
Submitted:
28 August 2024
Posted:
30 August 2024
You are already at the latest version
Abstract
Maternal obesity has been found to be impaired oxidative status in placenta and newborn which can lead to adverse pregnancy outcomes and long-term adverse influence on metabolic programming in the offspring. This study aimed to investigate the role of maternal obesity on maternal and umbilical cord plasma oxidative status and placental oxidative adaptation. Maternal obesity (n=20) defined as pre-pregnancy BMI ≥ 25 kg/m2 and maternal lean (n=20) defined as pre-pregnancy BMI < 25 kg/m2 were recruited into this study. Both groups were matched by gestational age at delivery. Maternal blood, umbilical cord blood and placental tissue were collected to assess nutritional content (cholesterol, triglyceride, and protein), oxidative stress marker (MDA and protein carbonyl) and antioxidant activity (SOD and catalase). Placenta protein expression (SOD2, catalase, UCP2 and Nrf2) was evaluated by western blot analysis. Catalase activity in maternal plasma significantly increased in maternal obesity group (p = 0.0200) with an increased trend in MDA and protein carbonyl levels. Umbilical cord plasma triglyceride, protein carbonyl and catalase activity significantly increased in maternal obesity compared with that in maternal lean (p = 0.0462, 0.0485, and 0.0348, respectively). Although placenta protein expression analysis exhibited significant decreased SOD2 (p = 0.0169) and catalase (p = 0.0067), accompanied by Nrf2 downregulation (p = 0.0453). An increased mitochondrial antioxidant UCP2 expressions was observed (p = 0.0143). Hence, our study provided evidence that maternal obesity is associated with placental and fetal oxidative stress with the parallel increased placental antioxidant UCP2 expression.
Keywords:
maternal obesity
; placenta
; oxidative stress
; antioxidants
1. Introduction
Obesity is one of the greatest public health problems of the 21st century worldwide with a higher prevalence in females than males [1]. This condition is of particular concern among women at reproductive age because of its impact in pregnancy, which affects health of at least two generations [2]. Maternal obesity is a stress condition that can eventually lead to inappropriate feto-placental development and function. Consequently, it may have a long-term adverse influence on metabolic programming in the offspring [3,4,5].
During pregnancy, there are metabolic changes in pregnant women in order to support the availability of nutrients to the developing placenta and fetus [6]. Maternal obesity has been found to be associated with metabolic dysregulation which initiates impropriate metabolic and oxidative status in both mother and their fetus [7,8]. The placenta is the organ responsible for interaction between mother and fetus which regulates many aspects of the intrauterine environment to the developing fetus including oxygen and nutrient delivery, the removal of waste products, and neutralization of reactive oxygen species (ROS) [9]. Thus, oxidative adaptation of the placenta may alter the impact of maternal obesity on fetal oxidative stress [10,11].
Pregnancy is considered as a state of maternal oxidative stress that can impact the placenta. However, oxidative stress in the placenta has been found to be heightened in obese pregnant women [10,12]. Our previous study regarding placental adaptation to maternal malnutrition in a rat model revealed a placental oxidative disbalance [13]. There are a range of enzymes that play a role in placental antioxidant defenses including superoxide dismutase (SOD), catalase, and glutathione peroxidase (GPx) [14]. In addition, due to rich of mitochondria in placenta tissue, mitochondrial antioxidant uncoupling protein 2 (UCP2) have been proposed to be a key moderator of oxidative stress defense in the placenta [14,15]. Importantly, expression of UCP2 has been found to be responsive to altered maternal nutrition [16]. However, there are conflicting results regarding antioxidant response of the placenta in obese pregnancy, some studies reported an increased placental antioxidant: SOD, catalase and GSH, with reduction of maternal plasma antioxidant activity [10,17]. Other studies demonstrated diminished placental total antioxidant capacity, SOD, and catalase activity, along with exacerbated oxidative and nitrosative stress markers [18,19]. All these seem to be demonstrated that maternal nutrition may plays an important role in placental oxidative balance. An increased ROS production in maternal obesity might predisposes the fetus to a state of oxidative stress.
Thus, the aim of this study was to investigate the effect of maternal obesity during pregnancy on maternal and umbilical cord plasma oxidative status and placental oxidative adaptation. We hypothesized that impairment of placental antioxidant defenses might contribute to neonatal oxidative stress under inappropriate maternal condition.
2. Results
The demographics and pregnancy outcome data are showed in Table 1. There was no significant difference in maternal age and gestation age at delivery between maternal lean and maternal obesity groups (p > 0.05). In maternal obesity group, pre-pregnancy weight, pre-pregnancy BMI and weight at delivery significantly higher than those with normal weight (p < 0.0001). Percentage of male neonatal gender of obese women was not significant different compared to those with normal weight (p > 0.05). Neonatal birth weight and length were not significant different between the two groups (p > 0.05). Interestingly, placental weight of maternal obesity was significantly higher compared to maternal lean (p = 0.0224) while feto-placental ratio was significantly lower in maternal obesity group (p = 0.0374).
To determine impact of maternal obesity on nutritional content in maternal and neonatal sides, we assess maternal and umbilical cord plasma of total cholesterol, triglyceride and protein content. No significant differences in maternal plasma level of cholesterol, triglyceride and protein content in maternal obesity when comparing with maternal lean control (cholesterol, p = 0.3078; triglyceride, p = 0.8172; protein content, p = 0.4588; Figure 1a, 1c, and 1e).
However, a significant higher level of umbilical cord plasma triglyceride was detected in maternal obesity (p = 0.0462; Figure 1d) compared with that in maternal lean, while no significantly different were observed in umbilical cord plasma cholesterol and protein content (p = 0.9753 and p = 0.3900, respectively; Figure 1b and 1f).
To determine whether maternal plasma of oxidative stress marker could be altered by maternal obesity, we examined the level of MDA and protein carbonyl. Maternal plasma MDA level and protein carbonyl trend to be increased in obesity compared to lean groups (p = 0.1453 and p = 0.1744, respectively; Figure 2a-2b).
Maternal plasma catalase activity significantly decreased in maternal obesity compared with that in maternal lean (p = 0.0200; Figure 3a) without significant alteration in SOD activity (p = 0.9520; Figure 3b).
Oxidative stress marker in umbilical cord plasma is presented in Figure 4. Protein carbonyl significantly higher in umbilical cord plasma of maternal obesity compared to maternal lean groups (p = 0.0485; Figure 4b). Umbilical cord plasma MDA level tended to be higher in maternal obesity compared to lean control (p = 0.2712; Figure 4a).
Regarding antioxidant activity of neonatal side, we evaluate catalase and SOD activity in umbilical cord plasma. Interestingly, umbilical cord plasma from maternal obesity had significantly higher catalase activity (p = 0.0348; Figure 5a) along with a trend of higher SOD activity compared to maternal lean (p = 0.1739; Figure 5b).
Regarding oxidative marker in placental tissue, MDA level was not significantly difference in maternal obesity compared with that in maternal lean control (p = 0.3415; Figure 6a). However, protein carbonyl in placenta significantly elevated in maternal obesity group compared to maternal lean group (p = 0.0300; Figure 6b).
The relative placental antioxidant protein expressions are showed in Figure 7a – 7d. Catalase and SOD2 expressions in placental tissue were significantly lower in maternal obesity compared to the maternal lean (p-value = 0.0067, and 0.0169, respectively; Figure 7a-b). Additionally, signaling pathway Nrf2 expression was significantly decreased in maternal obesity (p-value = 0.0453; Figure 7c). However, the mitochondrial antioxidant UCP2 was significantly higher in maternal obesity compared to the maternal lean (p-value = 0.0143; Figure 7d).
3. Discussion
In the present study, maternal obesity maintained maternal plasma of oxidative bal-ance as evidenced by an increased trend in MDA and protein carbonyl level with de-creased plasma catalase activity. Interestingly, this study observed placental oxidative adaptation indicated by decreased placental catalase and SOD2 along with enhanced UCP2 expressions. This placental response was associated with downregulation of Nrf2 signaling pathway. In addition, there were a significantly increased in umbilical cord protein carbonyl and antioxidant (catalase and SOD) activity implying an oxidative imbalance in newborn.
Obesity is a result of positive energy balance which characterized by excessive fat accumulation and chronic metabolic inflammation. Obesity during pregnancy has been found to be associated with dysregulation of lipid metabolism which might be drives the fetus to exposed with adverse intra-uterine environment [20,21]. This inappropriate condition is not only associated with an increased risk of obstetric complications and adverse neonatal health outcomes at birth, but it also affects fetal metabolic program-ming, potentially influencing long-term health [22]. Previous studies have demonstrated that nutritional and oxidative status during fetal development seems to impact metabolism occurring in adult life through different mechanisms [12,23,24]. Better under-standing the nutritional and oxidative statuses in maternal and feto-placental units may offer strategies to mitigate adverse health outcomes for both mothers and their off-spring.
