
Submitted:
10 September 2024
Posted:
11 September 2024
You are already at the latest version
Abstract
Background/Objectives: This study aimed to identify various risk factors associated with breast cancer and explore different treatment strategies based on socio-economic, hormonal, and clinical perspectives.; Methods: We analyzed socio-economic, hormonal, genetic, and clinical variables using data from 356 questionnaires obtained from breast cancer patients at Hassan II Regional Hospital in Agadir, Morocco ; Results:The study reveals that the average age of breast cancer patients is 50 ± 10.72 years, with a mode of 47 years and an age range from 29 to 94 years. Notably, women aged 38 are most frequently diagnosed with triple-negative breast cancer. Significant socio-economic trends were observed among the participants, with the majority being housewives (91%) and nearly half residing in rural areas (48.60%). High rates of illiteracy (74.72%) and financial difficulties (54.2%) pose challenges in accessing healthcare services. Psychological distress is prevalent, with 40.7% experiencing anxiety and 30.1% experiencing sadness. The use of oral contraceptives varies, with implications for breast cancer risk. Additionally, statistics on menarche and menopause suggest hormonal influences on breast cancer development. Histological analysis indicates a predominance of grade II invasive ductal carcinoma and left breast localization. Metastases are present in nearly 38.20% of cases. Notably, surgery as the primary treatment effectively treats medium-sized tumors while limiting metastasis. Furthermore, a comparison of treatment strategies reveals a preference for letrozole among postmenopausal patients and tamoxifen among premenopausal patients; Conclusions:These findings highlight the complexity of breast cancer risk factors and therapeutic approaches, emphasizing the importance of personalized care and targeted interventions.
Keywords:
Breast cancer
; socio-economic
; factors
; hormonal
; clinical
; treatments
; stategies
1. Introduction
Breast cancer is a major global health issue, ranking as the second leading cause of cancer-related deaths among women, with approximately 685,000 deaths in 2020 [1]. In Morocco, 11,747 new cases were diagnosed in women last year, representing about 19.8% of all new cancer cases and 38.9% of all female cancers. Among Arab women, breast cancer typically occurs in younger patients with larger tumors, often at a more advanced stage at diagnosis. Additionally, there is a higher incidence of axillary invasion, a greater proportion of hormone receptor-negative cases, higher tumor grades, and a distinct response to treatment [2]. A comprehensive understanding of disease dynamics and exploration of therapeutic strategies are essential for effectively addressing the challenge of breast cancer. Its impact extends beyond mere statistics, affecting various regions globally and emphasizing the importance of collaborative efforts to optimize treatment. For instance, breast cancer plays a central role in cancer research, being one of the most studied subtypes worldwide [3]. It is influenced by a range of risk factors, including socio-economic, hormonal, and genetic factors.
Regarding socio-economic factors, age is a key determinant in disease management. A significant proportion of breast cancer patients are over 50, with many exceeding 65 years [4] . Younger patients, particularly those under 50, face a higher risk of recurrence [5], while the overall risk of breast cancer gradually increases with age, from 1.5% at age 40 to over 4% in women aged 70 and above [6]. Additionally, there is a noticeable correlation between age and breast cancer subtype, with triple-negative breast cancer (TNBC) often prevalent in younger women and luminal A subtype more common in older women [4]. Meta-analyses suggest that parity may potentially reduce breast cancer risk, although evidence remains inconclusive due to conflicting study results [7,8]. Furthermore, the association between parity and breast cancer risk may vary based on factors such as estrogen receptor status and menopausal status.
Multiple pregnancies could be considered a plausible preventive factor for breast cancer, though further research is needed to clarify the underlying mechanisms. Conversely, a study involving 828 patients found that breast cancer is often diagnosed at more advanced stages in women who have had children compared to nulliparous women [9]. Additionally, women who breastfeed also tend to present with more advanced stages of breast cancer. Obesity is another significant risk factor, defined by a body mass index (BMI) of 30 kg/m² or more, and poses a major concern for breast cancer patients [10]. In postmenopausal women, a high BMI correlates with increased levels of estrone, estradiol, and free estradiol, suggesting a synergistic effect that exacerbates breast cancer risk [11]. Research consistently highlights the association between obesity and an increased risk of breast cancer [12]. In postmenopausal women, estrogen production in adipose tissue further amplifies this effect, especially when combined with a pro-inflammatory diet, increasing breast cancer risk. Overweight women diagnosed with breast cancer had an average rate of 35.52% between 2022 and 2023, underscoring the substantial impact of obesity on breast cancer incidence [13]. Moreover, physical activity is a crucial marker of a healthier lifestyle, as supported by extensive research [14]. Studies indicate that reduced physical function is associated with higher cancer mortality rates among survivors, potentially reflecting advanced breast cancer diagnoses [14]. Nadia Frikha and colleagues suggest that regular physical activity can reduce the risk of developing breast cancer by 15 to 20%, while women who walk three to five hours per week may experience a 20 to 50% reduction in the risk of recurrence of cancer-related mortality [15].
Moreover, the detection of breast cancer in close family members may suggest a genetic transmission of the disease. However, sporadic cases also occur within some families, complicating the accurate identification of family disease history [16]. Genetic factors play a significant role in breast cancer predisposition within families, as evidenced by the consistent family risk observed across different countries, environments, and cultures. A meta-analysis of 49 studies, including 48 case-control studies and one cohort study, confirmed this trend, highlighting a higher breast cancer risk for individuals with a family history of the disease. On average, these individuals had approximately a 2.21 times higher risk of developing breast cancer compared to those without a family history [17]. While periodic screening programs using mammography have proven effective in reducing breast cancer mortality and mitigating its impact, adherence to these programs faces several challenges. Common obstacles include financial constraints and limited socio-economic resources [18]. Low-income women often encounter these challenges, being less likely to have private health insurance or employment. In contrast, individuals with moderate (OR: 0.69) or high incomes (OR: 0.85) face fewer barriers to screening participation [19]. Additionally, transportation difficulties hinder access to healthcare facilities, resulting in a 26.4% reduction in screening participation. Among women with a low risk of breast cancer (<20%), those with higher educational levels, such as university graduates (132%), are more likely to undergo MRI screening [20]. Cancer patients often face psychological issues throughout their diagnosis and treatment journey, including depression, anxiety, and emotional distress. Studies show that depression affects 8 to 24% of these patients [21], while 19% exhibit anxiety symptoms [24]. Furthermore, a significant percentage of cancer survivors, 6.6%, suffer from severe psychological distress, a rate considerably higher than that observed in non-cancer adults (3.7%) [22].
Cancer-related fatigue (CRF) is a common and debilitating complication associated with cancer and its treatments. It is characterized by persistent and debilitating fatigue influenced by various factors such as cancer type and treatment modalities. Effective management of CRF is crucial for improving patient comfort and quality of life, as well as supporting the cancer recovery process [23]. To further explore the hormonal factors influencing breast cancer risk and treatment outcomes, various reproductive factors have been examined. Among these, age at first childbirth is a key determinant. Early childbirth has been associated with a lasting reduction in breast cancer risk, clarifying the complex interaction between reproductive events and cancer susceptibility [24] Additionally, breast cancer treatment stratification relies on molecular subtypes, with hormone-dependent cancers being a predominant category. Notably, estrogen receptor expression characterizes the majority of breast cancers, underscoring the therapeutic importance of estrogen deprivation to reduce recurrence risks [25].
Insights from [26] underscore the nuanced relationship between oral contraceptive use and breast cancer risk. Oral contraceptives containing ethinylestradiol below 50 µg have been associated with heightened breast cancer risks during and shortly after usage. However, this risk tends to taper off a decade post-discontinuation, with discernible differences in clinical staging among contraceptive users [27]. Furthermore, Systematic Review [28] underscores a pronounced elevation in breast cancer likelihood among hormonal contraceptive users, accentuating the imperative of understanding contraceptive influences on breast cancer susceptibility. The age at menarche, marking the onset of menstrual cycles, emerges as a potential risk modulator for breast cancer. Variability across demographics underscores its nuanced role, with early menarche subtly predisposing women to heightened breast cancer risks.
Notably, studies unveil an association between menarche preceding 13 years and increased breast cancer odds [29], further echoed in case-only studies distinguishing breast cancer subtypes [30]. In parallel, an intriguing landscape unfolds concerning bone metastases prevalence among breast cancer cohorts. In hormone receptor-positive (HR+) tumors, bone metastases feature in approximately 15% of cases, while up to 50% of HER2-positive breast cancer patients exhibit such metastatic spread [31]. The landscape is further nuanced by HER2 overexpression in a notable segment of breast cancer cases, coupled with hormone receptor positivity in a significant proportion, albeit with distinct prognostic implications [32,33].
The study of the various factors clinical associated with breast cancer helps in understanding its complex nature and multifaceted risk factors. Among the most prevalent forms of breast cancer are invasive ductal carcinoma, where malignant cells originate from the ducts and can spread beyond the breast, infiltrating neighboring tissues and potentially metastasizing to distant parts of the body. Another frequently encountered type is invasive lobular carcinoma, characterized by the growth of cancer cells within the lobules, with the potential to disseminate to nearby breast tissues and other regions of the body.
Expanding on the understanding of various breast cancer types, it is imperative to consider histological grading, a pivotal parameter providing critical biological insights independently of axillary status and tumor size. This grading system offers valuable information regarding tumor proliferation, aberrant cell architecture, nuclear displacement, and chromosomal instability, all of which are integral to assessing the disease prognosis [34]. The SBR grading score, ranging from 1 to 3, reflects the degree of resemblance between cancer cells and healthy breast cells.
A higher grade indicates a greater deviation in appearance and growth patterns of cancer cells compared to their healthy counterparts [35]. Type 2 diabetes, affecting over 15 million American women and steadily increasing, is associated with a higher risk of serious complications such as kidney, cardiovascular, retinal diseases, and cancer [36]. Moreover, diabetes is recognized as a risk factor for breast cancer [37], as it may lead to increased expression of aromatase, resulting in heightened local production of estrogen. Elevated estrogen levels can stimulate the growth of estrogen receptor-positive breast cancers (ER+) [38].
Breast cancer treatment strategies encompass a multidisciplinary approach tailored to individual patients. Early-stage breast cancer is often managed with conservative breast surgery or mastectomy, complemented by radiotherapy.
