
Submitted:
23 August 2024
Posted:
23 August 2024
You are already at the latest version
Abstract
This study checked whether vitamin D (Vit-D) supplementation improves the efficacy of resistance training (RT) in terms of increasing muscle strength and lean body mass (LBM) and influencing cardiorespiratory fitness (VO2max) in Vit-D insufficient middle-aged healthy men. Participants (n = 28) were quasi‐randomly assigned to one of the two groups, which, in a double‐blind manner, supplemented their diet daily with either Vit‐D (8000 IU; VD) or placebo (PLC) during participation in a 12‐week supervised RT program. During the intervention, serum Vit‐D concentrations increased 2.6‐fold (p < 0.001) in the VD group, while no changes occurred in the PLC group. Muscle strength gains (p < 0.001) as measured in seven exercises performed on RT equipment and increases (p < 0.001) in LBM were similar in the two groups. Total fat mass, percent total fat, and percent android fat decreased (p < 0.05) to a similar extent in both groups, but there was no change in VO2max in either group. In conclusion, in healthy Vit‐D insufficient middle-aged men engaged in resistance training, Vit‐D supplementation increases serum 25(OH)D levels but does not enhance gains in muscle strength and LBM or decreases in fat mass and fat percentage and does not affect cardiorespiratory fitness.
Keywords:
testosterone
; cortisol
; growth hormone
; parathormone
; insulin
; HOMA-IR
; cytokines
1. Introduction
Vitamin D (Vit-D) is considered a critical and important micronutrient for overall health [1,2], with much attention given to its importance in bone and skeletal muscle health [3,4].
The bioactive form of Vit-D acts through specific nuclear receptors (VDR) [5,6,7], which have been identified in most tissues of the human body [8,9,10]. In skeletal muscle, Vit-D exerts both genomic and non-genomic effects [11,12]. In human myoblasts, Vit-D has been shown to stimulate protein synthesis [13]. In older women, Vit-D supplementation increased intramyonuclear VDR concentration and muscle fiber size [14].
However, recent literature reviews on the effects of Vit-D supplementation on muscle strength, an important indicator of muscle health [15], have led to conflicting conclusions. Meta-analysis by Tomlinson et al. [16] showed that Vit-D supplementation increases both upper and lower limb muscle strength, while Han et al. [17], also based on meta-analysis, concluded that Vit-D supplementation does not improve muscle strength. Meta-analysis by Zhang et al. [18] revealed no impact of Vit-D supplementation on overall muscle strength outcomes. However, further analysis showed positive effect on lower limb muscle strength, but not upper limb muscle strength or muscle power. The authors [18] concluded, that different muscle groups and functions may respond differently to Vit-D supplementation. Chiang et al. [19], conducting a systematic literature review, found that Vit-D2 supplementation was ineffective at impacting muscle strength, whereas Vit-D3 ingestion had positive influence. Meta-analysis by Abshirini et al. [20] focused on the effect of Vit-D supplementation on hand grip strength. Their pooled findings showed that Vit-D did not influence hand grip strength. However, the subgroup analyses revealed that Vit-D supplementation improved hand grip strength with respect to dosages >1000 IU/day, a treatment duration of 3 months, and subjects with baseline serum 25(OH)D levels <30 ng/mL (75 nmol/L) [20]. Another meta-analysis [21] showed positive effect of Vit-D supplementation on lower extremity muscle strength. Of note, majority of the literature reviews cited above [16,17,18,19] included studies of relatively young athletic populations. Only Abshirini et al. [20] and Muir & Montero-Odasso [21] focused on data available for middle-aged and older subjects.
Undoubtedly, the most effective strategy for increasing muscle strength and mass is resistance training (RT) [22,23,24], but it is less clear whether combining Vit-D supplementation with RT improves its outcomes. Recent meta-analysis revealed that Vit-D supplementation had an additive effect to RT in increasing muscle strength of the lower limbs in older adults [25], but this conclusion was based on the results of only three studies. A more recent study [26] in elderly persons with or without chronic obstructive pulmonary disease showed the effectiveness of a 13-week RT program in increasing muscle mass and strength but found no additional effect of concomitant vitamin D supplementation on RT-associated changes in muscle mass or function.
Maximal oxygen uptake (VO2max) is often referred to as cardiorespiratory fitness and is considered an objective measure of health [27,28]. The functional state of the lungs, heart, blood vessels and skeletal muscles together with the oxygen transport capacity of the blood are the major determinants of an individual’s VO2max [29]. VDR is expressed in all these organs, i.e. lungs, heart, blood vessels, skeletal muscle [11,30,31,32]. Vit-D can promote erythropoiesis and hemoglobin synthesis [33], also affect the binding affinity of oxygen to hemoglobin [34]. Furthermore, Vit-D may be crucial for mitochondrial oxidative phosphorylation capacity [35]. Therefore, it is not surprising that an independent robust association have been observed between serum Vit-D levels and VO2max in adults over an age range of 20–73 years [36,37].
However, it is not clear whether Vit-D supplementation is effective in increasing VO2max. A recent literature review [38] concluded that Vit-D supplementation can significantly improve VO2max in elite athletes, but this claim was based on the results of only two studies. Research in athletes of varying levels and in recreationally active youth have yielded inconclusive results showing no effect [39,40] or a marginal positive influence [41] of Vit-D supplementation on VO2max. In some of the studies in young men [42,43] that reported a positive effect of vitamin D supplementation on cardiorespiratory fitness, VO2max was not actually measured but indirectly calculated. In elderly patients with chronic obstructive pulmonary disease participating in a rehabilitation program, Hornikx et al. [44] observed significantly greater improvements in VO2max and inspiratory muscle strength as a result of Vit-D supplementation compared to placebo.
Muscle mass and strength [45] as well as VO2max [46] decline with increased age and may lead to decreased quality of life, loss of independence and disability in elderly. Thus, measures that can forestall declines in muscle strength and VO2max may be important considerations for middle-aged adults that may help maintain better health status and reduce the risk of substantial decline in quality of life in older age. The literature cited above suggests that RT combined with Vit-D supplementation may be an effective intervention in this context, but the available data are limited and inconclusive, particularly for the middle-age population. Therefore, the objective of this study was to assess whether systematic RT combined with Vit-D supplementation is more effective in terms of increasing muscle strength and lean body mass (LBM) than the same RT program without Vit-D supplementation in Vit-D insufficient middle-aged healthy men. The secondary objective was to elucidate whether Vit-D supplementation during participation in RT program affects cardiorespiratory fitness in the same men.
2. Materials and Methods
2.1. Participants
Middle aged and older men (aged >50 years) were sent invitations to participate in the study via emails and phone calls that were obtained through personal contacts and various organizations’ mailing lists. The initial inclusion criterion was the absence of a chronic disease that would preclude participation in systematic physical training. Additional criteria were non-participation in competitive sports or resistance training programs and non-use of Vit-D supplements in the past year. The total number of men who expressed willingness to participate in the study and met these inclusion criteria was 31. At the first meeting with the research team, each potential participant received detailed information about the purpose of the study, the procedures related to participation in it and the time required for this. The men who chose to participate in the study then provided relevant verbal and written informed consent and donated the baseline venous blood sample. During the subsequent 4-week preparatory phase (Figure 1), one man dropped out of the study due to injury and two withdrew for personal reasons. All the remaining 28 men went through the 12-week main phase of the study, participating in at least 80% of the planned resistance training sessions, performing all the planned physical tests, and donating all the necessary blood samples. The age, height, body mass, and body mass index (mean ± SD) of these 28 men at the beginning of the preparatory phase of the study were 58.8 ± 4.4 years, 182.9 ± 6.3 cm, 90.03 ± 15.26 kg, and 26.9 ± 4.0 kg/m2, respectively.
2.2. Design and General Organization of the Study
The study was carried out according to a double-blind, placebo controlled, quasi-randomized protocol and it was divided into a 4-week preparatory and a 12-week main phase (Figure 1). The entire 16-week study took place from January to April, i.e. during the winter-spring period of the year, when the prevalence of Vit-D insufficiency and deficiency is high in Estonia [47,48].
In the the preparatory phase, participants were familiarized with RT equipment, taught to perform strength exercises technically correctly and instructed on documenting their regular diet and loading the information into a web-based platform Nutridata. This period also aimed to adapt participants to a consistent training schedule, equalize the training levels of the participants and to address the neural and learning adjustments that occur in the first weeks of starting systematic RT [49]. At the end of the preparatory phase, the participants were divided into two groups: one receiving a placebo (PLC) and the other Vit-D supplements (VD). This was done by arranging participants in ascending order of body mass and then assigning them to alternate groups. No significant differences in age, height, body mass, body mass index or Vit-D status were found between the groups at the beginning of the study (Table 1). According to the definitions proposed by Pludowski et al. [50], Vit-D status of the participants at this stage of the study was classified as deficient (9 men with serum 25(OH)D concentrations <50 nmol/L), insufficient (16 men with serum 25(OH)D concentrations ≥50 and <75 nmol/L), or sufficient (3 men with serum 25(OH)D concentrations 75–125 nmol/L). Since men with Vit-D deficiency and insufficiency accounted for 32% and 57%, respectively, and given that according to Heaney [51] the distinction between Vit-D deficiency and insufficiency may not be crucial, we describe the participants in this study generally as “Vit-D insufficient men”.
In the main phase of the study, participants attended in supervised RT sessions three times a week and consumed either Vit-D supplements or placebo daily. At the conclusion of each 4-week training cycle, muscle strength assessments were conducted. Participants were instructed to log their dietary intake for four consecutive days on three separate occasions using the Nutridata web-based platform in the main phase (Figure 1).
The participants underwent a maximal oxygen uptake (VO2max) test to measure their aerobic capacity and body composition assessment both before and after the main phase of the study (Figure 1). Body mass was measured, and blood samples were taken five times, starting before the beginning of the preparatory phase, and continuing with 4 week intervals until conclusion of the main phase (Figure 1).

Table 1.
Anthropometric characteristics and serum vitamin D concentrations in the two groups of participants at the beginning of the main phase of the study.
Table 1.
Anthropometric characteristics and serum vitamin D concentrations in the two groups of participants at the beginning of the main phase of the study.
| Variable | Placebo (n = 14) | Vitamin D (n = 14) |
|---|---|---|
| Age (years) | 58.3 ± 4.7 | 59.2 ± 4.2 |
| Height (cm) | 181.9 ± 5.6 | 183.9 ± 7.0 |
| Body mass (kg) | 90.01 ± 15.54 | 90.05 ± 15.56 |
| BMI (kg/m2) | 27.1 ± 4.0 | 26.6 ± 4.0 |
| 25(OH)D (nmol/L) | 62.5 ± 13.8 | 59.2 ± 19.5 |
Data are presented as mean ± SD. BMI, body mass index.
2.3. Supervised Resistance Training and Assessment of Muscle Strength
The RT program included 7 exercises [52] performed on special gym equipment: seated row, knee extension, biceps curl, triceps push-down, lateral pull-down (Precor, Woodinville, USA), leg press (David, Helsinki, Finland) and chest press (Technogym, Cesena, Italy). All training sessions in both the preparatory and main phases were supervised by a member of the research team and took place at the University of Tartu Sports Club. Training frequency was two sessions per week for the first two weeks of the preparatory phase, increasing to three sessions per week from the third week onward until the end of the study. Training sessions were scheduled in the morning or evening to accommodate individual daily routines of participants. Each session began with a 10‒15 min light warm-up performed on 200 m indoor running track, cycle, or rowing ergometer. The sequence of exercises within a session was flexible, except for the knee extension and leg press, which required an upper body exercise to be performed between them. Each exercise’s concentric and eccentric phases took about 1‒2 s. Rest periods between sets ranged from 1‒2 min, and the interval between different exercises was set at 3 min [53]. Participants were required to complete all sets of one exercise consecutively before moving on to the next exercise. The number of sets and repetitions varied throughout the study (Table 2). In the preparatory phase initial training weights for every exercise were determined by the supervisor, and in the main phase, training weights were adjusted based on a percentage of each individual’s one-repetition maximum (1RM), as outlined in Table 2. This way the weights aligned with each participant’s personal progress. 1RMs were estimated from five-repetition maximums (5RMs), as described by Baechle and Earle [54]. These 5RM tests were conducted at weeks ‒1, 4, 8, and 12 (Figure 1), and were used to set individual training weights for every exercise for the next 4-week training cycle. The 5RM testing protocol involved progressively increasing weights to determine the maximum weight lifted five times correctly. A detailed description of the 5RM assessment procedure is provided in our previous publication [55]. The 5RM values were ascertained in order of lateral pull-down, triceps push-down, leg press, and chest press during the first training session of the RM testing week. In the second session, seated row, knee extension, and biceps curl were assessed in that order. In addition to the 5RM tests, participants performed one remaining set of exercises in which no tests were performed in a given testing session. In the third training session of the RM testing week, participants performed one set of each exercise, as shown in Table 2.
