
Submitted:
12 September 2024
Posted:
13 September 2024
You are already at the latest version
Abstract
No consensus exists on whether acute aerobic exercise alters the glomerular filtration rate in older adults. Objective: To assess the immediate effects of three aerobic exercise intensities on the estimated glomerular filtration rate (eGFR) in healthy, sedentary older adults. Methods: Eighteen healthy, sedentary older adults (12 men and eight women) voluntarily participated in the study. The participants underwent three standardized aerobic exercise tests (100%, 80%, and 60% of the maximal heart rate) on a bicycle ergometer. Blood samples were collected to determine cholesterol, triacylglycerol, glucose, serum creatinine (Cr), Cystatin C (CysC) concentrations, and eGFR. Results: eGFR and serum concentrations of Cr and CysC were not modified at any exercise intensity. There was a negative correlation between blood total cholesterol vs. eGFR (R= -0.512, R= -0.582, R= -0.531; p <0.05) at rest, 60%, and 100% of the maximal heart rate, respectively. Besides, a negative correlation existed between age vs. eGFR at 60% of the maximal heart rate (R= -0.516; p <0.05). Conclusion: Short-time aerobic exercise of low, moderate, and vigorous intensity did not significantly affect eGFR and is considered safe for kidney function in healthy, sedentary older adults.
Keywords:
aerobic exercise
; cardiovascular risk factors
; chronic kidney dysfunction
; glomerular filtration rate
; sports medicine
1. Introduction
Chronic kidney disease (CKD) is a global health problem with a high prevalence worldwide (~12%) [1] , with 21.4% in older adults [2]. Low-intensity aerobic exercise has been proven to benefit these patients, decreasing complications and improving kidney function [3]. On the contrary, some studies have reported that a single high-intensity resistance training session causes acute kidney damage in healthy young volunteers [4], and others observe a temporary decrease in glomerular filtration rate (GFR) in sedentary, active adults over 64 years [5]. Indicating potential dangers of acute high-intensity exercise for older adults with CKD, exacerbated when exercise is performed for a long time and in dehydrating climatic conditions [6,7]. However, despite the importance of understanding the relationship between high-intensity exercise and kidney dysfunction, the immediate effects of three different exercise intensities (high, moderate, and low) on the renal function of older adults remain unstudied.
Conventional methods for assessing kidney function in older adults are often inadequate. The estimated glomerular filtration rate (eGFR) is the recommended method for earlier detection and better management of CKD in this population because GFR indicates the natural kidney dysfunction associated with aging [8].
There are several methods available for calculating GFR in humans: the 3-hour volume of distribution method, iohexol measured by HPLC-UV [9], the simplified one-compartment model corrected by the Bröchner-Mortensen formula [10], the camera-based method using 99mTc-DTPA [11], and p-amino hippuric acid clearance [12]. The most suitable methods for estimating GFR in clinical practice are serum creatinine (Cr) and cystatin C (CysC) concentrations. According to Laterza et al. (2002), CysC is considered a more reliable and accurate marker than Cr [13]; both methods have been utilized to assess kidney damage from acute intense exercise, such as after an ultramarathon [14].
Hence, this study aimed to assess the immediate effects of three aerobic exercise intensities on eGFR in healthy, sedentary older adults using serum concentrations of Cr and CysC. Understanding the acute responses of GFR to different exercise intensities can help healthcare professionals tailor exercise recommendations to their individual needs and identify those who may require closer monitoring during physical activity.
2. Materials and Methods
2.1. Participants
Sixty older adults were invited to participate in a cross-sectional study for convenience: 35 did not meet the inclusion criteria, five did not complete the tests, and two voluntarily left the study. Finally, 18 participants (12 men and eight women) completed the study (Figure 1). The inclusion criteria were 65 years or older, non-smoker, no evidence of kidney or liver dysfunction, and engaging in less than five days of moderate-intensity physical exercise or less than 30 minutes of walking daily. The exclusion criteria included inability to follow protocol instructions, mobility issues, and failure to perform a maximum exercise test on a bicycle ergometer.
2.2. Ethical Considerations
The Autonomous University of Baja California Ethics Committee approved this study (UABC-998/2020-2), which was conducted following the World Medical Association’s Declaration of Helsinki guidelines [15] and supervised by a sports physician. Before the study, participants voluntarily signed a written informed consent form.
2.3. Research Protocol
After an overnight fast, participants were required to visit the laboratory four times between 7:00 and 9:00 h (Figure 2). In the first session, a venous blood sample was collected, and a clinical history examination, a resting electrocardiogram, and a body fat percentage measurement (%BF) were performed. The second session involved a maximum exercise test under a standardized protocol [16]; the third and fourth sessions included two submaximal exercise tests at 80% or 60% of the maximal heart rate achieved during the maximum exercise test. Before each exercise test, participants drank 150 ml of water. The indoor environmental conditions during the exercise tests remained stable, with a temperature of 23°C and relative humidity of 30%. In addition, the participants were instructed to wear sports attire.