Axillary evaluation via sentinel lymph node biopsy aids in treatment planning. Locally advanced cases may require endocrine therapies, adjuvant chemotherapy, or neo-adjuvant systemic treatments. The classification of breast cancer subtypes informs personalized therapeutic interventions. Hormone receptor-positive subtypes like Luminal A exhibit favorable outcomes, while Luminal B may present challenges due to increased proliferation markers. HER2-positive cancers benefit from targeted therapies, whereas triple-negative breast cancer poses unique treatment hurdles [39]. Surgery constitutes a cornerstone of breast cancer treatment, offering two primary approaches: breast-conserving surgery (BCS) and mastectomy. BCS preserves healthy breast tissue, while mastectomy involves complete breast removal, often followed by reconstruction. Lymph node removal options include sentinel lymph node biopsy (SLNB) and axillary lymph node dissection (ALND), guided by various clinical factors [40].
Endocrine therapy is pivotal for hormone receptor-positive breast cancers, encompassing selective estrogen receptor modulators (SERMs) like tamoxifen, which regulate estrogen receptors and inhibit tumor progression. Selective estrogen receptor downregulators (SERDs) and aromatase inhibitors (AIs) offer alternatives, each with distinct efficacy profiles and side effect profiles [25,41,42]. Chemotherapy plays a systemic role in breast cancer treatment, administered in neoadjuvant or adjuvant settings based on tumor characteristics. Neoadjuvant chemotherapy reduces tumor size, facilitating breast-conserving surgery and aiding in prognostic assessment [43].
Targeted therapies specifically disrupt oncogenic cellular processes, addressing aberrant signaling pathways. For hormone receptor-positive cancers, investigational drugs like rapamycin and mTOR inhibitors show promise. HER2-positive breast cancers benefit from monoclonal antibodies like trastuzumab and pertuzumab, enhancing treatment efficacy.
Triple-negative breast cancer treatments include PARP inhibitors and CDK4/6 inhibitors, targeting specific molecular pathways associated with tumor growth and progression [44]. For HER2-positive (HER2+) breast cancers, the monoclonal antibody trastuzumab selectively inhibits the proliferation of HER2-overexpressing cells and has been approved for treating HER2+ MBC [44]. Adding trastuzumab to docetaxel improves progression-free survival and overall survival in patients with metastatic HER2+ breast cancer, with shorter survival observed in the docetaxel-alone group [45]. Another monoclonal antibody, pertuzumab, blocks heterodimerization and signal transduction via the MAPK and PI3K pathways in HER2-positive patients [46]. Monoclonal antibodies, such as trastuzumab, have been an effective therapeutic strategy for HER2+ breast cancers for over 20 years. However, primary and acquired resistance to anti-HER2 treatment remains a significant challenge, with up to 50% of patients developing brain metastases during the course of the disease [44].
Since 2010, lapatinib has been approved in combination with letrozole to treat advanced breast cancer in postmenopausal women, specifically when the tumor is both HER2-positive (HER2+) and hormone receptor-positive (HR+). Recent findings from the CHER-Lob trial have indicated that the combination of lapatinib and trastuzumab yields better results than using trastuzumab alone in the neoadjuvant treatment of early HER2-positive breast cancer in British Columbia [47]. For triple-negative breast cancer (TNBC), a highly aggressive subtype [48], olaparib received approval from the US FDA in 2018 for patients with HER2-negative (HER2-) germline BRCA mutations (gBRCAm). In October 2018, talazoparib also gained FDA approval.
Veliparib is often used in the neoadjuvant treatment of TNBC, although its efficacy is still debated [49]. CDK4/6 inhibitors, such as palbociclib, ribociclib, and abemaciclib, were recently approved in combination with endocrine therapy for advanced and/or metastatic HR+/HER2- breast cancer [50]. Furthermore, CDK4/6 inhibitors, including palbociclib and ribociclib, have been FDA-approved for TNBC treatment [51]. The epidermal growth factor receptor (EGFR) is a potential therapeutic target in 89% of TNBC patients [52], with tyrosine kinase inhibitors like gefitinib and monoclonal antibodies. The combination of gefitinib, carboplatin, and docetaxel can synergistically increase cytotoxicity in TNBC cells [53].
In this study, we examined various breast cancer risk factors, including socio-economic, hormonal, and clinical factors, as well as the therapeutic strategies implemented at Hassan II Hospital in Agadir, Morocco.
2. Materials and Methods
This research is based on the analysis of 356 questionnaires, collected over a period of three months, from breast cancer patients. The data was obtained from the Hassan II Regional Hospital in Agadir, Morocco, and encompassed socio-economic, hormonal, genetic, and clinical variables. The study aimed to investigate the diverse risk factors associated with breast cancer and explore various therapeutic strategies.
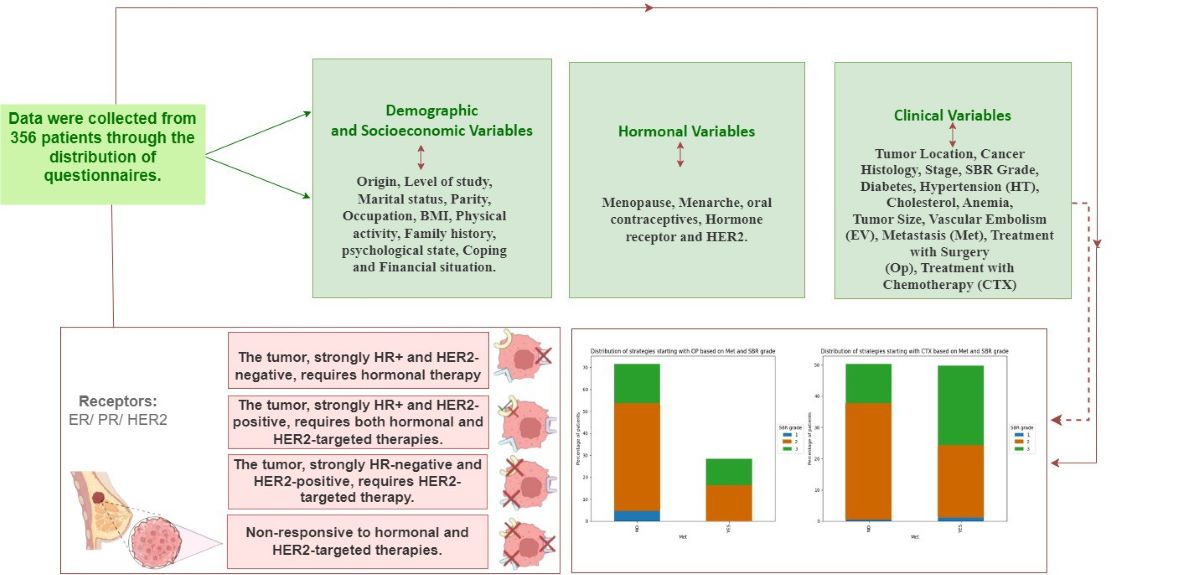
The variables are organized starting with Socio-Economic and demographic aspects, followed by hormonal aspects based on patient questionnaires, and finally clinical variables derived from medical record processing (Table 1).
The statistical analyses were performed using the software GraphPad Prism version 8.0.2.
3. Results and Discussions
3.1. Impact of Socio-Economic, Clinical, and Hormonal Variables
3.1.1. Socio-Economic Factors
In our study, we found that the average age of breast cancer patients was 50 ± 10.72 years. The mode was 47 years, and the age range extended from 29 to 94 years (Figure 1). Notably, our findings showed that women aged 38 years were the most frequently diagnosed with triple-negative breast cancer (TNBC), as illustrated in Figure 1.
According to the study [54], a total of 286,520 breast cancer patients were analyzed. The average age at diagnosis was 61 ± 13 years among white women and 58 ± 13 years among black women. Another study [55] reported an average age of 60 years at diagnosis. In contrast, our study found that the average age of breast cancer diagnosis among Moroccan women is 50 years. This suggests that Moroccan women are affected by breast cancer at a younger age compared to European and American women. Nearly half of the participants, 173 (48.60%), reside in rural areas, suggesting potential challenges in accessing healthcare due to geographical disparities. In contrast, 183 patients live in urban areas (Figure 2). However, in study [55], 88.2% of patients were from urban areas.
Additionally, the high illiteracy rate among the women in our study, with 266 (74.72%) being illiterate, indicates significant barriers to accessing information and raising awareness. Furthermore, the majority of our patients, approximately 324 (91%), are unemployed, and 193 (54.2%) face financial difficulties. Moreover, 143 (40.2%) of the women began their treatment without adequate psychological support or accompaniment, attending their treatment alone. These factors negatively impact the psychological health of the patients, as shown by the 145 (40.7%) who are anxious and the 107 (30.1%) who suffer from sadness. Only 104 (29.2%) of the patients exhibit a stable psychological state (Figure 3).
Additionally, our data reveal significant insights. Approximately 213 (59%) of the participants are married, and 73 (20.5%) are without children, while the majority, 175 (49.1%), have between one and three children. Furthermore, 48.87% of the participants fall into the "Overweight" category based on their BMI (as shown in Figure 4), highlighting the prevalence of obesity among those at risk for breast cancer. This underscores the critical need for targeted interventions and preventive measures against obesity to mitigate breast cancer risk. Additionally, about 69.94% of the participants are classified as inactive, indicating that a substantial portion of this population could benefit from increased physical activity to reduce breast cancer risk and improve overall health outcomes. Lastly, our findings also indicate that 48.87% of the women have a family history of breast cancer.
3.1.2. Hormonal Factors
In exploring the relationship between hormonal factors and breast cancer risk, our analysis focused on the following variables:
The results highlight a diverse use of oral contraceptives among the women surveyed, which has implications for breast cancer risk. Notably, 152 women (42.2%) chose not to use oral contraceptives, potentially reducing their exposure to associated risks. However, a significant proportion, including 73 (20.3%) and 48 (13.5%) women, have used these contraceptives for over 10 years and between 5 and 10 years, respectively, while 53 (14.9%) have used them for 1 to 5 years. Prolonged use of oral contraceptives has been associated with a slight increase in breast cancer risk, especially with long-term use. These findings highlight the complex relationship between contraceptive choices and breast cancer risk, emphasizing the importance of informed decision-making and personalized healthcare within this demographic.
Approximately 287 women (80.6%) experienced normal menstruation, beginning between ages 12 and 13. Only 3 women (0.8%) had early menarche, between ages 9 and 11, while 66 (18.5%) had late menarche, between ages 14 and 23. Additionally, our analysis revealed that 166 women (46.6%) were postmenopausal, as shown in Figure 5.
