
Submitted:
17 September 2024
Posted:
17 September 2024
You are already at the latest version
Abstract
The EXO+ hip protector was developed to minimize the risk of hip fractures in seniors following falls. This study evaluated its usability in a Singapore nursing home from the perspective of staff, focusing on Learnability, Efficiency, and Satisfaction. A mixed-method design was employed, with nursing home residents wearing the EXO+ daily for 8 weeks. Quantitative data on wear time was collected alongside qualitative insights from four repeated focus group discussions with care staff. In total, 15 residents (including 8 residents with cognitive impairments) and 9 staff participated. The analysis revealed six themes and fourteen subthemes related to EXO+’s usability. Residents wore the device for an average of 1.54 hours per day, with those having cognitive impairments showing increased wear times, especially in the mornings and on weekdays. Findings indicated that the EXO+ was learnable and satisfactory for nursing home use, provided there are adequate supporting features. The efficiency of the EXO+ was not fully measured since no falls were reported during the study period. The study offers valuable insights for potential design modifications and workflow adaptations to enhance the implementation of hip protectors in healthcare settings, highlighting facilitators and barriers to support device uptake.
Keywords:
Hip protector
; Nursing home
; Focus Group Discussion
; Singapore
; Usability Study
; Fall Incidence
1. Introduction
Falls pose a significant public health concern, ranking as the fifth leading cause of death in the older adult population globally (World Health Organisation [WHO], 2008). These incidents are exacerbated by age-related factors, such as impaired balance and mobility, medication, muscle weakness, the use of walking aids, and cognitive impairment (Montero-Odasso et al., 2022; Tyrovolas et al., 2016). Notably, falls lead to severe injuries, with hip fractures being the most common and having the most debilitating consequences in older individuals (Stevens et al., 2006; Rau et al., 2014), such as increased morbidity, disability, and mortality (Yong et al., 2019).
Institutionalised older adults have the highest incidence of falls, with an average of 40% of residents falling each year (Rubenstein and Josephson, 2002). The same prevalence number was found in a Singapore study where 42% of residents in a nursing home had fallen at least once in the last 2.5 years (Yap et al., 2003). The high occurrence of falls in nursing home settings is attributed to advanced age, frailty, environmental factors, and co-morbidities including gait disorders, cognitive decline, and orthostatic hypotension (Romli et al., 2017). This underscores the need for effective strategies to mitigate fall-related risks, particularly the risk of hip fractures.
Globally, various strategies have been trialed and employed to reduce fall rates and their impacts in nursing homes. These strategies include patient education, fall detection systems (Takatou et al., 2021) and exercise programs (Hewitt et al., 2018, Pepera et al., 2023). Exercise and physical training interventions have been implemented to improve muscle strength and balance to reduce falls in older adults residing in nursing homes (Montero-Odasso et al., 2022). However, while these strategies reduce the risks of falls, older adults who fall remain susceptible to adverse effects post-falls.
Post-fall hip protection interventions have been explored to understand their efficacy in reducing fall impacts. High-tech products such as the Anti-Fall Smart Vest System were introduced as a cushion that automatically deploys upon detection of a fall (Chen, 2022). However, due to their high costs, it is difficult for these interventions to be adopted at scale among most older adults, especially those in nursing homes. Cheaper alternatives like hip protectors have gained attention for their potential to prevent hip fractures post-falls. There are two primary types of hip protectors available. The first type involves a hard shell or shield that redirects the impact of a fall away from the trochanteric region and towards the surrounding soft tissues (Santesso et al., 2014). The second type consists of soft paddings that offer cushioning and absorb energy from the protected area (Cameron et al., 2002). Despite their potential benefits, hip protector production has remained largely unregulated, complicating the assessment of their effectiveness and compliance (Parker et al., 2006).
Hip protector usage in nursing homes has been demonstrated to reduce the risk of hip fractures in various studies (Sawka et al., 2005). Nonetheless, several studies have highlighted difficulties related to residents' adherence to wearing protectors (Santesso et al., 2014) due to factors such as discomfort and urinary incontinence (van Schoor, 2002). In Singapore, the use of hip protectors among nursing home residents is currently lacking. The only fall prevention clinical guideline in Singapore, published in 2005, didn’t recommend hip protectors, primarily due to poor acceptability and non-compliance resulting from discomfort and inadequate fit (Health Promotion Board, 2005). Given the hot and humid weather in Singapore, the Singapore Institute of Technology (SIT) developed a hip protector called EXO+ in 2018. The EXO+ hip protector is designed to minimise the risk of hip fractures post falls and features a lightweight and breathable mesh fabric, complemented by an elastic band at the hips. It is worn externally to prevent overheating and is convenient to use with Velcro straps. A recent pilot study on the EXO+ Hip Protector received positive feedback from inpatients in a community hospital in Singapore (SIT, 2022). However, no trials on the use of the EXO+ hip protector have been conducted in any local nursing homes.
Hence, this study aimed to comprehensively assess the usability of the EXO+ hip protector in a nursing home setting from the perspectives of the care staff. This study delved into three pivotal dimensions of usability crucial in practical applications: efficiency, learnability and satisfaction (Hornboek, 2006). Efficiency refers to the resources expended for the accuracy and completeness of hip protector usage. Learnability refers to the users’ attitude toward the ease of learning to use the hip protector. Satisfaction measures freedom from discomfort and positive attitudes toward the use of the product.
2. Materials and Methods
2.1. Design
A pilot usability study using a mixed-method design was conducted to understand the usability of the EXO+ hip protector through the experiences of the staff of a nursing home in Singapore. Due to the novel nature of the EXO+, the study follows a formative usability testing evaluation to detect issues with the hip protector and eliminate usability problems (Lewis, 2014). The quantitative data included the nursing home residents’ wear time of the EXO+, physical functions, cognitive functions, independence in self-care, history of falls and the number of fall incidents. The qualitative data included repeated focus group discussions (r-FGD) with care staff. The triangular design model was used to integrate the quantitative and qualitative data gathered from this study to achieve our study objectives (Creswell et al., 2004). Ethics approval was obtained from the Institutional Review Board of the Singapore Institute of Technology in 2023 (Institutional Review Board number: RECAS-0006) and the St Luke’s Eldercare Research Ethics Committee (Reference number: EX23002).
