Submitted:
06 September 2024
Posted:
09 September 2024
You are already at the latest version
Abstract
Purpose of review: In this review, we discuss the importance of digital health equity and how social determinants of health (and intersectionality with race, ethnicity, and gender) affect cardiovascular health-related outcomes in digital health trials. We propose strategies to improve digital health equity as we move to a digitally-connected world for healthcare applications and beyond.Recent findings: Digital health has immense promise to improve population health by reaching individuals in their homes, at their preferred times. However, initial data demonstrate decreased patient engagement and worse cardiovascular outcomes for racial and ethnic minorities, leading to unequal uptake of digital health technologies. In addition, while women generally have higher uptake of technology, they are less likely to be referred by clinicians for digital health interventions. We highlight several exemplar trials and analyze their methodology for replication in future digital health research.Summary: The promise of digital health equity has not been reached due to exclusionary practices. Specific focus must be placed on societal/governmental policies that enable digital inclusion, particularly of racial and ethnic minority populations and women, to ensure that the expansion of digital health technologies does not exacerbate existing health disparities.
Keywords:
digital health equity
; health disparities
; digital health
; digital accessibility
; digital divide
; cardiovascular disease
Introduction
Cardiovascular medicine is presently undergoing a digital revolution, with the rapid development and integration of digital health technologies throughout the continuum of health (see Figure 1) [1,2]. Digital health technologies comprise a wide variety of physical and software-based tools such as wearable sensors (e.g., smartwatches and continuous glucose monitors) [3,4], WiFi enabled remote-health monitoring (e.g., blood pressure and weight) [5,6], artificial intelligence algorithms and software applications that incorporate digital therapeutics (e.g., the My Heart Counts app and digital coaching prompts to increase physical activity) [7,8], and telemedicine/mobile health [9,10]. These digital health technologies are generally aimed at decentralizing care from the clinic/hospital setting to the homes and communities of the patients. Given the persistence of cardiovascular disease as the leading cause of morbidity and mortality in the developed world [11], these advancements in digital health technologies are welcome, as they offer clinicians increased quality and quantity of data to improve decision making. However, despite the promise of digital health technologies to improve equity in clinical care (by meeting patients in their own homes, at their own time), there is emerging evidence of widening disparities in clinical care, influenced by social determinants of health.
Social determinants of health refer to nonmedical factors that influence the conditions in which an individual is born, grows, works, lives, and ages [12]. Social determinants of health affect healthcare outcomes due to unequal distribution of resources and opportunities, which in turn result in health disparities [13]. Social determinants of health broadly fall into five categories: healthcare access and quality, education access and quality, social and community context, economic stability and the neighborhood, and the built environment [13]. Specific examples at the individual-level affecting cardiovascular health include (but are not limited to): gender identity, race, ethnicity, education, and employment.
Within digital health, it is well established that both the efficacy of digital interventions and the uptake of digital health technologies are influenced by the social determinants of health [14,15]. As new innovations and technologies are frequently adopted first by wealthier individuals, an “inverse care law” has been noted, whereby well-resourced individuals are both more likely to be aware of digital health technologies and incorporate these interventions to improve their health, with a resultant widening gap in health-related outcomes [16]. This limits the ability of digital health technologies to make a population-level impact by decreasing their reach to individuals and communities who would benefit the most from these innovations [17]. As a result, there remains a need to further improve the design and implementation of digital health technologies to ensure health equity.
In this review, we will discuss the importance of digital health equity in cardiovascular medicine in light of rapid technological developments over the past decade. We will also specifically discuss how race, ethnicity, and gender identity, as social determinants of health, affect outcomes in studies of digital health trials in cardiovascular medicine. Finally, we will propose several potential action items for future research and implementation to attempt to bridge the current gap in digital health equity.
Components of Digital Health Equity
Digital inclusion was coined as the “activities necessary to ensure equitable access to and use of information and communication technologies” in a seminal paper by Sieck et al [18]. Implicit in the concept of digital inclusion are two components: first, digital accessibility, or the ability of a patient to access the digital health technology (whether by smartphone or computer and including the potential need for broadband Internet service) [15,18]. Second, digital literacy, or the ability of a patient to use the digital health technology effectively (e.g., the ability to use a smartphone application effectively or connect their WiFi-enabled remote monitoring system to their home network) [15,18]. Due to the ubiquity of the internet in daily life – including housing, employment, and day-to-day functioning – digital inclusion was termed a “super social determinant of health,” as the ability to use and access online technologies influences all other social determinants of health [18].
The related concept of digital health equity arose at approximately the same time [14,15,19,20], with community recognition expanding rapidly as the SARS-CoV2 pandemic revealed inequity in health-related outcomes as much of the world adopted to a fully-digital healthcare environment [21,22,23,24]. Aligned with the ideal of health equity – where all people have the same opportunity to attain optimal health regardless of their social determinants of health – digital health equity strives to ensure that all digital technologies 1) improve health outcomes for all, 2) mitigate or reduce digital inequity, and 3) are equitably designed, developed, and implemented [25].
Within this context, digital determinants of health are an emerging concept that refers to the various factors within the digital environment that impacts individuals’ health outcomes, healthcare experiences and quality of life. While the precise definitions of digital determinants of health may vary, they share common elements: access to digital technologies, digital literacy, and the supporting infrastructure (broadband internet). These determinants also operate at multiple levels- individual, interpersonal, community and societal- and interact with the social determinants of health to influence how effectively individuals and communities are able to interact with digital health solutions [19,25,26]. Ultimately, the various definitions of digital determinants of health agree that they play a crucial role in enhancing or exacerbating health equity, depending on how they are addressed within the healthcare system (see Figure 2).
Although there is consensus on the broad definition of digital determinants of health, the definitions differ in their emphasis on specific elements. Some focus on technological factors like usability, personalization and algorithms as key drivers of health disparities [19]. Others emphasize social and communal aspects such as cultural beliefs, trust and digital bias that help shape interactions with digital technologies [25]. Additionally, some definitions include biological traits, though less commonly emphasized, as social constructs such as racism and ageism play a more significant role in health disparities [26]. Despite these differences, the definitions recognize the critical role of digital determinants of health in health equity, each through a slightly different lens.
