
Submitted:
27 August 2024
Posted:
27 August 2024
You are already at the latest version
Abstract
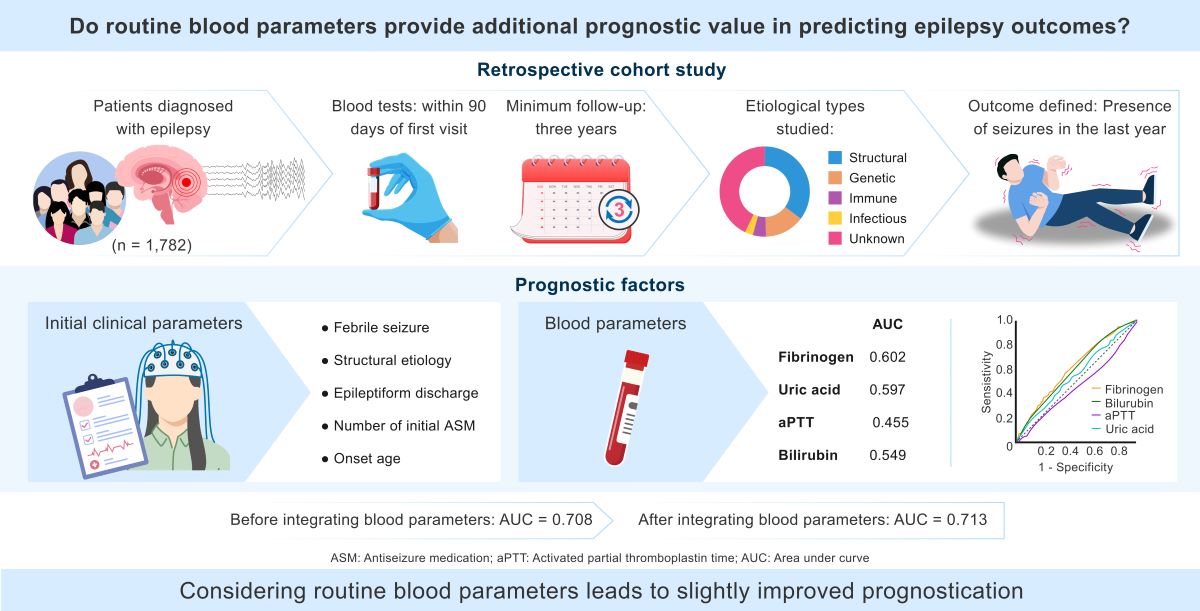
Background/Objectives: Determining the outcome of epilepsy is crucial for making proactive and timely treatment decisions, as well as for counseling patients. Recent research efforts have focused on using various imaging techniques and EEG for prognostication; however, there is insufficient evidence regarding the role of blood parameters. Our study aimed to investigate the additional prognostic value of routine blood parameters in predicting epilepsy outcomes. Methods: We analyzed data from 1,782 patients who underwent routine blood tests within 90 days of their first visit and had a minimum follow-up duration of three years. The etiological types were structural (35.1%), genetic (14.2%), immune (4.7%), infectious (2.9%), and unknown (42.6%). The outcome was defined as the presence of seizures in the last year. Results: Initially, a multivariate analysis was conducted based on clinical variables, MRI, and EEG data. This analysis revealed that sex, age of onset, epileptiform discharge, structural etiology, and the number of antiseizure medications were related to the outcome, with an area under curve (AUC) of 0.708. Among the blood parameters, fibrinogen, bilirubin, uric acid, and aPTT were significant, with AUCs of 0.602, 0.597, 0.455, and 0.549, respectively. Including these blood parameters in the analysis slightly improved the AUC to 0.713. Conclusions: Some blood parameters were found to be related to the final outcome, potentially paving the way to understanding the mechanisms of epileptogenesis and drug resistance.
Keywords:
epilepsy
; outcome
; prediction
; blood
1. Introduction
Despite dedicated medical treatment, approximately 30% of epilepsy patients suffer from recurrent seizures. Among medically intractable epilepsy patients, approximately half are surgically remediable. Given that a longer duration of epilepsy leads to poorer surgical outcome [1,2], prediction of the final outcome of medical treatment could save time until surgical resection and could also help in selecting candidates for novel treatment without delay [3], as well as assisting in patient counseling.
According to numerous previous articles, clinical factors related to drug resistance include onset age [4,5,6] the number of seizures [7], the response of initial antiseizure medication (ASM) [8], the presence of febrile seizures [5,9], and epilepsy duration [10,11]. electroencephalography (EEG) biomarkers, such as epileptiform discharges [12] are used to predict outcomes. Image factors include the presence of hippocampal sclerosis [4], and any structural etiology [13]. Liquid biomarkers have also been investigated; for example, serum High mobility group box 1 (HMGB1) and interleukin (IL)-1β have been related to epilepsy outcomes in the pediatric population [14] and neuron-specific enolase [15], has been used to predict the outcome. However, there is a paucity of large-scale human studies investigating blood parameters from routine clinical settings in epilepsy.
In this study, we aimed to focus on the routine blood parameters in relation to the final outcomes in a relatively large-sized population from single center.
2. Materials and Methods
2.1. The Study Population
A total of 2586 patients from SERENADE (Seoul national university hospital adult Epilepsy Retrospective cohort in the Era of Newer Antiseizure Drug Exposure), with clinical information, EEG, image data, and routine blood tests, were evaluated. The patients met the following criteria: 1) visited our epileptologists’ clinic from Jan 2008 to Jan 2018 for the first time; 2) diagnosed with epilepsy with the International League Against Epilepsy (ILAE) definition; 3) prescribed any ASM for more than three months; and 4) had at least a three-year or more follow-up period. This study was approved by the Seoul National University Hospital Institutional Review Board (2308-010-1455) and followed the principles of the Declaration of Helsinki. The requirement for written consent was waived due to the retrospective design.
