
Submitted:
03 September 2024
Posted:
05 September 2024
You are already at the latest version
Abstract
Artificial Intelligence (AI) is increasingly becoming integral to medical practice, potentially enhancing outcomes in thoracic surgery. AI-driven models have shown significant accuracy in diagnosing non-small cell lung cancer (NSCLC), predicting lymph node metastasis, and aiding in the efficient extraction of electronic medical records (EMR) data. Moreover, AI applications in robotic-assisted thoracic surgery (RATS) and perioperative management reveal potential in improving surgical precision, patient safety, and overall care efficiency. Despite these advancements, challenges such as data privacy, biases, and ethical concerns remain. This manuscript explores AI applications, particularly machine learning (ML) and natural language processing (NLP), in thoracic surgery, emphasizing their role in diagnosis and peri-operative management. It also provides a comprehensive overview of the current state, benefits, and limitations of AI in thoracic surgery, highlighting future directions in the field.
Keywords:
thoracic surgery
; AI
; Artificial Intelligence
; VATS
; RATS
; precision medicine
; precision surgery
1. Introduction
Artificial Intelligence is increasingly becoming an integral part of medical practice, improving patient and healthcare team outcomes, lowering costs, and influencing public health [1]. Surgery is predicted to be impacted by current advancements in AI, however, due to several drawbacks, it has not yet reached its full potential in the discipline. The amount of data generated today outpaces the human ability to handle it cognitively, and AI is poised to play a significant role in supporting the provision of tailored healthcare. For instance, current advances in AI have demonstrated great levels of accuracy in imaging and signal detection tasks. AI technologies in thoracic surgery have shown potential in enhancing the accuracy of diagnosis, the efficiency of treatment plans, and the effectiveness of postoperative care primarily through machine learning (ML) techniques and natural language processing (NLP) [2]. While NLP is changing the way clinical data and patient histories are processed and interpreted, ML algorithms are being used more and more for in-depth analysis of imaging data, helping in the diagnosis and classification of lung cancer [3]. As a result, clinical decision-making is made easier, medical errors are reduced, and patient care is provided more effectively and efficiently [3,4]. However, applications of AI in thoracic surgery are hurdled with certain difficulties. Some of these include limited generalizability, the need for well-annotated datasets for training, issues with data privacy, potential biases in AI algorithms, and ethical concerns [2]. This article explores the current state of AI in thoracic surgery, from diagnosis to preoperative planning, and intraoperative guidance to postoperative management, offering a comprehensive overview of its potential benefits and challenges.
2. Methodology
A comprehensive search was performed using the PubMed/MEDLINE, Cochrane, and Google Scholar databases. The articles were then screened for relevant studies by reviewing their abstracts with the following criteria. 1) Topics: AI in healthcare and surgery, AI and respiratory medicine, AI and pathology, AI and thoracic surgery. 2) Published in English and in a peer-reviewed journal. Next, two authors (M.U.A and J.K) comprehensively reviewed the full manuscripts for inclusion. There was no year limit. The inclusion criteria prioritized but were not limited to clinical trials and meta-analyses on the role of artificial intelligence in thoracic surgery published from 2021 onwards. Articles of interest that had been cited by the articles identified in the initial search were also reviewed.
3. Discussion:
3.1. Machine Learning and Natural Language Processing Applications in Thoracic Surgery
Thoracic surgery practice can be greatly aided by ML and NLP models, which aid in the diagnostic analysis of common and widespread diseases like non-small cell lung cancer (NSCLC). About 84% of lung cancer cases are NSCLC, posing a great burden on healthcare which is one of the greatest risks to human health due to its low 5-year relative survival rate of 25.0% [6]. Staging of NSCLC poses a great challenge to pulmonologists and thoracic surgeons because of limitations of invasive modalities such as mediastinoscopy and ultrasound-guided transbronchial needle aspiration [7]. While such modalities have better diagnostic capabilities over non-invasive modalities such as CT and PET scans, they are not routinely used in screening or in clinical practice on patients with severe comorbidities [8]. Researchers investigated employing statistical analysis or machine learning techniques to acquire nontrivial knowledge between the full patient attributes and lymph node metastasis status in order to achieve exact staging [8,9,10,11,12,13,14,15]. The majority of the clinical data, including tumor size, lymph node, tumor density, pleural indentation, and other information, are recorded in free-text format in electrical medical records (EMR), which makes it difficult to manually extract data. Manual extraction takes a lot of time and is prone human error. Thus, one major issue is how to efficiently extract this data to aid in later tasks like LNM prediction [16]. There has been an upsurge in the use of NLP models to extract this information automatically. Unfortunately, to date, this has not been widely adopted in thoracic surgery. In contrast, some medical fields have successfully implemented this technology. For instrance, Chen et al. [17] computed the Cancer of the Liver Italian Program score by extracting data from various clinical notes, such as CT reports and operation notes. To determine the TNM and clinicopathological stage of colorectal cancer in Australian patients, Martinez et al. [18] took data from pathology records. To evaluate patients’ chances of survival, Yuan et al. [19] extracted several features from EMRs using NLP methods. Another recent study by Hu et al. [7] developed a lymph node metastasis prediction model for patients with NSCLC by integrating NLP and ML with the EMR systems. They concluded every machine learning model outperformed the clinician’s assessment and the size requirement. The experimental results also demonstrated that the NLP model can effectively extract information from CT reports, aiding the lymph node metastasis prediction model’s development and updates, thereby facilitating its use in clinical settings.
Other areas where ML models have rapidly been adopted and show potential in thoracic surgery are diagnostic imaging and predictive analysis of surgical outcomes. These models will serve as a great addition for a surgeon to foresee the surgical outcomes in patients undergoing high-risk surgeries or in patients with severe co-morbidities. Kunze et al. [20] evaluated ML algorithms’ ability to predict clinically significant outcomes after orthopedic surgery and found that the currently available algorithms can easily discriminate the propensity to achieve clinically significant outcomes using the minimal clinically important difference with a fair to good performance as evidenced by C-statistics ranging from 0.6 to 0.95 in most analysis. Another study by Stam et al. [21] found that AI algorithms can precisely predict surgical complications in major abdominal surgeries, provided they are thoroughly tested and validated, and rely on a complete, balanced database. A 2023 study by Rana et al. [22], highlighted MRI and X-ray as key imaging modalities for surgical disease detection using ML and DL techniques, with MATLAB and SVM as commonly used tools. Convolutional neural networks and random forest were found to outperform other algorithms, suggesting the use of DL models with denoising approaches to improve accuracy. Common Glossary of Artificial Intelligence are reported in Table 1.
