
Submitted:
28 August 2024
Posted:
28 August 2024
You are already at the latest version
Abstract
Background: Ventilatory strategies in acute respiratory distress syndrome patients aim to mitigate the risk of acute lung injury (ALI). However, prolonged utilization of these strategies may precipitate alveolar carbon dioxide elevation and pH reduction. This scoping review endeavors to present extant knowledge concerning hypercapnia effects in experimental models, with or without ALI, specifically focusing on delineating the immunologically mediated pulmonary tissue damage; Methods: A systematic exploration encompassing PubMed, Web of Science, ScienceDirect, Cochrane Reviews, and Scielo databases was undertaken. Articles published between January 1, 2008, and December 31, 2022, were screened for their elucidation of hypercapnia's immunological impact on lung tissue, utilizing experimental or biological models, irrespective of ALI presence; Results: Following duplicate removal and predefined criteria filtering, 30 pertinent articles scrutinizing hypercapnia's influence on pulmonary epithelium were identified. It was observed that hypercapnia induces perturbations in innate immune response gene transcription, mediated via Nuclear Factor-kappa B attenuation. Furthermore, a compromised innate immune response against injurious agents was noted. Concurrently, disruption and subsequent resealing of alveolar epithelial cells were evidenced, primarily through Na/K-ATPase endocytosis, impeding fluid reabsorption at the alveolar epithelium level; Conclusions: In experimental settings, with or without ALI, hypercapnia's immunomediated mechanisms exacerbate innate immune system impairment and disrupt the respiratory epithelium's repair and healing processes.
Keywords:
acute lung injury
; acute respiratory distress syndrome
; hypercapnia
; anti-inflammatory response
; biological models
1. Introduction
Acute Lung Injury (ALI), clinically exemplified as Acute Respiratory Distress Syndrome (ARDS), stands as a condition causing substantial mortality annually, while also imposing a considerable financial burden on healthcare resources [1,2,3]. The implementation of "protective" ventilatory strategies for ARDS mitigation has been instrumental in reducing the incidence of Ventilator-Induced Lung Injury (VILI), mitigating organ failure, and curtailing mortality rates [4,5,6]. Nonetheless, these strategies may inadvertently result in alveolar carbon dioxide (CO2) elevation and subsequent pH decline over protracted periods [4,5]. This ancillary consequence has been embraced under the term "permissive hypercapnia," positing it as a beneficial approach in ARDS management, alongside obstructive pathologies, among others [7,8,9]. Recent investigations have underscored the clinical ramifications of hypercapnia, demonstrating its significance as an autonomous predictor of mortality [10,11], along with implying a heightened ARDS severity among patients exhibiting sustained hypercapnia [12,13]. However, current evidence pertaining to hypercapnia's clinical impact remains scant, with contradictory perspectives on its underlying pathophysiological mechanisms [14,15]. Preclinical endeavors have elucidated hypercapnia's impact across various cellular strata within lung tissue [10,12,15,16,17,18,19].
Initial perusal of literature failed to unearth systematic reviews delving into the subject matter. Undertaking a scoping review, therefore, assumes paramount importance, serving to map out available literature and discern its relevance in informing future clinical investigations.
To furnish available insights into hypercapnia's effects within experimental paradigms, both with and without ALI, this scoping review endeavors to pinpoint and delineate the immunologically mediated repercussions of hypercapnia at the pulmonary tissue level. The overarching objective of this scoping review is to present extant literature pertaining to hypercapnia's effects within experimental models, encompassing acute lung injury scenarios, to characterize the immunomediated pulmonary tissue damage. The central inquiry guiding this review is: What are the immunomediated effects of hypercapnia in experimental models, with or without acute lung injury?
2. Results
The electronic database search yielded 3541 records, supplemented by an additional 113 records sourced from alternative channels, resulting in a total of 3654 articles. Following deduplication using Endnote X8, 2371 unique articles remained. Subsequent screening of titles and abstracts led to the exclusion of 2289 articles. Thereafter, a detailed examination of 82 full-text articles was conducted by two research team members to assess their eligibility for inclusion in the scoping review, with an additional 52 articles excluded for failing to address the research question. Ultimately, 30 articles met the inclusion criteria (Figure 1; PRISMA Flow Diagram summarizing the search strategy). Furthermore, details of the experimental articles, including authorship, publication year, and country of origin, are provided in Table 1.
In the subsequent phase of the review, data extraction and synthesis of results from the included studies were conducted in accordance with the study objectives and research question. This extraction process adhered to the scoping review methodology delineated by Levac et al. [20]. Subsequently, these results were categorized based on the effect of hypercapnia on pulmonary tissue, particularly focusing on the respiratory epithelium and the innate immune response, defined as the primary line of defense, encompassing phagocytes (neutrophils and macrophages), dendritic cells, and complement proteins [21].
2.1. Innate Immune Response
Hypercapnia exerts transcriptional alterations within the innate immune response, as reported in 33.3% (n = 10/30) of the included articles [22,18,23,24,25,26,27,28,29,30]. Among the 10 experimental studies, 80% (8/10) indicated that the most prevalent mechanism by which hypercapnia modulates innate immune response transcription is by attenuating the canonical Nuclear Factor-kappa B (NF-kB) pathway [22,23,25,26,27,28]. Another notable effect observed in experimental studies is the compromised capacity of the innate immune response against external aggressors, documented in 50% (n = 15/30) of the reviewed articles [18,23,24,26,17,31,32,33,34,35,36,37], with particular emphasis on 4 in vivo models of ALI attributable to infectious agents, where hypercapnia adversely affected phagocytic activity [18,17,31,33]. Moreover, in one biological model, hypercapnia was found to reduce autophagy and bacterial viability [35]. Additionally, a subset of biological models identified hypercapnia's propensity to dampen the expression of genes associated with the inflammatory response [23,24,26,30,32,33,34,36,37]. Conversely, Gates et al.[33] demonstrated that hypercapnia exacerbated mortality, elevated bacterial load, and decreased pulmonary levels of interleukin 6 (IL-6) and tumor necrosis factor (TNF) during the early stages of infection in an ALI model induced by pneumonia (see Table 2).
2.2. Respiratory epithelium
Hypercapnia-induced disruption and subsequent resealing of alveolar epithelial cells were observed in 36.7% (n = 11/30) of the experimental studies included in the scoping review [22,38,39,40,41,42,43,44,45,46,47,48]. Mechanisms elucidated in these studies include reports of elevated CO2 levels promoting Na/K-ATPase endocytosis, thereby impeding fluid reabsorption at the alveolar epithelium [38,40,42,46,47,48]. Moreover, other investigations highlighted hypercapnia's impact on respiratory epithelium healing and repair [22,39,41,42,43,45]. See Table 2 for details.
3. Discussion
Authors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted. Our review delineated that in experimental models, with or without lung injury, hypercapnia, irrespective of metabolic acidosis, can influence innate cellular response by attenuating the canonical NF-kB pathway. This pathway serves as a pivotal transcription factor regulating genes associated with immunity, repair, and inflammation, thereby diminishing autophagy, bacterial death, and modulating the inflammatory response by attenuating IL-6 and TNF production [10,22,23,25,26,27,28,49,50,51]. Consequently, a reduced capacity of the innate immune response against aggressor agents ensues, affecting phagocyte activity, autophagy, bacterial death, and the expression of inflammatory molecules, thereby facilitating bacterial propagation and replication [30,31,32,33,34,35,36,37,52,53,54].
