
Submitted:
25 August 2024
Posted:
27 August 2024
You are already at the latest version
Abstract
Polycystic Ovarian Syndrome (PCOS) is a common endocrine condition that affects 8–13% of women of reproductive age and is one of the leading causes of anovulation and infertility. In Kazakhstan, the prevalence of this syndrome is particularly high compared to other countries and the global average. Currently, the diagnosis of polycystic ovarian syndrome is based on internationally established Rotterdam criteria, using hyperandrogenism, i.e. high testosterone levels, as a key parameter. These criteria are applied to diagnose PCOS in all female patients, although obese patients may have excess testosterone produced by adipose tissue. To avoid possible false PCOS diagnoses, an additional criterion could be considered to diagnose PCOS among obese women. Anti-Müllerian hormone (AMH) is promising as a more effective diagnostic criterion, since its level represents the state of the ovarian reserve and adipose tissue does not produce AMH. Therefore, the use of AMH instead of hyperandrogenism as a diagnostic criterion for PCOS among obese women might improve diagnostic precision and patient treatment. In this study, data on the levels of various hormonal indicators such as estrogen, progesterone, and others were analyzed for a large cohort of female patients with and without PCOS to explore possible correlations between these indicators, AMH, and testosterone. The findings suggest that the absence of a negative correlation between AMH and follicle-stimulating hormone (FSH), and a positive correlation of AMH with testosterone could support the use of AMH as a reliable additional criterion for PCOS diagnosis among obese women.
Keywords:
polycystic ovary syndrome (PCOS)
; obesity
; biomarker
; anti-Müllerian hormone (AMH)
; hyperandrogenism
1. Introduction
There are many studies indicating the negative effects of obesity on the reproductive health of women. Women with obesity are more likely to suffer from reproductive system disorders, including menstrual dysfunction, anovulation, infertility, difficulties in conception, and miscarriage [1]. Polycystic ovary syndrome (PCOS) is one of such pathologies, and its prevalence worldwide was estimated 276.35 per 100,000 with the number for Kazakhstan being significantly higher than worldwide and for many other countries - 417.23 per 100,00 [2]. The increased risk of PCOS is of particular importance, since 38-88% of women with PCOS suffer from overweight or obesity [3]. Furthermore, PCOS is associated with metabolic disruptions, an increased incidence of complications during pregnancy, infertility, endometrial carcinoma, diabetes mellitus, glucose intolerance, dyslipidemia, and cardiovascular disorders in the long run [4,5]. Therefore, it is crucial to determine an indicator that would allow the identification of women with obesity who are at a higher risk of developing PCOS. If such an indicator is identified, it would be possible to prevent the development of PCOS and start treatment as early as possible.
PCOS is characterized by a range of hormonal disruptions including decreased level of follicle-stimulating hormone (FSH) and increased level of luteinizing hormone (LH), abnormal gonadotropin-releasing hormone (GnRH) secretion, elevated serum androgens and insulin [6]. There are numerous symptoms and signs that make the process of PCOS diagnosis complicated. For example, oligo-anovulation, polycystic ovaries found by ultrasound investigation and hyperandrogenism have to be considered to diagnose PCOS currently [6]. Due to large number of these indicators, such identification can be complicated.
The level of anti-Müllerian hormone (AMH) is an indicator which has a high potential to facilitate this process. AMH is a peptide hormone that is synthesized in granulosa cells from an inert AMH precursor (proAMH) that can be further cleaved to yield a COOH-terminal dimer (AMHC; 25-kDa) and NH2-terminal dimer (AMHN; 120-kDa), which remain associated in a noncovalent complex form (AMHN,C) [7]. Both proAMH and complex AMHN,C can be present in the serum. AMH synthesis in granulosa cells begins with folliculogenesis and lasts till woman undergoes menopause [8]. Similar to other TGF-β family members, AMHC induces SMAD pathway in order to regulate stages of folliculogenesis and various neuroendocrine processes [9]. Hence, measuring AMH at any time of the menstrual cycle will give a complete clinical information necessary to assess the ovarian reserve [10]. Disruptions of the ovarian reserve caused by diseases of the female endocrine system will affect AMH levels. Particularly, many studies show that if a woman suffers from PCOS, the level of AMH in blood will be 2-3 times more than the normal level [11,12]. For this reason, the level of AMH can potentially reflect whether a woman with obesity is likely to develop PCOS.
One of the Rotterdam criteria used to diagnose PCOS is hyperandrogenism or excessive testosterone level. According to Wagner et al., ovaries and adrenal glands of women with obesity increase androgen production due to insulin resistance and hyperinsulinism. Moreover, Dr Wagner and her colleagues state that adipose tissue is the source of excess androgens in obese women since the androgen level in cohort with obesity was significantly higher than in the lean cohort [13]. Among premenopausal women adipose tissue is responsible for up to 50% of testosterone in serum [14]. This makes hyperandrogenism alone insufficient as a criterion to diagnose PCOS among obese women since not only PCOS but also obesity increases testosterone level. It may confuse doctors, allow incorrect PCOS diagnosis and prescription of wrong treatment.
Although there are many studies indicating higher risk of PCOS development in women with obesity, few studies focus on how to facilitate the process of PCOS diagnosis and identification of individuals who are more predisposed to develop PCOS. Necessity of such studies is highlighted by Malhorta et al. They conclude that elevated AMH levels correspond to more alarming metabolic, endocrinological and clinical criteria, thus making AMH useful in making treatment more personalized along with predicting responses to treatment and its outcomes [15]. Similarly, the study which focused on relationship between levels of AMH and other metabolic/hormonal substances in women with PCOS from Bangladesh noted the need in further studies. It states that more data is necessary to evaluate AMH potential [16]. Moreover, effectiveness of AMH in differentiation of PCOS phenotypes was indicated in the study by Ngyuen et al. [17]. Potential of AMH in differentiation of PCOS phenotypes shows that it can be potentially useful in assessing severity of disease and making prognosis. Therefore, the goal of this study is to identify if AMH or other biochemical criteria can be used as additional PCOS diagnostic criteria among obese women. Achieving this goal will help to make PCOS diagnosis more effective among patients with obesity to offer better treatment as early as possible. Moreover, AMH levels could be used to identify if a woman is under risk of PCOS development, thus allowing to offer her treatment and prevention therapies before PCOS develops.
2. Materials and Methods
The study involved 138 women who received medical consultations in the Department of Endocrinology at the Republican Diagnostic Center in the Republic of Kazakhstan. The study was conducted in accordance with the Declaration of Helsinki and approved by the 46th Ethics Committee of Republican Diagnostic Center (approval no. 0215PK02290). Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper. The women aged between 18 and 35 years were included in the study, while the women with clinically significant oncologic or cardiovascular diseases, hypertensive disease of stages 2–3, congenital disorders of lipid metabolism, pregnancy, lactation, smoking habits, and menopause were excluded from the study (Figure 1). One group of non-obese participants without PCOS was recruited as a control group (n = 46). The obese women’s body mass index (BMI) exceeded 30 kg/m2. They were divided into two groups based on the diagnosis of PCOS: 25 of them were designated to the group with PCOS (n = 25), and the remaining 67 were designated to the group without PCOS (n = 67) based on their diagnosis.
PCOS diagnosis was accomplished based on the Rotterdam Consensus of the European Experts. A woman is diagnosed with PCOS if she has any two of the following symptoms: 1) irregular menses (IM) (≤ 6 per year), oligoovulation, and/or anovulation; 2) excess androgen activity and secretion (hirsutism, acne) and/or biochemical hyperandrogenism; 3) typical changes on gynecologic ultrasound (≥ 12 follicles sized 2-9 mm).
Further investigation was based on the data obtained via the methods described below.
- 1)
- Survey of patients: this was conducted to collect anamnestic data to assess health and heredity.
- 2)
- Anthropometric data: measurements included height, weight, waist circumference, hip circumference, and blood pressure. The body mass index (BMI) was calculated using Quetelet’s index formula: weight (kg) / height (m2). Obesity was considered abdominal when the ratio of waist to hip measurement (WM/HM) in women was more than 0.8.
