
Submitted:
16 September 2024
Posted:
17 September 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
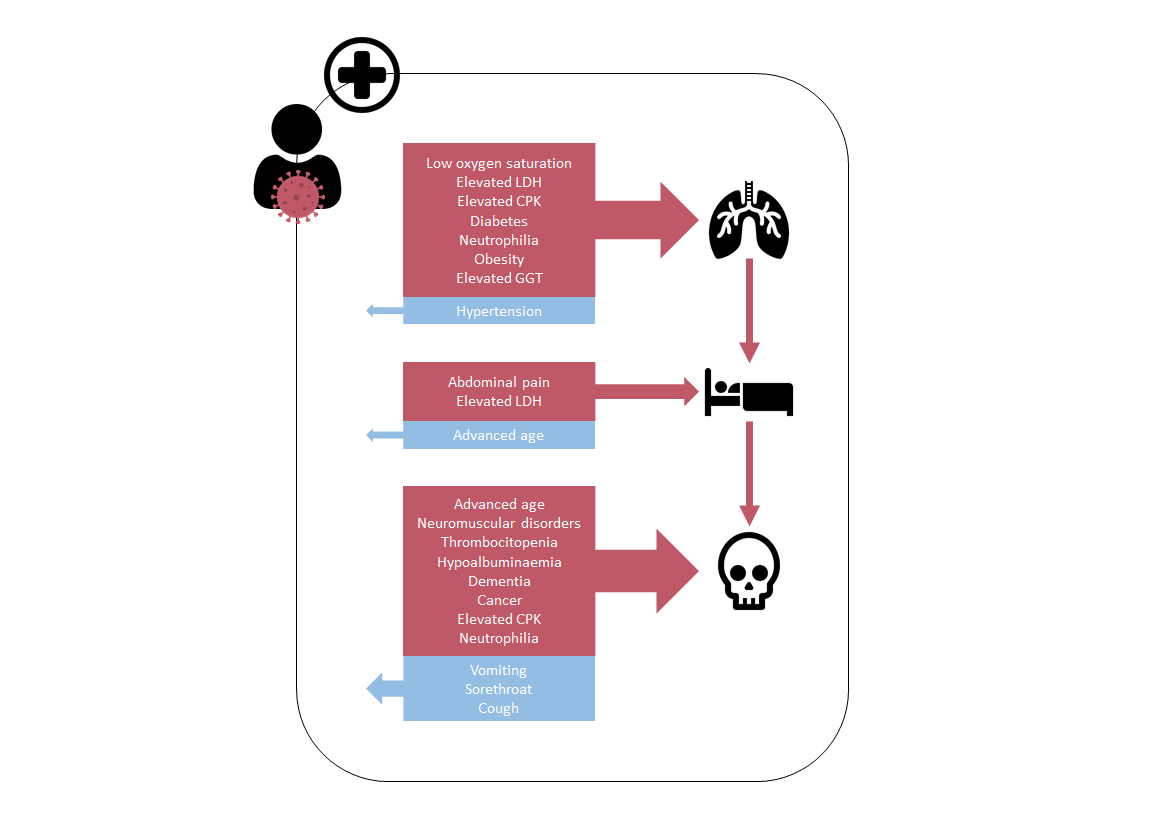
In the frame of the I-MOVE-COVID-19 project, a cohort of 2050 patients admitted in two Spanish reference hospitals between March 2020 and December 2021 was selected, and a range of clinical factors data were collected at admission to assess their impact on the risk COVID-19 severity outcomes through a multivariate adjusted analysis and nomograms. The need for ventilation and ICU admission were found directly associated with a higher mortality risk (OR 6.9 and 3.2, respectively). The clinical predictors of mortality were need for ventilation and ICU, advanced age, neuromuscular disorders, thrombocytopenia, hypoalbuminaemia, dementia, cancer, elevated CPK and neutrophilia (OR between 1.8 and 3.5), whilst the presence of vomiting, sore throat and cough diminished risk of death (OR 0.5, 0.2 and 0.1 respectively). Admission to ICU was predicted by the need for ventilation, abdominal pain and elevated LDH (OR 371.0, 3.6 and 2.2, respectively) as risk factors; otherwise, it was prevented by advanced age (OR 0.5). In turn, the need for ventilation was predicted by low oxygen saturation, elevated LDH and CPK, diabetes, neutrophilia, obesity and elevated GGT (OR between 1.7 and 5.2), whilst prevented by hypertension (OR 0.5). These findings could enhance patient management and strategic interventions to combat COVID-19.
Keywords:
COVID-19
; SARS-CoV-2
; severity
; mortality
; ventilation
; ICU
; clinical phenotype
1. Introduction
COVID-19 is a disease in response to a viral infection, the Severe Acute Respiratory Syndrome CoronaVirus 2 (SARS-CoV-2), which emerged in Wuhan, China, in December 2019. The clinical pathway may progress from asymptomatic to severe illness, like pneumonia, acute respiratory distress syndrome (ARDS) and fatal multi-organ dysfunction. Its effects can be characterised through clinical severity, regarding medical complications experienced by infected individuals. In this sense, this disease has been classified according to different definitions such as those of the World Health Organization [1].
The present study was conducted in the frame of the Multidisciplinary European hospital network for research, prevention and control of the COVID-19 pandemic (I-MOVE-COVID-19 hospital network) [2]. This consortium came from many partners already involved in the studies within the Influenza Monitoring Vaccine Effectiveness in Europe (I-MOVE) network [3] who rapidly adapted their infrastructure and protocols to include COVID-19 to their surveillance system for hospitalised cases in several countries when the novel coronavirus epidemic arrived. Spain joined this project with the participation of two hospitals that were able to provide a valuable information for COVID-19 surveillance in Europe [4], heading also a pilot model for COVID-19 and SARI surveillance at a national level [5].
During the period included in the present study, two notable variants of concern (VOCs) circulated, which were associated to different severity presentations. They were Alpha / B.1.1.7 in winter 2020 and Delta / B.1.617.2 in spring 2021 (named by Phylogenetic Assignment of Named Global Outbreak (PANGO) / lineage designation) [4]. Although COVID-19 vaccines have proven to be key to control the pandemic by reducing the incidence of COVID-19 infections, hospitalizations and deaths, the burden of COVID-19 clinical management is high [6] and SARS-CoV-2 continues evolving into new variants that are being monitored by international health authorities [7]. However, mainly host-related factors rather than viral genetic mutations drive the pathogenesis, and the severity of the COVID-19 episode depends especially on the host’s health condition level, and the presence of underlying risk factors and comorbidities [8,9].
Since clinical presentation of COVID-19 is polymorphic [10], it seemed obvious that patients with a phenotype characterized by a pool of risk factors showed several joined features at admission, which could predict the severity outcome. COVID-19 patients show a wide clinical spectrum, since COVID-19 affects multiple organ systems, including respiratory manifestations (e.g. shortness of breath, cough, sore throat), neuropsychiatric and cognitive symptoms (e.g. fatigue, headaches, loss of smell), cardiovascular presentations (e.g. chest pain, arrhythmias, thromboembolic events), and manifestations from other organ systems, such as endocrine, gastrointestinal, renal, and skin [11]; however, a meta-analysis in 5000 patients found that only dyspnoea was associated with severity [12]. Moreover, comorbidity and underlying conditions play a major role on disease prognosis [8,9], and they have been found associated to severe clinical outcomes [11], also being related to an encountered number of biomarkers [13], highlighting its effect on the systemic inflammation and immune response [14]. Furthermore, COVID-19 severity outcomes are also affected by sociodemographic factors, such as age, sex, occupation, housing situation (with crowded and/or intergenerational housing), and barriers in access to healthcare [15].
In this sense, the combination of sociodemographic, clinical, comorbidity, and metabolomics data improve the prediction accuracy of the models, and it seems useful to study associations with severity outcomes. Nevertheless, and to best of our knowledge, combining all those kind of features with the aim of predict several severity outcomes it only has been done until now in a small size of American COVID-19 patients [16]. Despite this, other previous studies had studied epidemiological and clinical characteristics regarding some severity outcome in other populations [10,17,18,19]. However, there are few published studies with large sample sizes describing the phenotype associated to severity outcomes in Spanish hospitalised COVID-19 patients [10,20].
Therefore, the present article aims to describe the phenotype at hospital admission associated to severe COVID-19 disease, in a sample of COVID-19 cases admitted in two reference hospitals in Spain between March 2020 and December 2021, in the context of the I-MOVE-COVID-19 project. This study provides a comprehensive assessment of a wide board of health-related features and their potential impact as predictors of severity, using ventilation, ICU admission and mortality as main outcomes.
2. Materials and Methods
2.1. Study Setting and Design
A retrospective multi-site observational study was conducted in the two tertiary care hospitals participating as the Spanish component of the I-MOVE-COVID-19 network, with data collected between 16th March 2020 and the end of 2021. The Miguel Servet (HUMS) and the Virgen de las Nieves (HUVN) University Hospitals, located in Zaragoza and Granada, respectively, are both reference hospitals for surveillance of respiratory infections in their region, with a capacity of more than 1300 bed each and covering a total catchment area of over 880.000 people.
