
Submitted:
02 September 2024
Posted:
04 September 2024
You are already at the latest version
Abstract
Work disparities experienced by nurses in long-term care (LTC) can impact the retention, well-being, and health of this workforce. Despite the significant impact disparities experienced by nurses have on the workforce and LTC sector, a review of the available literature on work disparities has not been conducted on work disparities experienced by nurses in LTC. Consequently, this scoping review aimed to explore the nature and extent of research on meso-level work disparities experienced by nurses in LTC and how such disparities are linked with nurse health and well-being. Five databases were searched: MEDLINE (Ovid), EMBASE (Ovid), PsycINFO (Ovid), and CINAHL (EBSCO host). Of the 5,652 articles retrieved, 16 studies published between 1997 and 2024 met the inclusion criteria. The average number of work disparities within each study was 3.06 (minimum = 1, maximum = 6, SD = 1.62). Types of work disparities across the 16 studies were work opportunities (n = 19), work treatment (n = 18), job security (n = 8), and work compensation (n = 8). Only four articles investigated the association of a work disparity with a variable of health and well-being. Future research on how macro-level disparities intersect with meso-level work disparities may inform a contextual understanding of how disparities transpire in the work of nurses in LTC. Studies are required to address the gaps in knowledge regarding how work disparities negatively influence the health of nurses to inform better retention, well-being, and health of nurses in LTC.
Keywords:
Work Disparities
; Long Term Care
; Continuing Care
; Nursing Staff
; Well-Being
; Health
; Nursing Governance
; Dissatisfaction
; Inequality
1. Introduction
Maintaining adequate work force participation and retention of nurses in the long-term care (LTC) sector is a global issue of interest [1,2,3]. Higher demand for LTC services [4] is expected due to the rapidly growing aging population [5]. Further, the LTC sector has experienced challenges in recruiting and retaining nurses, with projected nursing staffing shortages estimated to be approximately 58,600 by 2029 in Canada and 63,720 by 2030 in the United States within the LTC sector [4,6]. These systemic inequities and social challenges can lead to unintentional work disparities [7]. For instance, a common work disparity experienced by nurses is the difference in pay within work sector [8]. When filling shifts during the COVID-19 pandemic, higher-paid agency external nurses were required, as the few remaining lower-paid in-house nurses were already doing double shifts and managing heavy workloads [9]. Other disparities can be related to experiences of mismatch between demands and job resources in the workplace [10], including increased mandatory overtime [7] and the unfair distribution of work expected by some workers over others [11,12]. These types of disparities among groups of nurses in LTC are also linked with outcomes of job dissatisfaction [13], along with increased absence from work due to burnout-related strain and stress related to excessive physical or emotional labor [14]. While these examples represent some types of work disparities, the extent of work disparities experienced among groups of nurses in LTC, especially those that negatively impact health and well-being at work, is not fully understood. Further investigation is warranted to inform actions and initiatives to support nurse well-being and retention in LTC.
Work disparity is a complex construct expressed in various ways [15]. For instance, the National Institute of Occupational Safety and Health (NIOSH) [16] utilizes “health inequities” interchangeably with “health disparities” when drawing upon medical and social determinants of health models. Ndugga et al. [17] described disparities as “differences in health and health care between groups that stem from broader social and economic inequities.” Further, recognizing that disparities were inconsistently named or identified, members of the present research team [15] analyzed a sample of literature to develop a conceptual framework prior to the analysis associated with the present review. According to this framework [15], work disparities are defined as “[i]nequalities or differences experienced between groups of workers or collectives in the following four categories related to work: job security, work compensation, work opportunities, and workplace treatment. These inequalities or differences may be linked to differences in groups of workers and/or in group identities (collectives).” Common to the three descriptions of work disparities [15,16,17] is that an intersectional approach is needed to learn more about how disparities are manifested in different work contexts or sectors. Ultimately, intersectional research on both the meso- (workplace level) and macro- (system level) [18] categories of work disparities among groups of workers has the potential to advance this knowledge within the context of LTC. To initiate these types of analyses, the present scoping review study was designed using the meso-level disparities reflected in the work disparity conceptual framework [15].
Other gaps in knowledge relate to how work disparities among nurses in LTC are associated with health and well-being. For the purposes of this review, health and well-being refer to the overall physical, mental, and social state of individuals and groups achieved through doing the things they need, want, and are expected to do with respect to everyday activities that occupy time and bring meaning and purpose to life. This definition drew on two sources [19,20] and was intended to reflect an occupational perspective on the health and well-being of nurses. Information on links between work disparities to health and well-being may lend insights into ways to improve work practices that guide the day-to-day work of nurses, worker health programs at work, worker benefits, and the retention of nurses in LTC [15]. Le [21] noted that there is a need for health surveillance programs to support further knowledge on how health is impacted by groups of workers experiencing work disparities. Thus, the objectives of this scoping review study were to explore the nature and extent of literature on work disparities among nurses in LTC, with a focus on meso-level disparities and their association with nurse health and well-being. By conducting this review, this analysis is intended to support the identification of gaps in the research literature and opportunities to study work disparities experienced by nurses in LTC.
2. Materials and Methods
2.1. Study Design
In alignment with Arksey & O’Malley’s proposed framework [22], the present scoping review was conducted via the following stages: (1) identify research question (a review of literature and discussion of team members supported the identification of the research question); (2) identify relevant literature (the research team discussed with the team librarian and search terms were defined and revised after an initial search in Medline OVID); (3) study selection (inclusion and exclusion criteria were developed for title and abstract, and full text screening using Covidence); (4) data extraction (demographic data and data on work disparities and links to health were extracted into an Microsoft Excel file); and (5) data analysis (descriptive summaries using tabular data were completed). The scoping review methodology was selected based on the need to use a systematic process to identify, organize, and analyze information on studies related to disparities experienced by nurses in LTC. The work disparity conceptual framework proposed by Shaw et al. [15], including the definition of work disparities, terminology, and categories presented, was used to guide this review (see Appendix A for definitions of terminology used within the conceptual framework). Covidence software [23] was used for the de-duplication and screening processes. We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) Checklist in reporting this study [24] (see Table S1).