As per experimental investigations, the mechanism underlying hypercapnia's alteration of the respiratory epithelium, with or without metabolic acidosis, involves inhibiting fluid reabsorption at the alveolar epithelium level through various pathways. This includes an upsurge in cytosolic Ca++ concentration, initiating a cascade implicating calcium-calmodulin-dependent kinases, which induce AMPc-activated protein kinase expression, thereby promoting endocytosis and reducing Na/K-ATPase transporters on the basal membrane of the alveolar epithelium, ultimately impacting pulmonary clearance [38,40,42,44,46,47,48,55,56,57]. Another reported mechanism in preclinical models indicates that exposure to hypercapnia contributes to deficient respiratory epithelium repair by activating adenylate cyclase, thereby delaying the resealing and repair of alveolar epithelia [22,39,45].
3.1. Study Limitations
The aim of our study was to furnish a comprehensive scoping review encompassing all extant literature concerning the effects of hypercapnia in experimental models, with or without lung injury. Although our search strategy was designed in accordance with PRISMA guidelines, we acknowledge the potential omission of eligible studies from alternative databases. Furthermore, due to the adopted methodology, our review lacked a methodological quality assessment of the included studies. Despite these constraints, our review comprehensively encapsulated all experimental models, potentially guiding future research endeavors aimed at elucidating the immunological implications of hypercapnia and its clinical ramifications in patients with or without lung injury.
4. Materials and Methods
4.1. Eligibility criteria
The methodology employed in this review adheres to the scoping review methodologies delineated by Levac et al. in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses—Extension for Scoping Reviews (PRISMA-ScR) guidelines [20]. The principal aim was to delineate the immunologically mediated effects of hypercapnia on pulmonary tissue (Table A1). Solely studies conducted in experimental models were encompassed, given the absence of clinical investigations. The review exclusively considered data published in English and Spanish between January 1, 2008, and December 31, 2022.
4.2. Search strategy
A tripartite search strategy was enacted. Initially, exploration was confined to PubMed, Web of Science, ScienceDirect, Cochrane Reviews, and Scielo to identify terms and keywords present within titles and abstracts. Subsequently, a comprehensive search encompassing all identified keywords and terms across all enlisted databases was executed. Thirdly, manual perusal of reference lists was conducted to identify articles furnishing supplementary information.
4.3. Information sources
The search was conducted across diverse databases, namely PubMed, Web of Science, ScienceDirect, Cochrane Reviews, and Scielo. To encapsulate preclinical research, search terms encompassed experimental or biological models. The search strategy amalgamated MeSH terms and pertinent keywords, tailored to each database, encompassing acute lung injury, adult respiratory distress syndrome, pneumonia, in tandem with hypercapnia and anti-inflammation. Please refer to Table A2 for the exhaustive search strategy.
4.4. Data Extraction
Relevant data from included studies were methodically extracted to address the review query, in alignment with the methodological framework delineated by Levac et al. [20]. Extracted parameters encompassed the demographic profile of the studied population, experimental or biological models with or without ALI, focal domain, and the immunologically mediated ramifications of hypercapnia on pulmonary tissue. To classify the thematic underpinning of the research, precedence was accorded to antecedent investigations, which encompassed experimental models with or without ALI subjected to heightened CO2 concentration and their ensuing immunomodulatory ramifications.
4.5. Results mapping
The collated data are meticulously tabulated to furnish a comprehensive descriptive synopsis, commensurate with the overarching objective and inquiry of the scoping review.
5. Conclusions
Our scoping review elucidated significant insights in experimental models, with or without lung injury, pertaining to the role of hypercapnia and its immunomediated mechanisms. This characterization delineated a compromised innate immune system capacity, alongside alterations in respiratory epithelium repair and healing. Future clinical investigations are warranted to assess the immunomediated clinical advantages of hypercapnia.
Author Contributions
Conceptualization, E.O.-R. and J.C.-G.; writing—original draft preparation, E.O.-R., J.C.-G., D.R.-B., M.B.-L., E.G.-R. and C.D.-C.; project administration, E.O.-R.; writing—review and editing, E.O.-R., J.C.-G., D.R.-B., M.B.-L., E.G.-R., J.P.-P., J.V.-T., J.E.-G., and C.D.-C. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. All authors have read and agreed to the published version of the manuscript.
Funding
Not applicable.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data used and/or analyzed during the present study are available from the corresponding author upon reasonable request.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

Table A1.
Prisma-ScR checklist.
| Section | Item | PRISMA-ScR checklist item | Page # |
|---|---|---|---|
| Title | |||
| Title | 1 | Identify the report as a scoping review | 1 |
| Structured summary | 2 | Provide a structured abstract that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives | 1 |
| Introduction | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | 1, 2 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | 2 |
| Methods | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and if available, provide registration information, including the registration numbe | NA |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale | 10, 11 |
| Information sources | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed | 11 |
| Search | 8 | Present the full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | 11, Appendix A2 |
| Selection of sources of evidence | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review | 11 |
| Data charting process | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | 11, Figure 1. PRISMA-ScR checklist. |
| Data ítems | 11 | List and define all variables for which data were sought and any assumptions and simplifications made | 11 |
| Critical appraisal of individua sources of evidence | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate) | 11 |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | 11 |
| Result | |||
| Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram | Figure 1. PRISMA-ScR checklist. |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations | Table 2 |
| Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (see item 12) | |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | Table 2, figures 2 and 3 |
| Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives | Table 2 |
| Discussion | |||
| Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups | 2 - 10 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | 10 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | 11 |
| Funding | |||
| Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review | NA |
Table A2.
Search Strategy.