2.2. Participants
Following the I-MOVE-COVID-19 surveillance, risk factors, and vaccine effectiveness studies protocols [21,22,23], patients admitted to these hospitals during the study period were tested for SARS-CoV-2 detection and data were collected in a structured online questionnaire, including a comprehensive set of demographic, epidemiological and clinical variables. To manage the workload of data collection in periods of high incidence of COVID-19 admissions (from July 2020 and until the end of the study) a weekly sample of patients were systematically selected (those admitted on every Tuesday and Wednesday).
This study was conducted on a representative sample of 2050 patients who had a positive test for SARS-CoV-2 detection and were admitted to one of the aforementioned hospitals between two days prior and up to 28 days after their index positive swab. Patients who tested negative for SARS-CoV-2 PCR on nasopharyngeal swab, and those with missing data were excluded.
2.3. Laboratory Testing
The diagnosis and confirmation of SARS-CoV-2 were based on molecular tests performed on patients’ nasopharyngeal swab specimen collected by trained nurses. Concretely, CE-IVD Real-time PCR (real time reverse transcriptase-polymerase chain reaction) with at least two specific targets of SARS-CoV-2 RNA and an internal control to check the quality of the sample. Results were categorized according to the specifications of the manufacturer and following this classification: negative (absence of SARS-CoV2 target detection or detection over 38 Ct and detection of internal control), positive (detection of two SARS-CoV-2 target detection under 38 Ct) and inconclusive (only one SARS-CoV-2 target detection). Inconclusive samples were retested for clarification. If an inconclusive result persisted, a new sample of the participant was analysed.
Other laboratory determinations (shown on tables below) were performed on blood samples collected at the time of admission using standardised and similar methods available in the hospitals.
2.4. Data Collection
Data were obtained with standardized data collection forms from medical electronic records. They were anonymised and linked in a data repository. Consent was not required from individual patients, due to the pandemic emergency exemption and because these data were included as part of the pilot surveillance system of the future integrated respiratory surveillance in Spain [5]. Nonetheless, only summary data were extracted to minimize the risk of disclosure.
2.5. Outcomes of Interest
We described the epidemiological and clinical characteristics in relation to the main severity outcomes as dependent variables. These were the requirement for ventilation, intensive care unit (ICU) admission and death in COVID-19 hospitalised patients. As independent variables, we considered a long list of socio-demographics, underlying diseases, symptoms, and biochemical determinations (shown on tables below). Definitions of the variables were outlined in the generic published protocol [23].
2.6. Statistical Analysis
Descriptive analysis of each epidemiological and clinical variable by sex. C categorical variables as absolute and relative frequencies (n, %), and continuous variables are presented as mean and standard deviations (x̄ ± SD), but age as median and interquartile range (m, IQR). We exclude participants with >30% records with missing data for each specific analysis. Variables were excluded from the analysis if they had >30% records with missing data. Group wise comparisons were performed using Student’s t-test or Chi-square (χ2), and by applying Haldane Ascombe correction when needed.
Bivariate logistic regression models were used to assess the association between clinical variables and the main outcomes: need for ventilation, ICU admission and in-hospital mortality, with the OR and confidence interval (95%). Models were refitted with categories for continuous variables such as biochemistry results or clinical measurements at admission according to accepted values for standard range to obtain odds ratios by categories of low/within range/high values as appropriate.
Variables with statistical significance or near were carried forward to a multivariate logistic regression analysis based on the Akaike information criterion (AIC), assessing the independent association of each specific variable with each outcome. However, vaccination and admission centre were not included in these models because of potential biases (due to differences in vaccine availability). Final model was determined by stepwise selection criteria based on improvement in AIC, and its suitability was assessed using the area under the receiver operating characteristic curve (ROC AUC score), Nagelkerke’s R2 coefficient, accuracy, specificity and sensitivity values. Finally, nomograms for each model were established to provide a clinical tool so that, after visually normalising the ORs for each variable in the multivariate model, the sum of the points that the presence of each risk factor confers allows an estimate of the risk for each subject to be made. The score to determine the level of risk (low, high) for each nomogram was established from the percentile value of the predictors corresponding to the frequency found in the sample for each outcome.
Two-tailed p value was considered statistically significant when minor 0.05. All analyses and graphs have been carried out with free R software, MS Excel and MS PowerPoint.
2.7. Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and its subsequent modifications. The requirement for written informed consent was waived, given the context of emerging infectious disease. Nevertheless, the protocol was approved by the Ethics Committee of Andalucía, and by the managements of both centres.
3. Results
3.1. Descriptive Analysis
The characteristics of the studied sample of 2050 COVID-19 hospitalized COVID-19 patients, overall and stratified by sex, are presented in Table 1.
Regarding overall sociodemographic and clinical factors, there were slightly more men than women (53% vs. 47%), their median age was 64 years, and the most common age range was from 40 to 64 years (40%). HUVN admitted 41% participants whereas 59% were recruited at HUMS. Their vaccine coverage was 10% for COVID-19 (24% since it was available) and 39% for flu. They account for an average of 2.5 previous hospitalisations and 7 medical visits in the year prior to their admission (15% added up to more than 12).
In terms of the main severity outcomes, 15% cases died, 9% were admitted to ICU and 27% needed ventilation. On average, it took less than a week from the onset of symptoms to hospitalisation and 10 days to ICU admission. The length of stay was over a week for 60% participants and, on average, the stay was over 12 days at the hospital and almost 24 days at the ICU. The time between admission to hospital and ICU was about 4 days, and less than 8% of participants waited more than a week.
Chronic conditions were present in COVID-19 (almost 3 on average), being obesity and hypertension the most prevalent in nearly half of the sample (48%) with a BMI of 29.4 kg/m2 on average. Other frequent disorders were rheumatic disease (24%), diabetes (24%), and heart disease (20%).
Their most prevalent symptoms were cough (71 %), feverish (67%), dyspnoea (66%) and malaise (62%), followed by fever (34%), general deterioration (33%), myalgia (24%), diarrhoea (18%), and headache (16%).
Clinical measures were low on average for oxygen saturation (92%) and high respiratory rate (26 rpm on average). Indeed, low oxygen saturation was present in 62% participants, whilst other parameters such as systolic and diastolic blood pressure (SBP, SDP) and long QT were out of range in less than 15%.
Regarding biochemistry alterations, the most frequently observed deviations were high levels of ferritin and C-reactive protein (CRP) (99%), urea (95%), lactate dehydrogenase (LDH) (77%), D-dimer (68%), gamma-glutamyl transferase (GGT) (57%), and aspartate transaminase (AST) (47%), being also frequent to found high levels of alanine transaminase (ALT) (34%), hypoalbuminaemia (28%), high levels of creatinine phosphokinase (CPK) (25%), neutrophilia (18%), thrombocytopenia and high prothrombin time (17%).
Compared to women, men were younger and more likely to need ventilation and ICU admission, to have heart and lung diseases, to show fever and long QT, to show higher figures for diastolic and systolic blood pressure, and elevated figures for ALT, AST, total bilirubin, C-reactive protein, GGT, prothrombin time, and blood urea, as well as to present thrombocytopenia. Otherwise, men were less likely to be vaccinated against influenza, to account for medical visits, to have anaemia, asthma, dementia and rheumatic diseases, to show chest pain, coryza, diarrhoea, general deterioration, headache, nausea and vomiting, to show low SBP, DBP, and oxygen saturation, to show elevated D-dimer, neutrophilia and thrombocytophilia.
Additionally, temporal distribution in terms of month of admission for our COVID-19 hospitalised cases resulting from the recruitment implementation described in the 2.2 is shown in Figure 1.
Furthermore, their distribution by age and sex is represented in Supplementary Figure A1, showing there were more women in their 80’s but more men in their 50’s.
3.2. Bivariate Analysis
The results for the univariate analysis are presented as Supplementary tables in Appendix A.
As Table A1 shows, mortality was more likely among those who were older, visited more their physician previously, needed ventilation or admission at ICU, stayed longer at the hospital, waited longer for ICU, had more underlying conditions (including anaemia, cancer, dementia, diabetes, heart disease, hypertension, ictus, kidney disease, neuromuscular disorders, lung or rheumatic disease), showed confusion, general deterioration, tachycardia, neutrophilia, thrombocytopenia, hypoalbuminaemia, low SBP, DBP, oxygen saturation, elevated AST, bilirubin, CPK, D-dimer, LDH, prothrombin time and urea. Contrary, mortality was less likely among those who were flu vaccinated, and those who showed ageusia, anosmia, chest pain, cough, diarrhoea, fever, feverish, headache, myalgia, sore throat, and vomiting, lower figures for DBP and oxygen saturation, elevated ALT and GGT.
Besides, Table A2 shows that ICU admission was more likely among those of extreme age groups, who were hospitalised at HUVN, who had more than 12 medical visits last year, died or needed ventilation, whose stay was longer, who showed higher BMI, obesity, diabetes, showed abdominal pain, dyspnoea, low SBP and oxygen saturation, elevated ALT, AST, bilirubin, CPK, GGT, LDH, urea and neutrophilia. Otherwise, ICU admission was less frequent among those who were men, COVID-19 vaccinated, showed confusion, malaise, and higher oxygen saturation.
