
Submitted:
26 August 2024
Posted:
27 August 2024
You are already at the latest version
Abstract
Mediterranean diet has been widely suggested to exert significant beneficial effects on endothelial oxida-tive status and cardiometabolic health. Greek Orthodox monasteries, due to their specific nutritionaland sartorial habits, comprise a population which strictly adheres to nutritional patterns with restricted eating and a plant-based subset of the Mediter-ranean diet, often accompanied by profound hypovitaminosis D. Time –restricted eating is also adopted from a large part of general lay Greek population for health promoting reasons, without restrictions on an-imal product consumption, as imposed by Orthodox religious fasting. However, comparative effects of these nutritional patterns on oxidative stress markers remain scarce. The present study attempted to evaluate the effects of Christian Orthodox fasting (COF) in a group of vitamin D –deficient and overweight Orthodox nuns from Central and Northern Greece, compared to the implementation of TRE, 16:8 dietary regimen in a cohort of adult women from the general population from the same region, with regard to markers of endothelial oxidative status. A group of 50 women from two Orthodox monasteries in Northern Greece and one group of 50 healthy lay women were included. During enrollment a detailed recording of dietary habits was performed, along with a scientific registry of demographic and anthropometric characteristics (via bioimped-ance).Orthodox nuns followed a typical Orthodox fasting regimen[daily feeding window (8 am–4 pm)] whereas lay women followed a TRE 16:8 regimen with the same feeding time-window with recommenda-tion to follow a low-fat diet, without characteristics of the Mediterranean diet. We included a complete biochemical analysis, as well as calciotropic profiles [Calcium-Ca, Albumin, Parathyroid hormone-PTH, 25-hydroxyvitamin D- 25(OH)D] as well as and markers of TAC (trichloroacetic acid), (glutathione) GSH and thiobarbituric acid reactive substances (TBARS) concentrations, as markers of oxidative status. All groups were comparable at baseline for calcium, PTH and 25(OH)D concentrations, with no significant differences between groups. Orthodox nuns manifested a lower median GSH compared to con-trols (6.0 vs. 7.2, p 0.04) and a higher median TAC (0.92 vs. 0.77, p <0.001). TBARS comparisons showed no significant difference between the two groups. No significant associations of oxidative status with 25(OH)D, PTH and markers of glucose homeostasis were evident. Results of this small pilot study indicate that both dietary regimens have advantages over oxidative markers compared to each other, with increased TAC in the groups of Orthodox Nuns after a 16th week period of COF compared to a 16:8 TRE and increased GSH concentrations in the lay women group. Future randomized trials are required to investigate superiority or non-inferiority between these dietary patterns, in the daily clinical setting.
Keywords:
oxidative stress
; mediterranean diet
; time restricted eating
; orthodox fasting
Introduction
Christian Orthodox fasting (COF), is a vital subset of the Mediterranean diet (MD)
[1,2,3,4], which for religious reasons is considered to be deeply integrated in the cultural dietary behavior of a large part of the Greek population [5,6,7,8,9] for prolonged periods (from 120 to 180 d) annually [8].Orthodox monasteries follow this archetype pattern of diet throughout the year, with periods of more strict fasting rituals 2-6 weeks before religious celebrations, as a way of physical and mental prosperity and personal spiritual development [1,2]. However, besides the spiritual significance of COF, a plethora of cohort studies suggest that COF shares the beneficial effects of the typical MD by promoting specific cardioprotective mechanisms, including reduced intake of dietary cholesterol and fatty acids, thus providing optimal effects on plasma lipid concentrations [9,10]. These benefits have been mainly attributed to the integration of a plant-based diet along with characteristics of dietary restriction of animal products (meat, dairy products and eggs) [6] and restriction of caloric intake during COF periods [11,12,13,14]. We have previously reported on the beneficial effects of COF on the adipokine profile [7,8,14] as well as on glucose homeostasis in both monastic and general populations [15], as markers for prevention of cardiovascular dyshomeostasis, with the exception of profound hypovitaminosis—D in Orthodox Monks, mainly due to their sartorial habits [11,16].
Additionally, restriction of food intake in specific time—frames during the day, has also been hypothesized to contribute to the benefits described above, a characteristic which attracted significant scientific and public interest during the last decade, through various intermittent—fasting patterns, practiced worldwide as a health-promoting diet [17]. Time-restricted eating (TRE), includes specific time-frames of food intake during the day, which vary from 4-12 hours daily [e.g., 20 hours of fasting vs 4 hours of permitted food intake—20:4—as well as additional time frames (18:6,16:8 etc.)] [18]. On the other hand, impairment of antioxidative capacity of vascular endothelium is an established aggravating factor for development of endothelial dysfunction and future cardiovascular major events [19,20]. On that basis, a considerable number of previous studies [21,22,23,24] have suggested that MD is strongly associated with favorable effects on oxidative status, implying a potential pathway for exerting its well—established cardiovascular benefits. However, results on COF as a vital subset of MD and its effects on oxidative status, particularly compared to other healthy nutritional patterns widely adopted by the general population, remain scarce.
Additionally, these potential interactions have so far not been investigated in conjunction with other metabolic conditions associated with endothelial dysfunction, including impairment of vitamin D status and insulin resistance, particularly in vitamin D deficient and overweight individuals. These results could elucidate potential mechanisms of MD—related effects on antioxidative capacity and also elaborate on the research hypothesis, which indicates the macro- and micronutrient synthesis and increased intake of food antioxidants, rather than the timing of food intake, as the cornerstone of attained metabolic benefits.
The present study attempted to evaluate the effects of COF in a group of vitamin D –deficient and overweight Orthodox nuns from Central and Northern Greece,comparedto the implementation ofTRE16:8 dietary regimen in a cohort of adult women from the general population from the same region, with regard to markers of endothelial oxidative status.
Methods
Design
This was a cross-sectional study after a period of 16-week implementationof COF and TRE, in two groups of adult female nuns and lay women.
Study Population
We included 50 Christian Orthodox female adult nuns, from two different monasteries, 30–50 years of age, residing in the Central and Northern Greece and an age—matched cohort of 50 adult lay women from the same region.
