
Submitted:
30 August 2024
Posted:
02 September 2024
You are already at the latest version
Abstract
Background: The development of new technologies, interpretation of amputations as therapeutic failures by society, and high morbidity and mortality associated with external hemipelvectomies make these mutilating surgical procedures appear obsolete. Herein, we review the scientific literature on the topic and present two cases of high-grade ulcerated soft tissue sarcomas in the gluteal region showing exceptional behavior and different outcomes. Methods: We performed a literature review of the PubMed databases from 2022 to April 2024. Additionally, we present two cases of soft tissue sarcomas in 18- and 71-years old female patients, which were treated with extended external hemipelvectomies with anterior flap and in combination with abdomino-perineal amputation and colostomy in one case. Results: At 4 years of follow-up, case one is living a relatively normal life. She had an uncomplicated pregnancy and a cesarean section delivery. Case two underwent emergency surgery for intestinal perforation and sepsis. She died 2.5 months following the surgery. Conclusion: External hemipelvectomy for soft tissue sarcoma treatment is a demanding surgical procedure with purpose in selected cases after review by multidisciplinary committees and with informed patient consent. This should be similarly individualized and extended to other pathologies when possible
Keywords:
External hemipelvectomy
; Amputation
; Soft tissue sarcoma
; Pelvis
; Pelvis girdle
; Pregnancy
; Delivery
; Abdominoperineal amputation
; Colostomy
1. Introduction
Hemipelvectomy is a surgical procedure involving pelvic resection, indicated for tumors in this anatomical location. It can be further classified as internal (with limb preservation) or external (without limb preservation). Both types have advantages and disadvantages, as well as technical difficulties and complications, due to the complex regional anatomy of the pelvis.
Resection in an internal hemipelvectomy can affect zones I–IV of the pelvis [1], sometimes in a combined manner. Bone reconstruction may or may not be necessary, especially after resection of zones I and III. Although decided individually for each patient, options include iliofemoral pseudoarthrosis or arthrodesis using different grafts (allograft, free vascularized fibular graft, vascularized fibular autograft, or autoclaved autograft) or prosthetic reconstruction. Customized prosthetic reconstruction, supported by new technologies, is currently preferred, though this remains controversial [2,3,4,5,6].
Pelvic structures necessary for lower limb function include the sciatic nerve, femoral neurovascular bundle, and periacetabular region of the pelvis. If tumor resection requires removal of two of these three critical anatomic structures, the patient will have a nonfunctional limb and an external hemipelvectomy would be recommended [7]. This can be performed through the ilium (modified or conservative), sacroiliac joint (standard or classic), or sacral foramina (extended) [8,9,10]. Soft tissue coverage can be achieved using a posterior (gluteal) or anterior flap, although other myocutaneous flaps can also be used, including rectus abdominis flaps, ipsilateral external oblique flaps [11], and flaps from the amputated limb itself [12].
The incidence of limb-sparing procedures performed for treating musculoskeletal tumors is increasing, facilitated by the development of new technologies. Moreover, current society interprets mutilating procedures as therapeutic failures. For both these reasons, in addition to its inherent morbidity and mortality, external hemipelvectomy seems to have become an obsolete technique, as already stated in some classic articles [13]. This study intends to revisit external hemipelvectomy in the context of soft tissue sarcomas (STS), providing an updated literature review and two case reports that demonstrate unique presentations and behaviors.
2. Material and Methods
We conducted a literature search of the PubMed database from 2022 to April 30, 2024. Our search strategy utilized the following terms: (“sarcoma” [MeSH Terms] OR “Soft Tissue Neoplasms” [MeSH] OR “sarcoma” OR “soft tissue sarcom*” OR “soft-tissue sarcom*”) AND (“hemipelvectomy*” OR “hindquarter amputation*”). Additionally, references of included studies were manually assessed to identify possible studies of interest that were not captured in the search. We reviewed the sample of studies and compared the outcomes of external hemipelvectomies, particularly in comparison to internal hemipelvectomies.
Case 1
A 20-year-old woman with no relevant medical history visited the emergency department of our hospital. She indicated having undergone surgery 4 months ago in her native country (Morocco) for a tumor in the right gluteal region classified in the report she provided as dermatofibrosarcoma protuberans. Physical examination revealed a vegetative, ulcerated, bleeding lesion in the same region (Figure 1A). Magnetic resonance imaging (MRI) identified a large subcutaneous soft tissue mass measuring 15 × 12 cm in its craniocaudal and transverse planes, with multiple lobulations infiltrating the gluteal muscles, extensively contacting the iliac blade without infiltrating it, and extending beyond the median sacral crest (Figure 1B, 1C, and 1D). A core needle biopsy was performed, and AJCC stage IIIB pleomorphic spindle cell sarcoma with negative extension status was diagnosed.
After multidisciplinary discussion, preoperative embolization of the gluteal artery (Figure 2) was performed on January 2, 2020, followed by an anterior flap extended external hemipelvectomy (Figure 3). The diagnosis was confirmed with clear resection margins, and adjuvant chemotherapy was administered.
Case 2
A 71-year-old woman with a history of arterial hypertension, dyslipidemia, hypothyroidism being treated with medication, mild chronic renal failure, asymptomatic dissecting aortic aneurysm (incidental finding), and a melanoma of the back that underwent surgery 4 years earlier. She was transferred to our hospital on November 19, 2018, from another center due to a tumor in her right gluteal region that forced her to remain bedridden in a prone position. The lesion was biopsied, and she was diagnosed with AJCC stage IIIB high-grade soft tissue sarcoma. The patient reported that the tumor had appeared 3 months earlier and had rapidly grown since then. Physical examination revealed a large, ulcerated, bleeding, vegetative lesion (Figure 4). MRI showed a lesion measuring 17 × 12 × 13 cm and infiltrating the skin deep into the gluteus maximus muscle. Multiple disseminated satellite nodules were found occupying the fat planes of the posterior thigh, ischioanal fossa, greater sciatic notch, and internal obturator region. The anteromedial tumor margin was adherent and partially infiltrated the external anal sphincter and anal orifice (Figure 5). Extension status eliminated distant disease.
With a low level of awareness of the multifactorial etiology (attributed to the medication, catabolic condition, and onset of secondary polymicrobial sepsis caused by Streptococcus agalactiae, S. epidermidis, and Ruminococcus), a multidisciplinary discussion of the case was held. The patient's general condition was improved, and an urgent intervention was performed on November 22, 2018. An abdominoperineal resection with colostomy was performed (confirming perforation of the rectal ampulla) in combination with an anterior flap extended external hemipelvectomy (Figure 6).
3. Results
A literature search of the last 2 years found 29 articles in PubMed related to the subject. Addressing different aspects, seven articles corresponded to isolated cases [14,15,16,17,18,19,20], 14 to case series [2,3,4,21,22,23,24,25,26,27,28,29,30,31], two to meta-analyses or literature reviews [32,33], and two to updating articles [7,34]. The remaining publications concerned experimental studies [35,36,37,38]. Although most publications focused on internal hemipelvectomies [2,3,14,17,18,19,22,26,30,34,38] or alternatives to hemipelvectomy [20], the reviewed articles indicate that external hemipelvectomy remains a current procedure, even in the pediatric population [28].
Case 1
The patient’s immediate postoperative period was uneventful. She underwent a rehabilitation program and adapted to an external prosthesis for walking. A spontaneous pregnancy occurred 3 years and 6 months post-surgery. Relative rest was recommended from week 20, and absolute rest from week 28. The pregnancy and cesarean section conducted at 37 + 1 weeks of gestation were uneventful. The cesarean section was selected to protect the pelvic floor since the birth canal was assumed to be unstructured, although vaginal delivery was not contraindicated. Furthermore, fetal development and the puerperal course were normal (Figure 7 and Figure 8). After more than 4 years of follow-up, the patient currently shows no signs of local recurrence or distant disease. She experiences lumbar discomfort after prolonged standing and walks with the external orthosis and, occasionally, without it, with the aid of two crutches (Figure 9).