Table A3 shows that need for ventilation was more likely among those COVID-19 patients who were older, men, admitted at HUVN, flu vaccinated, had more previous medical visits last year, deceased, stayed at ICU, stayed longer, had higher BMI, cancer, diabetes, heart disease, hypertension, lung disease, and obesity, showed dyspnoea, low SBP and oxygen saturation, elevated AST, bilirubin, CRP, CPK, D-dimer, GGT, LDH, urea and neutrophilia. Contrary, ventilation were needed less likely among those who were COVID-19 vaccinated, showed anaemia, rheumatic disease, ageusia, anosmia, chest pain, coryza, diarrhoea, feverish, malaise, lower figures for SBP, DBP and oxygen saturation.
3.3. Multivariate Analysis
The independent associations of several risk factors with the severity outcomes computed by adjusted multivariate analysis are shown as forest plots in Figure 2. The statistics for the predictive models are shown in Table 2 including those for all the dataset and also its application on each hospital.
Mortality was directly associated with several factors: need for ventilation (OR 6.9, IC 95% 4.3-11.1), having advanced age (OR 3.5, IC 95% 2.6-4.7), ICU admission (OR 3.2, IC 95% 1.8-5.6), neuromuscular disorders (OR 2.9, IC 95% 1.2-2.9), thrombocytopenia (OR 2.2, IC 95% 1.4-3.6), elevated prothrombin time (OR 2.1, IC 95% 1.2-3.3), hypoalbuminaemia (OR 2.1, IC 95% 1.3-3.2), dementia (OR 2.0, IC 95% 1.1-3.6), cancer (OR 1.9, IC 95% 1.0-3.4), elevated CPK (OR 1.9, IC 95% 1.2-2.9) and neutrophilia (OR 1.8, IC 95% 1.1-2.9). Inverse associations with mortality were also found: having cough (OR 0.5, IC 95% 0.4-0.8), sore throat (OR 0.2, IC 95% 0.1-0.8) and vomiting (OR 0.1, IC 95% 0.0-06). Statistics for this model were AUC ROC = 0.803, Nagelkerke’s R2 = 0.294, accuracy = 0.813, specificity = 0.956, and sensitivity = 0.279.
ICU admission was found to be directly associated with need for ventilation (OR 371, IC 95% 90.8-1516.8), abdominal pain (OR 3.6, IC 95% 1.2-10.8), and elevated LDH (OR 2.2, IC 95% 1.2-10.8). Likewise, ICU admission was inversely associated with advanced age (OR 0.5, IC 95% 0.4-0.7). Statistics for this model were AUC ROC = 0.927, Nagelkerke’s R2 = 0.520, accuracy = 0.905, specificity = 0.984, and sensitivity = 0.141.
Need for ventilation was directly associated with low oxygen saturation (OR 5.2, IC 95% 2.8-9.4), elevated LDH (OR 3.0, IC 95% 1.5-6.3), elevated CPK (OR 2.4, IC 95% 1.5-3.7), diabetes (OR 2.3, IC 95% 1.4-3.9), neutrophilia (OR 2.2, IC 95% 1.3-3.7), obesity (OR 1.9, IC 95% 1.2-3.0) and elevated GGT (OR 1.7, IC 95% 1.1-2.7). On the contrary, hypertension was inversely associated with the need for ventilation (OR 0.5, IC 95% 0.3-0.8). Statistics for this model were AUC ROC = 0.906, Nagelkerke’s R2 = 0.471, accuracy = 0.881, specificity = 0.967, and sensitivity = 0.352.
Some factors lost their statistical significance when the models were applied to each hospital. For death, these were cough, hypoalbuminaemia, elevated CPK, sore throat and vomiting in HUMS, and cancer, dementia, neutrophilia, elevated prothrombin time, neuromuscular disorders, sore throat and vomiting in HUVN. For ICU admission, significance were lost for abdominal pain and elevated LDH in HUMS, and for elevated LDH and ventilation in HUVN. Ventilation did not show significance for elevated GGT, neutrophilia, hypertension and obesity in HUMS; and for diabetes, elevated CPK, GGT, LDH, neutrophilia and obesity in HUVN.
Finally, nomograms in Figure 3 were constructed for each outcome based on the above results. The risk of death was set as high for a score higher than 67, corresponding to a predictive value of 0.338, correspondent to nearly 70 points. High risk of ICU admission was set for a score of more than 85 points, corresponding to a model predictive value of more than 0.455. High risk of ventilation was set for a score of more than 58 points, corresponding to a model predictive value of 0.293.
4. Discussion
We described the clinical phenotypes at hospital admission associated to three different severity outcomes for COVID-19 confirmed cases: mortality, ICU admission and the need for ventilation. A large sample size (n = 2050) and a broad range of data collected during nearly two years since the start of the COVID-19 pandemic in Spain allowed us to assess a wide range of clinical parameters to characterize these phenotypes with a worst prognosis of the COVID-19 episode, including socio-demographic, underlying comorbidities and chronic conditions, and symptoms, physiological and biochemical markers presented during admission. Furthermore, describing associations between the phenotype characteristics and the severity outcomes allow us to compute a predictive model and to establish nomograms as clinical tools for each severity outcome.
There were a large number of studies regarding each feature and outcome included in our aim individually, but very few includes all of them or were made in such a large sample of Spanish COVID-19 patients. Despite this, since our data were shared on an European project, we can compare some assessments with the European data set results [4]. Regarding main outcomes, the situation of severity for the COVID-19 hospitalised patients appears to have been more favourable in Spain, as we found lower rates for death (15.1% vs. 18.8%), ICU admission (8.7% vs. 13.7%) and use of ventilation (26.7% vs. 38.4%), even accounting for a similar age and sex distribution on both studies (median age was 64.0 vs. 63.8 years, and 53.1% were men vs. 54.6%). On the contrary, our Spanish figures were much higher for pluripathology (two or more underlying conditions were present in 62.2% for Europeans but 70.6% for Spaniards –data not shown), and the prevalence for obesity (48.4% vs. 27.1%), hypertension (47.8% vs. 43.6%) and rheumatic diseases (24.5% vs. 6.3%) were higher, albeit heart disease (19.8% vs. 32.6%) and diabetes (23.8% vs. 26.1%) were lower. Nevertheless, on Spanish general population and beyond the I-MOVE study, the metabolic risk factors related with mortality and an elevation for the risk for transmissible diseases are also included at the top of the list of risk factors for mortality (hypertension 18.5%, diet 17.4%, smoking 14.1%, excess weight 12%, hyperglycaemia 8.7% and hyperlipidaemia 6.5%) [24], and smoking is even above the European median in Spain (23.1% vs 19.7%) [25].
Therefore, additional factors must be involved in these differences on severity outcomes by country, such as the way in which the pandemic crisis and health intervention strategies were managed. In this sense, Spanish Healthcare System has universal coverage and, before the pandemic, it was known as one of the best and most efficient in Europe, according to the World Economic Forum and to Bloomberg [26,27]. In addition, Spanish health system’s institutions and health professionals are highly trusted by the public opinion [28] and are supported by the government, which has a strong role [29]. This favoured and encouraged the implementation of early strong mandatory physical distancing measures, and prioritised vaccination policies for the elders, conditioning implications for patient management. Accordingly, our study reflects this situation not only on the severity outcomes, but on the higher median ICU stay for Spanish COVID-19 hospitalised patients, when compared to their European counterparts (23.9 vs. 18 days).
On the other hand, our findings on predictive risk factors for severity outcomes are consistent with literature [30], and in line with reports from previous large size studies in Spanish COVID-19 hospitalised patients, which described some risk factors strongly associated to death hazard, including a number of underlying conditions and higher inflammatory parameters [10], such as advanced age, low oxygen saturation, and high C-reactive protein [20].
Our final models were good or even greater according with the figures for AUC-ROC, accuracy and specificity (0.80-0.93, 0.81-0.90, and 0.96-0.98 respectively, although figures for Nagerkerke’s R2 and sensitivity were not so good (0.294-0.520 and 0.141-0.352). Dichotomisation of variables simplifies the interpretation and construction of the models, but can also facilitate such features profile.
It should be noted that none of the identified predictors appeared in the final models for all severity outcomes (however, age, elevated CPK, LDH, and neutrophilia appeared in two of them), and even several of them was found to be associated in a different (advanced age and hypertension) or not expected direction (vomiting, sore throat and cough for mortality). In this regard, we should point out some issues.
Advanced age may be directly associated with death and inversely with admission to the ICU, due to this condition does not benefit the patient when applying admission triage in a situation of work overload [31]. Besides, hypertension has been observed as a protective factor for need of ventilation. In this sense, it should be highlighted that SARS-CoV-2 uses angiotensin-converting enzyme 2 (ACE2) as a cell receptor for viral entry whilst ACE is the target for some therapeutic treatments for hypertension that could prevent vasoconstriction and disease conditions in Raynaud’s phenomenon; thus, patients treated for hypertension may have a different immune response to SARS-CoV-2 which could influence the severity of the disease and thus the need for respiratory support [32]. In addition, we may point out how the reporting of some symptoms (such as vomiting, sore throat and cough) may work as indicators of the disease manifestation, which may have facilitated its early diagnosis and treatment [33], fitting with the timeline of symptom presentation reported previously by other authors [34].
It is also important to note that none of the final models included sex, medical contacts (either admissions or visits), or time between events (such as days of stay) as predictors. This can easily be explained by the fact that it is not these factors per se but some associated conditions also present in the models that are playing a role in predicting the severity of COVID-19. However, these are easily identifiable factors, so their consideration could be useful in practice.
