Submitted:
18 September 2024
Posted:
19 September 2024
You are already at the latest version
Abstract
Regenerative medicine is an interdisciplinary field that combines stem cell technology and tissue engineering to replace or regenerate human cells, tissues, or organs and restore normal functions. The term 'regenerative medicine' was coined by William Haseltine at a 1999 conference on Lake Como. Since its inception in 1968, the field has offered clinical benefits for the regeneration, repair, and restoration of bones, skin, cartilage, neural tissue, and heart, as well as scaffold fabrication. Inorganic biomaterials play a crucial role in regenerative medicine, often surpassing traditional synthetic materials due to their adjustable intrinsic properties, such as size, topography, charge, and chemical stability. These properties enable a flexible cellular response within intracellular matrix environments and provide structural support for cell adhesion and tissue regeneration. Given the wide gamut of near-future potential applications of inorganic biomaterials, this article gives an overview of their emerging roles in stem cell regenerative research, tissue engineering, artificial skin and cartilage regeneration, neural nerve injuries, 3D bioprinting, and development of new inorganic bio-scaffolds. The review also addresses the challenges related to the clinical application and tissue compatibility of inorganic biomaterials, utilizing current state-of-the-art techniques.

Keywords:
regenerative medicine
; inorganic biomaterials
; nanoparticles
; tissue engineering
; nanotechnology
1. Introduction
Regenerative medicine is an emerging interdisciplinary field focused on developing methods to replace or repair damaged cells and restore tissue or organ function affected by trauma, chronic conditions, disease, aging, or congenital deformities [1,2]. Regenerative medicine combines the principles of chemistry, biology, and applied engineering to develop processes and therapies that can promote the regeneration of human cells, functional organs, and injured tissues to restore normal body functions [3,4]. By harnessing the human body's innate ability to self-heal, regenerative medicine is poised to revolutionize science, healthcare, and medicine [1]. Regenerative medicine is also used synonymously with ‘tissue engineering’ which relies on developing scaffolds that mimic the extracellular matrix (ECM) of tissues [5]. Examples of regenerative medicine include stem cell therapy, immunomodulation therapy, and tissue engineering [6]. Tissue engineering is the application of principles and methods of engineering and life sciences toward the fundamental understanding of structure-function relationships in normal and pathological mammalian tissues and the development of biological substitutes to restore, maintain, or improve tissue function [7]. The primal goal of tissue engineering is the regeneration of patients’ tissues and organs devoid of poor biocompatibility, functionality, and immune rejection [8].
Cells, scaffolds, and growth factors are the three main constituents for bone and cartilage formation in tissue engineering [9]. Cell synthesizes the matrix for the growth of new tissues [8]. Scaffold material, template, or artificial ECM act as substrates to load cells and growth factors and stimulate cell proliferation, differentiation, biosynthesis, and regeneration [9]. Growth factors are signaling molecules that direct cell behavior to stimulate the growth of new tissues and provide chemical cues to stem cells, regulating their biological responses and tissue differentiation [8,10]. Tissue engineering proceeds in the presence of a scaffold that provides the template for regeneration. Bone tissue engineering and enhancement of bone healing for orthopedic, craniofacial, and periodontal applications can be achieved using a group of multi-functional growth factors called bone morphological proteins (BMPs) [11]. BMPs belong to the transforming growth factor beta (TGFβ) superfamily and are important in controlling osteoblastogenesis, embryonic development, cellular function, differentiation, proliferation, morphogenesis, and apoptosis of various types of cells [12]. BMP signaling starts with BMP ligand binding to a transmembrane, heterotetrametric receptor complex composed of type I BMP receptors (BMPR) (ACVR1/ALK2, BMPR1A/ALK3, BMPR1B/ALK6) and type II BMPR (BMPR2, ActR-2A, ActR-2B) [13].
Stem cells are a class of primitive, non-specialized cells that exhibit the potential to self-renew and differentiate into other cell types such as liver cells, nerve cells, and cardiomyocytes [3,14,15]. Stem cells are broadly classified into embryonic stem cells (ESCs), adult stem cells (ASCs), and induced pluripotent stem cells (iPSCs) [16,17]. ASCs comprise mesenchymal stem cells (MSCs), myogenic stem cells, neural stem cells, and umbilical cord stem cells [18] while ESCs and iPSCs have higher self-regeneration and differentiation potential [19,20,21]. Stem cells are also classified as totipotent, pluripotent, multipotent, or unipotent, based on their differentiation ability [22]. A current thrust in regenerative medicine research is in cord blood stem cells that can offer patients the much-needed means to life-saving stem cell transplant [23]. Umbilical cord blood like bone marrow and peripheral blood, collected from the umbilical cord and placenta of healthy newborns, contains a rich source of blood-forming stem cells, which can renew and differentiate into other types of cells and find applications in transplants for patients suffering from leukemia, lymphoma, aplastic anemia, multiple myeloma, immune deficiency disorders, and for people facing difficulty finding matched adult donors [24]. Human umbilical cord blood stem cells, an alternative source of hematopoietic stem cells have expanded transplant eligibility for patients with neurodegenerative, cardiovascular disorders, and hematologic conditions, especially from minority groups (racial and ethnic) across the U.S. and worldwide [25,26,27]. Umbilical cord blood has advantages over bone marrow because cord blood does not require human leukocyte antigen tissue matching, has less incidence of graft vs host disease, and may be used allogenically [28,29]. MSCs are widely used for wound healing due to their abundance, high proliferation rate, multilineage differentiation capacity, and expression of paracrine factors [19]. MSCs hold promise in the regeneration of cardiac tissues and improve cardiac function [30,31,32]. Despite limitations in treatment modalities, costs involved, and limited success, stem-cell-based therapeutic strategies have emerged as a promising novel approach to enhancing regenerative wound healing [33,34,35].
Skin is the largest organ in the human body that is prone to damage, such as wear and tear, bruises, scars, ulcers, burns, wounds (infectious or chronic), and aging which can compromise its function and integrity [19,36]. Diverse cytokines, chemokines, growth factors, and cell signaling cascades are connected to the development of epidermal regeneration, health, and maintenance [19,36,37,38]. The Wnt (Wingless and INT-1) signal transduction cascade is involved in embryonic development, stem cell function, tissue homoeostatic self-renewal in adult organisms, skin development through canonical and noncanonical signaling pathways, and linked to the regulation of cell proliferation, differentiation, migration, and polarity of stem and cancer stem cells [39,40,41]. Due to the slow recovery and limited self-healing abilities of human skin, there is limited knowledge about preventing skin degeneration and identifying effective therapies for skin regeneration and rejuvenation [42].
The peripheral nervous system (PNS) is a network of 43 pairs of motor and sensory nerves that control the functions of sensation, movement, and motor coordination. The PNS comprises three types of cells: neuronal, glial, and stromal. Traumatic and infectious diseases can lead to peripheral nerve damage and long-lasting disability affecting both sensory and motor functions [43]. Recovery from peripheral nerve damage is an intractable challenge for clinical researchers, as it is a complex process typically managed through surgical nerve autografting; however, this method has disadvantages, as it often fails to achieve complete nerve recovery, nerve axon may not be able to extend due to presence of nerve gap [43]. Stem cells such as adipose-derived stem cells (ADSCs), MSCs, in particular bone marrow stem cells (BMSCs), and umbilical cord stem cells (endothelial progenitor cells, hematopoietic stem cells) with high proliferative capabilities, are suitable candidates for regenerating neural tissues [44,45,46,47]. Stem cell-based therapy in peripheral nerve injury can induce nerve regeneration and axonal remyelination by providing the microenvironment for peripheral nerve regeneration and regulating inflammatory cascade after injury [43,48]. Zeng and Zhang discussed innovative approaches for in vivo gene expression reprogramming in neural regeneration and repair [49]. However, continuous efforts are desirable to develop safe and effective therapies to understand the underlying mechanisms that regulate neuronal regeneration in the spinal cord.
Inorganic-based nanoparticles and biomaterials play a crucial role in regenerative medicine, often surpassing traditional synthetic materials due to their adjustable intrinsic properties, such as size, topography, charge, and chemical stability. The field of tissue engineering and regenerative medicine can vastly benefit from advancements in nanoscience and technology. Notably, inorganic-based bionanomaterials because of their tunable magnetic, optical, electronic, biophysical, and biochemical properties along with biocompatibility [50] can facilitate integration in regenerative medicine and tissue engineering to harness the innate potential of the body [51], support cellular in-growth tissue integration, control stem cell differentiation, in vivo stem cell tracking, and influence diverse cellular functions [5,52,53]. Hence, a synergistic amalgamation of these two research areas could be pivotal in pioneering innovations in disease treatment and therapy. In lieu of the relevance and current advancements, this review discusses the emerging roles of inorganic biomaterials and nanoparticles in stem cell regenerative research, tissue engineering, artificial skin and cartilage regeneration, neural nerve injuries, 3D bioprinting, and the development of novel inorganic bio-scaffolds. Although there are excellent reviews and studies focused on emergent developments in tissue engineering and regenerative medicine [7,50,52,54,55], this review primarily focuses on recent progress in the application of inorganic biomaterials in stem cell regenerative research, tissue engineering, artificial skin, cartilage regeneration, and wound healing. The review also addresses the challenges related to the clinical application and tissue compatibility of inorganic biomaterials, utilizing current state-of-the-art techniques.
2. Inorganic-Based Nanoparticles and Biomaterials as Scaffolds in Regenerative Medicine
Contemporary regenerative medicine strategies employ inorganic-based biomaterial scaffolds that mimic the ECM of tissues, thereby enhancing tissue regeneration and healing [1]. Scaffolding materials constitute the structural basis that, at best, can fully, or in part, mimic the native function of the ECM and help cells adhere, proliferate, and differentiate in vitro and in vivo following implantation [56,57]. The fabrication of bio-based inorganic material scaffolds facilitates the construction of substitute tissues that are biocompatible, safe, and easily biodegradable without releasing toxic byproducts [58]. These properties enable a flexible cellular response within the intracellular matrix environments and provide structural support for cell adhesion and tissue regeneration. Polymeric nanoparticles, lipid-based nanoparticles, and inorganic nanoparticles are widely studied in drug delivery, tissue engineering, and biomedical imaging applications [59,60,61] to enhance cell viability and achieve optimal cell-directing capabilities [32,61]. In the area of bone tissue engineering, inorganic biomaterials such as hydroxyapatite (HAP), HAP/poly(lactic-co-glycolic acid) composites, calcium phosphate-based biomaterials, polymer/ceramic composites are shown to be osteoinductive (ability to induce ectopic bone formation by instructing the surrounding in vivo environment to form bone) [62] and induce bone formation ectopically [57,63,64]. Hasan et al. reviewed the different applications of nanoparticles in tissue engineering [65]. Biomaterials for bone regeneration should be capable of osseointegration (integration into surrounding bone) and osteoconductive (supports bone growth and encourages the ingrowth of surrounding bone). Undoubtedly, inorganic biomaterials have broad prospects in regenerative medicine with a wide array of inorganic materials that endow regenerative function [66].
Figure 1 depicts a multifaceted approach involving cell therapy, biomaterials, and biomolecules or external stimulation for treating bone and muscle musculoskeletal disease using regenerative medicine.
Chen et al. [32] incorporated silica–iron oxide (silica-Fe3O4) nanoparticle, a superparamagnetic mesocellular foam, to guide cell injection, increase viability and cell retention by magnetic manipulation, and sustain the release of cargo in the survival of human MSCs essential for improved efficacy in stem cell therapy in cardiovascular diseases. Alternatively, porous nanomaterials such as mesoporous silica nanoparticles, metallic oxide nanoparticles, HAPs, and titanium dioxide nanotubes, due to their higher porosity and surface area have enabled drug delivery, imaging, osteoblast differentiation, and bone regeneration that mimic natural bone and implants [68].
In a recent study, Friggeri et al. [69] investigated the application of a multifunctional graphene oxide-polycaprolactone (GO-PCL) composite material as a 3D printing scaffold. The composite material exhibited antibacterial and adhesive growth properties, highlighting its potential applications in tissue engineering (Figure 2). The adsorption of solvent molecules by GO reduced bacterial adhesion during surgical procedures. The cellular adhesion on PCL-GO was significantly lower compared to PCL samples. The toxicity toward VERO cells of DMEM conditioned with PCL-GO scaffolds for 7 days was considerably lower compared to cells treated with DMEM conditioned with only PCL scaffold; there was no significant release of toxic molecules in the medium after 7 days of scaffold submersion in DMEM. The decreased cell adhesion in PCL-GO minimized biofouling risks in a surgical environment. Controlling the long-term cell adhesion ensured scaffold biodegradability and population over time, vital in promoting successful tissue regeneration.
Poly (L-lactic acid) (PLLA)/PCL matrix polymer containing gelatin nanofibers (GNFs) and gold nanoparticles (AuNPs) were fabricated for scaffolding applications in bone tissue engineering [70]. Gelatin is a biopolymer obtained from the hydrolysis of collagen, that is favorable for tissue engineering due to biocompatibility, biodegradability, low cost, low immunogenicity, and acceptable solubility properties [71]. The MG-63 cell proliferation and induced cytotoxicity on the fabricated scaffolds were measured using an MTT assay. The highest cell growth was obtained by PLA/PCL/GNF/AuNPs (80 ppm) at 72 h, which was statistically significant compared with the other group (Figure 3). AuNPs were nontoxic and biocompatible at optimum concentrations. The in vitro studies showed that 160 ppm concentration of AuNPs induced toxicity and 80 ppm AuNPs exhibited the highest cell proliferation. The in vivo studies showed that PCL/PLLA/Gel/80 ppm AuNPs induced the highest neo-bone formation, osteocyte in lacuna woven bone formation, and angiogenesis in the defect site. The low amount of AuNPs (80 ppm) incorporated in the scaffolds did not interrupt the normal functions of cells. Animal studies showed that PLA/PCL/GNF/AuNPs (80 ppm) scaffold induced the highest bone regeneration, and a combination of AuNPs and GNFs nanostructures mimicked the native structure of bone and stimulated bone healing process.
PCL, PCL/silk fibroin (SF), and PCL/SF/Au(SiO2) composite nanofibrous scaffolds were tested for their capability to support bone tissue regeneration of human MSCs (hMSCs) [72]. The hMSCs grown on PCL had a lower proliferation level than PCL/SF and PCL/SF/Au(SiO2) attributed to the absence of active binding sites in PCL. The cells grown on PCL/SF and PCL/SF/Au(SiO2) scaffolds has significantly higher proliferation levels (p < 0.05), compared to those grown on TCP and PCL, as the bioactive SF and Au(SiO2) increased the hydrophilicity of scaffold for cell adhesion [72]. The Au(SiO2) was essential for stimulating cell growth and tissue formation and the addition of SF and Au(SiO2) stimulated the proliferation of hMSCs without inducing toxicity.
Composite membranes based on polysulphone-modified multi-walled carbon nanotubes and short carbon fibers were synthesized to elucidate the physicochemical, mechanical, and biological properties [73]. The in vitro results suggested that the membranes were biocompatible in contact with MG-63 cells. The interaction mechanism between cells and composites depended on the porosity of membranes, the presence of carbon additives on the membrane surface, and surface chemistry. Sithole et al. [74] developed a novel 3D-printed biomaterial scaffold, to enhance and guide host cells’ growth for bone tissue regeneration. The 3D-printed biomaterial scaffolds were implanted in induced nasal bone defects of New Zealand white rabbits to examine the potential for bone tissue regeneration/formation. Osteoblast-like MG63 cells were utilized to culture the novel printed scaffold for 1, 3, and 7 days, respectively. The scaffold was significant for biological bone (e.g., Ca-P) as confirmed by energy-dispersive X-ray analysis. Figure 4 shows the SEM images on the 3D-printed biomaterial scaffolds seeded with osteoblast-like MG63 cells and without cells (control). Figure 4a depicts the 3D-printed biomaterial scaffold without cells (control) and seeded with osteoblast-like cells (Figure 4b and c). The cell adhesion on the rough surface was found to be advantageous for the development of implanted devices. The osteoblast-like MG63 cells and human BMP-7 protein were successfully seeded onto the novel 3D-printed biomaterial scaffolds. The in vitro experiments were performed to assess the performance of the 3D-printed biomaterial scaffold and the release of BMP-7 from the scaffold in a manner that mimicked the natural bone fracture healing process [74]. BMP-7 was proposed to adhere to the 3D-printed biomaterial scaffold’s surface, leading to an early burst release. However, maintaining a steady release of BMP-7 is also important, as high concentrations could cause adverse side effects such as heterotopic bone formation, edema, or inflammatory reactions.
A multilayer cell assembly technology that utilized a biodegradable nanochannel (BNC) membrane, hierarchically assembled from 3D manganese dioxide (MnO2) nanosheet aggregates was developed for rapid, accurate, and programmable 3D cell assembly applicable for tissue engineering, cell assembly, and disease modeling [75]. The cell assembly was crucial in creating single- and multicellular patterns with high precision and generating scaffold-free tissues after cell assembly. As membrane building blocks, MnO2 nanomaterial demonstrated fast biodegradation rates (1–3 orders of magnitude higher than present polymeric materials). The transplantation of 3D scaffold-free tissues generated using the BNC cell assembly method accelerated injury repair in both in vitro models and in vivo experiments. This study by Yang et al. [75] was a proof-of-concept application in modeling and treating wound healing with the potential for diverse clinical applications.