Estrogens play a vital role in breast cancer, primarily through their interaction with estrogen receptors ERα, ERβ, and the G protein-coupled estrogen receptor. These receptors are activated by estrogens and influence various oncological processes (Figure 5). For instance, ERα interacts with different growth factor receptors, affecting cancer progression. Activation of EGFR and HER receptors can lead to ERα phosphorylation, while interaction with VEGFR is associated with resistance to anti-estrogen treatments. Additionally, high expression of HGFR is linked to resistance to fulvestrant and a poor prognosis. RET promotes ERα phosphorylation in ERα-positive/HER2-negative cancers. Furthermore, the NOTCH receptor activates ERα even in the absence of estrogens by stimulating the PI3K/Akt/mTOR pathways. On the other hand, ERβ modulates growth factor receptor signaling by reducing migration and invasion in TNBC cells. It also influences HER2/HER3 and decreases VEGF production, which limits angiogenesis and tumor growth. Targeting ERβ could provide anti-proliferative and anti-angiogenic effects [56].
Histological characteristics of breast cancer are influenced by the tumor's molecular signature, including the presence of hormone receptors, which also reflects the tumor's cell of origin (Fig. 6). Patients are classified into four main groups: luminal A and B tumors, HER2-positive luminal tumors, and triple-negative basal tumors. These groups differ in terms of aggressiveness, metastatic behavior, and treatment options. In women, approximately 70 to 80% of breast cancers are hormone-dependent, expressing at least one type of hormonal receptor, such as estrogen and progesterone receptors (ER and PR) (Figure 5) [57].
Our study shows that 278 patients (78.1%) have breast cancer with positive hormonal receptors (HR+), of which 116 (32.6%) are also HER2 positive (HER2+). In contrast, approximately 56.18% of patients have HR+ breast cancer that is HER2 negative (HR+/HER2-), classified as luminal A. Additionally, 21.91% of patients have HR+ and HER2+ breast cancer, categorized as luminal B. Breast cancers with negative hormonal receptors and positive HER2 account for 10.67%, while triple-negative cancers, with both negative hormonal receptors and HER2, make up 11.24%.
3.1.3. Clinical Factors
Our study reveals significant clinical findings consistent with previous research, illustrating various aspects of breast cancer cases at the time of diagnosis. Histologically, invasive ductal carcinoma (IDC) emerged as the most common type, accounting for 355 cases (94.10%), followed by invasive lobular carcinoma (ILC) with approximately 16 cases (4.5%), while other less common types represented about 5 cases (1.41%). The distribution of tumor grades revealed a predominance of grade II cases, comprising 224 cases (62.9%), followed by grade III with around 120 cases (33.70%), and grade I representing approximately 12 cases (3.37%). Additionally, 168 patients (47.2%) were diagnosed at advanced stages (stages 3 and 4). In contrast to our study, which shows less effective early detection with 47.2% of patients diagnosed at advanced stages (stages 3 and 4), the study [62] indicates better early detection, with 50.2% of cases diagnosed at stage 1 and 37.2% at stage 2. Additionally, the study [62] reports that 22.4% of the tumors were well-differentiated, 41.9% moderately differentiated, and 31.5% poorly or undifferentiated. These statistics indicate a trend toward late-stage diagnosis, reflecting a lack of awareness regarding screening among the majority of patients, as shown in Figure 6.
The analysis of tumor localization reveals a slight predominance in the left breast, with approximately 189 cases (53.1%), compared to the right breast, which accounts for about 106 cases (44.9%). Bilateral cases are less common, representing around 7 cases (2%). The presence of vascular emboli was observed in 253 patients (71.1%), and metastases were found in 136 patients (38.2%), indicating advanced disease progression in some patients.
The average tumor size was measured at 2 cm. Additionally, 260 patients (73%) had tumors ranging from 1 to 3 cm in size, while 88 patients (24.7%) had tumors exceeding 10 cm (Figure 8). These results highlight a significant prevalence of intermediate and advanced tumor sizes, suggesting that the disease is often detected at more advanced stages. The high prevalence of vascular emboli and the presence of metastases in a substantial proportion of patients further emphasize this trend, indicating a more severe progression of the disease in our cohort.
Regarding personal medical history in our study population, we observed that 78 patients (21.9%) have comorbidities such as diabetes, 96 (27%) suffer from hypertension, 25 (7%) have cholesterol issues, and approximately 90 patients (25.3%) have anemia. This high prevalence of comorbidities indicates that these conditions may impact the progression of breast cancer and are associated with a more rapid advancement of the disease. Regarding the treatment strategies implemented at the Hassan II Regional Oncology Center in Agadir, five main approaches were identified: surgery (Op), chemotherapy (CTX), hormone therapy (HT), radiotherapy (RTH), and targeted therapy (TT). The majority of breast cancer patients underwent surgery (327 patients, or 91.9%). Approximately 317 patients (89%) received radiotherapy, 342 patients (96.1%) underwent chemotherapy, 264 patients (74.2%) were treated with hormone therapy, and 113 patients (31.7%) received targeted therapy (Figure 7).
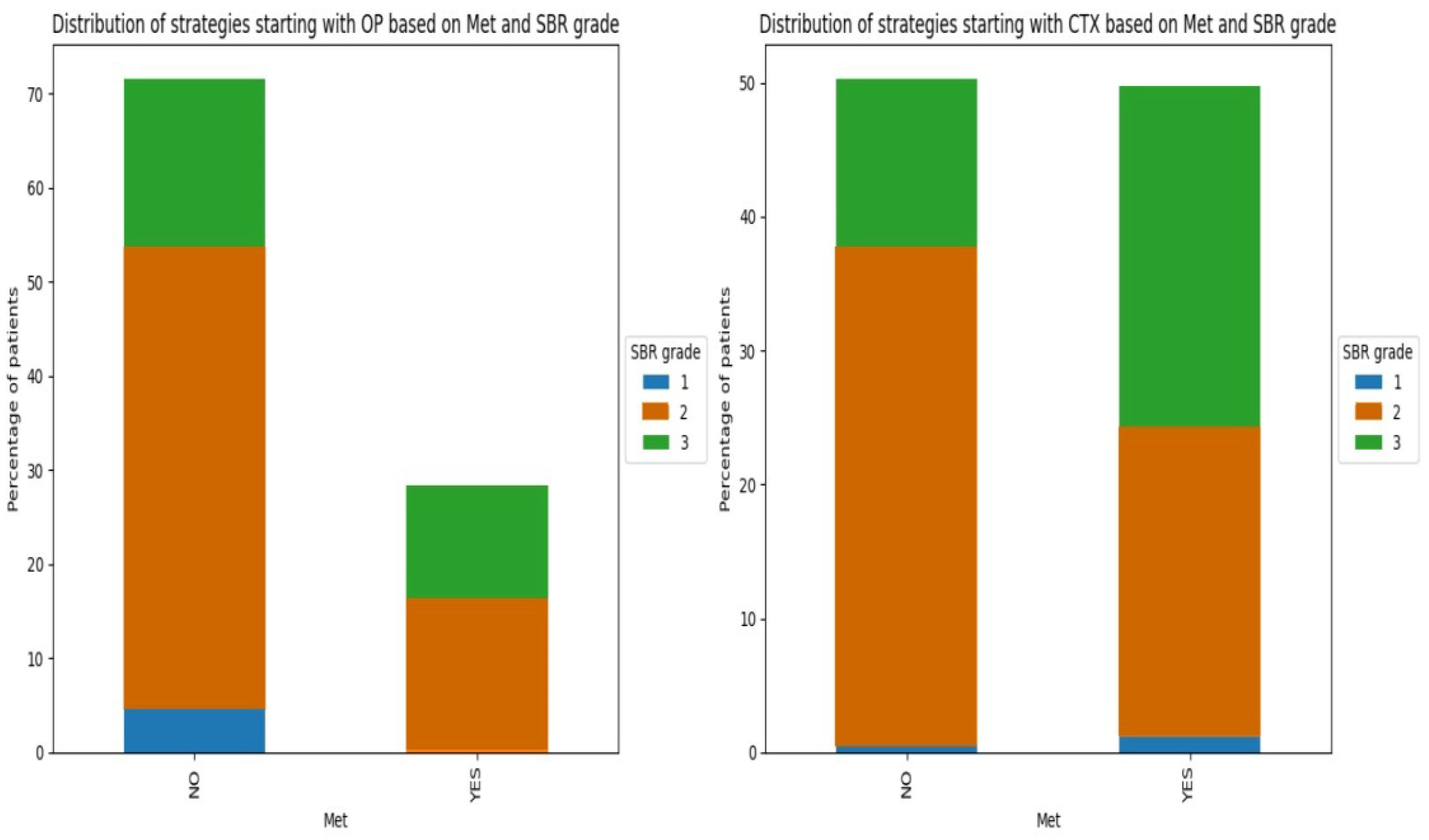
In reviewing the personalized treatment strategies adopted at the Hassan II Regional Oncology Center in Agadir, our investigation revealed a mosaic of approaches; each carefully designed to meet the unique needs of breast cancer patients. Grades 1 and 2 underwent surgery (OP) as their primary treatment. Notably, most of these patients showed no evidence of metastasis, indicating that the cancer remained localized to the primary site. These findings suggest that surgery, as a primary treatment modality, can effectively treat medium-sized tumors while preventing the cancer from spreading to other parts of the body. Conversely, patients who started chemotherapy (CTX) showed different trends, with approximately 50% having metastatic status and approximately 25% having grade 3 BRS (as illustrated in Figure 4). The initiation of CTX treatment aims to reduce tumor size (Figure 8).
Figure 8.
Distribution of strategies starting with CTX or OP based on Met and SBR Grade.
In Figure 9, we observe a comparison of treatment strategies based on the use of OP+CTX+RTH+HT (letrozole) and OP+CTX+RTH+HT (Tamoxifen) in breast cancer patients, categorized by age and menopausal status. It is noteworthy that the majority of patients using the hormonal treatment letrozole are menopausal, with an age distribution biased towards those over 52 years old. This trend suggests that letrozole, a commonly prescribed hormonal treatment for menopausal women, is preferred among older patients. Conversely, for patients using the hormonal treatment tamoxifen, the majority are premenopausal, with a predominant age range of less than 48 years old. This indicates a preference for tamoxifen, another hormone therapy option suited for premenopausal women, among younger patients, while letrozole is intended for menopausal women.
Our study on breast cancer has unveiled a myriad of significant findings providing insight into the challenges and intricate aspects of this disease. By examining data collected from 356 patients, several important trends were identified. Firstly, the average age of patients diagnosed with breast cancer was 50 years, with a notable concentration around 47 years old. This observation underscores the necessity for heightened vigilance across a broad spectrum of age groups. Additionally, we observed that women aged 38 were more prone to receiving a diagnosis of a specific type of breast cancer, triple-negative breast cancer. This discovery emphasizes the importance of understanding variations in incidence by age and cancer subtype for early and effective intervention. Regarding socio-economic factors, our study has illuminated several significant challenges. The vast majority of patients were homemakers, and nearly half resided in rural areas, potentially leading to difficulties in accessing healthcare. Furthermore, high levels of illiteracy and financial hardships were observed, highlighting additional obstacles faced by these patients in their treatment journey. Mental health was also a concern, with elevated rates of anxiety and sadness among patients, underlining the necessity of considering mental health in breast cancer treatment, as mental health issues can increase the risk of breast cancer and affect the expected outcomes of treatments.