2.2. Search Strategy
The search strategy was developed and refined in consultation with a Teaching and Learning Librarian who was part of the research team (MS). Two searches were conducted. An initial search was performed on MEDLINE (Ovid), EMBASE (Ovid), PsycINFO (Ovid), CINAHL (EBSCO host), and SCOPUS on January 25, 2024. To update the search and ensure that no additional articles met the inclusion criteria, a subsequent search was conducted on August 14, 2024 in MEDLINE (Ovid), EMBASE (Ovid), PsycINFO (Ovid) and on August 27, 2024 in CINAHL and SCOPUS. No date limits or language limits were applied to the search results. The full search strategy for MEDLINE (Ovid), which was adapted to the requirements of other databases (e.g., SCOPUS’ use of keywords only), can be found in Table S2. RIS files obtained from each database were uploaded to Covidence for further screening.
2.3. Study Selection
To facilitate study selection, the following categories provided by the Joanna Briggs Institute (JBI) [25] were used to organize the inclusion and exclusion criteria: (1) phenomenon of interest; (2) context; (3) types of participants; and (4) types of studies.
2.3.1. Phenomenon of Interest
This scoping review included studies that investigated work disparities of nurses in LTC (i.e., nurses in LTC were required to be part of at least one comparator group of an identified work disparity; see Appendix A for definition of ‘comparator group’). The rationale behind conducting the study was also required to be informed by concerns related to nurse health and well-being. For the purposes of the present analysis, categories of concerns related to health and well-being were grouped into four categories: (1) emotional health (e.g., burnout, stressors related to emotional strain of caregiving); (2) physical health (e.g., musculoskeletal, sprains, injuries, fatigue, physical strains due to exposures at work); (3) mental health (e.g., conditions listed on IDC-9 codes [26] including, depression and anxiety, along with psychological safety factors [27]); and (4) general health (i.e., a non-specific category where health was referred to in general).
2.3.2. Context
Studies that met the inclusion criteria included LTC settings (e.g., nursing homes, personal care homes, and residential care facilities). LTC settings are “residential homes that provide ongoing care to patients whose care needs cannot be met in the community,” where patients predominantly require this care due to “advancing age, disability, or declining health” [28]. Non-residential settings that provided care to patients over a short period of time (e.g., acute care settings, hospitals, and skilled nursing facilities) were excluded from the present analysis.
2.3.3. Types of Participants
Studies that met the inclusion criteria were required to have participants that were regulated and/or licensed nurses (e.g., Registered Nurses [RNs], Registered Practical Nurses [RPNs], Nurse Practitioners [NPs], Licensed Practical Nurses [LPNs], Enrolled Nurses [ENs], Assistant Practitioner Nurses [APs]). Studies with an exclusive focus on nursing managers/administrators; nursing students; personal support workers (e.g., nursing aides, healthcare aides, personal care aides, certified nursing assistants); and non-nursing healthcare personnel were excluded. Further, articles with ambiguity about the nurse’s involvement or where nurses were not clearly categorized as working in LTC settings were excluded.
2.3.4. Types of Studies
Peer-reviewed qualitative, quantitative, and mixed qualitative and quantitative primary studies that were available in English were included in the present analysis. Opinion-based pieces (e.g., editorials), scoping/systematic reviews, dissertations, and grey literature (e.g., newspaper articles, government documents) were excluded. No restrictions on publication year or geographic location were implemented.
2.4. Study Selection
Covidence software [23] was used to remove duplicates and conduct screening. Two independent authors (MM, AN for articles retrieved from the initial search; LS, KN for articles retrieved from the subsequent search) conducted title and abstract screening on de-duplicated studies identified from the database search. Conflicts were resolved through discussion. Full-text articles were retrieved for studies that meet the inclusion criteria and for studies whose relevance is unclear from the abstract. Two out of three authors (LS, MM, KN) then screened each full-text article independently. Disagreements were resolved through discussion to reach consensus with all full-text reviewers (LS, MM, KN).
2.5. Data Extraction
Three authors (LS, MM, KN) extracted and organized data from the included studies using a data extraction form. The development of the data extraction form was informed by the work disparity conceptual framework [15] to support the organization of data related to work disparity variables and comparator groups. In accordance with this framework, work disparities extracted were categorized into meso-level “variable of disparity” categories (i.e., job security, work compensation, work treatment, and work opportunity), comparator group identities, and comparator group subdivision categories. Data were independently extracted and categorized, as applicable, by one author and reviewed by at least one other author for completion (LS, MM, KN).
The following demographic data were extracted: author(s), year of publication, country, journal scope, type of study, study aim, methodology, study population, data analysis, number of work disparities, study findings, future directions for research, and use of work disparity terminology. Further, work disparities within the included articles were extracted, and the following information was used to categorize each of them: work disparity comparator groups, work disparity comparator group subdivision, variable of work disparity, and variable of work disparity categorization (see Appendix A for definitions). Other data needed to describe the nature of knowledge in the study of work disparities related to health and well-being were also extracted: study rationale associated with health and wellness, the type of health and/or well-being described within the study rationale (i.e., physical health, emotional health, mental health, and general health), and whether health and well-being were analyzed in relation to work disparities as part of the study analysis and/or using external literature.
2.6. Quality Appraisal
A quality appraisal of the qualitative and quantitative articles was conducted using a modified version of Hawker et al.’s quality appraisal criteria [29]. The tool consists of nine subscales to rate articles: (1) abstract and title; (2) introduction and aims; (3) method and data; (4) sampling; (5) data analysis; (6) ethics and bias; (7) results; (8) transferability and generalizability; and (9) implications and usefulness. The items in each subscale are rated on a 4-point scale, with ratings of very poor (1), poor (2), fair (3), and good (4). Each article received a total score within a range of 9-36; a score of 28-36 was associated with good quality, 20-27 for fair quality, 10-20 for poor quality, and less than 10 for very poor-quality articles [29]. Ratings were independently assigned by one author and reviewed by at least one other author for consensus (LS, MM, KN). Disagreements were to be resolved through discussion, although none occurred. Articles in this review were not excluded based on study quality but were utilized to inform the overarching findings of the review.
2.7. Data Synthesis
Results were organized to describe the nature and extent of work disparities found using narrative description and tabular formatting. This included categorizing the data according to: (1) study characteristics; (2) work disparity traits; and (3) health and well-being features. Descriptive statistics of individual variables (e.g., frequencies of identified work disparity characteristics) have been presented using narrative synthesis.
