
Submitted:
04 September 2024
Posted:
09 September 2024
You are already at the latest version
Abstract
Physical activity (PA) benefits are well-established, yet many US adults fail to meet PA guidelines. This is especially true for minorities facing social inequities. This study explored barriers and facilitators to PA among urban Midwestern minorities using a mixed-methods approach framed on the socio-ecological model. A cross-sectional survey was conducted among community-dwelling minorities. Participants were grouped as completing low (LLPA) or high (HLPA) weekly leisure-time PA for comparison. Quantitative analysis included MANOVA, follow-up ANOVAs, and calculation of effect sizes. Qualitative data were assessed using inductive thematic analysis. Twenty-nine adults (44.83% Black, 41.37% Latino) participated in the study. The HLPA group (n = 18) reported higher leisure-time PA (p = 0.001, d = 2.21) and total PA (p = 0.02, d = 1.00) compared to the LLPA group (n = 11). LLPA participants faced more personal barriers to PA (p = 0.02, d = -0.92). Common barriers identified in the interviews included a lack of time and financial costs. Facilitators included social support and available PA facilities. Both groups achieved USPA guidelines through different PA domains. Increasing social support and lowering PA-related costs could enhance participation. Addressing barriers and leveraging existing facilitators are crucial to increasing PA among minorities.
Keywords:
physical activity
; barriers and facilitators
; racial minorities
; health disparities
; mixed methods
1. Introduction
1.1. Physical Activity and Implications for General Health
Physical activity (PA) is defined as any bodily movement that results in energy expenditure beyond a resting metabolic rate [1]. PA can be categorized into four distinct categories: occupational (i.e., working a physical labor job), transportation (i.e., bicycling to work), household (i.e., gardening), and leisure-time (i.e., dog walking, exercising) [1,2]. Data on the health benefits of PA, specifically related to leisure-time PA, have been synthesized into what is now the United States PA (USPA) Guidelines for Americans [3] and the World Health Organization (WHO) Guidelines for PA and Sedentary Behavior [2]. Both guidelines recommend that adults aged >18 years should participate in at least 150 min/week of aerobic moderate-to-vigorous PA (MVPA) and engage in muscle strengthening activities that target all major muscle groups at least 2x/week These guidelines have been deemed attainable by most members of our society, including older adults, those with chronic health diseases, and individuals with physical or cognitive disabilities [2,3].
Data over the last two decades have suggested that meeting the USPA guidelines can promote lifelong health [4]. Moreover, regular PA is associated with many health benefits, including a reduced risk of developing chronic diseases, premature mortality, and improved mental health [2,5]. Evidence also suggests a dose-dependent relationship between PA and health, indicating that individuals who engage in higher amounts of PA, regardless of intensity, are more likely to have a lower risk of chronic disease [4] and improved overall health status [6].
Despite the well-known health benefits of PA, participation rates across the United States continue to remain low [7,8]. Currently only 1-in-4 adults in the United States meet the PA guidelines for aerobic and muscle-strengthening activities [9]. These low PA participation rates are particularly concerning when considering the implications of physical inactivity on general health. Physical inactivity is considered the fourth leading cause of all-cause mortality [10]—and is a primary risk factor for chronic illnesses such as obesity, type-2 diabetes, cardiovascular disease, and cancer [10,11,12]. Considering the significant health implications of physical inactivity, efforts to promote PA are crucial to ensure that individuals and communities can sustain long-term health, increase quality of life, and reduce the risk of illness and disability.
1.2. Health Disparities Faced by Underrepresented Racial Minorities
Data collected over recent decades suggest clear PA disparities between non-Hispanic White and underrepresented racial minorities (e.g., Black, Latino; hereafter “minorities”). Data have consistently shown that minorities are less likely to participate in regular PA than non-Hispanic White adults, regardless of the geographic region where they live [13,14,15]. To contextualize the PA disparities faced by minorities in the United States, it is essential to examine the social determinants of health (SDOH) that underpin these disparities. The SDOH refer to the conditions in an individual’s external environment that directly and indirectly affect their physical, mental, and emotional health [16]. These conditions have been shown to contribute to health disparities and include factors such as local/state economic conditions, education, health literacy, access to healthcare, and neighborhood environment [17].
Data suggest that minorities face considerable educational, economic, and social disparities that negatively affect their health outcomes [13,18]. More recent studies have shown that minorities are at a higher risk of contracting diseases such as COVID-19 [19] and have a higher incidence of preventable chronic illnesses [20,21,22]. Additional conditions that contribute to disparities include the built environment, which is defined as the human-made buildings and infrastructure that provide physical settings for individuals to live, work, learn, and engage in recreational activities [23]. Studies exploring the built environment have reported that minorities are more likely to live in communities with poorer walkability and limited access to resources [24,25,26], consequently resulting in worse health outcomes. Educational disparities are also faced by minorities, whereby these populations have been shown to have fewer opportunities to learn about healthy behaviors, such as PA [27,28]. Together, these data demonstrate that minorities face numerous disparities that make it difficult to adopt healthy behaviors. It is also evident that SDOHs play direct and indirect roles in the adoption of PA among minorities [29]. These data emphasize the need for investigators to account for such factors when promoting PA in these populations and to ensure that PA programs are constructed in a way that address inequities faced by minorities.
1.3. Barriers and Facilitators to Physical Activity Among Underrepresented Racial Minorities
Considering the disparities in regular PA participation faced by minority adults, it is evident that more work is required to facilitate opportunities and improve access to resources, which would support the adoption of PA behaviors for these populations. One way to start this process is to identify the barriers and facilitators to PA experienced by minority groups. To date, considerable work has been conducted to describe the barriers and facilitators to PA in numerous populations with physiological conditions, such as individuals with cancer [30,31,32], diabetes [33,34], and adults with disabilities [35]. Extensive studies have also been conducted to describe the barriers and facilitators to PA using age as the primary descriptive variable, including children [36,37], young adults [38,39], and older adults [40,41,42]. However, race or ethnicity is seldom reported in large and longitudinal population-based, adult studies in this body of literature [43]. This lack of race or ethnicity reporting consequently requires more attention from investigators.
Recent research has begun to elucidate the barriers and facilitators of physical activity among Latino populations in the United States, with a particular emphasis on female participants. Larson and colleagues [44] reported that barriers to PA for Latinas were linked to cultural norms around caregiving and cultural standards for body shape. Additional work in this population has reported that Latinas receive little social support for PA, despite having large, close-knit social networks [45]. This is confounded by the presence of various environmental barriers such as crime, extreme temperatures, traffic, lack of facilities to engage in PA, and fear of immigration enforcement [45,46,47]. Facilitators of PA in Latina populations have been shown to be similar to those of non–Latina Whites, with most research demonstrating that high self-efficacy and social support are motivating factors for engaging in PA [44,47]. The barriers and facilitators to PA have largely been understudied in Latino men [44], but existing work suggests that they share similar individual- and community-level barriers and facilitators when compared to Latinas [48].
The literature examining the barriers and facilitators to PA in Black adults in the United States has suggested that this population shares many of the same barriers with Latino community members. In an analysis of four national datasets, investigators demonstrated that Black adults were less likely to participate in PA if they had less education and a lower household income when compared to non-Hispanic White adults [49]. Other studies with a primary focus on older Black women have demonstrated that psychological constructs such as a lack of self-efficacy, social support, and the ability to self-regulate PA behaviors were barriers to PA participation [50,51,52]. Work in the same population has also shown that environmental factors such as neighborhood resource allocation and safety [52,53,54] can inhibit PA participation. The facilitators of PA documented in Black adults include factors such as perceived health benefits, social support from loved ones, and enjoyment derived from PA [51,53].
The literature on barriers and facilitators to PA participation outlined here suggests that minority populations face barriers to PA that align with various SDOH, including the built environment, educational attainment, and economic stability. However, several gaps remain in the literature that require further exploration. To date, data have primarily focused on minority groups situated in the Southwestern and Eastern portions of the United States, with minimal exploration of minorities in the midwestern region of the US. This region has numerous cultural, economic, and environmental differences from the aforementioned regions that make it distinct, which could alter the way previously reported barriers and facilitators influence PA participation. The literature on PA barriers and facilitators has also underreported how these factors differ between minority adults completing low and high amounts of PA. Exploring these differences may provide investigators with nuanced information that can better inform how individuals within the same group perceive and experience PA. Lastly, few studies have yet to fully elucidate how the long-term impacts of the COVID-19 pandemic have affected barriers and facilitators to PA in minority populations. COVID-19 intensified existing disparities faced by minority populations [55], including access to and opportunities to engage in PA [56]. Considering that many of the economic, social, and environmental impacts of the pandemic still exist today, it is necessary to explore how various factors influence PA participation.
1.4. Using the Socio-Ecological Model to Identify Barriers and Facilitators to Physical Activity
Theoretical frameworks provide investigators with structured and reproducible methodological approaches for answering research questions [57]. The use of theoretical frameworks can facilitate stronger PA programs in community settings by introducing consistent, structured, and holistic approaches to implementing such programs. Framing PA programs using theoretical models can help investigators and community stakeholders (i.e., health officials, legislatures, etc.) interpret program outcomes, better inform best practices for additional health programs, and provide stronger evidence for health-related policies. The present project explores the barriers and facilitators to PA in minorities using a socio-ecological model (SEM) [58]. The SEM suggests that health outcomes result from a complex interplay among individual, interpersonal, community, and societal domains that comprise an individual’s life. These domains encompass a wide range of factors, such as individual-level biology, interpersonal relationships, community resource availability, the built environment, and state/federal policies. It is important to note that this model suggests that factors in one domain can impact those in another domain, suggesting that it is necessary to account for all domains simultaneously to promote healthy behaviors.
The individual domain of the SEM encompasses factors related to an individual’s personal well-being, such as their psychological and physical states. Studies in the health behavior literature have demonstrated that various psychological constructs can play pivotal roles in PA participation. At the conscious level, work has shown that having an exercise identity (i.e., participating in PA is a key aspect of someone’s self-concept) can lead individuals to be more physically active [59]. Habit formation allows PA to be initiated with less conscious effort and reduces the mental burden necessary to continue PA in the long term [60,61]. Regarding the role of physical health, previous studies have suggested that individuals who perceive themselves as having physical limitations or a low level of physical fitness are less likely to engage in PA [41,62]. Together, these intrapersonal factors have been shown to play key roles in the adoption and maintenance of PA.
The interpersonal domain of the SEM can encompass the various social relationships an individual has and whether they feel socially supported to participate in a behavior. Social support refers to the perceived availability of social resources and support from an individual’s social relationships and comprises five distinct forms [63]: emotional (i.e., receiving encouragement), companionship (i.e., having a sense of belonging, having an activity partner), instrumental (i.e., having the resources needed to carry out a behavior), informational (i.e., having easily accessible information on how to perform a behavior), and validation (i.e., seeking others for social comparison, normative behavior). Social support has been shown to be a key factor that can help individuals remain physically active [64,65]. Conversely, lack of social support has been documented as a barrier to participation in regular PA [44]. These data suggest that social support plays a pivotal role in regular PA engagement.
The community domain of the SEM includes the social and physical settings where individuals live. The built environment is of particular interest to investigators and community stakeholders given its demonstrated direct impact on health outcomes [6]. Previous work has demonstrated that built environments possessing PA-supportive features (e.g., gyms and green spaces) can facilitate more PA [66,67] than communities that lack these attributes. Other neighborhood and built environment factors, such as crime rate, neighborhood walkability, and the prevalence of inclement weather [24,25,26,68], have also been shown to impact PA participation. Together, these data suggest a complex relationship between built environment factors and PA participation, underscoring the need to explore these factors when considering potential barriers and facilitators to PA in minorities.
The societal domain of the SEM comprises state/federal policies, social norms, and cultural norms that broadly influence individuals and communities. Public policies that distribute funds and resources to communities can have direct downstream impacts on PA participation [18,28]. Policies that shape the built environment, such as Complete Streets [69] and neighborhood zoning laws [70] can also play pivotal roles in individual and community level PA trends by instituting pedestrian-friendly features as a community default. To further support this point, recent work suggests that community residents are more likely to have good health if their neighborhoods have implemented pedestrian-friendly policies [71]. Cultural and social norms have also been shown to influence PA participation, particularly among minority populations. Studies conducted in Black and Latino communities have suggested that cultural and social norms surrounding caregiving and prioritization of the family unit over individual pursuits [44,72] are barriers to PA. Cumulatively, this domain of the SEM emphasizes the need for multifaceted strategies to promote PA, which take into account both top-down policy measures and underlying cultural norms present in diverse communities.
1.5. Study Purpose
The primary purpose of this study was to explore and contextualize the barriers and facilitators to PA faced by urban, midwestern, minority adults. The specific aims of this investigation were to: 1) qualitatively and quantitatively describe the existing barriers and facilitators to PA participation among minority community members and 2) explore differences in barriers and facilitators to PA between minorities who are completing high and low amounts of leisure-time PA. It was hypothesized that 1) minority adults would report barriers and facilitators that would span across all four domains of the SEM, and that 2) minorities completing low amounts of leisure-time PA would report more barriers and fewer facilitators to PA.
