Submitted:
05 September 2024
Posted:
06 September 2024
You are already at the latest version
Abstract
Background/Objectives: Intervertebral disc degeneration is the most common cause of low back pain (LBP) and lumbosciatica is a major challenge to healthcare systems worldwide. ''For years, ozone therapy has been used with excellent results in intervertebral disc disease and in patients with LBP, thanks to its anti-inflammatory and pain-relieving action.'' At the other side, the repair effect fulfilled by porcine collagen, is a novelty to approach this pathology. In vitro studies have demonstrated the positive action of porcine collagen in extracellular matrix remodeling and homeostasis These tissue changes, associated with LBP, may suggest an indication for combined ozone/collagen treatment in patients with LBP. However, no studies have been reported regarding this combination of treatments. Methods: The present work compared two treatment groups (each of 10 LBP patients): A) Oxygen-Ozone Therapy (OOT) vs. B) OOT plus porcine collagen type 1 injections (COL I). Pain intensity and physiological function were assessed by the numerical rating scale (NSR) method. The Roland-Morrison questionnaire was used to assess disability. Patient data were acquired before, during and at six months of follow-up. Significant differences were assessed by ANOVA and T-Student test. Results: The analyses revealed significant statistical differences comparing the two arms, where, the OOT COL I treatment demonstrated a booster efficacy in pain, while the questionnaire revealed a reduction in disability. Conclusions:. The combination of these two therapies could be effective for the management of LBP. However no studies have been reported in literature regarding this therapeutic combination.
Keywords:
Low back pain (LBP)
; oxygen-ozone therapy (OOT)
; Porcine collagen type 1
; porcine collagen injection
; LBP clinical management: combination therapy
; Numerical Classification Scale (NRS)
; Roland Morris Questionnaire (RMD-Q)
1. Introduction
Low back pain (LBP) is a common disorder with a significant impact on patients in real life and their clinical behaviors, however, it represents a major impact within the socioeconomic community and healthcare facilities [1]. The prevalence of this disease is estimated to be between 22% and 65% per year and can reach up to 80% of the population, where LBP disease can have mild to severe manifestations. In about 60-80% of cases, no specific cause is diagnosed and the perceived pain is attributed to muscle or ligament tensions and only in 5-15% the causes of pain are associated with degenerative phenomena and disc injuries [1]. A herniated disc with symptoms is a degenerative disease of the intervertebral disc, which can present with low back pain, lumbosciatica or lumbocruralgia due to root compression. It causes pain, joint limitation of the lumbosacral tract and reduced autonomy in daily life [2]. However, lumbar disc herniation (LDH) is also frequently detected in asymptomatic individuals who undergo further diagnostic tests for other medical disorders and its prevalence is estimated at 57% [3]. LDH is therefore a common condition that, when symptomatic, has a prognosis that is not always favorable with a tendency to chronicity. [4]. Therefore, a considerable effort has been made to identify the most effective way to combat this condition in order to support and improve patients' conditions [5,6]. Recent guidelines suggest a different technical approach in order to combat, treat and cure LBP disease [7]. The American Society of Pain and Neuroscience (ASPN) has indicated several procedures and/or treatments including: anti-inflammatory therapy [8], ozone treatment [9,10,11], minimally invasive procedures [12,13], regenerative drugs [7,14,15,16] and surgery [17,18] . However, one treatment that has proven to be very effective in treating this condition has been ozone treatment. The effectiveness of oxygen-ozone therapy in medicine is now well defined and demonstrated in various fields, such as vascular diseases, orthopedics and dentistry [10]. The rationale for the use of oxygen-ozone infiltrative therapy (OOT) in the treatment of low back pain due to disc disease is based on the combination of the anti-inflammatory action with the action of accelerating the process of dehydration of the cartilage tissue of the disc. In particular, ozone oxidizes water-rich mucopolysaccharides resulting in dehydration of the protruding or herniated material [19]. The anti-inflammatory action is instead related to the oxidative capacity of the carbon-carbon double bond of arachidonic acid with a consequent reduction in the production of prostaglandins [20]. At the same time, the reactivation of the microcirculation facilitates the elimination of pro-inflammatory mediators [21].
In non-pathological discs, nerve afferents are limited to the outer third of the disc and are not found in the inner ring or the nucleus pulposus region [22]. In contrast, in pathological discs, nociceptive nerve fibers along with vascular segments may migrate into the central regions of the disc [23]. It is hypothesized that neurotransmitters along with changes within the extracellular matrix (ECM) itself and the presence of cytokines act on the nervous part of the disc. In addition, pain-related peptides and proinflammatory cytokines increase at this stage [22,23].
This explains the role of disc structures in low back pain and why in patients suffering from chronic low back pain, the fibers of the connective tissue have a different orientation than in a healthy subject. This is evident in the study of. Langevin et al; [24] in which ultrasound comparison between perimuscular connective tissue of the lumbar region in a group of subjects without low back pain and a group of subjects with chronic or recurrent low back pain for more than 12 months) demonstrating that the group with chronic low back pain had a perimuscular thickness 25% greater than normal subjects. The connective tissue of subjects with chronic low back pain appears disorganized, remodeled with infiltrations of adipose tissue and signs of fibrosis [25]. It is not yet possible to establish whether the observed tissue changes are the cause or consequence of chronic low back pain, but it is possible to provide the necessary substrate for favorable modernization. Tenocytes are specialized fibroblasts within the connective tissue, responsible remodeling of the extracellular matrix (ECM) influencing type I collagen turnover mechanisms (COL-I), the main component of the ECM [26,27]. The tendons are placed between the muscles and the bones and transfer the forces generated by muscle contraction to the skeleton [28]. In fact, porcine collagen type 1 is able to stimulate the contraction of fibroblasts that generate and exert forces on the ECM through the contraction itself. An optimal level of contractile capacity of fibroblasts is necessary to increase tensile strength and facilitate repair phenomena. Tropocollagen (consisting of three alpha helices) is the basic functional unit of mature collagen and represents the substrate necessary for the regeneration of collagen fibers. In fact, two different recently published studies have demonstrated the effectiveness of porcine collagen type 1 (COL I) supplementation in both synthesis and migration [29] and regeneration of collagen structure in connective tissues [30]. Nonetheless, the efficay and tolerability of porcine collagene type I was assesed previously [31,32]. To our knowledge, there are no studies on LBP patients treated simultaneously with OOT and COL I, to date. Indeed, In this study it was compared the OOT treatment in front of the combined action of OOT+COL I in patients affected by LBP and lumbosciatica, evaluating the improvement of pain, funcional statement and the level of disibality
2. Materials and Methods
The study was conducted from 2022, September to 2023, November. Fifty-seven consecutive patients affected by LBP or lumbosciatica, were screened in our institution. Using the formula for sample size evaluation (Power study: 85% and Adverse event: 10%), we obtained the N value (number of subject) equal to 18. Indeed, a total 20 patients out of 57 (35.08%; 10 males and 10 females) were enrolled in order to receive treatments, (mean 58 years; CI 38:79). The remaining 37 patients had at the least one of exclusion criteria.
The exclusion criteria included: acute radicular signs in the lower extremities; oncological pathologies in the active phase and/or under investigation, cognitive impairment and patients reluctant to give informed consent.
