
Submitted:
28 August 2024
Posted:
28 August 2024
You are already at the latest version
Abstract
Background
The increasing number of elderly individuals in South Korea, now entering a super-aging era, underscores the growing importance of understanding their specific oral health needs. This study investigated changes in oral health conditions, salivary parameters, halitosis, systemic diseases, and medication usage with aging.
Methods
This study was retrospectively conducted using the medical records of patients who presented with complaints of xerostomia or halitosis between August 2020 and May 2023. A total of 274 patients (66 males, 208 females, mean age 59.39 ± 16.10 years) were included in this study.
Results
Aging was found to be significantly associated with the presence of sticky saliva, poor oral hygiene, tongue coating, and halitosis (all p < 0.05). Correlation analyses further revealed significant associations between aging and several conditions, including hypertension (r = 0.495, p < 0.001), diabetes mellitus (r = 0.255, p < 0.001), amlodipine usage (r = 0.249, p = 0.001), osteoporosis (r = 0.195, p = 0.001), cardiovascular disease (r = 0.150, p = 0.013), and the presence of tongue coating (r = 0.205, p = 0.001). Conversely, none of the salivary parameters demonstrated a significant relationship with aging. Furthermore, halitosis did not exhibit significant differences across age groups (all p > 0.05), with the exception of methyl mercaptan levels, which were notably higher among patients in their 20s (p = 0.049).
Conclusions
The findings of this study can help clinicians develop targeted strategies to address specific oral health challenges associated with aging in elderly patients.
Keywords:
aging
; oral health
; saliva
; halitosis
; systemic disease
; systemic medication
1. Introduction
South Korea is entering the age of super-aging society. The 2015 Census of Older People estimates that proportion of those who aged 65 and over in South Korea is 13.2%, and forecasts that the proportion will continue to rise and reach 20.0% in 2025, entering the super-aging society [1,2]. In the era of super-aging society, the importance of maintaining general health of elderly is steadily increasing, and one of the crucial factors in general healthcare of elderly is managing oral health [3]. Inadequate oral health management can result in various oral diseases, such as dental caries and periodontal disease, and elderly individuals with unmanaged oral conditions are at an elevated risk for systemic diseases, including diabetes mellitus, dementia, pulmonary infections, and cardiovascular disease [4,5,6]. Therefore, a thorough understanding of the oral health status and related factors in the elderly is essential for effective management.
Elderly individuals experience various changes in their oral health, which can complicate oral health management. Xerostomia is a common condition among the elderly, with previous studies indicating a significantly higher prevalence of subjective dry mouth sensations as age increases [7,8,9]. Aging is associated with a marked reduction in the function of the submandibular and sublingual glands, leading to a decreased salivary flow rate and changes in the composition of whole saliva, resulting in sticky saliva [10,11]. This reduced salivary flow and sticky saliva can impair the oral self-cleansing mechanism, increasing the risk of oral conditions related to poor oral hygiene, such as food impaction, tongue coating, and calculus deposition [12]. Poor oral hygiene can directly cause halitosis, as oral health problems are responsible for more than 90% of halitosis cases [13]. While the relationship between age and halitosis remains debated, several studies have reported a high prevalence of halitosis among the elderly due to an increase in oral health-related issues [14,15,16].
Furthermore, an important aspect of aging is the increased prevalence of systemic diseases and medication usage. In South Korea, the prevalence of systemic diseases is significantly higher among the elderly and has been steadily rising over time [17]. Correspondingly, the use of systemic medications is also increasing globally, with particularly high levels of medication usage observed in the elderly [18,19]. Previous studies have demonstrated that systemic diseases, systemic medication use, and oral health are interrelated and can exacerbate one another; for instance, diabetes mellitus can lead to xerostomia, and poor oral hygiene can worsen hypertension [3,20]. Therefore, the increased prevalence of systemic diseases and medication use among the elderly must be carefully considered to effectively maintain both oral and systemic health in this population.
Despite the growing need to understand the oral health conditions, systemic diseases, and medication usage among the elderly, there remains a lack of comprehensive studies investigating changes in oral health, salivary parameters, halitosis, and systemic medication use with aging, particularly those involving large patient cohorts. This study aims to examine the changes in oral health conditions, salivary parameters, halitosis, systemic diseases, and medication usage associated with aging. The primary hypothesis of this study is that aging is associated with a higher prevalence of poor oral health conditions, xerostomia, halitosis, systemic diseases, and increased medication usage, and that there may be complex interrelationships among these factors.
2. Materials and Methods
2.1. Research Subjects and Groups
This study targeted patients aged between teens to 80s who visited the Department of Orofacial Pain and Oral Medicine at Kyung Hee University Dental Hospital from August 2020 to May 2023, complaining xerostomia or halitosis. For sample size calculation, we used G*Power software (ver. 3.1.9.7; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany), found that 220 participants were suitable for statistical analysis (α level = 0.05, the power = 0.90, and the effect size = 0.5). After screening, 303 patients were selected, and 29 patients were excluded due to the insufficient medical records. A total 274 patients (66 males, 208 females, mean age 59.39 ± 16.10) were enrolled in this study. Patients were then divided into eight age groups according to 10-year increments: teens into age group 1, 20s into age group 2, and so on until age group 8.
2.2. Evaluation of Saliva
Evaluation of salivary parameters was performed at the patients’ initial visit, using GC Saliva Check Buffer kits (GC Company, Tokyo, Japan). Evaluated salivary parameters were salivary flow rate, salivary pH, and salivary buffer capacity, using the spitting method. First, patients were ordered to spit their saliva for 10 minutes in resting state. The amount of collected saliva was recorded as unstimulated flow rate (UFR). After measuring UFR, a salivary pH test strip was inserted into the unstimulated whole saliva, and salivary pH was recorded according to the color change of test strip (Figure 1). Next, patients were ordered to chew paraffin wax gum for 2 minutes, and spit their saliva for 5 minutes. This amount of collected saliva was recorded as stimulated flow rate (SFR). After measuring SFR, stimulated whole saliva was dropped onto the three areas of the buffer test strip using a pipette, and salivary buffer capacity was recorded according to the color change of buffer test strip with the salivary buffer indicator (Figure 2). In terms of diagnosis criteria, normal UFR is 0.3-0.4ml/min, and normal SFR is 1.5-2.0ml, while hyposalivation is diagnosed when UFR is under 0.1ml/min or SFR is under 0.7ml/min [21]. Normal salivary pH is between 6.7-7.3, and abnormal salivary pH is under 6.3 [22]. Additionally, since there are several measuring methods for salivary buffer capacity, this study followed the guideline of manufacturer of salivary test kit, GC company, where score between 10-12 is normal salivary buffer capacity, 6-9 is low, and 0-5 is very low. All of the salivary evaluation procedures were performed by skilled dentists and dental hygienists, trained in standardized examination protocol.
2.3. Evaluation of Halitosis
The level of halitosis was also evaluated at the patients’ initial visit. Halitosis examination was conducted using the TwinBreasor II (IsenLab, Gyeonggido, Korea), which separates and measures hydrogen sulfide (H2S) and methyl mercaptan (CH3SH) in parts per billion (ppb). Prior to the halitosis measurement, patients were instructed to refrain from smoking and eating food for 30 minutes. With the mouth closed, a syringe for gas collection was placed deeply into the patients’ oral cavity without touching the tongue or saliva, and gas was collected. Collected gas was inserted to the device and analyzed, and the results were derived and recorded (Figure 3). VSC was calculated with sum of H2S and CH3SH. Halitosis was diagnosed when H2S is over 112ppb or CH3SH is over 26ppb [23].
2.4. Evaluation of Oral Health Condition
The oral health condition of each patient was evaluated and recorded during their first visit by skilled dentists. Sticky saliva was identified when frothy or viscous saliva was observed with the naked eye. Oral hygiene was categorized into three grades—good, moderate, and poor—based on the clinician's subjective assessment. Calculus deposition was recorded when visible calculus was detected. Tongue coating was noted if the patient exhibited a white or yellowish coating on the posterior two-thirds of the tongue. Oral ulcers were documented if any visible ulcers were present on the oral mucosa. Oral candidiasis was confirmed through a swab culture, which involved collecting an oral specimen with a sterile transport swab (Transystem, COPAN, Italy), culturing it in the appropriate medium, and evaluating the resulting specimen. All culture procedures followed the criteria established by the Department of Laboratory Medicine at Kyung Hee University Medical Center.
2.5. Evaluation of Systemic Disease and Medication
Systemic diseases and medication of patients were collected from the questionnaire at the patients’ initial visit. Systemic diseases were divided into hypertension, diabetes mellitus, osteoporosis, and cardiovascular disease, which are the four most prevalent systemic disease. Patients with overlapping diseases among hypertension, diabetes mellitus, osteoporosis, and cardiovascular disease were classified repeatedly to each group. Medications of patients were also recorded by classifying the medications into four categories: Amlodipine tab (amlodipine), Metformin tab (metformin), Alend tab (alendronate), and Lasix tab (furosemide).