- 3)
-
Laboratory indicators:
- a.
- Lipid profile: total cholesterol and triglycerides were measured by the enzymatic colorimetric method using the COBAS INTEGRA analyzer (Roche Diagnostics, Basel, Switzerland). Low-density lipoproteins (LDL) and high-density lipoproteins (HDL) were measured by the homogeneous enzymatic colorimetric method using the Roche/Hitachi cobas c analyzer (Roche Diagnostics, Basel, Switzerland).
- b.
- Fasting glucose level: measured by the standard enzymatic method using the Roche/Hitachi cobas c analyzer (Roche Diagnostics, Basel, Switzerland).
- c.
- Glycated hemoglobin (HbA1c): measured by turbidimetric inhibition immunoassay using a Roche analyzer (Roche Diagnostics, Basel, Switzerland).
- d.
- Hormone levels: levels of thyrotropic hormone, prolactin, estrogens, progesterone, follicle-stimulating hormone (FSH), luteinizing hormone (LH), testosterone, and insulin were measured by Eclia electrochemiluminescence immunoassay using the Elecsys and cobas e analyzer (Beckman Coulter, Inc., Brea, CA, USA). The level of anti-Müllerian hormone (AMH) was measured by ELISA. Levels of adiponectin and resistin were measured by the ELISA method using specific monoclonal antibodies.
- 4)
- Ultrasound investigations (U/S): these were carried out on the seventh day of the menstrual cycle using the Logiq E9 (GE HealthCare, Chicago, IL, USA) with ML6-15 Mhz linear array transducer and IС 5-9 Mhz transvaginal curvilinear transducer. The investigations included 250 pelvic ultrasounds, 250 thyroid ultrasounds, and 250 breast ultrasounds.
The power calculation was performed using G*Power 3.1.9.7 software. With an effect size of 0.8 and a sample size of 25 participants in the PCOS group, the power was 0.92 for the group comparison analysis and 0.99 for the correlational analysis. Statistical data were analyzed using GraphPad Prism 10 software (GraphPad Software, San Diego, CA, USA) and Microsoft Excel (Microsoft Corporation, Redmond, WA, USA). The normality of the data distribution was tested using the D’Agostino-Pearson criterion. The Kruskal-Wallis nonparametric test and post-hoc Dunn’s test were used to compare median values of the indicators among the control group and obese women with and without PCOS. Descriptive statistical data, as well as the results of the Kruskal-Wallis nonparametric test and post-hoc Dunn’s test, are summarized in Supplementary Table S1. Two-tailed Spearman’s correlation analysis was used to relate the level of AMH in the blood to other hormonal parameters (for the AMH – Testosterone correlation analysis in obese PCOS patients, a one-tailed Spearman’s test was used, as we hypothesized a positive correlation based on data suggesting that in PCOS, elevated testosterone stimulates the production of AMH [18]). ROC analysis was used to test the specificity and sensitivity of AMH as a biomarker for PCOS diagnosis. A p-value of less than 0.05 was considered statistically significant.
3. Results
3.1. General Parameters
There is no statistically significant difference in age between the control group and obese women with or without PCOS, as only women below 36 years of age were included in this study (ANOVA: p > 0.05; Figure 2A).
BMI is a general parameter that differs between patients from the control group and those with obesity and PCOS (Figure 2B). There is no statistical difference in BMI between obese female patients without PCOS and those with PCOS. However, a significant difference exists between the control group and obese women who do not suffer from PCOS. The significance level is nearly the same for these two differences in BMI (p < 0.0001).
3.2. Hormonal Parameters
Statistically significant differences in AMH serum concentrations are found between all groups (Figure 3A). Significance is lower for the difference between the control group and obese women with PCOS, although other differences are similar in significance.
Testosterone serum concentrations are significantly different between patients from the control group and obese patients with PCOS (Figure 3B). A difference of the same significance level is identified between obese patients without PCOS and those with PCOS. No significant difference is found between the control group and obese women who are not diagnosed with PCOS.
Likewise, FSH levels are significantly different between the control group and obese patients with PCOS (Figure 3C). This parameter is different between obese female patients who do not suffer from PCOS and women who suffer from both obesity and PCOS, but the significance level is lower.
The next parameter with statistically significant differences between the groups is LH (Figure 3D). Serum levels of LH for women with obesity and PCOS are different from both the control group and obese women without PCOS. However, the difference from the latter group is of higher significance than the difference from the control group. No difference is found between women from the control group and obese patients without PCOS.
The control group and obese women without PCOS are statistically different in estradiol levels (Figure 3F). No other significant differences are found between the groups.
The control group and obese patients without PCOS are also different in insulin levels (Figure 3I). The control group is also different from obese women suffering from PCOS, but obese women without PCOS and those with PCOS are significantly different.
Similarly, the adiponectin serum concentration of the control group is significantly different from the other two groups (Figure 3J). No significant difference is found between obese women without PCOS and those with PCOS.
Resistin serum levels are statistically different between the control group and obese patients without PCOS (Figure 3K). A difference is also identified between the control group and obese patients suffering from PCOS, but with a lower significance level. Groups with obesity are not statistically different in resistin levels.
The AMH level in the blood was further analyzed for its specificity and sensitivity for being used as a biomarker for PCOS diagnosis and was found to be highly reliable for this purpose (area under curve = 0.9069; p < 0.0001; Figure 4).
3.3. Metabolic Parameters
Glucose median levels in the blood were found to be significantly elevated in the blood of obese women regardless of the PCOS diagnosis compared to controls (Figure 5A).
The level of glycated hemoglobin is not different between the groups (Figure 4B).
Regarding cholesterol serum concentration, the only statistically significant difference is found between the control group and obese women who are not diagnosed with PCOS (Figure 5C).
A statistically significant difference in HDL levels exists between all three groups (Figure 5D). Even though the significance level is similar for the difference between the control group and the other two groups, the difference between the groups with obesity is less significant.
LDL serum levels were found to be increased in obese patients compared to control and are not statistically different from each other (Figure 5E).
Similarly, the triacylglycerol blood level is higher in obese women compared to control, and no significant difference exists between the groups with obesity (Figure 5F).
3.4. Correlation between AMH and Some Hormonal Parameters
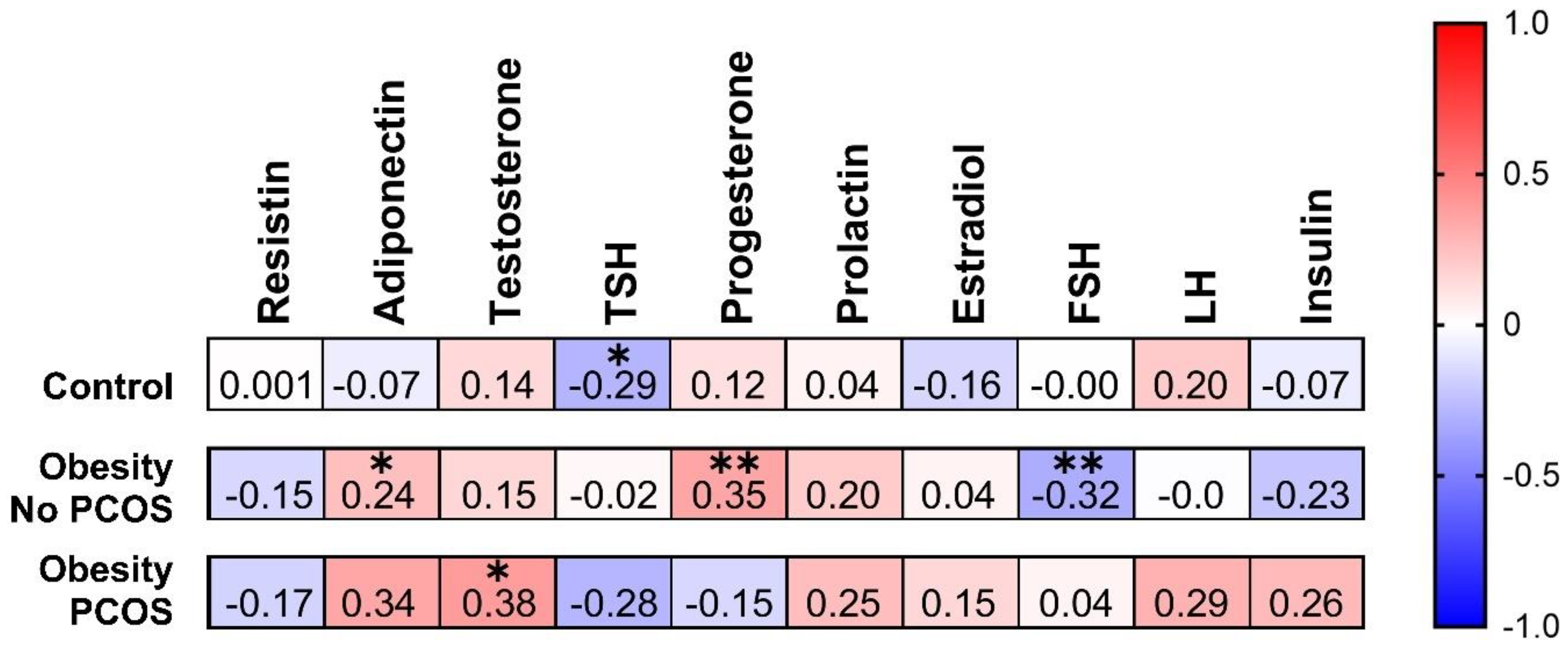
A statistically significant negative correlation can be observed between AMH and TSH in the control group (Figure 6). Another significant negative correlation can be noted
between AMH and FSH among obese women without PCOS.