2.4. Dietary Supplementation
Throughout the main phase of the study, participants were instructed to administer gelatine capsules containing either vitamin D3 or placebo. The Vit-D and placebo capsules were identical, they could not be distinguished by appearance and participants were provided with them in a double-blind manner. The product codes for Vit-D and placebo capsules were ST45851 and ST47202, respectively (Diafarm A/S, Vejle, Denmark). The daily dose of supplemental Vit-D was 8000 IU. In the main phase, following each training session, all participants ingested 50 g of a whey-based dietary supplement (Whey 80, Elite Fitness OY, Helsinki, Finland). Each 50 g serving of this supplement provided 40 g of pure whey protein, 2.5 g of carbohydrates, 3.5 g of fats, and 200 kcal of energy. At the end of each workout, the training supervisor personally handed out the supplement, instructing participants to dissolve the whey powder in about 0.5 L of water and consume it within 30 min. Standardization of protein intake during early post-workout recovery was deemed important because consuming protein in this period influences muscle protein synthesis [56,57], and post-workout changes in muscle protein synthesis are linked to the degree of muscle hypertrophy that manifests as a result of several weeks RT [58].
2.5. Monitoring of Dietary Intake
At weeks 2, 6, and 11 of the main phase (Figure 1), participants recorded their food intake over four consecutive days on the Nutridata platform. Each recording period included one non-training day, typically during the weekend, when participants were not engaged in their regular work. Participants granted a member of the research team access to their Nutridata entries, allowing this individual to conduct detailed dietary analyses on both an individual and group basis. Throughout the study, participants were instructed to maintain their usual dietary patterns and to avoid from consuming any supplements except those provided by the research team member, i.e. Vit-D or placebo and whey protein.
2.6. Assessment of Body Size and Composition
The height of the subjects was determined to an accuracy of 5 mm using a stadiometer (Seca bodymeter 206, Seca GmbH, Hamburg, Germany). Body mass (BM) without clothing was measured following an overnight fast on five occasions throughout the study (Figure 1) to the precision of 1 g using an electronic scale (CH3G-150I Combics, Sartorius AG, Goettingen, Germany). Before and at the end of the main phase (Figure 1) participants underwent dual-energy X-ray absorptiometry (DXA) body composition analysis (Hologic Discovery W model; Hologic, Inc., Marlborough, USA). Measurements included the lean mass of the torso, arms and legs, alongside the mass and percentage of android fat and the total fat mass and percentage.
2.7. Assessment of Maximal Oxygen Uptake
Participants took a graded exercise test on a motorized treadmill both before and after the main phase of the study (Figure 1) to assess their maximum oxygen uptake and related parameters. The equipment used included a Viasys/Jaeger LE300 C motorized treadmill (Viasys Healthcare GmbH, Hoechberg, Germany), a MasterScreen CPX breath-by-breath metabolic system (Viasys Healthcare GmbH, Hoechberg, Germany), and a heart rate monitor Polar Electro (Finland). An incremental walking test begun with a 1.5% incline and a constant speed of 6.0 km/h. The treadmill’s incline was increased by 3.5% every three minutes while maintaining the speed, until the participant could no longer continue. The highest average oxygen uptake over a 30-s period towards the end of the test was recorded to determine the maximal oxygen uptake (VO2max). Achievement of VO2max was confirmed if the participant had reached a respiratory exchange ratio (RER) greater than 1.00 and a heart rate exceeding 90% of their predicted maximum based on age, as the criteria set by Davis et al. [59].
2.8. Blood Sampling and Analyses
During the study, participants had five venous blood samples drawn at specified times: at the beginning of the preparatory phase, after the preparatory phase concluded, and after the 4th, 8th, and 12th week of the main phase (Figure 1). All the samples were collected after two days of rest, following a roughly 12-hour overnight fast, either on a Monday or Tuesday morning. The blood was drawn into 5 mL Vacutainer serum tubes, which were let to clot for 10 min at room temperature. The samples were then centrifuged for another 10 min at 3000 rpm (2000g) at a temperature of 4 °C using an Eppendorf 5804R centrifuge (Eppendorf AG in Hamburg, Germany). Post-centrifugation, the samples were kept at 4 °C until analyses, the serum specimens for measurement of cytokine levels were maintained at ‒25 °C.
All five blood samples were analysed for serum 25(OH)D. Concentrations of various biomarkers - testosterone, growth hormone (GH), insulin-like growth factor-1 (IGF-1), cortisol, parathormone (PTH), calcium (Ca), ionized Ca, urea, creatine kinase (CK), glucose, ferritin, and insulin - were measured in the samples taken just before the main phase and right after the 8th and 12th week (Figure 1). These analyses were conducted at the United Laboratories of Tartu University Hospital. In the blood sample taken before and after the main phase (Figure 1), serum cytokine levels for interleukin 1α (IL-1α), interleukin 1β (IL-1β), interleukin 4 (IL-4), interleukin 6 (IL-6), interleukin 8 (IL-8), interleukin 10 (IL-10), tumor necrosis factor alpha (TNF-α), and monocyte chemoattractant protein 1 (MCP-1) were measured. The cytokine analysis was performed at the Institute of Biomedicine and Translational Medicine of the University of Tartu.
The IDS-iSYS Multi-Discipline Automated Analyzer (Immunodiagnostic Systems Limited, Copenhagen, Denmark) was used to measure serum concentrations of 25(OH)D, IGF-1, and GH using the chemiluminescence immunoassay method. The electrochemiluminescence immunoassay (ECLIA) on the Cobas 6000 analyzer (Roche Diagnostics GmbH, Tokyo, Japan) was used to determine levels of testosterone, cortisol, PTH, and CK, and insulin. For serum Ca and urea concentration measurements, the same Cobas 6000 analyzer was employed, using the photometrical NM-BAPTA method and a kinetic test with urease and glutamate dehydrogenase, respectively. Ionized Ca was measured with an ion-selective electrode method on a Prime ES analyzer (Roche, Mannheim, Germany). Serum glucose levels were quantified using the hexokinase enzymatic method on a Roche/Hitachi Cobas 6000 c501 analyzer (Roche Diagnostics GmbH, Mannheim, Germany). The homeostasis model assessment of insulin resistance (HOMA-IR) index was calculated using the formula: HOMA-IR = (serum glucose (mmol/L) × serum insulin (μU/mL))/22.5 [60].
The Evidence Investigator Cytokine and Growth Factors High-Sensitivity Array based on the sandwich chemiluminescent immunoassay, version V1.4.1 (RANDOX Laboratories Ltd., Crumlin, United Kingdom) was used for simultaneous quantitative detection of cytokines.
2.9. Statistical Analysis
Data were analysed using Statistica 13.3 software (TIBCO Software Inc., Palo Alto, CA, USA). All data were checked for normal distribution using the Kolmogorov–Smirnov test, which revealed that IL-1α, and IL-1β were not normally distributed and were therefore log-transformed. A two-way repeated analysis of variance ANOVA with a between factor of group (VD vs. PLC) and within factor of time was used to evaluate the differences within and between the groups. If a significant main effect or interaction occurred, Tukey’s honestly significant difference post hoc analysis was used to locate differences between the means. The mean values of different parameters registered at a single time point were compared using Student’s t test for independent variables. Significance was set at p < 0.05 level. Data are presented as means ± SD.
3. Results
Energy and nutrient intake of the participants is shown in Table 3. As compliance of many participants with requirements of reporting daily energy and nutrients intake was low, only reliable data, that were limited to six men from both groups, are presented. No main effects of group or time or group by time interaction (in all cases p > 0.05) occurred for any of the dietary parameters measured.
For serum 25(OH)D levels, significant main effects of group (F = 47.91) and time (F = 113.29), and a significant group by time interaction (F = 170.25) were observed (p < 0.0001 in all cases) (Figure 2). At weeks ‒4 and 0, serum 25(OH)D concentrations were similar in the two groups. At week 4, i.e. 4 weeks after starting Vit-D and placebo administration, serum 25(OH)D levels were significantly higher in the VD group than in the PLC group (83.0 ± 13.7 nmol/L vs. 49.9 ± 13.6 nmol/L, respectively; p = 0.0002). In the VD group, serum 25(OH)D continued to rise throughout the rest of the main phase of the study, remaining consistently significantly higher than in the PLC group, reaching a level of 142.7 ± 20.1 nmol/L at week 12. In the PLC group, there was a significant (p = 0.010) decrease in serum 25(OH)D from week ‒4 to week 4, after which 25(OH)D remained consistently low from 51.0 ± 12.3 to 50.3 ± 12.2 nmol/L until week 12.
Compliance to the RT protocol was high (91.5% on average) and similar in the two groups (91% in PLC and 92% in VD). A significant main effect of time was observed for 1RM for all seven exercises: leg press (F = 133.03), knee extension (F = 158.90), chest press (F = 351.12), triceps push-down (F = 132.29), biceps curl (F = 209.50), lateral pull-down (F = 143.11), and seated row (F = 176.44) (p < 0.0001 in all cases) (Table 4). However, no significant main effect of group or group by time interaction was observed for 1RM for any of the exercise (p > 0.05 in all cases). In both groups, the greatest increase in 1RM was seen in knee extension (69.3% and 83.6% in VD and PLC, respectively), and the smallest change in triceps push-down (23.3% and 26.4% in VD and PLC, respectively) (Figure 3).
Significant main effects of time were found for body mass (F = 4.68; p = 0.005), total fat mass (F = 18.05), total fat percentage (F = 48.88), android fat percentage (F = 29.62), total lean mass (F = 78.34), trunk lean mass (F = 29.19), arms lean mass (F = 33.86), and legs lean mass (F = 28.20) (p < 0.001 in all cases) (Table 5). No significant main effect of time was observed for android fat mass (F = 3.059; p = 0.092). There were no main effects of group or group by time interactions for any of the body composition parameter (p > 0.05 in all cases). Over the 12-week RT program, both the PLC and VD groups exhibited significant increases in total lean mass, trunk lean mass, arms lean mass, and legs lean mass, as well as decreases in total fat mass, fat percentage and android fat percentage (p < 0.05 in all cases). However, there were no significant between-group differences in the extent of changes in any body composition parameter (p > 0.05 in all cases).
A significant main effect of time was found for relative VO2max (mL/min/kg) levels (F = 5.158; p = 0.032), with no significant main effect of group (p = 0.473) or group by time interaction (p = 0.839) (Table 6). A small (2.3%) overall decrease in relative VO2max occurred between weeks 0 and 12 (p = 0,031). For absolute VO2max (L/min), there was no significant main effect of group (p = 0.533) or time (p = 0.146), nor a significant group by time interaction (p = 0.551). No significant main effect of group (p = 0.841) or time (p = 0.062), nor group by time interaction (p = 0.445), were observed for the RER. A significant group by time interaction occurred for peak HR (F = 4.979; p = 0.035) with no significant main effects of time (p = 0.406) or group (p = 0.301). No significant main effects of group or time, or group-by-time interactions, were observed for ventilation (VE) and breathing frequency (BF) (p > 0.05 in all cases) (Table 6).