3. Results
3.1. Search Results
A total of 5,652 records were identified from all databases after both searches. Following de-duplication, title and abstract screening were performed on the remaining records (n = 3,403) and resulted in 464 articles. Full-text screening was executed on all retrieved studies (n = 464). After this process, a total of 16 articles met the inclusion criteria and were included in the present review. See Figure 1 for the PRISMA flowchart diagram.
Figure 1. PRISMA Flowchart. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71.
3.2. Eligible Source Characteristics
Sixteen articles published between 1997 and 2024 met the inclusion criteria following screening (see Table 1 for study characteristics). Articles originated from the United States (n = 7), the Netherlands (n = 2), Sweden (n = 2), Germany (n = 1), Korea (n = 1), Slovenia (n = 1), Spain (n = 1), and the United Kingdom (n = 1). While most sources conducted a cross-sectional survey (n = 9), studies also conducted national surveys (n = 3), qualitative analyses (n = 2), a mixed-methods study (n = 1), and a causal model of turnover and a predictive study (n = 1). The average number of work disparities within each study was 3.06 (minimum = 1, maximum = 6, SD = 1.62). Most articles (n = 13) did not make use of work disparity terminology (e.g., “work disparity,” “inequality,” and “inequity”) to describe the work disparities within that given study. Of the three that did employ such terminology, two articles used “inequalities” and one used “disparity of working conditions” as descriptors. Hawker and Payne’s (2002) quality appraisal identified that 14 studies were of good quality, two were of fair quality, and none were of poor quality.
3.3. Work Disparities
A total of 53 work disparities were identified from the 16 studies that met the inclusion criteria (see Table S3 for the complete list of work disparities). The group identity comparison variable across all identified work disparities was as follows: professional status (n = 14), location of work (n = 10), age (n = 8), race (n = 7), gender (n = 6), marital status (n = 3), experience (n = 2), education status (n = 1), geographic location (n = 1), and number of children (n = 1). Out of the 53 work disparities, 19 were classified as a “work opportunity”, 18 as a “workplace treatment”, and 8 as being related to “job security” and “work compensation”, respectively. Comparator group subdivisions of work disparities were classified as: 7 “simple intragroup”, 14 “simple intergroup”, 21 “mixed intragroup”, and 11 “mixed intergroup” disparities. A matrix presenting the number of work disparities with each comparator group subdivision in comparison to each variable of disparity category is provided in Table 2.
3.3. Health and Well-Being
The background rationale for each study in this review noted that nurses experienced several types of health conditions and/or disruptions in relation to well-being in LTC. Specifically, types of health and well-being emphasized physical health (n = 8), general health (n = 4), emotional health (n = 4), and mental health (n = 8). Not all studies investigated health and well-being links to work disparity. Four studies investigated the association of an identified work disparity with a variable of health and well-being as part of their analysis. Five studies used external literature to describe the association between a variable of health and well-being and an identified work disparity. See Table S4 for health and well-being data for all included studies.
4. Discussion
This scoping review describes work disparities experienced by nurses in the LTC sector within the research literature. A total of 16 articles conducted in seven countries over 26 years (1997–2024) met the inclusion criteria (see Table 1 for study characteristics). Further, 53 work disparities were identified, extracted, and categorized from these articles (see Table S3). Results provide an insight into the complexity of examining work disparities for nurses in LTC, what is known, how work disparities have been studied, and what is needed to advance research on the work disparities of nurses in the LTC sector.
Findings from this study suggest that the concept of work disparities is complex, difficult to understand, and challenging to research. Work disparities have not been consistently expressed using common terminology across the nursing literature in LTC [15]. Within the present review, only three articles used “work disparity” and/or similar terminology (i.e., “inequalities” and “disparity of working conditions”) to describe the work disparities present within their studies, while the remaining articles (n = 13) did not. Moreover, ways to categorize and analyze different types of work disparities with the nuance and reflection of different workplace settings and contexts are predominantly absent within the research literature for nurses in LTC. In response, the authors of the present scoping review were required to create a conceptual framework that provided definitions and categorizations (see [15]) to allow for the identification and exploration of work disparities. With work disparities being a complex yet necessary concept to analyze, the absence of a mechanism to conduct research and understand work disparities suggests that a gap is present on this topic and that increased research to develop such frameworks is required to allow for the understanding of the day-to-day experiences and inequities experienced by nurses in LTC.
The use of the work disparity conceptual framework terminology [15] supported the framing of the 53 work disparities identified from the 16 included studies into four meso-level work disparity categories (i.e., work opportunities [n = 19], work treatment [n = 18], job security [n = 8], work compensation [n = 8]). These categories offer an initial and novel starting point to make the knowledge on the work disparities in the LTC sector more readily understood and apparent in research. These results highlight that inequitable or in accessible opportunities for career growth or growth within the workplace and differences in work practices are areas that LTC organizations may begin to investigate, address, and focus on approaches to prevent the negative health and social impacts on nurses. The precarity of the nature of work in LTC nursing (part-time versus-full time) for groups of workers related to job security and differences in pay or access to health benefits among groups of nurses may have links to poor retention, and nurses' dissatisfaction in working in LTC. Future attention on examining these four categories at the meso-level may provide a more consistent approach in investigating work disparities. However, further knowledge of macro-level disparities for nurses in LTC, along with how meso- and macro-level work disparities intersect [15,17,30], is required. Shaw and colleagues [30,31,32] and Ndugga et al. [17] have advocated that research into macro-level issues is warranted to advance systemic and contextual knowledge of how systemic inequities manifest work disparities that emerge at the meso-level. Thus, to advance knowledge of work disparities that are experienced by groups of nurses in LTC, an intersectoral approach will help inform where there are opportunities to make changes in this sector.
