
Submitted:
15 September 2024
Posted:
16 September 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background:
The Covid-19 pandemic was in reality a syndemic there the balance between a multitude of biological (Nature-made) and socio-political (men-made) factors determined individually the outcome of every single infection, on a scale of nothing-to-fatal. Blaming the virus for everything bad that happened to us after January 2020 is incorrect. Now, in ~ 2 years distance from the syndemic, it may be timely and possible to uncover the human contribution to this historical event and learn of it.
Objective:
To identify and use some qualitative approach to estimate the objective, statistical / epidemiological ‘value’ of the virus-selected individuals (in age-normalized groups) for the rest of the society. This non-political, non-religious approach may be the only way to understand the benefit / cost ratio of actions and emergency orders we had to survive in addition to the virus itself.
Methods:
Statistical data were obtained from publicly available official databases, including the relevant actuarial tables and evaluated by widely used statistical methods. The estimation of statistical/epidemiological ‘value of life’ was based, strictly and exclusively, on the real age and the statistically calculated Residual Life Expectancy (RLE, i.e. remaining years alive at a given age).
The American healthcare expenses were compared to the corresponding healthcare costs/capita in other similarly well-developed west-European countries. This was the only available method to get some ideas about the magnitude of the well-established (rational) healthcare spending and compare it to the American standards.
Results
1) Life expectancy uninterruptedly increased in USA since 1933, due to continuous reduction of Mortality Rate of the youngest and oldest citizens. COVID didn’t stop the population growth (+8.2 M /2020-2023).
2) The total count of Excess COVID associated Deaths (XCD) is ~ 2-times as much as the official statistic was able to explain by virus infection. It is speculated that these Complementary Covid Deaths (CCD) are probably the unexpected side-effects of the pandemic related emergency orders.
3) The worldwide ‘longevity’ trend exponentially increased the healthcare expenses, especially the care of elderly. However the USA is unique in this aspect and the healthcare costs are irrationally much higher than in any other country.
4) We can see a large economic incentive in the development of excesses under COVID syndemic.
Conclusions
The harm of the COVID virus - as well as the benefits of the mandatory, emergency actions during the pandemic - were grossly over-estimated. Professional, unbiased (non-religious, non-political) and independent reviews are strongly recommended.
Keywords:
COVID-19
; pandemic
; USA
; mortality
; lethality
; age
; aging
; life expectancy
; actuary table
; virus
; political
; death
; healthcare expenditure
; medical
; pharmaceutical
; true
; hearsay
; viral test
; underlying cause of death
; UCOD
Introduction
The COVID pandemic (2020-2022) forces the population of many countries to face and reevaluate the deepest and darkest echelons of human life: our fears of dying, religious believes, trust in science and authority. The virus-related chapter is over, but the socio- economic consequences are very much alive. Fundamental aspects of this historical event are still hidden, important questions remains unanswered, or unsatisfactorily answered. We are living with a politically enforced consensus stating that the COVID pandemic was a terribly dangerous fatal enemy of the human life, but We – the brave people, led by our vice politicians and scientific authorities, brilliant doctors and super-effective pharmaceutical industry – came out victoriously of the war with the ‘hidden enemy’(called even the ‘China virus’).
However a less authoritarian and much more realistic understanding is emerging: 1) Initiated by Senator Dr Rand Paul an investigation is in progress regarding the possible involvement of NIH in the active financing and advising a “gain of function” research in China, which ultimately resulted in the birth of the first COVID-19 variant [1]. 2) Fm. President Donald Trump started a long series of court examinations to elucidate the possible misuse of the COVID epidemic for political purposes during the presidential election 2021 [2]. 3) Texas governor and jurist Greg Abbott and attorney general Ken Paxton are suing Pfizer for misrepresenting the efficacy of their mRNA COVID-19 vaccine and conspiration to censor public disclosure [3]. 4) Project Veritas reported that Pfizer conducts extensive research – for many years – to design lethal pathogens which can – by some way and some time – contribute to the need and use of their therapeutic vaccine products [4]. 5) The return of the critical reviews of the diagnostic and statistical support for the COVID epidemic in USA is on the way [5]. 6) Florida State Surgeon General Calls for Halt in the Use of COVID-19 mRNA Vaccines [6]. 7) Kansas AG accuses Pfizer of misrepresenting COVID vaccine, hiding safety risks [7].
A realistic and objective evaluation of the real costs and benefits of the actions taken during the COVID pandemic is necessary to understand (and learning from) the events during this historical period.
Methods
Statistical data were obtained from publicly available official databases, including the relevant actuarial tables and evaluated by widely used statistical methods.
The estimation of statistical/epidemiological ‘value of life’ was based, strictly and exclusively, on the real age and the statistically calculated Residual Life Expectancy (RLE, i.e. remaining years alive at a given age).
The American healthcare expenses were compared to the corresponding healthcare costs/capita in other similarly well-developed west-European countries. This was the only available method to get some ideas about the magnitude of the well-established (rational) healthcare spending and compare it to the American standards.
Results
A. BIOLOGICAL PARAMETERS OF LIFE IN USA
- 1.
- General Life expectancy
Convincing experience tells that all individual life-length is biologically determined and it varies from species to species. The maximal possible life expectancy for humans is – say - 120 years [8]. However the actual average life expectancy depends on the people themselves i.e. the socio-political milieu of the time and place of living. The most used parameters of life expectancy are:
- -
- Initial Life Expectancy (ILE) [9]: It is the expected number of years alive at the moment of birth;
- -
- Residual Life Expectancy (RLE) [10] : It is the expected number of years alive at a certain age;
- -
- Accomplished Life Expectancy (ALE): It is the final number of years alive at the moment of deaths. This parameter describes how well a person succeeded to live until the statistically expected (average) lifetime.
- 2.
- Age Normalized Death Rates, MR(i)
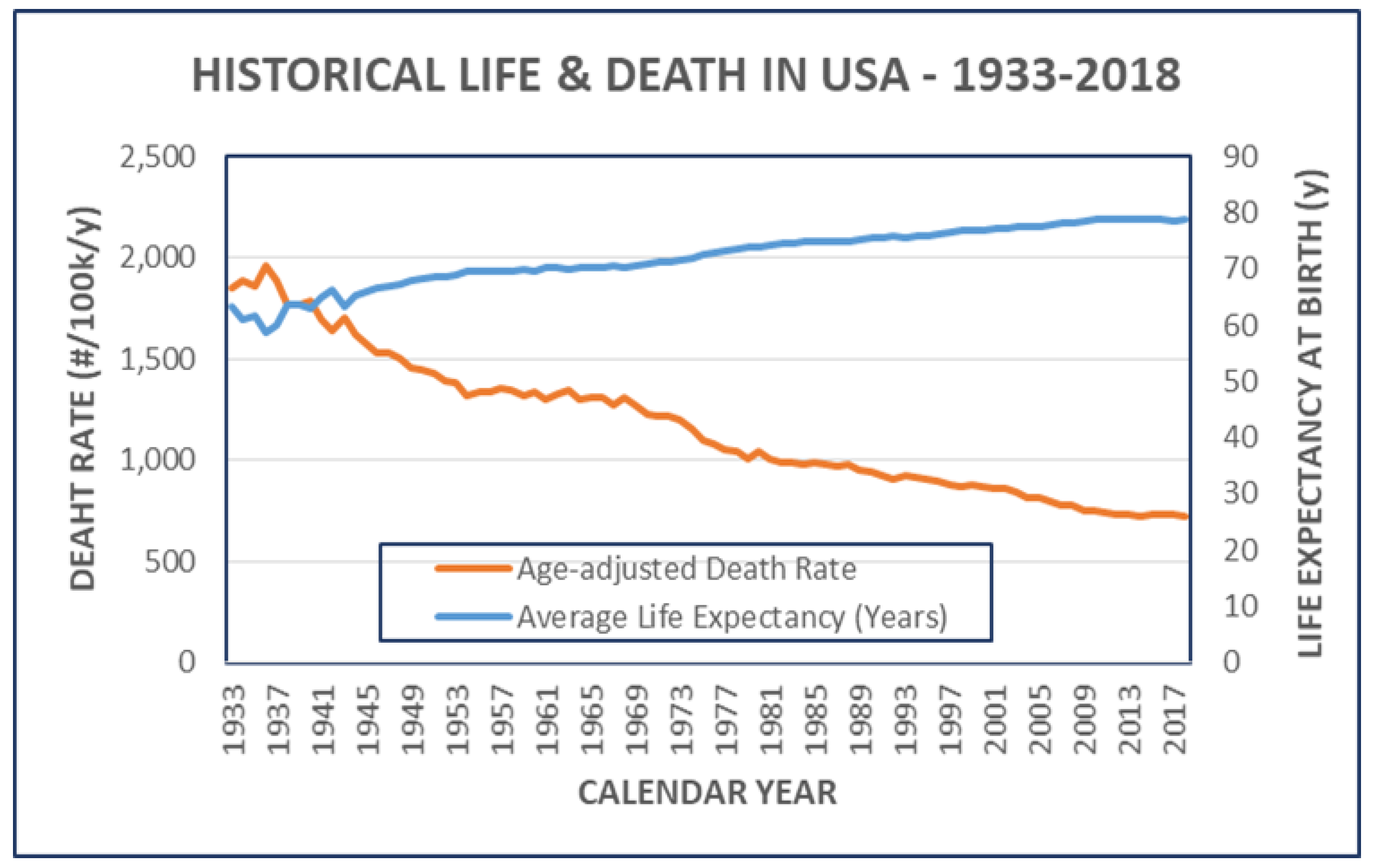
- The successive increase of the expectable years of individual lives - and the associated decrease of the MRs – was continuous, almost a century, without major variation (Figure 1).
Figure 1.
Historical Life & Death in USA – 1033-2018.
However the contribution of different age-groups is very different. The Deaths Rates are close to zero for persons between ages ~ 4 to 50 but exponentially increases after 50 until the factual deaths. Medical and social healthcare improvements postpone, but never prevent the occurrence of natural deaths (Figure 2).
These continuous decrease of death rates has little effect on the age-related size of the population before age ~ 65 and over ~ 80 years. However the number and life-time of persons in the ‘transition age’ [65-80] are markedly increasing (Figure 3).
B. SOCIO- ECONOMIC PARAMETERS OF ‘LONGEVITY’
Longer life and the associated benefits are not free. Being alive is certainly very desirable (genetically programmed) condition, consequently the ‘maintenance fee’ can be very high. An objective approach to the life and death equation is possible only if a) the Life has some (any) measurable value for the involved persons and communities; b) the person and communities have the necessary resources -equivalent to this calculated value – to maintain and increase the number of years alive.