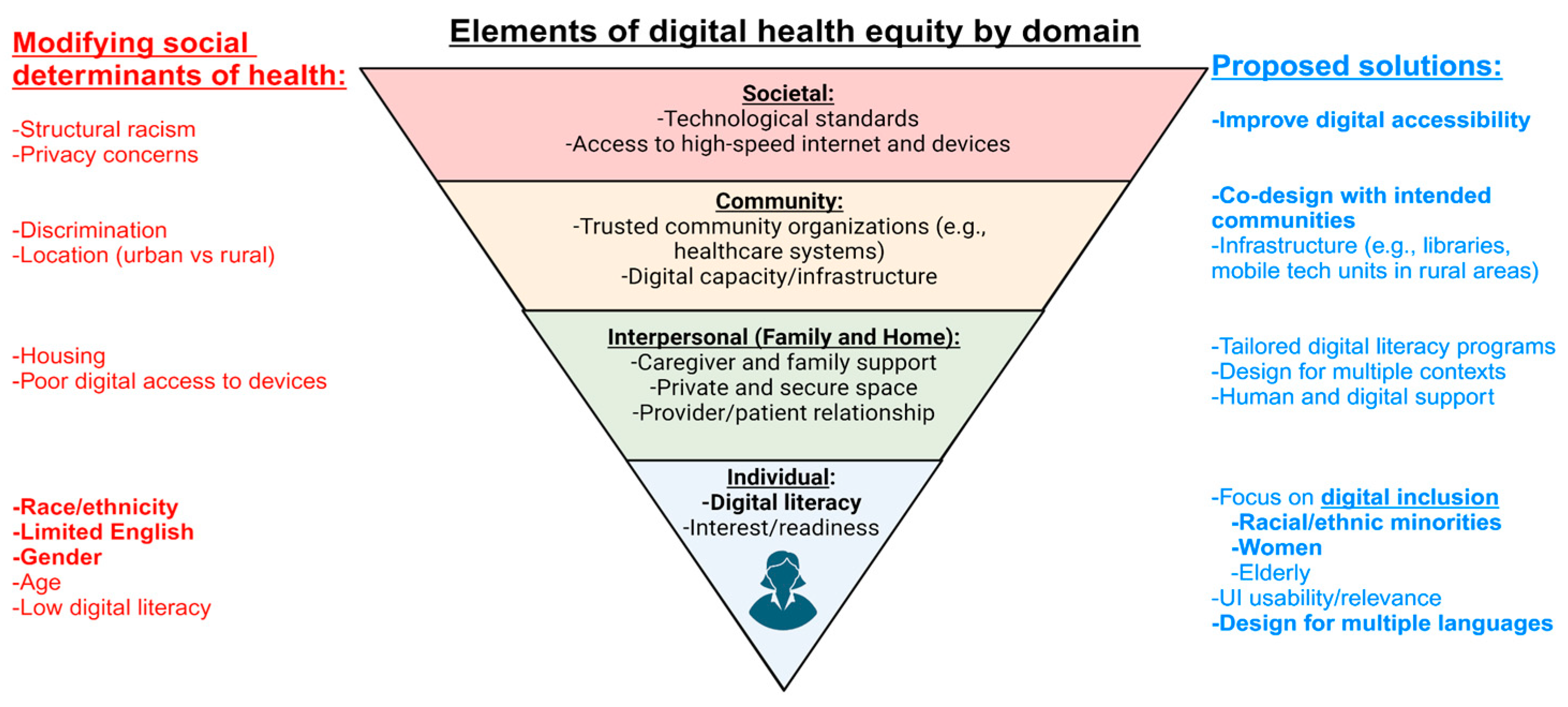
We conceptualize digital health equity as having different interconnected domains, represented by an inverted pyramid (see Figure 2), whereby each domain is affected by those “above” it (e.g., societal changes will have effects at the community, interpersonal, and individual level). Within this conceptualization, there are modifying social determinants of health at each domain level (though they too can affect downstream domains). We further propose solutions at each domain level (elaborated on in the Future Directions/Recommendations section to follow).
Social Determinants of Health Affect Health Outcomes in Cardiovascular Digital Health Studies:
Online Patient Portals and Telemedicine:
Based on cross-sectional data of 253,829 patients from the National Health Interview Survey from 2011-2018, the use of telemedicine or patient portals for medical care increased from 12.5% to 27.5% in the United States (US) [27]. However, non-Hispanic Black (thereafter referred to as “Black”) and Hispanic/Latinx patients were approximately 25% less likely to use online patient portals or telemedicine than White or Asian patients [27]. Correlated demographic factors were also associated with decreased online patient portal or telemedicine use: being born in a country other than the US, lower family income, lower education attainment, and lack of insurance were all associated with significantly decreased online patient portal or telemedicine use [27]. Interestingly, women were approximately 50% more likely to use online patient portals or telemedicine as compared with men [27]. Regarding cardiovascular disease, patients with obesity (+6%), prior atherosclerotic disease (+7%), diabetes (+27%), and hypertension (+35%) were more likely to use online patient portals or telemedicine, likely reflecting the need for intensive biomarker monitoring and clinical follow-up (see Figure 1) [27].
During the SARS-CoV2 pandemic, a cross-sectional study of telemedicine use in 90,991 patients at a tertiary care center in New York was performed, finding that Black and Hispanic/Latinx patients were approximately 40% and 20%, respectively, less likely to use telemedicine as compared to White patients [21]. The multivariable regression model also found that having Spanish as the preferred language was associated with a 54% decrease in telemedicine use [21]. Similar to the aforementioned trends across the US in 2011-2018 [27], women were 45% more likely to use telemedicine as compared with men, and those with a history of cardiac disease were 18% more likely to use telemedicine [21]. A separate analysis of the 2021 California Health Interview Survey participants found that patients with limited English proficiency were 37% less likely to use telemedicine and were 42% more likely to report a worse experience with video visits specifically, as compared with in-person visits [10].
Remote Monitoring of Cardiovascular Disease:
The rapid proliferation of WiFi-enabled devices that can send home-measurements of blood pressure, weight, and glucose levels to clinicians can lead to improved control of associated chronic conditions and decreased morbidity and mortality [1]. However, despite the increased prevalence and morbidity/mortality of cardiovascular disease in Black and Hispanic/Latinx patients, few digital health trials have reported or included diverse populations and fewer have been performed in racial and ethnic minority groups [28].
Continuous glucose monitors for management of diabetes largely eliminate the need for fingersticks and can lead to increased glycemic control [29]. However, prescription and use of continuous glucose monitors are uneven, with users typically younger and more likely to have private health insurance [30]. Cross-sectional analyses of patients with type 1 diabetes demonstrate that Black patients are less likely to use continuous glucose monitors even after adjustment for insurance status and type [31]. In addition, healthcare providers recommended digital health technologies at a significantly decreased rate to racial and ethnic minorities and those on public insurance [32]. Similarly, despite continuous glucose monitors now being recommended by major endocrinology societies for type 2 diabetes, prescription rates are significantly lower for Black and Hispanic/Latinx patients as compared with White patients [33]. Finally, despite the benefit of continuous glucose monitors for pregnant women with type 1 diabetes, the majority of women are not prescribed devices [34]. Moreover, in trials of pregnant women with type 1 diabetes referred to continuous glucose monitors that demonstrated superior maternal/fetal outcomes with tighter glucose control, the majority of patients were of European ancestry [35].
