Submitted:
07 September 2024
Posted:
09 September 2024
You are already at the latest version
Abstract
Background - Compared to the da Vinci platform, there is limited experience with the Hugo RAS platform for colorectal surgery in Europe. This difference is especially notable when considering a single complex procedure, such as total colectomy. Aim - To demonstrate the feasibility and safety of using the Hugo RAS for assisted total colectomy. Clinical case- Female patient: eighteen-year-old with Familial Adenomatous Polyposis (FAP). Her IBM was 19. She underwent a total colectomy with ileorectal anastomosis using the Hugo RAS platform. The procedure took 230 minutes and had no complications. The postoperative period was uneventful. She was discharged from the hospital on the third postoperative day. Conclusion - The Hugo RAS platform is one of the emergent minimally invasive robotic platforms that can be used even in total colectomy if the proper patient selection is made. The placement choice of arms and trocars was crucial to obtain a similar operative time of the single laparoscopic approach. The certification of Hugo’s new instruments, such as energy devices and staplers, will make this platform even more competitive.
Keywords:
Hugo RAS Total colectomy
; Robotic total colectomy
; Minimally Invasive Surgical Procedure
; Robotic colorectal surgery
; Familial Adenomatous polyposis
; Robotic technical surgery aspects
1. Introduction
World robotic surgery implementation for colorectal surgery was made in a progressive but slow way due to the economic aspects. It is undeniable that robotic platforms enhanced three-dimensional visualization and improved dexterity. The robotic system can provide better visualization of pelvic structures, better dissection, and greater ease in creating anastomoses. On the other hand, it is more ergonomic for the surgeon. These aspects can translate into clinical practice in reducing morbidity, shorter length of stay, and potentially better long-term results than the laparoscopic approach [1]. The drawbacks include extended operative time, higher initial investment, and increased consumables costs [1].
The platform DaVinci® by Intuitive Surgical in Sunnyvale, CA, USA, is a robotic system placed in reference center hospitals more than two decades ago, and upgrades have made it the robotic system reference. The new emergent robotics platform intends to be an alternative to the pioneer. For that to happen, new systems must be competitive in terms of feasibility, safety, results presented, and associated lower costs when compared to the da Vinci robotic-assisted system.
The advantages of robotic surgery are real for segmental colon resection, which seems to be consensual [1,2]. Still, it is impossible to have the same certainty when we focus on total colectomy [3]. Total colectomy is a more complex procedure that requires working in the four quadrants. Moving the patient-side surgical cart in the middle of the surgery makes the procedure more complex and associated with a longer operative time. The new model of DaVinci®, the XI boom-mounted system, partially resolves that problem [4]. Even so, the number of total colectomies performed worldwide with a robot system remains restricted [5].
The Hugo RAS® is one of the emergent and promising robotic systems. The modular Hugo RAS® allows operating using up to four arm carts [6,7]. It has been available in our center for one year. To date, we have performed sixty colorectal procedures assisted by the Hugo RAS system.
We described a total colectomy realized with Hugo RAS®, the first one published worldwide, referring to the technical aspects of the procedure to account for a safe and effective procedure.
2. Materials and Methods
Patient
The selected patient is an 18-year-old female with an index case of Familial Adenomatous polyposis (FAP). The diagnosis was suspected after the patient had an ophthalmologic exam, which revealed the presence of congenital hypertrophy of the retinal pigment epithelium (CHRPE) in both eyes (Figure 1a).
Based on this unexpected finding, the patient was submitted to a colonoscopy (Figure 1b) and a genetic study that confirmed the diagnosis. She presented a heterozygote pathogen variant in the APC gene. The parents’ colonoscopy and genetic study were normal.
She was psychologically stable and capable of following medical orientation. She and her family have regular medical appointments in cancer hereditary consultation of the Gastroenterology Service.
She was oriented for colorectal surgical consultation because she presented more than 500 polyps, some polyps type laterally spread lesions with low and high-grade adenomatous lesions. She had a small number of polyps in her rectum that were removed by endoscopy (Figure 1c).
After explaining the pros and cons of a total colectomy with ileorectal anastomosis versus a reconstructive proctocolectomy, the option was to do a total colectomy with an ileorectal anastomosis and close endoscopic surveillance of the rectum after surgery.
The scheduled surgery was in April 2024. The patient was hospitalized in April 2024, and she had made the surgical intestinal preparation with oral antibiotics and oral laxatives.
Platform Hugo RAS
A Hugo RAS® platform was available for robotic surgery. Four arms and one extra tower with a monitor were utilized. The console was placed in the operating room. The instruments for the robot were the camera, monopolar curved shears, bipolar Cadiere forceps, and Cadiere forceps. The instruments for the assistant port were Medtronic stapler (SigniaTM stapling system), Covidien EEA circular stapler, a device for insufflation and smoke evacuation and filtration, laparoscopic shears, hem-o-lock endoscopic applicator and hem-o-lock clips.