2.6. Statistical Analysis
Data were analyzed using IBM SPSS for Windows (version 26.0; IBM Corp., Armonk, NY, USA). Descriptive statistics, including means and standard deviations, were calculated to summarize the data. The distribution of categorical data was analyzed using the χ² test and Bonferroni tests for the equality of proportions. Analysis of variance (ANOVA) followed by Tukey’s post-hoc test was employed to compare parameter values among different age groups. Cramer’s V analysis was conducted to identify associations between aging and other oral and systemic parameters. The correlation coefficients (r) were calculated to assess the strength of the correlations, ranging from -1 to 1, with values closer to ±1 indicating stronger relationships. Linear regression analysis and generalized linear models were used to explore the relationship between aging and oral health. Given that systemic diseases and medication use were strong contributors to aging, an adjusted model accounting for these factors was employed to isolate the relationship between aging and oral health. The adjusted generalized linear model was constructed with age as the dependent variable and oral health conditions and salivary parameters as independent variables. The correlation coefficients (B), standard errors, p-values, and 95% confidence intervals (95% CIs) were calculated. For all analyses, statistical significance was set at a two-tailed p-value of < 0.05.
2.7. Ethics Approval and Consent to Participate
The procedures for human subjects in this study were conducted according to the ethical standards of the Committee on Human Experimentation of our institution and the 1975 Declaration of Helsinki. This study was approved by the appropriate ethics review board of the Kyung Hee University Dental Hospital (IRB No. KH-DT23022). Informed consent was obtained from all participants in this study.
3. Results
3.1. Gender and Age Distribution of Patients
Age and gender distribution of patients are presented in Table 1. Of the 274 participants of the study, 66 (22.8%) were male and 208 (71.7%) were female, for about 1:3 ratio of females to males. The number of patients for each age group is as follows: 9 individuals (3.3%) in their teens (age group 1), 10 (3.6%) in their 20s (age group 2), 11 (4.0%) in their 30s (age group 3), 30 (10.9%) in their 40s (age group 4), 63 (23.0%) in their 50s (age group 5), 66 (24.1%) in their 60s (age group 6), 67 (24.5%) in their 70s (age group 7), and 18 (6.6%) in their 80s (age group 8). Mean age of total patients was 59.39 ± 16.10.
3.2. Salivary Parameters by Age Group
Salivary parameters for age groups are displayed in Figure 4 and Figure 5. Across the age groups, there was no significant difference in the UFR (p = 0.229), SFR (p = 0.971), salivary pH (p = 0.606), and salivary buffer capacity (p = 0.344). For UFR, age group 2 had the lowest mean value (0.28±0.18 ml/min) and age group 8 had the highest mean value (0.60±0.36 ml/min). For SFR, age group 1 had the lowest mean value (1.27±0.39 ml/min) and age group 8 had the highest mean value (1.51±0.64 ml/min). All of the age groups were in the normal range of salivary flow rate. For salivary pH, age group 2 had abnormal salivary pH (6.18±0.62), which was the lowest mean value among the age groups. Also, all of the age groups showed slightly lower salivary pH than normal range except for age group 8 (6.77±0.63), which was the highest mean value among the age groups. For salivary buffer capacity, only age group 1 (10.67±1.22) and age group 3 (10.82±1.25) had normal salivary buffer capacity, and age group 3 had the highest mean value. Other age groups had lower salivary buffer capacity than normal range, and age group 2 had the lowest mean value (9.00±2.67).
3.3. VSC Levels by Age Group
VSC levels for different age groups are presented in Table 2 and Figure 5C. Age group 2 showed significantly higher mean level of CH3SH (152.00±214.96 ppb) than the other age groups (p = 0.049), and it was the only age group with higher level of CH3SH than normal range. For H2S, age group 2 had the highest mean value (410.00±579.82 ppb) followed by age group 3 (318.50±635.00 ppb), and both groups had the higher level of H2S than normal range. However, relationship between H2S and age groups was not statistically significant (p = 0.393). For VSC, age group 2 had the highest mean value (112.40±355.44 ppb), but it was not statistically significant difference with the other age groups (p = 0.051). The percentage of patients diagnosed with halitosis was highest in age group 2 (10.0%), followed by age group 4 (3.3%), age group 5 (3.2%), age group 6 (3.0%), age group 7 (1.5%), and age groups 1, 3, and 8 (0.0%). However, the prevalence of halitosis did not show a significant association with age group (p = 0.807).
3.4. Distribution of Representative Systemic Diseases by Age Group
Distribution of the four representative systemic diseases is displayed in Figure 6. There was a significant difference in the prevalence of hypertension across the age groups (p = 0.001), with significantly higher incidence in older age groups (age group 7 and 8) than other age groups. The prevalence of hypertension was highest in age group 8 (77.8%), and was in the decreasing order of age group 7 (64.2%), age group 6 (42.4%), age group 5 (19.0%), age group 4 (10.0%), age group 3 (9.1%), age group 1 (0.0%), and age group 2 (0.0%). Regarding to diabetes mellitus, prevalence of diabetes mellitus was also significantly different across the age groups (p = 0.010) with significantly higher incidence in older age groups (age group 7 and 8) than other age groups. It was highest in age group 7 (22.4%), and in the decreasing order of age group 8 (22.2%), age group 6 (13.6%), age group 5 (4.8%), age group 4 (3.3%), and age group 1,2, and 3 (0.0%).
In contrast, there was not statistically significant difference in prevalence of osteoporosis (p = 0.099) and cardiovascular disease (p = 0.235) across the age groups. Prevalence of osteoporosis was highest in age group 8 (11.1%), followed in decreasing order of age group 7 (10.4%), age group 6 (3.0%), age group 5 (1.6%), and age groups 1, 2, 3, and 4 (0.0%). Prevalence of cardiovascular disease was highest in age group 6 (22.4%), followed by in decreasing order of age group 7 (22.2%), age group 8 (13.6%), age group 5 (4.8%), and age groups 1, 2, 3, and 4 (0.0%).
3.5. Correlation between Age, Halitosis, and Salivary Flow Rate
Table 3 presents the result of correlation analysis between age, halitosis, and salivary flow rate. VSC and complaint of halitosis were strongly correlated (r = 0.621, p < 0.001). UFR and SFR also showed a statistically strong correlation (r = 0.513, p < 0.001).
3.6. Correlations between oral health, systemic disease, and medication with aging
The associations between oral health, systemic medication, systemic disease, and aging are summarized in Table 4. Among the oral health conditions, tongue coating showed a significant association with aging (r = 0.205, p = 0.001). In terms of systemic medications, amlodipine was the only medication significantly associated with aging (r = 0.249, p = 0.001). Furthermore, all four systemic diseases were strongly correlated with aging, with hypertension showing the strongest correlation (r = 0.495, p < 0.001), followed by diabetes mellitus (r = 0.255, p < 0.001), osteoporosis (r = 0.195, p = 0.001), and cardiovascular disease (r = 0.150, p = 0.001).
3.7. Generalized Linear Model of Oral Health, Salivary Parameters and Aging
A generalized linear model was employed to predict aging using oral health conditions and salivary parameters. In this model, aging was selected as the independent variable, while oral health conditions and salivary parameters were treated as dependent variables. The results of the generalized linear model are presented in Table 5. Among the oral health conditions, oral hygiene was found to be strongly associated with aging, with both poor oral hygiene (B = 11.752, 95% CI = 2.219–21.286, p = 0.016) and moderate oral hygiene (B = 6.903, 95% CI = 1.880–11.926, p = 0.007) showing significant relationships. Notably, poor oral hygiene exhibited the largest coefficient value among the factors analyzed. Other oral health conditions that were significantly associated with aging included the presence of sticky saliva (B = 6.039, 95% CI = 1.368–10.709, p = 0.011), the presence of tongue coating (B = 4.615, 95% CI = 0.681–8.549, p = 0.021), and the presence of halitosis (B = 0.774, 95% CI = 0.216–1.332, p = 0.043). In contrast, none of the salivary parameters showed a significant relationship with aging (all p > 0.05).
4. Discussion
In this study, we aimed to investigate the changes in salivary parameters, halitosis, systemic diseases, systemic medication usage, and oral health conditions with increasing age. The findings indicated that increasing age was significantly associated with the presence of sticky saliva, poor oral hygiene, tongue coating, and halitosis, as demonstrated by the generalized linear model. Additionally, there was a correlation between increasing age and both amlodipine usage and four systemic diseases. In contrast, no significant relationship was found between salivary parameters and increasing age. When analyzing age groups, CH3SH levels were significantly higher in age group 2, whereas VSC, H2S, and salivary parameters did not differ significantly across age groups. Moreover, the prevalence of hypertension and diabetes mellitus was significantly higher in age groups 7 and 8, while the prevalence of osteoporosis and cardiovascular disease did not vary across age groups.