The variables used to compare groups within the 53 identified work disparities were categorized as part of this analysis, with the most frequently mentioned being professional status (n = 14), location of work (n = 10), age (n = 8), race (n = 7), gender (n = 6), and the least being marital status (n = 3), experience (n = 2), education status (n = 1), geographic location (n = 1), and number of children (n = 1). These categories suggest that a diversity of issues is being investigated within research related to nurses in LTC, all of which were reported to be relevant with regards to the treatment and experiences of nurses in LTC in the 16 studies in this review. In these studies, professional status was used to compare groups. Given that the professional status of nursing staff in long term care varies and that there can be shifts in education (e.g., through bridging programs from RPN’s to LPN’s and LPN’s to RN’s [33]), the variables of professional status, experience, and educational status will continue to be needed to identify emergent disparities that may arise due to these changes for nurses in LTC. While comparing groups of nurses using variables such as work location, geographical location, or number of children may support a contextual understanding of work life disparities, results suggest that they have not been frequently investigated. However, results from this review also suggest that specific variables that impact nurses in LTC have not been adequately investigated to date, and others may be needed, including, but not limited to, socioeconomic status, sexual orientation, religious identity, and physical ability. Ndugga et al. [17] have argued for an increased focus on these variables, with a specific emphasis on social determinants of health, to deepen the understanding of the lived experiences of nurses. Recognizing the importance of diversity, equity, and inclusivity within LTC contexts at policy and community of practice levels [34,35], these findings suggest that research needs to be conducted on a broader scale and account for a larger diversity of backgrounds when investigating work disparities in relation to nurses in LTC [17].
Adhering to the conceptual framework proposed by Shaw et al. [15], this scoping review categorized work disparities in accordance with the four ways that nurses in LTC (i.e., target group) may be compared with other groups within the healthcare system. Specifically, work disparities were categorized as simple intragroup (n = 7), simple intergroup (n = 14), mixed intragroup (n = 21), and mixed intergroup disparities (n = 11; see Table S3). Results revealed that work disparities of nurses in LTC were studied more often as part of a mixed group with other healthcare workers (i.e., as part of mixed intragroup/intergroup disparities [n = 32]) and less often as isolated, homogenous groups solely including nurses from LTC (i.e., as simple intragroup/intergroup disparities [n = 21]). While the value of each type of comparison has not been evaluated, such observations suggest that definitive conclusions on the experiences of nurses in LTC are difficult to ascertain because most research on work disparities has included nurses in LTC as part of a larger group. Future research, where experiences solely within nurses in LTC (i.e., simple intragroup disparities) or solely between nurses in LTC and another healthcare group (i.e., simple intergroup disparities) are analyzed, will be beneficial in enriching work disparity literature. The matrix of comparator group subdivisions of work disparities (see explanation in [15]) may support such study designs and help provide clarity on the framing of the comparator groups in studies of work disparities.
Key areas of health concerns related to nurses in LTC informed the need for an examination of differences and inequities. The most salient health concerns were physical health (n = 8), general health (n = 4), emotional health (n = 4), and mental health (n = 8; see Table S4). Despite the importance of health and wellbeing as drivers that underscored the research investigations, only four out of the 16 included studies examined specific health outcomes or used measures as part of their research design (Table S4). Such results suggest that insufficient information exists on how to identify the health impact of work disparities on workers. This finding is consistent with Le’s [21] observations and suggests that more knowledge on how to approach health surveillance, which considers the intersection of the worker, the workplace, and the broader nursing context, is necessary. Research related to the resilience of nurses is required to support the understanding of how resilience links to health in relationship to challenging work demands in the LTC sector [36,37,38]. For instance, the focus on building individual resilience has prompted a breadth of training for nurses in LTC [39,40,41]. However, an emphasis on resilience is only one aspect of supporting better health and the retention of nurses in this sector. More knowledge on the types of work disparities that impact the health and well-being of nursing staff in LTC, beyond individual resilience, may also inform opportunities to improve the retention of groups of nurses working in the LTC sector. An intersectoral approach that considers perspectives and knowledges across occupational health and safety organizations, ministries of health and LTC administration, researchers in workforce planning, organizational health and well-being, occupational science, physical therapy science, and nursing science, as well as nursing professional, regulatory, and/or labour associations, can elucidate the association between health and work disparities, such that a holistic understanding of the experiences of nurses in LTC may be taken into account and responded to on a higher level.
4.1. Strengths and Limitations
The strength of this review study is the use of a novel conceptual framework to structure the findings that was specifically developed to understand work disparities in the LTC for nurses [15]. The terminology supported the search, selection, and data extraction needed to inform a description of what exists in the literature that relates to the health and well-being of nurses and how work disparities can be understood within the workplace, as well as guide future studies on such disparities. Another strength of this review is the comprehensive search of multiple databases using a librarian’s support and multiple reviewers, which supported the integrity of the search and selection processes. A strength of the included literature is that this review focused specifically on knowledge of inequities of licenced nurses in the LTC sector which revealed a realm of meso-level work disparities that may impact the health for this group of nurses.
Alternatively, this review did not include grey literature, which may have limited other information that could expand knowledge of meso-factors that shape work disparities in LTC for groups of nurses. Further, studies were limited to articles available in English therefore relevant knowledge may have been missed and future work is needed to expand the search to other languages. A limitation of the included literature was that geographical representation was discovered to be restricted to Korea, Europe, the USA, the UK, and Scandinavia. Given that work disparities experienced by nurses in LTC are situated globally and shortages of nurses are forecasted within other regions (e.g., Canada), more work that studies disparities and their impact on groups of nurses is warranted on a global scale.
5. Conclusions
This scoping review revealed the extent and nature of knowledge present in the research literature with regards to meso-level work disparities experienced by nurses in LTC. Results suggest that work disparities are a complex phenomenon to analyze and revealed gaps in the literature with studies analyzing work disparities experienced by nurses in LTC. Further examination of macro-level factors is indicated to move towards an intersectoral approach in the study of the complex issue of work disparities. Future research is warranted to expand the conceptual understandings, tools, and instruments with regards to examining work disparities. Furthermore, more studies are required to increase the scope of understanding of the link between work disparities and health and retention. In doing so, such research may enable policy, practice, and resources to increase retention and facilitate better work for nurses in LTC.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) Checklist; Table S2. MEDLINE (Ovid) Search Strategy for Work Disparities Experienced by Nurses in Long-Term Care (LTC) conducted on January 25, 2024; Table S3. Work Disparities Identified from Included Studies; Table S4. Health and Well-Being Association within Included Articles.
Author Contributions
Conceptualization, LS, MM, KN, DC, MS, NG, AG, AN; methodology, LS, MM, KN, AN; validation, LS, MM, KN, AN; formal analysis, MM, LS, KN; investigation, LS, MM, KN; data curation, LS, MM, KN; writing—original draft preparation, LS, MM.; writing—review and editing, LS, MM, KN, DC, MS, NG, AG; visualization, MM; supervision, LS, DC; funding acquisition, LS, DC.