| Search number | Search terms |
|---|---|
| 1 | Pneumonia |
| 2 | Hypercapnia |
| 3 | Acute respiratory distress syndrome (ARDS) |
| 4 | Ventilator-Associated Pneumonia (VAP) |
| 5 | Anti-Inflammatories |
| 6 | Anti-Inflammatories |
| 7 | 1 AND 2 AND 3 |
| 8 | 4 AND 2 |
| 9 | 5 AND 2 AND 1 |
References
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA [Internet]. 2016 Feb 23;315(8):788. [CrossRef]
- Máca J, Jor O, Holub M, Sklienka P, Burša F, Burda M, et al. Past and Present ARDS Mortality Rates: A Systematic Review. Respir Care [Internet]. 2017 Jan;62(1):113–22. [CrossRef]
- Wu N, Hanrahan J, Bornstein J, Chen S-Y. Healthcare costs utilization and costs of patients hospitalized with acute respiratory distress syndrome (ARDS) in US commercially-insured individuals and Medicare beneficiaries. In: 21 Acute Critical Care [Internet]. European Respiratory Society; 2015. p. PA2139. [CrossRef]
- Amato MBP, Barbas CSV, Medeiros DM, Magaldi RB, Schettino GP, Lorenzi-Filho G, et al. Effect of a Protective-Ventilation Strategy on Mortality in the Acute Respiratory Distress Syndrome. N Engl J Med [Internet]. 1998 Feb 5;338(6):347–54. [CrossRef]
- The Acute Respiratory Distress Syndrome Network. Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome. N Engl J Med [Internet]. 2000 May 4;342(18):1301–8. [CrossRef]
- Petrucci N, De Feo C. Lung protective ventilation strategy for the acute respiratory distress syndrome. Cochrane Database Syst Rev [Internet]. 2013 Feb 28; [CrossRef]
- Tuxen D V., Williams TJ, Scheinkestel CD, Czarny D, Bowes G. Use of a Measurement of Pulmonary Hyperinflation to Control the Level of Mechanical Ventilation in Patients with Acute Severe Asthma. Am Rev Respir Dis [Internet]. 1992 Nov;146(5_pt_1):1136–42. [CrossRef]
- Hickling KG, Henderson SJ, Jackson R. Low mortality associated with low volume pressure limited ventilation with permissive hypercapnia in severe adult respiratory distress syndrome. Intensive Care Med [Internet]. 1990 Sep;16(6):372–7. [CrossRef]
- Hickling KG, Walsh J, Henderson S, Jackson R. Low mortality rate in adult respiratory distress syndrome using low-volume, pressure-limited ventilation with permissive hypercapnia: A prospective study. Crit Care Med [Internet]. 1994 Oct;22(10):1568–78. [CrossRef]
- Shigemura M, Lecuona E, Sznajder JI. Effects of hypercapnia on the lung. J Physiol [Internet]. 2017 Apr 15;595(8):2431–7. [CrossRef]
- Nin N, Muriel A, Peñuelas O, Brochard L, Lorente JA, Ferguson ND, et al. Severe hypercapnia and outcome of mechanically ventilated patients with moderate or severe acute respiratory distress syndrome. Intensive Care Med [Internet]. 2017 Feb 20;43(2):200–8. [CrossRef]
- Chonghaile MN, Higgins BD, Costello J, Laffey JG. Hypercapnic Acidosis Attenuates Lung Injury Induced by Established Bacterial Pneumonia. Anesthesiology [Internet]. 2008 Nov 1;109(5):837–48. [CrossRef]
- Madotto F, Rezoagli E, McNicholas BA, Pham T, Slutsky AS, Bellani G, et al. Patterns and Impact of Arterial CO2 Management in Patients With Acute Respiratory Distress Syndrome. Chest [Internet]. 2020 Nov;158(5):1967–82. [CrossRef]
- Gendreau S, Geri G, Pham T, Vieillard-Baron A, Mekontso Dessap A. The role of acute hypercapnia on mortality and short-term physiology in patients mechanically ventilated for ARDS: a systematic review and meta-analysis. Intensive Care Med [Internet]. 2022 May 16;48(5):517–34. [CrossRef]
- Masterson C, Horie S, McCarthy SD, Gonzalez H, Byrnes D, Brady J, et al. Hypercapnia in the critically ill: insights from the bench to the bedside. Interface Focus [Internet]. 2021 Apr 6;11(2):20200032. [CrossRef]
- Beitler JR, Malhotra A, Thompson BT. Ventilator-induced Lung Injury. Clin Chest Med [Internet]. 2016 Dec;37(4):633–46. [CrossRef]
- O’Croinin DF, Nichol AD, Hopkins N, Boylan J, O’Brien S, O’Connor C, et al. Sustained hypercapnic acidosis during pulmonary infection increases bacterial load and worsens lung injury*. Crit Care Med [Internet]. 2008 Jul;36(7):2128–35. [CrossRef]
- Wang N, Gates KL, Trejo H, Favoreto S, Schleimer RP, Sznajder JI, et al. Elevated CO 2 selectively inhibits interleukin-6 and tumor necrosis factor expression and decreases phagocytosis in the macrophage. FASEB J [Internet]. 2010 Jul 24;24(7):2178–90. [CrossRef]
- Matthay MA, Zemans RL, Zimmerman GA, Arabi YM, Beitler JR, Mercat A, et al. Acute respiratory distress syndrome. Nat Rev Dis Prim [Internet]. 2019 Mar 14;5(1):18. [CrossRef]
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med [Internet]. 2018 Oct 2;169(7):467–73. [CrossRef]
- Reyes Martín E, Prieto Martín A, Díaz Martín D, Álvarez-Mon Soto M. Inmunidad innata e inmunidad adaptativa. Med - Programa Form Médica Contin Acreditado [Internet]. 2013 Mar;11(28):1760–7. [CrossRef]
- O’Toole D, Hassett P, Contreras M, Higgins BD, McKeown STW, McAuley DF, et al. Hypercapnic acidosis attenuates pulmonary epithelial wound repair by an NF- B dependent mechanism. Thorax [Internet]. 2009 Nov 1;64(11):976–82. [CrossRef]
- Cummins EP, Oliver KM, Lenihan CR, Fitzpatrick SF, Bruning U, Scholz CC, et al. NF-κB Links CO2 Sensing to Innate Immunity and Inflammation in Mammalian Cells. J Immunol [Internet]. 2010 Oct 1;185(7):4439–45. [CrossRef]
- Oliver KM, Lenihan CR, Bruning U, Cheong A, Laffey JG, McLoughlin P, et al. Hypercapnia Induces Cleavage and Nuclear Localization of RelB Protein, Giving Insight into CO2 Sensing and Signaling. J Biol Chem [Internet]. 2012 Apr;287(17):14004–11. [CrossRef]
- Contreras M, Ansari B, Curley G, Higgins BD, Hassett P, O’Toole D, et al. Hypercapnic acidosis attenuates ventilation-induced lung injury by a nuclear factor-κB–dependent mechanism. Crit Care Med [Internet]. 2012 Sep;40(9):2622–30. [CrossRef]
- Yang W, Yue Z, Cui X, Guo Y, Zhang L, Zhou H, et al. Comparison of the effects of moderate and severe hypercapnic acidosis on ventilation-induced lung injury. BMC Anesthesiol [Internet]. 2015 Dec 30;15(1):67. [CrossRef]
- Masterson C, O’Toole D, Leo A, McHale P, Horie S, Devaney J, et al. Effects and Mechanisms by Which Hypercapnic Acidosis Inhibits Sepsis-Induced Canonical Nuclear Factor-κB Signaling in the Lung. Crit Care Med [Internet]. 2016 Apr;44(4):e207–17. [CrossRef]
- Horie S, Ansari B, Masterson C, Devaney J, Scully M, O’Toole D, et al. Hypercapnic acidosis attenuates pulmonary epithelial stretch-induced injury via inhibition of the canonical NF-κB pathway. Intensive Care Med Exp [Internet]. 2016 Dec 22;4(1):8. [CrossRef]
