
Submitted:
11 September 2024
Posted:
12 September 2024
You are already at the latest version
Abstract
Existing scales assessing family relations are usually quite long. Our aim was to develop and validate the Family Functioning and Cohesion Scale (FFCS), a self-reported short instrument consisting of 14 items. The validation of the FFCS was based on its administration through an online platform to 481 subjects living in 46 different countries around the world. Cronbach's alpha was 0.85 (ranging from 0.83 to 0.86 if any one item was deleted), signifying high internal consistency. The scale can be considered as a sole factor based on its high consistency, while factor analysis produced three factors corresponding to “communication”, “anger/resentment/aggression” and “values and beliefs”. Test-retest reliability correlation coefficient was found to be 0.88 at a 2-week interval. As far as external validity is concerned, the correlation coefficient of the FFCS with the General Functioning subscale of the McMaster Family Assessment Device (FAD) was 0.83. The high measures of consistency, reliability, and validity of the FFCS, combined with its short length, make it an invaluable tool for use in research as well as in any professional dealing with families in the clinical fields of psychiatry, psychology, social work or any other relevant specialty.
Keywords:
Family cohesion
; intrafamily relations
; family functioning
; scale
1. Introduction
Family is considered to be the primary source of attachment, nurturing, and socialization for humans in our society. Even though it has changed forms over the centuries, it continues to be an important, if not the most important, social unit. There are several definitions about family. In 1940 the U.S. Census Bureau adopted a definition of the family and ever since it has remained constant. According to this most traditional definition, “family is a group of two people or more related by birth, marriage, or adoption and residing together; all such people are considered as members of one family” [1,2,3].
A family can be described as a system which, through the bonds, relationships and interactions of its members, promotes their healthy development and evolution. As the primary source of development and socialization, family is one of the most important frameworks through which communication, social and other skills are formed, skills which are necessary for human survival and development [4]. Each family member is considered to be unique, with their own personality, attitude, integrity, feelings, thoughts and beliefs. Healthy bonds between members and the maintenance of balance and boundaries within the family are associated with the physical and mental health of its members. In a systematic review by Holtom-Viesel and Allan [5], there was evidence to suggest that families who had members with eating disorders, have worse family functioning than controls; similar findings have been reported in families of drug addicts [6]. Furthermore, in the systematic review of Lewandowski et al. [7] it was found that many studies showed a negative association between family functioning and disability, with the studies that were included in the review revealing poorer functioning in families of youth with chronic pain compared to healthy adolescents or population norms.
Cohesion is an important concept of group dynamics theory; it arises when bonds link members of a social group to one another and to the group as a whole. Without at least some degree of cohesion, groups are expected to disintegrate as members gradually withdraw from the group. A cohesive group will be more likely to prosper over time, since it retains its members and allows them to reach goals that would elude a more incoherent aggregate [8].
The cohesion within the family is strongly related to the latter’s functioning and it depends on various social determinants such as economic status, cultural identity, religious values, level of education, immigration and social isolation. It is also influenced by larger-scale events such as war, economic crises etc., since the family is the smallest social structure and is in constant interaction with the wider community [9,10,11].
It is important for professionals working with families, such as psychiatrists, psychologists, social workers etc., to have a short and easy-to-use tool to evaluate family cohesion in order to provide comprehensive assistance. The aim of the current study was to develop such a scale that would be helpful in the daily practice of those professionals.
Most of the existing scales which look into family structure, interactions and functioning are usually quite long. The McMaster Family Assessment Device (FAD) is a 60-item self-report scale [12,13], the Family Environment Scale (FES) is a 90-item scale [14], the Family Adaptability and Cohesion Evaluation Scale (FACES IV) is an 84-item scale [15]. Also, most of the existing scales are based on theoretical models depending on the scientific fields they come from; most are based on the systemic theory (FACES IV) or on cognitive theory (Family Communication Patterns Questionnaire) [16].
The atheoretical approach in psychiatry was first introduced by DSM-III and ICD-10 for the diagnosis of mental disorders. The third edition of DSM [17], published in 1980, constitutes a true nosological revolution because it remained atheoretical. The DSM-III offered a classification which intentionally ignored the etiological models of mental disorders and was focused on the task of providing unambiguous descriptions of these disorders by means of precise and exhaustive phenomenological diagnostic criteria [18]. Following this atheoretical approach, the Family Functioning and Cohesion Scale (FFCS) was developed as a short tool to assist any professionals in assessing functioning and cohesion of families.