3.2. Advanced AI Applications in Thoracic Surgery
3.2.1. Identification of High-Risk Patients
Predictive analysis for the identification of high-risk patients is one of the most common applications of artificial intelligence. Several supervised and unsupervised ML models are utilized for the purpose of predicting binary events like readmission and mortality. A few examples of such incentives are the risk stratification index (RSI) [25], the American College of Surgeons National Surgical Quality Program (ACS NSQIP) [26], the revised cardiac risk index [27,28], and preoperative Score to predict postoperative Mortality [29]. An artificial neural network (ANN) method was created using genome sequencing data to guide safer and more successful warfarin dosing; in patients with international normalized ratios (INRs) >3.5, the algorithm predicted the therapeutic dose with an accuracy of 83% [30]. For instance, an ANN-based model used to stratify post-operative bleeding risk in patients undergoing cardiac pulmonary bypass had a 92% accuracy rate [31]. To forecast the requirement for prolonged ventilation during coronary bypass grafting (AUC = 0.71–0.73), another ANN algorithm was created [32]. Patient safety could be significantly improved in these circumstances with early intervention. Other predictive models have deployed ML techniques for the purpose of estimating the postoperative discharge destination to the floor within 24 hours of the surgery [33]. To increase these models’ predicted accuracy, full and real-time patient data is an absolute necessity.
3.2.2. Predicting and Detecting Complications
AI-powered sensors and continuous monitoring would play a massive role in aiding a thoracic surgeon in the early detection of complications. Thoracic surgery involves several postoperative pulmonary complications, such as respiratory function and infections that frequently develop after major surgery, adding to the mortality rates, prolonged hospital stays and increased costs [34,35,36]. Moreover, early-stage treatment of lung disorders may decrease the probability of bad outcomes, further emphasizing the need for early detection. To minimize such complications and aid in early detection, AI can assist in the development of prediction algorithms and decision support systems, while novel sensors and ongoing monitoring can aid in the collection of substantial volumes of physiological or electronic health record data [37]. The most frequently utilized classical model in thoracic surgery is the Assess Respiratory Risk in Surgical Patients in Catalonia (ARISCAT) score. ARISCAT was developed by Canet et al. [38] to foresee PPC in surgical patients using logistic regression (LR), which is the only score scale that maintains discriminator power for external acknowledgment [39]. ARISCAT score attained an AUROC of 0.80 in a prospective validation study with 5,859 patients [39]. Furthermore, Bolourani et al. [40] created a ML model to predict respiratory failure following pulmonary lobectomy in 4,062 patients. The AUROC was not given, even though the sensitivity and specificity were 83.3% and 94.5%, respectively. Chen et al.‘s study [41] examined several machine-learning methods, such as LR, SVM, RF, adaptive boosting, and GBM, to predict the risk of pneumonia in 786 patients following orthotopic liver transplantation. This study identified 14 factors, including laboratory and clinical variables, that were linked to postoperative pneumonia. Furthermore, opioid-induced respiratory depression frequently occurs in the postoperative general care unit. Early diagnosis of such respiratory episodes is now possible due to new portable and wearable monitoring technologies [42,43,44]. Since these events occur way before the true code-blue events, early identification, and intervention may provide an opportunity to avert disastrous consequences [45]. Score scales such as Prediction of Opioid-Induced Respiratory Depression in Patients Monitored by capnoGraphY are the first step in the prediction of the risk of respiratory depression using multivariable regression modeling on continuous oximetry and capnography data, followed by the next step is pattern detection with DL techniques [46].
Timely and effective treatment can make the crucial difference between saving a life and losing it. Such crucial calls can sometimes be mishandled by the surgeon in charge, but AI-driven decision support systems may help prevent these errors. Even during routine clinical care, interventions based on high-quality evidence are routinely miscalculated and not provided. Such high-quality evidence and patient data can be combined by a decision support system to provide point-of-care recommendations. For instance, Joosten et al. [47] demonstrated a positive effect on neurocognitive recovery by precisely titrating liquids, analgesics, and anesthesia using three closed-loop devices. AI can assist in the development of professional societies’ guidelines and recommendations in the lack of high-quality evidence. It can also assist in the development of guidelines-based decision support systems. Using decision assistance and image-based navigational tools, hospitals can address inefficiencies and clinical issues faced by physicians during surgery by implementing AI and predictive analytics in conventional ORs [37]. Certain AI systems can assist in anticipating complications, ensuring smoother surgeries, and quicker recovery by assessing the probability of problems even before a patient is carried into the operating room. AI is already proving to be an extremely important aid by improving the identification of target areas, such as through the OR “black box” platform, which records and analyzes surgical procedures to identify potential issues. For instance, one hospital discovered frequent OR door openings during surgery due to the suture cart being outside the room, leading to its relocation back inside [37]. The complex OR environment can benefit from digitalization and AI integration, as seen with the Triton system, which uses AI and infrared technology to analyze sponge photos and quantify blood loss [48].
3.2.3. Perioperative Management
Artificial Intelligence can serve as a potent tool in perioperative thoracic surgery management by enhancing diagnostic processes, performing tumor staging, facilitating predictive analysis, enabling robotic-assisted surgeries, and reducing postoperative complications and mortality rates. Rapid Diagnostic Assessment and Tumor Staging can differ between survival and death during preoperative management. A recent study conducted by Ye et al. experimented with a deep-learning radiomics model to predict high-risk pathologic pulmonary nodules in patients through CT semantics [49]. Their proposed combined model yielded an area under the receiver operating characteristic curve (AUC) values of 0.872 and 0.814 in the training and external validation cohorts, respectively. Decision curve analysis (DCA) assures that the proposed models provide a net benefit in predicting high-risk pathological pulmonary nodules early on, which helps in providing rapid aid [49]. Similarly, such radiomics and clinical features can be combined to form comprehensive models to predict recurrence risk in NSCLC patients. A study extracted a total of 1562 radiomic features and retained 29 features after feature selection [50]. A COX multivariate regression model determined the N stage as the independent risk factor for postoperative recurrence. The AUC values of the radiomics-clinical comprehensive model were 0.972 and 0.937 in training and test cohorts respectively, these values far surpass the standalone clinical or radiomics models [50]. Another study conducted by Blüthgen et al. evaluated CT-derived radiomics for the thymic epithelial tumor stage and the presence of myasthenia gravis MG and concluded its usefulness as an imaging biomarker for thymic epithelial tumor histology and TNM staging [51]. Deep learning models’ efficiency in determining tumor stages was further cemented by two other studies conducted by Chen et al. [52,53], where both studies respectively dwelled on the use of CT image analytics through machine learning models for the identification of lung adenocarcinoma and high-risk tumor areas. The promising results from their computational study confirm that such a method provides a reliable basis for adenocarcinoma diagnosis supplementary to the pathological examination.
