
Submitted:
14 September 2024
Posted:
17 September 2024
You are already at the latest version
Abstract
Objective: The main purpose of this meta-analysis was to assess the efficacy and safety of Oncolytic Viruses (OVs) in glioma therapy. Methods: We searched the literature in PubMed, EMBASE, Web of Science, and the Cochrane Library. The primary outcomes assessed were overall survival (OS), progression-free survival (PFS), objective response rate (ORR), and adverse events (AEs). The risk of bias was evaluated by sensitivity analysis and publication bias. Results: We identified 21 studies with 440 patients in this meta-analysis. In the single-arm analysis, the results showed that the 1-year OS rate was 47% (95% CI: 34%-61%, I2 = 75%) and the 2-year OS rate was 14% (95% CI: 10%-20%, I2 = 0%). The median OS was 12.48 months (95% CI: 10.71-14.25, I2 = 96%). The 1-year PFS rate was 13% (95% CI: 5%-24%, I2 = 0%), with the median PFS being 4.01 months (95% CI: 2.99-45.03, I2 = 96%). The pooled estimate of ORR was 7% (95% CI: 3%-12%, I2 = 23%). Funnel plots for median PFS were asymmetric with Egger’s test P < 0.01 indicating publication exists. The incidence of OVs-related AEs was 49% (95% CI: 20%-79%, I2 = 95%), and AEs > grade 3 was 8% (95% CI: 3%-16%, I2 = 62%). Conclusion: This meta-analysis indicated that OVs therapy was relatively safe but did not significantly extend survival in patients with gliomas.
Keywords:
Glioma
; Oncolytic viruses
; Drug efficacy
; Drug safety
; Meta-analysis
1. Introduction
Gliomas represent the most prevalent malignant tumor of the central nervous system, comprising 49% glioblastomas (GBM) and 30% diffusely infiltrating low-grade gliomas (LGG) [1]. The CBTRUS Statistical Report illustrates that GBM exhibits a higher prevalence among adults compared to children, with incidence rates escalating with age, peaking in the 75-84 age bracket [2]. GBM is considered one of the most malignant forms of glioma and is characterized by a median survival time of approximately 8 months [2,3]. The standard treatment protocol, known as the Stupp regimen, involves maximal surgical resection of tumor tissue while preserving neural integrity, supplemented by radiotherapy and temozolomide chemotherapy, the latter being the primary chemotherapeutic agent for gliomas [4]. Nevertheless, the prognosis for gliomas remains dismal, with a mere 6.8% survival rate at the five-year mark post-diagnosis of GBM [2]. Advanced age, propensity for radiotherapy resistance, and incomplete tumor resection all serve as negative prognostic indicators for malignant gliomas [5].
Oncolytic viruses (OVs) are a novel class of tumor immunotherapeutic agents. These viruses, whether occurring naturally or genetically modified, exhibit a characteristic of selectively targeting tumor cells, thereby eliciting replication within tumor cells and subsequent tumor cell lysis [6]. Upon infecting tumor cells, OVs trigger various mechanisms including apoptosis, necrosis, and autophagy induction, thereby culminating in the destruction of the malignant cells [7]. This property renders OVs a highly promising modality in anti-tumor immunotherapy [8,9]. Following the FDA approval of the first OV drug, talimogene laherparepvec (T-VEC), for the treatment of advanced melanoma in 2015, clinical trials investigating OVs as monotherapies or in combination with other modalities have been initiated across a broad spectrum of cancers including gliomas, bladder, and colorectal cancers [10,11]. Notably, a modified herpes simplex virus (HSV) received approval for the treatment of brain cancers, such as GBM, in Japan in 2021. Numerous preclinical studies have reported promising outcomes, demonstrating significant anti-tumor activity of OVs against gliomas and a prolongation in survival in animal models [12,13,14,15]. However, the efficacy of OVs in improving the prognosis of gliomas in clinical trials remains controversial. Consequently, we conducted this meta-analysis to systematically assess the feasibility of OVs application in gliomas.
2. Materials and Methods
2.1. Search Strategy
We searched the Embase, PubMed, Web of Science, and Cochrane Library databases for literature published since the establishment of the database until August 2024, with no language restrictions. Keywords included “oncolytic virus”, “Virus, Oncolytic”, “oncolytic treatment”, “oncolytic adenovirus”, “oncolytic virotherapy”, “oncolytic immunotherapy”, and “oncolytic vaccine”, and “glioma” “glioblastoma”, “glial tumor”, “astrocytoma” “oligodendroglioma”, and “ependymoma”. The detailed search strategy was listed in the Supplementary Table S1.
2.2. Study Selection
We pre-registered this meta-analysis (PROSPERO ID: CRD42024577506) and utilized Covidence for study screening.
We included all clinical studies of patients with primary or recurrent glioma treated with oncolytic viruses. These studies can provide viral interventions (virus family, mode of administration, dose, duration of administration) and patient outcomes (overall survival (OS), progression-free survival (PFS), and objective response rate (ORR)). Studies were rejected if they meet the following criteria: (1) in vitro or animal experiments; (2) Viral interventions or patient outcomes are not available; and (3) case reports or conference abstract.
2.3. Data Extraction
Two authors independently screened the literature and then extracted data, with a third researcher overseeing the process. Any disagreements were resolved through group discussions.
The extracted data includes (1) Study characteristics: author, year, country, study phase, and number of participants; (2) Patient information: diagnosis, gender, and age; (3) Treatment strategy: viral family, delivery method, dose and duration, combination administration; (4) Primary clinical outcomes: OS, PFS, ORR, and AEs.
2.4. Quality Assessment
The Cochrane Risk of Bias Tool (ROB2) was used to evaluate the quality of randomized controlled trial (RCT), and NOS was used in retrospective cohort studies and prospective case-control studies.
2.5. Statistical Analysis
All the analyses were performed by R (Version 4.4.1). Methods for evaluating heterogeneity include the Cochran Q test and I2 statistics. The source of heterogeneity was investigated by subgroup analysis. Funnel plot, Egger’s test, and Begg’s test were conducted to evaluate publication bias. P < 0.05 meant that the difference was statistically significant.
3. Results
3.1. Studies Selection and Characteristics
As shown in Figure 1, we retrieved a total of 4348 articles in 4 databases and deleted 1688 duplicates. By sifting through the titles and abstracts of the articles, we removed 2540 irrelevant articles. The remaining 120 articles were surveyed by full-text reading and 99 articles were then excluded. Finally, 21 articles with 440 patients were included [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36].
The detailed baseline characteristics of the included studies were shown in Table 1. This meta-analysis included 14 phase I studies, 2 phase II studies, and 5 phase I/II studies with publication years ranging from 2000 to 2024. Concerning the delivery method, 19 studies utilized intratumoral administration, and 2 studies utilized intravenous administration.
3.2. Overall Survival by Single-Arm Meta-Analysis
To explore the effect of OVs on OS in glioma patients, we pooled 21 articles containing 22 single-arm studies [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36]. The forest plot showed that the median OS of glioma patients receiving OVs therapy was 12.43 months (95% CI: 10.65-14.21, I2 = 96%, P < 0.01) (Figure 2A). Subgroup analysis revealed recurrent glioma was an important source of heterogeneity in this meta-analysis (Table 2). The sensitivity analysis results of the median OS suggested that no studies should be ruled out (Figure 2B). The funnel plot for the median OS was symmetric and both Egger’s test (P = 0.15) and Begg’s test results exhibited no obvious difference (P = 0.76) (Figure 2C).
We further pooled the OS data at 1-year 14 studies [16,17,18,19,21,22,23,24,25,31,33,34,35] and 2-year (11 studies) [16,17,18,19,23,24,25,31,34,35,36] from glioma patients treated with OVs therapy. As shown in Figure 3, 1-year and 2-year OS rates for glioma patients were 47% (95% CI: 34%-61%, I2 = 75%, P < 0.01) and 14% (95% CI: 10%-20%, I2 = 0%, P = 0.87), respectively.
3.3. Progression-Free Survival by Single-Arm Meta-Analysis
A subsequent analysis of PFS data from18 single-arm studies in 17 publications found that the median PFS of glioma patients receiving OVs therapy was 3.92 months (95% CI: 2.93-4.92, I2 = 95%, P < 0.01) (Figure 4A) [16,18,19,20,21,22,23,24,25,26,27,29,30,31,33,34,35]. Although no statistical difference, OVs showed a longer PFS in the treatment of newly diagnosed (ND) glioma (Table 3). Based on the sensitive analysis result of median PFS, no research needs to be ruled out (Figure 4B). The funnel plot for the median PFS was asymmetric with significant differences in Egger’s test (P < 0.01) (Figure 4C) indicating publication exists.
3.4. Objective Response Rate by Single-Arm Analysis
We then included 10 studies with 190 patients to evaluate the effect of OVs on ORR in glioma patients
To assess the effect of OVs on ORR in glioma patients, we included studies with 10 studies with 190 patients for analysis [18,19,21,22,23,25,26,33,35,36]. The pooled estimate of ORR was 7% (95% CI: 4%-12%, I2 = 33%, P = 0.14) (Figure 6).