The arms of de Hugo RAS® were placed on each patient’s side.
Medtronic technical support was present at the time of surgery.
Surgical Procedure
Resume
The surgery was performed sequentially on the right colon - phase II, the left colon, and the pelvis – phase IV. The section of the rectum was made with a stapler. End of the robotic phase. Start of the laparoscopic - phase V.
Steps description of the procedure
Phase I - Initial steps and System Configuration
A - Port placement principles
The patient is on the operation table at 60 cm high.
The schematic port placement was marked on the patient (Figure 2).
Four ports are positioned diagonally from the left hypochondrium to the right iliac fossa. The robotic trocars were two of 8 mm and two of 11 mm. The robotic trocars of 11 mm were one for the camera; the other one was utilized with traditional laparoscopic material when needed and so, avoiding the need of a second assistant trocar also on the left side of the patient. One trocar of 12 mm is placed on the lateral edge of the transition from the superior right quadrant to the inferior right quadrant. This trocar is utilized for the insufflation and smoke evacuation and filtration system (Palliare TM), hemo-o-lock application, SigniaTM stapler utilization, etc.
B - Patient and bed position
Laparoscopic approach to position the patient and prepare the anatomical field to start robotic colectomy.
The table was placed in a 10 grade of Trendelenburg and 10 grade of lateral left side.
C - System Configuration
Docking the arms:
- 8 mm (arm in lateral-superior left position) Tilt (+30º) – dock – 45º - reserve
- 11 mm (arm in the lateral inferior left position) Tilt (+30º) – dock – 145º- endoscope /assistant port
- 8 mm (arm in the lateral inferior right position) Tilt (-15º) – dock – 225º- surgeon left hand (for the bipolar)
- 11mm. surgeon right hand (monopolar curved shears) Tilt (-15º) – dock – 315º and to use also for laparoscopic hem-o-lock application
Laparoscopic port:
- Assistant port and insufflation /aspiration system
Phase II - Assisted robotic right colectomy
Steps of robotic right colectomy in Figure 3.
Phase III - System Reconfiguration
Change of the position of the patient – Same Trendelenburg (10 to 15º), right lateral side tilt (10 to 15º)
Arms new docking (Figure 4):
- 8 mm (arm in lateral-superior left position) Tilt (-15º) – dock – 45º surgeon left hand with Cadiere grasper
- 8 mm (arm in lateral inferior left position) Tilt (-15º) – dock – 145º- surgeon right hand (monopolar curved shears)
- 11 mm (arm in the lateral inferior right position) Tilt (+30º) – dock – 225º- endoscope
- 11mm (arm in the lateral-superior right position) Tilt (+30º) – dock – 315º- reserve (Cadiere bipolar forceps)
Laparoscopic port:
- a)
- Assistant port and insufflation /aspiration system
Phase IV - Assisted robotic left colectomy
Steps of robotic left colectomy in Figure 5.
PHASE V – Laparoscopic assisted phase.
- A.
- Suprapubic incision,
- A.
- Extraction of the surgical specimen.
- A.
- Ileorectal anastomosis
General description of the procedure
Phase I – configuration of the system
For the robotic procedure, the patient is placed in a modified lithotomy position. After pneumoperitoneum is created with a Veress needle in the incision made for the camera, a total of five ports are placed, as shown in Figure 2.
The patient is then placed in a 10º Trendelenburg position with a 15º right lateral side tilt.
The arms are docked (Figure 2).
Phase II – right colectomy (Figure 3)
The procedure begins on the right side with entry into the retroperitoneum in the avascular portion of the mesentery between the superior mesenteric vein and the ileocolic vessels. The retroperitoneal structures, including the third portion of the duodenum and the pancreas, are bluntly dissected posteriorly; ileocolic vessels are isolated and divided close to their origin. Dissection proceeds along the superior mesenteric vein axis to identify the right colic artery and vein (when present) and the middle colic artery and vein. All vascular pedicles are controlled with Hem-o-lock clips. The mesentery of the right colon is mobilized from medial to lateral, leaving behind the pancreas, duodenum, and retroperitoneal structures. The great omentum is then opened to enter the lesser sac and complete the mobilization of the right colon.
Phase III – System re-docking
The robot’s arms are then detached from the trocars; the patient is repositioned with the left side lateral tilt of 15º up. The robotic arms are then reconnected to the trocars. The instruments are changed in (Figure 4).
Phase IV – Robotic left colectomy (Figure 5)
The inferior mesenteric artery and vein are divided, and a medial-to-lateral approach detaches the left mesocolon from the pancreas tail, the ureter, and gonadal vessels. The left paracolic gutter is opened to the splenic flexure, which is taken down. The great omentum is completely disconnected from the left side of the transverse colon which is also completely released. . After the sigmoid is detached from the lateral attachments, mesorectal partial dissection is performed, and the rectum is divided below the colorectal transition. All vascular pedicles are controlled with Hem-o-locks.