As for positive correlations, one can be noted between AMH and adiponectin among overweight women without PCOS. Similarly, there is positive correlation between AMH and progesterone in the same group. One more positive correlation is noticed between AMH and testosterone for the obese women suffering from PCOS.
4. Discussion
The Rotterdam criteria include hyperandrogenism as one of the factors used to differentiate women with PCOS from those without PCOS. Secretion of testosterone by excessive adipose tissue may hinder reliability of it as an independent diagnostic criterion. Moreover, obesity induces considerable changes in the interplay between different metabolic and hormonal parameters. Therefore, there is a need to introduce additional criterion of PCOS diagnosis among obese women. There is a significant correlation between AMH and testosterone among obese women suffering from PCOS. Furthermore, changes in normal interplay between hormonal parameters induced by obesity are represented by correlations between AMH and other hormonal parameters such as TSH, adiponectin, progesterone and FSH. According to Lv et al., women suffering from PCOS at a young age exhibit symptoms such as high testosterone levels and chronic anovulation, whereas older women primarily experience disruptions in metabolic parameters, obesity, and insulin resistance [22]. The results of our study show that obese women with PCOS are significantly younger than obese women without PCOS. Additionally, there are differences in metabolic parameters between these two groups, including cholesterol and HDL levels. Using AMH as a criterion in addition to testosterone would help to differentiate changes in hormonal status of patients caused by obesity along with age and changes induced by PCOS.
One of the possible explanations for this could be disruptions in regulation of AMH expression which is mediated by testosterone. Dilaver et al. (2019) suggested that testosterone is converted to estradiol by aromatase [18]. Estradiol affects ERβ receptors, thus reducing AMH level. In addition, precursor of testosterone called dihydrotestosterone directly impedes pathways of AMH synthesis. In patients with PCOS increased expression of Erα receptors alters the receptor ratio necessary for this mechanism and elevates AMH level. Furthermore, extremely high levels of dihydrotestosterone often discovered among PCOS patients induce dose-related increase in AMH synthesis. The results of their in vitro experiments confirmed that these interactions indeed could take place, even though more studies are needed to make this model more reliable. The results of our study support this finding because positive correlation was observed between AMH and testosterone in PCOS group, while there is no significant correlation in other groups.
The results of many studies suggest that PCOS does not affect the correlation between AMH and FSH. High FSH levels inhibit AMH secretion in infantile mice and cows [19,20]. The results of our study suggest that there is no negative correlation between FSH and AMH in obese women suffering from PCOS and healthy control group, as the Spearman coefficients are not significant. Meanwhile, significant negative correlation was found between AMH and FSH for obese women without PCOS.
To explain this correlation, numerous studies investigated the interaction between AMH and FSH. One of the studies states that factors GDF9 and BMP15 from oocytes are involved in regulation of AMH in granulosa cells synthesizing it. In particular, these factors stimulate p300-mediated acetylation of histones in nuclei of granulosa cells by cooperating with Smad2/3 and PI3K/Akt signaling. As a result, the genes involved in AMH synthesis are expressed since access to DNA becomes easier. Repression of this pathway is realized by Gonadotropin-Inducible Ovarian Transcription Factor 1 (GIOT1) belonging to a family of zinc-finger proteins. GIOT1 has Krüppel-associated box A domain that functions as repressor of transcription which can directly interact with either/both Smad2/3 and p300. Moreover, GIOT1 expands another protein with repressor functions called HDAC2. This mechanism also mediates inhibition of AMH expression by FSH [21]. The inhibition typically results in a negative correlation between these two hormones.
Our findings partially correspond with this mechanism because there is significant negative correlation between AMH and FSH among obese women without PCOS. Absence of this correlation in PCOS group could be due to hormonal disbalance observed in these patients. Such disbalance could lead to prevalence of other mechanisms of AMH regulation. Therefore, further studies are needed to investigate how PCOS disrupts FSH-mediated inhibition of AMH. One more discrepancy is that no significant correlation of these substances was found for healthy control subjects. This highlights the need in further investigations of other hormonal mechanisms involved in AMH regulation. Despite these discrepancies, AMH remains consistently high in patients suffering from PCOS. Hence, it can be concluded that AMH is useful marker of diagnosing PCOS. Obesity can disrupt either the expression or the effect of GDF9 and BMP15 factors, leading to the absence of a correlation between AMH and FSH.
Estradiol levels are usually low in women suffering from PCOS. In a study by Masjedi and colleagues, a cohort of women with PCOS had significantly lower estradiol levels compared to healthy women [23]. Among women with obesity or excess weight, estradiol levels were found to be lower than in women without obesity, regardless of other factors like age, smoking, and race [14]. Although the mechanism explaining the relationship between low estradiol and obesity is not fully understood, it is clear that disruptions in estradiol metabolism are involved in the causation of obesity in women. AMH mediated inhibition of aromatase enzyme that converts testosterone to estradiol can be one of the possible explanations, as it was described in the previous paragraph. The results of this study partly align with expectations, as female obese patients without PCOS had significantly lower estradiol levels than normal-weight women. The unexpected finding was that women with both PCOS and obesity had estradiol levels almost the same as the control cohort. Even though the mechanism underlying this observation is unclear, the existence of an interplay between obesity and PCOS is supported by this finding. It also helps to address the goal of this study, as such inconsistency makes estradiol an inappropriate indicator of PCOS among obese women.
Resistin and adiponectin are two important adipokines secreted by the adipose tissue. They act like hormones and play an important role in regulating metabolic activity. Numerous studies showed a possible association of resistin and adiponectin with obesity and PCOS. In our study, serum levels of resistin were found to be significantly increased in the obese subjects (p < 0.0001) and in PCOS patients (p < 0.01) when compared to controls, whereas adiponectin was found to be significantly lower (p < 0.0001) in both obesity and PCOS. There was no significant difference in both adiponectin and resistin levels between obese and PCOS groups. At least two studies support our findings. Seow et al. (2004) reported an over-expression of resistin in obesity and PCOS patients and suggested that resistin could be a contributing factor to the pathogenesis of PCOS [24]. Hu et al. (1996) showed that the expression of adiponectin mRNA was significantly reduced in obesity [25]. To address the possible association between these two adipokines and PCOS, Nambiar et al. (2016) analyzed the genetic polymorphisms of adiponectin and resistin and found that serum adiponectin and resistin levels were significantly correlated with BMI, but not with PCOS [26].