Inclusion Criteria: Lumbosacral MRI with evidence of herniated disc or multiple disc protrusions, persistent low back pain for at least six months, NSAID and painkiller therapy discontinued for at least two weeks, cortisone therapy discontinued for at least two months. Patients suffering from low back pain (value of numerical rating scale>4.0) for more than six months who underwent MRI of the lumbosacral spine and evidence of disc disease were included in the study. Patients were divided into two equal groups: group A and group B. Each treatment arm (A and B) comprised 5 males and 5 females. Patients with LBP and lumbosciatica were 5vs5 and 4vs6 in group A and B, respectively (Table 1).
All patients (A and B) were treated with intramuscular paravertebral injections of O2O3 (concentration equal to 10 ug/ml; OOT treatment). The total volume administered corresponds to 20 ml divided into four injection sites (5 ml per injection site), through the 32G needle (size: 0.7 mm x 32 mm). All patients underwent treatment twice a week for a total of 8 consecutive infiltrative treatments (one month). Patients included in group B additionally received intramuscular administration of a vial containing 2 ml of Porcine Collagen type 1 (MD-LUMBAR, Guna, Milan, Italy; COL I) divided into 4 injection site (0.5 ml per injection site), through a 27G needle (size: 0.4x 19mm).
Collagen injection was performed after 20 minutes of lumbar administration of O2O3 (Figure 1). In order to select the injection point, the physicians evaluated the interest point by MRI image evaluation. The injection point of patient was evaluated through palpation to locate the boundary space between two vertebrae (i.e. L5 and S1).
All data were acquired at the following time points: T0 (patient enrollment), T1 (after one month of treatment), at T2 (end of treatment), and T3 (six months after treatment). The level of pain in LBP patients were obtained through a numerical rating scale (NRS; range 0-10; 0= no pain and 10= full pain). In order to assess treatment-associated outcomes, the Roland Morris Disability Questionnaire (RMD-Q) was used. .The level of disability was established through the responses received by 24 different questions. A binomial evaluation (0/1; 0=ability; 1=inability) was possible for each. The total score of the questionnaire was obtained by summing the points attributed by the patients. The total result can range from 0 (equals no disability), from 24 (equals haevy inability). In fact, the reduction in the total score of RMD-Q means an improvement in physiological function. The reduction in NRS score was interpreted as a positive outcome after treatment. The delta viarition of NRS were obtained by comparing the follow-up points (T1, T2, T3) with respect to the T0 point (starting point).
Functional improvement was also assessed. Forward flexion and lateral flexion (right and left) were quantified in cm, measuring the distance from the fingertips to the ground, at the moment of maximum flexion uttered by the patient. The analyses were performed via the GraphPAD software (California, US), using both ANOVA and Student's Test. Statistically significant values were considered when p-values were <0.05.
3. Results
3.1. NRS Analysis
All patients were assessed with the NRS scale at time T0 before starting treatment. The mean pre-treatment NRS score was 6.5± 1.95 and 6.8± 1.53 for group A and group B, respectively. No statistical differences were observed between the two groups at the beginning of the protocols (Figure 2A). Similarly, the positive reduction in NRS was observed in two groups (Figure 2B and Figure 2C), where the mean values were 3.9± 2.55 and 3.8± 2.50 for group A and group B, respectively. At these two checkpoints, we can assume that there were no statistical differences by comparing the two treatments. However, comparing the follow-up breakpoint, we observed statistical differences in terms of the mean value of NRS (Figure 2B, p<0.001) and their delta change of cognete NRS over time (Figure 2D; p<0.001). In particular, after the treatment, we obtained a reduction of 5.2 points in the NRS scale (average value) in the OOT+COL I treatment instead of 3.6 points (NRS scale) in the OOT treatment alone. However, the percentage difference in reduction was 55.385% and 76.471% in group A and B, respectively. A total of 21% was present between the two treatment arms (Figure 2D). As a final concept, we carefully observed the delta NRS difference between the two treatment groups at point T2, where the changes in the NRS value (expressed as the improvement of the delta point per month) are zero in OOT and 1.4 in OOT+COL I. In addition, at six months of follow-up the effect of the addition of COL I treatment seems to better preserve the results obtained with OOT alone (Figure 2B and Figure 2D).
3.2. Functional improvements: forward bending, lateral flexions (LF) and level disability (Roland and Morris questionnaire)
Function improvement analyses show a positive trend on OOT+COL I treatment compared to those observed in OOT treatment alone (group B). The difference observed in the forward flexion analyses reveals that the OOT+COL I treatment (group B) had the mean distance values between all three visits. In particular, we observed an antiparallel trend by comparing the two groups. The OOT arm increased its main values during the visit, while OOT+COL I treatments decreased them (p<0.0001). The result could indicate that OOT+COL I treatment seems to be more effective both in the short term and in the lung. In fact, the distribution of data could indicate that OOT+COL I treatment also maintained its effect as a booster and better maintenance, compared to OOT treatment (Figure 3A). Similarly, the OOT+COL I treatment (group B) clarified a level of superiority over the OOT treatment (Figure 3C) with regard to the disability questionnaire. So far, we would like to mention that the decrease in RMD-Q represents a successful treatment. In the red columns we can see that the level of disability decreases between visits, while the same parameter in the green columns (OOT treatment only) remains stable after the second visit (p<0.001). In fact, comparing the average value visit per visit, we observed at least 5.0 points of difference between the average values (Figure 4C). Looking for lateral, right (Figure 3B), and left (Figure 3D) flexion, no significant differences were obtained from the ANOVA analyses between OOT and OOT+COL I treatment (p>0.05). However, the results regarding patients included in group B (Figure 3B and Figure 3D), showed better results. Overall, we can assess that no inferiority level of OOT+COL I treatment could be accepted. Movement analyses in the OOT+COL I groups revealed that the patients' body trunk appears to be more flexible, particularly when looking for the forward flexion parameter.
3.3. Functional Improvements: Analyses by Pathologies
The analyses of functional improvement were carried out spitting the patients’s tretments according the two pathologies investigated (LBP and lumbosciatica; Figure 4) and their associated treatments. The following parameters: forward bending (Figure 4A), lateral flexion to the right (LFR; Figure 4B), Disability questionnaire (Figure 4C) and; Figure 4D), lateral flexion to the left (LFL), were evaluated reporting the delta differences between visit T2 and visit T0 (T2-T0). Negative values were considered a positive factor for the effectiveness of the treatment. For each graph, the global analyses avoiding the type of pathology, were reported. These analyses were performed following the same composition of Figure 4. In addition to Figure 4, significant statistical differences were observed in Plots A and B (p<0.001). Whereas, no statistically significant difference was observed in both plots B and D (p=NS). However, all analyses revealed a higher positive trend (more negative values) of OOT+COL I treatment in all parameters analyzed (Figure 4A, Figure 4B, Figure 4C and Figure 4D). Specifically, we observed the following:
- The OOT+COL I treatments increased forward flexion in patients with LBP compared to those with lumbosciatica. Furthemere, OOT+COL I treatment improved forward flexion in both pathologies (p<0.001).
- The OOT+COL I treatments improved better disability condition level in patients with lumbosciatica compared to those with LBP. Again, OOT+COL I treatment improved disability in both pathologies (p<0.01).
- No statistically significant differences were observed in lateral flexion analyses . However, the LFR results analyzed returned a probability value very close to significance (p=0.0606).
- So far, even in these analyses, non-inferiority levels have been achieved for both pathologies investigated. Indeed, in our personal impression the combined approach (OOT+COL I) acts as booster improving the clinical condition of both LBP and lumbosciatica patients.
