Submitted:
03 September 2024
Posted:
04 September 2024
You are already at the latest version
Abstract
Objectives: To develop and validate the Communities Geriatric Mild Cognitive Impairment Risk Calculator (CGMCI-Risk), aimed at aiding community healthcare workers in the early identification of individuals at high risk of Mild Cognitive Impairment (MCI); Methods: Based on nationally representative community survey data, backward stepwise regression was employed to screen the variables, and logistic regression was utilized to construct the CGMCI-Risk. Internal validation was conducted using bootstrap resampling, while external validation was performed using temporal validation. The area under the receiver operating characteristic curve (AUROC), calibration curve, and decision curve analysis (DCA) were employed to evaluate the CGMCI-Risk in terms of discrimination, calibration, and net benefit, respectively; Results: The CGMCI-Risk model included variables such as age, educational level, sex, exercise, garden work, TV watching or radio listening, Instrumental Activity of Daily Living (IADL), hearing, and masticatory function. The AUROC was 0.781 (95% CI = 0.766 to 0.796). Calibration curve showed strong agreement, and the DCA suggested substantial clinical utility. In external validation, the CGMCI-Risk model maintained similar performance with an AUROC of 0.782 (95% CI = 0.763 to 0.801); Conclusions: CGMCI-Risk is an effective tool for assessing cognitive function risk within the community. It uses readily predictor variables, allowing community healthcare workers to identify the risk of MCI in older adults over a three-year span.
Keywords:
Mild Cognitive Impairment
; cognitive disorder
; cognitive function
; community health
; healthcare
; prediction model
; risk model
1. Introduction
Mild Cognitive Impairment (MCI) is an intermediate stage between normal aging and dementia, often considered a clinical state that precedes Alzheimer's disease (AD) [1,2]. The global prevalence of MCI among community-dwelling adults aged 50 and older was over 15% [3]. In China, the prevalence of MCI among individuals aged 60 and above is 15.5%, with the number of affected reaching 38.77 million [4]. It is estimated that over 50% of individuals diagnosed with MCI will develop dementia within five years, with only a small percentage will maintain stable cognitive function [5]. In the absence of timely diagnosis, patients may exhibit impairments in two or more cognitive domains, such as memory, language, executive function, perceptual speed and visuospatial abilities [6,7,8]. These impairments can severely affect the patients’ independence in daily life and place a significant burden on caregivers and families, ultimately increasing societal burden [9]. Therefore, it is crucial to identify individuals at high risk for MCI as early as possible.
Prior research has identified several risk factors affecting cognitive function in older adults. Demographic characteristics such as age, sex, educational level, and marital status have all been shown to significantly impact cognitive impairment [10,11]. A significant body of research has established a link between cognitive decline and various physical health conditions. These include basic activities of daily living (BADL) [12], instrumental activities of daily living (IADL) [13], body mass index (BMI) [14], blood pressure [15], vision [16], hearing [17], and chronic diseases such as diabetes and stroke [18]. Additionally, lifestyle factors such as exercise [19], diet [20], smoking, and alcohol use [21], have been shown to have a considerable impact on cognitive function in older adults. At the biological level, evidence indicates that sex hormones [22] and hemoglobin levels [23] are linked to cognitive dysfunction. Ferri et al. [24] established a strong correlation between depressive states and cognitive decline. Additionally, Gui et al. [25] identified a clear association between the APOEε4 allele and MCI. Numerous factors influence cognitive function in the elderly, and risk factors varying across studies. Developing a prediction model for MCI is therefore essential for the early identification, prevention, and treatment [26].
In prior literature, Huang et al. [27] developed an MCI prediction model using data from 478 community-dwelling middle-aged and older adults (≥45 years old). The predictors included age, sex, educational level, place of residence, and reading, with an area under the receiver operating characteristic curve (AUROC) of 0.870. This model lacks external validation, and its predictive effect may be biased. Ma et al. [28] developed an MCI risk prediction model for older adults (≥60 years old) using public datasets. This risk prediction model used different MCI assessment methods during the development and validation phases, which may impact the stability and accuracy of the model. Additionally, MCI prediction models have been developed for other specific patient populations, including those with hypertension [29], diabetes [30], and stroke [31]. While prediction tools for these populations are available, variations in study populations and study designs have resulted in a diversity of model variables. MCI prediction models have also been developed using data from various data sources, including neuro biomarkers like A-β amyloid [32] and tau protein [33], neuroimaging variables such as brain microstructure [34], and genetics such as mitochondria-related genes [35]. The predictive accuracy of these models has significantly improved; however, implementing these biomarker tests in community settings remains challenging. Consequently, the objective of this study was to develop and validate a risk prediction model, known as CGMCI-Risk, for MCI in community-dwelling older adults. This model aims to help community healthcare professionals identify high-risk MCI groups, thereby facilitating the optimization of prevention and intervention strategies.
2. Materials and Methods
2.1. Dataset
The data were obtained from the Chinese Longitudinal Healthy Longevity Survey (CLHLS). The CLHLS is one of the largest national longitudinal studies examining the health status of older adults in China. It includes eight surveys conducted in 23 provinces, municipalities, and autonomous regions between 1998 and 2018. The sampling area covered approximately 85% of China’s total population [36]. The CLHLS dataset includes basic information, health assessments, personality traits, lifestyle factors, personal backgrounds, and indicators of physical health. All eligible participants who consented signed an informed consent form. For older adults unable to sign the form themselves, consent was provided by a family member on their behalf.
2.2. Design and participants
In this study, the CLHLS cohort data from 2008 to 2011 was selected as the derivation set, and the CLHLS cohort data from 2011 to 2014 was used as the temporal validation set for the model. The study population included community-dwelling older adults aged 60 years and older with healthy cognition. Individuals who were institutionalized or who self-reported or were diagnosed with dementia were excluded. Figure 1 presents flowchart of sample selection in the present study. This study was conducted in accordance with the TRIPOD reporting specifications [37].
2.3. Assessment of MCI
Cognitive functioning was assessed using the Chinese Mini-Mental State Examination (CMMSE), which consists of 24 items assessing general cognitive ability, reactivity, attention and calculation, recall, and language comprehension and coordination. Each correct response earns one point, while incorrect responses receive zero points. Question 6, "Count the number of food groups in one minute," has a maximum score of seven, making the total score range from zero to thirty. Based on previous research [38,39], the CMMSE score below 24 was considered as MCI.
2.4. Definition of candidate variables
In accordance with previous research on cognitive dysfunction in older adults [10,40,41], 41 candidate variables were selected from the CLHLS survey data for analysis in this study. The variables were grouped into four categories. 1) Demographic characteristics, these include age, educational level, sex, ethnic group, place of residence, marital status, and cohabitant status. 2) Health status and lifestyle, these included BMI, medical expenses, baseline CMMSE score, sleep duration, BADL, IADL, physical performance test (PPT), chronic diseases, masticatory function, vision, hearing, frequency of intake of fruits, fresh vegetables, animal protein, plant protein and tea, house work, field work, garden work, raise domestic animals or pets, read newspapers or books, TV watching or radio listening, playing cards or mahjong, social activities, smoke, alcohol use, and exercise. 3) Mental health, it includes resilience score, life satisfaction, health satisfaction, sleep satisfaction, and financial satisfaction. 4) Community and family support, this includes child support and community services. See Supplementary Materials Table S1 for information on candidate variables.
2.5. Sample size
2.6. Missing value
Values marked as "missing", "unclear" and "unanswerable" were considered as missing data. Individuals with more than 5% of their variables missing were excluded from the analysis. Missing values were imputed using the nearest neighbor (KNN) method, which involves estimating the value of a missing data point based on the mean (for numeric variables) or the most common (for categorical variables) value observed in the K participants who are most similar to the participant with the missing value [44]. In this study, the value of K was set to 5.