The positive correlation between AMH and adiponectin, as well as the reduced level of AMH in women with obesity without PCOS, suggests that excessive adipose tissue typically suppresses AMH secretion. Some previous research reports that obesity may negatively impact AMH levels [27]. However, since there is no such correlation in patients with both PCOS and obesity, and they exhibit excessive AMH levels, it appears that the suppression of AMH by adipose tissue can be disrupted by PCOS. This further supports the hypothesis that normal ranges of biochemical indicators cannot be used to diagnose reproductive diseases in women with obesity. Obesity may exacerbate disruptions caused by reproductive diseases to such an extent that normal ranges of biochemical indicators do not show deviations characteristic of a particular disease.
Another biochemical criterion affected by PCOS is progesterone level. Numerous studies report that progesterone levels are decreased among women who suffer from PCOS. Research conducted by Estienne and his colleagues reveals that women of normal weight who were diagnosed with PCOS had lower progesterone levels than women without PCOS [28]. Also, the study by Daghestani and his colleagues found that a cohort diagnosed with PCOS had progesterone levels approximately five times lower than those in the control group [29]. Surprisingly, in this research, there was no significant difference in progesterone levels between women with obesity and PCOS and the healthy control group. In contrast, women with obesity without PCOS had lower progesterone levels. This finding indicates that progesterone is affected by both obesity and PCOS, making it inappropriate as an indicator of PCOS among obese women. Furthermore, there is a significant positive correlation between AMH and progesterone among women with obesity without PCOS. Since this tendency is not observed in both control and PCOS groups, it is likely that hormonal disruptions induced by obesity alone can interfere with the normal interplay between AMH and progesterone metabolic pathways.
As to the negative correlation between AMH and TSH in healthy control group, this finding coincides with previous studies. Decrease in levels of TSH along with decline in number of antral follicles produced were observed in one of the studies [30]. Since antral and pre-antral follicles secrete AMH [31], it is rational to expect that healthy subjects will have inverse relationship between these two substances.
Regarding LH, numerous studies report elevated blood levels of this hormone in women who suffer from PCOS. According to a study conducted by Ambiger and colleagues, LH levels were elevated among women diagnosed with PCOS compared to healthy women [32]. One possible mechanism behind this phenomenon could be constant disruptions in estrogen and progesterone levels, which impair the function of the hypothalamic pulse generator. This leads to the pituitary gland becoming excessively sensitive to gonadotropin-releasing hormone (GnRH) or changes in the secretion patterns of GnRH, resulting in elevated LH levels [33]. Similar findings are reported in the study by Shrivastava and Conigliaro, which states that hyperinsulinemia partially leads to PCOS by elevating LH and GnRH levels through its influence on both the pituitary gland and hypothalamus [34].
The results of our study confirm elevations in LH blood concentration. However, it is interesting to note that many obese women who do not suffer from PCOS also had elevated LH concentrations, suggesting that obesity disrupts the regulation of LH secretion, which may lead to symptoms resembling PCOS in obese women. However, there were no statistically significant differences in blood LH levels between obese women with PCOS and those without PCOS. Therefore, LH levels cannot be used as a criterion to diagnose PCOS.
In general, the results of this study support the hypothesis made at the beginning of the research. Indicators other than AMH and testosterone mostly do not coincide with expectations for women with either PCOS or obesity, suggesting that obesity and PCOS interfere with normal metabolism and disrupt biochemical indicators. Such extreme disruption of indicators complicates the diagnosis of reproductive system diseases. Therefore, there is a need for the introduction of an additional biochemical criterion that allows accurate and consistent diagnosis of reproductive disorders. For PCOS in particular, AMH showed consistency as it was high only among women with both obesity and PCOS. Hence, AMH appears to be a more appropriate additional biochemical criterion for PCOS diagnosis compared to other biochemical indicators. However, more studies are needed on the metabolic relationship between obesity and PCOS to assess the relevance of AMH in this role.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Statistical parameters including median, lower quartile, upper quartile, Kruskal-Wallis nonparametric test indicators and post-hoc Dunn’s test indicators.
Author Contributions
Conceptualization, A.D. and T.T.; methodology, M.M. and A.D.; formal analysis, M.M., A.D. and A.T.; investigation, M.M. and A.D.; resources, A.D.; data curation, M.M., A.D. and A.T.; writing—original draft preparation, M.M. and A.D.; writing—review and editing, M.M., A.T., B.A. and T.T.; visualization, M.M., A.T. and B.A; supervision, T.T.; project administration, T.T.; funding acquisition, A.D. and T.T. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the 46th Ethics Committee of Republican Diagnostic Center (approval no. 0215PK02290).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
All data supporting the findings of this study can be made available to researchers upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
AMH, anti-Müllerian hormone; BMI, body mass index; FSH, follicle-stimulating hormone; GnRH, gonadotropin-releasing hormone; LH, luteinizing hormone; PCOS, polycystic ovary syndrome; TSH, thyroid-stimulating hormone
References
- Silvestris, E.; de Pergola, G.; Rosania, R.; Loverro, G. Obesity as disruptor of the female fertility. Reprod. Biol. Endocrinol. 2018, 16, 22. [Google Scholar] [CrossRef]
- Miazgowski, T.; Martopullo, I.; Widecka, J.; Miazgowski, B.; Brodowska, A. National and regional trends in the prevalence of polycystic ovary syndrome since 1990 within Europe: the modeled estimates from the Global Burden of Disease Study 2016. Arch. Med. Sci. 2021, 17, 343–351. [Google Scholar] [CrossRef]
- Barber, T.M.; Dimitriadis, G.K.; Andreou, A.; Franks, S. Polycystic ovary syndrome: insight into pathogenesis and a common association with insulin resistance. Clin. Med. 2016, 16, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Christ, J.P.; Cedars, M.I. Current guidelines for diagnosing PCOS. Diagnostics (Basel) 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wu, Q.; Hao, Y.; Jiao, M.; Wang, X.; Jiang, S.; Han, L. Measuring the global disease burden of polycystic ovary syndrome in 194 countries: Global Burden of Disease Study 2017. Hum. Reprod. 2021, 36, 1108–1119. [Google Scholar] [CrossRef] [PubMed]
- De Leo, V.; Musacchio, M.C.; Cappelli, V.; Massaro, M.G.; Morgante, G.; Petraglia, F. Genetic, hormonal and metabolic aspects of PCOS: an update. Reprod. Biol. Endocrinol. 2016, 14, 38. [Google Scholar] [CrossRef]
- Pankhurst, M.W.; McLennan, I.S. Human blood contains both the uncleaved precursor of anti-Mullerian hormone and a complex of the NH2- and COOH-terminal peptides. Am. J. Physiol. Endocrinol. Metab. 2013, 305, E1241–E1247. [Google Scholar] [CrossRef]