Phase V – Assisted laparoscopic phase
An assisted Pfannenstiel incision is made, and the ileum is sectioned. After the ileum section and surgical specimen extraction, the head of 28 EEA circular stapler was introduced in the ileum. The ileorectal anastomosis was made after the introduction of the body of the machine by the anus.
The ileorectal anastomosis integrity test is made with methylene blue.
The ports were closed with VicrylTM and staples.
Figure 6 represents the surgical specimen.
3. Results
Operating time was 253 min. Blood loss was irrelevant.
The postoperative period was uneventful. She had gas emission and started enteric nutrition on the first day. She initiated a liquid diet on the second day. She had stools and was discharged from the hospital on the post-operative third day.
The anatomopathological study reveals: macroscopy – an ileocecal colectomy piece comprising a 5 cm ileum segment, 8 cm ileocecal appendix, and 80 cm colon plus anastomosis rings. Microscopy – Colon with multiple adenomas of predominantly tubular architecture, some tubulovillous, most with low-grade dysplasia, but with several foci of high-grade dysplasia in a context of familial adenomatous polyposis (without adenocarcinoma). Anastomosis rings without adenomas.
One month later, she had four bowel movements during the day and one at night. The patient had no complaints at that time, and her abdominal appearance was satisfactory (Figure 7).
5. Discussion
The DaVinci surgical system by Intuitive Surgical in Sunnyvale, CA, USA, is yet the gold standard in robotic-assisted surgery due to its surgeon-friendly interface and market implementation. The main issue with DaVinci is the costs associated with the initial investment and the final price of the procedure. The high associated cost is a significant obstacle to its worldwide implementation. After two decades of DaVinci’s monopoly, new robotic platforms have been approved for clinical use. One is the Hugo RAS® system, which is as safe as DaVinci and offers reduced prices. This platform was recently made available in the European market. The main surgical experience with this platform is in the urologic area, with some international publications [8,9,10]. In Europe, the experience with Hugo Ras® in colorectal surgery is small [11,12], mainly if we refer to total colectomy. To our knowledge, this present case is the first assisted total colectomy published with the Hugo RAS® platform worldwide. The necessity of working in more than one abdominal quadrant in colorectal surgery implies greater complexity and added difficulty in robotic technical planning [13].
Santo António ULS, a University Hospital in Porto, Portugal, acquired the Hugo Platform in January 2023. The surgeons of urology and general surgery teams, after a training program at Orsi Academy with Medtronic support, started surgeries of prostate, colorectal, and obesity. The first surgeries were made in April 2023. Since that date, sixty colorectal surgeries have been performed. Recently, a total colectomy in a select patient was performed successfully. Revising the literature, little was written about the experience in robotic total colectomy, mainly with the Hugo system. Compared with the DaVinci Xi system, the obvious advantage of assisted total colectomy with Hugo is the reduction of costs, which can influence the decision to implement one system to the detriment of the other.
For this reason, we describe our first experience with the Hugo RAS system, namely the technical aspects of the procedure and the difficulties of managing this platform. On the other hand, we reflect on the pros and cons of robotic versus laparoscopic total colectomy and the importance of selecting the correct patient for a robotic approach in centers with still an initial small experience like ours.
There are several differences between the DaVinci and Hugo platforms. The main difference is the existence of four independent arms. The position of the arms is crucial for the ease and feasibility of the procedure to avoid arm collision and the possibility of use in different quadrants. The problem is more complex in total colectomy because the port’s location must be chosen for the right colectomy (Figure 2) and after the left colectomy (Figure 4). The number and position of the ports are quite different from how we handle them in the Hugo RAS system and how Centers of significant volume do it with the DaVinci Xi system [4,5]. On the other hand, in the middle of the operation, it is necessary to change the surgical table inclination, redocking the arms and the instrument’s position in the arms.. Possibly, this step takes more time than with DaVinci Xi. Other technical differences are the existence and utilization of a port for the assistant (Figure 2 and 4) for introducing a device for insufflation and smoke evacuation and filtration and the instruments of laparoscopic when necessary, such as shears, hem-o-lock endoscopic applicator, aspirator device, endoscopic stapler (SigniaTM). To avoid making another port for the assistant during the right colectomy, the port assistant is assumed by port 4, alternating with the port surgeon’s right hand (monopolar curved shears) (Figure 2). The way we performed the assisted total colectomy after the colorectal transition section with a SigniaTM introduced by the assistant port and the sigmoid colon referenced with a grasper, the robotic phase is finished. The assisted laparoscopic phase is Initiated and performed as already described. The Hugo platform doesn’t yet have the robotic stapler and the vessel sealer device approved/certified. Currently, Hugo RAS energy devices are only bipolar and monopolar. We prefer to use the hem-o-lock system for vessels of larger caliber and, for the anastomoses, the SigniaTM laparoscopic stapler. This way, we surpass Hugo’s difficulties and disadvantages compared with DaVinci.