2.7. Statistical analysis
The study data were statistically analyzed using R (version 4.3.2). The numeric variables were analyzed according to the distribution characteristics of the variables. Variables with approximately normal distributions were described using means and standard deviations. Comparisons between groups were performed using the independent samples t-test. Numeric variables with severe skewed distributions were described using medians and interquartile ranges (IQR). Comparisons between groups were performed using non-parametric tests. Categorical variables were described as frequencies and percentages. Comparisons between groups were performed using the chi-square test. All tests were performed with two-sided p<0.05 as statistically significant differences. The R packages used in this study include: "pmsampsize" (version 1.1.3), "VIM" (version 6.2.2),"tableone" (version 0.13.2), "MASS" (version 7.3-60), "rms" (version 6.7-1), "pROC" (version 1.18.5), "rmda" (version 1.6), "caret" (version 6.0-94), and "nomogramEx" (version 3.0).
2.8. Model development and validation
A backward stepwise regression analysis was employed to screen the variables in accordance with the Akaike Information Criterion (AIC) minimization principle. The screened predictor variables were then included in the first multivariate logistic regression analysis, and subsequently, significant predictor variables were included in the second logistic regression analysis until all predictor variables in the model were shown to be significant. The CGMCI-Risk model was developed using logistic regression. Scores for each variable were extracted using the R package "nomogramEx" (version 3.0), which contributed to the formation of the CGMCI-Risk model.
The AUROC [45], calibration curve [46], and DCA [47] were employed to evaluate the discriminatory power, calibration, and clinical utility of CGMCI-Risk, respectively. The AUROC ranged from 0 to 1, with a value of 1 indicating 100% correct predictions [45]. The Hosmer-Lemeshow (H-L) goodness-of-fit (GOF) test was employed to construct calibration plots, which were utilized to assess the degree of agreement between the predicted risk and actual status of MCI. In a calibration plot, the x-axis represents the predicted probability, the y-axis represents the observed probability, and the diagonal line represents a perfect prediction [48]. DCA calculates the net benefit through a series of risk-probability thresholds and analyzes the value and consequences of the decision under consideration [49]. The robustness of the model was evaluated through the application of bootstrap resampling and temporal validation. The accuracy, sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) of CGMCI-Risk were subsequently reported.
3. Results
3.1. Participants
Of the 6,058 participants in the derivation set (median [IQR] age was 79 [71, 87] years), 933 (16.3%) developed MCI within 3 years, 2963 (48.9%) were female and 3,095 (51.1%) were male. Of the 4,448 participants in the temporal validation set (median [IQR] age was 79 [73, 87] years), 635 (14.1%) developed MCI within 3 years, 2,205 (49.1%) were female and 2,283 (50.9%) were male. More cohort characteristics of the derivation set and temporal validation set are presented in Supplementary Materials Table S2.
3.2. CGMCI-Risk development and validation
The set of variables with a minimum AIC value of 4,548 was screened by backward stepwise regression analysis. The first multivariate logistic regression analysis was performed using the screened variables, the statistically insignificant variables were removed, and the multivariate logistic regression model was reconstructed using the remaining significant variables. The eventually multivariate logistic regression model included age, educational level, sex, exercise, garden work, TV watching or radio listening, IADL, hearing, and masticatory function. The results are shown in Supplementary Materials Table S3. Based on this model, the CGMCI-Risk tool was developed to calculate disease scores, with personalized results obtained by inputting the appropriate values or options. The corresponding scores for each parameter are presented in Supplementary Materials Table S4. The equation that describes the relationship between the predicted risk value and the sum of the parameters scores is as follows:
Risk = 0.852405178 - 4.17e-07 * Total Points³ + 0.000194207 * Total Points² - 0.022360467 * Total Points.
We provide this CGMCI-Risk model with a user-friendly web platform that enables the estimation of normative deviation scores from any sample with minimal technical and computing requirements: http://g152335m31.imdo.co/Communities Geriatric Mild Cognitive Impairment Risk Calculator.
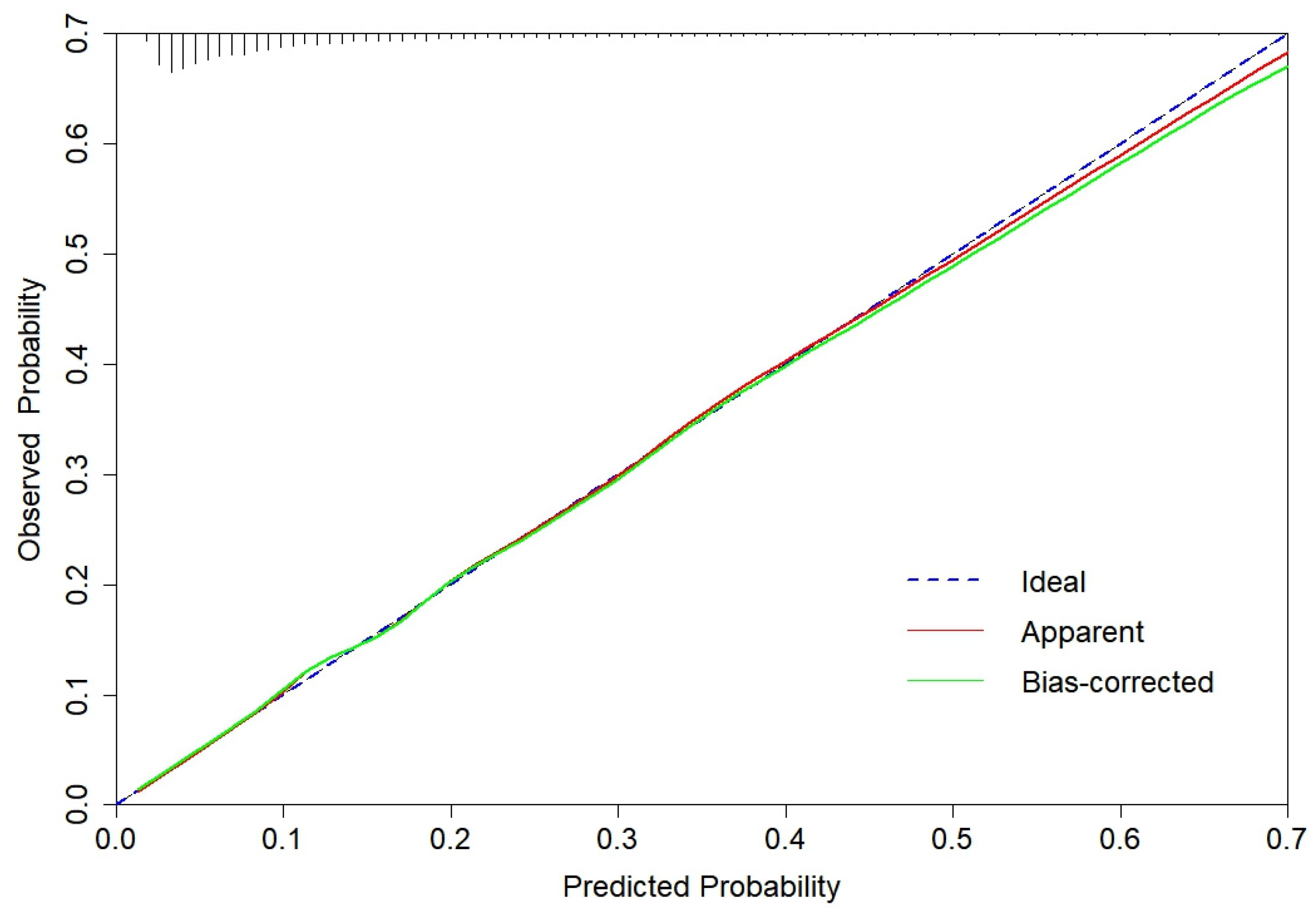
The CGMCI-Risk model demonstrated robust discriminatory power in identifying MCI risk in community-dwelling older adults, with an AUROC of 0.781 (Figure 2). The accuracy, sensitivity, specificity, NPV, and PPV of CGMCI-Risk in the derivation set were 0.717, 0.710, 0.719, 0.927 and 0.330, respectively. The study employed the H-L GOF test to assess the consistency between the model's predicted probability and the actual probability (p = 0.146). Calibration plots were also constructed to facilitate this assessment. The results demonstrated a robust correlation between the actual and predicted probabilities, with a mean absolute error (MAE) of 0.011 and a mean square error (MSE) of 0.00023 (Figure 3). The DCA illustrated that CGMCI-Risk offers a greater net benefit compared to full treatment or no treatment when the risk threshold ranges from 4% to 57% (Figure 4).