2.2. Collected Data Characteristics
The patients’ lists and laboratory results were extracted from the clinical database warehouse in our institution. Additionally, investigators reviewed electronic medical records thoroughly, including sex, onset age, number of seizures before ASM initiation, newly diagnosed vs. referred case, seizure classification, epilepsy classification, etiology, history of febrile convulsion, family history of epilepsy, and epilepsy surgery history. Data from routine blood tests, including white blood cells (WBCs), hemoglobin, platelets, neutrophils, lymphocytes, monocytes, eosinophils, basophils, absolute neutrophil counts (ANCs), MCV, MCH, MCHC, RDW, protein, albumin, bilirubin, aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, calcium, phosphorus, glucose, blood urea nitrogen, creatinine, uric acid, Na/K/Cl, tCO2, prothrombin time, activated partial thromboplastin time (aPTT), fibrinogen, and total cholesterol, were collected only in cases sampled within 90 days of the first visit. The routine blood test was performed at an outpatient clinic or on admission according to the individual situation in the real world.
Magnetic resonance imaging (MRI) lesions were defined as the most relevant lesion in the patient’s epilepsy, based solely on MRI through a consensus of three experienced epileptologists (KIP, SH, and SKL). In surgical cases, the pathologic diagnosis takes priority when there is a discrepancy between the pathologic and radiologic diagnoses. EEG findings were defined on the first one during the entire follow-up duration, irrespective of the routine or video-EEG. The epileptic waveforms include periodic discharge, rhythmic discharge, and rhythmic or isolated spike/wave. The final outcome was defined by seizures that occurred during the last year of follow-up, enabling classification as seizure-free or seizure-persistent. In surgical cases, the outcome was assessed based on the most recent year before the surgery.
2.3. Statistical Analysis
The numerical values are expressed as numbers or mean ± standard deviation. Student’s t-test was used for continuous variables, and the Mann‒Whitney test was used for non-continuous variables. A Chi-square test was also performed. To ensure the independent factor status of the final outcome, we performed multiple linear regressions including variables that showed significance in univariate analysis and potentially meaningful variables. The statistical significance was set as a two-tailed p-value < 0.05. SPSS (version 25, IBM, Chicago, IL, United States) or GraphPad Prism (version 9, Dogmatics, San Diego, CA, United States) was used for all statistical analyses.
3. Results
This cohort comprised the total population of patients who visited our epilepsy center for the first time over ten years, from 2008 to 2017. Among 2586 patients in the entire cohort, 1782 patients (female 45.7%) who had routine blood test results within three months of the initial clinic visit were finally analyzed. Comparing the final outcome between the presence and absence of the initial blood test, we found that there was no significant difference in outcome (p=0.676).
The gap between the first visit and epilepsy onset was 6.9±9.6 years (range, 0-65). Among them, newly diagnosed patients are the population who had no history of epilepsy treatment or were managed for less than six months following the clinic visit, if any, at our center. The proportions of newly diagnosed patients were 52.1%. The onset age of epilepsy was 29.6±19.6, and the age of the first visit to our center was 37.5±18.0. Following the 2017 ILAE classification, focal epilepsy, generalized epilepsy, combined, and unknown were 1387 (77.8%), 275 (15.4%), 98 (5.5%), and 22 (1.2%), respectively. Regarding etiology, structural (626, 35.1%) was the most common. Genetic (253, 14.2%), immune (84, 4.7%), infectious (51, 2.9%), hypoxic (5, 0.3%), and metabolic (3, 0.1%) followed, in order of frequency. However, 760 patients (42.6%) had an unknown etiology (Table 1). EEG data, routine or long-term, were available in 1631 patients (91.5%). MRI under an epilepsy-specific protocol in our institution was obtained in 1553 (87.1%) patients. Surgical intervention, including resective operation and vagal nerve stimulation, was performed in 58 patients (3.3%).
The final seizure freedom rate was 65.8%, representing 1,173 patients. We sought to identify independent determinants of the final outcome using initial clinical status, EEG, and MRI data. Multivariate analysis revealed that five clinical parameters were significantly associated with the final outcome: sex (p=0.008), epilepsy onset age (p<0.001), epileptiform discharges on EEG (p<0.001), number of ASMs (p<0.001), and structural etiology (p=0.007) (Table 2).
Based on multiple logistic regression analysis, we developed the following equation to predict the final outcome:
Equation 1 = (-0.331 X sex) + (0.456 X epileptiform discharge) + (0.428 X structural etiology) + (0.505 X number of initial ASM) - (0.029 X onset age).
In this model, male sex, presence of epileptiform discharges, and structural etiology are coded as 1. The area under the curve (AUC) for this model was 0.708 (p<0.001).
In the next step, we conducted a similar analysis incorporating routine blood parameters. Multiple logistic regression identified febrile seizures (p=0.038), epileptiform discharges (p<0.001), structural etiology (p=0.002), number of initial ASMs (p<0.001), onset age (p=0.001), fibrinogen (p<0.001), uric acid (p=0.011), aPTT (p=0.003), and bilirubin (p=0.020) as independent prognostic factors (Table 3) (Figure 1a).
The following equation was developed based on this analysis: Equation 2 = (0.511 X Febrile seizure) + (0.538 X Epileptiform discharge) + (0.562 X Structural etiology) + (0.415 X Number of initial ASM) - (0.026 X Onset age) - (0.57 X bilirubin) - (0.118 X uric acid) + (0.045 X aPTT) - (0.004 X fibrinogen). The AUC was 0.713 (p<0.001), which was slightly improved compared to the equation 1 not considering the blood parameters. The AUCs for fibrinogen, bilirubin, uric acid, and aPTT were 0.602, 0.597, 0.549, and 0.455, respectively (Figure 1b).
Focusing on blood fibrinogen levels, which had the highest AUC among the blood parameters, we found that fibrinogen levels were significantly higher in the seizure-free group compared to the seizure-persistent group (Figure 1a,c). Patients in the high quartile group for fibrinogen levels had a better final outcome than those in the low quartile group (p<0.01).
Multiple linear regression with fibrinogen level as the dependent variable showed that final outcome, sex, structural/infectious etiology, WBC, ANC, albumin, time since recent seizure, and the number of initial ASMs were significantly associated with fibrinogen levels (p values = 0.010, 0.009, 0.029, <0.001, <0.001, 0.004, <0.001, 0.030, and <0.001, respectively) (Table S1). The correlations between fibrinogen levels and associated factors are illustrated in Figure 2a. Female sex, structural or infectious etiology, and recent seizure were associated with higher fibrinogen levels (Figure 2b).
