
Submitted:
11 September 2024
Posted:
12 September 2024
You are already at the latest version
Abstract
Emerging risk factors for childhood (<5 years) anemia cases in low-income countries have not been limited to COVID-19 and the spread of infectious diseases, hidden hunger, and other economic factors. Yet the effects of climatic factors, such as ambient temperatures, on child anemia have been in its infancy. In this population-based study, we study the region-specific associations between child anemia and ambient temperatures in 43 countries of Africa from 2000-2019. Using generalized linear regression models, we found that after adjusting for key covariates, the risk that temperatures pose on child anemia varies across the four African regions (Western, Eastern, Central, and Southern). This suggests that ambient temperatures have varying effects on child anemia by region. Other studies are needed in other low-income settings to expand our findings.
Keywords:
Child anemia
; temperatures
; Africa
; Low-income
Introduction
Anemia is characterized by a hemoglobin level below the 5th percentile for a given age [1]. With nearly 1.92 billion people, or one-fourth of the world’s population, affected in 2021, anemia is a widely prevalent blood condition with a 420 million increase in occurrences over the past few decades [2]. Children are the most anemia-affected age group, with the World Health Organization (WHO) reporting that around 40% of children aged 6-59 months had anemia globally [3]. In Africa during 2019, nearly 103 million children were affected by anemia [3]. Furthermore, anemia reached an economic burden of US $14,535 per patient annually, 54% higher than the $9,451 average cost for non-anemic patients [4].
Past studies suggest that low socioeconomic status [5], maternal education [6], nutritional deficiencies [7], and air pollution [8] have been linked to increased anemia in children. However, temperature change is an underrepresented risk factor that warrants further research [9]. Globally, Africa is one of the most susceptible regions to climate change, with ambient temperatures on the rise [10]. It is still unclear whether global warming affects childhood anemia, particularly in low and middle-income countries (LMICs) [9]. A past study also showed for each 1°C increase in annual temperature, the odds of anemia prevalence rise by 1.138 [95% CI: 1.134–1.142] [9]. Moreover, African countries with higher temperatures report a higher prevalence of anemia among children, whereas those with lower temperatures show lower anemia rates [9]. On the other hand, colder temperatures have also been linked with adverse child health effects, including respiratory disease and infant mortality, suggesting that colder temperatures may also be an important area of focus [11]. This association underscores the importance of focusing on temperature as a critical risk factor for childhood anemia [9].
We hypothesize that there will be regional differences between temperatures and child anemia in Africa. Consequently, this study aims to address the knowledge gap between temperatures and the prevalence of anemia rates in children from African data in the past two decades. The findings can serve as a basis for creating new future policies to reduce the burden of child anemia.
Methods
This is a population based study for Africa from 2000-2019. Data for the number of children (<5 years of age) with anemia for 43 African nations, segregated into four regions (Table 1). This outcome data was obtained from the World Health Organization (WHO). Prevalence of child anemia considered the ratio of annual number of children with anemia to the country-specific population for children less than 5 years of age. Aside from our primary outcome, exposure data for country-specific annual mean air temperature data from 2000-2019 was obtained from World Bank: https://www.kaggle.com/datasets/palinatx/mean-temperature-for-countries-by-year-2014-2022?resource=download.
We included covariate data on country-specific annual mean air pollution (specifically NO2 in μg/m3), cereal yield (in tonnes per hectare), gross domestic product (GDP), prevalence of child stunting, prevalence of reproductive women with anemia (moderate levels), average children’s hemoglobin, and annual trend.
We modelled the region-specific associations between the annual number of children and average air temperatures using generalized linear model, specifically negative binomial regression using autocorrelation order 1 (i.e., AR1). This is because the outcome’s variance was much greater than its mean, leading to overdispersion of data. Model coefficients were exponentiated to be interpreted as rate ratios (RR) for each 1℃ rise in annual mean air temperatures. 95% confidence intervals were evaluated at P<0.05 using Student’s two-sided t-tests. Microsoft Excel (V.2021) and RStudio (V.4.1.1) were used for computation, analyses and figure composition.