Yang et al. [76] developed a biodegradable hybrid inorganic nanoscaffold-based method for improving the transplantation of human patient-derived neural stem cells (NSCs), selective differentiation, and drug delivery. The developed biodegradable hybrid inorganic nanoscaffold showed an upregulated ECM-protein binding affinity, efficient drug loading with sustained drug delivery capability, and innovative magnetic resonance imaging-based drug release monitoring. By seeding human induced pluripotent stem cell (hiPSC)-derived NSCs as a model system on laminin-coated 3D-MnO2 nanoscaffold, a significant enhancement of neuronal differentiation (43% increase) and neurite outgrowth (11-fold increase) was observed.
3. Nanotechnology Strategies in Regenerative Medicine and Wound Healing
The application of nanotechnology in tissue engineering and stem cell biology has fostered new frontiers in research [77]. The novel design principles and characterization techniques, tunable intrinsic properties, and functional specificity can stimulate the integration of nanomaterials in regenerative medicine therapies [55]. A fundamental understanding of cell topographies especially insights on how the surrounding environment affects cellular behavior, and underlying physical interactions such as cell adhesion, proliferation using scaffold materials, and differentiation is essential in regulating signaling behavior and fate in regenerative medicine [55,78]. Brovkina and Dashinimaev reviewed various regenerative medicine approaches in diabetes mellitus [79]. Li et al. [80] reviewed the application of nanotechnology (nanomedicine, nanomedicine carriers, nanocontrast agents, and nanosensors) in diabetes management and diabetic regenerative medicine. Nanomaterial scaffolds that mimic the natural ECM assist in cell-scaffold interactions, formation of implanted/transplanted tissue-like structures, adhesion and exchange of oxygen, and transport of nutrients [80]. To improve therapeutic efficacy in diabetes management, nanoparticles were considered to modulate insulin release in response to changes in glucose concentration and protect insulin from degradation in the gastrointestinal environment [81,82,83]. Polymeric nanoparticles, nanocapsules, liposomes, and lipid nanoparticles are commonly employed in diabetes treatment [59]. These nanoparticle carriers can transport drugs to the target site, cross the intestinal epithelial barrier by protecting from environmental conditions, increase drug adsorption, and enhance receptor-mediated endocytosis [84,85]. The application of inorganic nanoparticles and polymer nanocomposite materials in early diagnosis and diabetes regenerative medicine has been reviewed [81,86,87,88].
3.1. Engineered Nanomaterials
Engineered nanomaterials or precisely engineered nano-bio interfaces have been shown to mimic the natural ECM and facilitate stem cell proliferation, migration, and differentiation into desired cell types [89,90], bone and cartilage repair, and nerve regeneration [90,91,92]. At the molecular level, engineered nanomaterials can be tailored by modulating the surface properties to provide localized, sustained release of biological molecules and increase therapeutic efficacy [93]. Przekora reviewed the application of engineered biomaterials in bone and cartilage regeneration for long-lasting antimicrobial protection [94]. Wu et al. developed nanotopography patterns in the forms of nano-(pillars, holes, and grills) on polycarbonate surfaces to study their effects on human MSC chondrogenesis [95]. Using nanoimprinting, nano-pillar, nano-hole, and nano-grill patterns were considered to represent topological cues in cartilage collagen fibril orientation. The nanotopographies were patterned on PCL film and chondroitin sulfate was immobilized on the surfaces to provide a chondro-inductive biochemical cue for MSC chondrogenesis [96,97]. MSCs on nano-grill and non-patterned surfaces showed an increased proliferation rate with significantly higher DNA amount at day 14 compared to day 1. The initial proliferation on the nano-grill was similar to the non-patterned surface but stopped by day 14. Comparatively, MSCs on nano-pillar and nano-hole surfaces underwent negligible proliferation; the DNA amount throughout the culture period was not significantly higher than that at day 1. The different nano-patterned topography affected the proliferation profile of MSCs. Significantly higher upregulation of hyaline chondrogenic markers and type II collagen was detected on nano-pillar and nano-hole surfaces, while expression of this marker was delayed, and were at lower levels on the nano-grill surface. The study demonstrated the effect of nano-topography on MSC chondrogenic differentiation; nano-topographical pattern triggered changes in MSC morphology and cytoskeletal structure, thereby affecting cell aggregation and differentiation.
3.2. Carbon Nanomaterials
Popov et al. proposed the application of carbon nanotubes as movable components of nano-electron mechanical systems (NEMS), nano-syringes, and jet nano-engines [98]. Carbon nanotube-based NEMS actuation was achieved using a nanomanipulator, electric field, and magnetic field. The electric dipole charged the movable core of the nanotube's wall and produced a dipole. A carbon nanotube with one open and another closed end served as a dipole that could be actuated with the help of a non-uniform electric field [98]. Chen et al. [99] investigated the application of iron-platinum alloy NPs for magnetic resonance imaging, regenerative medicine, hyperthermic ablation of cancer, and stem cell therapy.
Wang et al. [100] fabricated carbon nanotube-based composite scaffolds for cartilage tissue engineering. The single-wall carbon nanotubes (SWNT) were functionalized with -COOH groups (SWNT-COOHs) to reduce the biodegradation of native collagen in vivo and enhance biomechanical properties for composite scaffolds in tissue repair. The BMSC proliferation on the composite scaffold suggested that cells could enter the scaffold for adhesion and proliferation. At 7 days, the number of BMSCs in 2.0 wt% group was significantly higher than the 0, 0.5, and 1.0 wt% groups, and there was no obvious difference in the number of BMSCs between the three groups. To evaluate the restorative effects of scaffolds, a rabbit model of articular cartilage defects was constructed and filled with composite scaffolds (Figure 5). At four weeks after implantation, cartilage defects in the control group were hollow, and reddish granulation tissue at the bottom surface of defects was observed. Better filling of defects was observed in 0 wt%, 0.5 wt%, 1.0 wt% and 2.0 wt% groups, and no degradation was observed in the composite scaffolds. At eight weeks, the repairing effect of cartilage defects was improved, and the hollow in the control group was reduced by half. Increasing SWNT-COOH content promoted cell proliferation, but the longer degradation cycle of SWNT-COOH in vivo led to the lack of space for new tissues, resulting in poor repair effects.
The chondrogenic property of multi-walled carbon nanotubes (MWCNT) and hyaluronic acid (HA) as bio-ink additives was investigated for cartilage regeneration [101]. Live/dead analysis was performed to determine the hMSC-AT viability in the 3D scaffolds. A constant decrease in the total viability of cells was observed in the control medium. The biggest decline in cell viability was observed in the differentiation medium, despite the cells having the highest transcriptional activity. The decline in cell viability was not observed in MWCNT constructs, which indicated a protective effect on the cells. This may be due to the resemblance of CNT to collagen fibrils, which may have a stimulating effect on the cells. Scaffolds with MWCNTs and HA showed the highest viability of cells. MWCNTs had a favorable influence on cell viability while the inclusion of HA had a negative impact on the integrity of constructs.
Polyhydroxylated fullerene, fullerol was studied for the osteogenic differentiation of human ADSCs [102]. The effect of fullerol on osteogenic differentiation was determined independently and in combination with the osteogenic medium. The expression of osteogenic markers was elevated in the presence of a high dose of fullerol. Fullerol inhibited the gene expression of adipogenic markers and expression of osteogenic markers in mouse bone marrow stromal cell line, D1 cells. Fullerol was shown to be nontoxic toward human ADSCs at doses up to 10 μM, pre-treatment, co-treatment of fullerol enhanced the osteogenic capacity of human ADSCs in culture, and fullerol stimulated gene expression of FoxO1 and its target genes Runx2 and SOD2. As osteogenesis and adipogenesis are regarded to be closely correlated with the capacity of the progenitor cells during bone regeneration, fullerol was shown to inhibit the differentiation of marrow stromal cells and OP9 preadipocytes into adipocytes due to its scavenging activity against intracellular ROS. The study suggested that fullerol could serve as a novel pharmaceutical candidate to produce augmented bone regeneration.
CNT-coated and textured polydimethylsiloxane (PDMS) scaffolds were studied to support the growth of chondrocytes-cells that produce and maintain cartilage [103]. The COOH functionalization led to improved cell adhesion. In this study, four different scaffold architectures, namely flat (F) and textured (T) PDMS (F-PDMS and T-PDMS) were coated with multi-wall CNT-COOH (F-PDMS-CNT and T-PDMS-CNT) to enhance the nanoscale characteristics. The addition of CNTs atop PDMS produced an isotropic fibrous architecture and enhanced roughness that mimicked the structure in native cartilage. The chondrocytes were observed to form clusters to minimize cellular contact with the substrate. The nano level roughness increased by ∼270% and improved cell adhesion was observed with the addition of CNT coating on PDMS scaffolds.
Graphene oxide (GO) and reduced GO mats were investigated for neuronic differentiation of ADSCs which are the alternatives to MSCs and their ability to differentiate into neuron-like cells [104]. The study demonstrated that graphene nanomaterial-based mats served as suitable stem cell culture platforms for the neurogenic differentiation of ADSCs and GO accelerated the differentiation of ADSCs into neuron-like cells. Neuron-like cells exhibited typical neuronal morphology, and the growth, proliferation, and neurogenic differentiation rates of ADSCs seeded on GO mats were reported to be superior to those on other substrates.
PCL-based nanocomposite scaffolds in combination with GO nano-shells and osteogenic drugs, i.e. dexamethasone and simvastatin were fabricated to investigate the differentiation, cell viability, and biomineralization on MSCs and tissue restoration due to the local and controlled release of drugs [105]. The maximum release of dexamethasone from PCL/Dex and PCL/GO-Dex was 69.61 and 49.97%, while simvastatin release from PCL/Sim and PCL/GO-Sim was 84.02 and 99.27%, respectively. In presence of GO, less drug was encapsulated in scaffolds which may be due to the π-π stacking interactions between the drug and the GO nanosheets. Compared to other compositions and osteogenic mediums, PCL/GO-Dex nanocomposite had a higher ability to induce differentiation of MSCs to bone cells. Although the cell viability increased on PCL/GO and PCL/Dex scaffolds compared to PCL cultured for 7 days, it did not change significantly after 14 days.
Carbon nanofibers containing protein and protease inhibitors were synthesized to improve the therapeutic effect of carbon nanofibers on chronic wounds [106]. The preloaded particles were evenly distributed in the nanofibers. The proteins retain the biological activity and were continuously released from the nanofibers for more than four weeks. The carbon nanofibers exhibited good cell compatibility and supported cell adhesion and proliferation. Shen et al. [107] reported the inhibitory effect of carbon black (Printex 90) on the osteogenesis of bone-marrow-derived MSCs and the role of mitochondria in CB Printex 90-induced suppression of MSC osteogenesis. Printex 90 dosage of 0.03 μg/mL or below had no detrimental effect on cell viability. For osteogenic differentiation, Printex 90 was added to the osteogenic induction medium, replacing the regular culture medium once MSCs seeded in the culture plates reached 60% confluence [107]. Printex 90 caused the downregulation of osteoblastic markers, reduced the activity of alkaline phosphatase (ALP), and poor mineralization of osteogenically induced MSCs.
3.3. Bioactive Glass-Ceramic Nanoparticles and Nano-Silica Hydrogels
Bioactive glass is a group of inorganic bioactive materials based on Na2O, CaO, P2O5, and SiO2 systems that have shown to improve the vascularization, osteoblast adhesion, restoration, and reconstruction of the mineralized hard tissues, and differentiation of MSCs making them suitable candidates for bone regeneration medicine and stimulate the growth of regenerated tissues [108,109,110,111]. Bioactive glass is the first example of biomaterial discovered by Larry L. Hench in 1969 [112,113] that provided an alternative; second-generation, interfacial bonding of an implant with host tissues. Bioactive glass-ceramics fall under the category of Class A bioactive materials, characterized by their ability to support osteoconduction (growth of bone along the implant surface) and osteoinduction (the activation and recruitment of osteoprogenitor cells by the material, promoting bone growth directly on its surface) [114,115]. Over the years, studies have explored the potential of bioactive glass in the regeneration of cardiac, lung, and peripheral nerve tissues, restoration of the musculoskeletal system, and wound healing. Gerhardt and Boccaccini reviewed the fabrication methods of bioactive glass and glass-ceramic scaffolds and recent developments in tissue engineering [114]. The synthesis of sol–gel-derived bioactive glass nanoparticles (BGNs) in a 62 SiO2–34.5 CaO–3.2 P2O5 (mol %) composition in binary and ternary systems were performed along with the structural, morphological, and elemental characterization using Fourier transform infrared spectroscopy, X-ray diffraction analysis, scanning electron microscopy, elemental analysis, transmission electron microscopy, and solid-state nuclear magnetic resonance [116]. The osteoconductive behavior of BGN was assessed via in vitro biomineralization studies. For method 1 (M1) BGNs, the vibration peaks that confirmed the presence of a calcium phosphate phase after immersion in SBF were significantly lower than the spectra of method 2 (M2) BGNs. BGNs fabricated using the M2 protocol exhibited half network connectivity than M1 BGNs protocols due to higher calcium incorporation and can undergo a faster bioactive response. The details of the fabrication process are provided in the associated reference [116].
A three-dimensional porous bioactive glass-ceramic scaffold coated with HA-fatty acid was characterized for the first time by De Luca et al. [108] as bone tissue-engineering materials. To measure the bioactivity, HA-fatty acid conjugates were deposited on glass-derived scaffolds. The in vitro bioactivity tests showed a moderate increase in the solution pH (from 7.40 to 7.56 after 1 week), which was associated with the ion release from the surface of the scaffold to the simulated body fluid (SBF). The scaffolds soaked for 48 h in SBF showed the formation of a new phase composed of calcium-phosphate globular agglomerates. The coating of HA-fatty acid conjugate had no detrimental impact on the apatite-forming ability of the scaffolds. These novel bioactive glass-ceramic scaffold biomaterials hold promise for bone repair due to their apatite-forming and tissue regenerative potential.
AuNPs/Au and Ag NPs-containing bioactive glasses in biopolymer composites were studied to enhance bone regeneration and tested in vivo and in vitro on fibroblast and osteoblast cell lines [117]. The compatibility of Alg-Pll-BGAuSP and Alg-Pll-BGAuNCs composites was investigated. The overall viability for the human fibroblast cell line (BJ CRL 2522TM) was between 91 and 110% after 24 h, with the highest viability (110%) obtained in the presence of Alg-Pll-βTCP/HA sample. Alg-Pll-BGAuSP composite (104%) showed the most beneficial effects for bone proliferation. A multifunctional bioactive Si−Ca−P−Mo glass-ceramic nanoparticle (BBGN) with inlaid molybdate nanocrystals was synthesized for post-surgical melanoma therapy and skin reconstruction [118]. The BBGN exhibited strong antioxidant activity, high photothermal conversion efficiency, low toxicity, and efficient infection therapy. The broad-spectrum antibacterial efficiency against Staphylococcus aureus (S. aureus), Escherichia coli (E. coli), and MRSA in vitro was considered. After contact with BBGN-Mo (B-M) samples for 12 h, three bacterial strains were not significantly inhibited compared to the control group. B-0 M with 10 min of 808 nm laser irradiation (B-0M+) showed a 32.7% kill ratio for S. aureus, a 47.6% kill ratio for E. coli, and a 46.8% ratio for MRSA, while the control+ group showed no obvious antibacterial effect (<10%). More than 98.9% of S. aureus, E. coli, and MRSA were killed after being cultured with the B-15M+ groups. These results confirmed that the effective photothermal property of B-15 M could provide a better therapeutic condition for infected wounds after surgery.
Khatami et al. reported the osteogenic properties of alginate-nano-silica hydrogels enriched with collagen and gelatin on human osteoblast-like MG-63 cells [119]. The osteogenic potential was measured by alkaline phosphatase activity. The addition of collagen and gelatin increased the cell proliferation rate. Biochemical analysis and Alizarin red S staining showed collagen-induced osteogenesis by induction of alkaline phosphatase and matrix mineralization.
A novel silver-doped (BG-Ag) and gold-doped (BG-Au) quaternary 46S6 bioactive glass was synthesized and the cytotoxic effect was studied on osteosarcoma MG-63 cells for potential bone regeneration application [120]. The melt-derived BG was doped with 0.006 and 0.01 ppm concentrations for AgNPs (AuNPs) yielding BG-Ag1 (BG-Au1) and BG-Ag2 (BG-Au2) composites. The cell proliferation profiles of osteosarcoma MG-63 cells upon treatment with different concentrations of BG, BG-Ag1, BG-Ag2, BG-Au1, and BG-Au2 was considered. BG, BG-Ag1, BG-Ag2, BG-Au1, and BG-Au2 induced the proliferation of the MG-63 cells in different patterns. As these formulations were in low dosages (0, 2, 4, 6, 8, and 10 μg ml−1), it suggested that the elevation pattern in the cell proliferation occurred even at low concentrations. The proliferation of MG-63 cells significantly increased relative to the control recording 141.25% at a dosage of 6 μg ml−1. Even though the proliferation declined significantly to 128.40% and 128.61% at dosages of 8 and 10 μg ml−1, respectively, it remained higher than the control. These results demonstrated the good compatibility of BG and metal-doped BG nanohybrids with MG63 cells and their non-cytotoxic effect on these cells [120].
