Submitted:
03 September 2024
Posted:
05 September 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Emerging evidence suggests that patients suffering from COVID-19 may experience neurocognitive symptoms. Besides, other studies indicate a probable association between leukocyte telomere length (LTL) and neurocognitive changes in subjects with post-COVID-19 condition. Our study was designed to determine the correlation between telomere length and cognitive changes in subjects post-COVID-19. The study included 256 subjects, categorized based on SARS-CoV-2 infection from 2020 to 2023. On the other hand, those subjects who have a psychiatric diagnosis are considered. Besides, the MoCA and MMSE scales were applied. Telomere length was determined using a Polymerase Chain Reaction, and statistical analysis was employed ANOVA and X2 tests. We identified a decrease in LTL in individuals with post-COVID-19 conditions compared to those without SARS-CoV-2 infection (p≤0.05). However, no association was found between LTL and cognitive impairment in subjects post-COVID-19. The findings suggest that LTL is affected by SARS-CoV-2 infection. Nonetheless, this important finding requires further research by monitoring neurological changes in subjects with post-COVID condition.
Keywords:
telomere length
; cognitive changes
; post-COVID-19
; SARS-CoV-2
1. Introduction
The COVID-19 pandemic affected the mental and physical health of the world's population. After the SARS-CoV-2 active infection was resolved, some symptoms remained in the patient, and this condition is known as post-COVID-19 condition Existing evidence shows that symptoms are dizziness, headache, fatigue, inattention, memory disorders, sleep disorders, anxiety, depression, obsessive-compulsive disorder, paresthesia, altered consciousness, acute cerebrovascular disease, ataxia, seizures, neuropathic pain, impairment of taste, smell, or vision [1,2,3,4]. Recently, metabolic, functional, and structural alterations in the brain of post-COVID-19 patients are related to changes in cognition and emotion processing. Likewise, Azcue et al. (2022) found a correlation between cognition, processing speed, abstraction capacity, visuospatial capacity, and decreased olfactory function in post-COVID-19 patients [5].
On the other hand, telomeres are repetitive sequences at the end of eukaryotic chromosomes, and they ensure genome integrity by preventing fusion between adjacent chromosomes [6]. The decrease in LTL in humans is related to the senescence process (biological aging). Existing evidence suggests that shorter TL and telomere dysfunction are associated with advancing age, as well as with obesity, smoking, type 2 diabetes, hypertension, chronic kidney disease, COPD, cardiovascular disease, and neurocognitive disorders [6,7].
Recent studies have shown that a shorter LTL is associated with a greater severity of COVID-19 [8,9,10]. Del Brutto et al. (2022) found that individuals with COVID-19 and mild symptoms risk developing late cognitive impairment compared to those without clinical and serological evidence of SARS-CoV-2 infection [11]. Scarabino et al. (2022) propose that telomere shortening is progressive in patients with cognitive impairment compared to a control group [12]. In contrast, Zhan et al. (2018) found that higher TL is associated with higher levels of cognitive ability [13]. Various studies have been consistent with these findings, and higher TL has been reported to be related to longer life expectancy [7,12].
The purpose of this research was to explore the association between telomere length and cognitive changes in and post-COVID-19 subjects and individuals with psychiatric conditions.
2. Materials and Methods
Participants
A total of 256 people (106 women and 148 men) aged between 18 and 68 were involved. They were divided into four groups:
Group I. Without SARS-CoV-2 infection, seventy-five patients with a previous psychiatric diagnosis before the COVID-19 pandemic were included.
Group II. With SARS-CoV-2 infection, 62 patients have at least one established psychiatric diagnosis.
Group III. Without SARS-CoV-2, 39 individuals without psychiatric conditions
Group IV. With SARS-CoV-2 infection, 80 individuals with COVID-19 without diagnosed psychiatric conditions were involved.
Study Design
COVID-19 diagnosis: To identify the participation of SARS-CoV-2 on telomere length, we employed samples before the COVID-19 pandemic of previous studies realized by our work team. From these samples, we included individuals with psychiatric conditions in Group I and those without conditions in Group III. The diagnosis of COVID-19 in subjects from groups II and IV was confirmed with a positive PCR test for SARS-CoV-2 before sample collection.
Psychiatric evaluation: The subjects in Groups I and II have psychiatric conditions: Mood and emotional disorders, Neurodevelopmental disorders, Neurodegenerative disorders, and Disorders due to brain damage or dysfunction. They were evaluated and diagnosed by a psychiatrist according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) [14]. Group IV included subjects who recovered from SARS-CoV-2 infection between August 2021 and December 2023. A face-to-face survey was administered to this group for the first time in 2021 (SI) and the second in 2023 (SII). Socio-demographic diagnostic scales (socio-demographic questionnaire, clinical history) and scales for assessing neurocognitive (Mini-Mental State Examination, MMSE, and Montreal Cognitive Assessment, MoCA) were used. All participants signed an informed consent for participation in the study.
