as long-term bed rest needs [8].
The criteria for endolymphatic sac decompression via the external auditory canal are aligned with those for the traditional posterior approach, requiring strict adherence before surgery. Most peripheral vestibular disorders respond well to conservative therapies. Corticosteroid injections into the middle ear represent a secondary treatment option for Meniere’s disease; Tympanic injection of gentamicin serves as an intermediate step between secondary and tertiary surgical interventions [15,16]. Surgery may be considered in patients who experience persistent vertigo symptoms, significant impairment of quality of life, and non-responsiveness to medication and other conservative treatments. Surgical indications include stage IV unilateral Meniere’s disease; stage III partial syndrome with failed endolymphatic sac surgery, speech recognition rate below 50%, and a strong preference for surgery [17]. Prior to surgical intervention, it is essential to confirm the diagnosis and affected side, exhaust all conservative treatment options, and engage in individualized discussions during consultation about the benefits and risks of the proposed surgical procedure. The criteria for endolymphatic sac blockage surgery aimed at controlling vertigo must be rigorously controlled. Internationally, several scholars have proposed the development of disease progression prediction models using imaging techniques; Surgery is not recommended if there is a high risk of bilateral progression [18,19]. In addition, surgical intervention becomes more appropriate when the vestibular apparatus of the deaf ear is compromised or useful hearing is absent in the affected ear. It should be noted that this procedure does not improve hearing in general; Therefore, care must be taken to protect the ossicular chain and other structures if residual hearing remains in the affected ear.
This study selectively blocks horizontal semicircular canals for the following reasons. Firstly, the eye movements during vertigo attacks in patients with Meniere’s disease are predominantly horizontal (the vertical component can be ignored). When the anterior and posterior semicircular canals on the same side are simultaneously stimulated, the vertical components of the eye movements are opposite in direction and cancel each other, resulting in weak torsional nystagmus [20]. The eye movements mainly originate in horizontal semicircular canals. Second, blocking horizontal semicircular canals only results in a lower risk of hearing loss compared to blocking multiple semicircular canals. The study found that the probability of further hearing loss in the affected ear was approximately 30 percent after three SCCO procedures, and 23.8 percent and 20 percent, respectively, after two and one SCO procedures [4]. Third, the balance disorder response after horizontal SCO is less severe, and vestibular central compensation can be established more quickly compared to multiple SCO. In addition, the degree of vestibular oculomotor reflex function impairment was similar between the two surgical methods. Compared to unilateral labyrinthectomy, unilateral semicircular canal occlusion can produce a sustained physical stimulus, leading to a significant increase in the excitatory neurotransmitter (glutamate) and neuromodulator (5-HT) concentrations in the ipsilateral vestibular nucleus, thereby altering the balance of excitatory neurotransmitters in the bilateral vestibular system and facilitating vestibular compensation [21,22]. In the case of occlusion of only the horizontal semicircular canal, the duration of the imbalance is short and the time required for vestibular central compensation to build up is shorter and more complete. During follow-up, one patient was found to have significantly improved symptoms of dizziness, but had residual symptoms of unsteady gait. Patients reported feeling as if they were walking on water and had to rely on a cane. Tinnitus and ringing in the ears went away, and hearing remained the same. Upon examination of the patient’s medical history, it was found that the affected ear had not undergone vestibular rehabilitation as directed by the physician after the surgery, which, in addition to the surgical factors, may have been the main cause of the patient’s poor vestibular function. In addition, the patients were older and had more severe symptoms before surgery, which may also have affected vestibular function compensation after surgery. Therefore, precise surgery combined with early vestibular rehabilitation is the way to ensure the effectiveness of the treatment.
5. Conclusions
The transcanal approach with horizontal semicircular canal occlusion under ear endoscope can significantly alleviate vertigo symptoms of Meniere’s disease without damaging hearing, but the effect on tinnitus is unknown. The procedure can significantly improve a patient’s quality of life, but can cause unpredictable balance disorders. By applying endoscopy to the surgical treatment of vertigo, this study broadens the scope of vertigo surgery and enriches the means for individualized and comprehensive treatment of vertigo. Post-operative patients need no head wrap, mild pain, long-term bed rest is not required, and the features of minimal incision, no incision, and rapid recovery are more acceptable to patients. In addition, the indications for this approach are the same as those for the conventional surgical approach. Still, more cases are needed to assess clinical cure rates, prognosis, and adverse reactions. In summary, the endoscopic transcanal approach to horizontal semicircular canal occlusion is safe, effective, easy for patients to accept, and a viable alternative treatment for patients with Meniere’s disease who have been conservatively treated for more than six months and do not have useful hearing.