A significant group by time interaction occurred for parathormone levels (F = 8.768; p = 0.0005), with no main effect of time or group (p > 0.05 in both cases) (Table 7). In PLC group parathormone levels increased by 22.8% from week 0 to week 12 (p = 0.008). A significant main effect of time (F = 8.357; p = 0.0007), but not that of group (p = 0.916) occurred for cortisol. An overall decrease of 16.1% (p = 0,002) in cortisol levels was evident from week 0 to week 12, but there was no significant group by time interaction for cortisol (p = 0.787). No main effects of group or time, nor group by time interactions were observed for IGF-1, testosterone, growth hormone and insulin levels (p > 0.05 in all cases) (Table 7).
No significant main effects of group and time, or group-by-time interactions were observed for serum levels of IL-1α, IL-1β, IL-4, IL-6, IL-8, IL-10, TNF-α, and MCP-1, or for the IL-10/TNF-α ratio (p > 0.05 in all cases; Table 8).
There were no significant main effects of group or time and no group-by-time interactions for hemoglobin and glucose concentrations (in all cases p > 0.05; Table 9). A significant main effect of time (F = 7.595; p = 0.0013), but not that of group (p = 0.837) or group-by-time interaction (p = 0.984) occurred for serum ferritin levels (Table 9). Overall serum ferritin levels decreased from 194.4 ± 116.3 μg/L at week 0 to 167.6 ± 105.2 μg/L at week 12, i.e. by an average 13.8% (p = 0.011). There was a significant group-by-time interaction (F = 3.532; p = 0.036), but no significant main effects of group or time (in both cases p > 0.05) for HOMA-IR (Table 9).
Table 8.
Serum cytokine levels during 12-week supplementation and resistance training period.
| Variables | Placebo (n = 14) | Vitamin D (n = 10) | ||
|---|---|---|---|---|
| Week 0 | Week 12 | Week 0 | Week 12 | |
| IL-1α (pg/mL) | 0.09 ± 0.12 | 0.08 ± 0.13 | 0.05 ± 0.06 | 0.05 ± 0.08 |
| IL-1β (pg/mL) | 1.02 ± 0.71 | 1.06 ± 0.83 | 0.83 ± 0.24 | 0.75 ± 0.19 |
| IL-4 (pg/mL) | 1.08 ± 0.32 | 1.21 ± 0.48 | 1.07 ± 0.35 | 1.02 ± 0.32 |
| IL-6 (pg/mL) | 0.81 ± 0.58 | 0.80 ± 0.44 | 1.07 ± 0.67 | 1.11 ± 0.78 |
| IL-8 (pg/mL) | 10.20 ± 4.77 | 9.92 ± 4.92 | 11.24 ± 4.84 | 10.25 ± 3.90 |
| IL-10 (pg/mL) | 0.60 ± 0.43 | 0.55 ± 0.28 | 0.47 ± 0.18 | 0.42 ± 0.13 |
| TNF-α (pg/mL) | 2.68 ± 0.95 | 2.58 ± 1.11 | 2.44 ± 0.91 | 2.40 ± 0.65 |
| IL-10/TNF-α | 0.21 ± 0.09 | 0.21 ± 0.06 | 0.20 ± 0.08 | 0.18 ± 0.06 |
| MCP-1 (pg/mL) | 219.1 ± 60.7 | 225.3 ± 94.5 | 201.3 ± 93.2 | 196.9 ± 90.5 |
Data are presented as mean ± SD. IL, interleukin; TNF-α, tumor necrosis factor alpha; MCP-1, monocyte chemoattractant protein 1.
No main effects of group or time or group-by-time interactions were observed for serum ionized calcium and calcium concentrations and creatine kinase activity (in all cases p > 0.05; Table 10). A significant main effect of time (F = 3.824; p = 0.028) and group-by-time interaction (F = 4.704; p = 0.013) with no significant main effect of group (p = 0.555) occurred for serum urea levels. In VD group only, a significant increase in serum urea level was observed in week 8 (p = 0.005) and week 12 (p = 0.036) compared to week 0 (Table 10).
4. Discussion
The primary objective of this study was to assess whether systematic RT combined with Vit-D supplementation is more effective in terms of increasing muscle strength and LBM than the same RT program without Vit-D supplementation in Vit-D insufficient healthy middle-aged men. The results show that over the course of 12 weeks of RT, 1RM increased significantly and to a similar extent in all seven exercises in both the VD and PLC groups. During the same period, serum 25(OH)D increased approximately 2.6-fold in the VD group but remained stably low in the PLC group. These data are consistent with previous findings of a positive impact of RT on muscle strength in middle-aged men [61,62,63] but indicate that Vit-D supplementation does not potentiate the effects of RT in this age and sex group.
Four previous studies [26,53,64,65] have also shown that Vit-D supplementation has no additional effect on RT in increasing muscle strength in middle-aged and elderly individuals. However, in two studies the participants were exclusively [65] or mostly (90%) [64] elderly women. It should also be noted that these two studies only measured maximal isometric quadriceps strength [65] or quadriceps and handgrip strength [64]. Given that testosterone can influence the RT-induced gains in muscle strength [66,67] and that Vit-D supplementation can increase serum testosterone levels [68,69], sex differences in the effect of Vit-D supplementation on the efficacy of RT cannot be excluded a priori. It is also relevant to evaluate the potential effect of combined RT and Vit-D supplementation on strength gains in different muscle groups, as they may respond differently to vitamin D supplementation [18]. Nevertheless, our data presented here on middle-aged men agree with those obtained in studies of older women [64,65] and show that RT improves muscle strength, but Vit-D supplementation does not increase the efficacy of RT. In addition, our muscle strength data from seven different exercises show no differences between muscle groups in terms of response to the Vit-D supplementation in middle-aged men.
Agergaard et al. [53] investigated the possible effects of Vit-D supplementation during 12 weeks of systematic RT on the quadriceps muscle strength gain in somewhat older healthy men (60–75 years) than our participants (52–66 years) and found no additive effect of Vit-D on either muscle hypertrophy or muscle strength. However, they observed improved muscle quality (increased muscle strength/cross sectional area ratio) in Vit-D supplemented group compared to placebo group. In healthy subjects and patients with chronic obstructive pulmonary disease (age 56–77 years; 46% men), Vit-D supplementation during 13 weeks of RT did not affect maximal muscle strength, assessed as unilateral knee extension and leg press or bilateral chest press [26]. Our data showing absence of an additive effect of Vit-D supplementation on muscle strength gains during RT are generally consistent with those of these researchers [26,53], but extend to much more muscle groups in a slightly younger age group of men.
In our participants, 12 weeks of systematic RT had no effect on body weight but induced significant positive health-related changes in body composition consisting of significant decreases in total fat mass, total fat percentage and android fat percentage. At the same time, significant increases occurred in total lean mass, trunk lean mass and appendicular lean mass.
However, all changes in body composition were of similar extent in the VD and PLC groups, indicating that vitamin D supplementation did not increase the efficacy of RT. Mølmen et al. [26] reported increases in total lean mass, total fat mass and visceral fat mass, which are in good agreement with our findings, showing efficacy of RT with no additive effect of Vit-D supplementation.
One of our considerations for why vitamin D might improve the efficacy of RT in terms of muscle strength gains in middle-aged men was the vitamin’s potential positive effect on testosterone levels [68,69]. However, in our participants, Vit-D supplementation had no effect on serum testosterone or other hormones (insulin, growth hormone, IGF-1, cortisol) that may affect muscle protein metabolism and muscle function. Similar findings were reported by other researchers [26,64].
The secondary objective of this study was to elucidate whether systematic RT or Vit-D supplementation during participation in RT program affects cardiorespiratory fitness in Vit-D insufficient healthy middle-aged men. Our results show no effect of 12 weeks of RT with or without concomitant Vit-D supplementation on absolute VO2max. Overall, a small (2.3%) decrease in relative VO2max occurred during 12 weeks of RT.
We considered assessment of the potential effect of interventions applied in this study on VO2max important by several reasons. First, skeletal muscle oxidative capacity that is among the factors determining VO2max, is dependent on the mitochondrial function [70], and systematic RT may lead to positive mitochondrial adaptations [71,72,73]. Second, in middle-aged to elderly subjects, systematic RT may produce significant increases in VO2max that are as large as in case of aerobic training [74], or slightly smaller [75,76]. Third, VDR is expressed in all human organs, the function of which may influence VO2max [11,30,31,32], Vit-D can promote erythropoiesis and hemoglobin synthesis [33] and affect the binding affinity of oxygen to hemoglobin [34]. Finally, Vit-D may be crucial for mitochondrial oxidative phosphorylation capacity [35]. Nevertheless, 12 weeks of RT with or without concomitant Vit-D supplementation did not influence blood hemoglobin levels or absolute VO2max in our participants. At the same time, there was a small but statistically significant decrease in relative VO2max, probably due to a tendency to gain weight.
An overall significant 13.8% decline in serum ferritin levels across the 12-week supplementation and RT period indicates a decrease in body’s iron stores [77] and is consistent with our previous observation in young Vit-D deficient men who completed similar RT program with concomitant Vit-D supplementation [78]. However, serum ferritin levels <35 μg/L, indicating iron-deficient state [77], occurred only in two participants at week 0 and in one of these two participants also at weeks 8 and 12. Both men belonged into the VD group. Considering that hemoglobin concentrations were constantly >130 g/L in all participants, i.e. there were no manifestations of anemia, and that iron deficiency without anemia does not affect VO2max [77], it seems unlikely that low iron status masked the potential effect of Vit-D supplementation on VO2max in our participants. Moreover, Shoemaker et al. [79] demonstrated significant training-induced increases in VO2max despite 73% decreases in serum ferritin levels in young men. The reasons why training loads can lead to a decrease in ferritin levels are not entirely clear and they may differ in different situations. It has been speculated that the improvement of various aspects of performance against the background of a decrease in serum ferritin may reflect training tolerance of athletes [80] and physiological adaptation reactions, for example, at the level of intensification of the synthesis of iron-containing enzyme proteins [81].
Previous studies on middle-aged adults [72] and elderly men [73] demonstrated mitochondrial adaptations as a result of 10 and 6 weeks of RT, respectively, but VO2max was not measured by these researchers. In studies showing a significant positive effect of RT on VO2max [74,75], the duration of systematic RT was 6 months, i.e., twice as long as in our participants. Thus, the RT program in our participants may have been too short-term to induce measurable changes in VO2max.
In our participants, there were no between-group differences or changes across time in physiological parameters measured during VO2max tests (respiratory exchange ratio, maximal heart rate, maximal breath frequency, maximal pulmonary ventilation). These findings are consistent with the lack of meaningful changes in VO2max. Interestingly, Kujach et al. [39] have observed increases in maximal breath frequency and maximal lung ventilation due to Vit-D supplementation in college aged males.
Bioactive form of Vit-D is known to inhibit and stimulate the production of pro- and anti-inflammatory cytokines, respectively [7,82,83]. In young healthy Vit-D deficient men, 12 weeks of RT with concomitant Vit-D supplementation improved the inflammatory status as reflected by an increase in the serum IL-10/TNF-α ratio [78]. In the middle-aged men in the present study, RT and Vit-D supplementation did not exhibit this kind of interaction, and no changes were observed in any of the measured cytokine levels. The reasons for the discrepancy in the results of these two studies remain unclear, but it can be assumed that they may be partly related to the fact that our middle-aged men had higher pre-intervention Vit-D status compared to young participants in the previous [78] study. On the other hand, recent findings of Silva et al. [84] show that 12 weeks of RT per se, i.e. without Vit-D supplementation, may have an anti-inflammatory effect, including a strong tendency to improved IL-10/TNF-α ratio, in middle-aged and elderly patients with chronic obstructive pulmonary disease (COPD). The difference between our data and that of Silva et al. [84] regarding the anti-inflammatory effect of RT in middle-aged and elderly people, may be at least partially explained by the fact that COPD is an inflammatory disease [85], but our subjects were healthy men.