Funding
This research received no external funding. Internal research startup funds were used to support highly qualified trainees and research assistants from Western University.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A. Work Disparity Conceptual Framework Terminology
| Term | Definition | |
| 1. Variable of work disparity | Any defined factor, construct, or characteristic of inequality, or factor of unfairness/difference. Four categories were identified based on a sample of the literature on work disparities experienced in LTC for nurses: job security, work compensation, work opportunities, and/or workplace treatment. | |
| 1a. Measure of disparity | Values that quantitatively/qualitatively measure, examine, and/or explore variables of work disparity. | |
| 1b. Categories | Examples* | |
| 1b(i). Job Security | Hiring /dismissal practices, Intent to leave, Retention, Recruitment | |
| 1b(ii). Work Compensation | Wages, Benefits, Paid-vacation days, Health insurance | |
| 1b(iii). Work Opportunities | Ability to be promoted in an organization, Development opportunities, Exposure to challenging/meaningful work, Amount of work provided | |
| 1b(iv). Workplace Treatment | Discrimination, Expectations/demands of performance (e.g., emotional labor, cognitive labor demands), Recognition of contributions, Work satisfaction | |
| 2. Comparator Group | A group of individuals (workers) composed of members of the workforce. | |
| 2a. Group identity | The identity associated with each individual comparator group (e.g., gender, race, socioeconomic status, residency status, educational status, profession, indigenous status, work setting, age, sexuality, disability, height, identities 2SLGBTQAI plus, weight, ethnicity, and religion). | |
| 2b. Group identity Comparison Variable | The group identity that differentiates one comparator group from the other for a specific work disparity (e.g., if a work disparity is identified between old and young workers, the group identity comparison variable would be ‘age’). The group identity comparison variable must be related to the demographic variables and must not be subjective in nature (e.g., job satisfaction cannot be a group identity comparison variable because it is a subjective measure). | |
| Note. Reprinted with permission from IOS Press | ||
References
- Bourgeault, I.L.; Maier, C.B.; Dieleman, M.; Ball, J.; MacKenzie, A.; Nancarrow, S.; Nigenda, G.; Sidat, M. The COVID-19 Pandemic Presents an Opportunity to Develop More Sustainable Health Workforces. Hum. Resour. Health 2020, 18, 83. [Google Scholar] [CrossRef]
- Government of Ontario A Better Place to Live, a Better Place to Work: Ontario’s Long-Term Care Staffing Plan (2021-2025); 2020.
- American Association of Colleges of Nursing Fact Sheet: Nursing Shortage; 2024.
- Ontario Long Term Care Association [OLTCA] The Data: Long-Term Care in Ontario. Available online: https://www.oltca.com/about-long-term-care/the-data/ (accessed on 25 July 2024).
- United Nations Global Issues: Ageing. Available online: https://www.un.org/en/global-issues/ageing (accessed on 25 July 2024).
- HRSA Health Workforce Nurse Workforce Projections, 2020-2035; 2022.
- Bae, S.-H.; Brewer, C. Mandatory Overtime Regulations and Nurse Overtime. Policy Polit. Nurs. Pract. 2010, 11, 99–107. [Google Scholar] [CrossRef]
- Wagner, L.M.; Bates, T.; Spetz, J. The Association of Race, Ethnicity, and Wages Among Registered Nurses in Long-Term Care. Med. Care 2021, 59, S479–S485. [Google Scholar] [CrossRef]
- Holroyd-Leduc, J.M.; Laupacis, A. Continuing Care and COVID-19: A Canadian Tragedy That Must Not Be Allowed to Happen Again. CMAJ Can. Med. Assoc. J. J. Assoc. Medicale Can. 2020, 192, E632–E633. [Google Scholar] [CrossRef]
- Blanco-Donoso, L.M.; Moreno-Jiménez, J.; Amutio, A.; Gallego-Alberto, L.; Moreno-Jiménez, B.; Garrosa, E. Stressors, Job Resources, Fear of Contagion, and Secondary Traumatic Stress Among Nursing Home Workers in Face of the COVID-19: The Case of Spain. J. Appl. Gerontol. 2021, 40, 244–256. [Google Scholar] [CrossRef]
- Ostaszkiewicz, J.; O’Connell, B.; Dunning, T. “We Just Do the Dirty Work”: Dealing with Incontinence, Courtesy Stigma and the Low Occupational Status of Carework in Long-Term Aged Care Facilities. J. Clin. Nurs. 2016, 25, 2528–2541. [Google Scholar] [CrossRef]
- Zhang, H.; Li, H.; Tian, W.; Liu, W.; Yang, Y. The Influence of Professional Identity on Work Engagement among Nurses Working in Nursing Homes in China. J. Nurs. Manag. 2022, 30, 3022–3030. [Google Scholar] [CrossRef]
- White, E.M.; Aiken, L.H.; McHugh, M.D. Registered Nurse Burnout, Job Dissatisfaction, and Missed Care in Nursing Homes. J. Am. Geriatr. Soc. 2019, 67, 2065–2071. [Google Scholar] [CrossRef]
- Boamah, S.A.; Kalu, M.E.; Havaei, F.; McMillan, K.; Belita, E. Predictors of Nursing Faculty Job and Career Satisfaction, Turnover Intentions, and Professional Outlook: A National Survey. Healthcare 2023, 11, 2099. [Google Scholar] [CrossRef] [PubMed]
- Shaw, L.; Masood, M.; Neufeld, K.; Connelly, D.M.; Stanley, M.; Guitar, N.A.; Garnett, A.; Nikkhou, A. A Conceptual Framework for Defining Work Disparities: A Case of Nurses in Long Term Care. (under review WORK 2024).
- Leong, F.T.L.; Eggerth, D.E.; Chang, C.-H. (Daisy); Flynn, M.A.; Ford, J.K.; Martinez, R.O. Introduction. In Occupational health disparities: Improving the well-being of ethnic and racial minority workers; APA/MSU series on multicultural psychology; American Psychological Association: Washington, DC, US, 2017; pp. 3–21; ISBN 978-1-4338-2692-4.
- Ndugga, N.; Pillai, D.; Artiga, S. Disparities in Health and Health Care: 5 Key Questions and Answers. KFF 2024.
