
Submitted:
15 September 2024
Posted:
17 September 2024
You are already at the latest version
Abstract
Anticholinergic burden (ACB) from medications has been associated with adverse outcomes in older people. Aim: To conduct a non-randomised feasibility study of an intervention to Reduce anticholinerGic burdEN in oldER pATiEnts (REGENERATE) to inform a subsequent definitive trial. Methods: The development and evaluation of an ACB reduction intervention was guided by the Medical Research Council framework. Findings from preliminary studies, two systematic reviews and two qualitative studies informed the design of a mixed-method feasibility study. The study was conducted in one UK primary care site. The clinical pharmacist identified and invited potentially eligible patients, reviewed their medications and made recommendations to reduce the ACB as needed. Patients completed surveys at baseline, and 6- and 12- weeks post intervention. A purposive sample of patients and healthcare professionals was interviewed. Results: There was an 16/20 response; 14/16 attended the pharmacist led consultation and completed the baseline questionnaire and 13/14 completed both follow-up questionnaire. The sustainability of deprescribing was confirmed. The results suggest the potential of the intervention to reduce side effects from medications and improve quality of life (EQ-5D-5L). The interviews showed patients were happy with the study processes, and the medication changes, and were satisfied with the pharmacist’s consultation. Conclusions: This feasibility study demonstrated that a deprescribing/reducing ACB intervention in older people is feasible in a primary care setting and may benefit patients. Well-designed RCTs and cost-effectiveness studies should be undertaken to confirm the benefits of ACB deprescribing in primary care settings. Trial registration: ClinicalTrials.gov no. NCT04660838
Keywords:
Anticholinergic burden
; Deprescribing
; Feasibility study
1. Introduction
The population is ageing which is associated with gradual decrease in physical and mental health coupled with a growing risk of disease and multi-morbidity [1]. Hence, polypharmacy in older people is common, leading to more side effects from medicines and drug interactions [2]. Medications with anticholinergic properties are commonly prescribed in older adults for a wide variety of common clinical conditions including Parkinson’s disease, depression, chronic obstructive pulmonary disease, urinary incontinence, and allergic rhinitis [3,4,5]. Their use is steadily increasing with estimates varying from 37% to 63% of the population depending on the clinical setting [6,7,8].
Anticholinergic medicines, as their name implies, block acetylcholine neurotransmission [9]. The term “anticholinergic burden” or “ACB” refers to the cumulative anticholinergic action resulting from the concomitant use of one or more anticholinergic medicines. A growing body of evidence suggests that a high anticholinergic burden (ACB) is linked to adverse outcomes such as poor physical functioning, dementia, falls, and mortality in older people [10]. There is limited published research on the clinical effectiveness of interventions to reduce ACB [11].
Deprescribing is the process of medication withdrawal or dose reduction to correct or prevent medication-related complications, improve outcomes, and reduce costs [12]. Both general deprescribing and ACB drug deprescribing have the goal of reducing medication burden, risk of falls, hospitalisation and death and improving and/or preserving cognitive function [13,14]. Whilst there is a growing body of evidence for the benefit of, and optimum approaches to, deprescribing in general there have been no definitive trials of its value when focused on ACB drugs. To address this gap in research, a feasibility study was developed and evaluated following the Medical Research Council framework for complex interventions [15]. The preliminary work involved a quantitative systematic review [11], a qualitative systematic review [16], and qualitative interviews with patients and health care professionals [17]. The findings of these preliminary studies were combined into a logic model (Supplemental material 1) which informed the design of a mixed-method feasibility study to investigate remaining areas of uncertainty that needed to be resolved prior to conducting a definitive randomized controlled trial.
To conduct a non-randomised feasibility study of an intervention to Reduce anticholinerGic burdEN in oldER pATiEnts (REGENERATE) to inform a subsequent definitve trial.
2. Materials and Methods
This single-arm, non-randomised feasibility study was conducted in one primary care setting (GP practice) in the Grampian Health Board area, Scotland UK, with a registered population of 8,231 people. The study was conducted from July 2021 to February 2022. The trial was registered on ClinicalTrials.gov no. NCT04660838 and was approved by the North of Scotland Research Ethics committee and Grampian Research and Development.
The primary objectives were to test processes of patient participant identification, to assess recruitment and retention rates of patient participants, and to review potential outcome measures and data collection processes. The secondary objective was to explore the acceptability of the intervention to patients and healthcare professionals.
Participant Inclusion Criteria, Identification, and Recruitment:
Patients were eligible for inclusion if they were: 65 years, on one or more long-term drugs (prescribed for a minimum of 6 weeks) with ACB potential (ACoB scale ≥3; defined according to Boustani et al. [18]) and able to provide informed consent. The exclusion criteria were: patients with severe mental illness (such as diagnosis of severe anxiety, severe depression, severe dementia etc.), terminally ill (life expectancy less than 6 months), or in the opinion of a responsible clinician were not suitable for participation, or were taking part in another similar study.
The study site was identified through personal networks. The pharmacist initially applied a computer search to a sample of 200 patients, randomly selected from the practice records, to identify those 65 years and having an Anticholinergic Cognitive Burden scale ≥3. A pharmacist and GP screened the list of those potentially eligible against the full inclusion and exclusion criteria and maintained a log of exclusions with reasons. From the list of those eligible, the pharmacist approached blocks of 20, initally by phone to explain the study, then mailing an invitation pack from the GP practice (signed by the delegated primary care pharmacist). A stamped addressed envelope was included for returning an Expression of Interest form to the research team. The main researcher AN phoned the patients to give them an opportunity to ask questions and took their verbal recorded informed consent. The names and IDs (assigned for each individual patient) of those agreeing to take part were forwarded to the primary care pharmacist (see below). There was a target recruitment of 10 patients and patients were approached in successive groups of 20 until the target was achieved.