Results
Over the twenty years of our study from 43 countries, within four regions of Africa, there were a total of 1,775,405,490 children with anemia reported by WHO data. Out of the four African regions, West Africa bared the highest proportion of child anemia cases (44.3%), whereas Southern Africa has the lowest proportion (2.9%). Table 1 shows the total annual number of children with anemia for each country and corresponding region from 2000-2019.
On a geographic perspective, the prevalence of child anemia are observed to be the highest over Western and Eastern Africa (Figure 1A). Similarly annual mean air temperatures are also highest in Western Africa reaching 29℃, whereas the lowest mean air temperature in Southern Africa 13℃ throughout the 2000 to 2019 period (Figure 1B).
Our models suggest that for each 1℃ rise in air temperature the RR for children anemia in Western [0.989 (P=0.0013)], Eastern [0.993 (P=0.001)], Central [1.023 (P<0.0001)], and Southern Africa [1.005 (P=0.006)] had differing magnitude associations. The main findings from this suggests that Central and Southern African regions had a positive association between child anemia and air temperatures, whereas Western and Eastern regions had a negative association. Overall, Central Africa had the strongest effect of annual mean air temperatures on child anemia from 2000-2019.
Discussion
Our findings from the WHO between 2000-2019 show that Eastern and Western Africa demonstrated an inverse relationship between the prevalence of childhood anemia and temperature, whereas Central and Southern Africa exhibit a direct relationship. One previous study also found regional differences in Africa with an association between ambient heat and child mortality [12]. This past study also showed a 1.27 risk ratio [95% CI: 1.19–1.36] for child mortality in Eastern Africa associated with heat exposure while also showing a 0.92 risk ratio [95% CI: 0.88–0.97] for child mortality in Southern Ghana, Côte d’Ivoire, and Nigeria - all countries located in Western Africa [12]. Brimicombe et al. [12] study is consistent with ours in that there are regional differences in the association between temperature and child health. Although these results do not directly correspond with our data, they provide further evidence suggesting regional differences in the association between childhood health factors, such as anemia, and temperature.
The biological pathways linking temperature to childhood anemia are complex, involving various environmental effects [9]. Warmer temperatures increase parasite spread, heightening malaria risk and consequently raising anemia rates, with studies suggesting that this effect on childhood anemia is significantly mediated through malaria infection [13,14,15]. Moreover, the prevention of anemia was shown to result from avoidance of exposure to heat, which further links increased heat with a rise in anemia [16]. Although previous studies have linked the lack of fluid retention with the severity of anemia, further research is needed to reach a definitive conclusion [17]. A history of diarrhea has also been identified as a risk factor for childhood anemia, with an adjusted odds ratio of 2.44 [95% CI: 1.03-3.85], indicating a significant association between diarrhea and anemia [18]. Additionally, high temperatures in combination with drought can worsen water shortages, causing poor sanitation and hygiene, contributing to environmental enteric dysfunction – a significant risk factor for childhood anemia [19,20]. Conversely, a previous study also found that cold temperatures affect child health by increasing severe neonatal infections, such as pneumonia and sepsis, which can further exacerbate an infant’s physiological susceptibility to heat and cold in Africa [21]. Additionally, a past study indicates that child mortality in South Africa was associated with both cold and heat and the total attributable mortality was 3.4%, mostly from cold (3.0%) rather than heat (0.4%), using confidence intervals determined by an approximate parametric bootstrap estimator [22,23].
Overall, the impacts of climate change on temperature-related neonatal mortality were largest in countries that had relatively high baseline neonatal mortality rates and experienced large temperature increases due to climate change (Sierra Leone, Ethiopia, Liberia, Mali, Guinea, Benin, Cameroon, Nigeria, Angola, Timor-Leste, Haiti) [21]. Thus, colder temperatures have been associated with negative child health outcomes, such as respiratory diseases and infant mortality, indicating that cold temperatures should be further analyzed.
