
Submitted:
02 September 2024
Posted:
03 September 2024
You are already at the latest version
Abstract
Little is known about skeletal muscle thickness, echogenicity, and muscle quality (handgrip strength /muscle thickness) in breast cancer-related lymphedema (BCRL). Using B-mode ultrasound, we recorded the raw radiofrequency data of the affected (AA) and unaffected (UA) arms of women (n=20) with BCRL, and in 20 control women with no lymphedema (CA). The data were converted into images and measurements of skin, subcutaneous fat and muscle thickness were obtained. Within a designated region of interest, muscle echo-intensity was assessed using computer graded grey scale and muscle thickness was measured using ImageJ2. Handgrip strength was measured using standard dynamometry. We found that forearm muscle thickness was similar among AA, UA, and CA. When compared to the unaffected and control arms, the affected arm had a significantly higher (p 0.013) muscle echo-intensity. When compared to the AA, handgrip strength was similar to UA (p 0.401) but lower than CA (p 0.05). We conclude that the use of B-mode ultrasound is a reliable method to assess muscle thickness and EI in BCRL. When comparing AA to UA, the elevated levels of muscle EI in AA did not influence strength or muscle quality. The elevated EI in AA is a marker of abnormal health that needs to be further explored.
Keywords:
breast cancer-related lymphedema
; ultrasound
; skeletal muscle thickness
; muscle echo intensity
; muscle quality
1. Introduction
Breast cancer-related lymphedema (BCRL) is a common yet misunderstood condition and is associated with significant changes in tissue composition of the affected arm. Using ultrasound techniques, it is common to observe that forearm skin [1,2,3,4,5] and subcutaneous fat thickness [5,6,7,8] in the lymphedema arm are significantly greater than the contralateral arms. To date, the few studies that have examined the skeletal muscle size (thickness and volume) in BCRL have shown inconsistent findings. In studies using MRI protocols, skeletal muscle volume has displayed no differences between the affected and unaffected arm [9,10]. Conversely, Brorson et al. [11] found a significant increase in muscle mass while Jeon et al. [12] reported a decrease in muscle thickness in the arm with lymphedema. Moreover, Crescenzi et al. [10] found no differences in muscle volume of the affected arm when compared to the arms of a group of healthy women. More clarity is needed with the measurement of muscle thickness and volume, especially since muscle thickness is an important component for the development of muscle strength [13]. However, there is no study that has compared muscle thickness with strength development in BCRL.
It is well known that there is normally a strong positive correlation between skeletal muscle size and strength development. In healthy individuals, forearm muscle thickness is an important physiological factor that contributes to handgrip strength [13,14,15]. Increases in forearm muscle thickness has been correlated with an increase in handgrip strength [14]. With respect to women with BCRL, there are several studies that have measured handgrip strength but none has related it to muscle forearm thickness. Moreover, measurements of maximal voluntary isometric contraction between the affected and unaffected arms have been inconsistent with some studies reporting decreases in the affected arm strength when compared to the contralateral limb [16,17,18] while others have shown no differences between arms [19,20,21,22]. The differences in muscle strength among BCRL studies may be related to some component within skeletal muscle itself. One important factor that could possibly influence strength development is a change in muscle echo intensity that could affect muscle quality. What role does echo intensity and skeletal muscle quality (forearm strength development per unit of muscle thickness) play in handgrip strength output in BCRL remains to be seen.
Skeletal muscle quality may be more functionally important and relevant measure than simple muscle mass or thickness as it incorporates echo intensity. A promising ultrasonic measure of muscle health is echo intensity that is characterized by hypoechogenic (dark) regions representing fluid and skeletal muscle protein while the hyperechogenic “white streaks” identify non-contractile, intramuscular elements such as adipose tissue and fibro-collagen lesions [23,24]. Stock and Thompson [25] have reported numerous studies that have used B-mode ultrasound derived echo intensity to identify functional declines in muscle strength. Echo intensity has been shown to be related to muscle quality (ratio of handgrip strength to a unit of muscle thickness) and it has been found to better identify skeletal muscle functional deficits in the elderly population [26,27]. Furthermore, Aruna et al. [14] showed that as forearm muscle echo intensity increased, handgrip strength decreased in both young men and women. Thus, this index of forearm muscle quality may provide a more realistic and clinically relevant assessment of functional arm capacity in BCRL. To date, no study has compared echo intensity and muscle quality in the affected and unaffected arms of women with BCRL.
In the present study, we will describe tissue compositional changes in the affected and unaffected forearms in women with stage 2 BCRL. In particular, we will measure the forearm skeletal muscle thickness using B-mode ultrasound imaging with the intent to compare skeletal muscle thickness between the affected and unaffected arms. As well, we will compare the results of the BCRL group to a cohort of women without lymphedema. We will use this data to determine if muscle echo intensity of the affected forearms of BCRL is greater than that found in the unaffected and non-lymphedema control arms. This will be evident by greater amounts of hyperechogenic material present in the affected arm in BCRL. There has been no study that has confirmed the appearance of elevated echo intensity levels and its influence if any in the forearm musculature of women with BCRL. The results of this study will help us better describe important changes in skeletal muscle tissue composition and quality as well as the factors that may influence the health and functionality of skeletal muscle in the arms of women with BCRL.
2. Materials and Methods
2.1. Participants
A convenience sample of forty women was recruited: 20 women (56 ± 14.8 years) with Stage 2 BCRL from the McGill Lymphedema Research Program and an additional 20 women (48 ± 20.8 years) from the Montreal community who did not present with lymphedema. The women were matched according to their BMI. Certified lymphedema specialists classified the lymphedema stage according to the International Society of Lymphology guidelines. Inclusion criteria for the lymphedema group were: (1) unilateral Stage 2 BCRL in the stable, maintenance stage, and (2) had been treated for unilateral breast cancer. Inclusion criteria for the non-lymphedema control group were: (1) participants had no history of breast cancer, lymphedema, or any other inflammatory disease, and (2) were in generally good health. Exclusion criteria included the following: (1) women currently receiving treatment for breast cancer, (2) those who had lymphedema other than Stage 2 or bilaterally, and (3) who had been diagnosed with other diseases (e.g., liver, heart, kidney, etc.). Demographic data of the participants are found in Table 1.
This study was approved by the McGill University Health Centre Research Ethics Board (MUHC-REB). All patients provided written informed consent prior to participating in the study and had their height, weight, body composition, bilateral grip strength and ultrasound measurements taken in one clinic visit.
2.2. Anthropometrics
The weight of each participant was measured using a digital scale (Detecto, Model 750, ± 0.1 kg), and height measurements were taken against a wall mounted height scale (Seca, ± 0.1 cm).