- Keogh CE, Scholz CC, Rodriguez J, Selfridge AC, von Kriegsheim A, Cummins EP. Carbon dioxide-dependent regulation of NF-κB family members RelB and p100 gives molecular insight into CO2-dependent immune regulation. J Biol Chem [Internet]. 2017 Jul;292(27):11561–71. [CrossRef]
- Liu Y, Chacko BK, Ricksecker A, Shingarev R, Andrews E, Patel RP, et al. Modulatory effects of hypercapnia on in vitro and in vivo pulmonary endothelial–neutrophil adhesive responses during inflammation. Cytokine [Internet]. 2008 Oct;44(1):108–17. [CrossRef]
- Ni Chonghaile M, Higgins BD, Costello JF, Laffey JG. Hypercapnic acidosis attenuates severe acute bacterial pneumonia-induced lung injury by a neutrophil-independent mechanism*. Crit Care Med [Internet]. 2008 Dec;36(12):3135–44. [CrossRef]
- Peltekova V, Engelberts D, Otulakowski G, Uematsu S, Post M, Kavanagh BP. Hypercapnic acidosis in ventilator-induced lung injury. Intensive Care Med [Internet]. 2010 May 6;36(5):869–78. [CrossRef]
- Gates KL, Howell HA, Nair A, Vohwinkel CU, Welch LC, Beitel GJ, et al. Hypercapnia Impairs Lung Neutrophil Function and Increases Mortality in Murine Pseudomonas Pneumonia. Am J Respir Cell Mol Biol [Internet]. 2013 Nov;49(5):821–8. [CrossRef]
- Nardelli LM, Rzezinski A, Silva JD, Maron-Gutierrez T, Ornellas DS, Henriques I, et al. Effects of acute hypercapnia with and without acidosis on lung inflammation and apoptosis in experimental acute lung injury. Respir Physiol Neurobiol [Internet]. 2015 Jan;205:1–6. [CrossRef]
- Casalino-Matsuda SM, Nair A, Beitel GJ, Gates KL, Sporn PHS. Hypercapnia Inhibits Autophagy and Bacterial Killing in Human Macrophages by Increasing Expression of Bcl-2 and Bcl-xL. J Immunol [Internet]. 2015 Jun 1;194(11):5388–96. [CrossRef]
- Casalino-Matsuda SM, Wang N, Ruhoff PT, Matsuda H, Nlend MC, Nair A, et al. Hypercapnia Alters Expression of Immune Response, Nucleosome Assembly and Lipid Metabolism Genes in Differentiated Human Bronchial Epithelial Cells. Sci Rep [Internet]. 2018 Sep 10;8(1):13508. [CrossRef]
- Casalino-Matsuda SM, Berdnikovs S, Wang N, Nair A, Gates KL, Beitel GJ, et al. Hypercapnia selectively modulates LPS-induced changes in innate immune and DNA replication-related gene transcription in the macrophage. Interface Focus [Internet]. 2021 Apr 6;11(2):20200039. [CrossRef]
- Vadász I, Dada LA, Briva A, Trejo HE, Welch LC, Chen J, et al. AMP-activated protein kinase regulates CO2-induced alveolar epithelial dysfunction in rats and human cells by promoting Na,K-ATPase endocytosis. J Clin Invest [Internet]. 2008 Jan 10; [CrossRef]
- Nichol AD, OʼCronin DF, Howell K, Naughton F, OʼBrien S, Boylan J, et al. Infection-induced lung injury is worsened after renal buffering of hypercapnic acidosis. Crit Care Med [Internet]. 2009 Nov;37(11):2953–61. [CrossRef]
- Welch LC, Lecuona E, Briva A, Trejo HE, Dada LA, Sznajder JI. Extracellular signal-regulated kinase (ERK) participates in the hypercapnia-induced Na,K-ATPase downregulation. FEBS Lett [Internet]. 2010 Sep 24;584(18):3985–9. [CrossRef]
- Vohwinkel CU, Lecuona E, Sun H, Sommer N, Vadász I, Chandel NS, et al. Elevated CO2 Levels Cause Mitochondrial Dysfunction and Impair Cell Proliferation. J Biol Chem [Internet]. 2011 Oct;286(43):37067–76. [CrossRef]
- Vadász I, Dada LA, Briva A, Helenius IT, Sharabi K, Welch LC, et al. Evolutionary Conserved Role of c-Jun-N-Terminal Kinase in CO2-Induced Epithelial Dysfunction. Königshoff M, editor. PLoS One [Internet]. 2012 Oct 8;7(10):e46696. [CrossRef]
- Lecuona E, Sun H, Chen J, Trejo HE, Baker MA, Sznajder JI. Protein Kinase A-Iα Regulates Na,K-ATPase Endocytosis in Alveolar Epithelial Cells Exposed to High CO 2 Concentrations. Am J Respir Cell Mol Biol [Internet]. 2013 May;48(5):626–34. [CrossRef]
- Gwoździńska P, Buchbinder BA, Mayer K, Herold S, Morty RE, Seeger W, et al. Hypercapnia Impairs ENaC Cell Surface Stability by Promoting Phosphorylation, Polyubiquitination and Endocytosis of β-ENaC in a Human Alveolar Epithelial Cell Line. Front Immunol [Internet]. 2017 May 23;8. [CrossRef]
- Cortes-Puentes GA, Westerly B, Schiavo D, Wang S, Stroetz R, Walters B, et al. Hypercapnia Alters Alveolar Epithelial Repair by a pH-Dependent and Adenylate Cyclase-Mediated Mechanism. Sci Rep [Internet]. 2019 Jan 23;9(1):349. [CrossRef]
- Kryvenko V, Wessendorf M, Morty RE, Herold S, Seeger W, Vagin O, et al. Hypercapnia Impairs Na,K-ATPase Function by Inducing Endoplasmic Reticulum Retention of the β-Subunit of the Enzyme in Alveolar Epithelial Cells. Int J Mol Sci [Internet]. 2020 Feb 21;21(4):1467. [CrossRef]
- Gabrielli NM, Mazzocchi LC, Kryvenko V, Tello K, Herold S, Morty RE, et al. TRAF2 Is a Novel Ubiquitin E3 Ligase for the Na,K-ATPase β-Subunit That Drives Alveolar Epithelial Dysfunction in Hypercapnia. Front Cell Dev Biol [Internet]. 2021 Jul 2;9. [CrossRef]
- Kryvenko V, Wessendorf M, Tello K, Herold S, Morty RE, Seeger W, et al. Hypercapnia Induces Inositol-Requiring Enzyme 1α–Driven Endoplasmic Reticulum–associated Degradation of the Na,K-ATPase β-Subunit. Am J Respir Cell Mol Biol [Internet]. 2021 Dec;65(6):615–29. [CrossRef]
- Curley G, Laffey JG, Kavanagh BP. Bench-to-bedside review: Carbon dioxide. Crit Care [Internet]. 2010;14(2):220. [CrossRef]
- Morales Quinteros L, Bringué Roque J, Kaufman D, Artigas Raventós A. Importance of carbon dioxide in the critical patient: Implications at the cellular and clinical levels. Med Intensiva (English Ed [Internet]. 2019 May;43(4):234–42. [CrossRef]
- Vadász I, Hubmayr RD, Nin N, Sporn PHS, Sznajder JI. Hypercapnia: A Nonpermissive Environment for the Lung. Am J Respir Cell Mol Biol [Internet]. 2012 Apr;46(4):417–21. [CrossRef]
- Curley GF, Kavanagh BP, Laffey JG. Hypocapnia and Hypercapnia. In: Murray and Nadel’s Textbook of Respiratory Medicine [Internet]. Elsevier; 2016. p. 1527–1546.e8. [CrossRef]
- Curley G, Hayes M, Laffey JG. Can “permissive” hypercapnia modulate the severity of sepsis-induced ALI/ARDS? Crit Care [Internet]. 2011;15(2):212. [CrossRef]
- Silvestre C, Vyas H. Is permissive hypercapnia helpful or harmful? Paediatr Child Health (Oxford) [Internet]. 2015 Apr;25(4):192–5. [CrossRef]
- Hamacher J, Hadizamani Y, Borgmann M, Mohaupt M, Männel DN, Moehrlen U, et al. Cytokine–Ion Channel Interactions in Pulmonary Inflammation. Front Immunol [Internet]. 2018 Jan 4;8. [CrossRef]
- Baloğlu E, Mairbäurl H. In Search of a Sensor: How Does CO 2 Regulate Alveolar Ion Transport? Am J Respir Cell Mol Biol [Internet]. 2021 Dec;65(6):571–2. [CrossRef]
- Vadász I, Sznajder JI. Gas Exchange Disturbances Regulate Alveolar Fluid Clearance during Acute Lung Injury. Front Immunol [Internet]. 2017 Jul 4;8. [CrossRef]
Figure 1.