Hypertension affects a large proportion of US adults, with studies showing that Black and Hispanic/Latinx adults have lower awareness and control of their blood pressure [36]. A recent meta-analysis of 28 studies (representing 8,257 participants) of digital health technologies and hypertension management that emphasized recruitment of racial and ethnic minorities found significant decreases in systolic blood pressure at both 6- (-4.30 mmHg) and 12-months (-4.24 mmHg) of follow-up [6], in line with prior meta-analyses of randomized clinical trials [37]. Notably, 60% of the meta-analyzed participants were women, and subgroup analysis of studies that only recruited either Black or Hispanic/Latinx individuals did not find an effect on statistical heterogeneity, suggesting that digital health technologies improve hypertension management across all genders and racial and ethnic subgroups [6].
Heart failure affects >6.7 million people in the US, yet despite significant improvements in medication and device therapies, there remains a significant risk of rehospitalization and an overall decreased quality of life [38]. Despite the theoretical benefit of telemedicine in heart failure (managing volume status to prevent rehospitalization), large randomized trials have failed to demonstrate benefit in reducing heart failure hospitalizations [39,40,41]. Recent meta-analysis of 10,981 patients from 28 trials did demonstrate a modest improvement of telemedicine in reducing heart failure hospitalizations and improving quality of life [42]. However, this meta-analysis did not consider sensitivity analyses by race, ethnicity, or gender [42]. Due to the SARS-CoV2 pandemic, care of heart failure patients shifted toward telemedicine, with telemedicine visits showing similar efficacy to in-person visits in reducing mortality and hospitalization [43]. However, visual contact (e.g., video visits) were found to be significantly superior to telephone visits for the prevention of both Emergency Department visits and death [43]. While no direct sensitivity analyses by race, ethnicity, or gender were included, we note that White (>81%) men (>65%) comprised the majority of the analyzed cohort and that Black patients had a higher proportion of telephone versus in-person visits (18.5% versus 15.2%) [43]. Moreover, Hispanic/Latinx patients only comprised 1.6-1.9% of the studied cohort [43].
Given that weight changes have only a 10-20% sensitivity for episodes of heart failure exacerbation [44], there has been a shift toward devices that can assess ambulatory cardiac pressures. One of the best studied devices is CardioMEMS, an implantable pulmonary artery pressure monitor that has shown efficacy in reducing heart failure hospitalizations [45]. In a follow-up randomized trial that was affected by the SARS-CoV2 pandemic, there were significant interactions between CardioMEMS use among women and Black patients, with both groups deriving greater cardiovascular benefit as compared with men and White patients, respectively [46]. This has been hypothesized to be due to implicit bias, whereby women and Black patients are referred to trials for heart failure at greater symptom stages and hence, derive greater benefit from the intervention [47]. Post-approval studies have noted a consistent effect by gender and race/ethnicity [48,49], with one analysis of a national registry redemonstrating a potentially greater benefit of CardioMEMS in women as compared with men [50]. However, despite these benefits, the national registry data indicates that there is significantly lower utilization of CardioMEMS in women compared with men, with no significant differences observed by race and ethnicity [50]. These findings highlight the ongoing disparities in adoption of heart failure technologies, warranting further investigation and more targeted interventions.
Smartphone Applications and Wearables:
Based on 2023 surveys of US adults, smartphone use has rapidly proliferated throughout the country, with >90% of women (compared with >91% of men), >84% and >91% of Black and Hispanic/Latinx adults (compared with >91% of White adults) owning such a device [51]. Trends of decreased smartphone ownership were associated with lower educational attainment and income [51]. The use of smartphones and associated wearable devices to track and monitor health was assessed in a recent national survey, finding that 46% and 42% of the general population and those with or at-risk for cardiovascular disease, respectively, tracked their health goals with smartphones and/or wearable devices [52]. Younger patients of higher socioeconomic status and educational attainment were more likely to use smartphones and/or wearable devices [52]. Notably, both women and Black adults were also more likely to use their smartphones and/or wearable devices to track their health goals [52]. When accounting for socioeconomic differences, Black individuals reported higher usage of smart devices for health tracking compared to White individuals, despite no significant difference when only demographic factors were considered. Barriers to adoption included cost, lack of knowledge about the devices and reluctance to commit to usage. Majority of patients expressed interest in using digital health devices and learning how it could improve their health, however, cost and understanding were significant barriers that prevented them from realizing the full benefits of wearable digital devices [53].
Early studies into the use of smartphone applications have shown that they can increase short-term physical activity [8], with personalized text-prompts demonstrating superiority to a one-size-fits-all approach [7]. However, numerous other studies of smartphone-based interventions have shown no significant improvements [54] or waning effects over-time, likely due to decreased user engagement [55]. Moreover, we note that the vast majority of the studies in this field are catered primarily to a highly-educated and tech-savvy population, highlighting the importance of recognizing the inverse care law [16].
Challenges and Barriers:
Currently, digital health lacks a unified nomenclature for digital health equity. This is perhaps best exemplified by the digital determinants of health, of which we found at least three different definitions [19,25,26]. Moreover, what is meant by digital health varies from group to group, with some including only smartphone applications and wearables and others referring to patient portals and telehealth/telemedicine. As a result, a codified statement from the field clearly defining nomenclature is necessary to advance the field.
Separately, with the rapid technological development and shift of clinical care to the digital realm, there is a rising concern for data security and privacy issues [56]. The diversity and volume of health-related data make it an attractive target for cyber-attacks. Data breaches not only erode patient trust and confidence in healthcare systems and providers, but also have deleterious individual-level effects. As we continue to transition to ever-more digital environments for clinical care, the integration of robust cybersecurity strategies will be of high priority to ensure patient privacy and data security [56].