Chronic Vit-D deficiency is associated with insulin resistance [86]. Six-month Vit-D supplementation in obese Vit-D insufficient adolescents [87] and 12 weeks of RT in obese middle-aged men [88] improved insulin resistance which was reflected in a significant decrease in HOMA-IR index. In our normal weight middle-aged men, 12 weeks of RT with or without Vit-D supplementation did not affect serum glucose and insulin levels or HOMA-IR. Our results are consistent with those of three previous studies in overweight and obese young adults with varying Vit-S status [89], overweight and obese middle-aged older adults with sufficient Vit-D status and type 2 diabetes [90], and normal weight young Vit-D deficient men [78] who participated in a similar 12-week RT program with concomitant Vit-D supplementation.
In our VD group participants, the daily dose of supplemental Vit-D was 8000 IU, but the tolerable upper intake level of Vit-D established for adults is 4000 IU per day [91]. On the other hand, a daily dose of 10000 IU is considered the lowest-observed-adverse-effect-level of Vit-D intake [91], and the position of The Endocrine Society is that daily intake of this amount may be necessary to treat Vit-D deficiency [92]. Nevertheless, Vit-D oversupply may lead to serious health problems including formation of kidney stones, calcification of soft tissues and vasculature [50,93]. Hypercalcemia is a sensitive marker of the potential harmful effects of Vit-D [92,94,95]. It is widely accepted that hypercalcemia induced by vitamin D intoxication usually only occur at serum 25(OH)D concentrations above 375 nmol/L and is very rare [92,95,96]. In our VD group participants, serum calcium levels remained unchanged throughout the study period. The highest 25(OH)D concentrations in their serum occurred at week 12 and were in the range of 120.7–188.1 nmol/L, i.e. well below the critical level.
In our PLC group participants, serum 25(OH)D levels did not increase during the RT and placebo supplementation period and were in the range of 23.5–63.1 nmol/L at week 12. Vit-D insufficiency may lead to secondary hyperparathyroidism that has negative implications for cardiovascular and bone health [97,98]. In PLC group, but not in VD group, serum parathormone levels increased during the 12 weeks of RT and supplementation, but still remained within the physiologically normal range. Thus, the data discussed in the last two sections show that neither high-dose vitamin D supplementation nor placebo posed a risk to the health of our participants.
Our participants donated blood samples always in the morning after two resting days. Under these conditions, fasting serum urea concentrations below 7.5 mmol/L and moderate levels of creatine kinase activity suggest that our participants tolerated training loads well and started each consecutive training week in a well-recovered state [99].
The main strengths of our study are the supervised RT and dietary supplementation program and high compliance rate of participants with both requirements. On the other hand, the main limitation of the study was the low compliance of the subjects with the guidelines for reporting daily energy and nutrient intake for three 3-day periods of the 12-week intervention. Although all participants verbally confirmed that their usual diet did not change during their participation in the study, and the data of the men who followed the corresponding instructions correctly for at least half the duration of the study confirm that, our data remain incomplete in this regard. Nevertheless, we are not aware of any circumstances that directly or indirectly would indicate that changes in habitual diet could have masked the possible effects of Vit-D supplementation on the outcomes of our study.
5. Conclusions
In conclusion, in healthy Vit-D insufficient middle-aged men engaged in 12-week RT program, Vit-D supplementation increases serum 25(OH)D levels and avoids increases in serum parathormone concentration but does not enhance RT-induced gains in muscle strength and LBM or decreases in fat mass and fat percentage. 12-week RT with or without concomitant Vit-D supplementation does not affect cardiorespiratory fitness, serum pro- and anti-inflammatory cytokine levels or HOMA-IR, an index of insulin resistance.
Author Contributions
Conceptualization, L.S., M.M., E.U. and V.Ö.; formal analysis, S.T. and V.Ö; investigation, L.S., S.T., M.M., E.M., L.M., M.L., K.T., A.P., M.Z. and E.U.; methodology, L.S.; M.M., S.T. and V.Ö.; supervision, M.Z., E.U., and V.Ö.; visualization, S.T.; writing-original draft, L.S., S.T. and V.Ö.; writing-review and editing, M.M., M.Z. and E.U. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by Estonian Ministry of Education and Research (institutional research funding IUT 20-58 and PRG 435), by the Institute of Sport Sciences and Physiotherapy of the University of Tartu (baseline research funding), and Institute of Clinical Medicine of the University of Tartu (baseline research funding).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Research Ethics Committee of the University of Tartu (protocol no. 278/M-12; 19.02.2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author (vahur.oopik@ut.ee).
Acknowledgments
The authors thank the participants for their time and cooperation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bendik, I.; Friedel, A.; Roos, F.F.; Weber, P.; Eggersdorfer, M. Vitamin D: a critical and essential micronutrient for human health. Front. Physiol. 2014, 5, 248. [CrossRef]
- Starck, C.S.; Cassettari, T.; Beckett, E.; Marshall, S.; Fayet-Moore, F. Priority nutrients to address malnutrition and diet-related diseases in Australia and New Zealand. Front. Nutr. 2024, 11, 1370550. [CrossRef]
- Holick, M.F. Vitamin D and bone health: What vitamin D can and cannot do. Adv. Food Nutr. Res. 2024, 109, 43–66. [CrossRef]
- Shoemaker, M.E.; Salmon, O.F.; Smith, C.M.; Duarte-Gardea, M.O.; Cramer, J.T. Influences of vitamin D and iron status on skeletal muscle health: A narrative review. Nutrients 2022, 14, 2717. [CrossRef]
- DeLuca, H.F. Overview of general physiologic features and functions of vitamin D. Am. J. Clin. Nutr. 2004, 80, 1689S–1696S. [CrossRef]
- Bikle, D.D. Vitamin D metabolism, mechanism of action, and clinical applications. Chem. Biol. 2014, 21, 319–329. [CrossRef]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, molecular mechanism of action, and pleiotropic effects. Physiol. Rev. 2016, 96, 365–408. [CrossRef]
- Zittermann, A. Vitamin D in preventive medicine: Are we ignoring the evidence? Br. J. Nutr. 2003, 89, 552–572. [CrossRef]
- Holick, M.F. Medical progress: Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281.
- Norman, A.W. From vitamin D to hormone D: Fundamentals of the vitamin D endocrine system essential for good health. Am. J. Clin. Nutr. 2008, 88, 491S–499S. [CrossRef]
- Girgis, C.M. Vitamin D and skeletal muscle: Emerging roles in development, anabolism and repair. Calcif. Tissue Int. 2020, 106, 47–57. [CrossRef]
- Pojednic, R.M.; Ceglia, L. The emerging biomolecular role of vitamin D in skeletal muscle. Exerc. Sport Sci. Rev. 2014, 42, 76–81. [CrossRef]
- Romeu Montenegro, K.; Carlessi, R.; Cruzat, V.; Newsholme, P. Effects of vitamin D on primary human skeletal muscle cell proliferation, differentiation, protein synthesis and bioenergetics. J. Steroid Biochem. Mol. Biol. 2019, 193, 105423. [CrossRef]
- Ceglia, L.; Niramitmahapanya, S.; da Silva Morais, M.; Rivas, D.A.; Harris, S.S.; Bischoff-Ferrari, H.; Fielding, R.A.; Dawson-Hughes, B. A randomized study on the effect of vitamin D3 supplementation on skeletal muscle morphology and vitamin D receptor concentration in older women. J. Clin. Endocrinol. Metab. 2013, 98, E1927–E1935. [CrossRef]
- Prado, C.M.; Landi, F.; Chew, S.T.H.; Atherton, P.J.; Molinger, J.; Ruck, T.; Gonzalez, M.C. Advances in muscle health and nutrition: A toolkit for healthcare professionals. Clin. Nutr. 2022, 41, 2244–2263. [CrossRef]
- Tomlinson, P.B.; Joseph, C.; Angioi, M. Effects of vitamin D supplementation on upper and lower body muscle strength levels in healthy individuals. A systematic review with meta-analysis. J. Sci. Med. Sport 2015, 18, 575–580. [CrossRef]
- Han, Q.; Li, X.; Tan, Q.; Shao, J.; Yi, M. Effects of vitamin D3 supplementation on serum 25(OH)D concentration and strength in athletes: A systematic review and meta-analysis of randomized controlled trials. J. Int. Soc. Sports Nutr. 2019, 16, 55. [CrossRef]
- Zhang, L.; Quan, M.; Cao, Z.-B. Effect of vitamin D supplementation on upper and lower limb muscle strength and muscle power in athletes: A meta-analysis. PLoS ONE 2019, 14, e0215826. [CrossRef]
- Chiang, C.M.; Ismaeel, A.; Griffis, R.B.; Weems, S. J. Effects of vitamin D supplementation on muscle strength in athletes: A systematic review. J. Strength Cond. Res. 2017, 31, 566–574. [CrossRef]
- Abshirini, M.; Mozaffari, H.; Kord-Varkaneh, H.; Omidian, M.; Kruger M.C. The effects of vitamin D supplementation on muscle strength and mobility in postmenopausal women: a systematic review and meta-analysis of randomised controlled trials. J. Hum. Nutr. Diet. 2020, 33, 207–221. [CrossRef]
- Muir, S.W.; Montero-Odasso, M. Effect of vitamin D supplementation on muscle strength, gait and balance in older adults: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2011, 59, 2291–2300. [CrossRef]
- McKendry, J.; Currier, B.S.; Lim, C.; Mcleod, J.C.; Thomas, A.C.Q.; Phillips, S.M. Nutritional supplements to support resistance exercise in countering the sarcopenia of aging. Nutrients 2020, 12, 2057. [CrossRef]
- Phillips, S.M. Nutritional supplements in support of resistance exercise to counter age-related sarcopenia. Adv. Nutr. 2015, 6, 452–460. [CrossRef]
- Westcott, W.L. Resistance training is medicine: effects of strength training on health. Curr. Sports Med. Rep. 2012, 11, 209–216. [CrossRef]
- Antoniak, A.E.; Greig, C.A. The effect of combined resistance exercise training and vitamin D3 supplementation on musculoskeletal health and function in older adults: A systematic review and meta-analysis. BMJ Open 2017, 7, e014619. [CrossRef]
- Mølmen, K.S.; Hammarström, D.; Pedersen, K.; Lian Lie, A.C.; Steile, R.B.; Nygaard, H.; Khan, Y.; Hamarsland, H.; Koll, L.; Hanestadhaugen, M.; et al. Vitamin D3 supplementation does not enhance the effects of resistance training in older adults. J. Cachexia Sarcopenia Muscle 2021, 12, 599–628. [CrossRef]
- Heyward, V.H. Advanced Fitness Assessment and Exercise Prescription, 6th ed.; Human Kinetics: Champaign, IL, USA, 2010; pp. 65–101.
- Raghuveer, G.; Hartz, J.; Lubans, D.R.; Takken, T.; Wiltz, J.L.; Mietus-Snyder, M.; Perak, A.M.; Baker-Smith, C.; Pietris, N.; Edwards, N.M.; et al. Cardiorespiratory fitness in youth ‒ an important marker of health: A scientific statement from the American Heart Association. Circulation 2020, 142, e101‒e118. [CrossRef]
- Kenney, W.L.; Wilmore, J.H.; Costill, D.L. Physiology of Sport and Exercise, 6th ed.; Human Kinetics: Champaign, IL, USA, 2015; pp. 262–284.