Internal validation employed bootstrap resampling 1,000 times with AUROC, sensitivity, and specificity of 0.776, 0.977, and 0.125, respectively. Temporal validation set was conducted using data from the CLHLS cohort from 2011 to 2014. The AUROC, sensitivity, and specificity were 0.782, 0.765, and 0.666, respectively (Figure 2). The calibration curve and DCA are similar to the derivation set indicate that the CGMCI-Risk is an effective tool for identifying older adults at risk for MCI in the community (Figure 4 and Figure 5), thereby providing a foundation for early cognitive intervention by community healthcare workers.
4. Discussion
In this study, CGMCI-Risk was developed based on a dataset comprising 6,058 samples, and its external validity was subsequently temporal validated with an additional 4,488 samples. The AUROC values demonstrated consistent performance, with a mean of approximately 0.8, indicating a high degree of discriminative ability. The calibration curve demonstrated excellent consistency, and DCA validated its utility, establishing a robust tool for MCI risk assessment in community-dwelling older adults. The CGMCI-Risk incorporates age, educational level, sex, exercise, garden work, TV watching or radio listening, IADL, hearing, and masticatory function.
Age and sex are significant non-intervention factors in cognitive impairment. The prevalence of MCI increases with age. As a consequence of the aging process, the volume of the cerebral cortex and hippocampus diminishes [50]. This results in a blockage of information delivery, which in turn impairs cognitive function [50]. Yesavage et al. [51] modeling the prevalence and incidence of AD and MCI. Primary found of the model include that the conversion rate from normal cognitive state to MCI increased from 1% per year at age 60 to 11% at age 85. This suggests that age is a significant risk factor for the development of MCI. A meta-analysis of the association between sex and MCI revealed that women are a risk factor for MCI [52]. The role of estrogen in neurogenesis in the hippocampus is significant, and fluctuations in its levels may be associated with an increased risk of MCI in female [53]. Furthermore, women are more prone to the formation of ApoEε4-associated neurogenic fiber tangles, which may contribute to an elevated risk of cognitive impairment [54]. A review of the literature reveals a correlation between educational attainment and a number of factors related to cognitive functioning, including the thickness of the cerebral cortex, gray matter volume, and neural network connectivity [55]. Individuals with higher levels of education tend to demonstrate superior cognitive functioning [56], whereas illiteracy or lower educational attainment represents a substantial risk factor for MCI [57].
There is a strong correlation between IADL and cognitive function. As IADL declines, older adults may also experience a decline in cognitive abilities [13]. This association may be attributed to the fact that sustained stimulation of cerebral function through IADL preserves the activity and plasticity of the brain's neural networks, thereby assisting in the mitigation of cognitive decline [58]. A reduction in IADL may also result in a decline in socialization among older adults, which may further impact their cognitive function [59]. Hearing impairment represents a significant risk factor for the onset of MCI. A study investigating the impact of hearing on cognitive function demonstrated that individuals with normal hearing exhibited superior performance on cognitive assessments [60]. This may be attributed to the fact that hearing impairment can result in alterations to brain structure and function [17]. Examples of these changes include a decline in brain signals, degeneration of the auditory cortex, loss of neurons and neuron branches, and a reduction in overall brain volume [61]. Such alterations may impact the brain's capacity to process and perceive sound, potentially contributing to cognitive decline. Tooth loss can result in difficulty chewing, which may affect nutrient absorption and cognitive function in the brain [62]. Momose et al. [63] and Onozuka et al. [64] have demonstrated increased hemodynamic responses in the prefrontal cortex and hippocampus during chewing, which plays a crucial role in cognitive function. Research has indicated a correlation between tooth loss and chewing difficulties and cognitive decline [65], while effective mastication has been shown to have a beneficial impact on the prevention of MCI [66].
Regular exercise has been demonstrated to exert a beneficial influence on the brain [67]. A research study demonstrated that sustained exercise can delay the onset of cognitive impairment in older adults [68]. An intervention study by Kim and colleagues also confirmed that exercise may improve cognitive function in older adults aged 65 and above [19]. Regular exercise has been demonstrated to facilitate the formation of neural connections between regions of the brain that are essential for optimal cognitive function [69]. Furthermore, it facilitates the release of brain-derived neurotrophic factor (BDNF) in the brain, which is instrumental in promoting neuronal growth, connectivity, and maintenance [70,71]. It is hypothesized that gardening may confer benefits with respect to cognitive function in older adults. Findings from a four-year longitudinal study indicate that gardening may be a significant factor in the reversal of MCI in older adults [72]. In addition to providing enriching stimulation [73], gardening has been shown to result in significantly higher levels of BDNF, which can lead to improvements in both physical and cognitive functioning [74]. Furthermore, the role of passive activities such as watching television or listening to the radio in cognitive impairment has been demonstrated. Lin et al. [75] and Major et al. [76] have shown that these activities can significantly improve cognitive performance in older adults. However, Jung et al. [77] posit that television viewing may be associated with an increased risk of cognitive impairment in later life. This may be attributed to the fact that prolonged television viewing is frequently linked to sedentary behavior, which can result in inadequate physical activity or reduced time spent gardening. Consequently, watching television or listening to the radio may become a risk factor [76].
Currently, more than 55 million individuals worldwide are affected by dementia, with AD representing approximately 60 to 70 percent of dementia cases [78]. MCI progresses to AD at a rate of 10 to 15 percent per year, whereas the rate of transition to AD in normal older adults is only 1 to 2 percent per year [79]. Although current clinical interventions may not be capable of curing these diseases, timely recognition and diagnosis are essential for improving patient prognosis and reducing the burden on caregivers [80]. CGMCI-Risk enhances accessibility and feasibility of assessment and optimizes healthcare worker engagement. It is particularly suited to community settings, providing community healthcare workers with a foundational resource for conducting early cognitive interventions.
The CGMCI-Risk model was developed to identify high-risk groups for MCI in community-dwelling older adults. Although laboratory parameters, imaging features, biomarkers, and genetic indicators have significant potential for MCI prediction, they were excluded in this study due to logistical and operational feasibility in a real-world community setting. In addition, the three-year interval for MCI assessment may introduce bias and fail to capture subtle disease changes. The elevated mortality rate among older adults may also lead to increased data loss and impact assessment precision. The CGMCI-Risk model was developed based on Chinese community-dwelling older adults and while promising for use in community settings, requires further validation for its applicability in different care facilities and cultural backgrounds.
5. Conclusions
The CGMCI-Risk model incorporates factors such as age, educational level, sex, exercise, garden work, TV watching or radio listening, IADL, hearing, and masticatory function. This tool can be used in community settings to help healthcare providers identify older adults in the community at elevated risk for MCI within three-year.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, J.C., Y.S. and Q.X.; methodology, J.C.; supervision, Y.S. and Q.X.; project administration, Y.S., Q.X. J.C. and K.Y.; investigation, Q.F., K.Y. and L.Z.; data curation, J.C.; resources, K.Y., L.Z. and J.C.; formal analysis, J.P., Q.F. and J.C.; software, Q.F., J.P. and J.C.; validation, Q.F. and J.C.; visualization, J.C. and L.Z.; writing—original draft preparation, J.C.; writing—review and editing, Y.S., Q.X. and J.C.; funding acquisition, Y.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by Technology Program of Hangzhou Municipality (no.20212013B02, Z20200051).
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki. The data were derived from the CLHLS, which has approved by the Biomedical Ethics Committee of Peking University (IRB00001052-13074, approved on 14 January 2015). The data used in this study was approved by the Peking University Open Data Research Platform.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data were obtained from the CLHLS. Links to public datasets analyzed during the study: https://doi.org/10.18170/DVN/WBO7LK.