Case 2
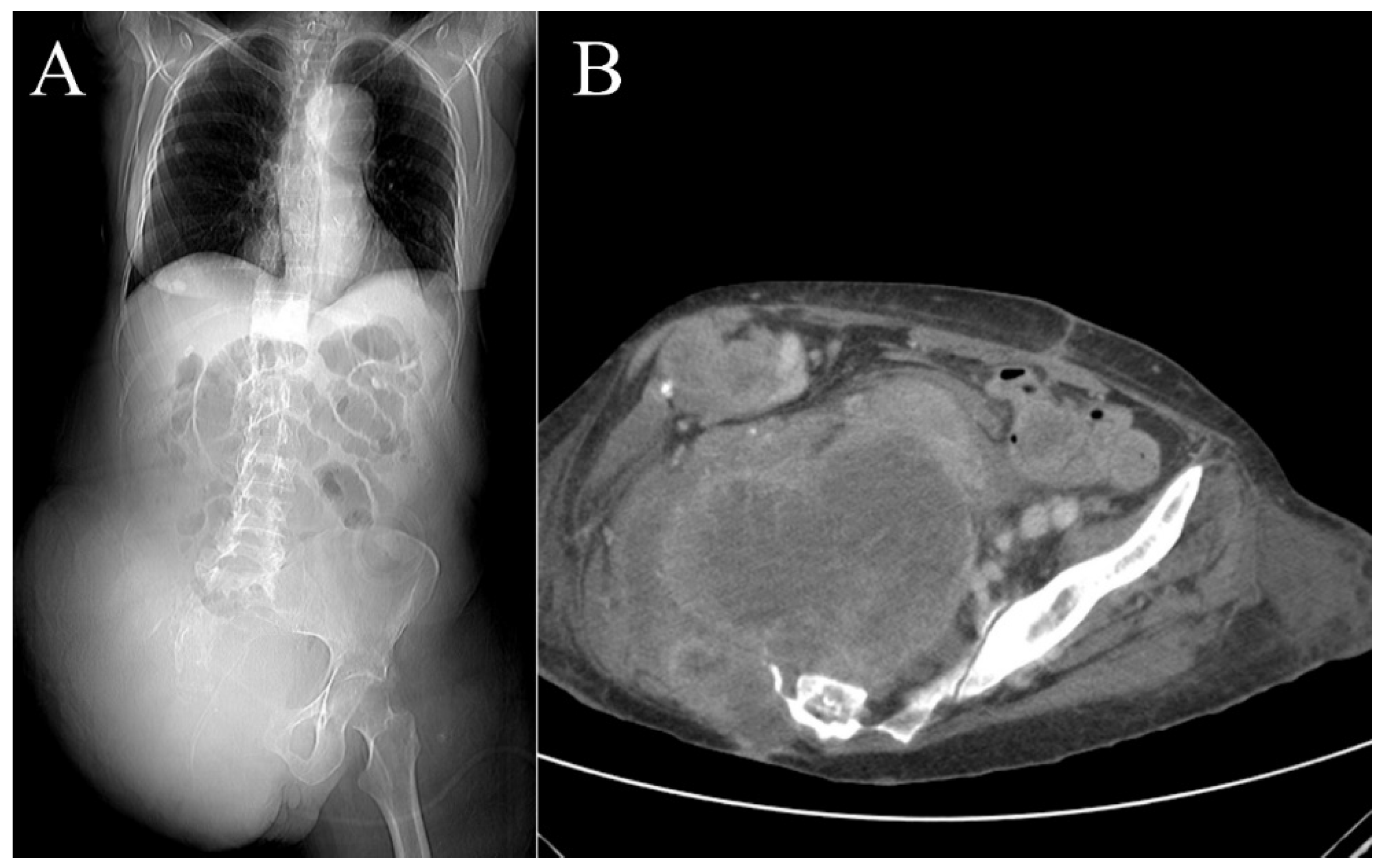
The patient developed metabolic acidosis, third spacing, and anasarca in the immediate postoperative period, with active bleeding from the colostomy. An abdominal computed tomography scan revealed active arterial bleeding in the cecum in the context of ischemic colitis, which was shortly followed by local recurrence of the sarcoma and lung metastasis (Figure 10). Due to hemodynamic instability and a fluctuating confusional state, supportive care was initiated and persisted until the patient’s death on February 2, 2019.
4. Discussion
Currently, amputations performed in orthopedic surgical oncology are often perceived by society and a large part of the medical community as a sign of treatment failure. This may be the case when it is caused by a complication from a previous surgery, but not when it is selected as the primary treatment for an aggressive or malignant tumor that cannot be resected with clear margins or when resection is followed by a dysfunctional reconstruction. Compared with limb-conserving surgery, amputations are performed in approximately 10% of patient with sarcoma [39]. These previous considerations are also applicable to hemipelvectomy, a procedure first performed by Billroth in 1891, although the patient survived only for a few hours. The first successful hemipelvectomy was performed in 1895 by Girard [40].
In conservative surgery of soft tissue sarcomas of the pelvis girdle, preservation of the major neurovascular structures is a necessary condition, although resection of one or both main nerves does not represent an absolute contraindication for a conservative procedure [13]. On the other hand, an ulcerated tumor would be [41], as it was in the two cases presented in our study. Except for local recurrence after internal hemipelvectomy and palliative indications, external hemipelvectomy remains a priori curative surgical procedure. Laitinen et al. recalled that in the modern era, the main indication for major pelvic resections, including hindquarter amputation, is for local control of malignant tumor [33]. In this context, when treating malignant musculoskeletal tumors, the priority is to preserve life, then limb, and lastly, limb function.
The most common soft tissue sarcomas of the pelvic girdle are undifferentiated pleomorphic sarcoma and liposarcoma. Local surgical treatment is guided by the same principles as those of soft tissue sarcomas in other anatomical locations, albeit with the constraints of the previously described difficulties due to regional anatomy. Moreover, similar to bone sarcomas, most are diagnosed at a larger size compared with those usually found in other more accessible locations for physical examination. Furthermore, frequent involvement of soft tissues essential for coverage in internal hemipelvectomy compromises limb-sparing surgery.
Comparatively, and without distinguishing between bone sarcomas and soft tissue sarcomas, external and internal hemipelvectomies generally do not show significant differences regarding complications, with an overall mortality rate of ≤9% and a postoperative complication rate of 20–75% [4,41,42,43]. The most frequent complications are surgical wound infections and flap necrosis, especially in anterior flaps [13,42,44]. Among all other possible complications, urogenital trauma is estimated to occur in 1.8–2.9% of cases [4] and total complications in this anatomical region are between 8–18% [43].
Flap necrosis treatment varies. However, it can be prevented by including the gluteus maximus muscle in posterior flaps, and the rectus femoris and vastus intermedius muscles in anterior flaps [13]. Infections occur in 10–70% of patients due to different reasons [4,43,45]. Guder et al. [43] compared internal and external hemipelvectomies and reported that complications are more frequent in the former, especially in cases of reconstruction as well as type II and III resections, possibly due to the proximity and sacrifice of lymphatic vessels. Another case series showed that reconstructive procedures, while maintaining joint stability, are associated with more complications [4,32,43]. A 2022 meta-analysis encourages the use of internal hemipelvectomy in pelvic sarcoma treatment, due to lower risk of surgical site infections [32].
Regarding oncological outcomes, survival after a potentially curative hemipelvectomy depends on several factors, including tumor histology and size, disease stage, patient’s general condition, and resection type [43,46]. Whether the hemipelvectomy was internal or external is not as important [32,47]. However, mean survival in these patients is highly variable. If the patient is disease-free 5 years post-surgery, sarcoma-induced mortality risk is low [48]. The same applies to local recurrences, except for bone chondrosarcoma, where late recurrences are more frequent.
Functional outcomes are particularly important following any type of hemipelvectomy. Regarding quality of life, no differences have been reported between internal and external hemipelvectomies, although those who underwent external hemipelvectomy report more phantom limb pain. Beck et al. reported that few of the patients who underwent hemipelvectomy were independent at discharge, although most were independent 6 years later with respect to daily living activities [42]. However, long-term studies have also reported that limb function deteriorates after internal hemipelvectomy, decreasing by 23% over a follow-up period of 23–38 years [48].
External hemipelvectomy often results in better mobility at discharge, although it subsequently causes more pain, increased bladder dysfunction, and difficulty climbing stairs in half of patients [41,42]. The same study showed that 4.4% of patients walked without external aids, 81% used crutches, 9% used wheelchairs, and 6% remained bedridden [42]. Regarding the use of prostheses, most patients did not need them as they moved better without them, limiting their use for standing and cosmetic reasons. Of the four surviving patients who underwent external hemipelvectomy in a case series by Guder et al., two used wheelchairs (one for a short time) and the other two used crutches for short distances and wheelchairs for long distances [43].
Emotional outcomes after hemipelvectomy have been poorly investigated in scientific literature and are often limited to the corresponding section of the Musculoskeletal Tumor Society scoring system (MSTS). Finally, financial implications are difficult to calculate accurately, since social costs due to various disabilities, prosthetic changes, and those affecting the overall quality of life should all be included [49].
The two cases in our study exemplify the two extremes of the possible outcomes of an external hemipelvectomy: one good oncological and functional outcome and one poor outcome with multiple complications. Both serve to ensure that patients are properly informed prior to the procedure. Our first patient should be further discussed with respect to her pregnancy and subsequent delivery.
Only 14 deliveries after hemipelvectomy had been published in the literature until 2008 [50], although other previous articles had reported a few isolated cases [51,52,53]. Only two new cases have been published since then [40,54]. Although most tumors were bone tumors and flap type was unspecified, vaginal delivery remains possible. However, hemipelvectomy is associated with an increased risk of fetal malposition due to the altered pelvic anatomy and a caesarean section should be considered. In any case, a gynaecological assessment is essential.
5. Conclusions
External hemipelvectomy with curative purposes is a surgical procedure that is still being performed in specific cases of soft tissue sarcomas after a multidisciplinary committee case review and with patient consent. This should be individualized in a similar manner for and extended for other pathologies when possible.