4. Discussion
In this study, we found that several blood parameters measured within three months after first visit to our center, were associated with the final outcome of epilepsy in a large cohort. Considering the routine blood parameters, the prognostication is slightly improved compared to when analyzing only clinical variables, MRI and EEG.
Among blood parameters, we found the fibrinogen, uric acid, bilirubin and aPTT was associated with the final outcome. Among those, we focused on blood fibrinogen, which is the novel and had the highest AUC value. Blood fibrinogen is produced by the liver and plays a role in inflammatory and coagulation cascades in a wide spectrum of neurological diseases, including stroke, spinal cord injury, brain trauma, multiple sclerosis, and Alzheimer’s disease [16]. In acute traumatic brain injury [17], fibrinogen in blood extravasates into the brain parenchyma across disrupted blood‒brain barriers and interacts with brain cells, producing reactive oxidative species and inflammatory cytokines such as IL-6 and C-C motif chemokine ligand 2 (CCL2) and finally leading to neuro-inflammatory cascades. The penetrating fibrinogen after traumatic brain injury activates microglia and astroglia, leading to subsequent cell damage, which is mediated by Transforming growth factor (TGF)-β signaling [18]. Furthermore, induced IL-6 further amplifies fibrinogen [19]. IL-6 peaks at 1-2 days in humans [20], correlating in time with the fibrinogen level. In addition, a more activated fibrinolytic system by traumatic brain injury decreases fibrinogen concentration. Therefore, it has been considered a marker of inflammation or coagulopathy.
Several previous clinical studies demonstrated an apparently harmful association, showing high fibrinogen and low attention/executive function in mild cognitive impairment [21] and progression to dementia [22]. Since fibrinogen has been regarded as a systemic inflammatory marker, the status of hyperfibrinogenemia as a poor prognostic factor was explained by its inflammatory action. In epilepsy, ample evidence has accumulated that systemic inflammation crosstalk with brain-borne inflammation, leading to epileptogenesis. The patients with a higher seizure burden showed higher levels of blood markers of inflammation, such as C-reactive protein and IL-6 [23]. However, we found that a high fibrinogen level was associated with a good final outcome in this study.
Neuro-inflammatory processes can be diverse, and systemic immune reactions are more complex in the epilepsy process. The generally accepted concept is that systemic immunity aggravates epilepsy, which has been proven in animal and clinical studies. Blocking leukocyte-endothelial adhesion prevents epilepsy in animal models [24]. An animal study also supports that the reduction in recruiting circulating immune cells decreased brain-borne neuroinflammation and neuronal damage using the chemokine receptor 2-knockout model [25]. The results from our prior clinical study also indicated an immediate increase in serum IL-6 concentration following generalized tonic‒clonic seizures [26], supporting the established concept of a positive feedback loop between seizures and systemic inflammation. However, another study contradicted this finding, where T-cell/B-cell depleted mice showed exacerbated seizures following use of kainic acid [27]. The contradictory story might be due to different models of epilepsy and, more importantly, different time points during the course of epilepsy. The neuro-inflammatory role may differ between immediately after a seizure and during the inter-seizure baseline state. It needs to be considered that the pro-inflammatory process can be balanced with the anti-inflammatory process.
Although the mechanism is unclearly explained, the data supporting high fibrinogen levels as a factor indicative of good prognosis in neurological disease also exist. Low fibrinogen concentration after traumatic injury was associated with an unfavorable prognosis [28,29]. Another study showed a positive association of blood fibrinogen in patients with amyotrophic lateral sclerosis [30]. In this study, a high level of blood γ-fibrinogen, which accounts for ~8% of plasma fibrinogen, was associated with a better disease outcome. Although that paper suggested alternative microglial activation, called M2, as a possible mechanism, the protective mechanism of fibrinogen is still obscure. Plasma fibrinogen was lower in idiopathic generalized epilepsy [31] than in controls, which is consistent with our result in part despite the small number of patients included, implying that seizures are related to low plasma fibrinogen. However, this study did not show a difference when comparing seizure-free or not possibly due to the small number of study populations.
Fibrinogen acts both on thrombosis and neuroinflammation. This study showed that fibrinogen was independently associated with the number of WBCs and ANC, which are known as immune and inflammatory markers. Therefore, inflammatory mechanisms rather than thrombosis seem to be more attributed to the epilepsy mechanism. Alongside inflammatory reactions, fibrinolysis occurs in epilepsy [32]. We can speculate that seizures themselves induce fibrinolysis, akin to traumatic brain injury. This speculation is supported by the finding that a shorter interval between sampling and recent seizures is associated with a higher fibrinogen level (Table S1).
A statistical relationship between the blood level of fibrinogen and the infectious etiology of epilepsy, suggests a plausible direct influence of the infectious cause on fibrinogen levels. However, it is essential to emphasize that the association between fibrinogen levels and the good final outcome was not a result of infection because the statistics revealed that neither infectious nor immune etiology had a significant relationship with the final outcome. Interestingly, the fibrinogen level is associated with the number of ASMs. The lower the number of ASMs was, the higher the fibrinogen level. From this finding, we speculate that ASM can influence systemic inflammatory markers or, more specifically, fibrinogen levels. Findings presented in previous papers also support this assumption [33,34,35,36]. Certain ASMs might play an anti-inflammatory role, which is evidenced by low fibrinogen.
A shorter aPTT is associated with a better outcome in epilepsy. The mechanism by which aPTT influences epilepsy outcomes is not yet understood. However, a shorter aPTT, indicating an increased intrinsic pathway, can produce more fibrinogen with higher turnover in the coagulation pathway. How this independently links to the outcome needs to be clarified in further studies.
A high level of uric acid is also associated with a better outcome in epilepsy. A previous study involving 5,672 epilepsy patients demonstrated that the hyperuricemic group, prior to their epilepsy diagnosis, had a lower conversion rate to drug-resistant epilepsy [37]. Although our final outcome was dichotomized into seizure-free or not, and our population included referred patients from other hospitals, the association between uric acid levels and seizure outcomes is consistent with previous findings. This paper suggested that the protective role of uric acid is due to its antioxidant effect, which counteracts seizure-induced oxidative stress. Elevated serum uric acid levels are often related to the excessive consumption of red meat. The habit of consuming a high-protein diet, including excessive meat intake, might contribute to the protective effect against seizures, similar to the effects of a ketogenic diet.