Future Directions/Recommendations:
Digital Accessibility through Societal and Governmental Policy:
Given the importance of digital inclusion in our modern, highly-connected society, it is imperative that governments and regulatory agencies act to ensure digital accessibility for all. This is primarily achieved at the societal domain (see Figure 2) via policies that enable digital health equity: nationwide high-speed internet access and subsidized device ownership. Digital redlining, or the preferential installation of high-speed internet in high-income communities thereby limiting digital accessibility in lower income and higher racial and ethnic minority neighborhoods, continues to be prevalent in the US [57]. To combat this, the US government allows those on federal assistance to obtain discounted smartphones and internet service through the Lifeline program; however, service is often unreliable and there is a cap on data and minutes, limiting usefulness to low-income individuals [58]. We note that the federal Affordable Connectivity Program was passed in 2022, which will provide discounted high-speed internet and devices in conjunction with a renewal and broadening of eligibility for the Lifeline program in the US. However, given the known problems with the Lifeline program and ongoing digital redlining, we believe that further legislation is needed to ensure digital accessibility for all within the US and ensure digital health equity.
Community Co-Design of Digital Health Interventions:
Community co-design, or the engagement and integration of the specific preferences of the intended audience prior to and during the design of a digital health intervention, is a common theme in trials that demonstrated efficacy in improving cardiovascular health [59,60,61]. Community co-design improves usability, acceptability, and adoption among targeted populations and is especially important when engaging with communities historically marginalized by clinical research (see Figure 2) [62]. As an example, the Fostering African American Improvement in Total Health (FAITH!) trial developed a digital health intervention to improve overall cardiovascular health by engaging with local churches, creating a diverse advisory board for oversight, and frequently engaging in social events to overcome barriers caused by social determinants of health [59].
Additional benefits of community-based interventions, as highlighted in the MOYO study and through the usage of Community-Based Participatory Research, include a focus on addressing community-identified social, structural, environmental, and policy priorities. By centering the design and implementation of digital health technologies around the specific needs and challenges of the community, this approach ensures that interventions are directly relevant and effective. This co-design methodology not only enhances the effectiveness of the technology but also provides a deeper understanding of the potential barriers and facilitators to community adoption, ultimately supporting more successful and sustainable health outcomes [60].
Focus on Digital Inclusion:
At the individual level, there is a need to prioritize specific groups that suffer health-related disparities to ensure digital inclusion of all peoples; in our review, we focus on women and racial and ethnic minorities, but this includes the elderly, among many other potential patient populations. Moving forward, it is crucial to over-represent and specifically recruit these groups in trials of digital health technologies to ensure that the inverse care law does not become a self-fulfilling prophecy.
Women are more likely to use digital health technologies, but their cardiovascular health symptoms are often minimized leading to delays in diagnostics and lower levels of evidence-based referrals and therapeutics [63,64,65,66]. Even in cases with clear inclusion criteria and strong evidence of benefit (e.g., continuous glucose monitors for pregnant women with type 1 diabetes), provider awareness and prompt referral is lacking, leading to continued health-related disparities [34]. These gaps in recognizing cardiovascular symptoms and risks in women across the lifespan may explain the consistent benefit that is observed with CardioMEMS implantation. Combined with the lower referral rate in women, this suggests that women are often referred for the device only when their symptoms are more advanced as compared with men [47,50].
Similarly, although the majority of digital health studies demonstrated worse health-related outcomes in Black and Hispanic/Latinx patients, trials that specifically attempted to recruit a diverse population demonstrated consistent benefit of their digital interventions across racial and ethnic groups [6,50]. This in part reflects the community co-design of individual trials [59,67], but also emphasizes the importance of creating a broad evidence base in clinical trials that can then be extrapolated into clinical practice. As an example, in part due to over-recruitment of racial and ethnic minority populations during the trial phase of CardioMEMS, post-approval analyses have not found significant differences in referrals for either Black or Hispanic/Latinx patients for the device [48,49,50].
The evidence from federally qualified health centers strongly supports the need to address barriers that prevent the adoption of digital health technologies among underserved populations. While patients in these settings expressed a clear motivation to use digital health tools, factors such as cost, lack of information, and the need for targeted education and support were obstacles. These findings emphasize the importance of providing accessible educational materials and high-touch methods such as personalized guidance on using fitness trackers, language support, and assistance [53]. Addressing these barriers is crucial to ensuring that patients from disadvantaged communities can fully benefit from digital health innovations.
Multilingual Digital Health Technology Development:
We note that for the vast majority of digital health trials, being able to read/communicate in English was an inclusion criteria [68], explicitly excluding a large proportion of potential Hispanic/Latinx patients (among numerous other racial and ethnic minorities). One potential solution is to employ community health workers that are fluent in Spanish and culturally sensitive to the targeted Hispanic/Latinx population, which have been shown to improve uptake and acceptability of digital health interventions in prior work [69]. However, a more inclusive approach would involve developing multilingual digital health technologies and incorporating elements of the community co-design method described above. As an example, an early trial of physical activity promotion in the Hispanic/Latinx community tested Carmen, a virtual Spanish-speaking coach that could only be interacted with at libraries that participants would commute to/from, versus trained community health workers, finding that both approaches significantly increased physical activity levels [70,71,72]. With the rapid advances in large language models fluent in Spanish, similar approaches of designing fluent and culturally-sensitive digital health technologies should be possible in the near future.
Moreover, ensuring that the nomenclature used in the field and in studies is culturally nuanced is vitally important. Various studies have highlighted how terminology, particularly in relation to devices, can create barriers to adoption among marginalized populations. For example, Spanish-speaking patients expressed hesitation toward using "fitness trackers" due to concerns about potential surveillance or tracking of their movements [53]. This not only reduces adoption rates but also poses challenges for recruiting these populations into studies, as such concerns can deter participation.
Conclusions:
Digital health technologies have the potential to transform cardiovascular medicine by incorporating vast amounts of health-related data to better inform and personalize clinical decision making to each individual patient. However, the promise of digital health must be tempered with early data that suggests that it may worsen existing health disparities, particularly in racial and ethnic minorities and women. By being mindful of how the social determinants of health can affect cardiovascular outcomes in trials of digital health technologies, clinicians and researchers will be better equipped to navigate the complex pathways of societal, community, interpersonal, and individual factors, on the quest to strive for digital health equity.
Funding
D.S.K. is supported by the Wu-Tsai Human Performance Alliance as a Clinician-Scientist Fellow, the Stanford Center for Digital Health as a Digital Health Scholar, the Robert A. Winn Diversity in Clinical Trials Career Development Award, and NIH 1L30HL170306. F.R. was funded by grants from the NIH National Heart, Lung, and Blood Institute (R01HL168188; R01HL167974; R01HL169345), the American Heart Association/Harold Amos Medical Faculty Development program, and the Doris Duke Foundation (Grant #2022051).