- Lim, K.; Molostvov, G.; Lubczanska, M.; Fletcher, S.; Bland, R.; Hiemstra, T.F.; Zehnder, D. Impaired arterial vitamin D signaling occurs in the development of vascular calcification. PLoS ONE 2020, 15, e0241976. [CrossRef]
- Menezes, R.J.; Cheney, R.T.; Husain, A.; Tretiakova, M.; Loewen, G.; Johnson, C.S.; Jayaprakash, V.; Moysich, K.B.; Salgia, R.; Reid, M.E. Vitamin D receptor expression in normal, premalignant, and malignant human lung tissue. Cancer Epidemiol. Biomarkers Prev. 2008, 17, 1104–1110. [CrossRef]
- O’Connell, T.D.; Simpson, R.U. Immunochemical identification of the 1,25-dihydroxyvitamin D3 receptor protein in human heart. Cell Biol. Int. 1996, 20, 621–624. [CrossRef]
- Smith, E.M.; Tangpricha, V. Vitamin D and anemia: Insights into an emerging association. Curr. Opin. Endocrinol. Diabetes Obes. 2015, 22, 432–438. [CrossRef]
- Dahlquist, D.T.; Dieter, B.P.; Koehle, M.S. Plausible ergogenic effects of vitamin D on athletic performance and recovery. J. Int. Soc. Sports Nutr. 2015, 12, 33. [CrossRef]
- Latham, C.M.; Brightwell, C.R.; Keeble, A.R.; Munson, B.D.; Thomas, N.T.; Zagzoog, A.M.; Fry, C.S.; Fry, J.L. Vitamin D promotes skeletal muscle regeneration and mitochondrial health. Front. Physiol. 2021, 12, 660498. [CrossRef]
- Ardestani, A.; Parker, B.; Mathur, S.; Clarkson, P.; Pescatello, L.S.; Hoffman, H.J.; Polk, D.M.; Thompson, P.D. Relation of vitamin D level to maximal oxygen uptake in adults. Am. J. Cardiol. 2011, 107, 1246–1249. [CrossRef]
- Marawan, A.; Kurbanova, N.; Qayyum, R. Association between serum vitamin D levels and cardiorespiratory fitness in the adult population of the USA. Eur. J. Prev. Cardiol. 2019, 26, 750–755. [CrossRef]
- Wyatt, P.B.; Reiter, C.R.; Satalich, J.R.; O’Neill, C.N.; Edge, C.; Cyrus, J.W.; O’Connell, R.S.; Vap, A.R. Effects of vitamin D supplementation in elite athletes: A systematic review. Orthop. J. Sports Med. 2024, 12, 23259671231220371. [CrossRef]
- Kujach, S.; Lyzwinski, D.; Chroboczek, M.; Bialowas, D.; Antosiewicz, J.; Laskowski, R. The effect of vitamin D3 supplementation on physical capacity among active college-aged males. Nutrients 2020, 12, 1936. [CrossRef]
- Todd, J.J.; McSorley, E.M.; Pourshahidi, L.K.; Madigan, S.M.; Laird, E.; Healy, M.; Magee, P.J. Vitamin D3 supplementation using an oral spray solution resolves deficiency but has no effect on VO2max in Gaelic footballers: Results from a randomised, double-blind, placebo-controlled trial. Eur. J. Nutr. 2017, 56, 1577–1587. [CrossRef]
- Brzeziański, M.; Migdalska-Sęk, M.; Czechowska, A.; Radzimiński, Ł.; Jastrzębski, Z.; Brzeziańska-Lasota, E.; Sewerynek, E. Correlation between the positive effect of vitamin D supplementation and physical performance in young male soccer players. Int. J. Environ. Res. Public Health 2022, 19, 5138. [CrossRef]
- Jastrzębska, M.; Kaczmarczyk, M.; Michalczyk, M.; Radzimiński, Ł.; Stępień, P.; Jastrzębska, J.; Wakuluk, D.; Suárez, A.D; López Sánchez, G.F; Cięszczyk, P.; et al. Can supplementation of vitamin D improve aerobic capacity in well trained youth soccer players? J. Hum. Kinet. 2018, 61, 63–72. [CrossRef]
- Ramezani Ahmadi, A.; Mohammadshahi, M.; Alizadeh, A.; Ahmadi Angali, K.; Jahanshahi, A. Effects of vitamin D3 supplementation for 12 weeks on serum levels of anabolic hormones, anaerobic power, and aerobic performance in active male subjects: A randomized, double-blind, placebo-controlled trial. Eur. J. Sport Sci. 2020, 20, 1355–1367. [CrossRef]
- Hornikx, M.; Van Remoortel, H.; Lehouck, A.; Mathieu, C.; Maes, K.; Gayan-Ramirez, G.; Decramer, M.; Troosters, T.; Janssens, W. Vitamin D supplementation during rehabilitation in COPD: A secondary analysis of a randomized trial. Respir. Res. 2012, 13, 84. [CrossRef]
- Cruz-Jentoft, A.J.; Dawson Hughes, B.; Scott, D.; Sanders, K.M.; Rizzoli, R. Nutritional strategies for maintaining muscle mass and strength from middle age to later life: A narrative review. Maturitas 2020, 132, 57–64. [CrossRef]
- Hawkins, S.; Wiswell, R. Rate and mechanism of maximal oxygen consumption decline with aging: implications for exercise training. Sports Med. 2003, 33, 877–888. [CrossRef]
- Kull, M.; Kallikorm, R.; Tamm, A.; Lember, M. Seasonal variance of 25(OH)D in the general population of Estonia, a Northern European country. BMC Public Health 2009, 9, 22. [CrossRef]
- Ööpik, V.; Timpmann, S.; Rips, L.; Olveti, I.; Kõiv, K.; Mooses, M.; Mölder, M.H.; Varblane, M.A.; Lille, H.-R.; Gapeyeva, H. Anabolic adaptations occur in conscripts during basic military training despite high prevalence of vitamin D deficiency and decrease in iron status. Mil. Med. 2017, 182, e1810. [CrossRef]
- Hulmi, J.J.; Laakso, M.; Mero, A.A.; Häkkinen, K.; Ahtiainen, J.P.; Peltonen, H. The effects of whey protein with or without carbohydrates on resistance training adaptations. J. Int. Soc. Sports Nutr. 2015, 12, 48. [CrossRef]
- Pludowski, P.; Takacs, I.; Boyanov, M.; Belaya, Z.; Diaconu, C.C.; Mokhort, T.; Zherdova, N.; Rasa, I.; Payer, J.; Pilz, S. Clinical practice in the prevention, diagnosis and treatment of vitamin D deficiency: A central and eastern European expert consensus statement. Nutrients 2022, 14, 1483. [CrossRef]
- Heaney, R.P. Assessing vitamin D status. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 440–444. [CrossRef]
- Levinger, I.; Goodman, C.; Hare, D.L.; Jerums, G.; Toia, D.; Selig, S. The reliability of the 1RM strength test for untrained middle-aged individuals. J. Sci. Med. Sport 2009, 12, 310–316. [CrossRef]
- Agergaard, J.; Trøstrup, J.; Uth, J.; Iversen, J.V.; Boesen, A.; Andersen, J.L.; Schjerling, P.; Langberg, H. Does vitamin D intake during resistance training improve the skeletal muscle hypertrophic and strength response in young and elderly men? - A randomized controlled trial. Nutr. Metab. (London) 2015, 12, 32. [CrossRef]
- Baechle, T.R.; Earle, R.W. Essentials of Strength Training and Conditioning. National Strength & Conditioning Association (US), 3rd ed.; Human Kinetics; Champaign, IL, USA, 2008.
- Savolainen, L.; Timpmann, S.; Mooses, M.; Mäestu, E.; Medijainen, L.; Tõnutare, L.; Ross, F.; Lellsaar, M.; Unt, E.; Ööpik, V. Vitamin D supplementation does not enhance resistance training-induced gains in muscle strength and lean body mass in vitamin D deficient young men. Eur. J. Appl. Physiol. 2021, 121, 2077–2090. [CrossRef]
- Moore, D.R.; Robinson, M.J.; Fry, J.L.; Tang, J.E.; Glover, E.I.; Wilkinson, S.B.; Prior, T.; Tarnopolsky, M.A.; Phillips, S.M. Ingested protein dose response of muscle and albumin protein synthesis after resistance exercise in young men. Am. J. Clin. Nutr. 2009, 89, 161–168. [CrossRef]
- Yang, Y.; Breen, L.; Burd, N.A.; Hector, A.J.; Churchward-Venne, T.A.; Josse, A.R.; Tarnopolsky, M.A.; Phillips, S.M. Resistance exercise enhances myofibrillar protein synthesis with graded intakes of whey protein in older men. Br. J. Nutr. 2012, 108, 1780–1788. [CrossRef]
- Damas, F.; Phillips, S.M.; Libardi, C.A.; Vechin, F.C.; Lixandrão, M.E.; Jannig, P.R.; Costa, L.A.R.; Bacurau, A.V.; Snijders, T.; Parise, G.; et al. Resistance training-induced changes in integrated myofibrillar protein synthesis are related to hypertrophy only after attenuation of muscle damage. J. Physiol. 2016, 594, 5209–5222. [CrossRef]
- Davis, J.A. Direct determination of aerobic power. In Physiological Assessment of Human Fitness, 2nd ed.; Maud, P.J., Foster, C., Eds.; Human Kinetics: Champaign, IL, USA, 2006; pp. 9–18.
- Vogeser, M.; König, D.; Frey, I.; Predel, H.G.; Parhofer, K.G.; Berg, A. Fasting serum insulin and the homeostasis model of insulin resistance (HOMA-IR) in the monitoring of lifestyle interventions in obese persons. Clin. Biochem. 2007, 40, 964–968. [CrossRef]
- Bemben, M.G.; Witten, M.S.; Carter, J.M.; Eliot, K.A.; Knehans, A.W.; Bemben, D.A. The effects of supplementation with creatine and protein on muscle strength following a traditional resistance training program in middle-aged and older men. J. Nutr. Health Aging 2010, 14, 155–159. 10.1007/s12603-009-0124-8.