Medical and healthcare resources are only a small, but significant part of many options that people and societies possess to pay the price of longevity.
- 1.
- The ‘value’ of life.
Every individual life has an arbitrary monetary value. This is well known for some professionals, like military and insurance experts and they are coldly calculating and using this value. Private persons however are not supposed to know about it, even less, to speak about it. It is taboo.
The general, public consensus teaches, that the value of life is unmeasurable [11]. However there still may be a way to set a well measurable statistical value for lives in a group for statistical purposes (but never for valuing an individual person’s life). This is strictly limited for the calculation and comparison on the life-to-life bases.
It is supposed that when comparing two completely anonymous persons (we don’t know anything about them except their chronological age) the younger is reasonably more valuable - in this statistical, ‘live-to-live’ comparison test – than the older. The reasoning is very simple: the younger has more years to live (higher RLE value) than the older and consequently in case of death the loss of younger is higher than the loss of the older one. This mathematical/statistical reasoning may work, but only as long as you really don’t know anything individual about the compared persons, except their age.
- 2.
- The ‘price’ of increasing RLE (longevity).
Life is a free gift from the Nature (God?). It has no value for the Nature. Any values associated with Life are strictly human creations. A person’s life has value – first of all – for the person itself, followed by value for his/her family, friends, followed by the great society around him. Human lives are measured by other human lives. These values can be positive or negative, or both.
Apart from the never ending philosophical and religious speculations, the human lives - here and now – have strong positive value. The explanation is simple: more people prefer living than not. Consequently the count of all humans (defined as carriers of 44+2 chromosomes) is steadily increasing. The positive attitude to Life is expressed by two fundamentally different ways: reproduction and longevity.
- -
- Survival and prosperity through reproduction: this is the original, collectivistic way of staying alive by propagating your individual chromosomes. This method is often the only one available.
- -
- Survival and prosperity through longevity: this might be called the egoistic way, because it is based on concentrating the life experience in fewer number of individuals instead of dispersing it to many descendants.
The industrially more developed countries (higher BNP) are on the ‘longevity’ way: they restrain their aggression to others and invest into healthcare. The ‘longevity’ investments seems to be logical, when the religious believe in the ‘life-after-this-life’ became unrealistic for more and more persons. The “believe in God” philosophy is successively replaced by the “believe in yourself” or - even worse - “believe in your doctor” mentality.
There are three different approaches to try setting a measurable and comparable value on the human life. *First: the value of life for the individual himself can be based on the statistical calculation of alive/dead ratio for all individuals (or the RLE) in the same age. It directly gives an objective comparison with other individuals in the same and different age-groups. *Second: the value of life for the collective depends on the accumulated number of available years alive for all individuals in the same age-group, i.e. it is RLE multiplied by the size (#) of the group (Figure 4). This two calculations give very similar results, as expected, except minor differences depending on the variation in the size of the age-groups.
*Third: the value of life can be estimated even based on the Annual Per Capita Healthcare Costs [12] by age. Historical records indicate the correlation between increasing Life Expectancy and the healthcare costs, in every developed industrial country (Figure 5A).
Figure 5A.
Development & Costs of ‘Longevity’ in Leading Countries. Bars indicate healthcare costs ($/year/capita). Lines indicate Life Expectancy at Birth (ILE, Y: years). AUS: Australia, CAN: Canada, GBR: Great Britain, JPN: Japan, USA: United States of America. The values in USA are emphasized by red color and thick line.
Figure 5A.
Development & Costs of ‘Longevity’ in Leading Countries. Bars indicate healthcare costs ($/year/capita). Lines indicate Life Expectancy at Birth (ILE, Y: years). AUS: Australia, CAN: Canada, GBR: Great Britain, JPN: Japan, USA: United States of America. The values in USA are emphasized by red color and thick line.
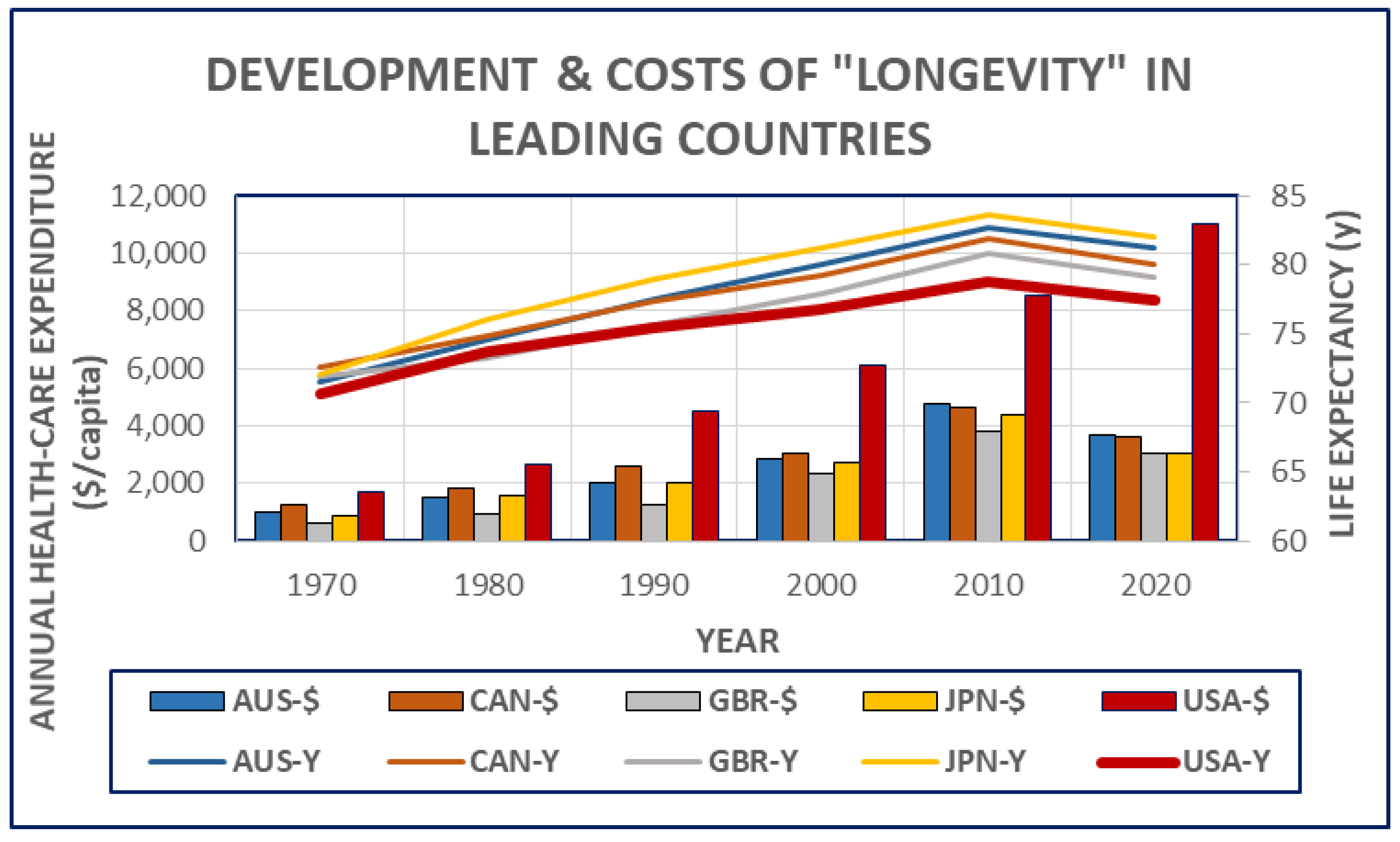
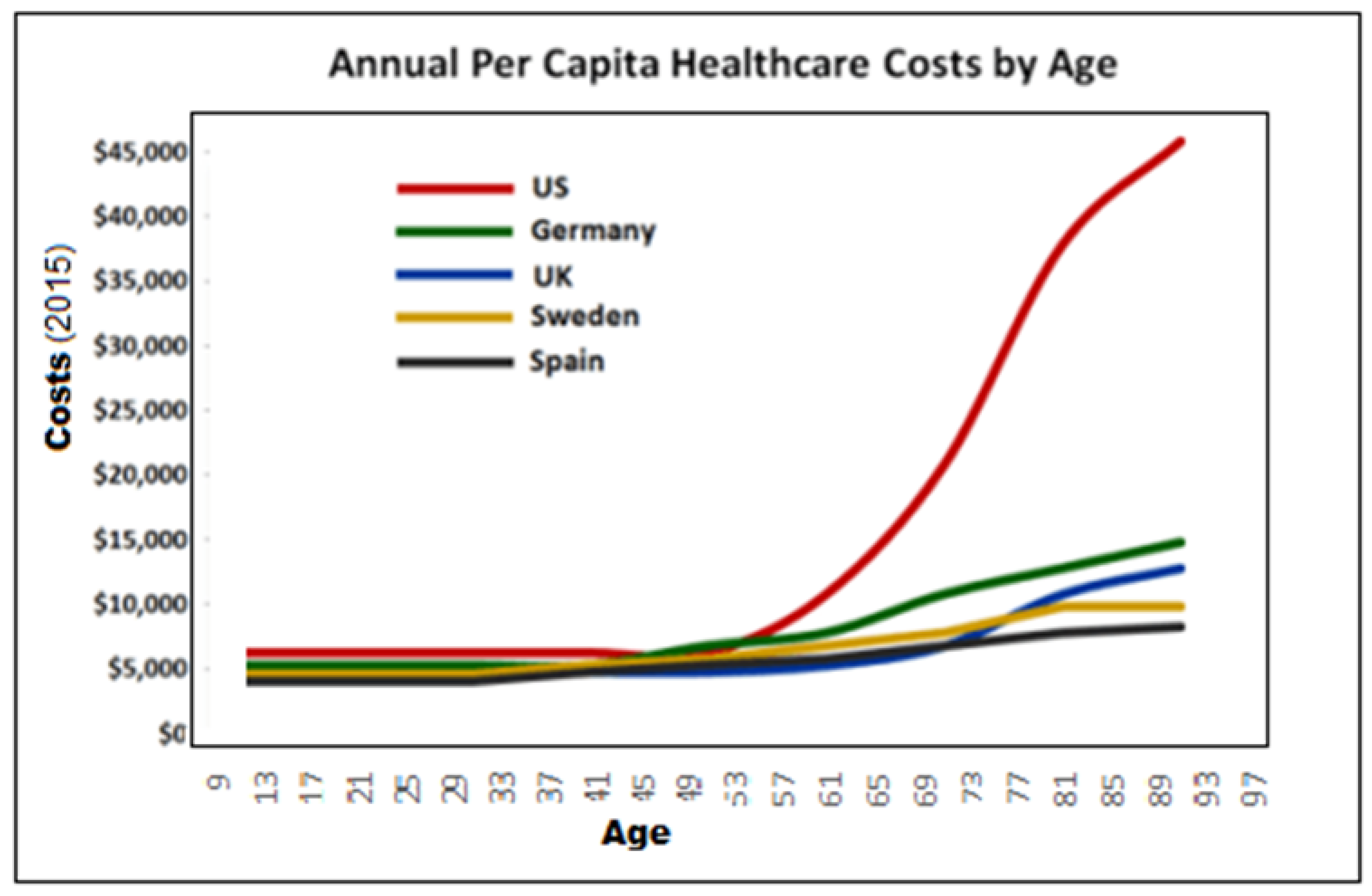
The rapid increase of healthcare costs, in the proximity of death, is not surprising. However the increase of per capita costs for senior-care in USA is very large compared to other equally well developed western countries (Figure 5B).