2. Materials and Methods
2.1. Study Design
2.2. Participant Recruitment and Eligibility Criteria
Community-dwelling minority adults were recruited from an urban Midwestern County between January and June 2024, using random sampling. Existing community partners within the target county aided in the dissemination of study recruitment materials via word of mouth, the promotion of recruitment flyers, and email correspondence with community members. The study staff also promoted recruitment materials on social media platforms, posts in public libraries, and tabling at local health-based events. Inclusion criteria were self-identification as a racial minority, being a resident living within a specified geographic area, and being >18 years old. Exclusion criteria included, not having access to a phone or computer, being unable to read and speak English or Spanish fluently, and inability to provide written informed consent. The participants were screened by phone or video calls and provided written informed consent before enrollment in the study. Individuals did not have an existing relationship with the primary investigator at the time of enrollment and were made aware of the research team’s reasons for and interest in the research topic. Participants were compensated with a $25.00 gift card for completing the study.
2.3. Study Survey
Participants completed a 30 – 45 minute electronic survey that aimed to explore potential barriers and facilitators to PA across the various domains of the SEM. Upon obtaining informed consent, participants were sent a link that directed them to the survey and instructed them to complete the survey in one sitting. The survey was completed on a personal computer or mobile device. A paper copy of the survey was made available upon request. All surveys were delivered by the principal investigator who was trained in conducting mixed-methods research.
The study survey comprised various sets of previously validated questionnaires that aimed to assess current weekly PA levels, as well as factors such as PA habit formation, exercise self-identity, perceptions of social support, and influences of the physical environment. The survey was linguistically and culturally translated into Spanish for application to Spanish-speaking demographics of the surveyed area by a fluent Spanish-speaking member of the research team. A different fluent Spanish-speaking member of the research team then back-translated the translated survey, ensuring that all translated items maintained semantic, idiomatic, and grammatical equivalence compared to the original English versions. Finally, the survey was refined for comprehension and understanding through pilot testing with Spanish-speaking community members.
2.3.1. International Physical Activity Questionnaire
The International Physical Activity Questionnaire – Long Form (IPAQ-LF) provides a set of well-developed survey questions that provide self-reported weekly estimates of PA [76]. The long-form questionnaire assesses weekly PA across the four established domains (occupational, transportational, household, and leisure-time PA) with acceptable concurrent and construct validity [76] as well as good test-retest reliability [77]. Participants were asked to report the weekly frequency (i.e., days per week and minutes per day) of light, moderate, and vigorous intensity activities performed across each domain, which were then analyzed to determine weekly minutes.
2.3.2. Barrier Analysis Survey
The Barrier Analysis Survey is a qualitative rapid assessment tool created to assess barriers and facilitators of a target health behavior [78,79]. The survey includes a combination of standardized open- and closed-ended questions framed on the Health Belief Model and the Theory of Reasoned Action, as well as questions that assess participant perceptions related to access to resources, policy, and culture [78,79]. The set of standardized questions [79] was adapted to explore the determinants of behavior associated with participating in PA. All questions were presented as part of the survey and placed towards the beginning to account for participant response fatigue [80,81].
2.3.3. Physical Activity Barrier Questionnaire
The Physical Activity Barrier Questionnaire (PABQ) is a 24-item questionnaire that assesses potential barriers to PA in adults aged >18 years. The questionnaire followed the SEM, wherein questions are categorized into three domains: personal, social environment, and physical environment [82]. All items are scored on a Likert scale ranging from 1 (“strongly disagree” ) to 5 (“strongly agree”). Previous reporting has demonstrated the survey to have good internal consistency (α = 0.86) as well as strong face and content validity [82].
2.3.4. Exercise Identity Scale
The Exercise Identity Scale (EIS) is a 9-item scale that assesses the salience of individuals identifying with exercise as an integral part of their self-concept [83]. The questions were delivered on a 5-point Likert scale and anchored by a stem that contextualizes each item within their personal exercise experience (e.g., “The following questions concern your personal beliefs about exercise. Please indicate the degree to which you agree or disagree with each statement when thinking about your exercise participation.”). Previous work has shown the EIS to have good internal reliability (α = 0.82 – 0.95) and criterion validity [84].
2.3.5. Physical Activity & Social Support Scale
The Physical Activity and Social Support Scale (PASSS) is a 20-item scale that assesses the perceived presence of social support related to PA among adults [63]. The PASSS has been shown to measure the five forms of social support (i.e., companionship, emotional, informational, instrumental, and validation) with good internal reliability (α = 0.89) and acceptable discriminant and convergent validity. Survey items were prefaced with a statement regarding the different ways in which an individual can receive support before prompting respondents to indicate how true a statement relates to the PA they engage in on a 7-point Likert scale, with 1 = never true and 7 = always true [63].
2.3.6. Self-Report Behavioral Automaticity Index
The Self-Report Behavioral Automaticity Index (SRBAI) is a validated 4-item instrument that has been shown to be a valid and internally reliable (α = 0.86) survey capable of characterizing the automaticity of a habit in adults [60]. The SRBAI items were slightly modified to assess the preparatory phase of habit [85] by adjusting the question stem (i.e., “When I prepare to exercise”), which was then followed by the four items on the scale. Items were presented on a 5-point Likert scale, with 1 = strongly disagree and 5 = strongly agree [60,85].
2.4. Participant Demographics
Participants were asked to respond to questions regarding their race/ethnicity, height/weight, income, education, the community they lived in, and how long they had been residents of their community.
2.5. Determination of Study Groups
Participants were labelled into one of two groups for analysis based on self-reported PA from the IPAQ-LF: Low Leisure Physical Activity (LLPA) or High Leisure Physical Activity (HLPA). Individuals in the LLPA group were those who reported completing <150 min/week of leisure-time PA. Individuals in the HLPA group were those who reported completing >150min/week of leisure-time PA. Leisure-time PA was calculated by summing the reported weekly minutes of leisure-time walking and exercise derived from the IPAQ-LF. The emphasis on leisure-time PA as a differentiator between groups is consistent with PA messaging focused on promoting leisure and exercise PA prominently within both the United States and WHO PA guidelines [2,3].
2.6. Data Analysis
2.6.1. Sample Size
An a priori power analysis using G-Power [86] was performed to conduct a cross-sectional analysis with two groups and ten response variables. Power analysis revealed that a sample of 76 participants was needed to detect significant differences (p = 0.05) at a medium effect size (F2 = 0.25) with a power (1 − β error probability) set at 0.80 for all primary quantitative outcome measures [87]. Cohen’s d was used to identify the effect size difference between groups. The estimation of effect size differences provides an acceptable way to quantify the magnitude of the difference between group means. Effect size estimates were interpreted using guidance provided by Ferguson [88], which suggests that an effect size d of 0.41 or greater is the recommended minimum effect size necessary to achieve a practically significant effect (RMPE).
2.6.2. Quantitative Data Analysis
SPSS (version 29.0) was used to conduct all analyses, including the computation of descriptive and inferential statistics. Survey composite scores were calculated by first converting Likert scale items to numeric values and subsequently summing item scores to obtain the sub-domain and total survey scores. Prior to the hypothesis tests, the Little Missing Completely at Random (MCAR) test [89] was performed to identify whether data were missing at random. If the criteria of MCAR and other data patterns were met, multiple imputations (MI) were used to estimate missing data [90,91]. The primary hypotheses were tested by conducting a MANOVA to assess the multivariate effects of the independent variables (weekly leisure-time PA min/week) on the dependent variables (survey composite and sub-composite scores). Significant tests at the multivariate level were further explored using one-way ANOVA. Weekly amounts of PA by domain were tested by conducting a series of ANOVAs. Differences in demographics data were assessed by independent samples t-tests. Cohen’s d was computed for between group differences among study groups for all primary outcomes [87,88].
2.6.3. Qualitative Data Analysis
Participant responses to the standardized set of open-ended questions from the Barrier Analysis questionnaire were transferred to an Excel sheet verbatim and verified by the primary investigator. Themes and subthemes were derived from the data using inductive thematic analysis [92], a flexible method that seeks to understand participants’ experiences, thoughts, and behaviors through the active construction of themes derived from a dataset. This analysis approach comprises a six-step process that involves 1) familiarization with the data, which was achieved by reading and re-reading participant responses; 2) establishing coding rules and generating initial codes; 3) searching for initial themes; 4) reviewing and refining initial themes; 5) defining and naming themes and sub-themes; and 6) producing a final report [92].
Multiple strategies were undertaken to ensure the credibility, dependability, confirmability, and transferability of these data. Two study team members analyzed the transcripts separately and then came together to discuss their interpretations of the data. The inter-rater reliability agreement threshold was set to ≥ 70%. A consensus among the research team personnel was reached for all initial codes before the subsequent coding and generation of themes commenced. During all discussions, a “critical friends” approach was undertaken [93]. In this approach, critical dialogue between members of the researcher team was undertaken, whereby members gave voice to their interpretations of the data in relation to other study staff who listened and offered critical feedback. The aim of this approach is to encourage reflexivity and provide a theoretical sounding board to encourage the exploration of multiple alternative explanations and interpretations of data. This approach has been shown to be acceptable for demonstrating rigor in analyzing qualitative data [93,94]. The participants did not provide feedback on the qualitative findings at this stage of the study. Data were reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines [95].
3. Results
After screening to ensure individuals met the study’s inclusion criteria, 29 participants completed the survey (LLPA, n = 11; HLPA, n = 18). The majority of participants were female (86.21%) and educated (65.52% held a bachelor’s degree or more); 44.83% identified themselves as Black, and 41.37% identified themselves as Latino. Independent samples t-tests did not reveal differences in demographics variables (p > 0.05). Participants in the HLPA group engaged in more leisure-time PA (LLPA = 44.55 ± 48.40 min/week, HLPA = 448.89 ± 227.43 min/week; F(1, 27) = 33.39, p = 0.001, d = 2.21) at the time of enrollment. RMPE differences were observed between groups for body mass (d = -0.53) and body mass index (BMI, d = -0.42). Remaining demographics can be found in Table 1. A full description of the participant flow through screening and informed consent is shown in Figure 1.
3.1. Missing Data Analysis
Missing data analysis revealed that 0.088% of the data were incomplete. Little’s MCAR test found the data to be completely missing at random (χ2 = 0.00, DF = 154, p = 1.00). Since the proportion of missing data observed was below 5.00%, missing data were ignored during analysis, and MI was not conducted [90].
3.2. Self-Reported Physical Activity
Full descriptions of the PA domain-specific means, standard deviations, and between-group differences can be found in Table 2. Participants in the HLPA group reported engaging in significantly more total PA (F(1, 27) = 6.80, p = 0.02), total walking PA (F(1, 27) = 6.91, p = 0.01), leisure-time walking PA (F(1, 27) = 22.08, p < 0.001), and exercise MVPA (F(1, 27) = 12.34, p = 0.002) than those in the LLPA group. While not significant, practical effect size differences were observed, favoring the HLPA group for occupational walking PA (d = 0.54), total occupational PA (d = 0.53), and total MVPA (d = 0.67).
3.3. Quantitative Survey Results
The MANOVA testing survey composite scores was found to be statistically non-significant between groups (F(1,27) = 1.18, p = 0.37; Wilk's λ = 0.61), but yielded a practical effect size difference (partial η2 = 0.40) at the multivariate level [88]. Follow-up univariate tests revealed that the LLPA group faced significantly more personal barriers to PA than the HLPA group (F(1, 27) = 5.72, p = 0.02, d = -0.92). Total composite scores for the PABQ were significantly different between groups (LLPA = 60.73 ± 19.90, HLPA = 47.44 ± 12.84; F(1, 27) = 4.81, p = 0.04, d = -0.84). Total composite scores for the PASSS were not statistically significant, but did achieve a practical effect size difference (LLPA = 59.00 ± 13.21, HLPA = 67.00 ± 20.31; F(1, 27) = 1.35, p = 0.26, d = 0.44) [87,88]. Full descriptions of survey composite score means, standard deviations, and between-group differences can be found in Table 3.
3.4. Qualitative Survey Results
Inductive thematic analysis revealed that the HLPA group had 11 distinct barriers to PA and 16 distinct facilitators to PA. The LLPA group had 11 distinct barriers to PA and 12 distinct PA facilitators. Analysis revealed that both groups shared six barriers and eight PA facilitators. Descriptions of prominent barriers and facilitators across each of the SEM domains are below. A full description of identified barriers to PA for both groups with associated quotes can be found in Table 4. A full description of identified facilitators to PA for both groups with associated quotes can be found in Table 5.
3.4.1. Personal Level Barriers
Lack of Time. Inductive thematic analysis revealed that both groups repeatedly mentioned that their work schedules made it difficult to find time to be active. One participant from the LLPA group mentioned that “Balancing full time work and part time school [makes it hard for me to be active],” while another LLPA group participant mentioned that “[Physical activity] takes time away from work, causing me to give up sleep, take an unpaid lunch break, and/or work longer hours.” These quotes suggest that scheduling PA into daily and weekly schedules was an issue for these participants. While individuals in the HLPA group also reported work schedules as a factor that limited their time to be active, HLPA group members mentioned that school, family obligations, and other responsibilities prevented them from finding time to be active. One participant mentioned that "School… discourages me from being active as [school] takes up too much time in my schedule." Another participant stated that "Family obligations, work obligations, and lack of time [makes it hard to be active]". A third participant highlighted that having two jobs made it exceedingly difficult to be active, stating that "Finding time [makes it hard to be active]. I have two jobs that take up every single day all day." Together, these quotes suggest that participants have various competing life demands that make it complicated to be physically active.