To evaluate the safety of OVs in the treatment of gliomas, we analyzed the OVs-related adverse events (AEs). In total, 9 studies with 233 patients were included in the analysis of AEs related to OVs [17,18,21,22,23,26,27,35,36], and 13 studies with 268 patients were included in the analysis of AEs > grade 3 [16,17,18,19,21,22,23,24,25,27,30,34,35]. The results showed that the incidence of OVs-related AEs was 49% (95% CI: 20%-79%, I2 = 95%, P < 0.01) (Figure 7A), and AEs > grade 3 was 8% (95% CI: 3%-16%, I2 = 62%, P < 0.01) (Figure 7B).
4. Discussion
To assess the efficacy and safety of OVs in the treatment of gliomas, 21 articles with 440 patients were included in this meta-analysis. Our results revealed that OVs therapy did not prolong OS and PFS in this meta-analysis. In glioma patients treated with OVs, the incidence of AEs was 49%, and the incidence of AEs ≥ grade 3 was only 8%, suggesting that OVs were relatively safe in glioma.
The median OS and PFS in glioma patients treated with OVs therapy were 12.48 months and 4.01 months, respectively. A recently published meta-analysis delineated a median OS range from 7.2 to 16 months and a median PFS range from 5.1 to 12 months among patients with recurrent high-grade glioma undergoing re-irradiation combined with systematic therapy [37]. Notably, despite optimal treatment approaches, GBM patients typically exhibit a median OS of merely 12-15 months [38]. Furthermore, a prior investigation conducted by our research team established a median PFS of 3.72 months for PD-1/PD-L1 therapy in glioma patients [39]. These findings collectively suggested that OVs fail to confer a survival advantage in the context of gliomas management. Due to differences in the subtype, stage, and inherent heterogeneity of glioma, only a portion of glioma patients will eventually benefit from OVs treatment, so how to screen glioma patients for oncolytic virus therapy and select the appropriate oncolytic virus therapy for them is still a great challenge.
The tumor immune microenvironment, comprising glioma cells, various immune cells, and diverse chemokines and cytokines, has been implicated in the suboptimal efficacy of several immunotherapies [40,41]. Among the non-tumor cells within this milieu, tumor-associated macrophages (TAMs) are predominant, and the intricate interplay between TAMs and OV-infected tumors has been proposed as a significant factor contributing to the therapeutic ineffectiveness of OVs [42,43]. TAMs undergo polarization influenced by different microenvironmental factors and cytokines, displaying distinct phenotypic characteristics, conventionally categorized into M1 and M2 types [44]. M1 TAMs instigate a pro-inflammatory response, while M2 TAMs engage in an anti-inflammatory response, characterized by the expression of surface proteins following stimulation with interleukin-10 (IL-10) and transforming growth factor beta (TGF-β). Following administration of OVs, beyond direct tumor lysis, infected tumor cells release chemoattractants such as CCL2, which recruit macrophages and microglia to the injection site. This recruitment prompts polarization of TAMs towards the M1 phenotype, fostering an immune response against tumor proliferation [44,45]. Nonetheless, this cascade also triggers an antiviral response, thereby attenuating the therapeutic efficacy of OVs. During the lytic cycle of lysosomal virus infection, both innate and adaptive immunity are engaged, leading to rapid recruitment and activation of macrophages into virus-infected tumor cells. These polarized pro-inflammatory macrophages secrete chemokines and cytokines, activating other innate immune cells like natural killer cells and dendritic cells (DCs), thus bolstering the antiviral immune response and facilitating viral clearance via phagocytosis [46]. Additionally, TAM-induced secretion of TNF-α was observed to stimulate extracellular apoptotic pathways, substantially diminishing viral replication [47]. In vitro investigations have corroborated that TNF-α inhibitors markedly enhanced the overall efficacy of lysovirus therapy [48,49]. Furthermore, infected tumor cells exhibit heightened release of type I interferon, which not only impedes the intracellular viral life cycle but also augments the recruitment of antigen-presenting cells, dendritic cells, innate lymphocytes, and ultimately, tumor-specific cytotoxic T-lymphocytes [50,51].
Another challenge encountered in systemic administration of OVs is its limited diffusion ability within tumor tissues to effectively cross the blood-brain barrier. Additionally, systemic administration of OVs is vulnerable to neutralization by complement and antibodies, as well as early uptake by circulating macrophages, thereby further reducing the viral load that reaches glioma cells [52]. Among the 21 studies included in this meta-analysis, local administration was utilized for efficient virus transport, which encompassed intratumoral administration as well as convection-enhanced delivery (CED). Intratumoral administration, being the most commonly employed method, ensures localized high drug concentrations within the tumor. However, invasive procedures like CED, implantation in the residual cavity post-tumor removal, and other modalities present challenges in terms of repeated drug administration [53]. At present, various drug loading systems and delivery techniques are being explored to overcome the obstacles associated with gliomas drug delivery modalities. These approaches encompass nanoparticle modification, exosome modification, autologous mesenchymal stem cells, and others. Encouragingly, preclinical studies have demonstrated improved delivery outcomes [54,55,56,57]. We are eagerly anticipating and firmly believe that, in the near future, effective therapeutic concentrations within the brain can be achieved through systemic delivery or more convenient delivery methods, resulting in groundbreaking advancements in glioma treatment.
5. Conclusions
The OVs therapy is relatively safe but is not effective in extending the survival of glioma patients.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Search strategy in the different database.
Author Contributions
Conceptualization, Y.F.Z. and W.J.Z.; methodology, Y.F.Z.; software, Y.F.Z.; validation, S.D., and Z.Z.L.; data curation, L.J.Z., J.Y., S.D., and Z.Z.L.; writing—original draft preparation, Y.F.Z.; writing—review and editing, W.J.Z., Y.F.Z., L.J.Z., J.Y., S.D., Z.Z.L., and Q.Q.Y.; supervision, Q.Q.Y.; project administration, Q.Q.Y.; funding acquisition, W.J.Z. and Q.Q.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the Hunan Provincial Natural Science Foundation of China (No.2024JJ5621, No.2024JJ5620 and No.2022JJ80047).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Schaff LR, Mellinghoff IK. Glioblastoma and Other Primary Brain Malignancies in Adults: A Review. JAMA. 2023; 329: 574-87.
- Ostrom QT, Cioffi G, Waite K, Kruchko C, Barnholtz-Sloan JS. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2014-2018. Neuro Oncol. 2021; 23: iii1-iii105. [CrossRef]
- Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, Hawkins C, Ng HK, Pfister SM, Reifenberger G, Soffietti R, von Deimling A, Ellison DW. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol. 2021; 23: 1231-51. [CrossRef]
- Weller M, van den Bent M, Preusser M, Le Rhun E, Tonn JC, Minniti G, Bendszus M, Balana C, Chinot O, Dirven L, French P, Hegi ME, Jakola AS, et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat Rev Clin Oncol. 2021; 18: 170-86. [CrossRef]
- Tan AC, Ashley DM, Lopez GY, Malinzak M, Friedman HS, Khasraw M. Management of glioblastoma: State of the art and future directions. CA Cancer J Clin. 2020; 70: 299-312. [CrossRef]
- Ma R, Li Z, Chiocca EA, Caligiuri MA, Yu J. The emerging field of oncolytic virus-based cancer immunotherapy. Trends Cancer. 2023; 9: 122-39. [CrossRef]
- Yan Z, Zhang Z, Chen Y, Xu J, Wang J, Wang Z. Enhancing cancer therapy: the integration of oncolytic virus therapy with diverse treatments. Cancer Cell Int. 2024; 24: 242. [CrossRef]
- Wu YY, Sun TK, Chen MS, Munir M, Liu HJ. Oncolytic viruses-modulated immunogenic cell death, apoptosis and autophagy linking to virotherapy and cancer immune response. Front Cell Infect Microbiol. 2023; 13: 1142172. [CrossRef]
- Yang C, Hua N, Xie S, Wu Y, Zhu L, Wang S, Tong X. Oncolytic viruses as a promising therapeutic strategy for hematological malignancies. Biomed Pharmacother. 2021; 139: 111573. [CrossRef]
- Larocca CA, LeBoeuf NR, Silk AW, Kaufman HL. An Update on the Role of Talimogene Laherparepvec (T-VEC) in the Treatment of Melanoma: Best Practices and Future Directions. Am J Clin Dermatol. 2020; 21: 821-32. [CrossRef]
- Zhu X, Fan C, Xiong Z, Chen M, Li Z, Tao T, Liu X. Development and application of oncolytic viruses as the nemesis of tumor cells. Front Microbiol. 2023; 14: 1188526. [CrossRef]
- Bommareddy PK, Wakimoto H, Martuza RL, Kaufman HL, Rabkin SD, Saha D. Oncolytic herpes simplex virus expressing IL-2 controls glioblastoma growth and improves survival. J Immunother Cancer. 2024; 12.