Orthodox nuns (but not lay women), with a baseline 25-hydroxyvitamin D concentrations ≥ 20 ng/ml (as initially evaluated from the same initial cohort –results published previously [12,13,14,15]) were excluded. Additional exclusion criteria for both groups were: body mass index (BMI)≤ 25, amenorrhea ≥ 3 months, pregnancy, presence of chronic kidney disease, severe liver disease, diagnosis of prediabetes (fasting glucose 100–125 mg/dL or glycated hemoglobin 5.7–6.4% or blood glucose 140–199 mg/dL at 2 h post 75 g glucose load) or diabetes mellitus (fasting glucose ≥ 126 mg/dL or glycated hemoglobin ≥ 6.5% or blood glucose ≥ 200 mg/dL at 2 h post 75 g glucose load), dyslipidemia, arterial hypertension, or uncontrolled hypothyroidism (not adequately controlled or first diagnosed and not treated), (recent surgery or severe infections (during the past 3 months), administration of medications that can alter body weight, glucose and lipid metabolism (e.g., statins, corticosteroids, antipsychotics),intake of vitamins or mineral supplements, physical disabilities and/or neurodegenerative disorders that could affect physical activity, acute infections and chronic degenerative diseases.
Dietary Patterns
Orthodox nuns with at least 16 weeks adherence to COF were included in the study, whereas women from the general population, followed TRE for 16 weeks, after a wash-out period of 3 weeks, before inclusion in the study. Orthodox nuns followed the Athonian type of fasting as previously described [1,2,3,4], abstaining from consumption of animal products (meat, poultry, eggs, dairy and cheese), with the exception of seafood and fish, which fasters were permitted to eat on two specific weekdays, while the general population group was allowed to eat low-fat meat products, without specific distribution and cut-offs of macronutrients and daily caloric intake.
Orthodox nuns group adopted an 8 h eating interval (08.00 to 16.00), as dictatedby typical monastery dietary rules, which are obligatory for all residents of the monastery, while TRE group consumed food from 09:00 to 17:00. Adherence to dietary plans was evaluated with a 3-day food record (two weekdays and one weekend day) at the end of the study period, while the Nutrition Analysis Software Food Processor [https://esha.com/products/food- processor/ (accessed on 2 August 2024)] [25] was used to analyze food records. Finally, levels, frequency and duration of physical activity, divided in light, moderate and intense physical activity, were recorded for all participants, according to AHA recommendations [26].
Anthropometric Measurements and Biochemical Analysis
Anthropometric measurements and biochemical analyses were performed in both groups using standardized procedures. Exact methods, reference ranges, equipment used, and other details were previously analytically described [11]. In brief, body weight (BW) was recorded to the nearest 0.01 kg using a calibrated computerized digital balance (K-Tron P1-SR, Onrion LLC, Bergenfield, NJ, USA); each participant was barefoot and lightly dressed during measurement. BMI was calculated as the ratio of weight in kilograms divided by the height in meters squared (kg/m2) [27]. Body fat (BF) mass and percentage, visceral fat (VF), muscle mass, fat-free mass, and total body water were measured using bioelectrical impedance analysis (SC-330 S, Tanita Corporation, Tokyo) [28]. Blood samples were drawn in the morning, after a 12 h overnight fast by antecubital venipuncture, and the samples were stored at −20oC prior to analysis. Calcium (Ca) concentrations were evaluated using the COBAS8000 automated analyzer system (Roche Diagnostics GmbH, D-68298 Mannheim, Germany). Parathyroid hormone (PTH) and 25(OH)D, were tested in the COBAS e 602 immunochemistry module using electro-chemiluminescence (ECL) technology (Roche Diagnostics GmbH, D-68298 Mannheim, Germany). Reference ranges of values as well as inter- and intra-assay coefficients of variation for the examined parameters are as follows: Ca: 8.4–10.2 mg/dl, 0.8–1.3% and 0.5–1.3%; PTH: 15–65 pg/mL (or 1.6–6.9 pmol/L), 1.1–2.0% and 2.5–3.4%; 25(OH)D: ≥ 30 ng/mL, 2.2–6.8% and 3.4–13.1%.Insulin resistance was calculated using the homeostasis model assessment (HOMA-IR) formula described by Matthews et al. [29] as follows: FPI (mU/mL) x FPG (mmol/L)/ 22.5, where FPI stands for fasting plasma insulin and FPG for fasting plasma glucose.
Markers of Oxidative Status
Determination of Glutathione (GSH) Concentration in Blood
GSH concentration was determined according to the method of Reddy et al. [30] as previously described [31]. At first, 400 μL of RBCL was mixed with 400 μL of 5% trichloroacetic acid (TCA), respectively, and centrifuged (15,00× g, 5 min, 5 °C). Afterwards, 300 μL of the supernatant was mixed with 90 μL of 5% TCA and centrifuged (15,00× g, 5 min, 5 °C). The resulting supernatant was collected and used as the biological sample for the assay. Regarding the assay, 20 μL of the biological samplewas mixed with 660 μL of phosphate buffer (67 mM, pH = 7.95) and 330 μL of 5,5-dithiobis(2-nitrobenzoic acid) (DTNB) (1 mM). The samples were vortexed and incubated for 45 min in the dark at room temperature (RT), and the optical density was measured at 412 nm. GSH concentration was calculated based on the millimolar extinction coefficient of 2-nitro-5-thiobenzoate (TNB) (13.6 L/mmol/cm).
Determination of Total Antioxidant Capacity (TAC) Concentrations in Blood
TAC levels were evaluated based on the protocol of Janaszewska and Bartosz [32]. More elaborately, 20 μL of plasma was mixed with 480 μL or 460 μL of phosphate buffer (10 mM, pH = 7.4), respectively, and, immediately, 500 μL of 2,2-diphenyl-1-picrylhydrazyl radical (DPPH•) solution (0.1 mM) was added. The samples were vortexed, incubated for 1 h in the dark at RT, and centrifuged (15,00× g, 3 min, 25 °C). Finally, the optical density was measured at 520 nm. TAC levels were expressed as the mmol of DPPH• reduced to the corresponding hydrazine by the antioxidant compounds present in plasma or tissue homogenates.