Our results also underscored the significance of hormonal factors in breast cancer. The use of oral contraceptives and patterns of menarche and menopause were all associated with implications for breast cancer risk, underscoring the complexity of this disease and the need for individualized approaches in managing hormonal treatments. Regarding clinical characteristics, we observed a predominance of IDC breast cancer types, as well as trends in treatment modalities used. For example, surgery was the most common treatment modality for moderate-sized tumors, while preferences for certain hormonal treatments varied depending on the menopausal status of patients.
4. Conclusions
Our comprehensive analysis of breast cancer risk factors and treatment strategies offers valuable insights that can significantly impact patient care and decision-making processes within healthcare institutions. By delving into the socio-economic, hormonal, and clinical aspects of breast cancer, our study sheds light on the multifaceted nature of this disease and underscores the importance of personalized, tailored approaches to diagnosis and treatment.
Our findings highlight the critical role of early detection and intervention, particularly in light of the varied incidence rates across different age groups and cancer subtypes. Understanding these nuances allows for the implementation of targeted screening programs and treatment protocols, ultimately improving patient outcomes and survival rates.
Moreover, our study identifies socioeconomic disparities and access barriers that impede optimal care delivery, emphasizing the need for tailored support systems and interventions to address these challenges. By recognizing and addressing factors such as illiteracy, financial hardships, and geographical disparities, healthcare providers can ensure equitable access to quality care for all patients, regardless of their background or circumstances.
Furthermore, our analysis underscores the importance of integrating mental health support into breast cancer treatment protocols, given the prevalence of anxiety and sadness among patients. By addressing psychological distress and providing holistic, patient-centered care, healthcare institutions can enhance overall treatment efficacy and patient satisfaction.
On the clinical front, our study elucidates trends in treatment modalities and their effectiveness in managing breast cancer. By identifying optimal treatment pathways based on tumor characteristics and patient demographics, our findings can inform clinical decision-making and accelerate the development of standardized treatment protocols. Additionally, our comparison of treatment strategies highlights the importance of considering individual patient factors, such as menopausal status, in selecting the most appropriate therapy, thereby optimizing treatment outcomes and minimizing adverse effects.
Overall, our study contributes valuable insights to the field of breast cancer research and clinical practice, offering actionable recommendations to improve patient care, streamline treatment protocols, and ultimately, save lives. By leveraging data-driven approaches and adopting a multidisciplinary, patient-centered approach, healthcare institutions can enhance the effectiveness and efficiency of breast cancer management, paving the way for a brighter, healthier future for all affected individuals.
Author Contributions
Fatima Ezahra Mouas and Latifa Doudach : Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, review & editing. Boutaina Addoum, Mohammed Attaleb, and Mohammed El mzibri : Methodology, Software, Writing review & editing. Laila Benbacer, Ghizlane Raise and Taoufiq Fechtali: Data curation, Investigation, Methodology and Supervision.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
The data used in this research were obtained from Hassan II Hospital in Morocco, and research ethics approval was obtained from the Ministry of Health in Morocco under No. 3758, dated July 12, 2023.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data used in this study are not publicly available due to privacy restrictions and ethical requirements. These data contain sensitive information that cannot be shared in order to protect the privacy of the participants.
Acknowledgments
The authors thank the breast cancer patients who participated in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jafarian, A.H.; Kooshki forooshani, M.; Rasoliostadi, A.; Mohamadian roshan, N. Vascular Mimicry Expression in Invasive Ductal Carcinoma; A New Technique for Prospect of Aggressiveness. Iran J Pathol 2019, 14, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Chouchane, L.; Boussen, H.; Sastry, K.S.R. Breast Cancer in Arab Populations: Molecular Characteristics and Disease Management Implications. The Lancet Oncology 2013, 14, e417–e424. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2022. CA A Cancer J Clinicians 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- McGuire, A.; Brown, J.; Malone, C.; McLaughlin, R.; Kerin, M. Effects of Age on the Detection and Management of Breast Cancer. Cancers 2015, 7, 908–929. [Google Scholar] [CrossRef] [PubMed]
- O’Shaughnessy, J.; Gradishar, W.; O’Regan, R.; Gadi, V. Risk of Recurrence in Patients With HER2+ Early-Stage Breast Cancer: Literature Analysis of Patient and Disease Characteristics. Clinical Breast Cancer 2023, 23, 350–362. [Google Scholar] [CrossRef]
- Łukasiewicz, S.; Czeczelewski, M.; Forma, A.; Baj, J.; Sitarz, R.; Stanisławek, A. Breast Cancer—Epidemiology, Risk Factors, Classification, Prognostic Markers, and Current Treatment Strategies—An Updated Review. Cancers 2021, 13, 4287. [Google Scholar] [CrossRef] [PubMed]
- Azubuike, S.O. Relationship between Parity and Breast Cancer Risk: A Critical Review of Evidence (with Focus on Sub-Saharan Africa). International Journal of Noncommunicable Diseases 2023, 8, 66–74. [Google Scholar] [CrossRef]
- Veisi, P.; Nikouei, M.; Cheraghi, M.; Shahgheibi, S.; Moradi, Y. The Association between the Multiple Birth and Breast Cancer Incidence: An Update of a Systematic Review and Meta-Analysis from 1983 to 2022. Arch Public Health 2023, 81, 76. [Google Scholar] [CrossRef] [PubMed]
- Ak, N.; Tuz, Z.; Aydin, E.; Ferhatoğlu, F.; Sari, M.; Paksoy, N.; Doğan, İ.; Yildiz, A.; Di̇Şçi̇, R.; Sai̇P, P.M. The Effect of Parity, Breastfeeding History, and Duration on Clinical and Pathological Characteristics of Breast Cancer Patients. Turkish Journal of Medical Sciences 2024, 54, 229–238. [Google Scholar] [CrossRef]
- LeVee, A.; Mortimer, J. The Challenges of Treating Patients with Breast Cancer and Obesity. Cancers 2023, 15, 2526. [Google Scholar] [CrossRef]
- Nikolaos Tzenios OBESITY AND BREAST CANCER: THE ROLE OF ADIPOSE TISSUES AND HORMONES. EPRA 2023, 178–180. [CrossRef]
- Ajabnoor, G.M.A. The Molecular and Genetic Interactions between Obesity and Breast Cancer Risk. Medicina 2023, 59, 1338. [Google Scholar] [CrossRef] [PubMed]
- Hajji-Louati, M.; Cordina-Duverger, E.; Laouali, N.; Mancini, F.-R.; Guénel, P. A Case–Control Study in France Showing That a pro-Inflammatory Diet Is Associated with a Higher Risk of Breast Cancer. Sci Rep 2021, 11, 17019. [Google Scholar] [CrossRef] [PubMed]
- Coleman, C.; Yan, C.H.; Ko, N.Y.; Nabulsi, N.A.; Hoskins, K.F.; Chiu, B.C.-H.; Calip, G.S. Physical Functioning, Frailty and Risks of Locally-Advanced Breast Cancer among Older Women. The Breast 2022, 64, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Frikha, N.; Chlif, M. Un aperçu des facteurs de risque du cancer du sein. Bulletin de l’Académie Nationale de Médecine 2021, 205, 519–527. [Google Scholar] [CrossRef]
- Obeagu, E.I.; Obeagu, G.U. Breast Cancer: A Review of Risk Factors and Diagnosis. Medicine 2024, 103, e36905. [Google Scholar] [CrossRef]
- Wang, H.; MacInnis, R.J.; Li, S. Family History and Breast Cancer Risk for Asian Women: A Systematic Review and Meta-Analysis. BMC Med 2023, 21, 239. [Google Scholar] [CrossRef]
- Ponce-Chazarri, L.; Ponce-Blandón, J.A.; Immordino, P.; Giordano, A.; Morales, F. Barriers to Breast Cancer-Screening Adherence in Vulnerable Populations. Cancers 2023, 15, 604. [Google Scholar] [CrossRef]
- Henderson, L.M.; O’Meara, E.S.; Haas, J.S.; Lee, C.I.; Kerlikowske, K.; Sprague, B.L.; Alford-Teaster, J.; Onega, T. The Role of Social Determinants of Health in Self-Reported Access to Health Care Among Women Undergoing Screening Mammography. Journal of Women’s Health 2020, 29, 1437–1446. [Google Scholar] [CrossRef]
- Krebber, A.M.H.; Buffart, L.M.; Kleijn, G.; Riepma, I.C.; de Bree, R.; Leemans, C.R.; Becker, A.; Brug, J.; van Straten, A.; Cuijpers, P.; et al. Prevalence of Depression in Cancer Patients: A Meta-analysis of Diagnostic Interviews and Self-report Instruments. Psycho-Oncology 2014, 23, 121–130. [Google Scholar] [CrossRef]