4. Discussion
Low back pain (LBP) continues to be one of the most common causes of functional and social limitation and absence from work, affecting over 80% of the general population worldwide [33,34]The diagnosis of LBP is usually associated with lumbar radiculopathy, with a prevalence of between 9.9% and 25% [35]. However, The intervertebral disc plays an important role in maintaining the normal spinal complex. Several disc pathologies, including internal disc rupture, tears, degeneration, and height loss, can predispose patients to disc-associated back pain and its complications [7]. In order to fight clinically the LBP, the The American Society of Pain and Neuroscience (ASPN) has indicated several procedures and/or treatments including: anti-inflammatory therapy [8], ozone treatment [9,10,11], minimally invasive procedures [12,13], regenerative drugs [7,14,15,16] and surgery [17,18]. However, looking for the ASPN document , never clear indication recording OOT was highlighted, specially analyzing the indication for injectable therapy [7]. Nonetheless, the literature emphasizes the efficacy and safety of ozone therapy for low back pain (LBP) due to lumbar disc herniation [1,36,37,38]. Most articles have shown that OOT treatment improved outcomes in both pain [1,10,39] and functional status [40,41] with treatment including ozone vs ozone-free group (controls) [21]. This fact seems to be in agreement with several studies, in which similar results are reported [1]. However, looking at different articles can highlight several limitations in these studies. First, different protocols were used in each study, with different concentrations and doses of ozone, routes of application, and methods for evaluating the results [20]. Usually, OOT therapy is not combined with other medical strategies. So far, it may be very difficult to understand whether using OOT treatment alone can improve the condition of patients with LBP [2]. In this study we compared and analyzed two different treatments against low back pain and lumbosciatica: OOT injection and OOT injection + administration of porcine collagen type 1 (COL I). It is known that OOT treatment affects the anti-inflammatory process and (nevertheless) disc dehydration [42], while collagen injection seems to privilege the management of collagen I metabolism, with regard to its synthesis, migration and regeneration [29,30]. The modification of these physiological phenomena is considered the basis of the biological resolution of LBP pathologies. Although many studies have involved the use of ozone only in LBP pathologies [1,11,40,41], while, no one study reported the combination of OOT and COL I.
This study analyzed 20 patients with LBP comparing the effect of OOT+COL I treatment to OOT alone. Usually, the physicians assessed the resolution of pain status, using (mostly) VAS ratings instead of the likert algorithm NRS (Numeric Pain Rating Scale) [14]. In the present study, we evaluated pain as the first parameter according to the NRS scale. Our result showed much better results comparing OOT+COL I (group B) to OOT alone (group A), looking for pain resolution, improved movement, and reduced disability condition of patients. The arm containing patients treated with OOT+COL I revealed better results than those obtained in the OOT arm alone, within all the parameters investigated. In particular, significant statistical differences were found by analysing: the evolution of pain (p<0.0001), the forward flexion parameter (p=0.001), Figure 2, Figure 3 and Figure 4) and in the reduction of disability (Figure 3C and Figure 4C). In addition, the OOT+COL I treatment also positively influenced LPB patients and lumbosciatica patients.
Combination treatment (OOT+COL I), seems to play a fundamental role in improving pain and physiological condition in the short and long term (Six-month of follow-up. In any case, the levels of absence of inferiority were evaluated taking into account all the parameters investigated. The combination of these treatment regimens (OOT+COL I) has not been evaluated previously in LBP patients and therefore, we have no matching parameters. The combined action of the injective medical device (MD-LUMBAR) and intra-muscular injection therapy with O2O3 seems to confirm a booster effect in patients suffering from LBP and lumbosciatica. It is reasonably valid to assume that the combined treatment can act as a booster by simultaneously promoting the anti-inflammatory effect of ozone treatment [44] and the regenerative effect of collagen [29]. This approach could also be called "regenerative medicine", according to the criteria of the American Society of Pain and Neuroscience (ASPN) guidelines [14]. It is important to understand that not all biologics used in regenerative medicine are equivalent. the patient's health status and comorbidities, the medications the patient takes, the parameters and the protocol used for cell collection influence or may influence the final result of mesenchymal stem cell (MSC) collection. Because these variables could not be fully controlled, clinical trials evaluating regenerative medicine for LBP in discogenic disease, including prolotherapy, protein-rich plasma (PRP), cell therapy, and other intra-disc injections, were reviewed [14]. The ASPN guidelines do not mention the use of porcine collagenase in the regenerative medicine chapter, however the action of porcine collagen type 1 affects collagen turnover [29,30] and its safety and efficacy [31,32] were reported in previous studies. Probably, the efficacy of COL I medical device might be associated with the connective tissue structure, characterized by the presence of the Extracellular Matrix (ECM). [29] The ECM, present in all tissues, represents the substrate on which tissue cells can adhere, migrate, proliferate and differentiate. It consists of macromolecules (proteoglycans and specialized proteins such as elastin and fibronectin) that influence tissue cell functions, indirectly controlling physiological, pathophysiological and pathological phenomena. The connective tissue is structurally characterized by the presence of the Extracellular Matrix (ECM) [30] . The ECM, present in all tissues, represents the substrate on which tissue cells can adhere, migrate, proliferate and differentiate. It consists of macromolecules (proteoglycans and specialized proteins such as elastin and fibronectin) that influence tissue cell functions, indirectly controlling physiological, pathophysiological and pathological phenomena [45]. Considering these reasons, the results of the present study confirm the positive effects of OOT COLI treatment demonstrating the efficacy on both short-term and long-term painful symptoms. COL I dmedical device, strongly boots the action of ozone, establishing a metabolic synergism against LBP and lumbosciatic diseases. In addition COL I improves motor function of the spine by demonstrating improved forward flexion and improves the overall disability condition of patients with both low back pain and lumbosciatica.
Although the treatments with added porcine collagen type 1 improve lateral flexions of the spine (right and left) overall, the data do not indicate a significant difference compared to treatments with OOT alone. The addition of porcine collagen type 1, by injection, can open three interesting points of reflection. 1) The self-diffusion capacity of the medical device (MD-LUMBAR) highlights the ability of collagen molecules to enrich the site of interest, where, the EUS-guided injection could be a non-mandatory approach, but remain still recommended.
2) The combined action of OOT+COL I maximises the effect of the therapy, as a booster, in patients affected by LBP and lumbosciatica.
3) At the same time, the regenerative properties of porcine collagen type 1 could lead to this treatment being included within the branch of regenerative medicine.
Although the results of the present study strongly suggest the benefit for patients with LBP and lumbosciatica, the results did not report any confirmation of modification of the patient's morpho-physiological conditions. However, the indications of the Italian health system avoid MRI investigation, in the absence of symptoms. Furthermore, this aspect is also underlined in the guidelines for non-surgical treatment, in which the authors confirmed the non-need for MRI imaging, if the symptoms are not present (PICO 4 point) [43]. Certainly the total number of patients analyzed is not very large, however the sample size analyzed was found to be sufficient. Further studies with higher sample sizes will be necessary for the possible confirmation of the results presented in this study.
5. Conclusions
Previously, no studies had been conducted regarding the combined use of OOT and porcine collagen type 1 injection. The combination of these two injective therapies has been shown to be safe, feasible and effective. No adverse events were found in any patient. Therfore, the addition of porcine collagen I treatment to OOT has been shown to boots the results obtained with ozone-based treatment alone in the short and long time. Furter investigation including a high number of patients, might be useful in order to confirm the results in this proof of concept study.