- Li S, Guo Y, Ning W, Chen Y, Xu J, Zhao C, Wang J, Qu Y, Zhang M, Wang P, Wang Y, Wang S, Zhang H. Oncolytic virus Ad-TD-nsIL-12 inhibits glioma growth and reprograms the tumor immune microenvironment. Life Sci. 2024; 336: 122254. [CrossRef]
- Martinez-Velez N, Garcia-Moure M, Marigil M, Gonzalez-Huarriz M, Puigdelloses M, Gallego Perez-Larraya J, Zalacain M, Marrodan L, Varela-Guruceaga M, Laspidea V, Aristu JJ, Ramos LI, Tejada-Solis S, et al. The oncolytic virus Delta-24-RGD elicits an antitumor effect in pediatric glioma and DIPG mouse models. Nat Commun. 2019; 10: 2235. [CrossRef]
- Soldozy S, Skaff A, Soldozy K, Sokolowski JD, Norat P, Yagmurlu K, Sharifi KA, Tvrdik P, Park MS, Kalani MYS, Jane JA, Syed HR. From Bench to Bedside, the Current State of Oncolytic Virotherapy in Pediatric Glioma. Neurosurgery. 2020; 87: 1091-7. [CrossRef]
- Chiocca EA, Abbed KM, Tatter S, Louis DN, Hochberg FH, Barker F, Kracher J, Grossman SA, Fisher JD, Carson K, Rosenblum M, Mikkelsen T, Olson J, et al. A phase I open-label, dose-escalation, multi-institutional trial of injection with an E1B-Attenuated adenovirus, ONYX-015, into the peritumoral region of recurrent malignant gliomas, in the adjuvant setting. Mol Ther. 2004; 10: 958-66. [CrossRef]
- Desjardins A, Gromeier M, Herndon JE, Beaubier N, Bolognesi DP, Friedman AH, Friedman HS, McSherry F, Muscat AM, Nair S, Peters KB, Randazzo D, Sampson JH, et al. Recurrent Glioblastoma Treated with Recombinant Poliovirus. New England Journal of Medicine. 2018; 379: 150-61. [CrossRef]
- Fares J, Ahmed AU, Ulasov IV, Sonabend AM, Miska J, Lee-Chang C, Balyasnikova IV, Chandler JP, Portnow J, Tate MC, Kumthekar P, Lukas RV, Grimm SA, et al. Neural stem cell delivery of an oncolytic adenovirus in newly diagnosed malignant glioma: a first-in-human, phase 1, dose-escalation trial. Lancet Oncol. 2021; 22: 1103-14. [CrossRef]
- Forsyth P, Roldán G, George D, Wallace C, Palmer CA, Morris D, Cairncross G, Matthews MV, Markert J, Gillespie Y, Coffey M, Thompson B, Hamilton M. A phase I trial of intratumoral administration of reovirus in patients with histologically confirmed recurrent malignant gliomas. Mol Ther. 2008; 16: 627-32. [CrossRef]
- Freeman AI, Zakay-Rones Z, Gomori JM, Linetsky E, Rasooly L, Greenbaum E, Rozenman-Yair S, Panet A, Libson E, Irving CS, Galun E, Siegal T. Phase I/II trial of intravenous NDV-HUJ oncolytic virus in recurrent glioblastoma multiforme. Mol Ther. 2006; 13: 221-8. [CrossRef]
- Friedman GK, Johnston JM, Bag AK, Bernstock JD, Li R, Aban I, Kachurak K, Nan L, Kang KD, Totsch S, Schlappi C, Martin AM, Pastakia D, et al. Oncolytic HSV-1 G207 immunovirotherapy for pediatric high-grade gliomas. New England Journal of Medicine. 2021; 384: 1613-22. [CrossRef]
- Galanis E, Dooley KE, Keith Anderson S, Kurokawa CB, Carrero XW, Uhm JH, Federspiel MJ, Leontovich AA, Aderca I, Viker KB, Hammack JE, Marks RS, Robinson SI, et al. Carcinoembryonic antigen-expressing oncolytic measles virus derivative in recurrent glioblastoma: a phase 1 trial. Nature Communications. 2024; 15: 493. [CrossRef]
- Gállego Pérez-Larraya J, Garcia-Moure M, Labiano S, Patiño-García A, Dobbs J, Gonzalez-Huarriz M, Zalacain M, Marrodan L, Martinez-Velez N, Puigdelloses M, Laspidea V, Astigarraga I, Lopez-Ibor B, et al. Oncolytic DNX-2401 Virus for Pediatric Diffuse Intrinsic Pontine Glioma. N Engl J Med. 2022; 386: 2471-81. [CrossRef]
- Geletneky K, Hajda J, Angelova AL, Leuchs B, Capper D, Bartsch AJ, Neumann JO, Schöning T, Hüsing J, Beelte B, Kiprianova I, Roscher M, Bhat R, et al. Oncolytic H-1 Parvovirus Shows Safety and Signs of Immunogenic Activity in a First Phase I/IIa Glioblastoma Trial. Mol Ther. 2017; 25: 2620-34. [CrossRef]
- Kicielinski KP, Chiocca EA, Yu JS, Gill GM, Coffey M, Markert JM. Phase 1 clinical trial of intratumoral reovirus infusion for the treatment of recurrent malignant gliomas in adults. Mol Ther. 2014; 22: 1056-62. [CrossRef]
- Lang FF, Conrad C, Gomez-Manzano C, Yung WKA, Sawaya R, Weinberg JS, Prabhu SS, Rao G, Fuller GN, Aldape KD, Gumin J, Vence LM, Wistuba I, et al. Phase I Study of DNX-2401 (Delta-24-RGD) Oncolytic Adenovirus: Replication and Immunotherapeutic Effects in Recurrent Malignant Glioma. J Clin Oncol. 2018; 36: 1419-27. [CrossRef]
- Ling AL, Solomon IH, Landivar AM, Nakashima H, Woods JK, Santos A, Masud N, Fell G, Mo X, Yilmaz AS, Grant J, Zhang A, Bernstock JD, et al. Clinical trial links oncolytic immunoactivation to survival in glioblastoma. Nature. 2023; 623: 157-66. [CrossRef]
- Markert JM, Liechty PG, Wang W, Gaston S, Braz E, Karrasch M, Nabors LB, Markiewicz M, Lakeman AD, Palmer CA, Parker JN, Whitley RJ, Gillespie GY. Phase Ib trial of mutant herpes simplex virus G207 inoculated pre-and post-tumor resection for recurrent GBM. Molecular Therapy. 2009; 17: 199-207. [CrossRef]
- Markert JM, Medlock MD, Rabkin SD, Gillespie GY, Todo T, Hunter WD, Palmer CA, Feigenbaum F, Tornatore C, Tufaro F, Martuza RL. Conditionally replicating herpes simplex virus mutant, G207 for the treatment of malignant glioma: results of a phase I trial. Gene Therapy. 2000; 7: 867-74. [CrossRef]
- Markert JM, Razdan SN, Kuo HC, Cantor A, Knoll A, Karrasch M, Nabors LB, Markiewicz M, Agee BS, Coleman JM, Lakeman AD, Palmer CA, Parker JN, et al. A phase 1 trial of oncolytic HSV-1, G207, given in combination with radiation for recurrent GBM demonstrates safety and radiographic responses. Mol Ther. 2014; 22: 1048-55. [CrossRef]
- Samson A, Scott KJ, Taggart D, West EJ, Wilson E, Nuovo GJ, Thomson S, Corns R, Mathew RK, Fuller MJ, Kottke TJ, Thompson JM, Ilett EJ, et al. Intravenous delivery of oncolytic reovirus to brain tumor patients immunologically primes for subsequent checkpoint blockade. Science Translational Medicine. 2018; 10: eaam7577. [CrossRef]