Determination of LTL
Peripheral blood samples were collected from all study participants. These were collected in EDTA tubes and stored at -80°C in a safe place in the INMEGEN psychiatric and neurodegenerative disease genomics laboratory. Subsequently, they were processed for DNA extraction from leukocytes using the Gentra purge kit from Qiagen and the determination of LTL [15].
Polymerase Chain Reaction (PCR) to Measure LTL
After DNA isolation, DNA quantity and quality were assessed by spectrophotometry (Nanodrop, 2000). A real-time polymerase chain reaction (rt-PCR) was performed to measure the average telomere length. Other studies have reported the primers used in this study [16]. The QuantStudio 6 Flex real-time PCR system (Thermo Fisher Scientific) was used to generate standard curves, Ct values for telomere, and reference gene signals [15]. We divide the LTL into four categories using quartiles: Very short.
(0 - 0.0062 2-ΔΔCT), Short (0.0062 - 0.0189 2-ΔΔCT), Medium (0.0189 - 0.1075 2-ΔΔCT) and Large (> 0.1075 2-ΔΔCT)
Instruments
The scale used to assess cognitive function and determine the index of global cognitive function was the Mini-Mental State Examination (MMSE). The 35-item version was used, with scores above 24 indicating no cognitive impairment and below 24 representing probable cognitive impairment [17,18,19]. The Montreal Cognitive Assessment (MoCA) was the scale used to identify mild cognitive dysfunction; a score greater than 26 indicates normal cognitive function, and 1 point was added to patients with ≤12 years of schooling [19,20,21].
Analysis of Data
Data were expressed as interval variables (mean ± SD) and categorical variables (number, %), both at baseline (T0) and at follow-up (T1). The groups were analyzed using the chi-square and the two groups t- Student t-tests. Subjects with COVID-19 were included in a multivariate analysis of variance (MANOVA) model to evaluate changes in cognitive function between LTL classification; partial eta squared (ƞp2) was used for size effect comparison. Results were considered significant p≤ 0.05. All statistical analyses were performed using SPSS-26 and Prism (version 9.0) software.
3. Results
The mean age observed was 42.06 ± 11.67 years, and there was a greater frequency of men (148) (Table 1). Group I (29.3%) and Group IV (31.3%) presented a more significant distribution of individuals. The most frequent psychiatric disorder was the diagnosis of schizophrenia, with 80 patients (Table 1). In this study, the mean LTL was 0.46 ± 1.28 (2-ΔΔCT); besides, we found a relationship between LTL and age, showing that older individuals had short telomere longitude (p≤0.05).
3.1. Relationship between LTL and Groups
Table 2 shows that the group I presented an LTL higher with respect to all groups (1.052±1.74). In contrast, group IV showed the shortest telomeric length compared to other groups I, II, and III (0.49±0.65) (Table 2).
In the participation of SARS-CoV-2 infection on LTL, lower LTL was observed in individuals with COVID-19 compared to subjects without SARS-CoV-2 infection (p≤0.05) (Figure 1A). In addition, persons who did not have a psychiatric disorder presented a lower LTL than patients with a psychiatric condition (p≤0.05) (Figure 1B).
3.2. Relationship between LTL and Cognitive Changes in Subjects with Post-COVID-19 Condition
Characteristics of the group IV were 52.5% male and 47.5% female, with a mean age of 43 ± 9.9 years. In addition, they showed cognitive changes using the MOCA and MMSE scales (62% and 27.5%, respectively). We found that cognitive changes persist two times due to scores by MOCA (<24) and MMSE (<26) were similar in SI and SII. We observed no association between LTL and cognitive changes in SI and SII using MOCA and MMSE. (Table 3).
However, individuals with post-COVID-19 condition with medium LTL had a higher MMSE score in the second survey compared to the first survey (p=0.023)
Interestingly, when we analyze persons with cognitive changes and without cognitive changes, according to the LTL, we observe no association between LTL in the group with cognitive changes compared to a group without cognitive changes in subjects with post-COVID-19 assessed by MOCA (p=0.27 and 0.22) and MMSE (p= 0.22) (Table 5).
4. Discussion
In this study, shorter LTL was observed in post-COVID-19 individuals without psychiatric disorders. Regarding the cognitive assessment, no association was found between LTL and changes in cognition in post-COVID-19 individuals. Previous studies indicate an association between short LTL and severe COVID-19 infection in patients [8,22]. In this sense, individuals with short telomeres show a reduced capacity for T cell proliferation and a higher proportion of senescent T cells [23,24]. Similarly, reports indicate that COVID-19 patients may experience T-cell lymphopenia, which is associated with telomere shortening and the severity of the disease [22,23,25]. According to Mahmoodpoor et al. (2023), patients with severe COVID-19 have a shorter LTL than those with moderate disease [26]. Anderson et al. (2022) detected a lower average relative length of chromosomes in the peripheral blood leukocytes of COVID-19 patients compared to a group without COVID-19 [27].