Author's contributions
"Conceptualization, L.S.; methodology, L.S., E.DP., S.M.; software interpretation, L.S.; validation, L.S.; E.DP., S.M.; formal analysis, E.DP., S.M.; investigation, L.S. and E.DP., resources, L.S.; data care, S.M.; writing: preparation of the original project, L.S.; writing: revision and editing, E.DP., visualization, L.S.; E.DP., S.M.; supervision, L.S.; project administration, L.S. All authors have read and accepted the published version of the manuscript." Please see the CRediT taxonomy for the explanation of the term. Authorship must be limited to those who have contributed substantially to the work reported.
Informed consent statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data obtained from this study are available for consultation. The data controller is Dr. Liliana Sgarbi
Conflicts of interest
The authors declare that they have no conflicts of interest.
References
- Costa, T.; Linhares, D.; Ribeiro da Silva, M.; Neves, N. Ozone Therapy for Low Back Pain. A Systematic Review. Acta Reumatol. Port. 2018, 43, 172–181. [PubMed]
- Hashemi, M.; Poorfarokh, M.; Mohajerani, S.A.; Jalili, P.; Akhyani, V.; Barikani, A.; Farivar, F. Injection of Intradiscal O2-O3 to Reduce Pain and Disability of Patients With Low Back Pain Due to Prolapsed Lumbar Disk. Anesthesiol. Pain Med. 2014, 4. [CrossRef] [PubMed]
- Paoloni, M.; Di Sante, L.; Cacchio, A.; Apuzzo, D.; Marotta, S.; Razzano, M.; Franzini, M.; Santilli, V. Intramuscular Oxygen-Ozone Therapy in the Treatment of Acute Back Pain With Lumbar Disc Herniation: A Multicenter, Randomized, Double-Blind, Clinical Trial of Active and Simulated Lumbar Paravertebral Injection. Spine 2009, 34, 1337–1344. [CrossRef] [PubMed]
- Bonetti, M.; Zambello, A.; Leonardi, M.; Princiotta, C. Herniated Disks Unchanged over Time: Size Reduced after Oxygen–Ozone Therapy. Interv. Neuroradiol. 2016, 22, 466–472. [CrossRef] [PubMed]
- Wang, F.; Sun, R.; Zhang, S.-D.; Wu, X.-T. Comparison of Thoracolumbar versus Non-Thoracolumbar Osteoporotic Vertebral Compression Fractures in Risk Factors, Vertebral Compression Degree and Pre-Hospital Back Pain. J. Orthop. Surg. 2023, 18, 643. [CrossRef]
- Zhang, S.; Gu, M.; Zhang, T.; Xu, H.; Mao, S.; Zhou, W. Effects of Exercise Therapy on Disability, Mobility, and Quality of Life in the Elderly with Chronic Low Back Pain: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Orthop. Surg. 2023, 18, 513. [CrossRef]
- Sayed, D.; Grider, J.; Strand, N.; Hagedorn, J.M.; Falowski, S.; Lam, C.M.; Tieppo Francio, V.; Beall, D.P.; Tomycz, N.D.; Davanzo, J.R.; et al. The American Society of Pain and Neuroscience (ASPN) Evidence-Based Clinical Guideline of Interventional Treatments for Low Back Pain. J. Pain Res. 2022, Volume 15, 3729–3832. [CrossRef]
- Derby, R.; Lee, S.-H.; Date, E.S.; Lee, J.-H.; Lee, C.-H. Size and Aggregation of Corticosteroids Used for Epidural Injections. Pain Med. 2008, 9, 227–234. [CrossRef]
- Cantele, F.; Tognolo, L.; Caneva, F.; Formaggio, E.; Copetti, V.; Venturin, A.; Caregnato, A.; Masiero, S. Influence of Pain-Related Psychological Factors on Therapeutic Outcomes in Patients with Chronic Low Back Pain after Oxygen-Ozone Treatment: A Case-Series. Eur. J. Transl. Myol. 2021, 31. [CrossRef]
- Biazzo, A.; Corriero, A.S.; Confalonieri, N. Intramuscular Oxygen-Ozone Therapy in the Treatment of Low Back Pain. Acta Bio Medica Atenei Parm. 2018, 89, 41–46. [CrossRef]
- Sconza, C.; Leonardi, G.; Kon, E.; Respizzi, S.; Massazza, G.; Marcacci, M.; Di Matteo, B. Oxygen-Ozone Therapy for the Treatment of Low Back Pain: A Systematic Review of Randomized Controlled Trials. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 6034–6046. [CrossRef] [PubMed]
- Franke, J.; Greiner-Perth, R.; Boehm, H.; Mahlfeld, K.; Grasshoff, H.; Allam, Y.; Awiszus, F. Comparison of a Minimally Invasive Procedure versus Standard Microscopic Discotomy: A Prospective Randomised Controlled Clinical Trial. Eur. Spine J. 2009, 18, 992–1000. [CrossRef] [PubMed]
- Jain, S.; Deer, T.; Sayed, D.; Chopra, P.; Wahezi, S.; Jassal, N.; Weisbein, J.; Jameson, J.; Malinowski, M.; Golovac, S. Minimally Invasive Lumbar Decompression: A Review of Indications, Techniques, Efficacy and Safety. Pain Manag. 2020, 10, 331–348. [CrossRef] [PubMed]
- Sayed, D.; Grider, J.; Strand, N.; Hagedorn, J.M.; Falowski, S.; Lam, C.M.; Tieppo Francio, V.; Beall, D.P.; Tomycz, N.D.; Davanzo, J.R.; et al. The American Society of Pain and Neuroscience (ASPN) Evidence-Based Clinical Guideline of Interventional Treatments for Low Back Pain. J. Pain Res. 2022, Volume 15, 3729–3832. [CrossRef]
- Akeda, K.; Ohishi, K.; Masuda, K.; Bae, W.C.; Takegami, N.; Yamada, J.; Nakamura, T.; Sakakibara, T.; Kasai, Y.; Sudo, A. Intradiscal Injection of Autologous Platelet-Rich Plasma Releasate to Treat Discogenic Low Back Pain: A Preliminary Clinical Trial. Asian Spine J. 2017, 11, 380–389. [CrossRef]
- Levi, D.; Horn, S.; Tyszko, S.; Levin, J.; Hecht-Leavitt, C.; Walko, E. Intradiscal Platelet-Rich Plasma Injection for Chronic Discogenic Low Back Pain: Preliminary Results from a Prospective Trial. Pain Med. 2015, pnv053. [CrossRef]
- Galica, R.J.; Hayek, S.M.; Veizi, E.; McEwan, M.T.; Katta, S.; Ali, O.; Aziz, N.; Sondhi, N. Intrathecal Trialing of Continuous Infusion Combination Therapy With Hydromorphone and Bupivacaine in Failed Back Surgery Patients. Neuromodulation Technol. Neural Interface 2018, 21, 648–654. [CrossRef]
- Verrills, P.; Mitchell, B.; Vivian, D.; Sinclair, C. Peripheral Nerve Stimulation: A Treatment for Chronic Low Back Pain and Failed Back Surgery Syndrome? Neuromodulation Technol. Neural Interface 2009, 12, 68–75. [CrossRef]
- Andreula, C.F.; Simonetti, L.; De Santis, F.; Agati, R.; Ricci, R.; Leonardi, M. Minimally Invasive Oxygen-Ozone Therapy for Lumbar Disk Herniation. AJNR Am. J. Neuroradiol. 2003, 24, 996–1000.