Besides, some factors deserve additional regard, although (due to our sample characteristics) we have excluded their presence in our final predictive models to avoid different kind of biases. COVID-19 and flu vaccination has been shown to be effective in reducing severity outcomes which is reflected on its inverse associations with mortality (for flu vaccination), need of ventilation and ICU admission (for COVID-19 vaccination). However, flu vaccination was found directly associated to the need of ventilation; this may be explained by the increased efforts of vaccination campaigns in those at higher risk (e.g. COPD patients), as well as a very low vaccine coverage. Anyway, the lack of effectiveness of COVID-19 vaccination for mortality, or even its perceived risk for the need for ventilation, may be biased on our participants by the timeliness of vaccination availability, as we already mentioned.
Finally, models did not fit the same when applied to each hospital’s data, showing several statistical differences. This was to be expected since the hospital datasets reflected important differences, e.g. more participants admitted to ICU and in need of ventilation at HUVN. However, working with both datasets together allowed us to build a more robust and useful predictive model for other Spanish hospitals. Notwithstanding, it should be noted that severity outcomes do not depend only on differences on SARS-CoV-2 incidence and strains, but also on characteristics of the catchment area of population and resources availability of each health care centre.
4.1. Limitations and Strengths
Firstly, COVID-19 mortality figures could be overestimated as cause of death as this was not included in the definition of the outcome (primary outcome was all-cause mortality during the index hospital admission, regardless of the recorded cause of death), since it would compromise the timeliness of the surveillance system.
On the other hand, data collection methods affected the data completeness of certain variables, resulting in missing data. Even though missing data was excluding only for the analysis of each variable (to prevent loss of power), this may have impacted the accuracy of results and their generalisability. Poor reporting from the health care workers when they were overloaded with work (especially at first cases) also may contribute to this type of bias. Additionally, covid-19 vaccination coverage data may be biased by vaccine availability and difficulty of calculation, as the population was vaccinated in a staggered manner according to age and other priority conditions.
In this sense, the lower predictive ability for the need of ventilation model could be explained by the fact that our analysis did not include specification of the type of ventilation (i.e. whether ventilation was mechanical or not). However, including only those patients with mechanical ventilation would not have substantially improved our results either, as the sample size would be smaller and thus also the power and reliability of our findings.
Despite these challenges, the design of definitions of the variables studied and data collection were carried out according to a published robust protocol from a European project of excellence (H2020). A wide list of clinical sociodemographic and clinical variables was assessed on a high sized sample. All this has implications for the high accuracy revealed by the high AUC scores obtained in the multivariate analysis. Furthermore, the study was conducted in two tertiary referral hospitals, located in different Spanish regions; therefore, it may be representative of the country population.
In addition, to our knowledge, this is the first study describing predictive models and nomogram tools on the phenotype association to mortality, ICU stay, and the need of ventilation, all at once, in Spanish COVID-19 hospitalised patients, and through a wide range of factors at admission, including underlying conditions, as well as symptoms and biochemical parameters.
Furthermore, this study contributed to the European I-MOVE-COVID-19 surveillance system, and laid the groundwork for launching COVID-19 Spanish official surveillance system. Likewise, it highlights the importance of monitoring hospitalised patients to understand phenotypes features, which may predict severe outcomes, in order to be useful to public health response, especially regarding emergent diseases.
5. Conclusions
This study assessed the clinical phenotype of Spanish COVID-19 hospitalised patients regarding three main severity outcomes by computing predictive models, which in turn have enabled the development of nomograms as clinical tools for prognosis.
Mortality, ICU admission and need for ventilation were found affected by the role of several risk factors (advanced age; diagnose of obesity, cancer, diabetes and neuromuscular disorders; presence of abdominal pain and cough; low blood levels of oxygen saturation, platelets and albumin; elevated blood levels of CPK, GGT, LDH, neutrophils, and elevated prothrombin time), as well as protective factors (diagnose of hypertension; presence of cough, sore throat and vomiting). Predictive models including these features allowed the construction of nomograms as clinical tools to assess the severity risk of illness for different outcomes. Furthermore, additional useful associations have been identified, such as vaccination status, number of underlying conditions (diseases and previous medical visits or admissions), and characteristics of the stay (such as time between events or the centre were being admitted).
These findings should be considered in order to improve COVID-19 patient management and strategic interventions including policy measures to prevent and combat COVID-19, allocating the available resources more efficiently, and avoiding the over-stressing of the healthcare system. Studies with similar approaches may be useful to address these issues on future emerging diseases.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Appendix A includes: Figure A1: Spanish COVID-19 hospitalised cases by age and sex (I-MOVE-COVID19 study); Table A1: Factors associated with death in Spanish COVID-19 hospitalised patients (I-MOVE-COVID19 study); Table A2: Factors associated with ICU admission in Spanish COVID-19 hospitalised patients (I-MOVE-COVID19 study); Table A3: Factors associated with ventilation in Spanish COVID-19 hospitalised patients (I-MOVE-COVID19 study).
Author Contributions
Conceptualization, Clara Mazagatos and Amparo Larrauri; Data curation, Miriam Latorre-Millán, María Rodríguez del Águila and Clara Mazagatos; Formal analysis, Miriam Latorre-Millán, María Rodríguez del Águila and Laura Clusa; Funding acquisition, Clara Mazagatos and Amparo Larrauri; Investigation, Miriam Latorre-Millán, María Rodríguez del Águila, Laura Clusa, Clara Mazagatos, María Fernández and Ana Milagro; Methodology, Miriam Latorre-Millán, María Rodríguez del Águila, Clara Mazagatos, Amparo Larrauri, María Fernández and Ana Milagro; Project administration, Miriam Latorre-Millán, Clara Mazagatos, Amparo Larrauri, María Fernández and Ana Milagro; Resources, Clara Mazagatos, Amparo Larrauri, María Fernández, Antonio Rezusta and Ana Milagro; Supervision, Amparo Larrauri, María Fernández and Ana Milagro; Visualization, Clara Mazagatos and Amparo Larrauri; Writing – original draft, Miriam Latorre-Millán and María Rodríguez del Águila; Writing – review & editing, Miriam Latorre-Millán, María Rodríguez del Águila, Laura Clusa, Clara Mazagatos, Amparo Larrauri, María Fernández, Antonio Rezusta and Ana Milagro.
Funding
This research was funded by European Union’s Horizon 2020 Research And Innovation Programme, grant number 101003673, called “Advancing knowledge for the clinical and public health response to the novel coronavirus epidemic”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and was approved by the Ethics Committee of Andalucía (code f12f8377d78c34a25d6935eff535cd26715e2b8c and date of 2020/04/15).
Informed Consent Statement
Patient consent was waived due to the pandemic emergency exemption and because these data were included as part of the pilot surveillance system of the future integrated respiratory surveillance in Spain [5]. Nonetheless, only summary data were extracted to minimize the risk of disclosure.
Data Availability Statement
Due to data protection policies in the hospitals, the complete dataset used for this study is not publicly available but data can be accessed upon request to the corresponding author.
Acknowledgments
We thank all the staff involved in the IMOVE-COVID-19 study, including collaborators at the hospitals (who participated in data collection, data production and data register, including Laboratories and Admission Units), as well as colleagues from the Epidemiology National Centre, Epiconcept, and the I-MOVE-COVID-19 network for their support with the implementation of the study.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study, in neither the collection, analyses, nor interpretation of data, the writing of the manuscript, or in the decision to publish the results.
References
- World Health Organization. WHO COVID-19: Case Definitions Available online: https://iris.who.int/bitstream/handle/10665/360579/WHO-2019-nCoV-Surveillance-Case-Definition-2022.1-eng.pdf?sequence=1 (accessed on 25 July 2024).
- I-MOVE-COVID-19 network. I-MOVE-COVID-19 Available online: https://www.imoveflu.org/i-move-covid-19/ (accessed on 25 July 2024).
- I-MOVE network. I_MOVE Influenza - Monitoring Vaccine Effectiveness in Europe Available online: https://www.imoveflu.org/ (accessed on 25 July 2024).
- Mutch, H.; Young, J.J.; Sadiq, F.; Rose, A.M.; Evans, J.M.; European COVID-19 hospital surveillance analysis writing group Enhanced Surveillance of Hospitalised COVID-19 Patients in Europe: I-MOVE-COVID-19 Surveillance Network, February 2020 to December 2021. Euro Surveill. Bull. Eur. Sur Mal. Transm. Eur. Commun. Dis. Bull. 2023, 28, 2200669. [CrossRef]
- Mazagatos, C.; Delgado-Sanz, C.; Monge, S.; Pozo, F.; Oliva, J.; Sandonis, V.; Gandarillas, A.; Quiñones-Rubio, C.; Ruiz-Sopeña, C.; Gallardo-García, V.; et al. COVID-19 Vaccine Effectiveness against Hospitalization Due to SARS-CoV-2: A Test-Negative Design Study Based on Severe Acute Respiratory Infection (SARI) Sentinel Surveillance in Spain. Influenza Other Respir. Viruses 2022, 16, 1014–1025. [CrossRef]
- Richards, F.; Kodjamanova, P.; Chen, X.; Li, N.; Atanasov, P.; Bennetts, L.; Patterson, B.J.; Yektashenas, B.; Mesa-Frias, M.; Tronczynski, K.; et al. Economic Burden of COVID-19: A Systematic Review. Clin. Outcomes Res. CEOR 2022, 14, 293–307. [CrossRef]
- COVID-19 Variants | WHO COVID-19 Dashboard Available online: https://data.who.int/dashboards/covid19/variants (accessed on 25 July 2024).