Author Contributions
Conceptualization, Y.S. and J.Y.; methodology, Y.S., Y.L. and E.W.; validation, Y.L. and R.Z.; investigation, J.Y., Y.L. and M.S.; data curation, M.S. and E.W.; writing—original draft preparation, M.S. and H. Z.; writing—review and editing, L.X. and Q.C.; supervision, Y.S.; project administration, Y.S.; funding acquisition, Y.S. and J.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Key Program of the National Natural Science Foundation of China (No. 81230021), the Foundation for Innovative Research Groups of Hubei Province (No. 2023AFA038), the National Key Research and Development Program of China (Nos. 2021YFF0702303, 2023YFE0203200), the National Natural Science Foundation of China (No. 82071058), the Basic Research Support Program of Huazhong University of Science and Technology (No.2024BRA019).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the Ethical Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China (Reference number [2023] 0602-01, approval date: 4 September 2023). All patients have provided written informed consent for participating in this study and publishing their case details.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
All data included in this study are available upon reasonable request by contact with the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Paparella, M. M.; Kimberley, B. P. , Pathogenesis of Menière’s disease. J. Vestib. Res. 1990, 1, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Cai, Q.; Leng, Y.; Sun, Y. , Semicircular canal occlusion. J. Clin. Otorhinolaryngol. 2024, 38, 122–126 (in Chinese with English abstract), (in Chinese with English abstract). [Google Scholar]
- Parnes, L. S.; McClure, J. A. , Posterior semicircular canal occlusion for intractable benign paroxysmal positional vertigo. Ann. Otol. Rhinol. Laryngol. 1990, 99 (5 Pt 1), 330–334. [Google Scholar] [CrossRef]
- Li, X.; Lyu, Y.; Li, Y.; Jian, H.; Wang, J.; Song, Y.; Kong, L.; Fan, Z.; Wang, H.; Zhang, D. , Triple Semicircular Canal Plugging versus Labyrinthectomy for Meniere Disease: A Retrospective Study. Laryngoscope 2023, 133, 3178–3184. [Google Scholar] [CrossRef] [PubMed]
- Kong, W. J. , Endoscopic ear surgery: flash in the pan or transformative innovation? J. Clin. Otorhinolaryngol. 2018, 32, 427–434 (in Chinese with English abstract), (in Chinese with English abstract). [Google Scholar]
- Kong, W. J.; Ding, X. Y.; Wang, Y. F.; Wang, W. Q.; Wang, X.; Wang, W.; Sun, Y.; Tang, W. L.; Li, X. P.; Zhang, W.; Chen, Y.; Wang, Z. Y.; Yang, H. D.; Yang, Q.; Zhao, Y.; Hou, Z. H.; Cui, Y.; Yu, Y. J. , Endoscopic ear surgery: flash in the pan or transformative innovation? (Ⅱ). J. Clin. Otorhinolaryngol 2018, 32, 1531–1541 (in Chinese with English abstract), (in Chinese with English abstract). [Google Scholar]
- Guideline of diagnosis and treatment of Meniere disease (2017). Chin. J. Otorhinolaryngol. Head Neck Surg. 2017, 52, 167–172 (in Chinese with English abstract), (in Chinese with English abstract).