- Borde, R.; Hortobágyi, T.; Granacher, U. Dose-response relationships of resistance training in healthy old adults: A systematic review and meta-analysis. Sports Med. 2015, 45, 1693–1720. [CrossRef]
- Buch, A.; Kis, O.; Carmeli, E.; Keinan-Boker, L.; Berner, Y.; Barer, Y.; Shefer, G.; Marcus, Y.; Stern, N. Circuit resistance training is an effective means to enhance muscle strength in older and middle aged adults: A systematic review and meta-analysis. Ageing Res. Rev. 2017, 37, 16–27. [CrossRef]
- Bunout, D.; Barrera, G.; Leiva, L.; Gattas, V.; de la Maza, M.P.; Avendaño, M.; Hirsch, S. Effects of vitamin D supplementation and exercise training on physical performance in Chilean vitamin D deficient elderly subjects. Exp. Gerontol. 2006, 41, 746–752. [CrossRef]
- Uusi-Rasi, K.; Patil, R.; Karinkanta, S.; Kannus, P.; Tokola, K.; Lamberg-Allardt, C.; Sievänen, H. Exercise and vitamin D in fall prevention among older women: A randomized clinical trial. JAMA Intern. Med. 2015, 175, 703–711. [CrossRef]
- Häkkinen, K.; Pakarinen, A. Serum hormones and strength development during strength training in middle-aged and elderly males and females. Acta Physiol. Scand. 1994, 150, 211–219. [CrossRef]
- Kvorning, T.; Andersen, M.; Brixen, K.; Madsen, K. Suppression of endogenous testosterone production attenuates the response to strength training: A randomized, placebo-controlled, and blinded intervention study. Am. J. Physiol. Endocrinol. Metab. 2006, 291, E1325–E1332. [CrossRef]
- Canguven, O.; Talib, R.A.; El Ansari, W.; Yassin, D.J.; Al Naimi, A. Vitamin D treatment improves levels of sexual hormones, metabolic parameters and erectile function in middle-aged vitamin D deficient men. Aging Male 2017, 20, 9–16. [CrossRef]
- Pilz, S.; Frisch, S.; Koertke, H.; Kuhn, J.; Dreier, J.; Obermayer-Pietsch, B.; Wehr, E.; Zittermann, A. Effect of vitamin D supplementation on testosterone levels in men. Horm. Metab. Res. 2011, 43, 223–225. [CrossRef]
- Jacobs, R.A.; Rasmussen, P.; Siebenmann, C.; Díaz, V.; Gassmann, M.; Pesta, D.; Gnaiger, E.; Nordsborg, N.B.; Robach, P.; Lundby, C. Determinants of time trial performance and maximal incremental exercise in highly trained endurance athletes. J. Appl. Physiol. 2011, 111, 1422–1430. [CrossRef]
- Groennebaek, T.; Jespersen, N.R.; Jakobsgaard, J.E.; Sieljacks, P.; Wang, J.; Rindom, E.; Musci, R.V.; Bøtker, H.E.; Hamilton, K.L.; Miller, B.F.; et al. Skeletal muscle mitochondrial protein synthesis and respiration increase with low-load blood flow restricted as well as high-load resistance training. Front. Physiol. 2018, 9, 1796. [CrossRef]
- Mesquita, P.H.C.; Lamb, D.A.; Parry, H.A.; Moore, J.H.; Smith, M.A.; Vann, C.G.; Osburn, S.C.; Fox, C.D.; Ruple, B.A.; Huggins, K.W.; et al. Acute and chronic effects of resistance training on skeletal muscle markers of mitochondrial remodeling in older adults. Physiol. Rep. 2020, 8, e14526. [CrossRef]
- Ruple, B.A.; Godwin, J.S.; Mesquita, P.H.C.; Osburn, S.C.; Vann, C.G.; Lamb, D.A.; Sexton, C.L.; Candow, D.G.; Forbes, S.C.; Frugé, A.D.; et al. Resistance training rejuvenates the mitochondrial methylome in aged human skeletal muscle. FASEB J. 2021, 35, e21864. [CrossRef]
- Werner, C.M.; Hecksteden, A.; Morsch, A.; Zundler, J.; Wegmann, M.; Kratzsch, J.; Thiery, J.; Hohl, M.; Bittenbring, J.T.; Neumann. F.; et al. Differential effects of endurance, interval, and resistance training on telomerase activity and telomere length in a randomized, controlled study. Eur. Heart J. 2019, 40, 34–46. [CrossRef]
- Waters, D.L.; Aguirre, L.; Gurney, B.; Sinacore, D.R.; Fowler, K.; Gregori, G.; Armamento-Villareal, R.; Qualls, C.; Villareal, D.T. Effect of aerobic or resistance exercise, or both, on intermuscular and visceral fat and physical and metabolic function in older adults with obesity while dieting. J. Gerontol. A Biol. Sci. Med. Sci. 2022, 77, 131–139. [CrossRef]
- An, J.; Su, Z.; Meng S. Effect of aerobic training versus resistance training for improving cardiorespiratory fitness and body composition in middle-aged to older adults: A systematic review and meta-analysis of randomized controlled trials. Arch. Gerontol. Geriatr. 2024, 126, 105530. [CrossRef]
- Peeling, P.; Blee, T.; Goodman, C.; Dawson, B.; Claydon, G.; Beilby, J.; Prins, A. Effect of iron injections on aerobic-exercise performance of iron-depleted female athletes. Int. J. Sport Nutr. Exerc. Metab. 2007, 17, 221–231. [CrossRef]
- Savolainen, L.; Timpmann, S.; Mooses, M.; Medijainen, L.; Tõnutare, L.; Ross, F.; Lellsaar, M.; Piir, A.; Zilmer, M.; Unt, E.; Ööpik, V. Vitamin D supplementation has no impact on cardiorespiratory fitness, but improves inflammatory status in vitamin D deficient young men engaged in resistance training. Nutrients 2022, 14, 5302. [CrossRef]
- Shoemaker, J.K.; Green, H.J.; Coates, J.; Ali, M.; Grant, S. Failure of prolonged exercise training to increase red cell mass in humans. Am. J. Physiol. 1996, 270, H121–126. [CrossRef]
- My, G.; Marsigliante, S.; Bianco, A.; Zangla, D.; Silva, C.M.D.; Muscella, A. Biological, psychological, and physical performance variations in football players during the COVID-19 lockdown: A prospective cohort study. Int. J. Environ. Res. Public Health 2022, 19, 2739. [CrossRef]
- Timpmann, S.; Rips, L.; Olveti, I.; Mooses, M.; Mölder, H.; Varblane, A.; Lille, H.-R.; Gapeyeva, H.; Ööpik, V. Seasonal variation in vitamin D status does not interfere with improvements in aerobic and muscular endurance in conscripts during basic military training. Nutrients 2024, 16, 1306. [CrossRef]
- Cannell, J.J.; Grant, W.B.; Holick, M.F. Vitamin D and inflammation. Dermatoendocrinol. 2014, 6, e983401. [CrossRef]
- Colotta, F.; Jansson, B.; Bonelli, F. Modulation of inflammatory and immune responses by vitamin D. J. Autoimmun. 2017, 85, 78–97. [CrossRef]
- Silva, B.S.A.; Lira, F.S.; Rossi, F.E.; Ramos, D.; Uzeloto, J.S.; Freire, A.P.C.F.; de Lima, F.F.; Gobbo, L.A.; Ramos, E.M.C. Inflammatory and metabolic responses to different resistance training on chronic obstructive pulmonary disease: A randomized control trial. Front. Physiol. 2018, 9, 262. [CrossRef]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [CrossRef]
- Trimarco, V.; Manzi, M.V.; Mancusi, C.; Strisciuglio, T.; Fucile, I.; Fiordelisi, A.; Pilato, E.; Izzo, R.; Barbato, E.; Lembo, M.; et al. Insulin resistance and vitamin D deficiency: A link beyond the appearances. Front. Cardiovasc. Med. 2022, 9, 859793. [CrossRef]
- Belenchia, A.M.; Tosh, A.K.; Hillman, L.S.; Peterson, C.A. Correcting vitamin D insufficiency improves insulin sensitivity in obese adolescents: A randomized controlled trial. Am. J. Clin. Nutr. 2013, 97, 774–781. [CrossRef]
- Nikseresht, M. Comparison of serum cytokine levels in men who are obese or men who are lean: Effects of nonlinear periodized resistance training and obesity. J. Strength Cond. Res. 2018, 32, 17871795. [CrossRef]
- Carrillo, A.E.; Flynn, M.G.; Pinkston, C.; Markofski, M.M.; Jiang, Y.; Donkin, S.S.; Teegarden, D. Impact of vitamin D supplementation during a resistance training intervention on body composition, muscle function, and glucose tolerance in overweight and obese adults. Clin. Nutr. 2013, 32, 375–381. [CrossRef]
- Miller, E.G.; Nowson, C.A.; Dunstan, D.W.; Kerr, D.A.; Menzies, D.; Daly, R.M. Effects of whey protein plus vitamin D supplementation combined with progressive resistance training on glycaemic control, body composition, muscle function and cardiometabolic risk factors in middle-aged and older overweight/obese adults with type 2 diabetes: A 24-week randomized controlled trial. Diabetes Obes. Metab. 2021, 23, 938–949. [CrossRef]
- EFSA NDA Panel; Turck, D.; Bohn, T.; Castenmiller, J.; De Henauw, S.; Hirsch-Ernst, K.-I.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; Pentieva, K.; et al. Scientific opinion on the tolerable upper intake level for vitamin D, including the derivation of a conversion factor for calcidiol monohydrate. EFSA J. 2023, 21, 1–219. [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [CrossRef]
- Bouillon, R. Comparative analysis of nutritional guidelines for vitamin D. Nat. Rev. Endocrinol. 2017, 13, 466–479. [CrossRef]
- Heaney, R.P.; Davies, K.M.; Chen, T.C.; Holick, M.F.; Barger-Lux, M.J. Human serum 25-hydroxycholecalciferol response to extended oral dosing with cholecalciferol. Am. J. Clin. Nutr. 2003, 77, 204–210. [CrossRef]
- Janoušek, J.; Pilařová, V.; Macáková, K.; Nomura, A.; Veiga-Matos, J.; Silva D.D.D.; Remião, F.; Saso, L.; Malá-Ládová, K.; Malý, J.; et al. Vitamin D: sources, physiological role, biokinetics, deficiency, therapeutic use, toxicity, and overview of analytical methods for detection of vitamin D and its metabolites. Crit. Rev. Clin. Lab. Sci. 2022, 59, 517–554. [CrossRef]
- Pilz, S.; Zittermann, A.; Trummer, C.; Theiler-Schwetz, V.; Lerchbaum, E.; Keppel, M.H.; Grübler, M.R.; März,W.; Pandis, M. Vitamin D testing and treatment: a narrative review of current evidence. Endocr. Connect. 2019, 8, R27–R43. [CrossRef]
- Stojanovic, O.I.; Lazovic, M.; Lazovic, M.; Vuceljic, M. Association between atherosclerosis and osteoporosis, the role of vitamin D. Arch. Med. Sci. 2011, 7, 179–188. [CrossRef]
- Mirhosseini, N.; Rainsbury, J.; Kimball, S.M. Vitamin D supplementation, serum 25(OH)D concentrations and cardiovascular disease risk factors: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2018, 5, 87. [CrossRef]
- Viru, A.; Viru, M. Biochemical Monitoring of Sport Training; Human Kinetics: Champaign, IL, USA, 2001.
Figure 1.
Study design. Arrows indicate time points for measuring body mass (BM), body composition (DXA), and maximal oxygen uptake (VO2max), venous blood sampling (Blood), and beginning (PLC/VD+) and end (PLC/VD‒) of placebo or vitamin D supplementation. Grey and striped cells indicate the weeks during which muscle strength was assessed and 4-day food diaries were filled, respectively.
Figure 1.
Study design. Arrows indicate time points for measuring body mass (BM), body composition (DXA), and maximal oxygen uptake (VO2max), venous blood sampling (Blood), and beginning (PLC/VD+) and end (PLC/VD‒) of placebo or vitamin D supplementation. Grey and striped cells indicate the weeks during which muscle strength was assessed and 4-day food diaries were filled, respectively.
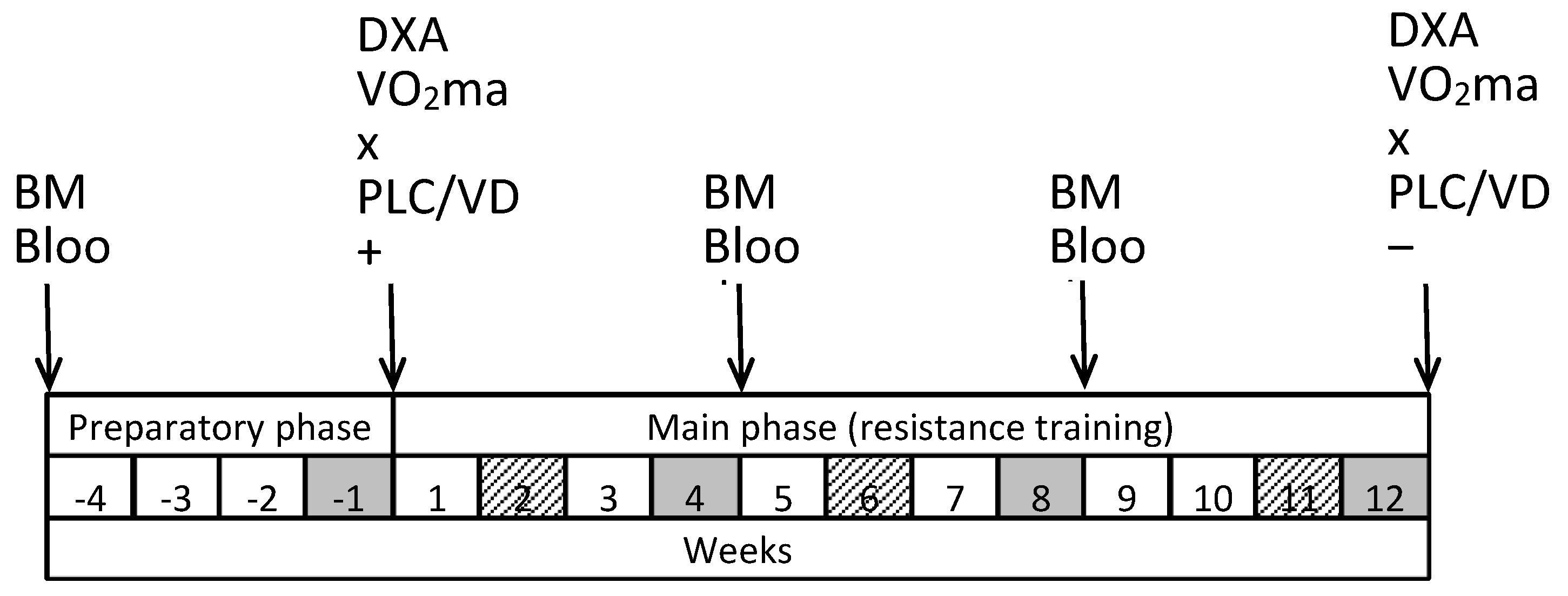
Figure 2.