2.3. Body Composition
All participants underwent a full-body dual-energy X-ray absorptiometry (DXA) scan to determine body composition (Lunar Prodigy Advance, GE Healthcare, Madison, WI, USA). Body fat (total, segmental and percentage) and lean body mass of each participant was calculated using enCORE 2006 v.10.50.086 software on Microsoft Windows XP. Each participant removed all jewelry and laid supine on the scanning bed with legs internally rotated using a plastic form with Velcro straps. Care was taken to ensure the participant was relaxed and lying with all limbs within scanning borders.
2.4. Perometry
Following the DXA scan, all participants underwent bilateral volumetric measurements with the Pero-System Type 350 NT (Peroplus 2000, 2014.). Patients were asked to sit with their legs uncrossed, with their feet flat on the floor with the knees flexed at a 90-degree angle. The Perometer was then adjusted accordingly to the participant’s height such that their arm was abducted to 90 degrees with the palm facing down and with the tip of the middle finger resting on the appropriate location of the machine. The machine was then moved along the length of the patient’s arm to obtain a volume measure of the entire arm.
2.5. Forearm Circumference
Participants were instructed to sit comfortably on a chair with their back rested and their arms in a supinated position on their thighs. Measurements were taken with a 100-cm cloth tape measure (+/- 0.1 cm) from the forearms approximately 10cm above the wrist landmark.
2.6. Handgrip Strength
Handgrip strength (HGS) was measured using a standard dynamometer (Jamar, Sammons Preston, Bolingbrook, IL) following previously validated procedures [28]. Briefly, each participant was seated comfortably in a chair with their shoulder fully adducted, elbow flexed to 90 degrees and their forearm parallel to their thigh, with their feet firmly planted on the floor. Two trials per side were completed with one minute of rest between trials. The highest value of the two trials was used.
2.7. Ultrasound Data Recording
Ultrasound (US) measurements were taken on the dorsum of the forearm at the proximal radial head (proximal forearm), approximately 20% of the distance between the olecranon and styloid process of the 5th digit. This landmark was denoted with skin safe ink to facilitate consistent US placement. Each participant was seated comfortably with the test arm resting palm down on a treatment table set at mid-chest height. The US radio-frequency data was collected using an Alpinion E-Cube 12 system (Bothell, WA, USA) with the L3-12H transducer with a center frequency of 10 MHz and the sampling rate of 40MHz. The US head was held perpendicular to a gel pad separating the transducer from the skin with ample gel on both sides. The use of a gel pad on the skin of the forearm was used to minimize any variation of surface compression caused by the probe. A single static, axial (head on view) image per location was recorded to an external USB storage device.
2.8. Data Conversion
This study used an US system capable of recording raw image data for post-processing of the images. The post-processing was conducted by an image analysis expert (JW) trained by a radiologist (MB) with a specialty in musculoskeletal imaging. Each data file contained radiofrequency data, and the pixel-by-pixel information used to create the image. Mathworks (Matlabs r2017b) scripting was used to strip non-image related data, and the remaining information was converted into an image. Open-source software, ImageJ2 (http://imagej.net) was then used to set the image scale (0.0288mm/pixel) and record measurements for tissue thickness and echo intensity.
Figure 1 demonstrates the 1 cm2 grid overlay that was placed on each image to ensure measurements for skin and subcutaneous fat were taken at the center. Skin thickness was measured from the bottom of the gel pad at the first set of echo intense lines (skin surface) to the next set of echo intense lines at the border of the subcutaneous fat. Subcutaneous fat thickness was measured from the bottom of the skin layer to the fascial layer covering the muscle. Skeletal muscle thickness was measured from the center of the radius at the bottom of the image up to the fascia separating the subcutaneous fat layer from the muscle. The muscles that are included in the thickness measurements include the brachioradialis, extensor carpi radialis longus, extensor carpi radialis brevis, and the supinator muscles.
Muscle echo intensity was also measured with ImageJ2. A rectangular selection was used to represent our region of interest (ROI) standardizing the measurement between images. The rectangular ROI dimensions for echo intensity was 25% of the muscle thickness by 500 pixels wide, centered at the point their muscle thickness was measured.
2.9. Statistical Analyses
All data were tested for normality using the Shapiro-Wilk test. For the analysis of paired means (AA vs UA), the Wilcoxon Signed-Rank test was used to determine differences in US and strength parameters (skin thickness, subcutaneous fat thickness, muscle thickness, echo intensity, handgrip strength, and muscle quality) and arm characteristics (total limb volume and forearm circumference). For the analysis of unpaired means (AA vs CA, UA vs CA), the Mann-Whitney U test was used. Spearman rank correlation was calculated to determine the association between subcutaneous fat thickness and echo intensity. Independent t-tests were used to compare the lymphedema and non-lymphedema group characteristics. To measure the intra-rater reliability, the means and standard deviations for the US parameters from measurement 1 and 2 were calculated dependent t-tests was used to assess systematic error and relative reliability (R) with the same evaluator. The threshold for statistical significance was set apriori at p ≤ 0.05. All values are shown as medians with interquartile ranges (IQR). Analyses were performed using NCSS Statistical Software, version 11 (329 North 1000 East, Kaysville, UT).
3. Results
3.1. Lymphedema and Non-Lymphedema Group Demographics and Clinical Data (Table 1):
The lymphedema group weighed more (p = 0.03), had a greater percent body fat (p = 0.023) and total fat (p = 0.021) compared to the non-lymphedema women. However, lean body mass (LBM) was not significantly different between groups (p = 0.363).
3.2. Total Limb Volumes and Forearm Circumferences (Table 2):
The total limb volume (TLV) of the affected limb was significantly (p≤0.05) larger than the contralateral side and there was an inter-limb difference of 327±433 ml. Furthermore, the forearm circumference (FC) of the affected arm was significantly greater than the unaffected (p≤0.022) and non-lymphedema control arms (p≤0.002).
3.3. Skin, Subcutaneous Fat, and Skeletal Muscle Thickness (Table 3):
Skin thickness (ST) in the affected arms was significantly greater than the unaffected (p≤0.001) and non-lymphedema control arms (p≤0.004). Similarly, subcutaneous fat thickness (FT) in the affected arms was also significantly greater than the unaffected (p≤0.001) and non-lymphedema control arms (p≤0.001) arms. However, skeletal muscle thickness (MT) showed no differences among the three groups.
