
Submitted:
29 August 2024
Posted:
30 August 2024
You are already at the latest version
Abstract
(1) Background: although current theories of Post-Traumatic Stress Disorder (PTSD) had focused on depressed mood and intrusion, the mechanism through which depression increases the risk of PTSD remains unclear. Research has concentrated on the hyper-active negative valence system (NVS) (e.g., increased fear and threat responses), but a significant role for hypo-active positive valence system (PVS) (e.g., less neural activation towards rewards) was conceivable. (2) Methods: To investigate the implicit processing in a refugee’s sample, ratings of arousal, dominance, and valence for 60 IAPS pictures (positive, neutral, and negative) were collected from 42 individuals with probable PTSD, and 26 trauma-exposed individuals (M age = 28.49 years, SD = ± 7.78). (3) Results: ANOVAs revealed a main group effect (η2p = 0.379) on arousal, dominance, and valence dimensions, and pictures’ categories (η2p = 0.620). Participants with PTSD responded to unpleasant images with enhanced arousal and lower valence ratings compared with individuals without PTSD. Moreover, arousal ratings were negatively correlated with valence (r = - 0.709, p < 0.01). (4) Conclusions: Our findings supported evidence according to which PTSD origins a state of maladaptive hyperarousal and difficulties in regulating emotions. Positive stimuli are considered less pleasant providing evidence for a complementary involvement of NVS and PVS in PTSD development.
Keywords:
Post-Traumatic Stress Disorder
; emotional numbing
; valence
; arousal
; reward system
; trauma
; refugees
1. Introduction
Post-Traumatic Stress Disorder (PTSD) was recognized as a disorder in 1980 [1]. Approximately 6-8% of the general population is identified with PTSD at some point in their lives making the diagnosis quite common. PTSD is widespread characterized by maladaptive fear responses following a traumatic event [2,3,4,5,6,7,8,9]. PTSD experienced by refugees has been linked to poor self-reported quality of life. Refugees are typically exposed to multiple types of traumatic events in their countries of origin. These events are often repeated, prolonged and interpersonal in nature, and have been demonstrated to have deleterious effects on mental health [9,10,11]. The effect of war on refugees’ lives is not temporary but persists over many years. Potentially traumatic events commonly experienced by refugees and asylum-seekers in their home countries include interpersonal violence, sexual violence, life-threatening injuries, witnessing death of loved ones, and torture. The extent of exposure to traumatic events may vary according to several factors including area/country of origin, characteristics of conflict and personal factors such as gender, age, ethnicity, and sexual orientation. The exposure to potentially traumatic events contributes considerably to psychopathology [3,12]. Elevated rates of psychological disorders including Major Depressive Disorder (MDD) and PTSD are frequently reported among refugees and asylum-seeker populations [13,14,15,16,17,18,19,20]. In addition, refugees face several daily challenges during displacement, as well as in the post-migration environment, including those related to lack of resources, family separation, social isolation and discrimination, socioeconomic factors, and immigration and refugee policies [16,21,22,23,24,25]. The growing number of displaced individuals worldwide and their disproportionately high rates of mental disorders have prompted the World Health Organization (WHO) to call upon treatment services to be responsive to the needs of asylum-seekers and refugees [26].
Considerable evidence sustains abnormalities in affective processing. Psychophysiological research provided evidence for increased amygdala activation and decreased activation in prefrontal cortical areas as well as reduced hippocampal volumes in PTSD, leading to a hypothetically over-reactive threat detection, possibly diminished regulatory control, and disrupted adaptive memory processes. Furthermore, the hyper-active negative valence system (NVS) - with increased physiological reactivity to aversive stimuli and reduced habituation of these reactions - has been involved in PTSD symptomatology. However, the heterogeneity of symptom profiles may be coupled with distinct aspects. It was showed that hyperarousal symptoms may be associated with increased neural responsiveness to negative stimuli and difficulties down-regulating emotions, with increased attentional focus to possibly threatening stimuli constantly demonstrated. Conversely, findings suggested that re-experiencing symptoms may be related with effortful suppression of intrusive emotions and thoughts. Moreover, avoidance and numbing may manifest as an overall disengagement from emotional processing with reduced neural responsiveness. To date, popular theoretical models of PTSD and psychophysiological research have mainly focused on the inhibition system - fear learning, maintenance, and extinction - due to the nature of the disorder’s fear-related symptoms [15,27,28,29,30]. Even though less explored, PTSD also involves depressive symptomatology, such as emotional numbing which is related to the reward system. The investigation of the relationship between PTSD and the reward system is not conclusive regarding whether reward system deficits are distinct from negative valence symptoms [3,31,32]. The reward system concerns an aggregate of neural circuitry that process appetitive stimuli - including the limbic system (septal area, thalamus, hypothalamus, amygdala), basal ganglia (containing the ventral and dorsal striatum), prefrontal cortex (ventromedial prefrontal cortex, in particular), ventral tegmental area (VTA), and substantia nigra. This system depends on neurotransmitters including serotonin, dopamine, and norepinephrine. Both opioid and cannabinoid systems are involved [3,33]. Some evidence suggests that PTSD might imply hypo-active positive valence system (PVS) (e.g., less neural activation towards rewards), as revealed by defective reward anticipation, diminished approach (reward-seeking) behavior, and reduced hedonic responses to rewards [27,34,35,36]. Abnormal reward-seeking and risky behaviors are in the PTSD criterion E2. Notably, PTSD is also highly comorbid with substance abuse (e.g.: alcohol, nicotine, cannabis, and opioids). Elevated levels of external reward seeking may be indication of reward system dysfunction in PTSD [37,38,39]. On the other hand, this maladaptive dimension in PTSD could be the consequence of an enhanced responsivity to negative stimuli [32]. In this perspective, considerable evidence relates this condition to oversensitivity of the negative system, revealing among PTSD individuals increased response to aversive or threatening stimuli [27,40], potentially reflecting symptoms of hyperarousal and intrusion (i.e., re-experiencing) [41]. The role of the neural negative valence system (NVS) in PTSD has been constantly recognized as atypically heightened salience network activation [42,43,44]. PTSD appears to be linked with biased neural valence processing, as indicated by hyper-responsivity to negative aversive stimuli and hypo-responsivity to positive rewarding stimuli [24,45,46]. However, depending on the involved methodologies and paradigms, the relative contribution of emotional processing to the development of PTSD remains mostly unknown [31,47] and there is still a need for further research to form a more definite picture [48]. Properly characterizing PTSD symptoms associated with the reward system, could empower professionals to effectively recognize predictive factors for the disorder, appropriately diagnose it [49,50,51] also developing treatments program that go beyond reversal of fear sustaining the prevention of weak outcomes, such as risk behaviors [52,53,54,55]. On the other hand, some evidence does support the existence of reward learning deficits in the neural circuits of individuals with PTSD [27,56,57,58,59]. Accordingly, addressing these issues may guide research toward a better understanding of mental disorders and their underlying psychological, neural, and biological mechanisms, ultimately leading to improved treatments through the diagnostic specificity, which is essential to develop precise interventions.
With the aim to focus implicit processing abnormalities of affective pictures in PTSD and potential underlying dimensions, we choose as research’s participants immigrants and refugees, as these groups have been frequently exposed to severe potentially traumatic experiences. Among this population, we compared individuals with a probable PTSD with people who had experienced identical events but did not fulfill PTSD criteria. We were able to examine participants having no history of diagnosis and treatment involving psychoactive medication or drug abuse. By comparing these groups, we intended at disentangle between effects related to trauma exposure and those related to the presence of PTSD. We explored these questions: (1) What is the effect of probable PTSD on affective evaluations of positive, negative, and neutral items? (2) What is the effect of trauma-exposure on affective ratings? Firstly, with respect to the presented literature, we suggested that if the disorder involves a numbing, then participants with probable PTSD would show lower valence ratings (i.e., less pleasure affect) and/or larger ratings of arousal/activation (i.e., reduced emotional activation) in response to negative photographs compared with the trauma-exposed individuals.
2. Materials and Methods
2.1. Participants
For the current study, a convenience sample of 69 trauma-exposed people was recruited between September 2019 and February 2020 at the Coop Dimora D’Abramo refugee’s center from Consorzio di Solidarietà Sociale Oscar Romero established in Reggio Emilia, Italy. Inclusion criteria were defined as: (a) age between 18 and 60 years; (b) status refugee or asylum seeker, which is defined according to the UNHCR (UNHCR, 2018); (c) exposure to relevant potentially traumatic events; (d) informed consent. The exclusion criteria were: (a) missing informed consent; (b) age under 18 years or over 60 years; (c) current risk of suicidality established on clinical judgement; (e) self-reported as having a color-vision deficit. Following enrollment, participants were further subdivided according to PTSD symptoms (Probable PTSD Group vs. Trauma-exposed Group).