The ACB Reduction Intervention
The primary care pharmacist undertook refresher training on ACB, and an introduction to the study processes through video recorded talks, watched at a time convenient to themself. The pharmacist reviewed the medication record of each participating patient and agreed a time and date for a telephone consultation, during which the pharmacist discussed the need to deprescribe or switch a drug to reduce the ACB. The pharmacist, a qualified Independent Prescriber, implemented the agreed change, updated the patient’s medical record and completed a pharmaceutical care plan (PCP) (based on one used in a previous study (https://sites.uea.ac.uk/chipps). The patient was advised about any new medications that they had been prescribed, and informed about potential side effects.
No second consultation with the pharmacist or GP was routinely scheduled. Patients were asked to contact their pharmacist/clinician/GP if they had any subsequent changes in symptoms or were experiencing any unwanted side effects. The GP and the study team were then notified of any symptoms or medication changes by the pharmacist who also updated the PCP. Patients were advised that in an emergency they could contact the Chief Investigator (PKM) a medical consultant in Care of the Elderly.
Data Collection and Management:
Response, recruitment, and retention: The responsible clinician (or authorised depute) was asked to complete a standard form recording the total number of patients for whom they were responsible, the numbers identified as potentially eligible from the random sample of 200, the numbers excluded on screening and reasons, and the numbers invited with dates. Patients were identified by a unique identification (ID) number.
AN kept a record using a study log of the numbers invited, the numbers expressing interest, the numbers giving informed consent, the numbers attending the first consultation, the numbers providing baseline data, and the numbers providing follow-up data.
Pharmaceutical Care Plans-Medication changes recommended, implemented and sustained The PCP included details of the recommended changes and their implementation for each patient. PCPs were anonymised by the pharmacist prior to sending to the lead researcher (AN) at the end of the study period for data entry and analysis. Medication changes were categorised by drug groups (therapeutic class) and process measure (such as stop drug, change drug, reduce dose etc.). Sustainability of changes was assessed.
Patient survey: A questionnaire was developed and sent to the patients by post at baseline (immediately after the first consultation), 6 weeks and 12 weeks (Supplemental material 2). The baseline version included demographic data, consultation time, patients’ views on the intervention, and acceptability of intervention assessed by a Likert rating scale (5; strongly agree, 4; agree, 3; uncertain/not applicable, 2; disagree and 1; strongly disagree). Quality of life (QOL) was measured by EQ-5D-5L (Supplemental material 2 in section 5). There wase also an open text response option in each section of the questionnaire for participants to add any further relevant information. At 6 and 12 weeks the questionnaires asked about their views of the intervention, any subsequent medication changes, their quality of life and their views on the study processes (12 weeks only). Questionnaires were identified by ID number only. Patients were asked to complete and return the questionnaires to the CI, PKM, by pre-paid addressed envelope, who forwarded them to the lead researcher AN. Telephone calls were made to remind patients if the questionnaire had not been returned within 2 weeks.
Participant interviews: Semi-structured interviews were conducted with a purposive sample of patients (different age, gender, and type of ACB medication changes) with a target sample size of five to fit within existing resource and likely response rate. The primary care pharmacist and linked practice doctor were also invited to take part in an interview. AN contacted the interested participants to arrange a suitable date and time for interviews. The interviews were conducted virtually according to COVID-19 restrictions at the time, using phone or video calls.
An interview topic guide was developed specifically for each participant group (Supplemental material 3). The interviews were digitally recorded and transcribed verbatim either by AN or a University of Aberdeen approved external transcription company (NJC Secretarial).
Adverse Event and Adverse Reaction reporting procedure: Patients were asked to self-report any new or unexpected symptoms to their pharmacist/GP who reviewed these and made changes to the prescribed medications and/or advised the patient where necessary. The pharmacist/GP then reported the event to the research team, (and if initially reported to the pharmacist, to the GP), and the yellow card scheme (if necessary). AN and PKM assessed each event for seriousness (adverse event, adverse reaction, serious adverse event, serious adverse reaction), likely causality and whether expected or unexpected.
Sample size, data management and analysis: Recognising the high pharmacy staff workload during and after the COVID pandemic the pharmacist was asked to recruit a minimum of ten patient participants. This was a pragmatic decision based on balancing pharmacist capacity with a sample sufficient to address the study objectives. Data from the questionnaire surveys were entered into an SPSS V.27 spreadsheet by AN. Simple descriptive statistics were conducted for quantitative data. There was an initial plan to analyse open text responses thematically but due to limited resource and few responses these are not reported here. Interview data were transcribed and checked against the recording. Thematic analysis was used to generate themes and subthemes.
3. Results
Patient Identification, Recruitment and Retention
From 200 patients screened, 41 potential participants were identified as potentially eligibible. Afte further screening, nine patients were excluded due to severe mental illness or hearing difficulties. From the remaining 32, twenty patients were invited to take part in the study; four did not respond to the invitation and two declined to participate (one had problems with understanding the study processes; one was due to have an operation during the study period). Fourteen patients gave formal consent and attended the consultation with a primary care pharmacist. One patient was excluded due to an unsuccessful previous attempt to switch medication. Thirteen baseline, 6 weeks and 12 weeks follow up questionnaires were sent to patients and all of them were returned to the research team within two weeks. The number of patients in each step is presented in the CONSORT flow diagram (Figure 1). The response rate of participants was 16 of 20, recruitment rate was 14 of 20 and retention rate was 13 of 14.