- Thompson EM, Landi D, Brown MC, Friedman HS, McLendon R, Herndon JE, Buckley E, Bolognesi DP, Lipp E, Schroeder K, Becher OJ, Friedman AH, McKay Z, et al. Recombinant polio–rhinovirus immunotherapy for recurrent paediatric high-grade glioma: a phase 1b trial. The Lancet Child & Adolescent Health. 2023; 7: 471-8. [CrossRef]
- Todo T, Ino Y, Ohtsu H, Shibahara J, Tanaka M. A phase I/II study of triple-mutated oncolytic herpes virus G47∆ in patients with progressive glioblastoma. Nat Commun. 2022; 13: 4119. [CrossRef]
- van Putten EHP, Kleijn A, van Beusechem VW, Noske D, Lamers CHJ, de Goede AL, Idema S, Hoefnagel D, Kloezeman JJ, Fueyo J, Lang FF, Teunissen CE, Vernhout RM, et al. Convection Enhanced Delivery of the Oncolytic Adenovirus Delta24-RGD in Patients with Recurrent GBM: A Phase I Clinical Trial Including Correlative Studies. Clin Cancer Res. 2022; 28: 1572-85. [CrossRef]
- Todo T, Ito H, Ino Y, Ohtsu H, Ota Y, Shibahara J, Tanaka M. Intratumoral oncolytic herpes virus G47∆ for residual or recurrent glioblastoma: a phase 2 trial. Nat Med. 2022; 28: 1630-9. [CrossRef]
- Nassiri F, Patil V, Yefet LS, Singh O, Liu J, Dang RMA, Yamaguchi TN, Daras M, Cloughesy TF, Colman H, Kumthekar PU, Chen CC, Aiken R, et al. Oncolytic DNX-2401 virotherapy plus pembrolizumab in recurrent glioblastoma: a phase 1/2 trial. Nat Med. 2023; 29: 1370-8. [CrossRef]
- Marwah R, Xing D, Squire T, Soon YY, Gan HK, Ng SP. Reirradiation versus systemic therapy versus combination therapy for recurrent high-grade glioma: a systematic review and meta-analysis of survival and toxicity. J Neurooncol. 2023; 164: 505-24. [CrossRef]
- Ahmed R, Oborski MJ, Hwang M, Lieberman FS, Mountz JM. Malignant gliomas: current perspectives in diagnosis, treatment, and early response assessment using advanced quantitative imaging methods. Cancer Manag Res. 2014; 6: 149-70. [CrossRef]
- Zeng YF, Wei XY, Guo QH, Chen SY, Deng S, Liu ZZ, Gong ZC, Zeng WJ. The efficacy and safety of anti-PD-1/PD-L1 in treatment of glioma: a single-arm meta-analysis. Front Immunol. 2023; 14: 1168244. [CrossRef]
- Zhang X, Zhao L, Zhang H, Zhang Y, Ju H, Wang X, Ren H, Zhu X, Dong Y. The immunosuppressive microenvironment and immunotherapy in human glioblastoma. Front Immunol. 2022; 13: 1003651. [CrossRef]
- Liu J, Piranlioglu R, Ye F, Shu K, Lei T, Nakashima H. Immunosuppressive cells in oncolytic virotherapy for glioma: challenges and solutions. Front Cell Infect Microbiol. 2023; 13: 1141034. [CrossRef]
- Blitz SE, Kappel AD, Gessler FA, Klinger NV, Arnaout O, Lu Y, Peruzzi PP, Smith TR, Chiocca EA, Friedman GK, Bernstock JD. Tumor-Associated Macrophages/Microglia in Glioblastoma Oncolytic Virotherapy: A Double-Edged Sword. Int J Mol Sci. 2022; 23. [CrossRef]
- Liu X, Liu Y, Qi Y, Huang Y, Hu F, Dong F, Shu K, Lei T. Signal Pathways Involved in the Interaction Between Tumor-Associated Macrophages/TAMs and Glioblastoma Cells. Front Oncol. 2022; 12: 822085. [CrossRef]
- Mills CD, Kincaid K, Alt JM, Heilman MJ, Hill AM. M-1/M-2 macrophages and the Th1/Th2 paradigm. J Immunol. 2000; 164: 6166-73. [CrossRef]
- Bonapace L, Coissieux MM, Wyckoff J, Mertz KD, Varga Z, Junt T, Bentires-Alj M. Cessation of CCL2 inhibition accelerates breast cancer metastasis by promoting angiogenesis. Nature. 2014; 515: 130-3. [CrossRef]
- Denton NL, Chen CY, Scott TR, Cripe TP. Tumor-Associated Macrophages in Oncolytic Virotherapy: Friend or Foe? Biomedicines. 2016; 4. [CrossRef]
- Meisen WH, Wohleb ES, Jaime-Ramirez AC, Bolyard C, Yoo JY, Russell L, Hardcastle J, Dubin S, Muili K, Yu J, Caligiuri M, Godbout J, Kaur B. The Impact of Macrophage- and Microglia-Secreted TNFalpha on Oncolytic HSV-1 Therapy in the Glioblastoma Tumor Microenvironment. Clin Cancer Res. 2015; 21: 3274-85. [CrossRef]
- Valenzuela-Cardenas M, Gowan C, Dryja P, Bartee MY, Bartee E. TNF blockade enhances the efficacy of myxoma virus-based oncolytic virotherapy. J Immunother Cancer. 2022; 10. [CrossRef]
- Kyula JN, Khan AA, Mansfield D, Karapanagiotou EM, McLaughlin M, Roulstone V, Zaidi S, Pencavel T, Touchefeu Y, Seth R, Chen NG, Yu YA, Zhang Q, et al. Synergistic cytotoxicity of radiation and oncolytic Lister strain vaccinia in (V600D/E)BRAF mutant melanoma depends on JNK and TNF-alpha signaling. Oncogene. 2014; 33: 1700-12. [CrossRef]
- Weber L, Vieyres G. The Railmap of Type I Interferon Induction: Subcellular Network Plan and How Viruses Can Change Tracks. Cells. 2022; 11. [CrossRef]
- Bommareddy PK, Shettigar M, Kaufman HL. Integrating oncolytic viruses in combination cancer immunotherapy. Nat Rev Immunol. 2018; 18: 498-513. [CrossRef]
- Ferguson MS, Lemoine NR, Wang Y. Systemic delivery of oncolytic viruses: hopes and hurdles. Adv Virol. 2012; 2012: 805629. [CrossRef]
- Li L, Liu S, Han D, Tang B, Ma J. Delivery and Biosafety of Oncolytic Virotherapy. Front Oncol. 2020; 10: 475. [CrossRef]
- Chen L, Ma Z, Xu C, Xie Y, Ouyang D, Song S, Zhao X, Liu F. Progress in oncolytic viruses modified with nanomaterials for intravenous application. Cancer Biol Med. 2023; 20: 830-55. [CrossRef]
- Ahmed AU, Tyler MA, Thaci B, Alexiades NG, Han Y, Ulasov IV, Lesniak MS. A comparative study of neural and mesenchymal stem cell-based carriers for oncolytic adenovirus in a model of malignant glioma. Mol Pharm. 2011; 8: 1559-72. [CrossRef]
- Kim J, Zhu Y, Chen S, Wang D, Zhang S, Xia J, Li S, Qiu Q, Lee H, Wang J. Anti-glioma effect of ginseng-derived exosomes-like nanoparticles by active blood-brain-barrier penetration and tumor microenvironment modulation. J Nanobiotechnology. 2023; 21: 253. [CrossRef]
- Tseng YY, Chen TY, Liu SJ. Role of Polymeric Local Drug Delivery in Multimodal Treatment of Malignant Glioma: A Review. Int J Nanomedicine. 2021; 16: 4597-614. [CrossRef]
Figure 1.
The PRISMA flow chart of this meta-analysis.
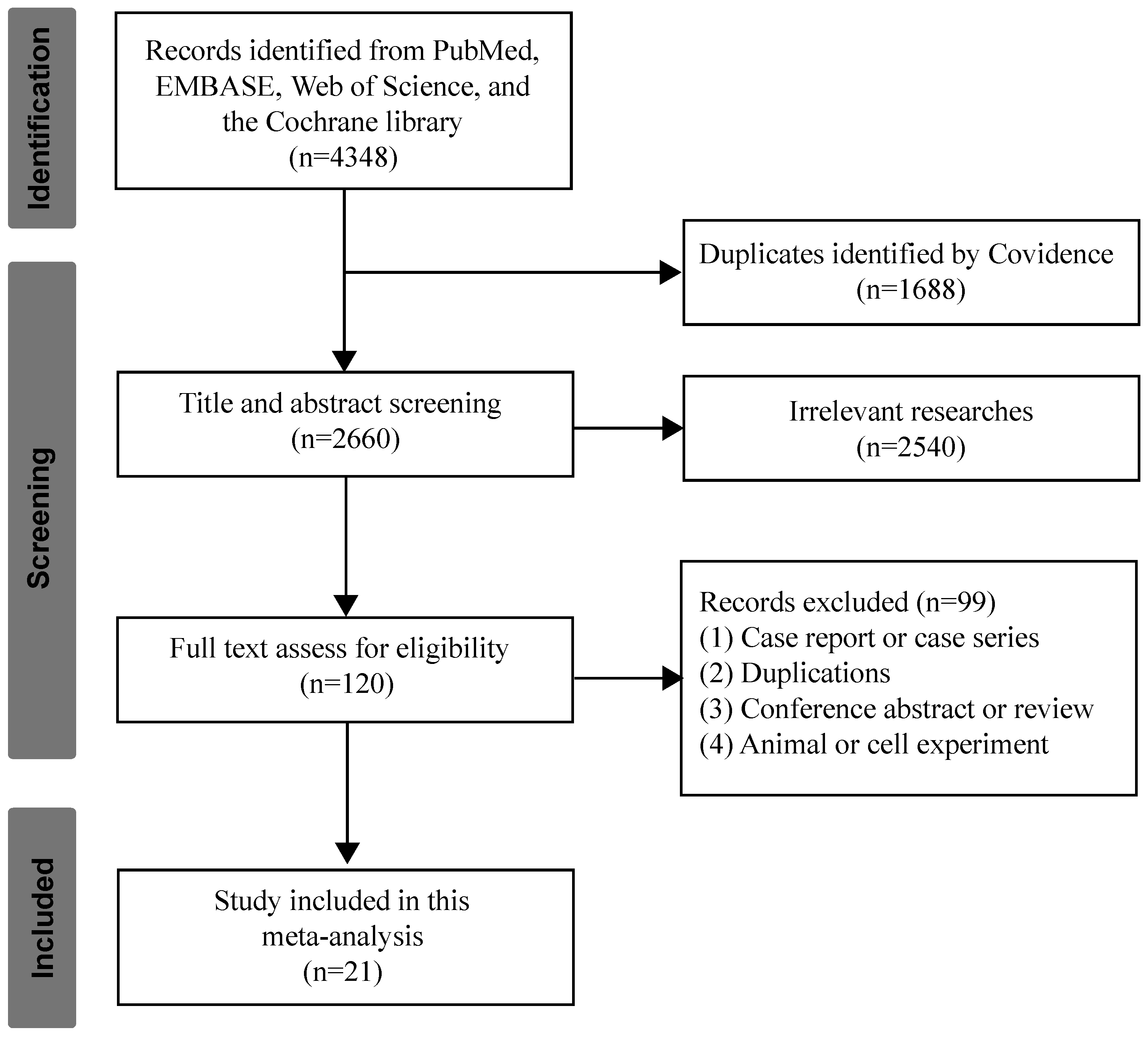
Figure 2.