2.2. Participants
Eligible residents were recruited through convenience sampling from two wards of the participating nursing home. The inclusion criteria included: 1) aged 60 and above; 2) high fall risk; 3) able to ambulate independently or with supervision; 4) able to understand and follow instructions in English/ Mandarin; and 5) able to self-transfer independently. Residents were further screened with an abbreviated mental test (AMT) to determine their cognitive function and split into two groups (Group A and Group B) (See Figure 1). Group A residents consisted of individuals with cognitive impairment (AMT scored less than 8), whereas Group B residents had no cognitive impairment (AMT scored 8 and above). All participants and/or the Next-of-Kin (NOK) (if residents’ AMT<8) provided written consent to participate in the study.
Care staff were recruited from the two wards in the participating nursing home. They were invited via email to participate in focus group discussion in the study if they met the following criteria: 1) direct involvement in caring for resident participants during the trial; 2) providing written consent to participate. Three to eight care staff were recommended as the optimal size for focus group discussions (Braun & Clarke, 2013).
2.3. Hip Protector Trial
While various studies suggested the period for hip protector trial ranging from two weeks (Cameron et al., 2010) to five months (Nemeth et al., 2022; Post et al., 2019) for hip protectors, we conducted a two-month trial period after consulting with the nursing home to ensure alignment with their operational requirements.
Participating residents were provided with one EXO+ hip protector each after a 30-minute training session on how to use the hip protector. They were asked to don the hip protectors when mobilising out of bed during the day (6 am to 6 pm). The hip protectors came in various sizes and were fitted based on individual measurements and comfort levels. The fitting of the hip protector was conducted by the staff and researchers during the training session.
2.4. Data Collection
Descriptive data including sociodemographics (e.g., age, gender); comorbidities and history of falls were then collected using a predesigned screening form. Functional statuses, such as cognitive function (Abbreviated Mental Test), physical functions (Timed Up and Go), and independence in self-care (Modified Barthel Index) were assessed at the baseline.
During the two-month trial, staff continuously monitored the duration of wear of the hip protector, reasons for not wearing the hip protector during ambulation, and details of falls that occurred during the trial were recorded daily on specially designed data recording forms.
Focus groups of smaller sizes (3-8 participants) are useful in gathering data for topics (Braun and Clarke, 2013), especially for initial exploration and problem identification (Morgan, 1998). Researchers can adapt questions for the following FGDs based on the discussion during an initial FGD, and the FGDs create space for participants to reflect on their experiences and make changes to their provision of care (Morgan et al., 2008).
Thus, four repeated FGD sessions with the participating staff were held during the trial at two-week intervals to gather crucial data including difficulties faced during the trial, potential solutions and whether implemented solutions were effective. A list of guided questions (Online supplementary file) was used by the researchers during the first FGD, with each session lasting around 45 minutes. Questions for each subsequent FGD were revised based on the responses and themes gathered from the previous FGD session. The fourth session was held after the trial, concluding the care staff’s experiences until data saturation was obtained.
2.5. Data Analysis
Older adult participants’ baseline characteristics (e.g. age, gender, ethnicity, physical functions, cognitive functions, independence in self-care and history of falls) were presented using descriptive statistics. A two-sample t-test was used to compare the means of baseline characteristics between two groups of residents. A p-value of less than 0.05 was considered a statistically significant difference between the two groups.
Each FGD was transcribed verbatim by the researchers in the original language, with each staff allocated a unique code to maintain anonymity. Transcripts were reviewed by the other researchers in the team to improve accuracy and uploaded to the Quirkos software for thematic analysis. Data analysis of each FGD was used to guide the development of the subsequent FGD to ensure the continuity of the questions being raised. A reflexive thematic analysis method with an inductive approach was adopted using the phases proposed by Braun and Clarke (2006).
Quantitative data findings were used to further supplement and understand the usability of the hip protector through analysis using distribution and variability of the descriptive data. Weekly meetings among the research team members were also held to review the analysis to establish standardisation and consensus.
3. Results
3.1. Quantitative Findings
This study recruited 15 eligible male residents from the participating wards. The recruited residents were further divided into two distinct groups (Group A vs. Group B) based on their cognitive functions (p<0.5), where Group A (n=8) had cognitive impairment with a mean AMT score of 3.3 and Group B (n=7) had no cognitive impairment with a mean AMT score of 9.3. The majority of residents were Chinese except two Malay residents in Group B. There was a higher percentage of residents in Group A (n=3) with a history of falls when compared with Group B (n=0) (p<.05). There was no significant difference in gender, ethnicity, mobility function (TUG), independence in self-care (MBI), or mobility status between the two groups of participants (p > .05).

Table 1.
Baseline Characteristics of the Participants .
| Group A (n = 8) | Group B (n = 7) | p | |
| Age, mean (± SD) | 81.4 (± 10.9) | 77.0 (± 9.1) | 0.256 |
| Gender (Male), n (%) | 8 (100%) | 7 (100%) | 1.000 |
| Ethnicity (Chinese), n (%) | 8 (100%) | 5 (71.4%) | 0.398 |
| Ethnicity (Malay), n (%) | 0 (0%) | 2 (28.6%) | 0.571 |
| Have ≥2 chronic health conditions, n (%) | 8 (100%) | 7 (100%) | 1.000 |
| AMT, mean (± SD) | 3.9 (± 3.0) | 8.6 (± 2.0) | .0001 |
| TUG, mean (± SD) | 26.0s (± 16.2s) | 14.9s (± 21.3s) | 0.341 |
| MBI, mean (± SD) | 80.9 (± 19.2) | 72.7 (± 15.3) | 0.383 |
| History of falls in the past 6 months, n (%) | 3 (37.55%) | 0 (0%) | 0.040 |
| Independent walking, n (%) | 7 (87.5%) | 3 (42.9%) | 0.264 |
| Wheelchair-bound, n (%) | 1 (12.5%) | 4 (57.1%) | 0.398 |
Note. AMT = Abbreviated Mental Test; TUG = Timed Up and Go; MBI = Modified Barthel Index .