Various reports suggest that COVID-19 severity accelerates shortening their length and deterioration of telomeres [24]. Furthermore, SARS-CoV-2 may cause deterioration of telomeres in leukocytes; existing evidence suggests that the shortening of T cell telomeres is associated with the immune response in individuals with viral infections (HIV, HBV, HCV, EBV, and CMV); this leads to extensive proliferation in T cells, resulting in telomere shortening, replicative impairment, and decreased immunocompetence [26]. The current investigations propose that individuals with short telomeres may have a suboptimal antiviral response to SARS-CoV-2 infection, potentially resulting in more severe and progressive COVID-19 disease [28]. In contrast, some authors indicate no correlation between TL and the severity of COVID-19 (invasive ventilation or death) in patients with SARS-CoV-2 infection [25,29,30].
Additionally, a study suggests that TL is involved in the pathogenesis of age-related neurodegenerative diseases such as Alzheimer's disease (AD) [31]. Our study found that individuals with COVID-19 had a shorter LTL than those without COVID-19, as reported in other studies. According to previous findings, Fu et al. (2022) reported a relationship between shorter LTL and AD [32]. In contrast, a population-based MRI study found an association between longer LTL and larger brain and hippocampal volumes [33]. Besides, Koh et al. (2020) have a relation to shorter LTL with cognitive impairment [34].
Another study observed that longer LTL is associated with higher general cognition and improved performance in the cognitive domains of attention, speed, and executive function. Gampawar et al. (2022) suggest that longer telomeres in development allow for a more significant number of cell divisions, leading to increased brain volume in old age [33]. Bersani et al. (2015) suggest that increasing serotonin levels boosts the expression of telomerase reverse transcriptase (TERT) and telomerase activity through PI3K/Akt signaling [35]; this leads to a lengthening of telomeres and induces growth factors that promote neurogenesis and balanced mental health [36].
On the other hand, Kitagishi et al. (2012) suggest an association between serotonin, TERT expression, and activation of the PI3K/Akt signaling pathway, indicating that treatment with antidepressants, lithium, and antipsychotics increases LTL [37]. Likewise, our results showed that the group of patients with psychiatric conditions showed a greater length compared to the group without psychiatric conditions, possibly due to the use of antidepressants, anxiolytics, and antipsychotic medications (Annex 1). Mayén-Lobo et al. (2021) found that patients with schizophrenia treated with Clozapine have a lower epigenetic age, indicating that this drug is an aging protector [38].
Wei et al. (2022) suggest that emotional exhaustion in nursing personnel who worked during the COVID-19 pandemic is associated with TL; they demonstrate that TL was significantly shorter during the pandemic than before it began, regardless of the nurse's age group [39]. Our study found that individuals with post-COVID-19 experienced cognitive exhaustion throughout the first year. However, it is not related to LTL. Grand et al. (2023) propose that if SARS-CoV-2 were to persist similarly to HCV, it could lead to severe and detrimental effects on the infected tissue, as well as genomic instability and DNA damage in individuals with psychiatric conditions [28].
In our study, we observed that men have longer LTL than women. LTL shortens after each cell division, affecting the regenerative capacity of tissues and, consequently, triggering a tissue homeostatic imbalance and susceptibility to degenerative diseases [8]. In line with other research, it has been reported that men have a shorter LTL than women [40]. Some authors have suggested that TL is sex-specific, with girls having longer telomeres than boys from birth [41], and this relationship continues with age [42]. Therefore, the cellular and molecular mechanisms of aging are preserved in women [43], leading to a longer lifespan for women than men [44]. In this sense, reducing oxidative stress and inflammation promotes the lengthening of telomeres by telomerase activity [45]. Some authors suggest that the shortening of LTL is a biological marker of stress-related alterations, participating in the physiological and genetic mechanisms of aging and various psychiatric disorders such as depression, post-traumatic stress disorder, and chronic stress [39,46]. Biological aging occurs due to molecular and cellular damage, as indicated by LTL and DNA methylation age (DNAmAge) [47]. A recent report suggests that SARS-CoV-2 may accelerate epigenetic aging and is involved in developing post-COVID-19 condition [48]. Similarly, another author reports that DNAm aging correlates with telomere shortening in patients with COVID-19 [49].
Limitations. Our study presented some limitations. First, we noted the limited involvement of individuals with a post-COVID-19 condition, resulting in a small sample size. Second, our multivariate analysis could not account for potential cofactors.
5. Conclusions
We found no association between LTL and cognitive changes in individuals with a post-COVID-19 condition; however, the subjects with SARS-CoV-2 infection presented a shorter LT LTL. Besides, patients with psychiatric disorders may have a higher LTL due to the use of antipsychotic, antidepressant, and anxiolytic medications, which is an interesting result. Based on these findings, clinical and mental health monitoring should be used in the population with post-COVID-19 conditions.