3.4. Handgrip Strength (HGS), Muscle Echo-Intensity (MEI), and Muscle Quality (HGS/MT (Table 4)
Handgrip strength of the affected and unaffected arms was not different. However, HGS was significantly lower (p≤0.048) in the affected arm when compared to the non-lymphedema controls. The echo intensity of the affected arms was significantly greater than the unaffected (p≤0.013) and non-lymphedema control arms (p≤0.001). Muscle quality (HGS/MT) was significantly lower in the affected arm than the non-lymphedema control (p≤0.025) but not in the unaffected arm.
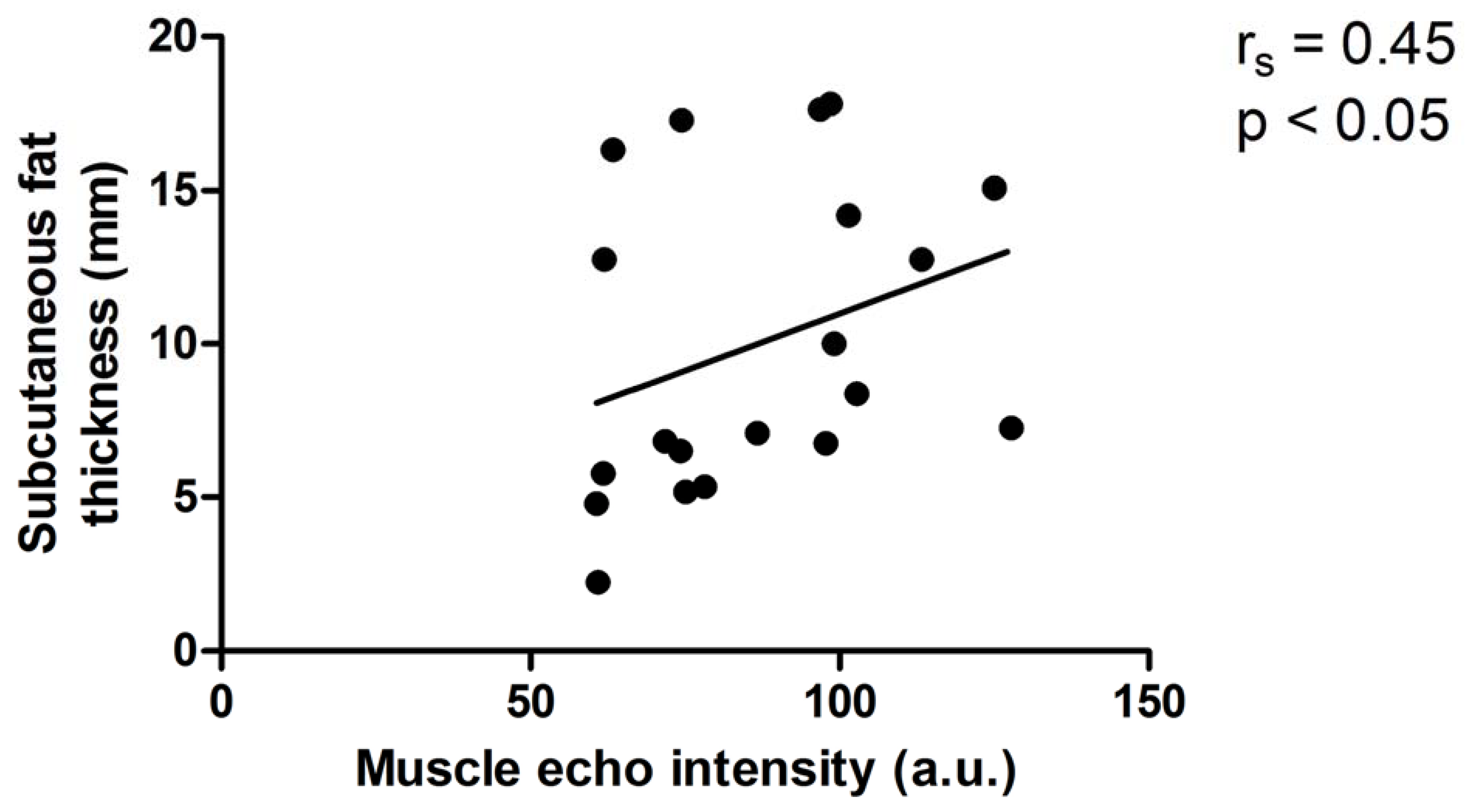
3.5. Relationships between 1) Subcutaneous Fat and Muscle Echo Intensity and 2) Forearm Circumference and Muscle Echo-Intensity in the Affected Arm (Figures 1&2)
Using Spearman rank correlation, there was a significant and positive relationship between subcutaneous fat thickness and muscle echo intensity (r=0.45, p≤0.05) in the affected arm.
3.6. Reliability of MT and MEI ultrasound analyses of the forearm images of the affected and unaffected arms. (Table 5)
The reliability for the MT and MEI values ranged from 0.990 to 0.995 and 0.839 to 0.996, respectively. The dependent t-tests across the two measurements evaluated systematic error and no bias was observed (p>0.05)
Figure 2.
Relationship between subcutaneous fat thickness and muscle echo intensity in the affected arm of women with lymphedema.
Figure 2.
Relationship between subcutaneous fat thickness and muscle echo intensity in the affected arm of women with lymphedema.
4. Discussion
The major findings in the present study were the following: 1) using B-mode ultrasound, forearm skeletal muscle thickness was similar in both the affected and unaffected arms of women with Stage 2 BCRL, as well as in the non-lymphedema controls, 2) muscle echo intensity was higher in the affected arm when compared to the unaffected and non-lymphedema controls, 3) handgrip strength was similar between the affected and unaffected arms despite a significantly greater echo intensity in the affected arm, and 4) there is a moderately positive correlation between subcutaneous fat thickness and skeletal muscle echo intensity in the affected arm.