Financial Costs Associated with PA. Cost was a prevalent personal barrier for both study groups as well as an identified sub-theme within other primary themes within the community and societal domains. Several participants mentioned that engaging in PA was expensive, and prohibited them from being active. One participant mentioned that "expensive gym memberships [discourage me from being active]"; while another participant mentioned “programs that are expensive and not local [discourage me from being active]." When asked about what would help facilitate PA, participants from both groups mentioned that free or reduced-cost PA resources would help them be more active. Proposed free or reduced cost resources included community PA class ("Free community offered classes, and physical events (yoga, dance, walking/running,) [would help me be more active]. A community gym offered at a free and or very reduced rate."), community walking programs ("I'm already interested in anything free, but especially if I have an interest in an activity like yoga. A community walking program would be very helpful and fun to get into."), and free access to local gyms ("Free gym memberships with a trainer [would help me be more active]").
3.4.2. Personal Level Facilitators
Knowledge of PA Benefits. A majority of participants across both groups reported knowing about the positive health benefits that can be achieved with regular PA. Two participants from the HLPA reported that they knew about the linear relationship between the amount of PA you do and the amount of health benefits you can achieve—one stating that they were "fairly knowledgeable [about the benefits of physical activity]. The more active you are, the better health you'll have." Participants from both groups commented that they knew that PA had many benefits for their physical health, such as keeping their heart and joints healthy ("Physical activity leads to good cardiac and joint mobility."). Participants also mentioned knowing about the link between PA and mental and emotional health. One participant stated the following regarding this link:
"If you don't use it, you will lose it. Staying active activates the happy hormone and relieves stress; it produces clarity of the mind… walking in nature produces some peace and grounding… Physical activity is providing a holistic measure for producing good health, mind, body, and spirit; good health is wealth."
Health Benefits Accrued from PA. Participants across both groups reported that PA has helped them gain health benefits in the past and that these past experiences motivate them to try to continue being active. Inductive thematic analysis revealed that the mental health benefits accrued from PA were a prevalent sub-theme, with several participants stating that PA helped them improve their mood, enhance their confidence, and decrease depressive thoughts. One participant from the LLPA group stated that "[physical activity] helps with sleep, mood, concentration, and balancing mental health struggles.” A different participant from the HLPA group stated that PA helped give them a "clear mind, good attitude, and decrease in depression,” while another participant from the same group stated that PA provided them with "better mental health, better mood, more energy and increase[d] productivity.”
3.4.3. Interpersonal Level Facilitators
Social Support. The majority of participants from both study groups reported that they had individuals in their lives who directly or indirectly supported them to be physically active. When asked about who in their life supports them in being active, participants mentioned that immediate family (i.e., parents, siblings, spouses, etc.) would encourage them. One participant mentioned that "my husband, my mother [support me]" to be active, while a different participant said, "My fiancé, kids, and best friend [support me]". In addition to immediate family support, others mentioned that they had social support from extended social circles, including friends ("Having a gym buddy [helps me stay active]."), work colleagues ("I do ‘Walking Wednesdays’ with colleagues."), and members of their community ("My community consists of active older adults who are generally very physically active). The general consensus among participants was that having others discourage them from being active was uncommon. As one participant put it: "I don't think I have ever run into someone that has discouraged me from being active."
3.4.4. Community and Societal Level Barriers
Lack of PA Facilities or Transit Options. One participant mentioned that "[Not having] a convenient gym [makes it hard to be active]"—while another participant stated, "[Not having] easy access to public transport [makes it harder to be active]." Two individuals in the LLPA group stated that inclement weather was a barrier to being active, one of which stated, "Some days, the weather doesn't allow for me to get outside and enjoy walking or driving to the local YMCA for group exercise."
3.4.5. Community and Societal Level Facilitators
Community PA Facility Availability. Both groups were clear that easier access to PA facilities in their community would facilitate more PA. When asked what community resources would make it easier for them to be active, several participants stated that having access to a free gym ("A good gym that was also free would help me be more active.") and having access to sports-specific facilities ("More places to play tennis or pickleball [would help me be more active]") would facilitate PA for them. As mentioned, cost was a prominent sub-theme in many of the responses. When asked about what community resources would help them be more active, one participant responded, "Free access to gym/ recreational activities and resources for beginners [would help me be more active]." A separate participant shared this sentiment, stating "Free or super reduced [gym] memberships [would help me be more active].”
Community PA Events and Programs. Inductive thematic analysis revealed that having more PA-related events and programs in their community would help participants be more active. Specifically, participants commented that regular pick-up sports games ("regular cricket games in [the] softball field. Having some table tennis tournaments”) and outdoor fitness programs ("Free community offered classes, and physical events (yoga, dance, walking/running,)…") would facilitate PA for them. Having employers support PA through sponsored programs was also reported by participants as a facilitator to PA. As one participant commented when asked about what policies support them being active, "Something with employment, money back for being active [would encourage me to be active]"
4. Discussion
The present study aimed to explore the existing barriers and facilitators to PA among urban Midwestern minorities using a concurrent mixed-methods approach framed by the SEM. This study is the first to the authors’ knowledge that has assessed the barriers and facilitators to PA using a theory-driven, mixed-methods approach in this regional population, and presents novel findings that can inform future PA interventional programs.
The present study revealed that the HLPA group engaged in higher weekly leisure-time PA than the LLPA group and exceeded the USPA Guidelines [3]and used the IPAQ-LF to document weekly PA performed by study participants across all PA domains [1]. The IPAQ-LF is an easily administered, globally validated survey [77] that can estimate PA with moderate validity compared with accelerometry-derived PA estimates [96]. Documenting PA across all domains is important to help investigators have a full understanding of someone’s weekly activity trends. Historically, estimates of PA have focused on activities performed almost exclusively during leisure time [97]. This tendency to measure only leisure-time PA may consequently result in the underestimation of an individual’s weekly PA levels [98].
The LLPA group achieved USPA guidelines primarily through occupational and household MVPA. These outcomes are consistent with those of previous studies [98,99,100], demonstrating that minorities are more likely to be categorized as meeting USPA guidelines when all domains are considered in the estimation of weekly PA. While these data are initially encouraging, recent studies suggest that not all PA domains have the same impact on health [101,102]. Work focusing on health outcomes stratified by the amount of occupational PA done suggest the presence of a “PA health paradox” [101]—whereby occupational PA has been shown to be associated with adverse impacts on cardiovascular health and all-cause mortality [103,104,105,106]. Given that minorities are more likely to work in more physically demanding occupations [107] and are less likely to engage in leisure-time PA [108], future work should aim to further document how PA across various domains impacts health outcomes in minorities, and investigate how these trends influence an individual’s willingness to participate in research and community PA programs.
Quantitative outcomes from this study revealed that participants completing low amounts of leisure PA reported more personal barriers to PA. These findings were further supported by the qualitative outcomes, which reported more personal barriers in the LLPA group. Regarding psychological barriers, the LLPA group reported having less motivation and discipline to be active as well as expressing a dislike for the physical sensations (i.e., soreness, sweating, etc.) associated with being active. These findings are consistent with previous studies [47,51] and lend further support to the presence of persistent personal barriers to PA in this population. The psychological barriers reported by participants align with the affective determinants of PA [109]. These determinants, such as how someone feels when performing an activity or having the motivation to engage in activity, have been shown to impact future PA behavior. Specifically, individuals who have positive associations between affective responses and PA are more likely to continue participation [110,111].
The quantitative results from the current study also suggest that the HLPA group was more likely to report a stronger exercise identity and exercise behavior that was more habitual. While not explicitly stated in participants’ quotes, several participants in the HLPA group alluded to the idea that PA was an important part of their lives, lending further support to the quantitative findings. To the authors’ knowledge, this is the first investigation in the existing literature on this topic to consider these psychological constructs when exploring potential barriers and facilitators to PA. Previous work has demonstrated a positive correlation between habit and PA participation [112], and suggests that having an existing habit can be predictive of future PA [61]. Numerous studies completed in new exercisers have shown that successfully building a PA habit can facilitate higher weekly PA [113,114]. In addition, having an exercise identity has been shown to help strengthen PA-related behaviors by positively impacting an individual's self-concept [59]. Taken together, future PA programs should consider embedding strategies that positively reinforce these constructs to help minorities adopt regular PA.
The qualitative results from this study suggested that the LLPA group had lower perceived physical capacity and was more conscious about the injury risks associated with PA. These voiced perceptions were further supported by the individual PABQ personal domain item response rates, which suggested that the LLPA group had physical limitations that prevented PA participation. Low physical capacity and the risk of injury are both prevalent barriers to PA among minorities [44,51,115]. These perceptions are consistent with previous work, suggesting that individuals are less likely to engage in PA if they have an injury or physical limitation [41,62]. USPA guidelines suggest that, assuming no contraindications are present, individuals of any ability or physical state can participate in PA. One approach to helping individuals build confidence to be active is to build and reinforce physical literacy, which refers to the competence, confidence, and knowledge to be physically active in a variety of environments. Physical literacy has been established as a key determinant of health in adults, with preliminary evidence suggesting a positive relationship between physical literacy and health outcomes [116]. Considering that many US states have been de-prioritizing K-12 physical education (the traditional route through which most people learn physical literacy) over the last 20 years [27,117], future work should aim to incorporate approaches to enhance physical literacy in K-12 settings to help individuals overcome their fear of injury and doubts of physical capacity.
Responses to the qualitative survey questions revealed that the lack of time to be active was a prominent barrier for both the study groups. This outcome is further supported by individual PABQ social environment domain item response rates, which suggest that both groups had life demands that limited their time to be physically active. These data further support previous literature reporting time to be a significant barrier to PA [42,44,45,51,115,118]. These findings are unsurprising considering that minorities are more likely to work long, irregular hours [119] that prevent the establishment of a PA habit and have different cultural norms around the family that may limit time for PA [45]. Finding strategies to help individuals accommodate these factors may in turn require a combination of different programmatic approaches, such as the implementation of action planning and adjusting how programs prescribe PA to participants. Action planning is a self-regulatory strategy shown to bridge the intention-behavior gap by helping individuals establish goals, plan for potential barriers, and improve time management [120]. Action planning has been successfully implemented in new exercisers [113,121], and may be a viable approach to help individuals find time to be active. In addition, PA program facilitators may consider adjusting program-facing activity recommendations to encourage shorter bouts of activity spread across the day (i.e., ~10 min bouts several times per day) over one longer bout per day (i.e., 3x/week for 45 min) to account for existing time constraints. This approach to PA engagement has been shown to lead to positive health benefits [122] and remains in line with the existing PA guidelines [3].
Financial cost appeared both as a primary theme and subtheme among participants’ responses, suggesting that participants had cost in mind when making decisions about being active. These qualitative data are further supported by the outcomes of the PABQ response rates to items related to cost, which suggest that more than half of the LLPA group participants and one-third of the HLPA group participants agreed that cost was a barrier to PA. Cost has repeatedly been reported as a barrier to PA participation [35,41,123,124]. This is largely unsurprising given the combination of existing disparities in wage earnings between minorities and non-Hispanic White adults [107], and existing sentiments around inflation and the cost of living in the United States [125]. Previous work done on minorities has attempted to address financial barriers by providing free or reduced-cost PA programs [126,127]; however, it is unclear to what extent these economic benefits continue for participants beyond the end of these interventions. Considering that economic stability is a key SDOH, future PA programs should consider the financial costs incurred by communities —prioritizing inexpensive PA options that can be sustained by communities beyond the conclusion of a study intervention or organizational program.
To the authors’ knowledge, this study is the first in the barriers and facilitators literature to use the PASSS [63] to assess all five established forms of social support. The findings from this study suggest that the LLPA group had less informational (i.e., having easy access to PA-supportive information and knowing how to use it) and instrumental (i.e., having the necessary resources and support to carry out PA) support than did the HLPA group. The lack of informational support may be partially attributed to the lack of health literacy among the participants. Studies on the association between health literacy and PA participation have shown that high levels of health literacy are associated with higher levels of PA and vice versa [128]. Regarding discrepancies in instrumental support, this may be attributed to minorities having fewer material or economic resources to lend others in their social circles to participate in PA. Considering the limited amount of work done to facilitate instrumental and information support for this demographic, future PA programs may need to develop novel approaches to facilitate these forms of social support to promote regular PA.
Both study groups reported in their qualitative responses to feeling social support for being physically active from immediate family and extended social circles. These data are partially supported by the outcomes from the PASSS emotional support subdomain composite score, which demonstrated similar scores between the two groups. This finding is consistent with previous work suggesting that emotional and companionship forms of social support are key facilitators to PA in minorities [33,115,129]. Randomized control trials in minorities have consistently shown that emotional and companionship support can lead to higher rates of PA and increased enjoyment [50,64,65,130]. Together, these results further support the key role that emotional and companionship support can play in helping individuals to remain active.