Several noteworthy details were recorded during the trial. This included the lack of falls amongst participants throughout the trial and several reasons quoted by residents for not wanting to wear the hip protector during ambulation. These reasons were often followed by long durations of non-use upon initial resistance to wear. The reasons included not seeing the need to wear, rashes, itchiness and feeling hot and uncomfortable.
3.1.1. Wear Time Trends
The wear time data (Figure 2) demonstrated several noteworthy trends.
Temporal Trends. Hip protector wear times generally followed the trend of an initial increase followed by a decrease, and subsequent fluctuations with slow increments before plateauing.
Group-based Trends. The trial saw several comparative trends. Group A residents were found to have consistently higher wear times than Group B residents. Additionally, residents’ wear time was higher in the morning (AM) compared to the afternoon (PM), and on weekdays compared to weekends.
3.2. Qualitative Findings
A total of 9 care staff participated in the repeated FGDs. The care staff consisted of one senior physiotherapist, 4 therapy assistants and 4 care partners. Six staff attended the first FDG, 4, 3 and 4 staff attended the second, third and fourth sessions, respectively. Only 2 care staff attended all four FGD sessions, while 2 attended two sessions and 5 attended at least one session. Each FGD lasted for 45 minutes on average.
Data saturation was achieved after 4 FGDs were conducted with 9 residential care staff during the trial period. Initial codes were generated from the data using the line-by-line coding method to generate common categories and then organised into subthemes and themes. Data analysis of each FGD was used to guide the development of the subsequent FGD to ensure the continuity of the questions being raised.
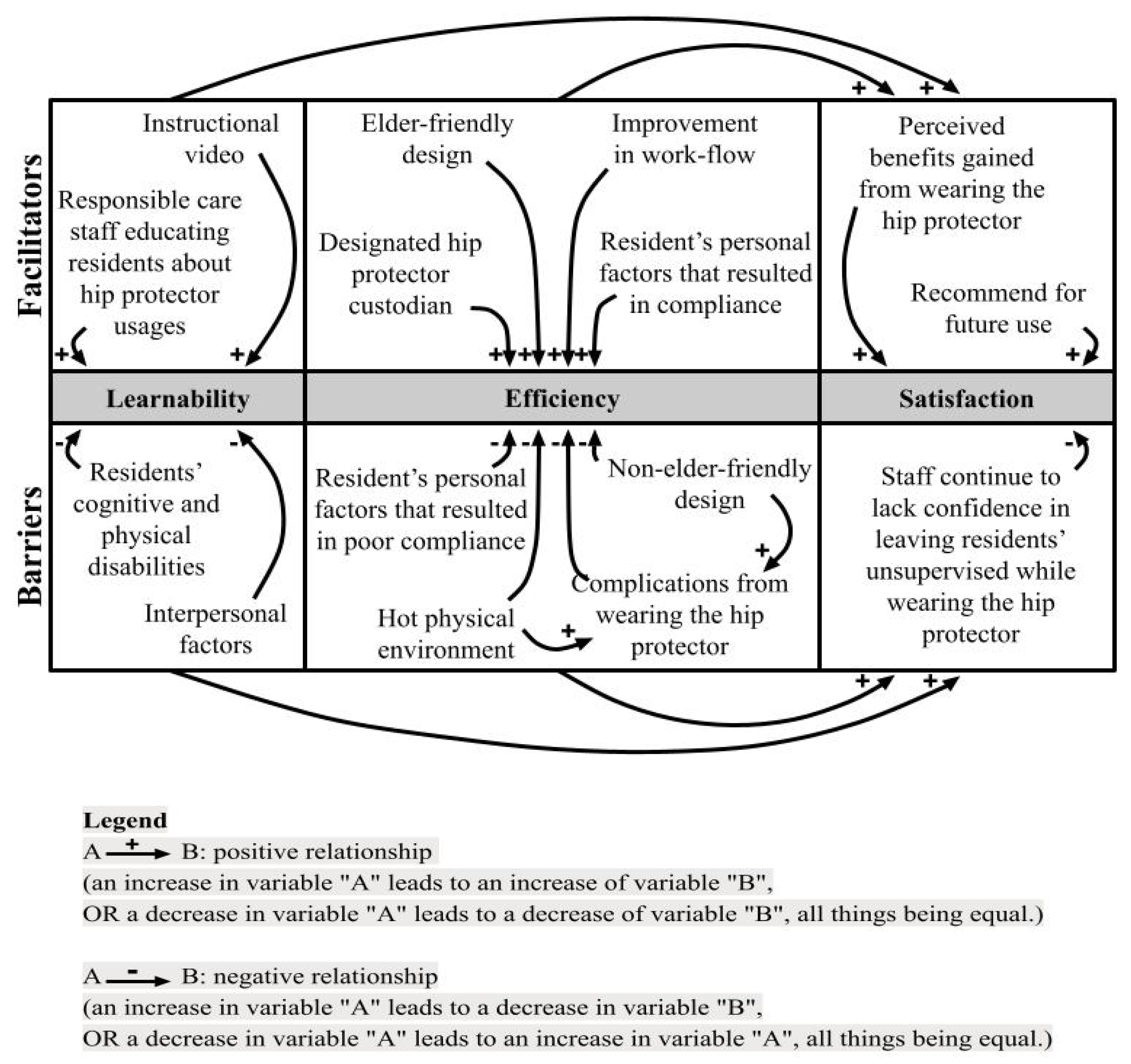
As shown in Figure 3, six main themes and fourteen subthemes emerged from the data analysis that served as barriers or facilitators for the hip protector’s (a) Learnability, (b) Efficiency, and (c) Satisfaction. Each theme encapsulates various subthemes that shed light on the factors influencing staff’s perception and experience with the hip protectors. The relationship between themes and subthemes was subsequently framed into the causal diagram as shown in Figure 3.