Hydrogels based on mesoporous silica nanoparticles (MSNs) due to their porous homogeneous structure, biocompatibility, high surface area, and easy modification of core and shell chemistry, are ideal candidates to mimic the ECM of native tissues and in regenerative medicine [121]. A thiol surface-functionalized MSNs (MSN-SH) capable of acting as a crosslinker with thiol-modified polyethylene glycol (PEG-SH) was developed [121]. The mechanical and self-healing properties of these 3D networks were investigated via macroscopic self-healing and rheological recovery tests. A higher MSN concentration of 7 wt% did not influence the self-healing behavior. The recovery of MSN7-PEG was slightly decreased after applying 500% strain due to the higher MSN content in the network. The hydrogels were stable under physiological conditions but degraded in a glutathione-containing environment over six weeks. The hMSCs were encapsulated inside MSN-PEG nanocomposites signifying that these materials may find application as bioinks in 3D printing technology.
3.4. Hydroxyapatites
Calcium phosphate (CaP)-based biomaterials due to their resemblance to the chemical composition of natural minerals are widely researched for cell attachment, proliferation, and differentiation in bone defect repair [122]. Various CaP-based biomaterials were utilized in bone regeneration, including tricalcium phosphate, hydroxyapatite (HAP), amorphous calcium phosphate, octacalcium phosphate, dicalcium phosphate anhydrous, dibasic calcium phosphate dihydrate, and tetracalcium phosphate [123]. HAP is the most thermally stable crystalline phase of CaP used in the form of ceramics or composite scaffolds with polymers [122]. Huang et al. [124] synthesized a biomimetic and injectable hydrogel scaffold based on nano-HAP, collagen (Col), and chitosan (Chi) as workable systemic minimally invasive scaffolds in bone-defect repair and bone tissue engineering. The results from SEM, TEM, and XPS suggested that Chi/HA/Col showed surface properties similar to physiological bone, and the peaks of the FT-IR spectrum were in cognate with the peaks associated with natural bone. A mixture of palladium and platinum (Pt) nanoparticles, called PAPLAL, was studied for aging-related skin pathologies in mice [125]. PAPLAL did not cause any morphological abnormalities, such as cell infiltration PAPLAL deposition, or cellular damage in mouse skin, and exhibited potent antioxidant activity (attributed to the effects of Pt nanoparticles) and attenuated aging-related skin pathologies in vivo.
Non-woven multifunctional nano- and microfiber scaffolds were fabricated using a block copolymer of PCL and poly(lactic acid) (PLA) (PL-b-CL) as a matrix and HAP as a functional agent, dissolved in a binary solvent mixture to produce electro spun scaffolds with porous fibers [126]. The nanofibrous scaffolds were shown to mimic bone ECM. SaOS-2, an osteosarcoma cell line, displayed several osteoblastic features, namely the capacity to deposit a mineralization-competent ECM as an in vitro model of mature osteoblasts. The cells grown on scaffolds with HAP exhibited significantly higher metabolic activity than pristine PL-b-CL. Cell adhesion results suggested that the cells adhered and proliferated, with no substantial cell loss during the experimental period. Cell attachment was influenced by the physical and chemical properties of the scaffolds, namely functional groups, solubility, crystallinity, electric charge, surface energy, surface roughness, topography, pore size, and stiffness. This was the first study to demonstrate that scaffolds created from a PCL and PLA block copolymer with embedded HAP NPs could enhance the potential of scaffolds for bone tissue engineering applications [126].
Chitosan (CS) hydrogel reinforced with hydroxyapatite nanorod (HAPNr) composite materials was developed for biomedical hydrogels and articular cartilage regeneration [127]. The in vitro cytotoxicity of the composite hydrogel towards L929 cell lines was tested using an MTT assay. The potential cytotoxicity of CS and CS/1.5HAPNr hydrogels was compared with the control. Phytohaemagglutinin exhibited the highest cell viability (112%) and CS/1.5 HAPNr (96 ± 0.41%) showed better cell proliferation than pristine CS (90 ± 0.63%). Thus, HAPNr incorporated into the CS matrix showed the best results in CS/1.5HAPNr composite gels. L929 mouse fibroblast cells exhibited a fusiform morphology, and most cells spread and proliferated on the culture plate. The developed hydrogels exhibited no apparent cytotoxicity to L929 within incubation for 72 h and without significant cytotoxicity towards mammalian cells. The CS/1.5HAPNr composite hydrogel may be a potential biomaterial for tissue engineering cartilage regeneration.
A biphasic cartilage and bone-like scaffold combined with HAP was developed for osteochondral tissue engineering [128]. Three types of self-organized biphasic artificial cartilage–HAP conjugates from only three cartilage components, HA, AG, and type II collagen in vitro were implanted into an osteochondral defect in rat knee joints, bone, and cartilage tissues (see Figure 6). The SEM micrographs revealed a fibrous, 3D reticulate structure (Figure 6B). Incubation of the chondrocytes with AG/HA/collagen complex for 1 or 2 weeks, suggested the chondrocytes to be homogeneously present on the scaffold. Cytoplasmatic extensions denominated the phylopodia, on the surface of the self-organized scaffolds, indicating that chondrocytes were alive within the tissue after the 2-week incubation (Figure 6C).
To investigate the role of scaffold implantation in knee cartilage defects, in control right knee joints, defects were filled with scar tissue and there were clefts between the scar tissue and the healthy surrounding cartilage tissue. In the left knee joints, defects were filled with repair tissue similar to the surrounding cartilage tissue. In the right knee joints, only fibrous scar tissue with hyperplasia of spindle-shaped fibroblastic cells was observed in the defect, with no regeneration of the cartilage tissue. In the scaffold-implanted left knee joint, a stratiform cartilage-like structure with the formation of cartilage cavities and the growth of chondrocytes was observed in the scaffold implantation hole, indicating initiation of cartilage regeneration induced by the implanted scaffold. The success rates of osteochondral tissue regeneration were 33% in the self-organized AG/HA/ collagen complex-inoculated group, 50% in the self-assembled AG/HA/collagen complex–HAP powder (40 nm size) conjugate-inoculated group, 75% in the self-assembled AG/HA/collagen complex–HAP powder (5 µm size) conjugate-inoculated group and 100% in the self-assembled AG/HA/ collagen complex–HAP block conjugate-implanted group [128]. The study showed evidence that the cartilage-like scaffold, without conjugated HAP, was insufficient to regenerate damaged subchondral bone tissue. The self-organized cartilage-like biomaterial conjugated with HAP has the potential to repair not only articular cartilage defects but also the degenerated subchondral bone in diseases with osteochondral defects.
Nano-crystalline hydroxyapatite (nHAP) was used to determine how the differentiation of hMSCs was influenced by nHAP loading and bone-like scaffolds [129]. The nHAP dispersed in polymeric composites at >22 wt% loading induced osteoblast differentiation in vitro via the PiT1 and Erk1/2 signaling pathways. When nHAP-poly(thioketal urethane) nHAP-PTKUR scaffolds were implanted in two anatomic sites in rats, the femoral diaphysis and femoral metaphysis, new cartilage was observed in the absence of nHAP at diaphyseal but not at the metaphyseal sites. New bone formation increased with nHAP loading at metaphyseal but not diaphyseal sites. Thus, nHAP composite scaffolds induced osteogenic differentiation of adherent endogenous progenitor cells in a dose-dependent manner. nHAP-PTKUR scaffolds promoted intramembranous and endochondral ossification dependent on material formulation and anatomic sites, indicating the importance of these factors as key regulators in assessing overall outcomes and the efficacy of novel biomaterials for bone regeneration.
Huang et al. [130] developed a gelatin/HAP hybrid material using microextrusion 3D bioprinting and enzymatic cross-linking as the scaffold for human umbilical cord blood-derived mesenchymal stem cells (hUCB-MSCs) differentiation and repair of knee cartilage defects. 10% of gelatin with 5% volume weight of HAP yielded the best gelation kinetics and rheological properties suitable for 3D printing, and this composition was then employed to print gelatin scaffolds. The cytotoxicity of hydrogel materials was measured by culturing hUCB-MSCs in the extracted solutions of the scaffolds (Figure 7A). Although HAP doping slightly increased the cytotoxicity, the extract solutions supported a high cell viability of >75% as shown in Figure 7B. The scaffold material promoted the proliferation of hUCB-MSCs as indicated by a continuous increase in the cell population (Figure 7C) and provided a platform for cell migration. The 3D printing of gelatin scaffolds assisted by enzymatic cross-linking, and HAP doping strengthened the ability of the gelatin scaffold to promote chondrogenic differentiation of stem cells. Gelatin/HAP scaffold with hUCB-MSCs repaired acute knee cartilage defects and holds promise in cartilage repair.
Composite materials based on chitosan, HAP, and riboflavin were shown to have an inhibitory effect on Staphylococcus aureus and exhibited higher antioxidant activity compared to pure chitosan [131]. The antioxidant and antimicrobial potential of the active biomaterial was examined. The incorporation of RF increased antioxidant activity compared to pure and HAP–doped chitosan; the inhibitory effect on Staphylococcus aureus and the number of colony-forming units was significantly reduced. The presence of riboflavin in the yeast extract was examined by vibration spectroscopy. The potential effect of RF on cell metabolic activity was tested using the MTT assay. The treatment with riboflavin increased cell metabolic activity significantly, especially when exposed to the isolated vitamin from a microorganism. Compared to existing technologies for chitosan/HAP scaffold, doping with riboflavin showed superior antimicrobial potential and antioxidant activity. Chitosan-collagen-HAP (Cs/Col/HAP) composites are bioactive, biocompatible, and multifunctional biomaterials that find application in tissue engineering [132]. SEM micrograph of the composite membrane showed that the chitosan membrane was aligned in fibers, with pores sizes in the range of 80 nm to 2 µm. The addition of collagen changed the morphology of the Cs membrane. At low collagen content, pleats were observed, and areas surrounded by fibers suggested that collagen regions were blended into the chitosan matrix. At high collagen content, a uniform morphology was observed characteristic of polymer blends. The cell viability was measured by MTS for buccal fat pad (hBFP)-MSCs. The membranes with the highest collagen and/or HAP content showed the highest cell adhesion values for in vitro cultured hBFP-MSC. The membranes with low collagen and/or low HAP content showed similar cell viability compared to pure chitosan membranes. The largest cell viability was obtained when both compounds were present in the chitosan membrane with the highest collagen and HAP (Cs/0.75collagen/0.75 HAP) content, showing 75% higher viability than pure chitosan. The study proposed that membranes obtained by combining chitosan with collagen and HAP enhanced cell adhesion ability, compared to the chitosan membranes alone.
A partially crystallized CaP and dicalcium phosphate anhydrate particles incorporated with black phosphorous nanosheets (BPNSs) was used to prepare calcium phosphate bone cements (CPCs) for potential application for bone regeneration [133]. The physicochemical, photothermal, biodegradability, cytotoxicity, and osteoinductive properties of CPCs was investigated to develop an innovative bone defect repair material. SEM images of cells adhered to the surface of bone cement was studied for 1 and 24 h. At 1 h, cell morphology on the CPC surface was spherical, but on the 100 BP/CPC surface, the morphology was irregular, and on the 200 BP/CPC surface, the morphology of cells was similar to that of 100 BP/CPC, and there were more pseudopodia. After 24 h of coculture, the cells on the three kinds of bone cements were long spindle-shaped, and many plate pseudopodia and filamentous pseudopodia appeared. The BP/CPC was able to promote cell adhesion in the early stage and established the biocompatibility of BP/CPC. The addition of black phosphorus enhanced the strength of the bone cement. BP/CPC induced cell growth and showed very low or no toxicity for MC3T3-E1 cells. Osteoblast development experiments indicated that BP/CPC under near-infrared conditions accelerated the mineralization of the bone cement and promoted the upregulation of osteogenic marker proteins in cells.
3.5. Magnesium Oxide Alloys
Magnesium (Mg) alloys were shown to stimulate bone formation, increase new bone quality, promote the growth of bone tissues, and induce bone cell activation [134,135,136]. Mg-based implants were also efficient in stabilizing fractures and aiding the healing process [137]. Lui et al. [135] developed a series of novel Mg-Cu alloys, Mg-0.05Cu, Mg-0.2Cu, and Mg-0.5Cu, and studied their osteogenesis and angiogenesis performance, and antibacterial properties in vitro to offer insights into the feasibility of orthopedic application. The proliferation of preosteoblasts (MC3T3-E1) and endothelial cells (HUVECs) in the extraction media of Mg-Cu alloys and pure Mg was studied for 1, 3, and 5 days. Less cell proliferation was observed from the Mg-Cu alloys after 3 and 5 days. Cu depressed MC3T3-E1 cell proliferation; in HUVECs, Mg-0.03Cu showed the most cell proliferation after 1, 3, and 5 days while Mg-0.57Cu exhibited the opposite response. The MC3T3-E1 cells cultured in Mg-0.03Cu and Mg-0.19Cu extracts showed more plump focal adhesion via well-organized F-actin stress fibers (red filaments) compared to pure Mg and Mg-0.57Cu. The aggregation of HUVECs diminished with an increase in Cu concentration, and the cell status deteriorated slightly, indicating that Mg-0.03Cu and Mg-0.19Cu extracts were favorable to the initial attachment and spreading of HUVECs and MC3T3-E1 cells. Thus, Mg-Cu alloys provided better antibacterial performance than pure Mg due to the synergistic effects of high alkalinity and Cu release, suggesting that the alloys had great potential in orthopedic applications.
Li et al. [136] reported the post-degradation effect of pure Mg, Mg-1Y, Mg-5Al, and Mg-2Ca alloys for the differentiation, proliferation, and gene expression of human mesenchymal stem cells (hMSCs). Mg2+ ions increased cell proliferation, and a maximum concentration of approximately 8.0 × 10-4 M was favorable for ATP production, above which ATP production began to decrease. Mg-2Ca alloy had minimal effect on osteogenic differentiation, with Mg-1Y and pure Mg having a superior effect on the proliferation and differentiation of hMSCs. A novel Ti-Mo-Cu alloy was developed for biomedical implant applications. Cu was added to the Ti-Mo matrix and the effects of Cu content on microstructure, tensile properties, cytocompatibility, and bacterial inhibitory effect were investigated. MC3T3-E1 cells were used to evaluate the cytocompatibility of Ti–10Mo-xCu alloy for bone implants. No adverse effects of Ti-10Mo-xCu alloy were generated on the MC3T3-E1 cell proliferation, and the cytotoxicity level was extremely low. With the increase in Cu content, the bacterial inhibitory rates of Ti-10Mo-xCu alloy increased gradually. The Ti-10Mo-3Cu alloy exhibited high strength, excellent cytocompatibility, good elongation, and bacterial inhibitory properties, suggesting their potential application as a medical implant material.
An immunomodulatory multicellular scaffold based on manganese silicate (MnS) nanoparticles with tendon/bone-related cells was fabricated for integrated regenerative recovery of tendon-to-bone injury [138]. The MnS nanoparticles were shown to enhance the specific differentiation of multicellular scaffolds via regulating macrophages. This was attributed to the secretion of PGE2 in macrophages induced by Mn ions. The tendon stem/progenitor cells (TSPCs) and BMSCs were distributed in the scaffold in a layered manner, and the multicellular MnS-based nanoparticles scaffolds were implanted into macrophage-depleted rats to reveal the role of immunomodulatory processes in the differentiation of scaffolds. The Mn ions stimulated macrophages to secrete more PGE2 and a notable enhancement in the secretion of PGE2 in macrophages suggested that Mn ions could induce the secretion of PGE2 in macrophages to enhance the tenogenic differentiation of TSPCs and osteogenic differentiation of BMSCs and promote tissue regeneration.
3.6. Gold Nanoparticles
AuNPs proffer tunable size, surface functionalization, unique physiochemical properties, and surface plasmon resonance with light at a wavelength of 520 nm [139], making it a suitable candidate in biomedicine, drug delivery, and bioimaging [140,141]. Using coarse-grained molecular dynamics, Gupta and Rai [142], reported the diffusion coefficient, interaction between AuNPs and skin lipids, and permeation ability of neutral AuNPs (2–5 nm) coated with dodecanethiol and surface charges (cationic and anionic) through a model skin lipid membrane (Figure 8). The neutral hydrophobic AuNPs disrupted the bilayer and penetrated with in ~200 ns, while charged AuNPs were adsorbed on the bilayer headgroup. The 2 nm AuNP did not induce significant structural changes in the bilayer while bigger AuNPs (3–5 nm) changed the structure and packing. The permeability was maximum for neutral 2 nm AuNP and minimum for 3 nm cationic AuNP. The AuNPs induced undulation in the bilayer which increased with the size of the AuNP. AuNP created vacancies in the bilayer interior. The permeation free energy calculation revealed that at the head group of the bilayer, a very small barrier existed for neutral hydrophobic AuNP while a free energy minimum was observed for charged AuNPs. Neutral hydrophobic AuNPs reduced the local and overall order parameter of the bilayers or in other words created more disruptions in the bilayer. The smaller neutral hydrophobic AuNP was more permeable compared to bigger AuNPs and charged AuNPs experienced resistance to permeation in the bilayer interior.
Lin et. al. [140] evaluated the biological performance (cell viability) of AuNPs towards MSCs by analyzing the optimal AuNP concentration for tissue engineering efficacy. The cell viability percentage of MSCs influenced by the various AuNP treatments at 24, 48, and 72 h was investigated. The semi-quantified data at 24 h showed that AuNPs at 1.25 and 2.5 ppm stimulated the lowest production of ROS. While MSCs were incubated with AuNP 1.25 and 2.5 ppm treatments, the proliferation and antioxidant capacity of MSCs was strengthened considerably (Figure 9). The MSC adhesion ability stimulated by the as-prepared AuNP solutions showed that MSCs’ morphology was enhanced when treated with 1.25 and 2.5 ppm AuNPs, demonstrating improved cell adhesion and migration capacity. This elucidated that AuNPs at 1.25 and 2.5 ppm concentrations were a better biocompatibility nanomaterial. The synthesized AuNPs fabricated with polymeric biomaterials had superior potential for clinical applications with good biosafety owing to the minimal toxicity effects without reducing agents.