Serum 25(OH)D concentrations. Data are presented as mean ± SD; n = 14 in placebo and n = 14 in vitamin D group. Significantly different (p < 0.05): * from Week ‒4; # from previous week; $ from placebo group.
Figure 2.
Serum 25(OH)D concentrations. Data are presented as mean ± SD; n = 14 in placebo and n = 14 in vitamin D group. Significantly different (p < 0.05): * from Week ‒4; # from previous week; $ from placebo group.
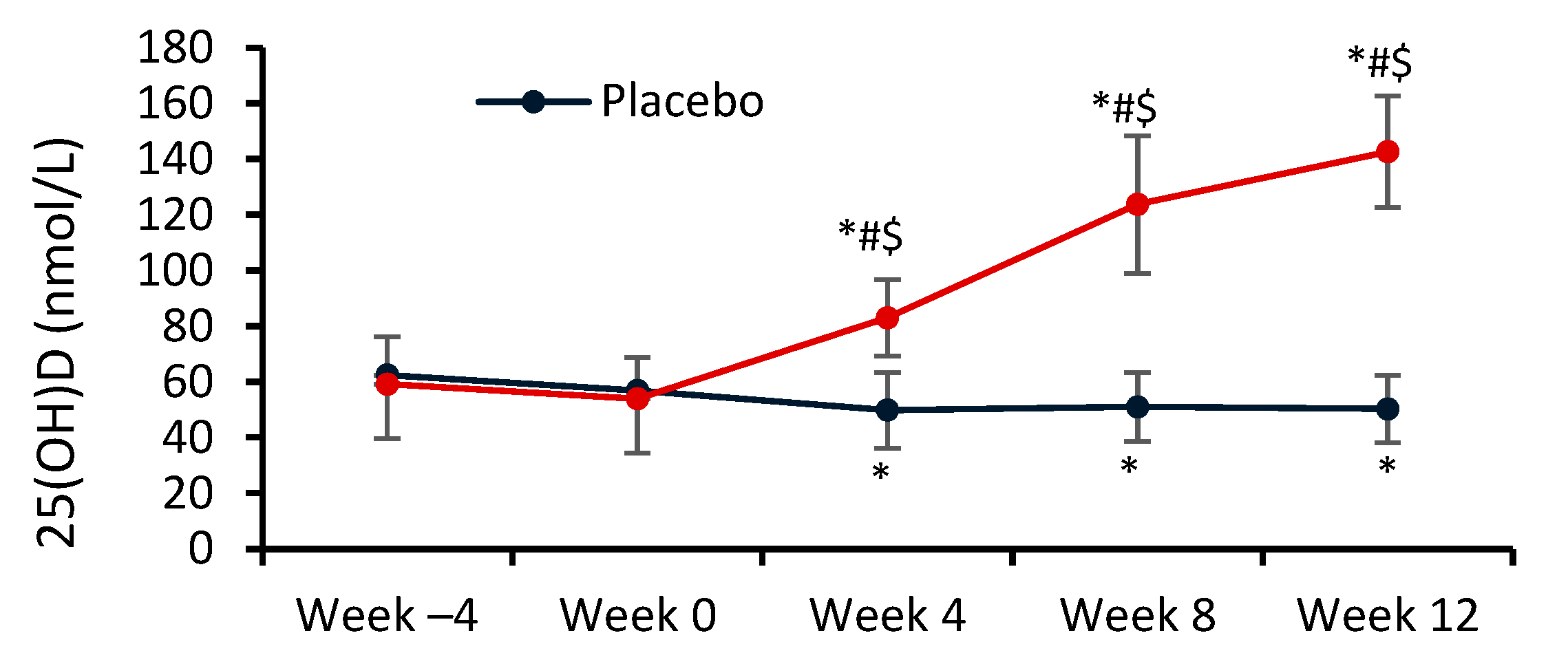
Figure 3.
Changes in 1-repetition maximum during 12-week supplementation and resistance training period. Data are presented as mean ± SD, n = 14 in placebo and n = 14 in vitamin D group.
Figure 3.
Changes in 1-repetition maximum during 12-week supplementation and resistance training period. Data are presented as mean ± SD, n = 14 in placebo and n = 14 in vitamin D group.
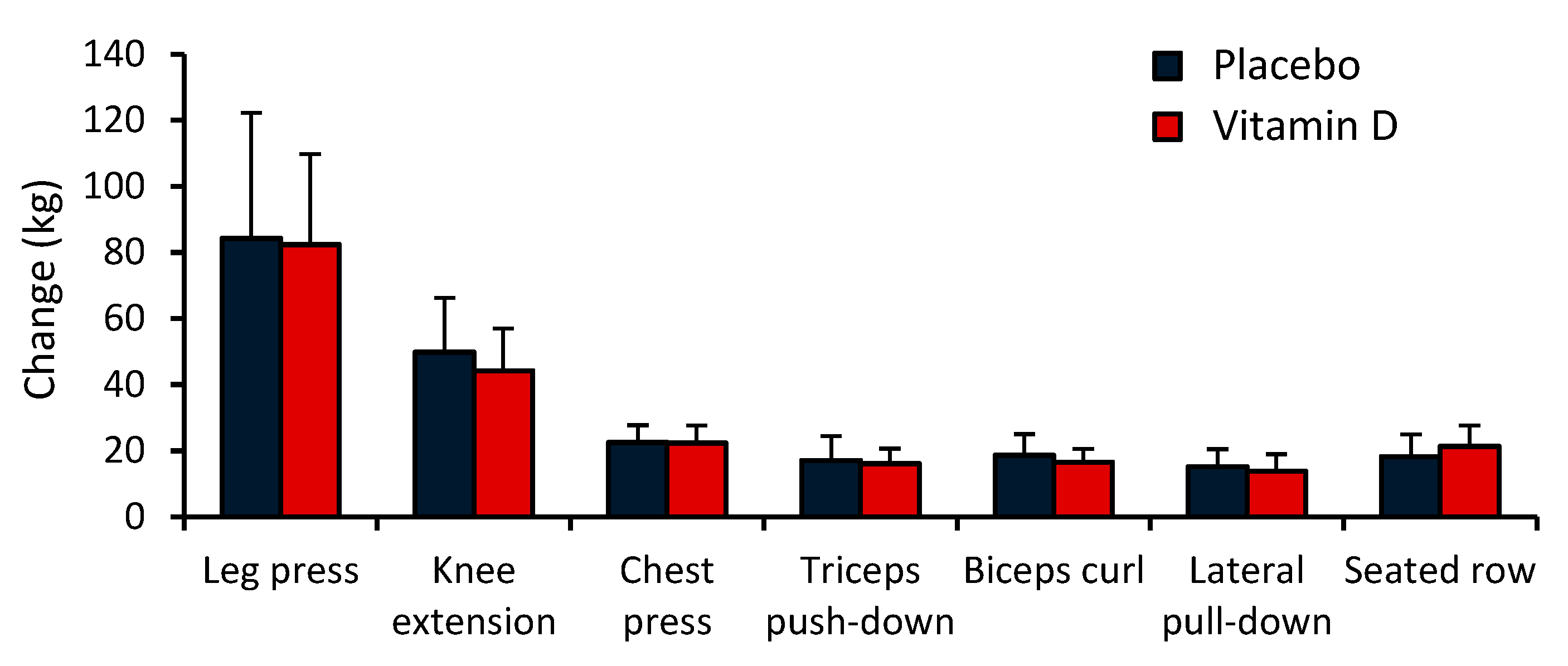
Table 2.
Distribution of training loads during the preparatory and main phase of the study.
| Phase | Week | SPW | Sets | Reps | Training loads (weight used) |
| Preparatory | ‒4 | 2 | 2 | 15‒20 | Chosen by supervisor |
| ‒3 | |||||
| ‒2 | 3 | 3 | 12‒15 | ||
| ‒1 | 3 | 1 | 12‒15 | ||
| Main | 1 | 3 | 3 | 12‒15 | 60%‒75% of the 1RM measured at week ‒1 |
| 2 | |||||
| 3 | |||||
| 4 | 3 | 1 | 12‒15 | ||
| 5 | 3 | 3 | 8‒12 | 60%‒75% of the 1RM measured at week 4 | |
| 6 | |||||
| 7 | 75%‒85% of the 1RM measured at week 4 | ||||
| 8 | 3 | 1 | 8‒12 | ||
| 9 | 3 | 3 | 8‒12 | 75%‒85% of the 1RM measured at week 8 | |
| 10 | |||||
| 11 | |||||
| 12 | 3 | 1 | 8‒12 |
1RM test weeks are presented in bold; 1RM, 1-repetition maximum; SPW, number of training sessions per week; Sets, number of sets of each exercise performed during each training session; Reps, number of repetitions per one set of each exercise.
Table 3.
Daily energy and nutrient intake.
| Variable | Group | Week 2 | Week 6 |
|---|---|---|---|
| Energy intake (kcal) | PLC | 2309 ± 259 | 2241 ± 431 |
| VD | 1953 ± 533 | 1942 ± 412 | |
| Protein (%) | PLC | 17.6 ± 2.7 | 15.9 ± 1.7 |
| VD | 16.9 ± 2.2 | 16.2 ± 2.5 | |
| Protein (g/kg) * | PLC | 1.15 ± 0.26 | 1.03 ± 0.34 |
| VD | 1.05 ± 0.41 | 0.98 ± 0.31 | |
| Fat (%) | PLC | 37.6 ± 3.3 | 39.5 ± 6.7 |
| VD | 38.3 ± 7.0 | 37.7 ± 4.2 | |
| Fat (g/kg) | PLC | 1.10 ± 0.21 | 1.10 ± 0.24 |
| VD | 1.04 ± 0.36 | 1.06 ± 0.44 | |
| Carbohydrates (%) | PLC | 41.7 ± 6.5 | 42.0 ± 6.7 |
| VD | 43.1 ± 8.3 | 43.9 ± 4.2 | |
| Carbohydrates (g/kg) | PLC | 2.81 ± 0.91 | 2.75 ± 0.97 |
| VD | 2.73 ± 1.10 | 2.70 ± 0.86 | |
| Vitamin D (μg) ** | PLC | 5.45 ± 3.74 | 4.27 ± 2.15 |
| VD | 9.28 ± 5.65 | 6.28 ± 3.89 | |
| Calcium (mg) | PLC | 908 ± 309 | 933 ± 330 |
| VD | 744 ± 316 | 643 ± 222 |
Data are presented as mean ± SD. n = 6 in PLC (placebo) and n = 6 in VD (vitamin D) group. * The amounts of protein in the table do not include 40 g of whey which was consumed only on the training days after each workout. ** For both groups, the table only shows the amounts of vitamin D that the subjects consumed with daily food and not in the form of a dietary supplement.