3.2.1. Learnability
Learnability encompasses staff perspectives on how easy it is for both residents and staff to understand and use the EXO+ hip protectors. Two subthemes were identified as facilitators of the learnability of the EXO+, while two other subthemes were identified as barriers towards the learnability of the EXO+.
- Facilitators Affecting Users’ Learnability.
Instructional Video. During the FGDs, the staff highlighted the instructional video as a valuable tool in assisting residents with understanding the usage of hip protectors, particularly appreciating its multilingual features.
I appreciate the video. Because there's visual feedback ... our care staff translated [to] Chinese and ... Malay. So, everybody understood. (S3)
Even though I don't understand Chinese, [and] even residents who don't understand anything, by seeing the demonstration, they will understand. (S5)
Education About Hip Protector Usage by Care Staff. Assigning dedicated staff members with good rapport to remind and re-educate residents on wearing hip protectors emerged as a facilitator for learnability.
I can …[help] him wear [it] because I can talk to him … But other staff he [does] not follow … he will just throw everywhere, he shouts and make noise. (S8)
Since ... S10 came back from hospital leave ... the wearing has become more … we need staff to remind the elderly to always wear it. (S1)
- Barriers Affecting Users’ Learnability.
Residents' Cognitive and Physical Disabilities. Conversely, participants identified residents' disabilities as a barrier to learning how to use the hip protectors, emphasizing the need for individualized training and repeated education.
He tends not to wear the … [hip] protector... because … he always … goes toilet ... because of incontinence (S7)
I think this training must be continued because they are very forgetful. (S4)
Interpersonal Factors. Poor interpersonal communication among staff and language barriers hindered residents' learnability of the hip protectors.
I was teaching them … how to wear. I tried to explain it to those who can only understand Chinese …, but my Chinese [is] not so good (S6)
I gave him (S2) the list of the elders … I am hoping that all the elders should be given [the hip protector], but I don't know why he (S2) never gave [it] to “R6”. (S1)
3.2.2. Efficiency
Efficiency explores how resources were expended for the accuracy and completeness of hip protector usage. Four subthemes were identified as facilitators, and four subthemes were identified as barriers.
- Facilitators Affecting Efficiency of the Use of Hip Protector.
Elder-friendly Design. Participants appreciated the elder-friendly design features of the hip protectors, such as accurate sizing, good use of materials and ease of adjustment. They noted that these features contributed to comfort and increased compliance in hip protector usage.
... with the hip protector, they were still able to do their everyday activities within the household. So, it didn’t hinder anything. (S3)
I like the easy-to-use part of it, so the Velcro [is] easy to adjust if there is a mistake you just open [it] up (S3)
Hip Protector “Custodian”. Having a designated staff with good rapport with the residents to oversee hip protector usage improved compliance, although limitations in manpower also resulted in constraints in interaction time with residents.
…If they trust you, they believe in you, then they will wear. (S1)
Reminders of wearing the hip protector were implemented and she's really very strict with the elders ... when S9 is there a full day, you can see the number of hours is increased. (S1)
I think compliance improves when someone is designated and focused specifically on the implementation of the hip protector in the ward. (S3)
she goes in the morning … But I can only put her once a day to remind her because she has other work to do (S1)
Improvement in Workflow. Participants described how incorporating hip protector usage into residents' daily routines and gradually increasing wear time helped residents acclimatize to wearing the protectors. This was a suggestion identified during and implemented after the second FGD.
We can sustain them for 2 hours in the morning, and 2 hours in the afternoon. (S1)
One hour for the whole day … And then … [for] the following week, there was 2 hours …[then] 4 hours. About 2-3 hours difference (S3)
When he (R10) goes to the toilet … he’s wearing the hip protector … it’s been a part of his routine (S7)
Residents’ Personal Factors That Resulted in Compliance. Personal factors, such as reduced resistance due to cognitive impairments, peer influence, and understanding the benefits of wearing hip protectors, positively influenced compliance among residents.
R14 is very particular … “Everybody has why I don’t have?” Ah is like that “I must have” (S4)
The easiest ones are the dementia elderly, they don't realise, they don’t understand. When S9 says “wear it”, they will wear it. (S1)
- Barriers Affecting the Efficiency of the Use of Hip Protector.
Non-elder-friendly Design. Some design features, such as the inconvenience and discomfort caused by the hip protectors and difficulties orientating their front and back discouraged residents from wearing them.
Even like the colour... black colour inside, brown colour outside … they wear “upside down”. (S2)
Some elders …like R10, feel itchy … maybe can consider changing the material so the material is more comfortable for them (S6)
Hot Physical Environment. Staff noted that the hot environment within the nursing home contributed to residents' discomfort while wearing the hip protectors, resulting in residents only wearing the hip protectors in the morning and not the afternoon.
Very hot ... they feel uncomfortable (S4)
They will wear it only in the morning. After lunch they remove it, and they will not wear it in the afternoon again. (S1)
Complications From Wearing the Hip Protectors. Residents experienced complications, such as rashes and the dislodging of Indwelling Urinary Catheter (IDC), while wearing the hip protectors.
Those that were compliant there are several others now find rashes, and itchiness. (S3)
R9 … was complaining of abdominal discomfort then apparently after 30 minutes, he dislodged his IDC. (S7)
Residents’ Personal Factors Resulting in Poor Compliance. Poor understanding of the purpose of wearing hip protectors and behavioural issues among residents hindered compliance.
People like R8 don't want to wear it. R15 also don't want to wear … most of the time, they say, "I'm in the wheelchair I don't need to walk, I don't do it at all." (S4)
Like R6 right, sometimes he (gets) aggressive … If they are not in a good mood … they will throw everything. (S8)
3.2.3. Satisfaction
Satisfaction explores the overall perception of staff regarding the benefits and drawbacks of the EXO+ hip protectors. Two subthemes indicated satisfaction with the EXO+. Conversely, one subtheme points towards dissatisfaction with the EXO+.
- Facilitators Affecting Care Staff’s Satisfaction.
Perceived Benefits Gained from Wearing the Hip Protector. Staff noted increased protection and perceived confidence in walking among residents as benefits of wearing the EXO+.