AuNPs were shown to promote the differentiation of osteoblastic MC3T3-E1 cells and antimycin A-induced mitochondrial dysfunction using an MTT assay [143]. MC3T3-E1 pre-osteoblastic cell line is widely used as a cell culture model for osteoblast differentiation. A significant increase in cell growth was revealed by the treatment of 5, 10, and 20 nm AuNPs at the concentrations of 1∼10, 2∼10, and 1∼10 μg/mL, respectively, which suggested that AuNPs did not induce any cytotoxicity and stimulated osteoblast growth. AuNPs having a diameter of 10 nm considerably promoted osteogenesis through activating earlier osteogenic differentiation. Thus, AuNP increased the bone matrix by stimulating ALP activity, collagen synthesis, and osteocalcin synthesis in osteoblastic MC3T3-E1 cells. AuNPs had a) a protective effect against oxidative stress-induced dysfunction in osteoblasts, b) a stimulating effect on the early differentiation stages of osteoblasts, and c) protecting osteoblasts from antimycin A-induced cell damage.
In soft tissue augmentation, AuNP-collagen constructs (AuNP-CC) were applied as soft tissue fillers to investigate the biodegradability and local tissue reaction of AuNP-collagen fillers compared to commercially available hyaluronic acid and cross-linked collagen fillers [144]. Two conjugates were constructed: AuNP-CC1 was fabricated with the addition of 10% of pre-polymerized porcine Type I collagen. AuNP-CC2 was fabricated with the addition of 3% glycerin. The tissue response (neovascularization and granulation tissue) scores for the cohorts were investigated at 1, 3, and 6 months. Cross-linked collagen, AuNP-CC1, and AuNP-CC2 demonstrated slight to mild neovascularization and scored in the mild to moderate range for granulation tissue. The AuNP-CC formulations scored in the slight to mild range for granulation tissue. By 6 months, the cross-linked collagen demonstrated mild to moderate neovascularization and was in the mild range for granulation tissue. The AuNP-CC formulations scored slight to mild in each category. Cross-linked collagen showed increased tissue response scores over time. AuNP-CC2 had a similar response with increasing tissue response scores, however, the irritancy scores were more stable over time. These responses indicated active resorption of the constructs along with active remodeling [144].
The biomedical applications of AuNPs have been extended to the wound-healing process [145,146]. Poomrattanangoon and Pissuwan [147] synthesized AuNPs coated with Collagen-I (Collagen-I@AuNPs) and human skin fibroblasts (HSF) were studied as model cells for wound closure, cell proliferation, pro-inflammatory responses, growth factor generation, and in vitro wound healing. Attenuated total reflectance (ATR)-FTIR measurements confirmed a change in the structure of Collagen-I and AuNPs resulting from the interaction between Collagen-I and AuNPs. The AuNPs and Collagen-I@AuNPs at different concentrations (3, 5, 10, 15, and 25 μg mL−1) were applied to HSF cells and cell viability was measured. When HSF cells were treated with Collagen-I@AuNPs, HSF cell viability was slightly higher than cells treated with only AuNPs. The cell viability of HSF cells after treating with 3, 5, 10, 15, and 25 μg mL−1 of Collagen-I@AuNPs were 100.38 ± 3.51, 101.87 ± 2.40, 101.43 ± 2.32, 97.18 ± 2.25, and 97.40 ± 1.18 % respectively (Figure 10). Compared to control cells, a significant reduction in cell viability was found in HSF cells treated with AuNPs at concentrations of 15 and 25 μg mL−1.
In vitro measurements using wound scratch assay were considered to study the effects of AuNPs and Collagen-I@AuNPs on wound healing. The scratched HSF cells treated with AuNPs and Collagen-I@AuNPs had a higher wound closure percentage than the control cells. The percentages of wound closure of ∼57.16 ± 1.31 and ∼67.67 ± 1.67 % were found in scratched HSF cells treated with AuNPs and Collagen-I@AuNPs for 24 h (Figure 11). After 24 h of treatment, Collagen-I@AuNPs (67.67 ± 1.67 % wound closure) accelerated the healing process of scratched HSF cells compared to AuNPs (57.16 ± 1.31 % wound closure). After 48 h, the percentage of wound closure in scratched HSF cells treated with AuNPs (91.01 ± 2.71 %) and Collagen-I@AuNPs (95.19 ± 1.67 %) increased compared to that at 24 h. The percentage of wound closure in untreated cells increased to 59.96 ± 2.66 %. This suggested that Collagen-I protein was vital in enhancing wound closure. The wound closure percentage of scratched HSF cells treated with AuNPs was enhanced, compared to untreated scratched HSF cells, which may be attributed to the antioxidative effects of AuNPs [147].
3.7. Biomimetic Natural Biomaterials
Lie et al. reviewed recent advances in the fabrication, functionality, and potential applications of biomimetic natural biomaterials [148]. Biomimetic natural biomaterials, due to their nontoxicity, non-genotoxicity, and non-teratogenicity to native healthy tissue, were incorporated into tissue engineering applications. Polylactic acid, polyhydroxyalkanoates and their derivatives, HA, alginate, cellulose, and chitosan, as well as collagen, gelatin, fibroin, poly-glutamic acids, and antimicrobial peptides, are the commonly used biomimetic natural biomaterials. The development of biomimetic natural biomaterials that replicate the biological and physicochemical characteristics of natural ECM incorporates additional functionalities and enhanced therapeutic effects, as illustrated in Figure 12.
4. Challenges with the Application of Inorganic Biomaterials in Regenerative Medicine
Clinical application of inorganic biomaterials in regenerative medicine confronts challenges, including, but not limited to, long-term fate in biocompatibility and bioaccumulation, nanoparticle/nanomaterial toxicity, better assessment tools, optimizing the mechanical properties, stem cell fate, and so on. The toxicity, carcinogenicity, bioaccumulation, and teratogenicity of nanoparticles are dose- and exposure-dependent [65]. Advances in materials science and engineering technology for designing and applying biomimetic 3D-printed degradable scaffolds have paved the way for pioneering research strategies in regenerative therapy [149]. E.g. a biocompatible, high-performance semicrystalline polymer, poly (ether-ether-ketone) (PEEK), named bone cement, was one of the most prominent candidates in manufacturing bone implants approved by the FDA [150,151]. Since PEEK is chemically inert and has poor integration, incorporating bioactive metals such as strontium or hydroxyapatite could stimulate cell differentiation [151,152]. Thus, the design and development of ‘immune interactive’ biomaterials can minimize immune response [153], such as mediating macrophage polarization, decreasing body rejection, and governing the outcome of tissue engineering and regenerative therapy [151].
Lele et al. [154] performed a detailed study of engineered biomaterials for different clinical trials and specific diseases. Ophthalmic disease had the highest number of clinical trials followed by diseases of blood vessels and the oral cavity (Figure 13). Clinical trials suggested that synthetic polymers can be used in the fabrication of contact lenses in the treatment of ophthalmic diseases, while natural polymers can be used in the treatment of skin diseases. Dental applications utilized autologous biomaterials, ceramics, and composites. Metals and combination materials, such as polymers coated on metals, were ubiquitous for treating coronary artery disease.
Tissue-engineered constructs have been used successfully in skin, bladder, bones, and cartilage repair [7]. Engineered tissue constructs can be assembled from primary cells or specific tissue culture lines: fibroblasts, endothelial cells, or cardiac muscle [155]. However, tissue constructs may not be able to seamlessly mimic the biological tissue due to differences in structure, organization, and lower cell density [155]. This gives rise to functional differences. Tissue engineering constructs also require a continued blood supply for long-term stability following implantation [156]. Thus, a continuing goal is to develop engineered tissue constructs with mechanical, structural, and functional properties that mimic biological tissue function and provide cues to diverse intercellular interactions.
Chronic wound healing is another area of regenerative medicine, currently undergoing clinical trials. Advanced wound care approaches, such as stem cells, biomaterials, and innovative treatment techniques are integrated to promote tissue regeneration and healing. However, there have been limited clinical case studies for bone tissue engineering using scaffolds and osteogenic cells, pointing to the slow advances in clinical tissue engineering [8,157]. Tissue rejection, challenges in surgical reconstruction, and lack of donor tissues are some of the major drawbacks that may impair the integration of inorganic biomaterials with natural tissues or organs to drive cell differentiation. Further, scalability, cost, regulatory issues, and uptake are other factors that largely limit the clinical translation of complex structures [158,159]. Also, ethical concerns concerning the utilization of tissue cells and human embryonic stem cells cannot be sidelined. Thus, clinical translation of regenerative medicine requires the development of appropriate guidelines for the safe and effective delivery of regenerative medicine strategies. The involvement of start-up corporations and enterprises is essential for streamlining the development of innovative therapies, and the speedy and effective delivery of regenerative medicine to physicians and patients [160]. These advances are pivotal in advancing cutting-edge research and facilitating clinical applications. By bridging the gap between laboratory research and practical implementation, they ensure that breakthroughs in regenerative medicine reach those in need more quickly and efficiently.
5. Conclusions
Regenerative medicine and tissue engineering integrate engineering, materials science, clinical translation, stem cell science, and biology to promote the regeneration of diseased tissues and the formation of new tissues and organ systems. Advances in regenerative engineering have significantly improved the management of traumatic patients requiring organ replacement and/or repair, while also promoting the development of biological substitutes for diseased or damaged tissues. These innovations offer renewed hope for augmenting patient recovery and long-term outcomes in severe injury, trauma, or chronic situations. The review provides a comprehensive perspective on recent progress, development, and application of inorganic-based nanoparticles and biomaterials in tissue engineering and regenerative therapy. At the intersection of biomaterial science and nanotechnology, inorganic biomaterials are extensively being studied for diagnostic, imaging, therapeutic delivery applications, and regenerative medicine. Development of inorganic biomaterials to stimulate new cells and regenerative tissue involves a detailed understanding of 1) fabrication techniques, 2) development of composition, morphology, and functionality, and 3) optimizing the mechanical and bioactive properties to obtain the desired function. Technical advances have facilitated the fabrication of engineered tissue constructs and tailor-made grafts that mimic natural tissue. Given the complexity of tissue engineering procedures, interdisciplinary collaboration between engineers, scientists, biologists, and clinical specialists is much sought to guide novel technological advancements in regenerative medicine. This review also discusses the challenges and opportunities of combining regenerative medicine strategies with inorganic-based nanoparticles and biomaterials. The increasing use of combined strategies in regenerative medicine presents a promising avenue for integrating current state-of-the-art techniques, applications, and prospects for their use in clinical trials and modern medicine.
Funding
This research received no external funding.
Conflicts of Interest
The author has no conflict of interest.
References
- Mao, A.S.; Mooney, D.J. Regenerative Medicine: Current Therapies and Future Directions. Proc. Natl. Acad. Sci. U.S.A. 2015, 112(47), 14452. [Google Scholar] [CrossRef] [PubMed]
- Mason, C.; Dunnill, P. A Brief Definition of Regenerative Medicine. Regen. Med. 2008, 3(1), 1. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Li, S.; Yu, Q.; Chen, T.; Liu, D. Application of Stem Cells in Regeneration Medicine. MedComm (2020) 2023, 4(4), e291. [Google Scholar] [CrossRef] [PubMed]
- McKinley, K.L.; Longaker, M.T.; Naik, S. Emerging Frontiers in Regenerative Medicine. Science 2023, 380(6647), 796. [Google Scholar] [CrossRef]
- Bianchi, E.; Vigani, B.; Viseras, C.; Ferrari, F.; Rossi, S.; Sandri, G. Inorganic Nanomaterials in Tissue Engineering. Pharmaceutics 2022, 14, 1127. [Google Scholar] [CrossRef]
- Salgado, A.J.; Oliveira, J.M.; Martins, A.; Teixeira, F.G.; Silva, N.A.; Neves, N.M.; Sousa, N.; Reis, R.L. Chapter One - Tissue Engineering and Regenerative Medicine: Past, Present, and Future. International Review of Neurobiology, Academic Press 2013, 108, 1. [Google Scholar] [CrossRef]
- O'Brien, F.J. Biomaterials & Scaffolds For Tissue Engineering. Materials Today 2011, 14(3), 88. [Google Scholar] [CrossRef]
- Ikada, Y. Challenges in Tissue Engineering. J. R. Soc. Interface 2006, 3(10), 589. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, W.; Yao, Q. Copper-based Biomaterials For Bone and Cartilage Tissue Engineering. J. Orthop. Translat. 2021, 29, 60. [Google Scholar] [CrossRef]
- Yun, Y.R.; Won, J.E.; Jeon, E.; Lee, S.; Kang, W.; Jo, H.; Jang, J.H.; Shin, U.S.; Kim, H.W. Fibroblast Growth Factors: Biology, Function, and Application For Tissue Regeneration. J. Tissue Eng. 2010, 2010, 218142. [Google Scholar] [CrossRef]
- Sheikh. Z.; Javaid, M.A.; Hamdan, N.; Hashmi, R. Bone Regeneration Using Bone Morphogenetic Proteins and Various Biomaterial Carriers. Materials (Basel), 2015, 8(4), 1778. [CrossRef]
- Katagiri, T.; Watabe, T. Bone Morphogenetic Proteins. Cold Spring Harb. Perspect. Biol. 2016, 8(6), a021899. [Google Scholar] [CrossRef] [PubMed]
- Lademann, F.; Hofbauer, L.C.; Rauner, M. The Bone Morphogenetic Protein Pathway: The Osteoclastic Perspective. Front. Cell Dev. Biol. 2020, 8, 586031. [Google Scholar] [CrossRef] [PubMed]
- Zakrzewski, W.; Dobrzyński, M.; Szymonowicz, M.; Rybak, Z. Stem Cells: Past, Present, and Future. Stem Cell Res. Ther. 2019, 10(1), 68. [Google Scholar] [CrossRef] [PubMed]
- Kolios, G.; Moodley, Y. Introduction to stem cells and regenerative medicine. Respiration 2013, 85(1), 3. [Google Scholar] [CrossRef]
- Abdal Dayem, A.M.; Saadeldin, I.M.; Zhang, S. Editorial: Crosslinking ROS signaling and stem cells. Front. Cell Dev. Biol. 2022, 10, 1101802. [Google Scholar] [CrossRef]
- Amini, A.R., Laurencin, C.T.; Nukavarapu, S.P. Bone Tissue Engineering: Recent Advances and Challenges. Crit. Rev. Biomed. Eng. 2012, 40(5), 363. [CrossRef]
- Zhang, C.P.; Fu, X.B. Therapeutic Potential of Stem Cells in Skin Repair and Regeneration. Chin. J. Traumatol. 2008, 11(4), 209. [Google Scholar] [CrossRef]
- Zhang, W.; Huang, X. Stem Cell-Based Drug Delivery Strategy For Skin Regeneration and Wound Healing: Potential Clinical Applications. Inflamm. Regen. 2023, 43(1), 33. [Google Scholar] [CrossRef]
