
Submitted:
26 August 2024
Posted:
27 August 2024
You are already at the latest version
Abstract
Aortic transection, a near-complete tear through the layers of the aorta, is a critical condition often resulting from trauma such as motor vehicle collisions. The urgency of managing aortic transection underscores the critical need for effective interventions. We report the case of a male in his early 50’s with no significant medical history who presented to the emergency department following a motor vehicle collision, sustaining multiple injuries including a descending thoracic aortic transection. Rapid diagnostic assessment confirmed the severity of the injury, necessitating immediate intervention. Endovascular aortic repair (EVAR) was successfully employed, highlighting its efficacy in managing acute aortic injuries. The patient responded well to treatment, underscoring the importance of timely intervention in improving patient outcomes. This case emphasizes the critical role of rapid diagnostic assessment and endovascular intervention in managing life-threatening thoracic aortic injuries, particularly in the acute setting.
Keywords:
Cardiovascular medicine
; Hypertension
; Interventional cardiology
; Surgical diagnostic tests
Background
Blunt traumatic aortic injury is the second most common cause of death due to trauma after head injury [1]. Traumatic aortic transection is the near complete tear through all layers of the Aorta due to trauma sustained in motor vehicle collision or fall. In the majority of cases high energy blunt trauma with rapid deceleration is the mechanism of injury often associated with multiple rib fractures. Injury can occur along the entire length of aorta, essentially from ascending aorta to the iliac bifurcation, near the aortic isthmus or along descending aorta [2]. This injury is potentially a life-threatening condition and patients who survive usually have partial thickness tears of aortic wall with pseudoaneurysm formation. Therefore, prompt diagnosis and immediate intervention is required. Several imaging modalities can be considered like chest x ray, CT chest, FAST scan [3]. The use of endovascular aortic repair (EVAR) has become increasingly prevalent due to its minimally invasive nature and effectiveness [4]. This case report highlights a case of traumatic descending thoracic aortic transection in a 50-year- old man managed successfully with Endo-Vascular Aortic Repair (EVAR) and discusses the clinical decision-making process in the management of such injuries and demonstrates its potential as a life-saving intervention.
Case Presentation
A male in his early 50’s with no prior medical history presented to the emergency department as a trauma code after a motor vehicle collision. He was a restrained front passenger in a vehicle traveling approximately 70 mph when it was struck on the passenger side by a semi- truck. Initially ambulatory on scene, the patient subsequently developed tachycardia and hypotension en route to the hospital. He sustained multiple injuries, including a descending thoracic aortic transection with a 1.5 cm pseudoaneurysm and periaortic hematoma, as well as right medial and lateral rib fractures, acetabular fracture, pubic symphysis fracture, inferior pubic rami fracture, and a pelvic sidewall hematoma.
Investigations
Diagnostic assessment included physical examination findings, hemodynamic monitoring, imaging studies (e.g., computed tomography angiogram), and interventional radiology procedures (e.g., angiography for aortic injury).
Differential Diagnosis
In cases of traumatic descending thoracic aortic transection, differential diagnoses include aortic dissection, which presents with similar symptoms of severe chest pain and often requires immediate imaging for differentiation. Aortic rupture, another critical consideration, manifests with sudden-onset chest pain and signs of shock, necessitating prompt intervention. Blunt cardiac injury can mimic symptoms of aortic transection and should be evaluated, especially in cases of high-impact trauma. Rib fractures with associated hemothorax or pneumothorax can also present similarly, requiring careful assessment to rule out aortic injury. Additionally, thoracic spine fractures with spinal cord injury can lead to neurological symptoms that may overlap with those of aortic transection. Finally, pulmonary contusion or laceration, common in thoracic trauma, should be considered in the differential diagnosis, particularly when evaluating for associated injuries.
Treatment
Therapeutic interventions included strict blood pressure control with an Esmolol drip, endovascular stenting repair (EVAR) for the aortic injury, Open Reduction Internal Fixation (ORIF) for acetabular and rib fractures, intercostal nerve cryoablation, intubation, and mechanical ventilation.