2.3.1. First Session
Each participant underwent a thorough examination by a physician, including a twelve-lead resting electrocardiogram (Welch Allyn 50, Spain). Clinical history, blood pressure (standard aneroid sphygmomanometer Model DS44, Welch Allyn), and blood samples used to determine cholesterol, triacylglycerols, and glucose (SPIN 120, Spain) were also obtained using standard equipment. The mean blood pressure was calculated [] [17]. Using standardized procedures and equipment from reputable manufacturers, trained study staff collected anthropometric data following the Official Mexican Standard [18]. Height (Estadiometer SECA, model 213, USA) and weight (digital scale Seca 700) measurements were used to determine Body Mass Index (BMI; kg·m-2), and bioimpedance (Inbody 720, UK) measurements were used to determine %BF. Additionally, participants were given 15 min to acclimate to the cycle ergometer (Monark 828E, Vansbro, Sweden).
2.3.2. Second Session
Before starting the maximal incremental exercise test on the cycle ergometer, the participants underwent a 4-minute warm-up cycling at 0 Watts. Following the warm-up, the work rate was increased by 15 W·min-1 until the participants reached exhaustion while maintaining a pedaling rate of 50 rpm throughout the test [16]. To determine that the exercise test was maximum, at least two of the following three fatigue indicators were considered: reaching the 9-10 level on the Borg Scale C-10 [19], inability to maintain 50 rpm for 10 seconds, and achieving 90% of their calculated maximum heart rate, which is 207 – 0.7 (age) [20]. Heart rate was continuously monitored during the tests using a POLAR monitor (model H7, Finland), and VO2max was estimated using validated formulas: Men Y = 10.51(Watts) + 6.35 (body mass, kg) - 10.49 (yr) + 519.3 ml·min−1; Women: Y = 9.39 (Watts) + 7.7 (body mass, kg) - 5.88 (yr) + 136.7 ml·min−1 [21]
2.3.3. Third and Fourth Sessions
The participants were randomly selected (random list in Excel) to complete two submaximal exercise tests using the cycle ergometer. Each test lasted 20 minutes and involved exercise at intensities of 60% and 80% of the maximum heart rate achieved during the maximum exercise test. The pedaling rate was maintained at 50 rpm throughout the test, and the workload was continuously adjusted to maintain a constant heart rate (±3 beats per minute)
2.4. Measurements of Concentrations of Cr and CysC
Blood samples were collected from the brachiocephalic vein while the participant was seated on the bike before and after each exercise test. The serum was then separated, divided into aliquots, and stored at -80°C until further analysis. Serum Cr concentrations were determined using the Jaffé colorimetric-kinetic method (creatinine kit from Spinreact), and serum CysC levels were determined using the enzyme-linked immunosorbent assay (ELISA) technique (R&D system kit). To account for the acute change in plasma volume due to physical exercise [22], post-exercise Cr and CysC values were adjusted for hemoconcentration [23]. The equations used to estimate the GFR are detailed in Table I (supplemental file).
2.5. Statistical Analysis
The variances of errors and the normal distribution of the data were assessed using Levene's and Shapiro-Wilk tests, respectively. The impact of the treatment (exercise tests) on blood concentrations of Cr, CysC, and eGFR was evaluated using the student's t-test for related samples or the W-Wilcoxon test. The relationships between variables were examined using Pearson's correlation. Statistical significance was set at p <0.05. All analyses were conducted with Jamovi Version 2.4 and figures with Prism Version 9.5 (2022, GraphPad Software, LLC).
3. Results
According to the analyzed health parameters (Table 1), the participants were in good health on average; however, they were overweight (26.8 ± 3.3 kg·m-2) and had low aerobic fitness (28.6 ± 7.1 ml·kg-1·min-1).
Besides, seven of the 18 individuals had a resting eGFR of less than 60 mL·min-1·1.73 m-2 on at least two occasions (Table II Supplementary file).
CysC and Cr serum concentrations and eGFR were not modified at any exercise intensity (Figure 3). However, a negative correlation was observed between blood total cholesterol vs. eGFR (R= -0.512, R= -0.582, R= -0.531; p <0.05) at rest, 60%, and 100% of the maximal heart rate measured during the maximal exercise test, respectively. Besides, a negative correlation was observed between age vs. eGFR at 60% of the intensity of the maximal heart rate (R= -0.516; p <0.05).
4. Discussion
The central outcome of this study indicated that a single aerobic exercise on a bicycle and short duration (≤20 min), at low (60%), moderate (80%), and high (100%) intensities did not affect serum concentrations of CysC, Cr, or eGFR in sedentary older adults (Figure 3). During physical exercise, the blood is redistributed throughout the different body compartments to hemodynamic factors, mechanoreceptor stimulation caused by muscle contractions, and rapid sympathetic nervous system activation [24,25,26]. This compartment redistribution increases the blood flow to active muscles and decreases the flow to less active and visceral organs, including the kidneys [24]. Consequently, this redistribution could decrease the glomerular filtration rate (GFR), exacerbated at higher muscle contractions [27] or when exercise is performed in dehydrating climatic conditions [28], especially in older adults who have already experienced a decline in GFR [5]. Under these arguments, one might expect a decrease in GFR during exercise. However, it has been shown that the reduction in blood circulation at the glomerulus level and, consequently, in GFR only occurs for a few seconds at the onset of exercise [5], so this work did not observe modifications in the baseline values at the final of the exercise.