- Duscher, D.; Barrera, J.; Wong, V.W.; Maan, Z.N.; Whittam, A.J.; Januszyk, M.; Gurtner, G.C. Stem Cells in Wound Healing: The Future of Regenerative Medicine? A Mini-Review. Gerontology 2016, 62(2), 216. [Google Scholar] [CrossRef]
- Hoang, D.M.; et al., Stem Cell-Based Therapy For Human Diseases. Signal Transduct Target Ther, 2022. 7(1), 272. [CrossRef]
- Rajabzadeh, N.; Fathi, E.; Farahzadi, R. Stem Cell-Based Regenerative Medicine. Stem Cell Investig. 2019, 6, 19. [Google Scholar] [CrossRef]
- Harris, D.T.; Badowski, M.; Ahmad, N.; Gaballa, M.A. The potential of cord blood stem cells for use in regenerative medicine. Expert Opin Biol Ther. 2007, 7(9), 1311. [Google Scholar] [CrossRef]
- Devi, S.; Bongale, A.M.; Tefera, M.A.; Dixit, P.; Bhanap, P. Fresh Umbilical Cord Blood-A Source of Multipotent Stem Cells, Collection, Banking, Cryopreservation, and Ethical Concerns. Life (Basel), 2023, 13(9), 1794. [CrossRef]
- Sanchez-Petitto, G.; Rezvani, K.; Daher, M.; Rafei, H.; Kebriaei, P.; Shpall, E.J.; Olson, A. Umbilical Cord Blood Transplantation: Connecting Its Origin to Its Future. Stem Cells Transl. Med. 2023, 12(2), 55. [Google Scholar] [CrossRef]
- Barker, J.N.; Byam, C.E.; Kernan, N.A.; Lee, S.S.; Hawke, R.M.; Doshi, K.A.; Wells, D.S.; Heller, G.; Papadopoulos, E.B.; Scaradavou, A.; Young, J.W.; van den Brink, M.R. Availability of Cord Blood Extends Allogeneic Hematopoietic Stem Cell Transplant Access to Racial and Ethnic Minorities. Biol. Blood Marrow Transplant 2010, 16(11), 1541. [Google Scholar] [CrossRef]
- Gragert, L.; et al. HLA Match Likelihoods For Hematopoietic Stem-Cell Grafts in the U.S. Registry. N. Engl. J. Med. 2014, 371(4), 339. [Google Scholar] [CrossRef]
- Weiss, M.L.; Troyer, D.L. Stem Cells in the Umbilical Cord. Stem Cell Rev. 2006, 2(2), 155. [Google Scholar] [CrossRef]
- Kurtzberg, J.; Lyerly, A.D.; Sugarman, J. Untying the Gordian Knot: Policies, Practices, and Ethical Issues Related to Banking of Umbilical Cord Blood. J. Clin. Invest. 2005, 115(10), 2592. [Google Scholar] [CrossRef]
- Hoover-Plow, J.; Gong, Y. Challenges For Heart Disease Stem Cell Therapy. Vasc. Health Risk Manag. 2012, 8, 99. [Google Scholar] [CrossRef]
- Mohr, A.; Zwacka, R. The Future of Mesenchymal Stem Cell-Based Therapeutic Approaches For Cancer - From Cells to Ghosts. Cancer Lett. 2018, 414, 239. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Zhao, E.R.; Hableel, G.; Hu, T.; Kim, T.; Li, J.; Gonzalez-Pech, N.I.; Cheng, D.J.; Lemaster, J.E.; Xie, Y.; Grassian, V.H.; Sen, G.L.; Jokerst, J.V. Increasing the Efficacy of Stem Cell Therapy via Triple-Function Inorganic Nanoparticles. ACS Nano 2019, 13(6), 6605. [Google Scholar] [CrossRef] [PubMed]
- Nourian Dehkordi, A.; Mirahmadi Babaheydari, F.; Chehelgerdi, M.; Raeisi Dehkordi, S. Skin Tissue Engineering: Wound Healing Based on Stem-Cell-Based Therapeutic Strategies. Stem Cell Res. Ther. 2019, 10(1), 111. [Google Scholar] [CrossRef] [PubMed]
- Butler, K.L.; Goverman, J.; Ma, H.; Fischman, A.; Yu, Y.M.; Bilodeau, M.; Rad, A.M.; Bonab, A.A.; Tompkins, R.G.; Fagan, S.P. Stem Cells and Burns: Review and Therapeutic Implications. J. Burn Care Res. 2010, 31(6), 874. [Google Scholar] [CrossRef]
- Chu, G.Y.; Chen, Y.F.; Chen, H.Y.; Chan, M.H.; Gau, C.S.; Weng, S.M. Stem Cell Therapy on Skin: Mechanisms, Recent Advances and Drug Reviewing Issues. J. Food Drug Anal. 2018, 26(1), 14. [Google Scholar] [CrossRef] [PubMed]
- Ojeh, N.; Pastar, I.; Tomic-Canic, M.; Stojadinovic, O. Cells in Skin Regeneration, Wound Healing, and Their Clinical Applications. Int. J. Mol. Sci. 2015, 16(10), 25476. [Google Scholar] [CrossRef] [PubMed]
- Díaz-García, D.; Filipová, A.; Garza-Veloz, I.; Martinez-Fierro, M.L. A Beginner's Introduction to Skin Stem Cells and Wound Healing. Int. J. Mol. Sci. 2021, 22(20), 11030. [Google Scholar] [CrossRef] [PubMed]
- Gurtner, G.C.; Werner, S.; Barrandon, Y.; Longaker, M.T. Wound Repair and Regeneration. Nature 2008, 453(7193), 314. [Google Scholar] [CrossRef]
- Clevers, H. Wnt/Beta-Catenin Signaling in Development and Disease. Cell 2006, 127(3), 469. [Google Scholar] [CrossRef]
- Logan, C.Y.; Nusse, R. The Wnt Signaling Pathway in Development and Disease. Annu. Rev. Cell Dev. Biol. 2004, 20, 781. [Google Scholar] [CrossRef]
- Holland, J.D.; Klaus, A.; Garratt, A.N.; Birchmeier, W. Wnt Signaling in Stem and Cancer Stem Cells. Curr. Opin. Cell Biol. 2013, 25(2), 254. [Google Scholar] [CrossRef]
- Tottoli, E.M.; Dorati, R.; Genta, I.; Chiesa, E.; Pisani, S.; Conti, B. Skin Wound Healing Process and New Emerging Technologies for Skin Wound Care and Regeneration. Pharmaceutics 2020, 12(8), 735. [Google Scholar] [CrossRef]
- Khaled, M.M.; Ibrahium, A.M.; Abdelgalil, A.I.; El-Saied, M.A.; El-Bably, S.H. Regenerative Strategies in Treatment of Peripheral Nerve Injuries in Different Animal Models. Tissue Eng. Regen. Med. 2023, 20(6), 839. [Google Scholar] [CrossRef]
- Frausin, S.; Viventi, S.; Verga Falzacappa, L.; Quattromani, M.J.; Leanza, G.; Tommasini, A.; Valencic, E. Wharton's Jelly Derived Mesenchymal Stromal Cells: Biological Properties, Induction of Neuronal Phenotype and Current Applications in Neurodegeneration Research. Acta Histochem. 2015, 117(4-5), 329. [CrossRef]
- Karimi, H. Nerve Regeneration and Stem Cells. Biomedical. J. Sci. & Tech. Res. 2019, 18(3). [CrossRef]
- Pan, M.; Wang, X.; Chen, Y.; Cao, S.; Wen, J.; Wu, G.; Li, Y.; Li, L.; Qian, C.; Qin, Z.; Li, Z.; Tan, D.; Fan, Z.; Wu, W.; Guo, J. Tissue Engineering With Peripheral Blood-Derived Mesenchymal Stem Cells Promotes the Regeneration of Injured Peripheral Nerves. Exp. Neurol. 2017, 292, 92. [Google Scholar] [CrossRef]
- Zhang, R.C.; Du, W.Q.; Zhang, J.Y.; Yu, S.X.; Lu, F.Z.; Ding, H.M.; Cheng, Y.B.; Ren, C.; Geng, D.Q. Mesenchymal Stem Cell Treatment For Peripheral Nerve Injury: A Narrative Review. Neural Regen. Res. 2021, 16(11), 2170. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.; Zhang, Y.; Gu, X.; Huang, L.; Zhang, K.; Qian, T.; Gu, X. Application of Stem Cells in Peripheral Nerve Regeneration. Burns. Trauma 2020, 8, tkaa002. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.W.; Zhang, C.L. Neuronal Regeneration After Injury: A New Perspective on Gene Therapy. Front. Neurosci. 2023, 17, 1181816. [Google Scholar] [CrossRef] [PubMed]
- Anselmo, A.C.; Mitragotri, S. A Review of Clinical Translation of Inorganic Nanoparticles. AAPS J, 2015, 17(5), 1041. [CrossRef]
- Zheng, X.; Zhang, P.; Fu, Z.; Meng, S.; Dai, L.; Yang, H. Applications of Nanomaterials in Tissue Engineering. RSC Adv. 2021, 11(31), 19041. [Google Scholar] [CrossRef] [PubMed]
- Brokesh, A.M.; Gaharwar, A.K. Inorganic Biomaterials for Regenerative Medicine. ACS Appl. Mater. Interfaces 2020, 12(5), 5319. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Luan, Z.; Li, J. Inorganic Nanoparticles-Based Systems in Biomedical Applications of Stem Cells: Opportunities and Challenges. Int. J. Nanomed. 2023, 18, 143. [Google Scholar] [CrossRef]
- Gao, Y.; Wang, X.; Fan, C. Advances in Graphene-Based 2D Materials for Tendon, Nerve, Bone/Cartilage Regeneration and Biomedicine. iScience 2024, 27(7), 110214. [Google Scholar] [CrossRef]
- Arora, P.; Sindhu, A.; Dilbaghi, N.; Chaudhury, A.; Rajakumar, G.; Rahuman, A.A. Nano-Regenerative Medicine Towards Clinical Outcome of Stem Cell and Tissue Engineering in Humans. J. Cell Mol. Med. 2012, 16(9), 1991. [Google Scholar] [CrossRef]
- Kim, Y.H.; Vijayavenkataraman, S.; Cidonio, G. Biomaterials and Scaffolds for Tissue Engineering and Regenerative Medicine. BMC Methods 2024, 1, 2. [Google Scholar] [CrossRef]
- Chan, B.P.; Leong, K.W. Scaffolding in Tissue Engineering: General Approaches and Tissue-Specific Considerations. Eur. Spine J. 2008, 17, Suppl 4(Suppl 4), 467. [CrossRef]
- Krishani, M.; Shin, W.Y.; Suhaimi, H.; Sambudi, N.S. Development of Scaffolds from Bio-Based Natural Materials for Tissue Regeneration Applications: A Review. Gels 2023, 9(2), 100. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, M.J.; Billingsley, M.M.; Haley, R.M.; Wechsler, M.E.; Peppas, N.A.; Langer, R. Engineering Precision Nanoparticles for Drug Delivery. Nat. Rev. Drug Discov. 2021, 20(2), 101. [Google Scholar] [CrossRef] [PubMed]
- Raju, G.S.R.; Dariya, B.; Mungamuri, S.K.; Chalikonda, G.; Kang, S.M.; Khan, I.N.; Sushma, P.S.; Nagaraju, G.P.; Pavitra, E.; Han, Y.K. Nanomaterials Multifunctional Behavior For Enlightened Cancer Therapeutics. Semin. Cancer Biol. 2021, 69, 178. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.J.; Jiang, X.C.; Li, Y.S.; Gao, J.Q. Inorganic Nanoparticle-Integrated Mesenchymal Stem Cells: A Potential Biological Agent For Multifaceted Applications. MedComm (2020), 2023, 4(4), e313. [Google Scholar] [CrossRef]
- Blokhuis, T.J.; Arts, J.J. Bioactive and Osteoinductive Bone Graft Substitutes: Definitions, Facts and Myths. Injury 2011, 42 Suppl 2, S26. [Google Scholar] [CrossRef]
- Amini, A.R.; Laurencin, C.T.; Nukavarapu, S.P. Bone Tissue Engineering: Recent Advances and Challenges. Crit. Rev. Biomed. Eng. 2012, 40(5), 363. [Google Scholar] [CrossRef]
- Devin, J.E.; Attawia, M.A.; Laurencin, C.T. Three-Dimensional Degradable Porous Polymer-Ceramic Matrices For Use in Bone Repair. J. Biomater. Sci. Polym. Ed. 1996, 7(8), 661. [Google Scholar] [CrossRef]
- Hasan, A.; Morshed, M.; Memic, A.; Hassan, S.; Webster, T.J.; Marei, H.E. Nanoparticles in Tissue Engineering: Applications, Challenges and Prospects. Int. J. Nanomedicine. 2018, 13, 5637. [Google Scholar] [CrossRef]
- Lee, J.H.; Park, T.G.; Park, H.S.; Lee, D.S.; Lee, Y.K.; Yoon, S.C.; Nam, J.D. Thermal and Mechanical Characteristics of Poly(L-lactic acid) Nanocomposite Scaffold. Biomaterials. 2003, 24(16), 2773. [Google Scholar] [CrossRef]
- Park, S.; Rahaman, K.A.; Kim, Y.C.; Jeon, H.; Han, H.S. Fostering Tissue Engineering and Regenerative Medicine to Treat Musculoskeletal Disorders in Bone and Muscle. Bioact. Mater. 2024, 40, 345. [Google Scholar] [CrossRef]
- Zhang, Q.; Xiao, L.; Xiao, Y. Porous Nanomaterials Targeting Autophagy in Bone Regeneration. Pharmaceutics 2021, 13(10), 1572. [Google Scholar] [CrossRef] [PubMed]
- Friggeri, G.; et al. Multifunctional Scaffolds For Biomedical Applications: Crafting Versatile Solutions with Polycaprolactone Enriched by Graphene Oxide. APL Bioeng. 2024, 8(1), 016115. [Google Scholar] [CrossRef] [PubMed]
- Samadian, H.; Khastar, H.; Ehterami, A.; Salehi, M. Bioengineered 3D Nanocomposite Based on Gold Nanoparticles and Gelatin Nanofibers for Bone Regeneration: In Vitro and In Vivo Study. Sci. Rep. 2021, 11(1), 13877. [Google Scholar] [CrossRef]
- Samadian, H.; et al. Electrospun Cellulose Acetate/Gelatin Nanofibrous Wound Dressing Containing Berberine for Diabetic Foot Ulcer Healing: In Vitro and In Vivo Studies. Sci. Rep. 2020, 10(1), 8312. [Google Scholar] [CrossRef] [PubMed]
- Gandhimathi, C.; Quek, Y.J.; Ezhilarasu, H.; Ramakrishna, S.; Bay, B.H.; Srinivasan, D.K. Osteogenic Differentiation of Mesenchymal Stem Cells with Silica-Coated Gold Nanoparticles for Bone Tissue Engineering. Int. J. Mol. Sci. 2019, 20(20), 5135. [Google Scholar] [CrossRef]
- Wedel-Grzenda, A.; Fraczek-Szczypta, A.; Terrones, M.; Elias, A.L. Lekka, M.; Menaszek, E.; Blazewicz, S. Polysulphone composite membranes modified with two types of carbon additives as a potential material for bone tissue regeneration. Bull. Mater. Sci. 2017, 40(1), 201. [Google Scholar] [CrossRef]
- Sithole, M.N.; Kumar, P.; Du Toit, L.C.; Erlwanger, K.H.; Ubanako, P.N.; Choonara, Y.E. A 3D-Printed Biomaterial Scaffold Reinforced with Inorganic Fillers for Bone Tissue Engineering: In Vitro Assessment and In Vivo Animal Studies. Int. J. Mol. Sci. 2023, 24(8), 7611. [Google Scholar] [CrossRef]
- Yang, L.; Rathnam, C.; Hou, Y.; Patel, M.; Cai, L.; Lee, K.-B. Rapid and Controllable Multilayer Cell Sheet Assembly via Biodegradable Nanochannel Membranes. Adv. Funct. Mater. 2024, 2403367. [Google Scholar] [CrossRef]
- Yang, L.; Chueng, S.D.; Li, Y.; Patel, M.; Rathnam, C.; Dey, G.; Wang, L.; Cai, L.; Lee, K.B. A Biodegradable Hybrid Inorganic Nanoscaffold for Advanced Stem Cell Therapy. Nat Commun. 2018, 9(1), 3147. [Google Scholar] [CrossRef]
- Baydar, S.Y.; Ay, H.F.; Cakir, R. Frontiers of Stem Cell Engineering For Nanotechnology-Mediated Drug Delivery Systems. ADMET DMPK, 2024, 12(2), 225. [CrossRef]
- Yang, Y.; Leong, K.W. Nanoscale Surfacing For Regenerative Medicine. WIREs Nanomed Nanobiotechnol. 2010, 2, 478. [Google Scholar] [CrossRef]
- Brovkina, O.; Dashinimaev, E. Advances and Complications of Regenerative Medicine in Diabetes Therapy. PeerJ, 2020, 8, e9746. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Liu, Y.; Wu, N. Application Progress of Nanotechnology in Regenerative Medicine of Diabetes Mellitus. Diabetes Res. Clin. Pract. 2022, 190, 109966. [Google Scholar] [CrossRef] [PubMed]
- Andreadi, A.; Lodeserto, P.; Todaro, F.; Meloni, M.; Romano, M.; Minasi, A.; Bellia, A.; Lauro, D. Nanomedicine in the Treatment of Diabetes. Int. J. Mol. Sci. 2024, 25, 7028. [Google Scholar] [CrossRef] [PubMed]
- Siwakoti, P.; Rennie, C.; Huang, Y.; Li, J.J.; Tuch, B.E.; McClements, L.; Xu, X. Challenges with Cell-based Therapies for Type 1 Diabetes Mellitus. Stem Cell. Rev. Rep. 2023, 19(3), 601. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Ji, K.; Wang, Y.; Gu, Z.; Wang, J. Materials and Carriers Development for Glucose-Responsive Insulin. Acc. Mater. Res. 2022, 3(9), 960. [Google Scholar] [CrossRef]
- Bakhru, S.H.; Furtado, S.; Morello, A.P.; Mathiowitz, E. Oral Delivery of Proteins by Biodegradable Nanoparticles. Adv. Drug Deliv. Rev. 2013, 65, 811. [Google Scholar] [CrossRef]
- Rabanel, J.M.; Aoun, V.; Elkin, I.; Mokhtar, M.; Hildgen, P. Drug-Loaded Nanocarriers- Passive Targeting and Crossing of Biological Barriers. Curr. Med. Chem. 2012, 19, 3070. [Google Scholar] [CrossRef]
- Veiseh, O.; Tang, B.C.; Whitehead, K.A.; Anderson, D.G.; Langer, R. Managing Diabetes with Nanomedicine: Challenges and Opportunities. Nat. Rev. Drug Discov. 2015, 14(1), 45. [Google Scholar] [CrossRef]
- Sharma, R.; Borah, S.J.; Bhawna, Kumar, S.; Gupta, A.; Kumari, V.; Kumar, R.; Dubeyg, K.K.; Kumar, V. Emerging Trends in Nano-Based Antidiabetic Therapeutics: A Path to Effective Diabetes Management. Mater. Adv. 2023, 4(15), 3091. [CrossRef]
- Liu, Y.; Zeng, S.; Ji, W.; Yao, H.; Lin, L.; Cui, H.; Santos, H.A.; Pan, G. Emerging Theranostic Nanomaterials in Diabetes and Its Complications. Adv. Sci. (Weinh). 2022, 9(3), e2102466. [Google Scholar] [CrossRef]
- Sonomoto, K.; Yamaoka, K.; Kaneko, H.; Yamagata, K.; Sakata, K.; Zhang, X.; Kondo, M.; Zenke, Y.; Sabanai, K.; Nakayamada, S.; Sakai, A.; Tanaka, Y. Spontaneous Differentiation of Human Mesenchymal Stem Cells on Poly-Lactic-Co-Glycolic Acid Nano-Fiber Scaffold. PLoS One. 2016, 11(4), e0153231. [Google Scholar] [CrossRef]
- Umer, A.; Ghouri, M.D.; Muyizere, T.; Aqib, R.M.; Muhaymin, A.; Cai, R.; Chen, C. Engineered Nano-Bio Interfaces for Stem Cell Therapy. Precis. Chem. 2023, 1(6), 341. [Google Scholar] [CrossRef] [PubMed]
- Teo, B.K.; Wong, S.T.; Lim, C.K.; Kung, T.Y.; Yap, C.H.; Ramagopal, Y.; Romer, L.H.; Yim, E.K. Nanotopography Modulates Mechanotransduction of Stem Cells and Induces Differentiation Through Focal Adhesion Kinase. ACS Nano 2013, 7(6), 4785. [Google Scholar] [CrossRef] [PubMed]