Overall survival of OVs in treatment of glioma. (A) The pooled estimate of median OS. (B) sensitive analysis of median OS. (C) funnel plot of median OS.
Figure 2.
Overall survival of OVs in treatment of glioma. (A) The pooled estimate of median OS. (B) sensitive analysis of median OS. (C) funnel plot of median OS.
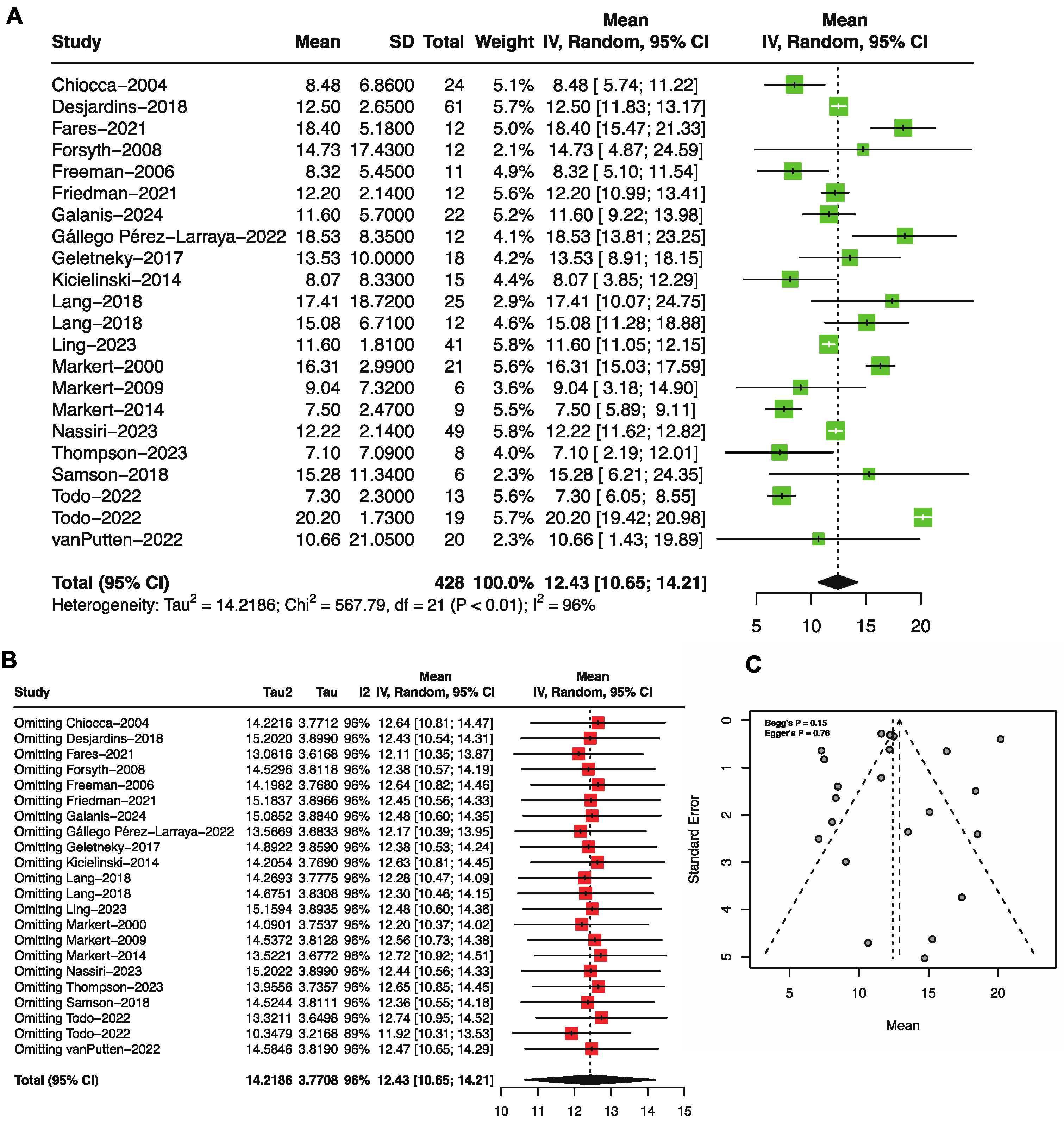
Figure 3.
Forest plot showing the (A) 1-year and (B) 2-year overall survival of glioma patients treated with OVs.
Figure 3.
Forest plot showing the (A) 1-year and (B) 2-year overall survival of glioma patients treated with OVs.
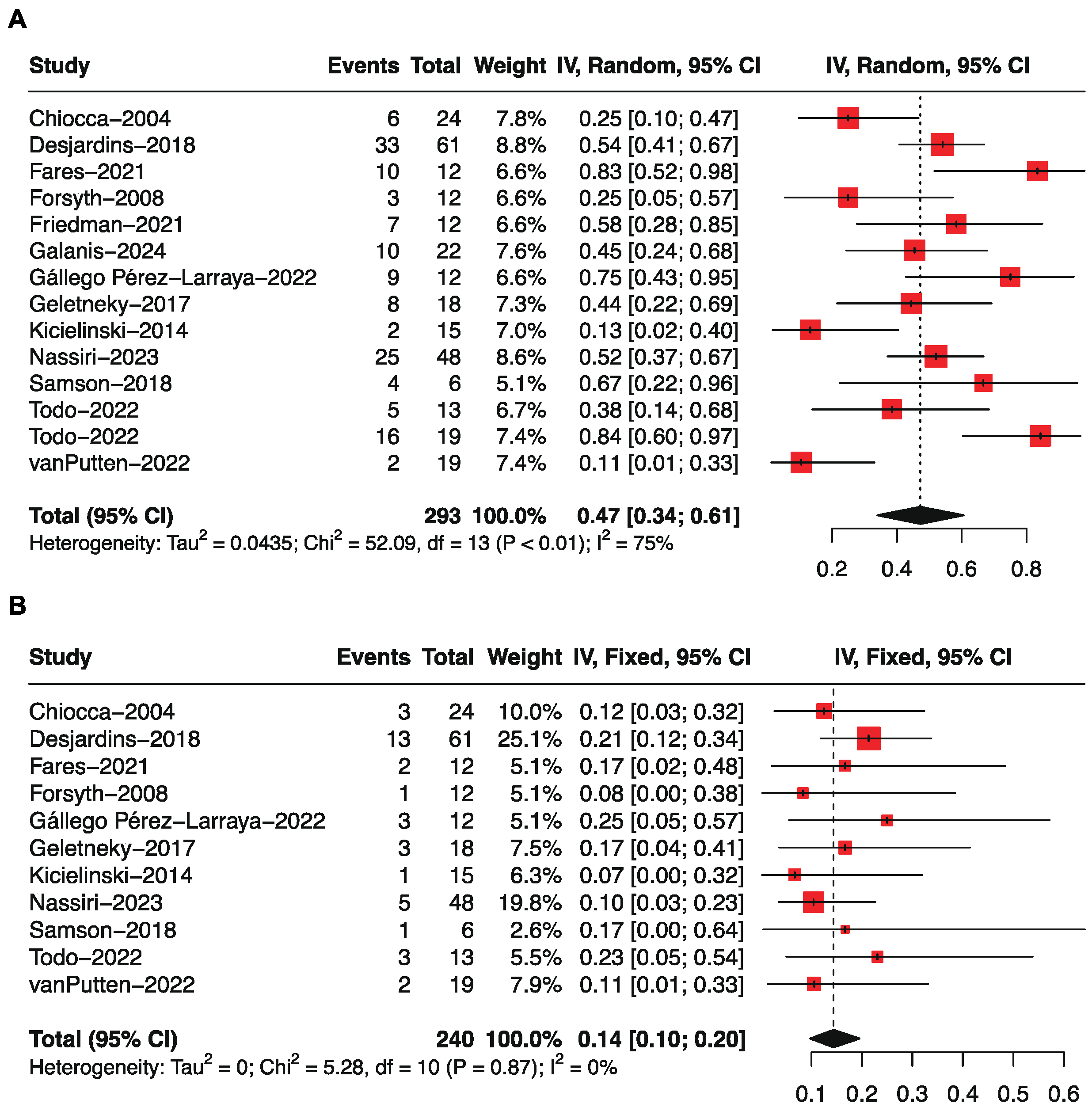
Figure 4.