- Rahimi-Movaghar, V.; Eslami, V. The Major Efficient Mechanisms of Ozone Therapy Are Obtained in Intradiscal Procedures. Pain Physician 2012, 15, E1007-1008. [CrossRef]
- Rome, Consensus Conference Italian Guidelines and Good Practices in Oxygen-Ozone Therapy 2024.
- Leo, B.M.; Walker, M.H.; Anderson, D.G. The Molecular Basis of Intervertebral Disc Degeneration. In Progress in Neurological Surgery; Freese, A., Simeone, F.A., Leone, P., Janson, C., Eds.; KARGER: Basel, 2005; pp. 5–29 ISBN 978-3-8055-7784-7.
- García-Cosamalón, J.; Del Valle, M.E.; Calavia, M.G.; García-Suárez, O.; López-Muñiz, A.; Otero, J.; Vega, J.A. Intervertebral Disc, Sensory Nerves and Neurotrophins: Who Is Who in Discogenic Pain? J. Anat. 2010, 217, 1–15. [CrossRef] [PubMed]
- Langevin, H.M.; Fox, J.R.; Koptiuch, C.; Badger, G.J.; Greenan- Naumann, A.C.; Bouffard, N.A.; Konofagou, E.E.; Lee, W.-N.; Triano, J.J.; Henry, S.M. Reduced Thoracolumbar Fascia Shear Strain in Human Chronic Low Back Pain. BMC Musculoskelet. Disord. 2011, 12, 203. [CrossRef] [PubMed]
- Langevin, H.M.; Stevens-Tuttle, D.; Fox, J.R.; Badger, G.J.; Bouffard, N.A.; Krag, M.H.; Wu, J.; Henry, S.M. Ultrasound Evidence of Altered Lumbar Connective Tissue Structure in Human Subjects with Chronic Low Back Pain. BMC Musculoskelet. Disord. 2009, 10, 151. [CrossRef] [PubMed]
- Kannus, P. Structure of the Tendon Connective Tissue. Scand. J. Med. Sci. Sports 2000, 10, 312–320. [CrossRef] [PubMed]
- Kjær, M. Role of Extracellular Matrix in Adaptation of Tendon and Skeletal Muscle to Mechanical Loading. Physiol. Rev. 2004, 84, 649–698. [CrossRef]
- Riley, G.P.; Harrall, R.L.; Constant, C.R.; Chard, M.D.; Cawston, T.E.; Hazleman, B.L. Glycosaminoglycans of Human Rotator Cuff Tendons: Changes with Age and in Chronic Rotator Cuff Tendinitis. Ann. Rheum. Dis. 1994, 53, 367–376. [CrossRef]
- Randelli, F.; Menon, A.; Giai Via, A.; Mazzoleni, M.; Sciancalepore, F.; Brioschi, M.; Gagliano, N. Effect of a Collagen-Based Compound on Morpho-Functional Properties of Cultured Human Tenocytes. Cells 2018, 7, 246. [CrossRef]
- Randelli, F.; Sartori, P.; Carlomagno, C.; Bedoni, M.; Menon, A.; Vezzoli, E.; Sommariva, M.; Gagliano, N. The Collagen-Based Medical Device MD-Tissue Acts as a Mechanical Scaffold Influencing Morpho-Functional Properties of Cultured Human Tenocytes. Cells 2020, 9, 2641. [CrossRef]
- Godek, P. Collagen Therapy in Lumbar Spondylosis – a Pilot Study. Does the Route of Administration Matter? Ortop. Traumatol. Rehabil. 2019, 21, 427–436. [CrossRef]
- Pavelka, K.; Jarosova, H.; Milani, L.; Prochazka, Z.; Kostiuk, P.; Kotlarova, L.; Meroni, A.M.; Sliva, J. Efficacy and Tolerability of Injectable Collagen-Containing Products in Comparison to Trimecaine in Patients With Acute Lumbar Spine Pain (Study FUTURE-MD-Back Pain). Physiol. Res. 2019, S65–S74. [CrossRef]
- Rivera, C.E. Lumbar Epidural Steroid Injections. Phys. Med. Rehabil. Clin. N. Am. 2018, 29, 73–92. [CrossRef] [PubMed]
- Van Tulder, M.; Koes, B.; Bombardier, C. Low Back Pain. Best Pract. Res. Clin. Rheumatol. 2002, 16, 761–775. [CrossRef] [PubMed]
- Van Boxem, K.; Cheng, J.; Patijn, J.; Van Kleef, M.; Lataster, A.; Mekhail, N.; Van Zundert, J. 11. Lumbosacral Radicular Pain. Pain Pract. 2010, 10, 339–358. [CrossRef] [PubMed]
- Barbosa, L.T.; Rodrigues, C.F.D.S.; Andrade, R.R.D.; Barbosa, F.T. The Effectiveness of Percutaneous Injections of Ozonotherapy in Low Back Pain. Rev. Assoc. Médica Bras. 2020, 66, 1146–1151. [CrossRef] [PubMed]
- Clavo, B.; Robaina, F.; Urrutia, G.; Bisshopp, S.; Ramallo, Y.; Szolna, A.; Caramés, M.A.; Fiuza, M.D.; Linertová, R. Ozone Therapy versus Surgery for Lumbar Disc Herniation: A Randomized Double-Blind Controlled Trial. Complement. Ther. Med. 2021, 59, 102724. [CrossRef]
- Elawamy, A.; Kamel, E.Z.; Hassanien, M.; Wahba, O.M.; Amin, S.E. Implication of Two Different Doses of Intradiscal Ozone-Oxygen Injection upon the Pain Alleviation in Patients with Low Back Pain: A Randomized, Single-Blind Study. Pain Physician 2018, 21, E25–E31.
- Davidovic, K.; Cotofana, S.; Heisinger, S.; Savic, S.; Alfertshofer, M.; Antonić, T.; Jovanović, S.; Ercegovac, M.; Muto, M.; Jeremić, D.; et al. Percutaneous Computed Tomography-Guided Oxygen-Ozone (O2O3) Injection Therapy in Patients with Lower Back Pain—An Interventional Two-Year Follow-Up Study of 321 Patients. Diagnostics 2023, 13, 3370. [CrossRef]
- Barbosa, D.C.; Ângelos, J.S.D.; Macena, G.M.J.D.; Magalhães, F.N.D.O.; Fonoff, E.T. Effects of Ozone on the Pain and Disability in Patients with Failed Back Surgery Syndrome. Rev. Assoc. Médica Bras. 2017, 63, 355–360. [CrossRef]
- De Sire, A.; Agostini, F.; Lippi, L.; Mangone, M.; Marchese, S.; Cisari, C.; Bernetti, A.; Invernizzi, M. Oxygen–Ozone Therapy in the Rehabilitation Field:State of the Art on Mechanisms of Action, Safety andEffectiveness in Patients with Musculoskeletal Disorders. Biomolecules 2021, 11, 356. [CrossRef] [PubMed]
- De Sire, A.; Marotta, N.; Ferrillo, M.; Agostini, F.; Sconza, C.; Lippi, L.; Respizzi, S.; Giudice, A.; Invernizzi, M.; Ammendolia, A. Oxygen-Ozone Therapy for Reducing Pro-Inflammatory Cytokines Serum Levels in Musculoskeletal and Temporomandibular Disorders: A Comprehensive Review. Int. J. Mol. Sci. 2022, 23, 2528. [CrossRef]
- Stochkendahl, M.J.; Kjaer, P.; Hartvigsen, J.; Kongsted, A.; Aaboe, J.; Andersen, M.; Andersen, M.Ø.; Fournier, G.; Højgaard, B.; Jensen, M.B.; et al. National Clinical Guidelines for Non-Surgical Treatment of Patients with Recent Onset Low Back Pain or Lumbar Radiculopathy. Eur. Spine J. 2018, 27, 60–75. [CrossRef] [PubMed]
- Clavo, B.; Martínez-Sánchez, G.; Rodríguez-Esparragón, F.; Rodríguez-Abreu, D.; Galván, S.; Aguiar-Bujanda, D.; Díaz-Garrido, J.A.; Cañas, S.; Torres-Mata, L.B.; Fabelo, H.; et al. Modulation by Ozone Therapy of Oxidative Stress in Chemotherapy-Induced Peripheral Neuropathy: The Background for a Randomized Clinical Trial. Int. J. Mol. Sci. 2021, 22, 2802. [CrossRef] [PubMed]
- Li, P.-B.; Tang, W.-J.; Wang, K.; Zou, K.; Che, B. Expressions of IL-1α and MMP-9 in Degenerated Lumbar Disc Tissues and Their Clinical Significance. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 4007–4013.