Author Contributions
Conceptualization, A.D.G.M. J.N.M.L and H.N; methodology, A.D.G.M., G.E.N.J., M.V.S, I.E.J.R.; validation, A.D.G.M., H.N., A.F.,C.A.T.Z and N.M.; formal analysis, G.N., G.V. P.M.O, M.G.M.; investigation, G.V. G.A,N.R.; writing—original draft preparation, G.E.V.J., A.D.G.M.; supervision, H.N. A.D.G.M., M.V.S, I.E.J.R; project administration, A.D.G.M. H.N.
Funding
This research received no external funding
Institutional Review Board Statement
This research followed Article 17 of the General Health Act regarding health research. All procedures are carried out according to the principles of the Declaration of Helsinki. The hospital bioethics committee approved the application for the socio-demographic study, clinical history, MMSE, and MoCA scales and sampling (HRAESM/DG/UEI/4672021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
To the participants who donated samples and information for the completion of this work
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurology 2020, 77, 683–690. [Google Scholar] [CrossRef]
- Mazza, M.G.; Palladini, M.; Poletti, S.; Benedetti, F. Post-COVID-19 Depressive Symptoms: Epidemiology, Pathophysiology, and Pharmacological Treatment. CNS Drugs 2022, 36, 681–702. [Google Scholar] [CrossRef]
- Nalbandian, A.; Desai, A.D.; Wan, E.Y. Post-COVID-19 Condition. Annual Review of Medicine 2023, 74, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. The Lancet Infectious Diseases 2022, 22, e102–e107. [Google Scholar] [CrossRef] [PubMed]
- Azcue, N.; Gómez-Esteban, J.C.; Acera, M.; Tijero, B.; Fernandez, T.; Ayo-Mentxakatorre, N.; Pérez-Concha, T.; Murueta-Goyena, A.; Lafuente, J.V.; Prada, Á.; et al. Brain fog of post-COVID-19 condition and Chronic Fatigue Syndrome, same medical disorder? Journal of Translational Medicine 2022, 20, 569. [Google Scholar] [CrossRef] [PubMed]
- Tsilingiris, D.; Tentolouris, A.; Eleftheriadou, I.; Tentolouris, N. Telomere length, epidemiology and pathogenesis of severe COVID-19. European Journal of Clinical Investigation 2020, 50, e13376. [Google Scholar] [CrossRef] [PubMed]
- Mongelli, A.; Barbi, V.; Gottardi Zamperla, M.; Atlante, S.; Forleo, L.; Nesta, M.; Massetti, M.; Pontecorvi, A.; Nanni, S.; Farsetti, A.; et al. Evidence for Biological Age Acceleration and Telomere Shortening in COVID-19 Survivors. International Journal of Molecular Sciences 2021, 22. [Google Scholar] [CrossRef]
- Sanchez-Vazquez, R.; Guío-Carrión, A.; Zapatero-Gaviria, A.; Martínez, P.; Blasco, M.A. Shorter telomere lengths in patients with severe COVID-19 disease. Aging 2021, 13, 1–15. [Google Scholar] [CrossRef]
- dos Santos, G.A.; Pimenta, R.; Viana, N.I.; Guimarães, V.R.; Romão, P.; Candido, P.; de Camargo, J.A.; Hatanaka, D.M.; Queiroz, P.G.S.; Teruya, A.; et al. Shorter leukocyte telomere length is associated with severity of COVID-19 infection. Biochemistry and Biophysics Reports 2021, 27, 101056. [Google Scholar] [CrossRef]
- Wang, Q.; Codd, V.; Raisi-Estabragh, Z.; Musicha, C.; Bountziouka, V.; Kaptoge, S.; Allara, E.; Di Angelantonio, E.; Butterworth, A.S.; Wood, A.M.; et al. Shorter leukocyte telomere length is associated with adverse COVID-19 outcomes: A cohort study in UK Biobank. eBioMedicine 2021, 70. [Google Scholar] [CrossRef]
- Brutto, O.H.D. Cognitive sequelae of COVID-19, a post-pandemic threat. Should we be worried about the brain fog? Arquivos de Neuro-Psiquiatria 2022, 80. [Google Scholar] [CrossRef] [PubMed]
- Scarabino, D.; Veneziano, L.; Mantuano, E.; Arisi, I.; Fiore, A.; Frontali, M.; Corbo, R.M. Leukocyte Telomere Length as Potential Biomarker of HD Progression: A Follow-Up Study. International Journal of Molecular Sciences 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Zhan, Y.; Clements, M.S.; Roberts, R.O.; Vassilaki, M.; Druliner, B.R.; Boardman, L.A.; Petersen, R.C.; Reynolds, C.A.; Pedersen, N.L.; Hägg, S. Association of telomere length with general cognitive trajectories: a meta-analysis of four prospective cohort studies. Neurobiology of Aging 2018, 69, 111–116. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association,: Arlington, VA, 2013. [Google Scholar]