- Antao, L.; Shaw, L.; Ollson, K.; Reen, K.; To, F.; Bossers, A.; Cooper, L. Chronic Pain in Episodic Illness and Its Influence on Work Occupations: A Scoping Review. Work Read. Mass 2013, 44, 11–36. [Google Scholar] [CrossRef]
- World Health Organization Constitution. Available online: https://www.who.int/about/governance/constitution (accessed on 25 August 2024).
- World Federation of Occupational Therapists (WFOT) About Occupational Therapy. Available online: https://wfot.org/about/about-occupational-therapy (accessed on 25 August 2024).
- Le, A. Occupational Health Disparities. Available online: https://synergist.aiha.org/202305-occupational-health-disparities (accessed on 17 August 2024).
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Covidence Title Page. Available online: https://www.covidence.org/ (accessed on 17 August 2024).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Aromataris, E.; Lockwood, C.; Porritt, K.; Pilla, B.; Jordan, Z. ; Editors JBI Manual for Evidence Synthesis. Available online: https://jbi-global-wiki.refined.site/space/MANUAL (accessed on 17 August 2024).
- Canadian Institute for Health Information ICD-9/CCP and ICD-9-CM. Available online: https://www.cihi.ca/en/icd-9ccp-and-icd-9-cm (accessed on 17 August 2024).
- Mental Health Commission of Canada National Standard. Available online: https://mentalhealthcommission.ca/national-standard/ (accessed on 19 August 2024).
- Ontario Health at Home Long-Term Care. Available online: https://ontariohealthathome.ca/long-term-care/ (accessed on 17 August 2024).
- Hawker, S.; Payne, S.; Kerr, C.; Hardey, M.; Powell, J. Appraising the Evidence: Reviewing Disparate Data Systematically. Qual. Health Res. 2002, 12, 1284–1299. [Google Scholar] [CrossRef]
- Shaw, L.; Rudman, D.L. Using Occupational Science to Study Occupational Transitions in the Realm of Work: From Micro to Macro Levels. Work Read. Mass 2009, 32, 361–364. [Google Scholar] [CrossRef]
- Shaw, L.; Jacobs, K.; Rudman, D.; Magalhaes, L.; Huot, S.; Prodinger, B.; Mandich, A.; Hocking, C.; Akande, V.; Backman, C.; et al. Directions for Advancing the Study of Work Transitions in the 21st Century. Work Read. Mass 2012, 41, 369–377. [Google Scholar] [CrossRef]
- Shaw, L.; Thoren, C.; Joudrey, K. Retrospective Review of Work Transition Narratives: Advancing Occupational Perspectives and Strategies. Work Read. Mass 2023, 76, 969–978. [Google Scholar] [CrossRef]
- Connelly, D.M.; Guitar, N.A.; Atkinson, A.N.; Janssen, S.M.; Snobelen, N. Learnings from Nursing Bridging Education Programs: A Scoping Review. Nurse Educ. Pract. 2023, 73, 103833. [Google Scholar] [CrossRef]
- Um, S. Reforming Long-Term Care Requires a Diversity and Equity Approach. Available online: https://policyoptions.irpp.org/magazines/may-2021/reforming-long-term-care-requires-a-diversity-and-equity-approach/ (accessed on 17 August 2024).
- Galik, E. Learning to Be an Ally: Promoting Diversity, Equity, and Inclusion in Long-Term Care. Caring Ages 2022, 23, 2. [Google Scholar] [CrossRef]
- Connelly, D.M.; Snobelen, N.; Garnett, A.; Guitar, N.; Flores-Sandoval, C.; Sinha, S.; Calver, J.; Pearson, D.; Smith-Carrier, T. Report on Fraying Resilience among the Ontario Registered Practical Nurse Workforce in Long-Term Care Homes during COVID-19. Nurs. Open 2023, 10, 4359–4372. [Google Scholar] [CrossRef]
- Baskin, R.G.; Bartlett, R. Healthcare Worker Resilience during the COVID-19 Pandemic: An Integrative Review. J. Nurs. Manag. 2021, 29, 2329–2342. [Google Scholar] [CrossRef]
- Cooper, A.L.; Brown, J.A.; Rees, C.S.; Leslie, G.D. Nurse Resilience: A Concept Analysis. Int. J. Ment. Health Nurs. 2020, 29, 553–575. [Google Scholar] [CrossRef]
- Clark, P.; Crawford, T.N.; Hulse, B.; Polivka, B.J. Resilience, Moral Distress, and Workplace Engagement in Emergency Department Nurses. West. J. Nurs. Res. 2021, 43, 442–451. [Google Scholar] [CrossRef]