The purpose of the present paper is to provide a detailed description of the FFCS and documentation on its validation.
2. Methods
2.1. Description of the Scale
The FFCS is a self-administered instrument consisting of fourteen items (see Appendix A). It focuses on the assessment of interpersonal relationships among family members, of their personal beliefs and of their interactions and behaviour in the family.
The respondents are requested to rate their degree of agreement on each one of 14 statements on family relationships and interactions in daily life. Each item of the FFCS can be rated on a four-point scale ''Completely true'', ''More true than false'', ''More false than true'' and ''Completely false''. For the items which contribute positively to a higher family cohesion (e.g. ''We always support each other'') the highest points (i.e. a score of ''3'') are given to the ''completely true'' statement (and a score of ''0'' to the ''completely false''), while for the ''negative'' items (e.g. '' There are episodes of physical violence in the family'') the score is reversed (see Scoring Rules in the Appendix A).
2.2. Sample and Assessment Procedures
Following the approval of the project by the institutional review ethics committee of Eginition Hospital, all subjects were approached through the network of the researchers and their collaborators, as well as through social media. On the Google Forms platform, which was used, all participants were first informed on the research nature of the project and those who gave their consent (N=481) proceeded with completing the FFCS. To evaluate test-retest reliability, a separate group (N=143) agreed to participate by providing their e-mail addresses, so they were assessed through the FFCS again at another time point two weeks later. The subscale for General Functioning of the McMaster Family Assessment Device (FAD) was also administered to this subgroup and was used as an external validator.
2.3. Data Analysis
Internal consistency was measured based on Cronbach's alpha for the whole scale, as well as for all but-one items (''alpha if item deleted''). The correlation of each item score to the total scale score (''item-total correlation'') was measured through Pearson's correlation coefficients. Additionally, the scale was subjected to factor analysis; the extraction of the factors was based on principal component analysis with the varimax rotation and the eigenvalue threshold was set at 1. Pearson's correlation coefficients were computed for the evaluation of test-retest reliability and for the external validation of the FFCS against the McMaster Family Assessment Device (FAD); the respective correlations pertained to total scale scores as well as (for test-retest) to single-item ratings. Finally, one-way ANOVA was used to detect possible differences in the total score of the FFCS and that of each item (Bonferroni corrected) among the four country groups in which the participants declared that they were residing (Greece, Rest of Europe & Australia, North/South America, Rest of the world). All assessments were performed and executed using the Statistical Package for Social Sciences for Windows, Version 28.0 [19].
3. Results
The FFCS was completed by 481 participants, living in various countries around the world (46 in total). The majority (57.8%) were from Greece, 22.9% were from the rest of Europe and Australia, 12.7% were from North or South America and 6.7% were from the rest of the world. Most of the participants (64.2%) were women, 54.1% were married and 95% were highly educated. About half of the participants were between 20 and 39 years old (Table 1).
Internal consistency measures of FFCS based on Cronbach’s alpha were found to be quite high for the total group (α=0.85) as well as for the group used in the test-retest reliability and external validity analysis (Table 2). Cronbach’s alpha remained practically unchanged when any one of the items was removed from the calculation (alpha if item deleted ranging from 0.83 to 0.86, Table 3). As also shown in Table 3, there were some items which did not strongly correlate with the scale overall, but, even for these items, Cronbach's alpha did not change significantly if any one of them was deleted. Factor analysis yielded three factors (with eigenvalues of ≥1, supported also by the screeplot shown in Figure 1) corresponding to “communication”, “anger/resentment/aggression” and “values and beliefs”; the loadings of each item on the factors is shown in Table 4.
As regards test-retest reliability, Pearson’s correlation coefficient was high (0.88 for the total score); scores for each individual item were found to be very satisfactory with p<0.001 for all (Table 5). More specifically, most items showed a high or moderate test-retest correlation coefficient, the highest value (r=0.85, denoting a high correlation) was for the item “There are episodes of physical violence in the family”. Two items “We all pray together” and “There are some members of the family who impose their wishes on others” showed a low (albeit statistically significant) correlation of the test and retest ratings. The correlation coefficient between total score of the FFCS and the FAD subscore for the family general functioning was high (0.83, p<0.001), providing evidence of high external validity. The ANOVA of the total score of the FFCS showed that country groups did not differ among them; for individual items, only the item “We all pray together” reached a statistically significant difference (p<0.014, after Bonferroni correction). For that item the mean value (±SD) was highest for country group “rest of the world” (2.59±1.21), followed by “North and South America” (1.75±1.01), “Greece” (1.54±0.90) and “rest of Europe and Australia” (1.37±0.75); in post-hoc analysis, the difference between “rest of the world” and each one of the other groups was statistically significant, as was the difference between “North and South America” and “rest of Europe and Australia”.