RISMA-ScR checklist.
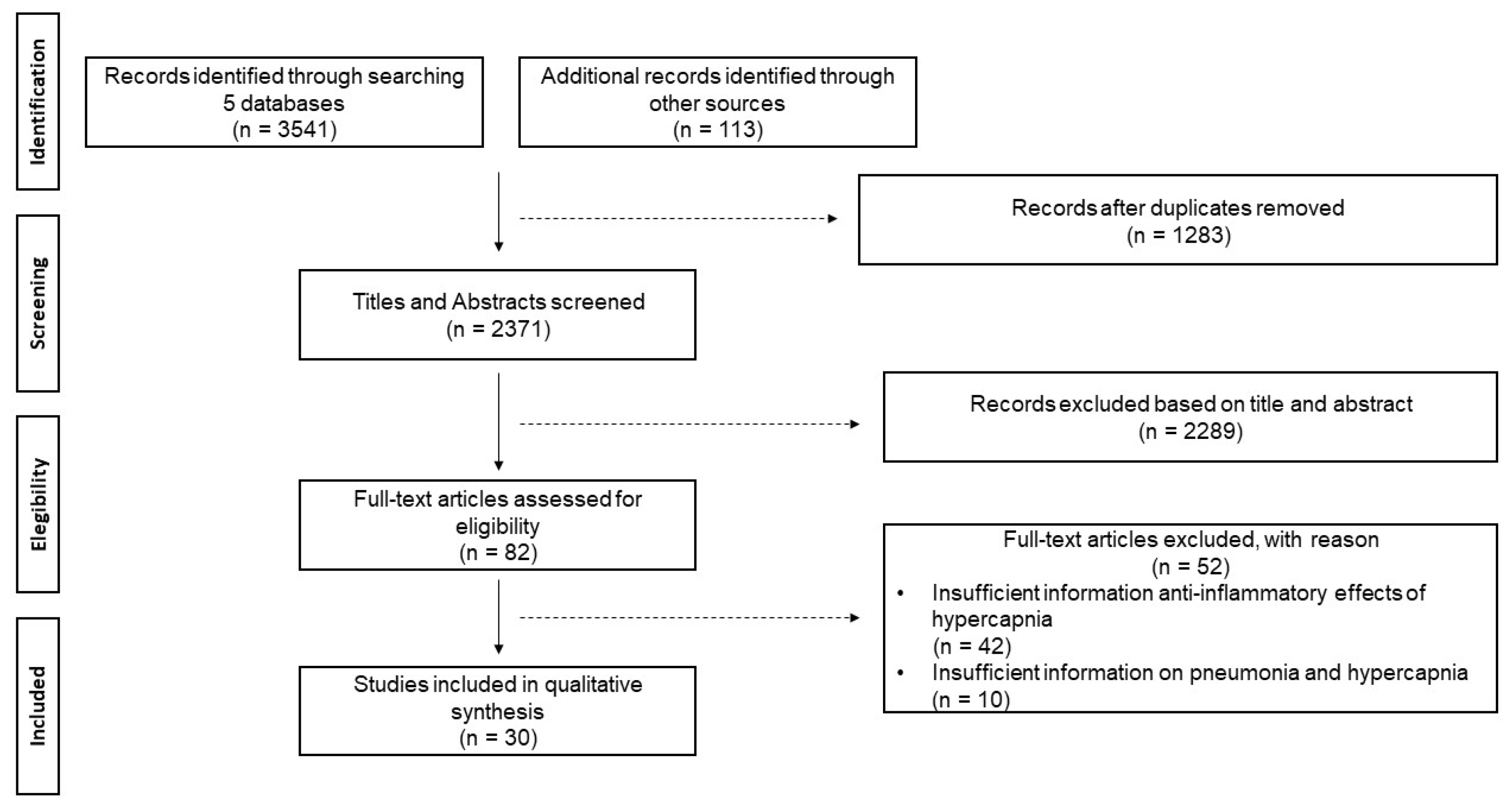
Figure 2.
Anti-inflammatory effects of hypercapnia in models experimental acute pulmonay injury. Hypercapnic acidosis attenuates the immune response and allows alveolar disruption that can allow bacterial propagation and replication. Abbreviations: ARDS: Acute Respiratory Distress Syndrome; V: Ventilation; Q: Perfusion. Designed by the Research Group in Intensive Medicine and Comprehensive Care (GRIMICI).
Figure 2.
Anti-inflammatory effects of hypercapnia in models experimental acute pulmonay injury. Hypercapnic acidosis attenuates the immune response and allows alveolar disruption that can allow bacterial propagation and replication. Abbreviations: ARDS: Acute Respiratory Distress Syndrome; V: Ventilation; Q: Perfusion. Designed by the Research Group in Intensive Medicine and Comprehensive Care (GRIMICI).
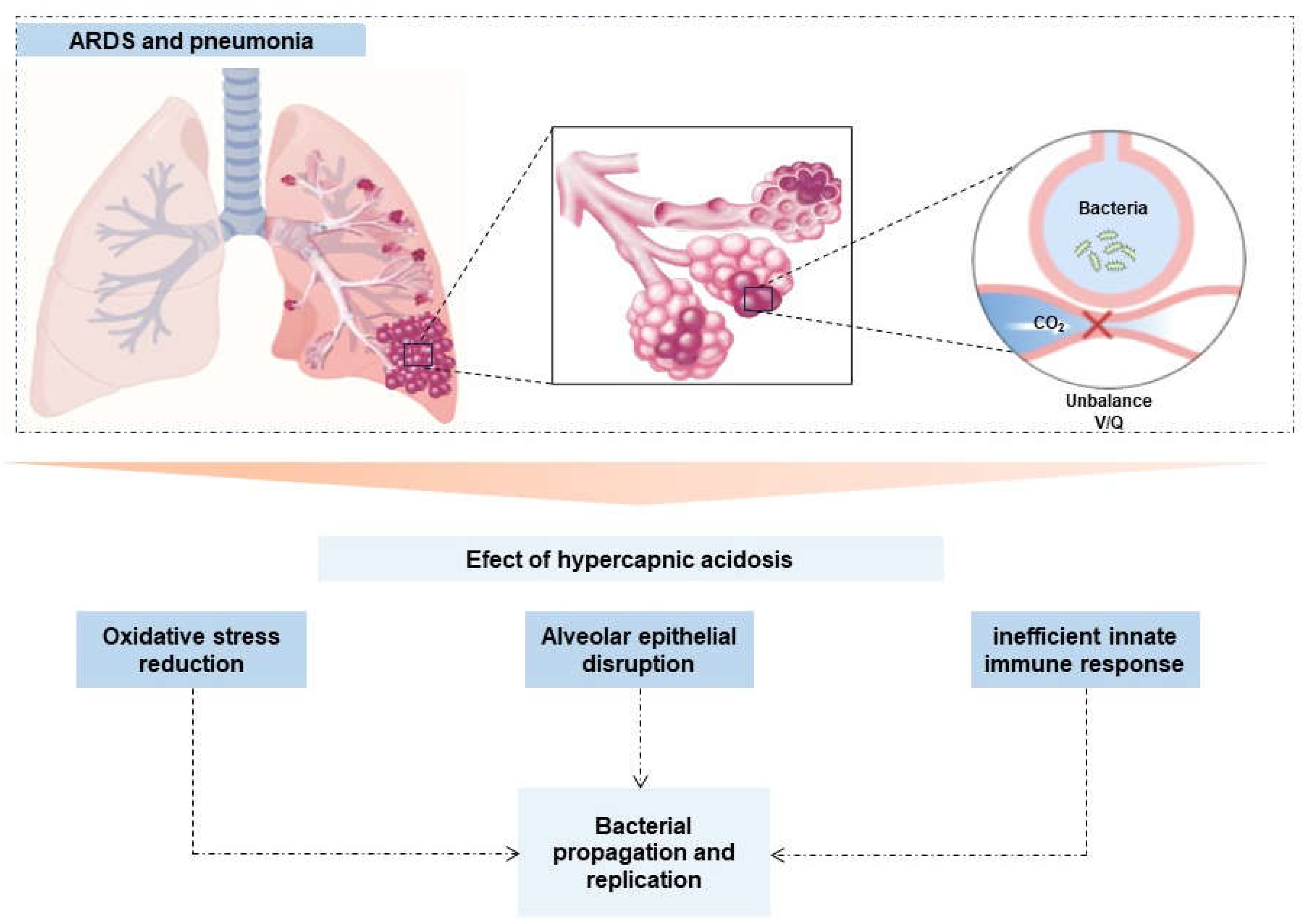
Figure 3.