Progression-free survival of OVs in treatment of glioma. (A) The pooled estimate of median PFS. (B) sensitive analysis of median PFS. (C) funnel plot of median PFS.
Figure 4.
Progression-free survival of OVs in treatment of glioma. (A) The pooled estimate of median PFS. (B) sensitive analysis of median PFS. (C) funnel plot of median PFS.
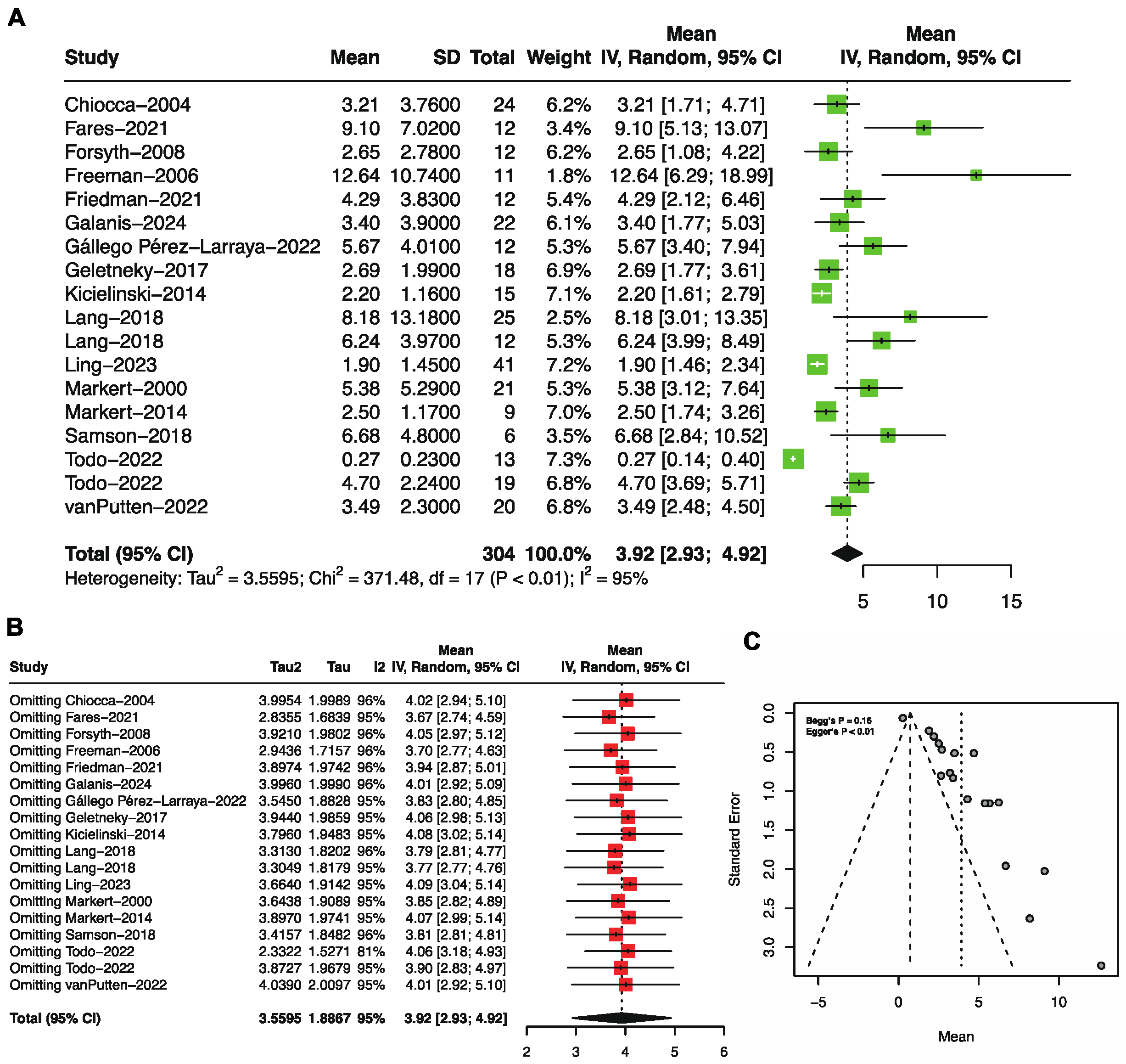
Figure 5.
Forest plot showing the 1-year progression-free survival of glioma patients treated with OVs.
Figure 5.
Forest plot showing the 1-year progression-free survival of glioma patients treated with OVs.
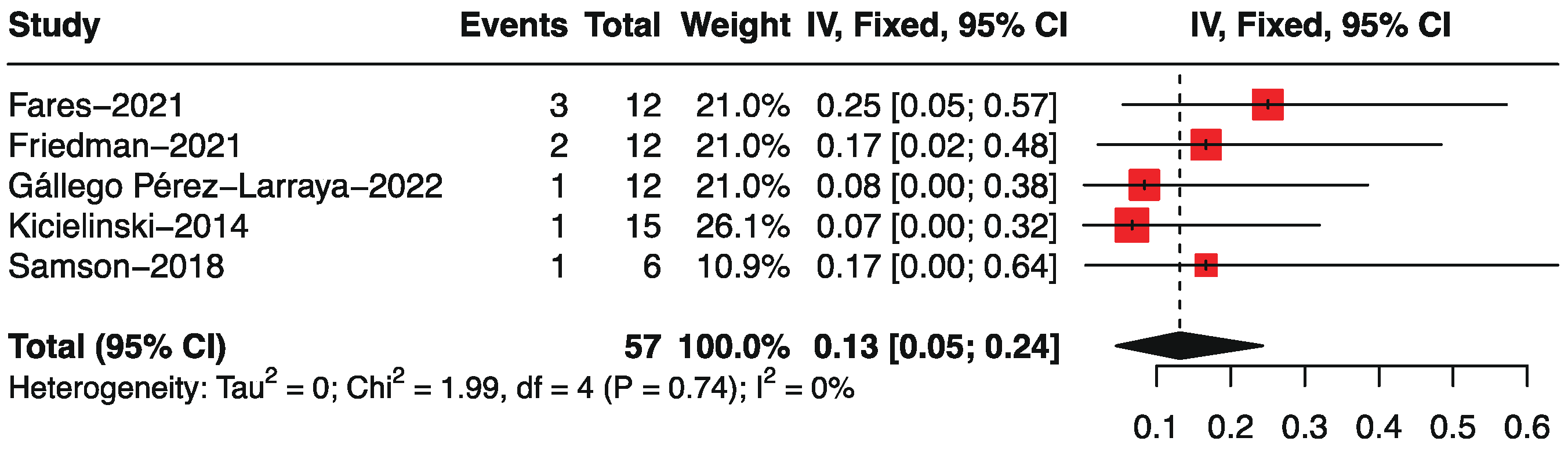
Figure 6.
Forest plot showing the objective response rate of glioma patients treated with OVs.3.5 The Safety of OVs in the Treatment of Gliomas.
Figure 6.
Forest plot showing the objective response rate of glioma patients treated with OVs.3.5 The Safety of OVs in the Treatment of Gliomas.