Intraoperative surgical management has also been flooded with artificial intelligence and deep learning model uses. Predictive analysis and robotic assistance throughout the treatment have provided a massive upper hand to the surgeons in performing the procedures with ease and smoothness. A deep learning prognostic model could assist in predicting the need for additional intraoperative placement of chest drainage after thoracoscopic lobectomy to prevent the risk of tension pneumothorax [54]. It was found that the incidence risk of tension pneumothorax was 4.53% and the nomogram makes it possible to decide on the intraoperative installation of an additional pleural drainage tube and prevent complications associated with postoperative lung collapse. Prolonged air leak is a serious and frequent complication post-lung resection surgery. AI was used to develop a useful risk predictor model to help recognize patients who might benefit from additional preventive procedures, and the model was successfully able to confirm significant prognostic risk factors and protective factors for prolonged air leak [55]. Although, after internal validation, the C statistic was found to be 0.63, which is too low to generate a reliable score in clinical practice [55]. The use of AI in intraoperative planning and surgical management remains a field for further study and development.
Artificial Intelligence (AI), Machine learning (ML), and Deep learning models are all equally transformative in postoperative surgical management in thoracic patients. Continuous monitoring of patients to predict future potential complications is a major leverage of AI for a thoracic surgeon. In a recent study conducted by Kadomatsu et al. [56] an elastic net regularized generalized linear model, a novel comorbidity risk score built especially for lung resection procedures was created. Data from 2018 and 2019 were used to validate this model, which examined 40 variables such as surgical methods, tumor-related characteristics, and patient status. The final 20-variable model performed noticeably better in predicting postoperative complications, with an AUC of 0.734, as opposed to 0.521 for the Charlson Comorbidity Index (CCI). Furthermore, AI models have been significantly developed for other critical care settings. For instance, a study by Frades et al. [57], aimed to create a mortality predictor for Intermediate Respiratory Care Unit (IRCU) patients using machine learning models. In the first year of implementation, the resulting model’s combination with multivariate logistic regression analysis considerably lowered failure rates by 50%, indicating its efficacy in mortality risk detection and real-time monitoring. As AI technologies continue to evolve, their integration into postoperative care protocols will likely become increasingly sophisticated, further enhancing recovery and long-term health outcomes for thoracic surgery patients.
3.2.4. Immunotherapy Guidance
AI has further emerged as a revolutionizing tool in immunotherapeutic guidance for thoracic surgery, particularly through model development for recognizing DNA methylation biomarkers, RNA sequencing, selecting effective drug targets, and gene classification. Deep learning AI models may be able to meet the unmet demand for non-invasive testing for the early diagnosis of lung malignancies by integrating imaging, clinical, and DNA methylation biomarkers to enhance the classification of pulmonary nodules [58]. In this prospective study conducted by He et al. [58], across 24 hospitals in China proposed a combined model, PulmoSeek Plus, which integrates clinical, imaging, and cell-free DNA methylation biomarkers to improve the classification of pulmonary nodules. The model achieved an AUC of 0.85 in the validation cohorts, outperforming the standalone CIBM and PulmoSeek models. With a sensitivity of 0.98 for early-stage lung cancer and a DCA indicating a substantial reduction in unnecessary surgeries and delayed treatments. In addition, AI has highlighted the role of dendritic cells in lung adenocarcinoma. Zhang et al. [59] conducted a study on lung adenocarcinoma and numerous other cancer patients undergoing immunotherapy, identifying 83 DC marker genes, this led to the development of a seven-gene signature that predicts the prognosis and treatment response. It was found that patients with lower risk scores responded better to immunotherapy and targeted therapies, and Cathepsin H emerged as a new protective biomarker for lung adenocarcinoma [59]. Similarly, an eight-gene risk model was successfully developed to predict esophageal squamous cell carcinoma induced by tricarboxylic acid (TCA) cycle [60]. The function assay suggested the CTTN gene’s role in cell proliferation and invasion through the EMT pathway and highlighted the importance of the TCA cycle’s importance in tumor immunity. The role of AI predictive and analytic models is further solidified by studies such as Li et al. [61], where cuproptosis is studied as a promising therapeutic modality for LUAD patients who have grown resistant to radiotherapy and chemotherapy. By identifying cuproptosis-related genes (CRGs) and constructing a three-layer ANN risk model, a robust prognostic value was demonstrated where low-risk group patients had immune “hot” tumors with anticancer activity and was more sensitive to immunotherapy, while high-risk group patients had immune “cold” tumors and were more sensitive to chemotherapy. Furthermore, another comprehensive study by Chen at al. [62] utilized machine learning techniques to develop an autophagy-related gene (ARG) classifier based on eight key ARGs. This classifier showed excellent diagnostic and prognostic performance (AUC > 0.85) across multiple datasets, outperforming traditional markers like procalcitonin and C-reactive protein. The model also correlated significantly with immune cell infiltration, immune pathways, and cytokine levels, effectively reflecting the immune microenvironment during sepsis [62]. Areas of AI applications in Thoracic Surgery are demonstrated in Table 2.
3.3. Limitations and Ethical Implications of Utilizing AI
While AI can have numerous advantages, as we highlighted, it also comes with its risks [64].
Regardless of the extent to which ML is employed, a robot is believed not to achieve fully autonomous thoughts. It is assumed to consistently replicate human cognitive processes, albeit with greater speed and logical consistency. As a result, human intuition and experience remain crucial factors. Surgeons frequently rely on instinct, and AI will most likely not be able to replace how humans approach—at least not yet fully [64]. Another major limiting factor for using AI in surgery is the financial burden of operating such advanced technology. Generalization and uniform standards of treatment will be impaired because not all regions can afford the technology. It’s possible that an algorithm created in one institution won’t apply to other universities directly. The model will be effectively tailored to reflect the clinical experience of that institution through the development of the algorithm. This presents advantages as well as disadvantages for prospective consumers [65]. The quantity and quality of the data that is provided determines how well the AI responds. The degree to which AI algorithms may be applied to different subgroups depends heavily on a number of criteria, including outliers, missing data, and how representative the included populations are. In fact, it’s critical to regularly update algorithms with fresh patient data so that they can adjust how decisions are made [66]. The types and quality of the data that are accessible to the algorithm restrict its outputs; for example, lung cancers that affect Caucasians in the EU do not share the same epidemiologic features as lung cancers that affect persons in Asia. Nonsmoking reasons account for a larger percentage of cancer cases in Asia, especially in women [67]. Therefore, there is a chance that selection bias will affect projections if specific populations or sexes are underrepresented.