Figure 5B.
Annual per Capita Healthcare Costs by Age. The lines indicate the age-dependency of healthcare costs ($, value in 2015) and comparison in some well developed countries in 2012 [13].
Figure 5B.
Annual per Capita Healthcare Costs by Age. The lines indicate the age-dependency of healthcare costs ($, value in 2015) and comparison in some well developed countries in 2012 [13].
- 3.
- Calculation of the cost/benefit ratio of a rational health care.
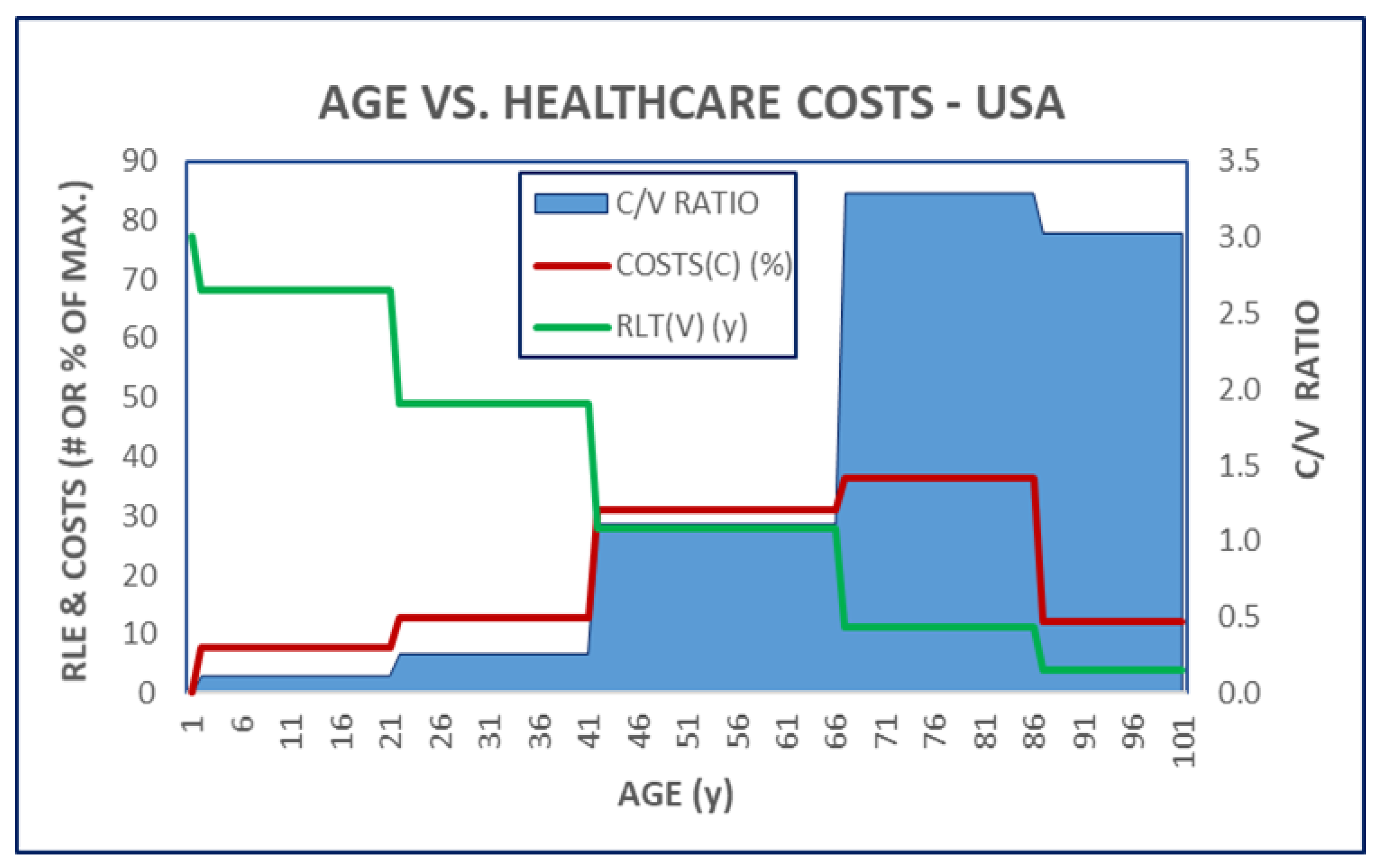
A neutral approach to estimate the benefit of healthcare is the calculation of its costs [14] in relation to changes of RLE. However it is necessary to keep in mind that any change of RLE depends on a large number of factor and not only on medical (and related) efforts (Figure 6).
Figure 6.
AGE v. HEALTHCARE COSTS IN USA. The Residual Life Expectancy (green line) and the Annual Healthcare Costs (red line) were expressed as % of the maximal available for different age categories of the population. The ratio of these two values (C/V) is indicated (Blue shaded area).
Figure 6.
AGE v. HEALTHCARE COSTS IN USA. The Residual Life Expectancy (green line) and the Annual Healthcare Costs (red line) were expressed as % of the maximal available for different age categories of the population. The ratio of these two values (C/V) is indicated (Blue shaded area).
C. THE INTERFERENCE OF COVID PANDEMIC WITH THE NORMAL LIFE OF AMERICANS
- 1.
- Excess Mortality [XM] during the Coronavirus pandemic (COVID-19) [15]
COVID added a new category of deaths to the traditional ‘all-cases-mortality’. It is called ‘Excess-Covid-Mortality (XCM) because it occurred simultaneously with the appearance of the virus infections and the pandemic-associated life changing conditions.
Excess Deaths of all causes including Covid Deaths [XD] = Total counts of Reported Deaths of all causes under pandemic [TRD] – Total Projected (or expected) Deaths of all causes without Covid pandemic [TPD]. The XD is often expressed as P-score (%)
XD=TRD – TPD
P-score = (TRD – TPD) / TPD
Excess mortality is a more comprehensive measure of the total impact of the pandemic on deaths than the confirmed COVID-19 death count alone. It captures not only the confirmed deaths, but also COVID-19 deaths that were not correctly diagnosed and reported as well as deaths from other causes that are attributable to the overall crisis conditions.
- Globally, the total number of excess deaths is estimated to be two to four times higher than the reported number of confirmed deaths due to COVID-19 (incl. both deaths confirmed by specific laboratory (viral) test or not [16]). The WHO confirmed [17] that the total number of excess deaths is substantially higher than the number of confirmed deaths due to COVID-19. Consequently the XM is the sum of two distinct categories
- a.
-
Total Covid Deaths (TCD) category contains cases there close connection to virus had been established, reported and became part of the COVID statistic:
- -
- there the Covid virus was the Underlying Couse of Death (UCOD) and it was confirmed by specific laboratory viral test (true Covid Deaths – [CD+]) and
- -
- there the Covid was suspected as contributor to the deaths but it hadn’t been confirmed by viral test (‘hearsay’ Covid Deaths – [CD?]) [5].
- b.
- Complementary Covid Deaths (CCD) category contains all kinds of excess deaths which occurred under the pandemic but association to Covid virus itself was not possible to establish and it hadn’t been part of the official Covid statistic. It is speculated that CCM is the result of life changing conditions associated with the extensive COVID regulations rather than the virus itself [18].
- 2.
- Effect on the Size of the Population in USA
The numerically large excess mortality caused by the COVID pandemic had very little visible effect on the population of a very large country, like USA (Figure 6). (Compare to Figure 3).
Figure 6.
Pre- and Post-COVID Population by Age and Years. The population count of USA, by age, before- (2015-2019) and under (2020-2023) the pandemic were compared.
Figure 6.
Pre- and Post-COVID Population by Age and Years. The population count of USA, by age, before- (2015-2019) and under (2020-2023) the pandemic were compared.
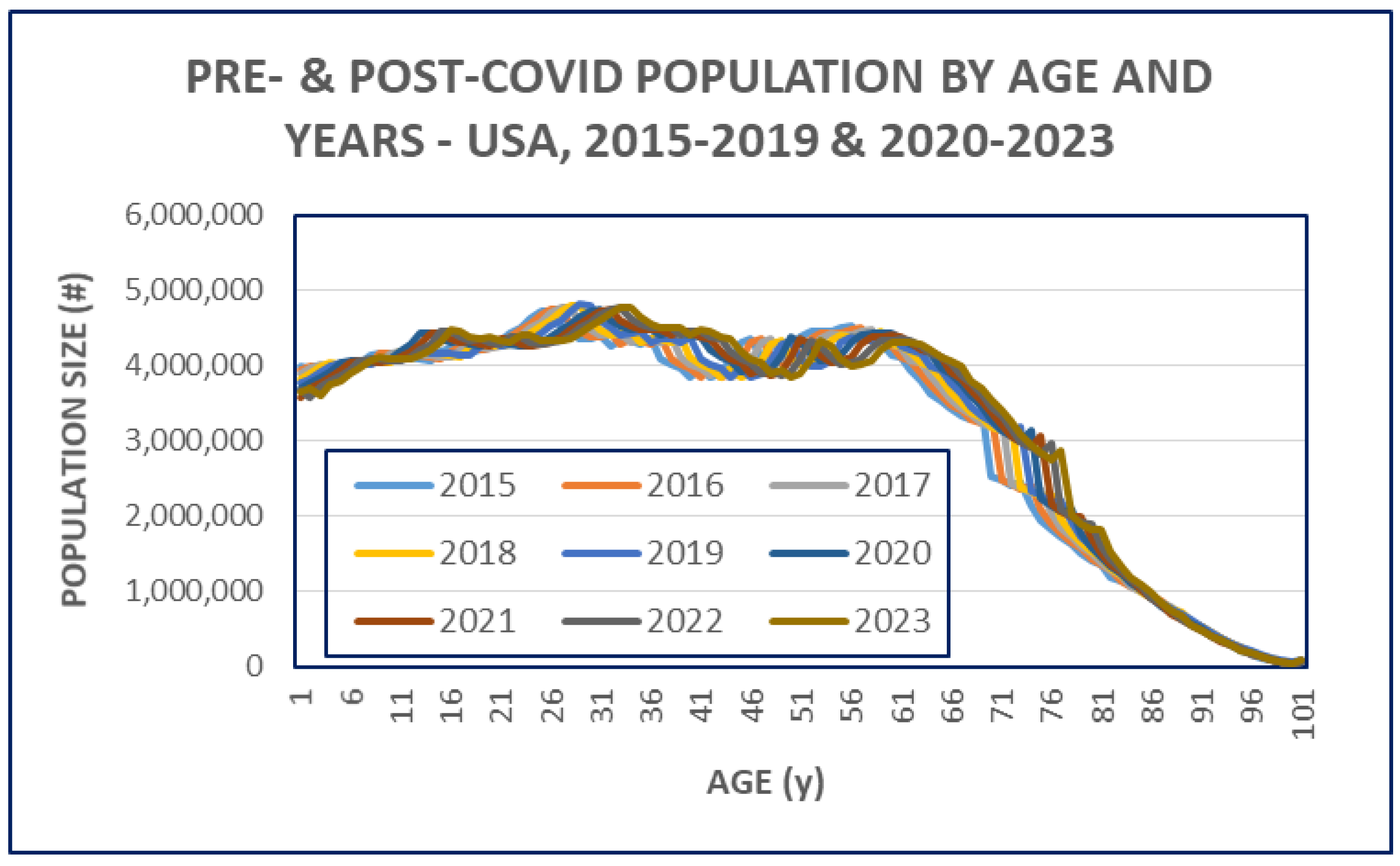
The estimated count of the total population grow with ~ 8 M persons during the pandemic, compared to the 5 years average directly before the COVID events. (Table 1)
- 3.