Anti-inflammatory effects of hypercapnia in models experimental acute pulmonay injury. A. The interaction of hypercapnia and NF-kB pathways is visualized. B. The interaction of hypercapnia with intracellular biological pathways is visualized to inactivate proinflammatory cytokines and promote apoptosis that leads to cellular damage. C. The interaction of hypercapnia in the respiratory epithelium is visualized, which entails the endocytosis of ENac and Na/K-ATPase, allowing alveolar disruption. D. Hypercapnia impairs mitochondrial dysfunction that leads to alveolar disruption and inhibits the pulmonary reparative role. Abbreviations: CO2: Carbon dioxide; O2: Oxygen; ATI: flattened alveolar type I; ATII: cuboidal alveolar type II; IκB: Inhibitor of kappa B; NF-κB: Nuclear Factor-kappa B; TNF: Tumor Necrosis Factor; Bcl-2: B-cell lymphoma 2; Bcl-xL: B-cell lymphoma-extra large protein; CXCL1: Chemokine Ligand 1; CXCL2: Chemokine Ligand 2; CXCL14: Chemokine Ligand 14; CCL28: Chemokine Ligand 28; ERK: Extracellular signal-regulated kinase; AMPK: AMP-activated protein kinase; PKC: Protein kinase C; JNK: c-Jun N-terminal kinases; AC: Adenylate cyclase; ENaC: Epithelial sodium channels; CCL2: Chemokine Ligand 2; ICAM1: Intercellular Adhesion Molecule 1; IDH2: Isocitrate dehydrogenase 2. ATP: Adenosine triphosphate. Designed by the Research Group in Intensive Medicine and Comprehensive Care (GRIMICI).
Figure 3.
Anti-inflammatory effects of hypercapnia in models experimental acute pulmonay injury. A. The interaction of hypercapnia and NF-kB pathways is visualized. B. The interaction of hypercapnia with intracellular biological pathways is visualized to inactivate proinflammatory cytokines and promote apoptosis that leads to cellular damage. C. The interaction of hypercapnia in the respiratory epithelium is visualized, which entails the endocytosis of ENac and Na/K-ATPase, allowing alveolar disruption. D. Hypercapnia impairs mitochondrial dysfunction that leads to alveolar disruption and inhibits the pulmonary reparative role. Abbreviations: CO2: Carbon dioxide; O2: Oxygen; ATI: flattened alveolar type I; ATII: cuboidal alveolar type II; IκB: Inhibitor of kappa B; NF-κB: Nuclear Factor-kappa B; TNF: Tumor Necrosis Factor; Bcl-2: B-cell lymphoma 2; Bcl-xL: B-cell lymphoma-extra large protein; CXCL1: Chemokine Ligand 1; CXCL2: Chemokine Ligand 2; CXCL14: Chemokine Ligand 14; CCL28: Chemokine Ligand 28; ERK: Extracellular signal-regulated kinase; AMPK: AMP-activated protein kinase; PKC: Protein kinase C; JNK: c-Jun N-terminal kinases; AC: Adenylate cyclase; ENaC: Epithelial sodium channels; CCL2: Chemokine Ligand 2; ICAM1: Intercellular Adhesion Molecule 1; IDH2: Isocitrate dehydrogenase 2. ATP: Adenosine triphosphate. Designed by the Research Group in Intensive Medicine and Comprehensive Care (GRIMICI).
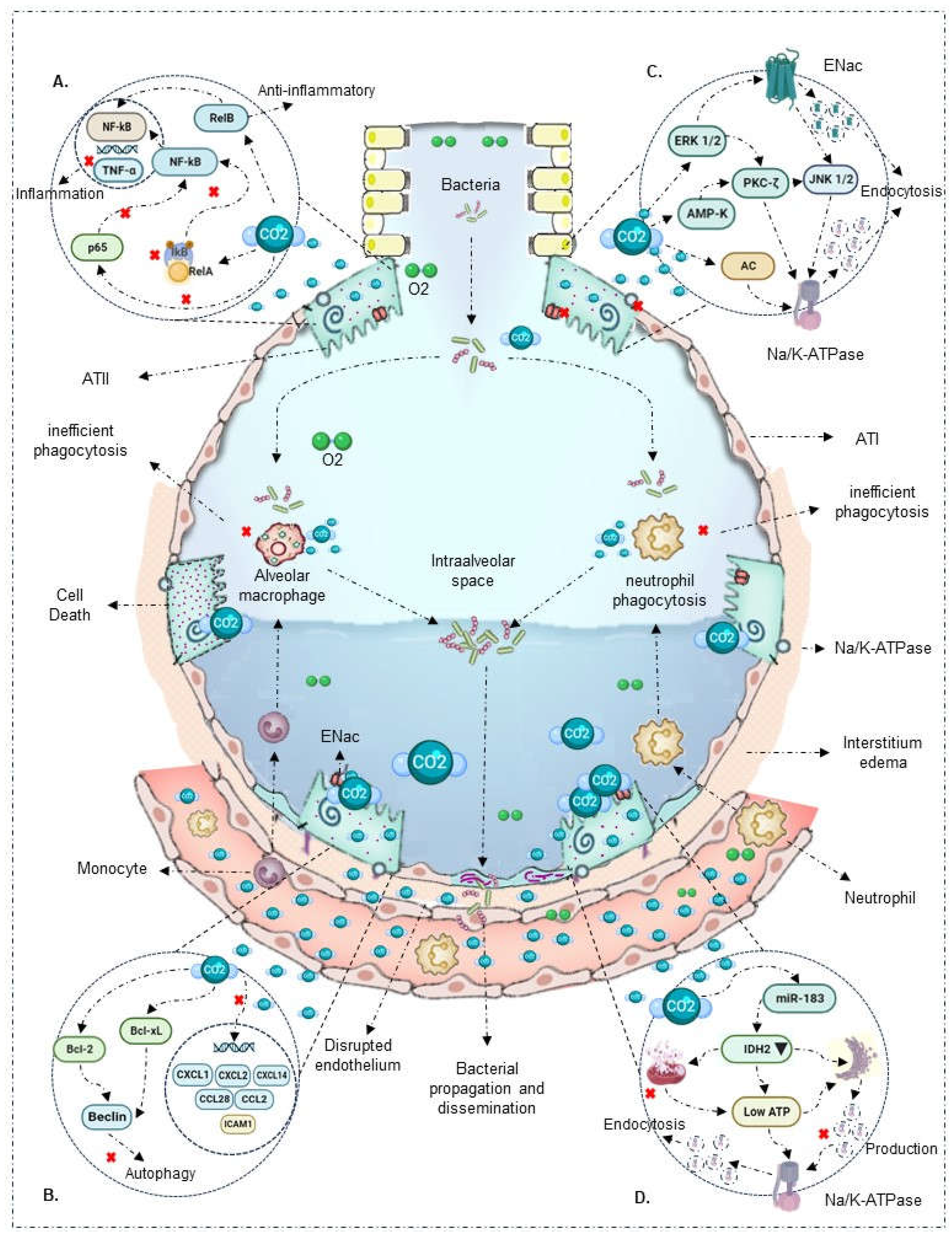
Table 1.