- Linden, W.; Vodermaier, A.; MacKenzie, R.; Greig, D. Anxiety and Depression after Cancer Diagnosis: Prevalence Rates by Cancer Type, Gender, and Age. Journal of Affective Disorders 2012, 141, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; Li, C.; Li, J.; Balluz, L.S. Physical Activity, Psychological Distress, and Receipt of Mental Healthcare Services among Cancer Survivors. J Cancer Surviv 2013, 7, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Schaab, M.; Wijlens, K.A.E.; Bode, C. Psychological Coping Factors Associated With Breast Cancer-Related Fatigue: A Systematic Review of Recent Evidence for Stages 0 to III. Clinical Breast Cancer 2023, 23, e401–e411. [Google Scholar] [CrossRef]
- Fraumeni JF Jr,; Lloyd JW,; Smith EM,; Wagoner JK. Cancer Mortality Among Nuns: Role of Marital Status in Etiology of Neoplastic Disease in Women. JNCI: Journal of the National Cancer Institute 1969. [CrossRef]
- Harbeck, N.; Penault-Llorca, F.; Cortes, J.; Gnant, M.; Houssami, N.; Poortmans, P.; Ruddy, K.; Tsang, J.; Cardoso, F. Breast Cancer. Nat Rev Dis Primers 2019, 5, 66. [Google Scholar] [CrossRef]
- Satish, S.; Moore, J.F.; Littlefield, J.M.; Bishop, I.J.; Rojas, K.E. Re-Evaluating the Association Between Hormonal Contraception and Breast Cancer Risk. BCTT 2023, Volume 15, 227–235. [Google Scholar] [CrossRef]
- Torres-de la Roche, L.A.; Acevedo-Mesa, A.; Lizarazo, I.L.; Devassy, R.; Becker, S.; Krentel, H.; De Wilde, R.L. Hormonal Contraception and the Risk of Breast Cancer in Women of Reproductive Age: A Meta-Analysis. Cancers 2023, 15, 5624. [Google Scholar] [CrossRef]
- Maurya, A.P.; Brahmachari, S. Association of Hormonal and Reproductive Risk Factors with Breast Cancer in Indian Women: A Systematic Review of Case–Control Studies. Indian Journal of Cancer 2023, 60, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Zheng, T.; Wang, A.; Hu, D.; Wang, Y. Molecular Mechanisms of Breast Cancer Metastasis by Gene Expression Profile Analysis. Molecular Medicine Reports 2017, 16, 4671–4677. [Google Scholar] [CrossRef]
- Kuksis, M.; Gao, Y.; Tran, W.; Hoey, C.; Kiss, A.; Komorowski, A.S.; Dhaliwal, A.J.; Sahgal, A.; Das, S.; Chan, K.K.; et al. The Incidence of Brain Metastases among Patients with Metastatic Breast Cancer: A Systematic Review and Meta-Analysis. Neuro-Oncology 2021, 23, 894–904. [Google Scholar] [CrossRef]
- Purdie, C.A.; Baker, L.; Ashfield, A.; Chatterjee, S.; Jordan, L.B.; Quinlan, P.; Adamson, D.J.A.; Dewar, J.A.; Thompson, A.M. Increased Mortality in HER2 Positive, Oestrogen Receptor Positive Invasive Breast Cancer: A Population-Based Study. Br J Cancer 2010, 103, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Gong, Y.; Liu, Y.-R.; Ji, P.; Hu, X.; Shao, Z.-M. Impact of Molecular Subtypes on Metastatic Breast Cancer Patients: A SEER Population-Based Study. Sci Rep 2017, 7, 45411. [Google Scholar] [CrossRef] [PubMed]
- Gianni, L.; Pienkowski, T.; Im, Y.-H.; Roman, L.; Tseng, L.-M.; Liu, M.-C.; Lluch, A.; Staroslawska, E.; de la Haba-Rodriguez, J.; Im, S.-A.; et al. Efficacy and Safety of Neoadjuvant Pertuzumab and Trastuzumab in Women with Locally Advanced, Inflammatory, or Early HER2-Positive Breast Cancer (NeoSphere): A Randomised Multicentre, Open-Label, Phase 2 Trial. The Lancet Oncology 2012, 13, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Elston, C.W.; Ellis, I.O. Pathological Prognostic Factors in Breast Cancer. I. The Value of Histological Grade in Breast Cancer: Experience from a Large Study with Long-term Follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Gu, K. ; C C Cowie; M I Harris Diabetes and Decline in Heart Disease Mortality in US Adults. JAMA 1999, 281, 1291. [Google Scholar] [CrossRef]
- Gunter, M.J.; Hoover, D.R.; Yu, H.; Wassertheil-Smoller, S.; Rohan, T.E.; Manson, J.E.; Li, J.; Ho, G.Y.F.; Xue, X.; Anderson, G.L.; et al. Insulin, Insulin-Like Growth Factor-I, and Risk of Breast Cancer in Postmenopausal Women. JNCI Journal of the National Cancer Institute 2009, 101, 48–60. [Google Scholar] [CrossRef]
- Lu, Y.; Hajjar, A.; Cryns, V.L.; Trentham-Dietz, A.; Gangnon, R.E.; Heckman-Stoddard, B.M.; Alagoz, O. Breast Cancer Risk for Women with Diabetes and the Impact of Metformin: A Meta-analysis. Cancer Medicine 2023, 12, 11703–11718. [Google Scholar] [CrossRef]
- Guidelines for Diagnosis and Treatment of Advanced Breast Cancer in China (2022 Edition). Journal of the National Cancer Center 2024, 4, 107–127. [CrossRef]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E. Early Breast Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Annals of Oncology 2019, 30, 1194–1220. [Google Scholar] [CrossRef]
- Weiss, A.; King, T.A. What Is the Role of Neoadjuvant Endocrine Therapy for Breast Cancer? Advances in Surgery 2022, 56, 275–286. [Google Scholar] [CrossRef]
- Cucciniello, L.; Gerratana, L.; Del Mastro, L.; Puglisi, F. Tailoring Adjuvant Endocrine Therapy in Early Breast Cancer: When, How, and How Long? Cancer Treatment Reviews 2022, 110, 102445. [Google Scholar] [CrossRef] [PubMed]
- Rouzier, R.; Perou, C.M.; Symmans, W.F.; Ibrahim, N.; Cristofanilli, M.; Anderson, K.; Hess, K.R.; Stec, J.; Ayers, M.; Wagner, P.; et al. Breast Cancer Molecular Subtypes Respond Differently to Preoperative Chemotherapy. Clinical Cancer Research 2005, 11, 5678–5685. [Google Scholar] [CrossRef]
- Tsimberidou, A.-M. Targeted Therapy in Cancer. Cancer Chemother Pharmacol 2015, 76, 1113–1132. [Google Scholar] [CrossRef]
- Stanowicka-Grada, M.; Senkus, E. Anti-HER2 Drugs for the Treatment of Advanced HER2 Positive Breast Cancer. Curr. Treat. Options in Oncol. 2023, 24, 1633–1650. [Google Scholar] [CrossRef] [PubMed]
- von Minckwitz, G.; du Bois, A.; Schmidt, M.; Maass, N.; Cufer, T.; de Jongh, F.E.; Maartense, E.; Zielinski, C.; Kaufmann, M.; Bauer, W.; et al. Trastuzumab Beyond Progression in Human Epidermal Growth Factor Receptor 2–Positive Advanced Breast Cancer: A German Breast Group 26/Breast International Group 03-05 Study. JCO 2009, 27, 1999–2006. [Google Scholar] [CrossRef]
- Swain, S.M.; Baselga, J.; Kim, S.-B.; Ro, J.; Semiglazov, V.; Campone, M.; Ciruelos, E.; Ferrero, J.-M.; Schneeweiss, A.; Heeson, S.; et al. Pertuzumab, Trastuzumab, and Docetaxel in HER2-Positive Metastatic Breast Cancer. N Engl J Med 2015, 372, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Guarneri, V.; Dieci, M.V.; Griguolo, G.; Miglietta, F.; Girardi, F.; Bisagni, G.; Generali, D.G.; Cagossi, K.; Sarti, S.; Frassoldati, A.; et al. Trastuzumab-Lapatinib as Neoadjuvant Therapy for HER2-Positive Early Breast Cancer: Survival Analyses of the CHER-Lob Trial. European Journal of Cancer 2021, 153, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.; Wu, Y.; Song, B.; Yi, M.; Yan, Y.; Mei, Q.; Wu, K. Recent Advances in Targeted Strategies for Triple-Negative Breast Cancer. J Hematol Oncol 2023, 16, 100. [Google Scholar] [CrossRef]
- Geyer, C.E.; Sikov, W.M.; Huober, J.; Rugo, H.S.; Wolmark, N.; O’Shaughnessy, J.; Maag, D.; Untch, M.; Golshan, M.; Lorenzo, J.P.; et al. Long-Term Efficacy and Safety of Addition of Carboplatin with or without Veliparib to Standard Neoadjuvant Chemotherapy in Triple-Negative Breast Cancer: 4-Year Follow-up Data from BrighTNess, a Randomized Phase III Trial. Annals of Oncology 2022, 33, 384–394. [Google Scholar] [CrossRef]
- Braal, C.L.; Jongbloed, E.M.; Wilting, S.M.; Mathijssen, R.H.J.; Koolen, S.L.W.; Jager, A. Inhibiting CDK4/6 in Breast Cancer with Palbociclib, Ribociclib, and Abemaciclib: Similarities and Differences. Drugs 2021, 81, 317–331. [Google Scholar] [CrossRef]
- Abdelmalak, M.; Singh, R.; Anwer, M.; Ivanchenko, P.; Randhawa, A.; Ahmed, M.; Ashton, A.W.; Du, Y.; Jiao, X.; Pestell, R. The Renaissance of CDK Inhibitors in Breast Cancer Therapy: An Update on Clinical Trials and Therapy Resistance. Cancers 2022, 14, 5388. [Google Scholar] [CrossRef] [PubMed]
- Sobande, F.; Dušek, L.; Matějková, A.; Rozkoš, T.; Laco, J.; Ryška, A. EGFR in Triple Negative Breast Carcinoma: Significance of Protein Expression and High Gene Copy Number. Cesk Patol 2015, 51, 80–86. [Google Scholar] [PubMed]
- Sabbah, D.A.; Hajjo, R.; Sweidan, K. Review on Epidermal Growth Factor Receptor (EGFR) Structure, Signaling Pathways, Interactions, and Recent Updates of EGFR Inhibitors. CTMC 2020, 20, 815–834. [Google Scholar] [CrossRef] [PubMed]
- Nnorom, S.O.; Akinyemi, O.; Tran, J.; Baig, H.; Cornwell, E.E.; Frederick, W.A.; Wilson, L.L. Color or Money?: The Impact of Socioeconomic Status and Race/Ethnicity on Breast Cancer Mortality. The American Journal of Surgery 2022, 224, 1403–1408. [Google Scholar] [CrossRef]
- Azin, A.; Tahmasebi, H.; Brar, A.; Azin, S.; Ko, G.; Covelli, A.; Cil, T. Racial, Ethnic and Socioeconomic Disparities in Diagnosis, Treatment, and Survival of Patients with Breast Cancer. The American Journal of Surgery 2023, 225, 154–161. [Google Scholar] [CrossRef]
- Yan, S.; Ji, J.; Zhang, Z.; Imam, M.; Chen, H.; Zhang, D.; Wang, J. Targeting the Crosstalk between Estrogen Receptors and Membrane Growth Factor Receptors in Breast Cancer Treatment: Advances and Opportunities. Biomedicine & Pharmacotherapy 2024, 175, 116615. [Google Scholar] [CrossRef]
- Tavčar Kunstič, T.; Debeljak, N.; Fon Tacer, K. Heterogeneity in Hormone-Dependent Breast Cancer and Therapy: Steroid Hormones, HER2, Melanoma Antigens, and Cannabinoid Receptors. Advances in Cancer Biology - Metastasis 2023, 7, 100086. [Google Scholar] [CrossRef]
Figure 1.
Distribution of Age.