Despite these complex technical aspects, we safely did the assisted total colectomy spending surgical time, a patient hospital stay, and an excellent recovery similar or better to the laparoscopic total colectomy realized on our other patients with the same IMB, age range, and underlying the same pathology.
This can be stated only to selected patients. Generally, laparoscopic surgery is still the gold standard for centers with limited experience in assisted robotic colorectal surgery – much less operative time, fewer costs, and similar or better short outcomes regarding hospital stay and patient recovery.
6. Conclusions
In conclusion, the Hugo RAS platform is one of the emergent minimally invasive robotic platforms that can be used even in total colectomy if the proper patient selection is made. The placement choice of the arms and trocars was crucial to obtain a similar operative time of the single laparoscopic approach or DaVinci Xi boom-mounted system use.
The certification of Hugo’s new Instruments, such as energy devices and staplers, will make this platform even more competitive in the future.
Author Contributions
Conceptualization, M.D.S. and P.B.; methodology, M.D.S., and P.B.; writing—original draft preparation, M.D.S; writing—review and editing, M.D.S. and P.B..; supervision, M.D.S; project administration, M.D.S. All authors have read and agreed to the published version of the manuscript.”
Funding
Please add: This research received no external funding
Institutional Review Board Statement
The study did not require ethical approval.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper” if applicable.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Moghadamyeghaneh Z, Hanna MH, Carmichael JC, Pigazzi A, Stamos MJ, Mills S: Comparison of open, laparoscopic, and robotic approaches for total abdominal colectomy. Surgical endoscopy 2016, 30(7):2792-2798. [CrossRef]
- Kim HS, Oh BY, Chung SS, Lee RA, Noh GT: Short-term outcomes of single-incision robotic colectomy versus conventional multiport laparoscopic colectomy for colon cancer. Journal of robotic surgery 2023, 17(5):2351-2359. [CrossRef]
- Pervaiz SS, D’Adamo C, Mavanur A, Wolf JH: A retrospective comparison of 90-day outcomes, length of stay, and readmissions between robotic-assisted and laparoscopic colectomy. Journal of robotic surgery 2023, 17(5):2205-2209. [CrossRef]
- Jimenez-Rodriguez RM, Quezada-Diaz F, Tchack M, Pappou E, Wei IH, Smith JJ, Nash GM, Guillem JG, Paty PB, Weiser MR, Garcia-Aguilar J: Use of the Xi robotic platform for total abdominal colectomy: a step forward in minimally invasive colorectal surgery. Surgical endoscopy 2019, 33(3):966-971. [CrossRef]
- Hollandsworth HM, Stringfield S, Klepper K, Zhao B, Abbadessa B, Lopez NE, Parry L, Ramamoorthy S, Eisenstein S: Multiquadrant surgery in the robotic era: a technical description and outcomes for da Vinci Xi robotic subtotal colectomy and total proctocolectomy. Surgical endoscopy 2020, 34(11):5153-5159. [CrossRef]
- Ngu JC, Lin CC, Sia CJ, Teo NZ: A narrative review of the Medtronic Hugo RAS and technical comparison with the Intuitive da Vinci robotic surgical system. Journal of robotic surgery 2024, 18(1):99. [CrossRef]
- Prata F, Ragusa A, Tempesta C, Iannuzzi A, Tedesco F, Cacciatore L, Raso G, Civitella A, Tuzzolo P, Calle P, Pira M, Pino M, Ricci M, Fantozzi M, Prata S M, Anceschi U, Simone G, Scarpa R M, Papalia R. State of the Art in Robotic Surgery with Hugo RAS System: Feasibility, Safety and Clinical Applications. J Pers Med 2023, 13(8). [CrossRef]
- Brime Menendez R, Garcia Rojo E, Hevia Palacios V, Feltes Ochoa JA, Justo Quintas J, Lista Mateos F, Fraile A, Manfredi C, Belli S, Bozzini G, Romero Otero, J: Da Vinci vs. Hugo RAS for robot-assisted radical prostatectomy: a prospective comparative single-center study. World journal of urology 2024, 42(1):336. [CrossRef]
- Garcia Rojo E, Hevia Palacios V, Brime Menendez R, Feltes Ochoa JA, Justo Quintas J, Lista Mateos F, Touijer K, Romero Otero J: Da Vinci and Hugo RAS Platforms for robot-assisted partial nephrectomy: a preliminary prospective comparative analysis of the outcomes. Minerva Urol Nephrol 2024. [CrossRef]
- Ou HC, Marian L, Li CC, Juan YS, Tung MC, Shih HJ, Chang CP, Chen JT, Yang CH, Ou YC: Robot-Assisted Radical Prostatectomy by the Hugo Robotic-Assisted Surgery (RAS) System and the da Vinci System: A Comparison between the Two Platforms. Cancers 2024, 16(6). [CrossRef]
- Bianchi PP, Salaj A, Rocco B, Formisano G: First worldwide report on Hugo RAS surgical platform in right and left colectomy. Updates in surgery 2023, 75(3):775-780. [CrossRef]
- Romero-Marcos JM, Sampson-Davila JG, Cuenca-Gomez C, Altet-Torne J, Gonzalez-Abos S, Ojeda-Jimenez I, Galaviz-Sosa ML, Delgado-Rivilla S: Colorectal procedures with the novel Hugo RAS system: training process and case series report from a non-robotic surgical team. Surgical endoscopy 2024, 38(4):2160-2168. [CrossRef]
- Bourla C, Taoum C, Kante S, Mourregot A, Rouanet P, Colombo PE: Port placement strategies and management of the robotic system during total colectomy or total coloproctectomy for cancer - A video vignette. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland 2023, 25(8):1733-1735. [CrossRef]
Figure 1.