Maternal obesity has been found to be associated with an alteration in plasma lipids, glucose, and protein. This study was not observed any alterations in total choles-terol, triglyceride, and protein content in maternal plasma of obesity group. However, umbilical cord plasma from maternal obesity group has higher triglyceride level com-pared to the lean control. Similarly, there have been reports of an enhanced triglyceride level in the fetus and the placenta of mother complicated with metabolic disorder [8,17,25,26]. Moreover, there was evidence of dysregulation of placental fatty acid transporter and lipase enzyme in mother complicated with metabolic disorders which directly influence lipid transfers across the placenta to the fetus [25,26,27]. We hypothesized that maternal obesity might induce excessive free fatty acids to be transported to the fetus, resulting in increased fat accumulation in the form of triglycerides. Consequently, fetus with enhanced fat accumulation is more likely to grow up to be obese in childhood and adulthood [28,29]. Thus, our results may be attributed to the fact that, even when maternal nutrient levels are maintained within normal ranges, maternal obesity can impair fetal lipid metabolism, potentially increasing the risk of developing metabolic disorders later in life.
Additionally, maternal overnutrition has been found to be correlated with altered oxidative status in both mothers, placenta and their newborn [30,31]. During normal pregnancy, an increased ROS production is temporally correlated with an enhancement of antioxidant enzymes [32]. However, alterations in oxidative status in maternal obesity are still controversial [12,17,33]. To address this, we evaluated oxidative status in ma-ternal plasma through the evaluation of lipoperoxidation products, MDA and protein carbonyl along with catalase and SOD activity. The result showed that maternal obesity tended to have higher plasma level of MDA and protein carbonyl, which is accompanied by reduced catalase activity. Catalase is a crucial antioxidant responsible for reducing free radicals and converting final products of lipid peroxidation into inactive forms [34]. Lower catalase activity observed in maternal obesity could result from impaired antioxidant response or consuming antioxidants during an exposure of high ROS condition [18]. This impairment may be associated with diminish Nrf-2 signaling response or overactivation of xanthine oxidase which has been previously observed in maternal metabolic disorders [35,36]. Our result is in line with previous studies which presented that pregnant woman with obesity showed higher level of plasma MDA and other oxi-dative stress markers along with alteration in plasma antioxidants [12,18]. Hence, our data suggest that maternal obesity even in the absence of obstetric complications is as-sociated with oxidative imbalance.
There is some evidence that maternal nutrition influences oxidative status in the placenta. An appropriate balance between pro-oxidants and antioxidants is importance for maintaining placental homeostatic capacity as an adaptive response [10,13]. In physiological condition, radical molecules participate in cell signaling to regulate normal development and function of the placenta including angiogenesis, nutrient transport, hormone production, detoxification, and oxidative control. Conversely, excessive pro-duction of radicals disrupts placental function [37]. Therefore, we evaluate the role of maternal obesity on placental oxidative alteration. As expected, our study provided evidence that placental oxidative status was altered in maternal obesity. A significant in-creased placental protein carbonyl with compromising antioxidant enzyme expression was observed as evidence by decreased SOD2 and catalase along with it downstream signaling pathway Nrf2 expressions. In parallel, there was an enhanced expression of the mitochondrial antioxidant UCP2. Enzymatic antioxidant SOD2 and catalase are known to be general antioxidants found in mitochondria and peroxisomes, respectively [18]. Its expression is regulated by Nrf2 which is a key transcriptional regulator of the cellular response to oxidative stress [38]. A decreased in placental SOD2 and catalase could reflect an inactivation antioxidant system in placenta of obese mother [10]. Additionally, a significant reduction of Nrf2 protein expression observed in this study clearly explained the underlying mechanism of impaired placental antioxidant defense. Several studies were consistent with our results, demonstrating the high oxidative stress markers along with downregulate SOD, catalase, and GPx in placenta of maternal metabolic disorder [10,18,19]. In addition, UCP2 is considered as major mitochondrial antioxidant in the placenta [18]. As highly mitochondrial activity in the placenta and decreased in SOD and catalase expression, upregulation of UCP2 may be responsible for compensatory response to pro-oxidant state induced by maternal metabolic abnormality. Our finding highlights the role of UCP2 as a key regulator of oxidative balance in the placenta which was reported by previous study [11]. Unfortunately, even though overproduction of mitochondrial antioxidant UCP2 might be attributed to placental adaptation to an exacerbated ROS production, but this event accompanied by a subsequent increased placental protein carbonyl. Thus, it seems to indicate that antioxidant response in the placenta of maternal obesity might be insufficient to retrieve oxidative balance, which would eventually lead to placental dysfunction. However, further study of placental enzymatic activity could provide additive information.
Besides maternal and placental sides, we continue to demonstrate alteration in oxi-dative status of the newborn. We hypothesized that placental dysfunction induced by maternal obesity may be unable to protect the fetus to adverse oxidative effect. As expected, a significant increased protein carbonyl and a non-significant trend for in-creased MDA levels in umbilical cord plasma was observed in newborn born to maternal obesity compared to those born to normal weight mother. Protein carbonylation is a process of irreversible protein oxidative modifications which can be promoted by reactive oxygen species. Thus, protein carbonyl level is considered as general marker of oxidative stress-induced protein damage [39]. Lipids are also important targets for radical reactions. A trended increased of lipid peroxidation product in umbilical cord plasma could support the oxidative stress in the neonatal side. Fatty acid transferred via the placenta to the fetus and increased fat accumulation in adipose tissue might provide source of lipid peroxidation substrate for developing fetus which accelerates oxidative stress [30]. Our results are in line with reports in other studies, newborn of maternal obesity showed higher level of oxidative stress markers [31,40]. Regarding antioxidant response in neonatal side, our study revealed a significantly increased umbilical cord plasma catalase activity without any changes in SOD activity. Previous study reported that catalase plays a crucial role in response to oxidative stress under high H2O2 conditions whereas SOD shows an unaltered by this condition [41,42]. This possibly leading to no alteration in SOD activity. Thus, it seems possible that an increased catalase activity observed in newborn born to maternal obesity indicates an active antioxidant defense system in response to neutralize or mitigate the deleterious effect of ROS. Protein carbonyl could be considered as marker of neonatal oxidative stress. An enhancement of protein oxidative product along with an increased antioxidant enzymes activity indicating maternal obesity compromised neonatal oxidative status. Consequence, it may be a contributing factor of fetal programming, which lead to an increased susceptibility to oxidative stress related diseases in postnatal life [29,43].
Regarding neonatal outcome, there was no significant changes in neonatal birth weight and length. However, growth of baby was not relative to growth of placenta as indicated by low feto-placental ratio and high placental weight. The high weight of placenta has been found to be associated with increased capillary surface density of cot-yledon which leading to an increased available surface area for placental exchange and transport function [44]. However, the enlarged placenta needs more nutrients which may lead to incommensurate nutrients for the developing fetus [45]. These finding point out to impairs placental efficacy during metabolic-oxidative imbalance as previously described [46].
Hence, our study provided evidence that maternal obesity is associated with pla-cental and fetal oxidative stress with the parallel increased placental antioxidant expres-sion. The neonatal oxidative stress observed in obese pregnancy may be a contributing factor of fetal programming, which lead to an increased susceptibility to oxidative stress related diseases later in life. An appropriate nutritional management before and throughout pregnancy likely to be key to optimal pregnancy outcome.
4. Materials and Methods
4.1. Study Subjects
This study was approved by the the Khon Kaen University Ethics Committee for Human Research based on the Declaration of Helsinki and the ICH Good Clinical Practice Guidelines with study identification code HE651023. All participants were previously informed and gave their written consent to be included as study volunteers.
Forty-pregnant women attending the labor department for delivery at Srinagarind Hospital, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand were recruited into this cross-sectional study. Study groups are classified according to recommended body-mass index (BMI) cut-off points for determining overweight and obesity in Asian populations [47] which consisted of the maternal lean (pre-pregnancy BMI < 25 kg/m2) (n=20) and maternal obesity (pre-pregnancy BMI ≥ 25 kg/m2) (n=20). Both groups were matched by gestational age at delivery. All volunteer showed no history of chronic diseases including chronic hypertension, diabetes mellitus, kidney, liver, immune and respiratory diseases.
4.2. Characteristics of the Mothers and Their Offspring
The anthropometric data and pregnancy outcome including maternal age and gestational age at delivery, pre-pregnancy weight, pre-pregnancy BMI, weight at delivery, neonatal gender, neonatal birth weight and length, and placental weight were recorded from questionnaires by personal interview and medical records.