Skeletal muscle thickness measurements in lymphedema have been inconsistent with reports showing decreases [12], increases [11], and no differences [9,10] between the affected and unaffected arms. Jeon et al 2017 has shown that the muscle thickness of the proximal and distal regions of affected arm are lower that the unaffected arm. On the other hand, Brorson et al. [11] reported a 47% increase in muscle tissue of the affected limb when compared to the contralateral side using dual energy x-ray absorptiometry (DXA). Using B-mode ultrasonography, we have found from image samples of the dorsal region of the forearm skeletal muscle that thickness was similar in both arms of BCRL and in the arms of the non-lymphedema control group. This coincides with others who have shown that the muscle volume in the axillary mid upper arm region measured by MRI techniques was similar in both the affected (4925.5±495.5 ml) and unaffected (4848.4±646.7 ml) of women with BCRL as well as in a non-lymphedema control group (5100.8±927.8 ml) [10]. Similarly, Borri et al. [9] also found that using magnetic resonance imagery and image segmentation protocols that skeletal muscle volumes in the affected and unaffected arms in women with BCRL were essentially the same. Several possible reasons for this discrepancy include the time the measurements were done during the progression of lymphedema, the level of physical condition and age of the women, and the overall volume and the specific location measured of the affected arm. Of course, the measurement tool and the protocol may also affect the accuracy and precision of skeletal muscle thickness. The studies that have utilized MRI techniques have incorporated the entire arm from wrist to axillary region [9] which would be a more representative measure than that of a cross-section image of a particular arm segment. Although MRI is considered to be the gold standard of skeletal muscle assessment and incorporates both qualitative and quantitative measures of skeletal muscle [29], B-mode ultrasound has been shown to be comparable to MRI [30,31]. Moreover, ultrasound has been shown to be very safe, has relative low purchase and usage cost, is more operator friendly, as well as practical and portable for clinical and bedside measurements. Our reliability data would indicate with R values ranging from 0.990 to 0.995 for muscle thickness and 0.839 to 0.995 for echo intensity that our measurement technique and assessment protocol were robust. In addition to measuring forearm tissue thickness composition using ultrasonography, we also assessed another important muscle tissue characteristic such as echo intensity, a variable that has yet to be assessed in the affected and unaffected arms of women with BCRL.
Skeletal muscle echo intensity (EI) has evolved into a popular, credible, and reliable mode of measurement to describe possible anatomical discrepancies within skeletal muscle based upon the pixel intensity of an ultrasound image [25]. It is believed that the lighter pixels reflect more intramuscular lipid and fibrous tissue [23,24] in the selected region of muscle tissue, whereas the darker pixels represent fluid and contractile properties. The increased EI (greater number of lighter pixels) in the affected arm generally reflects greater amounts of intramuscular adipose tissue and or fibrous collagen streaks [23,24]. Other studies have reported greater EI in skin and subcutaneous fat in arms with lymphedema [3]; however, there have been no previous reports about skeletal muscle EI in this population. In the present study, we have shown that EI significantly increased in the affected arm when compared to the contralateral unaffected limb and the non-lymphedema control arm. Others have found elevated in EI in the skeletal muscle of the young [14], the elderly [26,27] and those who are experiencing sarcopenia [25]. In a previous publication from our laboratory using a cohort of the participants in the present study, we reported that skeletal muscle tissue strain (more strain equals more compliant and healthy tissue) was significantly lower in the arm with lymphedema when compared to the unaffected limb [32]. Thus, if we consider the observations of increased EI and the reduced muscle tissue strain as seen in lymphedema, it suggests that there are serious differences in tissue composition in the affected arm when compared to the unaffected arm. The question arises as to the importance of this increase in EI in the affected arm. Does an increase in EI influence the strength development in the affected arm in this cohort of women with BCRL? There is ample evidence to show that muscle quality (handgrip strength / muscle thickness) is significantly and negatively affected by elevated EI [13,14,25].
Muscle strength is believed to be the most reliable and valid indicator of muscle function, and the handgrip strength test is the preferred mode of evaluating maximum isometric force production of the forearm (Robert et al. 2011). There are some published discrepancies in handgrip strength between the affected and unaffected arms in BCRL. Although several studies have observed a difference in grip strength between arms in BCRL [16,17,18], with the greater strength found in the unaffected arm; others have found no differences between arms [19,20,21,22]. Absolute grip strength in lymphedema patients ranged from 14.6 – 20.9 kgs [19,20] which was somewhat lower that the values of the affected (23.0 kg) and unaffected (23.3 kg) found in the present study. However, in this study the affected arm strength output was lower that the non-lymphedema group (27.9 kg) but not in in the unaffected arm. It should be pointed out that the normative grip strength for healthy women between the ages of 40-60 years of age is approximately 27 kg. [34,35,36]. Our mean value for muscle strength in the non-lymphedema group was 27.9 kg which was similar to the normative strength values for healthy Canadian women and it was significantly higher than the force output by the affected arm. The fact that we observed similar strength values in the affected and unaffected arms suggests that whatever factors explain the lower strength output than non-lymphedema controls is most likely systemic in nature and not localized to either arm in BCRL. It is quite possible that even after 10 years, the women with lymphedema were experiencing some negative health-related quality of life issues. Jorgensen et al. [37] have reported that the negative quality of life indices of arm heaviness, stiffness, weakness, tingling, pain, and tightness along with impairments in recreational and household activities persist up to 10 years in women with long-term BCRL. Moreover, the effects of chemotherapy can be long-lasting (>10 years) and could affect musculo-skeletal functioning in the arms of BCRL [38]. Unfortunately, none of these studies incorporated ultrasound techniques to measure skeletal muscle thickness or echo-intensity. In the present study, we found no absolute strength differences between arms of BCRL which is similar to that observed by others [19,20,21,22]. Despite our findings of similar strength measures between arms, there was a significant inter-limb EI difference among the affected, unaffected, and non-lymphedema values as determined by the gray scale output from ultrasound images. Therefore, muscle quality may be a more representative measure of a relative strength (handgrip strength/ muscle thickness)
We found that muscle quality in the affected arm was significantly lower than that of the non-lymphedema group. This finding should come as no surprise due, in part to, the EI values being significantly lower in the non-lymphedema group. However, the comparisons of interest and importance are the affected and unaffected arm. The muscle quality between the BCRL arms was not different and therefore we cannot attach a functional importance to the elevated EI in the affected arm. Whether there is a clinical significance remains to be seen. We can now state that, in addition to the increased thicknesses of skin and subcutaneous fat, the elevated levels of skeletal muscle EI are now implicated in the development of abnormal tissue morphology in BCRL. Of interest, we found a moderate positive correlation between subcutaneous fat thickness and muscle EI. This suggests that subcutaneous fat in the arm with lymphedema may serve as a predictive signal for elevated EI. Knowing that greater subcutaneous fat thickness and elevated muscle EI are present in the affected arm, these findings may assist clinicians and health care professionals with the early diagnosis and staging of BCRL.
There are a number of important strengths to this study. First, the vast majority of studies have included women with BCRL of 5 years and less. In the present study, we recruited women with long-term lymphedema (10.5±6.2 yrs.). Since breast cancer survivors are living longer with this condition, it is important to examine and to characterize the tissue abnormalities that exist in these women as they age with lymphedema [38].