Outcome and Follow-up
Following surgical interventions and stabilization of respiratory status, the patient demonstrated significant improvement with continued progress under proper pain control.
Discussion
Aortic transection is a life-threatening condition characterized by tears in the inner layer of the aorta that leads to the formation of growing hematoma in the intima media space. Most commonly, it is caused by blunt trauma, though it also can be caused by penetrating injury.
There are no clinical findings specific for aortic injury. However, hypotension, external evidence of trauma, and altered mental status are common. Many patients with complete transection of the thoracic aorta die before arriving at the emergency department (ED) [5]. Those who survive arrival in the ED may have small tears or partial-thickness tears of the aortic wall with a pseudoaneurysm formation. The survival of patients after traumatic aortic injury depends on a clinician’s high index of suspicion, rapid diagnosis, and prompt management. [6]
Our case highlights the complex management of a 50-year-old male involved in a high-speed motor vehicle collision resulting in multiple traumatic injuries, including a descending thoracic
aortic transection, rib fractures, acetabular fractures, and pelvic fractures. Through a multidisciplinary approach involving trauma surgery, interventional radiology, orthopedic surgery, and critical care, the patient received timely and comprehensive care that ultimately led to a favorable outcome. The mechanism of injury in this case, involving a high-speed collision with a semi-truck, underscores the severity and complexity of the patient’s injuries. The initial presentation with tachycardia and hypotension raised concerns for internal hemorrhage and prompted expedited evaluation and management upon arrival at the emergency department.
Although the diagnosis of traumatic aortic injury is difficult it can be assisted with diverse imaging tools, such as chest X-ray, FAST and CT. Chest X-ray is a rapid and convenient approach for early diagnosis of aortic injury. The most significant manifestation is mediastinal widening. However, chest X-rays cannot provide satisfactory sensitivity and specificity. It has been reported that approximately 7.3%–44% of patients with aortic injury present with normal mediastinum [7]. Therefore, a normal chest X-ray imaging cannot completely exclude Aortic Dissection. FAST can also detect mediastinal widening rapidly and accurately; however, the sensitivity and specificity of FAST for diagnosis of patients with Aortic Dissection are also very low. The gold standard for diagnosis of TAI is CT of the chest, especially CTA of the thoracic and abdominal aorta, which achieves a sensitivity of nearly 100% [8]. Once the risk of TAI is suspected, chest CT needs to be implemented, especially for patients with chest or abdominal injuries obtained in a motor vehicle accident.
In our case diagnostic challenges were encountered in identifying the full extent of the patient’s injuries, particularly the aortic transection, which required advanced imaging modalities such as computed tomography angiogram (CTA) for accurate diagnosis. Prompt recognition of aortic injury was crucial, as untreated thoracic aortic transections carry a high mortality rate.
The management approach focused on rapid stabilization and strict blood pressure control to minimize the risk of further aortic injury or rupture. According to the Society for Vascular Surgery (SVS) if anatomy is favorable, EVAR should be preferred over open repair for all age groups. Lower morbidity, mortality and spinal cord ischemia have been reported with endovascular repair, as well as earlier hospital discharge [9]. Endovascular stenting repair (EVAR) was successfully performed to address the aortic transection, demonstrating the effectiveness of minimally invasive techniques in managing complex vascular injuries.
This case highlights the importance of rapid and accurate diagnosis in trauma settings. The successful application of EVAR in managing traumatic aortic injuries demonstrates its potential as a life-saving intervention. The multidisciplinary approach was crucial in addressing the complexity of the patient’s injuries, illustrating the challenges and advancements in the management of polytrauma patients.
Figure 1.
Chest X-ray demonstrating multiple right rib fractures (Green arrows) and mediastinal widening.
Figure 1.
Chest X-ray demonstrating multiple right rib fractures (Green arrows) and mediastinal widening.