Responses to the qualitative set of survey questions revealed that a lack of community PA facilities and public transit options was a barrier for both groups. Conversely, both groups reported that having more PA facilities/events and public transit options in their community would facilitate PA. Results from the PABQ revealed that the LLPA group perceived more physical environment barriers than the HLPA group. Having close proximity and easy access to PA facilities (i.e., gyms, outdoor fields, parks) has been reported to facilitate PA for other regional minority populations in the United States [47,115,131]. The built environment is a key SDOH that has been shown to have a direct impact on health outcomes [6,132]. A recent panel study further supports this assertion, demonstrating that residents are more likely to report having good health status (i.e., no incidence of chronic disease, meeting USPA guidelines) if their neighborhood environments have parks within walking distance; have higher walkability and biking scores; and have instituted Complete Streets policies [71]. Built environment policies such as Complete Streets [69] or zoning laws that dictate where community resources can be distributed play a pivotal role in community-level PA trends. Considering that minorities are more likely to reside in communities that lack PA resources and are more hazardous to pedestrians [44,133], more action must be taken by both investigators and legislators to provide PA-supportive environments for these communities.
4.1. Strengths and Limitations
This study has several strengths and limitations worth noting that aid in contextualizing these data. This project was executed using a cross-sectional study design, indicating that these data should be interpreted as associative rather than causal. It is also important to note the community and societal context in which the study’s participants reside (i.e., an urban Midwestern County with a growing minority population). In turn, these community and societal characteristics may limit the transferability of these findings to communities that share similar characteristics. PA estimates collected through self-report have been historically documented to be prone to reporting bias [134] and overestimate PA compared to accelerometers. Careful attention was given to selecting a self-report PA survey that has documented validity compared to accelerometers [96] and has wide transferability to different study populations [77]. Despite these limitations, this study advances existing literature by presenting a comprehensive approach to exploring barriers and facilitators to PA in minorities. Specifically, this study utilized a concurrent mixed methods study framed on the SEM, incorporating various scientific perspectives to answer the study’s specific aims. The present study also presented estimates of all four domains of PA, providing a complete picture of participants' weekly activity levels. Finally, this project incorporated numerous widely accessible, validated surveys that enhance comparability with future studies and improve methodological reproducibility.
5. Conclusions
The findings from this study emphasize the need for health researchers and professionals to consider how factors across the SEM prevent and support PA in minorities. Findings from this study suggest that minorities completing low levels of leisure-time PA require various personal level supports to be active, such as motivational messaging, assistance in forming a PA habit, and planning PA into their schedules. These data also suggest that social support and accountability are key factors that help individuals engage in PA. Most notably, these data demonstrate that the financial cost of PA is a key concern for this demographic and stresses the need for community organizations and research teams to offer PA options that are free or at a significantly reduced cost to communities. These offerings should be provided as close to the communities of interest as possible, and should aim to provide participants with various PA options that can be adapted to busy schedules. Taken together, these data can aid investigators and community stakeholders in constructing PA programs that address the key barriers faced by minorities.
Author Contributions
Conceptualization, R.A.A., N.K., S.M.B., and N.R.K.; methodology, R.A.A., N.K., S.M.B., and N.R.K.; software, R.A.A. and N.K.; validation, R.A.A., N.K., S.M.B., and N.R.K.; formal analysis, R.A.A.; investigation, R.A.A. and N.R.K.; resources, R.A.A., S.M.B., and N.R.K.; data curation, R.A.A.; writing—original draft preparation, R.A.A.; writing—review and editing, R.A.A., N.K., S.M.B., and N.R.K.; visualization, R.A.A.; supervision, N.K., S.M.B., and N.R.K.; project administration, R.A.A.; funding acquisition, N.R.K. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by Indiana University internal faculty research funds.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Indiana University (protocol code 21976, approved February 21, 2024).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
The authors would like to thank our community partners, Melissa M. Sherman, Ph.D., and Adriana M. Alamilla, M.S. for their support of this work.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical Activity, Exercise, and Physical Fitness: Definitions and Distinctions for Health-Related Research. Public Health Rep 1985, 100, 126–131.
- World Health Organization WHO Guidelines on Physical Activity and Sedentary Behavior; World Health Organization: Geneva, 2020; ISBN 978-92-4-001512-8.
- Office of Disease Prevention and Health Promotion Physical Activity Guidelines for Americans; 2nd ed.; U.S. Department of Health and Human Services: Washington DC, 2018;
- Warburton, D.E.R.; Bredin, S.S.D. Health Benefits of Physical Activity: A Systematic Review of Current Systematic Reviews. Current Opinion in Cardiology 2017, 32, 1–16. [CrossRef]
- Patterson, M.S.; Patterson, C.A.; Walsh, S.M.; Bernhart, J.A. A Five-Year Evaluation of the Bearfit Worksite Physical Activity Program. Occupational Medicine & Health Affairs 2017. [CrossRef]
- Seo, B.; Nan, H.; Monahan, P.O.; Duszynski, T.J.; Thompson, W.R.; Zollinger, T.W.; Han, J. Association between US Residents’ Health Behavior and Good Health Status at the City Level. Translational Journal of the American College of Sports Medicine 2024, 9, e000258. [CrossRef]
- Centers for Disease Control and Prevention Adult Physical Inactivity Outside of Work; Centers for Disease Control and Prevention, 2022;
- Elgaddal, N.; Kramarow, E.A.; Reuben, C. Physical Activity Among Adults Aged 18 and Over: United States, 2020; National Center for Health Statistics: Hyattsville, MD, 2022;
- Centers for Disease Control and Prevention CDC Releases Updated Maps of America’s High Levels of Inactivity; Center for Disease Control, 2022;
- World Health Organization Physical Inactivity Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3416 (accessed on 12 December 2022).
- Glynn, L.; Hayes, P.S.; Casey, M.; Glynn, F.; Alvarez-Iglesias, A.; Newell, J.; ÓLaighin, G.; Heaney, D.; O’Donnell, M.; Murphy, A.W. Effectiveness of a Smartphone Application to Promote Physical Activity in Primary Care: The SMART MOVE Randomised Controlled Trial. British Journal of General Practice 2014. [CrossRef]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of Physical Inactivity on Major Non-Communicable Diseases Worldwide: An Analysis of Burden of Disease and Life Expectancy. The Lancet 2012. [CrossRef]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.F.; Martin, B.W.; Lancet Physical Activity Series Working Group Correlates of Physical Activity: Why Are Some People Physically Active and Others Not? Lancet 2012, 380, 258–271. [CrossRef]
- Centers for Disease Control and Prevention Behavioral Risk Factor Surveillance System Available online: https://www.cdc.gov/brfss/index.html (accessed on 26 October 2022).
- Sohn, E.K.; Porch, T.; Hill, S.; Thorpe, R.J. Geography, Race/Ethnicity, and Physical Activity among Men in the United States. American Journal of Men S Health 2017. [CrossRef]
- Healthy People 2030; U.S. Department of Health and Human Services Social Determinants of Health Available online: https://health.gov/healthypeople/priority-areas/social-determinants-health (accessed on 26 April 2024).
- World Health Organization A Conceptual Framework for Action on the Social Determinants of Health. 2010, 76.
- Brownson, R.C.; Baker, E.A.; Housemann, R.A.; Brennan, L.K.; Bacak, S.J. Environmental and Policy Determinants of Physical Activity in the United States. Am J Public Health 2001, 91, 1995–2003. [CrossRef]
- Centers for Disease Control and Prevention COVID-19 Hospitalization and Death by Race/Ethnicity - 2022 Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html (accessed on 15 December 2022).
- Braveman, P.A.; Cubbin, C.; Egerter, S.; Williams, D.R.; Pamuk, E. Socioeconomic Disparities in Health in the United States: What the Patterns Tell Us. Am J Public Health 2010, 100, S186–S196. [CrossRef]
- GBD US Health Disparities Collaborators Cause-Specific Mortality by County, Race, and Ethnicity in the USA, 2000–19: A Systematic Analysis of Health Disparities. The Lancet 2023, 402, 1065–1082. [CrossRef]
- Teitler, J.; Wood, B.M.; Zeng, W.; Martinson, M.L.; Plaza, R.; Reichman, N.E. Racial-Ethnic Inequality in Cardiovascular Health in the United States: Does It Mirror Socioeconomic Inequality? Annals of Epidemiology 2021, 62, 84–91. [CrossRef]
- Seyedrezaei, M.; Becerik-Gerber, B.; Awada, M.; Contreras, S.; Boeing, G. Equity in the Built Environment: A Systematic Review. Building and Environment 2023, 245, 110827. [CrossRef]
- Althoff, T.; Sosič, R.; Hicks, J.L.; King, A.C.; Delp, S.L.; Leskovec, J. Large-Scale Physical Activity Data Reveal Worldwide Activity Inequality. Nature 2017, 547, 336–339. [CrossRef]
- Ramirez, A.; Aguilar, R.; Merck, A.; Sukumaran, P.; Gamse, C. The State of Latino Housing, Transportation, and Green Space: A Research Review; Robert Woods Johnson Foundation, 2019; p. 39;
- Saelens, B.E.; Sallis, J.F.; Frank, L.D. Environmental Correlates of Walking and Cycling: Findings from the Transportation, Urban Design, and Planning Literatures. ann. behav. med. 2003, 25, 80–91. [CrossRef]
- Slater, S.J.; Nicholson, L.; Chriqui, J.; Turner, L.; Chaloupka, F. The Impact of State Laws and District Policies on Physical Education and Recess Practices in a Nationally-Representative Sample of U.S. Public Elementary Schools. Arch Pediatr Adolesc Med 2012, 166, 311–316. [CrossRef]
- Alamilla, R.A.; Keith, N.R.; Hasson, R.E.; Welk, G.J.; Riebe, D.; Wilcox, S.; Pate, R.R. Future Directions for Transforming Kinesiology Implementation Science into Society. Kinesiology Review 2023, 12, 98–106. [CrossRef]