Conflicts of Interest
F.R. reports equity from Carta Healthcare and HealthPals, and consulting fees from HealthPals, Novartis, NovoNordisk, Esperion Therapeutics, Movano Health, Kento Health, Inclusive Health, Edwards, Arrowhead Pharmaceuticals, HeartFlow, iRhythm, and Cleerly outside the submitted work. D.S.K. reports grant support from Amgen.
References
- Martin, S.S. Centennial Collection: Health Applications of Digital Technologies. Circulation 2024, 149, 1701–1703. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.; Shandhi, M.M.H.; Master, H.; Dunn, J.; Brittain, E. Wearable Devices in Cardiovascular Medicine. Circ Res. 2023, 132, 652–670. [Google Scholar] [CrossRef] [PubMed]
- Perez, M.V.; Mahaffey, K.W.; Hedlin, H.; Rumsfeld, J.S.; Garcia, A.; Ferris, T.; et al. Large-Scale Assessment of a Smartwatch to Identify Atrial Fibrillation. N Engl J Med. 2019, 381, 1909–1917. [Google Scholar] [CrossRef] [PubMed]
- Prahalad, P.; Scheinker, D.; Desai, M.; Ding, V.Y.; Bishop, F.K.; Lee, M.Y.; et al. Equitable implementation of a precision digital health program for glucose management in individuals with newly diagnosed type 1 diabetes. Nat Med. 2024, 30, 2067–2075. [Google Scholar] [CrossRef] [PubMed]
- Azizi, Z.; Broadwin, C.; Islam, S.; Schenk, J.; Din, N.; Hernandez, M.F.; et al. Digital Health Interventions for Heart Failure Management in Underserved Rural Areas of the United States: A Systematic Review of Randomized Trials. J Am Hear Assoc: Cardiovasc Cerebrovasc Dis. 2024, 13, e030956. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.E.; Mszar, R.; Grimshaw, A.A.; Gunderson, C.G.; Onuma, O.K.; Lu, Y.; et al. Digital Health Interventions for Hypertension Management in US Populations Experiencing Health Disparities. JAMA Netw Open. 2024, 7, e2356070. [Google Scholar] [CrossRef] [PubMed]
- Javed, A.; Kim, D.S.; Hershman, S.G.; Shcherbina, A.; Johnson, A.; Tolas, A.; et al. Personalized digital behaviour interventions increase short-term physical activity: A randomized control crossover trial substudy of the MyHeart Counts Cardiovascular Health Study. Eur Hear J - Digit Heal. 2023, 4, 411–419. [Google Scholar] [CrossRef]
- Shcherbina, A.; Hershman, S.G.; Lazzeroni, L.; King, A.C.; O’Sullivan, J.W.; Hekler, E.; et al. The effect of digital physical activity interventions on daily step count: A randomised controlled crossover substudy of the MyHeart Counts Cardiovascular Health Study. Lancet Digital Heal. 2019, 1, e344–e352. [Google Scholar] [CrossRef]
- Creber, R.M.; Dodson, J.A.; Bidwell, J.; Breathett, K.; Lyles, C.; Still, C.H.; et al. Telehealth and Health Equity in Older Adults With Heart Failure: A Scientific Statement From the American Heart Association. Circ: Cardiovasc Qual Outcomes. 2023, 16, e000123. [Google Scholar]
- Rodriguez, J.A.; Khoong, E.C.; Lipsitz, S.R.; Lyles, C.R.; Bates, D.W.; Samal, L. Telehealth Experience Among Patients With Limited English Proficiency. JAMA Netw Open. 2024, 7, e2410691. [Google Scholar] [CrossRef]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [PubMed]
- Social determinants of health [Internet]. Available online: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1 (accessed on 6 August 2024).
- Social Determinants of Health - Healthy People 2030 | health.gov [Internet]. Available online: https://health.gov/healthypeople/priority-areas/social-determinants-health (accessed on 6 August 2024).
- Lyles, C.R.; Wachter, R.M.; Sarkar, U. Focusing on Digital Health Equity. JAMA 2021, 326, 1795–1796. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.A.; Clark, C.R.; Bates, D.W. Digital Health Equity as a Necessity in the 21st Century Cures Act Era. JAMA. 2020, 323, 2381–2382. [Google Scholar] [CrossRef] [PubMed]
- Lancet, T. 50 years of the inverse care law. Lancet. 2021, 397, 767. [Google Scholar] [CrossRef]
- Safavi, K.; Mathews, S.C.; Bates, D.W.; Dorsey, E.R.; Cohen, A.B. Top-Funded Digital Health Companies And Their Impact On High-Burden, High-Cost Conditions. Heal Aff. 2019, 38, 115–123. [Google Scholar] [CrossRef]
- Sieck, C.J.; Sheon, A.; Ancker, J.S.; Castek, J.; Callahan, B.; Siefer, A. Digital inclusion as a social determinant of health. npj Digit Med. 2021, 4, 52. [Google Scholar] [CrossRef]
- Richardson, S.; Lawrence, K.; Schoenthaler, A.M.; Mann, D. A framework for digital health equity. npj Digit Med. 2022, 5, 119. [Google Scholar] [CrossRef]
- Lyles, C.R.; Nguyen, O.K.; Khoong, E.C.; Aguilera, A.; Sarkar, U. Multilevel Determinants of Digital Health Equity: A Literature Synthesis to Advance the Field. Annu Rev Public Heal. 2022, 44, 383–405. [Google Scholar] [CrossRef]
- Chunara, R.; Zhao, Y.; Chen, J.; Lawrence, K.; Testa, P.A.; Nov, O.; et al. Telemedicine and Healthcare Disparities: A cohort study in a large healthcare system in New York City during COVID-19. J Am Méd Inform Assoc. 2020, 28, 33–41. [Google Scholar] [CrossRef]
- Ramsetty, A.; Adams, C. Impact of the digital divide in the age of COVID-19. J Am Méd Inform Assoc. 2020, 27, 1147–1148. [Google Scholar] [CrossRef]
- Crawford, A.; Serhal, E. Digital Health Equity and COVID-19, The Innovation Curve Cannot Reinforce the Social Gradient of Health. J Méd Internet Res. 2020, 22, e19361. [Google Scholar] [CrossRef]
- Budd, J.; Miller, B.S.; Manning, E.M.; Lampos, V.; Zhuang, M.; Edelstein, M.; et al. Digital technologies in the public-health response to COVID-19. Nat Med. 2020, 26, 1183–1192. [Google Scholar] [CrossRef]
- Lawrence, K. Digital Health. 2022, 121–130.