Table 4.
One-repetition maximum (1RM) strength (kg) during 12-week supplementation and resistance training period.
Table 4.
One-repetition maximum (1RM) strength (kg) during 12-week supplementation and resistance training period.
| Variable | Group | Week 0 | Week 4 | Week 8 | Week 12 |
|---|---|---|---|---|---|
| Leg press | PLC | 192.9 ± 33.0 | 228.5 ± 31.7 * | 249.5 ± 35.9 *# | 277.2 ± 45.6 *# |
| VD | 198.7 ± 45.1 | 231.6 ± 42.0 * | 249.4 ± 40.8 * | 281.1 ± 48.5 *# | |
| Knee extension | PLC | 59.6 ± 20.4 | 77.7 ± 24.1 * | 92.9 ± 25.3 *# | 109.5 ± 19.2 *# |
| VD | 63.9 ± 23.1 | 79.9 ± 26.0 * | 94.4 ± 24.1 *# | 108.1 ± 24.6 *# | |
| Chest press | PLC | 57.8 ± 12.8 | 66.0 ± 12.7 * | 72.3 ± 13.4 *# | 80.3 ± 13.9 *# |
| VD | 62.3 ± 15.2 | 69.4 ± 14.9 * | 76.6 ± 16.0 *# | 84.5 ± 17.3 *# | |
| Triceps push-down | PLC | 64.6 ± 10.0 | 70.5 ± 10.1 * | 75.8 ± 10.4 *# | 81.7 ± 10.4 *# |
| VD | 69.1 ± 10.8 | 75.5 ± 10.7 * | 80.2 ± 11.3 *# | 85.1 ± 12.5 *# | |
| Biceps curl | PLC | 52.3 ± 9.1 | 60.8 ± 10.4 * | 66.0 ± 11.5 *# | 70.9 ± 12.1 *# |
| VD | 53.7 ± 10.6 | 59.9 ± 10.6 * | 64.9 ± 10.5 *# | 70.2 ± 10.8 *# | |
| Lateral pull-down | PLC | 56.6 ± 12.4 | 60.9 ± 11.6 * | 65.0 ± 12.0 *# | 71.7 ± 11.6 *# |
| VD | 57.8 ± 11.3 | 61.0 ± 11.0 | 65.6 ± 10.4 *# | 71.7 ± 10.5 *# | |
| Seated row | PLC | 63.7 ± 12.1 | 70.1 ± 11.7 * | 75.8 ± 12.5 *# | 81.9 ± 13.3 *# |
| VD | 64.6 ± 13.2 | 72.4 ± 14.0 * | 78.8 ± 15.5 *# | 85.8 ± 16.0 *# |
Data are presented as means ± SD, n = 14 in PLC (placebo) and n = 14 in VD (vitamin D) group. Significantly different (p < 0.05): * from Week 0; # from previous week.
Table 5.
Body mass and body composition during 12-week supplementation and resistance training period.
Table 5.
Body mass and body composition during 12-week supplementation and resistance training period.
| Variable | Group | Week 0 | Week 12 | Change |
|---|---|---|---|---|
| Body mass (kg) | PLC | 90.01 ± 15.54 | 90.47 ± 14.72 | 0.46 ± 1.87 |
| VD | 90.05 ± 15.56 | 90.98 ± 15.14 | 0.93 ± 1.27 | |
| Total fat mass (kg) | PLC | 23.81 ± 7.66 | 22.59 ± 6.95 * | –1.23 ± 1.60 |
| VD | 24.42 ± 7.80 | 23.44 ± 7.90 * | –0.98 ± 1.11 | |
| Total fat (%) | PLC | 26.5 ± 4.5 | 25.0 ± 4.4 * | –1.5 ± 1.2 |
| VD | 27.2 ± 4.9 | 25.7 ± 4.8 * | –1.5 ± 1.1 | |
| Android fat mass (kg) | PLC | 2.18 ± 0.82 | 2.12 ± 0.75 | –0.06 ± 0.25 |
| VD | 2.34 ± 0.99 | 2.25 ± 0.97 | –0.09 ± 0.21 | |
| Android fat (%) | PLC | 32.0 ± 6.0 | 30.0 ± 6.5 * | –2.0 ± 1.9 |
| VD | 33.1 ± 7.2 | 31.3 ± 6.9 * | –1.7 ± 1.7 | |
| Total lean mass (kg) | PLC | 61.41 ± 8.45 | 63.24 ± 8.34 * | 1.82 ± 1.07 |
| VD | 60.76 ± 8.38 | 62.80 ± 8.15 * | 2.04 ± 1.24 | |
| Trunk lean mass (kg) | PLC | 30.85 ± 4.39 | 31.70 ± 4.30 * | 0.86 ± 0.75 |
| VD | 30.96 ± 4.37 | 31.80 ± 3.96 * | 0.85 ± 0.91 | |
| Arms lean mass (kg) | PLC | 7.12 ± 1.26 | 7.45 ± 1.23 * | 0.33 ± 0.24 |
| VD | 7.01 ± 1.13 | 7.50 ± 1.10 * | 0.49 ± 0.47 | |
| Legs lean mass (kg) | PLC | 20.10 ± 3.02 | 20.69 ± 3.02 * | 0.59 ± 0.44 |
| VD | 19.40 ± 2.93 | 19.98 ± 2.99 * | 0.59 ± 0.71 |
Data are presented as means ± SD, n = 14 in PLC (placebo) and n = 14 in VD (vitamin D) group. * Significantly different from Week 0 (p < 0.05).
Table 6.
VO2max, respiratory exchange ratio, peak heart rate, ventilation and breath frequency during VO2max test.
Table 6.
VO2max, respiratory exchange ratio, peak heart rate, ventilation and breath frequency during VO2max test.
| Variables | Placebo (n = 14) | Vitamin D (n = 14) | ||
|---|---|---|---|---|
| Week 0 | Week 12 | Week 0 | Week 12 | |
| VO2max (mL/min/kg) | 40.23 ± 6.10 | 39.26 ± 6.10 | 38.48 ± 6.15 | 37.67 ± 5.81 |
| VO2max (L/min) | 3.60 ± 0.55 | 3.52 ± 0.57 | 3.45 ± 0.52 | 3.42 ± 0.51 |
| RER | 1.11 ± 0.05 | 1.13 ± 0.05 | 1.12 ± 0.05 | 1.13 ± 0.05 |
| HR (beats/min) | 162.2 ± 13.1 | 165.5 ± 13.9 | 169.6 ± 12.9 | 168.1 ± 10.7 |
| VE (L/min) | 125.7 ± 23.0 | 128.9 ± 21.2 | 118.2 ± 21.6 | 121.7 ± 28.0 |
| BF (times/min) | 39.9 ± 9.3 | 40.1 ± 6.5 | 36.3 ± 5.4 | 38.1 ± 6.9 |
Data are presented as mean ± SD. RER, respiratory exchange ratio; HR, heart rate; VE, ventilation; BF, breath frequency.
Table 7.
Serum hormone concentrations during 12-week supplementation and resistance training period.
Table 7.
Serum hormone concentrations during 12-week supplementation and resistance training period.
| Variable | Group | Week 0 | Week 8 | Week 12 |
|---|---|---|---|---|
| Parathormone (pmol/L) | PLC | 4.29 ± 1.29 | 4.88 ± 1.70 | 5.27 ± 1.80 * |
| VD | 4.90 ± 1.17 | 4.38 ± 0.97 | 4.33 ± 1.05 | |
| Testosterone (nmol/L) | PLC | 18.6 ± 5.6 | 18.6 ± 6.1 | 17.7 ± 6.1 |
| VD | 18.8 ± 5.9 | 18.3 ± 5.3 | 17.8 ± 4.4 | |
| Cortisol (nmol/L) | PLC | 384.9 ± 111.1 | 320.5 ± 95.5 | 329.8 ± 92.7 |
| VD | 389.9 ± 109.2 | 335.0 ± 106.1 | 320.6 ± 82.0 | |
| Growth hormone (mU/L) | PLC | 0.777 ± 1.093 | 0.438 ± 0.341 | 0.744 ± 0.884 |
| VD | 0.420 ± 0.690 | 0.339 ± 0.216 | 0.364 ± 0.264 | |
| IGF-1 (μg/L) | PLC | 148.3 ± 32.9 | 149.0 ± 35.4 | 144.6 ± 27.6 |
| VD | 131.5 ± 28.9 | 143.7 ± 34.7 | 132.8 ± 28.7 | |
| Insulin (mU/L) | PLC | 8.75 ± 3.86 | 7.38 ± 2.99 | 8.61 ± 5.20 |
| VD | 7.59 ± 2.94 | 7.74 ± 2.53 | 6.46 ± 2.99 |
Data are presented as means ± SD, n = 14 in PLC (placebo) and n = 14 in VD (vitamin D) group. IGF-1, insulin-like growth factor-1. * Statistically significant within-group difference compared to week 0 (p < 0.05).
Table 9.
Serum hemoglobin, ferritin and glucose concentrations and HOMA-IR during 12-week supplementation and resistance training period.
Table 9.
Serum hemoglobin, ferritin and glucose concentrations and HOMA-IR during 12-week supplementation and resistance training period.
| Variable | Group | Week 0 | Week 8 | Week 12 |
|---|---|---|---|---|
| Hemoglobin (g/L) | PLC | 155.3 ± 6.7 | 154.2 ± 6.3 | 153.1 ± 5.4 |
| VD | 150.2 ± 9.9 | 149.3 ± 8.1 | 148.1 ± 10.0 | |
| Ferritin (μg/L) | PLC | 198.8 ± 106.0 | 166.8 ± 97.0 | 170.9 ± 99.2 |
| VD | 190.0 ± 129.7 | 157.2 ± 109.3 | 164.3 ± 114.6 | |
| Glucose (mmol/L) | PLC | 5.58 ± 0.60 | 5.44 ± 0.43 | 5.58 ± 0.44 |
| VD | 5.55 ± 0.55 | 5.70 ± 0.29 | 5.54 ± 0.44 | |
| HOMA-IR | PLC | 2.23 ± 1.22 | 1.79 ± 0.76 | 2.14 ± 1.30 |
| VD | 1.88 ± 0.77 | 1.96 ± 0.66 | 1.60 ± 0.76 |
Data are presented as means ± SD, n = 14 in PLC (placebo) and n = 14 in VD (vitamin D) group.
Table 10.
Serum metabolite concentrations and creatine kinase activity during 12-week supplementation and resistance training period.
Table 10.
Serum metabolite concentrations and creatine kinase activity during 12-week supplementation and resistance training period.
| Variable | Group | Week 0 | Week 8 | Week 12 |
|---|---|---|---|---|
| Ionized calcium (mmol/L) | PLC | 1.30 ± 0.06 | 1.28 ± 0.08 | 1.26 ± 0.05 |
| VD | 1.27 ± 0.07 | 1.26 ± 0.08 | 1.27 ± 0.03 | |
| Calcium (mmol/L) | PLC | 2.44 ± 0.08 | 2.43 ± 0.10 | 2.38 ± 0.09 |
| VD | 2.38 ± 0.10 | 2.43 ± 0.04 | 2.41 ± 0.09 | |
| Urea (mmol/L) | PLC | 6.09 ± 0.84 | 5.96 ± 0.88 | 6.18 ± 1.07 |
| VD | 5.75 ± 1.21 | 6.68 ± 1.39 * | 6.51 ± 1.47 * | |
| Creatine kinase (U/L) | PLC | 233.1 ± 174.1 | 170.6 ± 86.1 | 177.6 ± 72.2 |
| VD | 152.4 ± 75.6 | 122.4 ± 44.0 | 169.4 ± 78.6 |
Data are presented as means ± SD, n = 14 in PLC (placebo) and n = 14 in VD (vitamin D) group. * Statistically significant within-group difference compared to week 0 (p < 0.05).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