Moreover, most of the uses of AI-driven technology in surgery are yet in their infancy stage. The autonomous execution of complicated surgical procedures is not the same as simple independent tasks. ML is not always accurate or produces inaccurate results and hence it is a must to overview whatever decisions the AI software may suggest. IBM’s Watson for Oncology Cognitive Computing system, created in 2012, employs AI algorithms to provide therapy suggestions for a range of illnesses, including lung tumors. Oncologists at the Memorial Sloan Kettering Cancer Center (New York, NY, USA) trained the program to recognize important information related to a patient’s cancer, such as blood test results, pathology and imaging reports, and the existence of genetic mutations. The available treatment options broadly align with the standards of the National Comprehensive Cancer Network [66]. However, in 2018, IBM’s Watson faced criticism for making incorrect treatment recommendations in certain situations, potentially endangering the lives of the patients [68]. It is strictly contraindicated for a patient with lung squamous cell carcinoma to use bevacizumab, as recommended by the system. In June 2019, the American Society for Clinical Oncology heard an abstract about IBM’s Watson for Oncology Cognitive Computing system, which hinted at its potential to support multidisciplinary tumor board decision-making [69]. Another example backing this argument is a study that attempted to use ML for early pneumonia diagnosis, two sets of chest radiographs—one with pneumonia and the other without—were given to the algorithms so they could learn to distinguish between the two. The mark on the radiograph used to designate the right and left sides, which turned out to differ across the two hospitals, was the greatest predictive feature of pneumonia, according to the algorithm, which immediately determined this [70]. Because of this, ML still requires supervision at this point in its development.
To fully achieve the potential of AI in healthcare and surgery, four main ethical issues must be carefully addressed: (1) informed consent to utilize data, (2) safety and transparency, (3) algorithmic fairness and biases, and (4) data privacy are all crucial factors to consider [71]. The question of whether AI systems may be regarded as lawful is controversial from both a legal and political standpoint (Resolution of the European Parliament, 16 February 2017) [72]. The goal is to assist policymakers ensure that the ethically challenging circumstances brought about by implementing AI in healthcare settings are addressed [73]. Most legal discussions around artificial intelligence have focused on the issue of algorithmic transparency limitations. The use of AI in high-risk scenarios has raised the need for transparent, fair, and responsible AI design and governance. The two most crucial components of transparency are the information’s comprehensibility and accessibility [74]. It is common for information regarding the operation of algorithms to be purposefully made difficult to access [75]. Machines that can learn new behavioral patterns and function according to lose norms are said to pose a danger to our ability to assign blame to their creators or operators. We might not have anyone to hold responsible for any harm caused if AI is used [74,75]. The scale of the threat is uncertain, and using machines will drastically restrict our capacity to place responsibility and take charge of the decision-making process [76]. Modern computing approaches can obscure the reasoning behind the outputs of an AI system, making it difficult for non-technical clinical users to understand [77]. While AI systems like IBM’s Watson for Oncology are designed to support clinical decision-making by evaluating information and recommending patient care, the complexity of these systems can create challenges [74,75]. If widely adopted, AI systems could revolutionize clinical decision-making and reshape healthcare dynamics, making it crucial for clinicians to ensure the safe implementation of these technologies [78,79,80]. However, as this study tries to clarify, it is possible that AI will be able to get beyond these restrictions; at the moment, one can only hypothesize as to how AI will be able to get around some ethical and moral conundrums.
4. Conclusions
Artificial intelligence (AI) has shown potential in revolutionizing thoracic surgery by enhancing diagnostic accuracy, optimizing treatment plans, and improving postoperative care. AI models, such as those predicting lymph node metastasis in non-small cell lung cancer, have demonstrated comparable performance over traditional methods, aiding in precise staging and better clinical decision-making. Moreover, AI-driven robotic surgeries, perioperative intelligence, and predictive models for identifying high-risk patients and complications have paved the way for safer and more efficient surgical procedures.
Despite these advancements however, the integration of AI in thoracic surgery faces some challenges, including the need for extensive datasets, problems of data privacy, potential biases in AI models, and ethical concerns. Addressing these limitations requires continuous refinement of AI models, adherence to ethical guidelines, and the establishment of transparent and accountable AI systems. Looking ahead, the future of AI in thoracic surgery holds promise with the potential for more sophisticated AI-driven systems, advanced perioperative management models, and decision support systems that can integrate seamlessly into the clinical environment. More research and external validation will be essential to harness its full potential and ensure its effective application in thoracic surgery.
Figure 1.
Subcategories of Artificial Intelligence [5].
Figure 1.
Subcategories of Artificial Intelligence [5].
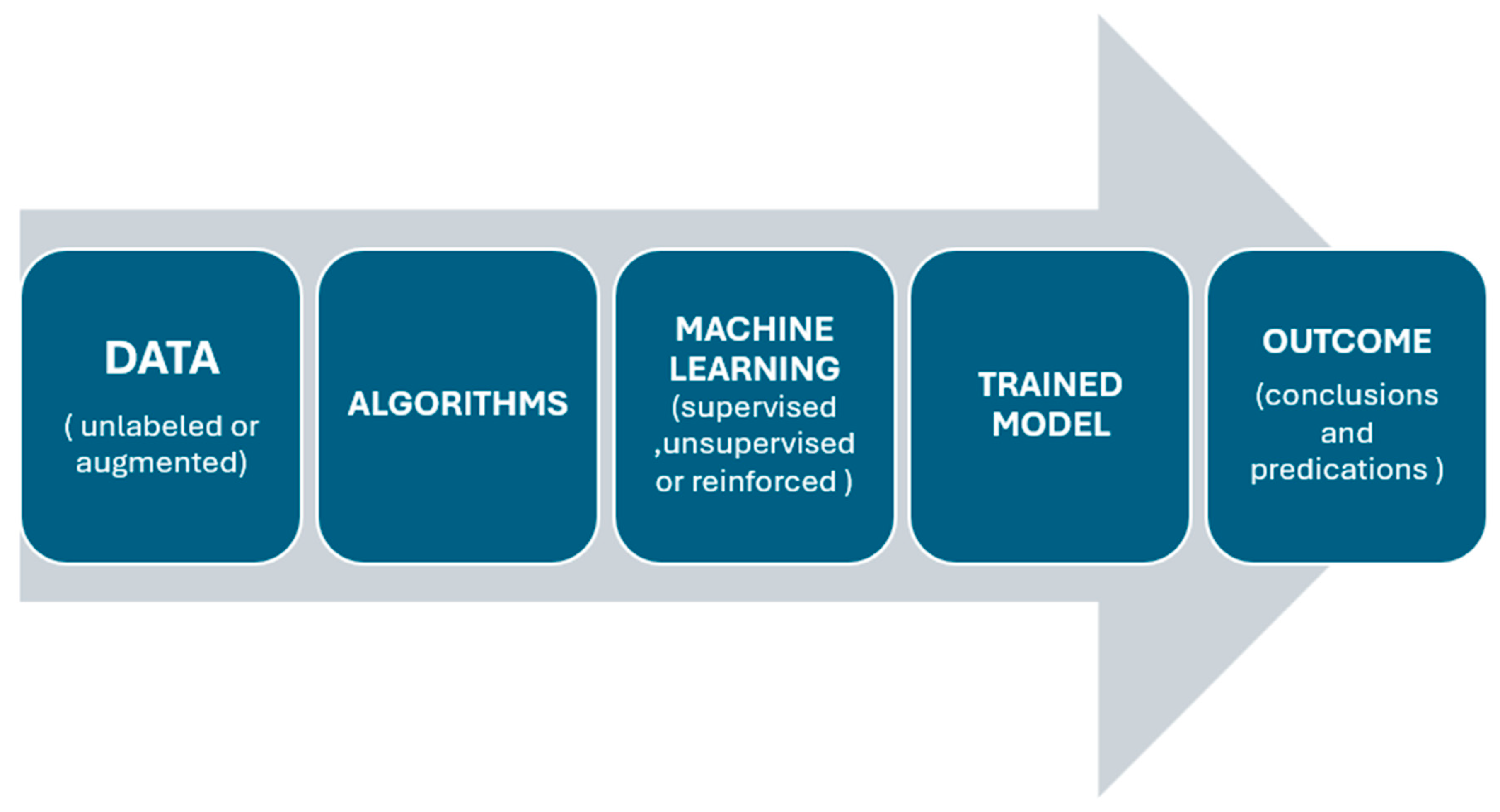
Figure 2.