- Moolhuijsen, L.M.E.; Visser, J.A. Anti-Müllerian Hormone and Ovarian Reserve: Update on Assessing Ovarian Function. J. Clin. Endocrinol. Metab. 2020, 105, 3361–3373. [Google Scholar] [CrossRef]
- di Clemente, N.; Racine, C.; Pierre, A.; Taieb, J. Anti-Müllerian hormone in female reproduction. Endocr. Rev. 2021. [Google Scholar] [CrossRef] [PubMed]
- La Marca, A.; Giulini, S.; Tirelli, A.; Bertucci, E.; Marsella, T.; Xella, S.; Volpe, A. Anti-Müllerian hormone measurement on any day of the menstrual cycle strongly predicts ovarian response in assisted reproductive technology. Hum. Reprod. 2007, 22, 766–771. [Google Scholar] [CrossRef] [PubMed]
- Pigny, P.; Merlen, E.; Robert, Y.; Cortet-Rudelli, C.; Decanter, C.; Jonard, S.; Dewailly, D. Elevated serum level of anti-mullerian hormone in patients with polycystic ovary syndrome: relationship to the ovarian follicle excess and to the follicular arrest. J. Clin. Endocrinol. Metab. 2003, 88, 5957–5962. [Google Scholar] [CrossRef] [PubMed]
- Cook, C.L.; Siow, Y.; Brenner, A.G.; Fallat, M.E. Relationship between serum müllerian-inhibiting substance and other reproductive hormones in untreated women with polycystic ovary syndrome and normal women. Fertil. Steril. 2002, 77, 141–146. [Google Scholar] [CrossRef]
- Wagner, I.V.; Savchuk, I.; Sahlin, L.; Kulle, A.; Klöting, N.; Dietrich, A.; Holterhus, P.-M.; Dötsch, J.; Blüher, M.; Söder, O. De Novo and Depot-Specific Androgen Production in Human Adipose Tissue: A Source of Hyperandrogenism in Women with Obesity. Obes. Facts 2022, 15, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.J.; Perfetti, T.A.; Hayes, A.W.; Berry, S.C. Obesity as a source of endogenous compounds associated with chronic disease: A review. Toxicol. Sci. 2020, 175, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, N.; Mahey, R.; Cheluvaraju, R.; Rajasekaran, K.; Patkar, D.; Prabhakar, P.; Rajput, M.; Upadhyay, A. Serum Anti-Mullerian Hormone (AMH) Levels Among Different PCOS Phenotypes and Its Correlation with Clinical, Endocrine, and Metabolic Markers of PCOS. Reprod. Sci. 2023, 30, 2554–2562. [Google Scholar] [CrossRef]
- Aalpona, F.Z.; Ananya, K.F.; Kamrul-Hasan, A.B. Correlation of Serum Anti-Mullerian Hormone with Clinical, Metabolic and Hormonal Parameters in Bangladeshi Women with Polycystic Ovary Syndrome: A Cross-sectional Study. Mymensingh Med. J. 2023, 32, 606–612. [Google Scholar]
- Nguyen, M.T.; Krishnan, S.; Phatak, S.V.; Karakas, S.E. Anti-Mullerian Hormone-Based Phenotyping Identifies Subgroups of Women with Polycystic Ovary Syndrome with Differing Clinical and Biochemical Characteristics. Diagnostics (Basel) 2023, 13. [Google Scholar] [CrossRef]
- Dilaver, N.; Pellatt, L.; Jameson, E.; Ogunjimi, M.; Bano, G.; Homburg, R.; D Mason, H.; Rice, S. The regulation and signalling of anti-Müllerian hormone in human granulosa cells: relevance to polycystic ovary syndrome. Hum. Reprod. 2019, 34, 2467–2479. [Google Scholar] [CrossRef]
- Dewailly, D.; Robin, G.; Peigne, M.; Decanter, C.; Pigny, P.; Catteau-Jonard, S. Interactions between androgens, FSH, anti-Müllerian hormone and estradiol during folliculogenesis in the human normal and polycystic ovary. Hum. Reprod. Update 2016, 22, 709–724. [Google Scholar] [CrossRef]
- Devillers, M.M.; Petit, F.; Cluzet, V.; François, C.M.; Giton, F.; Garrel, G.; Cohen-Tannoudji, J.; Guigon, C.J. FSH inhibits AMH to support ovarian estradiol synthesis in infantile mice. J. Endocrinol. 2019, 240, 215–228. [Google Scholar] [CrossRef]
- Roy, S.; Gandra, D.; Seger, C.; Biswas, A.; Kushnir, V.A.; Gleicher, N.; Kumar, T.R.; Sen, A. Oocyte-Derived Factors (GDF9 and BMP15) and FSH Regulate AMH Expression Via Modulation of H3K27AC in Granulosa Cells. Endocrinology 2018, 159, 3433–3445. [Google Scholar] [CrossRef]
- Lv, P.-P.; Jin, M.; Rao, J.-P.; Chen, J.; Wang, L.-Q.; Huang, C.-C.; Yang, S.-Q.; Yao, Q.-P.; Feng, L.; Shen, J.-M.; Feng, C. Role of anti-Müllerian hormone and testosterone in follicular growth: a cross-sectional study. BMC Endocr. Disord. 2020, 20, 101. [Google Scholar] [CrossRef] [PubMed]
- Masjedi, F.; Keshtgar, S.; Agah, F.; Karbalaei, N. Association Between Sex Steroids and Oxidative Status with Vitamin D Levels in Follicular Fluid of Non-obese PCOS and Healthy Women. J. Reprod. Infertil. 2019, 20, 132–142. [Google Scholar] [PubMed]
- Seow, K.-M.; Juan, C.-C.; Wu, L.-Y.; Hsu, Y.-P.; Yang, W.-M.; Tsai, Y.-L.; Hwang, J.-L.; Ho, L.-T. Serum and adipocyte resistin in polycystic ovary syndrome with insulin resistance. Hum. Reprod. 2004, 19, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Hu, E.; Liang, P.; Spiegelman, B.M. AdipoQ is a novel adipose-specific gene dysregulated in obesity. J. Biol. Chem. 1996, 271, 10697–10703. [Google Scholar] [CrossRef]
- Nambiar, V.; Vijesh, V.V.; Lakshmanan, P.; Sukumaran, S.; Suganthi, R. Association of adiponectin and resistin gene polymorphisms in South Indian women with polycystic ovary syndrome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 200, 82–88. [Google Scholar] [CrossRef]
- Oldfield, A.L.; Kazemi, M.; Lujan, M.E. Impact of Obesity on Anti-Mullerian Hormone (AMH) Levels in Women of Reproductive Age. J. Clin. Med. 2021, 10. [Google Scholar] [CrossRef]
- Estienne, A.; Mellouk, N.; Bongrani, A.; Plotton, I.; Langer, I.; Ramé, C.; Petit, C.; Guérif, F.; Froment, P.; Dupont, J. Involvement of chemerin and CMKLR1 in the progesterone decrease by PCOS granulosa cells. Reproduction 2021, 162, 427–436. [Google Scholar] [CrossRef]
- Daghestani, M.H.; Daghestani, M.H.; Warsy, A.; El-Ansary, A.; Omair, M.A.; Omair, M.A.; Hassen, L.M.; Alhumaidhi, E.M.; Al Qahtani, B.; Harrath, A.H. Adverse effects of selected markers on the metabolic and endocrine profiles of obese women with and without PCOS. Front Endocrinol (Lausanne) 2021, 12, 665446. [Google Scholar] [CrossRef]
- Liang, Z.; Xu, Z.; Liu, J. Mendelian randomization study of thyroid function and anti-Müllerian hormone levels. Front Endocrinol (Lausanne) 2023, 14, 1188284. [Google Scholar] [CrossRef]
- Jeppesen, J.V.; Anderson, R.A.; Kelsey, T.W.; Christiansen, S.L.; Kristensen, S.G.; Jayaprakasan, K.; Raine-Fenning, N.; Campbell, B.K.; Yding Andersen, C. Which follicles make the most anti-Mullerian hormone in humans? Evidence for an abrupt decline in AMH production at the time of follicle selection. Mol. Hum. Reprod. 2013, 19, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Ambiger, S.; B. Patil, S.; M., R.; Dhananjaya, S. Role of leutenising hormone LH and insulin resistance in polycystic ovarian syndrome. Int. J. Reprod. Contracept. Obstet. Gynecol. 2017, 6, 3892. [Google Scholar] [CrossRef]
- Johansson, J.; Stener-Victorin, E. Polycystic ovary syndrome: effect and mechanisms of acupuncture for ovulation induction. Evid. Based Complement. Alternat. Med. 2013, 2013, 762615. [Google Scholar] [CrossRef]
- Shrivastava, S.; Conigliaro, R.L. Polycystic Ovarian Syndrome. Med. Clin. North Am. 2023, 107, 227–234. [Google Scholar] [CrossRef]
Figure 1.
Flow chart representing the selection of patients for the control group (n = 46), obese patients without polycystic ovary syndrome (no PCOS: n = 67), and obese patients with polycystic ovary syndrome (PCOS: n = 25).
Figure 1.
Flow chart representing the selection of patients for the control group (n = 46), obese patients without polycystic ovary syndrome (no PCOS: n = 67), and obese patients with polycystic ovary syndrome (PCOS: n = 25).