Clinical aspects: a) CHRPE in right eye ocular fundus b) Hundreds of adenomatous polyps and laterally spread lesions throughout the colon c) Small number of polyps in her rectum that were removed by endoscopy.
Figure 1.
Clinical aspects: a) CHRPE in right eye ocular fundus b) Hundreds of adenomatous polyps and laterally spread lesions throughout the colon c) Small number of polyps in her rectum that were removed by endoscopy.
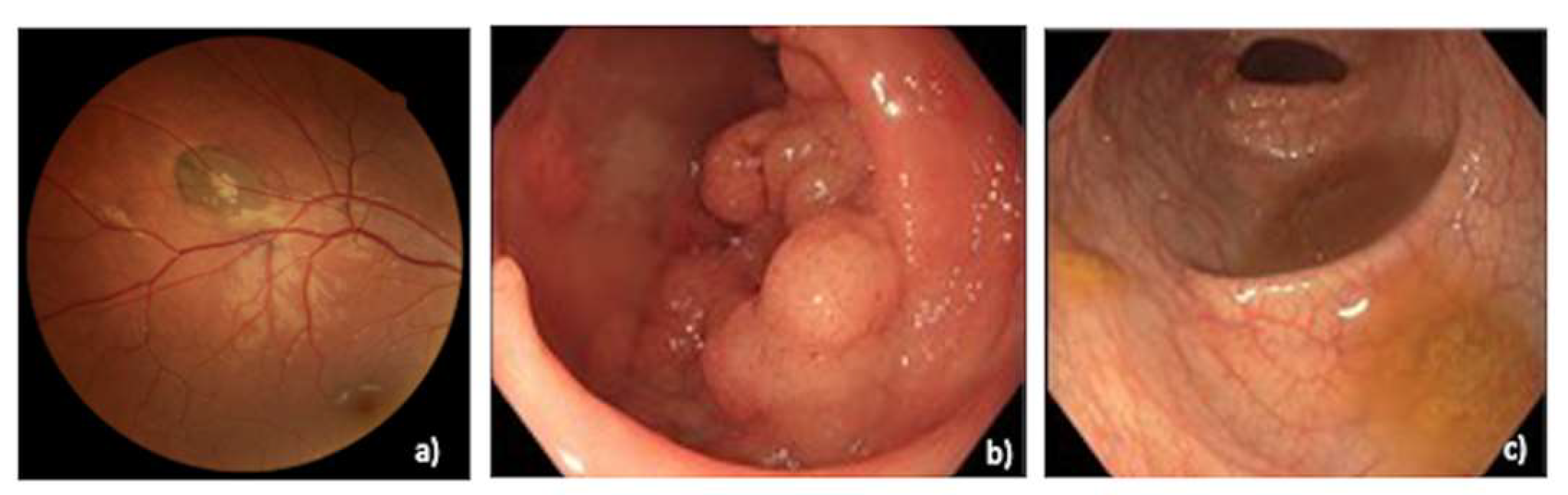
Figure 2.
Ports position and system configuration for right colectomy.