Process and Steps in Artificial Intelligence [5].
Figure 2.
Process and Steps in Artificial Intelligence [5].
References
- Matheny, M.E.; Whicher, D.; Thadaney Israni, S. Artificial Intelligence in Health Care: A Report From the National Academy of Medicine. JAMA 2020, 323, 509–510. [Google Scholar] [CrossRef] [PubMed]
- Abbaker, N.; Minervini, F.; Guttadauro, A.; Solli, P.; Cioffi, U.; Scarci, M. The future of artificial intelligence in thoracic surgery for non-small cell lung cancer treatment a narrative review. Front. Oncol. 2024, 14, 1347464. [Google Scholar] [CrossRef] [PubMed]
- Research NC for E health. Norwegian Centre for E-health Research. Artificial Intelligence in Health Care - The Hope, the Hype, the Promise, the Peril. Available online: https://ehealthresearch.no/en/reports/other/artificial-intelligence-in-health-care-the-hope-the-hype-the-promise-the-peril (accessed on 8 June 2024).
- Case, N. How To Become A Centaur. J Des Sci [Internet]. 2018 Jan 8. Available online: https://jods.mitpress.mit.edu/pub/issue3-case/release/6 (accessed on 8 June 2024).
- Vaidya, Y.P.; Shumway, S.J. Artificial intelligence: The future of cardiothoracic surgery. J Thorac Cardiovasc Surg [Internet]. 2024 Apr 27;0(0). Available online: https://www.jtcvs.org/article/S0022-5223(24)00371-4/fulltext (accessed on 21 August 2024).
- Cancer Facts & Figures 2021 | American Cancer Society [Internet]. Available online: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2021.html (accessed on 10 June 2024).
- JMIR Medical Informatics - Using Natural Language Processing and Machine Learning to Preoperatively Predict Lymph Node Metastasis for Non–Small Cell Lung Cancer With Electronic Medical Records: Development and Validation Study [Internet]. Available online: https://medinform.jmir.org/2022/4/e35475#ref1 (accessed on 10 June 2024).
- Development of a nomogram for preoperative prediction of lymph node metastasis in non-small cell lung cancer: a SEER-based study - Zhang - Journal of Thoracic Disease [Internet]. Available online: https://jtd.amegroups.org/article/view/41481/html (accessed on 10 June 2024).
- Lv, X.; Wu, Z.; Cao, J.; Hu, Y.; Liu, K.; Dai, X.; et al. A nomogram for predicting the risk of lymph node metastasis in T1–2 non-small-cell lung cancer based on PET/CT and clinical characteristics. Transl Lung Cancer Res [Internet]. 2021 Jan;10(1). Available online: https://tlcr.amegroups.org/article/view/47129 (accessed on 10 June 2024).
- Development and Validation of a Clinical Prediction Model for N2 Lymph Node Metastasis in Non-Small Cell Lung Cancer - The Annals of Thoracic Surgery [Internet]. Available online: https://www.annalsthoracicsurgery.org/article/S0003-4975(13)01366-0/fulltext (accessed on 10 June 2024).
- Occult mediastinal lymph node metastasis in FDG-PET/CT node-negative lung adenocarcinoma patients: Risk factors and histopathological study - Miao - 2019 - Thoracic Cancer - Wiley Online Library [Internet]. Available online: https://onlinelibrary.wiley.com/doi/10.1111/1759-7714.13093 (accessed on 10 June 2024).
- Prediction Model for Nodal Disease Among Patients With Non-Small Cell Lung Cancer. - Abstract - Europe PMC [Internet]. Available online: https://europepmc.org/article/MED/30710518 (accessed on 10 June 2024).
- A Clinical Prediction Rule to Estimate the Probability of Mediastinal Metastasis in Patients with Non-small Cell Lung Cancer - Journal of Thoracic Oncology [Internet]. Available online: https://www.jto.org/article/S1556-0864(15)31627-0/fulltext (accessed on 10 June 2024).
- A Prediction Model for Pathologic N2 Disease in Lung Cancer Patients with a Negative Mediastinum by Positron Emission Tomography - Journal of Thoracic Oncology [Internet]. Available online: https://www.jto.org/article/S1556-0864(15)33473-0/fulltext (accessed on 10 June 2024).
- Novel approach for predicting occult lymph node metastasis in peripheral clinical stage I lung adenocarcinoma - Song - Journal of Thoracic Disease [Internet]. Available online: https://jtd.amegroups.org/article/view/27808/20883 (accessed on 10 June 2024).
- Yim, W.W.; Yetisgen, M.; Harris, W.P.; Kwan, S.W. Natural Language Processing in Oncology: A Review. JAMA Oncol. 2016, 2, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Song, L.; Shao, Y.; Li, D.; Ding, K. Using natural language processing to extract clinically useful information from Chinese electronic medical records. Int J Med Inf. 2019, 124, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Cross-hospital portability of information extraction of cancer staging information - ScienceDirect [Internet]. Available online: https://www.sciencedirect.com/science/article/abs/pii/S0933365714000669?via%3Dihub (accessed on 11 June 2024).
- Performance of a Machine Learning Algorithm Using Electronic Health Record Data to Identify and Estimate Survival in a Longitudinal Cohort of Patients With Lung Cancer | Artificial Intelligence | JAMA Network Open | JAMA Network [Internet]. Available online: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2781685 (accessed on 11 June 2024).