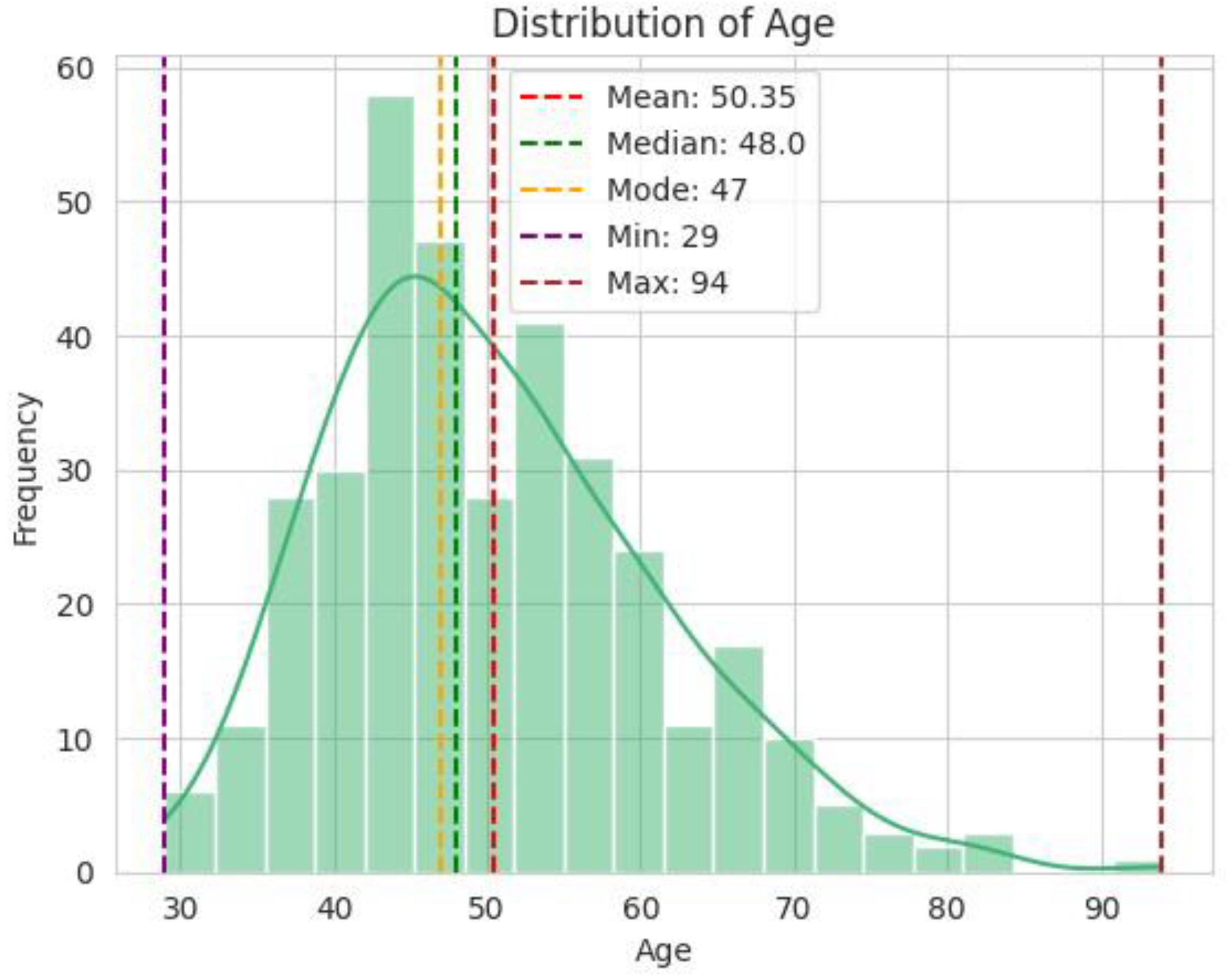
Figure 2.
Correlation between TNBC and Age.
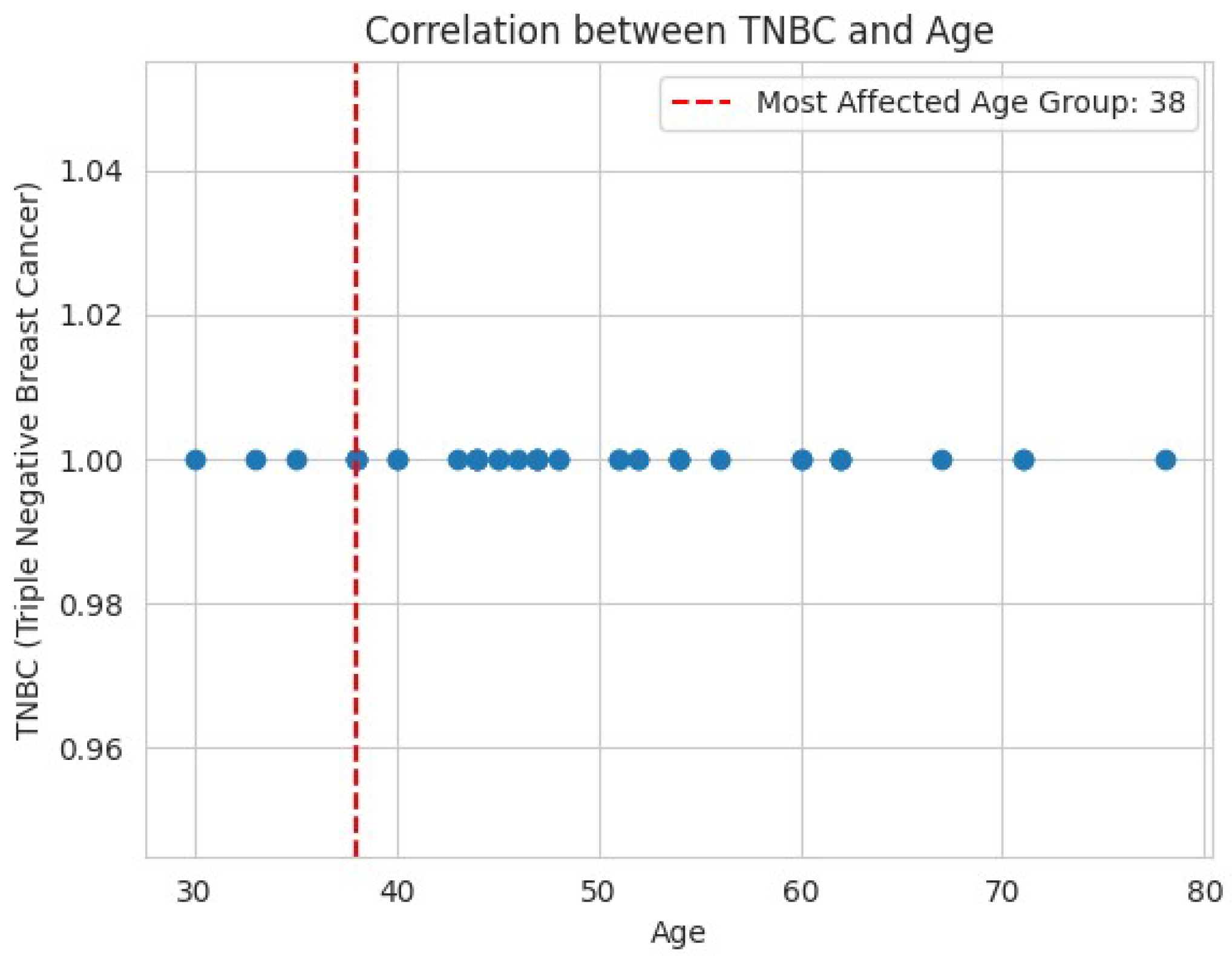
Figure 3.
Distribution of Demographic and Socioeconomic Variables.
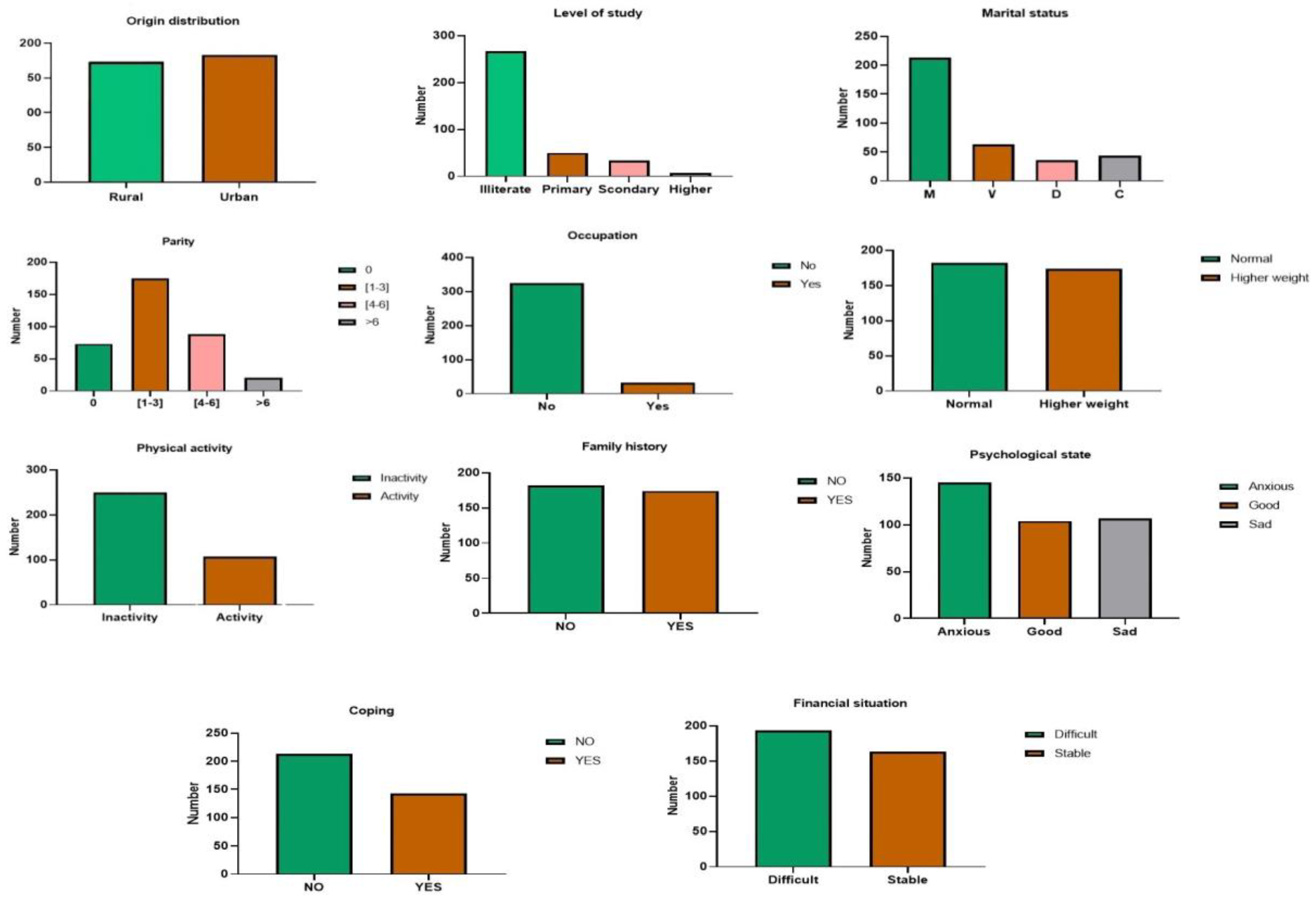
Figure 4.