- Lin, L.-C.; Huang, Y.-C.; Carter, P.; Zuniga, J. Resilience among Nurses in Long Term Care and Rehabilitation Settings. Appl. Nurs. Res. ANR 2021, 62, 151518. [Google Scholar] [CrossRef]
- Zhai, X.; Ren, L.-N.; Liu, Y.; Liu, C.-J.; Su, X.-G.; Feng, B.-E. Resilience Training for Nurses: A Meta-Analysis. J. Hosp. Palliat. Nurs. JHPN Off. J. Hosp. Palliat. Nurses Assoc. 2021, 23, 544–550. [Google Scholar] [CrossRef]
- Banaszak-Holl, J.; Castle, N.G.; Lin, M.K.; Shrivastwa, N.; Spreitzer, G. The Role of Organizational Culture in Retaining Nursing Workforce. The Gerontologist 2015, 55, 462–471. [Google Scholar] [CrossRef]
- Baughman, R.A.; Stanley, B.; Smith, K.E. Second Job Holding Among Direct Care Workers and Nurses: Implications for COVID-19 Transmission in Long-Term Care. Med. Care Res. Rev. MCRR 2022, 79, 151–160. [Google Scholar] [CrossRef]
- Bratt, C.; Gautun, H. Should I Stay or Should I Go? Nurses’ Wishes to Leave Nursing Homes and Home Nursing. J. Nurs. Manag. 2018, 26, 1074–1082. [Google Scholar] [CrossRef]
- Castle, N.G.; Degenholtz, H.; Rosen, J. Determinants of Staff Job Satisfaction of Caregivers in Two Nursing Homes in Pennsylvania. BMC Health Serv. Res. 2006, 6, 60. [Google Scholar] [CrossRef] [PubMed]
- Dill, J.; Duffy, M. Structural Racism And Black Women’s Employment In The US Health Care Sector. Health Aff. Proj. Hope 2022, 41, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Duijs, S.E.; Abma, T.; Plak, O.; Jhingoeri, U.; Abena-Jaspers, Y.; Senoussi, N.; Mazurel, C.; Bourik, Z.; Verdonk, P. Squeezed out: Experienced Precariousness of Self-Employed Care Workers in Residential Long-Term Care, from an Intersectional Perspective. J. Adv. Nurs. 2023, 79, 1799–1814. [Google Scholar] [CrossRef] [PubMed]
- Elwér, S.; Aléx, L.; Hammarström, A. Gender (in)Equality among Employees in Elder Care: Implications for Health. Int. J. Equity Health 2012, 11, 1. [Google Scholar] [CrossRef]
- Hasson, H.; Arnetz, J.E. Nursing Staff Competence, Work Strain, Stress and Satisfaction in Elderly Care: A Comparison of Home-Based Care and Nursing Homes. J. Clin. Nurs. 2008, 17, 468–481. [Google Scholar] [CrossRef] [PubMed]
- Kiyak, H.A.; Namazi, K.H.; Kahana, E.F. Job Commitment and Turnover among Women Working in Facilities Serving Older Persons. Res. Aging 1997, 19, 223–246. [Google Scholar] [CrossRef]
- Krsnik, S.; Erjavec, K. Influence of Sociodemographic, Organizational, and Social Factors on Turnover Consideration Among Eldercare Workers: A Quantitative Survey. Int. J. Environ. Res. Public. Health 2023, 20, 6612. [Google Scholar] [CrossRef]
- Min, D.; Cho, E.; Kim, G.S.; Lee, K.H.; Yoon, J.Y.; Kim, H.J.; Choi, M.H. Factors Associated with Retention Intention of Registered Nurses in Korean Nursing Homes. Int. Nurs. Rev. 2022, 69, 459–469. [Google Scholar] [CrossRef]
- Rahnfeld, M.; Wendsche, J.; Ihle, A.; Müller, S.R.; Kliegel, M. Uncovering the Care Setting-Turnover Intention Relationship of Geriatric Nurses. Eur. J. Ageing 2016, 13, 159–169. [Google Scholar] [CrossRef]
- Ten Hoeve, Y.; Drent, G.; Kastermans, M. Factors Related to Motivation, Organisational Climate and Work Engagement within the Practice Environment of Nurse Practitioners in the Netherlands. J. Clin. Nurs. 2024, 33, 543–558. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Punnett, L.; Mawn, B.; Gore, R. Working Conditions and Mental Health of Nursing Staff in Nursing Homes. Issues Ment. Health Nurs. 2016, 37, 485–492. [Google Scholar] [CrossRef]
Figure 1.
PRISMA Flowchart. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71..
Figure 1.
PRISMA Flowchart. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71..
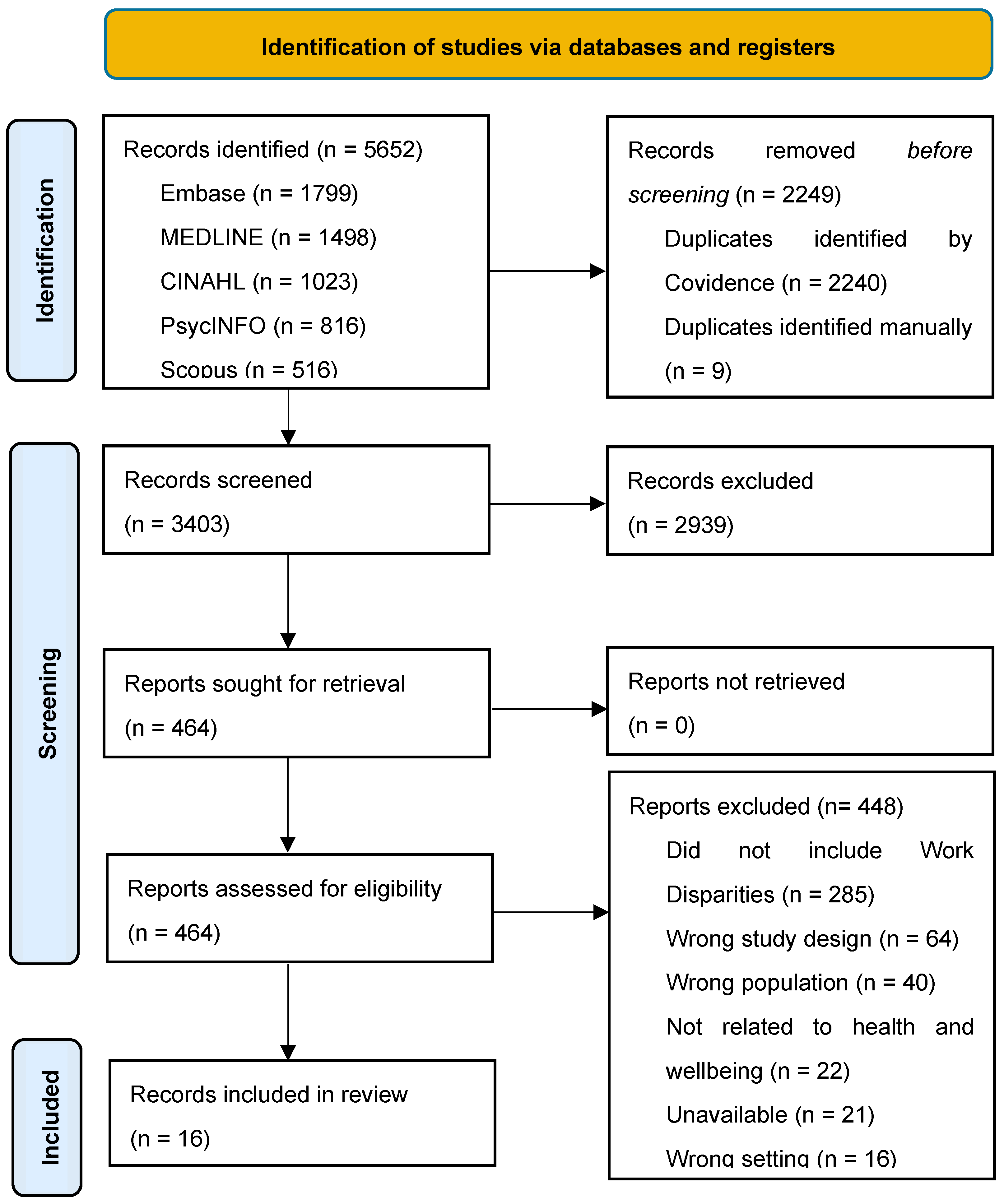

Table 1.