- Cuevas Diaz, P.; Nicolini, H.; Nolasco-Rosales, G.A.; Juarez Rojop, I.; Tovilla-Zarate, C.A.; Rodriguez Sanchez, E.; Genis-Mendoza, A.D. Telomere Shortening in Three Diabetes Mellitus Types in a Mexican Sample. Biomedicines 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Sanabria, M.; Martínez-Magaña, J.; Nicolini-Sánchez, H.; Guzmán-Sánchez, R.; Genis-Mendoza, A.D. Asociación entre la longitud de los telómeros y deterioro cognitivo en adultos mayores. Revista Española de Geriatría y Gerontología 2022, 57, 320–324. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Beaman, S.R.d.; Beaman, P.E.; Garcia-Peña, C.; Villa, M.A.; Heres, J.; Córdova, A.; Jagger, C. Validation of a Modified Version of the Mini-Mental State Examination (MMSE) in Spanish. Aging, Neuropsychology, and Cognition 2004, 11, 1–11. [Google Scholar] [CrossRef]
- Avila-Avila, A.; Sosa-Tinoco, E.; Pacheco-Pacheco, J.; Escobedo-Acosta, M.G.; Bautista-Eugenio, V.; González-García, V.; Blano-Campero, E.J.; Negrete-Redondo, M.I.; Deyta-Pantoja, A.L.; Gutiérrez-Robledo, L.M.F. Guía de instrumentos de evaluación geriátrica integral. 2020. [Google Scholar]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. Journal of the American Geriatrics Society 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Aguilar-Navarro, S.G.; Mimenza-Alvarado, A.J.; Palacios-García, A.A.; Samudio-Cruz, A.; Gutiérrez-Gutiérrez, L.A.; Ávila-Funes, J.A. Validity and reliability of the Spanish Version of the Montreal Cognitive Assessment (MoCA) for the detection of cognitive impairment in Mexico. Revista Colombiana de Psiquiatría (English Edition) 2018, 47, 237–243. [Google Scholar] [CrossRef]
- Patel, R.; Kooner, J.S.; Zhang, W. Comorbidities associated with the severity of COVID-19, and differences across ethnic groups: a UK Biobank cohort study. BMC Public Health 2023, 23, 1566. [Google Scholar] [CrossRef]
- Aviv, A. Short telomeres and severe COVID-19: The connection conundrum. eBioMedicine 2021, 70. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Zhang, F.; Shi, Y.; Chen, Y.; Shi, B.; Yu, G. Causal association of epigenetic aging and COVID-19 severity and susceptibility: A bidirectional Mendelian randomization study. Frontiers in Medicine 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Haridoss, M.; Ayyasamy, L.; Bagepally, B.S. Is COVID-19 severity associated with telomere length? A systematic review and meta-analysis. Virus Genes 2023, 59, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Mahmoodpoor, A.; Sanaie, S.; Eskandari, M.; Behrouzi, N.; Taghizadeh, M.; Roudbari, F.; Emamalizadeh, B.; Sohrabifar, N.; Kazeminasab, S. Association between leukocyte telomere length and COVID-19 severity. Egyptian Journal of Medical Human Genetics 2023, 24, 37. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.J.; Susser, E.; Arbeev, K.G.; Yashin, A.I.; Levy, D.; Verhulst, S.; Aviv, A. Telomere-length dependent T-cell clonal expansion: A model linking ageing to COVID-19 T-cell lymphopenia and mortality. eBioMedicine 2022, 78. [Google Scholar] [CrossRef]
- Grand, R.J. SARS-CoV-2 and the DNA damage response. Journal of General Virology 2023, 104. [Google Scholar] [CrossRef]
- Retuerto, M.; Lledó, A.; Fernandez-Varas, B.; Guerrero-López, R.; Usategui, A.; Lalueza, A.; García-García, R.; Mancebo, E.; Paz-Artal, E.; Sastre, L.; et al. Shorter telomere length is associated with COVID-19 hospitalization and with persistence of radiographic lung abnormalities. Immunity & Ageing 2022, 19, 38. [Google Scholar] [CrossRef]
- Reeves, J.; Kooner, J.S.; Zhang, W. Accelerated ageing is associated with increased COVID-19 severity and differences across ethnic groups may exist. Frontiers in Public Health 2022, 10. [Google Scholar] [CrossRef]
- Levstek, T.; Kozjek, E.; Dolžan, V.; Trebušak Podkrajšek, K. Telomere Attrition in Neurodegenerative Disorders. Frontiers in Cellular Neuroscience 2020, 14. [Google Scholar] [CrossRef]
- Fu, J.; Ji, X.; Liu, J.; Chen, X.; Shang, H. Meta-analysis of the Connection Between Alzheimer Disease and Telomeres. Alzheimer Disease & Associated Disorders 2022, 36. [Google Scholar]