- Chidambaram, S.; Jain, B.; Jain, U.; Mwavu, R.; Baru, R.; Thomas, B.; et al. An introduction to digital determinants of health. PLOS Digit Heal. 2024, 3, e0000346. [Google Scholar] [CrossRef]
- Mahajan, S.; Lu, Y.; Spatz, E.S.; Nasir, K.; Krumholz, H.M. Trends and Predictors of Use of Digital Health Technology in the United States. Am J Med. 2021, 134, 129–134. [Google Scholar] [CrossRef]
- Hernandez, M.F.; Rodriguez, F. Health Techequity: Opportunities for Digital Health Innovations to Improve Equity and Diversity in Cardiovascular Care. Curr Cardiovasc Risk Rep. 2023, 17, 1–20. [Google Scholar] [CrossRef]
- Avoke, D.; Elshafeey, A.; Weinstein, R.; Kim, C.H.; Martin, S.S. Digital Health in Diabetes and Cardiovascular Disease. Endocr Res. 2024, 49, 124–136. [Google Scholar] [CrossRef]
- Mayberry, L.S.; Guy, C.; Hendrickson, C.D.; McCoy, A.B.; Elasy, T. Rates and Correlates of Uptake of Continuous Glucose Monitors Among Adults with Type 2 Diabetes in Primary Care and Endocrinology Settings. J Gen Intern Med. 2023, 38, 2546–2552. [Google Scholar] [CrossRef]
- Noor, N.; Kamboj, M.K.; Triolo, T.; Polsky, S.; McDonough, R.J.; Demeterco-Berggren, C.; et al. Hybrid Closed-Loop Systems and Glycemic Outcomes in Children and Adults With Type 1 Diabetes: Real-World Evidence From a U.S.-Based Multicenter Collaborative. Diabetes Care. 2022, 45, e118–e119. [Google Scholar] [CrossRef]
- Odugbesan, O.; Addala, A.; Nelson, G.; Hopkins, R.; Cossen, K.; Schmitt, J.; et al. Implicit Racial–Ethnic and Insurance-Mediated Bias to Recommending Diabetes Technology: Insights from T1D Exchange Multicenter Pediatric and Adult Diabetes Provider Cohort. Diabetes Technol Ther. 2022, 24, 619–627. [Google Scholar] [CrossRef]
- Isaacs, D.; Bellini, N.J.; Biba, U.; Cai, A.; Close, K.L. Health Care Disparities in Use of Continuous Glucose Monitoring. Diabetes Technol Ther. 2021, 23, S-81–S-87. [Google Scholar] [CrossRef]
- Venkatesh, K.K.; Powe, C.E.; Buschur, E.; Wu, J.; Landon, M.B.; Gabbe, S.; et al. Disparities in Continuous Glucose Monitoring Use Among Women of Reproductive Age with Type 1 Diabetes in the T1D Exchange. Diabetes Technol Ther. 2023, 25, 201–205. [Google Scholar] [CrossRef]
- Feig, D.S.; Donovan, L.E.; Corcoy, R.; Murphy, K.E.; Amiel, S.A.; Hunt, K.F.; et al. Continuous glucose monitoring in pregnant women with type 1 diabetes (CONCEPTT): A multicentre international randomised controlled trial. Lancet. 2017, 390, 2347–2359. [Google Scholar] [CrossRef]
- Aggarwal, R.; Chiu, N.; Wadhera, R.K.; Moran, A.E.; Raber, I.; Shen, C.; et al. Racial/Ethnic Disparities in Hypertension Prevalence, Awareness, Treatment, and Control in the United States, 2013 to 2018. Hypertension 2021, 78, 1719–1726. [Google Scholar] [CrossRef]
- Lu, X.; Yang, H.; Xia, X.; Lu, X.; Lin, J.; Liu, F.; et al. Interactive Mobile Health Intervention and Blood Pressure Management in Adults. Hypertension. 2019, 74, 697–704. [Google Scholar] [CrossRef]
- Stevenson, L.W.; Ross, H.J.; Rathman, L.D.; Boehmer, J.P. Remote Monitoring for Heart Failure Management at Home. J Am Coll Cardiol. 2023, 81, 2272–2291. [Google Scholar] [CrossRef]
- Chaudhry, S.I.; Mattera, J.A.; Curtis, J.P.; Spertus, J.A.; Herrin, J.; Lin, Z.; Phillips, C.O.; Hodshon, B.V.; et al. Telemonitoring in Patients with Heart Failure. N Engl J Med. 2010, 363, 2301–2309. [Google Scholar] [CrossRef]
- Ong, M.K.; Romano, P.S.; Edgington, S.; Aronow, H.U.; Auerbach, A.D.; Black, J.T.; et al. Effectiveness of Remote Patient Monitoring After Discharge of Hospitalized Patients With Heart Failure: The Better Effectiveness After Transition–Heart Failure (BEAT-HF) Randomized Clinical Trial. JAMA Intern Med. 2016, 176, 310. [Google Scholar] [CrossRef]
- Koehler, F.; Winkler, S.; Schieber, M.; Sechtem, U.; Stangl, K.; Böhm, M.; et al. Telemedical Interventional Monitoring in Heart Failure (TIM-HF), a randomized, controlled intervention trial investigating the impact of telemedicine on mortality in ambulatory patients with heart failure: Study design. Eur J Hear Fail. 2010, 12, 1354–1362. [Google Scholar] [CrossRef]
- Takeda, A.; Martin, N.; Taylor, R.S.; Taylor, S.J. Disease management interventions for heart failure. Cochrane Database Syst Rev. 2019, 2019, CD002752. [Google Scholar] [CrossRef]
- Sammour, Y.; Main, M.L.; Austin, B.A.; Magalski, A.; Sperry, B.W. Outpatient Management of Guideline-Directed Medical Therapy for Heart Failure Using Telehealth: A Comparison of In-Office, Video, and Telephone Visits. J Card Fail. 2022, 28, 1222–1226. [Google Scholar] [CrossRef]
- Adamson, P.B. Pathophysiology of the transition from chronic compensated and acute decompensated heart failure: New insights from continuous monitoring devices. Curr Hear Fail Rep. 2009, 6, 287. [Google Scholar] [CrossRef]
- Abraham, W.T.; Adamson, P.B.; Bourge, R.C.; Aaron, M.F.; Costanzo, M.R.; Stevenson, L.W.; et al. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: A randomised controlled trial. Lancet. 2011, 377, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Lindenfeld, J.; Zile, M.R.; Desai, A.S.; Bhatt, K.; Ducharme, A.; Horstmanshof, D.; et al. Haemodynamic-guided management of heart failure (GUIDE-HF): A randomised controlled trial. Lancet. 2021, 398, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- Mastoris, I.; DeFilippis, E.M.; Martyn, T.; Morris, A.A.; Spall, H.G.V.; Sauer, A.J. Remote Patient Monitoring for Patients with Heart Failure: Sex- and Race-based Disparities and Opportunities. Card Fail Rev. 2023, 9, e02. [Google Scholar] [CrossRef] [PubMed]
- DeFilippis, E.M.; Henderson, J.; Axsom, K.M.; Costanzo, M.R.; Adamson, P.B.; Miller, A.B.; et al. Remote Hemodynamic Monitoring Equally Reduces Heart Failure Hospitalizations in Women and Men in Clinical Practice. Circ: Hear Fail. 2021, 14, e007892. [Google Scholar]
- Paul, L.D.; Moinul, S.; Urina-Jassir, M.; Gopal, D.M.; Ayalon, N. Expanding Pulmonary Artery Pressure Monitoring to Racially and Socially Diverse Populations: A Pilot CardioMEMS Program. Am J Méd Sci. 2024, 368, 408–410. [Google Scholar] [CrossRef]
- Markson, F.; Abe, T.A.; Adedinsewo, D.; Olanipekun, T.; Shamaki, G.R.; Kesiena, O.; et al. Sex Differences in CardioMEMS Utilization and Impact on Readmissions and Mortality in Heart Failure Patients. JACC: Hear Fail. 2023, 11, 1760–1762. [Google Scholar] [CrossRef]
- Center, P.R. Demographics of Mobile Device Ownership and Adoption in the United States [Internet]. Available online: https://www.pewresearch.org/internet/fact-sheet/mobile/.