We also found that high serum level of bilirubin was associated with the good outcome. The previous animal study with piglet model of seizure demonstrated that bilirubin treatment before and after seizure induction significantly decreased the reactive oxygen species production in cerebral vessels and astrocytes, highlighting the role of antioxidant effect of bilirubin [38].
The study had several limitations. First, blood samples were taken at various time points following a recent seizure. As previously mentioned, it is imperative to consider that acute seizures can influence blood parameters. Thus, we included this covariate in the statistical analysis. Second, we did not assess other acute inflammatory markers, such as C-reactive protein or interleukins. It is possible that, even in cases with high levels of fibrinogen without infectious or immune etiology, there may exist a specific subgroup of patients in whom the inflammatory response plays a more prominent role in epilepsy. Further research using multiple markers of inflammation in more refined populations is needed to clarify this aspect. Third, this study only included subjects who underwent blood sampling within three months after their first visit. This three-month period aligns with our clinical setting, where blood tests are typically performed at admission after the first outpatient visit, usually between one to three months. This approach may have introduced selection bias by not including the entire population of epilepsy patients. However, the final outcome did not differ based on the presence or absence of the initial blood test.
5. Conclusions
While the mechanisms of all blood parameters influencing epilepsy outcomes were not clearly explained, we attempted to incorporate the routine blood parameters to predict the epilepsy outcome in a large population from single institution. Although the predictive power dose not drastically improved by incorporating blood parameters, this approach enables us to gain deeper insights into the mechanistic role of blood markers in epilepsy. More studies in drug-naïve patients and observation of longitudinal changes as well as external validation are necessary to verify our results.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Multiple linear regression for fibrinogen level
Author Contributions
Conceptualization, KIP and SKL.; methodology, HS.; formal analysis, KIP, HS, SH; investigation, JM, STL, KHJ, JKY, KC.; resources, KIP, STL, KYJ, SKL.; data curation, SH.; writing—original draft preparation, KIP, HS, SH.; writing—review and editing, KIP, HS, SH, JM, STL, KHJ, KYJ, KC, SKL.; visualization, KIP.; supervision, SKL.; funding acquisition, KIP. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Korea Health Industry Development Institute, the Ministry of Health & Welfare, Republic of Korea, grant number RS-2023-00265638. The APC was also funded by the Korea Health Industry Development Institute, the Ministry of Health & Welfare, Republic of Korea, grant number RS-2023-00265638.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the Seoul National University Hospital (2308-010-1455).
Informed Consent Statement
Patient consent was waived due to the retrospective design.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available on reasonable request.
Acknowledgments
none
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Park, K. I.; Lee, S. K.; Chu, K.; Jung, K. H.; Bae, E. K.; Kim, J. S.; Lee, J. J.; Lee, S. Y.; Chung, C. K. Withdrawal of antiepileptic drugs after neocortical epilepsy surgery. Ann Neurol 2010, 67(2), 230–238. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S. W.; Lee, S. K.; Hong, K. S.; Kim, K. K.; Chung, C. K.; Kim, H. Prognostic factors for the surgery for mesial temporal lobe epilepsy: longitudinal analysis. Epilepsia 2005, 46(8), 1273–1279. [Google Scholar] [CrossRef] [PubMed]
- Son, H.; Park, K. I.; Shin, D. S.; Moon, J.; Lee, S. T.; Jung, K. H.; Jung, K. Y.; Chu, K.; Lee, S. K. Lesion Detection Through MRI Postprocessing in Pathology-Proven Focal Cortical Dysplasia: Experience at a Single Institution in the Republic of Korea. J Clin Neurol 2023, 19(3), 288–295. [Google Scholar] [CrossRef] [PubMed]
- Roy, P. L.; Ronquillo, L. H.; Ladino, L. D.; Tellez-Zenteno, J. F. Risk factors associated with drug resistant focal epilepsy in adults: A case control study. Seizure 2019, 73, 46–50. [Google Scholar] [CrossRef]
- Tripathi, M.; Padhy, U. P.; Vibha, D.; Bhatia, R.; Padma Srivastava, M. V.; Singh, M. B.; Prasad, K.; Chandra, S. P. Predictors of refractory epilepsy in north India: a case-control study. Seizure 2011, 20(10), 779–783. [Google Scholar] [CrossRef]
- Stroup, D. F.; Berlin, J. A.; Morton, S. C.; Olkin, I.; Williamson, G. D.; Rennie, D.; Moher, D.; Becker, B. J.; Sipe, T. A.; Thacker, S. B. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283 (15), 2008-2012.