- Effect on the Detailed Mortality Parameters
However a very detailed analyses and comparison of all possible age groups (0-100 years old persons) with each other revels some restructuring of the population pattern (Figure 7 and Table 2). The negative change of MR in age groups (0-14) pinpoints the possible “beneficiaries” of the pandemic.
The calculated weekly Excess COVID Mortality (XCM) was up to 60 % over the historically expected ‘usual’ counts of deaths, corresponding to the well-known COVID mortality peeks. Less kids (age 0-14 years) died during the pandemic than expected suggesting that at least one group of people might have benefited from the exceptional rules under 2020-2023. The average XCM didn’t return to the original zero value at the end of this period of records (Figure 8).
An even deeper look at the nature and origin of the extra deaths under COVID pandemic is possible when dividing it into its natural subgroups as described above. It is especially valuable to have a closer look at the ratio of deaths which were possible to connect to the COVID virus (TCD) and those which were not possible to connect to the virus at all (CCD). (Table 3 and Figure 9A,B).
The average P-Score of the population (all ages) was around 20-25% during the first two years of the pandemic, but it dropped to the 5-10% level 2022-2023 and remained above zero after. Both components of the extra deaths (XCD) showed the similar pattern of changes.
However the virus related (TCD) and unrelated (CCD) components were changing differently. This difference depends on the definition of the COVID mortality.
- -
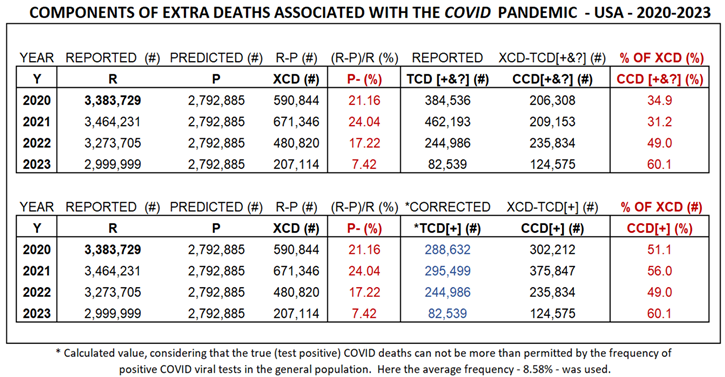
- Relying on the official definition - that pools the ‘true’ [CD+] cases with the un-supported ‘hearsay’-based causes [CD?] - the CCD/XCD ratio is starting ~35% but increasing to ~ 60% by time. (Upper part of Table 3 and Figure 9A)
- -
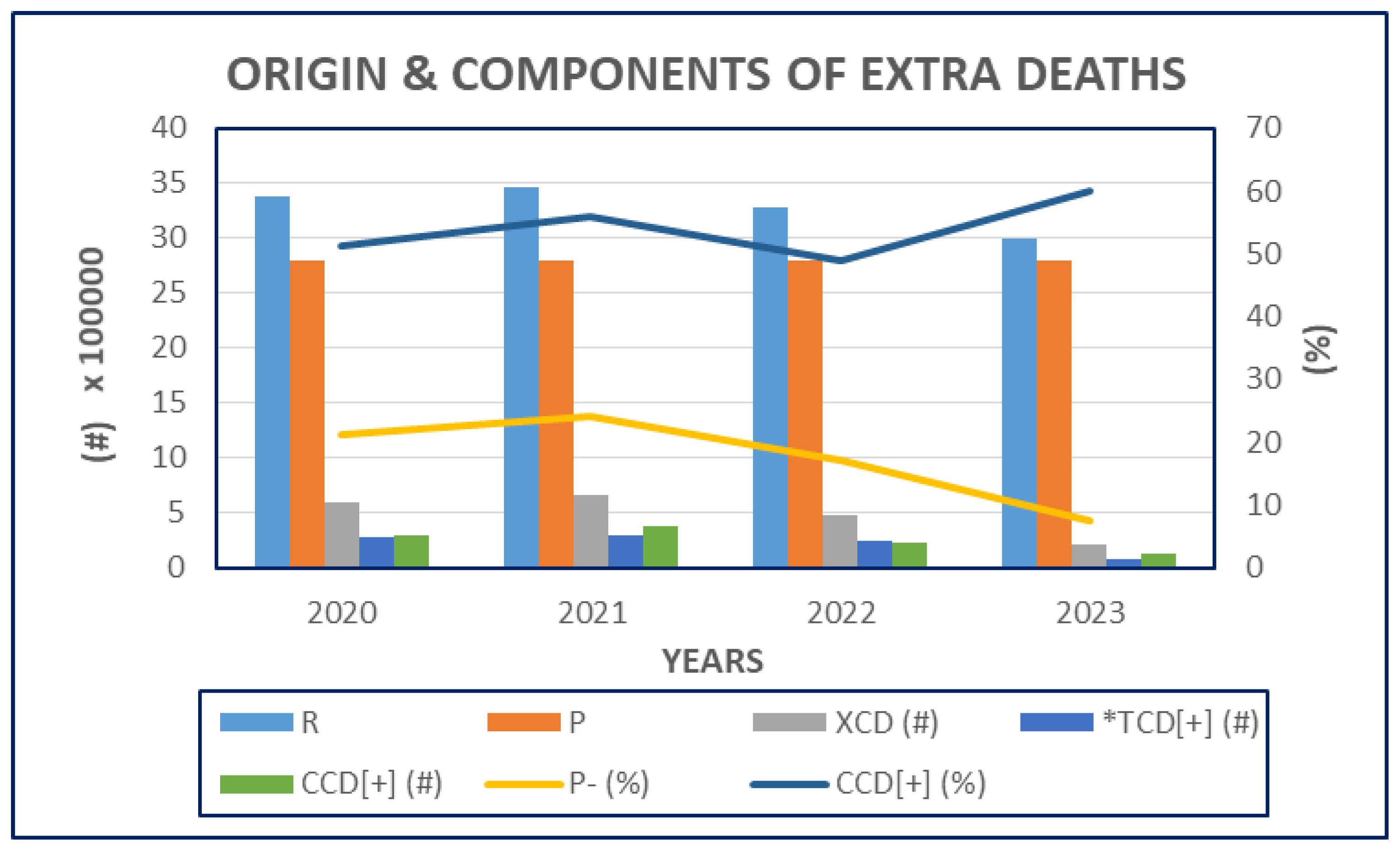
- Using the evidence-based definition, that requests that the diagnosis is substantiated by specific laboratory viral test, the count of true-COVID deaths [CD+] is lower than reported and the corresponding CCD is higher: the CCD/XCD ratio is starting at ~ 50% with a slight increase by the years (~60%). (Lower part of Table III and Figure 9B).
These differences have no practical consequences today, the XCD counts remain the same, and ‘death is death’. However it might have significance when objectively evaluating the true magnitude of the COVID danger and compare it to the value of the human reaction.
Figure 9A.
Origin & Components of Excess Covid Associated Mortality – Using CDC method. The bars (left axis) represent the reported (R) and projected (P) counts of the population, the calculated excess COVID associated mortality (XCM); the total reported count of pooled (true) and “hearsay” COVID deaths (TCD[+&?]) and the calculated number of Collateral Covid Deaths (CCD) in the indicated years of pandemic. The lines (right axis) are indicating the corresponding P-Scores (P-) and the proportion of CCDs of the XCDs .
Figure 9A.
Origin & Components of Excess Covid Associated Mortality – Using CDC method. The bars (left axis) represent the reported (R) and projected (P) counts of the population, the calculated excess COVID associated mortality (XCM); the total reported count of pooled (true) and “hearsay” COVID deaths (TCD[+&?]) and the calculated number of Collateral Covid Deaths (CCD) in the indicated years of pandemic. The lines (right axis) are indicating the corresponding P-Scores (P-) and the proportion of CCDs of the XCDs .