- Zhang, X.; Tan, Y.; Ling, Y.; Lu, G.; Liu, F.; Yi, Z.; Jia, X.; Wu, M.; Shi, B.; Xu, S.; et al. Viral and Host Factors Related to the Clinical Outcome of COVID-19. Nature 2020, 583, 437–440. [CrossRef]
- Fadl, N.; Ali, E.; Salem, T.Z. COVID-19: Risk Factors Associated with Infectivity and Severity. Scand. J. Immunol. 2021, 93, e13039. [CrossRef]
- Gutiérrez-Gutiérrez, B.; Del Toro, M.D.; Borobia, A.M.; Carcas, A.; Jarrín, I.; Yllescas, M.; Ryan, P.; Pachón, J.; Carratalà, J.; Berenguer, J.; et al. Identification and Validation of Clinical Phenotypes with Prognostic Implications in Patients Admitted to Hospital with COVID-19: A Multicentre Cohort Study. Lancet Infect. Dis. 2021, 21, 783–792. [CrossRef]
- Factsheet on COVID-19 Available online: https://www.ecdc.europa.eu/en/infectious-disease-topics/z-disease-list/covid-19/factsheet-covid-19 (accessed on 25 July 2024).
- Talukder, A.; Razu, S.R.; Alif, S.M.; Rahman, M.A.; Islam, S.M.S. Association Between Symptoms and Severity of Disease in Hospitalised Novel Coronavirus (COVID-19) Patients: A Systematic Review and Meta-Analysis. J. Multidiscip. Healthc. 2022, 15, 1101–1110. [CrossRef]
- Shoaib, N.; Noureen, N.; Munir, R.; Shah, F.A.; Ishtiaq, N.; Jamil, N.; Batool, R.; Khalid, M.; Khan, I.; Iqbal, N.; et al. COVID-19 Severity: Studying the Clinical and Demographic Risk Factors for Adverse Outcomes. PloS One 2021, 16, e0255999. [CrossRef]
- Battaglini, D.; Lopes-Pacheco, M.; Castro-Faria-Neto, H.C.; Pelosi, P.; Rocco, P.R.M. Laboratory Biomarkers for Diagnosis and Prognosis in COVID-19. Front. Immunol. 2022, 13, 857573. [CrossRef]
- Mazzalai, E.; Giannini, D.; Tosti, M.E.; D’Angelo, F.; Declich, S.; Jaljaa, A.; Caminada, S.; Turatto, F.; De Marchi, C.; Gatta, A.; et al. Risk of Covid-19 Severe Outcomes and Mortality in Migrants and Ethnic Minorities Compared to the General Population in the European WHO Region: A Systematic Review. J. Int. Migr. Integr. 2023, 1–31. [CrossRef]
- Charkoftaki, G.; Aalizadeh, R.; Santos-Neto, A.; Tan, W.Y.; Davidson, E.A.; Nikolopoulou, V.; Wang, Y.; Thompson, B.; Furnary, T.; Chen, Y.; et al. An AI-Powered Patient Triage Platform for Future Viral Outbreaks Using COVID-19 as a Disease Model. Hum. Genomics 2023, 17, 80. [CrossRef]
- Rello, J.; Storti, E.; Belliato, M.; Serrano, R. Clinical Phenotypes of SARS-CoV-2: Implications for Clinicians and Researchers. Eur. Respir. J. 2020, 55, 2001028. [CrossRef]
- Lusczek, E.R.; Ingraham, N.E.; Karam, B.S.; Proper, J.; Siegel, L.; Helgeson, E.S.; Lotfi-Emran, S.; Zolfaghari, E.J.; Jones, E.; Usher, M.G.; et al. Characterizing COVID-19 Clinical Phenotypes and Associated Comorbidities and Complication Profiles. PloS One 2021, 16, e0248956. [CrossRef]
- Azoulay, E.; Zafrani, L.; Mirouse, A.; Lengliné, E.; Darmon, M.; Chevret, S. Clinical Phenotypes of Critically Ill COVID-19 Patients. Intensive Care Med. 2020, 46, 1651–1652. [CrossRef]
- Berenguer, J.; Ryan, P.; Rodríguez-Baño, J.; Jarrín, I.; Carratalà, J.; Pachón, J.; Yllescas, M.; Arriba, J.R.; COVID-19@Spain Study Group; Fundación SEIMC-GESIDA; et al. Characteristics and Predictors of Death among 4035 Consecutively Hospitalized Patients with COVID-19 in Spain. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2020, 26, 1525–1536. [CrossRef]
- Rose, A.M.; Kissling, E.; Valenciano, M. European Study of Risk Factors for Severe Disease among Hospitalised COVID-19 Patients: I-MOVE-COVID-19 Protocol. 2021. [CrossRef]
- Rose, A.M.; Kissling, E.; Valenciano, M. European Study of COVID-19 Vaccine Effectiveness against Hospitalised SARI Patients Laboratory-Confirmed with SARS-CoV-2: I-MOVE-COVID-19 Generic Protocol. 2021. [CrossRef]
- Ladbury, G.; Rose, A.M.; Kissling, E.; Valenciano, M. COVID-19 European Hospital Surveillance: I-MOVE-COVID-19 Draft Generic Protocol. 2021. [CrossRef]
- Global Burden of Disease Study 2019 (GBD 2019) Data Resources | GHDx Available online: https://ghdx.healthdata.org/gbd-2019 (accessed on 26 July 2024).
- Tobacco Consumption Statistics Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Tobacco_consumption_statistics (accessed on 26 July 2024).
- Miller, L.J.; Lu, W. These Are the Economies With the Most (and Least) Efficient Health Care. Bloomberg.com 2018.
- Schwab, K. The Gobal Competitiveness Report, 2019; World Economic Forum, 2020;
- Jovell, A.; Blendon, R.J.; Navarro, M.D.; Fleischfresser, C.; Benson, J.M.; DesRoches, C.M.; Weldon, K.J. Public Trust in the Spanish Health-Care System. Health Expect. 2007, 10, 350–357. [CrossRef]
- Wendt, C.; Kohl, J.; Mischke, M.; Pfeifer, M. How Do Europeans Perceive Their Healthcare System? Patterns of Satisfaction and Preference for State Involvement in the Field of Healthcare. Eur. Sociol. Rev. 2010, 26, 177–192. [CrossRef]
- Wu, G.; Yang, P.; Xie, Y.; Woodruff, H.C.; Rao, X.; Guiot, J.; Frix, A.-N.; Louis, R.; Moutschen, M.; Li, J.; et al. Development of a Clinical Decision Support System for Severity Risk Prediction and Triage of COVID-19 Patients at Hospital Admission: An International Multicentre Study. Eur. Respir. J. 2020, 56, 2001104. [CrossRef]
- Wehrfritz, A.; Schmidt, J.; Bremer, F.; Lang, A.; Welzer, J.; Castellanos, I. Ethical Conflicts Associated with COVID-19 Pandemic, Triage and Frailty—Unexpected Positive Disease Progression in a 90-year-old Patient: A Case Report. Clin. Case Rep. 2023, 11, e7710. [CrossRef]
- Tanzadehpanah, H.; Lotfian, E.; Avan, A.; Saki, S.; Nobari, S.; Mahmoodian, R.; Sheykhhasan, M.; Froutagh, M.H.S.; Ghotbani, F.; Jamshidi, R.; et al. Role of SARS-COV-2 and ACE2 in the Pathophysiology of Peripheral Vascular Diseases. Biomed. Pharmacother. 2023, 166, 115321. [CrossRef]
- World Health Organization Clinical Management of Severe Acute Respiratory Infection When COVID-19 Is Suspected. Interim Guidance. Available online: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected (accessed on 25 July 2024).
- Zayet, S.; Gendrin, V.; Klopfenstein, T. Natural History of COVID-19: Back to Basics. New Microbes New Infect. 2020, 38, 100815. [CrossRef]
Figure 1.
Spanish COVID-19 hospitalised cases by month (I-MOVE-COVID19 study).