Author Contributions
Conceptualization, L.R.R.P.; Methodology, L.R.R.P., P.C.R., and J.E.V.R.; Validation and Formal Analysis, P.C.R., L.C.G., M.E.N., E.V.G., J.C.C.P., M.M.F., and J.E.V.R.; Writing – Original Draft Preparation, L.R.R.P.; Writing – Review & Editing, L.R.R.P.; Visualization, P.C.R., L.C.G., M.E.N., E.V.G., J.C.C.P., M.M.F., and J.E.V.R.; Supervision, L.R.R.P.; Funding Acquisition, J.E.V.R. L.R.R.P.: Attending surgeon specialized in Orthopedic Oncology. Main surgeon of the cases, involved in drafting and revising of the manuscript. Corresponding author. Developed the study concept, did the final data analysis and provided the major clinical input in writing and revising of the manuscript. P.C.R.: Attending surgeon specialized in Orthopedic Oncology. She took part in the patient's surgery and contacted her to acquire the data for the study. She was involved in methodology and revising of the manuscript. L.C.G.: Attending surgeon specialized in Orthopedic Oncology. She contacted with the patient to acquire the data for the study. She was involved in revising of the manuscript. M.E.N.: Attending surgeon specialized in Orthopedic Oncology. He took part in the patient's surgery. She was involved in revising of the manuscript. E.V.G.: Attending surgeon specialized in Gynaecology and Obstetrics. She participated in the follow-up of the patient's pregnancy and delivery. She was involved in revising of the manuscript. J.C.C.P.: Attending surgeon specialized in Orthopedic Oncology. He was involved in revising of the manuscript. M.M.F.: Attending surgeon specialized in Orthopedic Oncology. She initially treated patient number 2 and referred her to our hospital. She was involved in revising of the manuscript. J.E.V.R.: Attending surgeon specialized in Orthopedic. He was involved in methodology and revising of the manuscript. Each autor has contributed significantly to, and is willing to take public responsibility for this study: its design, data acquisition, and analysis and interpretation of data. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the ethics committee of the Instituto de Investigación +12, University Hospital 12 de Octubre, Madrid (2024).
Informed Consent Statement
Informed consent was obtained from the surviving patient included in this study. For non-surviving patient, data were irreversibly anonymized, as recommended by the ethics committee.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
All authors have no financial and personal relationships with other people or organizations that could inappropriately influence (bias) this work.
Abbreviations
AJCC: American Joint Committee on Cancer; MRI: Magnetic Resonance Imaging; MSTS: Musculoskeletal Tumor Society; STS: soft tissue sarcoma.
References
- Enneking, W.F.; Dunham, W.K. Resection and reconstruction for primary neoplasms involving the innominate bone. J. Bone Joint Surg. Am. 1978, 60, 731–746. [Google Scholar] [CrossRef]
- Benady, A.; Gortzak, Y.; Sofer, S.; Ran, Y.; Rumack, N.; Elias, A.; Efrima, B.; Golden, E.; Segal, O.; Merose, O.; et al. Internal Hemipelvectomy for primary bone sarcomas using intraoperative patient specific instruments- the next step in limb salvage concept. BMC Musculoskelet. Disord. 2022, 23, 1012. [Google Scholar] [CrossRef]
- Crimì, A.; Binitie, O.T.; Crimì, F.; Letson, G.D.; Joyce, D.M. Outcomes and complications of pelvic chondrosarcomas treated using navigation guidance and multidisciplinary approach: Is the tumor volume a prognostic factor? J. Clin. Med. 2022, 11, 7111. [Google Scholar] [CrossRef]
- Karaka, M.O.; Özbek, E.A.; Özyildiran, M.; Merter, A.; Basarir, K.; Yildez, H.Y.; Sağlık, Y. External and internal hemipelvectomy: a retrospective análisis of 68 cases. Jt. Dis. Relat. Surg. 2022, 33, 132–141. [Google Scholar] [CrossRef] [PubMed]
- Laitinen, M.K.; Parry, M.C.; Albergo, J.I.; Grimer, R.J.; Jeys, L.M. Is computer navigation when used in the surgery of iliosacral pelvic bone tumours safer for the patient? Bone Joint J. 2017, 99-B, 261–266. [Google Scholar] [CrossRef]
- Wang, J.; Min, L.; Lu, M.; Zhang, Y.; Wang, Y.; Luo, Y.; Zhou, Y.; Duan, H.; Tu, C. What are the complications of three-dimensionally printed, custom-made, integrative hemipelvic endoprostheses in patients with primary malignancies involving the acetabulum, and whats is the function of these patients? Clin. Orthop. Relat. Res. 2020, 478, 2487–2501. [Google Scholar] [CrossRef] [PubMed]
- Lewis, V.O.; Kemp, A.; Roubaud, M.J.; Ajay, D.; Westney, O.L.; Smith, T. 3rd.; Dang, A.Q.; Hagan, K.; Roland, C.L.; Penny. A.; et al. Multidisciplinary approach to hemipelvectomy for pelvic sarcomas. JBJS Rev. 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Malawer, M.M.; Buch, R.G.; Thompson, W.E.; Sugarbaker, P.H. Major amputations done with palliative intent in the treatment of local bony complications associated with advanced cancer. J. Surg. Oncol. 1991, 47, 121–130. [Google Scholar] [CrossRef]
- Chretien, P.A.; Sugarbaker, P.H. Surgical technique of hemipelvectomy in the lateral position. Surgery 1981, 90, 900–909. [Google Scholar]
- Karakousis, C.P.; Emrich, L.J.; Driscoll, D.L. Variants of hemipelvectomy and their complications. Am. J. Surg. 1989, 158, 404–408. [Google Scholar] [CrossRef]
- Chandrasekhar, B.; Sloan, G.M.; Beatty, J.D. The external oblique myoscutaneous flap for extended hemipelvectomy reconstruction. Cancer 1988, 62, 1022–1025. [Google Scholar] [CrossRef] [PubMed]
- Roulet, S.; Le Nail, L.R.; Vaz, G.; Babinet, A.; Dumaine, V.; Sallot, A.; Rosset, P. Free fillet lower leg flap for coverage after hemipelvectomy or hip disarticulation. Orthop. Traumatol. Surg. Res. 2019, 105, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Apffelstaedt, J.P.; Driscoll, D.L.; Spellman, J.E.; Velez, A.F.; Gibbs, J.F.; Karakousis, C.P. Complications and outcome of external hemipelvectomy in the management of pelvic tumors. Ann. Surg. Oncol. 1996, 3, 304–309. [Google Scholar] [CrossRef]
- Asavamongkolkul, A.; Chotikawanich, E. Late distal ureteral structure in internal hemipelvectomy without bone reconstruction: A case report. Res. Rep. Urol. 2022, 14, 275–280. [Google Scholar]
- Balko, J.; Ozaniak, A.; Krskova, L.; Strizova, Z.; Lischke, R.; Zamecnik, J. Patient with composite haemangioendothelioma containing angiosarcoma-like areas in the setting of congenital lymphoedema mimicking Stewart-Treves syndrome: a case report. Diagn. Pathol. 2023, 18, 76. [Google Scholar] [CrossRef] [PubMed]
- Kayani, B.; Clarkson, P.; Ng, T.; Masri, B.A. A sarcoma masquerading as a pseudotumor after total hip arthroplasty: A case report. JBJS Case Connect. 2023, 13. [Google Scholar] [CrossRef]
- Kumar, R.; Mohanan, S. Periosteal Ewing sarcoma: Imaging features and clinical outcomes in 7 patients. J. Comput. Assist. Tomogr. 2023, 47, 78–85. [Google Scholar] [CrossRef]
- Mahran, M.A.; Khalifa, A.A.; El-Sayed, A. Pelvis reconstruction by proximal femur upshifting and total hip arthroplasty after radical resection of an adolescent patient pelvic Ewing's sarcoma, a case report, and literature review. Int. J. Surg. Case Rep. 2023, 106, 108146. [Google Scholar] [CrossRef]
- Papalia, G.F.; Ariyaratne, S.; Sison, J.; Morris, G.; Vaiyapuri, S.; Kurisunkal, V.; Botchu, R. An unusual cystic presentation of pelvic skeletal Ewing sarcoma: a case series. Skeletal Radiol. 2024, 16. [Google Scholar] [CrossRef]
- Sag, A.A.; Riedel, R.F.; Eward, W.C.; Visgauss, J.D.; Brigman, B.E. Hydropneumodissection-assisted cryoablation of recurrent sarcoma adjacent to the sciatic nerve as a limb-sparing alternative to hindquarter amputation. J. Vasc. Interv. Radiol. 2023, 34, 923–926. [Google Scholar] [CrossRef]
- Baines, A.J.; Babazadeh-Naseri, A.; Dunbar, N.J.; Lewis, V.O.; Fregly, B.J. Bilatera asymmetry of bone density adjacent to pelvic sarcomas: A retrospective study using computed tomography. J. Orthop. Res. 2022, 40, 644–653. [Google Scholar] [CrossRef] [PubMed]
- Dunbar, N.J.; Zhu, Y.M.; Madewell, J.E.; Penny, A.N.; Fregly, B.J.; Lewis, V.O. Changes in psoas muscle size and ambulatory function after internal hemipelvectomy without reconstruction. Bone Joint J. 2023, 105-B, 323–330. [Google Scholar] [CrossRef]