The stability of eGFR across different exercise intensities observed in this study may be attributed to several physiological mechanisms. 1) The kidneys possess a robust autoregulatory system that helps maintain relatively constant renal blood flow and GFR despite fluctuations in systemic blood pressure during exercise [7]. 2) The 20-minute exercise sessions in our study were not long enough to elicit significant changes in kidney function, unlike prolonged exercise sessions, which result in dehydration and reduced renal perfusion in older adults [6]. 3) Physical exercise at low intensities offers protective effects on kidney function [3].
Our results align with those of Poussel et al. (2020), who found no significant GFR modifications after an extreme endurance event such as ultramarathons in highly-trained individuals [14]. However, this differs from those of Poortmans & Ouchinsky (2006), who reported a 30% reduction in GFR after a maximal exercise test in adults over 64 years [5]. This discrepancy could be attributed to 1) the exercise duration mentioned above; 2) participant characteristics: our sample was primarily comprised of healthy older adults, which may differ from other studies in terms of fitness levels or underlying health conditions; and 3) methodological differences: variations in the methods to estimate or measure GFR in different studies could result in discrepancies.
On the other hand, there is a natural and progressive decline in kidney function with age [29], primarily due to structural and vascular changes such as nephrosclerosis, loss of renal mass, and impaired angiogenesis [30]. These changes result in altered renal blood flow and decreased GFR in this population [8]. The natural reduction in GFR is generally not clinically significant under normal conditions, and the kidney retains its functionality at an advanced age, but it could be critical during acute illnesses and pathological conditions. This study highlights no associations between age and eGFR at the basal level but at 60% of maximal exercise intensity, which tells us that GFR measurements during low-intensity exercise are more sensitive than those at rest.
According to the KDIGO guidelines [31], individuals with GFR <60 mL·min·1.73 m2 of body surface area undergo chronic kidney disease; these values are linked to a high mortality ratio and fatal vascular events in individuals >70 years of age [32], besides affects the medication doses and the management of several diseases [33]. In this sense, this study revealed a high prevalence of low eGFR. Seven participants (38.9%) had a resting eGFR value <60 mL·min·1.73 m2 registered on two occasions. These findings align with the results of Abdulkader et al. (2017), who reported impaired GFR in 19.3% of older adults, with 96.5% of those with associated comorbidities [34]. Additionally, Mohan et al. (2022) report that approximately 37 million adults in the United States are affected by chronic kidney disease [35]. Though a reduced resting GFR is considered normal and benign in aged persons [7], regular monitoring of kidney function is necessary in these adults.
The significant negative correlation between eGFR and total cholesterol observed at the onset of the exercise tests demonstrates the high sensitivity of health status evaluation carried out under stress conditions, a relationship that must continue to be studied. CKD is independently associated with increased cardiovascular disease risk; numerous studies have proven this close relationship [32,34]. This study is one of the first to illustrate the connections in the context of acute exercise in older adults, which warrants further exploration.
The strengths of this study include controlled experiments, examining three exercise intensities, utilizing both Cr and CysC for GFR estimation, and focusing on older adults. The Cr as a biomarker for kidney function is influenced by factors such as stress, muscle mass, and dietary protein intake, which may be particularly relevant in older adults [36]. Conversely, CysC is less affected by these factors and may provide a more accurate estimation of the GFR [37]. However, both biomarkers could provide a more comprehensive assessment of the effect of acute exercise on kidney function. The limitations include a small sample size according to the program, a short duration of submaximal exercise, and the absence of direct GFR measurement.
5. Conclusions
The results of this study indicate that short-time exercise at low, moderate, and vigorous intensity does not significantly impact eGFR and is considered safe for kidney function in healthy older adults. The correlations detected between eGFR post-exercise and blood cholesterol may require a more comprehensive assessment and controlled renal function studies post-acute exercise. Given the high prevalence of deficient eGFR, regular monitoring of kidney function in older people engaged in moderate—and high-intensity exercise is advised. This highlights the importance of tailoring exercise recommendations to individuals' needs and specific abilities.
This work will contribute to determining the most effective exercise regimen for preserving or enhancing kidney health in older individuals and provide reassurance regarding exercise recommendations for this demographic group.
6. Future Research Directions
Further investigation into the mechanisms that link GFR and cholesterol during exercise is recommended. Besides, focus on examining the impact of exercise on GFR in older adults with pre-existing kidney disease or cardiovascular conditions to identify the specific exercise-intensity levels at which kidney stress becomes more evident.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: title; Table S1: title; Video S1: title.
Author Contributions
All authors contributed equally to the development of this manuscript by making several critical revisions and approving the final version.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by Ethics Committee (UABC-998/2020-2).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Everyone who contacts the corresponding author will have access to the required data. (aramos@uacj.mx).