4.3. Maternal Plasma Collection
A maternal venous blood sample (10 ml) was obtained before the time of delivery from the arm veins of the mothers using ethylenediaminetetraacetic acid (EDTA) tubes. The blood was centrifuged with 3,500 rpm for 15 min and plasma was separated and stored at -80 °C until analysis. Plasma was used to measure nutrition contents (total cholesterol, triglyceride and protein), oxidative stress markers (MDA and protein carbonyl), antioxidants (SOD and catalase) activity.
4.4. Umbilical Cord Plasma Collection
Immediately after the birth of the newborn and separation of newborn and umbilical cord, the umbilical cord was clamped, and another clamp was placed 8-10 inches away from the first. The blood sample (10 ml) was collected promptly from the section between the clamps in a tube containing EDTA. The blood was centrifuged with 3,500 rpm for 15 min and plasma was separated and stored at -80 °C until analysis. Umbilical cord plasma was used to measure nutrition contents (total cholesterol, triglyceride and protein), oxidative stress markers (MDA and protein carbonyl), antioxidants (SOD and catalase) activity.
4.5. Placental Sample Collection
Placental samples were randomly harvested immediately following delivery, within 10 min of delivery. Small fragments of villous (~100 mg) were isolated from the central area of the placenta, then were placed on ice and washed with phosphate buffer solution (PBS) to eliminate the blood. The placental samples were stored at -80°C until further analysis.
4.6. Assessment of Plasma and Placental MDA
The levels of MDA in maternal plasma, umbilical cord plasma and placental tissue were assessed following the previously described protocol [48]. In brift, 150 μL plasma were reacted with the stock reagent containing 10% TCA, 5 mmol/L EDTA, 8% SDS and 0.5 μg/mL BHT. The mixture was incubated for 10 min at room temperature and added with 0.6% TBA. Afterward, the mixture was boiled in a water bath for 30 min. After cooling, the mixture was centrifuged at 1000× g for 10 min. The absorbance of the supernatant was measured at 532 nm by a spectrophotometer. 1,1,3,3-tetraethoxypropane was used to generate a standard curve. Data were expressed as nmol/mg protein.
4.7. Assessment of Plasma and Placental Protein Carbonyl
Plasma protein carbonyl content was determined via 2,4-dinitrophenylhydrazine (DNPH) derivatization and spectrophotometric analysis at 370 nm, as previously described [49]. The extinction coefficient of DNPH is then employed to convert absorbance into protein carbonyl concentration (nmol/mg protein).
4.8. Assessment of Plasma Catalase Activity
Catalase activity in maternal plasma, umbilical cord plasma and placental tissue was assessed following the previously described protocol [48]. In brief, 20 µL of plasma or standard solution was added to the microplate. The mixture of substrate containing 65 μmol/mL of H2O2 in 60 mmol/L PBS (pH 7.4) was added. After incubation at 37 °C for 1 min, 100 µL of ammonium Molybdate ((NH4)6 Mo7O24 .4 H2O) was added to stop the reaction. The yellow complex was determined under a 405 nm wavelength. Catalase from bovine liver (Sigma-Aldrich, United States) was used to generate standard curve. Data were expressed as U/mg protein.
4.9. Assessment of Plasma SOD Activity
Plasma SOD activity was assessed using the SOD Assay Kit - WST (Dojindo Laboratories, Japan) based on colorimetric analysis. The procedure included: add 20 µl of sample solution to each well, with 20 µl of ultrapure H2O to each blank well; add the working solution, dilution buffer, and enzyme solution; incubating at 37 °C for 20 minutes; and measured absorbance at 450 nm with a microplate reader. SOD activity was calculated as the %inhibition rate/mg of protein.
4.10. Assessment of Plasma Protein Content and Lipids
Maternal blood and umbilical cord blood were used for measurement of lipid profile; total cholesterol, and triglycerides. The measurement was done at Community Medical Laboratory, Faculty of Associated Medical Sciences, Khon Kaen University.
Protein concentration in plasma samples were quantified using the Bradford assay.
Briefly, diluted samples were incubated with Bradford reagent, and the absorbance at a specific wavelength (595 nm) were measured using a microplate reader. A standard curve generated with protein standard (BSA) were employed to convert absorbance values into protein concentration.
4.11. Placental Protein Extraction and Expression Analysis
Placental samples were homogenized in PBS containing proteolytic enzyme inhibitors (Complete-Mini; Roche), using an Ultra-Turex homogenizer (Bioblock Scientific, Illkirch, France). After homogenization, placental samples were centrifuged for 30 min at 4,000 rpm and the supernatant (protein extracts) was collected for western blot analysis.
Placental antioxidant protein expression was measured by using 30-50 ug protein samples. Placental protein was separated by 10% - 12% SDS-PAGE gels. Primary antibodies against SOD2 (Santa Cruz Biotechnology, Heidelberg, Germany; 1:1000), catalase (Sigma-Aldrich, St. Louis, MO, USA; 1:2000), UCP2 (Santa Cruz Biotechnology, Heidelberg, Germany; 1:1000), and Nrf2 (Santa Cruz Biotechnology, Heidelberg, Germany; 1: 500) were applied overnight at 4◦C. After washing, secondary antibody (anti-mouse IgG peroxidase conjugated) was applied for 1 hr. at room temperature. Blots was washed and incubated in commercially enhanced chemiluminescence reagents (ECL Prime, Amersham Bioscience, Little Chalfont, Buckinghamshire, UK), and bands were detected by ChemiDoc XRS+ imaging system (Bio-Rad, USA). Blots were re-incubated with β-actin antibody (Santa Cruz Biotechnology, Heidelberg, Germany; 1:4000 final dilution) as internal control. Expression values of SOD2, catalase, UCP2 and Nrf2 were normalized with β-actin.
4.12. Statistical Analysis
Data was statistically analyzed using the Graph-Pad Prism software version 9.3.1 (GraphPad, USA). The Kolmogorov-Smirnov test was used to analyze the normality of the data. Data with normal distribution were expressed as mean ± standard error of mean (SEM). The comparison between the two groups was done by using Student´s t-test and Pearson’s Chi-square. The differences were considered significant when p < 0.05.
5. Conclusions
This study provides evidence that maternal nutrition plays an important role in alteration of maternal feto-placental oxidative balance. The neonatal oxidative stress observed in obese pregnancy may be a key downstream moderator of fetal programming, which lead to an increased susceptibility to oxidative stress related diseases in later life. The results provide scientific evidence to perform nutritional counselling to women in reproductive age to improve maternal-fetal health and reducing the impact of fetal programming in the future generations.
Author Contributions
Conceptualization, T.J., S.P., K.K., S.M.A., and W.S.I,; methodology, S.P., T.J., K.K., S.M.A., and W.S.I,; validation, S.P., S.M.A., P.R.-R and W.S.I,; formal analysis, T.J. S.P., S.M.A., and W.S.I,; investigation, S.P., K.K., T.J., M.I., P.R.-R and W.S.I,; writing—original draft preparation, S.P., T.J., K.K., S.M.A., P.R.-R and W.S.I., All authors have read and agreed to the published version of the manuscript.
Funding
This research is funded by the Young Researcher Development Project of Khon Kaen University Year 2022, Thailand and by the Research Institute for Human High Performance and Health Promotion (HHP&HP), Khon Kaen University, Thailand and Invitation Research Grant (No. IN67029), Faculty of Medicine, Khon Kaen University, Thailand.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and the ICH Good Clinical Practice Guidelines and approved by the the Khon Kaen University Ethics Committee for Human Research, Khon Kaen University, Khon Kaen, Thailand with study identification code HE651023 (Date of approval; 22 March 2022). .
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is contained within the article. Additional raw data can be obtained from the corresponding author on request.