- Ludin, A.; Gur-Cohen, S.; Golan, K.; Kaufmann, K.B.; Itkin, T.; Medaglia, C.; Lu, X.J.; Ledergor, G.; Kollet, O.; Lapidot, T. Reactive Oxygen Species Regulate Hematopoietic Stem Cell Self-Renewal, Migration and Development, as well as their Bone Marrow Microenvironment. Antioxid. Redox Signal. 2014, 21(11), 1605. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Liu, D.; Zhang, C.; Sun, J.; Feng, W.; Liang, X.J.; Wang, S.; Zhang, J. Defect-Related Luminescent Hydroxyapatite-Enhanced Osteogenic Differentiation of Bone Mesenchymal Stem Cells Via an ATP-Induced cAMP/PKA Pathway. ACS Appl. Mater. Interfaces. 2016, 8(18), 11262. [Google Scholar] [CrossRef]
- Przekora, A. Current Trends in Fabrication of Biomaterials for Bone and Cartilage Regeneration: Materials Modifications and Biophysical Stimulations. Int. J. Mol. Sci. 2019, 20(2), 435. [Google Scholar] [CrossRef]
- Wu, Y.N.; Law, J.B.; He, A.Y.; Low, H.Y.; Hui, J.H.; Lim, C.T.; Yang, Z.; Lee, E.H. Substrate Topography Determines the Fate of Chondrogenesis from Human Mesenchymal Stem Cells Resulting in Specific Cartilage Phenotype Formation. Nanomedicine 2014, 10(7), 1507. [Google Scholar] [CrossRef]
- Wu, Y.N.; Yang, Z.; Hui, J.H.; Ouyang, H.W.; Lee, E.H. Cartilaginous ECM Component-Modification of the Micro-Bead Culture System For Chondrogenic Differentiation of Mesenchymal Stem Cells. Biomaterials 2007, 28(28), 4056. [Google Scholar] [CrossRef]
- Varghese, S.; Hwang, N.S.; Canver, A.C.; Theprungsirikul, P.; Lin, D.W.; Elisseeff, J. Chondroitin Sulfate Based Niches For Chondrogenic Differentiation of Mesenchymal Stem Cells. Matrix Biol. 2008, 27(1), 12. [Google Scholar] [CrossRef]
- Popov, A.M.; Lozovik, Y.E.; Fiorito, S.; Yahia, L. Biocompatibility and Applications of Carbon Nanotubes in Medical Nanorobots. Int. J. Nanomed. 2007, 2(3), 361. [Google Scholar]
- Chou, S.W.; Shau, Y.H.; Wu, P.C.; Yang, Y.S.; Shieh, D.B.; Chen, C.C. In Vitro and in Vivo Studies of FePt Nanoparticles for Dual Modal CT/MRI Molecular Imaging. J. Am. Chem. Soc. 2010, 132(38), 13270. [Google Scholar] [CrossRef]
- Wang, J.; Huang, C.; Wang, Y.; Chen, Y.; Ding, Z.; Yang, C.; Chen, L. Exploration of the Single-Walled Carbon Nanotubes’ Influence for Cartilage Repair, Colloid. Surf. A: Physicochemi. Engr. Aspects. 2020, 606, 125520. [Google Scholar] [CrossRef]
- Szymański, T.; Semba, J.A.; Mieloch, A.A.; Cywoniuk, P.; Kempa, M.; Rybka, J.D. Hyaluronic Acid and Multiwalled Carbon Nanotubes as Bioink Additives for Cartilage Tissue Engineering. Sci. Rep. 2023, 13(1), 646. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Li, C.J.; Wan, Y.; Smith, P.; Shang, G.; Cui, Q. Antioxidative Fullerol Promotes Osteogenesis of Human Adipose-Derived Stem Cells. Int. J. Nanomed. 2014, 9, 4023. [Google Scholar] [CrossRef]
- Elídóttir, K.L.; Scott, L.; Lewis, R.; Jurewicz, I. Biomimetic Approach to Articular Cartilage Tissue Engineering Using Carbon Nanotube-Coated and Textured Polydimethylsiloxane Scaffolds. Ann. N. Y. Acad. Sci. 2022, 1513(1), 48. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.Q.; Yan, K.; Shi, C.; Xu, X.; Wang, T.; Li, R.; Dong, W.; Zheng, J. Neurogenic Differentiation of Adipose Derived Stem Cells on Graphene-Based Mat. Mater. Sci. Eng. C Mater. Biol. Appl. 2018, 90, 685. [Google Scholar] [CrossRef] [PubMed]
- Rostami, F.; Tamjid, E.; Behmanesh, M. Drug-Eluting PCL/Graphene Oxide Nanocomposite Scaffolds For Enhanced Osteogenic Differentiation of Mesenchymal Stem Cells. Mater. Sci. Eng. C Mater. Biol. Appl. 2020, 115, 111102. [Google Scholar] [CrossRef]
- Wei, S., et al., Carbon Nanomaterials in the Treatment of Infectious Bone Defects and Wound Scars after Wushu Fractures. Journal of Chemistry, 2020. 2020: p. 1-9.
- Shen, Y.; Wu, L.; Qin, D.; Xia, Y.; Zhou, Z.; Zhang, X.; Wu, X. Carbon Black Suppresses the Osteogenesis of Mesenchymal Stem Cells: The Role of Mitochondria. Part Fibre Toxicol. 2018, 15(1), 16. [Google Scholar] [CrossRef]
- De Luca, S.; Verdoliva, V.; Kargozar, S.; Baino, F. Bioactive Glass-Ceramic Scaffolds Coated with Hyaluronic Acid-Fatty Acid Conjugates: A Feasibility Study. J. Funct. Biomater. 2023, 14(1), 26. [Google Scholar] [CrossRef]
- Cannio, M.; Bellucci, D.; Roether, J.A.; Boccaccini, D.N.; Cannillo, V. Bioactive Glass Applications: A Literature Review of Human Clinical Trials. Materials (Basel). 2021, 14(18), 5440. [Google Scholar] [CrossRef]
- Sergi, R.; Bellucci, D.; Cannillo, V. A Review of Bioactive Glass/Natural Polymer Composites: State of the Art. Materials (Basel). 2020, 13(23), 5560. [Google Scholar] [CrossRef]
- El-Rashidy, A.A.; Roether, J.A.; Harhaus, L.; Kneser, U.; Boccaccini, A.R. Regenerating Bone with Bioactive Glass Scaffolds: A Review of in vivo Studies in Bone Defect Models. Acta Biomater. 2017, 62, 1. [Google Scholar] [CrossRef] [PubMed]
- Fiume, E.; Barberi, J.; Verné, E.; Baino, F. Bioactive Glasses: From Parent 45S5 Composition to Scaffold-Assisted Tissue-Healing Therapies. J. Funct. Biomater. 2018, 9(1), 24. [Google Scholar] [CrossRef] [PubMed]
- Hench, L.L. The Story of Bioglass. J. Mater. Sci. Mater. Med. 2006, 17(11), 967. [Google Scholar] [CrossRef] [PubMed]
- Gerhardt, L.C.; Boccaccini, A.R. Bioactive Glass and Glass-Ceramic Scaffolds for Bone Tissue Engineering. Materials (Basel) 2010, 3(7), 3867. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.R. Bioactive Ceramics and Glasses. In: Boccaccini A.R., G.J.E., editors. Tissue Engineering Using Ceramics and Polymers. 1st ed. Volume 1. Woodhead Publishing Limited CRC Press; Cambridge, UK: 2007. pp. 52–71.
- Xynos, I.D.; Hukkanen, M.V.; Batten, J.J.; Buttery, L.D.; Hench, L.L.; Polak, J.M. Bioglass 45S5 Stimulates Osteoblast Turnover and Enhances Bone Formation In vitro: Implications and Applications for Bone Tissue Engineering. Calcif. Tissue Int. 2000, 67(4), 321. [Google Scholar] [CrossRef]
- Dreanca, A., et al., The Evaluation of the Osteopromoting Capabilities of Composites Based on Biopolymers and Gold/Silver Nanoparticles Doped Bioactive Glasses on an Experimental Rat Bone Defect. Biomed Mater. 2023, 18(5). [CrossRef]
- Niu, W.; Chen, M.; Guo, Y.; Wang, M.; Luo, M.; Cheng, W.; Wang, Y.; Lei, B. A Multifunctional Bioactive Glass-Ceramic Nanodrug for Post-Surgical Infection/Cancer Therapy-Tissue Regeneration. ACS Nano 2021, 15(9), 14323. [Google Scholar] [CrossRef]
- Khatami, N.; Khoshfetrat, A.B.; Khaksar, M.; Zamani, A.R.N.; Rahbarghazi, R. Collagen-Alginate-Nano-Silica Microspheres Improved the Osteogenic Potential of Human Osteoblast-Like MG-63 Cells. J. Cell Biochem. 2019, 120(9), 15069. [Google Scholar] [CrossRef]
- Mostafa, A.A.; El-Sayed, M.M.H.; Emam, A.N.; Abd-Rabou, A.A.; Dawood, R.M.; Oudadesse, H. Bioactive Glass Doped with Noble Metal Nanoparticles for Bone Regeneration: in vitro Kinetics and Proliferative Impact on Human Bone Cell Line. RSC Adv. 2021, 11(41), 25628. [Google Scholar] [CrossRef]
- Zengin, A.; Castro, J.P.O.; Habibovic, P.; van Rijt, S.H. Injectable, Self-Healing Mesoporous Silica Nanocomposite Hydrogels with Improved Mechanical Properties. Nanoscale 2021, 13(2), 1144. [Google Scholar] [CrossRef]
- Hou, X.; Zhang, L.; Zhou, Z.; Luo, X.; Wang, T.; Zhao, X.; Lu, B.; Chen, F.; Zheng, L. Calcium Phosphate-Based Biomaterials for Bone Repair. J. Funct. Biomater. 2022, 13(4), 187. [Google Scholar] [CrossRef]
- Xiao, D.; Zhang, J.; Zhang, C.; Barbieri, D.; Yuan, H.; Moroni, L.; Feng, G. The Role of Calcium Phosphate Surface Structure in Osteogenesis and the Mechanisms Involved. Acta Biomater. 2020, 106, 22. [Google Scholar] [CrossRef] [PubMed]
- Zhi, H.; Qingling, F.; Bo, Y.; Songjian, L. Biomimetic Properties of an Injectable Chitosan/Nano-Hydroxyapatite/Collagen Composite. Mater. Sci. Eng.: C 2011, 31(3), 683. [CrossRef]
- Shibuya, S.; Ozawa, Y.; Watanabe, K.; Izuo, N.; Toda, T.; Yokote, K.; Shimizu, T. Palladium and Platinum Nanoparticles Attenuate Aging-Like Skin Atrophy via Antioxidant Activity in Mice. PLoS One 2014, 9(10), e109288. [Google Scholar] [CrossRef] [PubMed]
- Leal, F.; Nirwan, V.; Gonçalves, A.M.; Panitschewski, N.; Filová, E.; Fahmi, A.; Costa, P.F. (2023). Bio-Inspired Nanoporous Scaffold: Electrospun Hybrid Fibers Based on Self-Assembled Block Copolymer Mineralized with Inorganic Nanoparticles for Bone Tissue Engineering. Int. J. Polym. Mater. Polym. Biomater. 2023, 73(12), 1054. [Google Scholar] [CrossRef]
- Kumar, B.Y.S.; Isloor, A.M.; Kumar, G.C.M.; Inamuddin Asiri, A.M. Nanohydroxyapatite Reinforced Chitosan Composite Hydrogel with Tunable Mechanical and Biological Properties for Cartilage Regeneration. Sci Rep. 2019, 9(1), 15957. [Google Scholar] [CrossRef]
- Kumai, T.; Yui, N.; Yatabe, K.; Sasaki, C.; Fujii, R.; Takenaga, M.; Fujiya, H.; Niki, H.; Yudoh, K. A Novel, Self-Assembled Artificial Cartilage-Hydroxyapatite Conjugate for Combined Articular Cartilage and Subchondral Bone Repair: Histopathological Analysis of Cartilage Tissue Engineering in Rat Knee Joints. Int. J. Nanomedicine 2019, 14, 1283. [Google Scholar] [CrossRef]
- Boller, L.A.; Shiels, S.M.; Florian, D.C.; Peck, S.H.; Schoenecker, J.G.; Duvall, C.; Wenke, J.C.; Guelcher, S.A. Effects of Nanocrystalline Hydroxyapatite Concentration and Skeletal Site on Bone and Cartilage Formation in Rats. Acta Biomater. 2021, 130, 485. [Google Scholar] [CrossRef]
- Huang, J.; et al. 3D Printed Gelatin/Hydroxyapatite Scaffolds for Stem Cell Chondrogenic Differentiation and Articular Cartilage Repair. Biomater Sci. 2021, 9(7), 2620. [Google Scholar] [CrossRef]
- Gaweł, J.; Milan, J.; Żebrowski, J.; Płoch, D.; Stefaniuk, I.; Kus-Liśkiewicz, M. Biomaterial Composed of Chitosan, Riboflavin, and Hydroxyapatite for Bone Tissue Regeneration. Sci. Rep. 2023, 13(1), 17004. [Google Scholar] [CrossRef]
- Becerra, J.; Rodriguez, M.; Leal, D.; Noris-Suarez, K.; Gonzalez, G. Chitosan-Collagen-Hydroxyapatite Membranes for Tissue Engineering. J. Mater. Sci. Mater. Med. 2022, 33(2), 18. [Google Scholar] [CrossRef]
- Ma, S.; Wei, Y.; Sun, R.; Xu, H.; Liu, X.; Wang, Y.; Liang, Z.; Hu, Y.; Lian, X.; Ma, X.; Huang, D. Calcium Phosphate Bone Cements Incorporated with Black Phosphorus Nanosheets Enhanced Osteogenesis. ACS Biomater. Sci. Eng. 2023, 9(1), 292. [Google Scholar] [CrossRef]
- Witte, F.; Kaese, V.; Haferkamp, H.; Switzer, E.; Meyer-Lindenberg, A.; Wirth, C.J.; Windhagen, H. In vivo Corrosion of Four Magnesium Alloys and the Associated Bone Response. Biomaterials 2005, 26(17), 3557. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Fu, X.; Pan, H.; Wan, P.; Wang, L.; Tan, L.; Wang, K.; Zhao, Y.; Yang, K.; Chu, P.K. Biodegradable Mg-Cu Alloys with Enhanced Osteogenesis, Angiogenesis, and Long-Lasting Antibacterial Effects. Sci. Rep. 2016, 6, 27374. [Google Scholar] [CrossRef] [PubMed]
- Li, R.W.; Kirkland, N.T.; Truong, J.; Wang, J.; Smith, P.N.; Birbilis, N.; Nisbet, D.R. The Influence of Biodegradable Magnesium Alloys on the Osteogenic Differentiation of Human Mesenchymal Stem Cells. J. Biomed. Mater. Res. A. 2014, 102(12), 4346. [Google Scholar] [CrossRef] [PubMed]
- Fischerauer, S.F.; Kraus, T.; Wu, X.; Tangl, S.; Sorantin, E.; Hänzi, A.C.; Löffler, J.F.; Uggowitzer, P.J.; Weinberg, A.M. In vivo Degradation Performance of Micro-Arc-Oxidized Magnesium Implants: A Micro-CT Study in Rats. Acta Biomater. 2013, 9(2), 5411. [Google Scholar] [CrossRef]
- Du, L.; Wu, J.; Han, Y.; Wu, C. Immunomodulatory Multicellular Scaffolds For Tendon-to-Bone Regeneration. Sci. Adv. 2024, 10(10), eadk6610. [Google Scholar] [CrossRef]
- Oliveira-Filho, G.B.; Atoche-Medrano, J.J.; Aragón, F.F.H.; Mantilla Ochoa, J.C.; Pacheco-Salazar, D.G.; da Silva, S.W.; Coaquira, J.A.H. Core-Shell Au/Fe3O4 Nanocomposite Synthesized by Thermal Decomposition Method: Structural, Optical, and Magnetic Properties . Appl. Surf. Sci. 2021, 563, 150290. [Google Scholar] [CrossRef]
- Lin, R.H.; et al. Favorable Biological Performance Regarding the Interaction between Gold Nanoparticles and Mesenchymal Stem Cells. Int. J. Mol. Sci. 2022, 24(1), 5. [Google Scholar] [CrossRef]
- Hu, X.; Zhang, Y.; Ding, T.; Liu, J.; Zhao, H. Multifunctional Gold Nanoparticles: A Novel Nanomaterial for Various Medical Applications and Biological Activities. Front. Bioeng. Biotechnol. 2020, 8, 990. [Google Scholar] [CrossRef]
- Gupta, R.; Rai, B. Effect of Size and Surface Charge of Gold Nanoparticles on their Skin Permeability: A Molecular Dynamics Study. Sci. Rep. 2017, 7, 45292. [Google Scholar] [CrossRef]
- Suh, K.S.; Lee, Y.S.; Seo, S.H.; Kim, Y.S.; Choi, E.M. Gold Nanoparticles Attenuates Antimycin A-Induced Mitochondrial Dysfunction in MC3T3-E1 Osteoblastic Cells. Biol. Trace Elem. Res. 2013, 153(1-3), 428. [CrossRef]
- Grant, S.A.; Zhu, J.; Gootee, J.; Snider, C.L.; Bellrichard, M.; Grant, D.A. Gold Nanoparticle-Collagen Gels for Soft Tissue Augmentation. Tissue Eng Part A. 2018, 24(13-14), 1091. [CrossRef]
- Nunan, R.; Harding, K.G.; Martin, P. Clinical Challenges of Chronic Wounds: Searching for an Optimal Animal Model to Recapitulate their Complexity. Dis Model Mech. 2014, 7(11), 1205. [Google Scholar] [CrossRef]
- Mendes, C.; et al. Microcurrent and Gold Nanoparticles Combined with Hyaluronic Acid Accelerates Wound Healing. Antioxidants (Basel), 2022; 11, 11, 2257. [Google Scholar] [CrossRef]
- Poomrattanangoon, S.; Pissuwan, D. Gold Nanoparticles Coated with Collagen-I and Their Wound Healing Activity in Human Skin Fibroblast Cells. Heliyon 2024, 10(13), e33302. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Yu, J.M.; Gan, Y.C.; Qiu, X.Z.; Gao, Z.C.; Wang, H.; Chen, S.X.; Xiong, Y.; Liu, G.H.; Lin, S.E.; McCarthy, A.; John, J.V.; Wei, D.X.; Hou, H.H. Biomimetic Natural Biomaterials For Tissue Engineering and Regenerative Medicine: New Biosynthesis Methods, Recent Advances, and Emerging Applications. Mil. Med. Res. 2023, 10(1), 16. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; et al. Prospects and Challenges For the Application of Tissue Engineering Technologies in the Treatment of Bone Infections. Bone Res. 2024, 12(1), 28. [Google Scholar] [CrossRef] [PubMed]
- Senra, M.R.; Marques, M.F.V.; Monteiro, S.N. Poly (Ether-Ether-Ketone) For Biomedical Applications: From Enhancing Bioactivity to Reinforced-Bioactive Composites-An Overview. Polymers (Basel), 2023, 15(2), 373. [CrossRef]
- Cao, D.; Ding, J. Recent Advances in Regenerative Biomaterials. Regen. Biomater. 2022, 9, rbac098. [Google Scholar] [CrossRef]
- Sun, Y.; Liu, X.; Tan, J.; Lv. D.; Song, W.; Su, R.; Li, L.; Liu, X.; Ouyang, L.; Liao, Y. Strontium Ranelate Incorporated 3D Porous Sulfonated PEEK Simulating MC3T3-E1 Cell Differentiation. Regen. Biomater. 2020, 8(1), rbaa043. [CrossRef]
- Vasconcelos, D.P.; Águas, A.P.; Barbosa, M.A.; Pelegrín, P.; Barbosa, J.N. The Inflammasome in Host Response to Biomaterials: Bridging Inflammation and Tissue Regeneration. Acta Biomater. 2019, 83, 1. [Google Scholar] [CrossRef]
- Lele, M.; Kapur, S.; Hargett, S.; Sureshbabu, N.M.; Gaharwar, A.K. Global Trends in Clinical Trials Involving Engineered Biomaterials. Sci. Adv. 2024, 10(29), eabq0997. [Google Scholar] [CrossRef]
- Elson, E.L.; Genin, G.M. Tissue Constructs: Platforms for Basic Research and Drug Discovery. Interface Focus 2016, 6(1), 20150095. [Google Scholar] [CrossRef]
- Hench, L.L.; Thompson, I. Twenty-First Century Challenges for Biomaterials. J. R. Soc. Interface 2010, 7 Suppl 4(Suppl 4), S379. [CrossRef]
- Sharma, P.; Kumar, P.; Sharma, R.; Bhatt, V.D.; Dhot, P.S. Tissue Engineering; Current Status & Futuristic Scope. J. Med. Life 2019, 12(3), 225. [Google Scholar] [CrossRef]
- Chandra, P.K.; Soker, S.; Atala, A. Chapter 1—Tissue Engineering: Current Status and Future Perspectives. In: Lanza, R., Langer, R., Vacanti, J.P., and Atala, A., eds. Principles of Tissue Engineering (Fifth Edition). London, UK: Academic Press, 2020, pp. 1–35.