As discussed, there are regional differences in the association between child anemia and temperature in Africa. Understanding how temperatures are directly linked to childhood anemia in low-income regions such as Africa is essential for addressing resulting health issues. [24]. Specifically, high temperatures and anemic rates in Western Africa, Central Africa, and parts of Eastern Africa have been affected by several factors, such as malnutrition and malaria infection, which have mediated the associations between annual mean temperature and childhood anemia by 11.40% and 9.74%, respectively [9]. On the other hand, infections are a risk factor for childhood anemia [8] and cold temperatures have been shown to increase pneumonia risk by 1.06 times [95% CI: 0.98–1.14] in children [25], thus suggesting that colder temperatures are also associated with increased infection rates. Additionally, other factors, such as poverty or lack of education, have also been linked with influencing childhood anemia [26].
This study was limited by the data being generalized to regions of Africa, which did not allow for the consideration of specific disparities such as healthcare access [27], access to adequate nutrition [28,29], and sufficient sanitation [30], in turn leading to increased rates of childhood anemia that may have confounded the results. Additionally, since topographic elevation has been found to be associated with temperature [31], the generalization of data to large regions may have impaired the temperature data collected due to the possibility of topographic variations within each region affecting the occurrence of ambient temperatures. The study did not consider other regional risk factors such as maternal education [32] and access to water within households [30] which may also contribute to an increase in child anemia. Northern Africa was also not assessed in this study since there is limited data regarding childhood anemia prevalence over time in this region. Nonetheless, the data collected in the study is able to support a regional association between ambient temperatures and the prevalence of childhood anemia in Africa.
Author Credits
Dr. Muhammed Saeed: Original Idea, Paper Review, Data Collection, Data Review, Writing, Final Review; Harris Majeed: Original Idea, Paper Review, Data Collection, Writing, Final Review; Mohammad R. Saeed: Data Collection, Paper draft. Data Review; Harris Khokar: Data Collection; Writing of draft. Adeena Zaidi: Data Collection; Writing of draft and administration. Sami Khan: Data Collection Writing of draft; Binish Arif Sultan: Review.
References
- Janus J, Moerschel SK. Evaluation of anemia in children. American Family Physician [Internet]. 2010 Jun 15;81(12):1462–71. Available from: https://pubmed.ncbi.nlm.nih.gov/20540485/.
- The Lancet: New study reveals global anemia cases remain persistently high among women and children. Anemia rates decline for men. | Institute for Health Metrics and Evaluation [Internet]. Institute for Health Metrics and Evaluation. 2023 [cited 2024 Aug 13]. Available from: https://www.healthdata.org/news-events/newsroom/news-releases/lancet-new-study-reveals-global-anemia-cases-remain-persistently#:~:text=Topics&text=One%2Dfourth%20of%20the%20global.
- World Health Organization. Anaemia [Internet]. www.who.int. 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/anaemia.
- Nissenson, Allen R., et al. “Economic Burden of Anemia in an Insured Population.” Journal of Managed Care Pharmacy, vol. 11, no. 7, Sept. 2005, pp. 565–74. [CrossRef]
- Yang F, Liu X, Zha P. Trends in Socioeconomic Inequalities and Prevalence of Anemia Among Children and Nonpregnant Women in Low- and Middle-Income Countries. JAMA Network Open. 2018 Sep 28;1(5):e182899.
- Khan JR, Awan N, Misu F. Determinants of anemia among 6–59 months aged children in Bangladesh: evidence from nationally representative data. BMC Pediatrics. 2016 Jan 11;16(1):6-10.
- Martinez-Torres V, Torres N, Davis JA, Corrales-Medina FF. Anemia and Associated Risk Factors in Pediatric Patients. Pediatric Health Med Ther. 2023;14:267-280. Published 2023 Sep 4. [CrossRef]
- Amegbor, PM. Amegbor PM. Early-life environmental exposures and anaemia among children under age five in Sub-Saharan Africa: An insight from the Demographic & Health Surveys. Science of The Total Environment. 2022 Aug 1;832:154957.
- Zhu Y, He C, Gasparrini A, Vicedo-Cabrera AM, Liu C, Jovine Bachwenkizi, et al. Global warming may significantly increase childhood anemia burden in sub-Saharan Africa. One Earth. 2023 Oct 1;6(10):5-7.