Determination of Thiobarbituric acid Reactive Substances (TBARS) Concentrations in Blood
TBARS levels were determined by a slightly modified method by Keles et al. [33]. Specifically, 100 μL of plasma was mixed with 500 μL of Tris-HCl (200 mM, pH = 7.4) and 500 μL of 35% TCA and incubated for 10 min at RT. After that, 1 mL of sodium sulfate (Na2SO4) (2 M) and thiobarbituric acid (TBA) (55 mM) solution was added, and the samples were placed in a water bath for 45 min at 95 °C. After incubation, the samples were cooled on ice for 5 min, 1 mL of 70% TCA was added, and the samples were centrifuged (11,20× g, 3 min, 25 °C). The resulting supernatant was used to measure the optical density at 530 nm. TBARS levels were calculated by applying the molar extinction coefficient of malonyl dialdehyde (ΜDA) (156,000 L/mol/cm).
Determination of GSH Concentration in Blood
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki on the human trial performance. Written informed consent for inclusion in the study was given by participants. Official written approval for the inclusion of the Orthodox nuns group was given by the Holy Supervision Council of the monasteries, after submission of the full study protocol 12 months before study initiation.
Statistical Analysis
Continuous variables are reported as means and S.D.’s. Dietary and nutrient intake on were compared using paired samples t-test. Age differences between the groups with light, moderate and intense physical activity were tested using one-way analysis of variance with Tukey post hoc test. The effect of level of physical activity on overall health markers was tested with analysis of covariance to control for age. Normality of distribution was tested with one sample Kolmogorov– Smirnov test (exact statistics).
The among-group comparison was made using nonparametric Mann-Whitney U test. Linear regression was used for multi-adjusted analysis.Assumptions were checked for each statistical analysis. Level of significance was set at P <0.05(non-directional). Data were analyzed using SPSS v22.
Results
Orthodox nuns were older than lay women (median age 42 vs. 38, p<0.001) but did not differ in median weight and BMI(Table 1).Groups did not differ in body fat (%), lean body mass (%) and waist circumference,as well as degrees of physical activity, with the exception of intense activity, in which lay women reported higher rates. Regarding nutritional analysis,lay women consumed higher amounts of carbohydrates (gr) (194.3 ± 23.4 vs 159.6 ± 21.8),total and saturated fat (24.4± 0.6 vs 21.0 ± 0.1and 16.4 ± 0.0 and 12.7±0.0,respectively) whereas Orthodox nuns reported higher amounts of protein and fibre intake (36.1± 0.8 vs 24.2 ± 0.8).