Participant Demography, Outcomes and Experiences of Intervention
Most patients were male (n= 8/13); median (IQR) age was 72 years (68.5- 75.5). The mean (SD) number of medications was 7.62 (3.18) and patients had an Anticholinergic Cognitive Burden (ACoB) score of 3, 4 or 6 (Table 1). Patient views on the acceptability of the intervention as assessed by the Likert responses are presented (Table 2). All participants answered all questions, and all responses had face validity, confirming this data collection method was acceptable and feasible. All patients thought the duration of the consultation was appropriate, and they were happy with the pharmacist’s consultation and medication review. The ACB medication changes for individual patients are summarised (Table 3); most of medication changes involved a switch. At three months one patient had reverted to their original medication and two patients were on a combination of the new medicine and occasional low dose of original medication. The QOL as measured by EQ-5D-5L at baseline, 6 weeks and 12 weeks is shown (Table 4). Overall scores show few problems. The respondents reported lowest scores for self-care and highest in pain/discomfort but differences are small. The utility of EQ-5D-5L was calculated by the utility equation by taking the utility score of 1 (complete health) and subtracting the coefficients of the 5 dimensions. The values of EQ-5D-5L utility [median (IQR)] are 0.592 (-0.515, 0.859), 0.667 (-0.402, -1.411) and 0.655 (-1.411, 1.000) at baseline, six weeks and 12 weeks follow up, respectively.
Most patients were happy to be randomised in a future study. Six interviews were conducted with five patients and one primary care pharmacist. One GP could not take part in an interview but provided written responses to the question by email. The themes and subthemes are shown (Table 5) illustrated by verbatim quotes identified by participant ID, gender, and age. Overall patients suggested the study processes were acceptable. They were happy about the medication changes, satisfied with the pharmacist consultation, and some reported reduced side effects compared before the medication change.

Table 3.
Summary of individual patient ACB medication changes recorded in the Pharmaceutical Care Plan at baseline, 6 and 12 weeks.
Table 3.
Summary of individual patient ACB medication changes recorded in the Pharmaceutical Care Plan at baseline, 6 and 12 weeks.
| Participant ID | Gender |
Age (years) |
ACoB score Baseline |
ACoB score 6 weeks |
ACoB score 12 weeks |
Old treatment | New treatment | Sustainability |
| P1 | Male | 72 | 3 | 0 | 0 | Amitriptyline 25mg tablets one at night | Pregabalin 50mg capsules one three times daily | Patient remained on new medication |
| P2 | Male | 75 | 3 | 0 | 0 | Hydroxyzine hydrochloride 10mg tablets one at night | Fexofenadine 180mg tablets one at night and added an emollient-Zerobase to see if helps itch | Patient remained on new medication |
| P3 | Male | 73 | 3 | 0 | 0 | Tolterodine 2mg capsules one daily | Mirabegron 25mg tablets one daily | No improvement on 25mg dose so increased to 50mg and then remained on new medication |
| P4 | Female | 69 | 3 | 0 | 0 | Solifenacin 5mg tablets one daily | Mirabegron tablets 50mg one daily | Patient remained on new medication |
| P5 | Male | 77 | 3 | 0 | 0 | Chlorphenamine 4mg tablets | Fexofenadine 180mg tablets one daily | Patient remained on new medication |
| Participant ID | Gender |
Age (years) |
ACoB score Baseline |
ACoB score 6 weeks |
ACoB score 12 weeks |
Old treatment | New treatment | Sustainability |
| P7 | Male | 67 | 6 | 1 | 1 | Cetirizine 10mg tablets Amitriptyline 10mg tablets |
Fexofenadine 180mg tablets one daily Pregabalin capsules 75mg one twice daily |
Patient remained on new medication but with pregabalin increased to 150mg twice daily |
| P8 | Female | 70 | 4 | 1 | 1 | Amitriptyline 10mg tablets three at night Co-codamol 30/500 tablets |
Reduce dosage to 20mg over the next 2 weeks with a view to stopping altogether Naproxen 500mg tablets one twice daily |
The patient has stopped completely with no adverse effects The patient was managing with naproxen but due to struggling to sleep at night started taking occasional co-codamol |
| Participant ID | Gender |
Age (years) |
ACoB score Baseline |
ACoB score 6 weeks |
ACoB score 12 weeks |
Old treatment | New treatment | Sustainability |
| P9 | Male | 68 | 6 | 3 | 3 | Chlorphenamine 4mg tablets one three times daily Cetirizine 10mg tablets once daily Amitriptyline 10mg one at night |
All previous medications stopped. Replaced by fexofenadine 180mg tablets once daily | The patient was still not sleeping well. -chlorphenamine 4mg tablets once at night added back Otherwise, patient remained on new medication with no adverse effects |
| Participant ID | Gender |
Age (years) |
ACoB score Baseline |
ACoB score 6 weeks |
ACoB score 12 weeks |
Old treatment | New treatment | Sustainability |
| P10 | Male | 76 | 6 | 1 | 4 | Solifenacin 5mg tablets Nefopam 30mg tablets Co-codamol 30/500mg tablets |
Mirabegron 50mg one daily Reduce dose of nefopam if able and replace with increasing dose of co-codamol, to a regular four times daily as opposed to when required |
Mirabegron did not help urinary urgency at all. Stopped and reverted back to solifenacin but higher dose Patient stopped taking nefopam completely after increase in dosage of co-codamol |
| P11 | Female | 66 | 6 | 0 | 0 | Hyoscine butylbromide 10mg tablets Hydroxyzine 10mg tablets |
Mebeverine 135mg tablets one three times daily Peppermint oil capsules 0.2ml one three times daily Fexofenadine 180mg tablets one daily |
Patient remained on new medication |
| Participant ID | Gender |
Age (years) |
ACoB score Baseline |
ACoB score 6 weeks |
ACoB score 12 weeks |
Old treatment | New treatment | Sustainability |
| P12 | Male | 71 | 3 | 3 | 3 | Amitriptyline 50mg tablets | Amitriptyline 30mg tablets Mirtazapine 15mg tablets |
Currently taking 35mg amitriptyline as at lower dose sleep was disturbed Patient remained on new medication |
| P13 | Female | 75 | 6 | 0 | 0 | Solifenacin 5mg tablets Dicycloverine 10mg tablets |
Mirabegron 50mg tablets Peppermint capsules /mebeverine 135mg tablets |
The patient remained on the new medication |
| P14 | Male | 79 | 3 | 0 | 0 | Solifenacin 5mg tablets two times daily | Mirabegron 50mg tablets | The patient remained on new medication |
Note: ACoB = Anticholinergic Cognitive Burden.