4. Discussion
The development of the FFCS was based on the need to provide an easy-to-use tool to professionals who deal with families in order to assist them in evaluating family relations and providing their clients with comprehensive and integrated care according to their needs. Thus, the total score of the FFCS provides a rough estimation of the degree of family functioning and cohesion, while a low rating on any one item provides an indication that attention should be focused on the specific aspect of family life. Furthermore, the subscales (factors), which emerged in the factor analysis of the FFCS, provide additional information on the three main areas of possible familial dysfunction, i.e. “communication”, “anger/resentment/aggression” and “values and beliefs”.
The FFCS has a high internal consistency and external validity. Four of its 14 items showed a lower correlation with the scale in total, but all of them were also found to belong to the scale, since the removal of any one of them did not change substantially the Cronbach’s alpha value. The item “We all pray together” had the lowest correlation of all, probably because religious rituals do not seem to be strongly related to other aspects of family functioning; we have, however, kept this item on the scale, since praying may be important to some families and we believe that the relevant information is useful to professionals dealing with them. The other three items with a relatively low item-total correlation are all associated with overt verbal and physical violence or the presence of a dominant member in the family. It seems that this pattern might also be relatively independent of other aspects of family function.
The external validity of the FFCS was based on its correlation with the McMaster Family Assessment Device sub-scale on family functioning. The FAD has been developed in 1983 [12] and it has been used in various studies for understanding the relationship of family functioning to a wide range of mental and physical health problems across different cultures [20,21,22]. The correlation coefficient between the FFCS and the FAD subscale was very satisfactory (r=0.83).
Based on test-retest reliability measures, the whole FFCS and each of its items were found to be stable in time. The item with the highest correlation coefficient between the two measures taken in two weeks time was “There are episodes of physical violence in the family”. Physical violence, thus, emerges as the most temporally stable characteristic of family life, one that, if it has taken place is not forgotten or “undone”. This is in accordance with numerous studies which show that physical violence within the family stays in memory of all members who have experienced it and that, when it occurs, it is consistently reported by all members; it is indeed well-documented that exposure to physical violence within the family can have a lasting profound effect on the individuals involved on the physical, emotional, and psychological level, and memories of such experiences can be persistent [23,24,25].
Finally, the results of the ANOVA showed that the total score of the FFCS and all but one of its items are rated in a similar fashion independent of geographic area of residence; the only item which differed among country groups was the item “We all pray together”. This result shows that, in general, the performance of the FFCS follows similar patterns around the world.
In conclusion, the short length and atheoretical approach of the FFCS, its excellent psychometric properties and its three factors, each of which assesses specific needs and problems of the families under examination, make it a useful instrument for use in research as well as in any professional dealing with families in the clinical fields of psychiatry, psychology, social work or any other relevant specialty.
Author Contributions
Conceptualization, Vagioula Tsoutsi and Dimitris Dikeos; Data curation, Vagioula Tsoutsi and Dimitris Dikeos; Formal analysis, Vagioula Tsoutsi and Dimitris Dikeos; Funding acquisition, Vagioula Tsoutsi and Dimitris Dikeos; Investigation, Vagioula Tsoutsi and Dimitris Dikeos; Methodology, Vagioula Tsoutsi and Dimitris Dikeos; Project administration, Vagioula Tsoutsi and Dimitris Dikeos; Resources, Vagioula Tsoutsi and Dimitris Dikeos; Supervision, Vagioula Tsoutsi and Dimitris Dikeos; Validation, Vagioula Tsoutsi and Dimitris Dikeos; Visualization, Vagioula Tsoutsi and Dimitris Dikeos; Writing – original draft, Vagioula Tsoutsi and Dimitris Dikeos; Writing – review & editing, Vagioula Tsoutsi and Dimitris Dikeos; Both authors have read and agreed to the published version of the manuscript.