- Gampawar, P.; Schmidt, R.; Schmidt, H. Telomere length and brain aging: A systematic review and meta-analysis. Ageing Research Reviews 2022, 80, 101679. [Google Scholar] [CrossRef]
- Koh, Z.Y.; Law, F.; Chew, J.; Ali, N.; Lim, W.S. Impact of Coronavirus Disease on Persons with Dementia and Their Caregivers: An Audit Study. Ann Geriatr Med Res 2020, 24, 316–320. [Google Scholar] [CrossRef]
- Bersani, F.S.; Lindqvist, D.; Mellon, S.H.; Penninx, B.W.J.H.; Verhoeven, J.E.; Révész, D.; Reus, V.I.; Wolkowitz, O.M. Telomerase activation as a possible mechanism of action for psychopharmacological interventions. Drug Discovery Today 2015, 20, 1305–1309. [Google Scholar] [CrossRef] [PubMed]
- Epel, E.S.; Prather, A.A. Stress, Telomeres, and Psychopathology: Toward a Deeper Understanding of a Triad of Early Aging. Annual Review of Clinical Psychology 2018, 14, 371–397. [Google Scholar] [CrossRef] [PubMed]
- Kitagishi, Y.; Kobayashi, M.; Kikuta, K.; Matsuda, S. Roles of PI3K/AKT/GSK3/mTOR Pathway in Cell Signaling of Mental Illnesses. Depression Research and Treatment 2012, 2012, 752563. [Google Scholar] [CrossRef] [PubMed]
- Mayén-Lobo, Y.G.; Martínez-Magaña, J.J.; Pérez-Aldana, B.E.; Ortega-Vázquez, A.; Genis-Mendoza, A.D.; Dávila-Ortiz de Montellano, D.J.; Soto-Reyes, E.; Nicolini, H.; López-López, M.; Monroy-Jaramillo, N. Integrative Genomic–Epigenomic Analysis of Clozapine-Treated Patients with Refractory Psychosis. Pharmaceuticals 2021, 14. [Google Scholar] [CrossRef]
- Wei, H.; Aucoin, J.; Kuntapay, G.R.; Justice, A.; Jones, A.; Zhang, C.; Santos, H.P., Jr.; Hall, L.A. The prevalence of nurse burnout and its association with telomere length pre and during the COVID-19 pandemic. PLOS ONE 2022, 17, e0263603. [Google Scholar] [CrossRef]
- Campisi, M.; Cannella, L.; Celik, D.; Gabelli, C.; Gollin, D.; Simoni, M.; Ruaro, C.; Fantinato, E.; Pavanello, S. Mitigating cellular aging and enhancing cognitive functionality: visual arts-mediated Cognitive Activation Therapy in neurocognitive disorders. Frontiers in Aging Neuroscience 2024, 16. [Google Scholar] [CrossRef]
- Jylhävä, J.; Pedersen, N.L.; Hägg, S. Biological Age Predictors. eBioMedicine 2017, 21, 29–36. [Google Scholar] [CrossRef]
- Gardner, M.; Bann, D.; Wiley, L.; Cooper, R.; Hardy, R.; Nitsch, D.; Martin-Ruiz, C.; Shiels, P.; Sayer, A.A.; Barbieri, M.; et al. Gender and telomere length: Systematic review and meta-analysis. Experimental Gerontology 2014, 51, 15–27. [Google Scholar] [CrossRef]
- Hägg, S.; Jylhävä, J. Sex differences in biological aging with a focus on human studies. eLife 2021, 10, e63425. [Google Scholar] [CrossRef] [PubMed]
- Zhao, E.; Crimmins, E.M. Mortality and morbidity in ageing men: Biology, Lifestyle and Environment. Reviews in Endocrine and Metabolic Disorders 2022, 23, 1285–1304. [Google Scholar] [CrossRef]
- Ahmed, W.; Lingner, J. Impact of oxidative stress on telomere biology. Differentiation 2018, 99, 21–27. [Google Scholar] [CrossRef]
- Shalev, I.; Entringer, S.; Wadhwa, P.D.; Wolkowitz, O.M.; Puterman, E.; Lin, J.; Epel, E.S. Stress and telomere biology: A lifespan perspective. Psychoneuroendocrinology 2013, 38, 1835–1842. [Google Scholar] [CrossRef]
- López-Otín, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. Hallmarks of aging: An expanding universe. Cell 2023, 186, 243–278. [Google Scholar] [CrossRef]
- Nolasco-Rosales, G.A.; Alonso-García, C.Y.; Hernández-Martínez, D.G.; Villar-Soto, M.; Martínez-Magaña, J.J.; Genis-Mendoza, A.D.; González-Castro, T.B.; Tovilla-Zarate, C.A.; Guzmán-Priego, C.G.; Martínez-López, M.C.; et al. Aftereffects in Epigenetic Age Related to Cognitive Decline and Inflammatory Markers in Healthcare Personnel with Post-COVID-19: A Cross-Sectional Study. Int J Gen Med 2023, 16, 4953–4964. [Google Scholar] [CrossRef]
- Cao, X.; Li, W.; Wang, T.; Ran, D.; Davalos, V.; Planas-Serra, L.; Pujol, A.; Esteller, M.; Wang, X.; Yu, H. Accelerated biological aging in COVID-19 patients. Nature Communications 2022, 13, 2135. [Google Scholar] [CrossRef]
Figure 1.