Acknowledgments
We thank the women who participated in the study. We thank to staff of the labor department, Srinagarind Hospital, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand for their support for the collection of samples of this study. We thank to Department of Physiology, Faculty of Medicine, Universidad Autónoma de Madrid, Madrid, Spain for providing the reagents for western blot analysis.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tauqeer, Z.; Gomez, G.; Stanford, F.C. Obesity in Women: Insights for the Clinician. J Womens Health (Larchmt) 2018, 27, 444–457. [Google Scholar] [CrossRef]
- Poston, L.; Caleyachetty, R.; Cnattingius, S.; Corvalan, C.; Uauy, R.; Herring, S.; Gillman, M.W. Preconceptional and maternal obesity: epidemiology and health consequences. Lancet Diabetes Endocrinol 2016, 4, 1025–1036. [Google Scholar] [CrossRef] [PubMed]
- Kelly, A.C.; Powell, T.L.; Jansson, T. Placental function in maternal obesity. Clin Sci (Lond) 2020, 134, 961–984. [Google Scholar] [CrossRef] [PubMed]
- Lamothe, J.; Khurana, S.; Tharmalingam, S.; Williamson, C.; Byrne, C.J.; Lees, S.J.; Khaper, N.; Kumar, A.; Tai, T.C. Oxidative Stress Mediates the Fetal Programming of Hypertension by Glucocorticoids. Antioxidants (Basel) 2021, 10, 531. [Google Scholar] [CrossRef]
- Palaska, E.; Antoniou, E.; Tzitiridou-Chatzopoulou, M.; Eskitzis, P.; Orovou, E. Correlation between Breastfeeding, Maternal Body Mass Index, and Childhood Obesity. Epidemiologia (Basel) 2024, 5, 411–420. [Google Scholar] [CrossRef]
- Jovandaric, M.Z.; Babic, S.; Raus, M.; Medjo, B. The Importance of Metabolic and Environmental Factors in the Occurrence of Oxidative Stress during Pregnancy. Int J Mol Sci 2023, 24, 11964. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Chen, Y.; Mao, X.; Du, M. Maternal obesity impairs fetal mitochondriogenesis and brown adipose tissue development partially via upregulation of miR-204-5p. Biochim Biophys Acta Mol Basis Dis 2019, 1865, 2706–2715. [Google Scholar] [CrossRef]
- Anam, A.K.; Cooke, K.M.; Dratver, M.B.; O'Bryan, J.V.; Perley, L.E.; Guller, S.M.; Hwang, J.J.; Taylor, H.S.; Goedeke, L.; Kliman, H.J.; et al. Insulin increases placental triglyceride as a potential mechanism for fetal adiposity in maternal obesity. Mol Metab 2022, 64, 101574. [Google Scholar] [CrossRef]
- Johns, E.C.; Denison, F.C.; Reynolds, R.M. The impact of maternal obesity in pregnancy on placental glucocorticoid and macronutrient transport and metabolism. Biochim Biophys Acta Mol Basis Dis 2020, 1866, 165374. [Google Scholar] [CrossRef]
- Santos-Rosendo, C.; Bugatto, F.; Gonzalez-Dominguez, A.; Lechuga-Sancho, A.M.; M, M.R.; Visiedo, F. Placental Adaptive Changes to Protect Function and Decrease Oxidative Damage in Metabolically Healthy Maternal Obesity. Antioxidants (Basel) 2020, 9, 794. [Google Scholar] [CrossRef]
- Martino, J.; Sebert, S.; Segura, M.T.; Garcia-Valdes, L.; Florido, J.; Padilla, M.C.; Marcos, A.; Rueda, R.; McArdle, H.J.; Budge, H.; et al. Maternal Body Weight and Gestational Diabetes Differentially Influence Placental and Pregnancy Outcomes. J Clin Endocrinol Metab 2016, 101, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Yanez Blanco, A.; Diaz-Lopez, K.M.; Vilchis-Gil, J.; Diaz-Garcia, H.; Gomez-Lopez, J.; Medina-Bravo, P.; Granados-Riveron, J.T.; Gallardo, J.M.; Klunder-Klunder, M.; Sanchez-Urbina, R. Diet and Maternal Obesity Are Associated with Increased Oxidative Stress in Newborns: A Cross-Sectional Study. Nutrients 2022, 14, 746. [Google Scholar] [CrossRef]
- Phuthong, S.; Reyes-Hernandez, C.G.; Rodriguez-Rodriguez, P.; Ramiro-Cortijo, D.; Gil-Ortega, M.; Gonzalez-Blazquez, R.; Gonzalez, M.C.; Lopez de Pablo, A.L.; Arribas, S.M. Sex Differences in Placental Protein Expression and Efficiency in a Rat Model of Fetal Programming Induced by Maternal Undernutrition. Int J Mol Sci 2020, 22, 237. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.L.; Mark, P.J.; Lewis, J.L.; Mori, T.A.; Keelan, J.A.; Waddell, B.J. Antioxidant defenses in the rat placenta in late gestation: increased labyrinthine expression of superoxide dismutases, glutathione peroxidase 3, and uncoupling protein 2. Biol Reprod 2010, 83, 254–260. [Google Scholar] [CrossRef]
- Stark, M.J.; Hodyl, N.A.; Butler, M.; Clifton, V.L. Localisation and characterisation of uncoupling protein-2 (UCP2) in the human preterm placenta. Placenta 2012, 33, 1020–1025. [Google Scholar] [CrossRef] [PubMed]
- Gnanalingham, M.G.; Williams, P.; Wilson, V.; Bispham, J.; Hyatt, M.A.; Pellicano, A.; Budge, H.; Stephenson, T.; Symonds, M.E. Nutritional manipulation between early to mid-gestation: effects on uncoupling protein-2, glucocorticoid sensitivity, IGF-I receptor and cell proliferation but not apoptosis in the ovine placenta. Reproduction 2007, 134, 615–623. [Google Scholar] [CrossRef]
- Malti, N.; Merzouk, H.; Merzouk, S.A.; Loukidi, B.; Karaouzene, N.; Malti, A.; Narce, M. Oxidative stress and maternal obesity: feto-placental unit interaction. Placenta 2014, 35, 411–416. [Google Scholar] [CrossRef]
- Evans, L.; Myatt, L. Sexual dimorphism in the effect of maternal obesity on antioxidant defense mechanisms in the human placenta. Placenta 2017, 51, 64–69. [Google Scholar] [CrossRef]
- Vanderlelie, J.; Venardos, K.; Clifton, V.L.; Gude, N.M.; Clarke, F.M.; Perkins, A.V. Increased biological oxidation and reduced anti-oxidant enzyme activity in pre-eclamptic placentae. Placenta 2005, 26, 53–58. [Google Scholar] [CrossRef]
- Wan, Y.; Chen, Y.; Wu, X.; Yin, A.; Tian, F.; Zhang, H.; Huang, X.; Wu, L.; Niu, J. Mediation effect of maternal triglyceride and fasting glucose level on the relationship between maternal overweight/ obesity and fetal growth: a prospective cohort study. BMC Pregnancy Childbirth 2023, 23, 449. [Google Scholar] [CrossRef]
- Mannino, A.; Sarapis, K.; Moschonis, G. The Effect of Maternal Overweight and Obesity Pre-Pregnancy and During Childhood in the Development of Obesity in Children and Adolescents: A Systematic Literature Review. Nutrients 2022, 14, 5125. [Google Scholar] [CrossRef] [PubMed]
- Francis, E.C.; Kechris, K.; Johnson, R.K.; Rawal, S.; Pathmasiri, W.; Rushing, B.R.; Du, X.; Jansson, T.; Dabelea, D.; Sumner, S.J.; et al. Maternal Serum Metabolomics in Mid-Pregnancy Identifies Lipid Pathways as a Key Link to Offspring Obesity in Early Childhood. Int J Mol Sci 2024, 25, 7620. [Google Scholar] [CrossRef] [PubMed]
- Grilo, L.F.; Tocantins, C.; Diniz, M.S.; Gomes, R.M.; Oliveira, P.J.; Matafome, P.; Pereira, S.P. Metabolic Disease Programming: From Mitochondria to Epigenetics, Glucocorticoid Signalling and Beyond. Eur J Clin Invest 2021, 51, e13625. [Google Scholar] [CrossRef] [PubMed]
- Castilla-Peon, M.F.; Medina Bravo, P.G.; Sanchez-Urbina, R.; Gallardo-Montoya, J.M.; Soriano-Lopez, L.C.; Coronel Cruz, F.M. Diabetes and obesity during pregnancy are associated with oxidative stress genotoxicity in newborns. J Perinat Med 2019, 47, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Shook, L.L.; James, K.E.; Roberts, D.J.; Powe, C.E.; Perlis, R.H.; Thornburg, K.L.; O'Tierney-Ginn, P.F.; Edlow, A.G. Sex-specific impact of maternal obesity on fetal placental macrophages and cord blood triglycerides. Placenta 2023, 140, 100–108. [Google Scholar] [CrossRef]