Funding
No funding was received for conducting this study.
Institutional Review Board Statement
Institutional Ethics Committee Statement: The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Institutional Ethics Committee of the First Department of Psychiatry, Eginition Hospital, National and Kapodistrian University of Athens, Greece (222/27-05-2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author, but restrictions apply to the availability of these data, which were used under license from the First Department of Psychiatry, Eginition Hospital, National and Kapodistrian University of Athens for the current study, and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission from the First Department of Psychiatry, Eginition Hospital, National and Kapodistrian University of Athens.
Conflicts of Interest
The authors declare no conflict of interest regarding this work.
Appendix A
Family Functioning and Cohesion Scale (FFCS)
Please read each statement and then tick the appropriate box after considering your family’s usual practices.
- 1.
-
We tend to share the same beliefs (social, religious, political)
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
- 2.
-
We enjoy dining together
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
- 3.
-
We all pray together
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
- 4.
-
We feel better when we do not spend much time together
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
- 5.
-
All members of the family share the same values
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
- 6.
-
Decisions are usually taken by consensus
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
- 7.
-
There are some members of the family who impose their wishes on others
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
- 8.
-
We often get angry with each other
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
- 9.
-
We often yell at each other
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
- 10.
-
There are episodes of physical violence in the family
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
- 11.
-
We talk openly with each other
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
- 12.
-
We usually problem-solve together
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
- 13.
-
We always support each other
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
- 14.
-
We draw strength from one another
- ☐Completely true
- ☐More true than false
- ☐More false than true
- ☐Completely false
Scoring Rules
For items 1-3, 5-6 and 11-14 the scoring is as follows:
- Completely true: 3
- More true than false: 2
- More false than true: 1
- Completely false: 0
For items 4 and 7-10 the scoring is as follows:
- Completely true: 0
- More true than false: 1
- More false than true: 2
- Completely false: 3
- Factor 1 (communication) consists of items 2, 4, 6, 11-14
- Factor 2 (anger/resentment/aggression) consists of items 7-10
- Factor 3 (values and beliefs) consists of items 1, 3, 5
References
- P.C. Glick. American Families. John Wiley & Sons, New York, 1957.
- J. Fields, L. J. Fields, L. Casper. America’s families and living arrangements. Current Population Reports, Series Census Bureau, Washington, DC, 2001; pp 20–537.
- U.S. Census Bureau. Available online: https://www.census.gov/programs-surveys/cps/technical-documentation/subject-definitions.html (assessed 10 October 2023).
- S. Minuchin. Families and Family Therapy. Routledge, Abington, 2018.
- A. Holtom-Viesel, S. Allan. A systematic review of the literature on family functioning across all eating disorder diagnoses in comparison to control families. Clin. Psychol. 2014, 34, 29–43. [Google Scholar] [CrossRef]
- J. I. Zimic, Jakic V. Familial risk factors favoring drug addiction onset. J. Psychoactive Drugs 2012, 44, 173–185. [Google Scholar] [CrossRef]
- A. Lewandowski, T. Palermo, J. Stinson, S. Handley, C, Chambers. Systematic review of family functioning in families of children and adolescents with chronic pain. J. Pain 2010, 11, 1027–1038. [Google Scholar] [CrossRef]
- D.R. Forsyth. Components of cohesion. In: Group Dynamics, 5th ed.; Forsyth DR, Wadsworth Cengage Learning, Belmont, 2010, pp. 118–122.
- J. Georgas, J. W. J. Georgas, J. W. Berry, F. J. R. van de Vijver, Ç. Kağitçibaşi, & Y. H. Poortinga, (Eds.), Families across cultures: A 30-nation psychological study. 2006. [Google Scholar] [CrossRef]
- T. McNeill. Family as a social determinant of health: implications for governments and institutions to promote the health and well-being of families. Healthc. Q. 2010, 14, 60–67. [Google Scholar] [CrossRef]
- F. Booysen, F. Botha, E. Wouters. Conceptual causal models of socioeconomic status, family structure, family functioning and their role in public health. BMC Public Health 2021, 21, 191. [Google Scholar] [CrossRef]
- N. B. Epstein, L.M. Baldwin, D.S. Bishop. The McMaster family assessment device. J. Marital. Fam. Ther. 1983, 9, 171–180. [Google Scholar] [CrossRef]
- I. W. Miller, N.B. Epstein, D.S. Bishop, G.I. Keitner. The McMaster Family Assessment Device: Reliability and validity. J. Marital. Fam. 1985, 11, 345–356. [Google Scholar] [CrossRef]
- R.H. Moos, B.S. R.H. Moos, B.S. Moos. Family environment scale manual: Development, applications and research, 4th ed. Mind Garden Inc, Palo Alto California, 2009. [Google Scholar]
- D. Olson. FACES IV and the circumplex model: Validation Study. J. Marital. Fam. Ther. 2011, 37, 64–80. [Google Scholar] [CrossRef] [PubMed]
- S. Gupta, Geetika. Family Communication Patterns Questionnaire: Development and validation. Int. J. Recent. Technol. Eng. 2019, 8, 542–550.