Acknowledgments
A scholarship for postgraduate studies by Conahcyt funded this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hill, N.R.; Fatoba, S.T.; Oke, J.L.; Hirst, J.A.; O’Callaghan, C.A.; Lasserson, D.S.; Hobbs, F.D.R. Global Prevalence of Chronic Kidney Disease - A Systematic Review and Meta-Analysis. PLoS One 2016, 11, e0158765. [Google Scholar] [CrossRef] [PubMed]
- Amaral, T.L.M.; Amaral, C. de A.; Vasconcellos, M.T.L. de; Monteiro, G.T.R. Prevalence and factors associated to chronic kidney disease in older adults. Rev Saude Publica 2019, 53, 44. [Google Scholar] [CrossRef] [PubMed]
- Villanego, F.; Naranjo, J.; Vigara, L.A.; Cazorla, J.M.; Montero, M.E.; García, T.; Torrado, J.; Mazuecos, A. Impact of physical exercise in patients with chronic kidney disease: Sistematic review and meta-analysis. Nefrologia (Engl Ed) 2020, 40, 237–252. [Google Scholar] [CrossRef] [PubMed]
- Spada, T.C.; Silva, J.M.R.D.; Francisco, L.S.; Marçal, L.J.; Antonangelo, L.; Zanetta, D.M.T.; Yu, L.; Burdmann, E.A. High Intensity Resistance Training Causes Muscle Damage and Increases Biomarkers of Acute Kidney Injury in Healthy Individuals. PLoS One 2018, 13, e0205791. [Google Scholar] [CrossRef] [PubMed]
- Poortmans, J.R.; Ouchinsky, M. Glomerular Filtration Rate and Albumin Excretion after Maximal Exercise in Aging Sedentary and Active Men. J Gerontol A Biol Sci Med Sci 2006, 61, 1181–1185. [Google Scholar] [CrossRef]
- Bongers, C.C.W.G.; Alsady, M.; Nijenhuis, T.; Tulp, A.D.M.; Eijsvogels, T.M.H.; Deen, P.M.T.; Hopman, M.T.E. Impact of Acute versus Prolonged Exercise and Dehydration on Kidney Function and Injury. Physiol Rep 2018, 6, e13734. [Google Scholar] [CrossRef] [PubMed]
- Pryor, R.R.; Pryor, J.L.; Vandermark, L.W.; Adams, E.L.; Brodeur, R.M.; Schlader, Z.J.; Armstrong, L.E.; Lee, E.C.; Maresh, C.M.; Casa, D.J. Acute Kidney Injury Biomarker Responses to Short-Term Heat Acclimation. Int J Environ Res Public Health 2020, 17. [Google Scholar] [CrossRef]
- Ariev, A.L.; Kayukov, I.G.; Beresneva, O.N.; Parastaeva, M.M.; Essaian, A.M.; Kucher, A.G. Aging and kidneys: problems in evaluating of the glomerular filtration rate in elderly. Adv Gerontol 2019, 32, 614–626. [Google Scholar]
- Bibbo, G.; Munn, C.; Kirkwood, I. Comparison of Glomerular Filtration Rates Determined Using Two- and Single-Blood Sample Methods with a Three-Blood Sample Technique for 2922 Paediatric Studies. Nucl Med Commun 2019, 40, 1204–1210. [Google Scholar] [CrossRef]
- Gaspari, F.; Perico, N.; Remuzzi, G. Application of Newer Clearance Techniques for the Determination of Glomerular Filtration Rate. Curr Opin Nephrol Hypertens 1998, 7, 675–680. [Google Scholar] [CrossRef]
- Inoue, Y.; Ohtake, T.; Homma, Y.; Yoshikawa, K.; Nishikawa, J.; Sasaki, Y. Evaluation of Glomerular Filtration Rate by Camera-Based Method in Both Children and Adults. J Nucl Med 1998, 39, 1784–1788. [Google Scholar] [PubMed]
- Agarwal, R. Chromatographic Estimation of Iothalamate and P-Aminohippuric Acid to Measure Glomerular Filtration Rate and Effective Renal Plasma Flow in Humans. J Chromatogr B Biomed Sci Appl 1998, 705, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Laterza, O.F.; Price, C.P.; Scott, M.G. Cystatin C: An Improved Estimator of Glomerular Filtration Rate? Clin Chem 2002, 48, 699–707. [Google Scholar] [CrossRef]
- Poussel, M.; Touzé, C.; Allado, E.; Frimat, L.; Hily, O.; Thilly, N.; Rousseau, H.; Vauthier, J.-C.; Chenuel, B. Ultramarathon and Renal Function: Does Exercise-Induced Acute Kidney Injury Really Exist in Common Conditions? Front Sports Act Living 2019, 1, 71. [Google Scholar] [CrossRef] [PubMed]
- Hellmann, F.; Verdi, M.; Schlemper, B.R.J.; Caponi, S. 50th Anniversary of the Declaration of Helsinki: The Double Standard Was Introduced. Arch Med Res 2014, 45, 600–601. [Google Scholar] [CrossRef] [PubMed]
- Aström, H.; Jonsson, B. Design of Exercise Test, with Special Reference to Heart Patients. Heart 1976, 38, 289–296. [Google Scholar] [CrossRef]
- Miura, K.; Nakagawa, H.; Ohashi, Y.; Harada, A.; Taguri, M.; Kushiro, T.; Takahashi, A.; Nishinaga, M.; Soejima, H.; Ueshima, H. Four Blood Pressure Indexes and the Risk of Stroke and Myocardial Infarction in Japanese Men and Women: A Meta-Analysis of 16 Cohort Studies. Circulation 2009, 119, 1892–1898. [Google Scholar] [CrossRef]
- Mexican Ministry of Health Mexican Official Standard (NOM-167-SSA1-1997), for the provision of social assistance services for minors and older adults. Diario Oficial de la Federación 1999.