- Kunze, K.N.; Krivicich, L.M.; Clapp, I.M.; Bodendorfer, B.M.; Nwachukwu, B.U.; Chahla, J.; Nho, S.J. Machine Learning Algorithms Predict Achievement of Clinically Significant Outcomes After Orthopaedic Surgery: A Systematic Review. Arthrosc. J. Arthrosc. Relat. Surg. 2021, 38, 2090–2105. [Google Scholar] [CrossRef]
- Stam, W.T.; Goedknegt, L.K.; Ingwersen, E.W.; Schoonmade, L.J.; Bruns, E.R.; Daams, F. The prediction of surgical complications using artificial intelligence in patients undergoing major abdominal surgery: A systematic review. Surgery 2021, 171, 1014–1021. [Google Scholar] [CrossRef]
- Rana, M.; Bhushan, M. Machine learning and deep learning approach for medical image analysis: diagnosis to detection. Multimedia Tools Appl. 2022, 82, 26731–26769. [Google Scholar] [CrossRef]
- Salna, M. The Promise of Artificial Intelligence in Cardiothoracic Surgery. J Chest Surg. 2022, 55, 429–434. [Google Scholar] [CrossRef]
- scoping review of artificial intelligence applications in thoracic surgery | European Journal of Cardio-Thoracic Surgery | Oxford Academic [Internet]. Available online: https://academic.oup.com/ejcts/article/61/2/239/6380645?login=false (accessed on 21 August 2024).
- Broadly Applicable Risk Stratification System for Predicting Duration of Hospitalization and Mortality | Anesthesiology | American Society of Anesthesiologists [Internet]. Available online: https://pubs.asahq.org/anesthesiology/article/113/5/1026/10000/Broadly-Applicable-Risk-Stratification-System-for (accessed on 13 June 2024).
- Development and Evaluation of the Universal ACS NSQIP Surgical Risk Calculator: A Decision Aid and Informed Consent Tool for Patients and Surgeons - ScienceDirect [Internet]. Available online: https://www.sciencedirect.com/science/article/abs/pii/S1072751513008946 (accessed on 13 June 2024).
- 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines | Journal of the American College of Cardiology [Internet]. Available online: https://www.jacc.org/doi/abs/10.1016/j.jacc.2014.07.944 (accessed on 13 June 2024).
- Fronczek, J.; Polok, K.; Devereaux, P.; Górka, J.; Archbold, R.; Biccard, B.; Duceppe, E.; Le Manach, Y.; Sessler, D.; Duchińska, M.; et al. External validation of the Revised Cardiac Risk Index and National Surgical Quality Improvement Program Myocardial Infarction and Cardiac Arrest calculator in noncardiac vascular surgery. Br. J. Anaesth. 2019, 123, 421–429. [Google Scholar] [CrossRef]
- Preoperative Score to Predict Postoperative Mortality (POSPOM) | Anesthesiology | American Society of Anesthesiologists [Internet]. Available online: https://pubs.asahq.org/anesthesiology/article/124/3/570/14280/Preoperative-Score-to-Predict-Postoperative (accessed on 13 June 2024).
- Pavani, A.; Naushad, S.M.; Kumar, R.M.; Srinath, M.; Malempati, A.R.; Kutala, V.K. Artificial Neural Network-Based Pharmacogenomic Algorithm for Warfarin Dose Optimization. Pharmacogenomics 2015, 17, 121–131. [Google Scholar] [CrossRef]
- Huang, R.S.P.; Nedelcu, E.; Bai, Y.; Wahed, A.; Klein, K.; Tint, H.; Gregoric, I.; Patel, M.; Kar, B.; Loyalka, P.; et al. Post-Operative Bleeding Risk Stratification in Cardiac Pulmonary Bypass Patients Using Artificial Neural Network. Annals of Clinical & Laboratory Science 2015, 45, 181–186. [Google Scholar]
- Wise, E.S.; Stonko, D.P.; Glaser, Z.A.; Garcia, K.L.; Huang, J.J.; Kim, J.S.; Kallos, J.A.; Starnes, J.R.; Fleming, J.W.; Hocking, K.M.; et al. Prediction of Prolonged Ventilation after Coronary Artery Bypass Grafting: Data from an Artificial Neural Network. Hear. Surg. Forum 2017, 20, E007–E014. [Google Scholar] [CrossRef] [PubMed]
- Khanna, A.K.; Shaw, A.D.; Stapelfeldt, W.H.; Boero, I.J.; Chen, Q.; Stevens, M.; Gregory, A.; Smischney, N.J. Postoperative Hypotension and Adverse Clinical Outcomes in Patients Without Intraoperative Hypotension, After Noncardiac Surgery. Anesthesia Analg. 2021, 132, 1410–1420. [Google Scholar] [CrossRef] [PubMed]
- Opioid-induced respiratory depression increases hospital costs and length of stay in patients recovering on the general care floor | BMC Anesthesiology [Internet]. Available online: https://link.springer.com/article/10.1186/s12871-021-01307-8 (accessed on 13 June 2024).
- Epidemiology, practice of ventilation and outcome for patients at increased risk of postoperative pulmonary complications. Eur J Anaesthesiol. 2017, 34, 492–507. [CrossRef]
- Serpa Neto, A.; Hemmes, S.N.T.; Barbas, C.S.V.; Beiderlinden, M.; Fernandez-Bustamante, A.; Futier, E.; et al. Incidence of mortality and morbidity related to postoperative lung injury in patients who have undergone abdominal or thoracic surgery: a systematic review and meta-analysis. Lancet Respir Med. 2014, 2, 1007–1015. [Google Scholar] [CrossRef]
- Maheshwari, K.; Cywinski, J.B.; Papay, F.; Khanna, A.K.; Mathur, P. Artificial Intelligence for Perioperative Medicine: Perioperative Intelligence. Anesth Analg. 2023, 136, 637. [Google Scholar]
- Canet, J.; Gallart, L.; Gomar, C.; Paluzie, G.; Vallès, J.; Castillo, J.; Sabaté, S.; Mazo, V.; Briones, Z.; Sanchis, J.; et al. Prediction of Postoperative Pulmonary Complications in a Population-based Surgical Cohort. Anesthesiology 2010, 113, 1338–1350. [Google Scholar] [CrossRef]
- Mazo, V.; Sabaté, S.; Canet, J.; Gallart, L.; de Abreu, M.G.; Belda, J.; et al. Prospective external validation of a predictive score for postoperative pulmonary complications. Anesthesiology 2014, 121, 219–231. [Google Scholar] [CrossRef]
- Bolourani, S.; Wang, P.; Patel, V.M.; Manetta, F.; Lee, P.C. Predicting respiratory failure after pulmonary lobectomy using machine learning techniques. Surgery 2020, 168, 743–752. [Google Scholar] [CrossRef]
- Chen, C.; Yang, D.; Gao, S.; Zhang, Y.; Chen, L.; Wang, B.; et al. Development and performance assessment of novel machine learning models to predict pneumonia after liver transplantation. Respir Res. 2021, 22, 94. [Google Scholar] [CrossRef]
- Khanna, A.K.; Hoppe, P.; Saugel, B. Automated continuous noninvasive ward monitoring: future directions and challenges. Crit. Care 2019, 23, 194. [Google Scholar] [CrossRef] [PubMed]
- Khanna, A.K.; Ahuja, S.; Weller, R.S.; Harwood, T.N. Postoperative ward monitoring - Why and what now? Best Pract Res Clin Anaesthesiol. 2019, 33, 229–245. [Google Scholar] [CrossRef] [PubMed]
- Saugel, B.; Hoppe, P.; Khanna, A.K. Automated Continuous Noninvasive Ward Monitoring: Validation of Measurement Systems Is the Real Challenge. Anesthesiology. 2020, 132, 407–410. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.A.; Caplan, R.A.; Stephens, L.S.; Posner, K.L.; Terman, G.W.; Voepel-Lewis, T.; et al. Postoperative Opioid-induced Respiratory Depression: A Closed Claims Analysis. Anesthesiology 2015, 122, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Khanna, A.K.; Bergese, S.D.; Jungquist, C.R.; Morimatsu, H.; Uezono, S.; Lee, S.; Ti, L.K.; Urman, R.D.; McIntyre, R.; Tornero, C.; et al. Prediction of Opioid-Induced Respiratory Depression on Inpatient Wards Using Continuous Capnography and Oximetry: An International Prospective, Observational Trial. Anesthesia Analg. 2020, 131, 1012–1024. [Google Scholar] [CrossRef] [PubMed]
- Anesthetic Management Using Multiple Closed-loop Systems and Delayed Neurocognitive Recovery | Anesthesiology | American Society of Anesthesiologists [Internet]. Available online: https://pubs.asahq.org/anesthesiology/article/132/2/253/108808/Anesthetic-Management-Using-Multiple-Closed-loop (accessed on 13 June 2024).