- Wang, E.; Liu, B.; Wang, Y.; Yao, W.; Sun, Y. , Occlusion of the Lateral Semicircular Canal Through the External Ear Canal: A Case Report. Ear Nose Throat J 2022, 101, NP447–NP450. [Google Scholar] [CrossRef]
- Wolfovitz, A.; Grobman, A. B.; Babcock, T. A.; Angeli, S. I. , The pattern of hearing outcome following surgery of the semicircular canals. Laryngoscope Investig. Otolaryngol. 2019, 4, 132–137. [Google Scholar] [CrossRef]
- Fei, S.; Guangfei, L.; Jie, M.; Yiling, G.; Mingjing, C.; Qingxiang, Z.; Wei, M.; Shuangba, H. , Development of semicircular canal occlusion. Front. Neurosci. 2022, 16, 977323. [Google Scholar] [CrossRef]
- Parnes, L. S.; Agrawal, S. K.; Atlas, J. , Diagnosis and management of benign paroxysmal positional vertigo (BPPV). CMAJ. 2003, 169, 681–693. [Google Scholar] [PubMed]
- Ramakrishna, J.; Goebel, J. A.; Parnes, L. S. , Efficacy and safety of bilateral posterior canal occlusion in patients with refractory benign paroxysmal positional vertigo: case report series. Otol. Neurotol. 2012, 33, 640–642. [Google Scholar] [CrossRef]
- Anthony, P. F. , Utricular macular ablation for benign paroxysmal positional vertigo. Ear Nose Throat J. 1996, 75, 416–421. [Google Scholar] [CrossRef]
- Kartush, J. M.; Sargent, E. W. , Posterior semicircular canal occlusion for benign paroxysmal positional vertigo--CO2 laser-assisted technique: preliminary results. Laryngoscope 1995, 105 (3 Pt 1), 268–274. [Google Scholar] [CrossRef]
- Li, S.; Pyykkö, I.; Zhang, Q.; Yang, J.; Duan, M. , Consensus on intratympanic drug delivery for Menière’s disease. Eur Arch Otorhinolaryngol. 2022, 279, 3795–3799. [Google Scholar] [CrossRef] [PubMed]
- Nevoux, J.; Barbara, M.; Dornhoffer, J.; Gibson, W.; Kitahara, T.; Darrouzet, V. , International consensus (ICON) on treatment of Ménière’s disease. Eur. Ann. Otorhinolaryngol. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2018, 135 (1S), S29–S32. [Google Scholar] [CrossRef]
- Kong, W. J.; Liu, B.; Leng, Y. M.; Zhang, S. L. , Intensive reading of the guidelines of diagnosis and treatment of Meniere disease and benign paroxysmal positional vertigo. Chin. J. Otorhinolaryngol. Head Neck Surg. 2017, 52, 178–189 (in Chinese with English abstract), (in Chinese with English abstract). [Google Scholar]
- Moleon, M. D. C.; Torres-Garcia, L.; Batuecas-Caletrio, A.; Castillo-Ledesma, N.; Gonzalez-Aguado, R.; Magnoni, L.; Rossi, M.; Di Berardino, F.; Perez-Guillen, V.; Trinidad-Ruiz, G.; Lopez-Escamez, J. A. , A Predictive Model of Bilateral Sensorineural Hearing Loss in Meniere Disease Using Clinical Data. Ear Hear. 2022, 43, 1079–1085. [Google Scholar] [CrossRef]
- Bächinger, D.; Schuknecht, B.; Dlugaiczyk, J.; Eckhard, A. H. , Radiological Configuration of the Vestibular Aqueduct Predicts Bilateral Progression in Meniere’s Disease. Front. Neurol. 2021, 12, 674170. [Google Scholar] [CrossRef]
- Charpiot, A.; Rohmer, D.; Gentine, A. , Lateral semicircular canal plugging in severe Ménière’s disease: a clinical prospective study about 28 patients. Otol. Neurotol. 2010, 31, 237–240. [Google Scholar] [CrossRef]
- Mattson, M. P. , Excitotoxic and excitoprotective mechanisms: abundant targets for the prevention and treatment of neurodegenerative disorders. Neuromolecular Med. 2003, 3, 65–94. [Google Scholar] [CrossRef]
- Ma, F. R.; Liu, J. X.; Li, X. P.; Mao, J. J.; Zhang, Q. D.; Jia, H. B.; Mao, L. Q.; Zhao, R. , Effects of caloric vestibular stimulation on serotoninergic system in the media vestibular nuclei of guinea pigs. Chin. Med. J. (Engl.) 2007, 120, 120–124. [Google Scholar] [CrossRef]
Figure 1.
Fenestration of horizontal semicircular canal (A) and subcutaneous tissue tamponade of external auditory canal (B).
Figure 1.
Fenestration of horizontal semicircular canal (A) and subcutaneous tissue tamponade of external auditory canal (B).