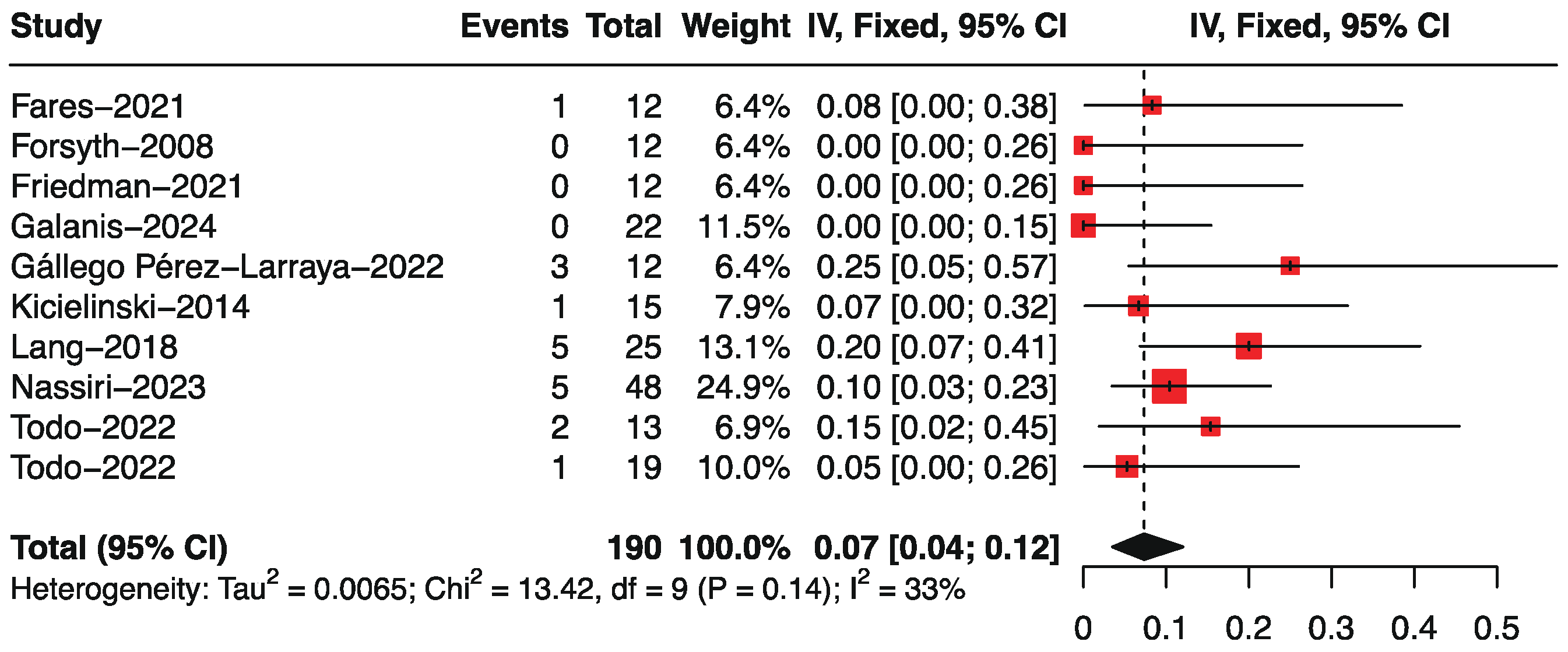
Figure 7.
Forest plot showing the AEs (A) and AEs > grade 3 (B) of glioma patients treated with OVs.
Figure 7.
Forest plot showing the AEs (A) and AEs > grade 3 (B) of glioma patients treated with OVs.
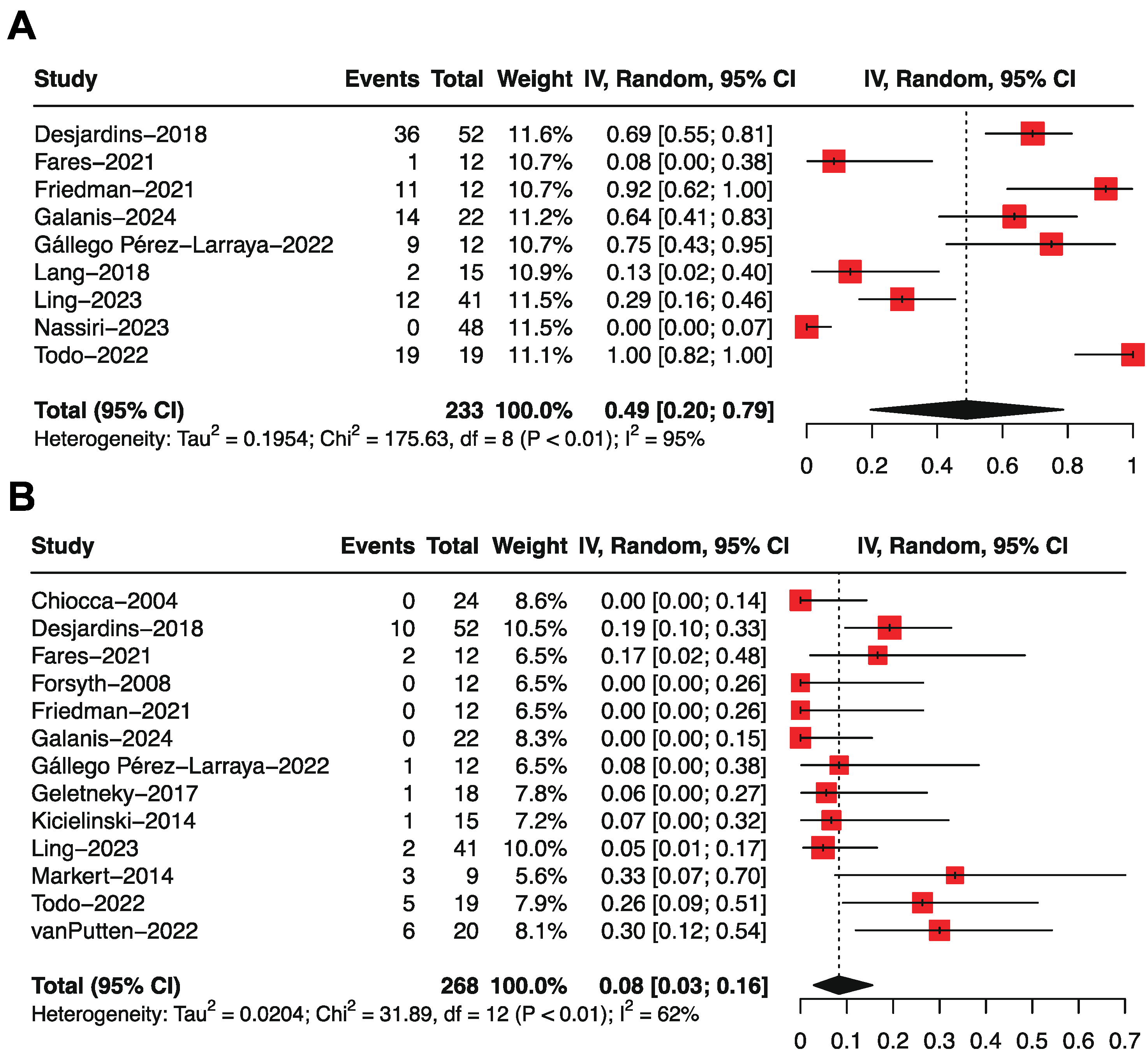

Table 1.
Baseline characteristic information of included research.