- Dwivedi, R.; Ramanujam, B.; Chandra, P. S.; Sapra, S.; Gulati, S.; Kalaivani, M.; Garg, A.; Bal, C. S.; Tripathi, M.; Dwivedi, S. N.; et al. Surgery for Drug-Resistant Epilepsy in Children. N Engl J Med 2017, 377(17), 1639–1647. [Google Scholar] [CrossRef]
- Kwan, P.; Brodie, M. J. Early identification of refractory epilepsy. N Engl J Med 2000, 342(5), 314–319. [Google Scholar] [CrossRef]
- Brodie, M. J. Outcomes in newly diagnosed epilepsy in adolescents and adults: Insights across a generation in Scotland. Seizure 2017, 44, 206–210. [Google Scholar] [CrossRef]
- Park, K. M.; Shin, K. J.; Ha, S. Y.; Park, J.; Kim, S. E.; Kim, S. E. Response to antiepileptic drugs in partial epilepsy with structural lesions on MRI. Clin Neurol Neurosurg 2014, 123, 64–68. [Google Scholar] [CrossRef]
- Brodie, M. J.; Barry, S. J.; Bamagous, G. A.; Norrie, J. D.; Kwan, P. Patterns of treatment response in newly diagnosed epilepsy. Neurology 2012, 78(20), 1548–1554. [Google Scholar] [CrossRef]
- Berg, A. T.; Shinnar, S. The risk of seizure recurrence following a first unprovoked seizure: a quantitative review. Neurology 1991, 41(7), 965–972. [Google Scholar] [CrossRef] [PubMed]
- Mohanraj, R.; Brodie, M. J. Early predictors of outcome in newly diagnosed epilepsy. Seizure 2013, 22(5), 333–344. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Chen, J.; Guo, H.; Ding, L.; Zhang, Y.; Xu, Y. High Mobility Group Protein B1 (HMGB1) and Interleukin-1beta as Prognostic Biomarkers of Epilepsy in Children. J Child Neurol 2018, 33(14), 909–917. [Google Scholar] [CrossRef] [PubMed]
- Chang, C. C.; Lui, C. C.; Lee, C. C.; Chen, S. D.; Chang, W. N.; Lu, C. H.; Chen, N. C.; Chang, A. Y.; Chan, S. H.; Chuang, Y. C. Clinical significance of serological biomarkers and neuropsychological performances in patients with temporal lobe epilepsy. BMC Neurol 2012, 12, 15. [Google Scholar] [CrossRef]
- Davalos, D.; Akassoglou, K. Fibrinogen as a key regulator of inflammation in disease. Semin Immunopathol 2012, 34(1), 43–62. [Google Scholar] [CrossRef]
- Sulimai, N.; Brown, J.; Lominadze, D. The Role of Nuclear Factor-Kappa B in Fibrinogen-Induced Inflammatory Responses in Cultured Primary Neurons. Biomolecules 2022, 12(12), 1741. [Google Scholar] [CrossRef]
- Peng, S.; Lv, K. The role of fibrinogen in traumatic brain injury: from molecular pathological mechanisms to clinical management. Eur J Trauma Emerg Surg 2022, 49, 1665–1672. [Google Scholar] [CrossRef]
- Vasse, M.; Paysant, J.; Soria, J.; Collet, J. P.; Vannier, J. P.; Soria, C. Regulation of fibrinogen biosynthesis by cytokines, consequences on the vascular risk. Haemostasis 1996, 26 Suppl 4, 331–339. [Google Scholar] [CrossRef]
- Morganti-Kossman, M. C.; Lenzlinger, P. M.; Hans, V.; Stahel, P.; Csuka, E.; Ammann, E.; Stocker, R.; Trentz, O.; Kossmann, T. Production of cytokines following brain injury: beneficial and deleterious for the damaged tissue. Mol Psychiatry 1997, 2(2), 133–136. [Google Scholar] [CrossRef]
- Pyun, J. M.; Ryoo, N.; Park, Y. H.; Kim, S. Fibrinogen Levels and Cognitive Profile Differences in Patients with Mild Cognitive Impairment. Dement Geriatr Cogn Disord 2020, 49(5), 489–496. [Google Scholar] [CrossRef]
- Xu, G.; Zhang, H.; Zhang, S.; Fan, X.; Liu, X. Plasma fibrinogen is associated with cognitive decline and risk for dementia in patients with mild cognitive impairment. Int J Clin Pract 2008, 62(7), 1070–1075. [Google Scholar] [CrossRef]
- Ishikawa, N.; Kobayashi, Y.; Fujii, Y.; Kobayashi, M. Increased interleukin-6 and high-sensitivity C-reactive protein levels in pediatric epilepsy patients with frequent, refractory generalized motor seizures. Seizure 2015, 25, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Fabene, P. F.; Navarro Mora, G.; Martinello, M.; Rossi, B.; Merigo, F.; Ottoboni, L.; Bach, S.; Angiari, S.; Benati, D.; Chakir, A.; et al. A role for leukocyte-endothelial adhesion mechanisms in epilepsy. Nat Med 2008, 14(12), 1377–1383. [Google Scholar] [CrossRef] [PubMed]
- Varvel, N. H.; Neher, J. J.; Bosch, A.; Wang, W.; Ransohoff, R. M.; Miller, R. J.; Dingledine, R. Infiltrating monocytes promote brain inflammation and exacerbate neuronal damage after status epilepticus. Proc Natl Acad Sci U S A 2016, 113(38), E5665–5674. [Google Scholar] [CrossRef] [PubMed]
- Shin, H. R.; Chu, K.; Lee, W. J.; Lee, H. S.; Kim, E. Y.; Son, H.; Moon, J.; Kim, N.; Jung, K. Y.; Jung, K. H.; et al. Neuropsychiatric symptoms and seizure related with serum cytokine in epilepsy patients. Sci Rep 2022, 12(1), 7138. [Google Scholar] [CrossRef] [PubMed]