Table 4.
Patient participant EQ-5D-5L scores* at baseline, 6 weeks and 12 weeks N=13.
| Items | Baseline (median; IQR) |
6 weeks follow up (median; IQR) |
12 weeks follow up (median; IQR) |
|---|---|---|---|
| Problems in mobility | 2 (1, 3) | 2 (1, 2.75) | 1.50 (1, 3.25) |
| Problems in self-care | 1 (1, 1) | 1 (1, 1) | 1 (1, 1.5) |
| Problems in usually activities | 2 (2, 2.50) | 1 (1, 2.75) | 1 (1, 3.25) |
| Pain/Discomfort | 2 (1.50, 3.50) | 2 (1, 3) | 2 (1, 3.25) |
| Anxiety/Depression | 1 (1, 2) | 2 (1, 2) | 1 (1, 2) |
* 1 = No, 2 = Mild, 3 = Moderate, 4 = Severe, 5 = Very Severe
Table 5.
Summary of patient participant interviews: Themes and sub-themes.
| Themes | Subthemes/exemplar quotes |
|---|---|
| Remembering the purpose of the study | Patients remembered the purpose of the study, i.e., was involved in medication changes in people aged 65 year and over to new medication to reduce side effects and improve quality of life. It was about trying to find out whether the medication that was routinely given to elderly people was still doing the best job. [P8, female,70y] Well, it was about my medication and I got my medication changed, that’s what it was about. [P4, female, 70y] |
| Process of the study |
What went well: Many patients suggested the process of study went well. They were happy about the medication changes and satisfied with the pharmacist consultation. They kept in touch with the pharmacist when they needed further help or had problems about medication usage. Well, it’s fine, I’m on new medication and it seems to be working out fine. The pharmacy has been in touch with me a couple of times and all’s well. [P4, female, 69y] Maybe … yes, just consultation or just touching base with the pharmacist, the pharmacist was good, and she did keep in touch but probably it would’ve been better to keep in touch just a little bit more, I think. But equally well I could have contacted her, she was available to be contacted so it wasn’t really a problem. [P8, female, 70y] The pharmacist noted that patients were happy with the information pack that explained them clearly and also additional telephone call from the pharmacist. The ones we picked were very positive about it, they were very interested. They appreciated the pack that you sent out with all that information which explained everything to them very clearly, although I had gone over very quickly the basics on the telephone. The fact that it was anonymous was good, they liked that idea. [Primary care pharmacist] The pharmacist was happy to conduct the research in her role. Patients felt positive about pharmacists’ involvement in this type of study. GP also valued the pharmacist’s opinion as he was not required to provide further input towards the plan and no patients complaint about the changes or anything else. It was very good, I enjoyed doing it. The patients were very positive,…[Primary care pharmacist] Pharmacist team manage this, and I was not involved as they found no issues requiring GP input [GP] |
|
What did not go so well: A few patients were excluded from the study because they were waiting for hospital admissions for procedures and pharmacist felt that timing was not right to make any changes due to their upcoming appointments. One or two of them I think we decided weren’t eligible because of the other drugs they were on, or they were awaiting a procedure at the hospital, and we didn’t want to change anything before they went on for that. That was quite a valid criticism. It’s just circumstances really. [Primary care pharmacist] The pharmacist suggested the monitoring paperwork was burdensome due to time consuming process and did not really fit to routine practice. She felt that six weeks is too long to monitor patients following medication changes. I think part of your paperwork it said three months review, six weeks review; those didn’t really fit what I was doing. Six weeks was too long to leave them, I was phoning them maybe two weeks, three weeks, or they were phoning me and saying it wasn’t going well. A shorter timeline for the initial review would be better. [Primary care pharmacist] | |
|
Difficulties in taking part in the study: One patient thought the questionnaires were quite repetitive due to similar questions asked in each follow-up time. It could be that he misunderstood the quality-of-life monitoring in the long period. However, Others suggested no difficulties in taking part in the study at all. Actually, found the questionnaires that you sent were quite repetitive. You were asking the same information. That’s really about all, you know, I can say. I filled in several questionnaires, and I seemed to be answering the same questions. [P2, Male, 75y] Not physically or anything. No, I was … as far as I can remember there were no difficulties in it at all. [P7, male, 67y] | |
| Patient-related outcomes |
General satisfaction and well being In general, patients were satisfied with the pharmacist consultation and were happy with medication changes that reduced their side effects of the medication. Well, it’s fine, I’m on new medication and it seems to be working out fine. The pharmacy has been in touch with me a couple of times and all’s well. [P4, female, 69y] When we first changed from my medication in the beginning, it was fine in that it helped me to sleep better, which was one of my big problems. After a while, the benefits seemed to wear off a bit and then my medication as changed again, which now suits me much better in all directions. It helps me to sleep better and it … yeah, yeah, the side effects, the constipation side effects if you like have gone. So that’s fine. [P8, female, 70y] |
|
Symptom control and side effects: Overall symptoms could be controlled better after medication changes. Patients were happy with a new medication or the alternatives that had fewer side effects. Well, yes, I kind of did wonder how’s this going to work? But you know this; I was happy to change to something else because I knew I wasn’t feeling great with the Buscopan. I know it does help for bloating and that, but I know when the lady said, “Take peppermint oil, I’ll try you with that”, I know peppermint is good for the stomach anyway. No, I was – the way I was feeling, Toney, I just wanted to try a change and see if it made a difference. [P11, female, 66y] Well, I’m not getting the same bloating the same. I do have IBS so I’ll always have that problem, but no, my tummy feels more comfortable from day to day. I’m quite happy to stick with that just now, yes. [P11, female, 66y] Yeah, for me it worked fine because my medication as changed. Now, I’m on something that suits me better with less sort of side effects… No, just … nothing worse, just better, just the symptoms were slightly better. [P8, female, 70y] | |