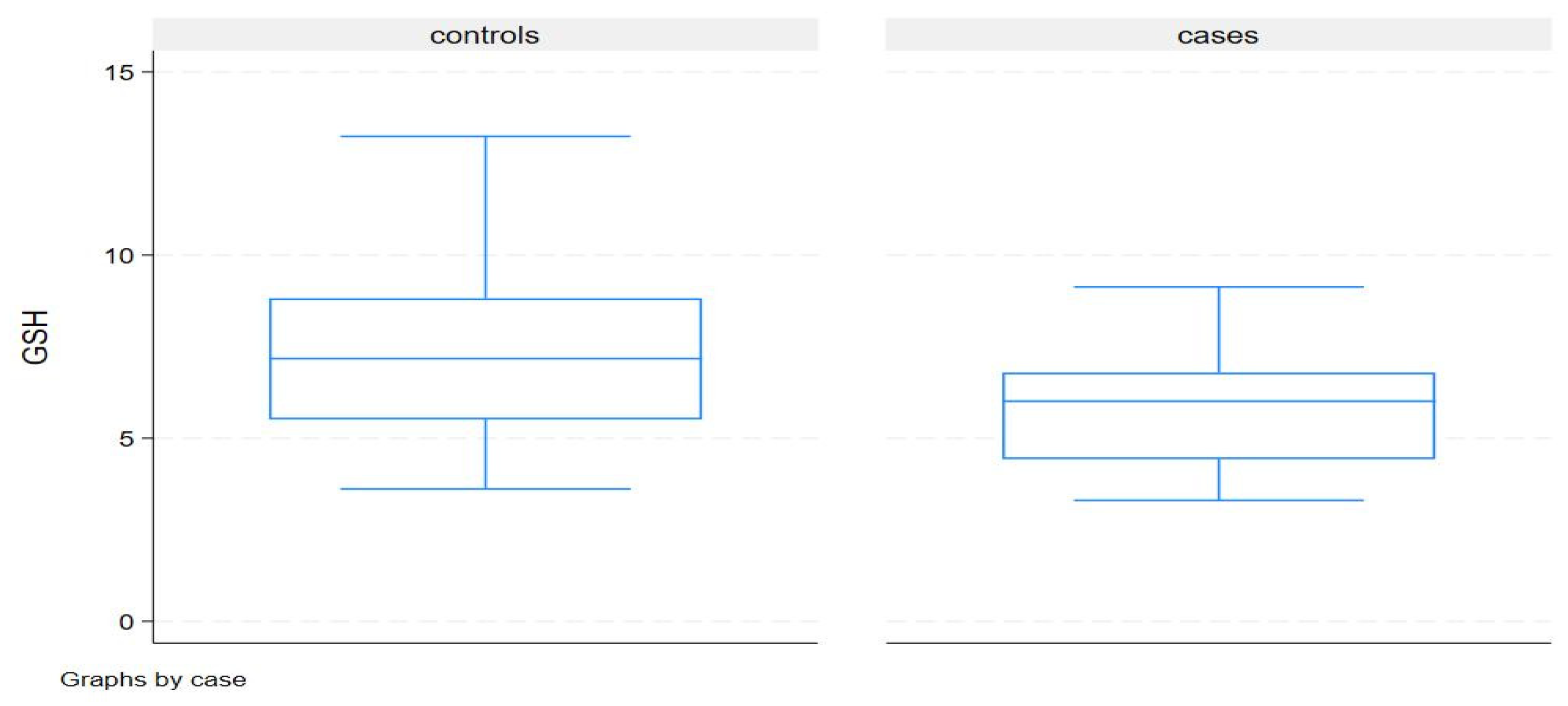
Although expected, according to the study protocol, hypovitaminosis D evident in the Orthodox nuns’ group, resulted in significantly higher median serum PTH than among lay women (45.6 vs. 19.4, p<.001), after adjusting for seasonal variation. In addition,after adjusting for age and 25(OH)D3 concentrations in linear regression across all patients, PTH had a significant positive association with age (+6.0 pg/ml per 10-year increase in age, p<0.001) and a significant negative association with serum 25(OH) D3 status (–0.61 pg/ml per ng/ml increase in serum D3). Orthodox nuns demonstrated lower median fasting insulin concentrations (5.3 vs. 7.2, p 0.02) compared to lay women and evenafter adjusting for age and BMI, the difference remained significant; Of major interest is the fact, that insulin concentrations lacked a significant association with BMI or age in both groups. Regarding redox status, Orthodox nuns manifested a lower median GSH compared to controls (6.0 vs. 7.2, p .04) and a higher median TAC (0.92 vs. 0.77, p <.001). TBARS comparisons showed no significant difference between the two groups. After adjusting for age in linear regression, Orthodox nuns had a lower GSH concentration in serum (mean difference -1.7; 95% CI -2.7 to = –0.7, p .001) compared to controls, while the age effect was not significant (p=0.45). After adjusting for age, nuns had a higher TAC concentration in serum (mean difference 0.19; 95% CI0.13 to0.26, p <.001), whereas after adjusting for age,BMI and total fat in linear regression, nuns had a lower GSH concentration in serum (mean difference –1.6; 95% significant (p=0.45). After adjusting for age, nuns had a higher TAC concentration in serum (mean difference 0.19; 95% CI0.13 to0.26, p <.001), whereas after adjusting for age,BMI and total fat in linear regression, nuns had a lower GSH concentration in serum (mean difference –1.6; 95% CI –2.6 to = –0.7, p .001) compared to lay women, while the age and BMI effects were not significant. After adjusting for age and BMI, nuns had a higher TAC concentration in serum (mean difference 0.21; 95% CI0.15 to 0.27 p <.001); age, BMI and total fat, effects were not significant. No significant associations of oxidative status with 25(OH)D, PTH and markers of glucose homeostasis were evident.
Figure 1.
Concentrations of TAC in Orthodox Nuns and lay women group.
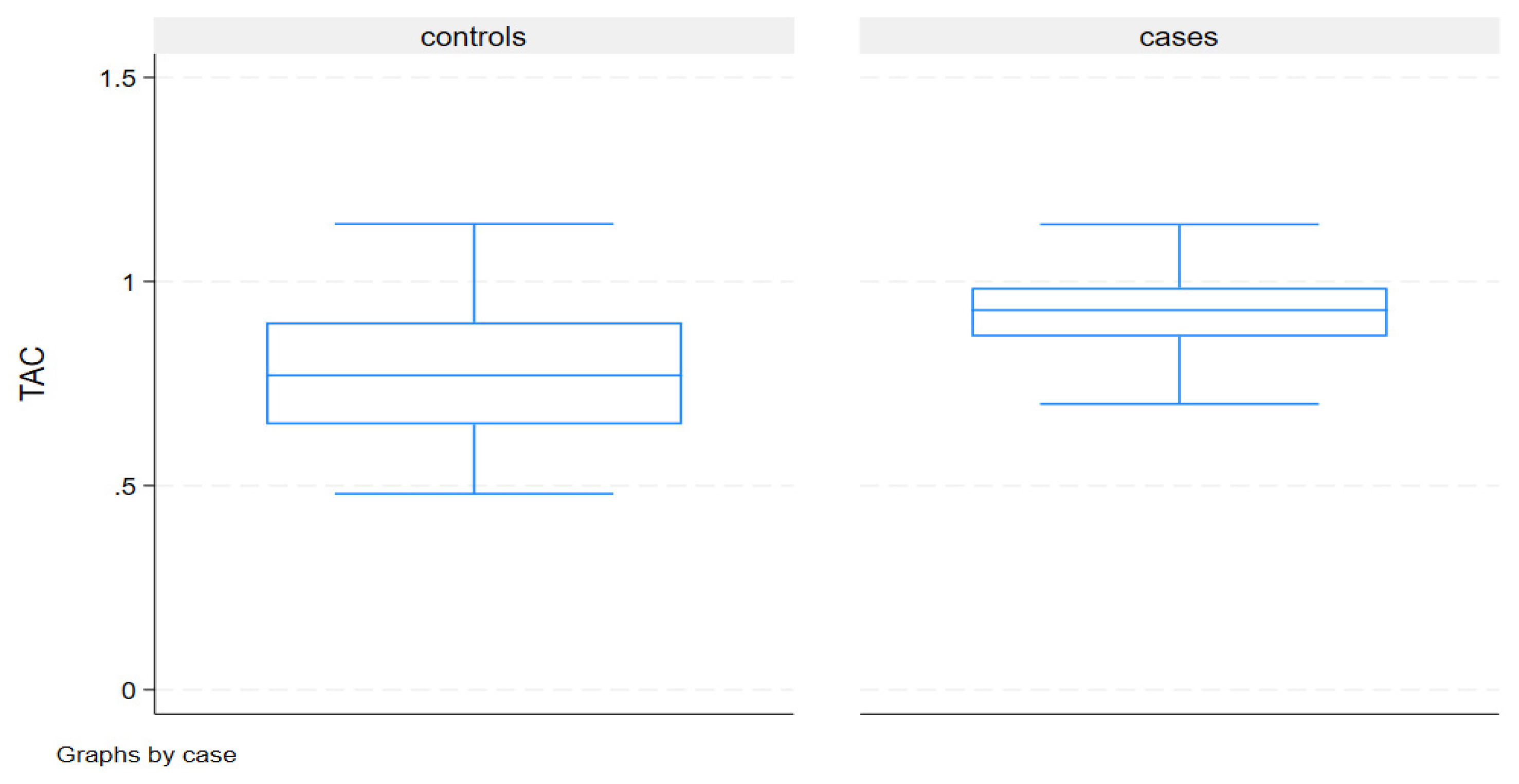
Figure 2.
Concentrations of GSH in Orthodox Nuns and lay women group.