- Zhou, J.; Bai, J.; Guo, Y.; Fu, L.; Xing, J. Higher Levels of Triglyceride, Fatty Acid Translocase, and Toll-Like Receptor 4 and Lower Level of HDL-C in Pregnant Women with GDM and Their Close Correlation with Neonatal Weight. Gynecol Obstet Invest 2021, 86, 48–54. [Google Scholar] [CrossRef]
- Keleher, M.R.; Erickson, K.; Kechris, K.; Yang, I.V.; Dabelea, D.; Friedman, J.E.; Boyle, K.E.; Jansson, T. Associations between the activity of placental nutrient-sensing pathways and neonatal and postnatal metabolic health: the ECHO Healthy Start cohort. Int J Obes (Lond) 2020, 44, 2203–2212. [Google Scholar] [CrossRef]
- Leonard, S.A.; Rasmussen, K.M.; King, J.C.; Abrams, B. Trajectories of maternal weight from before pregnancy through postpartum and associations with childhood obesity. Am J Clin Nutr 2017, 106, 1295–1301. [Google Scholar] [CrossRef]
- Wang, L.; O'Kane, A.M.; Zhang, Y.; Ren, J. Maternal obesity and offspring health: Adapting metabolic changes through autophagy and mitophagy. Obes Rev 2023, 24, e13567. [Google Scholar] [CrossRef]
- Phengpol, N.; Thongnak, L.; Lungkaphin, A. The programming of kidney injury in offspring affected by maternal overweight and obesity: role of lipid accumulation, inflammation, oxidative stress, and fibrosis in the kidneys of offspring. J Physiol Biochem 2023, 79, 1–17. [Google Scholar] [CrossRef]
- Hernandez-Trejo, M.; Montoya-Estrada, A.; Torres-Ramos, Y.; Espejel-Nunez, A.; Guzman-Grenfell, A.; Morales-Hernandez, R.; Tolentino-Dolores, M.; Laresgoiti-Servitje, E. Oxidative stress biomarkers and their relationship with cytokine concentrations in overweight/obese pregnant women and their neonates. BMC Immunol 2017, 18, 3. [Google Scholar] [CrossRef] [PubMed]
- Hussain, T.; Murtaza, G.; Metwally, E.; Kalhoro, D.H.; Kalhoro, M.S.; Rahu, B.A.; Sahito, R.G.A.; Yin, Y.; Yang, H.; Chughtai, M.I.; et al. The Role of Oxidative Stress and Antioxidant Balance in Pregnancy. Mediators Inflamm 2021, 9962860. [Google Scholar] [CrossRef]
- Ballesteros-Guzman, A.K.; Carrasco-Legleu, C.E.; Levario-Carrillo, M.; Chavez-Corral, D.V.; Sanchez-Ramirez, B.; Marinelarena-Carrillo, E.O.; Guerrero-Salgado, F.; Reza-Lopez, S.A. Prepregnancy Obesity, Maternal Dietary Intake, and Oxidative Stress Biomarkers in the Fetomaternal Unit. Biomed Res Int 2019, 5070453. [Google Scholar] [CrossRef] [PubMed]
- Alfonso-Prieto, M.; Biarnes, X.; Vidossich, P.; Rovira, C. The molecular mechanism of the catalase reaction. J Am Chem Soc 2009, 131, 11751–11761. [Google Scholar] [CrossRef] [PubMed]
- Biri, A.; Onan, A.; Devrim, E.; Babacan, F.; Kavutcu, M.; Durak, I. Oxidant status in maternal and cord plasma and placental tissue in gestational diabetes. Placenta 2006, 27, 327–332. [Google Scholar] [CrossRef]
- Psefteli, P.M.; Morris, J.K.; Ehler, E.; Smith, L.; Bowe, J.; Mann, G.E.; Taylor, P.D.; Chapple, S.J. Sulforaphane induced NRF2 activation in obese pregnancy attenuates developmental redox imbalance and improves early-life cardiovascular function in offspring. Redox Biol 2023, 67, 102883. [Google Scholar] [CrossRef]
- Ruano, C.S.M.; Miralles, F.; Mehats, C.; Vaiman, D. The Impact of Oxidative Stress of Environmental Origin on the Onset of Placental Diseases. Antioxidants (Basel) 2022, 11, 106. [Google Scholar] [CrossRef]
- Xia, Y.; Zhai, X.; Qiu, Y.; Lu, X.; Jiao, Y. The Nrf2 in Obesity: A Friend or Foe? Antioxidants (Basel) 2022, 11, 2067. [Google Scholar] [CrossRef]
- Song, Y.R.; Kim, J.K.; Lee, H.S.; Kim, S.G.; Choi, E.K. Serum levels of protein carbonyl, a marker of oxidative stress, are associated with overhydration, sarcopenia and mortality in hemodialysis patients. BMC Nephrol 2020, 21, 281. [Google Scholar] [CrossRef]
- Negro, S.; Boutsikou, T.; Briana, D.D.; Tataranno, M.L.; Longini, M.; Proietti, F.; Bazzini, F.; Dani, C.; Malamitsi-Puchner, A.; Buonocore, G.; et al. Maternal obesity and perinatal oxidative stress: the strength of the association. J Biol Regul Homeost Agents 2017, 31, 221–227. [Google Scholar]
- Rocha, S.; Gomes, D.; Lima, M.; Bronze-da-Rocha, E.; Santos-Silva, A. Peroxiredoxin 2, glutathione peroxidase, and catalase in the cytosol and membrane of erythrocytes under H2O2-induced oxidative stress. Free Radic Res 2015, 49, 990–1003. [Google Scholar] [CrossRef]
- Fukai, T.; Ushio-Fukai, M. Superoxide dismutases: role in redox signaling, vascular function, and diseases. Antioxid Redox Signal 2011, 15, 1583–1606. [Google Scholar] [CrossRef] [PubMed]
- Arogbokun, O.; Rosen, E.; Keil, A.P.; Milne, G.L.; Barrett, E.; Nguyen, R.; Bush, N.R.; Swan, S.H.; Sathyanarayana, S.; Ferguson, K.K. Maternal Oxidative Stress Biomarkers in Pregnancy and Child Growth from Birth to Age 6. J Clin Endocrinol Metab 2021, 106, 1427–1436. [Google Scholar] [CrossRef] [PubMed]
- Redmer, D.A.; Milne, J.S.; Aitken, R.P.; Johnson, M.L.; Borowicz, P.P.; Reynolds, L.P.; Caton, J.S.; Wallace, J.M. Decreasing maternal nutrient intake during the final third of pregnancy in previously overnourished adolescent sheep: effects on maternal nutrient partitioning and feto-placental development. Placenta 2012, 33, 114–121. [Google Scholar] [CrossRef]
- Correia-Branco, A.; Keating, E.; Martel, F. Maternal undernutrition and fetal developmental programming of obesity: the glucocorticoid connection. Reprod Sci 2015, 22, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Mando, C.; Calabrese, S.; Mazzocco, M.I.; Novielli, C.; Anelli, G.M.; Antonazzo, P.; Cetin, I. Sex specific adaptations in placental biometry of overweight and obese women. Placenta 2016, 38, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Consultation, W.H.O.E. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar]
- Poasakate, A.; Maneesai, P.; Rattanakanokchai, S.; Bunbupha, S.; Tong-Un, T.; Pakdeechote, P. Genistein Prevents Nitric Oxide Deficiency-Induced Cardiac Dysfunction and Remodeling in Rats. Antioxidants (Basel) 2021, 10, 237. [Google Scholar] [CrossRef]
- Ramiro-Cortijo, D.; Calle, M.; Rodriguez-Rodriguez, P.; Pablo, A.L.L.; Lopez-Gimenez, M.R.; Aguilera, Y.; Martin-Cabrejas, M.A.; Gonzalez, M.D.C.; Arribas, S.M. Maternal Antioxidant Status in Early Pregnancy and Development of Fetal Complications in Twin Pregnancies: A Pilot Study. Antioxidants (Basel) 2020, 9, 269. [Google Scholar] [CrossRef]
Figure 1.
Maternal plasma and umbilical cord plasma level of total cholesterol (a, b), triglyceride (c, d) and protein content (e, f) in maternal lean and maternal obesity groups. Results were expressed as mean ± SEM, n = 20 each. p-value was tested by Student´s t-test, *p < 0.05 relative to the maternal lean group.
Figure 1.
Maternal plasma and umbilical cord plasma level of total cholesterol (a, b), triglyceride (c, d) and protein content (e, f) in maternal lean and maternal obesity groups. Results were expressed as mean ± SEM, n = 20 each. p-value was tested by Student´s t-test, *p < 0.05 relative to the maternal lean group.