Figure 1.
Schematic representation of the subdivision of the two groups (A and B) treated with Oxigen-Ozone Treatment (OOT) and Porcine Collagen type 1 (COLI). To the left MRI drives the physician to select the points of injections.
Figure 1.
Schematic representation of the subdivision of the two groups (A and B) treated with Oxigen-Ozone Treatment (OOT) and Porcine Collagen type 1 (COLI). To the left MRI drives the physician to select the points of injections.
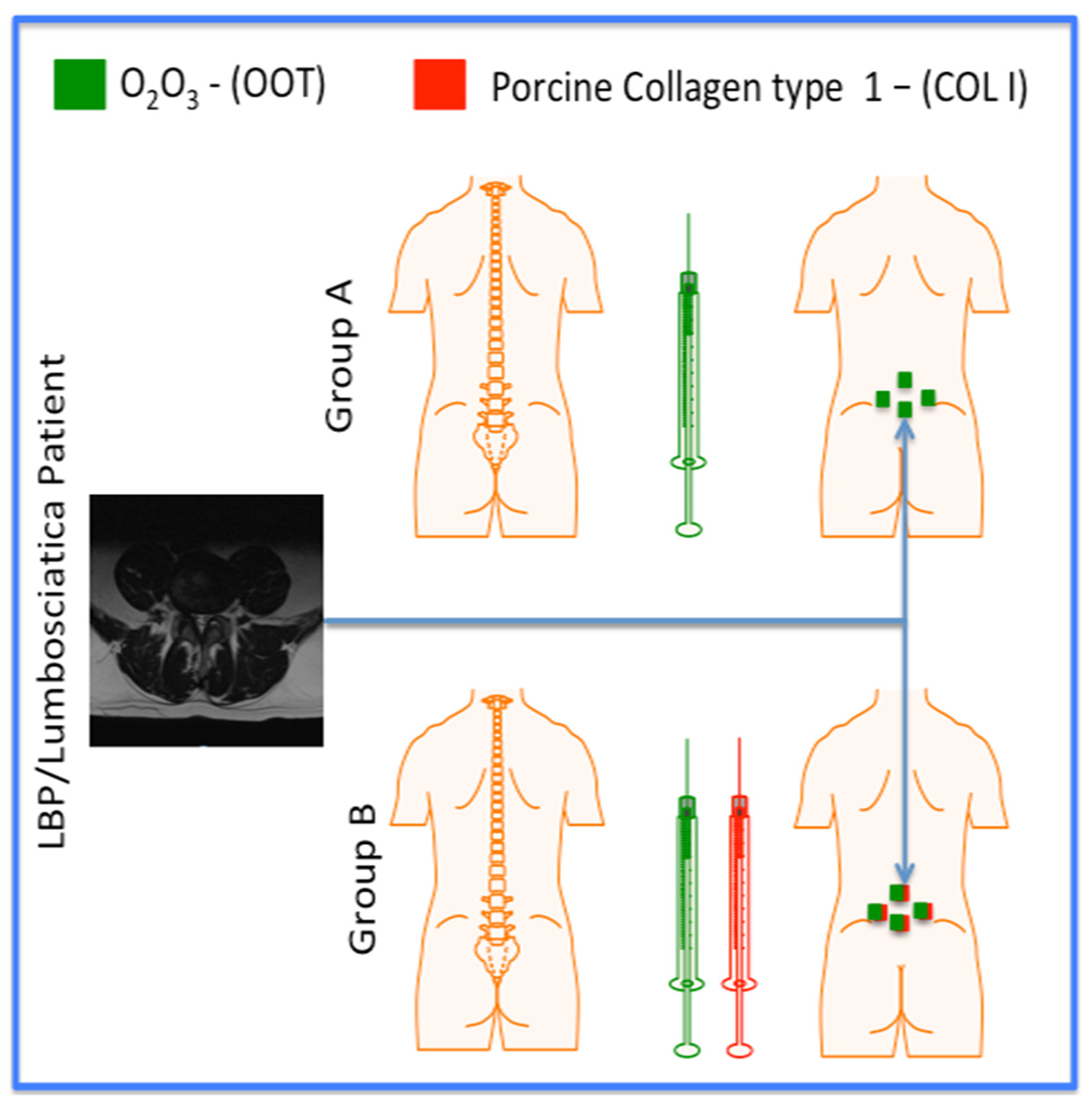
Figure 2.
Results of NRS analyses. A) distribution of NRS within the two cohorts of patients, prior to treatments; B) Analysis of the mean value of NRS in the follow-up period; C) NSR delta at T1 in both groups; D) Change in NRS Delta over time; E) NRS differences between T2 and T1. This graph strapulation indicates the rate of improvement of the NRS in the two groups.
Figure 2.
Results of NRS analyses. A) distribution of NRS within the two cohorts of patients, prior to treatments; B) Analysis of the mean value of NRS in the follow-up period; C) NSR delta at T1 in both groups; D) Change in NRS Delta over time; E) NRS differences between T2 and T1. This graph strapulation indicates the rate of improvement of the NRS in the two groups.