| Suggestions for improving in the future study | Patients valued regular review of medications and believed that it is quite important and needed. Just a review, a regular review of the medication that you’re on and what it’s still doing rather than just assuming that everything is fine, and it continues to be fine. [P8, female, 70y] The pharmacists suggested that the recruitment process could be improved in the definitive study. I suppose that cut out a certain amount of the population which is a shame in a way because some of the other people we might have been able to help more, but it would’ve meant going through their family, and I felt because it was a pilot, that perhaps that was a step too far on this occasion. Perhaps when you’re doing the full study you could consider people like that, but we would need to involve families and that just makes it more complicated. [Primary care pharmacist]Pharmacist also suggested paperwork needed to be improved to fit routine practice in the future direction. In addition, the initial monitoring period may need to be shortened to 2 weeks for close follow-up. The information pack was felt to be appropriate for use in the definitive trial. I think part of your paperwork it said three months review, six weeks review; those didn’t really fit what I was doing. Six weeks was too long to leave them, I was phoning them maybe two weeks, three weeks, or they were phoning me and saying it wasn’t going well. A shorter timeline for the initial review would be better. [Primary care pharmacist] Well, I think your paperwork could be slightly better, I found it a bit confusing you know, where to put things. I mean other than that, not really, no because I think your explanation package was very good, the education stuff that you sent me, the examples of what to change, you could have more of that, you could expand that list I think, to help people. [Primary care pharmacist] The pharmacists also suggested that well qualified and experienced pharmacists may be best suited for conducting the definitive trial or when its rolled out into practice to avoid confusions and complications related to authorisations and mistakes. The trust of GPs for experienced pharmacists is quite important as study did not need input form GPs. I think that to some extent depends on how experienced the pharmacist is and where their place in the team is. If you were a newly qualified pharmacist, you’d just arrived, you didn’t know anybody, you didn’t know the doctors, I think it would be more difficult. I would imagine if you’re going to roll this out, say somebody is going to do research like this, you would want to go for pharmacists who are well established and almost certainly have to be prescribers so that they can just get going, otherwise you’ve got that interface between the pharmacist, the patient and the doctor or the nurse and that just complicates the whole picture quite honestly. [Primary care pharmacist] |
| Willing to take part in a future trial | All patients, a primary care pharmacist and a GP expressed their interests to take part in future definitive trial. |
| Experiences in a training session for a pharmacist | The pharmacist expressed the important and value of the training session and its contents were quite important and extremely useful for her. In particular, it provided specific example of an alternative which made the decision-making process easier. Extremely useful. I think I would’ve struggled with the time constraints that I had to actually achieve as much as we did. It was very useful to have specific examples of what one drug could be changed to and the reason for that, it just made it easier for me just to go ahead and do things as opposed to having to think about it. If I had to work it all out for myself, it would’ve taken me longer and again, we’re back to time. [Primary care pharmacist Yes, yes, because the training gave you specific examples of what you could do, so we tended to search on the drugs that we knew we had a very simple, straightforward alternative to. That made the process, the decision-making process easier, I think. [Primary care pharmacist] |
4. Discussion
The REGENERATE feasibility study has shown that patients can be identifed and recruited from primary care setting by a primary care pharmacist. Seventy percent of patient participants invited attended the pharmacist led consultation and all but one accepted the recommended changes and completed the baseline and all follow up questionnaires. Data collection forms are suitable, and the data suggests that the intervention may be effective at reducing ACB. The participants’ survey responses and interviews demonstrated that the intervention is acceptable for both patients and healthcare professionals. Primary care may be an appropriate setting to conduct a future definitive trial and participants would be willing to take part and be randomized.
Strengths of the study included that it was based on the published literature and detailed qualitative work brought together in a logic model. The study showed a high response and retention rate, which might be due to good communication and a positive relationship between the primary care pharmacist and their patients, including the prior telephone conversation with the pharmacist before sending the invitation packs. Only one primary care pharmacist delivered the intervention in a single primary care setting, which is a strength as it can be assumed that the intervention was delivered consistently but also a limitation (see below). Fidelity to the intervention was supported by training and a detailed standard operating procedure, although without observation fidelity cannot be assumed.
Limitations were that findings from one pharmacist at one site might not be representative of the wider primary care pharmacist population and likewise the small sample size limits the generalizability. Virtual conduct of the interviews using telephone meant that non-verbal communication from patients could not be included. A potential solution to this is the use of other platforms such as MS TEAMS or Zoom meetings to conduct the patient interviews if face-to-face interviews are not possible. Further the interview with the doctor had to be replaced by a free text survey, which provided less rich information than an interactive interview.