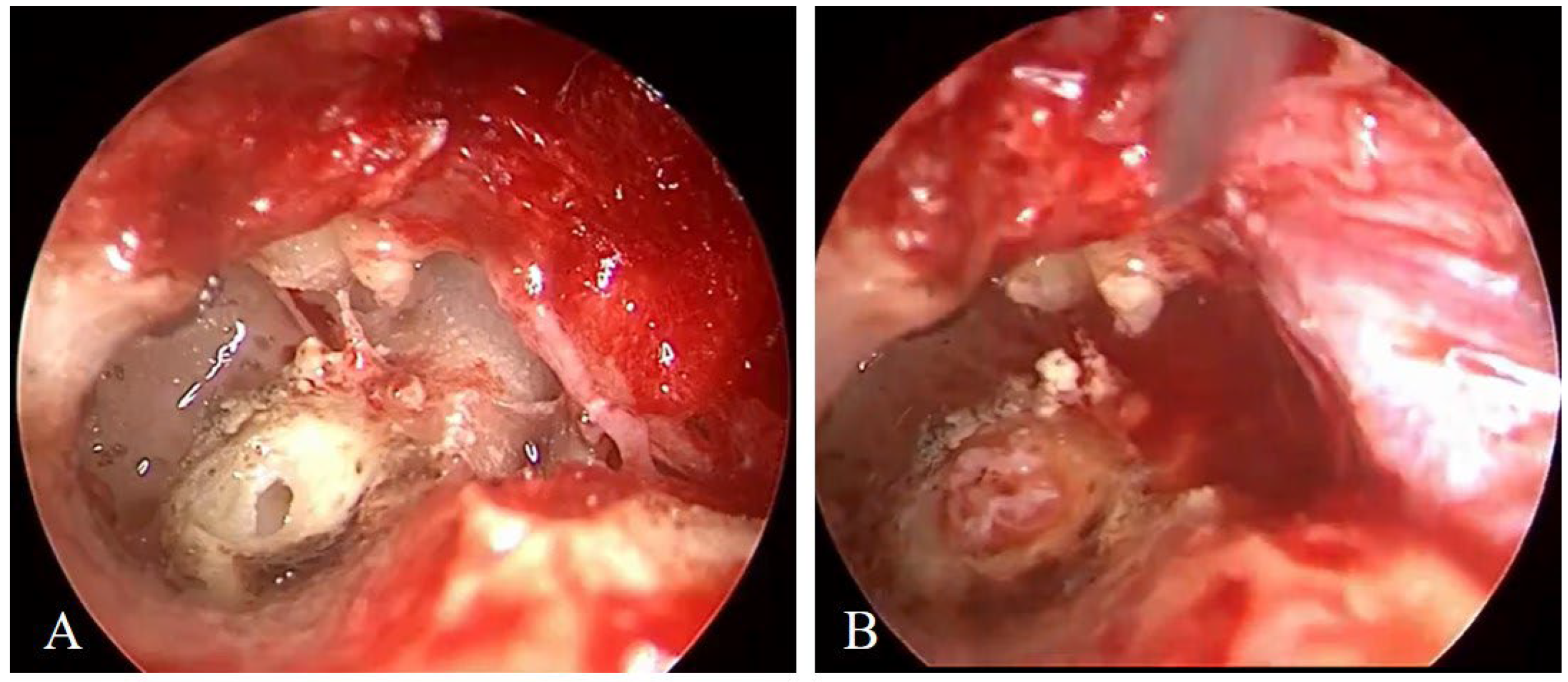
Figure 2.
Magnetic resonance imaging of the inner ear (A: Preoperative; B: Two weeks after surgery).
Figure 2.
Magnetic resonance imaging of the inner ear (A: Preoperative; B: Two weeks after surgery).