- Zattoni, M.; Mura, M. L.; Deprez, F.; Schwendener, R. A.; Engelhardt, B.; Frei, K.; Fritschy, J. M. Brain infiltration of leukocytes contributes to the pathophysiology of temporal lobe epilepsy. J Neurosci 2011, 31(11), 4037–4050. [Google Scholar] [CrossRef]
- Lv, K.; Yuan, Q.; Fu, P.; Wu, G.; Wu, X.; Du, Z.; Yu, J.; Li, Z.; Hu, J. Impact of fibrinogen level on the prognosis of patients with traumatic brain injury: a single-center analysis of 2570 patients. World J Emerg Surg 2020, 15(1), 54. [Google Scholar] [CrossRef]
- Sikka, M.; Sodhi, R.; Kotru, M.; Singh, G. Markers of Fibrinolysis in Indian Patients with Isolated Head Trauma. Asian J Neurosurg 2019, 14(1), 118–121. [Google Scholar] [CrossRef]
- Pronto-Laborinho, A. C.; Lopes, C. S.; Conceição, V. A.; Gromicho, M.; Santos, N. C.; de Carvalho, M.; Carvalho, F. A. γ’ Fibrinogen as a Predictor of Survival in Amyotrophic Lateral Sclerosis. Front Cardiovasc Med 2021, 8, 715842. [Google Scholar] [CrossRef]
- Liguori, C.; Romigi, A.; Izzi, F.; Placidi, F.; Nuccetelli, M.; Cordella, A.; Bernardini, S.; Biagio, M. N. Complement system dysregulation in patients affected by Idiopathic Generalized Epilepsy and the effect of antiepileptic treatment. Epilepsy Res 2017, 137, 107–111. [Google Scholar] [CrossRef]
- de la Fuente, C.; Monreal, L.; Ceron, J.; Pastor, J.; Viu, J.; Anor, S. Fibrinolytic activity in cerebrospinal fluid of dogs with different neurological disorders. J Vet Intern Med 2012, 26(6), 1365–1373. [Google Scholar] [CrossRef] [PubMed]
- Chen, H. F.; Xu, L. P.; Luo, Z. Y.; Yu, Z. Q.; Li, Z. Y.; Cui, Q. Y.; Qin, L. M.; Ren, Y. Y.; Shen, H. S.; Tang, J. Q.; et al. Valproic acid-associated low fibrinogen and delayed intracranial hemorrhage: case report and mini literature review. Drug Des Devel Ther 2013, 7, 767–770. [Google Scholar] [CrossRef] [PubMed]
- Goerdt, C.; Rubins, H. B.; Swaim, W.; Folsom, A. Can phenytoin lower plasma fibrinogen concentrations? Thromb Res 1995, 79(3), 231–236. [Google Scholar] [CrossRef] [PubMed]
- Bavoux, F.; Fournier-Perhilou, A. I.; Wood, C.; Francoual, C.; Boccara, J. F. Neonatal fibrinogen depletion caused by sodium valproate. Ann Pharmacother 1994, 28(11), 1307. [Google Scholar] [CrossRef]
- Dale, B. M.; Purdie, G. H.; Rischbieth, R. H. Fibrinogen depletion with sodium valproate. Lancet 1978, 1(8077), 1316–1317. [Google Scholar] [CrossRef]
- Koh, S.; Lee, D. Y.; Cha, J. M.; Kim, Y.; Kim, H. H.; Yang, H. J.; Park, R. W.; Choi, J. Y. Association between pre-diagnostic serum uric acid levels in patients with newly diagnosed epilepsy and conversion rate to drug-resistant epilepsy within 5 years: A common data model analysis. Seizure 2024, 118, 103–109. [Google Scholar] [CrossRef]
- Parfenova, H.; Leffler, C. W.; Basuroy, S.; Liu, J.; Fedinec, A. L. Antioxidant roles of heme oxygenase, carbon monoxide, and bilirubin in cerebral circulation during seizures. J Cereb Blood Flow Metab 2012, 32(6), 1024–1034. [Google Scholar] [CrossRef]
Figure 1.
Routine blood markers related to final epilepsy outcome. (a) The final outcome showed a significant correlation with the blood level of fibrinogen, uric acid, total bilirubin and activated partial thromboplastin. (b) Fibrinogen levels showed the highest area under the curve among statistically significant blood parameters on final outcome. (c) The distribution of fibrinogen levels in relation to the final outcome is illustrated, along with the corresponding number of patients in each bin. Bars indicate the number of patients in each bin, while circles represent the percentage of remission among the patients in the bins. SF, seizure-free; NSF, non-seizure-free; aPTT, activated partial thromboplastin.
Figure 1.
Routine blood markers related to final epilepsy outcome. (a) The final outcome showed a significant correlation with the blood level of fibrinogen, uric acid, total bilirubin and activated partial thromboplastin. (b) Fibrinogen levels showed the highest area under the curve among statistically significant blood parameters on final outcome. (c) The distribution of fibrinogen levels in relation to the final outcome is illustrated, along with the corresponding number of patients in each bin. Bars indicate the number of patients in each bin, while circles represent the percentage of remission among the patients in the bins. SF, seizure-free; NSF, non-seizure-free; aPTT, activated partial thromboplastin.
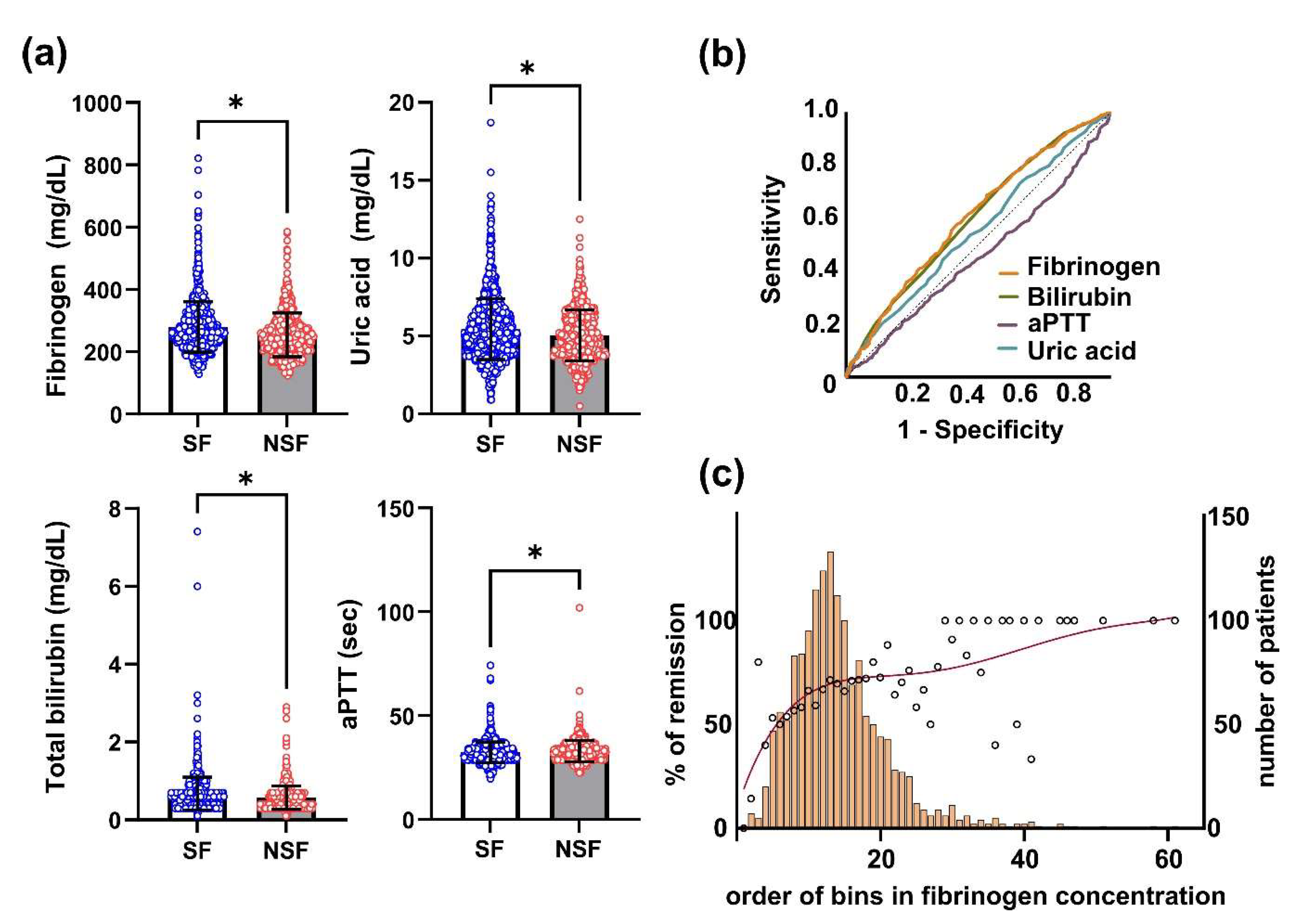
Figure 2.