LTL in subjects with COVID-19 and psychiatric conditions A) Subjects with COVID-19 disease and without COVID-19. B) Subjects with psychiatric conditions and without psychiatric conditions. Data are expressed by standard deviation; the Student T-test was performed, *p≤ 0.05.
Figure 1.
LTL in subjects with COVID-19 and psychiatric conditions A) Subjects with COVID-19 disease and without COVID-19. B) Subjects with psychiatric conditions and without psychiatric conditions. Data are expressed by standard deviation; the Student T-test was performed, *p≤ 0.05.
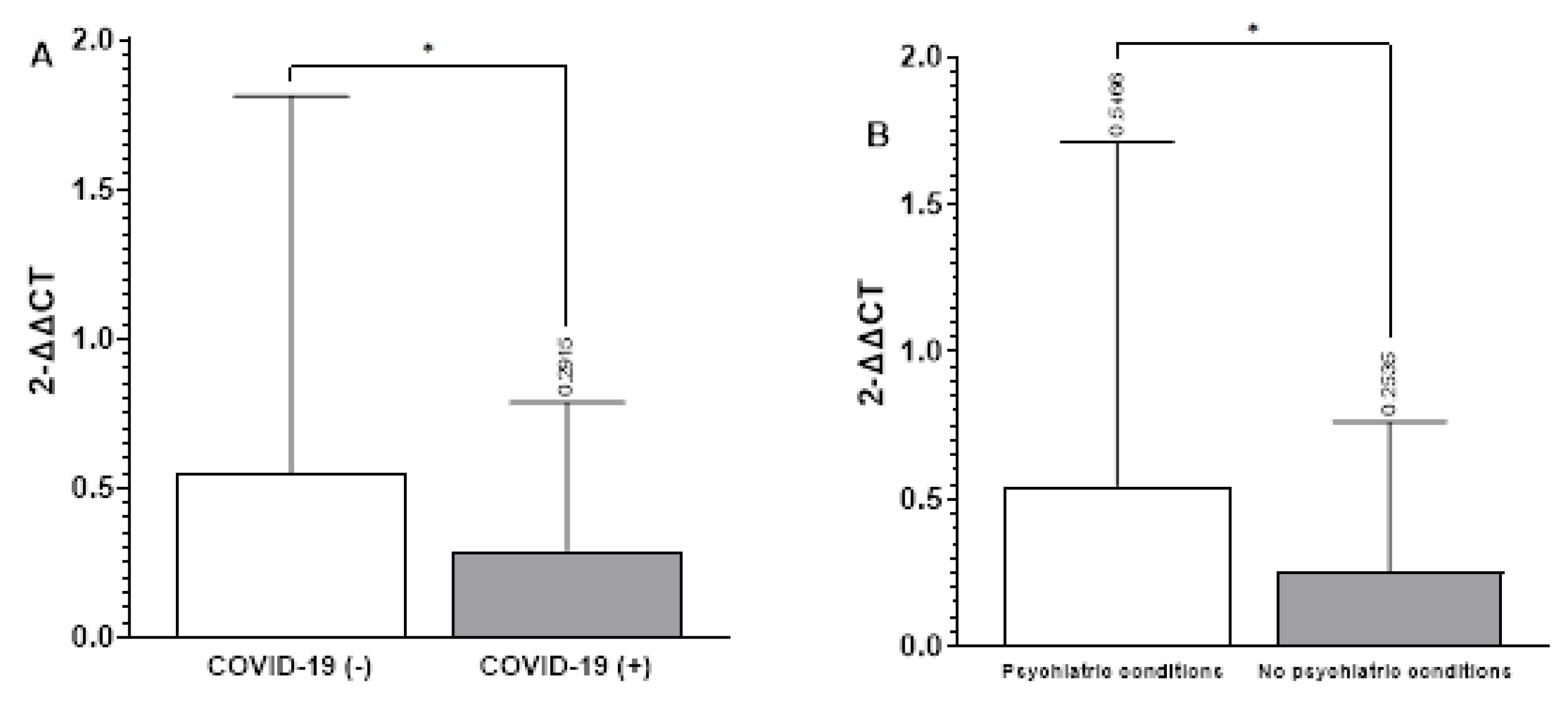

Table 1.
Sociodemographic and clinical characteristics in people with psychiatric disorders with COVID-19 (group I) and without COVID-19 (group II).
Table 1.