In this study, sticky saliva was significantly more likely to be observed in older adults. Sticky saliva, characterized by dehydrated saliva with high viscosity, is commonly associated with factors such as xerostomia, diabetes mellitus, oral infections, and the use of systemic medications, all of which are more prevalent among the elderly [24,25,26]. Additionally, sticky saliva is closely linked to decreased function of the submandibular gland [27]. With advancing age, there is a reduction in the number of acinar cells and an increase in fatty and fibrous tissue within the salivary glands [28]. These morphological changes are more likely to impair the function of the submandibular and sublingual glands than the parotid gland in the elderly [29]. This partial reduction in salivary gland function can lead to saliva with high viscosity, even when the salivary flow rate remains normal, which may be overlooked by clinicians who focus solely on xerostomia. Given that sticky saliva has a similar impact as xerostomia on oral conditions, such as reducing self-cleansing activity and lubrication [30], clinicians should also consider saliva viscosity in their assessments.
This study demonstrated that tongue coating becomes more prevalent with increasing age. Tongue coating is a significant contributing factor to various oral diseases, such as halitosis and taste disorders, and can also impact systemic health by spreading to the respiratory or digestive systems and affecting several metabolic pathways [31,32]. Tongue coating primarily consists of residual food, bacterial by-products, leukocytes, and keratinized debris, and its presence often indicates poor oral health and inadequate oral hygiene management [33]. Effective oral health management includes mechanical cleaning methods, such as tooth brushing and scaling, as well as oral self-cleansing. Reduced oral self-cleansing ability is closely associated with impaired salivary secretion and diminished motor function, particularly lingual motor function, in the elderly [34]. Moreover, the high prevalence of certain systemic diseases, such as diabetes mellitus and stroke, in older adults can affect oral hygiene and tongue function, contributing to tongue coating formation [35,36]. However, the precise etiology of tongue coating formation remains controversial and requires further investigation. Despite this, the finding that elderly patients exhibited more tongue coating in this study underscores the importance of managing tongue coating in this population.
In this study, overall oral hygiene significantly deteriorated with increasing age. Oral hygiene is indicative of general oral health conditions, and poor oral hygiene is frequently assessed based on the presence of specific oral symptoms, including xerostomia, sticky saliva, swollen tissues, ill-fitting dentures, dental caries, plaque or calculus deposition, and oral ulcers [37]. In the elderly, poor oral hygiene results from a higher occurrence of oral symptoms related to inadequate hygiene and a reduced ability to perform dental health-related behaviors, such as toothbrushing, swallowing, tongue movement, and visiting dental clinics [38]. These behaviors are closely linked to the patient's physical and cognitive abilities, and the decline in neuromuscular function and the high prevalence of systemic diseases in the elderly increase their risk of failing to maintain proper oral hygiene [38,39,40]. To effectively address poor oral hygiene in the elderly, dentists should consider not only the patient's oral health condition but also their need for nursing care and functional rehabilitation.
Regarding halitosis, this study presented mixed results. While the presence of halitosis was closely associated with aging in the generalized linear model, CH3SH levels were significantly higher in the group in their 20s, and there were no significant differences in H2S levels, VSC levels, or the prevalence of halitosis across the age groups. These findings align with previous studies suggesting that halitosis is not clearly associated with age, or that it is more prevalent among the elderly [15,16]. VSC, the primary cause of halitosis, are predominantly produced from poor oral health conditions, particularly periodontal disease and tongue coating. However, VSCs are directly produced by the oral microbiome through the breakdown of sulfur-containing amino acids from food debris, serum, and other substrates like tongue coating [41]. Poor oral hygiene, which provides a source for VSC production, is common in the elderly, making the high prevalence of halitosis in this population understandable. Nonetheless, the total amount of specific oral microbiomes, such as Firmicutes and Bacteroidetes, which are known to be associated with VSC production, does not change significantly with age. The proportion of these oral microbiomes may increase in younger individuals with systemic disease or poor oral hygiene, leading to halitosis in younger populations [42,43]. Therefore, the correlation between aging and halitosis remains controversial, and further studies with larger sample sizes and more variables are needed to accurately clarify these conflicting findings.
Contrary to the main hypothesis, salivary flow rate and salivary buffer capacity were not significantly related with aging. This is the controversial result with the previous studies that whole salivary flow rate tends to decrease in elderly [10,11]. In fact, several studies commonly reported that UFR is significantly lower in elderly, but it is controversial whether SFR is decreased in elderly [28,29]. SFR is mainly composed of saliva from parotid gland, whose function is not significantly decreased with increasing age, and thus it is possible that SFR is not significantly different with increasing age [29,44]. Also, regarding to UFR, a study reported that UFR is closely related with oral condition while SFR is not [44]. Since this study included only patients with oral discomfort, UFR of younger participants might be influenced to decrease by their poor oral condition, leading to the insignificant difference with elderly. Further studies would be needed to re-evaluate this result, with design of case-control study including healthy participants.
In this study, all analyzed systemic diseases were found to be associated with aging, with hypertension and diabetes mellitus demonstrating particularly strong correlations with both aging and specific age groups, which aligns with the findings of previous research [45,46]. Additionally, amlodipine, an antihypertensive medication, demonstrated a significant relationship with aging. These results underscore the importance of assessing systemic diseases and medication use in the management of oral health in the elderly. It is well-established that systemic diseases, related medications, and oral health conditions are closely interconnected [3,20]. Hypertension can lead to oral conditions such as angioedema, xerostomia, or lichenoid reactions in the oral mucosa, and patients with periodontal disease have an increased risk of developing hypertension. Additionally, patients using antihypertensive medications are at a higher risk of experiencing xerostomia, a condition that is typically more severe in the elderly [25]. Furthermore, diabetes mellitus can lead to xerostomia and an imbalance of oral microorganisms, resulting in taste disorders, an increased risk of oral candidiasis, and periodontal disease. Given that the prevalence of hypertension and diabetes mellitus is steadily increasing in South Korea [47,48], clinicians should place even greater emphasis on considering systemic diseases during oral healthcare, particularly for the elderly.
Despite the findings of this study, several limitations should be acknowledged. First, the evaluation of oral health relied on the subjective judgment of the examiners, which may have introduced inconsistencies. Additionally, the sample was retrospectively derived solely from patients who visited a single dental hospital, raising concerns about potential selection bias. Furthermore, the study did not include a control group, which necessitates caution in interpreting the results. Nevertheless, this study highlights several correlations between aging, oral health, salivary parameters, halitosis, systemic diseases, and systemic medication.
5. Conclusion
This study has comprehensively elucidated the changes and correlations among oral health conditions, salivary parameters, halitosis, systemic diseases, and systemic medication associated with aging. The findings highlight the higher prevalence of poor oral hygiene and systemic diseases among the elderly, underscoring the critical need for integrated management of oral health and related systemic conditions in this population, particularly in light of the growing elderly demographic in an aging society. By raising local awareness and incorporating these findings into healthcare planning for the elderly, this study has the potential to enhance the effectiveness of management strategies, ultimately contributing to improved quality of life and greater stability for elderly individuals.
Author Contributions
Writing and original draft preparation, Y-HL, SS and T-SK; conceptualization, Y-HL; methodology, Y-HL, SS and T-SK; software, Y-HL, SS and T-SK; validation and formal analysis, Y-HL; investigation, Y-HL, SS and T-SK; resources, Y-HL, SS and T-SK; data curation, Y-HL, SS and T-SK; writing, review, and editing, Y-HL, SS and T-SK; visualization, Y-HL, SS and T-SK; supervision, Y-HL; project administration, Y-HL. All authors contributed to and approved the submitted manuscript.
Funding
None.
Institutional Review Board Statement
The research protocol for this study was reviewed in compliance with the Declaration of Helsinki and approved by the Institutional Review Board of Kyung Hee University Dental Hospital in Seoul, South Korea (KHD IRB, IRB No-KH-DT23022). Informed consent was obtained from all the participants.
Informed consent statement
Informed consent was obtained from all the subjects involved in the study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflict of interests.
Consent for Publication
All authors consented to the publication of this manuscript.