Acknowledgments
We would like to express our gratitude to the Center for Healthy Aging and Development Studies and the Peking University Open Data Research Platform for their contributions to CLHLS.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Rajji, T.K. Transcranial Magnetic and Electrical Stimulation in Alzheimer's Disease and Mild Cognitive Impairment: A Review of Randomized Controlled Trials. Clinical pharmacology and therapeutics 2019, 106, 776-780. [CrossRef]
- Cong, L.; Ren, Y.; Wang, Y.; Hou, T.; Dong, Y.; Han, X.; Yin, L.; Zhang, Q.; Feng, J.; Wang, L.; Tang, S.; Grande, G.; Laukka, E.J.; Du, Y.; Qiu, C. Mild cognitive impairment among rural-dwelling older adults in China: A community-based study. Alzheimers Dement 2023, 19, 56-66. [CrossRef]
- Bai, W.; Chen, P.; Cai, H.; Zhang, Q.; Su, Z.; Cheung, T.; Jackson, T.; Sha, S.; Xiang, Y.T. Worldwide prevalence of mild cognitive impairment among community dwellers aged 50 years and older: a meta-analysis and systematic review of epidemiology studies. Age and ageing 2022, 51, afac173. [CrossRef]
- Jia, L.; Du, Y.; Chu, L.; Zhang, Z.; Li, F.; Lyu, D.; Li, Y.; Li, Y.; Zhu, M.; Jiao, H.; Song, Y.; Shi, Y.; Zhang, H.; Gong, M.; Wei, C.; Tang, Y.; Fang, B.; Guo, D.; Wang, F.; Zhou, A.; Chu, C.; Zuo, X.; Yu, Y.; Yuan, Q.; Wang, W.; Li, F.; Shi, S.; Yang, H.; Zhou, C.; Liao, Z.; Lv, Y.; Li, Y.; Kan, M.; Zhao, H.; Wang, S.; Yang, S.; Li, H.; Liu, Z.; Wang, Q.; Qin, W.; Jia, J.; COAST Group. Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health 2020, 5, e661-e671. [CrossRef]
- Gauthier, S.; Reisberg, B.; Zaudig, M.; Petersen, R.C.; Ritchie, K.; Broich, K.; Belleville, S.; Brodaty, H.; Bennett, D.; Chertkow, H.; Cummings, J.L.; de Leon, M.; Feldman, H.; Ganguli, M.; Hampel, H.; Scheltens, P.; Tierney, M.C.; Whitehouse, P.; Winblad, B.; International Psychogeriatric Association Expert Conference on mild cognitive impairment. Mild cognitive impairment. Lancet 2006, 367, 1262-1270. [CrossRef]
- Bennett, D.A.; Wilson, R.S.; Schneider, J.A.; Evans, D.A.; Beckett, L.A.; Aggarwal, N.T.; Barnes, L.L.; Fox, J.H.; Bach, J. Natural history of mild cognitive impairment in older persons. Neurology 2002, 59, 198-205. [CrossRef]
- Mapstone, M.; Steffenella, T.M.; Duffy, C.J. A visuospatial variant of mild cognitive impairment: getting lost between aging and AD. Neurology 2003, 60, 802-808. [CrossRef]
- Yuan, M.; Rong, M.; Long, X.; Lian, S.; Fang, Y. Trajectories of cognitive decline in different domains prior to AD onset in persons with mild cognitive impairment. Archives of Gerontology and Geriatrics 2024, 122, 105375. [CrossRef]
- Knopman, D.S.; Petersen, R.C. Mild cognitive impairment and mild dementia: a clinical perspective. Mayo Clinic proceedings 2014, 89, 1452-1459. [CrossRef]
- Zhang, Q.; Wu, Y.; Han, T.; Liu, E. Changes in Cognitive Function and Risk Factors for Cognitive Impairment of the Elderly in China: 2005-2014. International journal of environmental research and public health 2019, 16, 2847. [CrossRef]
- Kilander, L.; Nyman, H.; Boberg, M.; Lithell, H. Cognitive function, vascular risk factors and education. A cross-sectional study based on a cohort of 70-year-old men. Journal of internal medicine 1997, 242, 313-321. [CrossRef]
- Beker, N.; Ganz, A.; Hulsman, M.; Klausch, T.; Schmand, B.A.; Scheltens, P.; Sikkes, S.A.M.; Holstege, H. Association of Cognitive Function Trajectories in Centenarians with Postmortem Neuropathology, Physical Health, and Other Risk Factors for Cognitive Decline. JAMA network open 2021, 4, e2031654. [CrossRef]
- Spiers, N.A.; Matthews, R.J.; Jagger, C.; Matthews, F.E.; Boult, C.; Robinson, T.G.; Brayne, C. Diseases and impairments as risk factors for onset of disability in the older population in England and Wales: findings from the Medical Research Council Cognitive Function and Ageing Study. The journals of gerontology. Series A, Biological sciences and medical sciences 2005, 60, 248-254. [CrossRef]
- Kim, Y.; Yeom, H. Threshold effects of body mass index on cognitive function and heterogeneity by sex and cardiovascular risk factors. Frontiers in public health 2022, 10, 897691. [CrossRef]
- Zimmermann, M.; Wurster, I.; Lerche, S.; Roeben, B.; Machetanz, G.; Sünkel, U.; von Thaler, A.K.; Eschweiler, G.; Fallgatter, A.J.; Maetzler, W.; Berg, D.; Brockmann, K. Orthostatic hypotension as a risk factor for longitudinal deterioration of cognitive function in the elderly. European journal of neurology 2020, 27, 160-167. [CrossRef]
- Cao, K.; Hao, J.; Wang, N. Visual impairment as a risk factor of cognitive function impairment A six-year cohort study. European journal of ophthalmology 2023, 33, 2146-2153. [CrossRef]
- AAn, Y.Y.; Lee, E.S.; Lee, S.A.; Choi, J.H.; Park, J.M.; Lee, T.K.; Kim, H.; Lee, J.D. Association of Hearing Loss with Anatomical and Functional Connectivity in Patients with Mild Cognitive Impairment. JAMA otolaryngology-head & neck surgery 2023, 149, 571-578. [CrossRef]
- Yang, L.; Jin, X.; Yan, J.; Jin, Y.; Xu, S.; Xu, Y.; Liu, C.; Yu, W.; Zheng, P. Comparison of prevalence and associated risk factors of cognitive function status among elderly between nursing homes and common communities of China: A STROBE-compliant observational study. Medicine 2019, 98, e18248. [CrossRef]
- Kim, J.; Kang, S.; Hong, H.; Joo, M.; Kang, H. A Non-Randomized Combined Program of Walking and Low-Load Resistance Exercise Improves Cognitive Function and Cardiometabolic Risk Factors in Community-Dwelling Elderly Women. Healthcare (Basel) 2022, 10, 2106. [CrossRef]
- Wernicke, C.; Apostolopoulou, K.; Hornemann, S.; Efthymiou, A.; Machann, J.; Schmidt, S.; Primessnig, U.; Bergmann, M.M.; Grune, T.; Gerbracht, C.; Herber, K.; Pohrt, A.; Pfeiffer, A.F.H.; Spranger, J.; Mai, K. Long-term effects of a food pattern on cardiovascular risk factors and age-related changes of muscular and cognitive function. Medicine 2020, 99, e22381. [CrossRef]
- Li, C.C.; Chen, Y.F.; Liang, J.; Matthews, A.K.; Barnes, L.L. Trajectories of Multiple Behavioral Risk Factors and Their Associations with Cognitive Function Trajectories Among Older African Americans and White Americans. Journal of aging and health 2021, 33, 674-684. [CrossRef]
- Tang, S.; Huang, L.; Lin, F.; Chen, X.; Wang, Y.; Xu, J.; Wang, Y.; Gao, J.; Xiao, Q. Sex steroid and cognitive function among community-dwelling older men with or without vascular risk factors: a cross-sectional study. BMC geriatrics 2024, 24, 147. [CrossRef]
- Noma, T.; Kayo, G.; Kabayama, M.; Gondo, Y.; Yasumoto, S.; Masui, Y.; Sugimoto, K.; Akasaka, H.; Takami, Y.; Takeya, Y.; Yamamoto, K.; Ikebe, K.; Arai, Y.; Ishizaki, T.; Rakugi, H.; Kamide, K. Lower cognitive function as a risk factor for anemia among older Japanese women from the longitudinal observation in the SONIC study. Geriatrics & gerontology international 2023, 23, 334-340. [CrossRef]
- Ferri, F.; Deschênes, S.S.; Power, N.; Schmitz, N. Association between depressive symptoms, metabolic risk factors, and cognitive function: cross-sectional results from a community study in Quebec, Canada. Aging & mental health 2021, 25, 2003-2010. [CrossRef]
- Gui, W.; Qiu, C.; Shao, Q.; Li, J. Associations of Vascular Risk Factors, APOE and TOMM40 Polymorphisms with Cognitive Function in Dementia-Free Chinese Older Adults: A Community-Based Study. Frontiers in psychiatry 2021, 12, 617773. [CrossRef]
- Moons, K.G.; Royston, P.; Vergouwe, Y.; Grobbee, D.E.; Altman, D.G. Prognosis and prognostic research: what, why, and how? BMJ 2009, 338, b375. [CrossRef]