- Ashammakhi, N.; GhavamiNejad, A.; Tutar, R.; Fricker, A.; Roy, I.; Chatzistavrou, X.; Hoque Apu, E.; Nguyen, K.L.; Ahsan, T.; Pountos, I.; Caterson, E.J. Highlights on Advancing Frontiers in Tissue Engineering. Tissue Eng. Part B Rev. 2022, 28(3), 633. [Google Scholar] [CrossRef]
- Badylak, S.F.; Nerem, R.M. Progress in Tissue Engineering and Regenerative Medicine. Proc. Natl. Acad. Sci. U.S.A. 2010, 107(8), 3285. [Google Scholar] [CrossRef]
Figure 1.
An integrative approach that combines bioactive materials, biomolecules & external stimulation, and cell therapy in musculoskeletal disorders. Reproduced from Ref. [67] with permission of Elsevier under a Creative Commons license, https://creativecommons.org/licenses/by-nc-nd/4.0/.
Figure 1.
An integrative approach that combines bioactive materials, biomolecules & external stimulation, and cell therapy in musculoskeletal disorders. Reproduced from Ref. [67] with permission of Elsevier under a Creative Commons license, https://creativecommons.org/licenses/by-nc-nd/4.0/.
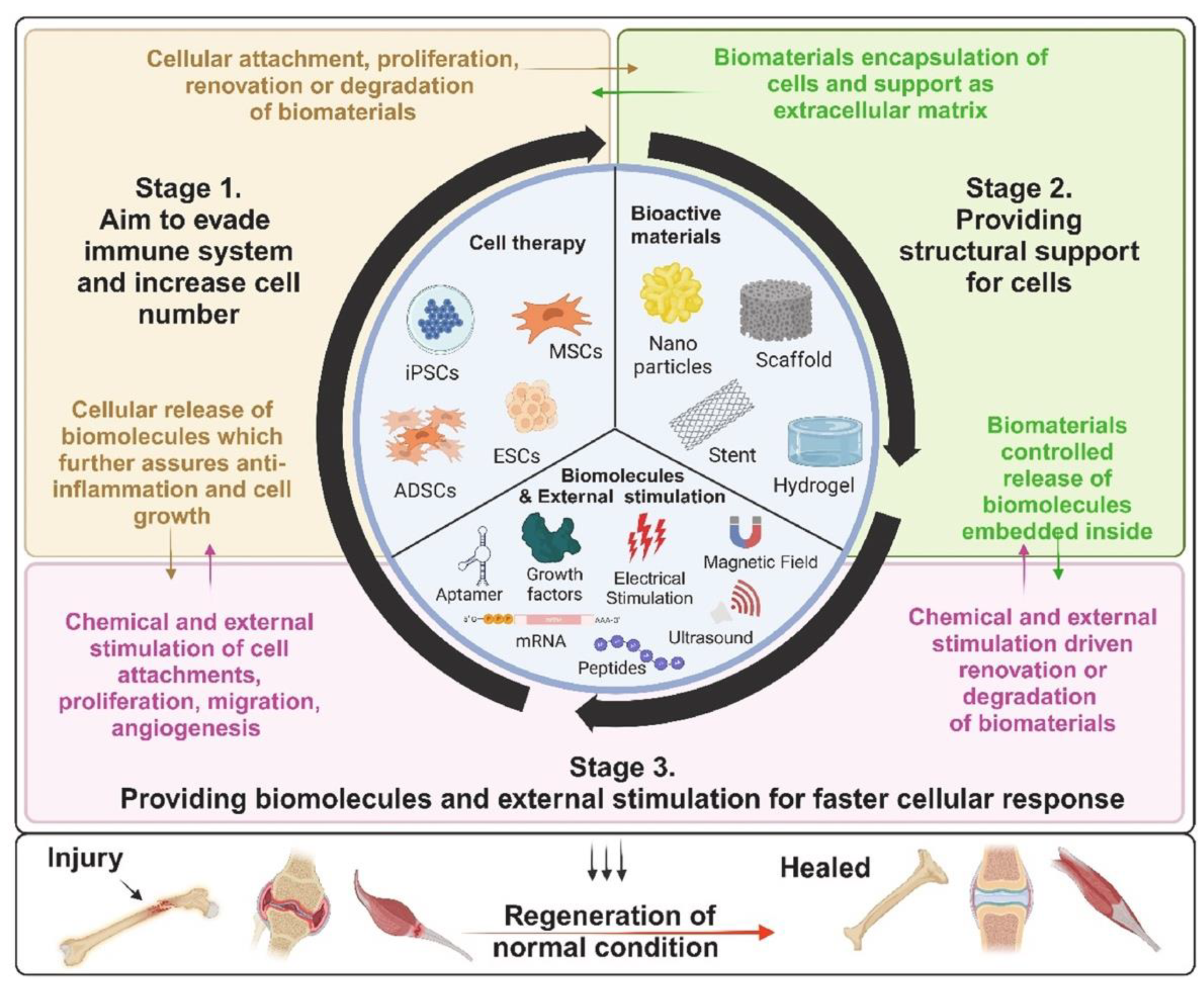
Figure 2.
(A) The viability of different cell lines grown on scaffolds or plastic wells evaluated using a luminescence assay. (B) Toxicity of DMEM exposed to scaffolds for 7 days and used to treat VERO cells seeded on 96 wells. Toxicity on VERO cells were evaluated after 6 or 24 h of treatment. (C) Fluorescence imaging of VERO cells surrounding grids of PCL-GO. Cells have been labeled with calcein (green) to evaluate viable cells and propidium iodide (red) to evaluate dead cells. The brightfield image of the same sample is shown in (D). (E) Evaluation of VERO cell viability on scaffolds washed with PBS or PBS+ethanol. (F) Cell viability on the scaffold after washing with DMEM (indicated with asterisks) or without DMEM washings. (G) and (H) Representative fluorescence images of cells surrounding grids (dashed lines) after DMEM washings, no red dead cells were visible. The scale bar was 100 m. The figure and caption are reproduced from Ref. [69]. Copyright © 2024,G. Friggeri, I. Moretti, F. Amato, A. G. Marrani, F. Sciandra, S. G. Colombarolli, A. Vitali, S. Viscuso,A. Augello, L. Cui, G. Perini, M. De Spirito, M. Papi, V. Palmieri. This article is distributed under aCreative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/).
Figure 2.
(A) The viability of different cell lines grown on scaffolds or plastic wells evaluated using a luminescence assay. (B) Toxicity of DMEM exposed to scaffolds for 7 days and used to treat VERO cells seeded on 96 wells. Toxicity on VERO cells were evaluated after 6 or 24 h of treatment. (C) Fluorescence imaging of VERO cells surrounding grids of PCL-GO. Cells have been labeled with calcein (green) to evaluate viable cells and propidium iodide (red) to evaluate dead cells. The brightfield image of the same sample is shown in (D). (E) Evaluation of VERO cell viability on scaffolds washed with PBS or PBS+ethanol. (F) Cell viability on the scaffold after washing with DMEM (indicated with asterisks) or without DMEM washings. (G) and (H) Representative fluorescence images of cells surrounding grids (dashed lines) after DMEM washings, no red dead cells were visible. The scale bar was 100 m. The figure and caption are reproduced from Ref. [69]. Copyright © 2024,G. Friggeri, I. Moretti, F. Amato, A. G. Marrani, F. Sciandra, S. G. Colombarolli, A. Vitali, S. Viscuso,A. Augello, L. Cui, G. Perini, M. De Spirito, M. Papi, V. Palmieri. This article is distributed under aCreative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/).
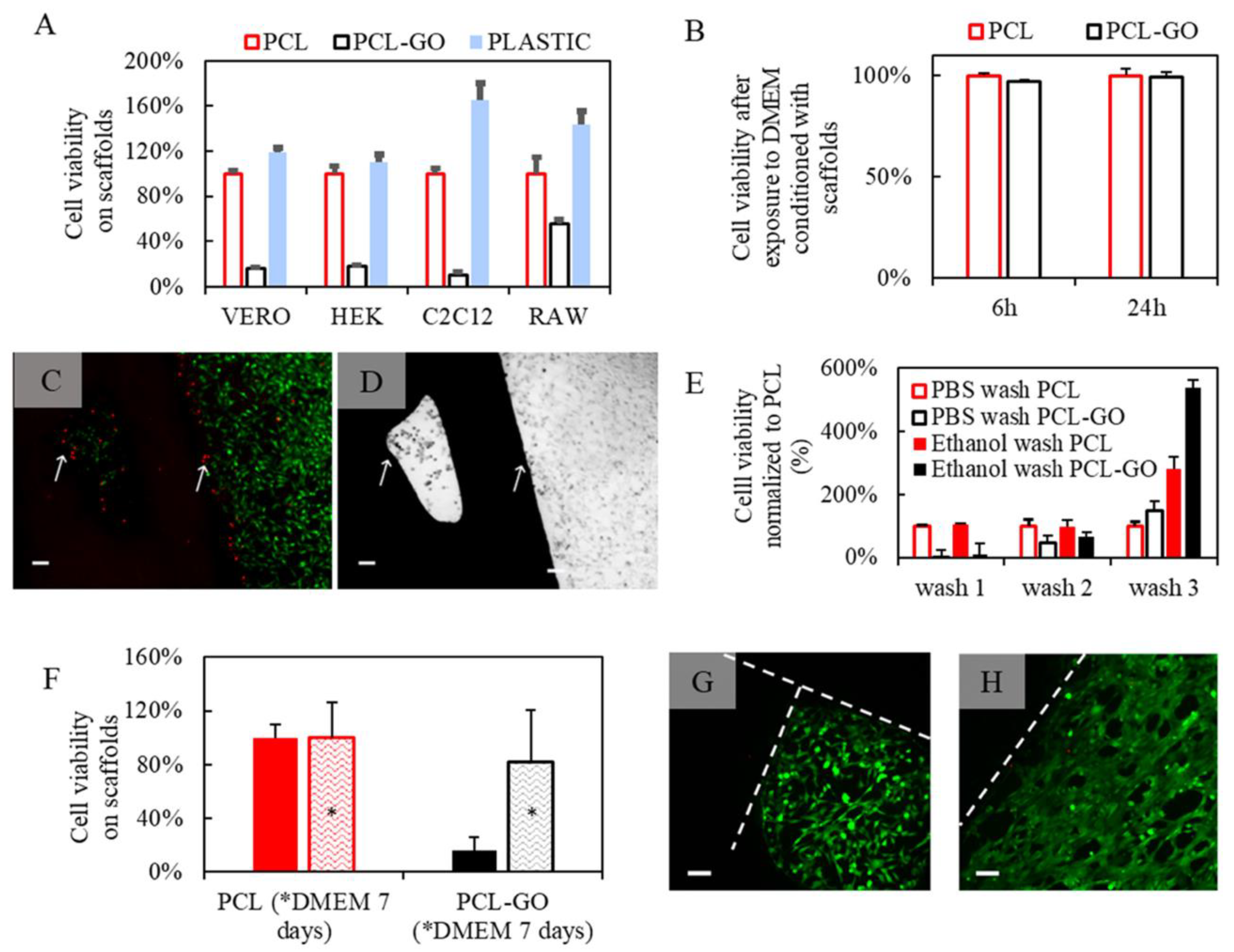
Figure 3.
MG-63 cell proliferation on the fabricated scaffolds was measured using an MTT assay at 24 and 72 h after cell seeding. Control: Tissue Culture Plate (TCP). Data represented as mean ± SD, n = 3. *p < 0.05 (obtained by one-way ANOVA). The Figure is reproduced from Ref. [71]. This article is licensed under a Creative Commons Attribution 4.0 International License, http://creativecommons.org/licenses/by/4.0/.
Figure 3.
MG-63 cell proliferation on the fabricated scaffolds was measured using an MTT assay at 24 and 72 h after cell seeding. Control: Tissue Culture Plate (TCP). Data represented as mean ± SD, n = 3. *p < 0.05 (obtained by one-way ANOVA). The Figure is reproduced from Ref. [71]. This article is licensed under a Creative Commons Attribution 4.0 International License, http://creativecommons.org/licenses/by/4.0/.