- Dvorak, Z.; Tomas, T.; Kubat, M.; Apostolopoulos, V.; Tawa, N. Free fillet lower leg flap with fenestration of the pelvis as prevention of vascular problem after hemipelvectomy. J. Plast. Reconstr. Aesthet. Surg. 2022, 75, 2845–2846. [Google Scholar] [CrossRef] [PubMed]
- Gosheger, G.; Ahrens, H.; Dreher, P.; Schneider, K.N.; Deventer, N.; Budny, T.; Heitkötter, B.; Schulze, M.; Theil, C. Evaluation of a novel classification system to predict local recurrence in sarcoma patients undergoing hemipelvectomy with iliosacral resection. Bone Joint J. 2022, 104-B, 290–296. [Google Scholar] [CrossRef]
- Hu, X.; Wen, Y.; Lu, M.; Luo, Y.; Zhou, Y.; Yang, X.; Tu, C.; Min, L. Biomechanical and clinical outcomes of 3D-printed versus modular hemipelvic prostheses for limb- salvage reconstruction following periacetabular tumor resection: a mid-term retrospective cohort study. J. Orthop. Surg. Res. 2024, 19, 258. [Google Scholar] [CrossRef]
- Khal, A.; Zucchini, R.; Sambri, A.; Leucuta, D.C.; Mariotti, F.; Donati, D.M.; De Paolis, M. Reconstruction of the pelvic ring in iliac or iliosacral resections: allograft or autograft? Musculoskelet. Surg. 2022, 106, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Lizcano-Suárez, A.R.; Clara-Altamirano, M.A.; Velázquez-Rodríguez, S.; Martínez-Said, H.; Villavicencio-Valencia, S.V.; García-Ortega, D.Y. Surgical margins as prognostic factor in pelvis chondrosarcoma. Cohort study in a sarcoma unit. Acta Ortop. Mex. 2023, 37, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Revuri, V.R.; Moody, K.; Lewis, V.; Mejia, R.; Harrison, D.J.; Ahmad, A.H. Pain and analgesia in children with cancer after hemipelvectomy: A retrospective analysis. Children (Basel) 2022, 9, 237. [Google Scholar] [CrossRef]
- Sambri, A.; Fiore, M.; Rottoli, M.; Bianchi, G.; Pignatti, M.; Bortoli, M.; Ercolino, A.; Ancetti, S.; Perrone, A.M.; De Iaco, P.; et al. A planned multidisciplinary surgical approach to treat primary pelvic malignancies. Curr. Oncol. 2023, 30, 1106–1115. [Google Scholar] [CrossRef]
- Vucicevic, R.S.; Zavras, A.G.; Fice, M.P.; Khan, Z.A.; Gusho, C.; Gasparro, M.; Gitelis, S.; Blank, A.; Colman, M.W. Internal hemipelvectomy: A single institution's learning curve and longitudinal experience. J. Surg. Oncol. 2024, 129, 981–994. [Google Scholar] [CrossRef]
- Zhang, L.; Michihata, N.; Matsui, H.; Fushimi, K.; Yasunaga, H.; Tsuda, Y.; Tanaka, S.; Kobayashi, H. Preoperative arterial embolization and wound complications after resection of malignant bone tumor in the pelvis: a nationwide database study. Jpn. J. Clin. Oncol. 2022, 52, 1176–1182. [Google Scholar] [CrossRef]
- Banskota, N.; Yang, H.; Fang, X.; Yuan, D.; Zhang, W.; Duan, H. Comparative study of pelvic sarcoma patients undergoing internal and external hemipelvectomy: A meta-analysis study. Front Surg. 2022, 9, 988331. [Google Scholar] [CrossRef] [PubMed]
- Laitinen, M.K.; Parry, M.C.; Morris, G.V.; Jeys, L.M. Pelvic bone sarcomas, prognostic factors, and treatment: A narrative review of the literature. Scand. J. Surg. 2023, 112, 206–215. [Google Scholar] [CrossRef]
- Roustemis, A.G.; Liontos, M.; Trikoupis, I.; Karampikas, V.; Goumenos, S.; Gavriil, P.; Kontogeorgakos, V.A.; Savvidou, O.; Papagelopoulos, P.J. Limb salvage and pelvic reconstruction with endoprosthesis after pelvic tumor resection: A narrative review. Cureus. 2024, 16, e56043. [Google Scholar] [CrossRef]
- Endo, Y.; Sakai, T.; Fukui, S.; Hori, A.; Echigo, R.; Matsunaga, S.; Kadosawa, T. Mid-to-caudal partial hemipelvectomy with limb preservation for ischial tumor in a dog. J. Vet. Med. Sci. 2022, 84, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Stokes, R.; Wustefeld-Janssens, B.G.; Hinson, W.; Wiener, D.J.; Hollenbeck, D.; Bertran, J.; Mickelson, M.; Chen, C.L.; Selmic, L.; Aly, A.; et al. Surgical and oncologic outcomes in dogs with malignant peripheral nerve sheath tumours arising from the brachial or lumbosacral plexus. Vet. Comp. Oncol. 2023, 21, 739–747. [Google Scholar] [CrossRef]
- Sullivan, M.H.; Mills, G.L.; Saifuddin, H.; Brinkman, E.J.; Carlsen, B.T.; Moran, S.L.; Houdek, M.T. Targeted muscle reinnervation to reduce postoperative pain in patients undergoing hindquarter resections. Anticancer Res. 2023, 43, 3513–3516. [Google Scholar] [CrossRef]
- Vega, M.M.; Li, G.; Shourijeh, M.S.; Ao, D.; Weinschenk, R.C.; Patten, C.; Font-Llagunes, J.M.; Lewis, V.O.; Fregly, B.J. Computational evaluation of psoas muscle influence on walking function following internal hemipelvectomy with reconstruction. Front Bioeng. Biotechnol. 2022, 10, 855870. [Google Scholar] [CrossRef]
- Kirilova, M.; Klein, A.; Lindner, L.H.; Nachbichler, S.; Knösel, T.; Birkenmaier, C.; Baur-Melnyk, A.; Dürr, H.R. Amputation for extremity sarcoma: indications and outcomes. Cancers (Basel) 2021, 13, 5125. [Google Scholar] [CrossRef]
- Browne, J.L.; Oudijk, M.A.; Holtslag, H.R.; Schereuder, H.W.R. Vaginal delivery after hemipelvectomy and pelvic radiotherapy for condrosarcoma. BMJ Case Rep. 2014, 2014, bcr2014205785. [Google Scholar] [CrossRef] [PubMed]
- Couto, A.G.H.; Araújo, B.; Torres de Vasconcelos, R.A.; Renni, M.J.; Da Fonseca, C.O.; Cavalcanti, L. Survival rate and perioperative data of patients who have undergone hemipelvectomý: a retrospective case series. World J. Surg. Oncol. 2016, 14, 255. [Google Scholar] [CrossRef] [PubMed]
- Beck, L.A.; Einertson, M.J.; Winemiller, M.H.; DePompolo, R.W.; Hoppe, K.M.; Sim, F.F. Functional outcomes and quality of life after tumor-related hemipelvectomy. Phys. Ther. 2008, 88, 916–927. [Google Scholar] [CrossRef]
- Guder, W.K.; Hardes, J.; Gosheger, G.; Henrichs, M.P.; Nottrott, M.; Streitbürger, A. Analysis of surgical and oncological outcome in internal and external hemipelvectomy in 34 patients above the age of 65 years at a mean follow-up of 56 months. BMC Musculoskeletal Disorders 2015, 16, 33. [Google Scholar] [CrossRef] [PubMed]
- Rena de Freitas, R.; Soares Crivellaro, A.L.; Pauka Mello, G.J.; Armani Neto, M.; De Freitas Filho, G.; Viani da Silva, L. Hemipelvectomy: Erasto Gaertner Hospital´s experiences with 32 cases in 10 years. Rev. Bras. Orthop. 2015, 45, 413–419. [Google Scholar] [CrossRef]
- Angelini, A.; Drago, G.; Trovarelli, G.; Calabrò, T.; Ruggieri, P. Infection after surgical resection for pelvic bone tumors: an analysis of 270 patients from one institution. Clin. Orthop. Relat. Res. 2014, 472, 349–359. [Google Scholar] [CrossRef]
- Baliski, C.R.; Schachar, N.S.; McKinnon, J.G.; Stuart, G.C.; Temple, W.J. Hemipelvectomy: a changing perspective for a rare procedure. Can. J. Surg. 2004, 47, 99–103. [Google Scholar]
- Yuen. A.; Ek, E.T.; Choong, P.F. Research: is resection of tumours involving pelvic ring justified? A review of 49 consecutive cases. Int. Semin. Surg. Oncol. 2005, 2, 9. [Google Scholar] [CrossRef]
- Sherman, C.E.; O´Connor, M.I.; Sim, F.H. Survival, local recurrence, and function after pelvic limb salvage at 23 to 38 years of followup. Clin. Orthop. Relat. Res. 2012, 470, 712–727. [Google Scholar] [CrossRef] [PubMed]
- Bruns, J.; Luessenhop, S.; Behrens, P. Cost análisis of three different surgical procedures for treatment of a pelvic tumour. Langenbeck´s Arch. Surg. 1998, 383, 359–363. [Google Scholar] [CrossRef]
- Heetkamp, A.; Feijen, H.W.H.; Papatsonis, D.N.M. Spontaneous delivery after hemipelvectomy because of condrosarcoma: a case report and review of the literature. Am. J. Perinatol. 2008, 25, 255–258. [Google Scholar] [CrossRef]
- Bergh, P.A.; Bonamo, J.; Breen, J.L. Pregnancy after hemipelvectomy: a case report and review of the literature. Int. J. Gynaecol. Obstet. 1988, 27, 277–283. [Google Scholar] [CrossRef]
- Chihara, I.G.; Osada, H.; Litsuka, Y.; Masuda, K.; Sekiya, S. Pregnancy after limb-sparing hemipelvectomy for Ewgin´s sarcoma. A case report and review of the literature. Gynecol. Obstet. Invest. 2003, 56, 218–220. [Google Scholar] [CrossRef]
- Snyder, D.J.; Thomas, R.L. Pregnancy complicated by hemipelvectomy: case presentations and review of the literature. Am. J. Perinatol. 1989, 6, 363–366. [Google Scholar] [CrossRef]
- Kakogawa, J.; Ogawa, M.; Suzuki, N. Tabata, T. Successful pregnancy after limb-sparing hemipelvectomy for Ewing sarcoma: Case report and literature review. Taiwan J. Obstet. Gynecol. 2021, 60, 787–790. [Google Scholar] [CrossRef]
Figure 1.