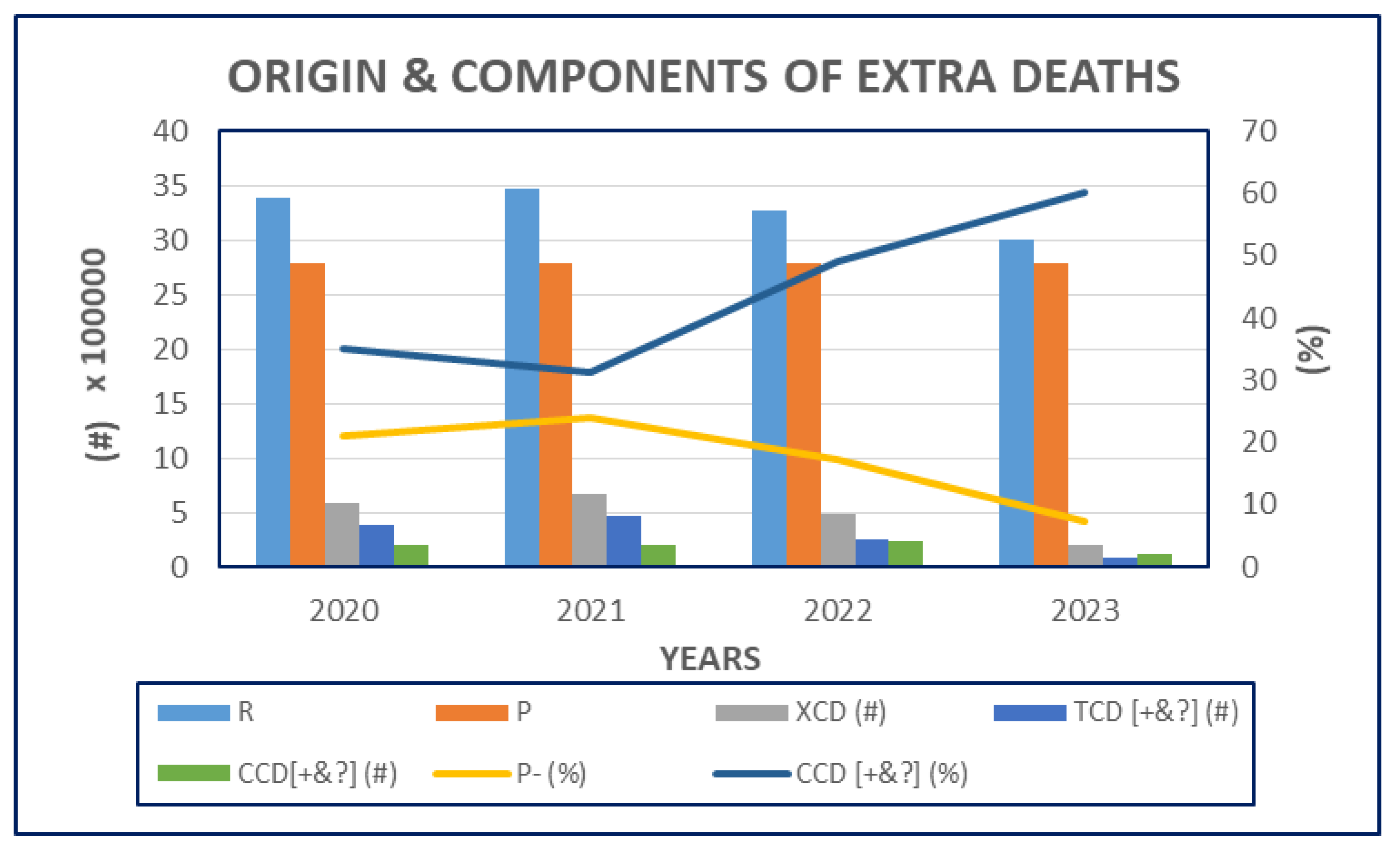
Figure 9B.
Origin & Components of Excess Covid Associated Mortality – Using the Evidence Based Method. This chart is identical to the FIGURE 9A, except that only true, test confirmed COVID deaths were included into the count of TCD [C+] and the “hearsay-based” causes (not supported by positive viral test, [C?]) were added to the CCD instead.
Figure 9B.
Origin & Components of Excess Covid Associated Mortality – Using the Evidence Based Method. This chart is identical to the FIGURE 9A, except that only true, test confirmed COVID deaths were included into the count of TCD [C+] and the “hearsay-based” causes (not supported by positive viral test, [C?]) were added to the CCD instead.
- 4.
- Effects on the Economy of the USA (short- and long-term)
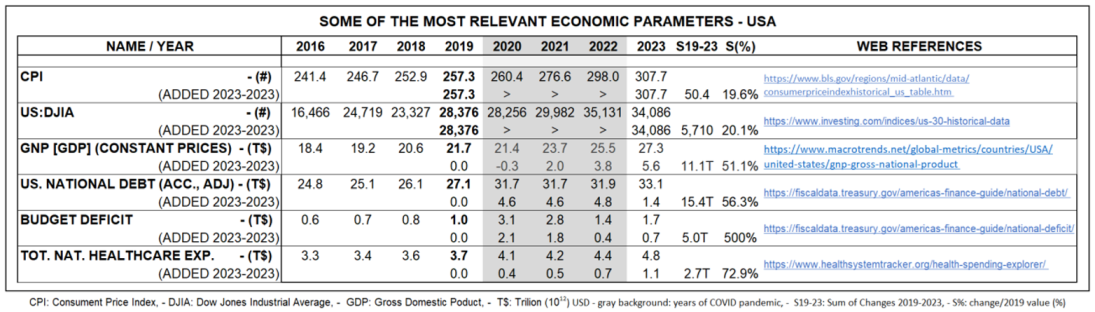
It is generally believed, that the COVID pandemic is solely responsible for (or at least major contributor to) the significantly increased expenses for the taxpayers, racketing healthcare costs, galloping inflation, uncontrolled increase of national debt (incl. generous printing of new money). However even if these statements are not entirely false, they are not entirely true either. More likely the virus served as a catalyst that amplified some of the already existing negative trends (weaknesses) of the recent political / social / economical structure of the USA. (Table IV).
Correct interpretation of economic meta-data is almost a “mission impossible” for a non-expert average American meanwhile the official interpretation is sometimes unreliable. Consequently subjective and extreme interpretations exist. Keeping in mind this difficulties we estimate the real costs of pandemic to be around 5 T$ total (corresponding to the extra budget deficit) and having two components: a) ‘virus-induced’ extra healthcare costs, 2.7 T$ and b) ‘men-made’ extra costs, 2.3 T$.

Table 4.
Caption.
 |
- 5.
- Effects on the ‘Perception’ of the Constitutional Structure and Laws of the USA
The American’s Constitutional rights having been violated, by the numerous restrains under the pandemic. However it was widely accepted as necessary under emergency conditions i.e. when the life and wellbeing of larger number of persons was seriously threatened by any natural or manmade condition(s). But a dilemma is existing – still not satisfactorily resolved – whether the emergency situation occurred as the result of a) the random and mindless accidental events in the Nature (like mutation) or b) the conscious but malicious intelligence of other arrogant and greedy Humans? What caused the emergency conditions: the virus (?), the sensation driven media (?) or both?
The answer might be found in the unusual nature of the COVID infection and the weaknesses deeply rooted in the human psychology.
- COVID is a syndemic [19].
It is a synergistic epidemics, where the occurrence and interaction of multiple diseases or health conditions exacerbate their individual impact, leading to complex health challenges and increased vulnerability in populations. It is well recognized that age and preexisting comorbidities acting synergistically when COVID becomes the UCOD. There is no one documented case of death caused by COVID of a previously healthy, young individual.
- b.
- Heterodoxy of COVID-19 [20].
COVID affects different people very differently: infected persons experience the disease very differently and this leads to serious disagreements regarding the dangerousness of the pandemic and what do we need to do to protect us. As the result we could see serious disagreements – up to the degree of animosity - develop between persons or groups of the society, involving even the most respected scientists (experts).
Stanford Professor J. P. A. Ioannidis broth to the scientific attention - already in 2020 [21] -
the importance of to differentiate promptly the true epidemic from an epidemic of false claims and potentially harmful actions. He particularly mentioned * fake news and censorship of critical scientific papers, * exaggerated pandemic estimates, * exaggerated Case Fatality Rate (CFR), * exaggerated exponential community spread, * extreme (aggressive) ‘protective’ measures, * harm from nonevidence-based judgements. Ioannidis issued warning for the potentially unwanted consequences of these false and inadequate claims, like * misallocation of resources, * economic and social disruption, * claims for ‘ones-in-a-century pandemic.
- c.
- COVID induced ‘nocebo’ effects [22].
In addition to well-known placebo effects, so-called “nocebo” effects also exist. Due to the placebo effect, a person recovers from an illness because they expect to recover. When a person suffers from a nocebo effect, on the contrary, they get ill just because they expect to become ill. When people expected to be infected with the “deadly China virus” every sneeze became the alarming sign of COVID infection even for otherwise cautious doctors. Not surprisingly COVID became the first and best choice when somebody died and the physicians were expected to state the UCOD on the death certificate. These nocebo generated “hearsay” COVID deaths occurred mostly in cases when the objective laboratory confirmation (specific COVID viral test) was missing of some reason.
- d.
The pandemic reignited the century old inherent political antagonism that was comfortably dormant in USA after the Cold War. Tons of publications blames the social conditions for the occurrence and deadliness of the pandemic. This is very unusual and surprising, because major catastrophes used to unite a nation: people first has to survive together, they can fight with each other later. (Just remember the effect of “September 11” on the American people).
Discussion
The human life is strongly protected by religious as well as secular laws. Killing -including mercy killing (euthanasia) and even suicide - are criminalized acts and punished by ‘heavenly’ and ‘earthy’ judges. This is at least the theory for public use. However killing in terms of crime & punishment is one of the most hypocritical theories ever created by the mankind. Deeply religious people were (or are) killing in the name of their religion, like under the most recognized periods of inquisitions in the 12th and 15th centuries. Killing a convicted felon is part of penal code of many legal systems even in recent times. Consequently the prohibition of murder is not generally valid. However there are groups which are more protected than others. Women are generally well protected. Pre-pubertal kids and very old persons are also well protected as person who are not capable to interfere with the established political & economic power of others.
The archetypal fear of being sick, injured and die is very strong and it is easy to find examples how different political and religious ideologies, cults were, and still are, able to generate massive revenue of this weakness. There is a practical need to calculate the material value of life (including the human life) for military and insurance purposes. However this kind of calculations are usually strongly opposed by the general public. Most people wants to believe in the ‘forever’ life and the limitless value of the living. Consequently they are hopelessly unprepared for rationally handling serious threats, like an epidemic.
Hoverer there might be one general value there consensus can be reached: a) living longer is better than shorter i.e. “longevity” has extra value; b) keeping alive two persons with the same residual years alive is better than only one; c) people are ready to pay practically any prize to keep themselves – and the so called “loved ones” – alive. This material approach to the objective value of life might explain the cost explosion of healthcare in the high GNP countries, with the USA as unchallenged leader.
Very large proportion of profit of the medical-pharmaceutical industry is directly related to senior care and terminal gerontology. Consequently a virus, like COVID is an existential threat to the most important market of this prosperous industry. It is no doubt that medical-pharmaceutical industry (and allies) were very successful to turn a potentially huge loss into an astronomical winning (tests and vaccines).
What did, on the other side, the public benefit from the active, aggressive and very costly defense policy against the COVID pandemic (compared to a passive reliance on the natural immune defense)? Honestly, nobody has the crystal ball to answer this ‘what if?’ question.