- Moyo E, Nhari LG, Moyo P, Murewanhema G, Dzinamarira T. Health effects of climate change in Africa: A call for an improved implementation of prevention measures. Eco-Environment & Health. 2023 May 8;2(2):75.
- Lakhoo DP, Blake HA, Chersich MF, Nakstad B, Kovats S. The Effect of High and Low Ambient Temperature on Infant Health: A Systematic Review. International Journal of Environmental Research and Public Health. 2022 Jul 26;19(15):9109.
- Brimicombe C, Wieser K, Monthaler T, Jackson D, Jeroen De Bont, Chersich MF, et al. Effects of ambient heat exposure on risk of all-cause mortality in children younger than 5 years in Africa: a pooled time-series analysis. The Lancet Planetary Health. 2024 Aug 1;
- Short EE, Caminade C, Thomas BN. Climate Change Contribution to the Emergence or Re-Emergence of Parasitic Diseases. Infect Dis (Auckl). 2017;10:1178633617732296. Published 2017 Sep 25. [CrossRef]
- ter Kuile FO, Terlouw DJ, Kariuki SK, Phillips-Howard PA, Mirel LB, Hawley WA, Friedman JF, Shi YP, Kolczak MS, Lal AA, et al. Impact of permethrin-treated bed nets on malaria, anemia, and growth in infants in an area of intense perennial malaria transmission in western Kenya. Am J Trop Med Hyg. 2003;68:68–77.
- Iannotti LL, Tielsch JM, Black MM, Black RE. Iron supplementation in early childhood: health benefits and risks. Am J Clin Nutr. 2006;84:1261–1276. [CrossRef]
- Awuah RB, Colecraft EK, Wilson ML, et al. Perceptions and beliefs about anaemia: A qualitative study in three agroecological regions of Ghana. Matern Child Nutr. 2021;17(4):e13181. [CrossRef]
- Hung SC, Kuo KL, Peng CH, Wu CH, Wang YC, Tarng DC. Association of fluid retention with anemia and clinical outcomes among patients with chronic kidney disease. J Am Heart Assoc. 2015;4(1):e001480. Published 2015 Jan 5. [CrossRef]
- Azmeraw M, Kassaw A, Habtegiorgis SD, et al. Prevalence of anemia and its associated factors among children aged 6-23 months, in Ethiopia: a systematic review and meta analysis. BMC Public Health. 2023;23(1):2398. Published 2023 Dec 2. [CrossRef]
- Humphrey JH, Jones AD, Manges A, Mangwadu G, Maluccio JA, Mbuya MNN, Moulton LH, Ntozini R, Prendergast AJ, et al. Sanitation Hygiene Infant Nutrition Efficacy SHINE Trial Team. The Sanitation Hygiene Infant Nutrition Efficacy (SHINE) Trial: Rationale, Design, and Methods. Clin Infect Dis. 2015;61:S685–S702. [CrossRef]
- Wilson SE, Rogers LM, Garcia-Casal MN, Barreix M, Bosman A, Cunningham J, Goga A, Montresor A, Tuncalp O. Comprehensive framework for integrated action on the prevention, diagnosis, and management of anemia: An introduction. Ann N Y Acad Sci. 2023;1524:5–9. [CrossRef]
- Dimitrova A, Dimitrova A, Mengel M, et al. Temperature-related neonatal deaths attributable to climate change in 29 low- and middle-income countries. Nat Commun. 2024;15:5504. [CrossRef]
- Scovronick N, Sera F, Acquaotta F, et al. The association between ambient temperature and mortality in South Africa: A time-series analysis. Environ Res. 2018;161:229-235. [CrossRef]
- Tobías, Aurelio; Armstrong, Ben; Gasparrini, Antonio. Brief Report: Investigating Uncertainty in the Minimum Mortality Temperature. Epidemiology 28(1):p 72-76, January 2017. |. [CrossRef]
- Brehm R, South A, George EC. Use of point-of-care haemoglobin tests to diagnose childhood anaemia in low- and middle-income countries: A systematic review. Tropical Medicine & International Health. 2023 Dec 3;
- Firdian Makrufardi, Triasih R, Nurnaningsih Nurnaningsih, Kian Fan Chung, Lin SC, Chuang HC. Extreme temperatures increase the risk of pediatric pneumonia: a systematic review and meta-analysis. Frontiers in pediatrics. 2024 Feb 2;12.