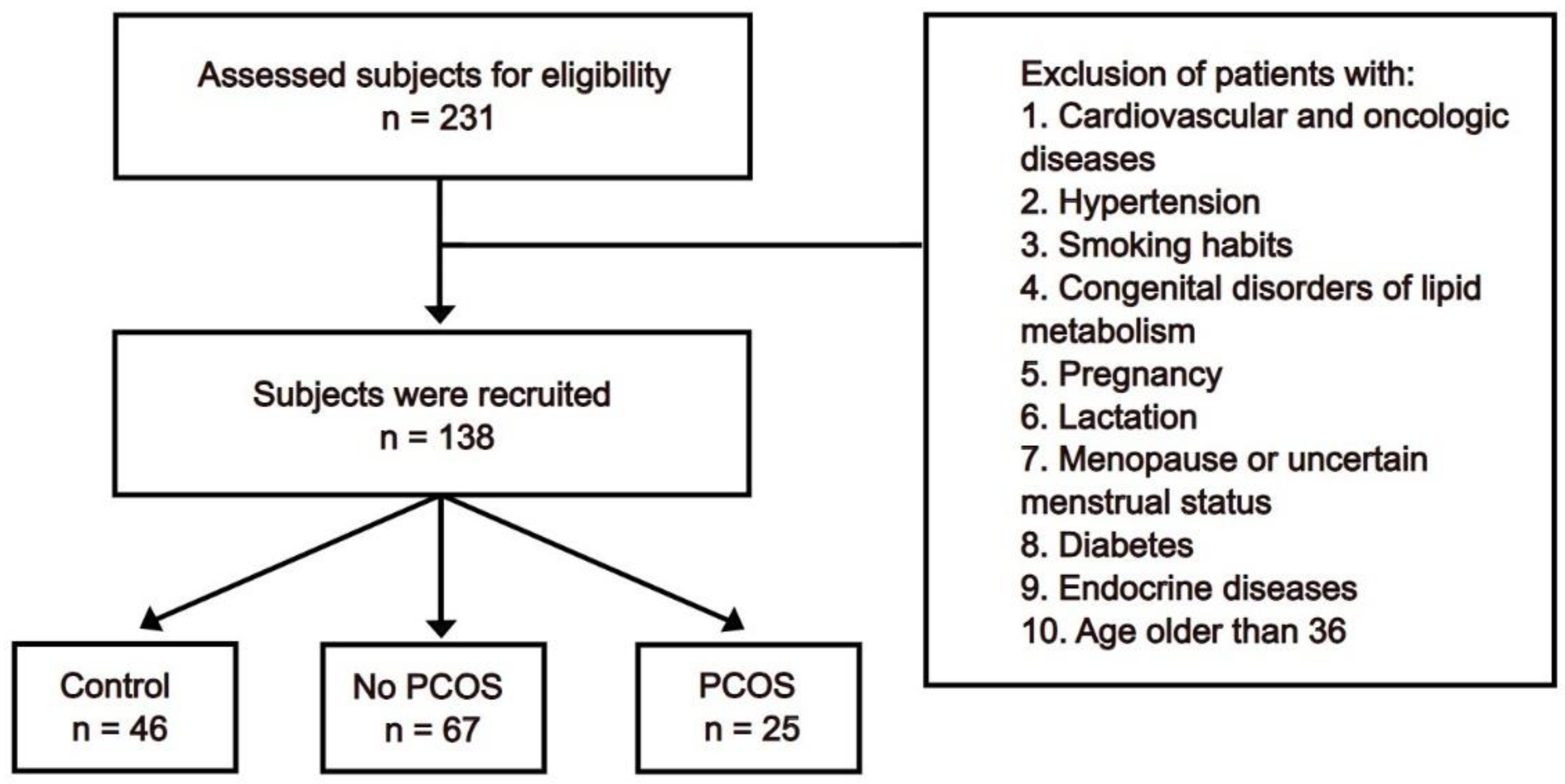
Figure 2.
Comparison between control group (n = 46) and study groups (obese group with or without PCOS (PCOS: n = 25; no PCOS: n = 67)) in terms of age and body mass index (BMI). (A) age; (B) BMI. Kruskal-Wallis nonparametric test and post hoc Dunn’s test. **** p < 0.0001. Median and IQR.
Figure 2.
Comparison between control group (n = 46) and study groups (obese group with or without PCOS (PCOS: n = 25; no PCOS: n = 67)) in terms of age and body mass index (BMI). (A) age; (B) BMI. Kruskal-Wallis nonparametric test and post hoc Dunn’s test. **** p < 0.0001. Median and IQR.
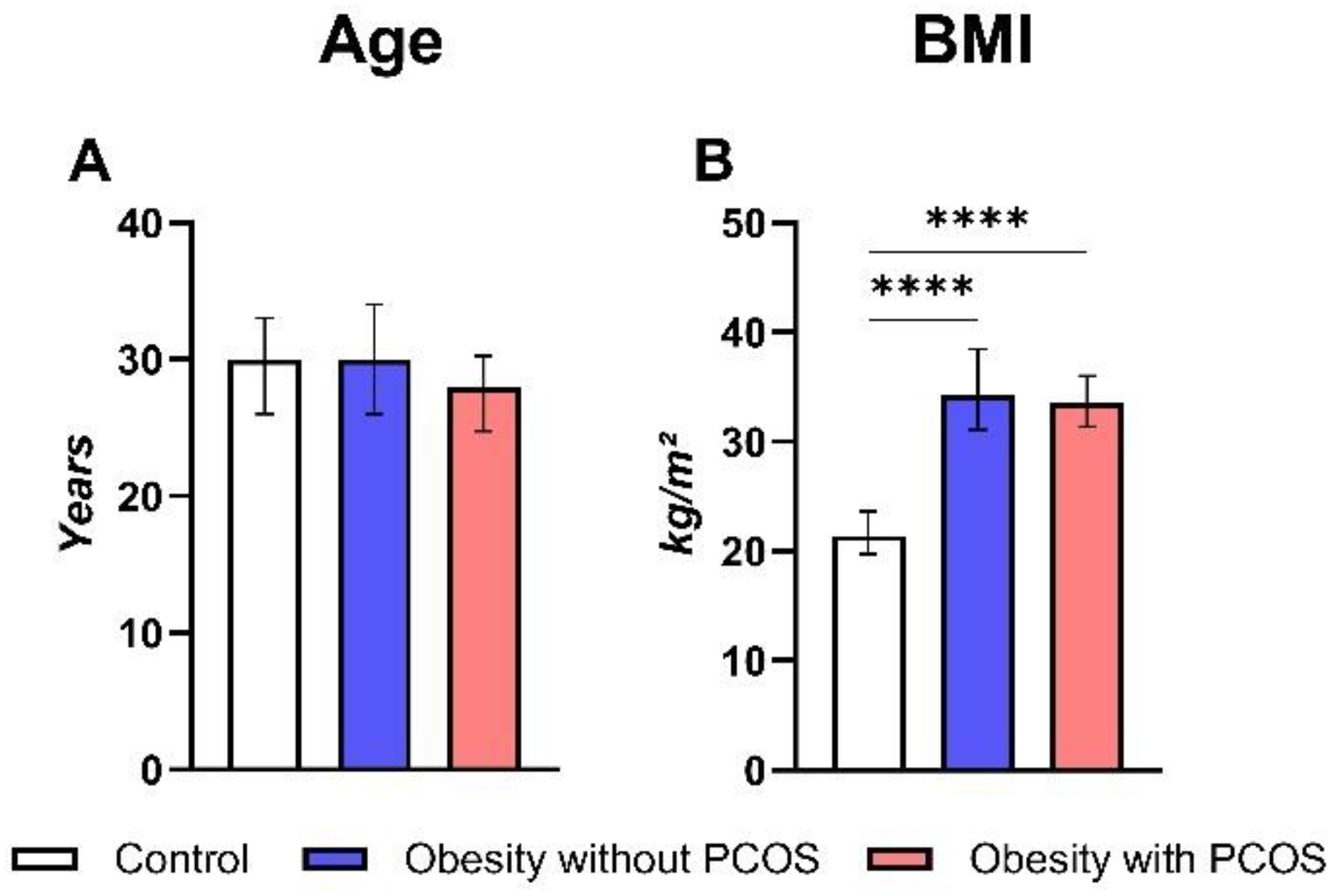
Figure 3.