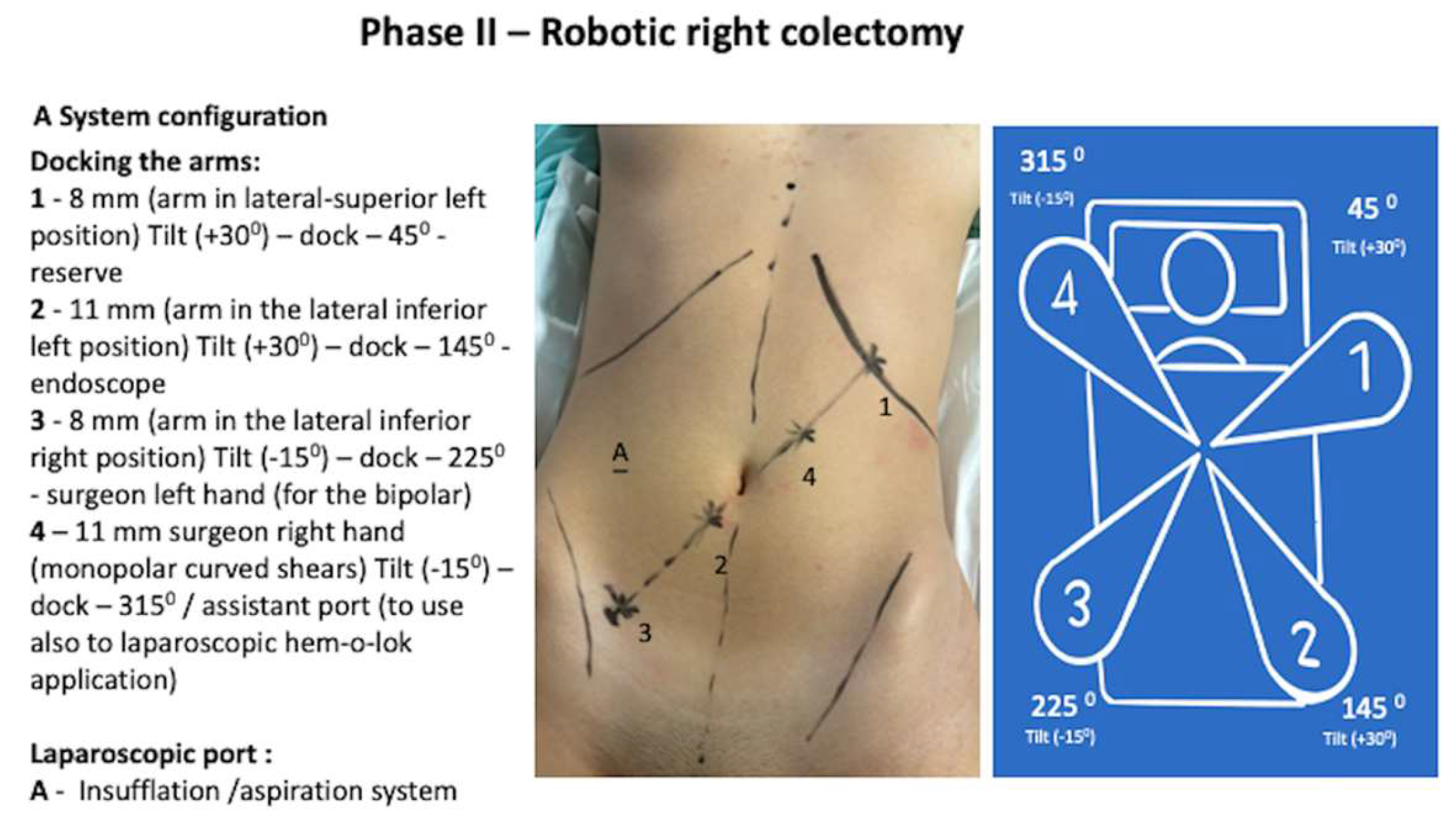
Figure 3.
Aspects of robotic right colectomy surgical steps.
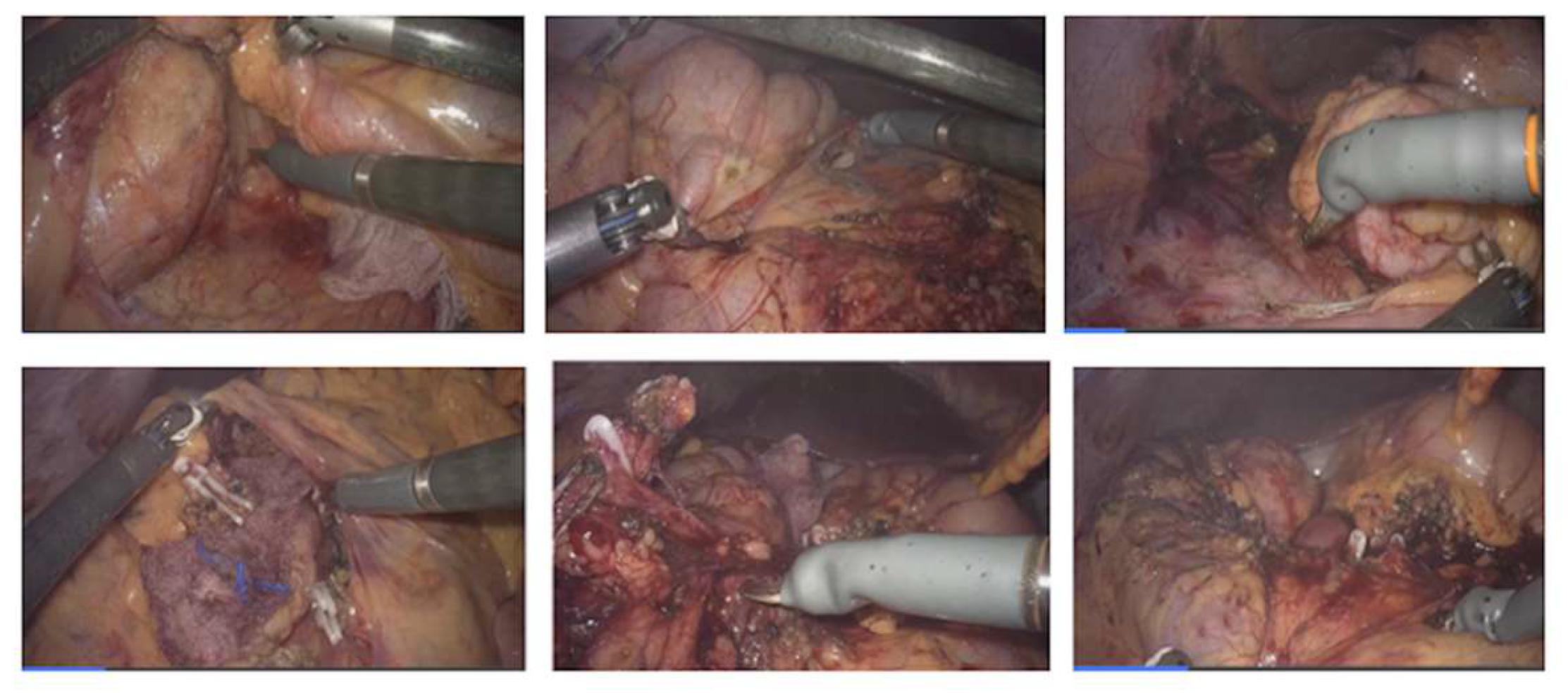