Study design and geographical location of the scoping review articles (in chronological order of publication by year).
Table 1.
Study design and geographical location of the scoping review articles (in chronological order of publication by year).
| Citacion | Year | Country | Type of study |
|---|---|---|---|
| Vadász I | 2008 Jan | USA | Experimental |
| O’Croinin DF | 2008 Jul | Ireland | Experimental |
| Liu Y | 2008 Aug | USA | Experimental |
| Chonghaile MN | 2008 Nov | Ireland | Experimental |
| Ni Chonghaile M | 2008 Dec | Ireland | Experimental |
| Nichol AD | 2009 Nov | Ireland | Experimental |
| O'Toole D | 2009 Nov | Ireland | Experimental |
| Wang N | 2010 Feb | USA | Experimental |
| Welch LC | 2010 Sep | USA | Experimental |
| Peltekova V | 2010 Oct | Canada | Experimental |
| Cummins EP | 2010 Oct | Ireland | Experimental |
| Vohwinkel CU | 2011 Oct | USA | Experimental |
| Oliver K | 2012 Apr | Ireland | Experimental |
| Contreras M | 2012 Sep | Ireland | Experimental |
| Vadász I | 2012 Oct | USA | Experimental |
| Lecuona E | 2013 May | USA | Experimental |
| Gates KL | 2013 Nov | USA | Experimental |
| Nardelli LM | 2015 Jan | Brazil | Experimental |
| Casalino-Matsuda SM | 2015 Apr | USA | Experimental |
| Yang W | 2015 Dec | China | Experimental |
| Masterson C | 2016 Apr | Ireland | Experimental |
| Horie S | 2016 Dec | Ireland | Experimental |
| Gwoździńska P | 2017 May | Germany | Experimental |
| Keogh C | 2017 Jul | Ireland | Experimental |
| Casalino-Matsuda SM | 2018 Sep | USA | Experimental |
| Cortes-Puentes GA | 2019 Jan | USA | Experimental |
| Kryvenko V | 2020 Feb | Germany | Experimental |
| Casalino-Matsuda SM | 2021 Apr | USA | Experimental |
| Gabrielli NM | 2021 Jul | Germany | Experimental |
| Kryvenko V | 2021 Dec | Germany | Experimental |
Table 2.
Summary of publications on the effects of hypercapnia on host defense and respiratory epithelium.
Table 2.
Summary of publications on the effects of hypercapnia on host defense and respiratory epithelium.
| Author | Experimental Model | Secondary Injury | CO2 Concentration | Immunomodulatory Effect |
|---|---|---|---|---|
| Alteration in transcription of innate response | ||||
| O'Toole et al., 2009 [22] |
In vitro: Confluent bronchial, respiratory, and alveolar A549 type II epithelial cells | No | 10%, 15% | Hypercapnia directly inhibits NF-κB activation |
| Liu et al., 2008 [30] |
In vivo (rats) and In vitro: Human pulmonary microvascular endothelial cells | LPS and bacterial TNF (24 hours) | 5%, 10% | In vitro model shows that 4 hours of hypercapnia and metabolic acidosis increase NF-κB expression |
| Wang N et al., 2010 [18] |
In vitro: THP-1 cells, human alveolar macrophages, RAW 264.7 mouse macrophages | Bacterial LPS and TLR | 5%, 9%, 12.5%, 20% | Hypercapnia attenuates TNF and IL-6 mRNA induction independently of extracellular metabolic acidosis. Also, it does not affect IkBα and RelA/p65 phosphorylation |
| Cummins et al., 2010 [23] |
In vitro: Respiratory epithelial cells | Endotoxin | 5%, 10% | Hypercapnia blocks IκBα phosphorylation, degradation, and p65 translocation, inactivating NF-κB |
| Oliver et al., 2012 [24] |
In vivo (rats) and In vitro: Alveolar epithelial A549 cells | No | 5%, 10% | Hypercapnia promotes RelB cleavage and localization during the non-canonical signaling pathway, exerting an anti-inflammatory and immunosuppressive effect |
| Contreras et al., 2012 [25] |
In vivo (rats) and In vitro: Alveolar epithelial A549 cells | No | 5% | Hypercapnia inactivates NF-κB in vivo and in vitro, maintaining cytoplasmic IκBα concentrations |
| Yang et al., 2015 [26] |
In vivo (rats) | None | CO2 ventilation: 35 - 150 mmHg | Hypercapnia reduced IkBα expression and NF-κB activity |
| Masterson et al., 2016 [27] |
In vivo (rats) and In vitro: Alveolar epithelial cells | Escherichia coli (4 hours) | Inspired CO2 ventilation: 5% | Hypercapnia inhibits p65 subunit translocation, reduces IκBβ intrinsic phosphorylation, IκBα concentrations, and maintains NF-κB inactivation |
| Horie et al., 2016 [28] |
In vitro: Bronchial and alveolar A549 cells | Lung stretch (24 - 120 hours) | 5%, 10% | Hypercapnia blocks IκBα phosphorylation, degrades proteins, inactivating NF-κB |
| Keogh C et al., 2017 [29] |
In vitro: Alveolar epithelial A549 cells | No | 5%, 10% | Hypercapnia promotes non-canonical NF-κB RelB/p100 activation, exerting an anti-inflammatory and immunosuppressive effect |
| Decease in innate immune response capacity | ||||
| O’Croinin et al., 2008 [17] |
In vivo (rats) | Escherichia coli (48 hours) | Inspired CO2 ventilation: 5% | Prolonged hypercapnia affects neutrophil phagocytic activity, worsening bacterial infection-induced lung injury |
| Liu et al., 2008 [30] |
In vivo (rats) and In vitro: Human pulmonary microvascular endothelial cells | LPS and bacterial TNF (24 hours) | 5%, 10% | 4 hours of hypercapnia increased neutrophil adhesion and expression of ICAM1, VCAM1, E-selectin, and IL-8, exhibiting a proinflammatory effect |
| Chonghaile et al., 2008 [12] |
In vivo (rats): Established pneumonia | Escherichia coli (6 hours) | Inspired CO2 ventilation: 5% | In a model of established pneumonia, hypercapnia increased TNF-α and IL-6 levels, improved airway pressures. In the presence of antibiotic therapy, it reduced bacterial count and pneumonia-induced histological injury |
| Ni Chonghaile et al., 2008 [31] |
In vivo (rats) | Escherichia coli (6 hours) | Inspired CO2 ventilation: 5% | During pulmonary sepsis, hypercapnia affects neutrophil phagocytic activity, reducing bacterial death and worsening lung injury |
| Nichol et al., 2009 [39] |
In vivo (rats) and In vitro: Bronchial epithelial cells | Endotoxin and Escherichia coli | Inspired CO2 ventilation: 5% | Buffered hypercapnia in the absence of metabolic acidosis does not alter phagocytic capacity and neutrophil concentration. However, it increases maximum airway pressure, exacerbating lung injury |