- Huang, M.; Gao, X.; Zhao, R.; Dong, C.; Gu, Z.; Gao, J. Development and validation of a nomogram for predicting mild cognitive impairment in middle-aged and elderly people. Asian journal of psychiatry 2022, 75, 103224. [CrossRef]
- Ma, X.; Huang, W.; Lu, L.; Li, H.; Ding, J.; Sheng, S.; Liu, M.; Yuan, J. Developing and validating a nomogram for cognitive impairment in the older people based on the NHANES. Frontiers in neuroscience 2023, 17, 1195570. [CrossRef]
- Zhong, X.; Yu, J.; Jiang, F.; Chen, H.; Wang, Z.; Teng, J.; Jiao, H. A risk prediction model based on machine learning for early cognitive impairment in hypertension: Development and validation study. Frontiers in public health 2023, 11, 1143019. [CrossRef]
- Yu, Q.; Jiang, X.; Yan, J.; Yu, H. Development and validation of a risk prediction model for mild cognitive impairment in elderly patients with type 2 diabetes mellitus. Geriatric Nursing 2024, 58, 119-126. [CrossRef]
- Dong, Y.; Ding, M.; Cui, M.; Fang, M.; Gong, L.; Xu, Z.; Zhang, Y.; Wang, X.; Xu, X.; Liu, X.; Li, G.; Zhao, Y.; Dong, Q. Development and validation of a clinical model (DREAM-LDL) for post-stroke cognitive impairment at 6 months. Aging 2021, 13, 21628-21641. [CrossRef]
- Momota, Y.; Bun, S.; Hirano, J.; Kamiya, K.; Ueda, R.; Iwabuchi, Y.; Takahata, K.; Yamamoto, Y.; Tezuka, T.; Kubota, M.; Seki, M.; Shikimoto, R.; Mimura, Y.; Kishimoto, T.; Tabuchi, H.; Jinzaki, M.; Ito, D.; Mimura, M. Amyloid-β prediction machine learning model using source-based morphometry across neurocognitive disorders. Scientific reports 2024, 14, 7633. [CrossRef]
- Pase, M.P.; Beiser, A.S.; Himali, J.J.; Satizabal, C.L.; Aparicio, H.J.; DeCarli, C.; Chêne, G.; Dufouil, C.; Seshadri, S. Assessment of Plasma Total Tau Level as a Predictive Biomarker for Dementia and Related Endophenotypes. JAMA neurology 2019, 76, 598-606. [CrossRef]
- Betrouni, N.; Jiang, J.; Duering, M.; Georgakis, M.K.; Oestreich, L.; Sachdev, P.S.; O'Sullivan, M.; Wright, P.; Lo, J.W.; Bordet, R.; Stroke and Cognition (STROKOG) Collaboration. Texture Features of Magnetic Resonance Images Predict Poststroke Cognitive Impairment: Validation in a Multicenter Study. Stroke 2022, 53, 3446-3454. [CrossRef]
- Yan, R.; Wang, W.; Yang, W.; Huang, M.; Xu, W. Mitochondria-Related Candidate Genes and Diagnostic Model to Predict Late-Onset Alzheimer's Disease and Mild Cognitive Impairment. Journal of Alzheimer's disease 2024, 99, S299-S315. [CrossRef]
- Center for Healthy Aging and Development Studies. Chinese Longitudinal Healthy Longevity and Happy Family Study (CLHLS-HF). Available online: https://opendata.pku.edu.cn/dataverse/CHADS (accessed on 15 August 2024).
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ 2015, 350, g7594. [CrossRef]
- Feng, Q.; Zhu, H.; Zhen, Z.; Gu, D. Self-Rated Health, Interviewer-Rated Health, and Their Predictive Powers on Mortality in Old Age. The journals of gerontology. Series B, Psychological sciences and social sciences 2016, 71, 538-550. [CrossRef]
- Goldschmidt, T.J.; Mallin, R.; Still, C.N. Recognition of cognitive impairment in primary care outpatients. Southern medical journal 1983, 76, 1264-1265, 1270. [CrossRef]
- Belessiotis-Richards, C.; Livingston, G.; Marston, L.; Mukadam, N. A cross-sectional study of potentially modifiable risk factors for dementia and cognitive function in India: A secondary analysis of 10/66, LASI, and SAGE data. International journal of geriatric psychiatry 2021, 37, 5661. [CrossRef]
- Dale, W.; Kotwal, A.A.; Shega, J.W.; Schumm, L.P.; Kern, D.W.; Pinto, J.M.; Pudelek, K.M.; Waite, L.J.; McClintock, M.K. Cognitive Function and its Risk Factors Among Older US Adults Living at Home. Alzheimer disease and associated disorders 2018, 32, 207-213. [CrossRef]
- Lee, C.C.; Chen, C.W.; Yen, H.K.; Lin, Y.P.; Lai, C.Y.; Wang, J.L.; Groot, O.Q.; Janssen, S.J.; Schwab, J.H.; Hsu, F.M.; Lin, W.H. Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients with Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone. Clinical orthopaedics and related research 2024, in press. [CrossRef]
- Riley, R.D.; Ensor, J.; Snell, K.I.E.; Harrell, F.E.Jr.; Martin, G.P.; Reitsma, J.B.; Moons, K.G.M.; Collins, G.; van Smeden, M. Calculating the sample size required for developing a clinical prediction model. BMJ 2020, 368, m441. [CrossRef]
- Andridge, R.R.; Little, R.J.A. A Review of Hot Deck Imputation for Survey Non-response. International statistical review 2010, 78, 40-64. [CrossRef]
- Mandrekar, J.N. Receiver operating characteristic curve in diagnostic test assessment. Journal of thoracic oncology 2010, 5, 1315-1316. [CrossRef]
- Van Calster, B.; McLernon, D.J.; van Smeden, M.; Wynants, L.; Steyerberg, E.W.; Topic Group ‘Evaluating diagnostic tests and prediction models’ of the STRATOS initiative. Calibration: the Achilles heel of predictive analytics. BMC medicine 2019, 17, 230. [CrossRef]
- Van Calster, B.; Wynants, L.; Verbeek, J.F.M.; Verbakel, J.Y.; Christodoulou, E.; Vickers, A.J.; Roobol, M.J.; Steyerberg, E.W. Reporting and Interpreting Decision Curve Analysis: A Guide for Investigators. European urology 2018, 74, 796-804. [CrossRef]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: a framework for traditional and novel measures. Epidemiology 2010, 21, 128-138. [CrossRef]
- Fitzgerald, M.; Saville, B.R.; Lewis, R.J. Decision curve analysis. JAMA 2015, 313, 409-410. [CrossRef]
- Li, X.; Xia, J.; Ma, C.; Chen, K.; Xu, K.; Zhang, J.; Chen, Y.; Li, H.; Wei, D.; Zhang, Z. Accelerating Structural Degeneration in Temporal Regions and Their Effects on Cognition in Aging of MCI Patients. Cerebral cortex 2020, 30, 326-338. [CrossRef]
- Yesavage, J.A.; O'Hara, R.; Kraemer, H.; Noda, A.; Taylor, J.L.; Ferris, S.; Gély-Nargeot, M.C.; Rosen, A.; Friedman, L.; Sheikh, J.; Derouesné, C. Modeling the prevalence and incidence of Alzheimer's disease and mild cognitive impairment. Journal of psychiatric research 2002, 36, 281-286. [CrossRef]
- Au, B.; Dale-McGrath, S.; Tierney, M.C. Sex differences in the prevalence and incidence of mild cognitive impairment: A meta-analysis. Ageing research reviews 2017, 35, 176-199. [CrossRef]
- Feng, L.; Bian, L.; Ning, C.; Zhang, P.; Zhao, Y.; Gao, Z.; Ping, P.; Fu, S. Positive associations between sex hormones, bone metabolism and cognitive impairment in Chinese oldest-old females. BMC psychiatry 2023, 23, 562. [CrossRef]
- Liu, M.; Paranjpe, M.D.; Zhou, X.; Duy, P.Q.; Goyal, M.S.; Benzinger, T.L.S.; Lu, J.; Wang, R.; Zhou, Y. Sex modulates the ApoE ε4 effect on brain tau deposition measured by (18)F-AV-1451 PET in individuals with mild cognitive impairment. Theranostics 2019, 9, 4959-4970. [CrossRef]
- Raine, P.J.; Rao, H. Volume, density, and thickness brain abnormalities in mild cognitive impairment: an ALE meta-analysis controlling for age and education. Brain imaging and behavior 2022, 16, 2335-2352. [CrossRef]
- Rolstad, S.; Nordlund, A.; Eckerström, C.; Gustavsson, M.H.; Blennow, K.; Olesen, P.J.; Zetterberg, H.; Wallin, A. High education may offer protection against tauopathy in patients with mild cognitive impairment. Journal of Alzheimer's disease 2010, 21, 221-228. [CrossRef]
- White, L.; Katzman, R.; Losonczy, K.; Salive, M.; Wallace, R.; Berkman, L.; Taylor, J.; Fillenbaum, G.; Havlik, R. Association of education with incidence of cognitive impairment in three established populations for epidemiologic studies of the elderly. Journal of clinical epidemiology 1994, 47, 363-374. [CrossRef]
- Kiosses, D. N.; Alexopoulos, G.S. IADL functions, cognitive deficits, and severity of depression: a preliminary study. American journal of geriatric psychiatry 2005, 13, 244-249.