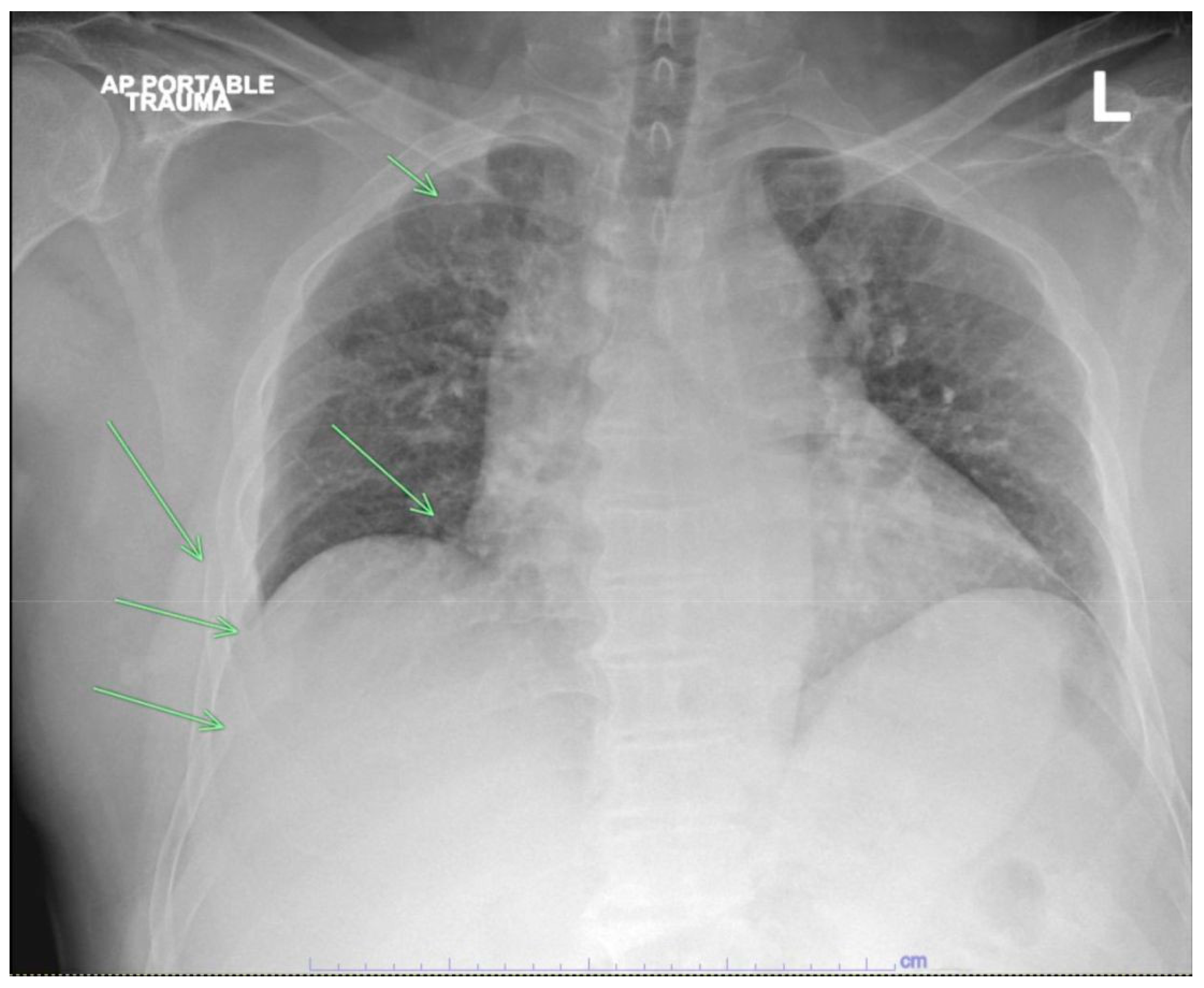
Figure 2.
Acute thoracic aortic injury, pseudoaneurysm, with associated periaortic hematoma detailed above. 2. Multiple right rib fractures detailed above. 3. Right pelvic fractures involving the right acetabulum, right pubic rami and right pubic symphysis with an associated right pelvic sidewall hematoma measuring 10 x 5 cm without evidence of active hemorrhage. 4. Suspected midline pancreatic grade 1 injury/laceration.
Figure 2.