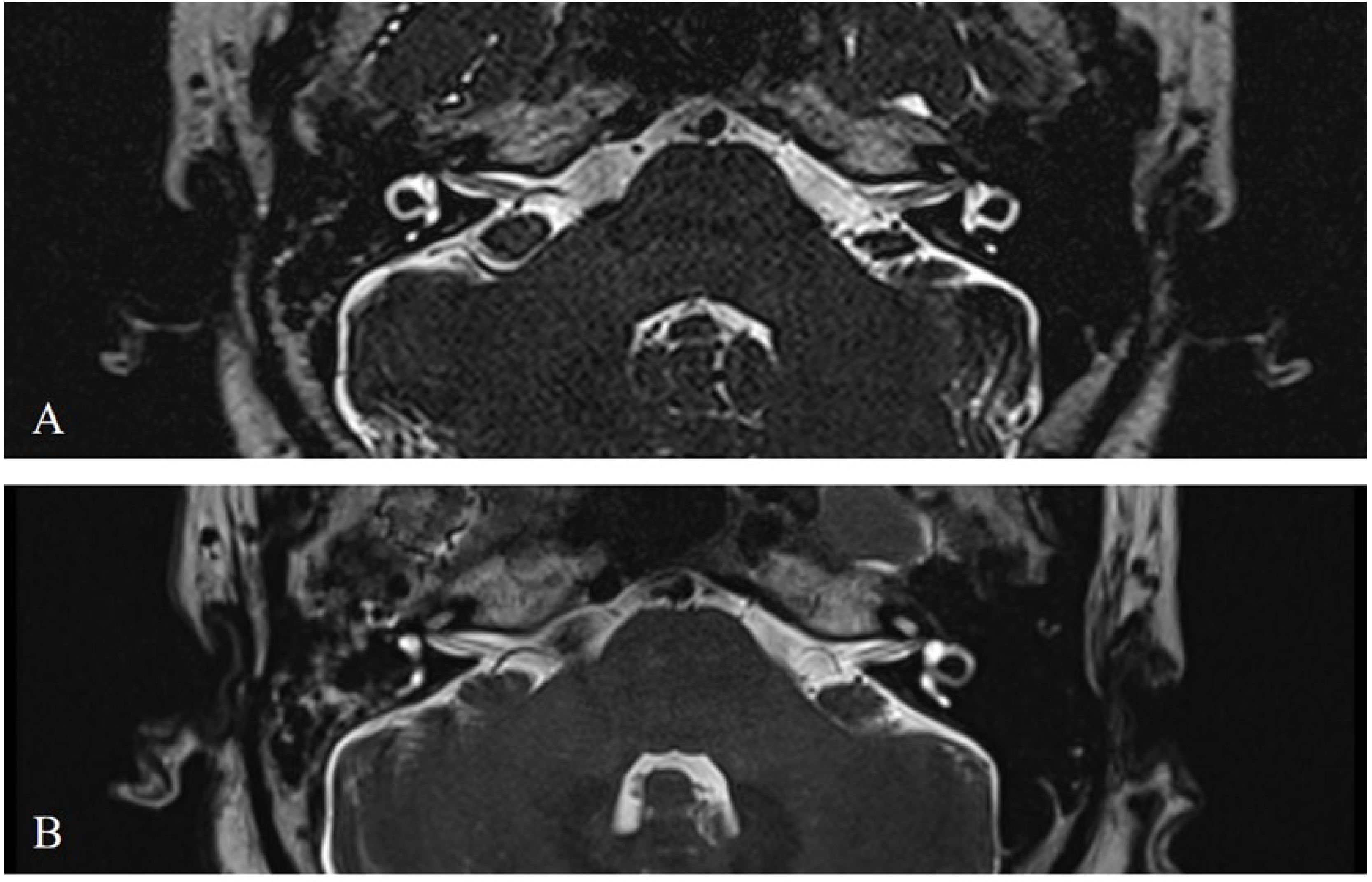
Figure 3.
Three-dimensional imaging of the membranous labyrinth after horizontal semicircular canal obstruction (A: healthy ear; B: surgical ear).
Figure 3.
Three-dimensional imaging of the membranous labyrinth after horizontal semicircular canal obstruction (A: healthy ear; B: surgical ear).