I think … client R10’s confidence level is there, [confidence] increased because of the hip protector. (S7)
I said, “If you don't want it, you can give it to other people”. “No”, he said “I will keep it” … He said it belonged to him. He will not give it to other people. (S8)
Recommend for Future Use. Staff expressed their intention to recommend the hip protectors based on their positive experiences.
If I compare that to the one that you were telling me, the one that needs to be worn underneath, then I prefer this. (S3)
It is comfortable the way they walk. It’s not really uneasy or it’s not really unsafe. That is my reason of maybe recommending it in a nursing home in the future. (S1)
- Barriers Affecting Care Staff’s Satisfaction.
Staff Continue to Lack Confidence in Leaving Residents Unsupervised While Wearing the Hip Protector. Despite positive experiences, some staff expressed ongoing concerns about residents' safety and the need for supervision.
We’re not very confident the reason is because these elders have co-morbidities, [and] pre-existing conditions. So they need constant supervision (S7)
I think this has nothing to do with the equipment. It’s just how we do our SOPs, how we supervise, and how we take care of the elderly. (S3)
3.2.4. Relationship Between Themes
The Learnability and Efficiency of the EXO+ hip protectors were found to directly impact residents' satisfaction with their usage (Figure 3). Factors influencing Learnability and Efficiency, such as instructional videos and elder-friendly design, were crucial in determining staff Satisfaction.
3.2.5. Relationship Between Quantitative and Qualitative Data
Learnability. Higher wear times in the morning (AM) and on weekdays can be attributed to the presence of more staff reminding and re-educating residents on wearing hip protectors during the AM hours.
Efficiency. Lower wear times during the PM hours could be attributed to the hotter afternoon temperatures and the discomfort arising from heat-related complications. Instances of rashes and other complications were associated with decreased wear time on specific dates. For example, wear time decreased following reports of rashes and itchiness among residents (Figure 2). Hip Protector “Custodian”. Similarly, the presence of more staff members overseeing hip protector usage in the morning and on weekdays could have improved compliance. A comparison between the wear time of residents with cognitive impairments (Group A) and those without (Group B) revealed that residents with cognitive impairments demonstrated higher compliance compared to those without, concurring with subthemes identified in the FGDs.
Satisfaction. Through the relation shown between Learnability and Efficiency (Figure 3), and a similar correlation between facilitators and barriers of the 2 outcomes and wear time, it can be postulated that satisfaction is positively correlated with wear time. Additionally, staff’s concerns about residents' safety and the need for supervision could lead to providing fewer opportunities for residents to ambulate, explaining lower average hip protector wear times.
3. Discussion
This study is the first to report on the usability of the EXO+ hip protector through the experiences of the staff of a nursing home in Singapore. Results indicated that the EXO+ is usable in a nursing home with appropriate environmental support and pre-implementation training. Through repeated Focus Group Discussions (FGDs) with the same group of care staff, subthemes impacting Learnability, Efficiency and Satisfaction with the hip protector were identified to facilitate work process changes in the nursing home. These were corroborated by quantitative data on hip protector wear times, with empirical trends and patterns observed closely tracking the qualitative insights. These subthemes are further discussed below with reference to the literature.
3.1. Learnability
Video and training. Positive feedback during the FGDs corroborates this finding, where the instructional video was mentioned to be helpful for patient education. Similarly, wear time data indicated high compliance rates at the beginning of the trial. Past research has found that similar training sessions promote the usage of hip protectors (Meyer et al., 2003), and that visual and auditory means of providing information prove beneficial in garnering the attention of the elderly (Ren et al., 2020). While beneficial, the video and training were ultimately unable to sustain continued hip protector usage as evident in the eventual reduction of wear time (Figure 2).
Responsible Care Staff Educating Residents About Hip Protector Usage. This pattern is consistent with previous literature, which has documented that higher adherence was found among residents who were more open to persuasion to wear the hip protectors (O’Halloran et al., 2007). This underscores the importance of allocating dedicated staff to ensure residents understand the purpose of hip protector usage, especially for those with cognitive impairments. Techniques tapping on existing memory strengths of the elderly with cognitive impairments, such as implicit memory techniques (Son et al., 2002), may also be used to retain the understanding of the purpose of wearing hip protectors.
3.2. Efficiency
Hip Protector “Custodian”. Compliance rates dipped two weeks into the trial due to side effects and staffing issues, challenges which were also observed in a similar study where the lack of staff reduced hip protector wear times (Korall et al., 2015). Similar to how dedicated staff can enhance patient understanding regarding the importance of hip protector usage, the hip protector “custodian” can support compliance by overseeing hip protector wearing.
Hot Physical Environment and Complications from Wearing the Hip Protectors. Complications, both from wearing the hip protector and those derived from hot physical environments, prove to be barriers impacting usability and wear time. These results are consistent with the previous finding that physical discomfort serves as a deterrent towards hip protector compliance (O’Halloran et al., 2007).
Residents’ Personal Factors That Impacted Compliance. Residents with cognitive impairments demonstrated higher compliance compared to those without. This is consistent with existing literature, which has documented that persons with cognitive impairments have higher compliance rates as they rely on staff to make decisions for them and are therefore more open to persuasion (O’Halloran et al., 2007). Despite increasing compliance, cognitive impairment was also shown to reduce the retention of information (Guerdoux et al., 2012), leading to greater dependency on care staff for assistance. This explains the lack of understanding of the purpose of hip protector usage despite training efforts. The prevalence of residents with cognitive impairments within nursing homes is high (Ang et al., 2006). Therefore, it is particularly important to be attentive to these considerations when implementing hip protectors within nursing homes.
3.2. Satisfaction
This finding is intuitive given the close relationship between Learnability, Efficiency and staff Satisfaction with the hip protector. It clarifies previous literature, which did not find a clear relationship between different usability measures (O’Halloran et al., 2007). Additionally, it appears that staff satisfaction and hip protector wear time are correlated, as evident from previous literature observing higher wear times in nursing homes with nursing staff having positive inclinations towards the hip protectors (Hubacher and Wettstein, 2001). However further research is necessary to establish the direction of causation between these variables.