2.2. Materials
2.2.1. Selection of the experimental stimuli
The tool used for emotion exposure in the present study was the International Affective Picture System (IAPS), which is currently employed in various research fields. The IAPS is a collection of photographic images that have been shown to induce positive, negative, or neutral affective states [60,61]. It presents three-dimensional values of arousal (the level of excitation), dominance, and valence (pleasantness or unpleasantness) of emotional responses, which are assessed through a standardized assessment in terms of valence (ranging from “pleasant” to “unpleasant”), arousal (ranging from “calm” to “excited”), and dominance (ranging from “in control of emotion” to “influenced by the emotion evoked by the picture”). Sixty photographs were chosen based on their normative rating from the International Affective Pictures System [62].
2.3. Measures
2.3.1. Questionnaire Measuring Demographics and Trauma Exposure
Exposure to potentially traumatizing events was determined by a semi-structured interview. Items involved traumas directed at the self and others. This interview collected information about socio-demographic (participants’ gender, age, education, marital status, religion, years in Italy, living with family, employment), and trauma- and displacement-related factors. The list of potentially traumatic experiences was based on events frequently experienced by refugee and asylum seekers [51,52,63,64,65] and aimed to collect much information as possible (a total of 13 categories of traumatic events was defined). Typical items included political imprisonment, assault, torture, witnessing murder, exposure to massacres, losses/separations of family or close others, and severe deprivation of medical care for self or others. We also entered an inventory of adversities such as insufficient food, inadequate finances, poor shelter, unemployment, and experiences of conflict. Participants indicated experiencing and/or witnessing each type of event through “yes/no” responses.
2.3.2. PTSD Symptom Screening
To detect PTSD symptoms the revised Part IV from the Harvard Trauma Questionnaire for measuring torture and trauma according to DSM-5 criteria for PTSD (HTQ-5) [63] was used. Part four of the HTQ covers 40 items related to PTSD and refugee-specific expressions of functional distress. However, the widespread modification of the diagnostic criteria for PTSD in the DSM-5 has necessitated the modification of Part 4 of the HTQ [2,63]. Vindbjerg and colleagues [66] have already proposed a first revision of the original tool (HTQ-PTSD-R), where the 16 items were sub-divided according to the DSM-5 into the four PTSD clusters: a) Intrusion symptoms; b) Avoidance; c) Negative alterations in cognitions and mood; d) Alterations in arousal and reactivity or into two subscales, an arousal-intrusion subscale (AIS) and an avoidance-numbing subscale (ANS) [66]. The main updates of the current version [12,63] were the addition of nine new items including two dissociative specifiers (items 17-25). Results of Mollica’s study showed that the internal consistency for the fourth part (0.96) was robust. This tool has been found to be valid and reliable across a large range of populations [64,65,67].
These 25 items are employed for the purposes of the present investigation. Participants are requested to report on a four-point Likert scale how much they had been troubled by a distinct symptom, ranging from “not at all” (1) to “extremely” (4), during the last week. The prevalence and severity of trauma symptoms were assessed using the mean item scores for the first HTQ-25 items. A standard cutoff score of 2.5, as reported by Mollica et al. [51] was adopted to indicate probable PTSD. The Italian validation of the tool [68] has showed an excellent internal consistency, revealing a HTQ five-factor solution as the best model, with satisfactory indexes of fit, and the best cut-off of 2.0 allowed discriminating for PTSD positive cases. This version was used for participants who preferred conducting the study in Italian language. Individuals can be regard as symptomatic if their mean score achieves the cut-off of ≥ 2.
2.3.3. Affective Ratings
Figure 1 illustrates the experimental procedure. To assess the three dimensions of pleasure, arousal, and dominance, the Self-Assessment Manikin (SAM) [60,69] was used. In this system, a graphic figure depicting values along each of the 3 dimensions on a continuously varying scale is used to indicate emotional reactions. Bradley and collaborators [60] argued that the assessment of each of these dimensions organize the response of the individuals to affective stimuli, which can be conceptualized considering two fundamentally motivational systems of avoidance (the defensive system) and approach (the appetitive system). The defensive system is primarily activated in contexts representing a threat to an organism’s survival, eliciting behaviors such as withdrawal or attack, while the appetitive system is primarily activated in contexts that promote the well-being and survival of the organism. These two systems account for two basic dimensions of emotion: valence and arousal. The first indicates which system is active, while the second reflects the intensity of the activation. Therefore, the emotional reaction elicited by affective stimuli may be described by its location on a two-dimensional affective space (ordinate = valence; abscissa = arousal). This way, the subjects exposed to the IAPS photographs can select any one of the images included on each scale or from between either of the two images that results in a scale of nine points for each dimension [69]. Ratings are scored such that 9 represents a high rating on each dimension and 1 represents a low rating on each dimension. The scale of emotional valence was used to estimate the extent of positive or negative reaction evoked by a given picture, ranging from 1 to 9 (1 for very negative emotions and 9 for very positive emotions). On the scale of arousal, participants estimated to what extent a specific picture makes them feel unaroused or aroused, ranging from 1 to 9 (1 for unaroused/relaxed and 9 for very much aroused, for instance agitated or excited). Lastly, the dominance dimension ranges from “out of control” to “in control” and is represented as a huge figure or as a tiny figure. Within the selected items [60,62,69], 28 presented positive events, 20 pictures with negative events, and 12 displayed neutral events. The three groups differed significantly from each other in IAPS normative valence ratings, their average arousing levels were 4.693 (SD = 0.959) for positive, 5.799 (SD= 0.948) for negatives, and 4.604 (SD = 1.288) for neutral photographs. The average dominance levels were of 5.672 (SD = 0.717) for positive, 3.743 (SD = 0.699) for negatives, and 4.971 (SD = 0.604) for neutral photographs, respectively.
2.4. Procedure
Study procedures were approved by the local Ethic Committee of the Area Vasta Emilia Nord - AVEN (Ref. 1156/2020/OSS/UNIPR) and were carried out in accordance with the Declaration of Helsinki. The participants were informed about the aim of the research and no identification or names were recorded to maintain confidentiality. The subjects’ consent was obtained after explaining information on the experiment. The study participants were informed of their right to refuse or stop participating at any time. The experimental sessions were completed by psychologists with master’s or doctoral-level qualifications, with the aid of experienced interpreters, when necessary. On the first session, the purpose of the study was explained to all participants and written consent was obtained. Once the information letter was read and the consent form signed, the semi-structured interview and the HTQ were administered in English or in Italian with the support of cultural mediators. Following this and the allocation to groups, a second session took place. Participants were seated in front of white screen and were informed that the aim of the study was to investigate how humans respond to pictures that represent different events occurring in life. Following this, the instructor stated the detailed explanation of the procedure, the instructions were presented, and the photographs were then shown sequentially. The experimenter first explained the meaning of valence, arousal, and dominance to the participants and then how to rate the pictures on a paper version of the SAM. Instructions were provided to specifically target the affective response associated with each stimulus. Pictures were presented on a monitor. Participants were instructed to rate how they felt while looking at each picture. A total of sixty pictures was presented with the following sequence: a warning slide displayed for 5 s, informing of the number of the picture to be rated. The picture itself followed and was shown for 6 s. Participants then had 15 s to rate the dimensions of valence, arousal, and dominance for each picture using a 9-point SAM [60].
The valence portion assesses the subject’s emotions over a range from pleasant to unpleasant, the arousal section assesses emotions ranging from calm to excited, and the dominance section assesses emotions ranging from controlled to uncontrolled states. Before starting the procedure, subjects went through two practice trials with the aim to familiarize themselves with the rating procedure: one positive and one negative. Before viewing a given IAPS picture, the instruction: “Please rate the next picture in line number n…” appeared in the center of the screen for 5 s. During this period, participants must search in their booklet the numerical code corresponding to the row where that picture should be rated. After 5-s, the first IAPS picture will present for 6 s.
Figure 1.
Experimental paradigm.