- Lee, J.J.; Park, M.K.; Kim, N.; Kim, L.; Kim, G.S. Longitudinal Relationship Between Baseline Social Frailty and Cognitive Impairment in Older Adults: 14-Year Follow-Up Results From the Korean Longitudinal Study of Ageing. Journal of the American Medical Directors Association 2024, 25, 105124. [CrossRef]
- Al-Yawer, F.; Pichora-Fuller, M.K.; Wittich, W.; Mick, P.; Giroud, N.; Rehan, S.; Phillips, N.A. Sex-Specific Interactions Between Hearing and Memory in Older Adults with Mild Cognitive Impairment: Findings From the COMPASS-ND Study. Ear and hearing 2023, 44, 751-767. [CrossRef]
- Loughrey, D.G.; Kelly, M.E.; Kelley, G.A.; Brennan, S.; Lawlor, B.A. Association of Age-Related Hearing Loss with Cognitive Function, Cognitive Impairment, and Dementia: A Systematic Review and Meta-analysis. JAMA otolaryngology-head & neck surgery 2018, 144, 115-126. [CrossRef]
- Marito, P.; Hasegawa, Y.; Tamaki, K.; Sta Maria, M.T.; Yoshimoto, T.; Kusunoki, H.; Tsuji, S.; Wada, Y.; Ono, T.; Sawada, T.; Kishimoto, H.; Shinmura, K. The Association of Dietary Intake, Oral Health, and Blood Pressure in Older Adults: A Cross-Sectional Observational Study. Nutrients 2022, 14, 1279. [CrossRef]
- Momose, T.; Nishikawa, J.; Watanabe, T.; Sasaki, Y.; Senda, M.; Kubota, K.; Sato, Y.; Funakoshi, M.; Minakuchi, S. Effect of mastication on regional cerebral blood flow in humans examined by positron-emission tomography with ¹⁵O-labelled water and magnetic resonance imaging. Archives of oral biology 1997, 42, 57-61. [CrossRef]
- Onozuka, M.; Fujita, M.; Watanabe, K.; Hirano, Y.; Niwa, M.; Nishiyama, K.; Saito, S. Mapping brain region activity during chewing: a functional magnetic resonance imaging study. Journal of dental research 2002, 81, 743-746. [CrossRef]
- Kossioni, A.E. The Association of Poor Oral Health Parameters with Malnutrition in Older Adults: A Review Considering the Potential Implications for Cognitive Impairment. Nutrients 2018, 10, 1079. [CrossRef]
- Lexomboon, D.; Trulsson, M.; Wårdh, I.; Parker, M.G. Chewing ability and tooth loss: association with cognitive impairment in an elderly population study. Journal of the American Geriatrics Society 2012, 60, 1951-1956. [CrossRef]
- Wang, F.; Gao, C.; Wang, Y.; Li, Z.; Zheng, F.; Luo, Y. Relationship Between Physical Exercise and Cognitive Function Among Older Adults in China: Cross-Sectional Population-Based Study. JMIR public health and surveillance 2024, 10, e49790. [CrossRef]
- Song, H.; Park, J. Effects of Changes in Physical Activity with Cognitive Decline in Korean Home-Dwelling Older Adults. Journal of multidisciplinary healthcare 2022, 15, 333-341. [CrossRef]
- Blume, G. R.; Royes, L.F.F. Peripheral to brain and hippocampus crosstalk induced by exercise mediates cognitive and structural hippocampal adaptations. Life sciences 2024, 352, 122799. [CrossRef]
- Walsh, J.J.; Tschakovsky, M.E. Exercise and circulating BDNF: Mechanisms of release and implications for the design of exercise interventions. Applied physiology, nutrition, and metabolism 2018, 43, 1095-1104. [CrossRef]
- Vedovelli, K.; Giacobbo, B.L.; Corrêa, M.S.; Wieck, A.; Argimon, I.I.L.; Bromberg, E. Multimodal physical activity increases brain-derived neurotrophic factor levels and improves cognition in institutionalized older women. GeroScience 2017, 39, 407-417. [CrossRef]
- Shimada, H.; Doi, T.; Lee, S.; Makizako, H. Reversible predictors of reversion from mild cognitive impairment to normal cognition: a 4-year longitudinal study. Alzheimer's research & therapy 2019, 11, 24. [CrossRef]
- Jarrott, S.E.; Gigliotti, C.M. Comparing Responses to Horticultural-Based and Traditional Activities in Dementia Care Programs. American Journal of Alzheimer's Disease and Other Dementias 2010, 25, 657-665. [CrossRef]
- Park, S.A.; Lee, A.Y.; Park, H.G.; Lee, W.L. Benefits of Gardening Activities for Cognitive Function According to Measurement of Brain Nerve Growth Factor Levels. International journal of environmental research and public health 2019, 16, 760. [CrossRef]
- Lin, W.; Yin, W.; Yuan, D. Association of home and community-based services and cognitive function of Chinese older adults: social participation as a mediator. BMC geriatrics 2023, 23, 691. [CrossRef]
- Major, L.; Simonsick, E.M.; Napolitano, M.A.; DiPietro, L. Domains of Sedentary Behavior and Cognitive Function: The Health, Aging, and Body Composition Study, 1999/2000 to 2006/2007. The journals of gerontology. Series A, Biological sciences and medical sciences 2023, 78, 2035-2041. [CrossRef]
- Jung, M.S.; Chung, E. Television Viewing and Cognitive Dysfunction of Korean Older Adults. Healthcare (Basel) 2020, 8, 547. [CrossRef]
- World Health Organization. Dementia Fact sheets on 15 March 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 15 August 2024).
- Gelosa, G.; Brooks, D.J. The prognostic value of amyloid imaging. European journal of nuclear medicine and molecular imaging 2012, 39, 1207-1219. [CrossRef]
- Patnode, C.D.; Perdue, L.A.; Rossom, R.C.; Rushkin, M.C.; Redmond, N.; Thomas, R.G.; Lin, J.S. Screening for Cognitive Impairment in Older Adults: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2020, 323, 764-785. [CrossRef]
Figure 1.