3.2. Limitations of the study
The interpretation of the results should be approached with caution in light of the following limitations. Firstly, the qualitative data was also solely collected by interviewing care staff. Interviewing residents directly about their views on the useability of the hip protectors might have provided another perspective on the topic. Additionally, although wear time data offered valuable insights into hip protector usage patterns and trends, the data alone cannot indicate the underlying reasons for hip protector utilisation or non-compliance. Trends in hip protector use appear to correlate with insights from qualitative data, corroborating staff observations. For instance, temporal fluctuations of a decline during the absence of the designated staff member overseeing compliance due to medical leave, and subsequent increase upon their return suggests a positive relationship between the presence of a hip protector “custodian” and wear time. However, it is possible that these trends were correlated with additional factors that are not evident from the quantitative data alone.
Secondly, no falls took place throughout the trial period. This could have been a result of the higher levels of caution amongst the older adult participants with closer supervision from the care staff during the 2-month trial period. As such, this study is unable to test the hip protector’s efficiency in its primary purpose of preventing hip fractures in the event of a fall. The short study duration also fell short of time norms for habit creation (Lally et al., 2010). It is therefore possible that different findings about hip protector useability might be observed over longer periods when hip protector usage had become habitual.
Finally, the study was conducted with a small homogenous sample. Participants were drawn from a single site, were of a single gender and had an ethnic makeup that was unrepresentative of the broader elderly population. Hence, the generalisability of findings to other nursing homes and settings may be limited.
3.2. Implications for Practice and Future Recommendations
The findings suggest that the inclusion of staff training and workflow adaptations, such as incorporating hip protector wear into daily routines and gradually increasing wear time, may enhance the Efficiency and Satisfaction of hip protectors in an applied setting. Repeated use of training material, such as training videos containing audio and visual prompts, can be incorporated into residents’ daily routines to aid the retention of information. Healthcare settings implementing the hip protector should consider appointing a hip protector “custodian” to maximise both the Learnability and Efficiency of the hip protector.
Certain enhancements in the hip protector's design are worth considering, particularly in terms of material selection to accommodate the warm climate in Singapore. This could come in the form of breathable mesh material, or materials such as bamboo fibre which are gentle on sensitive skin (Love and Neodrost, 2018).
Future studies should consider exploring EXO+’s effectiveness in mitigating fracture risks through a randomized clinical trial design, involving multiple nursing homes to establish distinct groups over an extended period (up to 6 months). Intervention groups would receive the EXO+ while participants are randomized into control or intervention groups. The primary outcome measure would be the incidence of falls in each group, with secondary outcome measures potentially encompassing the severity of falls, fall-related injuries, quality of life, and adherence to wearing the hip protector.
4. Conclusions
This study has shown that EXO+ hip protectors are usable in a Singaporean nursing home setting with appropriate supporting features. It also offers significant insights into potential modifications to the hip protector's design, along with adjustments in workflow, environmental accommodations, and pre-implementation protocols which could augment its usability. Healthcare settings where hip protectors will be implemented can build upon the various facilitators and barriers identified in the study to support device uptake. Further studies may be conducted on the robustness and accuracy of the usability of the EXO+ hip protector.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Figure S1: title; Table S1: title; Video S1: title.
Author Contributions
“Conceptualization, T.X., Y.V.L., L.S.X., Y.J.S. and A.L.X.; methodology, T.X.; formal analysis, T.X., Y.V.L., L.S.X., and Y.J.S.; data curation, T.X., Y.V.L., L.S.X., Y.J.S. and A.L.X.; writing—original draft preparation, Y.V.L.; writing—review and editing, T.X. and A.L.X.; supervision, T.X.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethics approval was obtained from the Institutional Review Board of the Singapore Institute of Technology in 2023 (Institutional Review Board number: RECAS-0006) and the St Luke’s Eldercare Research Ethics Committee (Reference number: EX23002).
Informed Consent Statement
Informed consent was obtained from all subjects or the Next-of-Kin of the subjects involved in the study.
Data Availability Statement
The data is unavailable due to institutional data protection policy. .
Acknowledgments
We would like to acknowledge all research participants involved in this study. We also would like to thank St Luke’s Eldercare, and its staff Ms. Cecilia Ma Llego and Ms. Susie Goh for providing resources and manpower in this study. .
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ang, Y.H.; Au, S.Y.; Yap, L.K.; Ee, C.H. Functional decline of the elderly in a nursing home. Singapore Medical Journal 2006, 47, 219–24. Available online: http://www.smj.org.sg/sites/default/files/4703/4703a6.pdf. [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qualitative Research in Psychology 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Successful Qualitative Research: A Practical Guide for Beginners; SAGE Publications Ltd.: London, 2013. [Google Scholar]
- Cameron ID Murray, G.R.; Gillespie, L.D.; Robertson, M.C.; Hill, K.D.; Cumming, R.G.; Kerse, N. Interventions for preventing falls in older people in nursing care facilities and hospitals. Cochrane Database of Systematic Reviews 2010, 1, CD005465–CD005465. [Google Scholar] [CrossRef]
- Chen. STM32-based Anti-fall Smart Vest System for the Elderly. 2017 IEEE 3rd Information Technology and Mechatronics Engineering Conference (ITOEC) IEEE; 2022; 6. [CrossRef]
- Creswell, J.W.; Fetters, M.D.; Ivankova, N.V. Designing a mixed methods study in primary care. Annals of Family Medicine 2004, 2, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Guerdoux, E.; Dressaire, D.; Martin, S.; Adam, S.; Brouillet, D. Habit and Recollection in Healthy Aging, Mild Cognitive Impairment, and Alzheimer’s Disease. Neuropsychology 2012, 26, 517–533. [Google Scholar] [CrossRef] [PubMed]
- Health Promotion Board. Falls Prevention Among Older Adults Living in The Community. Health Promotion Board. 2015. Available online: https://www.hpb.gov.sg/docs/default-source/pdf/cpg_falls_preventionb274.pdf.