References
- Jang, J.Y.; Lee, D.H. Effects of Oral Health Promotion Program on Oral Function in the Elderly. Korean J Health Serv Manag 2016, 10, 141–151. [Google Scholar] [CrossRef]
- Meng, K.H. Population aging and health promotion activities in Korea. J Korea Assoc Health Promot 2004, 2, 187–197. [Google Scholar]
- Gil-Montoya, J.A.; de Mello, A.L.; Barrios, R.; Gonzalez-Moles, M.A.; Bravo, M. Oral health in the elderly patient and its impact on general well-being: A nonsystematic review. Clin Interv Aging 2015, 10, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Richmond, S.; Chestnutt, I.; Shennan, J.; Brown, R. The relationship of medical and dental factors to perceived general and dental health. Community Dent Oral Epidemiol 2007, 35, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Kolltveit, K.M.; Tronstad, L.; Olsen, I. Systemic diseases caused by oral infection. Clin Microbiol Rev 2000, 13, 547–558. [Google Scholar] [CrossRef]
- Muller, F. Oral hygiene reduces the mortality from aspiration pneumonia in frail elders. J Dent Res 2015, 94, 14S–16S. [Google Scholar] [CrossRef]
- Lee, Y.H.; Won, J.H.; Auh, Q.S.; Noh, Y.K.; Lee, S.W. Prediction of xerostomia in elderly based on clinical characteristics and salivary flow rate with machine learning. Sci Rep 2024, 14, 3423. [Google Scholar] [CrossRef]
- Fornari, C.B.; Bergonci, D.; Stein, C.B.; Agostini, B.A.; Rigo, L. Prevalence of xerostomia and its association with systemic diseases and medications in the elderly: A cross-sectional study. Sao Paulo Med J 2021, 139, 380–387. [Google Scholar] [CrossRef]
- Jamieson, L.M.; Thomson, W.M. Xerostomia: Its prevalence and associations in the adult Australian population. Aust Dent J 2020, 65 (Suppl. S1), S67–S70. [Google Scholar] [CrossRef]
- Liu, B.; Dion, M.R.; Jurasic, M.M.; Gibson, G.; Jones, J.A. Xerostomia and salivary hypofunction in vulnerable elders: Prevalence and etiology. Oral Surg Oral Med Oral Pathol Oral Radiol 2012, 114, 52–60. [Google Scholar] [CrossRef]
- Yeh, C.K.; Johnson, D.A.; Dodds, M.W. Impact of aging on human salivary gland function: A community-based study. Aging (Milano) 1998, 10, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Dodds, M.W.J.; Haddou, M.B.; Day, J.E.L. The effect of gum chewing on xerostomia and salivary flow rate in elderly and medically compromised subjects: A systematic review and meta-analysis. BMC Oral Health 2023, 23, 406. [Google Scholar] [CrossRef]
- Lee, Y.H.; Hong, J.Y. Oral microbiome as a co-mediator of halitosis and periodontitis: A narrative review. Front Oral Health 2023, 4, 1229145. [Google Scholar] [CrossRef]
- Moreno, L.B.; Colussi, P.R.G.; Marostega, M.G.; Rosalen, N.P.; Rösing, C.K.; Muniz, F.W.M.G. Self-reported halitosis and associated factors among older adults: A cross-sectional study. J Oral Biol Craniofac Res 2022, 12, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, T.; Suzuki, N.; Nakano, Y.; Yasui, M.; Yoneda, M.; Shimazaki, Y.; Hirofuji, T.; Yamashita, Y. Discrimination of the oral microbiota associated with high hydrogen sulfide and methyl mercaptan production. Sci Rep 2012, 2, 215. [Google Scholar] [CrossRef]
- Yaegaki, K.; Sanada, K. Biochemical and clinical factors influencing oral malodor in periodontal patients. J Periodontol 1992, 63, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Agency, K.D.C.a.P. Korea Health Statistics 2022: Korea National Health and nutrition Examination Survey. Available online: https://knhanes.kdca.go.kr/ (accessed on 23 August 2024).
- Cho, H.J.; Chae, J.; Yoon, S.H.; Kim, D.S. Aging and the Prevalence of Polypharmacy and Hyper-Polypharmacy Among Older Adults in South Korea: A National Retrospective Study During 2010-2019. Front Pharmacol. 2022, 13, 866318. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Liu, K.; Shirai, K.; Tang, C.; Hu, Y.; Wang, Y.; Hao, Y.; Dong, J.Y. Prevalence and trends of polypharmacy in U.S. adults, 1999-2018. Glob Health Res Policy 2023, 8, 25. [Google Scholar] [CrossRef]
- Bozdemir, E.; Yilmaz, H.H.; Orhan, H. Oral mucosal lesions and risk factors in elderly dental patients. J Dent Res Dent Clin Dent Prospects 2019, 13, 24–30. [Google Scholar] [CrossRef]
- Villa, A.; Connell, C.L.; Abati, S. Diagnosis and management of xerostomia and hyposalivation. Ther Clin Risk Manag 2015, 11, 45–51. [Google Scholar] [CrossRef]
- Baliga, S.; Muglikar, S.; Kale, R. Salivary pH: A diagnostic biomarker. J Indian Soc Periodontol 2013, 17, 461–465. [Google Scholar] [CrossRef]
- Tonzetich, J.; Ng, S.K. Reduction of malodor by oral cleansing procedures. Oral Surg Oral Med Oral Pathol 1976, 42, 172–181. [Google Scholar] [CrossRef]
- Mata, A.D.; Marques, D.; Rocha, S.; Francisco, H.; Santos, C.; Mesquita, M.F.; Singh, J. Effects of diabetes mellitus on salivary secretion and its composition in the human. Mol Cell Biochem 2004, 261, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Elmi Rankohi, Z.; Shabanian, M.; Maleki, D. Oral Manifestations of Patients Taking Anti-Hypertensive Medications. Journal of Islamic Dental Association of IRAN 2020, 32, 83–88. [Google Scholar] [CrossRef]
- Ok, S.M.; Ho, D.; Lynd, T.; Ahn, Y.W.; Ju, H.M.; Jeong, S.H.; Cheon, K. Candida Infection Associated with Salivary Gland-A Narrative Review. J Clin Med 2020, 10, 97. [Google Scholar] [CrossRef] [PubMed]
- Beetz, I.; Schilstra, C.; Visink, A.; van der Schaaf, A.; Bijl, H.P.; van der Laan, B.F.; Steenbakkers, R.J.; Langendijk, J.A. Role of minor salivary glands in developing patient-rated xerostomia and sticky saliva during day and night. Radiother Oncol 2013, 109, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Vissink, A.; Spijkervet, F.K.; Van Nieuw Amerongen, A. Aging and saliva: A review of the literature. Spec Care Dent 1996, 16, 95–103. [Google Scholar] [CrossRef]
- Affoo, R.H.; Foley, N.; Garrick, R.; Siqueira, W.L.; Martin, R.E. Meta-Analysis of Salivary Flow Rates in Young and Older Adults. J Am Geriatr Soc 2015, 63, 2142–2151. [Google Scholar] [CrossRef]
- Beetz, I.; Schilstra, C.; van der Schaaf, A.; van den Heuvel, E.R.; Doornaert, P.; van Luijk, P.; Vissink, A.; van der Laan, B.F.; Leemans, C.R.; Bijl, H.P.; et al. NTCP models for patient-rated xerostomia and sticky saliva after treatment with intensity modulated radiotherapy for head and neck cancer: The role of dosimetric and clinical factors. Radiother Oncol 2012, 105, 101–106. [Google Scholar] [CrossRef]
- Seerangaiyan, K.; Juch, F.; Winkel, E.G. Tongue coating: Its characteristics and role in intra-oral halitosis and general health-a review. J Breath Res 2018, 12, 034001. [Google Scholar] [CrossRef]
- Li, Y.; Cui, J.; Liu, Y.; Chen, K.; Huang, L.; Liu, Y. Oral, Tongue-Coating Microbiota, and Metabolic Disorders: A Novel Area of Interactive Research. Front Cardiovasc Med 2021, 8, 730203. [Google Scholar] [CrossRef] [PubMed]
- Ogami, K.; Ueda, T.; Ryu, M.; Tajima, S.; Sakurai, K. Evaluation of Factors Associated with Tongue Coating Status in Elderly with Care Needs. Bull Tokyo Dent Coll 2018, 59, 163–169. [Google Scholar] [CrossRef]
- Kikutani, T.; Tamura, F.; Nishiwaki, K.; Suda, M.; Kayanaka, H.; Machida, R.; Yoshida, M.; Akagawa, Y. The degree of tongue-coating reflects lingual motor function in the elderly. Gerodontology 2009, 26, 291–296. [Google Scholar] [CrossRef]
- Tomooka, K.; Saito, I.; Furukawa, S.; Maruyama, K.; Eguchi, E.; Iso, H.; Tanigawa, T. Yellow Tongue Coating is Associated With Diabetes Mellitus Among Japanese Non-smoking Men and Women: The Toon Health. J Epidemiol 2018, 28, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Furuya, J.; Beniya, A.; Suzuki, H.; Hidaka, R.; Matsubara, C.; Obana, M.; Yoshimi, K.; Yamaguchi, K.; Hara, K.; Nakagawa, K.; et al. Factors associated with the number of microorganisms on the tongue surface in patients following acute stroke. J Oral Rehabil 2020, 47, 1403–1410. [Google Scholar] [CrossRef]
- Chalmers, J.M.; King, P.L.; Spencer, A.J.; Wright, F.A.; Carter, K.D. The oral health assessment tool--validity and reliability. Aust Dent J 2005, 50, 191–199. [Google Scholar] [CrossRef]
- Arai, K.; Sumi, Y.; Uematsu, H.; Miura, H. Association between dental health behaviours, mental/physical function and self-feeding ability among the elderly: A cross-sectional survey. Gerodontology 2003, 20, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Girestam Croonquist, C.; Dalum, J.; Skott, P.; Sjögren, P.; Wårdh, I.; Morén, E. Effects of Domiciliary Professional Oral Care for Care-Dependent Elderly in Nursing Homes - Oral Hygiene, Gingival Bleeding, Root Caries and Nursing Staff's Oral Health Knowledge and Attitudes. Clin Interv Aging 2020, 15, 1305–1315. [Google Scholar] [CrossRef] [PubMed]
- Patterson Norrie, T.; Villarosa, A.R.; Kong, A.C.; Clark, S.; Macdonald, S.; Srinivas, R.; Anlezark, J.; George, A. Oral health in residential aged care: Perceptions of nurses and management staff. Nurs Open 2019, 7, 536–546. [Google Scholar] [CrossRef]
- Sterer, N.; Rosenberg, M. Streptococcus salivarius promotes mucin putrefaction and malodor production by Porphyromonas gingivalis. J Dent Res 2006, 85, 910–914. [Google Scholar] [CrossRef]
- Sarafidou, K.; Alexakou, E.; Talioti, E.; Bakopoulou, A.; Anastassiadou, V. The oral microbiome in older adults –a state-of-the-art review. Archives of Gerontology and Geriatrics Plus 2024, 1. [Google Scholar] [CrossRef]
- Rizzardi, K.F.; Indiani, C.; Mattos-Graner, R.O.; de Sousa, E.T.; Nobre-Dos-Santos, M.; Parisotto, T.M. Firmicutes Levels in the Mouth Reflect the Gut Condition With Respect to Obesity and Early Childhood Caries. Front Cell Infect Microbiol 2021, 11, 593734. [Google Scholar] [CrossRef] [PubMed]
- Percival, R.S.; Challacombe, S.J.; Marsh, P.D. Flow rates of resting whole and stimulated parotid saliva in relation to age and gender. J Dent Res 1994, 73, 1416–1420. [Google Scholar] [CrossRef] [PubMed]
- Al Kibria, G.M.; Nemirovsky, A.; Sharmeen, A.; Day, B. Age-stratified prevalence, treatment status, and associated factors of hypertension among US adults following application of the 2017 ACC/AHA guideline. Hypertens Res 2019, 42, 1631–1643. [Google Scholar] [CrossRef]
- Sinclair, A.; Saeedi, P.; Kaundal, A.; Karuranga, S.; Malanda, B.; Williams, R. Diabetes and global ageing among 65-99-year-old adults: Findings from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res Clin Pract 2020, 162, 108078. [Google Scholar] [CrossRef]
- Kim, H.C.; Lee, H.; Lee, H.H.; Son, D.; Cho, M.; Shin, S.; Seo, Y.; Kim, E.J.; Korean Society of Hypertension -Hypertension Epidemiology Research Working Group. Korea Hypertension Fact Sheet 2023: Analysis of nationwide population-based data with a particular focus on hypertension in special populations. Clin Hypertens 2024, 30, 7. [Google Scholar] [CrossRef] [PubMed]
- Won, K.C.; Kwon, H.S.; Ko, S.H.; Bae, J.H.; Yang, Y.S.; Choi, J.H.; K., H. Diabetes fact sheet in Korea 2022. 2023.05.02 ed.; Won, K.C.: Korean Diabetes Association, 2022.