- American Psychiatric Association. Diagnostic and Statistical Manual for Mental Disorders; 3rd ed. (DSM–III). American Psychiatric Association, 1980.
- B. Hjørland. The Paradox of Atheoretical Classification. Knowledge Organization 2016, 43, 313–323. [Google Scholar] [CrossRef]
- IBM Corp. Released 2021. IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp.
- H. A. MacPherson, A.L. Ruggieri, R.E. Christensen, E. Schettini, K.L. Kim, S.A. Thomas, D.P. Dickstein. Developmental evaluation of family functioning deficits in youths and young adults with childhood-onset bipolar disorder. J. Affect. Disord. 2018, 235, 574–582. [Google Scholar] [CrossRef] [PubMed]
- G. G. Leibach, R.S. Everhart. Family assessment device: Real-world validity in urban families of children with asthma. J. Fam. Psychol. 2017, 31, 642–647. [Google Scholar] [CrossRef] [PubMed]
- G. I. Keitner, J. Fodor, C.E. Ryan, I.W. Miller, D.S. Bishop, N.B. Epstein. A cross-cultural study of major depression and family functioning. Can. J. Psychiatry, 1991, 36, 254–259. [Google Scholar] [CrossRef] [PubMed]
- L. Jobe-Shields, A.D. Moreland, R.F. Hanson, A. Amstadter, B.E. Saunders, D.G. Kilpatrick. Co-occurrence of witnessed parental violence and child physical abuse from a national sample of adolescents. J. Child. Adolesc. Trauma, 2018, 11, 129–139. [Google Scholar] [CrossRef] [PubMed]
- C. A. Moylan, T.I. Herrenkohl, C. Sousa, E.A. Tajima, R.C. Herrenkohl, M.J. Russo. The effects of child abuse and exposure to domestic violence on adolescent internalizing and externalizing behavior problems. J. Fam. Violence 2010, 25, 53–63. [Google Scholar] [CrossRef] [PubMed]
- T. I. Herrenkohl, C. Sousa, E.A. Tajima, R.C. Herrenkohl, C.A. Moylan. Intersection of child abuse and children’s exposure to domestic violence. Trauma Violence Abuse 2008, 9, 84–99. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Factor Analysis Screeplot.