Case 1. Clinical appearance (A) and coronal and axial magnetic resonance images (B,C,D).
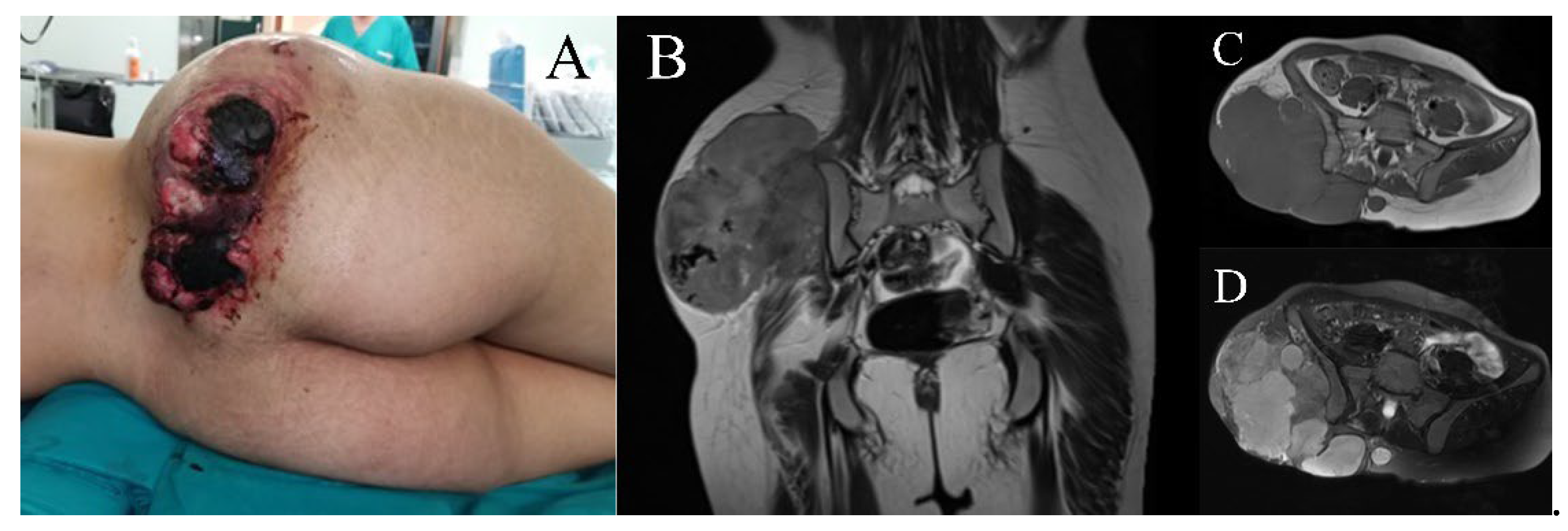
Figure 2.
Case 1. Control arteriography for preoperative embolization.
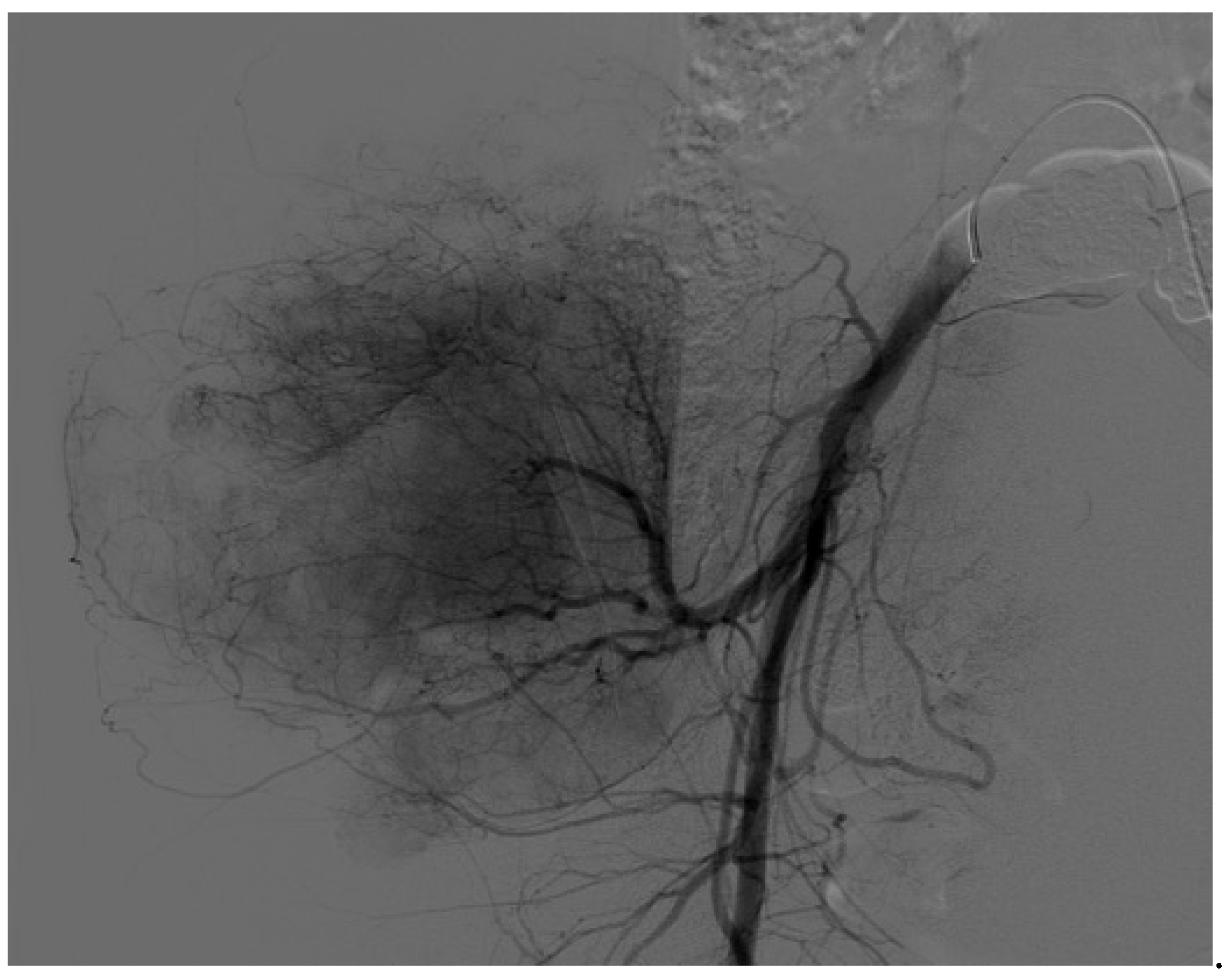
Figure 3.
Case 1. Surgical details of anterior flap hemipelvectomy, showing the femoral neurovascular bundle (A) and final coverage aspect (B). Amputation specimen (C) and postoperative radiography (D).
Figure 3.