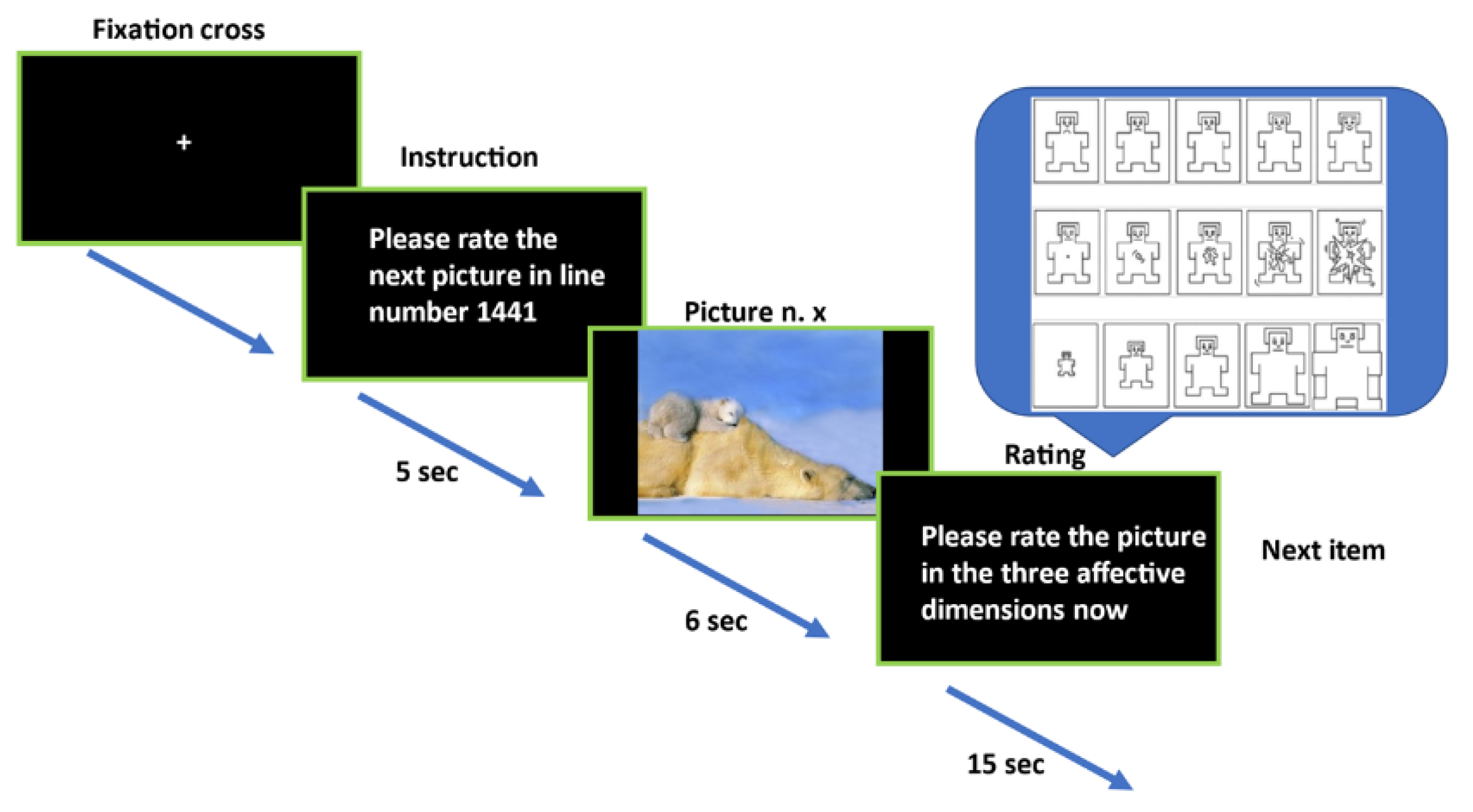
During this time, participants were instructed to pay maximum attention to the picture and the instruction “Please rate the picture in the three affective dimensions now” appeared into the center of the screen for 15 s. During this time lapse, participants rated the picture in the three affective dimensions in the row of their booklet. When the response time has elapsed, the next trial began. The images were presented in a random order under the following constraints: no more than two images from each affective condition/category (pleasant, unpleasant, neutral) and no more than three pictures from each content category appeared consecutively. The IAPS pictures were displayed on the whole screen, see [62]. Each trial lasted 26 s and the entire procedure took approximately 30 min. Participants who were found having a probable PTSD, received information on their condition, and they were forwarded at a nearby psychiatric unit.
2.5. Data Analysis
This study aimed to explore the differences in affective responses among trauma survivors, categorized as either having “Probable PTSD” or being merely “Trauma-exposed.” The PTSD classification was determined using the HTQ-5, with cutoff scores set at 2.5 for the English version and 2.0 for the Italian version (refer to Measures section). Emotional normality distribution was assessed with Kolmogorov-Smirnov test. Categorical data were represented with counts (n) and percentages (%), while continuous variables were reported as mean ± standard error (ES). For categorical variables, Pearson’s Chi-square and Fisher’s exact tests were employed when the Chi-square assumptions were not met. Continuous variables were compared using Student’s t-test, provided assumptions of normality and equal variances held; otherwise, the Mann-Whitney U test was used. A series of 2 × 3 ANOVAs were conducted to explore the main effects and interactions between two factors: group (Probable PTSD vs. Trauma-exposed) and emotional content of images (Positive vs. Neutral vs. Negative). These analyses were aimed at examining their influence on three emotional dimensions: Valence, Arousal, and Dominance. The effect sizes were estimated using partial eta-squared (η2p). Both trauma occurrence and the type of emotional content in images were treated as between-group factors. Lastly, Spearman’s correlation coefficients (r) were calculated to examine the relationships among valence, arousal, and dominance ratings within the sample. All analyses were performed using statistical software, IBM SPSS Statistics for Windows, Version 29.0. Armonk, NY: IBM Corp. The statistical threshold was set at p < 0.05.
3. Results
3.1. Sample Characteristics
Detailed information concerning the main sociodemographic and clinical characteristics assessed is provided in Table 1 where mean and percent of the main variables were reported. The present study included 68 participants; one subject was excluded due uncomplete data. Their mean age (±SD) was 28.493 (± 7.785) years, with age ranging from 18 to 53 years. Among the respondents, 58 (85.15 %) were male, 52 (78.45 %) were single. Most of the refugees in the sample named Nigeria as their country of origin (25%), followed by Pakistan (14.71%), Gambia (11.8%), Bangladesh (8.82%) and Ivory Coast (8.82%). A 44.1% of participants completed middle school followed by 29.4% without any qualification. Most of them are Muslim by religion (63.2%) followed by 35.3% of Christian religion. The most frequent means of arrival in Italy was by boat, followed by on foot (4%) and by train (4%), and before Italy, 89.7% had been in other countries. The majority were asylum seekers (86.4%) whereas 13.55% a refugee status. The mean years of stay in Italy was of 3.74 years (SD = 2.00). Regarding current occupation, 44 participants (64.7 %) were currently not occupied while 53 of them (77.9%) worked in their country of origin.
All participants fulfilled DSM-5 criterion “A” having been exposed (i.e., experienced, or directly witnessed) to several types of traumatic events. The most frequent type of trauma experienced included, threats (72.1%), having witnessed beatings of acquaintances (41.2%), unknown people (33.8%) or acquaintances’ rape (20.6%). Having witnessed death of acquaintances (54.4%), injured people (36%), suffered injuries themselves (32.4%), especially attributable to beatings (33.8%) and killing of relatives (25%) were also common. On average, trauma exposure occurred 5.44 years (SD=3.61) earlier).
Of the 68 participants, according to HTQ-5 scores, 26 met criteria for probable PTSD (Probable PTSD group, 22 Males) whereas 42 not met criteria for PTSD even though they had experienced significant traumatic experiences (Trauma-exposed group, 36 Males). The sociodemographic characteristics appear to be highly comparable between groups. The groups did not differ on age, education level and other characteristics of trauma exposure but only for scores from Part IV of the HTQ-5 for PTSD [t (66) = 11.66, p < 0.0001].