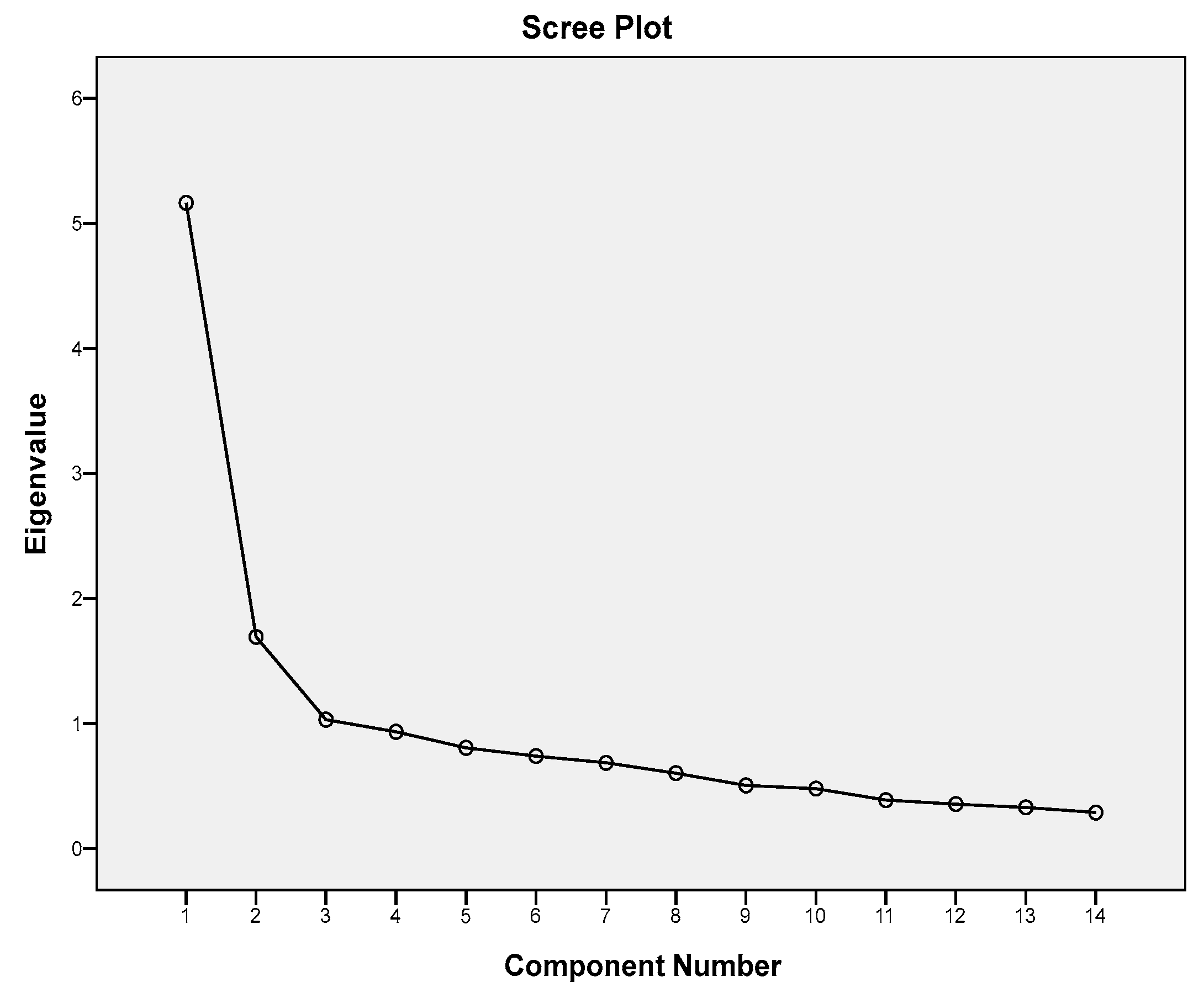

Table 1.
Sample characteristics.
| Demographics | N=481 (%) |
| Female | 309 (64.2%) |
| Married | 260 (54.1%) |
| Employed | 328 (68.2%) |
| High education | 457 (95%) |
| Age group | |
| Under 20 | 11 (2.3%) |
| 20-29 | 118 (24.5%) |
| 30-39 | 110 (22.9%) |
| 40-49 | 99 (20.6%) |
| 50-59 | 82 (17.0%) |
| 60-69 | 47 (9.8%) |
| 70 and above | 14 (2.9%) |
| Country group | |
| Greece | 278 (57.8%) |
| Rest of Europe & Australia | 110 (22.9%) |
| North/South America | 61 (12.7%) |
| Rest of the world | 32 (6.7%) |
Table 2.
Cronbach’s alpha of FFCS for whole sample and for the group of subjectswho participated in the test-retest and external validation study.
Table 2.
Cronbach’s alpha of FFCS for whole sample and for the group of subjectswho participated in the test-retest and external validation study.
| All subjects (n=481) | 0.85 |
| Test-retest group (n=143) | 0.88 |
Table 3.