Secondly, we conducted test-re-test calculations of our images for our variables of interest (muscle thickness and EI) to identify reliability, measurement error, and bias. Our test-retest reliability values were high for echo intensity (R range 0.763-0.996; n=5) and muscle thickness (R range 0.991-0.997; n=5) of the affected and unaffected arms. These values were similar to Vieira et al. [39] who conducted a reliability study using B-mode ultrasonography on the forearm flexors in young women and found their measures to be highly reliable, precise, and demonstrated little systematic error. Since all our measurements were done in post-processing, the image settings for gain, depth, and frequency were not changed and did not factor into any error. However, potential error could be found in identifying similar ROI placements. Based upon our reliability measures, this error was minimal and within acceptable ranges.
5. Study Limitations
This pilot study has limitations. First, the small sample sizes have placed a limitation on the robustness of our statistical comparisons. Secondly, we examined the forearm extensors which are located on the dorsal aspect of the arm and not the flexors which are well known to be the primary muscles for generating grip strength. There are no studies that have examined the tissue properties of the forearm muscle extensors in BCRL. Thus, it is not known if the tissue properties of the two groups of muscle are similar. However, along with the forearm flexors, the extensor muscles are known to be recruited [40,41,42] and to make significant contributions to isometric grip strength [43]. Thirdly, our ultrasound images were obtained from a rather narrow bandwidth of the forearm just distal to the elbow. Whether this regional slice is representative of the entire affected arm is currently unknown. It has previously been shown that the upper arm differs significantly from the lower portion of the arm in terms of skin and subcutaneous fat thicknesses [44]. Thus, it is conceivable that muscle thickness and echo intensity may differ according to measurement location.
6. Conclusions
We conclude that: 1) B-mode ultrasonography is a reliable modality for the measurement of muscle thickness and EI and may serve as a surrogate to MRI, 2) despite having similar muscle thickness and strength in the arms of BCRL, the elevated EI in the affected arm did not influence muscle quality and 3) since the amount of hyperechoic material in skeletal muscle is associated with subcutaneous fat thickness, it can serve in future studies as a predictor of increased EI in skeletal muscle of the arm with lymphedema.
Author Contributions
Methodology, image analysis, original manuscript draft, J.W.; Conceptualization, supervision, A.T; Methodology, imaging supervisor, M.B.; Statistical analysis and interpretation, L.R; Conceptualization, supervision, imaging protocol, H.R.; Conceptualization, supervision, review and editing of drafts, completed final draft, R.K. All authors have read and agreed to the published version of this manuscript.
Funding
We acknowledge the support of the Natural Sciences and Engineering Research Council of Canada – RGPIN-2020-04612 (HR), PERFORM Capital Equipment Grant (RDK, HR, AT), and Louis G. Johnson Foundation (RDK, HR, and AT).
Institutional Review Board Statement
All procedures in studies involving human participants were performed under an approved protocol and consent form in accordance with the ethical standards of the Research Institute of the McGill University Health Centre and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent Statement
Written informed consent was obtained from all participants prior to any involvement in the study.
Data Availability Statement
The data presented in this study are available following a reasonable request from the corresponding author. The data are not publicly available due to participants’ personal information.
Acknowledgments
The authors would like to thank Stefanie Fallone, Hoda Hashemi, and Zahra Vajihi for assistance with participant recruitment and ultrasound image collection. We are indebted to all the participants in this study.
Conflicts of Interest
All authors declare that they have no competing interests.
References
- Baran, E.; Ozcakar, L.; Ozgul, S.; Aksoy, S.; Akbayrak, T. Upper limb sensory evaluations and ultrasonic skin measurements in breast cancer-related lymphedema receiving complex decongestive physiotherapy. Supportive Care in Cancer 2021, 29, 6545–6553. [Google Scholar] [CrossRef] [PubMed]
- Mellor, R.; Bush, N.L.; Stanton, A.W.B.; Bamber, J.C.; Levick, J.R.; Mortimer, P.S. Dual-frequency ultrasound examination of skin and subcutis thickness in breast cancer-related lymphedema. Breast J 2004, 10, 496–503. [Google Scholar] [CrossRef]
- Suehiro, K.; Morikage, N.; Yamashita, O.; Harada, T.; Samura, M.; Takeuchi, Y.; Mizoguchi, T.; Nakamura, K.; Hamano, K. Skin and subcutaneous tissue ultrasonography features in breast cancer-related lymphedema. Ann. Vasc. Dis. 2016, 9, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Young, H-J. ; Jenkins, N.T.; Zhao, O.; McCully, K.K. Measurement of Intramuscular Fat by Muscle Echo Intensity. Muscle Nerve 2015, 52, 963–971. [Google Scholar] [CrossRef]
- Yusof, K.M.; Avery-Kiejda, K.A.; Ahmad Suhaimi, S.; Ahmad Zamri, N.; Rusli, M.E.F.; Mahmud, R.; Saini, S.M.; AbdulWahhab Ibraheem, S.; Abdullah, M.; Rosli, R. ; Assessment of potential risk factors and skin ultrasound presentation associated with breast cancer-related lymphedema in long-term breast cancer survivors. Diagnostics 2021, 11, 1303. [Google Scholar] [CrossRef]
- Choi, Y-H. ; Seo, K-S. Correlation among bioimpedance analysis, sonographic and circumferential measurement in assessment of breast cancer-related arm lymphedema. Lymphology 2014, 47, 123–133. [Google Scholar]
- Devoogdt, N.; Pans, S.; De Groef, A.; Geraerts, I.; Christiaens, M.R.; Neven, P.; Vergote, I.; Van Kampen, M. Postoperative evolution of thickness and echogenicity of cutis and subcutis of patients with and without breast cancer-related lymphedema. Lymphat. Res. Biol. 2014, 12, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Tassenoy, A.; Vermeiren, K.; Veen, P.; van der Stadnik, T.; Ridder, F.D.; Peters, E.; Van Schuerbeek, P.; Lamote, J.; Lievens, P. . Demonstration of tissue alterations by ultrasonography, magnetic resonance imaging and spectroscopy, and histology in breast cancer patients without lymphedema after axillary node dissection. Lymphology 2006, 39, 118–126. [Google Scholar]
- Borri, M.; Gordon, K.D.; Hughes, J.C.; Scurr, E.D. ; Koh, D-M.; Leach, M.O.; Mortimer, P.S.; Schmidt, M.A. Magnetic resonance imaging-based assessment of breast cancer-related lymphoedema tissue composition. Invest. Radiol.