Association of factors with the initial level of blood fibrinogen. (a) Correlation of fibrinogen level with meaningful continuous variables. (b) Comparison of fibrinogen with meaningful categorical variables. Sz, seizure; ANC, absolute neutrophil count, WBC, white blood cells.
Figure 2.
Association of factors with the initial level of blood fibrinogen. (a) Correlation of fibrinogen level with meaningful continuous variables. (b) Comparison of fibrinogen with meaningful categorical variables. Sz, seizure; ANC, absolute neutrophil count, WBC, white blood cells.
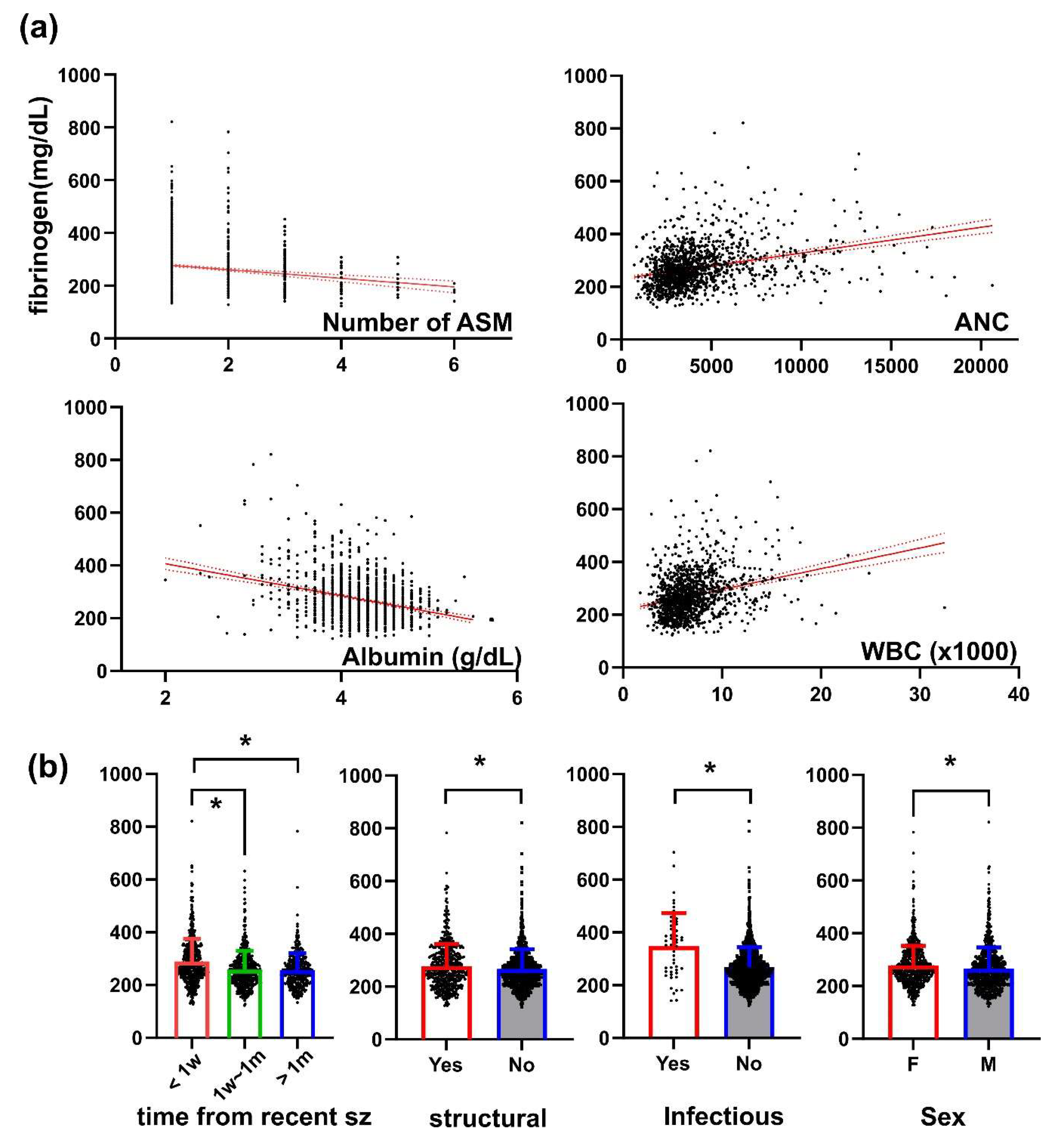

Table 1.