In our feasibility study the ACB score decreased from baseline after a primary care pharmacist provided the intervention. In addition, during the interviews, patients reported decreased side effects of medication after receiving the intervention. Likewise, other studies have shown that a pharmacist, either individually or as part of a team undertaking patient medication review followed by recommendations to the prescriber, can reduce ACB [11]. However, in our study, one primary care pharmacist could implement medication deprescribing to patients successfully on their own due to being qualified as an independent prescriber pharmacist. Likewise, other studies have shown that the deprescribing can be done successfully by pharmacists [22,23,24]. Based on the utility calculation of EQ-5D-5L in all patients during the study period, small improvements in QOL were reported at six weeks’ follow-up, which may be due to patients having a positive attitude about the intervention or medication changes. However, improvement in QOL at 12 weeks follow up decreased slightly compared with 6 weeks follow up but was still higher than at the baseline, However, we report these only as trends since a non-powered feasibility study cannot be used to assess effectiveness and therefore the changes were not tested for statistical significance.
Pharmacists may be well placed to provide this ACB intervention based on this study and as reported elsewhere [19]. Increasing use of pharmacists based in general practice and also in community pharmacy is supported in recent UK policy as way of managing workload in primary care and reducing pressure on GPs [20]. Deprescribing as a specific focus of medication review is also now well established [21] and the general barriers and facilitators are increasingly understood. However, deprescribing with the specific aim of reducing ACB is a highly specialised application which requires additional knowledge and judgement as most changes require a switch to an alternative medication. In 2026, all newly registered pharmacists in the UK will be qualified as independent prescribers and the ability to implement changes themselves will facilitate deprescribing in general and ACB reduction specifically. However, it is important that pharmacists delivering the intervention are operating within their level of competence, and if necessary, any future trial must ensure the pharmacists are experienced in ACB or are provided with relevant training.
5. Conclusions
Deprescribing helps to promote appropriate use of ACB medication. Pharmacists with independent prescribing rights are potentially able to deliver a successful deprescribing intervention, implementing recommended medication changes themselves with a potential to lower anticholinergic cognitive burden score and increase patients’ QOL. This feasibility study has shown that patients can be recruited and retained and would be willing to take part in a randomized definitive trial. Data collection forms are suitable, and the results suggest that the intervention may be effective at reducing ACB and is acceptable to patients and health care professionals. The next stage of this programme of work should be a randomized pilot study, followed by a definitive RCT to assess the effectiveness and efficiency of a pharmacist led ACB deprescribing intervention compared to current practice.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: ACB intervention logic model; Figure S1: Baseline questionnaire for patient participants; S2: Interviews guides for doctors, pharmacists and patients; S3.
Author Contributions
All authors have made substantial contributions to the conception or design of the work, analysis, or interpretation of data. AN drafted the first version of the paper and other authors revised this critically for important intellectual content, approved the final version of the manuscript and agreed to be accountable for all aspects of the work and to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.Conceptualization: A.N, C.B., M.C, R.N. and P.K.M.; Methodology, A.N, C.B., M.C, R.N. and P.K.M.; Investigation, A.N.; Data Curation, A.N. and P.K.M.; Writing – Original Draft Preparation, A.N.; Writing – Review & Editing, C.B., M.C, R.N. and P.K.M.
Funding
This research was funded by the University of Aberdeen.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the East of Scotland Research Ethics Committee (protocol code: 2-094-20 and date of approval: 8 April 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We would like to thank Mrs. Valerie Sillito for her role as a primary care pharmacist in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization, 2021-last update, Ageing and health. Available: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health [12/August, 2021].
- Maher, R.L., Hanlon, J.T. and Hajjar, E.R., 2014. Clinical consequences of polypharmacy in elderly. Expert Opinion on Drug Safety, 2014, 13(1), pp. 1-11. [CrossRef]
- Katzenschlager, R., Sampaio, C., Costa, J. and Lees, A. Anticholinergics for symptomatic management of Parkinson´s disease. Cochrane Database of Systematic Reviews, 2022, (3), pp. 1-19. [CrossRef]
- O’Donnell, K.L., Gnjidic, D., Nahas, R., Bell, J.S. and Hilmer, S.N. Anticholinergic burden: Considerations for older adults. Journal of Pharmacy Practice and Research, 2017 47(1), pp. 67-77. [CrossRef]
- Vardanyan, R.S. and Hruby, V.J. Anticholinergic drugs. In: R.S. VARDANYAN and V.J. HRUBY, eds, Synthesis of essential drugs, 2006. Elsevier, pp. 195-208.
- Rudolph, J.L., Salow, M.J., Anglini, M.C. and Mcglinchey, R.E. The anticholinergic risk scale and anticholinergic adverse effects in older persons. Arch Intern Med, 2008, 168(5), pp. 508-513. [CrossRef]
- Ancelin, M.L., Artero, S., Portet, F., Dupuy, A., Touchon, J. and Ritchie, K. Non-degenerative mild cognitive impairment in elderly people and use of anticholinergic drugs: longitudinal cohort study. British Medical Journal, 2006, 332, pp. 455-459. [CrossRef]
- Ehrt, U., Broich, K. and Larsen, J.P. Use of drugs with anticholinergic effect and impact on cognition in Parkinson’s disease: A cohort study. Journal of Neurology, Neurosurgery, and Psychiatry, 2010, 81, pp. 160-165.
- Kersten, H. and Wyller, T.B. Anticholinergic drug burden in older people’s brain - how well is it measured? Basic & clinical pharmacology & toxicology, 2014, 114(2), pp. 151-9.