- Hawes, A.; Smith, G.; McGinty, E.; Bell, C.; Bower, K.; LaVeist, T.; Gaskin, D.; Thorpe, R. Disentangling Race, Poverty, and Place in Disparities in Physical Activity. IJERPH 2019, 16, 1193. [CrossRef]
- Adamovich, T.; Watson, R.; Murdoch, S.; Giovino, L.; Kulkarni, S.; Luchak, M.; Smith-Turchyn, J. Barriers and Facilitators to Physical Activity Participation for Child, Adolescent, and Young Adult Cancer Survivors: A Systematic Review. J Cancer Surviv 2022. [CrossRef]
- Ning, Y.; Wang, Q.; Ding, Y.; Zhao, W.; Jia, Z.; Wang, B. Barriers and Facilitators to Physical Activity Participation in Patients with Head and Neck Cancer: A Scoping Review. Support Care Cancer 2022, 30, 4591–4601. [CrossRef]
- Sattar, S.; Haase, K.R.; Bradley, C.; Papadopoulos, E.; Kuster, S.; Santa Mina, D.; Tippe, M.; Kaur, A.; Campbell, D.; Joshua, A.M.; et al. Barriers and Facilitators Related to Undertaking Physical Activities among Men with Prostate Cancer: A Scoping Review. Prostate Cancer Prostatic Dis 2021, 24, 1007–1027. [CrossRef]
- O’Neal, L.J.; Scarton, L.; Dhar, B. Group Social Support Facilitates Adoption of Healthier Behaviors among Black Women in a Community-Initiated National Diabetes Prevention Program. Health Promotion Practice 2022, 23, 916–919. [CrossRef]
- Vilafranca Cartagena, M.; Tort-Nasarre, G.; Rubinat Arnaldo, E. Barriers and Facilitators for Physical Activity in Adults with Type 2 Diabetes Mellitus: A Scoping Review. IJERPH 2021, 18, 5359. [CrossRef]
- Nikolajsen, H.; Sandal, L.F.; Juhl, C.B.; Troelsen, J.; Juul-Kristensen, B. Barriers to, and Facilitators of, Exercising in Fitness Centres among Adults with and without Physical Disabilities: A Scoping Review. IJERPH 2021, 18, 7341. [CrossRef]
- Hesketh, K.R.; Lakshman, R.; van Sluijs, E.M.F. Barriers and Facilitators to Young Children’s Physical Activity and Sedentary Behaviour: A Systematic Review and Synthesis of Qualitative Literature. Obes Rev 2017, 18, 987–1017. [CrossRef]
- Nally, S.; Ridgers, N.D.; Gallagher, A.M.; Murphy, M.H.; Salmon, J.; Carlin, A. “When You Move You Have Fun”: Perceived Barriers, and Facilitators of Physical Activity from a Child’s Perspective. Front Sports Act Living 2022, 4, 789259. [CrossRef]
- Poobalan, A.S.; Aucott, L.; Clarke, A.; Smith, W.C.S. Physical Activity Attitudes, Intentions and Behaviour among 18-25 Year Olds: A Mixed Method Study. BMC Public Health 2012. [CrossRef]
- Peng, B.; Ng, J.Y.Y.; Ha, A.S. Barriers and Facilitators to Physical Activity for Young Adult Women: A Systematic Review and Thematic Synthesis of Qualitative Literature. Int J Behav Nutr Phys Act 2023, 20, 23. [CrossRef]
- Crombie, I.K.; Irvine, L.; Williams, B.; McGinnis, A.R.; Slane, P.W.; Alder, E.M.; McMurdo, M.E.T. Why Older People Do Not Participate in Leisure Time Physical Activity: A Survey of Activity Levels, Beliefs and Deterrents. Age Ageing 2004, 33, 287–292. [CrossRef]
- Franco, M.R.; Tong, A.; Howard, K.; Sherrington, C.; Ferreira, P.H.; Pinto, R.Z.; Ferreira, M.L. Older People’s Perspectives on Participation in Physical Activity: A Systematic Review and Thematic Synthesis of Qualitative Literature. Br J Sports Med 2015, 49, 1268–1276. [CrossRef]
- Wingood, M.; Peters, D.M.; Gell, N.M.; Brach, J.S.; Bean, J.F. Physical Activity and Physical Activity Participation Barriers among Adults 50 Years and Older during the COVID-19 Pandemic. Am J Phys Med Rehabil 2022, 101, 809–815. [CrossRef]
- U.S. Department of Health and Human Services Physical Activity Guidelines for Americans Midcourse Report: Implementation Strategies for Older Adults; U.S. Department of Health and Human Services: Washington DC, 2023;
- Larsen, B.A.; Noble, M.; Murray, K.; Marcus, B.H. Physical Activity in Latino Men and Women Facilitators, Barriers, and Interventions. American Journal of Lifestyle Medicine 2015, 9, 4–30. [CrossRef]
- Larsen, B.A.; Pekmezi, D.; Marquez, B.; Benitez, T.J.; Marcus, B.H. Physical Activity in Latinas: Social and Environmental Influences. Womens Health (Lond Engl) 2013, 9, 10.2217/whe.13.9. [CrossRef]
- Amesty, S. Barriers to Physical Activity in the Hispanic Community. Journal of Public Health Policy 2003. [CrossRef]
- Payán, D.D.; Sloane, D.C.; Illum, J.; Lewis, L.B. Intrapersonal and Environmental Barriers to Physical Activity among Blacks and Latinos. Journal of Nutrition Education and Behavior 2019, 51, 478–485. [CrossRef]
- Marquez, D.X.; Aguiñaga, S.; Campa, J.; Pinsker, E.C.; Bustamante, E.E.; Hernandez, R. A Qualitative Exploration of Factors Associated with Walking and Physical Activity in Community-Dwelling Older Latino Adults. J Appl Gerontol 2016, 35, 664–677. [CrossRef]
- Williams, W.M.; Yore, M.M.; Whitt-Glover, M.C. Estimating Physical Activity Trends among Blacks in the United States through Examination of Four National Surveys. AIMSPH 2018, 5, 144–157. [CrossRef]
- Anderson, E.; Wojcik, J.R.; Winett, R.A.; Williams, D.M. Social-Cognitive Determinants of Physical Activity: The Influence of Social Support, Self-Efficacy, Outcome Expectations, and Self-Regulation among Participants in a Church-Based Health Promotion Study. Health Psychol 2006, 25, 510–520. [CrossRef]
- Gothe, N.P.; Kendall, B.J. Barriers, Motivations, and Preferences for Physical Activity among Female African American Older Adults. Gerontology and Geriatric Medicine 2016, 2, 2333721416677399. [CrossRef]
- Mama, S.K.; McCurdy, S.A.; Evans, A.E.; Thompson, D.; Diamond, P.M.; Lee, R.E. Using Community Insight to Understand Physical Activity Adoption in Overweight and Obese African American and Hispanic Women: A Qualitative Study. Health Education & Behavior 2015, 42, 321–328. [CrossRef]
- Liu, C.K.; Afezolli, D.; Seo, J.; Syeda, H.; Zheng, S.; Folta, S.C. Perceptions of Physical Activity in African American Older Adults on Hemodialysis: Themes from Key Informant Interviews. Archives of Rehabilitation Research and Clinical Translation 2020, 2. [CrossRef]
- Keith, N.R.; Xu, H.; De Groot, M.; Hemmerlein, K.; Clark, D.O. Identifying Contextual and Emotional Factors to Explore Weight Disparities between Obese Black and White Women: Supplementary Issue: Health Disparities in Women. Clin Med�Insights�Womens�Health 2016, 9s1, CMWH.S34687. [CrossRef]
- Ala, A.; Wilder, J.; Jonassaint, N.L.; Coffin, C.S.; Brady, C.; Reynolds, A.; Schilsky, M.L. COVID-19 and the Uncovering of Health Care Disparities in the United States, United Kingdom and Canada: Call to Action. Hepatol Commun 2021, 5, 1791–1800. [CrossRef]
- Hasson, R.; Sallis, J.F.; Coleman, N.; Kaushal, N.; Nocera, V.G.; Keith, N. COVID-19: Implications for Physical Activity, Health Disparities, and Health Equity. American Journal of Lifestyle Medicine 2022, 16, 420–433. [CrossRef]
- Grant, C.; Osanloo, A. Understanding, Selecting, and Integrating a Theoretical Framework in Dissertation Research: Creating the Blueprint for Your “House.” Administrative Issues Journal: Connecting Education, Practice, and Research 2014, 4, 12–26.
- Sallis, J.F.; Owen, N. Ecological Models of Health Behavior. In Health behavior: Theory, research, and practice, 5th ed; Jossey-Bass/Wiley: Hoboken, NJ, US, 2015; pp. 43–64 ISBN 978-1-118-62898-0.
- Rhodes, R.E.; Kaushal, N.; Quinlan, A. Is Physical Activity a Part of Who I Am? A Review and Meta-Analysis of Identity, Schema and Physical Activity. Health Psychol Rev 2016, 10, 204–225. [CrossRef]
- Gardner, B.; Abraham, C.; Lally, P.; de Bruijn, G.-J. Towards Parsimony in Habit Measurement: Testing the Convergent and Predictive Validity of an Automaticity Subscale of the Self-Report Habit Index. Int J Behav Nutr Phys Act 2012, 9, 102. [CrossRef]
- Hagger, M.S.; Hamilton, K.; Phipps, D.J.; Protogerou, C.; Zhang, C.-Q.; Girelli, L.; Mallia, L.; Lucidi, F. Effects of Habit and Intention on Behavior: Meta-Analysis and Test of Key Moderators. Motivation Science 2023, 9, 73–94. [CrossRef]
- de Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millán-Calenti, J.C. Effects of Physical Exercise Interventions in Frail Older Adults: A Systematic Review of Randomized Controlled Trials. BMC Geriatr 2015, 15, 154. [CrossRef]
- Golaszewski, N.M.; Bartholomew, J.B. The Development of the Physical Activity and Social Support Scale. Journal of Sport and Exercise Psychology 2019, 41, 215–229. [CrossRef]
- Burner, E.; Lam, C.N.; Deross, R.; Kagawa-Singer, M.; Menchine, M.; Arora, S. Using Mobile Health to Improve Social Support for Low-Income Latino Patients with Diabetes: A Mixed-Methods Analysis of the Feasibility Trial of TExT-MED + FANS. Diabetes Technol. Ther. 2018, 20, 39–48. [CrossRef]
- Page-Reeves, J.; Murray-Krezan, C.; Regino, L.; Perez, J.; Bleecker, M.; Perez, D.; Wagner, B.; Tigert, S.; Bearer, E.L.; Willging, C.E. A Randomized Control Trial to Test a Peer Support Group Approach for Reducing Social Isolation and Depression among Female Mexican Immigrants. BMC Public Health 2021, 21, 119. [CrossRef]
- Dolash, K.; Meizi He; Zenong Yin; Sosa, E.T. Factors That Influence Park Use and Physical Activity in Predominantly Hispanic and Low-Income Neighborhoods. Journal of Physical Activity & Health 2015, 12, 462–469. [CrossRef]
- Webber, B.J.; Whitfield, G.P.; Moore, L.V.; Stowe, E.; Omura, J.D.; Pejavara, A.; Galuska, D.A.; Fulton, J.E. Physical Activity–Friendly Policies and Community Design Features in the US, 2014 and 2021. Prev. Chronic Dis. 2023, 20, 220397. [CrossRef]
- Obradovich, N.; Fowler, J.H. Climate Change May Alter Human Physical Activity Patterns. Nat Hum Behav 2017, 1, 0097. [CrossRef]
- Smart Growth America; National Complete Streets Coalition What Are Complete Streets? Available online: https://smartgrowthamerica.org/what-are-complete-streets/ (accessed on 7 November 2022).
- Chriqui, J.F.; Leider, J.; Thrun, E.; Nicholson, L.M.; Slater, S. Communities on the Move: Pedestrian-Oriented Zoning as a Facilitator of Adult Active Travel to Work in the United States. Front Public Health 2016, 4, 71. [CrossRef]
- Seo, B.; Nan, H.; Monahan, P.O.; Duszynski, T.J.; Thompson, W.R.; Zollinger, T.W.; Han, J. Association between Built Environment Policy and Good Health Status. Translational Journal of the American College of Sports Medicine 2024, 9, e000255. [CrossRef]
- Arena, R.; Pronk, N.P.; Woodard, C. The Influence of Social Vulnerability and Culture on Physical Inactivity in the United States – Identifying Hot Spots in Need of Attention. The American Journal of Medicine 2023, 0. [CrossRef]
- Creswell, J.W. Educational Research: Planning, Conducting, and Evaluating Quantitative and Qualitative Research; Fifth edition.; Pearson: Boston, 2015; ISBN 978-0-13-354958-4.
- Tashakkori, A.; Teddlie, C. Sage Handbook of Mixed Methods in Social and Behavioral Research; The Sage handbook of; Sage: Los Angeles, 2010; ISBN 978-1-4129-7266-6.