Discussion
To our knowledge, this the first cross-sectional study reporting preliminary results on the comparative effects of COF on oxidative status in vitamin D deficient Greek Orthodox nuns and TRE (16:8) dietary regimen in a group of lay women with vitamin D sufficiency. These results indicated: i) increased antioxidative capacity (TAC) in the group of Orthodox Nuns after a 16 week period of COF compared to a 16:8 TRE, ii) increased GSH levels in the lay women group compared to the group of Orthodox nuns as well as comparable of TBARS levels in both groups, after adjusting for several confounders, which suggest potential diverse effects of COF and TRE on oxidative status.
MD is a plant-based diet, rich in fruit, vegetables, nuts, herbs, with fewer fish and dairy products and with less red meat and red wine. MD includes various nutritional compounds, with well-established beneficial effects on oxidative status. A plethora of previous basic and clinical studies suggested that MD has been shown to be one of the healthiest eating patterns, with various metabolic benefits, partly mediated through its antioxidant capacity [34,35]. Dai et al. studied the ratio of reduced to oxidized glutathione (GSH / GSSG) in twins. The higher the ratio, the lower the oxidative stress, giving a result of a higher ratio up to 7% in individuals who followed the Mediterranean diet, regardless of the adjustment of the energy intake [36]. In a sub-cohort of The PREDIMED trial, participants with high cardiovascular risk were randomized to a Mediterranean diet supplemented with extra-virgin olive oil and manifested a significant reduction in cellular lipid levels and lipid oxidation, as well as malondialdehyde concentrations in mononuclear cells, without changes in serum glutathione peroxidase activity [37].
Documented benefits of MD include consumption ofunsaturated fatty acids, found in olive oil, which contain 3,3dimethyl-1-butanol, thuspreventing the formation of trimethylamine-1-oxide, one of the oxidants related to cardiovascular events [38,39].
Additionally, MD synthesis is rich in oleic-acid and alpha-linoleic-acid,found in nuts, fruit and vegetable flavonoids, as well as omega-3-polyunsaturated-fatty-acids, and fiber and polyphenols, all of which have anti-oxidative, anti-bacterial and anti-inflammatory effects [40,41,42]. Moreover, whole-grains, as a vital compound of MD, contain a polyaminecalled spermidine, which has been shown to extend chronological life-span in flies, nematodes, rodents, and human cells. Spermidine is known to inhibit histone acetyltransferases, which results in higher resistance to oxidative stress [43].
TRE has been also the objective of recent studies regarding its potential beneficial effects on cardiometabolic health. Given the fact that hormones undergo a circadian rhythm, metabolic and stress hormones as insulin, cortisol, growth hormone and melatonin undergo the same variation, giving different levels between a calorie-restricting diet and intermittent-fasting diet, which restricts the feeding time in certain hours [44]. Mc Allister et al. studied the impact of intermittent fasting on markers of cardiometabolic health, measuring several markers of inflammation, OS, and cardiometabolic health (insulin, ghrelin, leptin, glucagon, adiponectin, resistin, advanced glycated-end products (AGE), advanced oxidation protein products, total nitrite-nitrate levels, tumor necrosis factor-α, interleukin (IL)-6, IL-8, IL-10and showed that time-restricted feeding resulted in significant reductions in advanced oxidation protein products (∼31%) and AGEs (∼25%); however, no other changes were found [45]. Recent randomized clinical trials also demonstrated that a6-hr feeding period for 5 weeks improved insulin sensitivity, β-cell responsiveness and oxidative stress, irrespective of weight loss [46]. These results were also previously confirmed by other groups,where4- and 6-h TRE for 5 weeks, resulted in a reduction of 8-isoprostane, as a marker of oxidative stress to lipids,4-hydroxynonenal adducts, protein carbonyls and nitrotyrosine [47].
COF is a plant-based subset of the traditional MD followed for more than a thousand years from a large part of the Greek Orthodox general population for religious purposes from 90–150 days per year. Greek Orthodox monasteries adhere to this dietary regimen throughout the year, with the addition of TRE (usually 16:8) characteristics in their daily dietary regimen, which is strictly followed by all members of the monasterial community, comprising an optimal sample for nutritional studies .We have repeatedly reported on the effects on COF on body weight, lipid parameters, adipokines and vitamin D status, regarding the existence of severe hypovitaminosis D in Orthodox male monks, mainly due to their sartorial habits.
However, this is the first report on the effects of COF on oxidative equilibrium, particularly compared to a health –promoting pattern like TRE.
Our research hypothesis raised the question for non-inferiority of TRE compared to COF, in a vitamin D deficient monastic population (as most similar monastic communities in Greece), taking into account that women included in the TRE, were not instructed to follow a MD—specific dietary pattern. According to previous results, chronic vitamin D deficiency is a state of increased oxidative stress, which reduces the capacity of mitochondrial respiration, through modulating nuclear mRNA down regulating the expression of complex I of the electron transport chain, reducing of adenosine triphosphate (ATP),resulting in increased formation of ROS, augmenting oxidative stress [48].
Maintaining optimum levels of redox biomarkers is crucial for preventing oxidative damage, supporting detoxification processes, and ensuring proper immune function. Previous literature proposed that clustering of high and low GSH levels might provide strong causality for type 2 diabetes and metabolic syndrome [48]. Our results failed to suggest a superiority of COF over TRE, in a group with confirmed MD-type dietary regimen and TRE characteristics as Orthodox nuns, compared to a 16:8 without specific MD—related dietary characteristics.
A plausible explanation could be that the general population following a TRE pattern comply with a healthy dietary pattern, which despite not being identical to MD,also exerts benefits on GSH concentrations, always taking into account the limitations of this study. Another explanation, could lie on the potential adverse effects of hypovitaminosis D, evident in Orthodox nuns included in this study, on GSH concentrations, as previously reported [12]. Vitamin D supplementation in this group of vitamin D deficient nuns could elucidate this potential biological association on GSH status. TRE could also have independent beneficial effects on oxidative status, which are evident without strict adherence to a MD-related pattern, as previously reported [12]. Finally, our study failed to establish an association of impaired vitamin D status and oxidative markers, which could be attributed to its cross-sectional design. This study has several limitations and can only be considered as a pilot study, with findings which definitely require confirmation in a prospective study.