- The association between the introduction of quantitative assessment of postpartum blood loss and institutional changes in clinical practice: an observational study - International Journal of Obstetric Anesthesia [Internet]. Available online: https://www.obstetanesthesia.com/article/S0959-289X(19)30070-6/abstract (accessed on 13 June 2024).
- Development and Validation of a Deep Learning Radiomics Model to Predict High-Risk Pathologic Pulmonary Nodules Using Preoperative Computed Tomography - Academic Radiology [Internet]. Available online: https://www.academicradiology.org/article/S1076-6332(23)00461-0/abstract (accessed on 4 August 2024).
- Application of a Comprehensive Model Based on CT Radiomics and Clinical Features for Postoperative Recurrence Risk Prediction in Non-small Cell Lung Cancer - Academic Radiology [Internet]. Available online: https://www.academicradiology.org/article/S1076-6332(23)00662-1/fulltext (accessed on 4 August 2024).
- Computed tomography radiomics for the prediction of thymic epithelial tumor histology, TNM stage and myasthenia gravis | PLOS ONE [Internet]. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0261401 (accessed on 5 August 2024).
- Machine vision-assisted identification of the lung adenocarcinoma category and high-risk tumor area based on CT images: Patterns [Internet]. Available online: https://www.cell.com/patterns/fulltext/S2666-3899(22)00044-7?_returnURL=https%3A%2F%2Flinkinghub.elsevier.com%2Fretrieve%2Fpii%2FS2666389922000447%3Fshowall%3Dtrue (accessed on 5 August 2024).
- Chen, L.; Qi, H.; Lu, D.; Zhai, J.; Cai, K.; Wang, L.; Liang, G.; Zhang, Z. A deep learning based CT image analytics protocol to identify lung adenocarcinoma category and high-risk tumor area. STAR Protoc. 2022, 3, 101485. [Google Scholar] [CrossRef]
- Pikin, O.; Ryabov, A.; Alexandrov, O.; Larionov, D.; Martynov, A.; Toneev, E. Predictive model for additional intraoperative placement of chest drainage after thoracoscopic lobectomy. Khirurgiya. Zhurnal im. N.I. Pirogova 2023, 14–25. [Google Scholar] [CrossRef]
- Divisi, D.; Pipitone, M.; Perkmann, R.; Bertolaccini, L.; Curcio, C.; Baldinelli, F.; Crisci, R.; Zaraca, F.; Italian VATS group. Prolonged air leak after video-assisted thoracic anatomical pulmonary resections: a clinical predicting model based on data from the Italian VATS group registry, a machine learning approach. J. Thorac. Dis. 2023, 15, 849–857. [Google Scholar] [CrossRef]
- Kadomatsu, Y.; Emoto, R.; Kubo, Y.; Nakanishi, K.; Ueno, H.; Kato, T.; Nakamura, S.; Mizuno, T.; Matsui, S.; Chen-Yoshikawa, T.F. Development of a machine learning-based risk model for postoperative complications of lung cancer surgery. Surg. Today 2024, 1–8. [Google Scholar] [CrossRef]
- Patient Management Assisted by a Neural Network Reduces Mortality in an Intermediate Care Unit [Internet]. Available online: http://www.archbronconeumol.org/en-linkresolver-patient-management-assisted-by-neural-S0300289619305940 (accessed on 5 August 2024).
- Accurate classification of pulmonary nodules by a combined model of clinical, imaging, and cell-free DNA methylation biomarkers: a model development and external validation study - The Lancet Digital Health [Internet]. Available online: https://www.thelancet.com/journals/landig/article/PIIS2589-7500(23)00125-5/fulltext (accessed on 5 August 2024).
- Zhang, L.; Guan, M.; Zhang, X.; Yu, F.; Lai, F. Machine-learning and combined analysis of single-cell and bulk-RNA sequencing identified a DC gene signature to predict prognosis and immunotherapy response for patients with lung adenocarcinoma. J. Cancer Res. Clin. Oncol. 2023, 149, 13553–13574. [Google Scholar] [CrossRef]
- Liang, Y.; Tan, B.; Du, M.; Wang, B.; Gao, Y.; Wang, M. A tricarboxylic acid cycle-based machine learning model to select effective drug targets for the treatment of esophageal squamous cell carcinoma. Front Pharmacol [Internet]. 2023 Jun 13;14. Available online: https://www.frontiersin.org/journals/pharmacology/articles/10.3389/fphar.2023.1195195/full (accessed on 6 August 2024).
- Frontiers | Deep learning reveals cuproptosis features assist in predict prognosis and guide immunotherapy in lung adenocarcinoma [Internet]. Available online: https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2022.970269/full (accessed on 6 August 2024).