Figure 1.
Test strip for salivary pH and dental saliva pH indicator. After applying the test strip to collected saliva, color of the test strip was compared to a standard color chart to determine the closest match. In the presented figure, salivary pH was interpreted as 7.4.
Figure 1.
Test strip for salivary pH and dental saliva pH indicator. After applying the test strip to collected saliva, color of the test strip was compared to a standard color chart to determine the closest match. In the presented figure, salivary pH was interpreted as 7.4.
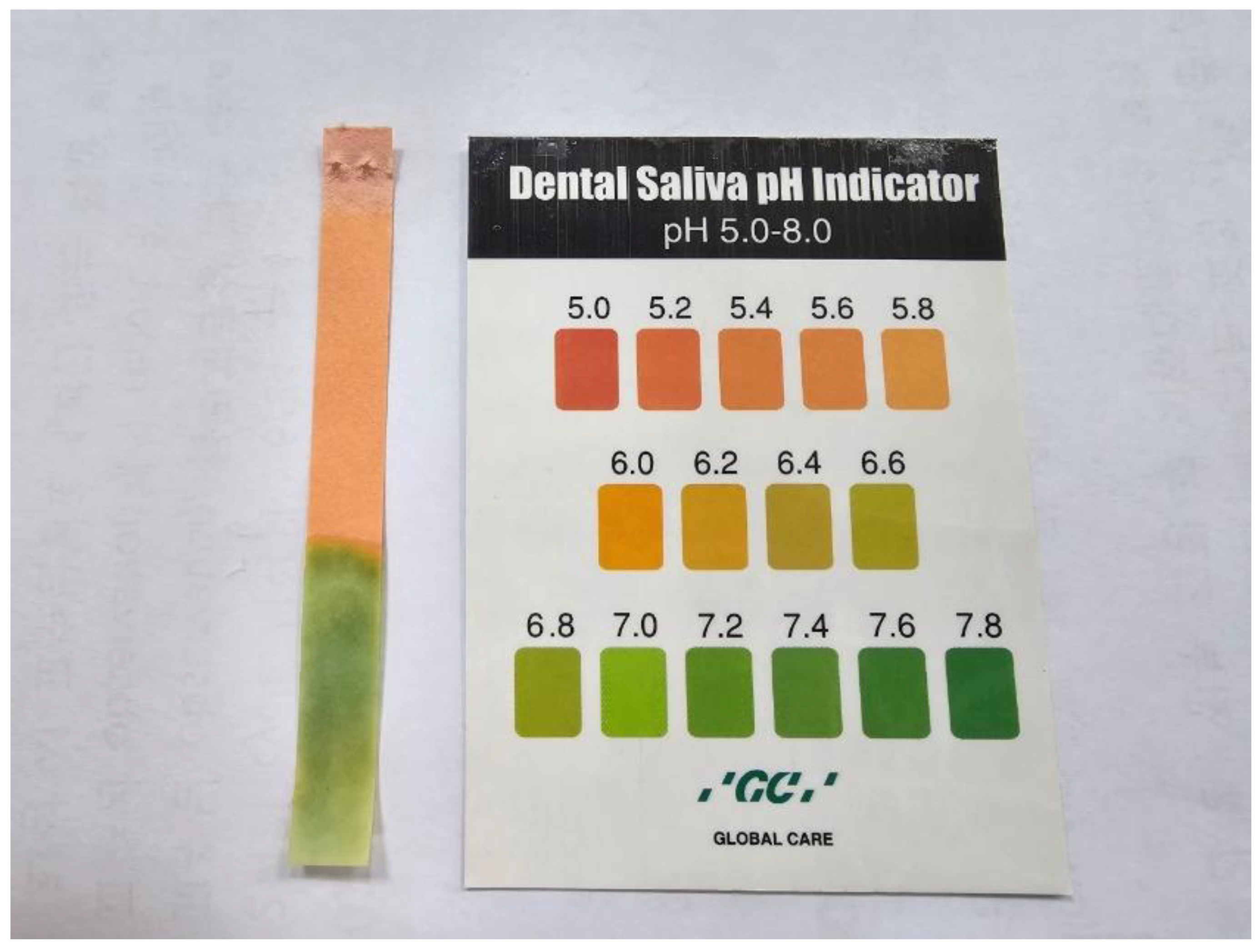
Figure 2.
Paraffin wax, buffer strip, and salivary buffer indicator. Patients were indicated to chew paraffin wax to collect stimulated salivary flow rate. Collected stimulated saliva was dropped on buffer strip, and changed color was recorded according to the salivary buffer indicator.
Figure 2.
Paraffin wax, buffer strip, and salivary buffer indicator. Patients were indicated to chew paraffin wax to collect stimulated salivary flow rate. Collected stimulated saliva was dropped on buffer strip, and changed color was recorded according to the salivary buffer indicator.