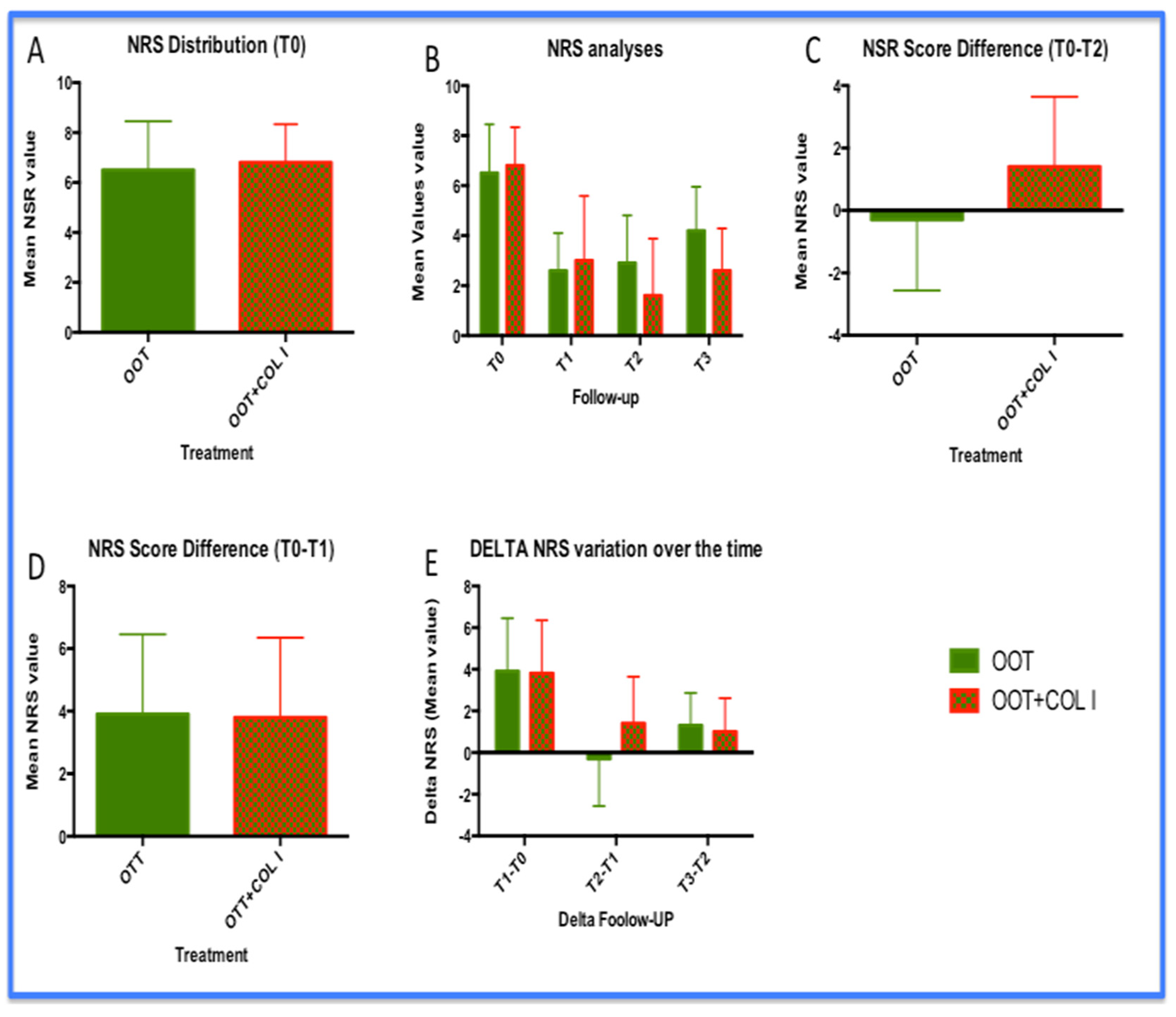
Figure 3.
Functional improuvement. Results of: A) forward bending; B) Lateral flexion to the right (LFR); C) Disability questionnaire; d) Lateral flexion to the left (LFR). In graphs A and C the decrease in their average value is statistically significant, where the differences between OOT vs OOT+COL I are evident (P<0.001). In addition, graph A shows an anti-parallel direction of the forward banding parameter. Conversely, the values reported in the analysis of the questionnaire revealed the same trend for the treatment with OOT vs OOT+COL I, but in the second treatment the decrease was constant over time compared to that observed in the OOT treatment alone. While, within graphs B and D (Lateral motion), the LFR and LFL analyses did not reveal significant differences comparing OOT vs OOT+COL I treatments. However, the positivity trend was observed in both motions and the result in LFR reached a very close significant value (p=0.0606). In addition, no inferiority level was observed for OOT+COL I compared to OOT treatment alone.
Figure 3.
Functional improuvement. Results of: A) forward bending; B) Lateral flexion to the right (LFR); C) Disability questionnaire; d) Lateral flexion to the left (LFR). In graphs A and C the decrease in their average value is statistically significant, where the differences between OOT vs OOT+COL I are evident (P<0.001). In addition, graph A shows an anti-parallel direction of the forward banding parameter. Conversely, the values reported in the analysis of the questionnaire revealed the same trend for the treatment with OOT vs OOT+COL I, but in the second treatment the decrease was constant over time compared to that observed in the OOT treatment alone. While, within graphs B and D (Lateral motion), the LFR and LFL analyses did not reveal significant differences comparing OOT vs OOT+COL I treatments. However, the positivity trend was observed in both motions and the result in LFR reached a very close significant value (p=0.0606). In addition, no inferiority level was observed for OOT+COL I compared to OOT treatment alone.
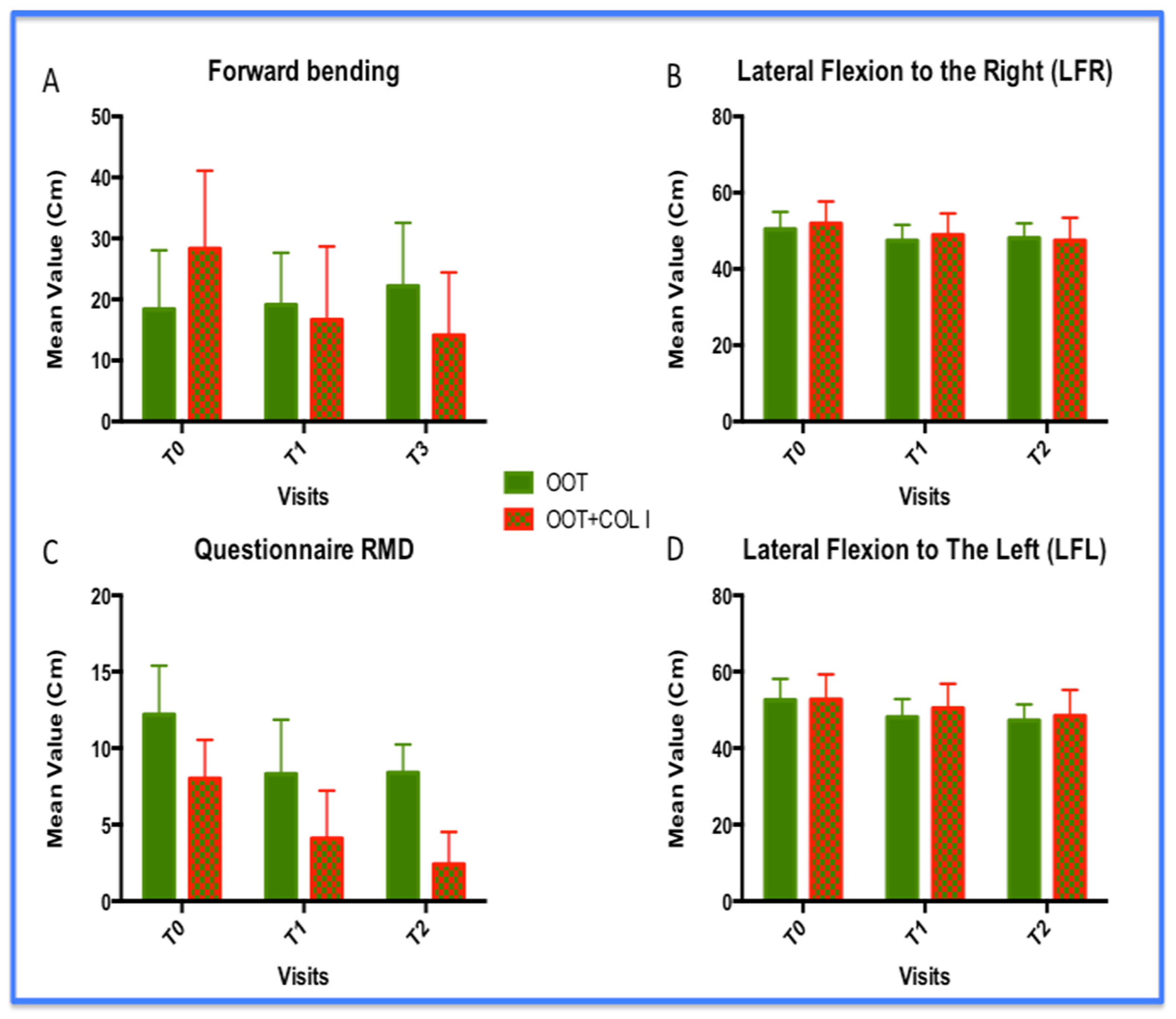
Figure 4.