| Author | Year | Country | Study design | N (M/F) | Age | Diagnose | Viral family | Delivery | Dose (duration) | Previous treatment | End Points |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Chiocca [16] | 2004 | USA | Phase I | 24 (17/7) | 52 (35–70) |
AA, AO, or GBM (Recurrent) |
ONYX-015, E1B-attenuated adenovirus | I.T. | 10^7 pfu inoculated into theresected tumor cavity | S: 24 RT:24 CT:24 |
OS, PFS |
| Desjardins [17] | 2018 | USA | Phase II (NCT01491893) | 61 (25/36) | 55 (20–75) |
GBM (Recurrent) |
PVSRIPO, polio–rhinovirus chimera | I.T. | 10^7–10^10 (7 doses) |
S: 61 RT: 61 CT: 61 BEV: 61 |
OS |
| Fares [18] | 2021 | UK | Phase I (NCT03072134) | 12 (7/5) | 52 (48–65) |
AA or GBM (ND) |
NSC-CRAd-S-pk7, adenovirus | I.T. | Corhort 1: 6.25 × 10^10 VP, Corhort 2: 1.25 × 10^11 VP, Cohort 3: 1.875 × 10^11 VP (1 dose) |
S: 12 | OS, PFS, ORR |
| Forsyth [19] | 2008 | USA | Phase I | 12 (5/7) | 53.5 (40–61) |
AA, AO, or GBM (Recurrent) | Reovirus | I.T. | 72h infusion of 10^7, 10^8, or 10^9 TCID50 | S: 12 RT: 12 CT: 10 |
OS, PFS, ORR |
| Freeman [20] | 2006 | USA | Phase I/II | 11 (5/6) | 44.5 | GBM (Recurrent) |
NDV-HUJ, Newcastle disease virus | I.V. | Part 1: 0.1, 0.32, 0.93, 5.9, and 11 BIU; Part 2: 11 BIU |
S: 10 Biopsy: 4 RT: 14 CT: 12 |
OS, PFS |
| Friedman [21] | 2021 | USA | Phase I (NCT02457845) | 12 (6/6) | 13.4 (7-18) |
AA or GBM (Recurrent) |
G207, HSV-1 | I.T. | 10^7-10^8 PFU | S: 12 RT: 12 CT: 12 BEV: 3 |
OS, PFS, ORR |
| Galanis [22] | 2024 | USA | Phase I/II (NCT00390299) | 22 (11/11) | 53.5 (37.0-69.0) |
AA or GBM (Recurrent) | MV-CEA, carcinoembryonic antigen-expressing oncolytic measles virus | I.T. | 2×10^6-2×10^7 PFU | CT: 22 BEV: 5 | OS, PFS, ORR |
| Geletneky [24] | 2017 | USA | Phase I/IIa (NCT01301430) | 18 (4/14) | 57.8 ± 10.6 | GBM (Recurrent) |
ParvOryx, H-1 parvovirus (H-1PV) |
I.T. | Arm1: 5×10^9 pfu; Arm2: 1×10^9 pfu | S: 18 RT: 18 CT: 18 |
OS, PFS |
| Kicielinski [25] | 2014 | USA | Phase I | 15 (5/10) | 51.52 (26.2–76.3) |
GBM, GS, AA, anaplastic mixed glioma, or AO (Recurrent) |
REOLYSIN, Reovirus | I.T. | 1×10^8-1×10^10 pfu | S: 15 RT: 15 CT: 15 |
OS, PFS, ORR |
| Lang [26] | 2018 | USA | Phase I (NCT00805376) | group A: 25(10/15); group B: 12 (6/6) |
group A: 52 (21-62), group B: 49 (29-60) | GBM, GS, or AA (Recurrent) |
DNX-2401, adenovirus | I.T. | 1×10^7–3×10^10 VP (1 dose) | S: 25 RT: 37 CT: 36 |
OS, PFS, ORR |
| Ling [27] | 2023 | USA | Phase I (NCT03152318) | 41 | 56 (27-74) |
GBM or HGG (Recurrent) |
CAN-3110, HSV | I.T. | 10^6–10^10 PFU | S: 38 RT: 41 CT: 41 BEV: 30 |
OS, PFS |
| Markert [29] | 2000 | USA | Phase I | 21 (14/7) | 54.1 (38–72) |
AA or GBM (Recurrent or progressive) |
G207, HSV | I.T. | 10^6-3×10^9 pfu injected over 2 min in 5 operative locations | S: 17 Biopsy: 4 RT: 21 CT: 10 | OS, PFS |
| Markert [28] | 2009 | USA | Phase Ib (F05041106) | 6 (4/2) | 54.5 (39–65) |
GBM (Recurrent) |
G207, HSV | I.T. | 1.5 × 10^8 pfu (2 doses) | S: 6 RT: 6 CT: 5 |
OS |
| Markert [30] | 2014 | USA | Phase I (NCT00157703) | 9 (3/6) | 50.4 (37–60) |
AA or GBM (Recurrent) |
G207, HSV | I.T. | 1.0 × 10^9 pfu (1 dose) | S: 9 RT: 9 CT: 9 |
OS, PFS |
| Nassiri [36] | 2023 | Canada | Phase I/II (NCT02798406) | 49 (20/29) | 53 (26–73) | GBM or GS (Recurrent) |
DNX-2401, adenovirus | I.T. | 5 × 10^8, 5 × 10^9 and 5 × 10^10 VP | S: 4, RT: 49 CT: 49 BEV: 6 |
OS, ORR |
| Pérez-Larraya [23] | 2022 | USA | Phase Ia (NCT03178032) | 12 (7/5) | 9 (3-18) | DIPG (ND) |
DNX-2401, adenovirus | I.T. | 1×10^10 and 5×10^10 VP | / | OS, PFS, ORR |
| Samson [31] | 2018 | UK | Phase Ib (EudraCT: 2011-005635-10) |
6 | 62 (45-66) | HGG (Recurrent) |
REOLYSIN, Reovirus | I.V. | 1×10^10 single dose | S: 6 RT: 6 CT: 6 BEV: 1 |
OS, PFS |
| Thompson [32] | 2023 | USA | Phase Ib (NCT03043391) | 8 (3/5) | 16.5 (11–18) |
HGG (Recurrent) |
PVSRIPO | I.T. | 5 × 10^7 | CT: 8 BEV: 2 | OS |
| Todo [33] | 2022 | Japan | Phase I/II (UMIN000002661) | 13 (5/8) | 46 (35–76) |
GBM (Recurrent) |
G47Δ, HSV | I.T. | Cohort 1: 6 × 10^8 pfu, Corhort 2: 2 × 10^9 pfu | S: 13 RT: 13 CT: 13 |
OS, PFS, ORR |
| Todo [35] | 2022 | Japan | Phase II (UMIN000015995) | 19 (4/15) | 50.89 (25-73) |
GBM (Residual or recurrent) |
G47Δ, HSV | I.T. | 1 × 10^9 pfu per dose (up to six doses) | S: 19 RT: 19 CT: 19 BEV: 7 |
OS, PFS, ORR |
| van Putten [34] | 2022 | USA | Phase I | 20 (8/12) | 53.5 (29–69) |
GBM (Recurrent) |
Delta24-RGD, adenovirus | I.T. | 10^7–1×10^11 VP | S: 19 RT: 20 CT: 19 BEV: 6 |
OS, PFS |
Notes: ND, newly diagnosed; I.T., intratumoral administration; I.V., intravenous administration; ADV, adenovirus; HSV, herpes simplex virus; NDV, newcastle disease virus. HGG, high-grade glioma; GBM, glioblastomas; AA, astrocytomas; AO, anaplastic oligodendroglioma; DIPG, diffuse intrinsic pontine glioma; GS, gliosarcoma; S, Surgery; RT, radiation therapy; CT, chemotherapy; BEV, bevacizumab; OS, overall survival; PFS, progression-free survival; ORR, objective response rate.
Table 2.
Subgroup analysis of pooled estimates of the median overall survival.
| Subgroup | No. of studies | Mean, months | 95% CI | P value between subgroups | heterogeneity within subgroups | |
|---|---|---|---|---|---|---|
| I2 (%) | P value | |||||
| Study Phase | 0.21 | |||||
| Phase I | 15 | 12.50 | 10.31, 14.70 | 88 | < 0.01 | |
| Phase I/II | 2 | 10.40 | 8.07, 12.74 | 100 | < 0.01 | |
| Phase II | 5 | 16.35 | 8.80, 23.89 | 100 | < 0.01 | |
| Diagnose | < 0.01 | |||||
| ND | 2 | 18.44 | 15.95, 20.93 | 0 | 0.96 | |
| Recurrent | 20 | 11.82 | 10.07, 13.57 | 97 | < 0.01 | |
| Administration | 0.53 | |||||
| I.T. | 20 | 12.57 | 10.71, 14.44 | 97 | < 0.01 | |
| I.V. | 2 | 10.45 | 4.16, 16.74 | 50 | 0.16 | |
| Viral family | 0.25 | |||||
| ADV | 7 | 14.31 | 11.17, 17.45 | 83 | < 0.01 | |
| HSV | 7 | 12.16 | 8.53, 15.79 | 99 | < 0.01 | |
| Reovirus | 3 | 11.27 | 5.91, 16.63 | 33 | 0.22 | |
| Poliovirus | 2 | 10.37 | 5.20, 15.54 | 78 | 0.03 | |
| NDV | 1 | 8.32 | 5.10, 11.54 | / | / | |
| Measles virus | 1 | 11.60 | 9.22, 13.98 | / | / | |
| Parvovirus | 1 | 13.5 | 8.91, 18.15 | / | / | |
Notes: ND, newly diagnosed; I.T., intratumoral administration; I.V., intravenous administration; ADV, adenovirus; HSV, herpes simplex virus; NDV, newcastle disease virus.
Table 3.
Subgroup analysis of pooled estimates of the median progression-free survival.
| Subgroup | No. of studies | Mean, months | 95% CI | P value between subgroups | heterogeneity within subgroups | |
|---|---|---|---|---|---|---|
| I2 (%) | P value | |||||
| Study Phase | 0.68 | |||||
| Phase I | 13 | 4.06 | 3.01, 5.12 | 80 | < 0.01 | |
| Phase I/II | 4 | 3.91 | 0.30, 8.12 | 94 | < 0.01 | |
| Phase II | 1 | 4.70 | 3.69, 5.71 | 95 | < 0.01 | |
| Diagnose | 0.05 | |||||
| ND | 2 | 6.98 | 3.71, 10.25 | 54 | 0.14 | |
| Recurrent | 16 | 3.54 | 2.61, 4.47 | 96 | < 0.01 | |
| Administration | 0.06 | |||||
| I.T. | 16 | 3.59 | 2.66, 4.51 | 96 | < 0.01 | |
| I.V. | 2 | 9.10 | 3.36, 14.84 | 60 | 0.12 | |
| Viral family | 0.25 | |||||
| ADV | 6 | 5.30 | 3.56, 7.05 | 70 | < 0.01 | |
| HSV | 6 | 2.99 | 1.42, 4.56 | 97 | < 0.01 | |
| Reovirus | 3 | 2.98 | 1.33, 4.63 | 62 | 0.07 | |
| NDV | 1 | 12.64 | 6.29, 18.99 | / | / | |
| Measles virus | 1 | 3.40 | 1.77, 5.03 | / | / | |
| Parvovirus | 1 | 2.69 | 1.77, 3.61 | / | / | |
Notes: ND, newly diagnosed; I.T., intratumoral administration; I.V., intravenous administration; ADV, adenovirus; HSV, herpes simplex virus; NDV, newcastle disease virus.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