In detail, the number of included participants was relatively small; however, this is a representative sample of Orthodox nuns, according to their dietary and physical activity plan. We have also not included a detailed analysis regarding the intake of the dietary antioxidatives in the two groups, which could explain diversity in markers of oxidative status. Finally, since no baseline evaluation, prior to the implementation of dietary interventions, was feasible for both groups, we were unable to establish causal associations.
In conclusion, results of this small pilot study indicate that both dietary regimens have advantages over oxidative markers, compared to each other, with increased TAC in the groups of Orthodox Nuns after a 16th-week period of COF in comparison to increased GSH concentrations in the lay women group following 16:8 TRE, and comparable concentrations of TBARS. Future randomized trials are required to investigate superiority or non-inferiority between these dietary patterns, in the daily clinical setting.
References
- Trepanowski, J.F.; Bloomer, R.J. The impact of religious fasting on human health. Nutr. J. 2010, 9, 57. [Google Scholar] [CrossRef] [PubMed]
- Sarri, K.O.; Linardakis, M.K.; Bervanaki, F.N.; Tzanakis, N.E.; Kafatos, A.G. Greek Orthodox fasting rituals: A hidden characteristic of the Mediterranean diet of Crete. Br. J. Nutr. 2004, 92, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Sarri, K.O.; Tzanakis, N.E.; Linardakis, M.K.; Mamalakis, G.D.; Kafatos, A.G. Effects of Greek Orthodox Christian Church fasting on serum lipids and obesity. BMC Public Health 2003, 3, 16. [Google Scholar] [CrossRef] [PubMed]
- Sarri, K.; Linardakis, M.; Codrington, C.; Kafatos, A. Does the periodic vegetarianism of Greek Orthodox Christians benefit blood pressure? Prev. Med. 2007, 44, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Karras, S.N.; Koufakis, T.; Adamidou, L.; Antonopoulou, V.; Karalazou, P.; Thisiadou, K.; Mitrofanova, E.; Mulrooney, H.; Petróczi, A.; Zebekakis, P.; et al. Effects of orthodox religious fasting versus combined energy and time restricted eating on body weight, lipid concentrations and glycaemic profile. Int. J. Food Sci. Nutr. 2021, 72, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Karras, S.N.; Koufakis, T.; Adamidou, L.; Polyzos, S.A.; Karalazou, P.; Thisiadou, K.; Zebekakis, P.; Makedou, K.; Kotsa, K. Similar late effects of a 7-week orthodox religious fasting and a time restricted eating pattern on anthropometric and metabolic profiles of overweight adults. Int. J. Food Sci. Nutr. 2021, 72, 248–258. [Google Scholar] [CrossRef] [PubMed]
- Karras, S.N.; Koufakis, T.; Adamidou, L.; Dimakopoulos, G.; Karalazou, P.; Thisiadou, K.; Makedou, K.; Kotsa, K. Effects of Christian Orthodox Fasting Versus Time-Restricted Eating on Plasma Irisin Concentrations among Overweight Metabolically Healthy Individuals. Nutrients 2021, 13, 1071. [Google Scholar] [CrossRef] [PubMed]
- Karras, S.N.; Koufakis, T.; Adamidou, L.; Dimakopoulos, G.; Karalazou, P.; Thisiadou, K.; Makedou, K.; Zebekakis, P.; Kotsa, K. Implementation of Christian Orthodox fasting improves plasma adiponectin concentrations compared with time-restricted eating in overweight premenopausal women. Int. J. Food Sci. Nutr. 2022, 73, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Azzeh, F.S.; Hasanain, D.M.; Qadhi, A.H.; Ghafouri, K.J.; Azhar, W.F.; Ghaith, M.M.; Aldairi, A.F.; Almasmoum, H.A.; Assaggaf, H.M.; Alhussain, M.H.; et al. Consumption of Food Components of the Mediterranean Diet Decreases the Risk of Breast Cancer in the Makkah Region, Saudi Arabia: A Case-Control Study. Front. Nutr. 2022, 9, 863029. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Vasilopoulou, E.; Georga, K. Macro- and micronutrients in a traditional Greek menu. Forum. Nutr. 2005, 57, 135–146. [Google Scholar]
- Karras, S.N.; Koufakis, T.; Petróczi, A.; Folkerts, D.; Kypraiou, M.; Mulrooney, H.; Naughton, D.P.; Persynaki, A.; Zebekakis, P.; Skoutas, D.; et al. Christian Orthodox fasting in practice: A comparative evaluation between Greek Orthodox general population fasters and Athonian monks. Nutrition 2019, 59, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Karras, S.N.; Persynaki, A.; Petróczi, A.; Barkans, E.; Mulrooney, H.; Kypraiou, M.; Tzotzas, T.; Tziomalos, K.; Kotsa, K.; Tsioudas, A.; et al. Health benefits and consequences of the Eastern Orthodox fasting in monks of Mount Athos: A cross-sectional study. Eur. J. Clin. Nutr. 2017, 71, 743–749. [Google Scholar] [CrossRef] [PubMed]
- 13 Karras, S.N.; Koufakis, T.; Adamidou, L.; Dimakopoulos, G.; Karalazou, P.; Thisiadou, K.; Zebekakis, P.; Makedou, K.; Kotsa, K. Different patterns of changes in free 25-hydroxyvitamin D concentrations during intermittent fasting among meat eaters and non-meat eaters and correlations with amino acid intake. Int. J. Food Sci. Nutr. 2023, 74, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Karras SN, Koufakis T, Popovic DS, Adamidou L, Karalazou P, Thisiadou K, Zebekakis P, Makedou K, KotsaK.Nutrients. 2023 Dec 9;15(24):5058. https://doi.org/10.3390/nu15245058 A Mediterranean Eating Pattern Combining Energy and Time-Restricted Eating Improves Vaspin and Omentin Concentrations Compared to Intermittent Fasting in Overweight Individuals.