- Levitt, H.M.; Bamberg, M.; Creswell, J.W.; Frost, D.M.; Josselson, R.; Suárez-Orozco, C. Journal Article Reporting Standards for Qualitative Primary, Qualitative Meta-Analytic, and Mixed Methods Research in Psychology: The APA Publications and Communications Board Task Force Report. American Psychologist 2018, 73, 26–46. [CrossRef]
- Hagströmer, M.; Oja, P.; Sjöström, M. The International Physical Activity Questionnaire (IPAQ): A Study of Concurrent and Construct Validity. Public Health Nutr 2005, 9, 755–762. [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Medicine & Science in Sports & Exercise 2003, 35, 1381–1395. [CrossRef]
- Davis, T.P. Barrier Analysis Facilitator’s Guide: A Tool for Improving Behavior Change Communication in Child Survival and Community Development Programs; Food for the Hungry: Washington DC, 2004;
- Kittle, B. A Practical Guide to Conducting a Barrier Analysis; Helen Keller International: New York, NY, 2017; Vol. 2;
- Egleston, B.L.; Miller, S.M.; Meropol, N.J. The Impact of Misclassification Due to Survey Response Fatigue on Estimation and Identifiability of Treatment Effects. Stat Med 2011, 30, 3560–3572. [CrossRef]
- Krosnick, J.A.; Alwin, D.F. An Evaluation of a Cognitive Theory of Response-Order Effects in Survey Measurement. Public Opinion Quarterly 1987, 51, 201–219. [CrossRef]
- Ibrahim, S.; Karim, N.A.; Oon, N.L.; Ngah, W.Z.W. Perceived Physical Activity Barriers Related to Body Weight Status and Sociodemographic Factors among Malaysian Men in Klang Valley. BMC Public Health 2013, 13, 275. [CrossRef]
- Anderson, D.; Cychosz, C.M. Development of an Exercise Identity Scale. Percept Mot Skills 1994, 78, 747–751. [CrossRef]
- Wilson, P.M.; Muon, S. Psychometric Properties of the Exercise Identity Scale in a University Sample. International Journal of Sport and Exercise Psychology 2008, 6, 115–131. [CrossRef]
- Kaushal, N.; Rhodes, R.E.; Meldrum, J.T.; Spence, J.C. The Role of Habit in Different Phases of Exercise. British J Health Psychol 2017, 22, 429–448. [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behavior Research Methods 2007, 39, 175–191. [CrossRef]
- Cohen, J. A Power Primer. Psychological Bulletin 1992, 112, 155–159. [CrossRef]
- Ferguson, C.J. An Effect Size Primer: A Guide for Clinicians and Researchers. Professional Psychology: Research and Practice 2009, 40, 532–538. [CrossRef]
- Schafer, J.L.; Graham, J.W. Missing Data: Our View of the State of the Art. Psychological Methods 2002, 7, 147–177. [CrossRef]
- Jakobsen, J.C.; Gluud, C.; Wetterslev, J.; Winkel, P. When and How Should Multiple Imputation Be Used for Handling Missing Data in Randomised Clinical Trials – A Practical Guide with Flowcharts. BMC Med Res Methodol 2017, 17, 162. [CrossRef]
- Manly, C.A.; Wells, R.S. Reporting the Use of Multiple Imputation for Missing Data in Higher Education Research. Res High Educ 2015, 56, 397–409. [CrossRef]
- Kiger, M.E.; Varpio, L. Thematic Analysis of Qualitative Data: AMEE Guide No. 131. Medical Teacher 2020, 42, 846–854. [CrossRef]
- Smith, B.; McGannon, K.R. Developing Rigor in Qualitative Research: Problems and Opportunities within Sport and Exercise Psychology. International Review of Sport and Exercise Psychology 2018, 11, 101–121. [CrossRef]
- McGannon, K.R.; Smith, B.; Kendellen, K.; Gonsalves, C.A. Qualitative Research in Six Sport and Exercise Psychology Journals between 2010 and 2017: An Updated and Expanded Review of Trends and Interpretations. International Journal of Sport and Exercise Psychology 2021, 19, 359–379. [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups. International Journal for Quality in Health Care 2007, 19, 349–357. [CrossRef]
- Wanner, M.; Probst-Hensch, N.; Kriemler, S.; Meier, F.; Autenrieth, C.; Martin, B.W. Validation of the Long International Physical Activity Questionnaire: Influence of Age and Language Region. Prev Med Rep 2016, 3, 250–256. [CrossRef]
- Quinn, T.D.; Barone Gibbs, B. Context Matters: The Importance of Physical Activity Domains for Public Health. Journal for the Measurement of Physical Behaviour 2023, 6, 245–249. [CrossRef]
- Whitfield, G.P.; Ussery, E.N.; Saint-Maurice, P.F.; Carlson, S.A. Trends in Aerobic Physical Activity Participation across Multiple Domains among US Adults, National Health and Nutrition Examination Survey 2007/2008 to 2017/2018. Journal of Physical Activity and Health 2021, 18, S64–S73. [CrossRef]
- Cohen, S.; Matthews, C.E.; Signorello, L.B.; Schlundt, D.G.; Blot, W.J.; Buchowski, M.S. Sedentary and Physically Active Behavior Patterns among Low-Income African-American and White Adults Living in the Southeastern United States. PLoS ONE 2013, 8, e59975. [CrossRef]
- Marquez, D.X.; Neighbors, C.J.; Bustamante, E.E. Leisure Time and Occupational Physical Activity among Racial or Ethnic Minorities. Medicine and Science in Sports and Exercise 2009, 42, 1086–1093. [CrossRef]
- Holtermann, A.; Krause, N.; Van Der Beek, A.J.; Straker, L. The Physical Activity Paradox: Six Reasons Why Occupational Physical Activity (OPA) Does Not Confer the Cardiovascular Health Benefits That Leisure Time Physical Activity Does. Br J Sports Med 2018, 52, 149–150. [CrossRef]
- Li, J.; Loerbroks, A.; Angerer, P. Physical Activity and Risk of Cardiovascular Disease: What Does the New Epidemiological Evidence Show? Current Opinion in Cardiology 2013, 28, 575–583. [CrossRef]
- Cillekens, B.; Huysmans, M.A.; Holtermann, A.; van Mechelen, W.; Straker, L.; Krause, N.; van der Beek, A.J.; Coenen, P. Physical Activity at Work May Not Be Health Enhancing. A Systematic Review with Meta-Analysis on the Association between Occupational Physical Activity and Cardiovascular Disease Mortality. Scandinavian Journal of Work, Environment & Health 2022, 48, 86–98. [CrossRef]
- Nakayama, J.Y.; Van Dyke, M.E.; Quinn, T.D.; Whitfield, G.P. Association between Leisure-Time Physical Activity and Occupation Activity Level, National Health Interview Survey—United States, 2020. Journal of Physical Activity and Health 2024, 21, 375–383. [CrossRef]
- Quinn, T.D.; Lane, A.; Pettee Gabriel, K.; Sternfeld, B.; Jacobs, D.R.; Smith, P.; Barone Gibbs, B. Thirteen-Year Associations of Occupational and Leisure-Time Physical Activity with Cardiorespiratory Fitness in CARDIA. Medicine & Science in Sports & Exercise 2023, 55, 2025–2034. [CrossRef]
- Quinn, T.D.; Lane, A.; Pettee Gabriel, K.; Sternfeld, B.; Jacobs, D.R.; Smith, P.; Barone Gibbs, B. Associations between Occupational Physical Activity and Left Ventricular Structure and Function over 25 Years in CARDIA. European Journal of Preventive Cardiology 2024, 31, 425–433. [CrossRef]
- U.S. Bureau of Labor Statistics Labor Force Characteristics by Race and Ethnicity, 2022; United States Department of Labor: Washington DC, 2023;
- Abildso, C.G.; Daily, S.M.; Meyer, M.R.U.; Perry, C.K.; Eyler, A. Prevalence of Meeting Aerobic, Muscle-Strengthening, and Combined Physical Activity Guidelines during Leisure Time among Adults, by Rural-Urban Classification and Region — United States, 2020. MMWR Morb Mortal Wkly Rep 2023, 72, 5. [CrossRef]
- Stevens, C.J.; Baldwin, A.S.; Bryan, A.D.; Conner, M.; Rhodes, R.E.; Williams, D.M. Affective Determinants of Physical Activity: A Conceptual Framework and Narrative Review. Front Psychol 2020, 11, 568331. [CrossRef]
- Ekkekakis, P. The Measurement of Affect, Mood, and Emotion: A Guide for Health-Behavioral Research; Cambridge University Press: Cambridge, UK ; New York, 2013; ISBN 978-1-107-01100-7.
- Ekkekakis, P.; Brand, R. Affective Responses to and Automatic Affective Valuations of Physical Activity: Fifty Years of Progress on the Seminal Question in Exercise Psychology. Psychology of Sport and Exercise 2019, 42, 130–137. [CrossRef]
- Feil, K.; Allion, S.; Weyland, S.; Jekauc, D. A Systematic Review Examining the Relationship between Habit and Physical Activity Behavior in Longitudinal Studies. Front Psychol 2021, 12, 626750. [CrossRef]
- Kaushal, N.; Rhodes, R.E.; Spence, J.C.; Meldrum, J.T. Increasing Physical Activity through Principles of Habit Formation in New Gym Members: A Randomized Controlled Trial. Ann Behav Med 2017, 51, 578–586. [CrossRef]
- Kaushal, N.; Rhodes, R.E. Exercise Habit Formation in New Gym Members: A Longitudinal Study. J Behav Med 2015, 38, 652–663. [CrossRef]
- Sebastião, E.; Chodzko-Zajko, W.; Schwingel, A. An In-Depth Examination of Perceptions of Physical Activity in Regularly Active and Insufficiently Active Older African American Women: A Participatory Approach. PLoS One 2015, 10, e0142703. [CrossRef]
- Cairney, J.; Dudley, D.; Kwan, M.; Bulten, R.; Kriellaars, D. Physical Literacy, Physical Activity and Health: Toward an Evidence-Informed Conceptual Model. Sports Med 2019, 49, 371–383. [CrossRef]
- Taber, D.R.; Chriqui, J.F.; Perna, F.M.; Powell, L.M.; Slater, S.J.; Chaloupka, F.J. Association between State Physical Education (PE) Requirements and PE Participation, Physical Activity, and Body Mass Index Change. Prev Med 2013, 57, 629–633. [CrossRef]
- Healy, S.; Patterson, F.; Biddle, S.; Dumuid, D.; Glorieux, I.; Olds, T.; Woods, C.; Bauman, A.E.; Gába, A.; Herring, M.P.; et al. It’s about Time to Exercise: Development of the Exercise Participation Explained in Relation to Time (EXPERT) Model. Br J Sports Med 2024, bjsports-2024-108500. [CrossRef]
- Han, W.-J. How Our Longitudinal Employment Patterns Might Shape Our Health as We Approach Middle Adulthood—US NLSY79 Cohort. PLOS ONE 2024, 19, e0300245. [CrossRef]
- Hagger, M.S.; Luszczynska, A. Implementation Intention and Action Planning Interventions in Health Contexts: State of the Research and Proposals for the Way Forward. Appl Psychol Health Well Being 2014, 6, 1–47. [CrossRef]
- Rebar, A.L.; Williams, R.; Short, C.E.; Plotnikoff, R.; Duncan, M.J.; Mummery, K.; Alley, S.; Schoeppe, S.; To, Q.; Vandelanotte, C. The Impact of Action Plans on Habit and Intention Strength for Physical Activity in a Web-Based Intervention: Is It the Thought That Counts? Psychology & Health 2023, 0, 1–21. [CrossRef]
- Ahmadi, M.N.; Hamer, M.; Gill, J.M.R.; Murphy, M.; Sanders, J.P.; Doherty, A.; Stamatakis, E. Brief Bouts of Device-Measured Intermittent Lifestyle Physical Activity and Its Association with Major Adverse Cardiovascular Events and Mortality in People Who Do Not Exercise: A Prospective Cohort Study. The Lancet Public Health 2023, 8, e800–e810. [CrossRef]
- Deslippe, A.L.; Soanes, A.; Bouchaud, C.C.; Beckenstein, H.; Slim, M.; Plourde, H.; Cohen, T.R. Barriers and Facilitators to Diet, Physical Activity and Lifestyle Behavior Intervention Adherence: A Qualitative Systematic Review of the Literature. Int J Behav Nutr Phys Act 2023, 20, 14. [CrossRef]
- Koh, Y.S.; Asharani, P.V.; Devi, F.; Roystonn, K.; Wang, P.; Vaingankar, J.A.; Abdin, E.; Sum, C.F.; Lee, E.S.; Müller-Riemenschneider, F.; et al. A Cross-Sectional Study on the Perceived Barriers to Physical Activity and Their Associations with Domain-Specific Physical Activity and Sedentary Behaviour. BMC Public Health 2022, 22, 1051. [CrossRef]
- Pew Research Center Public’s Positive Economic Ratings Slip; Inflation Still Widely Viewed as Major Problem; Pew Research Center, 2024; pp. 1–30;
- Marcus, B.H.; Dunsiger, S.; Pekmezi, D.; Benitez, T.; Larsen, B.; Meyer, D. Physical Activity Outcomes from a Randomized Trial of a Theory- and Technology-Enhanced Intervention for Latinas: The Seamos Activas II Study. J Behav Med 2022, 45, 1–13. [CrossRef]
- Marquez, D.X.; Wilbur, J.; Hughes, S.L.; Berbaum, M.L.; Wilson, R.S.; Buchner, D.M.; McAuley, E. B.A.I.L.A. - A Latin Dance Randomized Controlled Trial for Older Spanish-Speaking Latinos: Rationale, Design, and Methods. Contemp. Clin. Trials 2014, 38, 397–408. [CrossRef]
- Buja, A.; Rabensteiner, A.; Sperotto, M.; Grotto, G.; Bertoncello, C.; Cocchio, S.; Baldovin, T.; Contu, P.; Lorini, C.; Baldo, V. Health Literacy and Physical Activity: A Systematic Review. J Phys Act Health 2020, 17, 1259–1274. [CrossRef]
- Garcia, L.; Mendonça, G.; Benedetti, T.R.B.; Borges, L.J.; Streit, I.A.; Christofoletti, M.; Silva-Júnior, F.L.E.; Papini, C.B.; Binotto, M.A. Barriers and Facilitators of Domain-Specific Physical Activity: A Systematic Review of Reviews. BMC Public Health 2022, 22, 1964. [CrossRef]
- Heredia, N.I.; Walker, T.J.; Lee, M.; Reininger, B.M. The Longitudinal Relationship between Social Support and Physical Activity in Hispanics. AM J HEALTH PROMOT 2019, 33, 921–924. [CrossRef]
- Camhi, S.M.; Debordes-Jackson, G.; Andrews, J.; Wright, J.; Lindsay, A.C.; Troped, P.J.; Hayman, L.L. Socioecological Factors Associated with an Urban Exercise Prescription Program for Under-Resourced Women: A Mixed Methods Community-Engaged Research Project. IJERPH 2021, 18, 8726. [CrossRef]
- Travert, A.-S.; Sidney Annerstedt, K.; Daivadanam, M. Built Environment and Health Behaviors: Deconstructing the Black Box of Interactions—A Review of Reviews. IJERPH 2019, 16, 1454. [CrossRef]
- Serrano, N.; Leider, J.; Chriqui, J.F. Pedestrian-Oriented Zoning Moderates the Relationship between Racialized Economic Segregation and Active Travel to Work, United States. Preventive Medicine 2023, 177, 107788. [CrossRef]
- Sallis, J.F.; Saelens, B.E. Assessment of Physical Activity by Self-Report: Status, Limitations, and Future Directions. Research Quarterly for Exercise and Sport 2000, 71, 1–14. [CrossRef]
Figure 1.
Participant Study Flow Diagram. Forty-seven underrepresented racial minority adults ( ≥18 years) living within an urban Midwestern County were screened for eligibility; with twenty-nine participants consenting to and completing the study. Participants were recruited using various methods including social media, email newsletters, and word-of-mouth.
Figure 1.