Distribution of Demographic and Socioeconomic Variables.
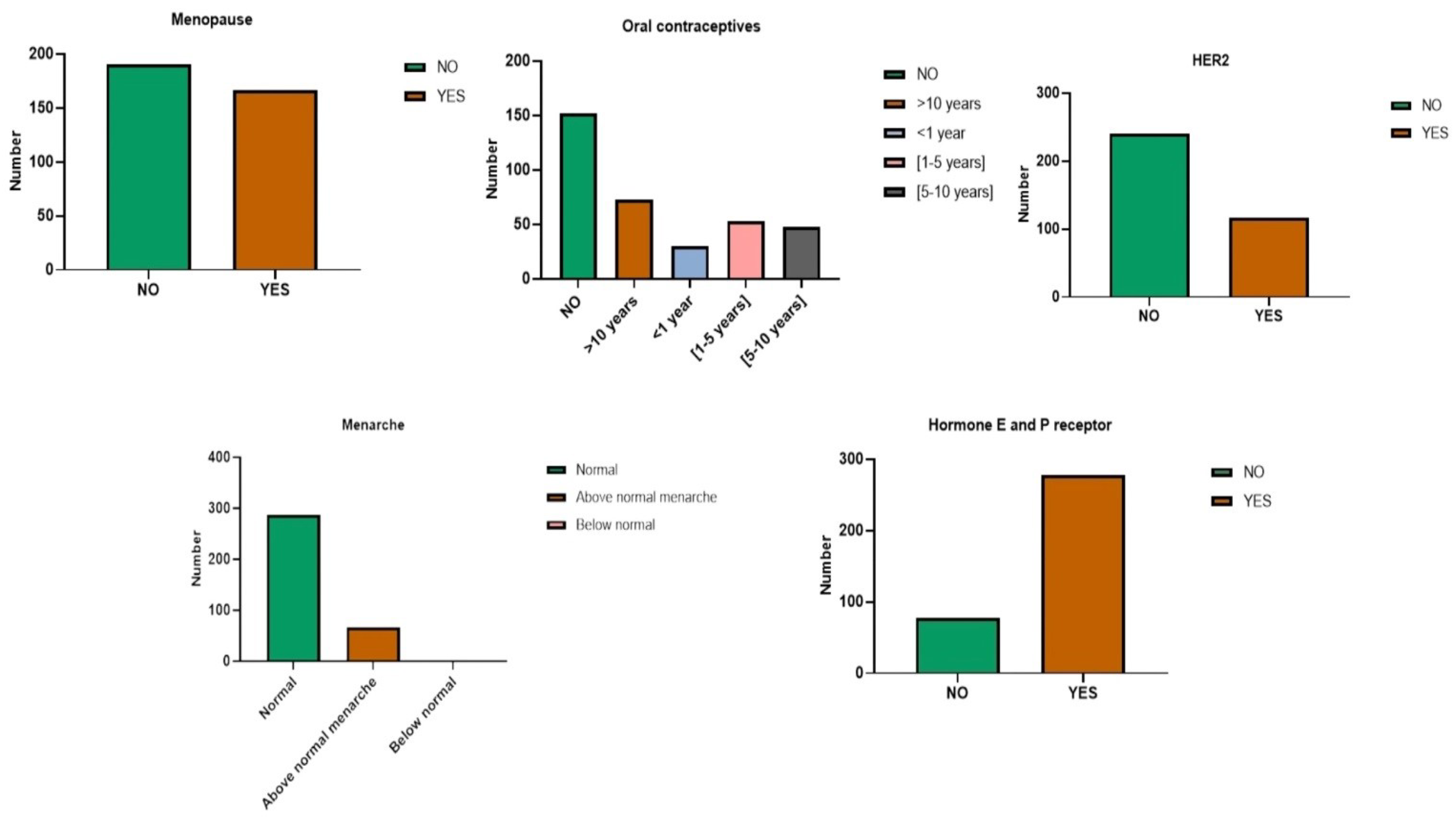
Figure 5.
Classification Based on Molecular Signatures.
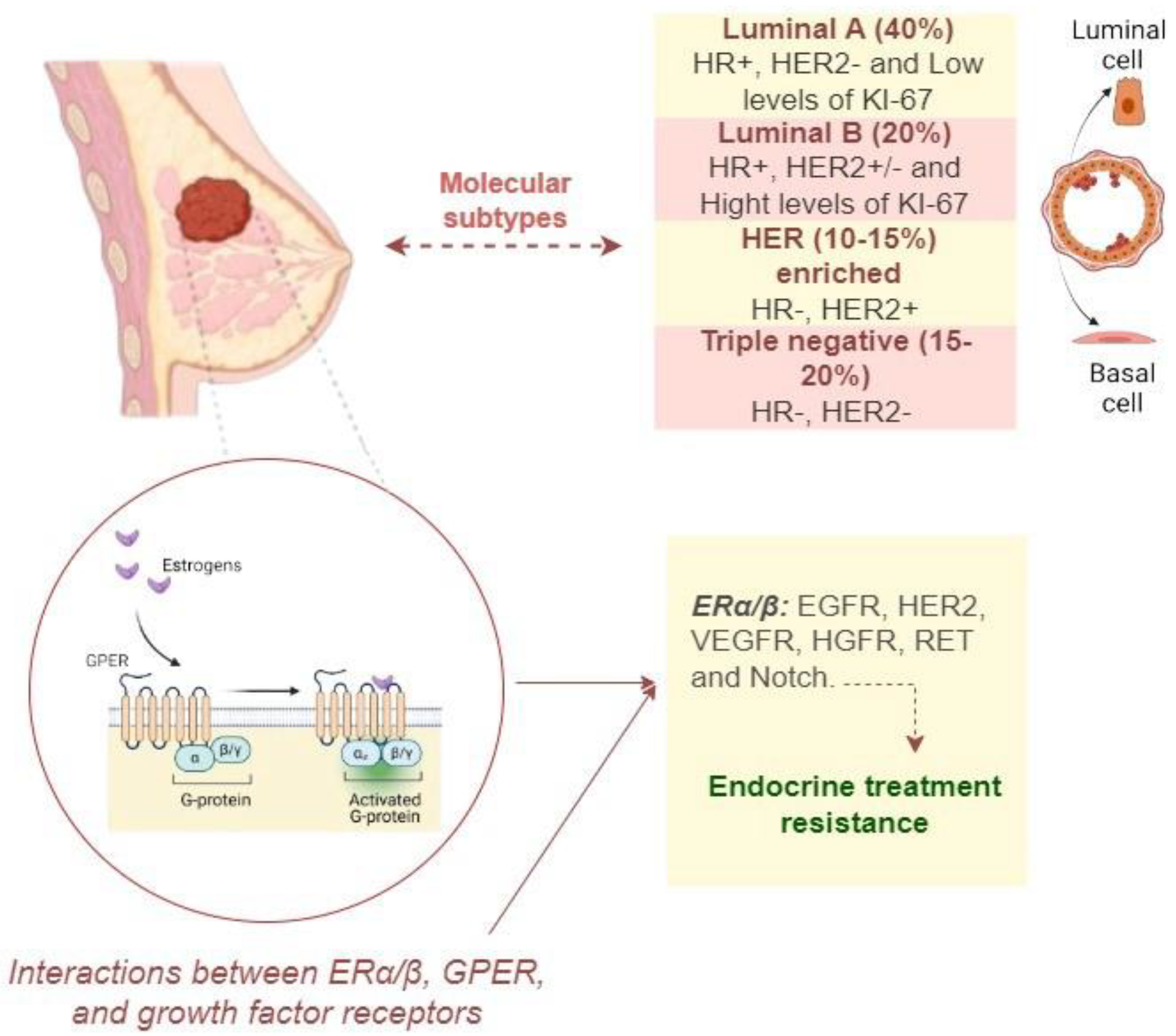
Figure 6.
Distribution of Histological Types, Tumor Grades, and Stages of Breast Cancer at Diagnosis.
Figure 6.
Distribution of Histological Types, Tumor Grades, and Stages of Breast Cancer at Diagnosis.