Acute thoracic aortic injury, pseudoaneurysm, with associated periaortic hematoma detailed above. 2. Multiple right rib fractures detailed above. 3. Right pelvic fractures involving the right acetabulum, right pubic rami and right pubic symphysis with an associated right pelvic sidewall hematoma measuring 10 x 5 cm without evidence of active hemorrhage. 4. Suspected midline pancreatic grade 1 injury/laceration.
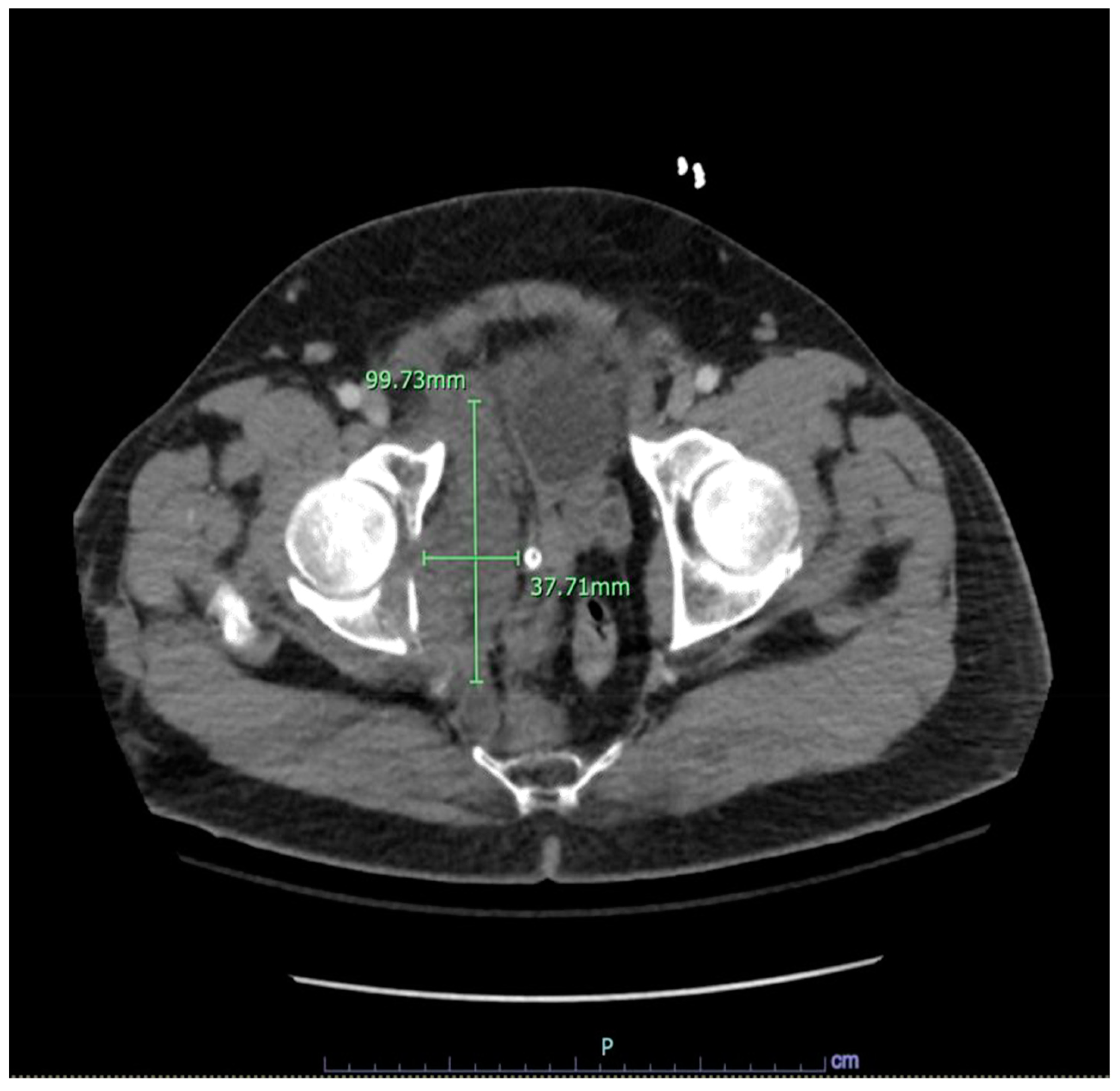
Figure 3.