The flowchart of participants selection process. Abbreviations: CMMSE, Chinese Mini-Mental State Examination.
Figure 1.
The flowchart of participants selection process. Abbreviations: CMMSE, Chinese Mini-Mental State Examination.
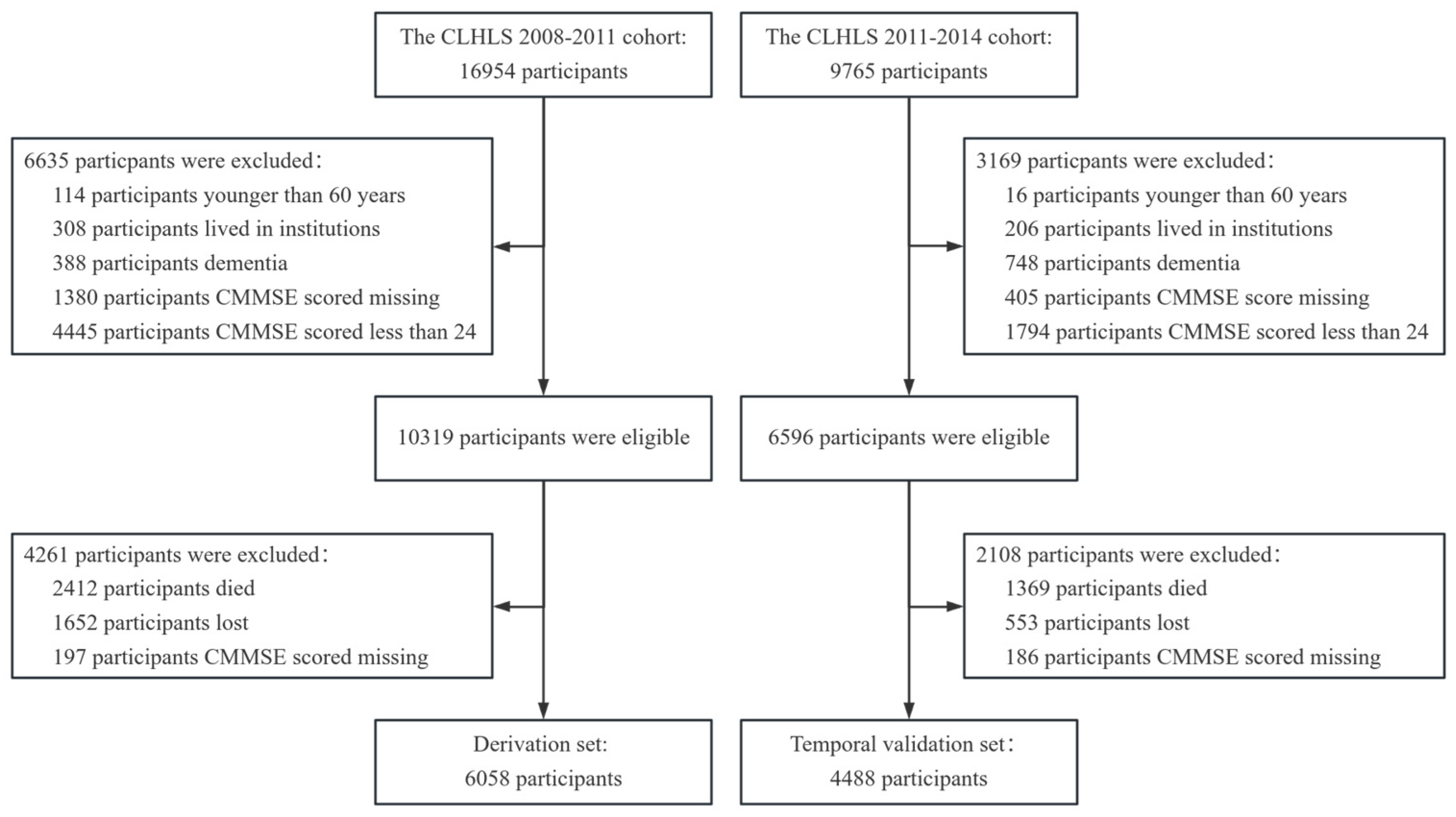
Figure 2.
The AUROC for derivation set and temporal validation set of CGMCI-Risk.
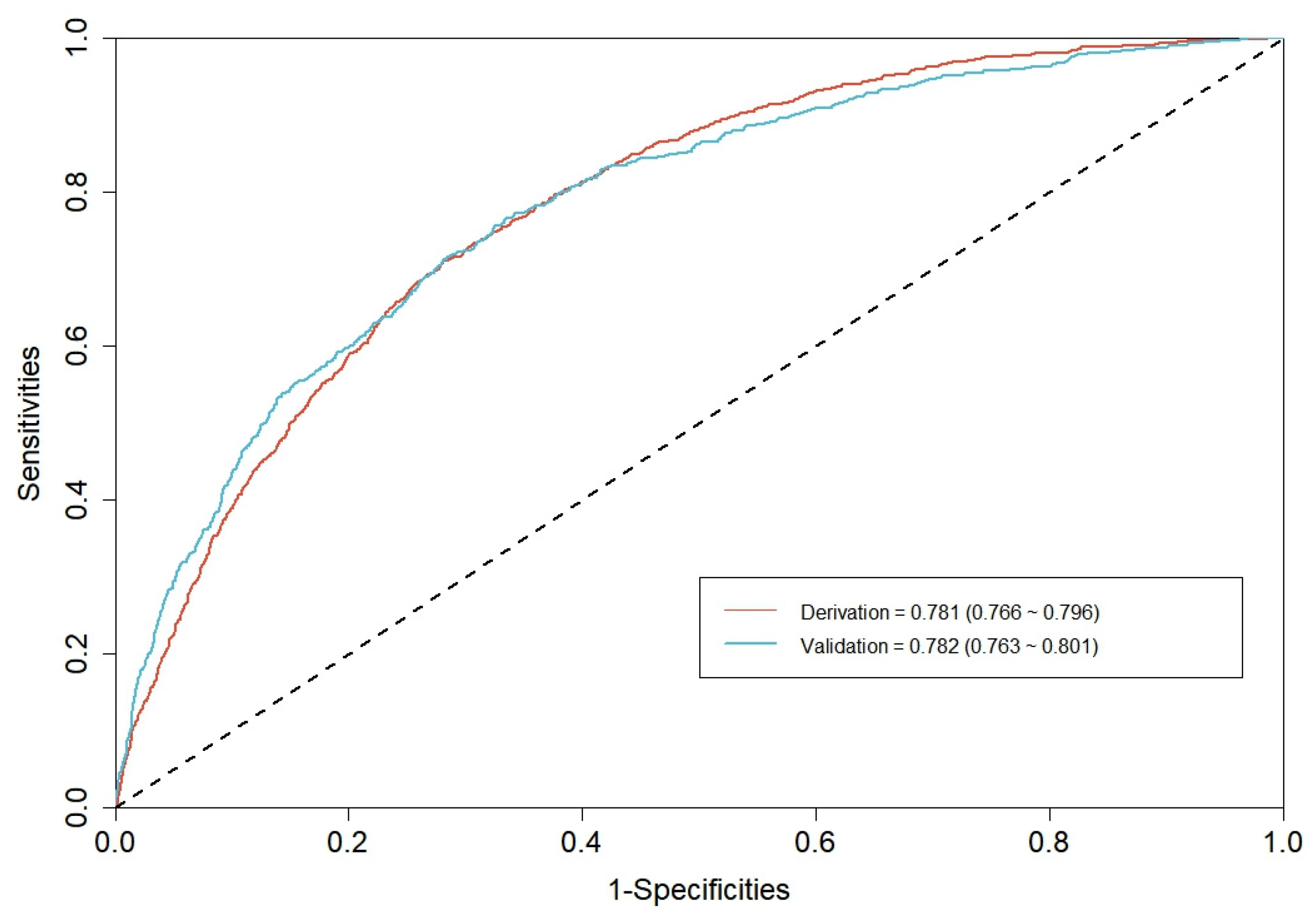
Figure 3.