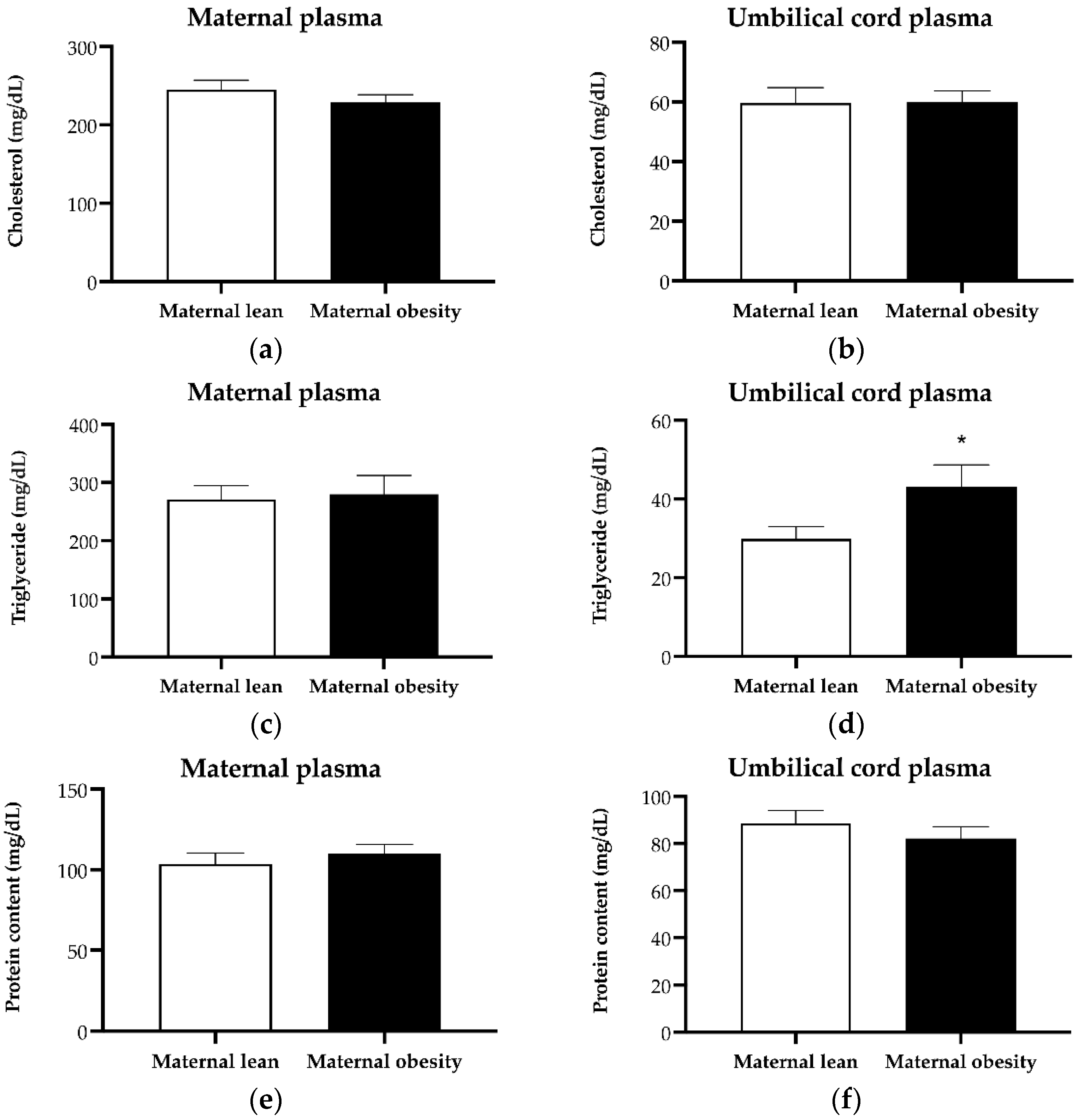
Figure 2.
Level of a) malondialdehyde (MDA) and b) protein carbonyl in maternal plasma of maternal lean and maternal obesity groups. Results were expressed as mean ± SEM, n = 20 each. p-value was tested by Student´s t-test.
Figure 2.
Level of a) malondialdehyde (MDA) and b) protein carbonyl in maternal plasma of maternal lean and maternal obesity groups. Results were expressed as mean ± SEM, n = 20 each. p-value was tested by Student´s t-test.
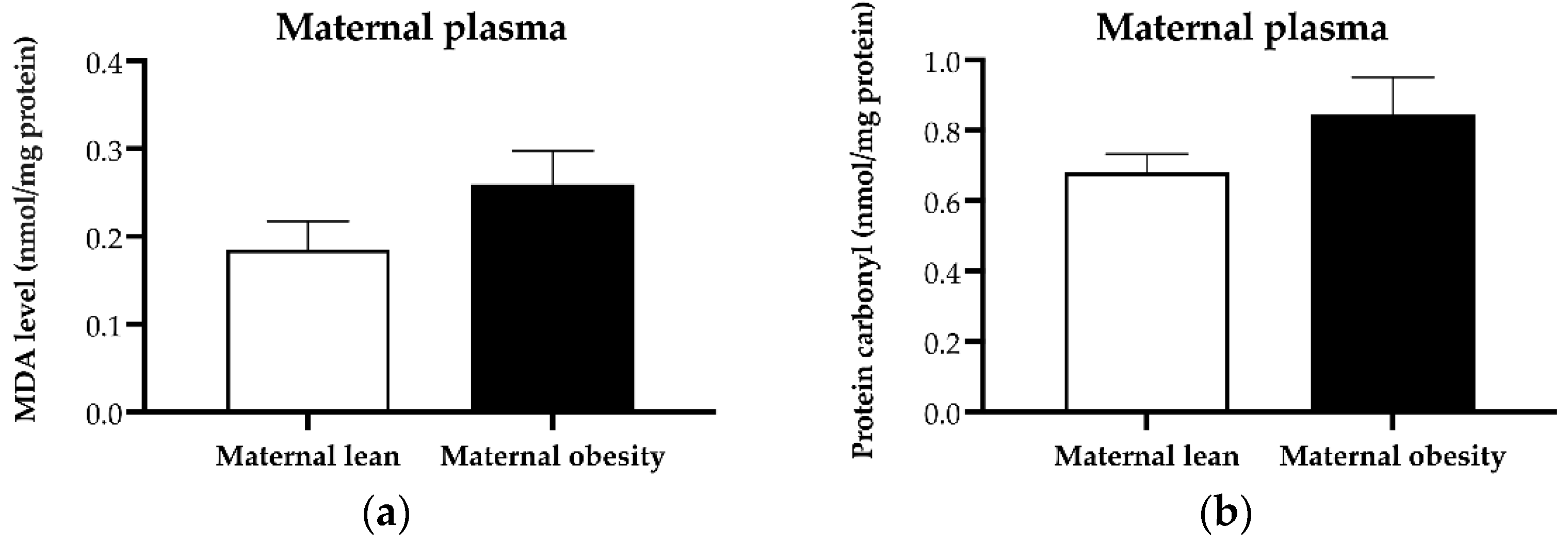
Figure 3.
Activity of a) catalase and b) superoxide dismutase (SOD) in maternal plasma of maternal lean and maternal obesity groups. Results were expressed as mean ± SEM, n = 20 each, p-value was tested by Student´s t-test, *p < 0.05 relative to the maternal lean group.
Figure 3.
Activity of a) catalase and b) superoxide dismutase (SOD) in maternal plasma of maternal lean and maternal obesity groups. Results were expressed as mean ± SEM, n = 20 each, p-value was tested by Student´s t-test, *p < 0.05 relative to the maternal lean group.
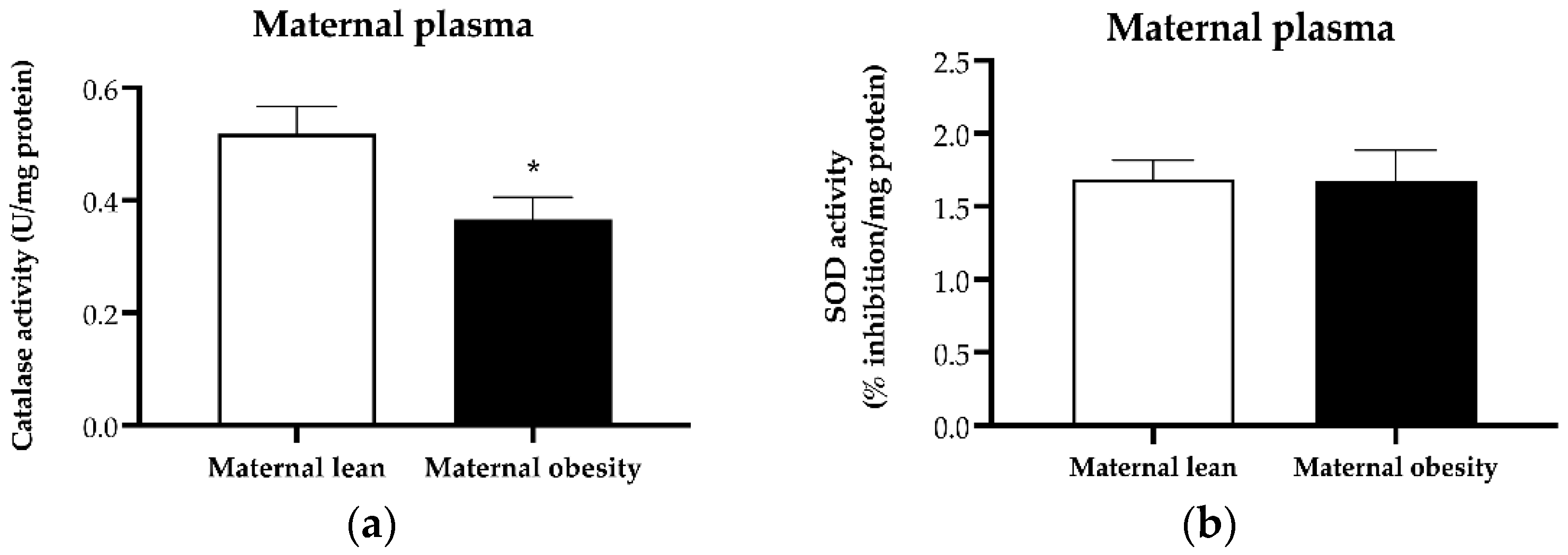
Figure 4.