Case 1. Surgical details of anterior flap hemipelvectomy, showing the femoral neurovascular bundle (A) and final coverage aspect (B). Amputation specimen (C) and postoperative radiography (D).
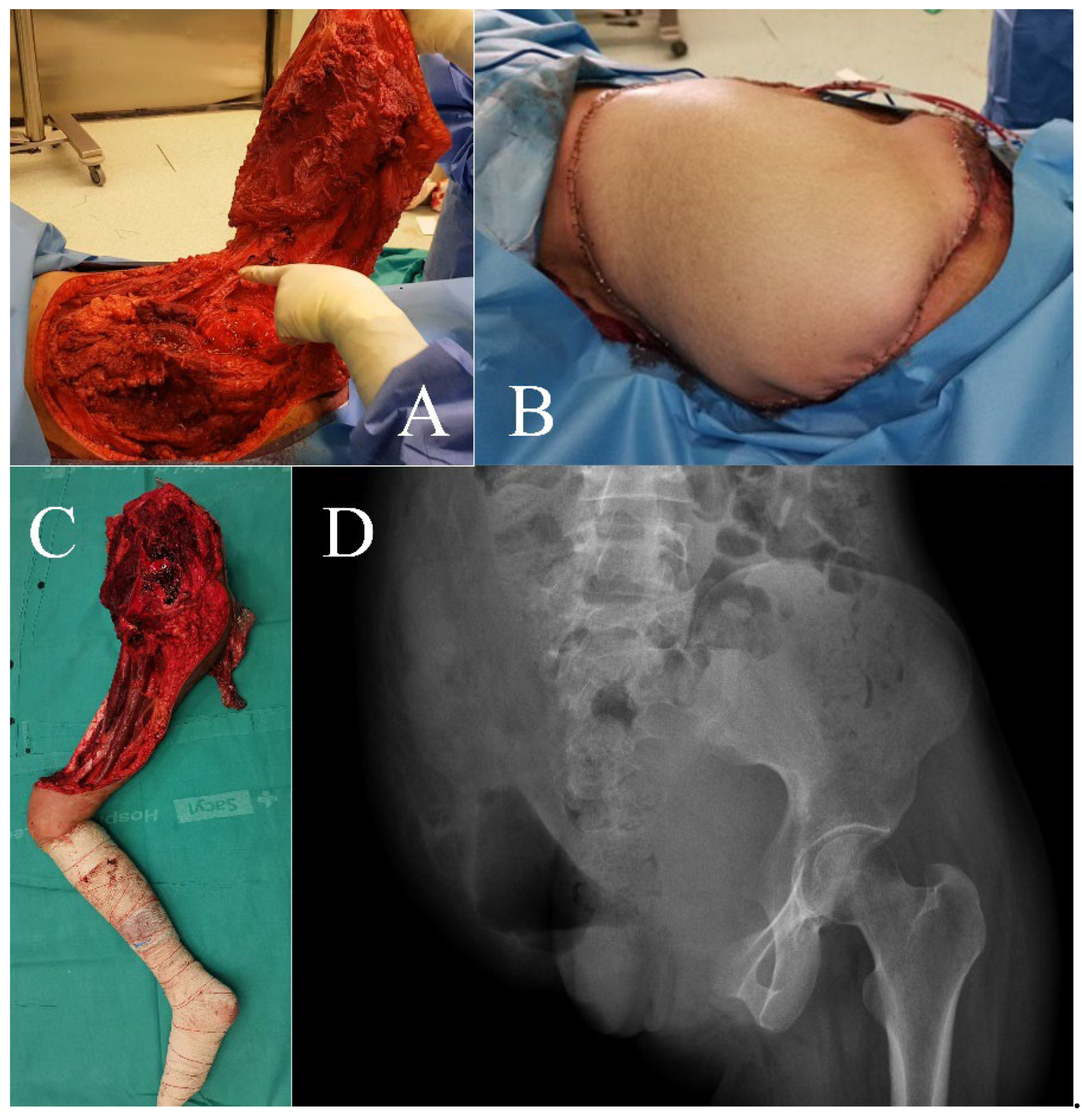
Figure 4.
Case 2. Clinical appearance of the patient.
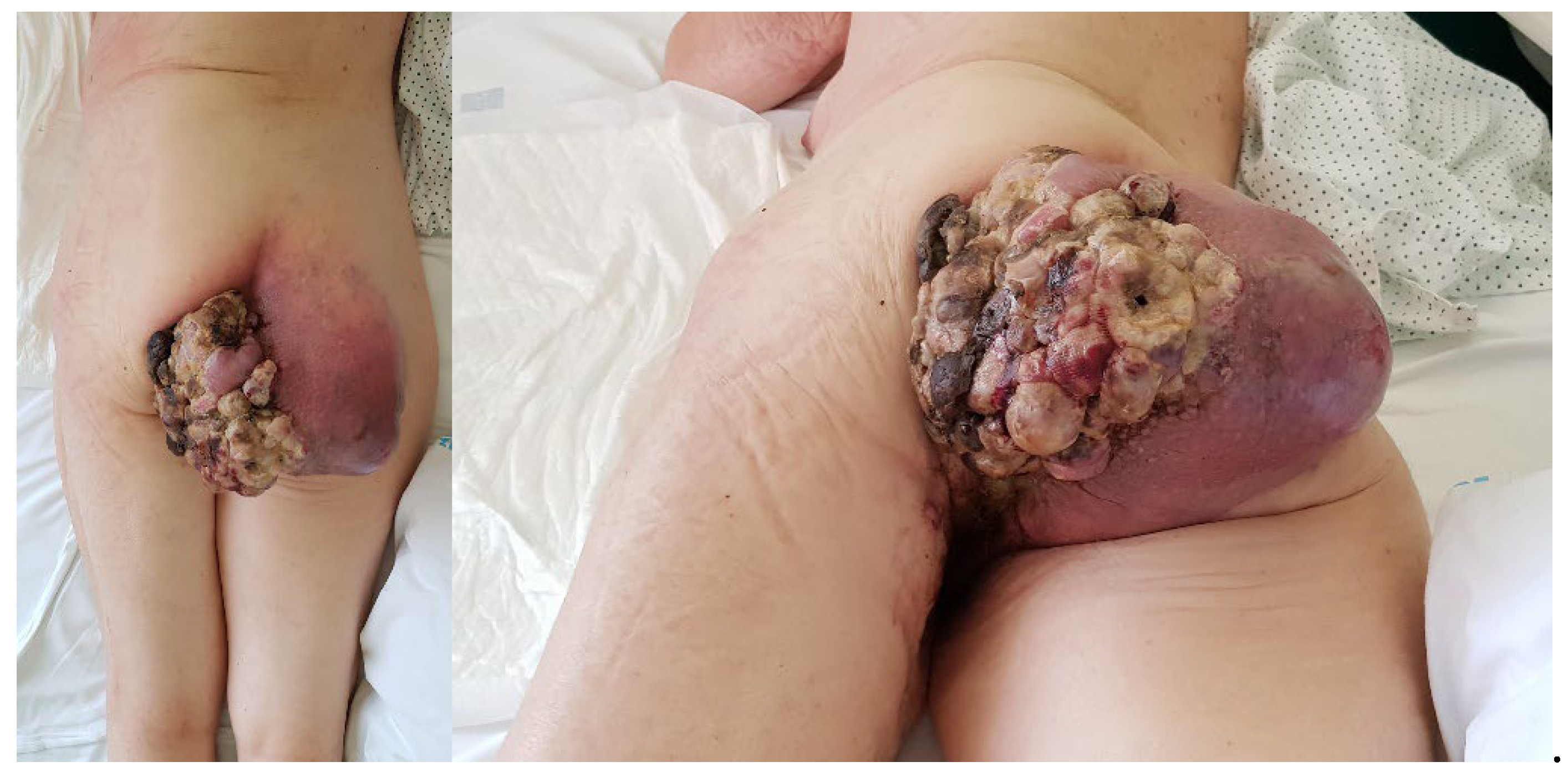
Figure 5.
Case 2. Coronal (A), axial (B), and sagittal (C) magnetic resonance images.