Comparison between control group (n = 46) and study groups (obese group with or without PCOS (PCOS: n = 25; no PCOS: n = 67)) in terms of serum levels of hormones. (A) serum anti-Müllerian hormone (AMH) protein concentration; (B) serum testosterone protein concentration; (C) serum follicle-stimulating hormone (FSH) level of enzymatic activity; (D) serum luteinizing hormone (LH) level of enzymatic activity; (E) serum thyroid-stimulating hormone (TSH) level of enzymatic activity; (F) serum estradiol protein concentration; (G) serum progesterone protein concentration; (H) serum prolactin protein concentration; (I) serum insulin level of enzymatic activity; (J) serum adiponectin protein concentration; (K) serum resistin protein concentration. Kruskal-Wallis nonparametric test and post hoc Dunn’s test. * p < 0.05, ** p < 0.01, *** p < 0.001, **** p < 0.0001. Median and IQR.
Figure 3.
Comparison between control group (n = 46) and study groups (obese group with or without PCOS (PCOS: n = 25; no PCOS: n = 67)) in terms of serum levels of hormones. (A) serum anti-Müllerian hormone (AMH) protein concentration; (B) serum testosterone protein concentration; (C) serum follicle-stimulating hormone (FSH) level of enzymatic activity; (D) serum luteinizing hormone (LH) level of enzymatic activity; (E) serum thyroid-stimulating hormone (TSH) level of enzymatic activity; (F) serum estradiol protein concentration; (G) serum progesterone protein concentration; (H) serum prolactin protein concentration; (I) serum insulin level of enzymatic activity; (J) serum adiponectin protein concentration; (K) serum resistin protein concentration. Kruskal-Wallis nonparametric test and post hoc Dunn’s test. * p < 0.05, ** p < 0.01, *** p < 0.001, **** p < 0.0001. Median and IQR.
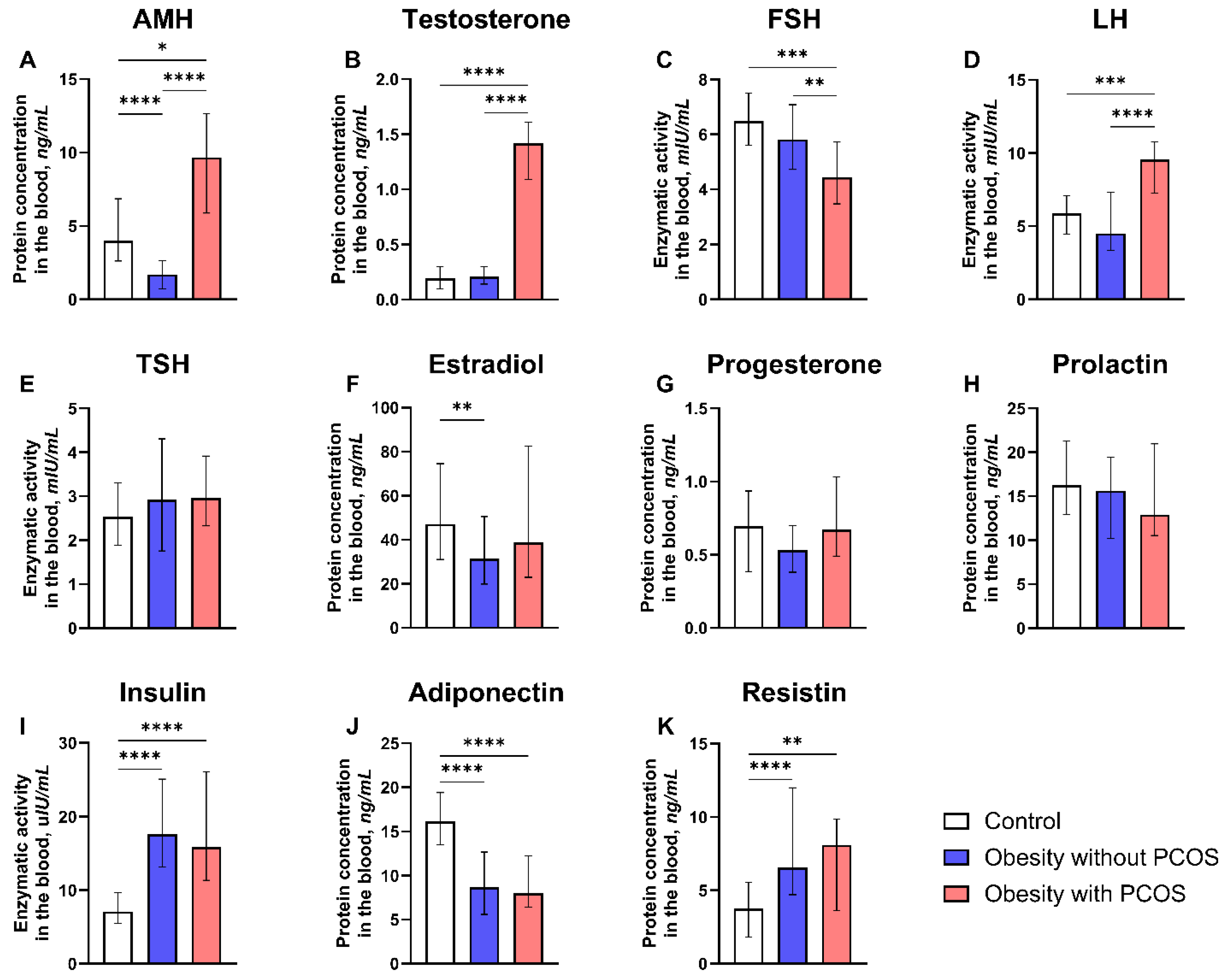
Figure 4.
ROC analysis of AMH specificity and sensitivity as a biomarker for PCOS diagnosis.