3.2. Emotional Ratings Analysis
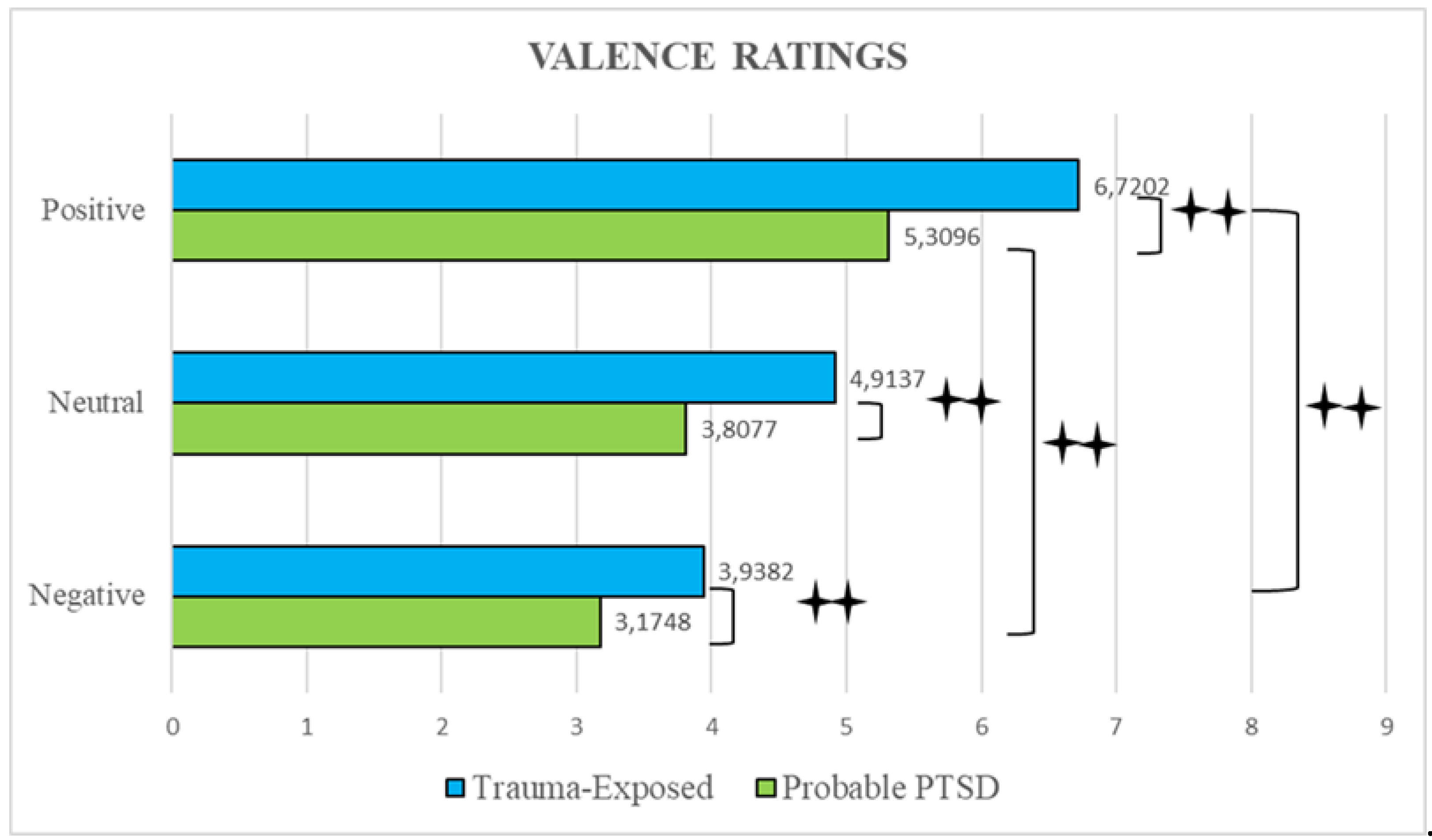
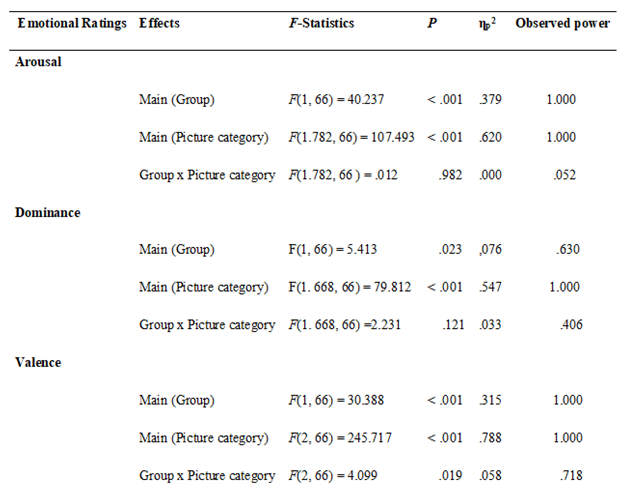
For each image, the mean valence, arousal and dominance ratings and the corresponding standard deviations (SD) were calculated. Mean of emotional ratings for pictures as a function of groups (Probable PTSD, Trauma-exposed) and conditions (positive, negative, and neutral images) are reported in Figure 2. SAM arousal, valence and dominance ratings were then analyzed in separate analyses of variance (ANOVAs), with group (Probable PTSD, Trauma-exposed) and pictures category (positive, neutral, negative) as between subjects’ factors revealing effects reported in Table 2. The mean arousal ratings of Probable PTSD group exceeded that of Trauma-exposed group and decreased across pictures category from negative (see Figure 2), to neutral, and positive. In the ANOVA (see Table 2) a significant main effect of group (p < 0.001, η2p = 0.379) for the arousal dimension was found, with pairwise comparisons showing higher ratings for the Probable PTSD group compared to the Trauma-exposed group (p < 0.001). As expected, a picture category main effect was also significant (p < 0.001, η2p = 0.620) with pairwise comparisons revealing that aversive pictures being rated as more arousing compared to neutral (p < 0.001) and pleasant (p < 0.001) pictures. Neutral pictures were also rated as more arousing than positive pictures (p < 0.001), and there was no significative interaction.

Table 1.
Socio-demographic and trauma-related events of the two subjects’ groups.
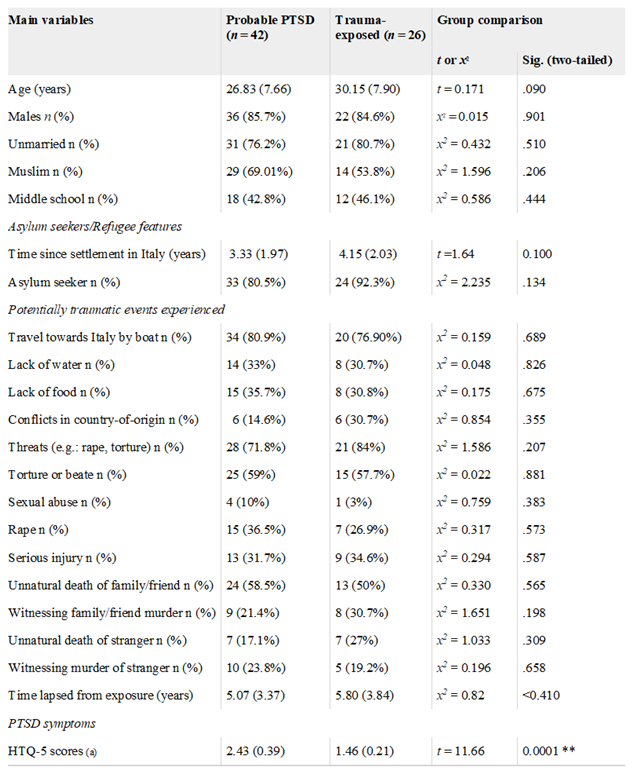
(a) Scores from Part IV of the Harvard Trauma Questionnaire for measuring torture and trauma according to DSM-5 criteria for PTSD (HTQ-5).
Note that for English version the cut-off was 2.5 whereas for the Italian version was 2.00.
Furthermore, individuals with probable PTSD responded to all images with lower valence relative to the controls for negative, positive, and for neutral pictures. With respect to the valence rating, a significant effect of group emerged from ANOVA (p < 0.001, η2p = 0.315). Here, Probable PTSD participants rated valence significantly less than Trauma-exposed individuals. There was an additional main effect of ‘picture category’ (p < 0.001, η2p = 0.788). Overall, positive pictures were rated as more pleasant compared to neutral (p < 0.001) and unpleasant (p < 0.001) pictures. Neutral pictures were also rated as more pleasant than unpleasant pictures (p < 0.001). Regarding dominance, the Probable PTSD group reported lower mean ratings for positive images compared to those produced by the Trauma-exposed group. Similarly, for neutral and negative pictures, the Probable PTSD group’s mean dominance ratings were lower than those of the control group. From the ANOVA, a main effect (p < 0.001, η2p = 0.547) was detected for of pictures’ category but not for group.
Figure 2a.
Mean arousal ratings for both groups.