Figure 4.
Port position (the same) and System reconfiguration for left colectomy.
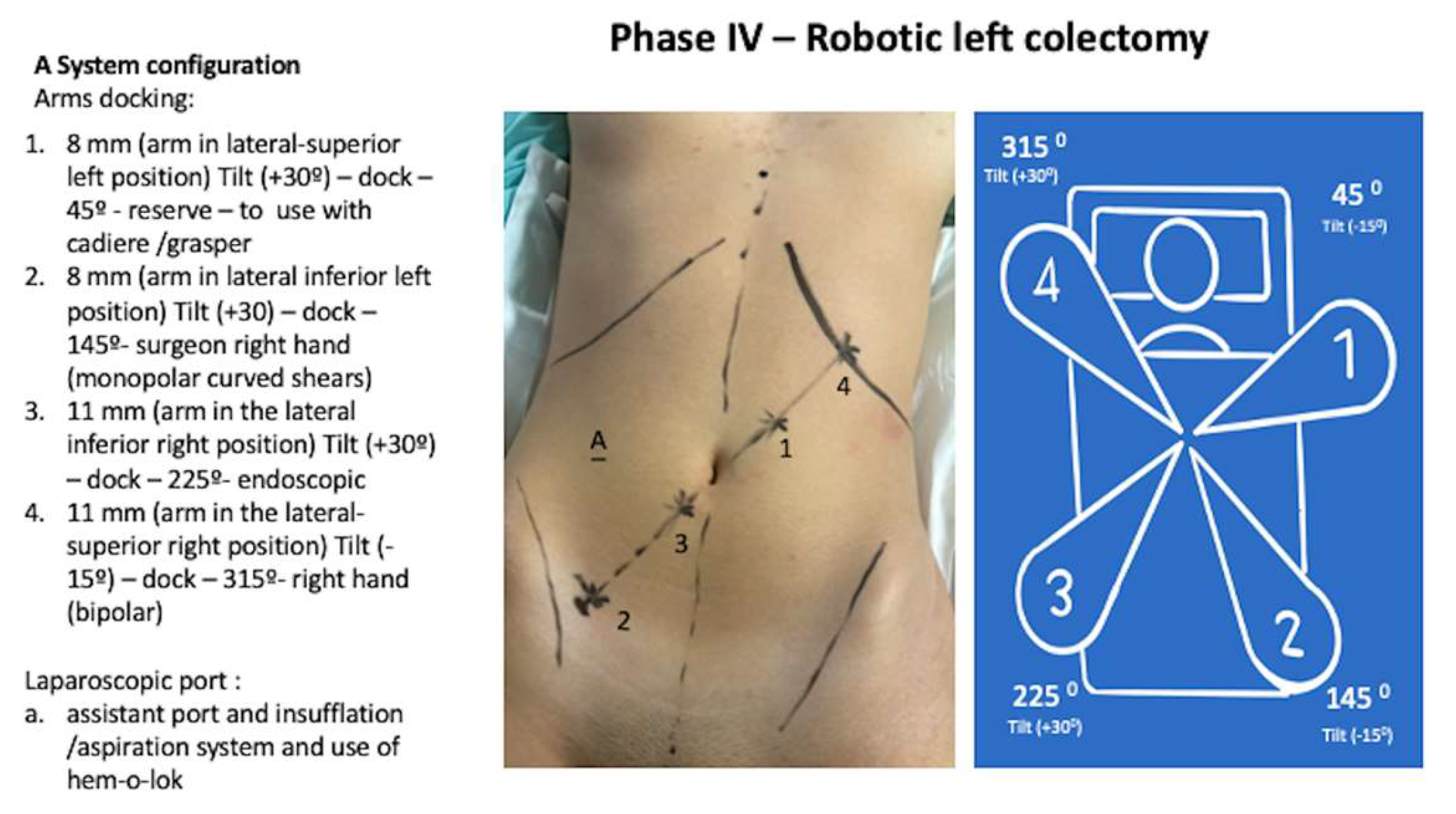
Figure 5.