Single item statistics.
| N=481 | |||
| Mean ±SD* | Item-total correlation | Cronbach's alpha if item deleted | |
| Total score of FFCS | 27.76±6.46 | - | - |
| Items | |||
| 1. We tend to share the same beliefs (social, religious, political). | 1.94±0.78 | 0.42 | 0.84 |
| 2. We enjoy dining together. | 2.40±0.74 | 0.57 | 0.83 |
| 3. We all pray together. | 0.59±0.95 | 0.15 | 0.86 |
| 4. We feel better when we do not spend much time together. | 2.05±0.86 | 0.51 | 0.83 |
| 5. All members of the family share the same values. | 1.98±0.79 | 0.60 | 0.83 |
| 6. Decisions are usually taken by consensus. | 2.05±0.72 | 0.60 | 0.83 |
| 7. There are some members of the family who impose their wishes on others. | 1.51±0.91 | 0.39 | 0.84 |
| 8. We often get angry with each other. | 1.63±0.81 | 0.53 | 0.83 |
| 9. We often yell at each other. | 1.99±0.86 | 0.35 | 0.84 |
| 10. There are episodes of physical violence in the family. | 2.87±0.48 | 0.27 | 0.84 |
| 11. We talk openly with each other. | 2.12±0.81 | 0.63 | 0.83 |
| 12. We usually problem-solve together. | 2.00±0.77 | 0.67 | 0.82 |
| 13. We always support each other. | 2.42±0.69 | 0.67 | 0.83 |
| 14. We draw strength from one another. | 2.21±0.79 | 0.59 | 0.83 |
*SD = standard deviation.
Table 4.
Factor Analysis: Rotated Component Matrix.
| Factors | |||
|---|---|---|---|
| 1: communication | 2: anger/resentment/aggression | 3: values and beliefs | |
| 1. We tend to share the same beliefs (social, religious, political). | .249 | .208 | .647 |
| 2. We enjoy dining together. | .571 | .231 | .282 |
| 3. We all pray together. | .114 | -.195 | .635 |
| 4. We feel better when we do not spend much time together. | .419 | .357 | .255 |
| 5. All members of the family share the same values. | .455 | .243 | .610 |
| 6. Decisions are usually taken by consensus. | .593 | .253 | .294 |
| 7. There are some members of the family who impose their wishes on others. | .230 | .579 | .025 |
| 8. We often get angry with each other. | .214 | .813 | .093 |
| 9. We often yell at each other. | .015 | .862 | -.010 |
| 10. There are episodes of physical violence in the house. | .332 | .432 | -.395 |
| 11. We talk openly with each other. | .749 | .170 | .137 |
| 12. We usually problem-solve together. | .810 | .120 | .170 |
| 13. We always support each other. | .821 | .149 | .078 |
| 14. We draw strength from one another. | .789 | .081 | .064 |
Table 5.
Test-retest reliability.
| N=143 | Test | Retest | Test-retest |
|---|---|---|---|
| Mean ±SD* | Mean ±SD* | Pearson correlation (r) | |
| Total score of FFCS | 26.85±6.34 | 27.82±6.36 | 0.88 |
| Items | |||
| 1. We tend to share the same beliefs (social, religious, political). | 1.85±0.74 | 1.87 ± 0.7 | 0.75 |
| 2. We enjoy dining together. | 2.44 ± 0.67 | 2.31 ± 0.77 | 0.64 |
| 3. We all pray together. | 0.31 ± 0.65 | 0.41 ± 0.71 | 0.45 |
| 4. We feel better when we do not spend much time together. | 2.00 ± 0.83 | 2.06 ± 0.81 | 0.62 |
| 5. All members of the family share the same values. | 1.90 ± 0.74 | 1.97 ± 0.73 | 0.73 |
| 6. Decisions are usually taken by consensus. | 1.91 ± 0.73 | 1.91 ± 0.66 | 0.69 |
| 7. There are some members of the family who impose their wishes on others. | 1.66 ± 0.8 | 1.75 ± 0.85 | 0.49 |
| 8. We often get angry with each other. | 1.50 ± 0.83 | 1.70 ± 0.77 | 0.64 |
| 9. We often yell at each other. | 1.85 ± 0.88 | 2.00 ± 0.82 | 0.70 |
| 10. There are episodes of physical violence in the house. | 2.82 ± 0.51 | 2.81 ± 0.51 | 0.85 |
| 11. We talk openly with each other. | 1.91 ± 0.76 | 2.07 ± 0.68 | 0.59 |
| 12. We usually problem-solve together. | 1.90 ± 0.78 | 2.08 ± 0.65 | 0.60 |
| 13. We always support each other. | 2.47 ± 0.65 | 2.54 ± 0.66 | 0.67 |
| 14. We draw strength from one another. | 2.34 ± 0.67 | 2.37 ± 0.68 | 0.77 |
*SD = standard deviation, P < 0.001 for all.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