- Balarajan Y, Ramakrishnan U, Özaltin E, Shankar AH, Subramanian S. Anaemia in low-income and middle-income countries. The Lancet [Internet]. 2011 Dec;378(9809):2123–35. Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(10)62304-5/fulltext.
- Kang N, Wang R, Lu H, Onyai F, Tang M, Tong M, et al. Burden of Child Anemia Attributable to Fine Particulate Matters Brought by Sand Dusts in Low- and Middle-Income Countries. Environmental Science & Technology. 2024 Jul 12;2024:12954.
- Shimanda PP, Amukugo HJ, Norström F. Socioeconomic factors associated with anemia among children aged 6-59 months in Namibia. Journal of Public Health in Africa. 2020 Apr 29;11(1):29-33.
- Nkulikiyinka R, Binagwaho A, Palmer K. The changing importance of key factors associated with anaemia in 6- to 59-month-old children in a sub-Saharan African setting where malaria is on the decline: analysis of the Rwanda Demographic and Health Survey 2010. Tropical Medicine & International Health. 2015 Oct 14;20(12):1722–32.
- Kothari MT, Coile A, Huestis A, Pullum T, Garrett D, Engmann C. Exploring associations between water, sanitation, and anemia through 47 nationally representative demographic and health surveys. Annals of the New York Academy of Sciences. 2019 Aug 1;1450(1):249–67.
- Ogwang BA, Chen H, Li X, Gao C. The Influence of Topography on East African October to December Climate: Sensitivity Experiments with RegCM4. Advances in Meteorology. 2014 Oct 21;2014:e143917.
- Choi HJ, Lee HJ, Jang HB, Park JY, Kang JH, Park KH, et al. Effects of maternal education on diet, anemia, and iron deficiency in Korean school-aged children. BMC Public Health. 2011 Nov 16;11(1):1-8.
Figure 1.
A) Annual country-specific child (<5 years) anemia prevalence; B) annual mean temperatures from 2000-2019.
Figure 1.
A) Annual country-specific child (<5 years) anemia prevalence; B) annual mean temperatures from 2000-2019.
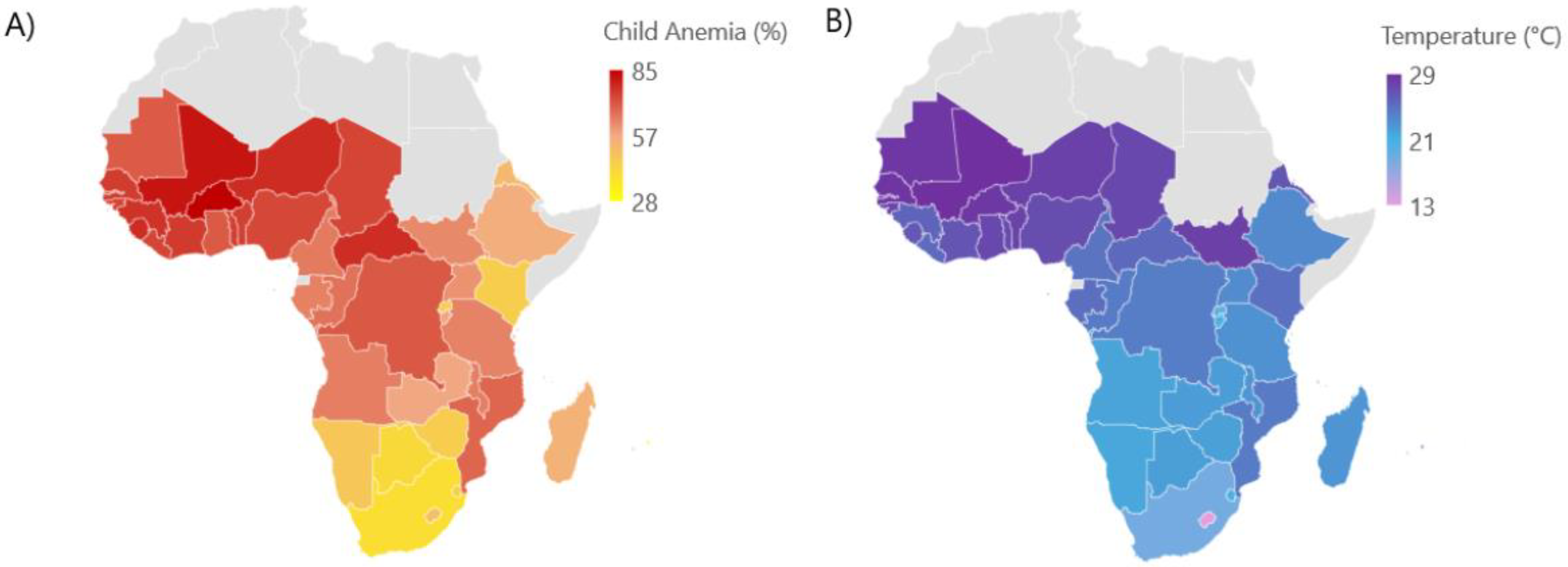

Table 1.