- Aminorroaya, A.; Dhingra, L.S.; Nargesi, A.A.; Oikonomou, E.K.; Krumholz, H.M.; Khera, R. Use of Smart Devices to Track Cardiovascular Health Goals in the United States. JACC: Adv. 2023, 2, 100544. [Google Scholar] [CrossRef]
- Holko, M.; Litwin, T.R.; Munoz, F.; Theisz, K.I.; Salgin, L.; Jenks, N.P.; et al. Wearable fitness tracker use in federally qualified health center patients: Strategies to improve the health of all of us using digital health devices. npj Digit Med. 2022, 5, 53. [Google Scholar] [CrossRef]
- Victoria-Castro, A.M.; Martin, M.L.; Yamamoto, Y.; Melchinger, H.; Weinstein, J.; Nguyen, A.; et al. Impact of Digital Health Technology on Quality of Life in Patients With Heart Failure. JACC: Hear Fail. 2024, 12, 336–348. [Google Scholar] [CrossRef]
- Dorsch, M.P.; Farris, K.B.; Rowell, B.E.; Hummel, S.L.; Koelling, T.M. The Effects of the ManageHF4Life Mobile App on Patients With Chronic Heart Failure: Randomized Controlled Trial. JMIR mHealth uHealth. 2021, 9, e26185. [Google Scholar] [CrossRef] [PubMed]
- Paul, M.; Maglaras, L.; Ferrag, M.A.; Almomani, I. Digitization of healthcare sector: A study on privacy and security concerns. ICT Express. 2023, 9, 571–588. [Google Scholar] [CrossRef]
- Alliance, N.D.I. Definitions [Internet]. Available online: https://www.digitalinclusion.org.
- Romm, T. Lacking a Lifeline: How a federal effort to help low-income Americans pay their phone bills failed amid the pandemic. Washington Post. 2021.
- Brewer, L.C.; Jenkins, S.; Hayes, S.N.; Kumbamu, A.; Jones, C.; Burke, L.E.; et al. Community-Based, Cluster-Randomized Pilot Trial of a Cardiovascular Mobile Health Intervention: Preliminary Findings of the FAITH! Trial. Circulation 2022, 146, 175–190. [Google Scholar] [CrossRef] [PubMed]
- Jr, H.A.T.; Francis, S.; Evans, C.R.; Harvey, M.; Newton, B.A.; Jones, C.P.; et al. Preventing Cardiovascular Disease Among Urban African Americans With a Mobile Health App (the MOYO App): Protocol for a Usability Study. JMIR Res Protoc. 2020, 9, e16699. [Google Scholar]
- Skolarus, L.E.; Cowdery, J.; Dome, M.; Bailey, S.; Baek, J.; Byrd, J.B.; et al. Reach Out Churches: A Community-Based Participatory Research Pilot Trial to Assess the Feasibility of a Mobile Health Technology Intervention to Reduce Blood Pressure Among African Americans. Heal Promot Pr. 2018, 19, 495–505. [Google Scholar] [CrossRef]
- Goodson, N.; Wicks, P.; Morgan, J.; Hashem, L.; Callinan, S.; Reites, J. Opportunities and counterintuitive challenges for decentralized clinical trials to broaden participant inclusion. npj Digit Med. 2022, 5, 58. [Google Scholar] [CrossRef]
- Rodriguez, F. Sex Disparities in Prevention of Atherosclerotic Cardiovascular Disease Across the Life Course. Circulation. 2023, 147, 523–525. [Google Scholar] [CrossRef]
- Smith, J.R.; Thomas, R.J.; Bonikowske, A.R.; Hammer, S.M.; Olson, T.P. Sex Differences in Cardiac Rehabilitation Outcomes. Circ Res. 2022, 130, 552–565. [Google Scholar] [CrossRef]
- Li, S.; Fonarow, G.C.; Mukamal, K.; Xu, H.; Matsouaka, R.A.; Devore, A.D.; et al. Sex and Racial Disparities in Cardiac Rehabilitation Referral at Hospital Discharge and Gaps in Long-Term Mortality. J Am Hear Assoc. 2018, 7, e008088. [Google Scholar] [CrossRef]
- Azizi, Z.; Adedinsewo, D.; Rodriguez, F.; Lewey, J.; Merchant, R.M.; Brewer, L.C. Leveraging Digital Health to Improve the Cardiovascular Health of Women. Curr Cardiovasc Risk Rep. 2023, 17, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Brewer, L.C.; Hayes, S.N.; Caron, A.R.; Derby, D.A.; Breutzman, N.S.; Wicks, A.; et al. Promoting cardiovascular health and wellness among African-Americans: Community participatory approach to design an innovative mobile-health intervention. PLoS ONE. 2019, 14, e0218724. [Google Scholar] [CrossRef] [PubMed]
- Miao, B.Y.; Sushil, M.; Xu, A.; Wang, M.; Arneson, D.; Berkley, E.; et al. Characterisation of digital therapeutic clinical trials: A systematic review with natural language processing. Lancet Digit Heal. 2024, 6, e222–e229. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Astudillo, K.; Velez, D.; Kelley, L.; Cobbs-Lomax, D.; Spatz, E.S. Use of Mobile Health Applications in Low-Income Populations. Circ: Cardiovasc Qual Outcomes. 2020, 13, e007031. [Google Scholar] [CrossRef]
- King, A.C.; Campero, M.I.; Sheats, J.L.; Sweet, C.M.C.; Hauser, M.E.; Garcia, D.; et al. Effects of Counseling by Peer Human Advisors vs Computers to Increase Walking in Underserved Populations. JAMA Intern Med. 2020, 180, 1481–1490. [Google Scholar] [CrossRef]
- King, A.C.; Bickmore, T.W.; Campero, M.I.; Pruitt, L.A.; Yin, J.L. Employing Virtual Advisors in Preventive Care for Underserved Communities: Results From the COMPASS Study. J Heal Commun. 2013, 18, 1449–1464. [Google Scholar] [CrossRef]
- King, A.C.; Campero, I.; Sheats, J.L.; Sweet, C.M.C.; Garcia, D.; Chazaro, A.; et al. Testing the comparative effects of physical activity advice by humans vs. computers in underserved populations: The COMPASS trial design, methods, and baseline characteristics. Contemp Clin Trials. 2017, 61, 115–125. [Google Scholar] [CrossRef]
Figure 1.