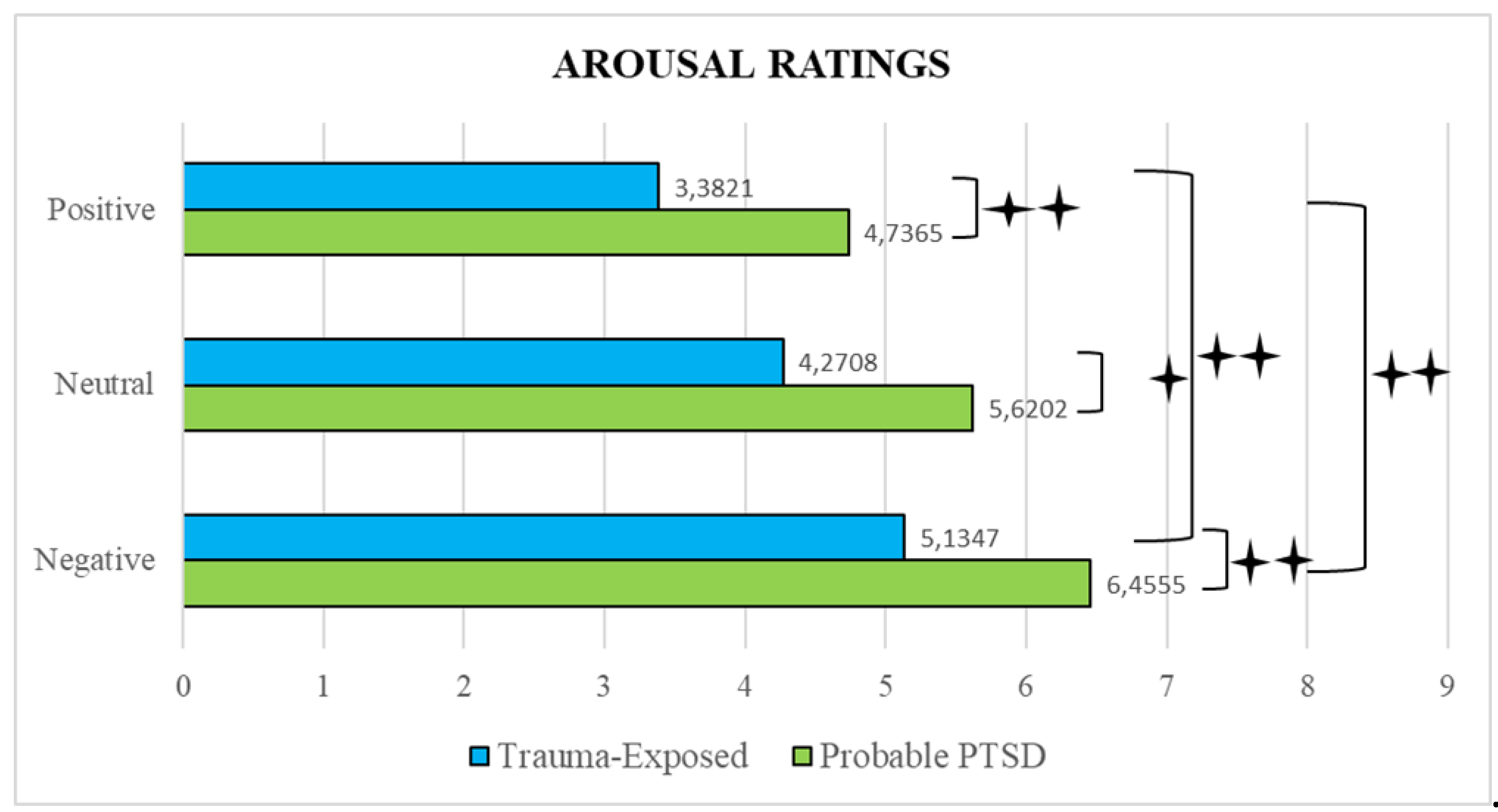
Figure 2b.
Mean dominance ratings for both groups.
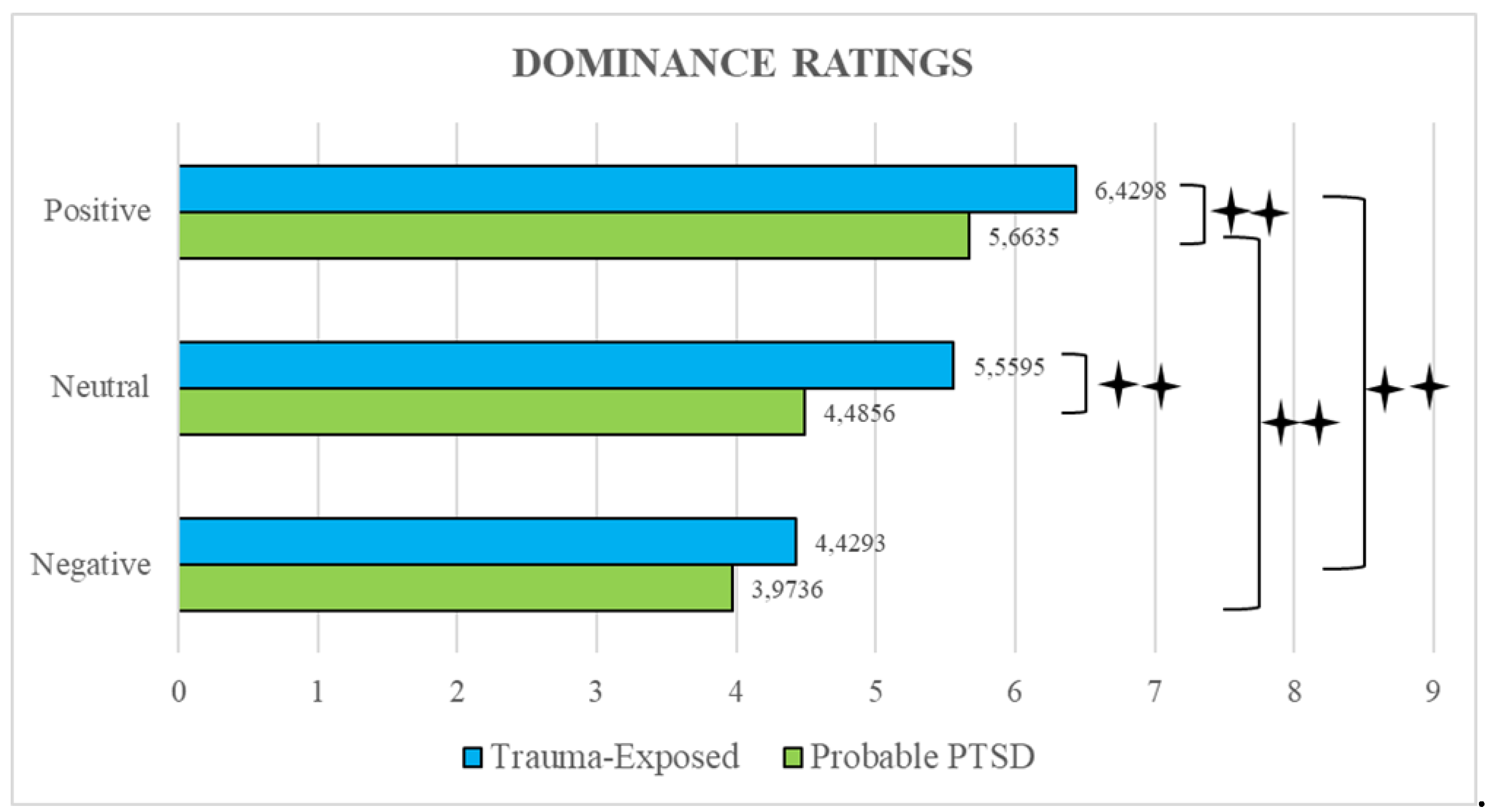
Figure 2c.
Mean valence ratings for both groups.
Pairwise comparisons showed enhanced dominance ratings for positive pictures compared to neutral (p < 0.001), and aversive pictures (p < 0.001). Further, neutral pictures displayed more dominance compared to negative ones (p < 0.001). The interaction between groups and picture categories did not reached significance but significant differences between groups (p < 0.005) emerged for positive and neutral images ratings.
Table 2.
ANOVA with group (Probable PTSD, Trauma-exposed) and pictures category (positive, neutral, negative) as between subjects’ factors.
Table 2.
ANOVA with group (Probable PTSD, Trauma-exposed) and pictures category (positive, neutral, negative) as between subjects’ factors.
3.3. Correlations between Ratings
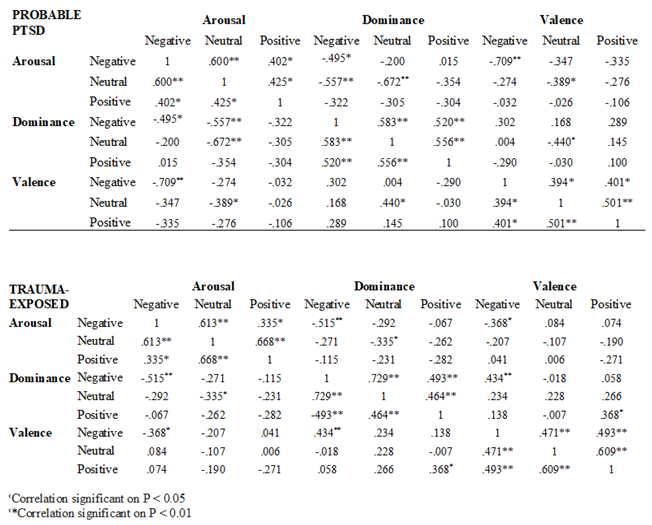
Correlations between emotive ratings for pictures across all stimuli conditions can be found in Table 3. Spearman’s correlation coefficients (r) were calculated to clarify the correlations between the valence, arousal, and dominance ratings in our sample. To explore the exact contributions of valence and arousal in affective processing, the occurrence of negative correlations between these dimensions was also tested within both groups, first for negative images, then for positive images and, finally, for neutral images.
Concerning the Probable PTSD group, results showed that for negative pictures, the arousal ratings were negatively correlated with valence ratings (r = - 0.709, p < 0.01) indicating that pictures with high arousal (negative) were associated with lower valence. Furthermore, arousal ratings were negatively correlated with dominance (r = - 0.495, p < 0.05). Regarding positive pictures, results from the Probable PTSD group failed to show any correlation between emotional ratings. On the contrary, among Trauma-exposed individuals, valence ratings were positively correlated with dominance ratings indicating that pictures with high valence (positive) were more highly dominant. Regarding neutral images, data indicated significant negative correlations between arousal and dominance, and valence and arousal only among the PTSD group. Conversely, for Trauma-exposed individuals a significant negative correlation was detected between arousal and dominance. Additional correlations are visible in Table 3.