Included Study Characteristics.
| Author (Year) | Country* | Type of Study | Aim | Study Sample | No. of WDs | Use of WD Terms† | Quality Appraisal Score‡ |
|---|---|---|---|---|---|---|---|
| Bae & Brewer (2010) [7] | USA | National Survey | To describe (a) the nature and occurrence of nurse mandatory and voluntary overtime as well as nurse paid on-call hours and (b) the associations with mandatory overtime regulations | N = 6,158 RNs | 6 | No | 30 (G) |
| Banaszak-Holl et al. (2015) [42] | USA | Cross-sectional Survey | To examine how organizational culture in nursing homes affects staff turnover. | N = 419 NH administrators | 1 | No | 31 (G) |
| Baughman et al. (2022) [43] | USA | National Survey | To estimate the rate at which direct care workers and nurses hold multiple jobs, the factors associated with multiple job holding, and the mix of employment across settings for those who do hold a second job. | N = 38,933 Direct care workers/Nurses | 5 | No | 33 (G) |
| Blanco-Donoso et al. (2021) [10] | SPA | Cross-sectional Survey | To analyze the psychological consequences of the COVID-19 pandemic on nursing home workers, as well as the influence of certain related stressors and job resources. | N = 228 NH workers | 2 | No | 33 (G) |
| Bratt & Gautun (2018) [44] | UK | Cross-sectional Survey | To investigate the prevalence of nurses’ wishes to leave work in elderly care services and aims to explain differences between younger and older nurses. | N = 4,945 Nurses | 2 | No | 35 (G) |
| Castle et al. (2006) [45] | USA | Cross-sectional Survey | To examine job satisfaction scores of these caregivers and what characteristics of these caregivers are associated with job satisfaction. | N = 574 NH caregivers | 6 | No | 33 (G) |
| Dill & Duffy (2022) [46] | USA | National Survey | To describe how structural racism and sexism shape the employment trajectories of Black women in the US health care system | N = 125,800 Healthcare workers | 2 | No | 32 (G) |
| Duijis et al. (2023) [47] | NET | Qualitative Analysis | To understand self-employed long-term-care workers' experiences of precariousness, and to unravel how their experiences are shaped at the intersection of gender, class, race, migration and age. | N = 23 Self-employed nurses and NAs in LTC | 2 | Yes; 'Inequalities' | 36 (G) |
| Elwér et al. (2012) [48] | SWE | Qualitative Analysis | To analyze what gender (in)equality means for the employees at a woman-dominated workplace and to discuss possible implications for health experiences | N = 45 NH workers | 4 | Yes; 'Inequalities' | 34 (G) |
| Hasson & Arnetz (2008) [49] | SWE | Cross-sectional Survey | To compare older people care nursing staff’s perceptions of their competence, work strain and work satisfaction in nursing homes and home-based care; and to examine determinants of work satisfaction in both care settings | N = 863 Nursing staff | 2 | No | 32 (G) |
| Kiyak et al. (1997) [50] | USA | Modelling predictive study | To integrate previous approaches to studying turnover in organizations serving elderly persons | N = 308 NH/community agency employees | 3 | No | 26 (F) |
| Krsnik & Erjavec (2023) [51] | SLO | Cross-sectional Survey | To use multivariate analysis to identify the factors at the macro-, meso-, and micro-level that influence LTC workers’ turnover in Slovenia, a typical Central and Eastern European country. | N = 452 LTC workers | 3 | No | 25 (F) |
| Min et al. (2022) [52] | KOR | Mixed-Methods | To identify the factors associated with retention intention among Registered Nurses in South Korean nursing homes | N = 155 RNs | 4 | No | 34 (G) |
| Rahnfeld et al. (2016) [53] | GER | Cross-sectional Survey | To examine mediators in the relationship between care setting and turnover intentions | N = 278 RNs and NAs | 1 | No | 29 (G) |
| TenHoeve et al. (2024) [54] | NET | Cross-sectional Survey | To explore motivation, organisational climate, work engagement and related factors within the practice environment of nurse practitioners | N = 586 NPs | 4 | No | 33 (G) |
| Zhang et al. (2016) [55] | USA | Cross-sectional Survey | To evaluate the association between working conditions and mental health among different nursing groups, and examine the potential moderating effect of job group on this association | N = 1,129 Nursing staff | 3 | Yes; 'Disparity of working conditions' | 32 (G) |
Note. WD: Work Disparities; RN: Registered Nurses; NP: Nurse Practitioner; NA: Nursing Aide; LTC: Long-Term Care; NH: Nursing Home * GER: Germany; KOR: Korea; NET: Netherlands; SLO: Slovenia; SPA: Spain; SWE: Sweden; UK: United Kingdom; USA: United States. † If yes, the article used work disparity terminology (e.g., “work disparity,” “inequality,” and “inequity”) to describe the work disparities within that given study. ‡ G: Good Quality (28-36 points); F: Fair Quality (20-27 points); P: Poor Quality (10-20 points.
Table 2.
Matrix Presenting Categories of Work Disparities (N = 53) from Literature Based on Nurses in LTC.
Table 2.
Matrix Presenting Categories of Work Disparities (N = 53) from Literature Based on Nurses in LTC.
| Comparator Group Subdivision | ||||||
| S-INTRA | S-INTER | M-INTRA | M-INTER | Total | ||
| Variable of Work Disparity Categorization | Job Security | 0 | 2 | 3 | 3 | 8 |
| Work Compensation | 1 | 2 | 3 | 2 | 8 | |
| Work Opportunities | 6 | 4 | 6 | 3 | 19 | |
| Workplace Treatment | 0 | 6 | 9 | 3 | 18 | |
| Total | 7 | 14 | 21 | 11 | 53 | |
Note. S-INTRA: Simple Intragroup Disparity; S-INTER: Simple Intergroup Disparity; M-INTRA: Mixed Intragroup Disparity; M-INTER: Mixed Intergroup Disparity
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