Sociodemographic and clinical characteristics in people with psychiatric disorders with COVID-19 (group I) and without COVID-19 (group II).
| Variable | F, Percentage, M ± S.D. | F, P |
|---|---|---|
| Age (years) | 42.06 ± 11.67 | |
| Sex | ||
| Female | 106, 41.4% | |
| Male | 148, 57.8% | |
| Groups | ||
| I | 75, 29.3% | |
| II | 39, 14.8% | |
| III | 62, 24.2% | |
| IV | 80, 31.3% | |
| Diagnosis | ||
| Mood and emotional disorders | 12, 15% | |
| Neurodevelopmental disorders | 17, 21% | |
| Neurodegenerative disorders | 5, 6% | |
| Schizophrenia | 80, 70% | |
| Telomere length (2-ΔΔCT) | 0.46 ± 1.28 | |
| Sex | ||
| Female | 0.58 ± 0.36 | 0.17 |
| Male | 1.58 ± 0.98 | |
| Telomere length vs age (years) | ||
| Very short | 42.34 ± 11.15 | 2.671, 0.048 |
| Short | 45.22 ± 11.92 | |
| Medium | 41.05 ± 11.68 | |
| Large | 39.63 ± 11.31 | |
Note. Numerical variables are expressed as mean and standard deviation (M and S.D) for variables with a normal distribution.
Table 2.
Telomere length of groups I, II, III, IV.
| LTL (2-ΔΔCT) | GIM ± S.D. | GIIM ± S.D. | GIIIM ± S. D | GIVM ± S. D | P |
|---|---|---|---|---|---|
| Very short | 0.004±0.0015 | 0.005±0.0004 | 00.002±0.0012 | 0.0035±0.0024 | |
| Short | 0.01±0.005 | 0.023±0.023 | 0.040±0.027 | 0.012±0.0047 | |
| Medium | 0.062±0.03 | 0.061±0.030. | 0.059±0.023 | 0.064±0.026 | |
| Large | 1.052±1.74* | 0.6±0.56 | 0.62±0.79 | 0.49±0.65 | 0.022 |
Note. Numerical variables are expressed as mean and standard deviation (M and S.D.), the interquartile range for variables with non-normal distribution. ANOVA test (p<0.05).
Table 3.
LTL and cognitive changes in subjects with COVID-19.
| Assessment | LTL | MOCA | MMSE | F | df | p | ƞp2 |
|---|---|---|---|---|---|---|---|
| Survey I | 1.457 | 6 | 0.198 | 0.185 | |||
| Very short | 23.20 ± 2.68 | 28.00 ± 4.30 | |||||
| Short | 23.00 ± 2.98 | 29.90 ± 4.93 | |||||
| Medium | 23.80 ± 1.92 | 33.40 ± 1.82 | |||||
| Large | 25.75 ± 2.50 | 29.75 ± 1.50 | |||||
| Survey II | 1.490 | 4 | 0.226 | 0.142 | |||
| Very short | 26.67 ± 3.22 | 34.33 ± 1.16 | |||||
| Short | - | - | |||||
| Medium | 24.50 ± 3.92 | 30.30 ± 2.75 | |||||
| Large | 25.78 ± 2.73 | 29.22 ± 4.12 |
Note: The MMSE and MOCA scores are expressed as mean (M) and standard deviation (SD); MANOVA tests were employed.
Table 4.
LTL and cognitive changes between surveys in subjects with post-COVID-19.
| Variable | Survey I | Survey II | p |
|---|---|---|---|
| MMSE vs LTL | |||
| Very short | 34 ±1.41 | 27.66 ± 4.51 | 0.163 |
| Short | - | - | - |
| Medium | 29.37 ± 2.9 | 32.45±2.46 | 0.023 |
| Large | 28.83 ± 036 | 29.66±4.18 | 0.732679 |
| MOCA vs LTL | |||
| Very short | 22.25±3.41 | 21.67± 4.16 | 0.37 |
| Short | 25.50 ±.71 | 25.50 ±.1.21 | 0.87 |
| Medium | 24.33±3.05 | 22.45 ± 3.50 | 0.79 |
| Large | 23± 0.5 | 22.78±4.38 | 0.22 |
Note: The MMSE and MOCA scores are expressed as mean (M), and standard deviation (SD); paired T Student tests for each LTL category were used.
Table 5.
Distribution of cognitive changes and telomere length in subjects with COVID-19.
| Cognitive changes | No cognitive changes | X2, p | |
|---|---|---|---|
| MMSE | 6, 15 % | 34, 85 % | |
| Very short | 3, 50.0% | 7, 20.6% | 3.92, 0.27 |
| Short | 1, 16.7% | 9, 26.5% | |
| Medium | 0, 0.0% | 10, 29.4% | |
| Large | 2, 33.3% | 8, 23.5% | |
| MoCA | 29, 72.5 % | 11, 27.5 % | |
| Very short | 9, 31.0% | 1, 9.1% | 4.39, 0.22 |
| Short | 5, 17.2% | 5, 45.5% | |
| Medium | 7, 24.1%, | 3, 27.3% | |
| Large | 8, 27.6% | 2, 18.2% |
Note: Cognitive changes and LTL categories are expressed as n (%); the Chi-square test was used.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