A very sensitive issue emerges when calculating the benefit/cost ration of an aggressive anti-virus policy. The total number of Excess Covid Associated Mortality (XCM) is about twice as much as the COVID Mortality (TCM). It is well known and confirmed fact that ~ 2-4 times more persons died during the pandemic than the count of real and recognized deaths caused directly by the COVID disease itself. The explanation is complex, like increase of suicide, domestic violance, misuse, neglected non-COVID diseases, et cetera. Statisticians tried to classify as many deaths as possible as COVID related to reduce the gap between true COVID Mortality and the excess COVID mortality and eliminate the Complementary, non-COVID deaths. However the gap still exists and rises some unpleasant questions: is it really possible that the state-enforced, excessive and mandatory pandemic defense killed as much persons as the COVID virus itself?
The recent actuary tables confirm that kids and seniors are the major beneficiary of improving socio- economic conditions. Elderly lives longer and spends (have to) more for healthcare than younger. They are spending their own, well-earned and saved money. It is easy to accept up to a rational level. It is not difficult to accept that the average per capita health care spending (related to the BNP of the respective countries) in well-developed west European countries indicates the rational magnitude of healthcare spending, even regarding the elderly.
What can possibly explain the excessive healthcare spending in the USA? Is this country more religious, has batter development in medical- pharmaceutical technology, has more respect for elderly than other well developed countries, like Germany, Sweden, Canada, Italy, England, and so on?
It is well recognized that old people are in the largest need of medical attention. This age related increase of demand for medical services is strongly amplified by the traditionally strongly profit oriented economy in the USA there the medical/pharmaceutical industry is one of the flagships. The practically all-covering health insurance system (including MediCare, MedicAid) programs effectively eliminates the consumer-control over medical expenses. Most Americans have no idea about the real costs of medical attention they are receiving, because it is covered by “somebody else”. The result is healthcare overconsumption, uncontrolled excessive growth of the medical/pharmaceutical “market”, year-after-year and predatory prices which remains largely invisible for the citizens.
The COVID virus showed very unusual characteristics: It infected uncontrollably, generally and equally every single member of the society, but it harmed only the biologically most vulnerable minority, meanwhile the waste majority of infected persons didn’t notice anything or, may be, some regular flu symptoms.
However, on the other hand, the aggressive defensive orders restricted the constitutional freedom of every generation Americans – that was temporarily accepted by the people with respect for the emergency situation. However some of the violations of the constitutionally guaranteed freedom, - like censorship, enforced “political correctness” - seems to last intolerably longer than it is compatible with the fundamental nature and established laws of Americans.
Conclusions & Summary
It is concluded, that
- -
- the value of “longevity” is increasing and it is already high in the USA;
- -
- The costs of longevity is extremely high in USA compared to well-developed west-European countries;
- -
- The COVID pandemic threatened the largest and most profitable market of the American health-care industry by accelerating the natural death process of elderly and seriously sick persons;
- -
- The state enforced defense policy was life-saving for the medical-pharmaceutical industry;
- -
- The benefit-cost ration of the pandemic rules is not uplifting, especially not when, it seems to be, that as much persons died due to the dramatic changes in life style (lockdown, isolation, et cet.) than as the result of the direct COVID disease.
It is recommended, that the people, media, politicians pay serious attention to review and reevaluate the events and consequences of defense actions with the sole purpose to learn from mistakes and not repeat them in the future. COVID pandemic – with all certainty was not the last pandemic in the history of mankind.
Acknowledgement
The medical profession is built on solid ethical standards [26]. A country’s medicine is as good as the commitment of its professionals to this standards and their character to keep their related promise (SIC: under oath) to the society. The author of this article wish to express his gratitude to his colleagues who are trying to guide this country through the massive fog associated with the American COVID syndemic.
Conflict of Interest
The author declare that he has no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Abbreviations
| 14+ | ||
| TCD | Total COVID Deaths | # |
| TCM | Total COVID Mortality | ratio |
| CCD | Complementary COVID Deaths | # |
| [CD+] | ‘true’ COVID Deaths confirmed by viral test | # |
| [CD?] | ‘hearsay’ COVID Deaths, not confirmed by viral test | # |
| [CD+/?] | pooled ‘true’ & ‘hearsay’ COVID deaths | # |
| XD | eXtra or eXcess Deaths | # |
| XCD | eXtra or eXcess COVID associated Deaths | # |
| XCM | Excess COVID Mortality | ratio |
| R | Reported | # |
| P | Predicted | # |
| UCOD | Underlying Couse Of Death | n. a |
| RLE | Residual Life Expectancy | years |
| ILE | Initial Life Expectancy | years |
| ALE | Accomplished Life Expectancy | years |
| MR | Mortality (death) Rate | ratio |
| TRD | Total counts of Reported Deaths | # |
| TPD | Total Projected (or expected) Deaths of all causes | # |
References
- https://www.paul.senate.gov/wp-content/uploads/2023/08/FILE_7353.pdf.
- Case 2:20-cv-00966-NR Document 4 Filed 06/29/20 - https://www.brennancenter.org/sites/default/files/2020-07/Trump%20Complaint.pdf.
- Press release by the Office of Attorney General of Texas on November 30, 2023. - https://texasattorneygeneral.gov/news/releases/attorney-general-ken-paxton-sues-pfizer-misrepresenting-covid-19-vaccine-efficacy-and-conspiring & [District Court of Lubbock County, TX, CIVIL DOCKET FOR CASE #: 5:23-cv-00312-C, filed Nov. 30, 2023] .
- PROJECT VERITAS FILMS PFIZER DIRECTOR OF R&D SAYING ‘MUTATING’ COVID-19 FOR NEW VACCINES IS UNDER CONSIDERATION - Jan 25, 2023.
- Biro JC: CRITICAL REVIEW OF THE DIAGNOSTIC AND STATISTICAL SUPPORT FOR COVID EPIDEMIC IN USA - JMIR Preprints. 18/05/2024:60679 - URL: https://preprints.jmir.org/preprint/60679. [CrossRef]
- Florida Department of Health - January 03, 2024 - a https://www.floridahealth.gov/newsroom/2024/01/20240103-halt-use-covid19-mrna-vaccines.pr.htm l.
- STATE OF KANSAS, ex rel., KRIS W. KOBACH, Attorney General, - Plaintiff, v.PFIZER INC., - Defendant.: Petition – 2024.06.17 - https://ag.ks.gov/docs/default-source/documents/2024-06-15-pfizer-complaint-(002).pdf.
- It was the legendary life length of Moses – the Jewish Prophet.
- The author’s terminology.
- The author’s terminology.
- Like the market value of Leonardo da Vinci-s Mona Lisa, hanged in the Louvre Museum forever. Living long or forever is one of the wildest phantasies of the Homo sapiens. Just to mention some variations in the subject: “aqua vitae”, “fountain of youth”, “philosopher’s stone”, “and elixir of life”. The religious concept of “afterlife” is probably one of the most powerful ideas of living-for-ever.
- Esteban Ortiz-Ospina and Max Roser (2017) - “Healthcare Spending” Published online at OurWor.
- The Year in Healthcare Charts. Available from: http://www.forbes.com/sites/danmunro/2012/12/30/2012-the-year-in-healthcare-charts/#33337736458f.
- SOURCE: Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statistics Group.- https://www.cms.gov/data-research/statistics-trends-and-reports/national-health-expenditure-data/state-residence dInData.org - https://ourworldindata.org/financing-healthcare.
- E. Mathieu, et al.: (2020) - "Coronavirus Pandemic (COVID-19)". Published online at OurWorldInData.org. Retrieved from: https://ourworldindata.org/coronavirus.
- Wang, H., et al. (2022). Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19-related mortality, 2020–21. The Lancet.- from: https://ourworldindata.org/coronavirus.
- Methods for estimating the excess mortality associated with the COVID-19 pandemic – WHO - 19 May 2023 - https://www.who.int/publications/m/item/methods-for-estimating-the-excess-mortality-associatedwith-the-covid-19-pandemic .
- Publications often not distinguish CCM from TCM as a separate category of XCM and ignoring the ‘man-made’ (human) contributions to the consequences of the pandemic.
- Shelke A, Shelke S, Acharya S, et al. (November 05, 2023) Synergistic Epidemic or Syndemic: An Emerging Pattern of Human Diseases. Cureus - 15(11): e48286. - https://pubmed.ncbi.nlm.nih.gov/38058320/. [CrossRef]
- Yaffa Shir-Raz at. Al. - Censorship and Suppression of Covid-19 Heterodoxy: Ta.ctics and Counter-Tactics - Minerva (2023) 61:407–433 - https://link.springer.com/article/10.1007/s11024-022-09479-4. [CrossRef]
- John P. A. Ioannidis - Coronavirus disease 2019: The harms of exaggerated information and non-evidence-based measures – Editorial - Eur J Clin Invest. 2020;50:e13222. - https://doi.org/10.1111/eci.13222 - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7163529/pdf/ECI-50-e13222.pdf.
- Philipp Bagus, José Antonio Peña-Ramos, and Antonio Sánchez-Bayón, “COVID-19 and the Political Economy of Mass Hysteria,” International Journal of Environmental Research and Public Health 18, no. 4 (2021): 1376. [CrossRef]
- Philipp Bagus, José Antonio Peña-Ramos, Antonio Sánchez-Bayón: Capitalism, COVID-19 and lockdowns - Business Ethics, Env & Resp. 2023;32:41–51. https://onlinelibrary.wiley.com/doi/pdf/10.1111/beer.12431. [CrossRef]
- Hart PS, Chinn S, Soroka S. Politicization and Polarization in COVID-19 News Coverage. Sci Commun. 2020 Oct;42(5):679-697. [CrossRef] [PubMed] [PubMed Central]
- Stroebe W, et al: Politicization of COVID-19 health-protective behaviors in the United States: Longitudinal and cross-national evidence. PLoS One. 2021 Oct 20;16(10):e0256740. [CrossRef]
- AMA Code of Medical Ethics - https://code-medical-ethics.ama-assn.org/.
Figure 2.
Annual Changes of Mortality Rates by Age Groups – USA: The thick red line emphasizes the first year of COVID pandemic (2020).
Figure 2.
Annual Changes of Mortality Rates by Age Groups – USA: The thick red line emphasizes the first year of COVID pandemic (2020).