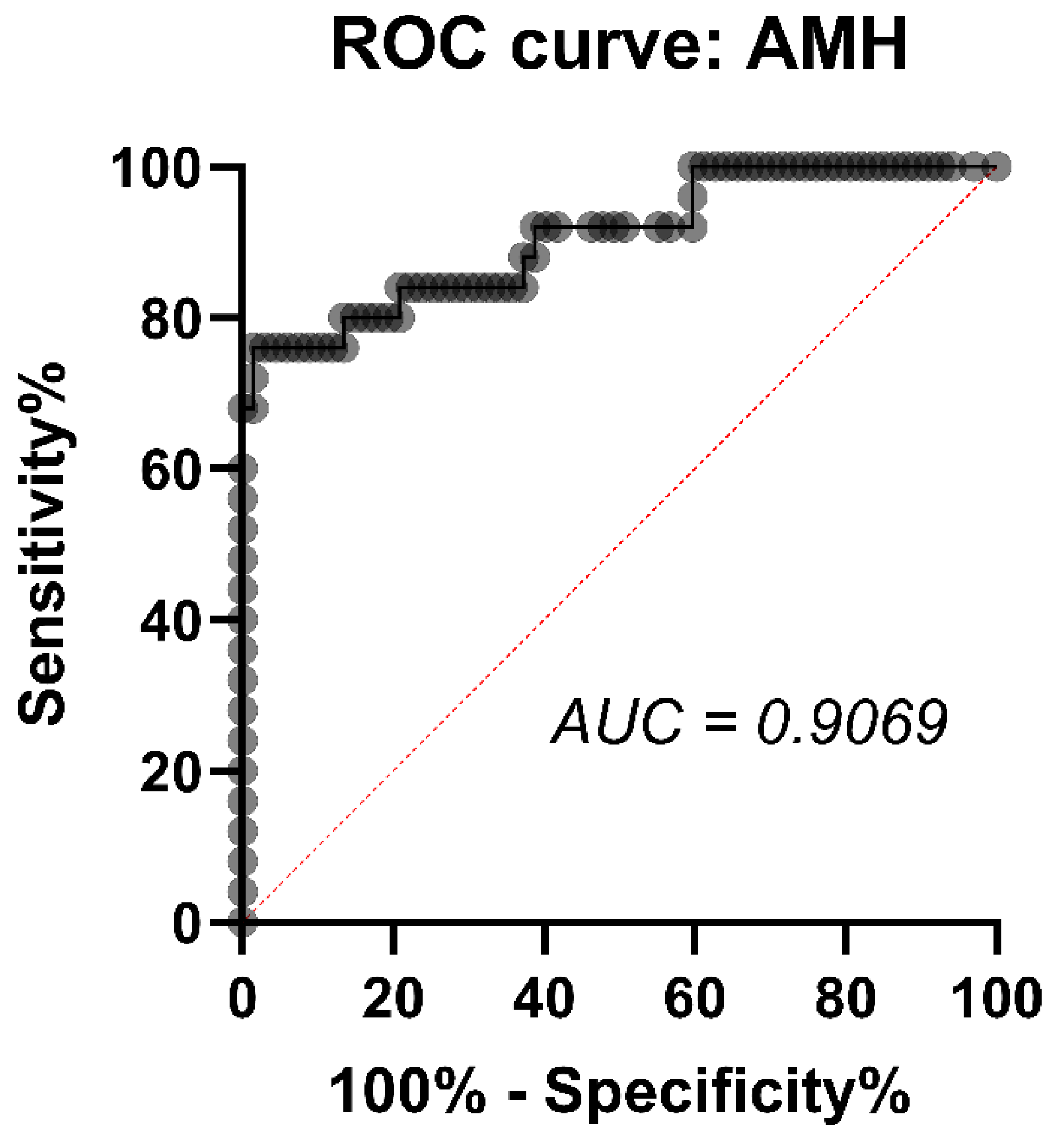
Figure 5.
Comparison between control group (n = 46) and study groups (obese group with or without PCOS (PCOS: n = 25; no PCOS: n = 67)) in terms of serum metabolites. (A) serum glucose level; (B) serum glycated hemoglobin level; (C) serum cholesterol level; (D) serum high density lipoprotein (HDL) level; (E) serum low density lipoprotein (LDL) level; (F) serum triacylglycerol levels. Kruskal-Wallis nonparametric test and post hoc Dunn’s test. *** p < 0.001, **** p < 0.0001. Median and IQR.
Figure 5.
Comparison between control group (n = 46) and study groups (obese group with or without PCOS (PCOS: n = 25; no PCOS: n = 67)) in terms of serum metabolites. (A) serum glucose level; (B) serum glycated hemoglobin level; (C) serum cholesterol level; (D) serum high density lipoprotein (HDL) level; (E) serum low density lipoprotein (LDL) level; (F) serum triacylglycerol levels. Kruskal-Wallis nonparametric test and post hoc Dunn’s test. *** p < 0.001, **** p < 0.0001. Median and IQR.
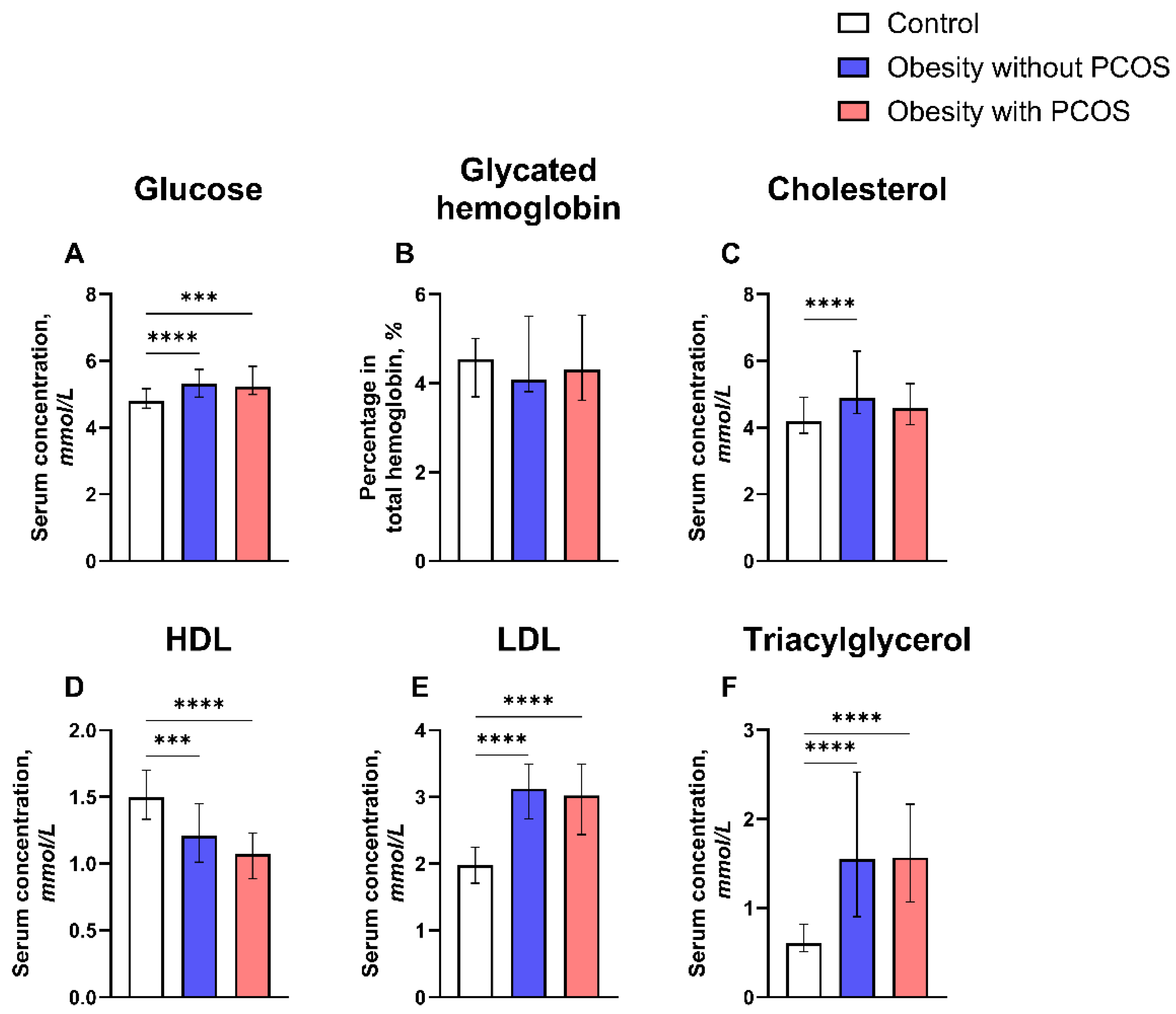
Figure 6.
Correlation coefficients from Spearman correlation analysis of AMH and hormonal parameters including testosterone, FSH, LH, TSH, estradiol, progesterone, prolactin and insulin for patients from the control group (no obesity, no PCOS; n = 46), obese patients without polycystic ovary syndrome (no PCOS; n = 67), and obese patients with polycystic ovary syndrome (PCOS; n = 25). * p < 0.05, ** p < 0.01. FSH, follicle-stimulating hormone; LH, luteinizing hormone; PCOS, polycystic ovary syndrome; TSH, thyroid-stimulating hormone.
Figure 6.
Correlation coefficients from Spearman correlation analysis of AMH and hormonal parameters including testosterone, FSH, LH, TSH, estradiol, progesterone, prolactin and insulin for patients from the control group (no obesity, no PCOS; n = 46), obese patients without polycystic ovary syndrome (no PCOS; n = 67), and obese patients with polycystic ovary syndrome (PCOS; n = 25). * p < 0.05, ** p < 0.01. FSH, follicle-stimulating hormone; LH, luteinizing hormone; PCOS, polycystic ovary syndrome; TSH, thyroid-stimulating hormone.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