Table 3.
Correlations between emotive ratings for pictures across all stimuli conditions.
4. Discussion
Our research aimed at investigating how the affective response differs between trauma survivors either suffering from probable PTSD or not. The main purpose of the present study was exploring whether a probable PTSD leads to a different rating of the emotional dimensions of valence (unpleasantness/pleasantness), arousal (calm/agitated), and dominance (domination/non-domination). We anticipated significant interactions across all trauma and emotional content conditions, except for neutral images. Specifically, it was expected that the Probable PTSD group would exhibit the highest arousal levels in response to negative images compared to the control group. However, given evidence on trauma’s impact on neural responses to reward systems, it was hypothesized that positive images would induce lower self-reported valence levels in the Probable PTSD group. Refugees and asylum seekers arrive in our country after dangerous journeys often crossing through Libya, where they are subjected to intimidation, torture or kidnapping before crossing the Mediterranean on precarious vessels. Furthermore, the participants often claimed to have witnessed violence of various kinds even against family and friends and/or strangers, events considered potentially traumatic events, as suggested by the criterion “A” from the DSM-5. Many participants witnessed death firsthand, assisting family members, friends, or strangers at the time of passing, due to natural causes such as illness and old age, but also to wasting due to lack of food and water or extreme heat and tiredness during the journey. Finally, it was witnessing the murder of one’s travel companions was also common. These especially harmful events probably favored the onset of PTSD. In fact, the administration of the HTQ-5 DSM-5 PTSD [63] revealed the disorder among 38.2% of cases. This prevalence is in line with the literature according to which PTSD in refugees and asylum seekers shows a prevalence rate between 23% and 88.3% [70], much higher than in the general population where it is between 0.2% and 3.8%.
5. Limitation and Future Directions
The study has several strengths, it included important variables, which were not considered in previous studies, such as comparing between individuals who developed a probable PTSD exposed to the same potentially traumatic events of individuals who did not develop traumatic symptoms, and group differences can be solely attributed to PTSD status because there were not substantial differences between groups. Furthermore, an updated standardized instrument for measuring PTSD was used. Nevertheless, several limitations of this work must be acknowledged. All the participants were recruited in the same center in Italy and the sample size is relatively small. Moreover, excluding individuals hosted by relatives or friends or living in unregistered camps, could be considered as a form of limitation bias of the present research. Considering the magnitude of our results, statistical power, and the cross-sectional design, any generalization of the findings must be approached with caution. Furthermore, the probable presence of depression, whose effects on emotion regulation, were not verified and could be confused with those of PTSD. It could be useful to include among the tools a test to verify the possible presence of depression so as not to have possible interference effects between the two disorders, often comorbid with each other. The level of education held by the participants may have made the interpretation of the 9-point SAM scales difficult. Since the number of points did not correspond to the number of stick figures of the SAM, some participants found it difficult to assign scores, tending to give extreme answers on one side or the other of the continuum. The use of the 9-point SAM scale could be changed to the 7-point or 5-point version, to facilitate the understanding of the assessment task by the participants. Some of the IAPs images selected in the study were challenging for the participants to interpret, especially those of neutral valence (e.g., mineral images) which may have been incorrectly interpreted. Assessing emotion processing using such subjective measures may be particularly problematic for refugees, who have difficulties in identifying and describing their own emotions. Furthermore, the setting itself may have been a trauma reminder for some individuals, although we put great effort into ensuring that the research situation was not evocative of trauma experiences (e.g., only psychologists conducted the experiment).
In the future, the study could be repeated with a larger sample size with subjects from different centers. Moreover, neurobiological measures of emotion including physiological, and neural measures, should improve our understanding of how people respond to emotional stimuli and regulate negative emotions to better characterize the clinical affective dysfunction. Finally, it would also be interesting to be able to have a gender-balanced sample to verify whether women with asylum seeker or refugee status are predisposed to developing PTSD, as is typical of the general population. Nevertheless, it is meaningful to explore the relationship between PTSD in the context of processing of aversive and rewarding stimuli. The findings from the present investigation have potential clinical implications. For example, the finding that low emotion regulation capacity (indexed by high arousal levels) in refugees linked to a possible diminished anger recovery following exposure to trauma related stimuli may point to the importance of targeting prolonged anger responses when implementing psychological interventions. Furthermore, this study highlighted that affective reaction to trauma-related cues does not only depend on the evocation of negative effects but also on their positive. Therefore, when focusing on individual’s emotions, the precise assessment of both is important. This also stands true for research that investigates affective reaction following trauma cues, with these findings advising that it is important to assess not only the negative response, but also the positive ones. Another key consideration is the sensitivity of the IAPS tool for measuring emotional processing. Researchers have questioned the sensitivity of the IAPS rating protocol for the assessment of PTSD-related emotional numbing and recommendations have been made to increase the sensitivity of the tool increasing the number of pictures and incorporating trauma-related images [47]. Finally, this study focused on picture-based stimuli. Using more complex stimuli, such as videos or virtual reality tasks, to explore attention allocation could elicit stronger or different reactions. Future investigations could employ novel technologies to evaluate attentional patterns in more complex threatening conditions. Despite the above limitations, these findings add to the literature within the trauma field, which implicates the role of impaired emotional processing in people with PTSD.
The results of exposure to visual stimuli of different emotional content (positive, negative, and neutral) have brought evidence supporting the anticipated hypotheses. The arousal dimension scores were on average higher among the Probable PTSD group rather than the control group. In particular, the statistical analyses carried out according to the pictures’ emotional dimension of valence (unpleasantness/pleasantness), arousal (calm/agitated), and dominance (domination/non-domination), showed how participants with the probable PTSD perceived themselves more agitated and with less control in front of any type of image compared to without PTSD individuals. Valence scores decrease more for positive and neutral images, and unpleasantness judgments are emphasized more for negative images. The dimensions of valence, dominance, and arousal were also significantly correlated with each other. The level of pleasantness was not significantly associated with the arousal level among both participants groups for the positive pictures. In negative pictures, both Probable PTSD and Trauma-exposed participants’ levels of pleasantness were inversely associated with arousal and dominance levels. It can be supposed that for the positive pictures, the Trauma-exposed subjects were more relaxed the more pleasant the image was, whereas for the negative images both groups of participants were more agitated and dominated the more unpleasant the image was.
The results partially confirmed evidence according to which PTSD causes a constant state of maladaptive hyper arousal and difficulties in regulating emotions facing environmental stimuli, regardless of whether they are positive, negative, or neutral, and disagree with those who argue that such difficulties arise only with negative stimuli [47]. It can be assumed that following exposure to several traumas in refugees/asylum seekers the PTSD onset establishes a generalization of the troubles in emotions regulation even towards stimuli that do not directly recall the traumatic events. Therefore, individuals with probable PTSD manage negative stimuli as more threatening than they really are and feel themselves in an exaggerated state of agitation that does not allow them to give due weight to what they see. Hence, the negative valence turned out to be as a strong reminder that might have triggered memories related to the individual traumatic experience and induced flashbacks. Moreover, positive stimuli are considered less pleasant, and this prevents them from fully enjoying them. Therefore, people who meet PTSD criteria exhibit great difficulties in regulating emotions. This finding is consistent with a six-factor model [71,72] in which the single symptom cluster of “negative alterations in mood and cognitions” from DSM-5 was additionally collapsed into a negative affect symptom cluster (negative affect potentiation) and an anhedonia symptom cluster (positive affect deterioration). Crucially, the Research Domain Criteria (RDoC) project started by the National Institutes of Mental Health (NIMH) indicated that negative valence and positive valence are two distinctive areas in the psychopathology [73,74].Authors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.
6. Conclusions
The probable PTSD group reported evidence of emotional processing dysfunction compared to the group of individuals who did not develop traumatic symptoms. Within the probable PTSD group there was significant evidence that the additional impact of trauma increased emotional processing dysfunction. Hence, our findings provide insight into the challenges faced by this population and shows that one important factor contributing to mental health difficulties in traumatized refugees may be altered emotion processing, such as (1) heightened emotional responses to past or current events (emotional reactivity) and (2) limited ability to manage heightened negative emotions and decreased positive emotions (emotion regulation). It is essential to recognize how individuals with PTSD process both negative and positive emotional information and how they regulate their emotions. Research has shown that PTSD in refugees and asylum seekers exposed to multiple traumas in their lifetime may promote different emotion and regulation processes compared to those who have been exposed to events of similar magnitude but who have not developed the disorder. Those who develop PTSD evaluate positive images as less pleasant and negative images as more unpleasant, are on average increasingly activated and have less self-control in the face of visual stimuli of any value. The affective and emotional states experienced by humans are complex and nuanced, and this property ultimately renders them problematic to investigate in a laboratory context in a way that delivers generalizable information concerning the mechanisms underlying their emergence and maintenance. Although these findings are promising in highlighting deficits in PTSD that relate to diminished positive affect symptoms, more work is needed to develop this field of study into one capable of producing clinically relevant strategies that will transform and improve trauma mental health care [32]. Therefore, this study also provides suggestions for future research indicating that interventional strategies should focus on desensitizing refugees with current or lifetime PTSD to traumatic emotional memories. Particular attention should also be given to improve their emotion regulation capabilities by managing symptoms of reduced positive affect/anhedonia.