- Crescenzi, R.; Donahue, P.M.C.; Garza, M.; Lee, C.A.; Patel, N.J.; Gonzalez, V.; Sky Jones, R.; Donahue, M.J. Elevated magnetic resonance imaging measures of adipose tissue deposition in women with breast cancer treatment-related lymphedema. Breast Cancer Res. Treat. 2022, 191, 115–124. [Google Scholar] [CrossRef]
- Brorson, H.; Ohlin, K.; Olsson, G.; Karlsson, M.K. Breast cancer-related chronic arm lymphedema is associated with excess adipose and muscle tissue. Lymphat. Res. Biol. 2009, 7, 3–10. [Google Scholar] [CrossRef]
- Jeon, Y.; Beom, J.; Ahn, S.; Bok, S.K. Ultrasonographic Evaluation of Breast Cancer-related Lymphedema. J. Vis. Exp. 2017, 119. [Google Scholar]
- Abe, T.; Loenneke, J.P.; Thiebaud,R. S.; Loftin, M. Morphological and functional relationships with ultrasound measured muscle thickness of the upper extremity and trunk. Ultrasound 2014, 22, 229–235. [Google Scholar] [CrossRef]
- Aruna, R. ; Sivarajan,; A.A,; Madhumitha, M.; Vasanth, C.J. Association of hand grip strength with Ultrasound-derived forearm muscle thickness and echo intensity in young Indian adults. J. Med. Ultrasound.
- Muraki, S.; Fukumoto, K.; Fukuda, O. Prediction of the muscle strength by the muscle thickness and hardness using ultrasound muscle hardness meter. Springer 2013, 2, 7. [Google Scholar] [CrossRef]
- Baklaci, M.; Eyigör, S.; Tanıgör, G.; Özgür İnbat, M.; Çalışkan Kabayel, S. Assessment of muscle strength and volume changes in patients with breast cancer-related lymphedema. Oncol. Res. Treat. 2020, 43, 584–591. [Google Scholar] [CrossRef] [PubMed]
- De Groef, A.; Van Kampen, M.; Tieto, E.; Schonweger, P.; Christiaens, M.-R.; Neven, P.; Geraerts, I.; Gebruers, N.; Devoogdt, N. Arm lymphedema and upper limb impairments in sentinel node-negative breast cancer patients: A one year follow-up study. Breast 2016, 29, 102–108. [Google Scholar] [CrossRef]
- Rietman, J.S.; Geertzen, J.H.; Hoekstra, H.J.; Baas, P.; Dolsma, W.V.; de Vries, J.; Groothoff, J.W.; Eisma, W.H.; Dijkstra, PU.; et al. Long term treatment related upper limb morbidity and quality of life after sentinel lymph node biopsy or stage I or II breast cancer. Eur. J. Surg. Oncol. 2006, 32, 148–52. [Google Scholar] [CrossRef] [PubMed]
- Gomes, P.R.L.; Freitas, I.F.Jr.; da Silva, C.B.; Gomes, I.C.; Rocha, A.P.R.; Salgado, A.S.I.; do Carmo, E.M. Short-term changes in handgrip strength, body composition, and lymphedema induced by breast cancer surgery. Rev. Bras. Ginecol. Obstet. 2014, 36, 36,244–50. [Google Scholar] [CrossRef] [PubMed]
- Giray, E.; Akyüz, G. Assessment of Family Caregiver Burden and Its Relationships Between Quality of Life, Arm Disability, Grip Strength, and Lymphedema Symptoms in Women with Postmastectomy Lymphedema: A Prospective Cross-Sectional Study. Eur. J. Breast Health 2019, 15, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Merchant, C.R.; Chapman, T.; Kilbreath, S.L.; Refshauge, K.M.; Krupa, K. Decreased muscle strength following management of breast cancer. Disability and Rehabilitation 2008, 30, 1098–1105. [Google Scholar] [CrossRef]
- Lee, D.; Hwang, J.H.; Chu, I.; Chang, H.J.; Shim, Y.H.; Kim, J.H. Analysis of factors related to arm weakness in patients with breast cancer-related lymphedema. Support Care Cancer 2015, 23, 2297–2304. [Google Scholar] [CrossRef]
- Pillen, S.; Arts, I.M.P.; Zwarts, M.J. Muscle ultrasound in neuromuscular disorders. Muscle Nerve 2008, 37, 679–693. [Google Scholar] [CrossRef] [PubMed]
- Pillen, S.; Tak, R.O.; Zwarts, M.J.; Lammens, M.M.; Verrijp, K.N.; Arts, I.M.; van der Laak, J.; Hoogerbrugge, P.M.; van Engelen, B.G.; Verrips, A. Skeletal muscle ultrasound: Correlation between fibrous tissue and echo intensity. Ultrasound Med. Biol. 2009, 35, 443–446. [Google Scholar] [CrossRef]
- Stock, M.J.; Thompson, B.J. Echo intensity as an indicator of skeletal muscle quality: applications, methodology, and future directions. Eur. J. Appl. Physiol. 2021, 121, 121,369–380. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Fujita, E.; Thiebaud, R.S.; Loenneke, J.P.; Akamine, T. Ultrasound-Derived Forearm Muscle Thickness Is a Powerful Predictor for Estimating DXA-Derived Appendicular Lean Mass in Japanese Older Adults. Ultrasound Med. Biol. 2016, 42, 2341–2344. [Google Scholar] [CrossRef]
- Abe, T.; Thiebaud, R.S.; Loenneke, J.P. Age-related change in handgrip strength in men and women: is muscle quality a contributing factor? Age (Dordr) 2016, 38, 28. [Google Scholar] [CrossRef] [PubMed]