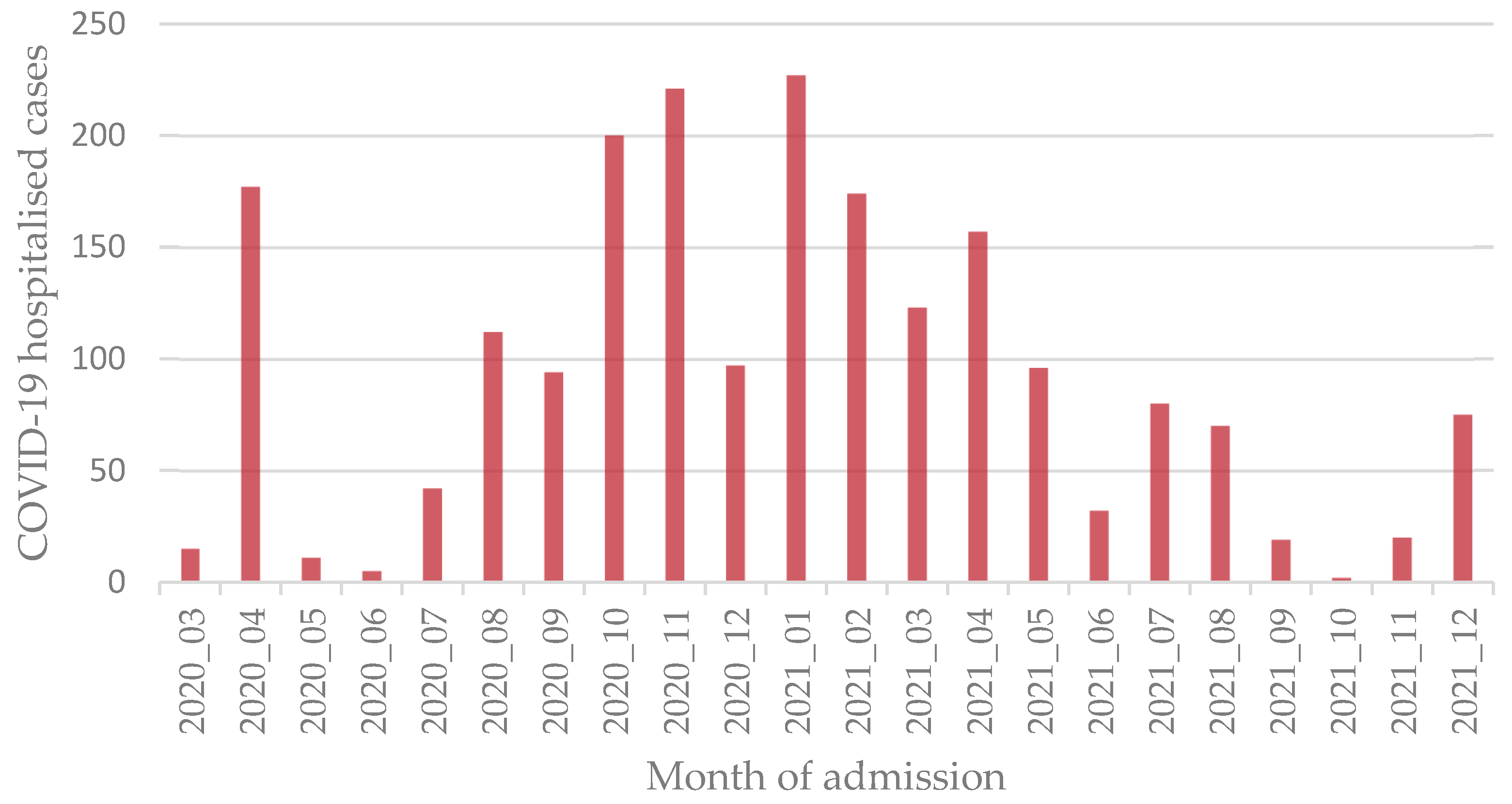
Figure 2.
Predictive factors associated with ventilation, ICU admission and death in Spanish hospitalised patients. I-MOVE-COVID19 study.
Figure 2.
Predictive factors associated with ventilation, ICU admission and death in Spanish hospitalised patients. I-MOVE-COVID19 study.
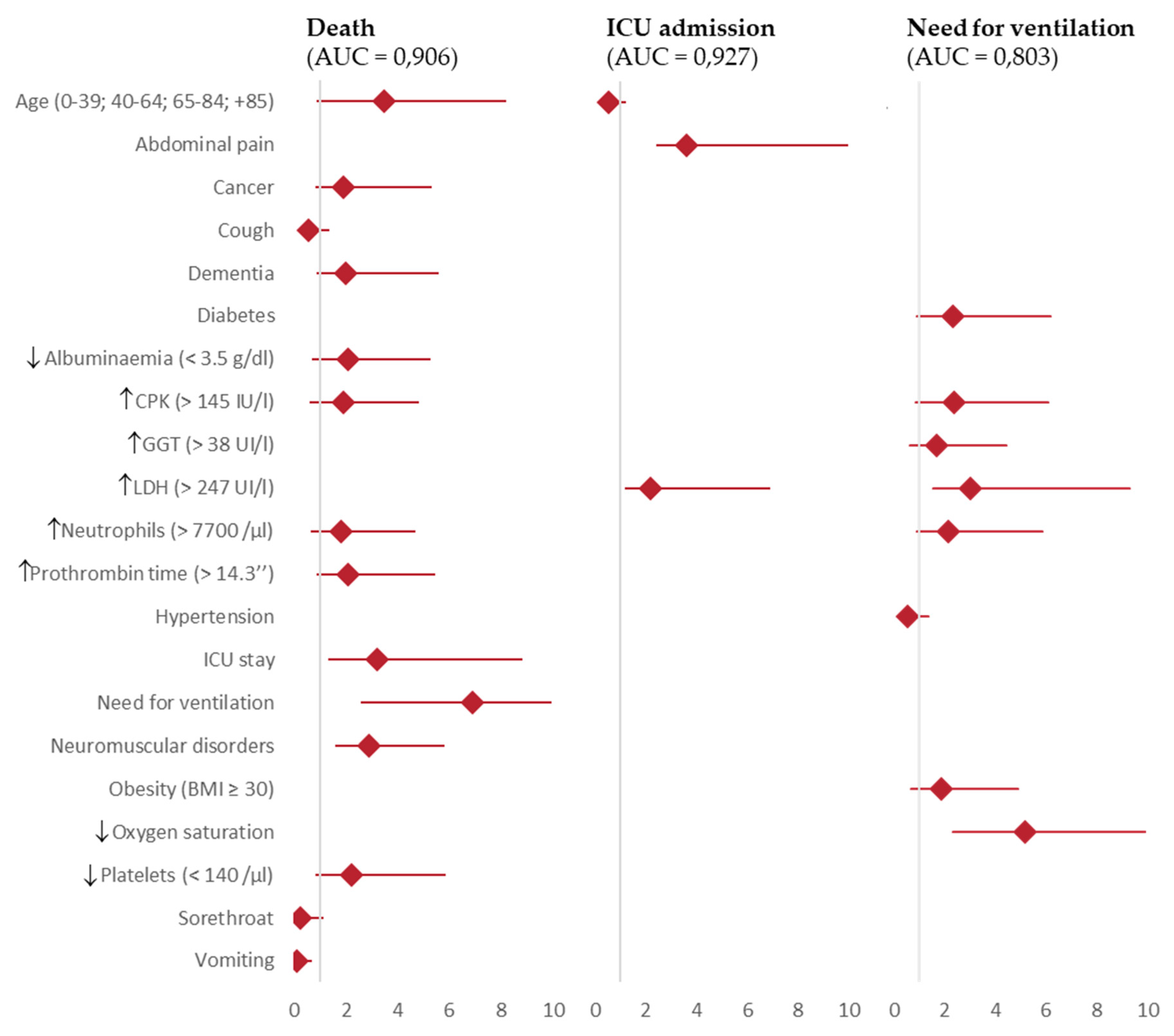
Figure 3.
Nomograms for predicting COVID-19 severity outcomes in Spanish hospitalised patients. I-MOVE-COVID19 study. A) Death, B) ICU admission, C) Need for ventilation.
Figure 3.
Nomograms for predicting COVID-19 severity outcomes in Spanish hospitalised patients. I-MOVE-COVID19 study. A) Death, B) ICU admission, C) Need for ventilation.
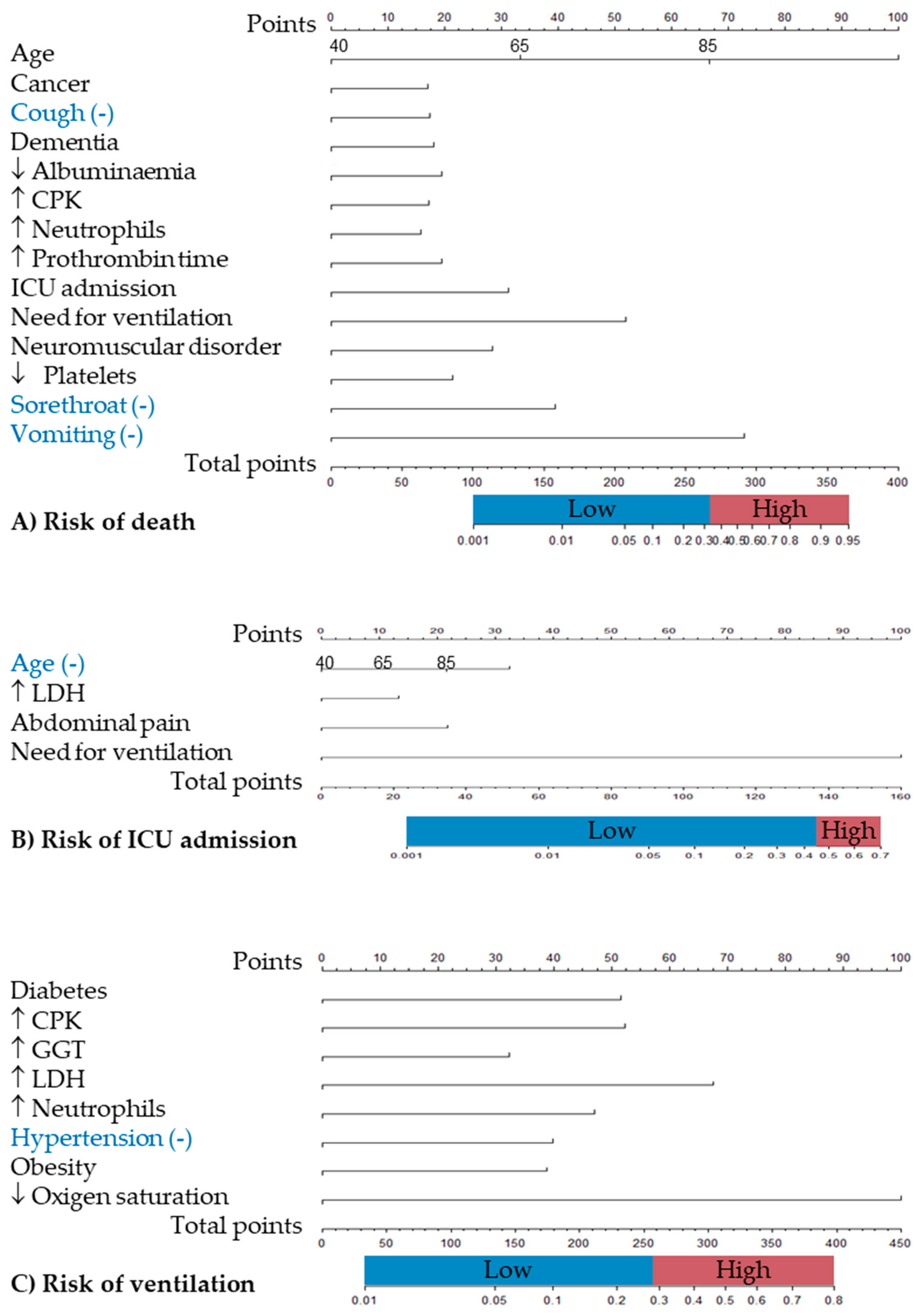

Table 1.