Author Contributions
Conceived, designed, and performed the experiment; analysis, interpretation of data, and drafting/revising of the manuscript: OP. Analyzed the data: MR. Supervision of statistical analysis: MM. All authors read and approved the final version of the manuscript
Funding
This research received no external funding.
Institutional Review Board Statement
The study involving human participants were reviewed and approved by the Ethic committee of Area Vasta Emilia Nord - AVEN (Ref. 1156/2020/OSS/UNIPR) and were carried out in accordance with the Declaration of Helsinki. (Italy). Written informed consent was obtained from all individual participants included in the study.
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The dataset generated during and/or analyzed during the current study is available from the author on reasonable request.
Acknowledgments
Author of this study would like to acknowledge the entire staff of the Dimora D’Abramo (RE, Italy) for their cooperation in the project. Moreover, she expresses appreciation to the master student Fabiana Vernazza for her collaboration in the data collection and study participants for their cooperation.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-III). Washington, DC: APA Publishing, 1980.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM V), Fifth Edition. Washington, DC: Author, 2013 https://psychiatryonline.org/doi/book/10.1176/appi.books.9780890425596.
- Bassir Nia, A., Bender, R., Harpaz-Rotem, I. Endocannabinoid system alterations in Posttraumatic Stress Disorder: A review of developmental and accumulative effects of trauma. Chronic Stress, 2019, 3, 2470547019864096. [CrossRef]
- Bryant, R.A. et al. Acute and chronic Posttraumatic Stress Symptoms in the emergence of Post traumatic Stress Disorder: A network analysis. JAMA Psychiatry, 2017, 74(2), 135-142. [CrossRef]
- Enman, N.M., Arthur, K., Ward, S.J., Perrine, S.A., Unterwald, E.M. Anhedonia, reduced cocaine reward, and dopamine dysfunction in a rat model of posttraumatic stress disorder. Biol Psychiatry, 2015, 78, 871-879. [CrossRef]
- Miethe, S.; et al. Posttraumatic stress symptoms and its association with rumination, thought suppression and experiential avoidance: A systematic review and meta-analysis. J Psychopathol Behav Assess, 2023, 45(2), 480-495. [CrossRef]
- Shepherd, L., Wild, J. Emotion regulation, physiological arousal, and PTSD symptoms in trauma-exposed individuals. J Behav Ther Exp Psychiatry, 2014, 45(3), 360-367. [CrossRef]
- Spiller, T.R. et al. Emotional reactivity, emotion regulation capacity, and posttraumatic stress disorder in traumatized refugees: An experimental investigation. J Trauma Stress, 2019, 32(1), 32-41. [CrossRef]
- Wisco, B.E. et al. Effects of trauma-focused rumination among trauma-exposed individuals with and without posttraumatic stress disorder: An experiment. J Trauma Stress, 2023, 36, 285-298. [CrossRef]
- Freitag S, Braehler E, Schmidt S, Glaesmer H. The impact of forced displacement in World War II on mental health disorders and health-related quality of life in late life - a German population-based study. Int Psychogeriatr, 2013, 25(2), 310-319. [CrossRef]
- Li, S.S., Liddell, B.J., Nickerson, A. The relationship between post-migration stress and psychological disorders in refugees and asylum seekers. Curr Psychiatry Rep, 2016, 18(9):82. [CrossRef]
- Sandahl, H., Vindbjerg, E., Carlsson, J. Treatment of sleep disturbances in refugees suffering from post-traumatic stress disorder. Transcult Psychiatry, 2017, 54, 806-23. [CrossRef]
- Bogic, M. et al. Factors associated with mental disorders in long-settled war refugees: Refugees from the former Yugoslavia in Germany, Italy, and the UK. Br J Psychiatry, 2012, 200, 216-223. [CrossRef]
- Jobst, S., Windeisen, M., Wuensch, A., Meng, M., Kugler, C. Supporting migrants and refugees with posttraumatic stress disorder: Development, pilot implementation, and pilot evaluation of a continuing interprofessional education for healthcare providers. BMC Med Educ, 2020, 20(1):311. [CrossRef]
- Koch, T., Liedl, A., Ehring, T. Emotion regulation as a transdiagnostic factor in Afghan refugees. Psych Trauma: Theory, Res, Pract, Policy, 2020, 12(3), 235. [CrossRef]
- Porter, M., Haslam, N. Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons: A meta-analysis. JAMA, 2005, 294(5), 602-612. [CrossRef]
- Mollica, R.F., McInnes, K., Poole, C., Tor, S. Dose-effect relationships of trauma to symptoms of depression and posttraumatic stress disorder among Cambodian survivors of mass violence. Br J Psychiatry, 1998, 173, 482-488. [CrossRef]
- Morina, N., Akhtar, A., Barth, J., Schnyder, U. Psychiatric disorders in refugees and internally displaced persons after forced displacement: A systematic review. Front Psychiatry, 2018, 9, 433. [CrossRef]
- Nickerson, A. et al. Impact of cognitive reappraisal on negative affect, heart rate, and intrusive memories in traumatized refugees. Clin Psychol Sci, 2017, 5, 497-512. [CrossRef]
- Steel, Z. et al. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: A systematic review and meta-analysis. JAMA, 2009, 302(5), 537-49. [CrossRef]
- Carta, M.G. et al. A follow-up on psychiatric symptoms and Post-Traumatic Stress Disorders in Tuareg refugees in Burkina Faso. Front Psychiatry, 2018, 9, 127. [CrossRef]
- Djelantik, A.A.A.M.J. et al. Post-migration stressors and their association with symptom reduction and non-completion during treatment for traumatic grief in refugees. Front Psychiatry, 2020, 11, 407. [CrossRef]
- Ehring, T., Quack, D. Emotion regulation difficulties in trauma survivors: The role of trauma type and PTSD symptom severity. Beh Ther, 2010, 41, 587-98. [CrossRef]
- Liddell, B.J. et al. Neural correlates of posttraumatic stress disorder symptoms, trauma exposure, and postmigration stress in response to fear faces in resettled refugees. Clin Psychol Sci, 2019, 27, 811-25. [CrossRef]
- Roberts, B., Ocaka, K.F., Browne, J., Oyok, T., Sondorp, E. Factors associated with post-traumatic stress disorder and depression amongst internally displaced persons in northern Uganda. BMC Psychiatry, 2008, 8(1), 38. [CrossRef]
- World Health Organization. Comprehensive mental health action plan 2013-2030. Geneva: World Health Organisation, 2021. https://www.who.int/publications/i/item/9789240031029.
- Ben-Zion, Z. et al. Neural responsivity to reward versus punishment shortly after trauma predicts long-term development of Posttraumatic Stress Symptoms. Biol Psychiatry: Cogn Neurosci Neuroimag, 2022, 7(2), 150-161. [CrossRef]
- McCurry, K.L., Fruehm B.C., Chiu, P.H., King-Casas B. Opponent effects of hyperarousal and re-experiencing on affective habituation in Posttraumatic Stress Disorder. Biol Psychiatry Glob Open Sci, 2020, 5(2), 203-212. [CrossRef]
- Kujawa, A., Klein, D.N., Pegg, S., Weinberg, A. Developmental trajectories to reduced activation of positive valence systems: A review of biological and environmental contributions. Develop Cogn Neurosci, 2020, 43, 100791. [CrossRef]
- White, S.F., Costanzo, M.E., Blair, J.R., Roy, M.J. (2014). PTSD symptom severity is associated with increased recruitment of top-down attentional control in a trauma-exposed sample. Neuroimage: Clin, 2014, 7, 19-27. [CrossRef]
- Chu, D.A., Bryant, R.A., Gatt, J.M., Harris, A.W.F. Failure to differentiate between threat-related and positive emotion cues in healthy adults with childhood interpersonal or adult trauma. J Psychiatric Res, 2016, 78, 31-41. [CrossRef]
- Fonzo, G.A. Diminished positive affect and traumatic stress: A biobehavioral review and commentary on trauma affective neuroscience. Neurob Stress, 2018, 9, 214-230. [CrossRef]
- Fischer, A.G., Ullsperger, M. An update on the role of serotonin and its interplay with dopamine for reward. Front Human Neurosci, 2017, 11, 484. https://www.frontiersin.org/articles/10.3389/fnhum.2017.00484/full.