Participant Study Flow Diagram. Forty-seven underrepresented racial minority adults ( ≥18 years) living within an urban Midwestern County were screened for eligibility; with twenty-nine participants consenting to and completing the study. Participants were recruited using various methods including social media, email newsletters, and word-of-mouth.
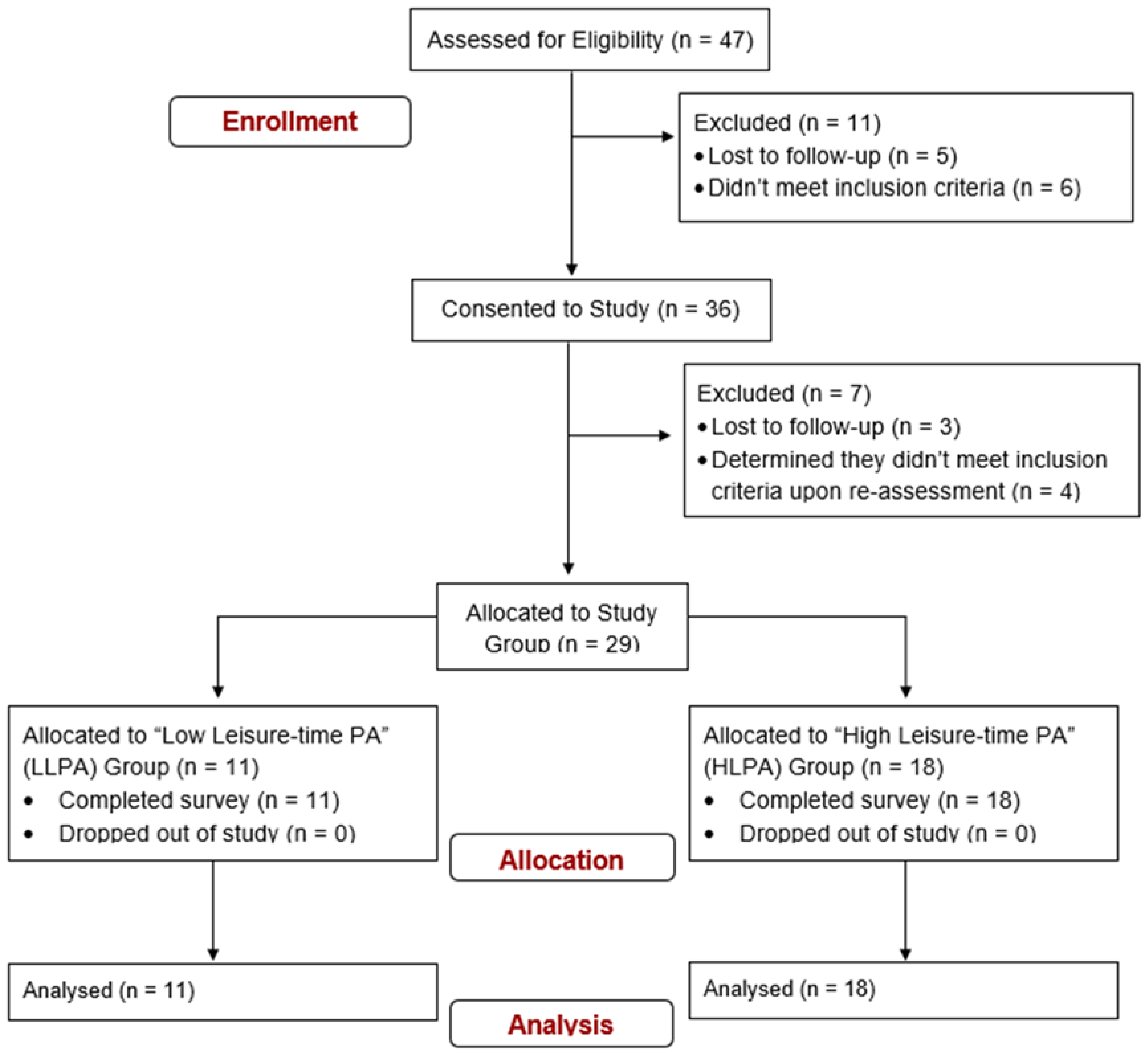

Table 1.
Participant Demographics. Twenty-nine community-dwelling underrepresented racial minority adults participated in this study. All data is self-reported. Data are reported as Mean (SD) where available.
Table 1.
Participant Demographics. Twenty-nine community-dwelling underrepresented racial minority adults participated in this study. All data is self-reported. Data are reported as Mean (SD) where available.
| Variable | LLPA | HLPA | p - value | Cohen’s d |
|---|---|---|---|---|
| Gender (n) | ||||
| Male | 1.00 | 3.00 | -- | -- |
| Female | 10.00 | 15.00 | -- | -- |
| Race/Ethnicity (%) | ||||
| Black | 63.63 | 33.33 | -- | -- |
| Hispanic/Latino | 5.55 | 33.33 | -- | -- |
| Asian | 27.27 | 27.28 | -- | -- |
| Middle Eastern | 0.00 | 5.66 | -- | -- |
| Education (% w/ Bachelors or More) | 54.45 | 72.22 | -- | -- |
| Employed Full Time (%) | 54.45 | 77.78 | -- | -- |
| Personal Income (% > $50,000/yr.) | 9.10 | 33.33 | -- | -- |
| Did Not Answer (%) | 18.18 | 16.67 | -- | -- |
| Age (yrs.) | 39.09 (18.21) | 38.44 (14.15) | 0.92 | -0.04 |
| Body Mass (kg) | 80.95 (16.13) | 73.23 (13.60) | 0.18 | -0.53 |
| Height (cm) | 165.45 (8.45) | 164.11 (7.94) | 0.67 | -0.16 |
| BMI (kg/m2) | 29.75 (6.24) | 27.32 (5.54) | 0.29 | -0.42 |
| Years in Community | 7.75 (8.81) | 10.18 (11.76) | 0.58 | 0.22 |
| Total Leisure-time PA (min/week) | 44.55 (48.40) | 448.89 (227.43) | 0.001* | 2.21 |
*p < 0.05. BMI = Body mass index. PA = Physical activity.
Table 2.
Self-Reported Domain-specific Physical Activity Outcomes and Effect Sizes. Values were computed from the International Physical Activity Questionnaire – Long Form delivered to participants as part of the study survey. All data are reported as minutes per week. Data are reported as Mean (SD).
Table 2.
Self-Reported Domain-specific Physical Activity Outcomes and Effect Sizes. Values were computed from the International Physical Activity Questionnaire – Long Form delivered to participants as part of the study survey. All data are reported as minutes per week. Data are reported as Mean (SD).
| Variable | LLPA | HLPA | p-value | Cohen’s d |
|---|---|---|---|---|
| Occupational PA | ||||
| MVPA | 169.55 (372.90) | 468.89 (903.25) | 0.31 | 0.40 |
| Walking PA | 95.45 (94.70) | 262.28 (379.35) | 0.17 | 0.54 |
| Total PA | 265.00 (412.98) | 731.17 (1062.74) | 0.18 | 0.53 |
| Transportational PA | ||||
| MVPA | 0.00 (0.00) | 10.00 (30.87) | 0.30 | 0.41 |
| Walking PA | 140.91 (178.81) | 178.56 (147.37) | 0.54 | 0.24 |
| Total PA | 140.91 (178.81) | 188.56 (164.30) | 0.47 | 0.28 |
| Household MVPA | 284.55 (327.63) | 273.78 (208.65) | 0.91 | -0.04 |
| Leisure-time PA | ||||
| Exercise MVPA | 40.00 (48.11) | 238.89 (182.78) | 0.00* | 1.34 |
| Walking PA | 4.55 (12.14) | 210.00 (143.69) | <.001* | 1.80 |
| Total PA | 44.55 (48.40) | 448.89 (227.43) | 0.001* | 2.21 |
| Summed Domain Totals | ||||
| Total MVPA | 494.09 (398.60) | 991.56 (883.55) | 0.09 | 0.67 |
| Total Walking PA | 240.91 (196.45) | 650.83 (491.01) | 0.01* | 1.01 |
| Total PA | 735.00 (521.94) | 1642.39 (1073.98) | 0.02* | 1.00 |
*p < 0.05. PA = Physical activity. MVPA = Moderate-to-vigorous physical activity.
Table 3.
Multivariate Analysis Summary Table for Survey Composite Scores. All survey data are expressed numerically. Survey questions for the PA Barrier Questionnaire, Self-Reported Behavioral Automaticity Scale, and PA Self-Efficacy Scale were delivered on a five-point Likert Scale, with 1 = strongly disagree and 5 = strongly agree. Survey questions for the PA Social Support Scale were delivered as Likert Scale items on a seven-point scale; with 1 = never true and 7 = always true.
Table 3.
Multivariate Analysis Summary Table for Survey Composite Scores. All survey data are expressed numerically. Survey questions for the PA Barrier Questionnaire, Self-Reported Behavioral Automaticity Scale, and PA Self-Efficacy Scale were delivered on a five-point Likert Scale, with 1 = strongly disagree and 5 = strongly agree. Survey questions for the PA Social Support Scale were delivered as Likert Scale items on a seven-point scale; with 1 = never true and 7 = always true.
| Composite Score | Group | Mean (SD) | dƒ | MS | F-statistic | p-value | Cohen’s d |
|---|---|---|---|---|---|---|---|
| PA Barrier Questionnaire (α = 0.92) | |||||||
| Personal | LLPA | 36.64 (12.53) | 10.00 | 556.14 | 5.72 | 0.02* | -0.92 |
| HLPA | 27.61 (7.88) | ||||||
| Social Environment | LLPA | 11.18 (3.57) | 10.00 | 34.18 | 2.758 | 0.11 | -0.64 |
| HLPA | 8.94 (3.49) | ||||||
| Physical Environment | LLPA | 12.91 (5.52) | 10.00 | 27.87 | 1.26 | 0.27 | -0.43 |
| HLPA | 10.89 (4.14) | ||||||
| Exercise Identity Scale (α = 0.89) | LLPA | 27.45 (7.90) | 10.00 | 141.07 | 2.79 | 0.11 | 0.64 |
| HLPA | 32.00 (6.61) | ||||||
| Self-Reported Behavioral Automaticity Scale (α = 0.97) | LLPA | 10.18 (5.06) | 10.00 | 72.68 | 3.19 | 0.09 | 0.68 |
| HLPA | 13.44 (4.60) | ||||||
| PA Social Support Scale (α = 0.84) | |||||||
| Emotional Support | LLPA | 15.73 (4.58) | 10.00 | 14.15 | 0.53 | 0.47 | 0.28 |
| HLPA | 17.17 (5.48) | ||||||
| Validation Support | LLPA | 11.09 (5.80) | 10.00 | 1.96 | 0.70 | 0.79 | -0.10 |
| HLPA | 10.56 (4.96) | ||||||
| Informational Support | LLPA | 13.18 (4.19) | 10.00 | 34.95 | 1.15 | 0.29 | 0.41 |
| HLPA | 15.44 (6.16) | ||||||
| Companionship Support | LLPA | 11.82 (3.71) | 10.00 | 6.62 | 0.22 | 0.64 | -0.18 |
| HLPA | 10.83 (6.32) | ||||||
| Instrumental Support | LLPA | 7.18 (6.82) | 10.00 | 231.12 | 3.79 | 0.06 | 0.75 |
| HLPA | 13.00 (8.33) | ||||||
*p < 0.05. PA = Physical activity.
Table 4.
Barriers to Physical Activity Described by Study Participants. Responses were prompted by asking participants to answer questions from the Barrier Analysis Qualitative Survey. Participants were instructed to be as thorough as possible when answering each question. Identified themes, sub-themes, and quotes are organized by socio-ecological model (SEM) domains. Quotes are shown verbatim with added clarification (denoted by brackets) to enhance readability and ease of interpretation.
Table 4.