Total annual number of children (<5 years) with anemia by African region and country, 2000-2019.
Table 1.
Total annual number of children (<5 years) with anemia by African region and country, 2000-2019.
| Region | Country | Number of Children with Anemia |
|---|---|---|
| East (n=613,660,310) | Burundi | 17,626,800 |
| Comoros | 1,187,090 | |
| Eritrea | 4,714,000 | |
| Ethiopia | 158,345,000 | |
| Kenya | 57,797,000 | |
| Madagascar | 36,580,000 | |
| Malawi | 32,383,000 | |
| Mauritius | 459,320 | |
| Mozambique | 56,049,000 | |
| Rwanda | 13,688,100 | |
| South Sudan | 18,374,200 | |
| Uganda | 74,517,000 | |
| United Republic of Tanzania | 96,414,000 | |
| Zambia | 27,740,000 | |
| Zimbabwe | 17,785,800 | |
| Central (n=323,793,130) | Angola | 55,729,000 |
| Cameroon | 43,674,000 | |
| Central African Republic | 10,984,700 | |
| Chad | 33,943,000 | |
| Congo | 8,928,000 | |
| Democratic Republic of the Congo | 167,170,000 | |
| Gabon | 3,003,400 | |
| Sao Tome and Principe | 361,030 | |
| South (n=50,795,450) | Botswana | 2,020,990 |
| Eswatini | 1,298,760 | |
| Lesotho | 2,545,000 | |
| Namibia | 2,724,700 | |
| South Africa | 42,206,000 | |
| West (n=787,156,600) | Benin | 22,949,200 |
| Burkina Faso | 47,534,000 | |
| Cote d’Ivoire | 50,802,000 | |
| Gambia | 4,291,700 | |
| Ghana | 49,904,000 | |
| Guinea | 27,065,000 | |
| Guinea-Bissau | 3,718,300 | |
| Liberia | 9,127,400 | |
| Mali | 46,473,000 | |
| Mauritania | 7,693,400 | |
| Niger | 53,040,000 | |
| Nigeria | 401,095,000 | |
| Senegal | 32,168,000 | |
| Sierra Leone | 15,842,100 | |
| Togo | 15,453,500 | |
| Total | 1,775,405,490 |
Table 2.
Regional-specific association models for annual child anemia and air temperatures from 2000-2019.
Table 2.
Regional-specific association models for annual child anemia and air temperatures from 2000-2019.
| Region | Number of Child with Anemia | Adjusted RR (P-value)* |
|---|---|---|
| West | 787,156,600 | 0.989 (P=0.0013) |
| East | 613,660,310 | 0.993 (P=0.001) |
| Central | 323,793,130 | 1.023 (P<0.0001) |
| South | 50,795,450 | 1.005 (P=0.006) |
* adjust for NO2, cereal yield, GDP, stunting, prevalence reproductive women anemia (moderate levels), child hemoglobin, and trend.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