- Wong, S. Grip strength reference values for Canadians aged 6 to 79: Canadian Health Measures Survey, 2007 to 2013. Statistics Canada - Health Reports 2016, 27, 8. [Google Scholar]
- McSharry, V.; Glennon, K.; Mullee, A.; Brennan, D. The impact of body composition on treatment in ovarian cancer: a current insight. Expert Rev. Clin. Pharmacol. 2021, 14, 14,1065–1074. [Google Scholar] [CrossRef]
- Sanada, K.; Kearns, C.F.; Midorikawa, T.; Abe, T. Prediction and Validation of Total and Regional Skeletal Muscle Mass by Ultrasound in Japanese Adults. Eur. J. Appl. Physiol. 2006, 96, 24–31. [Google Scholar] [CrossRef]
- Reeves, N.D.; Maganaris, C.N.; Narici, M.V. Ultrasonographic Assessment of Human Skeletal Muscle Size. Eur. J. Appl. Physiol. 2004, 91, 116–118. [Google Scholar] [CrossRef]
- Hashemi, H.S.; Fallone, S.; Boily, M.; Towers, A.; Kilgour, R.D.; Rivaz, H. Assessment of Mechanical Properties of Tissue in Breast Cancer-Related Lymphedema Using Ultrasound Elastography. IEEE, TUFFC, 2019, 66, 541–550. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A Review of the Measurement of Grip Strength in Clinical and Epidemiological Studies: Towards a Standardised Approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef]
- Hoffman, M.D.; Colley, R.C.; Doyon, C.; Wong, S.L.; Tomkinson, G.R.; Lang, J.J. Normative-referenced percentile values for physical fitness among Canadians. Statistics Canada Health Reports, 2019, 30, 14–22. [Google Scholar]
- Bohannon, R.W. ; Wang, Y-C.; Yen, S-C., Ed.; Grogan, K.A. Handgrip Strength: A Comparison of Values Obtained From the NHANES and NIH Toolbox Studies. American Journal of Occupational Therapy, 2019. [Google Scholar]
- Peters, M.J.H.; van Nes, S.I.; Vanhoutte, E.K.; Bakkers, M.; van Doorn, P.A.; Merkies, I.S.J.; Faber, C.G. ; on behalf of the PeriNomS Study group. Journal of the Peripheral Nervous System 2011, 16, 16,47–50. [Google Scholar]
- Jorgensen, M.G.; Toyserkani, N.M.; Hansen, F.G.; Bygum, A.; Sorensen, J.A. Impact of lymphedema on health-related quality of life up to 10 years after breast cancer treatment. NPJ Breast Cancer 2021, 7, 70. [Google Scholar] [CrossRef] [PubMed]
- Heins, M.J.; de Ligt, K.M.; Verloop, J.; Siesling, S.; Korevaar, J.C. on behalf of the PSCCR group. Adverse health effects after breast cancer up to 14 years after diagnosis. Breast 2022, 61, 22e28. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.; Siqueira, A.F.; Ferreira-Junior, J.B.; Pereira, P.; Wagner, D.; Bottaro, M. Ultrasound imaging in women’s arm flexor muscles: intra-rater reliability of muscle thickness and echo intensity. Braz. J. Phys. Ther. 2016, 20, 20,535–542. [Google Scholar] [CrossRef]
- Bystrim, S.; Kilbom, A. Physiological response in the forearm during and after isometric intermittent handgrip. Eur. J. Appl. Physiol. 1990, 60, 457–466. [Google Scholar] [CrossRef]
- Hagg, G.; Milerad, E. Forearm extensor and flexor muscle exertion during simulated gripping work-An electromyographic study. Clinical Biomechanics 1997, 12, 39–43. [Google Scholar] [CrossRef]
- Hoozemans, M.J.M.; van Dieën, J.H. Prediction of handgrip forces using surfacEMG of forearm muscles. J. Electromyogr. Kinesiol. 2005, 15, 358–366. [Google Scholar] [CrossRef]
- Dahlqvist, C.; Nordander, C.; Granqvist, L.; Forsman, M.; Hanson, G.-A. Comparing two methods to record maximal voluntary contractions and different electrode positions in recordings of forearm extensor muscle activity: Refining risk assessments for work-related wrist disorders. Work 2018, 59, 231–242. [Google Scholar] [CrossRef]
- Mander, A.; Venosi, S.; Menegatti, E.; Byung-Boong, L.; Neuhardt, D.; Maietti, E.; Gianesini, S. Upper limb secondary lymphedema ultrasound mapping and characterization. Int. Angiol. 2019, 38, 334–42. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Sample B-mode ultrasound images of the left forearm. Non-lymphedema arm (A) and Lymphedema arm (B). ST=skin thickness; SCFT= subcutaneous fat thickness; MT=muscle thickness; MEI=muscle echo-intensity. Note the “white streaks” of hyperechoic material in the lymphedema arm when compared to the arm without lymphedema.
Figure 1.
Sample B-mode ultrasound images of the left forearm. Non-lymphedema arm (A) and Lymphedema arm (B). ST=skin thickness; SCFT= subcutaneous fat thickness; MT=muscle thickness; MEI=muscle echo-intensity. Note the “white streaks” of hyperechoic material in the lymphedema arm when compared to the arm without lymphedema.
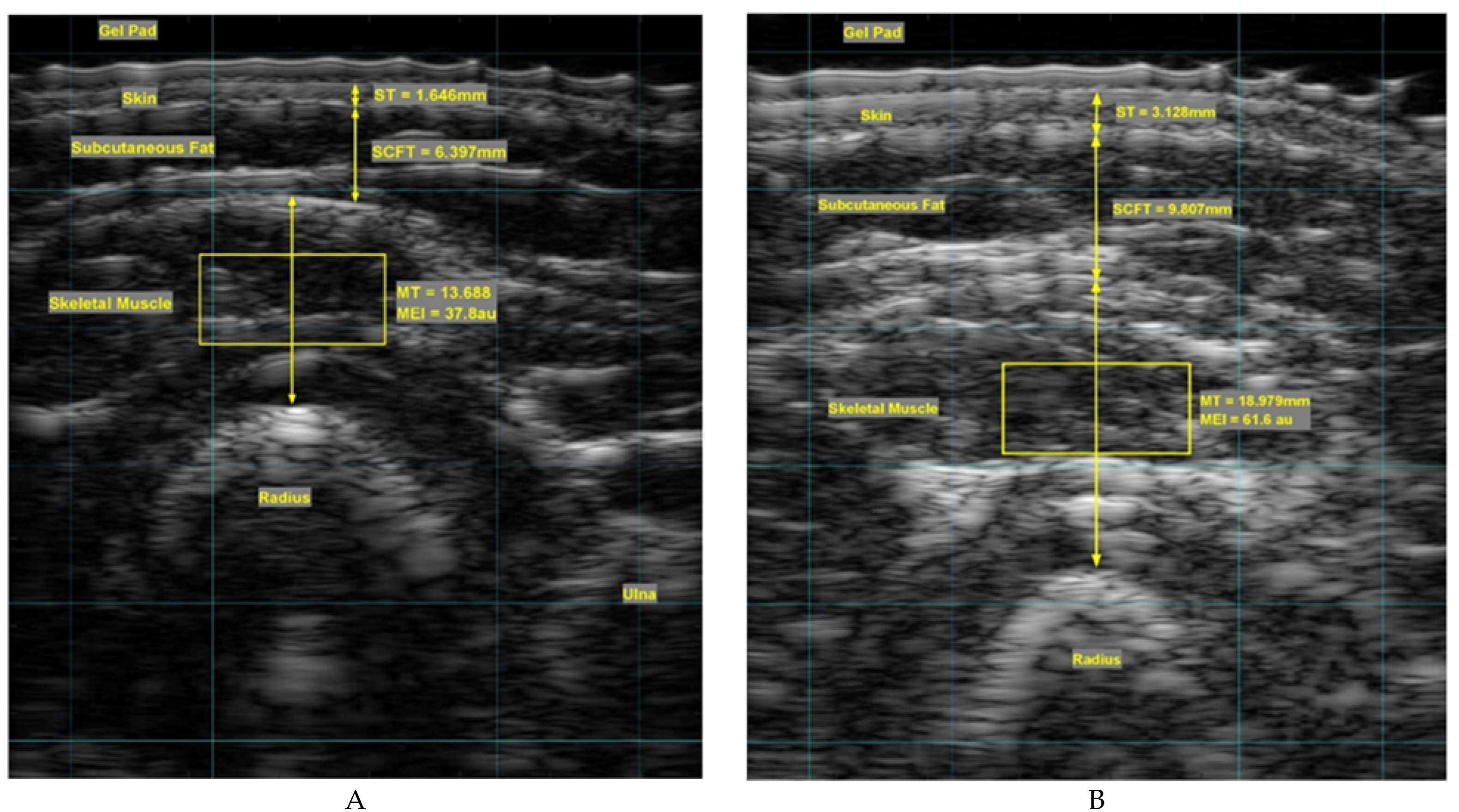

Table 1.