Barriers to Physical Activity Described by Study Participants. Responses were prompted by asking participants to answer questions from the Barrier Analysis Qualitative Survey. Participants were instructed to be as thorough as possible when answering each question. Identified themes, sub-themes, and quotes are organized by socio-ecological model (SEM) domains. Quotes are shown verbatim with added clarification (denoted by brackets) to enhance readability and ease of interpretation.
| Group | SEM Domain | Themes & Subthemes | Quotes |
|---|---|---|---|
| LLPA | Personal | Lack of Time | "Online classes [take up too much time]" |
| "Work schedule [takes up too much time]" | |||
| "[Physical activity] takes time away from work, causing me to give up sleep, take an unpaid lunch break, and/or work longer hours" | |||
| "Balancing full time work and part time school [makes it hard to be active]" | |||
| Physical Capacity | "[I have] low energy, lack of high workload," | ||
| Lack of Motivation | "Lack of motivation to be physically active [makes it difficult to be active]." | ||
| "Takes a lot of time to see the results. [I] need to be motivated internally to go out and be active." | |||
| Physical Sensations Associated w/ PA | "Body pains after the exercise [make it difficult to be active]" | ||
| "Weightlifting and other vigorous activity creates soreness." | |||
| "Sweating [makes activity difficult]" | |||
| "Taking extra showers that can sometimes lead to dryer skin" | |||
| Self-Doubt | "[I discourage] myself [from being active]" | ||
| Cost Assoc. w/ PA | *Prevalent Sub-Theme in Community domain themes | ||
| Stress | "[I] worry about day to day stuff [like] bills" | ||
| Risk of Injury | "Injuries can occur when active if not careful." | ||
| Interpersonal | Missing Out on Social Events | "[Physical activity] can become one of the reasons to skip some social events." | |
| Community | Inclement Weather | "Not having any reason to go outside of my home. Bad weather like snowing/raining/strong winds." | |
| "Some days, the weather doesn't allow for me to get outside and enjoy walking or driving to the local YMCA for group exercise." | |||
| Group | SEM Domain | Themes & Subthemes | Quotes |
| LLPA | Community | Lack of PA Facilities, Public Transit in Community | "[Not having] easy access to public transport [makes it harder to be active]." |
| HLPA |
Personal |
Lack of Time | "School… discourages me from being active as [physical activity] takes up too much time in my schedule." |
| "Family obligations, work obligations, and lack of time [make it hard to be active]" | |||
| "When I miss a day. When I don't get enough sleep. When I go out of town." | |||
| "Finding time. I have two jobs that take up every single day all day." | |||
| "Making time to do it and giving up other things that may be important [is a drawback of being active]" | |||
| Lack of Time | "Work schedules and requirements that limit your time or drain you physically [discourage me from being active]" | ||
| Lack of Motivation | "[Physical activity is] not easy, because it’s hard to get motivated" | ||
| "I don’t have the energy or the motivation [to be active]" | |||
| "Lack of motivation, lack of energy and lack of knowledge [makes it hard to be active]" | |||
| Pregnancy | "Being pregnant [makes it hard to be active], as time goes on once baby is here will be finding daycare" | ||
| "My mother [doesn’t support me being active] due to being almost 7 months [pregnant]" | |||
| Risk of Injury | "Possible risk for injury if you don't know what you're doing or don't have the correct form or stretch routine [is a drawback of being active]" | ||
| "Aches and injuries [are drawbacks to being active]" | |||
| "If you do not have proper training, you can do an exercise or lift a weight incorrectly causing harm to your body." | |||
| Physical Sensations Associated with PA | "{Being active] gets tiring and sometimes overwhelming" | ||
| "Feeling lethargic, reduced mental clarity, and sore all the time [is a drawback of being active]" | |||
| Cost Assoc. w/ PA | "Programs that are expensive and not local [discourage me from being active]" | ||
| "Expensive gym memberships [discourage me from being active]" | |||
| "It's expensive [to be active]" | |||
| Lack of Knowledge About PA | "[My] lack of knowledge on what [to] do in gym [discourages me from being active]" | ||
| Interpersonal | Lack of Social Support | "Being active alone [discourages me from being active]" | |
| Group | SEM Domain | Themes & Subthemes | Quotes |
| HLPA | Community | Lack of PA Facilities, Public Transit in Community | "{Not having] a convenient gym [makes it hard to be active]" |
| "Distance and transportation [to facilities discourage me from being active]" | |||
| Societal | Social Norms Around Pregnancy | "Pregnant women shouldn’t be active" | |
| Cultural Norms Around Autonomy and/or Independence | "A cultural belief that is often shared by people in my religion is that parents are always in control of their children, no matter what their age is. They can somewhat discourage me being active if they say that we have to do something on the day that I would like to be active." |
Table 5.
Facilitators to Physical Activity Described by Study Participants. Responses were prompted by asking participants to answer questions from the Barrier Analysis Qualitative Survey. Participants were instructed to be as thorough as possible when answering each question. Identified themes, sub-themes, and quotes are organized by socio-ecological model (SEM) domains. Quotes are shown verbatim with added clarification (denoted by brackets) to enhance readability and ease of interpretation.
Table 5.
Facilitators to Physical Activity Described by Study Participants. Responses were prompted by asking participants to answer questions from the Barrier Analysis Qualitative Survey. Participants were instructed to be as thorough as possible when answering each question. Identified themes, sub-themes, and quotes are organized by socio-ecological model (SEM) domains. Quotes are shown verbatim with added clarification (denoted by brackets) to enhance readability and ease of interpretation.
| Group | SEM Domain | Themes & Subthemes | Quotes | |
|---|---|---|---|---|
| LLPA | Personal | Knowledge of PA Benefits | "The activities that is done to stay fit and it is very important in one’s health" | |
| "It keeps the body functions in better condition." | ||||
| "It improves both mental and physical health including decreasing anxiety and depression, reducing conditions heart conditions, improve blood sugar levels, and improve cognitive and mental function." | ||||
| "Physical activity leads to good cardiac [health] and joint mobility." | ||||
| "It is like the elixir " | ||||
| Obtaining Health Benefits Sub-Themes: Physical Health, Mental Health, Emotional Health |
"[Being active] helps one stay fit" "Being physically active helps me stay mentally fit as well. Helps me feel good about myself. If I workout in the morning, I tend to make better eating decisions as I am aware of all the hard work I have done in the morning." |
|||
| Group | SEM Domain | Themes & Subthemes | Quotes | |
| Personal | Obtaining Health Benefits Sub-Themes: Physical Health, Mental Health, Emotional Health |
"I sleep better and keep a healthy weight" | ||
| "Better bone and muscle health. You don’t seem to age." | ||||
| "Mental health benefits, more energy, increased confidence [are benefits of being active]" | ||||
| "It helps with sleep, mood, concentration, and balancing mental health struggles" | ||||
| Beliefs About the Body's Value | "The fact that my body is my home, my safe space and I want to take care of it [encourages me to be active]." | |||
| Goal Setting | "Hav[ing] a goal [helps me be more active]" | |||
| Interpersonal | Social Accountability | "I [am encouraged to be active because I] have a service dog who needs to go on walks at least 2x/day" | ||
| "[Having a] group of people committed to exercising [encourages me to be active]" | ||||
| Social Support | "Having a gym buddy [helps me stay active]." | |||
| "My community consists of active older adults who are generally very physically active." | ||||
| "My husband, my mother [support me to be active]" | ||||
| "My parents (specifically my dad) and some of my friends who are also physically active [support me]" | ||||
| LLPA | Fostering Social Relationships | "Being active allows for social interactions with people in and around the gyms, pool, pickleball court." | ||
| Community PA Facility Availability | "[Having the] gym being open 24 hours [help me be active]." | |||
| "This summer I have a student rec membership, so I have access on the days I'm at campus." | ||||
| "Inexpensive gyms within short walking distance of my job. Gym showers… The proximity of the canal." | ||||
| "Regular cricket games in softball field. Having some table tennis tournaments." | ||||
| Community | PA Community Events or Programs Sub-Theme: Cost of PA |
"Regular cricket games in softball field. Having some table tennis tournaments." | ||
| "More sports tournaments/events. Having sport groups like TT group etc. Starting some learning sessions" | ||||
| "Free community offered classes, and physical events (yoga, dance, walking/running,). A community gym offered at a free and or very reduced rate." | ||||
| "Silver Sneakers and YMCA Fitness Centers [help me be active]" | ||||
| Supportive Environments for PA | "Gym, less busy roads for walks, closer outlets [would help me be active]" | |||
| "Free access to gym/ recreational activities and resources for beginners [would help me be active]" | ||||
| "Having access to [a] swimming pool, gymnasium, walking parks, bicycle paths" | ||||
| Group | SEM Domain | Themes & Subthemes | Quotes | |
| LLPA | Community | Age Appropriate PA Opportunities | "More resources for my age group [would help me be active]" | |
| Societal | Policies that Support and/ or Subsize PA (work, school, etc.) | "[Having access to] work sponsored programs. Canal sponsored programs [would help me be active]." | ||
| HLPA | Personal | Having a Goal and Routine | "I now have a routine. I do it in the morning before the day begins. I feel better when I exercise and sluggish when I don't." | |
| Enjoyment of PA | "[Physical activity is] something that genuinely makes me happy allowing me to enjoy it." | |||
| "Remembering the benefits of being physically active [helps me be active]" | ||||
| Knowledge of PA Benefits | "Sitting is the new smoking. In other words, you need to keep moving to stay healthy." | |||
| "I know that, for starters, physical activity doesn't just play a role in physical health. It also plays a part in a person's mental health." | ||||
| "Physical activity is good for strengthening your heart and body." | ||||
| "[I am] fairly knowledgeable [about the benefits of physical activity]. The more active you are, the better health you'll have" | ||||
| "If you don't use it, you will lose it. Staying active activates the happy hormone and relieves stress; it produces clarity of the mind, walking outside provides access to attaining vitamin D naturally and walking in nature produces some peace and grounding. Weightlifting helps combat bone loss and osteoporosis. Physical activity is providing a holistic measure for producing good health, mind, body, and spirit; good health is wealth." | ||||
| Resiliency | "I really do not care about what others think of me, but most people who knows me knows that I have always been pretty active: family, friends, colleagues." | |||
| Obtaining Health Benefits Sub-Themes: Physical Health, Mental Health, Emotional Health Positive Emotional Health |
"I notice the difference in my sleep, endurance, attitude, have more energy, helps with weight loss, healthy bones, mental stamina, bowel movements." “Emotional and physical wellbeing [is improved with activity]" "Clear mind, good attitude, and decrease in depression [are benefits of being active]" "Better mental health, better mood, more energy and increases productivity." "Improved sleep, mood, blood pressure and other health vitals. Decrease in obesity [are benefits]." "[Having lower] blood glucose level and [better] cardiovascular health" |
|||
| "Overall health would improve and physical appearance as well" | ||||
| Group | SEM Domain | Themes & Subthemes | Quotes | |
| HLPA | Personal | Fitness Technology | "My Apple Watch keeps me accountable." | |
| "Apple Fitness [encourages me to be active]" | ||||
| Having Resources Available to be Active | Having access to YouTube exercise videos, having a 10/month membership at planet fitness; I enjoy being active." | |||
| Interpersonal | Social Accountability | "Community or accountability partner [help me stay active]." | ||
| "Being fit impresses people that you have self-respect" | ||||
| Social Support | "I do ‘walking Wednesdays’ with colleagues." | |||
| "Pretty much everyone around me encourages me to be active." | ||||
| "I don't think I have ever run into someone that has discouraged me from being active." | ||||
| "My fiancé, kids, and best friend [support me to be active]" | ||||
| "Coworkers, roommates, parents, spouse [support me to be active]" | ||||
| "[Being active is a] way to make new friends." | ||||
| Community | Community PA Facility Availability Sub-Theme: Cost of PA |
"Having a gym at the property [makes it easier to be active]" | ||
| "I work at a gym, and I have a gym in my apartment complex." | ||||
| "Having an opportunity/space at work to work out for 30-60 minutes [would make it easier to be active]." | ||||
| "Exploring somewhere new and having a reason to leave the house" | ||||
| "More places to play tennis or pickleball [would help me be more active]" | ||||
| "Free gym memberships with a trainer [would help me be more active]" | ||||
| "Free access to gym/recreational activities and resources for beginners [would help me be more active]" | ||||
| "Free gym membership at work/on campus for staff [would help me be more active]" | ||||
| "[Having] a gym with a daycare nearby [would help me be more active]" | ||||
| PA Events or Programs | "One thing that [my employer] does is send out emails stating that there are activities taking place and other things like that. All these activities can help a person be more active." | |||
| "[My workplace wellness] program [encourage me to be active]" | ||||
| "Health and wellness promotion at [my job encourages me to be active]" | ||||
| "More diverse classes that are affordable [and] closer to home [would help me be more active]" | ||||
| "Being a [wellness program] ambassador [encourages me to be active]" | ||||
| Group | SEM Domain | Themes & Subthemes | Quotes | |
| HLPA | Community | Supportive Built Environments | "Where I work is conducive for walking and I do ‘walking Wednesdays’ with colleagues." | |
| "I am fortunate to have sidewalks, and an inexpensive health club 5 minutes away." | ||||
| "[Having facilities] close to my house, better sidewalks [would help me be more active]" | ||||
|
Societal |
Policies that Support and/or Subsize PA (i.e., work, school, etc.) | "More work from home ability [would help me be more active]" | ||
| "Decrease in insurance costs [encourage me to be active]" | ||||
| "I have Medicaid and they recently gave me a 6 month gym membership and a fitness tracker, so that’s a bit of encouragement" | ||||
| "Something with employment, money back for being active [would encourage me to be active]" | ||||
| Religious Beliefs Around the Body, Health |
"In my religion, physical and mental health is emphasized and is stated that they are both incredibly important to a person. All of these things help me be more active." | |||
| "Take care of your body, your body is your temple" | ||||
| "Body positivity movement and the Bible says our bodies are temples for the Holy Spirit and that we should take care of them. 1 Corinthians 6:19-20 Also, the Daniel fast from the book of Daniel encourages healthy eating." | ||||
| Knowledge of Racially Prevalent Health Conditions | "History of African Americans with high blood pressure and diabetes [encourages me to be active]" | |||
| "I don’t want to end up with high blood pressure or diabetes" | ||||
| Cultural PA Norms | "Grew up with hard work and physical labor being a part of my life" | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