- Hewitt, J.; Goodall, S.; Clemson, L.; Henwood, T.; Refshauge, K. Progressive resistance and balance training for falls prevention in long-term residential aged care: a cluster randomized trial of the Sunbeam Program. Journal of the American Medical Directors Association 2018, 19, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Hornboek, K. Current practice in measuring usability: Challenges to usability studies and research. International Journal of Human-Computer Studies 2006, 64, 79–102. [Google Scholar] [CrossRef]
- Hubacher, M.; Wettstein, A. Acceptance of hip protectors for hip fracture prevention in nursing homes. Osteoporosis International 2001, 12, 794–799. [Google Scholar] [CrossRef]
- Korall, A.M.; Feldman, F.; Scott, V.J.; Wasdell, M.; Gillan, R.; Ross, D.; Thompson-Franson, T.; Leung, P.; Lin, L. Facilitators of and barriers to hip protector acceptance and adherence in long-term care facilities: A systematic review. Journal of the American Medical Directors Association 2015, 16, 185–193. [Google Scholar] [CrossRef]
- Lally, P.; van Jaarsveld, C.H.M.; Potts, H.W.W.; Wardle, J. How are habits formed: Modelling habit formation in the real world. In European Journal of Social Psychology 2010, 40, 998–1010. [Google Scholar] [CrossRef]
- Love, W.E.; Nedorost, S.T. Fabric preferences of atopic dermatitis patients. Dermatitis 2009, 20, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J. R. Usability: Lessons Learned... and Yet to Be Learned. International Journal of Human-Computer Interaction 2014, 30, 663–684. [Google Scholar] [CrossRef]
- Meyer, G.; Warnke, A.; Bender, R.; Mühlhauser, I. Effect on hip fractures of increased use of hip protectors in nursing homes: Cluster randomised controlled trial. BMJ 2003, 326, 76. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; Van Der Velde, N.; Martin, F.C.; Petrovic, M.; Tan, M.P.; Ryg, J. ... & Masud, T. World guidelines for falls prevention and management for older adults: a global initiative. Age and Ageing 2022, 51, afac205. [CrossRef]
- Morgan, D.L. The Focus Group Guidebook. Sage Publications: California, USA, 1998; pp. 9–15. [Google Scholar]
- Morgan, D.; Fellows, C.; Guevara, H. Emergent methods to focus group research; Handbook for Emergent Methods; Hesse-Biber, S.N., Leavy, P., Eds.; The Guilford Press: New York, USA, 2008; pp. 189–206. [Google Scholar]
- Nemeth, B.; van der Kaaij, M.; Nelissen, R.; van Wijnen, J.-K.; Drost, K.; Blauw, G.J. Prevention of hip fractures in older adults residing in long-term care facilities with a hip airbag: A retrospective pilot study. BMC Geriatrics 2022, 22, 1–547. [Google Scholar] [CrossRef]
- O’Halloran, P.D.; WCran, G.; RO Beringer, T.; Kernohan, G.; Orr, J.; Dunlop, L.; JMurray, L. Factors affecting adherence to use of hip protectors amongst residents of nursing homes—A correlation study. International Journal of Nursing Studies 2007, 44, 672–686. [Google Scholar] [CrossRef]
- Parker, M.J.; Gillespie, W.J.; Gillespie, L.D. Effectiveness of hip protectors for preventing hip fractures in elderly people: Systematic review. BMJ 2006, 332, 571–573. [Google Scholar] [CrossRef]
- Pepera, G.; Krinta, K.; Mpea, C.; Antoniou, V.; Peristeropoulos, A.; Dimitriadis, Z. Randomized controlled trial of group exercise intervention for fall risk factors reduction in nursing home residents. Canadian Journal on Aging 2023, 42, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Post, E.; Komisar, V.; Sims-Gould, J.; Korall, A.; Feldman, F.; Robinovitch, S. Development of a stick-on hip protector: A multiple methods study to improve hip protector design for older adults in the acute care environment. Journal of Rehabilitation and Assistive Technologies Engineering 2019, 6, 2055668319877314–2055668319877314. [Google Scholar] [CrossRef]
- Rau, C.S.; Lin, T.S.; Wu, S.C.; Yang JC, S.; Hsu, S.Y.; Cho, T.Y.; Hsieh, C.H. Geriatric hospitalizations in fall-related injuries. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2014, 22, 63–63. [Google Scholar] [CrossRef]
- Ren, Y.; Guo, A.; Xu, Z.; Wang, T.; Wu, R.; Yang, W. Age-related functional brain connectivity during audio–visual hand-held tool recognition. Brain and Behavior 2020, 10, e01759-n/a. [Google Scholar] [CrossRef] [PubMed]
- Romli, M.H.; Tan, M.P.; Mackenzie, L.; Lovarini, M.; Suttanon, P.; Clemson, L. Falls amongst older people in Southeast Asia: A scoping review. Public Health 2017, 145, 96–112. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z.; Josephson, K.R. The epidemiology of falls and syncope. Clinics in Geriatric Medicine 2002, 18, 141–158. [Google Scholar] [CrossRef] [PubMed]
- Sawka, A.M.; Boulos, P.; Beattie, K.; Thabane, L.; Papaioannou, A.; Gafni, A. ,... & Adachi, J. D. Do hip protectors decrease the risk of hip fracture in institutional and community-dwelling elderly? A systematic review and meta-analysis of randomized controlled trials. Osteoporosis International 2005, 16, 1461–1474. [Google Scholar] [CrossRef] [PubMed]
- Santesso, N.; Carrasco-Labra, A.; Brignardello-Petersen, R.; Santesso, N. Hip protectors for preventing hip fractures in older people. Cochrane Database of Systematic Reviews 2014, 2014, CD001255–CD001255. [Google Scholar] [CrossRef]
- Singapore Institute of Technology (SIT). Bespoke hip protector enhances safety of fall-prone seniors. SIT’s Digital Newsroom. 2022. Available online: https://www.singaporetech.edu.sg/news/bespoke-hip-protector-enhances-safety-fall-prone-seniors.