Participant demographics and clinical data.
| Variable | Lymphedema (n=20) | Non-lymphedema (n=20) | P-Value |
|---|---|---|---|
| Age (yrs) | 56 ± 14.8 | 48 ± 20.8 | 0.184 |
| Height (m) | 1.62 ± 0.07 | 1.59 ± 0.06 | 0.198 |
| Weight (kg) | 84.6 ± 18.4 | 73.9 ± 11.1 | 0.030* |
| BMI (kg/m2) | 32.1 ± 7.2 | 29.0 ± 4.2 | 0.101 |
| Body Fat (%) | 47.5 ± 6.9 | 42.4 ± 6.4 | 0.023* |
| Total Fat (kg) | 39.1 ± 13.1 | 30.5 ± 8.1 | 0.021* |
| Total Lean (kg) | 41.6 ± 5.8 | 40.1 ± 4.5 | 0.363 |
| BMD (g/cm2) | -0.673 ± 1.077 | -0.110 ± 1.411 | 0.200 |
| BCRL duration (yrs) | 10.51 ± 6.21 | n/a |
All values are mean ± SD, *Significantly different from the control group.
Table 2.
Group comparisons of total limb volume and forearm circumference in women with and without lymphedema.
Table 2.
Group comparisons of total limb volume and forearm circumference in women with and without lymphedema.
| Variables | Medians (IQR) | P-values | ||||
|---|---|---|---|---|---|---|
| AA | UA | CA | AA vs UA | AA vs CA | UA vs CA | |
| Forearm circumference (cm) | 25.2 (22.3-27.3) |
21.6 (20.2-24.9) |
21.4 (20.3-22.4) |
0.022 | 0.002 | 0.579 |
| Total limb volume (ml) | 3297 (3052-3839) |
2809 (2652-3297) |
2993 (2345-3651) |
0.05 | 0.05 | 0.745 |
All data are expressed as medians and inter-quartile ranges (IQR; 25th -75th percentile), AA=affected arm; UA = unaffected arm; CA=control arm.
Table 3.
A comparison of tissue thicknesses of the forearm in women with and without lymphedema.
| Tissue Thickness (mm) | Medians (IQR) | P-values | ||||
|---|---|---|---|---|---|---|
| AA | UA | CA | AA vs UA | AA vs CA | UA vs CA | |
| Skin | 2.37 (1.73-3.07) |
1.66 (1.58-1.85) |
1.73 (1.61-1.90) |
0.001 | 0.004 | 0.597 |
| Subcutaneous fat | 7.81 (6.00-14.85) |
5.55 (3.98-8.32) |
5.12 (3.55-6.42) |
0.001 | 0.001 | 0.364 |
| Skeletal muscle | 11.54 (10.36-12.74) |
11.76 (10.27-13.67) |
11.07 (9.57-13.19) |
0.401 | 0.410 | 0.490 |
See Table 2 for legend.
Table 4.
Handgrip strength (HGS), muscle echo-intensity (MEI), and muscle quality measurements (HGS/MT).
Table 4.
Handgrip strength (HGS), muscle echo-intensity (MEI), and muscle quality measurements (HGS/MT).
| Variables | Median (IQR) | P-values | ||||
|---|---|---|---|---|---|---|
| AA | UA | CA | AA vs UA | AA vs CA | UA vs CA | |
| HGS (kg) | 23.0 (15.9-28.4) |
23.3 (19.5-28.0) |
27.9 (23.5-31.9) |
0.524 | 0.048 | 0.061 |
| MEI (a.u.) | 82.5 (65.5-100.9) |
70.4 (58.0-81.1) |
64.2 (57.1-75.6) |
0.013 | 0.001 | 0.394 |
| HGS/MT (kg/mm) | 1.77 (1.39-2.46) |
1.98 (1.75-2.48) |
2.38 (1.86-3.06) |
0.588 | 0.025 | 0.132 |
See Table 2 for legend; a.u. = arbitrary units.
Table 5.
Reliability of MT and MEI ultrasound analyses of the forearms of women with lymphedema and non-lymphedema controls.
Table 5.
Reliability of MT and MEI ultrasound analyses of the forearms of women with lymphedema and non-lymphedema controls.
| Ultrasound parameter | M1 | SD | M2 | SD | R | P-value | 95% CI |
|---|---|---|---|---|---|---|---|
| MT AA | 10.20 | 2.58 | 9.96 | 3.09 | 0.990 | 0.810 | 0.824-0.998 |
| MT UA | 10.85 | 3.32 | 11.24 | 3.49 | 0.993 | 0.109 | 0.881-0.999 |
| MT CA (right) | 10.34 | 1.61 | 10.28 | 1.85 | 0.992 | 0.671 | 0.859-0.999 |
| MT CA (left) | 11.42 | 2.10 | 11.39 | 2.03 | 0.995 | 0.764 | 0.852-0.998 |
| MEI AA | 69.90 | 3.92 | 73.82 | 8.55 | 0.839 | 0.197 | -0.125-0.997 |
| MEI UA | 59.73 | 13.32 | 60.17 | 13.27 | 0.996 | 0.414 | 0.938-0.991 |
| MEI CA (right) | 56.97 | 8.83 | 58.41 | 9.07 | 0.987 | 0.085 | 0.789-0.998 |
| MEI CA (left) | 54.16 | 10.55 | 54.24 | 10.57 | 0.991 | 0.901 | 0.906-0.999 |
M1=measurement 1; M2=measurement 2; SD=standard deviation; 95% CI= confidence intervals; R=reliability coefficient; n=5/ultrasound parameter.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