Treatment Vs Analysis of pathologies. Results of: A) forward bending; B) Lateral flexion to the right (LFR); C) Disability questionnaire; d) Lateral flexion to the left (LFL). The results reported the differences between the mean value obtained at the T0 visit and the T2 visit (T2-T0). Negative values represent the positive effects of treatments. In graphs A and C the decreasement in their average value is statistically significant (P<0.001), where the differences between OOT vs OOT+COL I are reversed as shown in figure 4A. In addition, Graph A shows an anti-parallel parameter of the direction of forward bands. Conversely, the values reported in the questionnaire analyses revealed a progressive positive trend for both treatments, however, in the OOT+COL I treatment, the decreasement was significantly higher than that observed in the OOT treatment alone. While, within graphs B and D (Lateral motion), the LFR and LFL analyses did not show significant differences comparing OOT vs OOT+COL I. However, the positivity trend was observed in both movements, and the result in LFR reached a very close significant value (p=0.0606). In addition, no inferiority level was observed for OOT+COL I compared to OOT treatments alone, considering all the parameters analyzed.
Figure 4.
Treatment Vs Analysis of pathologies. Results of: A) forward bending; B) Lateral flexion to the right (LFR); C) Disability questionnaire; d) Lateral flexion to the left (LFL). The results reported the differences between the mean value obtained at the T0 visit and the T2 visit (T2-T0). Negative values represent the positive effects of treatments. In graphs A and C the decreasement in their average value is statistically significant (P<0.001), where the differences between OOT vs OOT+COL I are reversed as shown in figure 4A. In addition, Graph A shows an anti-parallel parameter of the direction of forward bands. Conversely, the values reported in the questionnaire analyses revealed a progressive positive trend for both treatments, however, in the OOT+COL I treatment, the decreasement was significantly higher than that observed in the OOT treatment alone. While, within graphs B and D (Lateral motion), the LFR and LFL analyses did not show significant differences comparing OOT vs OOT+COL I. However, the positivity trend was observed in both movements, and the result in LFR reached a very close significant value (p=0.0606). In addition, no inferiority level was observed for OOT+COL I compared to OOT treatments alone, considering all the parameters analyzed.
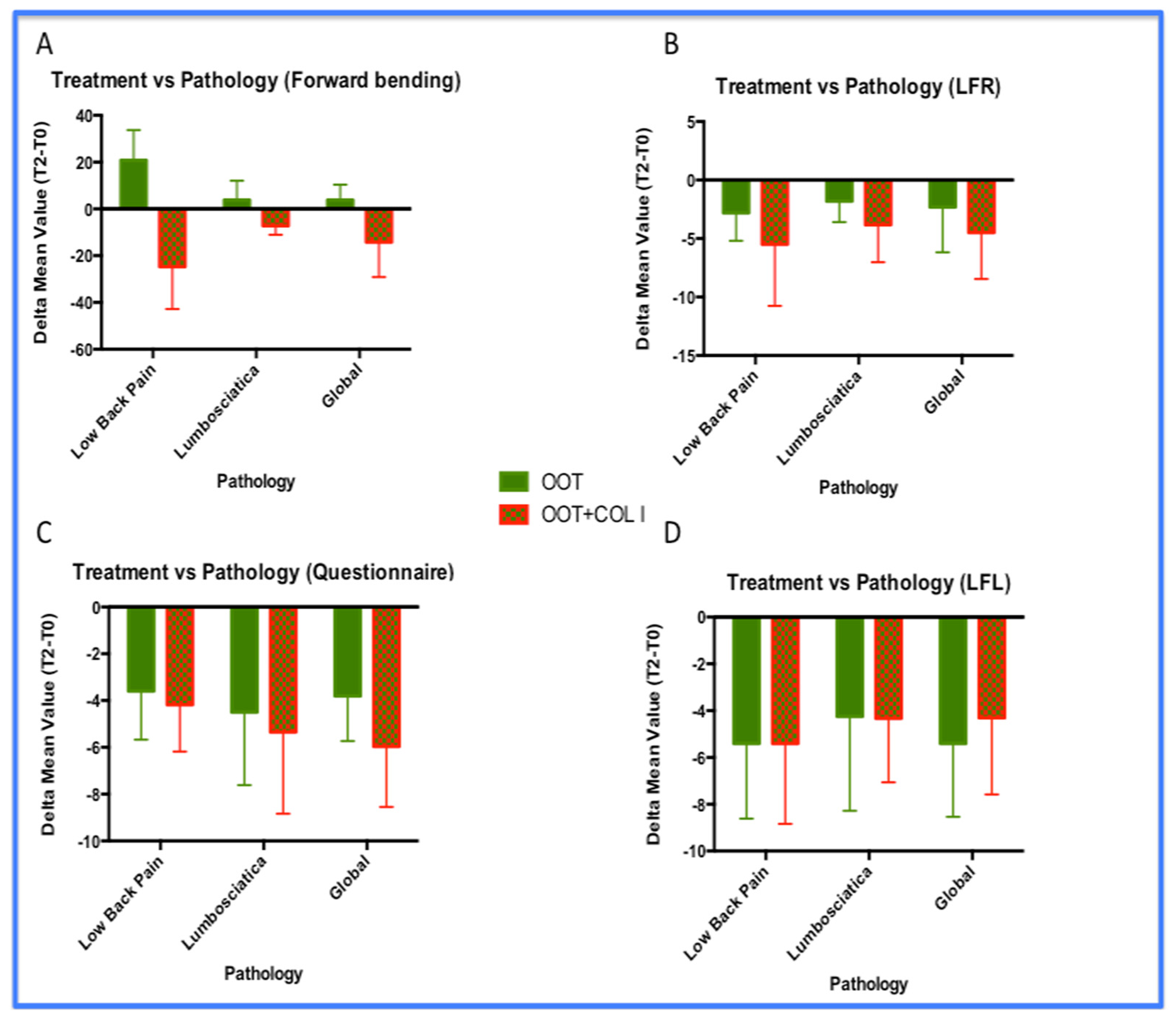

Table 1.
Characteristic of the treatments. Both treatments were administered over two months.
| Gruop | Treatment | Volume | Number of treatments |
|---|---|---|---|
| A (10; 5M and 5F) | O2O3 | 20 ml | 8 |
| B (10; 5M and 5F) | O2O3 + MD-LUMBAR | 20 ml + 2 ml | 8 |
Note: The number of patients enrolled for each arm is indicated in round brackets.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