- Ramos-Jiménez, A.; Wall-Medrano, A.; Hernández-Lepe, M.A.; Chávez-Treviño, G.; Guereca-Arvizuo, J.; Hernández-Torres, R.P. Borg’s category ratio-scale (CR-10) is useful to predict the onset of blood lactate accumulation (OBLA) in young Mexicans adults, regardless their body mass. CIENCIA ergo-sum 2019, 26, 7. [Google Scholar] [CrossRef]
- Gellish, R.L.; Goslin, B.R.; Olson, R.E.; McDonald, A.; Russi, G.D.; Moudgil, V.K. Longitudinal Modeling of the Relationship between Age and Maximal Heart Rate. Med Sci Sports Exerc 2007, 39, 822–829. [Google Scholar] [CrossRef]
- Storer, T.W.; Davis, J.A.; Caiozzo, V.J. Accurate Prediction of VO2max in Cycle Ergometry. Med Sci Sports Exerc 1990, 22, 704–712. [Google Scholar] [CrossRef]
- Bloomer, R.J.; Farney, T.M. Acute Plasma Volume Change with High-Intensity Sprint Exercise. J Strength Cond Res 2013, 27, 2874–2878. [Google Scholar] [CrossRef] [PubMed]
- Van Beaumont, W. Evaluation of Hemoconcentration from Hematocrit Measurements. J Appl Physiol 1972, 32, 712–713. [Google Scholar] [CrossRef] [PubMed]
- Fadel, P.J. Reflex Control of the Circulation during Exercise. Scand J Med Sci Sports 2015, 25 Suppl 4, 74–82. [Google Scholar] [CrossRef]
- Crecelius, A.R.; Kirby, B.S.; Luckasen, G.J.; Larson, D.G.; Dinenno, F.A. Mechanisms of Rapid Vasodilation after a Brief Contraction in Human Skeletal Muscle. Am J Physiol Heart Circ Physiol 2013, 305, H29–40. [Google Scholar] [CrossRef] [PubMed]
- Tschakovsky, M.E.; Rogers, A.M.; Pyke, K.E.; Saunders, N.R.; Glenn, N.; Lee, S.J.; Weissgerber, T.; Dwyer, E.M. Immediate Exercise Hyperemia in Humans Is Contraction Intensity Dependent: Evidence for Rapid Vasodilation. J Appl Physiol (1985) 2004, 96, 639–644. [Google Scholar] [CrossRef]
- Momen, A.; Handly, B.; Kunselman, A.; Leuenberger, U.A.; Sinoway, L.I. Influence of Sex and Active Muscle Mass on Renal Vascular Responses during Static Exercise. Am J Physiol Heart Circ Physiol 2006, 291, H121–126. [Google Scholar] [CrossRef]
- García-Trabanino, R.; Jarquín, E.; Wesseling, C.; Johnson, R.J.; González-Quiroz, M.; Weiss, I.; Glaser, J.; José Vindell, J.; Stockfelt, L.; Roncal, C.; et al. Heat Stress, Dehydration, and Kidney Function in Sugarcane Cutters in El Salvador--A Cross-Shift Study of Workers at Risk of Mesoamerican Nephropathy. Environ Res 2015, 142, 746–755. [Google Scholar] [CrossRef]
- Denic, A.; Glassock, R.J.; Rule, A.D. Structural and Functional Changes With the Aging Kidney. Adv Chronic Kidney Dis 2016, 23, 19–28. [Google Scholar] [CrossRef]
- Hommos, M.S.; Glassock, R.J.; Rule, A.D. Structural and Functional Changes in Human Kidneys with Healthy Aging. J Am Soc Nephrol 2017, 28, 2838–2844. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl 2013, 3, 1–150. [Google Scholar] [CrossRef]
- Gu, X.; Fang, X.; Ji, X.; Tang, Z.; Wang, C.; Guan, S.; Wu, X.; Liu, H.; Zhang, Z. Kidney Dysfunction Is Associated with Risk of Cardiovascular Events in Middle-Aged and Elderly Population with Hypertension: A 5-Year Community-Based Cohort Study in China. Clin Nephrol 2020, 93, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Verbeeck, R.K.; Musuamba, F.T. Pharmacokinetics and Dosage Adjustment in Patients with Renal Dysfunction. Eur J Clin Pharmacol 2009, 65, 757–773. [Google Scholar] [CrossRef] [PubMed]
- Abdulkader, R.C.R.M.; Burdmann, E.A.; Lebrão, M.L.; Duarte, Y.A.O.; Zanetta, D.M.T. Aging and Decreased Glomerular Filtration Rate: An Elderly Population-Based Study. PLoS One 2017, 12, e0189935. [Google Scholar] [CrossRef]
- Mohan, S.G.; Holmgren, N.J.; Jacobson, L.E.; Saxe, J.M.; West-Sell, S.A.; Williams, J.; Harper, P.; Jensen, C.D. Climate Factors May Influence Glomerular Filtration Rate in Nephrology Patients. The FASEB Journal 2022, 36. [Google Scholar] [CrossRef]
- Inker, L.A.; Schmid, C.H.; Tighiouart, H.; Eckfeldt, J.H.; Feldman, H.I.; Greene, T.; Kusek, J.W.; Manzi, J.; Van Lente, F.; Zhang, Y.L.; et al. Estimating Glomerular Filtration Rate from Serum Creatinine and Cystatin C. N Engl J Med 2012, 367, 20–29. [Google Scholar] [CrossRef]
- Ferguson, T.W.; Komenda, P.; Tangri, N. Cystatin C as a Biomarker for Estimating Glomerular Filtration Rate. Curr Opin Nephrol Hypertens 2015, 24, 295–300. [Google Scholar] [CrossRef]
Figure 1.