- Bruce, S.E. et al. Altered emotional interference processing in the amygdala and insula in women with Post-Traumatic Stress Disorder. Neuroimage Clin, 2012, 2, 43-49. [CrossRef]
- Park, J. et al. The association between alexithymia and posttraumatic stress symptoms following multiple exposures to traumatic events in North Korean refugees. J Psychosom Res, 2015, 78(1), 77-81. [CrossRef]
- Suarez-Jimenez, B. et al. Attention allocation to negatively-valenced stimuli in PTSD is associated with reward-related neural pathways. Psychol Med, 2023, 53, 4666-4674. [CrossRef]
- Kumar, P. et al. Differential effects of acute stress on anticipatory and consummatory phases of reward processing. Neurosci, 2014, 266, 1-12. [CrossRef]
- María-Ríos, C.E., Morrow, J.D. Mechanisms of shared vulnerability to Post-traumatic Stress Disorder and Substance Use Disorders. Front Behav Neurosci, 2020, 14, 6. [CrossRef]
- Seidemann, R., Duek, O., Jia, R., Levy, I., Harpaz-Rotem, I. The reward system and Post-Traumatic Stress Disorder: Does trauma affect the way we interact with positive stimuli? Chronic Stress, 2021, 5. [CrossRef]
- Ashley, V., Swick, D. Angry and fearful face conflict effects in Post-traumatic Stress Disorder. Front Psychol, 2019, 10, 136. [CrossRef]
- Catani, C., Adenauer, H., Keil, J., Aichinger, H., Neuner, F. Pattern of cortical activation during processing of aversive stimuli in traumatized survivors of war and torture. Eur Arch Psychiatry Clin Neurosci, 2009, 259(6), 340-351. [CrossRef]
- Dunkley, B.T., Wong, S.M., Jetly, R., Wong, J.K., Taylor, M.J. Post-traumatic stress disorder and chronic hyperconnectivity in emotional processing. Neuroimage: Clin, 2018, 20, 197-204. [CrossRef]
- Fani, N. et al. Attentional control abnormalities in posttraumatic stress disorder: Functional, behavioral, and structural correlates. J Affect Disord, 2019, 253, 343-351. [CrossRef]
- Zukerman, G., Pinhas, M., Ben-Itzhak, E., Fostick, L. Reduced electrophysiological habituation to novelty after trauma reflects heightened salience network detection. Neuropsychol, 2019, 134, 107226. [CrossRef]
- Nawijn, L. et al. Reward functioning in PTSD: A systematic review exploring the mechanisms underlying anhedonia. Neurosci Biobehav Rev, 2005, 51, 189-204. [CrossRef]
- Williams, C.L., Milanak, M.E., Judah, M.R., Berenbaum, H. (2018). The association between PTSD and facial affect recognition. Psychiatry Res, 2018, 265, 298-302. [CrossRef]
- Wolf, E.J., Miller, M.W., McKinney, A.E. Emotional processing in PTSD: Heightened negative emotionality to unpleasant photographic stimuli. J Nerv Ment Dis, 2009, 197(6), 419-426. [CrossRef]
- Feng, C.; et al. The time course of the influence of valence and arousal on the implicit processing of affective pictures. PLoS ONE, 2012, 7(1), e29668. [CrossRef]
- Berle, D. et al. Personal wellbeing in posttraumatic stress disorder (PTSD): Association with PTSD symptoms during and following treatment. BMC Psychol, 2018, 6(1), 7. [CrossRef]
- Doolan, E.L., Bryant, R.A., Liddell, B.J., Nickerson, A. The conceptualization of emotion regulation difficulties, and its association with posttraumatic stress symptoms in traumatized refugees. J Anxiety Disord, 2017, 50, 7-14. [CrossRef]
- Mollica, R., Massagli, L., Silove, D. Measuring trauma, measuring torture. Cambridge, MA: Harvard University, 2004.
- Kronick, R. Mental health of refugees and asylum seekers: Assessment and intervention. Can J Psychiatry, 2018, 63(5):290-296. [CrossRef]
- Madoro, D. et al. Post-Traumatic Stress Disorder and associated factors among internally displaced people in South Ethiopia: A cross-sectional study. Neuropsychiatr Dis Treat, 2020, 16, 2317-2326. [CrossRef]
- Shou, H. et al. Cognitive behavioral therapy increases amygdala connectivity with the cognitive control network in both MDD and PTSD. Neuroimage: Clinicl, 2017, 14, 464-470. [CrossRef]
- Watkins, L.E., Sprang, K.R., Rothbaum, B.O. Treating PTSD: A review of evidence-based psychotherapy interventions. Front Behav Neurosci, 2018, 12, 258. [CrossRef]
- Hayes, J., Van Elzakker, M., Shin, L. Emotion and cognition interactions in PTSD: A review of neurocognitive and neuroimaging studies. Front Integr Neurosci, 2012, 6, 89. [CrossRef]
- Lee, K.H. et al. Neural correlates of emotional reactivity and regulation in traumatized North Korean refugees. Transl Psychiatry, 2021, 11, 452. [CrossRef]
- Olson, E.A., Kaiser, R.H., Pizzagalli, D.A., Rauch, S.L., Rosso, I.M. Anhedonia in trauma-exposed individuals: Functional connectivity and decision-making correlates. Biol Psychiatry Glob Open Sci, 2017. https://www.sciencedirect.com/science/article/pii/S2451902217302008.
- Postel, C. et al. Variations in response to trauma and hippocampal subfield changes. Neurobiol Stress, 2021, 15, 100346. [CrossRef]
- Bradley, M.M., Lang, P.J. Measuring emotion: The Self-Assessment Manikin and the semantic differential, J Behav Ther Exp Psychiatry, 1994, 25(1), 49-59. [CrossRef]
- Blekić, W.; et al. Affective ratings of pictures related to interpersonal situations. Front Psychol, 2021, 12, 627849. [CrossRef]
- Lang, P.J., Bradley, M.M., Cuthbert, B.N. International affective picture system (IAPS): Affective ratings of pictures and instruction manual (Tech. Rep. A-8). University of Florida, 2008.
- Berthold, S.M. et al. The HTQ-5: Revision of the Harvard Trauma Questionnaire for measuring torture, trauma, and DSM-5 PTSD symptoms in refugee populations. Eur J Public Health, 2019, 29(3), 468-474. [CrossRef]
- Silove, D. et al. Screening for depression and PTSD in a Cambodian population unaffected by war: Comparing the Hopkins Symptom Checklist and Harvard Trauma Questionnaire with the structured clinical interview. J Nervous Mental Dis, 2007, 195(2), 152-157. [CrossRef]
- Sigvardsdotter, E., Malm, A., Tinghög, P., Vaez, M., Saboonchi, F. Refugee trauma measurement: A review of existing checklists. Public Health Rev, 2016, 37, 10. [CrossRef]
- Vindbjerg, E., Carlsson, J., Mortensen, E.L., Elklit, A., Makransky, G. The latent structure of post-traumatic stress disorder among Arabic-speaking refugees receiving psychiatric treatment in Denmark. BMC Psychiatry, 2016, 16, 1-10. [CrossRef]
- de Fouchier, C. et al. Validation of a French adaptation of the Harvard Trauma Questionnaire among torture survivors from sub-Saharan African countries. Eur J Psychotraumatol, 2012, 3, 10. [CrossRef]
- Pino, O.; et al. Post-traumatic outcomes among survivors of the earthquake in central Italy of August 24, 2016. A study on PTSD risk and vulnerability factors. Psychiatric Quart, 2021, 92, 1489-1511 (2021). [CrossRef]
- Lang, P.J., Bradley, M.M., Cuthbert, B.N. International Affective Picture System (IAPS): Instruction manual and affective ratings. Technical report A-5. University of Florida, 2001.
- Abu Suhaiban, H., Grasser, L. R., Javanbakht, A. Mental health of refugees and torture survivors: A critical review of prevalence, predictors, and integrated care. Int J Environ Res Public Health, 2019, 16(13), 2309. [CrossRef]
- Duan, H., Wang, L., Wu, J. Psychophysiological correlates between emotional response inhibition and posttraumatic stress symptom clusters. Scien Rep, 2018, 8, 16876. [CrossRef]
- Liu, P. et al. The underlying dimensions of DSM-5 posttraumatic stress disorder symptoms in an epidemiological sample of Chinese earthquake survivors. J Mood Disord, 2014, 28(4), 345-351. [CrossRef]
- Cuthbert, B.N., Kozak, M.J. Constructing constructs for psychopathology: The NIMH research domain criteria. J Abnor Psychol, 2013, 122(4), 928-937. [CrossRef]
- Förstner, B.R. et al. The associations of Positive and Negative Valence Systems, cognitive systems, and social processes on disease severity in anxiety and depressive disorders. Front Psychiatry, 2023, 16 (14), 1161097. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