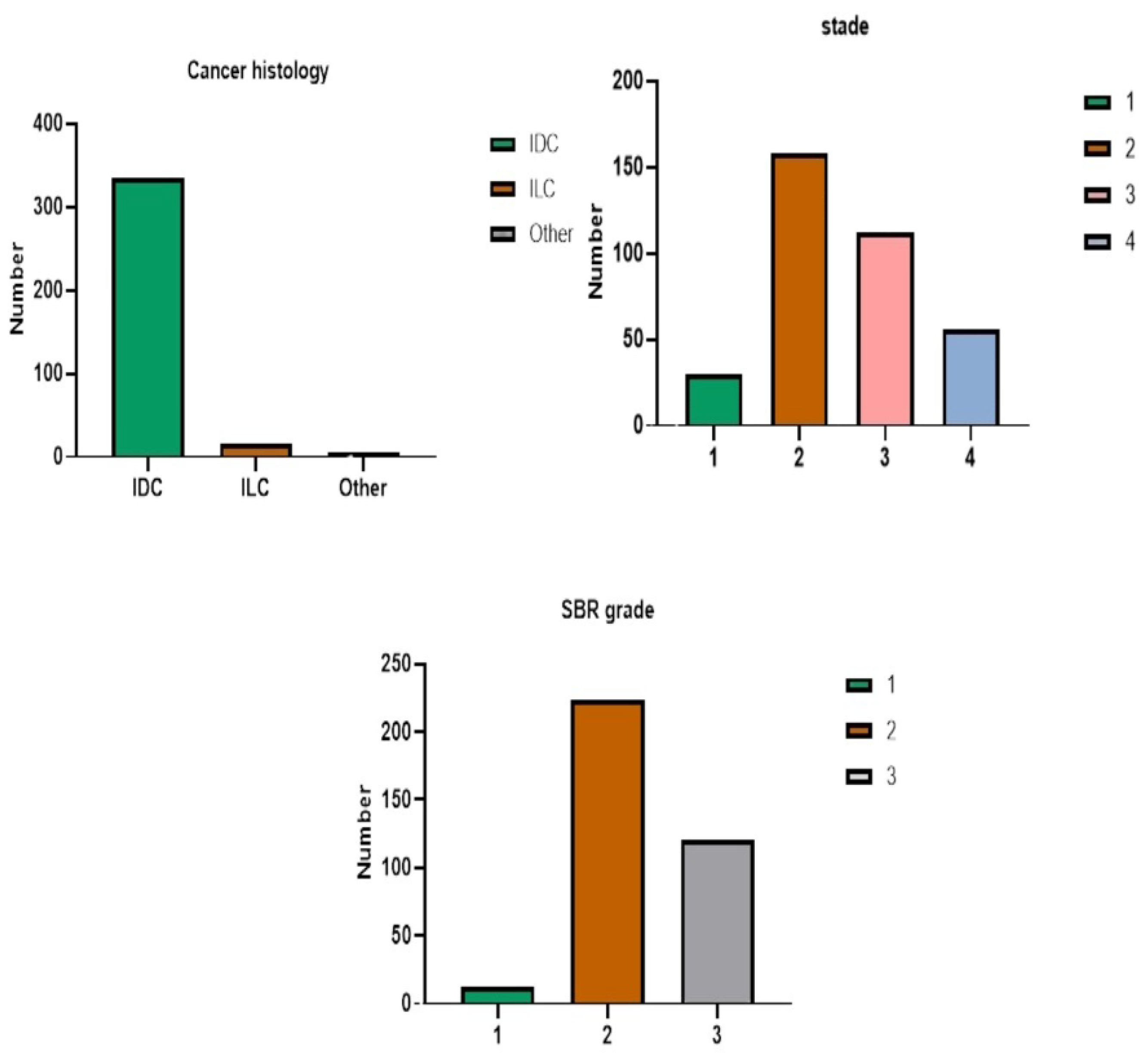
Figure 7.
Distribution of Clinical Variables.
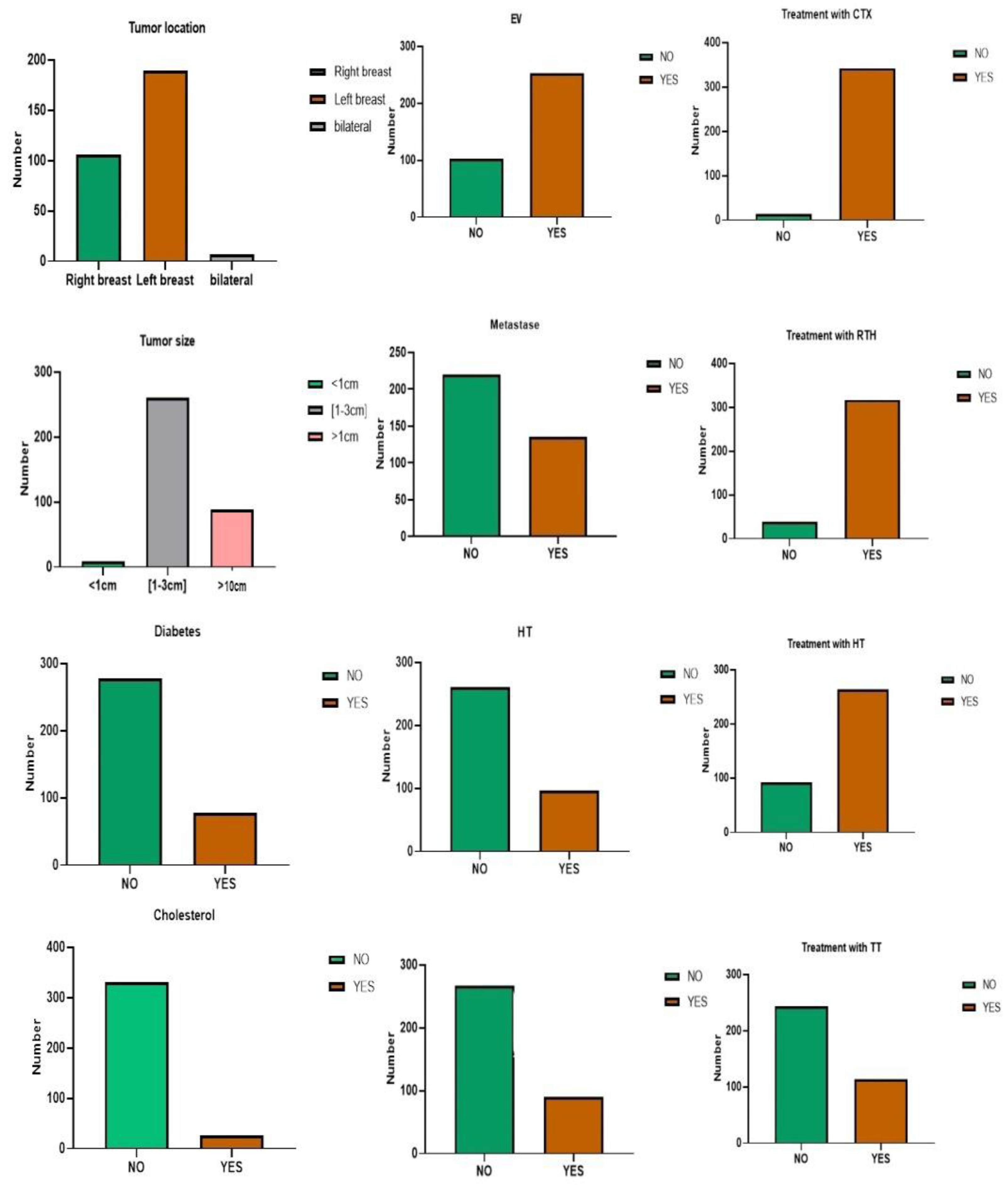
Figure 9.
Comparison of Treatment Strategies OP+CTX+RTH+HT (Letrozole) vs. OP+CTX+RTH+HT (Tamoxifen)) by Age and Menopausal Status.
Figure 9.
Comparison of Treatment Strategies OP+CTX+RTH+HT (Letrozole) vs. OP+CTX+RTH+HT (Tamoxifen)) by Age and Menopausal Status.
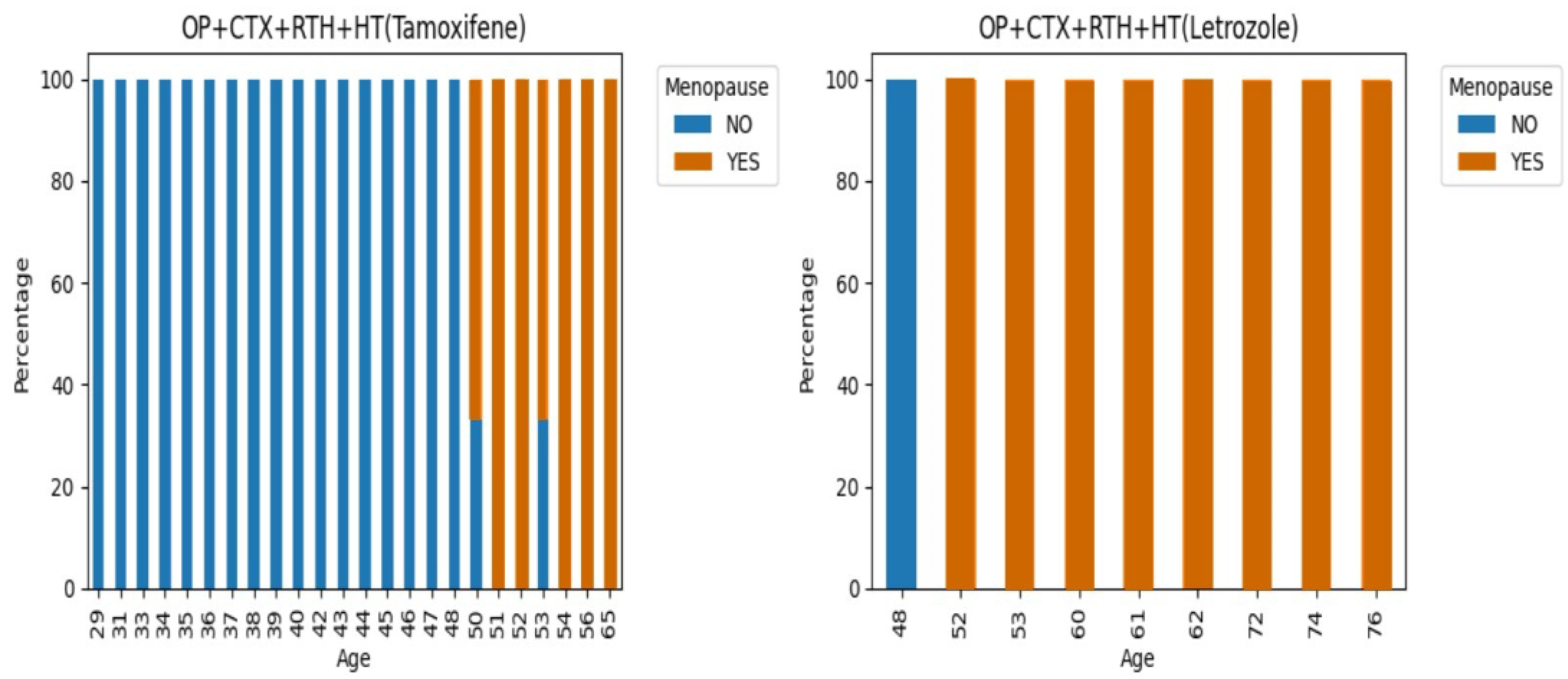

Table 1.
This is a table. Tables should be placed in the main text near to the first time they are cited.
Table 1.
This is a table. Tables should be placed in the main text near to the first time they are cited.
| Field | Variables |
|---|---|
| Socio-economic and demographic aspects | Origin, Level of study, Marital status, Parity, Occupation, BMI, Physical activity, Family history, psychological state, Coping and Financial situation. |
| Hormonal aspects | Menopause, Menarche, oral contraceptives, Hormone receptor and HER2. |
| Clinical aspects | Tumor Location, Cancer Histology, Stage, SBR Grade, Diabetes, Hypertension (HT), Cholesterol, Anemia, Tumor Size, Vascular Embolism (EV), Metastasis (Met), Treatment with Surgery (Op), Treatment with Chemotherapy (CTX), Treatment with Hormone Therapy (HT), Treatment with Radiotherapy (RT), Treatment with Targeted Therapy (TT). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