CT scan revealing a flap coursing across the medial wall of descending aorta with an associated pseudoaneurysm of size 1.5cm protruding anteromedially.
Figure 3.
CT scan revealing a flap coursing across the medial wall of descending aorta with an associated pseudoaneurysm of size 1.5cm protruding anteromedially.
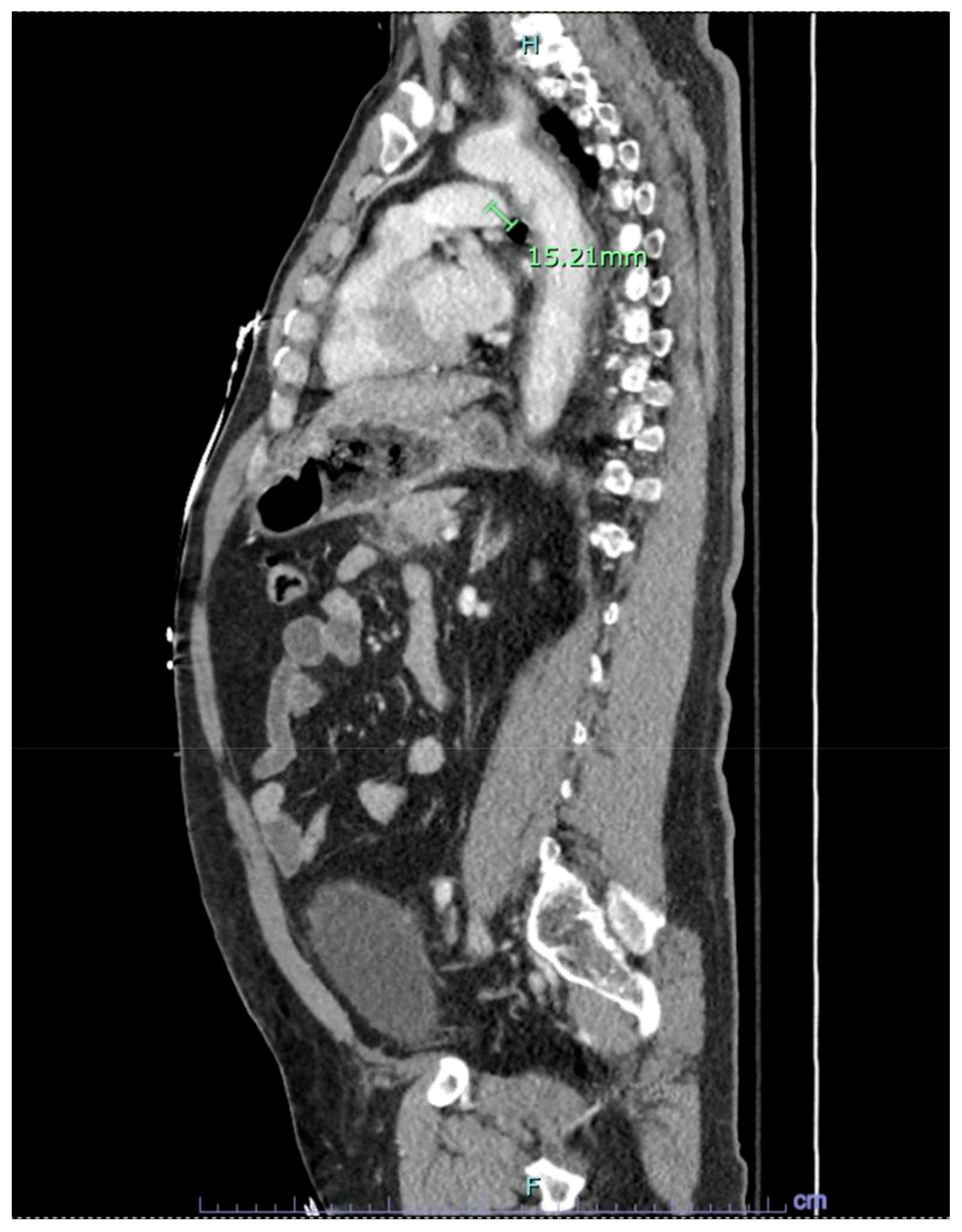
Figure 4.