- Karras SN, Koufakis T, Dimakopoulos G, Popovic DS, Kotsa K. Changes in dietary intake of aspartic acid during and after intermittent fasting correlate with an improvement in fasting glucose in overweight individuals. J Diabetes. 2023 Feb;15(2):181-184. doi: 10.1111/1753‐0407.13351. CrossRef].
- Karras SN, A Persynaki, A Petróczi, E Barkans, H Mulrooney, M Kypraiou 1, T Tzotzas, K Tziomalos, K Kotsa, A Tsioudas, C Pichard, D P Naughton Health benefits and consequences of the Eastern Orthodox fasting in monks of Mount Athos: a cross-sectional study Eur J Clin Nutr. 2017 Jun;71(6):743-749. doi: 10.1038/ejcn.2017.26. Epub 2017 Mar 22.
- Manoogian ENC, Laferrère B Time-restricted eating: What we know and where the field is going..Obesity (Silver Spring). 2023 Feb;31 Suppl 1(Suppl 1):7-8. doi: 10.1002/oby.23672.
- Koppold DA, Breinlinger C, Hanslian E, Kessler C, Cramer H, Khokhar AR, Peterson CM, Tinsley G, Vernieri C, Bloomer RJ, Boschmann M, Bragazzi NL, Brandhorst S, Gabel K, Goldhamer AC, Grajower MM, Harvie M, Heilbronn L, Horne BD, Karras SN, Langhorst J, Lischka E, Madeo F, Mitchell SJ, Papagiannopoulos-Vatopaidinos IE, Papagiannopoulou M, Pijl H, Ravussin E, Ritzmann-Widderich M, Varady K, Adamidou L, Chihaoui M, de Cabo R, Hassanein M, Lessan N, Longo V, Manoogian ENC, Mattson MP, Muhlestein JB, Panda S, Papadopoulou SK, Rodopaios NE, Stange R, Michalsen A.International consensus on fasting terminology. Cell Metab. 2024 Aug 6;36(8):1779‐1794.e4. doi: 10.1016/j.cmet.2024.06.013. Epub 2024 Jul 25.
- Wang X, He B.Endothelial dysfunction: molecular mechanisms and clinical implications. MedComm (2020). 2024 Jul 22;5(8):e651. doi: 10.1002/mco2.651. eCollection 2024 Aug.
- Sharebiani H, Mokaram M, Mirghani M, Fazeli B, Stanek A .The Effects of Antioxidant Supplementation on the Pathologic Mechanisms of Metabolic Syndrome and Cardiovascular Disease Development..Nutrients. 2024 May 27;16(11):1641. doi: 10.3390/nu16111641.
- Dobroslavska P, Silva ML, Vicente F, Pereira P Mediterranean Dietary Pattern for Healthy and Active Aging: A Narrative Review of an Integrative and Sustainable Approach.Nutrients. 2024 May 31;16(11):1725. doi: 10.3390/nu16111725.
- Rezig L, Ghzaiel I, Ksila M, Yammine A, Nury T, Zarrouk A, Samadi M, Chouaibi M, Vejux A, Lizard G Cytoprotective activities of representative nutrients from the Mediterranean diet and of Mediterranean oils against 7-ketocholesterol- and 7 beta-hydroxycholesterol-induced cytotoxicity: Application to age-related diseases and civilization diseases..Steroids. 2022 Nov;187:109093. doi: 10.1016/j.steroids.2022.109093. Epub 2022 Aug 24.
- Khalil M, Shanmugam H, Abdallah H, John Britto JS, Galerati I, Gómez-Ambrosi J, Frühbeck G, Portincasa P The Potential of the Mediterranean Diet to Improve Mitochondrial Function in Experimental Models of Obesity and Metabolic Syndrome..Nutrients. 2022 Jul 28;14(15):3112. doi: 10.3390/nu14153112.
- Oliveira JS, da Silva JA, de Freitas BVM, Alfenas RCG, Bressan J.A Mediterranean diet improves glycation markers in healthy people and in those with chronic diseases: a systematic review of clinical trials.Nutr Rev. 2024 May 8:nuae045. https://doi.org/10.1093/nutrit/nuae045. Online ahead of print.
- Greek National Dietary Guidelines for Adults. Available online: http://www.fao.org/nutrition/education/food- dietary- guidelines/regions/countries/greece/en/ (accessed on 25 July 2024).
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014, 129, S102–S138. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global database on body mass index. Accessed February 5, 2016. Available at: www.who.int/nutrition/databases/bmi/en/.
- Tanita Academy. Understanding your measurements. Available at: http:// tanita.eu/. Accessed May 25, 2018.
- Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: Insulin resistance and b-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985;28:412–9.
- Reddy Y., Murthy S., Krishna D., Prabhakar M.C. Role of Free Radicals and Antioxidants in Tuberculosis Patients. Indian J. Tuberc. 2004;51:213–218.
- Veskoukis A.S., Kyparos A., Paschalis V., Nikolaidis M.G. Spectrophotometric Assays for Measuring Redox Biomarkers in Blood. Biomarkers. 2016;21:208–217. doi: 10.3109/1354750X.2015.1126648.
- Janaszewska A., Bartosz G. Assay of Total Antioxidant Capacity: Comparison of Four Methods as Applied to Human Blood Plasma. Scand. J. Clin. Lab. Invest. 2002;62:231–236. doi: 10.1080/003655102317475498.
- Keles M.S., Taysi S., Sen N., Aksoy H., Akçay F. Effect of Corticosteroid Therapy on Serum and CSF Malondialdehyde and Antioxidant Proteins in Multiple Sclerosis. Can. J. Neurol. Sci. 2001;28:141–43. doi: 10.1017/S0317167100052823.
- Calder PC, Ahluwalia N, Brouns F et al.. Dietary factors and low-grade inflammation in relation to overweight and obesity. Br J Nutr. 2011;106 (Suppl. 3):S5–78. doi:10.1017/S0007114511005460.
- Emilio Ros E. , Martínez-González M , Estruch R , Salas-Salvadó JS, Montserrat M Fitó M , Martínez JA , Corella D Mediterranean diet and cardiovascular health: Teachings of the PREDIMED study Adv Nutr. 2014 May 14;5(3):330S-6S.