Level of a) malondialdehyde (MDA) and b) protein carbonyl in umbilical cord plasma of maternal lean and maternal obesity groups. Results were expressed as mean ± SEM, n = 20 each. p-value was tested by Student´s t-test.
Figure 4.
Level of a) malondialdehyde (MDA) and b) protein carbonyl in umbilical cord plasma of maternal lean and maternal obesity groups. Results were expressed as mean ± SEM, n = 20 each. p-value was tested by Student´s t-test.
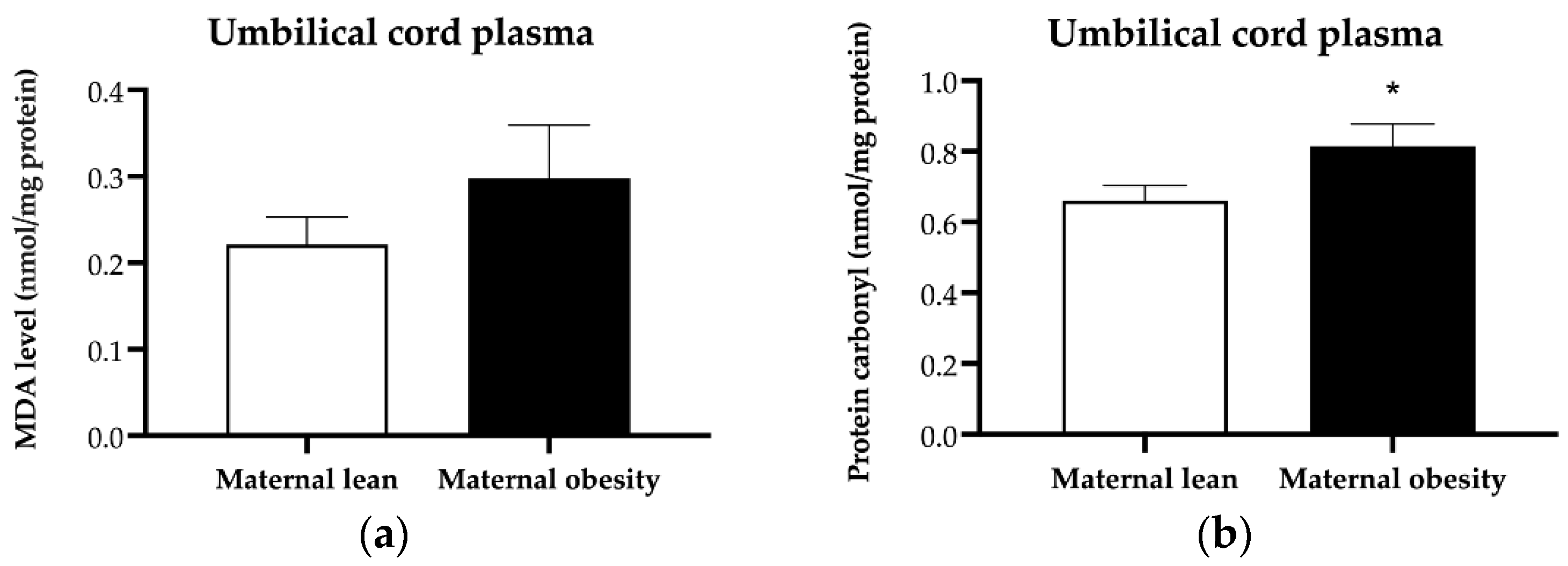
Figure 5.
Activity of a) catalase and b) superoxide dismutase (SOD) in umbilical cord plasma of maternal lean and maternal obesity groups. Results were expressed as mean ± SEM, n = 20 each. p-value was tested by Student´s t-test. *p < 0.05 relative to the maternal lean group.
Figure 5.
Activity of a) catalase and b) superoxide dismutase (SOD) in umbilical cord plasma of maternal lean and maternal obesity groups. Results were expressed as mean ± SEM, n = 20 each. p-value was tested by Student´s t-test. *p < 0.05 relative to the maternal lean group.
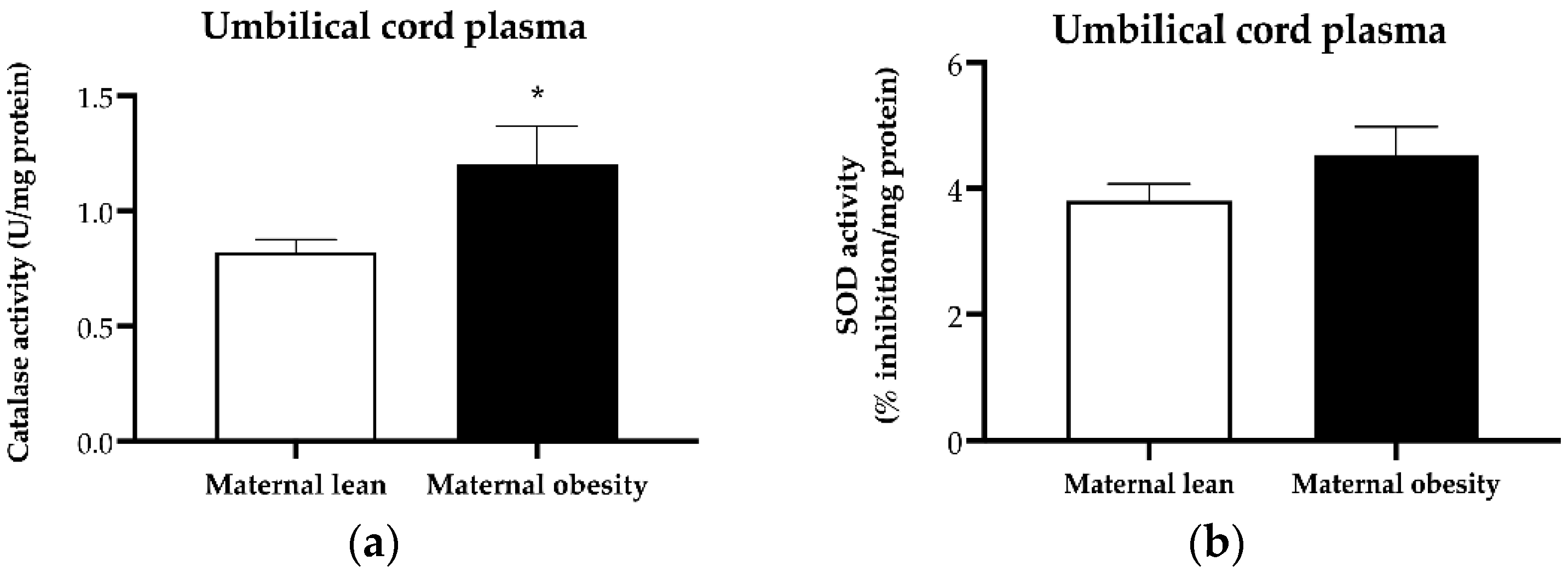
Figure 6.
Level of a) malondialdehyde (MDA) and b) protein carbonyl in placental tissue of mater-nal lean and maternal obesity groups. Results were expressed as mean ± SEM, n = 20 each. p-value was tested by Student´s t-test.
Figure 6.
Level of a) malondialdehyde (MDA) and b) protein carbonyl in placental tissue of mater-nal lean and maternal obesity groups. Results were expressed as mean ± SEM, n = 20 each. p-value was tested by Student´s t-test.