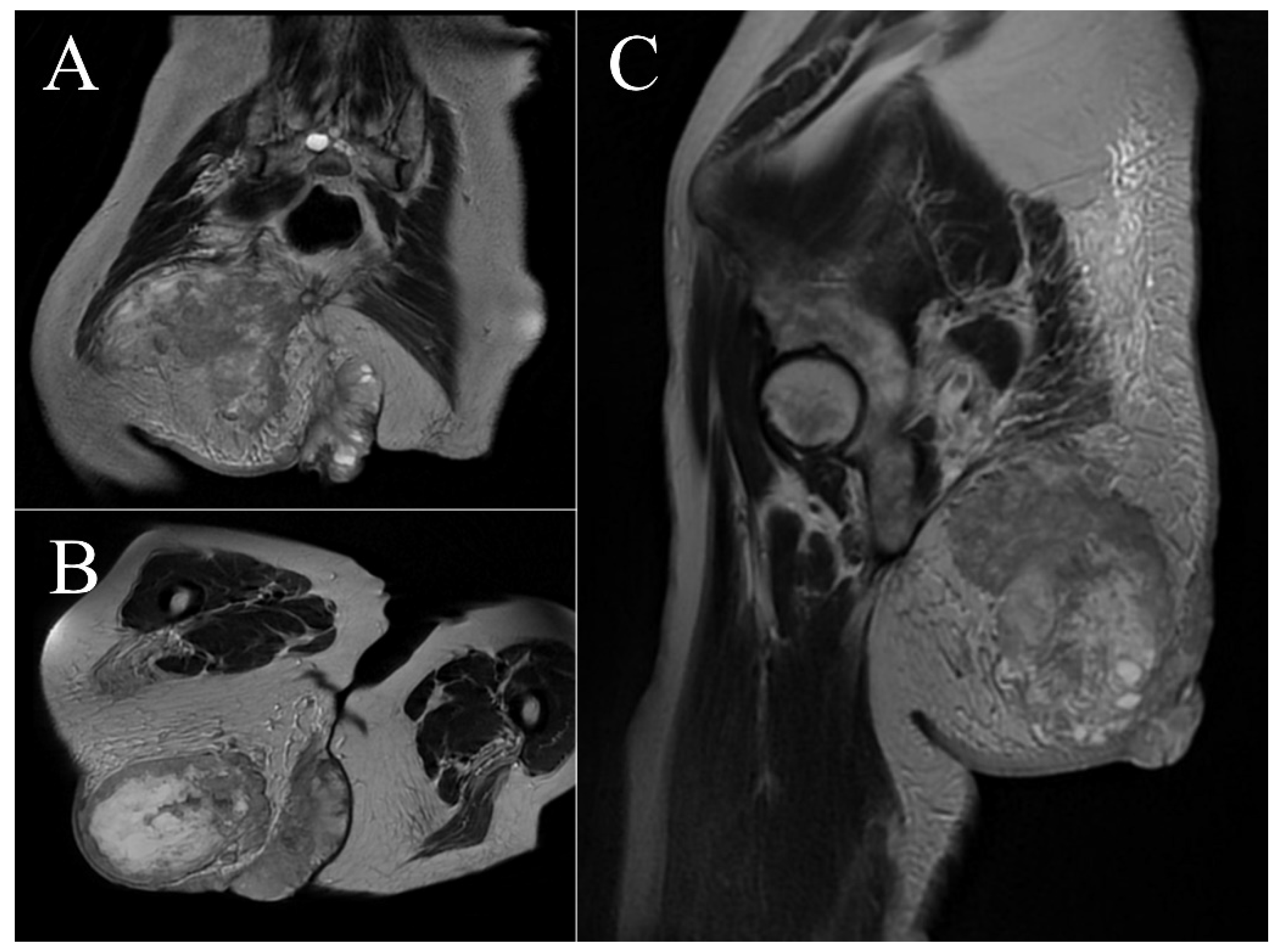
Figure 6.
Case 2. Surgical details of anterior flap hemipelvectomy (A), amputation specimen (B,C), and final clinical aspect with the associated colostomy (D).
Figure 6.
Case 2. Surgical details of anterior flap hemipelvectomy (A), amputation specimen (B,C), and final clinical aspect with the associated colostomy (D).
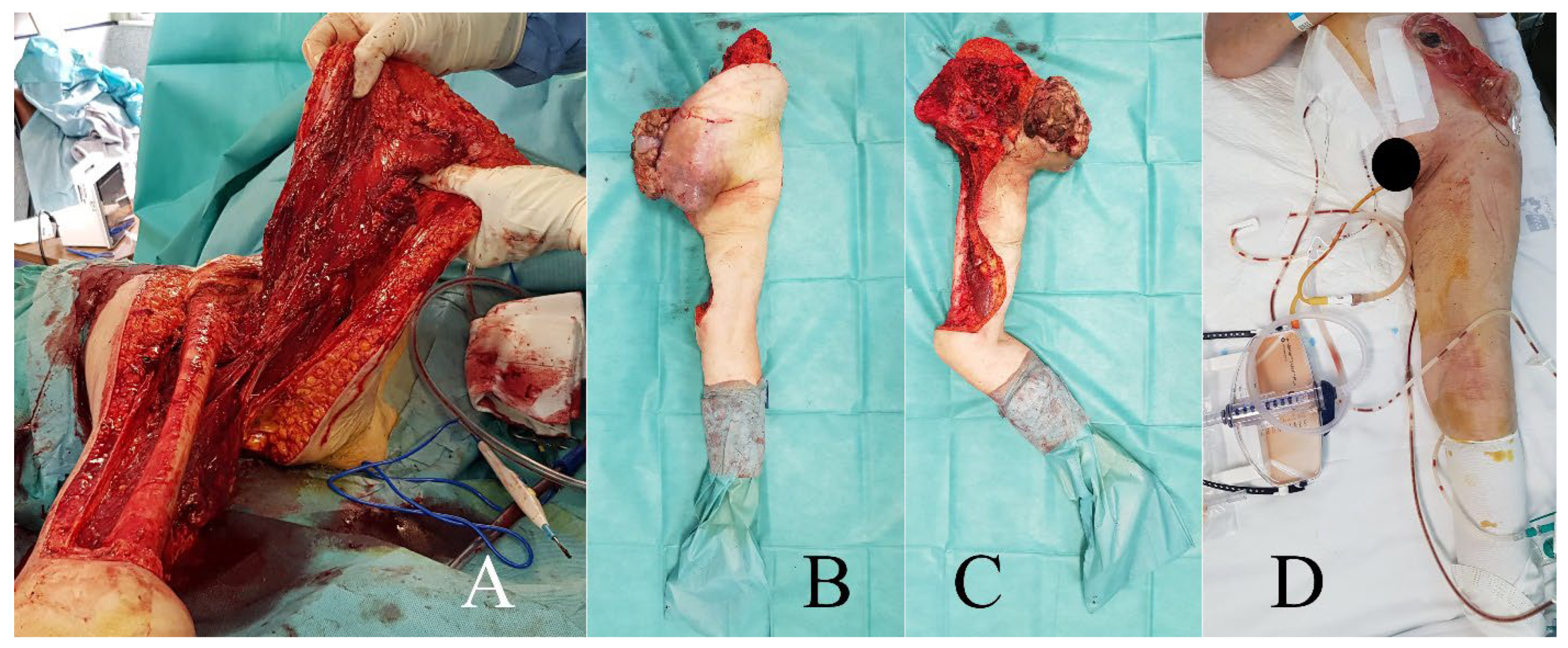
Figure 7.
Case 1. Ultrasound assessment of the patient’s pregnancy, showing the fetus in the uterine cavity.
Figure 7.
Case 1. Ultrasound assessment of the patient’s pregnancy, showing the fetus in the uterine cavity.
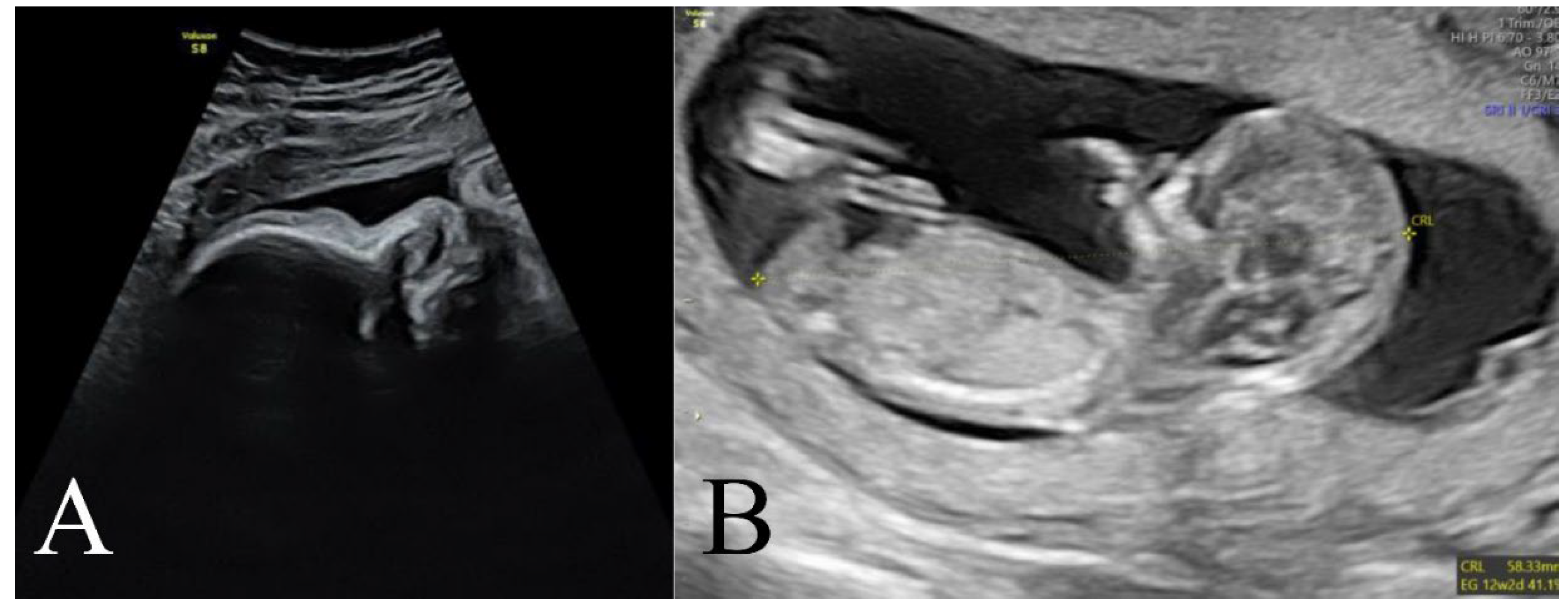
Figure 8.