- Ablett, A.D., Wood, A.D., BarrA, R., Guillot, J., Black, A.J., Macdonald, H.M., Reid, D.M. and Myint, P.K. A high anticholinergic burden is associated with a history of falls in the previous year in middle-aged women: findings from the Aberdeen prospective osteoporosis screening study. Annals of Epidemiology, 2018, 28, pp. 557-562. [CrossRef]
- Nakham, A., Myint, P.K., Bond, C.M., Newlands, R., Loke, Y.K. and Cruickshank, M. Interventions to reduce anticholinergic burden in adults aged 65 and older: A systematic review. Journal of the American Medical Directors Association, 2020, 21(2), pp. 170-180. [CrossRef]
- Krishnaswami, A., Steinman A. M., Goyal, P., Zullo, R.A., Anderson, S.T., Birtcher, K.K., Goodlin, J.S., Maurer, S.M., Alexander, P.K., Rich, W.M. and Tjia, J. Deprescribing in older adults with cardiovascular disease. Journal of the American College of Cardiology, 2019, 73(20), pp. 2584-2595.
- Michael, S. and Reeve, E. Deprescribing. https://www.uptodate.com/contents/deprescribing#:~:text=Common%20goals%20for%20deprescribing%20include,to%20improving%20quality%20of%20life. edn. UpToDate, 2022.
- Olasehinde-Williams, O., July, 2020-last update, Deprescribing guide, 2020. Available: https://southendccg.nhs.uk/your-health-services/healthcare-professionals/medicines-management/medicines-management-resources/2308-deprescribing-guide/file [April/03, 2020].
- Craig, P., Dieppe, P., Macintyre, S., Michie, S., Nazareth, I. and Petticrew, M., 2019-last update, Developing and evaluating complex interventions: Following considerable development in the field since 2006, MRC and NIHR have jointly commissioned an update of this guidance to be published in 2019. Available: https://mrc.ukri.org/documents/pdf/complex-interventions-guidance/ [05/01, 2021].
- Stewart, C., Gallacher, K., Nakham, A., Cruickshank, M., Newlands, R., Bond, C., Myint, P.K., Bhattacharya, D. and Mair, F.S. Barriers and facilitators to reducing anticholinergic burden: a qualitative systematic review. International Journal of Clinical Pharmacy, 2021, 43, pp. 1451-1460. [CrossRef]
- Cunningham, Y., Wood, C., Stewart, C., Nakham, A., Newlands, R., Gallacher, K.I., Quinn, T.J., Ellis, G., Lowrie, R., Myint, P.K., Bond, C. and Mair, F.M. Understanding Stakeholder Views Regarding the Design of an Intervention Trial to Reduce Anticholinergic Burden: A Qualitative Study. Frontiers in Pharmacology, 2021, 12, pp. 1-10. [CrossRef]
- Boustani, M., Campbell, N., Munger, S., Maidment, I. and Fox, C. Impact of anticholinergics on the aging brain: A review and practical application. Aging Health, 2008, 4(3), pp. 311-320. [CrossRef]
- Bruhn, H., Bond, C.M., Elliott, A.M. Pharmacist led management of chronic pain in primary care: results from a randomised controlled exploratory trial. BMJ Open, 2013, 3:e002361. [CrossRef]
- Wickware, C. When will England get a ’Pharmacy First’ service? The Pharmaceutical Journal, 2023, 310(7969). [CrossRef]
- Okeowo, D.A., Zaidi, S.T.R., Fylan, B. and Alldred, D.P. Barriers and facilitators of implementing proactive deprescribing within primary care: a systematic review. International Journal of Pharmacy Practice, 2023, 31(2), pp.126-152. [CrossRef]
- Kua, C., Mak, V.S.L. and Lee, S.W.H. Health Outcomes of Deprescribing Interventions among older residents in nursing homes: A systematic review and meta-analysis. Journal of the American Medical Directors Association, 2019, 20(3), pp. 362-372. [CrossRef]
- Thillainadesan, J., Gnjidic, D., Green, S. and Hilmer, S.N. Impact of deprescribing interventions in older hospitalised patients on prescribing and clinical outcomes: a systematic review of randomised trials. Drugs Aging, 2018, 35(4), pp. 303-319.
- Ulley, J., Harrop, D., Ali, Ali, Alton, S. and Davis, S.F. Deprescribing interventions and their impact on medication adherence in community-dwelling older adults with polypharmacy: a systematic review. BMC Geriatrics, 2019, 19(15), pp. 1-13. [CrossRef]
Figure 1.
CONSORT flow diagram.