Epidemiological and clinical characteristics of Spanish COVID-19 hospitalized patients, by sex (I-MOVE-COVID19 study).
Table 1.
Epidemiological and clinical characteristics of Spanish COVID-19 hospitalized patients, by sex (I-MOVE-COVID19 study).
| All 2050 (100%) |
Women 961 (46.8%) |
Men 1089 (53.1%) |
p value | |
|---|---|---|---|---|
| Sociodemographic and clinical factors | ||||
| Age, grouped (0-39; 40-64; 65-84; 85+ years) | <0.001 | |||
| Age 0-39 years | 215 (10.5) | 106 (11.0) | 109 (10.0) | |
| Age 40-64 years | 810 (39.5) | 332 (34.5) | 478 (43.9) | |
| Age 65-84 years | 723 (35.3) | 359 (37.4) | 364 (33.5) | |
| Age 85+ years | 301 (14.7) | 164 (17.1) | 137 (12.6) | |
| Centre (HUVN) | 833 (40.6) | 374 (38.9) | 459 (42.1) | 0.137 |
| Covid-19 vaccinated (only when available) | 215 (23.6) | 91 (22.1) | 124 (24.8) | 0.345 |
| Flu vaccinated | 794 (39.1) | 394 (41.4) | 400 (37.1) | 0.050 |
| Number of previous hospitalizations (last year), mean ± SD | 2.5 ± 3.2 | 2.4 ± 2.1 | 2.7 ± 3.8 | 0.653 |
| Number of previous medical visits (last year), mean ± SD | 6.8 ± 7.1 | 7.7± 7.4 | 6.1± 6.9 | 0.009 |
| Previous medical visits last year >12 | 89 (15.2) | 48 (18.4) | 41 (12.6) | 0.053 |
| Outcomes | ||||
| Mortality | 309 (15.1) | 138 (14.4) | 171 (15.7) | 0.402 |
| ICU stay | 179 (8.8) | 70 (39.1) | 109 (60.9) | 0.031 |
| Need for ventilation | 548 (27.4) | 223 (23.7) | 325 (30.5) | <0.001 |
| Time between events | ||||
| Days from onset to admission, mean ± SD | 6.6 ± 12.4 | 6.2 ± 12.7 | 6.9 ± 12.1 | 0.166 |
| Days from onset to ICU, mean ± SD | 9.9 ± 4.6 | 9.7 ± 5.1 | 9.9 ± 4.2 | 0.750 |
| Days of stay, mean ± SD | 12.2 ± 14.6 | 11.9 ± 16.4 | 12.6 ± 12.7 | 0.263 |
| Days of stay (> 7 days) | 1248 (60.9) | 569 (59.7) | 679 (62.8) | 0.159 |
| Days of ICU stay, mean ± SD | 23.9 ± 20.2 | 23.9 ± 21.9 | 24.0 ± 19.2 | 0.969 |
| Days from admission to ICU, mean ± SD | 3.8 ± 3.3 | 3.8 ± 3.8 | 3.8 ± 2.9 | 0.881 |
| Days from admission to ICU >7 | 14 (7.8) | 6 (8.6) | 8 (7.3) | 0.765 |
| Underlying conditions | ||||
| Anaemia | 241 (11.8) | 138 (14.4) | 103 (9.5) | <0.001 |
| Asthma | 171 (8.4) | 117 (12.2) | 54 (5.0) | <0.001 |
| Body mass index (BMI), mean ± SD | 29.4 ± 5.7 | 29.4 ± 6.1 | 29.4 ± 5.3 | 0.831 |
| Cancer | 161 (7.9) | 70 (7.3) | 91 (8.4) | 0.376 |
| Dementia | 197 (9.6) | 111 (11.6) | 86 (7.9) | 0.005 |
| Diabetes | 487 (23.8) | 220 (22.9) | 267 (24.5) | 0.396 |
| Heart disease | 405 (19.8) | 161 (16.8) | 244 (22.4) | 0.002 |
| Hypertension | 978 (47.8) | 461 (48.1) | 517 (47.6) | 0.818 |
| Ictus | 124 (6.1) | 50 (5.2) | 74 (6.8) | 0.134 |
| Immunodeficiency | 39 (1.9) | 16 (1.7) | 23 (2.1) | 0.464 |
| Kidney disease | 211 (10.3) | 103 (10.8) | 108 (9.9) | 0.550 |
| Lung disease | 216 (10.6) | 69 (7.2) | 147 (13.5) | <0.001 |
| Liver disease | 87 (4.3) | 33 (3.4) | 54 (5.0) | 0.089 |
| Neuromuscular disorders | 110 (5.4) | 50 (5.2) | 60 (5.5) | 0.767 |
| Obesity | 548 (48.4) | 287 (50.7) | 261 (46.0) | 0.115 |
| Rheumatic disease | 501 (24.5) | 290 (30.2) | 211 (19.4) | <0.001 |
| Symptoms | ||||
| Abdominal pain | 59 (2.9) | 34 (3.6) | 25 (2.3) | 0.098 |
| Ageusia | 159 (7.9) | 86 (9.0) | 73 (6.8) | 0.061 |
| Anosmia | 169 (8.4) | 88 (9.3) | 81 (7.5) | 0.061 |
| Chest pain | 263 (12.9) | 147 (15.4) | 116 (10.8) | 0.002 |
| Chills | 67 (3.3) | 30 (3.2) | 37 (3.5) | 0.706 |
| Confusion | 76 (3.7) | 37 (3.9) | 39 (3.6) | 0.774 |
| Coryza | 67 (3.3) | 46 (4.8) | 21 (2.0) | <0.001 |
| Cough | 1435 (70.6) | 685 (71.9) | 750 (69.5) | 0.242 |
| Diarrhoea | 368 (18.1) | 196 (20.5) | 172 (16.0) | 0.008 |
| Dizzy | 92 (4.5) | 47 (4.9) | 45 (4.2) | 0.426 |
| Dyspnoea | 1334 (65.6) | 629 (65.9) | 705 (65.3) | 0.756 |
| Fever | 680 (33.5) | 286 (30.0) | 394 (36.6) | 0.002 |
| Feverish | 1365 (67.1) | 637 (66.6) | 728 (67.5) | 0.666 |
| General deterioration | 671 (33.1) | 346 (36.2) | 325 (30.2) | 0.004 |
| Headache | 327 (16.1) | 171 (17.9) | 156 (14.5) | 0.036 |
| Malaise | 1249 (61.5) | 588 (61.6) | 661 (61.4) | 0.928 |
| Myalgia | 481 (23.7) | 236 (24.7) | 245 (22.8) | 0.298 |
| Nausea | 159 (7.8) | 97 (10.2) | 62 (5.8) | <0.001 |
| Sore throat | 102 (5.0) | 53 (5.6) | 49 (4.6) | 0.307 |
| Tachycardia | 572 (28.1) | 257 (26.8) | 315 (29.2) | 0.225 |
| Vomiting | 130 (6.4) | 83 (8.7) | 47 (4.4) | <0.001 |
| Clinical measures | ||||
| SBP (mm Hg), mean ± SD | 129 ± 21.2 | 126.5± 21.6 | 131.1± 20.5 | <0.001 |
| SBP < 90 mm Hg | 42 (2.2) | 29 (3.3) | 13 (1.3) | 0.004 |
| DBP (mm Hg), mean ± SD | 74.4 ± 13.4 | 73.4± 13.7 | 75.3± 13.1 | 0.002 |
| DBP < 60 mm Hg | 228 (12.2) | 123 (13.9) | 105 (10.7) | 0.033 |
| Heart rate (bpm), mean ± SD | 91 ± 21.2 | 91.1 ± 21.0 | 90.8 ± 21.4 | 0.728 |
| Long QT | 50 (6.5) | 16 (4.3) | 34 (8.5) | 0.020 |
| Oxygen saturation (%), mean ± SD | 92.2 ± 5.7 | 92.4 ± 5.7 | 92.1 ± 5.7 | 0.174 |
| Low oxygen saturation | 1134 (62.2) | 500 (58.8) | 634 (65.2) | 0.005 |
| Respiratory rate (rpm), mean ± SD | 25.8 ± 26.6 | 27.9 ± 37.2 | 23.8 ± 8.1 | 0.142 |
| Biochemical alterations | ||||
| Hypoalbuminaemia (albumin < 3.5 g/dl) | 469 (28.1) | 230 (29.9) | 239 (26.6) | 0.128 |
| ALT > 35 UI/l | 676 (33.7) | 259 (27.3) | 417 (39.3) | <0.001 |