Screened participation.
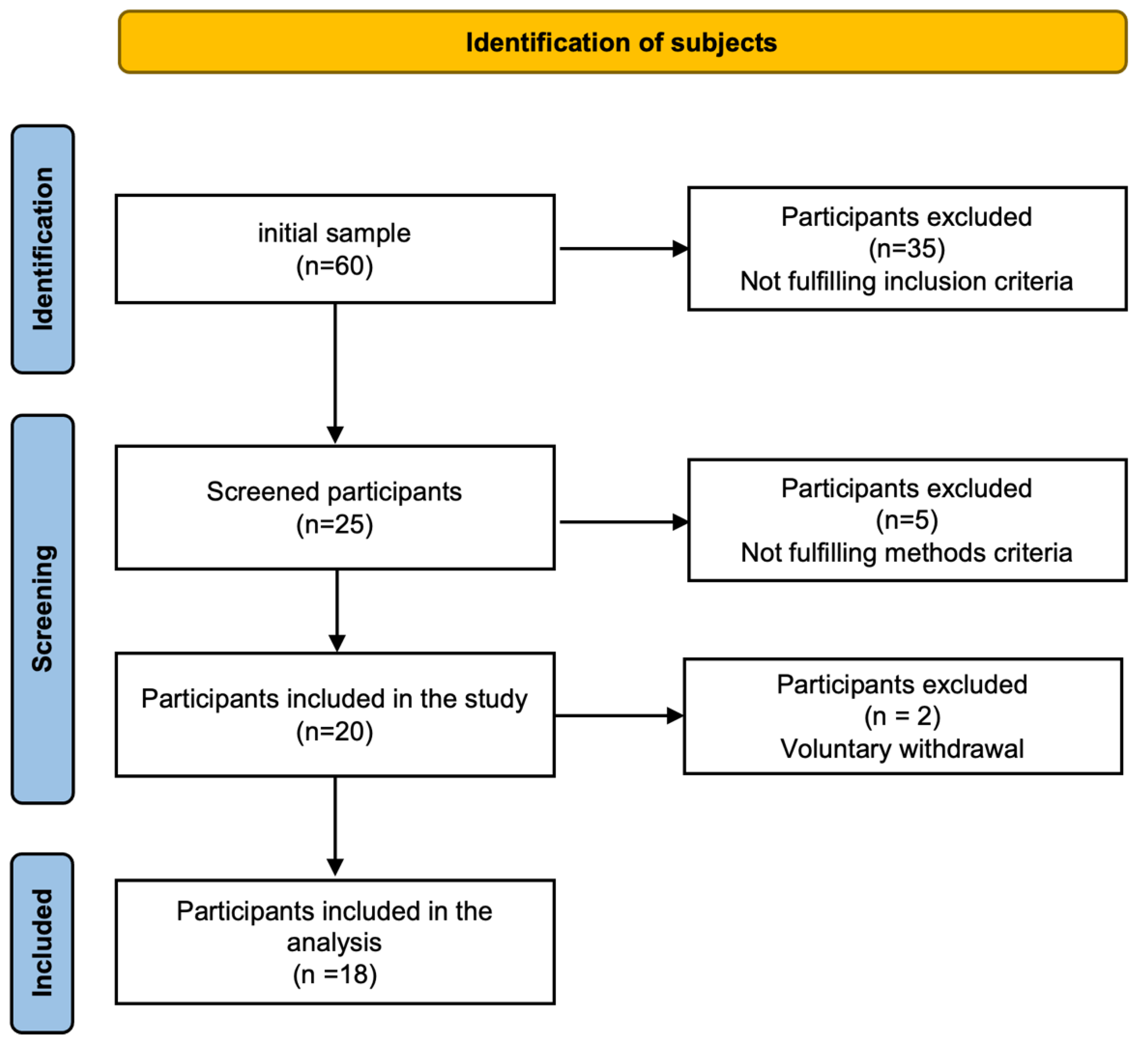
Figure 2.