The calibration curve for derivation set of CGMCI-Risk.
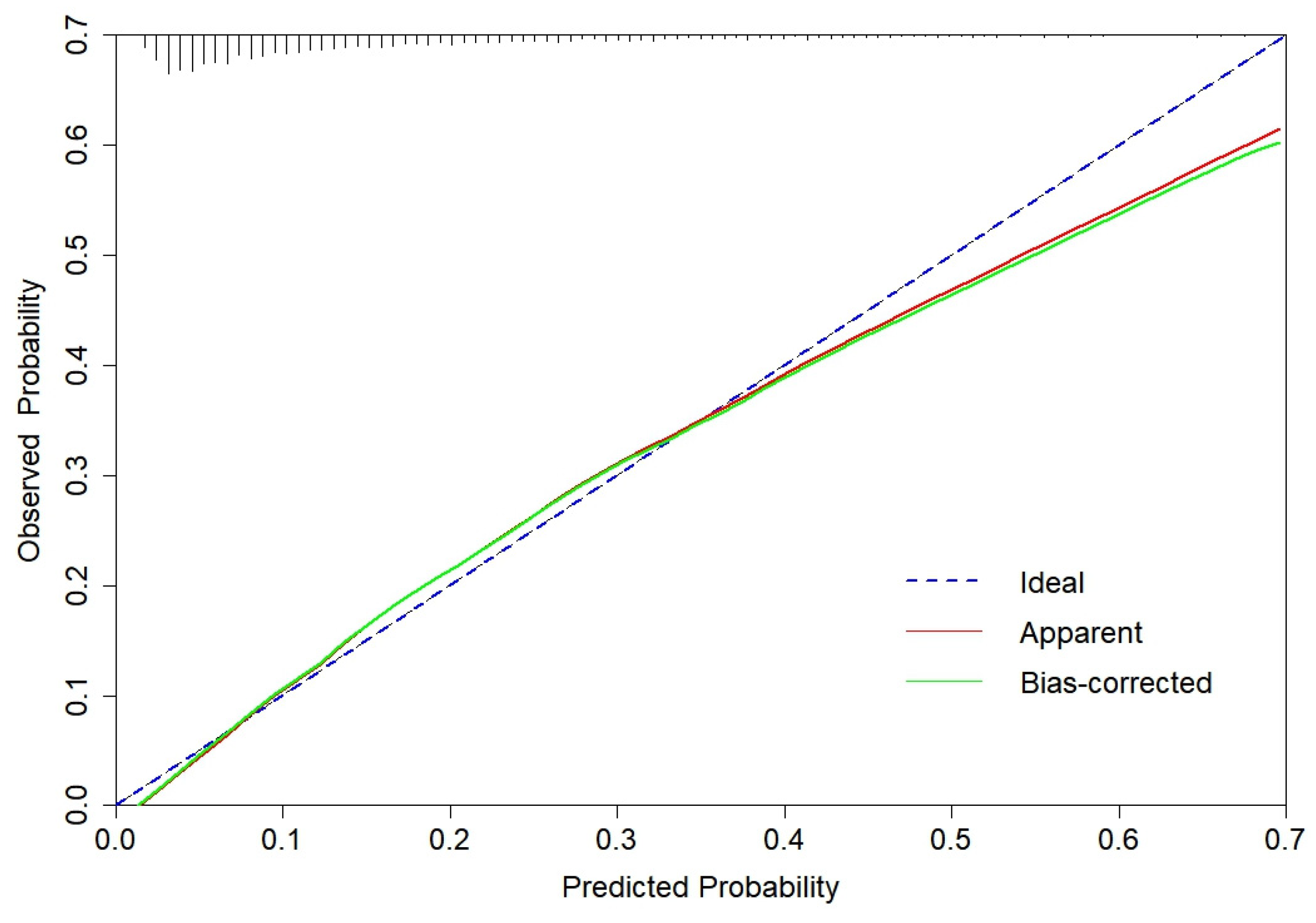
Figure 4.
The DCA for derivation set and temporal validation set of CGMCI-Risk.
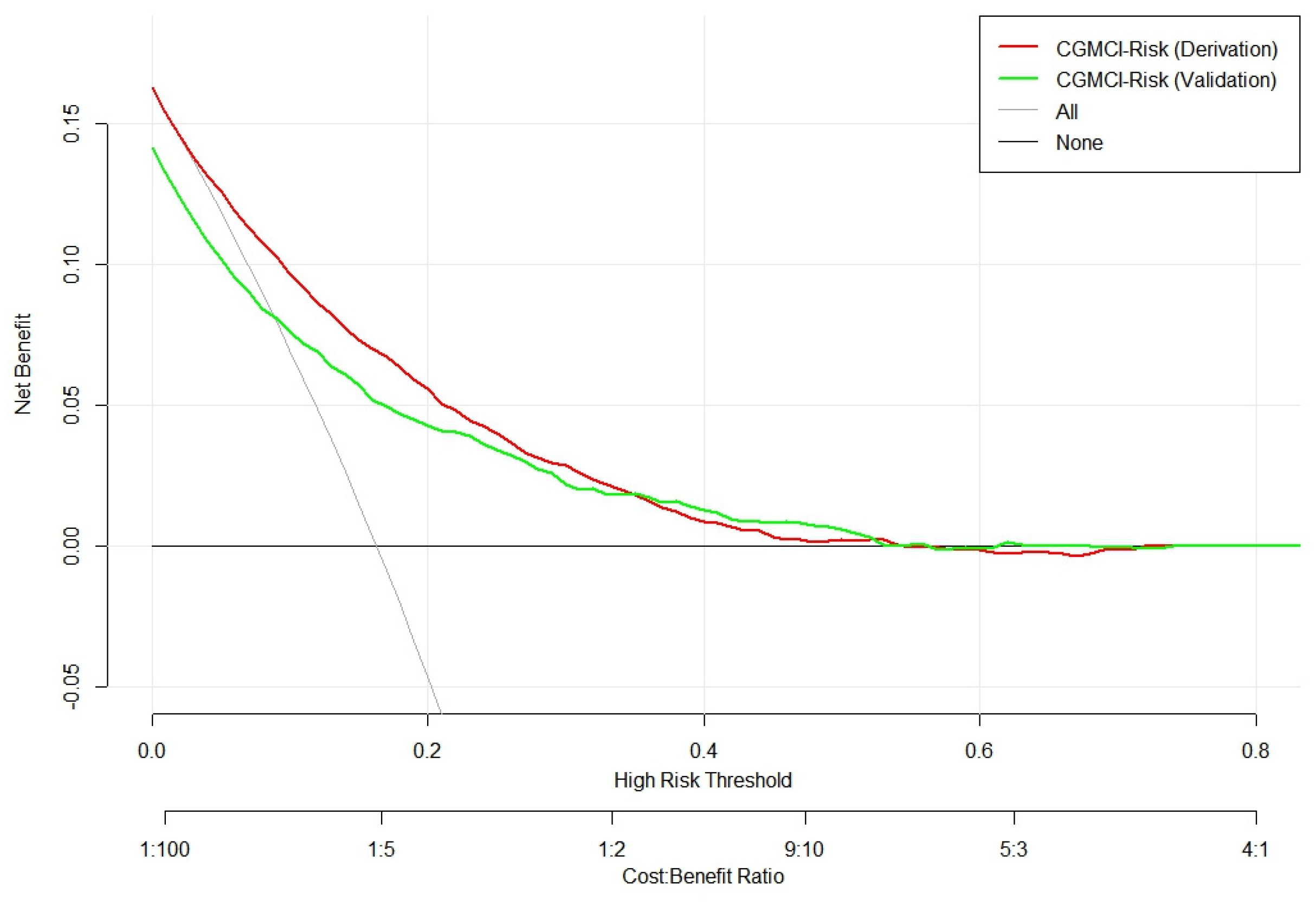
Figure 5.
The calibration curve for temporal validation set of CGMCI-Risk.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