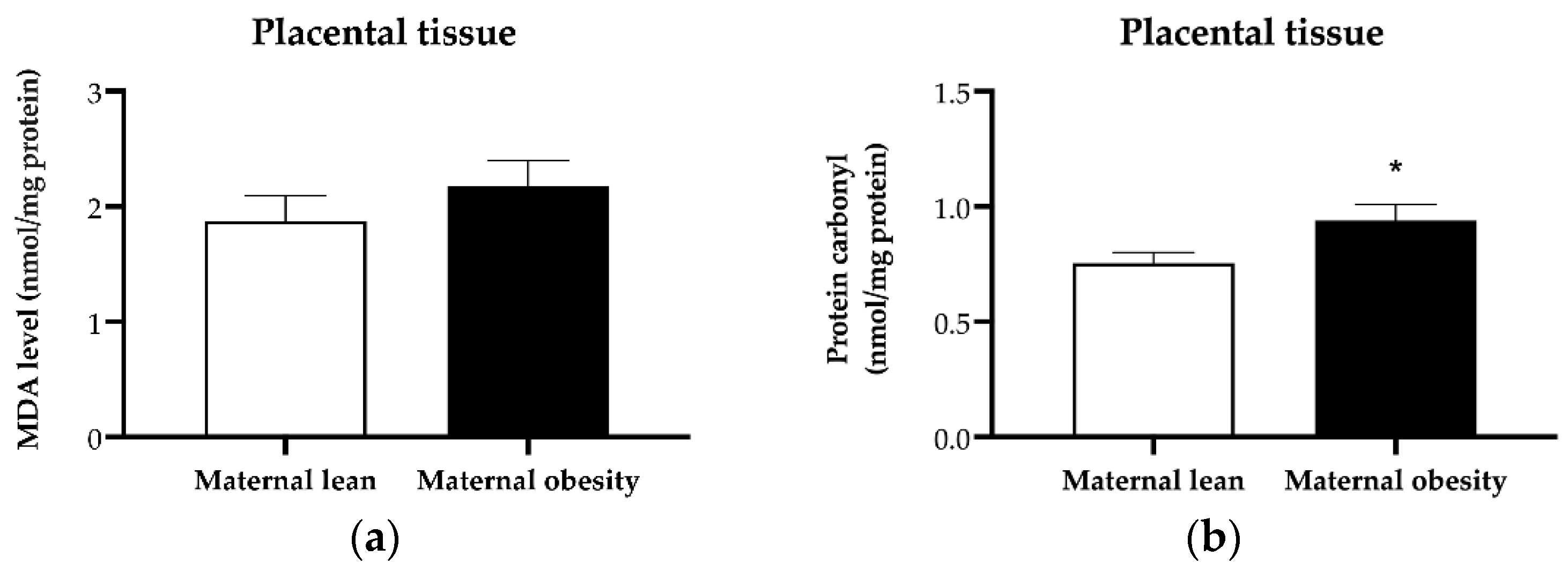
Figure 7.
Placental protein expression of a) catalase, b) SOD2 c) Nrf2 and d) UCP2 measured by western blot analysis of maternal lean and maternal obesity groups (n=4/group). Results were reported as mean ± SEM. p-value was tested by Mann Whitney test. *p < 0.05 relative to the maternal lean group.
Figure 7.
Placental protein expression of a) catalase, b) SOD2 c) Nrf2 and d) UCP2 measured by western blot analysis of maternal lean and maternal obesity groups (n=4/group). Results were reported as mean ± SEM. p-value was tested by Mann Whitney test. *p < 0.05 relative to the maternal lean group.
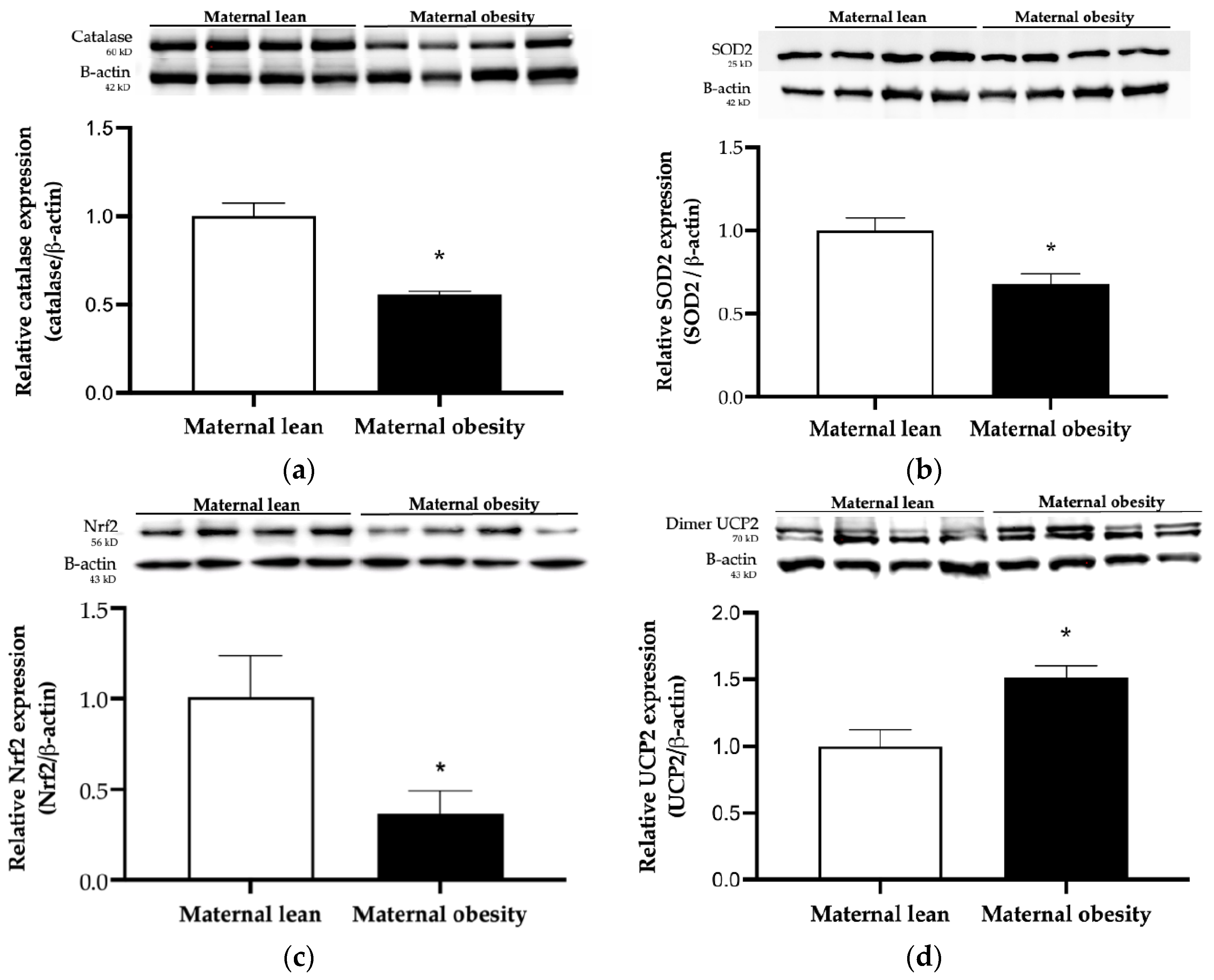

Table 1.
Demographics and pregnancy outcome data.
| Parameter | Maternal lean | Maternal obesity | p-value |
|---|---|---|---|
| Maternal age at delivery (year) | 27.65 ± 0.85 | 30.30 ± 1.20 | 0.0779 |
| Gestational age at delivery (weeks) | 38.71 ± 0.21 | 38.81 ± 0.28 | 0.7744 |
| Pre-pregnancy weight (kg) | 52.56 ± 1.29 | 75.32 ± 1.79 *** | <0.0001 |
| Pre-pregnancy BMI (kg/m2) | 20.26 ± 0.45 | 29.40 ± 0.58 *** | <0.0001 |
| Weight at delivery (kg) | 66.90 ± 2.10 | 90.64 ± 2.22 *** | <0.0001 |
| Neonatal gender, male n (%) | 10 (50) | 11 (55) | 0.7575 |
| Neonatal birth weight (g) | 3083 ± 101 | 3327 ± 110 | 0.1103 |
| Neonatal length (cm) | 49.20 ± 0.57 | 49.21 ± 0.59 | 0.9898 |
| Placental weight (g) | 581.50 ± 28.02 | 701.50 ± 41.89 * | 0.0224 |
| Feto-placental ratio | 5.43 ± 0.19 | 4.87 ± 0.16 * | 0.0374 |
Results were reported as mean ± SEM or n (%). n=20 each group. p-value was tested by Student´s t-test for continuous variables and Pearson’s Chi-square test for categorical data. *p < 0.05, ***p < 0.0001 relative to the maternal lean group.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