- Son, G.-R.; Therrien, B.; Whall, A. Implicit Memory and Familiarity Among Elders with Dementia. Journal of Nursing Scholarship 2002, 34, 263–267. [Google Scholar] [CrossRef]
- Stevens, J.A.; Ryan, G.; Kresnow, M. Fatalities and Injuries from Falls Among Older Adults — United States, 1993–2003 and 2001–2005. MMWR: Morbidity and Mortality Weekly Report 2006, 55, 1221–1224. [Google Scholar]
- Takatou, K.; Shinomiya, N. Cloud-based fall Detection System with Passive RFID Sensor Tags and Supervised Learning. 2021 IEEE 10th Global Conference on Consumer Electronics (GCCE) 2021, 153–156. [Google Scholar] [CrossRef]
- Tyrovolas, S.; Koyanagi, A.; Lara, E.; Ivan Santini, Z.; Haro, J.M. Mild cognitive impairment is associated with falls among older adults: Findings from the Irish Longitudinal Study on Ageing (TILDA). Experimental Gerontology 2016, 75, 42–47. [Google Scholar] [CrossRef]
- van Schoor, N.M.; Deville, W.L.; Bouter, L.M.; Lips PT, A.M.; Lips, P. Acceptance and compliance with external hip protectors: A systematic review of the literature. Osteoporosis International 2002, 13, 917–924. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization [WHO]. WHO global report on falls prevention in older age. 2008. Available online: https://www.who.int/publications/i/item/WHO%20global%20report%20on%20falls%20prevention%20in%20older%20age.
- Yap, P.; Au, S.; Ang, Y.H.; Kwan, K.Y.; Ng, S.C.; Ee, C. Who are the residents of a Nursing Home in Singapore? Singapore Medical Journal 2003, 44, 65–73. [Google Scholar] [PubMed]
- Yong, E.L.; Ganesan, G.; Kramer, M.S.; Logan, S.; Lau, T.C.; Cauley, J.A.; Tan, K.B. Hip fractures in Singapore: ethnic differences and temporal trends in the new millennium. Osteoporosis International 2019, 30, 879–886. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Distribution of Participants (Nursing Home Residents and Care Staff).

Figure 2.
Wear time data (Group A vs Group B and AM vs PM).
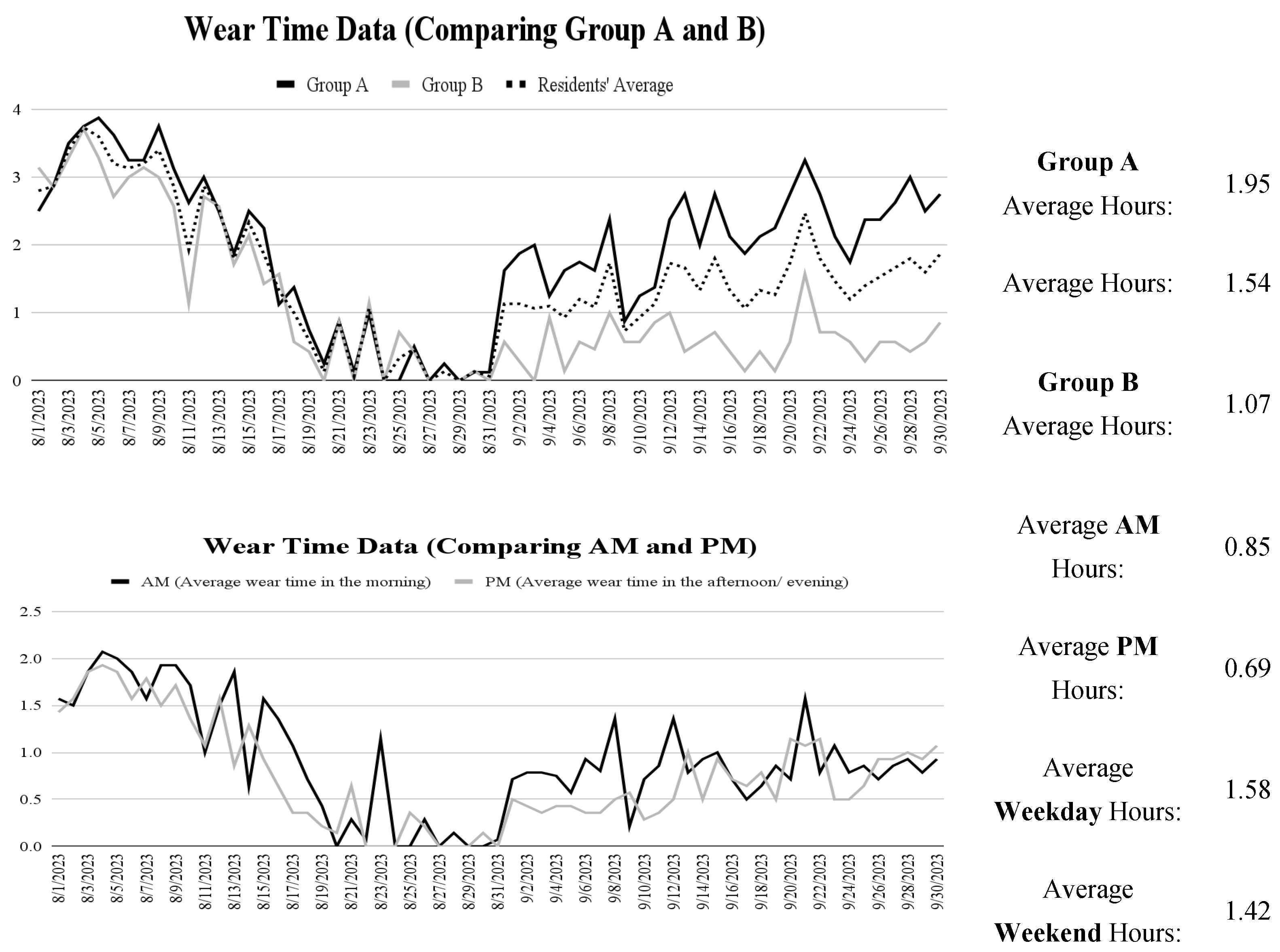
Figure 3.
Casual relationship diagrams of themes and subthemes. .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