| Wang N et al., 2010 [18] |
In vitro: THP-1 cells, human alveolar macrophages, RAW 264.7 mouse macrophages | Lipopolysaccharides and bacterial TLR | 5%, 9%, 12.5%, 20% | Hypercapnia inhibits macrophage phagocytosis |
| Peltekova et al., 2010 [32] |
In vivo (rats) | Harmful ventilation | Inspired CO2 ventilation: 0%, 5%, 12%, 25% | Hypercapnia decreases TNFα levels and increases nitrotyrosine formation, enhancing lung injury |
| Cummins et al., 2010 [23] |
In vitro: Respiratory epithelial cells | Endotoxin | 5%, 10% | Hypercapnia reduces proinflammatory response gene expression (CCL2, ICAM1, and TNF-α) |
| Oliver et al., 2012 [24] |
In vivo (rats) and In vitro: Alveolar epithelial A549 cells | No | 5%, 10% | Hypercapnia suppresses TNF-α expression independent of pH |
| Gates et al., 2013 [33] |
In vivo (rats) | Pseudomonas aeruginosa (96 hours) | Inspired CO2 ventilation: 10% | In a model of established pneumonia, hypercapnia alters neutrophil phagocytic capacity, increases bacterial load and dissemination to other organs, and reduces early cytokine response (IL-6, TNF) |
| Nardelli et al., 2015 [34] |
In vivo (rats) | Paraquat | PaCO2 ventilation: 35 - 80 mmHg | Hypercapnia, independent of acidosis, reduces IL-6, IL-1β, and type III pro-collagen expression. It also decreases neutrophil count and apoptosis processes |
| Casalino-Matsuda et al., 2015 [35] |
In vitro: Human alveolar macrophages | No | 5%, 15% | Hypercapnia increases anti-apoptotic factors Bcl-2, Bcl-xL, inhibiting Beclin 1 and autophagy and bacterial death |
| Yang et al., 2015 [26] |
In vivo (rats) | None | CO2 ventilation: 35 - 150 mmHg | Hypercapnia attenuates TNF-α levels independent of pH |
| Casalino-Matsuda et al., 2018 [36] |
In vitro: Bronchial epithelial cells | Lung injury (24 hours) | 20% | Sustained hypercapnia for 24 hours alters the regulation of immunoregulatory genes such as CXCL1, CXCL2, CXCL14, CCL28, IL-6R, and TLR4 |
| Casalino-Matsuda et al., 2021 [37] |
In vitro: Human alveolar macrophages, RAW 264.7 mouse macrophages | No | 20% | Hypercapnia downregulates NF-κB pathway genes, type I interferon and antiviral signaling genes, cytokines, and other associated genes |
| Disruption and resealing of alveolar epithelial cells | ||||
| Vadász et al., 2008 [38] |
In vitro: Alveolar epithelial cells | No | PaCO2: 60 - 120 mmHg | Hypercapnia increases AMPK overexpression, inducing PKC-ζ activation, promoting Na/K-ATPase endocytosis, and inhibiting alveolar fluid reabsorption |
| Nichol et al., 2009 [39] |
In vivo (rats) and In vitro: Bronchial epithelial cells | Endotoxin and Escherichia coli | Inspired CO2 ventilation: 5% | Buffered hypercapnia, without metabolic acidosis, decreases lung cell wound repair rate |
| O'Toole et al., 2009 [22] |
In vitro: Confluent bronchial, respiratory, and alveolar A549 type II epithelial cells | No | 10%, 15% | Hypercapnia decreases lung cell wound healing through a mechanism associated with direct NF-Κb activation inhibition |
| Welchl et al., 2010 [40] |
In vitro: Alveolar epithelial cells | No | 5% | Hypercapnia activates ERK 1/2, promoting Na/K-ATPase endocytosis and inhibiting alveolar fluid reabsorption |
| Vohwinkel et al., 2011 [41] |
In vitro: Alveolar epithelial A549 cells and fibroblasts | No | 5% | Hypercapnia increases microRNA-183 expression, downregulating isocitrate dehydrogenase 2 expression, affecting mitochondrial function and cell proliferation |
| Vadász et al., 2012 [42] |
In vitro: Alveolar epithelial cells | No | PaCO2: 60 - 120 mmHg | Hypercapnia induces JNK activation, leading to Na/K-ATPase downregulation and alveolar epithelial dysfunction |
| Lecuona et al., 2013 [43] |
In vitro: Alveolar epithelial cells | No | PaCO2: 60 - 120 mmHg | Hypercapnia activates soluble adenylate cyclase CO2/HCO3-sensitive, stimulating cAMP production and PKA activity, favoring Na/K-ATPase endocytosis and alveolar epithelial dysfunction |
| Gwoździńska et al., 2017 [44] |
In vitro: Alveolar epithelial A549 cells | No | 5% | Hypercapnia promotes ERK/AMPK/JNK axis activation, affecting ENaC cellular activity via polyubiquitination mechanism |
| Cortes-Puentes et al., 2019 [45] |
In vitro: Alveolar epithelial cells | No | 80 Torr | Hypercapnia activates soluble adenylate cyclase, delaying lung membrane resealing and alveolar epithelial cell repair |
| Kryvenko et al., 2020 [46] |
In vitro: Alveolar epithelial A549 and rat type II cells | No | 5%, 15% | Hypercapnia causes Na/K-ATPase-β retention in the endoplasmic reticulum and significant reduction in the alveolar membrane |
| Gabrielli et al., 2021 [47] |
In vitro: Alveolar epithelial A549 cells | No | 5% | Hypercapnia promotes ubiquitination of E3 ligase, favoring Na/K-ATPase β subunit endocytosis and degradation mediated by PKC-ζ |
| Kryvenko et al., 2021 [48] |
In vitro: Alveolar epithelial A549 cells | No | 5% | Hypercapnia affects Na/K-ATPase β subunit in the endoplasmic reticulum and basal membrane |
Abbreviations: cAMP: Cyclic adenosine monophosphate; PKA: Protein kinase A; ERK: Extracellular signal-regulated kinase; AMPK: AMP-activated protein kinase; JNK: c-Jun N-terminal kinases; ENaC: Epithelial sodium channels; PKC: Protein kinase C; NF-κB: Nuclear Factor-kappa B; PKC: Protein kinase C; ERK: Extracellular signal-regulated kinase; JNK: c-Jun N-terminal kinases; CCL2: Chemokine Ligand 2; ICAM1: Intercellular Adhesion Molecule 1; VCAM1: molécula de citoadhesión vascular 1; TNF: Tumor Necrosis Factor; IL-1: Interleukin 1; IL-6: Interleukin 6; IL-8: Interleukin 8; Bcl-2: B-cell lymphoma 2; Bcl-xL: B-cell lymphoma-extra large protein; CXCL1: Chemokine Ligand 1; CXCL2: Chemokine Ligand 2; CXCL14: Chemokine Ligand 14; CCL28: Chemokine Ligand 28; TLR4: Toll-Like Receptor 4; IκB: Inhibitor of kappa B; LPS: Lipopolysaccharides; TLR: Toll-Like Receptor; mRNA: Messenger Ribonucleic Acid.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