Demographics of the study population.
| Clinical parameters | Number of patients (%) |
|---|---|
| Sex (Female : Male) | 814 : 968 (45.7% : 54.3%) |
| Onset age | |
| mean ± SD (range) | 31.0 ± 20.2, (0-91) |
| Missing, N | 32 |
| Age of first visit (range) | 37.5 ± 18.0 (6-91) |
| Follow-up duration, month (range) | 104.5 ± 30.5 (36-161) |
| Epilepsy duration, year | |
| mean ± SD (range) | 6.3 ± 9.5 (0-56) |
| Missing, N | 32 |
| Newly diagnosed | 1026 (57.6%) |
| Unknown | 166 (9.3%) |
| Seizure types | |
| Focal | 1476 (82.9%) |
| Generalized | 281 (15.8%) |
| Unknown | 23 (1.3%) |
| Missing, N | 2 |
| Epilepsy classification | |
| Focal | 1387 (77.8%) |
| Generalized | 275 (15.4%) |
| Combined | 98 (5.5%) |
| Unknown | 22 (1.2%) |
| Etiology | |
| Structural | 626 (35.1%) |
| Genetic | 253 (14.2%) |
| Immune | 84 (4.7%) |
| Infectious | 51 (2.9%) |
| Hypoxic | 5 (0.3%) |
| metabolic | 3 (0.2%) |
| Unknown | 760 (42.6%) |
| History of febrile seizure | 138 (7.7%) |
| Family history of epilepsy | 55 (3.1%) |
| Presence of epileptiform discharge on EEG | |
| N (%) | 429 (26.3%) |
| Missing, N | 151 |
| Lesion on MRI | |
| N (%) | 764 (49.2%) |
| Missing, N | 229 |
| Hippocampal sclerosis | |
| N (%) | 101 (6.5%) |
| Missing, N | 229 |
| Final seizure-free | 609 (34.2%) |
| Number of initial ASMs | Range 1-6 (median 1) |
| Sampling time from a recent seizure | |
| <1 week | 608 (39.8%) |
| 1 week~1 month | 539 (35.3 %) |
| >1 month | 379 (24.8%) |
SD, standard deviation; N, number of patients; ASM, antiseizure medication.
Table 2.
Multiple logistic regression for the final outcome using clinical status, EEG, and MRI.
| B | SE | Wald | P value | Exp (B) | |
|---|---|---|---|---|---|
| Sex (Male = 1) | -0.331 | 0.125 | 6.976 | 0.008 | 0.719 |
| Febrile seizure | 0.438 | 0.228 | 3.692 | 0.055 | 1.550 |
| Epileptiform discharge | 0.456 | 0.138 | 10.981 | <0.001 | 1.577 |
| MRI lesion | 0.070 | 0.155 | 0.203 | 0.653 | 1.072 |
| Focal seizure | 0.917 | 0.842 | 1.185 | 0.276 | 2.501 |
| generalized epilepsy | 1.292 | .846 | 2.334 | 0.127 | 3.640 |
| Structural etiology | 0.428 | 0.158 | 7.311 | 0.007 | 1.533 |
| Genetic etiology | -0.680 | 0.504 | 1.823 | 0.177 | 0.507 |
| Hippocampal sclerosis | 0.436 | 0.257 | 2.883 | 0.090 | 1.546 |
| Number of initial ASM | 0.505 | 0.085 | 35.420 | <0.001 | 1.657 |
| Age at first visit | -0.002 | 0.008 | 0.052 | 0.819 | 0.998 |
| Onset age | -0.029 | 0.007 | 17.266 | <0.001 | 0.971 |
| Follow-up duration | 0.002 | 0.002 | 1.000 | 0.317 | 1.002 |
| Constant | -1.680 | 0.898 | 3.494 | 0.062 | 0.186 |
SE, standardized error.
Table 3.
Prognostic factors including blood parameters.
| B | SE | Wald | P value | Exp (B) | |
|---|---|---|---|---|---|
| Clinical parameters | |||||
| Sex (Male = 1) | -0.045 | 0.171 | 0.068 | 0.794 | 0.956 |
| Febrile seizure | 0.511 | 0.246 | 4.301 | 0.038 | 1.666 |
| Epileptiform discharge | 0.538 | 0.153 | 12.340 | <0.001 | 1.712 |
| MRI lesion | 0.008 | 0.174 | 0.002 | 0.963 | 1.008 |
| Focal seizure | 1.654 | 1.191 | 1.929 | 0.165 | 5.229 |
| Generalized epilepsy | 0.925 | 0.943 | 0.962 | 0.327 | 2.522 |
| Structural etiology | 0.562 | 0.178 | 10.016 | 0.002 | 1.755 |
| Genetic etiology | -0.417 | 0.601 | 0.481 | 0.488 | 0.659 |
| Hippocampal sclerosis | 0.400 | 0.280 | 2.039 | 0.153 | 1.492 |
| Number of initial ASM | 0.415 | 0.093 | 19.946 | <0.001 | 1.514 |
| Age at first visit | 0.003 | 0.009 | 0.139 | 0.709 | 1.003 |
| Onset age | -0.026 | 0.008 | 10.428 | 0.001 | 0.975 |
| Follow-up duration | 0.000 | 0.002 | 0.015 | 0.902 | 1.000 |
| Blood parameters | |||||
| WBC | -0.048 | 0.127 | 0.141 | 0.707 | 0.953 |
| Neutrophil | 0.026 | 0.025 | 1.142 | 0.285 | 1.027 |
| Lymphocyte | 0.022 | 0.023 | 0.906 | 0.341 | 1.022 |
| ANC | 0.000 | 0.000 | 0.158 | 0.691 | 1.000 |
| albumin | -0.059 | 0.216 | 0.076 | 0.783 | 0.942 |
| bilirubin | -0.570 | 0.245 | 5.431 | 0.020 | 0.565 |
| AST | 0.000 | 0.003 | 0.003 | 0.956 | 1.000 |
| glucose | -0.002 | 0.002 | 0.571 | 0.450 | 0.998 |
| BUN | -0.026 | 0.019 | 1.874 | 0.171 | 0.974 |
| creatinine | 0.294 | 0.229 | 1.646 | 0.199 | 1.342 |
| Uric acid | -0.118 | 0.046 | 6.540 | 0.011 | 0.888 |
| aPTT | 0.045 | 0.015 | 8.532 | 0.003 | 1.046 |
| fibrinogen | -0.004 | 0.001 | 11.815 | <0.001 | 0.996 |
| constant | -3.705 | 2.626 | 1.991 | 0.158 | 0.025 |
WBC, white blood cell; ANC, absolute neutrophil count; AST, aspartate transferase; BUN, blood urea nitrogen; aPTT, activated partial thromboplastin.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