Case 1. Clinical appearance of the patient at the time of delivery.
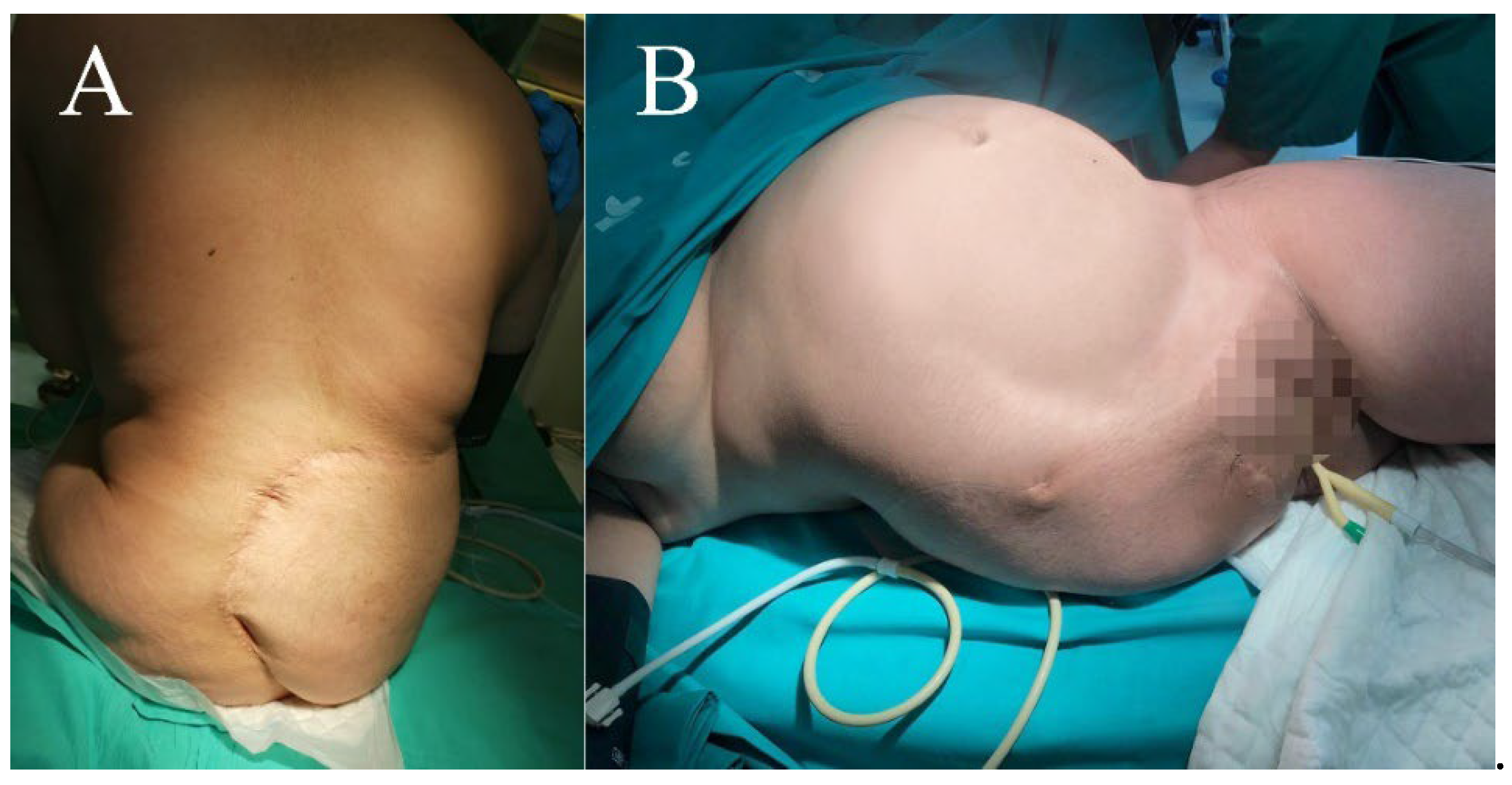
Figure 9.
Case 1. Clinical appearance of the patient at different timepoints of functional recovery.
Figure 9.
Case 1. Clinical appearance of the patient at different timepoints of functional recovery.
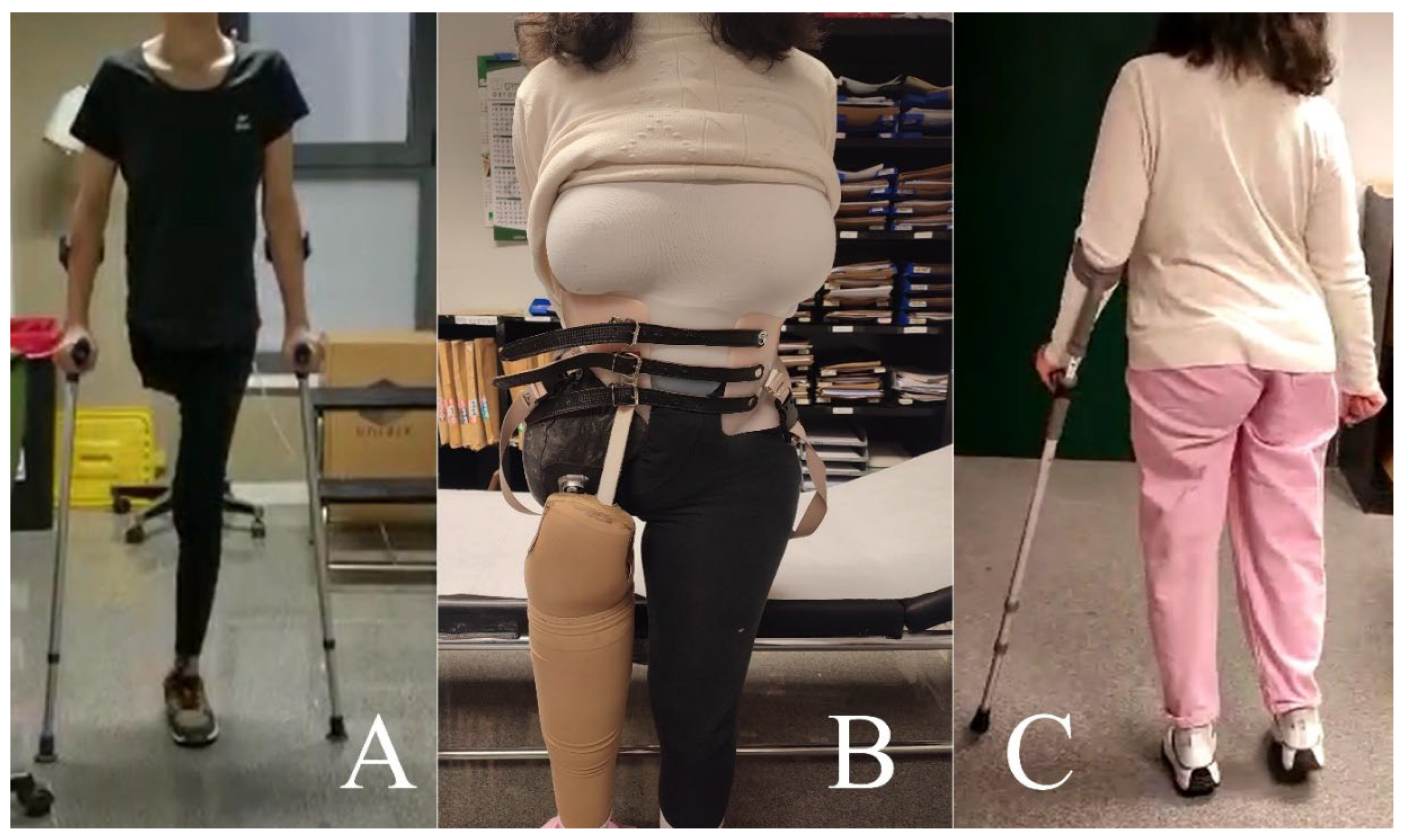
Figure 10.
Case 2. Postoperative computed tomography scan of the patient showing the extended hemipelvectomy and tumor recurrence.
Figure 10.
Case 2. Postoperative computed tomography scan of the patient showing the extended hemipelvectomy and tumor recurrence.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