Research protocol.
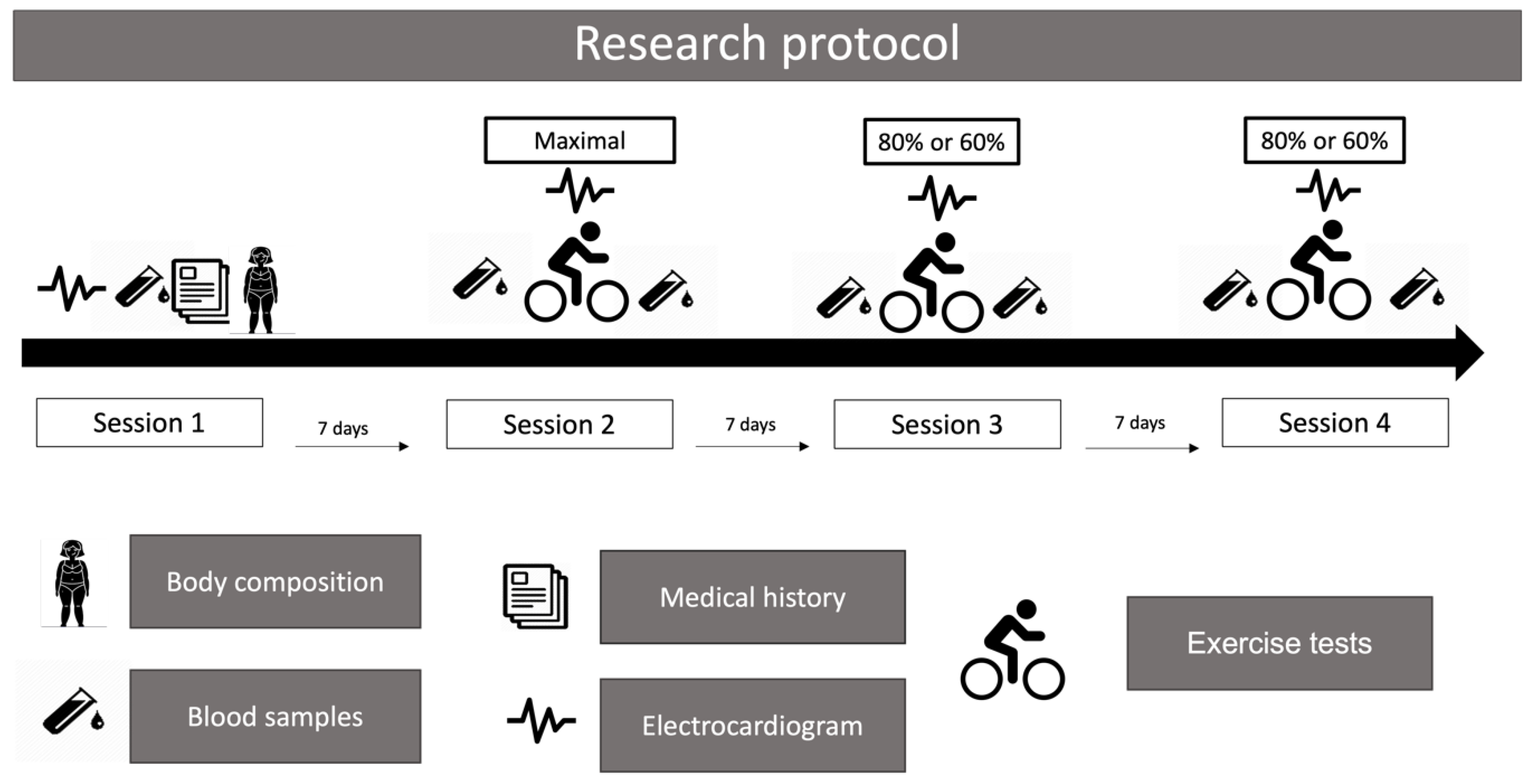
Figure 3.
Effect of exercise tests on serum concentration of a) Cystatin C, b) Creatinine, and estimated glomerular filtration rate (eFGR) calculated by serum concentration of c) Cystatin C (CysC), d) Creatinine (Cr).
Figure 3.
Effect of exercise tests on serum concentration of a) Cystatin C, b) Creatinine, and estimated glomerular filtration rate (eFGR) calculated by serum concentration of c) Cystatin C (CysC), d) Creatinine (Cr).