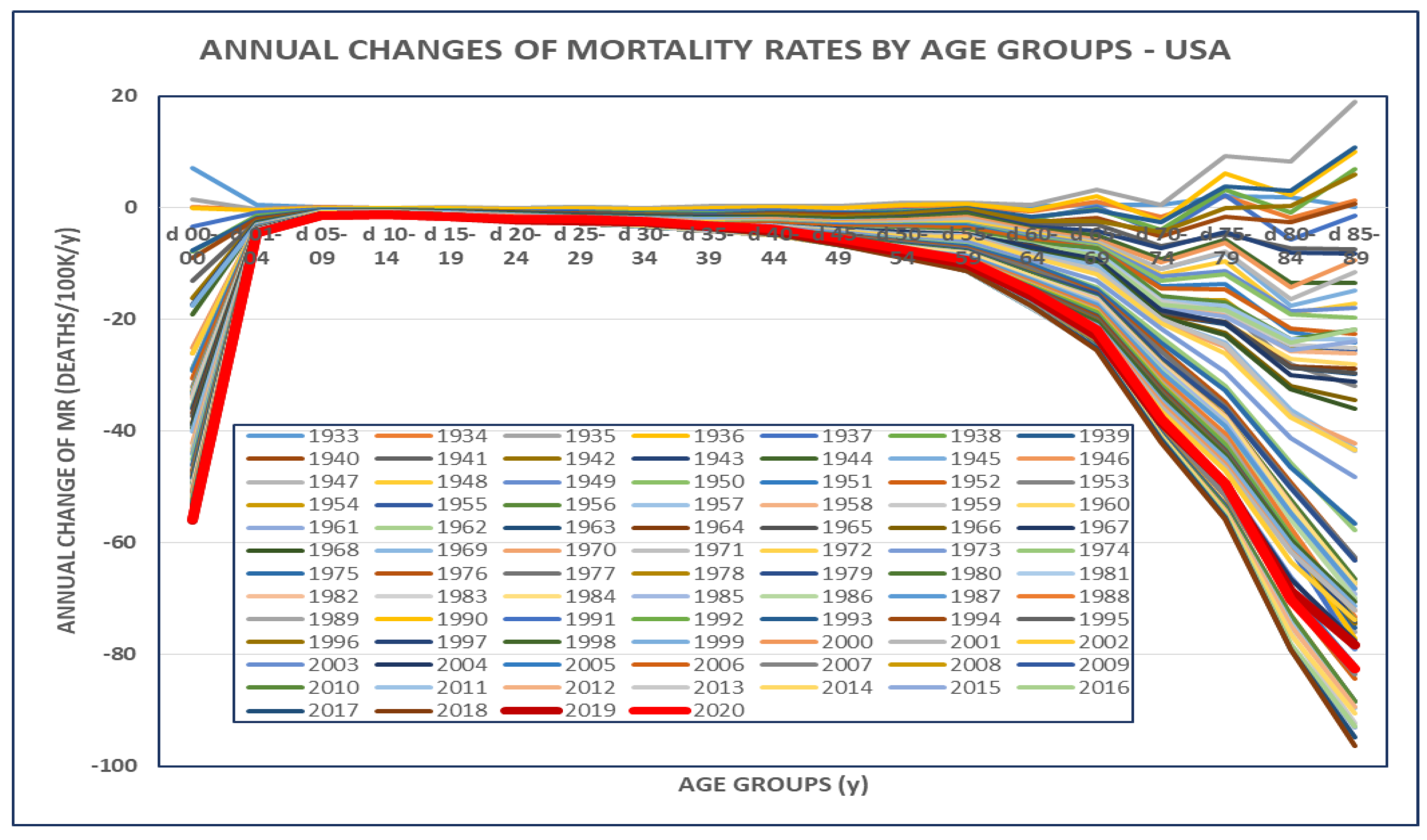
Figure 3.
Population of USA by Age – 2010-2019: The arrow and the shaded area indicates the phase-shift of population-waves toward the higher ages, i.e. the population “pattern” is very similar in 2010 (POP2010 – yellow line) and 2019 (POP2019 – blue line) but shifted right ~ ca 9 years.
Figure 3.
Population of USA by Age – 2010-2019: The arrow and the shaded area indicates the phase-shift of population-waves toward the higher ages, i.e. the population “pattern” is very similar in 2010 (POP2010 – yellow line) and 2019 (POP2019 – blue line) but shifted right ~ ca 9 years.
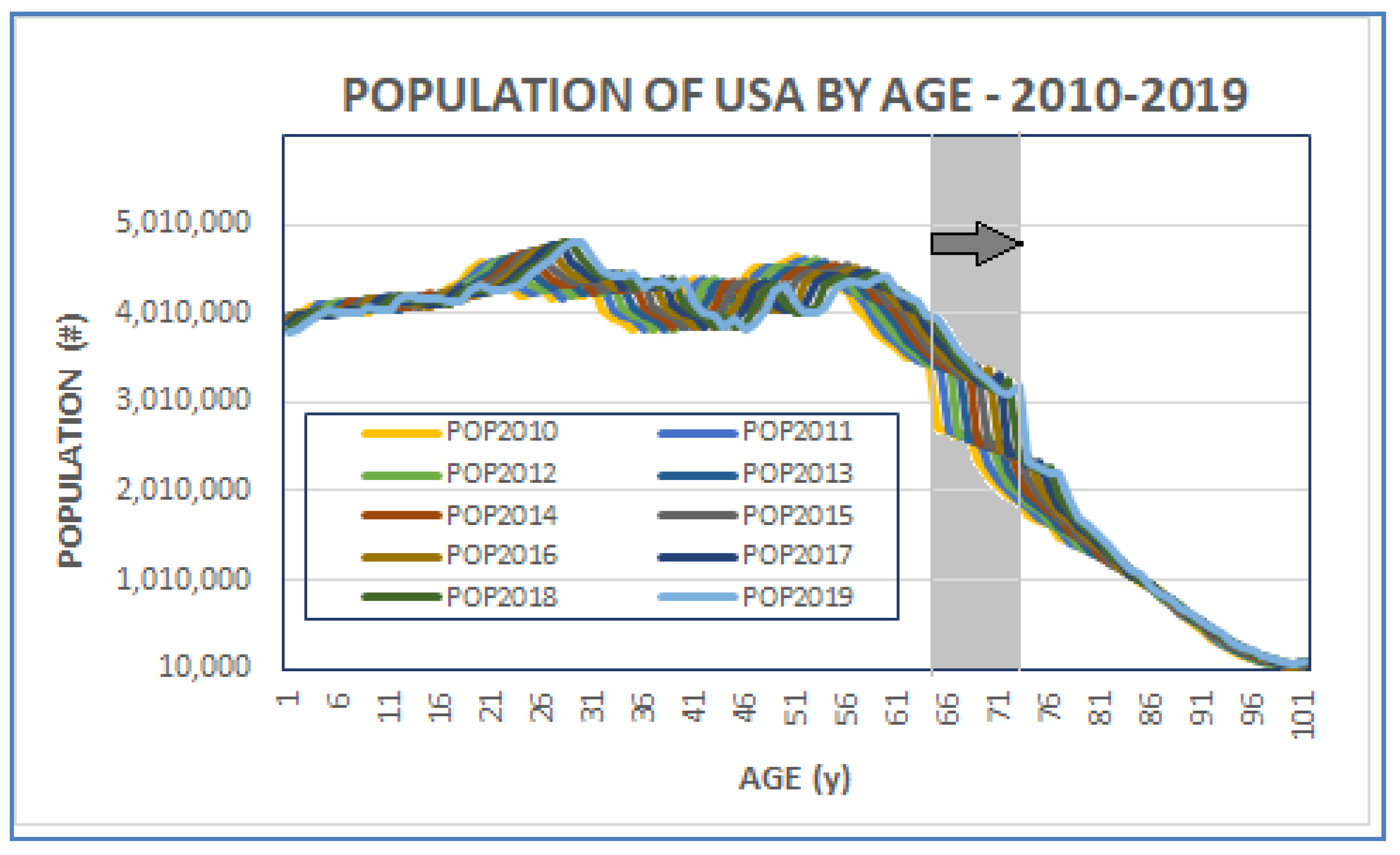
Figure 4.
Estimation of the ‘Value’ of Life by Age Groups – Individually & Collectively. The gray line indicates the individual Residual Life Expectancy (RLE) as percentage (%) of Initial Life Expectancy (ILE=77.4y) by age groups (right axis). The yellow line indicates the collective RLE of an age group expressed as % of total RLE (y/1M) (right axis). The blue line indicates the % of the USA’ population (POP=328 M) by age groups (left axis).
Figure 4.
Estimation of the ‘Value’ of Life by Age Groups – Individually & Collectively. The gray line indicates the individual Residual Life Expectancy (RLE) as percentage (%) of Initial Life Expectancy (ILE=77.4y) by age groups (right axis). The yellow line indicates the collective RLE of an age group expressed as % of total RLE (y/1M) (right axis). The blue line indicates the % of the USA’ population (POP=328 M) by age groups (left axis).
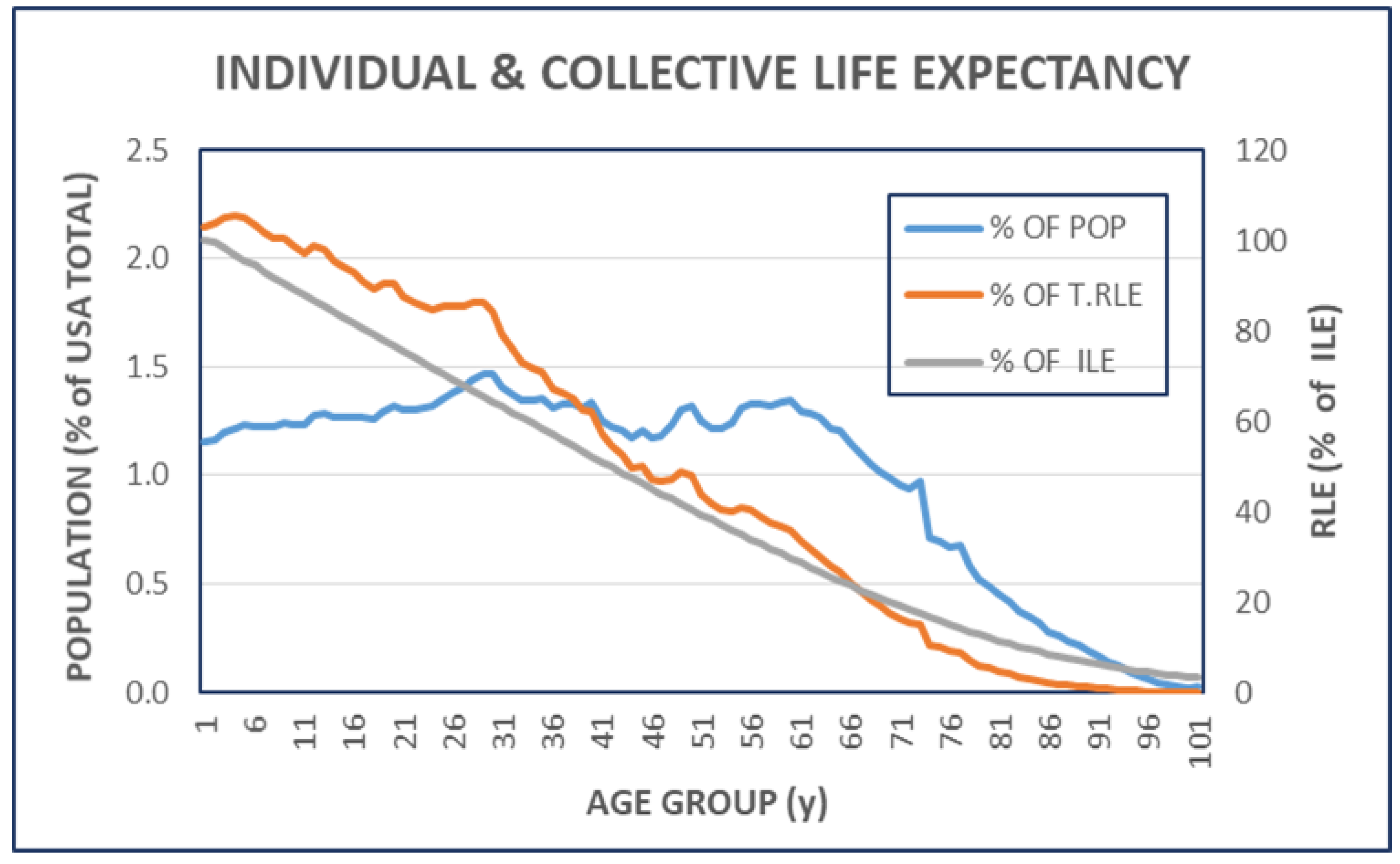
Figure 7.