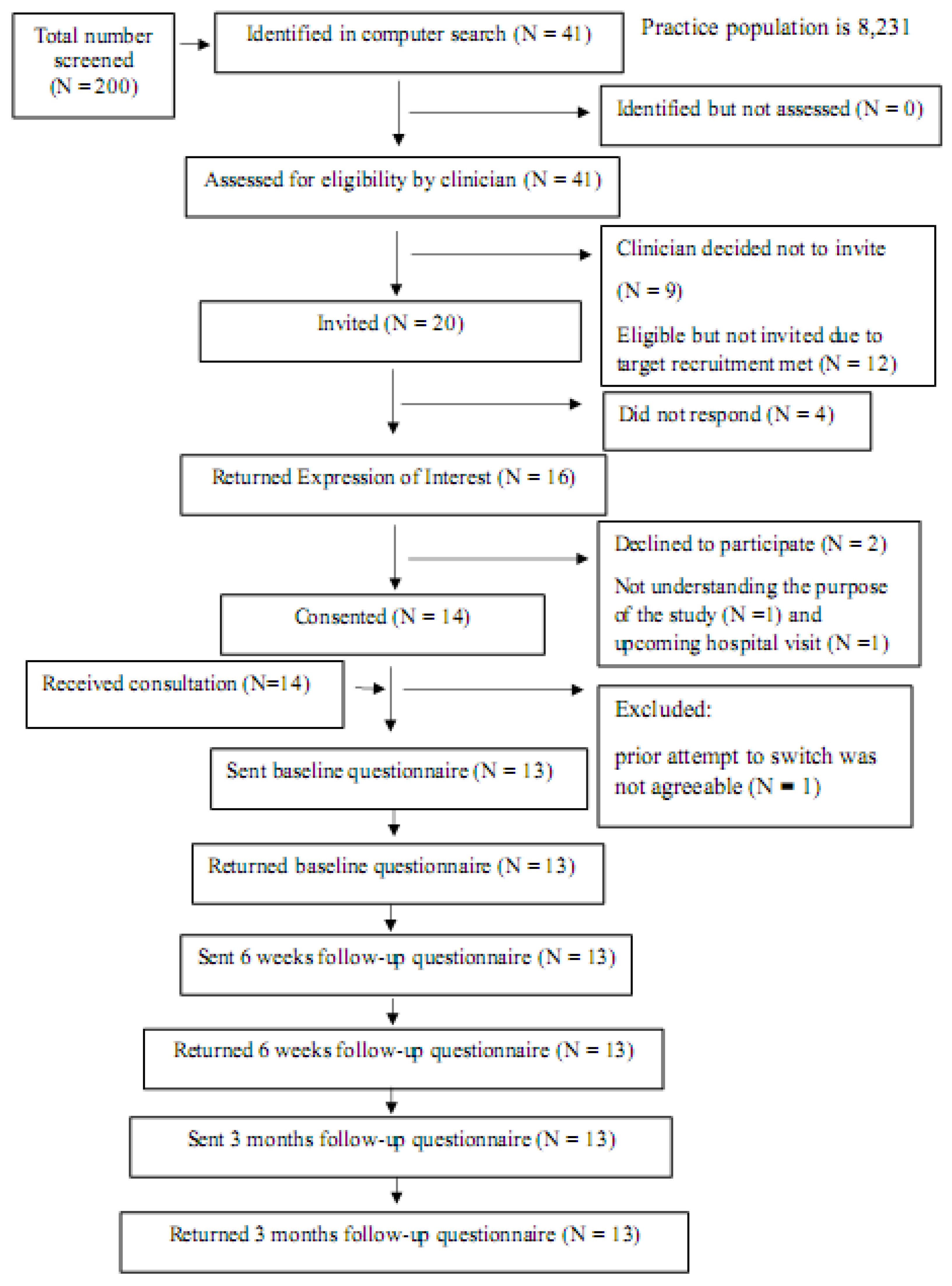
Table 1.
Summary of patient characteristics at baseline N=13.
| Characteristics | N* |
|---|---|
| • Males • Females |
8 5 |
| Age in years • 65-69 • 70-74 • 75-79 |
3 5 5 |
| Number of medications (mean ±SD) | 7.62 (±3.18) |
| Anticholinergic Cognitive Burden score • 3 • 4 • 6 |
7 1 5 |
| The median time (IQR) for the initial consultation with the primary care pharmacist | 15 minutes (12.5- 20 minutes). |
* Due to small denominator (13) percentage is not reported.
Table 2.
Patient participant responses to Likert * statements about their experiences and views at baseline, 6-and 12-weeks (N=13).
Table 2.
Patient participant responses to Likert * statements about their experiences and views at baseline, 6-and 12-weeks (N=13).
| Items | Baseline (median; IQR) | 6 weeks follow up (median; IQR) | 12 weeks follow up (median; IQR) |
|---|---|---|---|
| The pharmacist appeared well informed | 5 (4, 5) | - | - |
| The pharmacist listened to what I had to say | 5 (4, 5) | - | - |
| The pharmacist answered all my concerns | 5 (4, 5) | - | - |
| I would rather have seen a doctor | 3 (2 ,3) | - | - |
| I would rather have seen a nurse | 3 (2,3) | - | - |
| Happy with my consultation with the pharmacist | 5 (4, 5) | - | - |
| Good idea to change medication to reduce chance of unwanted side effects | 5 (4.50, 5) | - | - |
| The study purpose was clear. | 5 (4, 5) | - | - |
| Given enough information to decide whether to participate. | 5 (4, 5) | - | - |
| The new approach to your medication | |||
| Happy to discuss medicines with the pharmacist. | - | 5 (4, 5) | 5 (4, 5) |
| The symptoms of illness are controlled | - | 3 (2, 4) | 4 (4, 5) |
| No concerns related to new approach for reviewing medicines | - | 4 (4,5) | 4 (4,5) |
| Happy with the changes made to my medicines | - | 4 (3, 4.50) | 3 (3, 5) |
| Unhappy with the changes made to medicines | - | 3 (2, 3) | 3 (3,3) |
| Currently on a new medication | - | 4 (3, 5) | 4 (3, 4) |
| Changed back to my old medicines | - | 3 (2, 3) | 2 (2, 3) |
| About the study processes | |||
| The questionnaires were clear | - | - | 5 (4, 5) |
| The questionnaires were easy to complete | - | - | 5 (4, 5) |
| Happy to complete the questionnaires | - | - | 5 (4, 5) |
| Study participation did not take up too much time | - | - | 5 (4, 5) |
| Study participation did not give any stress | - | - | 5 (4, 5) |
| Consider participating in a future study examining similar issues | - | - | 5 (4, 5) |
| Recommend a friend to take part in this kind of study | - | - | 5 (3, 5) |
| Interested in being part of a patient advisory group for future studies | - | - | 3 (2, 5) |
| Further study should be encouraged in this area | - | - | 5 (4, 5) |
* 5 = Strongly agree, 4 = Agree, 3 = Unapplicable/Uncertain, 2 = Disagree, 1 = Strongly disagree.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