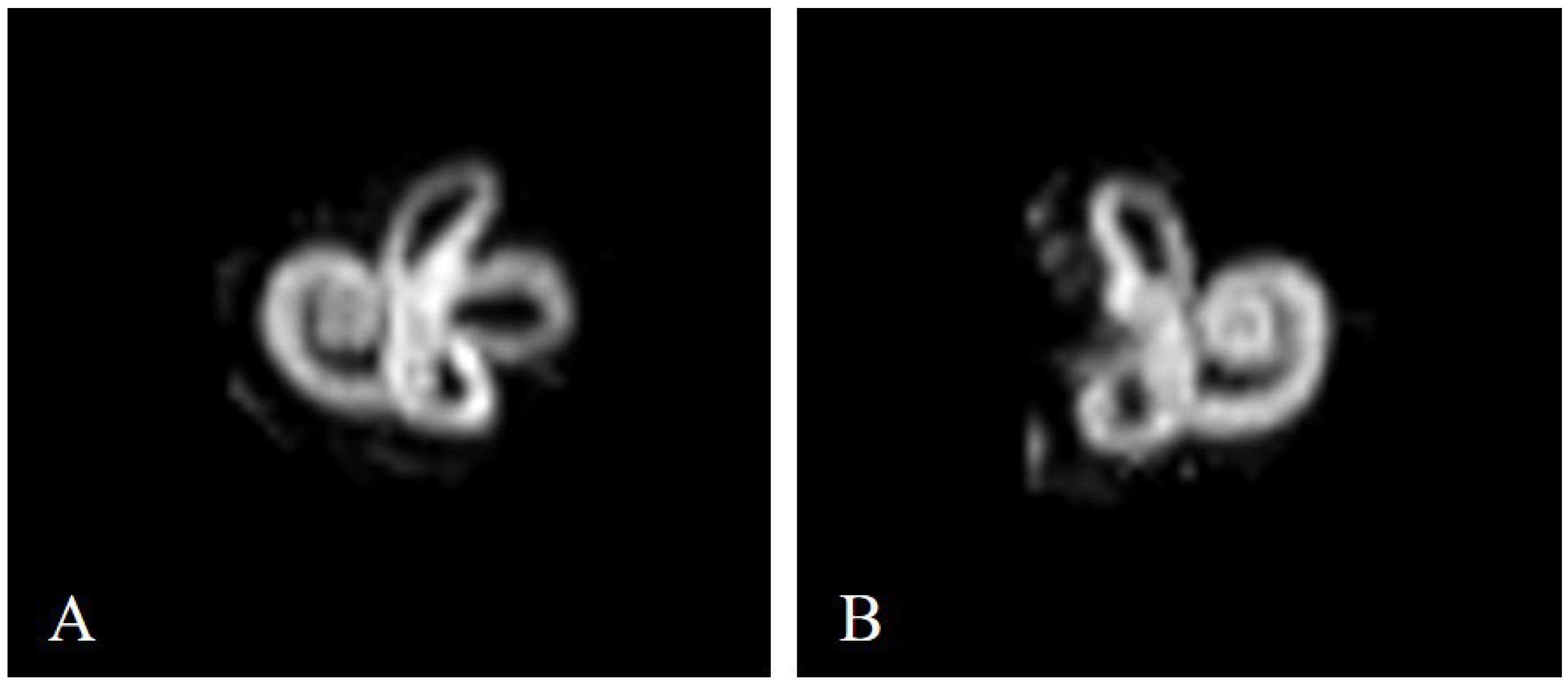

Table 1.
Information and symptoms of patients.
| Patient |
Age (years) |
Gender | Duration(years) | Pre-operation | Post-operation (follow-up more than 6 months) | |||||
| Vertigo | Hearing (diseased ear) | Tinnitus and/or ear fullness | Vertigo | Hearing (diseased ear) | Tinnitus and/or ear fullness | Adverse reaction | ||||
| 1 | 64 | male | 4 | Recurrent vertigo with no relief after 1 year of tympanic injection of dexamethasone. | 70dB HL | Persistent tinnitus with ear fullness | No attack | No progress | No paroxysmal exacerbation | No special discomfort |
| 2 | 63 | female | 3 | Frequent episodes, each lasting more than half an hour. The patient had been suffering from paroxysmal vertigo for more than 20 days before the surgery. | 73dB HL | Persistent tinnitus, patient denies ear fullness | No attack | No progress | No paroxysmal exacerbation | No special discomfort |
| 3 | 72 | female | 2 | Attacks occur 1-2 times a week, each lasting more than an hour. | deaf | Persistent, progressive tinnitus with ear fullness | No attack | No progress | Almost controlled, each tinnitus < 1 min | The patient has an unsteady gait and needs to walk with the help of a cane. |
| 4 | 48 | female | 3 | Recurrent paroxysmal vertigo, lasting more than half an hour each time, with no effect of medication. | The ABR response threshold was 20dBnHL | Fluctuating tinnitus, occasional ear fullness | No attack | No progress | No paroxysmal exacerbation | The patient is mildly dizzy, but does not affect life or work. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