Aspects of robotic left colectomy surgical steps.

Figure 6.
Surgical specimen (colon close and open).
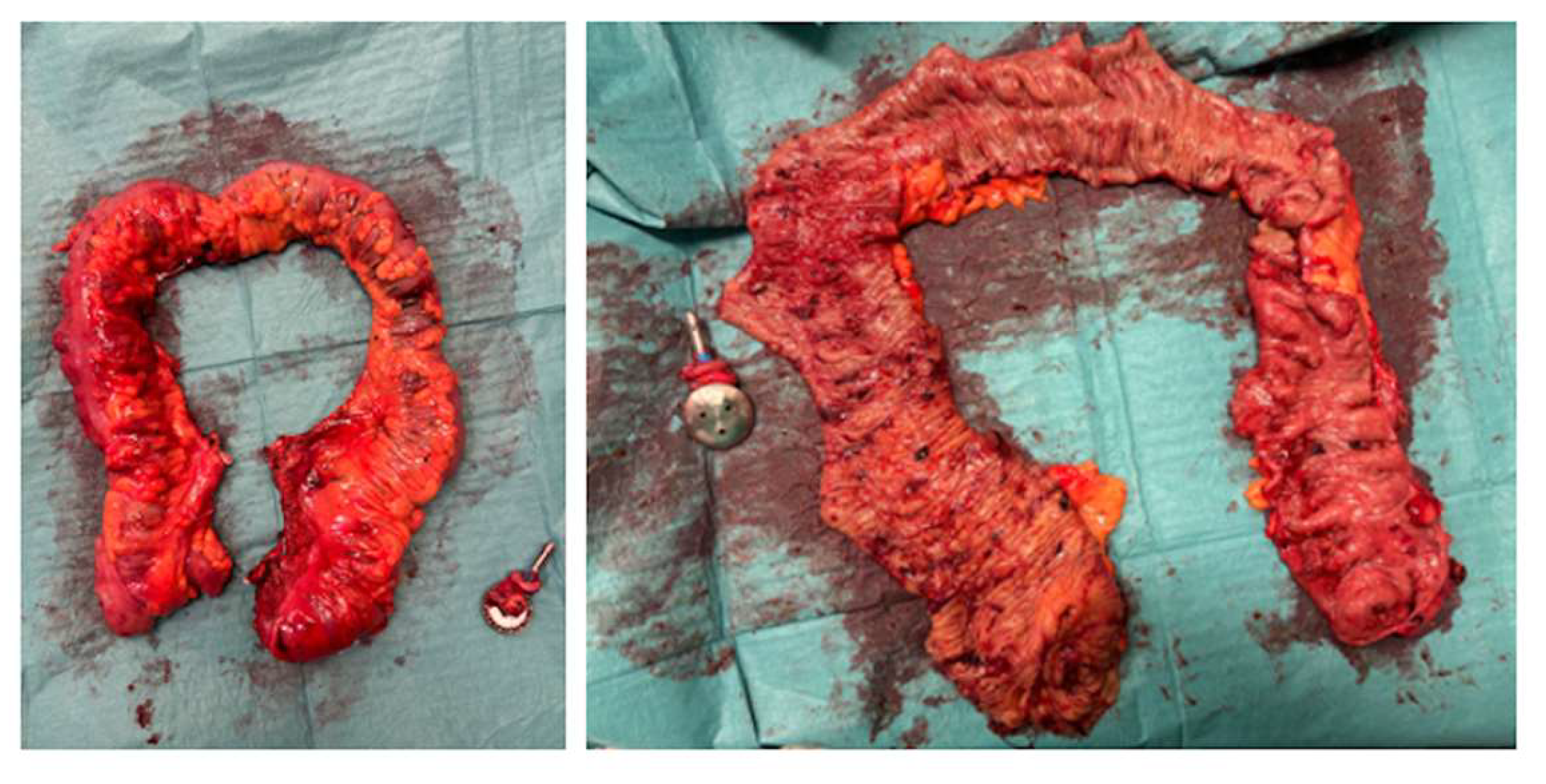
Figure 7.
Abdomen aspect thirty days after surgery.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