Population Changes Associated to COVID Pandemic in USA, 2020-2023. The difference (bars, left axis) and the ratio (line, right axis) of population, by age groups, before and under the COVID pandemic are shown. The average of annual population counts 2010-2019 and 2020-2023 were used. (See even TABLE II).
Figure 7.
Population Changes Associated to COVID Pandemic in USA, 2020-2023. The difference (bars, left axis) and the ratio (line, right axis) of population, by age groups, before and under the COVID pandemic are shown. The average of annual population counts 2010-2019 and 2020-2023 were used. (See even TABLE II).
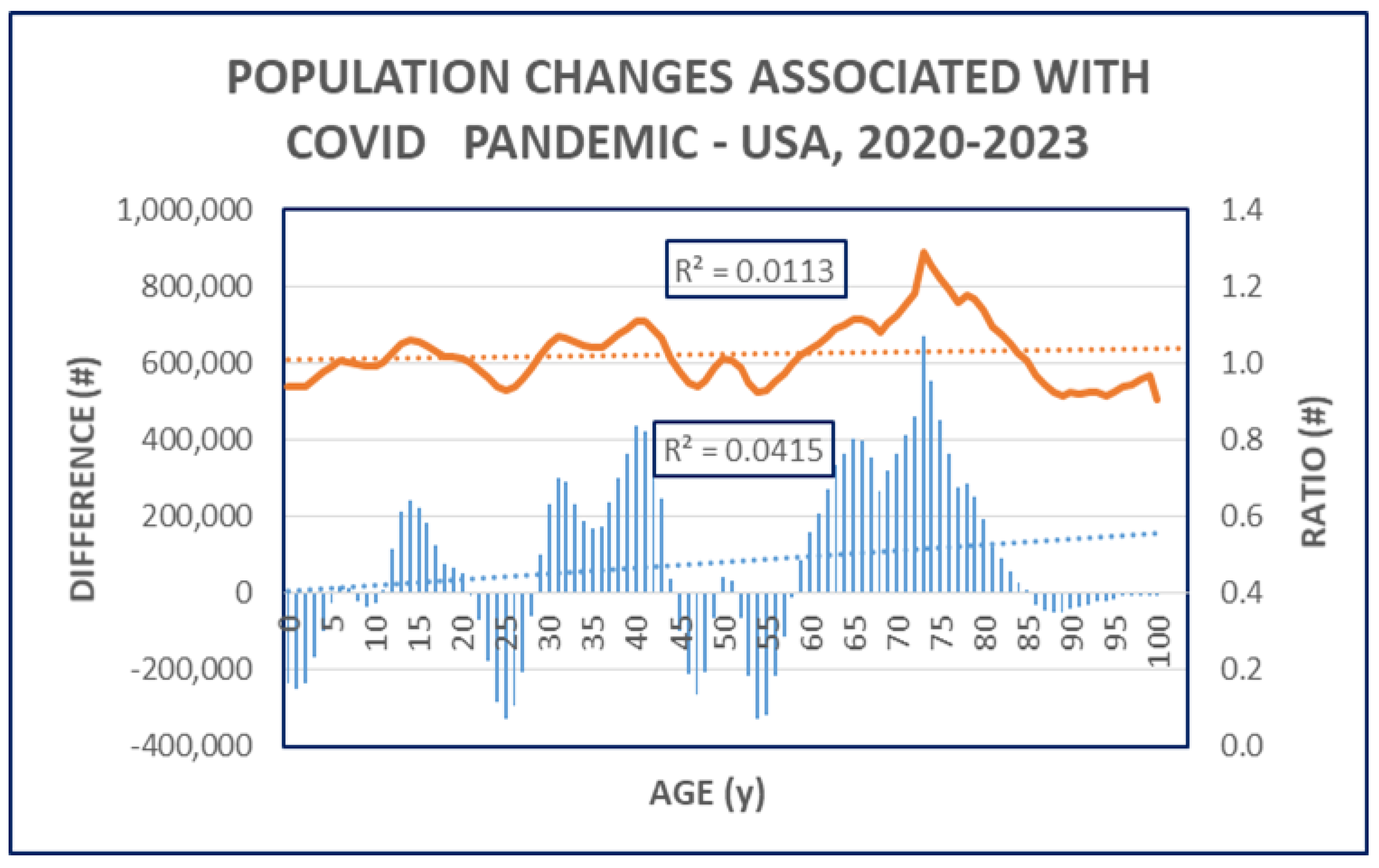
Figure 8.
Calculated Excess Mortality by Age-groups & Weeks of Years. The weekly variation of the average P-Scores (%) of different age groups is illustrated by lines. The shaded area emphasizes the negative P-Scores almost exclusively belonging to the youngest age group.
Figure 8.
Calculated Excess Mortality by Age-groups & Weeks of Years. The weekly variation of the average P-Scores (%) of different age groups is illustrated by lines. The shaded area emphasizes the negative P-Scores almost exclusively belonging to the youngest age group.
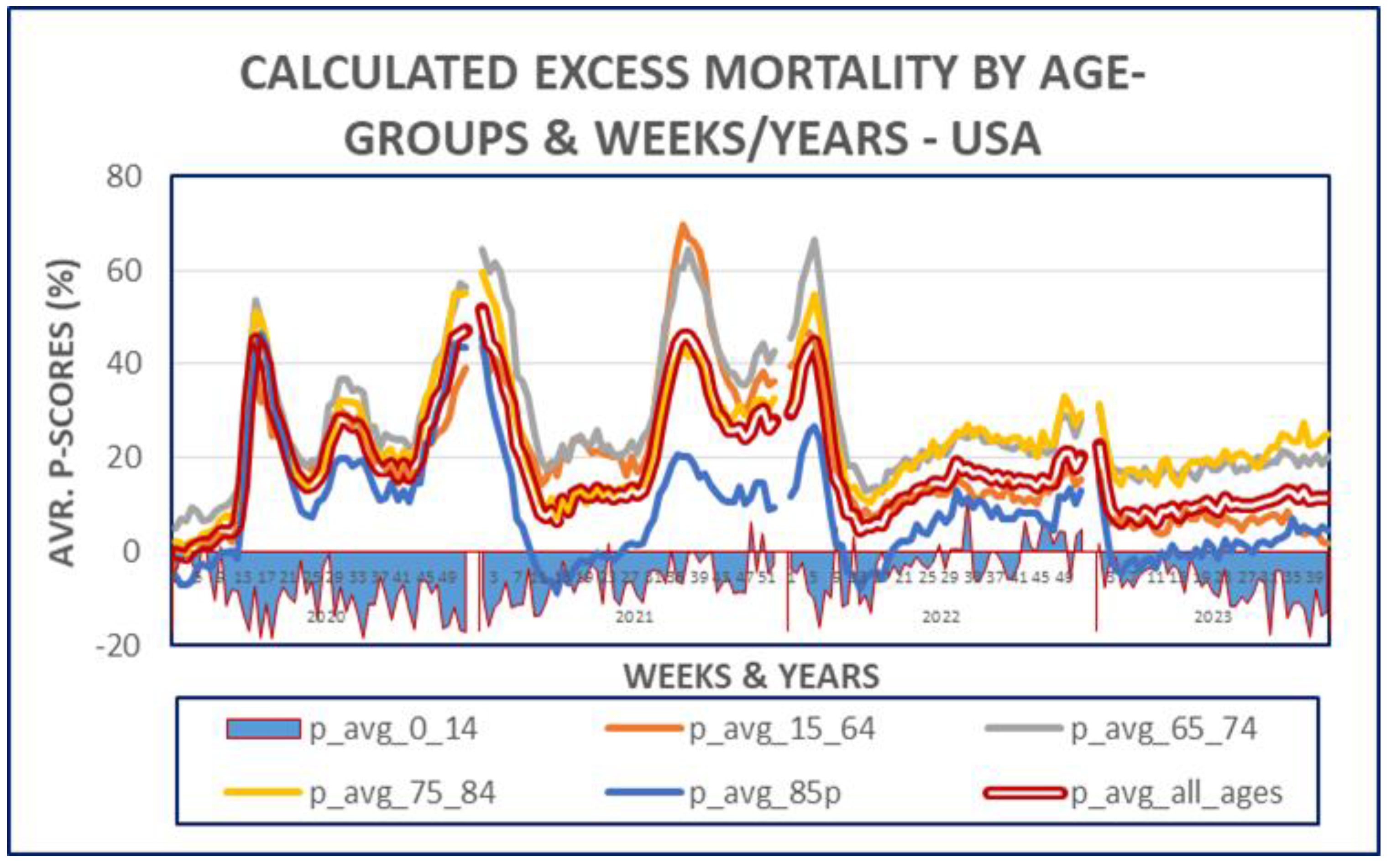
Table 1.
Caption.
 |
Table 2.
Caption.
 |
Table 3.
Caption.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