CT Angiography with contrast visualizing aortic arch and descending aorta preplacement of the stent.
Figure 4.
CT Angiography with contrast visualizing aortic arch and descending aorta preplacement of the stent.

Figure 5.
Postoperative 3D reconstruction CTA (Posterior view) illustrating the aortic repair with a stent. Shows no contrast extravasation.
Figure 5.
Postoperative 3D reconstruction CTA (Posterior view) illustrating the aortic repair with a stent. Shows no contrast extravasation.

Learning Points/Take Home Message
- This case underscores the efficacy of endovascular aortic repair (EVAR) in managing traumatic descending thoracic aortic transection, highlighting the importance of prompt intervention and collaborative care in trauma scenarios.
- Emergent endovascular repair emerges as the preferred modality for addressing traumatic distal thoracic aortic transection due to its minimally invasive nature and potential for favorable outcomes.
- In patients with multiple traumas and traumatic thoracic aortic rupture, endovascular therapy shows potential for achieving favorable short- and mid-term outcomes compared to traditional thoracotomy repair.
- Endovascular repair presents a favorable option for patients with concurrent injuries or comorbidities that increase the risks associated with open surgery, offering a safer alternative with minimal complications.
- As vascular surgeons increasingly integrate endovascular techniques for both traumatic and nontraumatic aortic emergencies, these interventions are poised to assume a pivotal role in future clinical practice, ensuring excellent long-term results.
References
- de Mestral C, Dueck A, Sharma SS, Haas B, Gomez D, Hsiao M, Hill A, Nathens AB. Evolution of the incidence, management, and mortality of blunt thoracic aortic injury: a population- based analysis. J Am Coll Surg. 2013 Jun;216(6):1110-5. [CrossRef] [PubMed]
- Sabra MJ, Dennis JW, Allmon JC, Gautam S, Habib J. Identification of unique characteristics and the management of blunt traumatic aortic injuries occurring at unusual locations in the descending thoracic aorta. J Vasc Surg. 2019 Jan;69(1):40-46. [CrossRef] [PubMed]
- D’Souza D, Elfeky M, Chieng R, et al. Thoracic aortic injury. Reference article, Radiopaedia.org (Accessed on 08 Apr 2024). [CrossRef]
- Elkbuli A, Dowd B, Spano PJ 2nd, Smith Z, Flores R, McKenney M, Boneva D. Thoracic Endovascular Aortic Repair Versus Open Repair: Analysis of the National Trauma Data Bank. J Surg Res. 2020 Jan; 245:179-182. [CrossRef] [PubMed]
- S. Sevitt, “The mechanisms of traumatic rupture of the thoracic aorta,” British Journal of Surgery, vol. 64, no. 3, pp. 166–173, 1977. [CrossRef]
- Williams JS, Graff JA, Uku JM, Steinig JP: Aortic injury in vehicular trauma. Ann Thorac Surg. 1994, 57:726-730. [CrossRef]
- J. H. Woodring and M. L. Dillon, “Radiographic manifestations of mediastinal hemorrhage from blunt chest trauma,” The Annals of Thoracic Surgery, vol. 37, no. 2, pp. 171–178, 1984.
- Edwards R, Khan N. Traumatic aortic injury: Computed tomography angiography imaging and findings revisited in patients surviving major thoracic aorta injuries. SA J Radiol. 2021 Mar 12;25(1):2044. [CrossRef] [PubMed]
- Lee WA, Matsumura JS, Mitchell RS, Farber MA, Greenberg RK, Azizzadeh A, Murad MH, Fairman RM. Endovascular repair of traumatic thoracic aortic injury: clinical practice guidelines of the Society for Vascular Surgery. J Vasc Surg. 2011 Jan;53(1):187-92. [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