| AST > 35UI/l | 917 (46.9) | 384 (41.7) | 533 (51.5) | <0.001 |
| Hyperbilirubinaemia >1.2 mg/dl | 87 (4.4) | 16 (1.7) | 71 (6.8) | <0.001 |
| C-reactive protein > 1 mg/dl | 1984 (98.6) | 931 (98.5) | 1053 (98.7) | 0.746 |
| CPK > 145 IU/L | 366 (25.5) | 115 (17.9) | 251 (31.6) | <0.001 |
| D-dimer (> 500 μg/ml | 1327 (68.0) | 649 (71.2) | 678 (65.2) | 0.005 |
| Eosinophilia (> 500 eosinophils/μl) | 92 (4.6) | 47 (5.0) | 45 (4.2) | 0.420 |
| Ferritin > 200 ng/ml | 1970 (99.6) | 922 (99.4) | 1048 (99.8) | 0.111 |
| GGT > 38 UI/l | 1126 (57.0) | 467 (50.5) | 659 (62.8) | <0.001 |
| LDH > 247 UI/L | 1462 (77.5) | 679 (77.0) | 783 (78.0) | 0.602 |
| Neutrophilopenia (< 1500 neutrophils/μl) | 40 (2.0) | 21 (2.2) | 19 (1.8) | 0.485 |
| Neutrophilia (> 7700 neutrophils /μl) | 374 (18.4) | 157 (16.5) | 217 (20.2) | 0.030 |
| Thrombocytopenia (< 140 platelets /μl) | 350 (17.3) | 123 (12.9) | 227 (21.2) | <0.001 |
| Thrombocytophilia (> 370 platelets /μl) | 115 (5.7) | 66 (6.9) | 49 (4.6) | 0.022 |
| Prothrombin time > 14.3 seconds | 335 (17.1) | 123 (13.4) | 212 (20.3) | <0.001 |
| Urea in blood > 20 mg/ml | 1902 (94.9) | 858 (91.6) | 1044 (97.8) | <0.001 |
| Data is expressed by absolute (n) and relative (%) frequencies for categorical variables, and by mean (x̅) ± standard deviation (SD) for quantitative variables. Figures in bold point for significant differences (p value ≤ 0.05). Abbreviations: HUVN: Virgen de las Nieves University Hospital, ICU: Intensive Care Unit, SBP: systolic blood pressure, DBP: diastolic blood pressure, ALT: alanine transaminase, AST: aspartate transaminase, CPK: creatinine phosphokinase, GGT: gamma-glutamyl transferase, LDH: lactate dehydrogenase. The reference categoryfor age is 0-40 years. | ||||
Table 2.
Predictive factors for ventilation, ICU admission and death in Spanish hospitalised patients (I-MOVE-COVID19 study).
Table 2.
Predictive factors for ventilation, ICU admission and death in Spanish hospitalised patients (I-MOVE-COVID19 study).
| Death Adjusted OR (IC 95%) |
ICU admission Adjusted OR (IC 95%) |
Need for ventilation Adjusted OR (IC 95%) |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| All | HUMS | HUVN | All | HUMS | HUVN | All | HUMS | HUVN | |
| Age (<40; 40-64; 65-84; +85 years) | 3.5 (2.6 – 4.7)*** | 4.2 (2.4-7.4)*** | 3.1 (2.1-4.6)*** | 0.5 (0.4 – 0.7)*** | 0.6 (0.3-0.9)* | 0.5 (0.4-0.7)*** | |||
| Abdominal pain | 3.6 (1.2 – 10.8)* | 3.2 (0.4-28.2) | 3.8 (1.1-13.6)* | ||||||
| Cancer | 1.9 (1.04 – 3.4)* | 3.0 (1.1-8.5)* | 1.7 (0.8-3.8) | ||||||
| Cough | 0.5 (0.4 – 0.8)** | 0.6 (0.3-1.2) | 0.6 (0.3-1.0)* | ||||||
| Dementia | 2.0 (1.1 – 3.6)* | 5.3 (2.1-13.5)*** | 0.6 (0.2-1.6) | ||||||
| Diabetes | 2.3 (1.4 – 3.9)*** | 2.5 (1.4-4.6)** | 1.9 (0.6-5.6) | ||||||
| Hypoalbuminaemia (< 3.5 g/dl) | 2.1 (1.3 – 3.2)*** | 1.2 (0.6-2.3) | 3.9 (2.0-7.9)*** | ||||||
| Elevated CPK (> 145 IU/l) | 1.9 (1.2 – 2.9)** | 1.7 (0.8-3.4) | 2.1 (1.2-3.8)* | 2.4 (1.5 – 3.7)*** | 2.2 (1.3-3.9)** | 2.4 (0.9-6.6) | |||
| Elevated GGT (> 38 UI/l) | 1.7 (1.1 – 2.7)* | 1.3 (0.8-2.3) | 2.8 (0.9-8.8) | ||||||
| Elevated LDH(> 247 UI/l) | 2.2 (1.0 – 4.7)* | 2.5 (0.4-28.2) | 1.9 (0.7-5.6) | 3.0 (1.5 – 6.3)** | 3.2 (1.4-7.5)** | 0.8 (0.1-5.5) | |||
| Elevated neutrophils (> 7700 /μl) | 1.8 (1.1 – 2.9)* | 4.4 (2.0-9.4)*** | 1.3 (0.7-2.4) | 2.2 (1.3 – 3.7)** | 1.8 (0.9-3.4) | 2.4 (0.7-8.3) | |||
| Elevated prothrombin time (> 14.3’’) | 2.1 (1.2 – 3.3)** | 3.4 (1.6-7.1)*** | 1.2 (0.6-2.4) | ||||||
| Hypertension | 0.5 (0.3 – 0.8)** | 0.7 (0.4-1.2) | 0.3 (0.1-0.8)* | ||||||
| ICU stay | 3.2 (1.8 – 5.6)*** | 4.0 (1.2-12.8)* | 2.5 (1.3-4.9)** | ||||||
| Need for ventilation | 6.9 (4.3-11.1)*** | 11.5 (4.7-28.2)*** | 9.9 (4.5-21.7)*** | 371 (90.8 – 1516.8)*** | 213.4 (50.3-906.3)*** | 5.6e-8 (0-inf) | |||
| Neuromuscular disorders | 2.9 (1.2 – 2.9)** | 6.9 (2.4-19.5)*** | 0.5 (0.1-2.4) | ||||||
| Obesity (BMI ≥ 30) | 1.9 (1.2 – 3.0** | 1.2 (0.7-2.2) | 0.5 (0.1-3.3) | ||||||
| Low oxygen saturation | 5.2 (2.8 – 9.4)*** | 4.9 (2.4-10.0)*** | 4.9 (1.3-19.3)* | ||||||
| Low platelets (< 140 /μl) | 2.2 (1.4 – 3.6)*** | 2.2 (1.0-4.6)* | 2.7 (1.4-5.3)** | ||||||
| Sorethroat | 0.2 (0.1 – 0.8)* | 1.4e-8 (0.0-inf) | 0.5 (0.1-2.0) | ||||||
| Vomiting | 0.1 (0.0 – 0.6)* | 2.9e-8 (0.0-inf) | 0.1 (0.0-1.0)) | ||||||
| Area under ROC curve | 0.906 | 0.939 | 0.896 | 0.927 | 0.944 | 0.887 | 0.803 | 0.789 | 0.755 |
| Nagelkerke’s R2 | 0.471 | 0.571 | 0.462 | 0.520 | 0.522 | 0.480 | 0.294 | 0.231 | 0.266 |
| Accuracy | 0.881 | 0.918 | 0.873 | 0.905 | 0.950 | 0.837 | 0.813 | 0.855 | 0.663 |
| Specificity | 0.967 | 0.973 | 0.961 | 0.984 | 0.996 | 0.963 | 0.956 | 0.989 | 0.605 |
| Sensivity | 0.352 | 0.532 | 0.388 | 0.141 | 0.073 | 0.165 | 0.279 | 0.909 | 0.712 |
| Abbreviations: CPK: creatinine phosphokinase, GGT: gamma-glutamyl transferase, LDH: lactate dehydrogenase ICU: Intensive Care Unit, BMI: body mass index. p value: ***≤0.001; **≤0.01; *≤0.05. The reference for age category is 0-40 years. All data were used for the multivariate model adjustment. | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