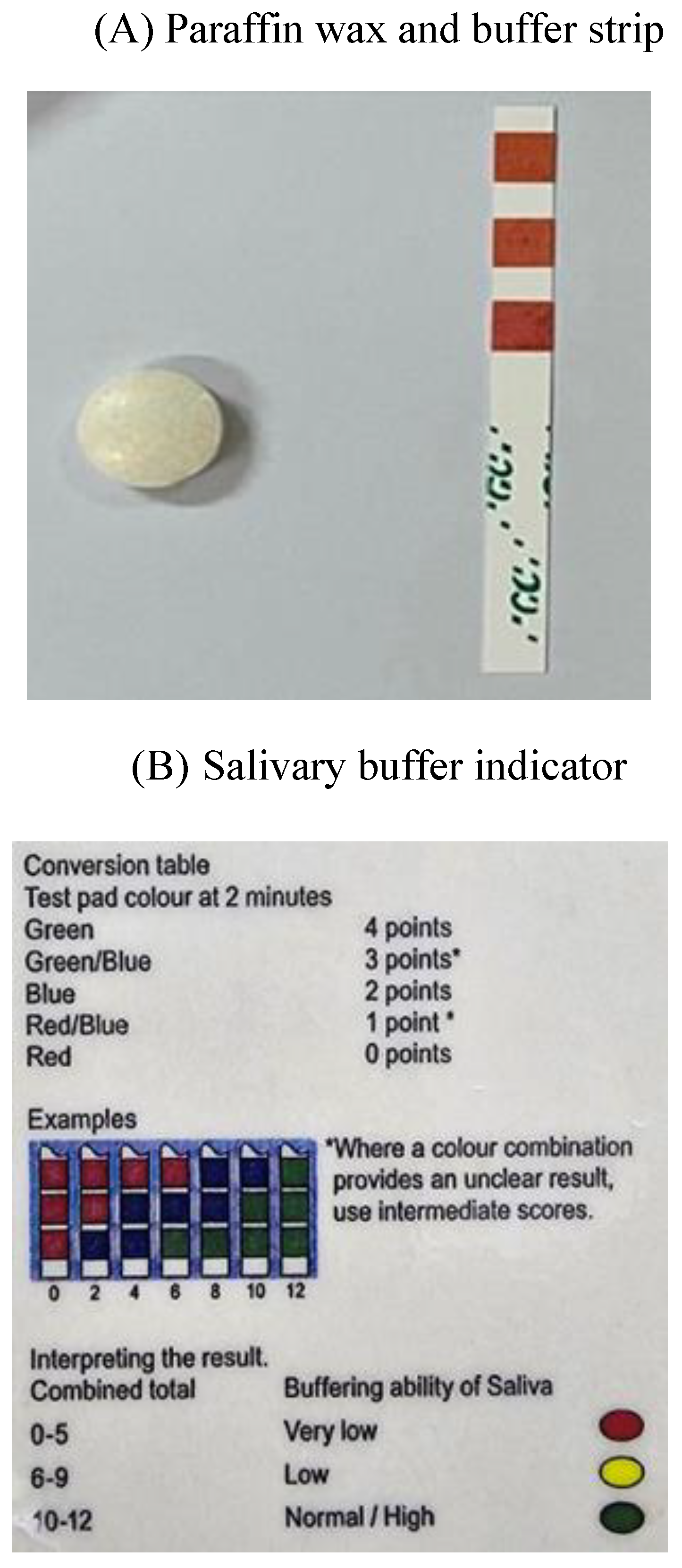
Figure 3.
Result page of halitosis evaluation. Levels of hydrogen sulfide (H2S), methyl mercaptan (CH3SH) were recorded.
Figure 3.
Result page of halitosis evaluation. Levels of hydrogen sulfide (H2S), methyl mercaptan (CH3SH) were recorded.
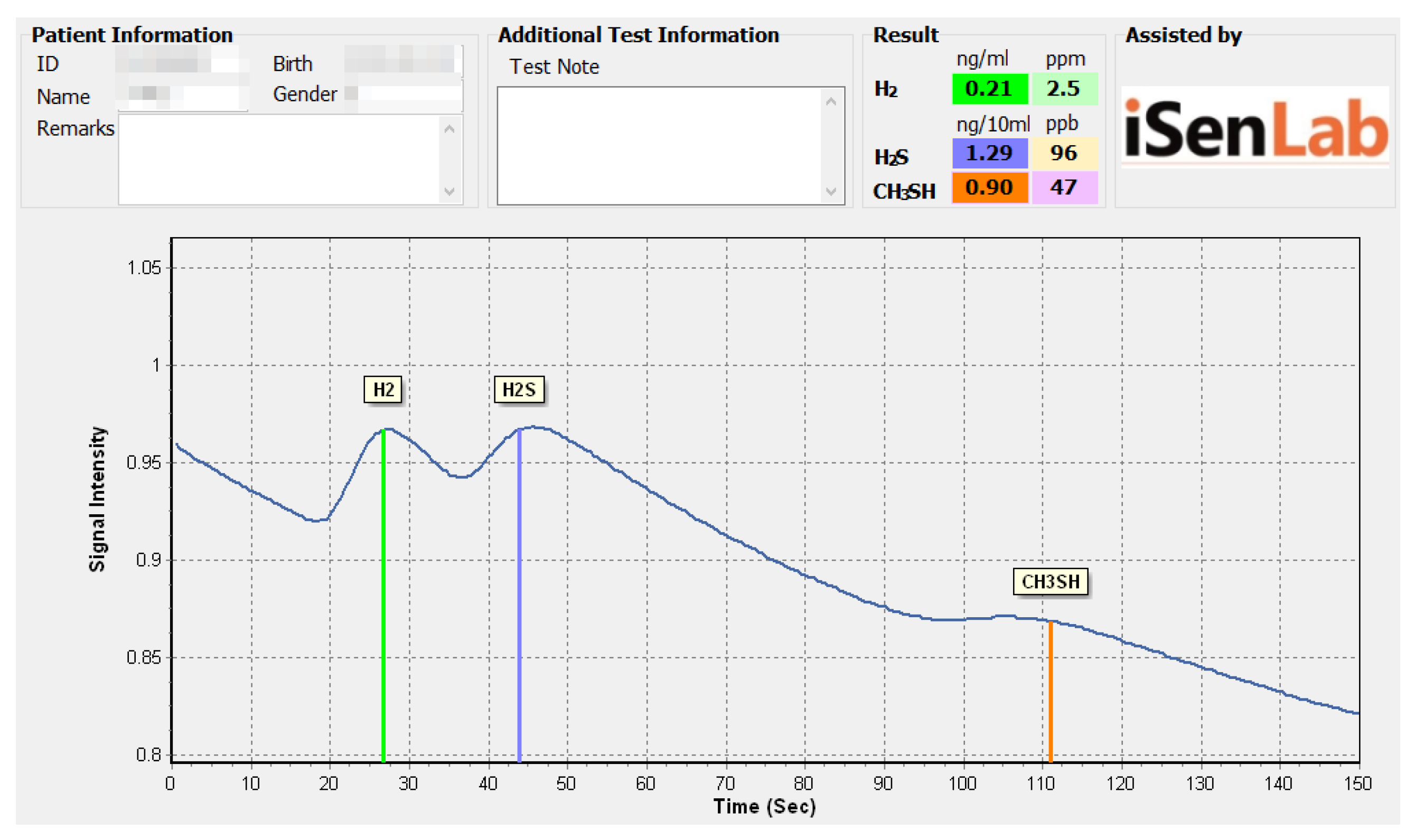
Figure 4.
Salivary flow rate by age group. The results of this analysis were obtained by ANOVA and post-hoc analysis. There was no significant difference in UFR and SFR across the age groups (all p > 0.05). UFR: Unstimulated Flow Rate, SFR: Stimulated Flow Rate.
Figure 4.
Salivary flow rate by age group. The results of this analysis were obtained by ANOVA and post-hoc analysis. There was no significant difference in UFR and SFR across the age groups (all p > 0.05). UFR: Unstimulated Flow Rate, SFR: Stimulated Flow Rate.

Figure 5.
Salivary parameters and VSC levels by age group. The results of this analysis were obtained by ANOVA and post-hoc analysis. There was no significant difference in salivary pH and buffer capacity across the age groups (all p > 0.05). * p < 0.05 indicates a significantly higher mean level of CH3SH in age group 2, compared with other age groups. H2S: Hydrogen sulfide, CH3SH: Methyl mercaptan, VSC: Volatile Sulfur Compounds.
Figure 5.
Salivary parameters and VSC levels by age group. The results of this analysis were obtained by ANOVA and post-hoc analysis. There was no significant difference in salivary pH and buffer capacity across the age groups (all p > 0.05). * p < 0.05 indicates a significantly higher mean level of CH3SH in age group 2, compared with other age groups. H2S: Hydrogen sulfide, CH3SH: Methyl mercaptan, VSC: Volatile Sulfur Compounds.