Digital health for cardiovascular medicine across the lifespan. Digital health spans numerous digital technologies, including but not limited to, smartphone applications (apps), smartwatches/wearable devices, telemedicine/telehealth, remote monitoring via connected devices, and virtual cardiac rehabilitation. Through the theoretical lifespan of an individual and their relative cardiovascular health, some proposed uses of digital health technologies are presented.
Figure 1.
Digital health for cardiovascular medicine across the lifespan. Digital health spans numerous digital technologies, including but not limited to, smartphone applications (apps), smartwatches/wearable devices, telemedicine/telehealth, remote monitoring via connected devices, and virtual cardiac rehabilitation. Through the theoretical lifespan of an individual and their relative cardiovascular health, some proposed uses of digital health technologies are presented.
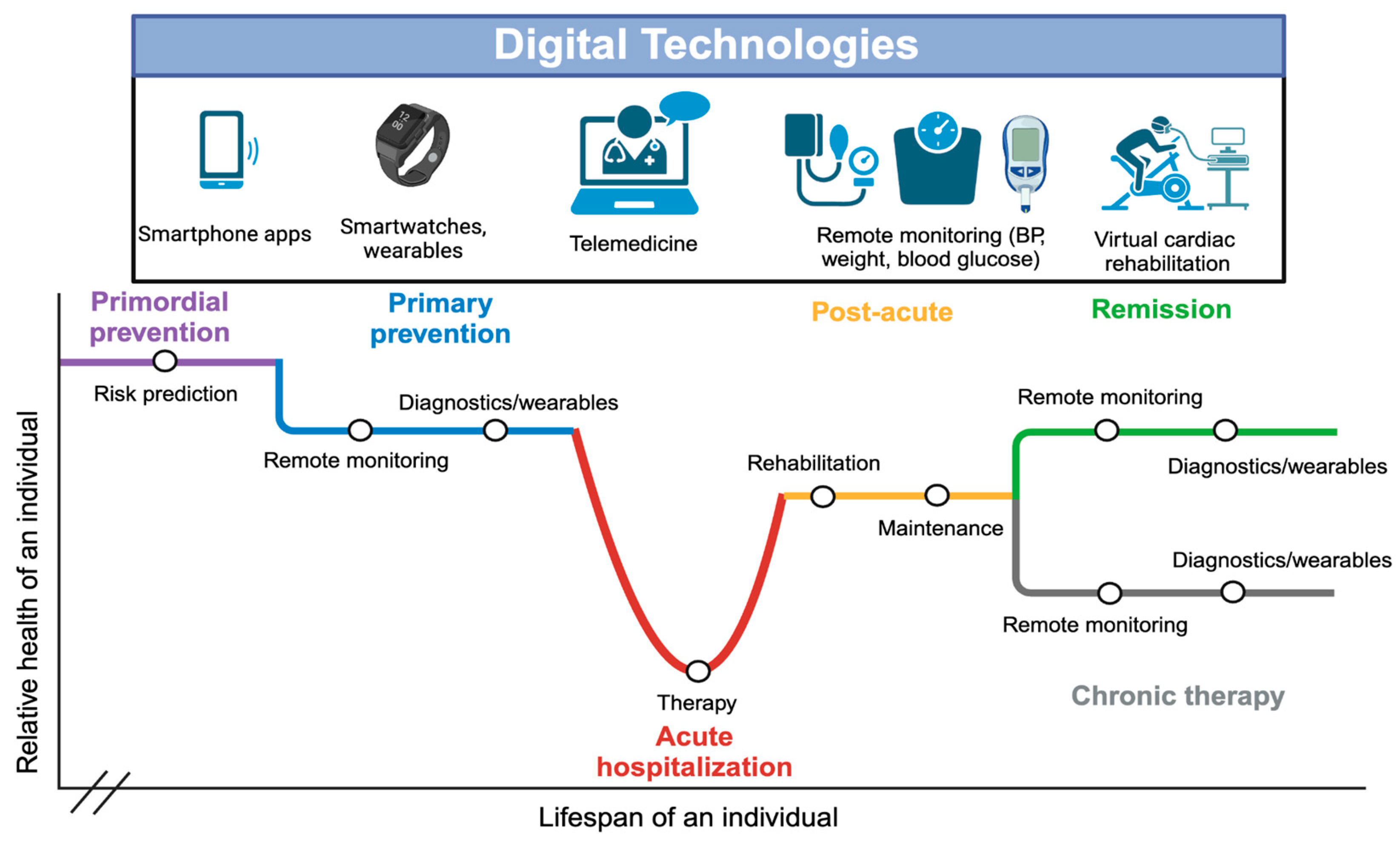
Figure 2.
Elements of digital health equity by domain, their modifying social determinants of health, and proposed solutions to improve digital health equity. With the inverted pyramid structure, each domain influences those that are downstream (e.g., societal solutions will have effects at the community, interpersonal, and individual levels). Bolded text are highlighted in the body of our review.
Figure 2.
Elements of digital health equity by domain, their modifying social determinants of health, and proposed solutions to improve digital health equity. With the inverted pyramid structure, each domain influences those that are downstream (e.g., societal solutions will have effects at the community, interpersonal, and individual levels). Bolded text are highlighted in the body of our review.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