- Chen, Z.; Zeng, L.; Liu, G.; Ou, Y.; Lu, C.; Yang, B.; Zuo, L. Construction of Autophagy-Related Gene Classifier for Early Diagnosis, Prognosis and Predicting Immune Microenvironment Features in Sepsis by Machine Learning Algorithms. J. Inflamm. Res. 2022, 15, 6165–6186. [Google Scholar] [CrossRef] [PubMed]
- Bellini, V.; Valente, M.; Rio, P.D.; Bignami, E. Artificial intelligence in thoracic surgery: a narrative review. J Thorac Dis [Internet]. 2021 Dec;13(12). Available online: https://jtd.amegroups.org/article/view/56034 (accessed on 1 August 2024).
- Gupta, A.; Singla, T.; Chennatt, J.J.; David, L.E.; Ahmed, S.S.; Rajput, D. Artificial intelligence: A new tool in surgeon’s hand. J Educ Health Promot. 2022, 11, 93. [Google Scholar] [CrossRef] [PubMed]
- Use of Artificial Intelligence for the Preoperative Diagnosis of Pulmonary Lesions - ScienceDirect [Internet]. Available online: https://www.sciencedirect.com/science/article/abs/pii/0003497589905924 (accessed on 1 August 2024).
- Etienne H, Hamdi S, Roux ML, Camuset J, Khalife-Hocquemiller T, Giol M, et al. Artificial intelligence in thoracic surgery: past, present, perspective and limits. Eur Respir Rev [Internet]. 2020 Sep 30;29(157). Available online: https://err.ersjournals.com/content/29/157/200010 (accessed on 1 August 2024).
- The International Epidemiology of Lung Cancer: Geographical Distribution and Secular Trends - Journal of Thoracic Oncology [Internet]. Available online: https://www.jto.org/article/S1556-0864(15)30445-7/fulltext (accessed on 1 August 2024).
- Ross, C.; Swetlitz, I. IBM’s Watson supercomputer recommended ‘unsafe and incorrect’cancer treatments, internal documents show. Stat 2018, 25, 1–10. [Google Scholar]
- A prospective blinded study of 1000 cases analyzing the role of artificial intelligence: Watson for oncology and change in decision making of a Multidisciplinary Tumor Board (MDT) from a tertiary care cancer center. | Journal of Clinical Oncology [Internet]. Available online: https://ascopubs.org/doi/10.1200/JCO.2019.37.15_suppl.6533 (accessed on 1 August 2024).
- Rajpurkar, P.; Irvin, J.; Zhu, K.; Yang, B.; Mehta, H.; Duan, T.; et al. CheXNet: Radiologist-Level Pneumonia Detection on Chest X-Rays with Deep Learning [Internet]. arXiv; 2017. Available online: http://arxiv.org/abs/1711.05225 (accessed on 14 June 2024).
- Ethical and legal challenges of artificial intelligence-driven healthcare - ScienceDirect [Internet]. Available online: https://www.sciencedirect.com/science/article/pii/B9780128184387000125?via%3Dihub (accessed on 14 June 2024).
- Rodrigues, R. Legal and human rights issues of AI: Gaps, challenges and vulnerabilities. J. Responsible Technol. 2020, 4, 100005. [Google Scholar] [CrossRef]
- The ethics of AI in health care: A mapping review - ScienceDirect [Internet]. Available online: https://www.sciencedirect.com/science/article/abs/pii/S0277953620303919?via%3Dihub (accessed on 14 June 2024).
- Naik, N.; Hameed, B.M.Z.; Shetty, D.K.; Swain, D.; Shah, M.; Paul, R.; et al. Legal and Ethical Consideration in Artificial Intelligence in Healthcare: Who Takes Responsibility? Front Surg [Internet]. 2022 Mar 14; 9. Available online: https://www.frontiersin.org/articles/10.3389/fsurg.2022.862322 (accessed on 14 June 2024).
- Migliore, M. VATS surgery for anatomical lung resection: a different approach for every surgeon. Video-Assisted Thorac. Surg. 2016, 1, 31–31. [Google Scholar] [CrossRef]
- Albrecht, J.P. REPORT on the proposal for a regulation of the European Parliament and of the Council on the protection of individuals with regard to the processing of personal data and on the free movement of such data (General Data Protection Regulation) | A7-0402/2013 | European Parliament [Internet]. Available online: https://www.europarl.europa.eu/doceo/document/A-7-2013-0402_EN.html (accessed on 14 June 2024).
- There Is No Techno-Responsibility Gap | Philosophy & Technology [Internet]. Available online: https://link.springer.com/article/10.1007/s13347-020-00414-7 (accessed on 14 June 2024).
- Clinical AI: opacity, accountability, responsibility and liability | AI & SOCIETY [Internet]. Available online: https://link.springer.com/article/10.1007/s00146-020-01019-6 (accessed on 14 June 2024).
- Migliore, M. Video-assisted thoracic surgery techniques for lung cancer: which is better? Future Oncology 2016, 12, 1–4. [Google Scholar] [CrossRef]
- Migliore, M.; Halezeroglu, S.; Mueller, M.R. Making precision surgical strategies a reality: are we ready for a paradigm shift in thoracic surgical oncology? Future Oncology 2020, 16, 1–5. [Google Scholar] [CrossRef]

| Algorithm | Models’ creation from mathematical approaches to data |
|---|---|
| Model | The mathematical function produced by the algorithm using the training set of data. |
| Artificial intelligence | A branch of computer science that focuses on teaching machines to perform tasks that traditionally require human intellect |
| Machine Learning | A subfield of artificial intelligence Where computers can learn from experience and recognize patterns in data without the need for explicit programming |
| Deep learning | This area of machine learning uses multilayer neural networks to examine data and create representations that resemble human thought processes. |
| Supervised learning | Subdivision of ML where the algorithm learns from labeled training data This is for the purpose of classification or prediction of new data. |
| Unsupervised learning | A subset of machine learning where computer algorithms are trained on unlabeled training data to find patterns and draw conclusions. |
| Computer vision | Artificial Intelligence field that allows computers to identify, understand, and react to visual input data |
| Natural language processing | AI field that enables computers to understand, interpret, and react to voice or text input |
Table 2.
Areas of AI applications in Thoracic Surgery [63].
Table 2.
Areas of AI applications in Thoracic Surgery [63].
| Applications areas | Examples |
|---|---|
| Preoperative Phase | Early detection of lung cancer. Genetic review and decision making chemo vs immunotherapy. |
| Diagnosis | Improve diagnostic accuracy and reduce false-positive rates. Radiology, liquid biopsy, histology. |
| Operative phase | Enhancing surgical, safety, accuracy, and decision-making in robotic-assisted surgery |
| Surgical skills assessment | |
| Surgical planning optimization | |
| Postoperative phase | Predict complications and mortality risks post-surgery. |
| Enhancing risk stratification. | |
| Support clinical decision-making | |
| Education | Educational support and surgical training feedback. |
| Management | Improving operating room scheduling and efficiency |
| Optimize overall resource utilization | |
| And cost-effectiveness enhancement |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