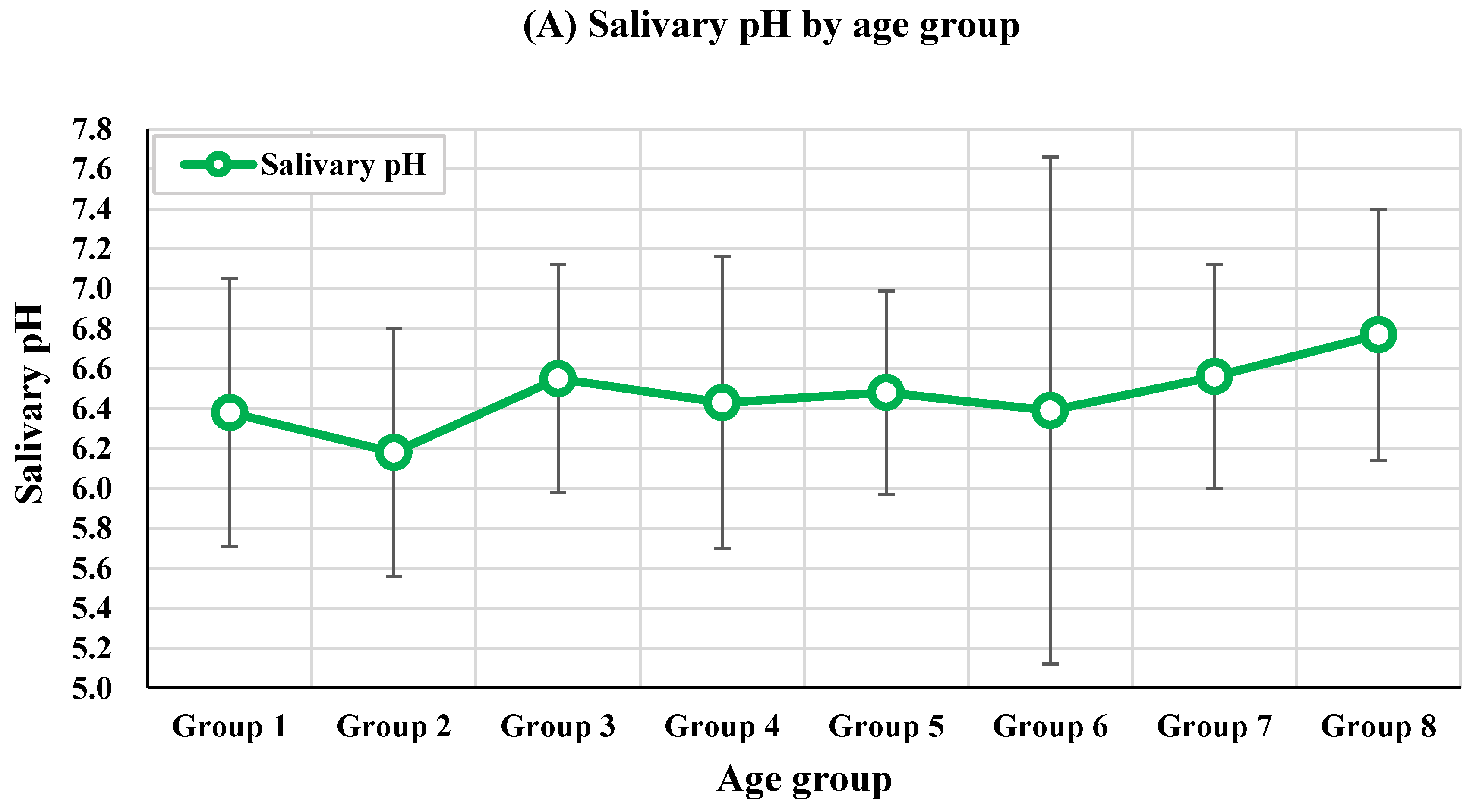
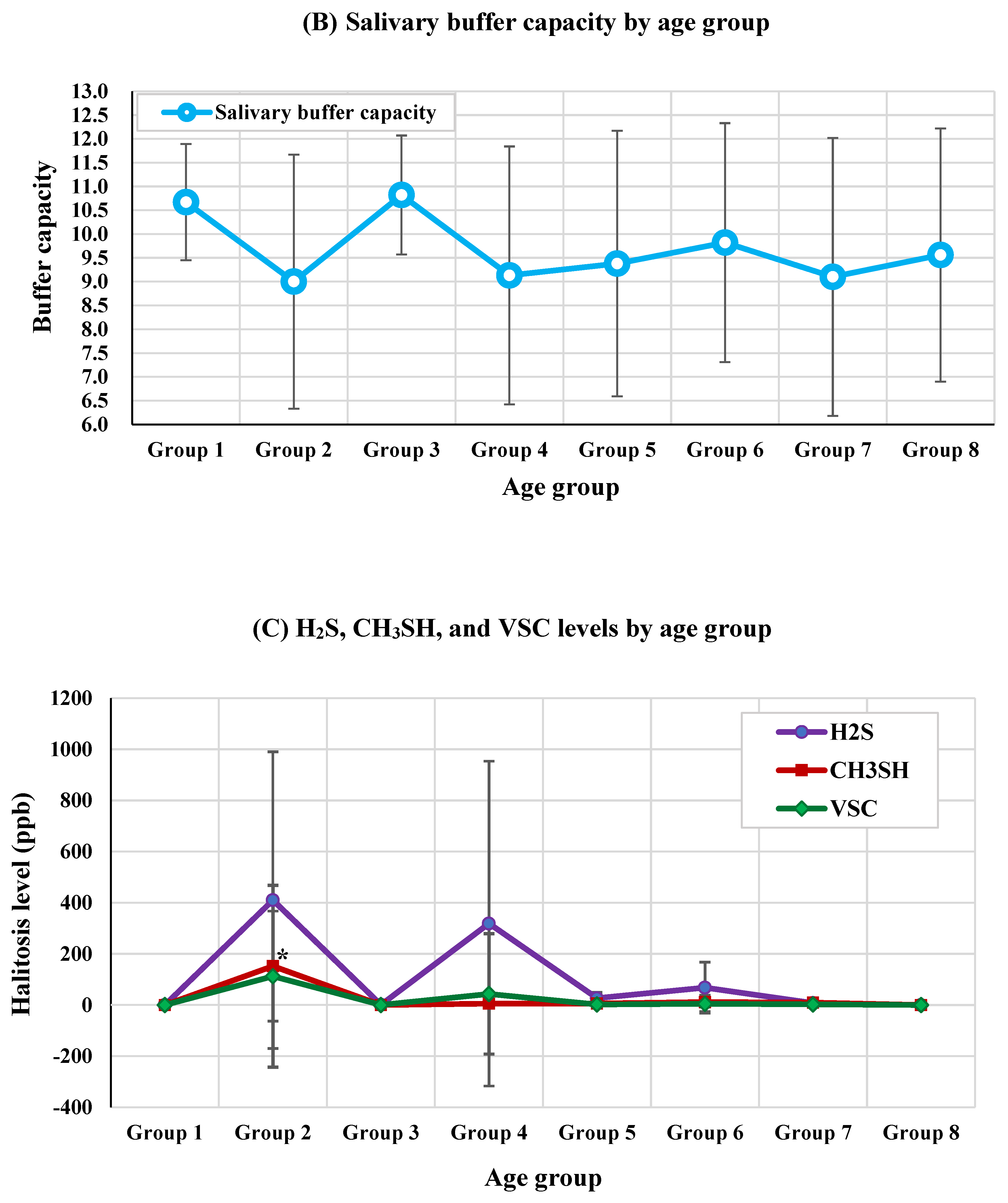
Figure 6.
Distribution of representative systemic diseases by age group. The results of this analysis were obtained by Pearson chi-square test and post-hoc analysis. *** p < 0.001 indicates a significant difference of prevalence of hypertension in age group 7 and 8, compared with age group 1 to 6. ** p < 0.01 indicates a significant difference of prevalence of diabetes mellitus in age group 7 and 8, compared with age group 1 to 6.
Figure 6.
Distribution of representative systemic diseases by age group. The results of this analysis were obtained by Pearson chi-square test and post-hoc analysis. *** p < 0.001 indicates a significant difference of prevalence of hypertension in age group 7 and 8, compared with age group 1 to 6. ** p < 0.01 indicates a significant difference of prevalence of diabetes mellitus in age group 7 and 8, compared with age group 1 to 6.
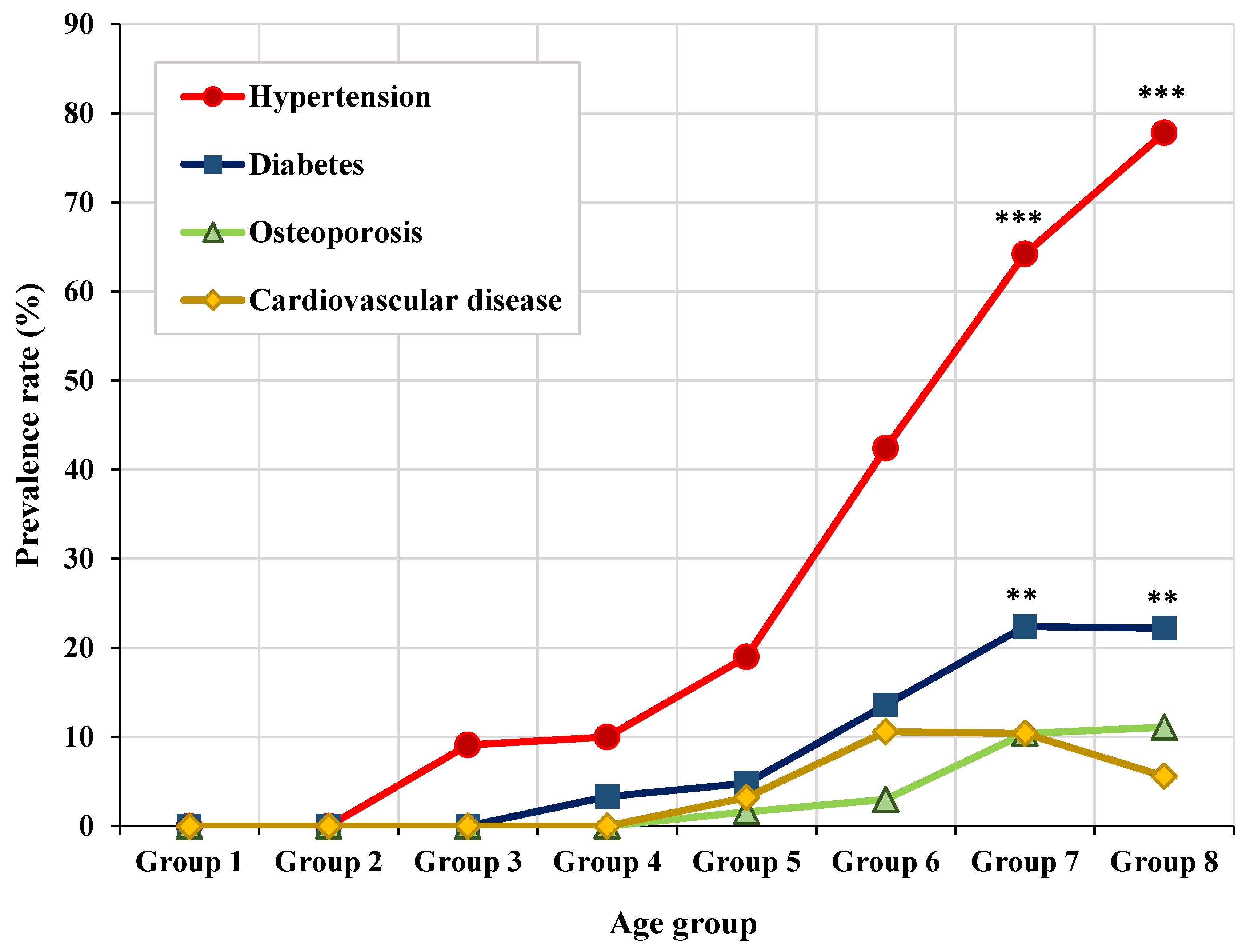

Table 1.