- Dai J, Jones DP, Goldberg J, Ziegler TR, Bostick RM, Wilson PW, Manatunga AK, Shallenberger L, Jones L, Vaccarino V. Association between adherence to the Mediterranean diet and oxidative stress. Am J Clin Nutr. 2008 Nov;88(5):1364-70.
- Fitó M, Guxens M, Corella D et al.; PREDIMED Study Investigators. Effect of a traditional Mediterranean diet on lipoprotein oxidation: a randomized controlled trial. Arch Intern Med. 2007;167:1195–1203. https://doi.org/10.1001/archinte.167.11.1195 [Google Scholar].
- Tosti V, Bertozzi B, Fontana L. Health Benefits of the Mediterranean Diet: Metabolic and Molecular Mechanisms. J Gerontol A Biol Sci Med Sci. 2018 Mar 2;73(3):318-326.
- Calabrese CM, Valentini A, Calabrese G. Gut Microbiota and Type 1 Diabetes Mellitus: The Effect of Mediterranean Diet. Front Nutr. 2021 Jan 13;7:612773.
- Widmer, R.J.; Flammer, A.J.; Lerman, L.O.; Lerman, A. The Mediterranean diet, its components, and cardiovascular disease. Am.J. Med. 2015, 128, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Hooper, L.V.; Littman, D.R.; Macpherson, A.J. Interactions between the microbiota and the immune system. Science 2012, 336, 1268–1273MD. [Google Scholar] [CrossRef] [PubMed]
- Zhou, N.; Gu, X.; Zhuang, T.; Xu, Y.; Yang, L.; Zhou, M. Gut Microbiota: A Pivotal Hub for Polyphenols as Antidepressants. J. Agric. Food. Chem. 2020, 68, 6007–6020. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg T, Abdellatif M, Schroeder S et al. Cardioprotection and lifespan extension by the natural polyamine spermidine. Nat Med. 2016;22:1428–1438. doi:10.1038/nm.4222.
- Alex E. Mohr, Carissa McEvoy, Dorothy D. Sears, Paul J. Arciero, Karen L. Sweazea,Impact of intermittent fasting regimens on circulating markers of oxidative stress in overweight and obese humans: A systematic review of randomized controlled trials,Advances in Redox Research, Volume 3, 2021, 100026.
- McAllister, MJ, Gonzalez, AE, and Waldman, HS. Impact of time restricted feeding on markers of cardiometabolic health and oxidative stress in resistance-trained firefighters. J Strength Cond Res 36(9): 2515-2522, 2022.
- Sutton EF, Beyl R, Early KS, Cefalu WT, Ravussin E, Peterson CM. Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes. Cell Metab. 2018 Jun 5;27(6):1212-1221.e3.
- Cienfuegos S, Gabel K, Kalam F, Ezpeleta M, Wiseman E, Pavlou V, Lin S, Oliveira ML, Varady KA. Effects of 4- and 6-h Time-Restricted Feeding on Weight and Cardiometabolic Health: A Randomized Controlled Trial in Adults with Obesity. Cell Metab. 2020 Sep 1;32(3):366-378.
- Wimalawansa SJ. Vitamin D Deficiency: Effects on Oxidative Stress, Epigenetics, Gene Regulation, and Aging. Biology (Basel). 2019 May 11;8(2):30.

| Orthodox nuns (n=50) | Lay women(n=50) | p | |
|---|---|---|---|
| Demographics | |||
| Age (years) | 42(36-50) | 38 (34-42) | 0.03 |
| Weight (kg) | 71.5(64-82) | 66(60-87) | 0.31 |
| BMI (kg/m2) | 27.0(24.2-29.0) | 26.8(22.0-32.0) | 0.19 |
| Body fat (%) | 24.5 ± 9.4 | 22.1 ± 8.1 | 0.23 |
| Lean body mass (%) | 39.9 ± 6.3 | 41.2 ± 7.1 | 0.15 |
| Waist circumference (cm) | 92.4 | 89.1 | 0.11 |
| Physical activity | |||
| Light | N = 9 | N = 7 | 0.31 |
| Moderate | N = 27 | N = 25 | 0.48 |
| Intense | N = 14 | N = 18 | 0.03 |
| Years of monasticism | 10.5 ± 9.8 - - | ||
| Deaconship of Orthodox Nuns | Baker(3);Botanist(2);Cook(5);Cooking assistant (5);Dining assistant (5); Ecclesiastical chanter (6); Gardener (3); Housekeeper (3); Iconographer (6); Laundry assistant (4); Pharmacist (2); | ||
| Energy (kcal) | 1565.9 ± 64.5 | 1890.0 ± 71.0 | <0.01 |
| Carbohydrates (g) | 159.6 ± 21.8 | 194.3 ± 23.4 | 0.03 |
| Protein (g) | 89.2 ± 1.3 | 72.3 ± 1.3 | 0.04 |
| Daily fat intake (g) | 21.0 ± 0.1 | 24.4 ± 0.6 | 0.02 |
| Daily saturated fat intake (g) | 12.7 ± 0.0 | 16.4 ± 0.0 | 0.01 |
| Total fibre intake (g) | 36.1 ± 0.8 | 24.2 ± 0.8 | 0.02 |
| 25-hydroxy-vitamin D3 (ng/Ml) | 15.7 (11.4-19.8) | 26.1 (18.2-31.9) | 0.02 |
| PTH (pg/ml) | 45.6(39.6-54.7) | 19.4(13.1-28.5) | <0.001 |
| Calcium (mg/dl) | 9.4 (9.1-9.7) | 9.1(8.8-9.3) | 0.15 |
| Insulin (IU/L) | 5.3 (3.4-6.7) | 7.1(4.7-11) | 0.02 |
| Fasting glucose (mg/dl) | 84.4 ± 10.1 | 89.2±9.7 | 0.43 |
| HOMA-IR | 1.02 ± 0.4 | 1.26 ± 0.7 | 0.21 |
| Oxidative status | |||
| TAC | 0.93(0.87-0.99) | 0.77 (0.65-0.90) | <.001 |
| GSH | 6.0(4.4-6.8) | 7.2(5.5-8.8) | 0.04 |
| TBARS | 7.3(5.8-8.3) | 7.6(6.9-8.4) | 0.28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