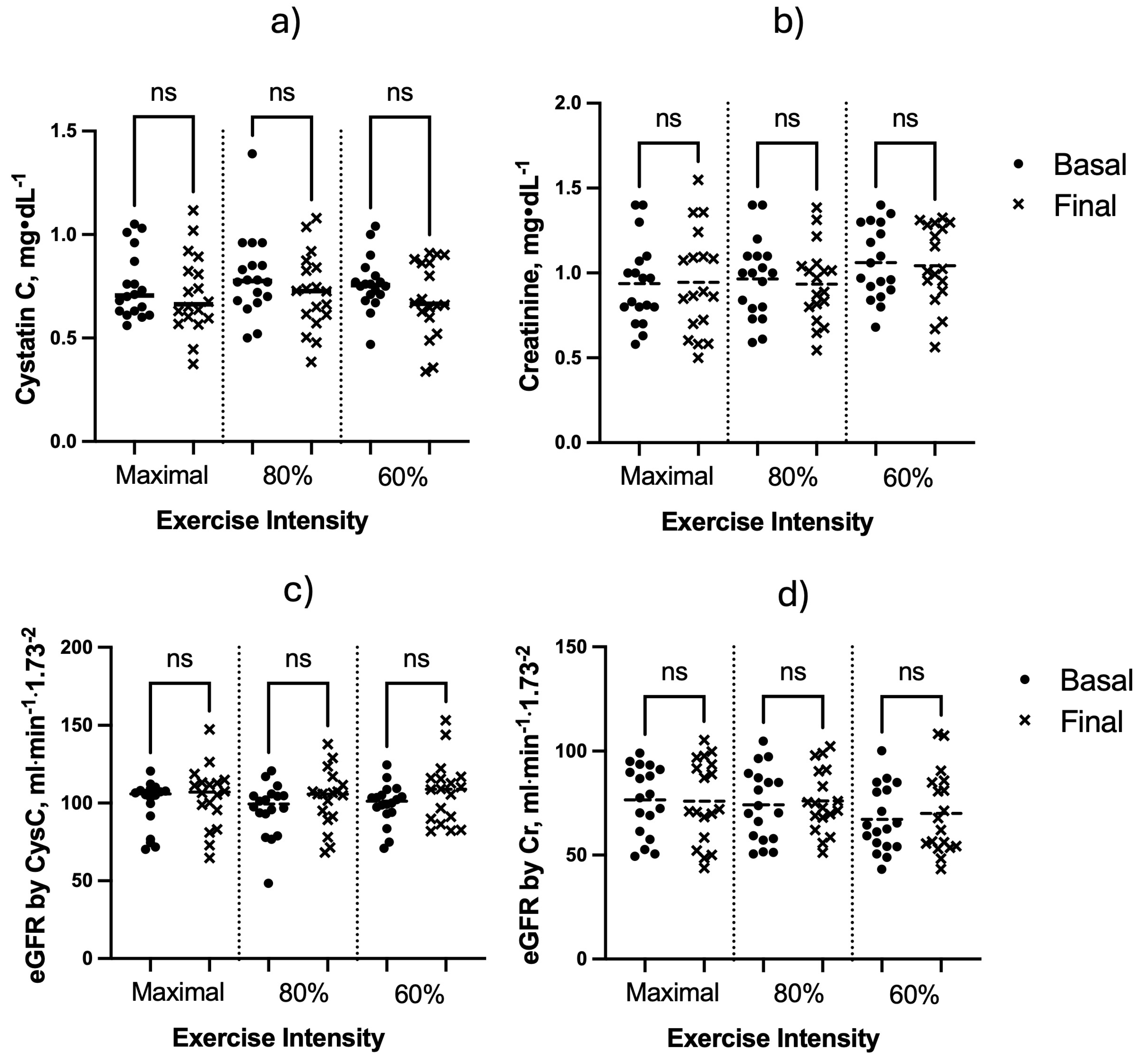

Table 1.
Participants' characteristics.
| Age (years) | 70.1 ± 5.1 |
| Weight (kg) | 71.0 ± 10.9 |
| Height (cm) | 163.3 ± 7.6 |
| BMI (kg·m-2) | 26.8 ± 3.3 |
| Fat mass (%) | 24.1 ± 5.5 |
| Systolic blood pressure (mmHg) | 124.7 ± 13.1 |
| Diastolic blood pressure (mmHg) | 78.9 ± 10.2 |
| Mean blood pressure (mmHg) | 94.2 ± 10.3 |
| Glucose (mg·dl-1) | 103 ± 13 |
| Cholesterol (mg·dl-1) | 185 ± 34 |
| Triacylglycerol (mg·dl-1) | 127 ± 41 |
| Creatinine (mg·dl-1) | 0.937 ± 0.246 |
| Cystatin C (mg·dl-1) | 0.753 ± 0.161 |
| eGFR by Cr (mL·min·1.73 m2) | 76.5 ± 16.7 |
| eGFR by CysC (mL·min·1.73 m2) | 99.3± 15.4 |
| VO2 max (ml·kg-1·min-1) | 28.6 ± 7.1 |
| HRmax (beats·min-1) | 148 ± 13 |
BMI: Body mass index, Cr = Creatinine, CysC = Cystatin C, eGFR = Estimated glomerular filtration rate, HRmax: maximum heart rate, VO2 max: maximum oxygen consumption. Values are mean ± SD.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