Gender and age distribution.
| Features | n (%) | Male n (%) | Female n (%) | p-value | |
|---|---|---|---|---|---|
| Sex | Male | 66 (24.1) | - | - | - |
| Female | 208 (75.9) | ||||
| Age | Group 1 (age 10s) | 9 (3.3) | 5(55.6%) | 4(44.4%) | 0.028* |
| Group 2 (age 20s) | 10 (3.6) | 6(60.0%) | 4(40.0%) | ||
| Group 3 (age 30s) | 11 (4.0) | 3(27.3%) | 8(72.7%) | ||
| Group 4 (age 40s) | 30 (10.9) | 6(20.0%) | 24(80.0%) | ||
| Group 5 (age 50s) | 63 (23.0) | 11(17.5%) | 52(82.5%) | ||
| Group 6 (age 60s) | 66 (24.1) | 13(19.7%) | 53(80.3%) | ||
| Group 7 (age 70s) | 67 (24.5) | 19(28.4%) | 48(71.6%) | ||
| Group 8 (age 80s) | 18 (6.6) | 3(16.7%) | 15(83.3%) | ||
| Total | 274 (100.0) | 66(24.1%) | 208(75.9%) | ||
The results of this analysis were derived using chi-square tests and post-hoc analyses. Significance set at p < 0.05. *p < 0.05; ** p < 0.01; *** p < 0.001.
Table 2.
Halitosis levels by age group.
| Features | Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | Group 6 | Group 7 | Group 8 | p-value | Post-hoc |
| Age 10s (n = 9) |
Age 20s (n = 10) |
Age 30s (n = 11) |
Age 40s (n = 30) |
Age 50s (n = 63) |
Age 60s (n = 66) |
Age 70s (n = 67) |
Age 80s (n = 18) |
|||
| Mean±SD or n (%) | Mean±SD or n (%) | Mean±SD or n (%) | Mean±SD or n (%) | Mean±SD or n (%) | Mean±SD or n (%) | Mean±SD or n (%) | Mean±SD or n (%) | |||
| Age (year) | 15.89±3.26 | 24.20±1.74 | 36.27±3.04 | 45.33±3.09 | 54.57±3.07 | 64.26±2.88 | 74.04±2.91 | 82.72±2.22 | <0.001*** | Age group 1<2<3<4<5<6<7<8 |
| H2S (ppb) | 0.00±0.00 | 410.00±579.82 | 1.00±1.00 | 318.50±635.00 | 26.50±22.81 | 68.00±99.58 | 7.89±12.34 | 0.00±0.00 | 0.393 | - |
| CH3SH (ppb) | 0.00±0.00 | 152.00±214.96 | 0.00±0.00 | 5.25±9.18 | 6.00±6.93 | 11.50±20.37 | 9.22±16.86 | 0.00±0.00 | 0.049* | Age group 2 > Others |
| VSC (ppb) | 0.00±0.00 | 112.40±355.44 | 0.273±0.65 | 43.17±235.49 | 2.06±9.74 | 4.82±32.00 | 2.30±10.50 | 0.00±0.00 | 0.051 | - |
| Halitosis | 0 (0.0%) | 1 (10.0%) | 0 (0.0%) | 1 (3.3%) | 2 (3.2%) | 2 (3.0%) | 1 (1.5%) | 0 (0.0%) | 0.807 |
The results of this analysis were obtained by ANOVA and post-hoc analysis. Significance set at p < 0.05. *p < 0.05; ** p < 0.01; *** p < 0.001. Statistically significant results are indicated in bold. SD: Standard Deviation, H2S: Hydrogen sulfide, CH3SH: Methyl mercaptan, VSC: Volatile Sulfur Compounds.
Table 3.
Correlations between age, halitosis, and salivary flow rate.
| Correlation | VSC (ppb) |
Halitosis | UFR (mL/min) |
SFR (mL/min) |
|
|---|---|---|---|---|---|
| Age (years) | Correlation Coefficient | 0.052 | 0.054 | −0.024 | 0.082 |
| p-value | 0.392 | 0.371 | 0.690 | 0.178 | |
|
VSC (ppb) |
Correlation Coefficient | 1.000 | 0.621 | 0.038 | 0.083 |
| p-value | <0.001*** | 0.533 | 0.171 | ||
| Halitosis | Correlation Coefficient | 1.000 | −0.010 | 0.074 | |
| p-value | 0.871 | 0.221 | |||
|
UFR (mL/min) |
Correlation Coefficient | 1.000 | 0.513 | ||
| p-value | <0.001*** | ||||
| SFR (mL/min) |
Correlation Coefficient | 1.000 | |||
| p-value | |||||
The results of this analysis were obtained using Cramer’s V analysis. Significance set at p < 0.05. ***p < .001. Statistically significant results are indicated in bold. UFR: Unstimulated Flow Rate, SFR: Stimulated Flow Rate, VSC: Volatile Sulfur Compounds, VAS: Visual Analog Scale.
Table 4.
Correlations between medications by age and oral health.
| Features | Aging | ||
|---|---|---|---|
| Correlation coefficient | p-value | ||
| Oral health | Sticky saliva | 0.022 | 0.721 |
| Oral hygiene | 0.087 | 0.152 | |
| Calculus deposition | 0.005 | 0.930 | |
| Tongue coating | 0.205 | 0.001*** | |
| Ulcer | 0.023 | 0.701 | |
| Oral candidiasis | 0.063 | 0.299 | |
| Systemic medication | Amlodipine | 0.249 | 0.001*** |
| Metformin | 0.031 | 0.614 | |
| Alendronate | 0.118 | 0.051 | |
| Furosemide | 0.068 | 0.278 | |
| Systemic disease | Hypertension | 0.495 | <0.001*** |
| Diabetes mellitus | 0.255 | <0.001*** | |
| Osteoporosis | 0.195 | 0.001** | |
| Cardiovascular diseases | 0.150 | 0.013* | |
The results of this analysis were obtained by Cramer’s V analysis. Significance set at p < 0.05. *p < .05; **p < .01; ***p < .001. Statistically significant results are indicated in bold.
Table 5.
A generalized linear model using oral health and salivary parameters to predict aging.
| Parameter | B | SE | 95% Wald CI | p-value | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Sticky saliva [ref.=none] | 6.039 | 2.383 | 1.368 | 10.709 | 0.011* |
| Oral hygiene_poor [ref.=good] | 11.752 | 4.864 | 2.219 | 21.286 | 0.016* |
| Oral hygiene_moderate [ref.=good] | 6.903 | 2.563 | 1.880 | 11.926 | 0.007** |
| Calculus deposition [ref.=none] | 2.533 | 5.711 | -8.660 | 13.725 | 0.657 |
| Oral ulcer [ref.=none] | -5.036 | 3.5272 | -11.949 | 1.877 | 0.153 |
| Tongue coating [ref.=none] | 4.615 | 2.007 | 0.681 | 8.549 | 0.021* |
| Halitosis [ref.=none] | 0.774 | 0.307 | 0.216 | 1.332 | 0.043* |
| Oral candidiasis [ref.=none] | -0.348 | 1.207 | -2.714 | 2.018 | 0.773 |
| Salivary pH | 0.308 | 1.239 | -2.120 | 2.735 | 0.804 |
| Saliva buffer capacity | -0.132 | 0.372 | -0.861 | 0.598 | 0.724 |
| UFR | 6.332 | 3.649 | -0.821 | 13.484 | 0.083 |
| SFR | -0.439 | 1.539 | -3.455 | 2.578 | 0.776 |
The results were obtained using a generalized linear model. In the generalized linear model, we obtained the adjusted model for systemic diseases and systemic medication. Significance set at p < 0.05. *p < .05; **p < .01. Statistically significant results are indicated in bold. UFR: unstimulated salivary flow rate, SFR: stimulated salivary flow rate, SE: standard error, CI: confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