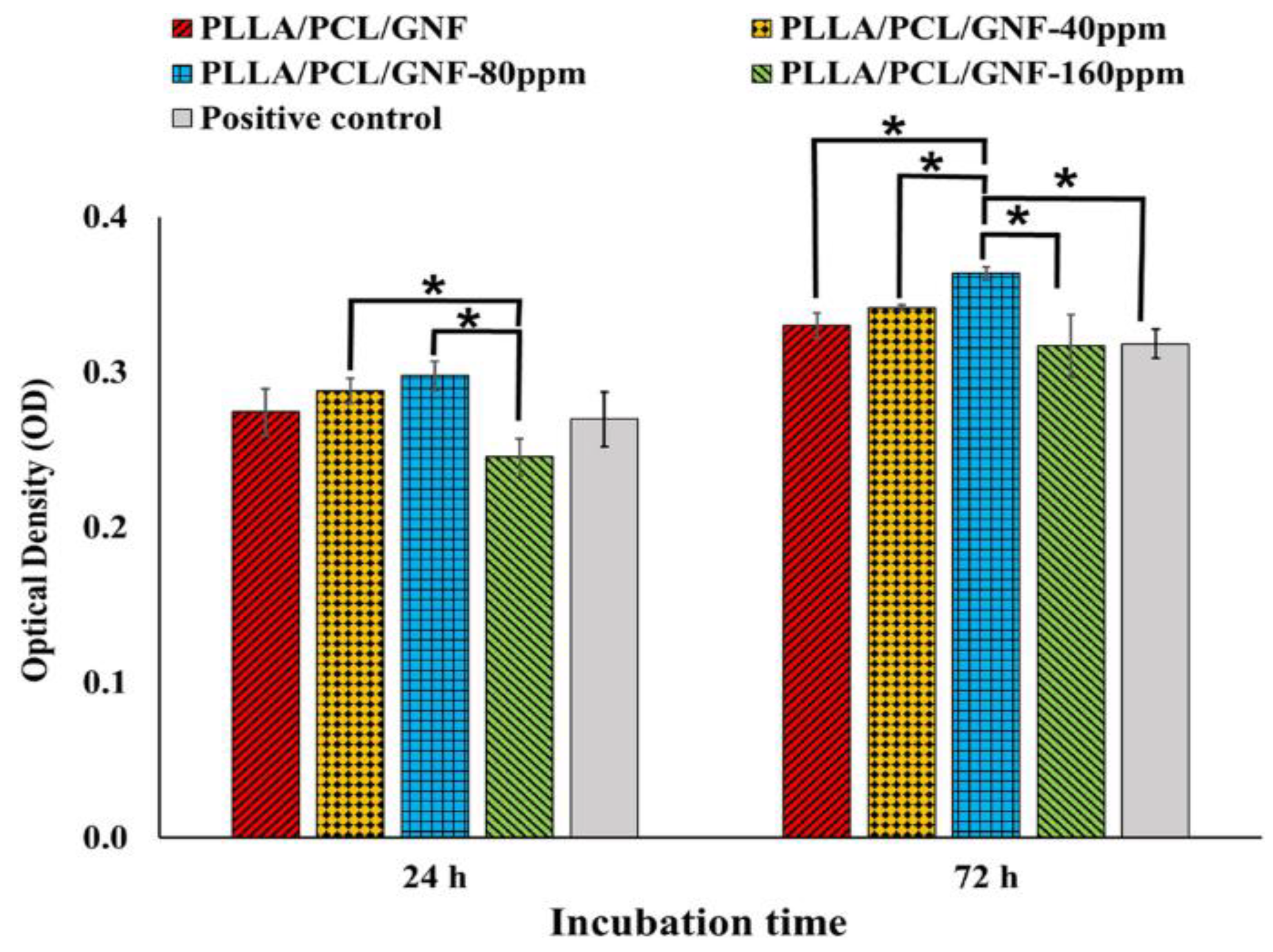
Figure 4.
The SEM images on 3D-printed biomaterial scaffolds seeded with osteoblast-like MG-63 cells and the scaffold without cells (control). (a) reference scaffold (scaffold without cells), (b) day 7 cell adhered on the surface of the printed scaffold, (c) magnified image of day 7 of cell adhered to the printed scaffold surface. Reprinted with permission from Ref. [74]. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Figure 4.
The SEM images on 3D-printed biomaterial scaffolds seeded with osteoblast-like MG-63 cells and the scaffold without cells (control). (a) reference scaffold (scaffold without cells), (b) day 7 cell adhered on the surface of the printed scaffold, (c) magnified image of day 7 of cell adhered to the printed scaffold surface. Reprinted with permission from Ref. [74]. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
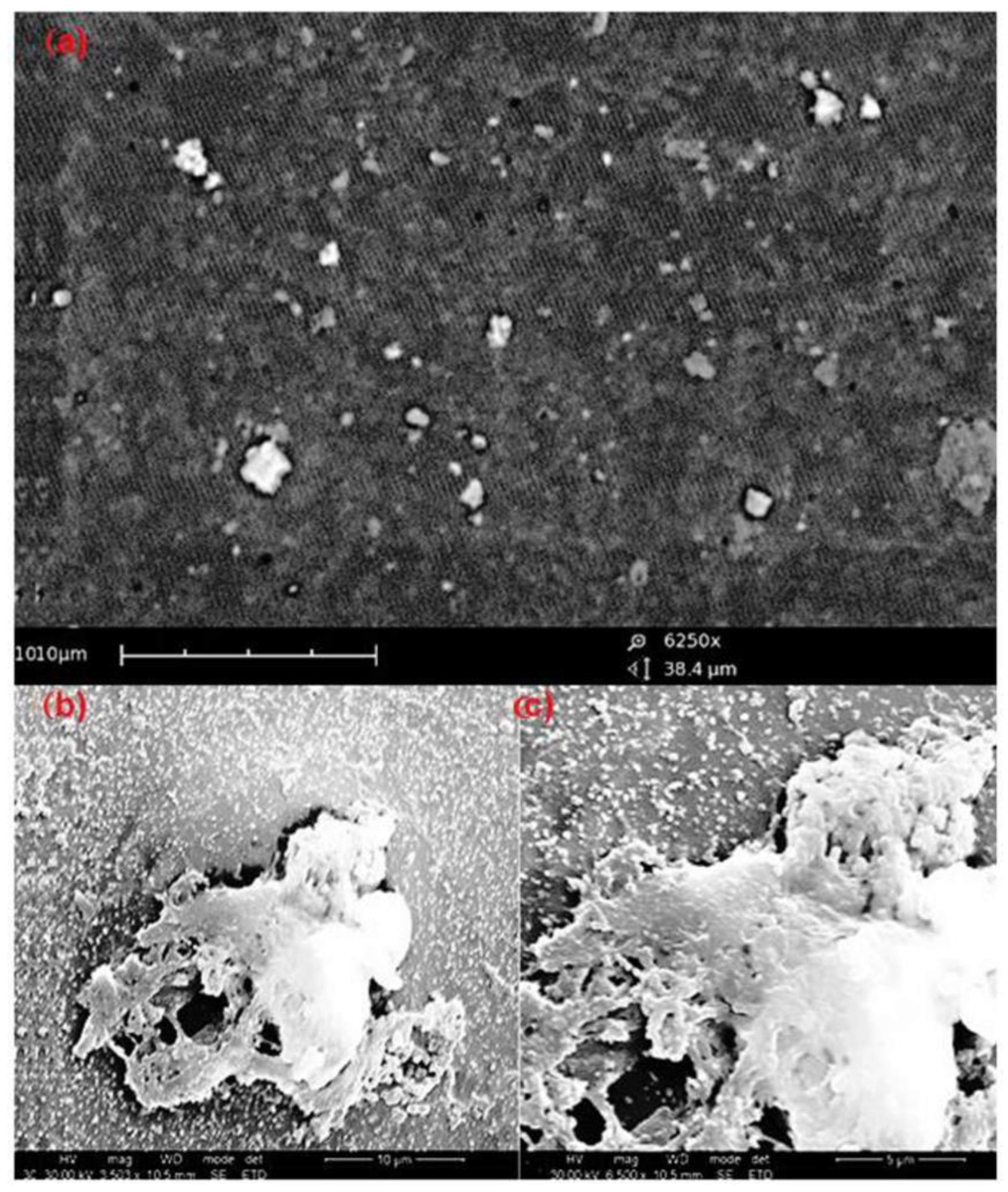
Figure 5.
A rabbit model depicting articular cartilage defects and gross observation of defects in the allotted time after operation. Reprinted with permission from Ref. [100] from Elsevier.
Figure 5.
A rabbit model depicting articular cartilage defects and gross observation of defects in the allotted time after operation. Reprinted with permission from Ref. [100] from Elsevier.
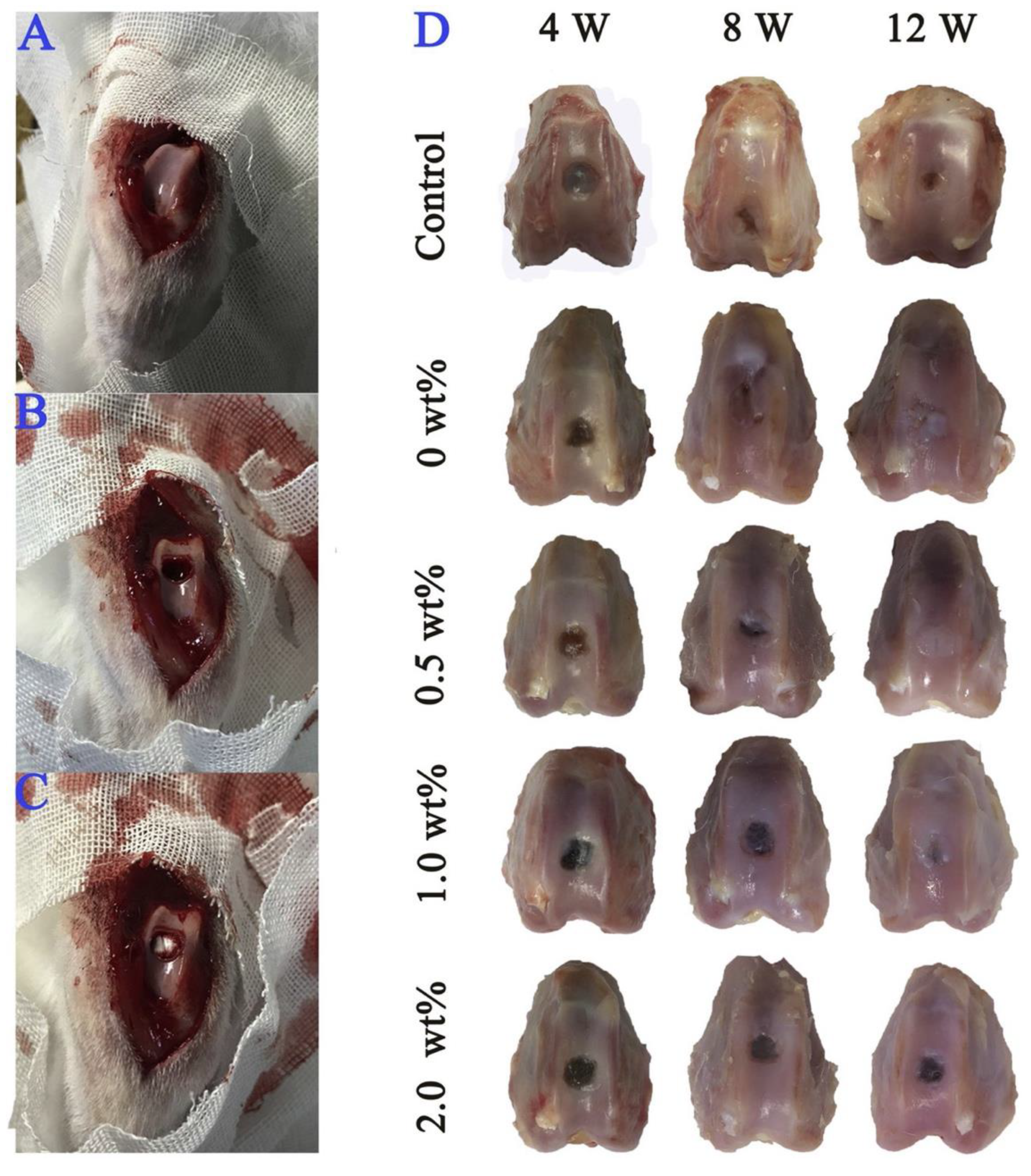
Figure 6.
Self-organized cartilage-like scaffold formed from HA, AG and type II collagen for articular cartilage tissue engineering. (A) Macroscopic image of self-organized cartilage-like scaffold. (B) Self-organized AG/HA/collagen complex as observed by SEM. (C) After 1- and 2-week incubation of chondrocytes with the self-organized AG/HA/collagen complex, chondrocytes were present on the scaffold of fibers forming the complex. Reprinted with permission from Ref. [128]. Copyright © 2019 Kumai et al. This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution–Non Commercial (unported, v3.0) License (http://creativecommons.org/licenses/by-nc/3.0/).
Figure 6.
Self-organized cartilage-like scaffold formed from HA, AG and type II collagen for articular cartilage tissue engineering. (A) Macroscopic image of self-organized cartilage-like scaffold. (B) Self-organized AG/HA/collagen complex as observed by SEM. (C) After 1- and 2-week incubation of chondrocytes with the self-organized AG/HA/collagen complex, chondrocytes were present on the scaffold of fibers forming the complex. Reprinted with permission from Ref. [128]. Copyright © 2019 Kumai et al. This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution–Non Commercial (unported, v3.0) License (http://creativecommons.org/licenses/by-nc/3.0/).
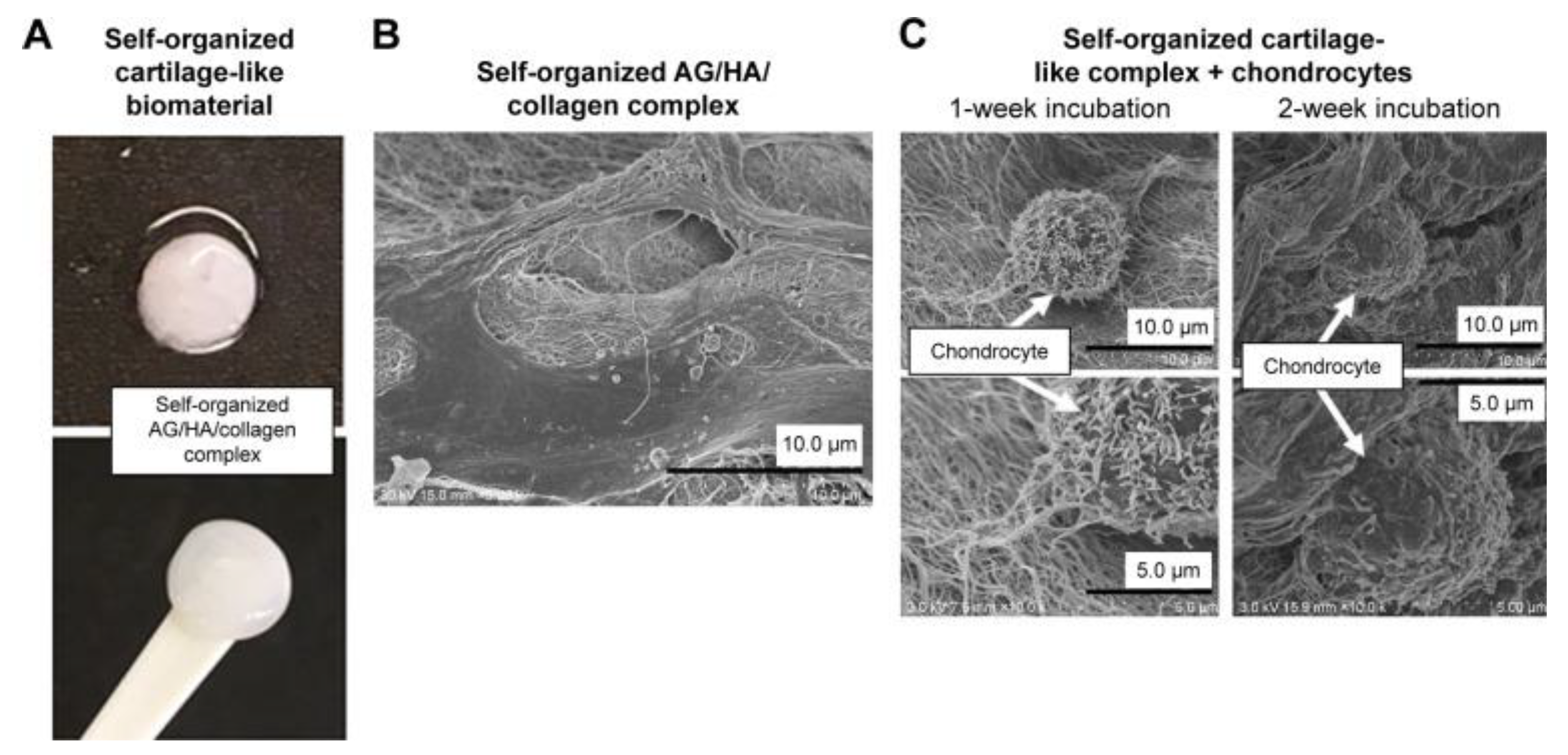
Figure 7.
Proliferation and induction of hUCB-MSCs on scaffolds. (A) Schematic illustration of the experimental design. (B) Cytotoxicity measurement of the scaffold extraction solutions. *, p < 0.05. (C) Proliferation of the cells on the scaffolds. Reprinted with permission from Ref. [130] from Royal Society of Chemistry.
Figure 7.
Proliferation and induction of hUCB-MSCs on scaffolds. (A) Schematic illustration of the experimental design. (B) Cytotoxicity measurement of the scaffold extraction solutions. *, p < 0.05. (C) Proliferation of the cells on the scaffolds. Reprinted with permission from Ref. [130] from Royal Society of Chemistry.
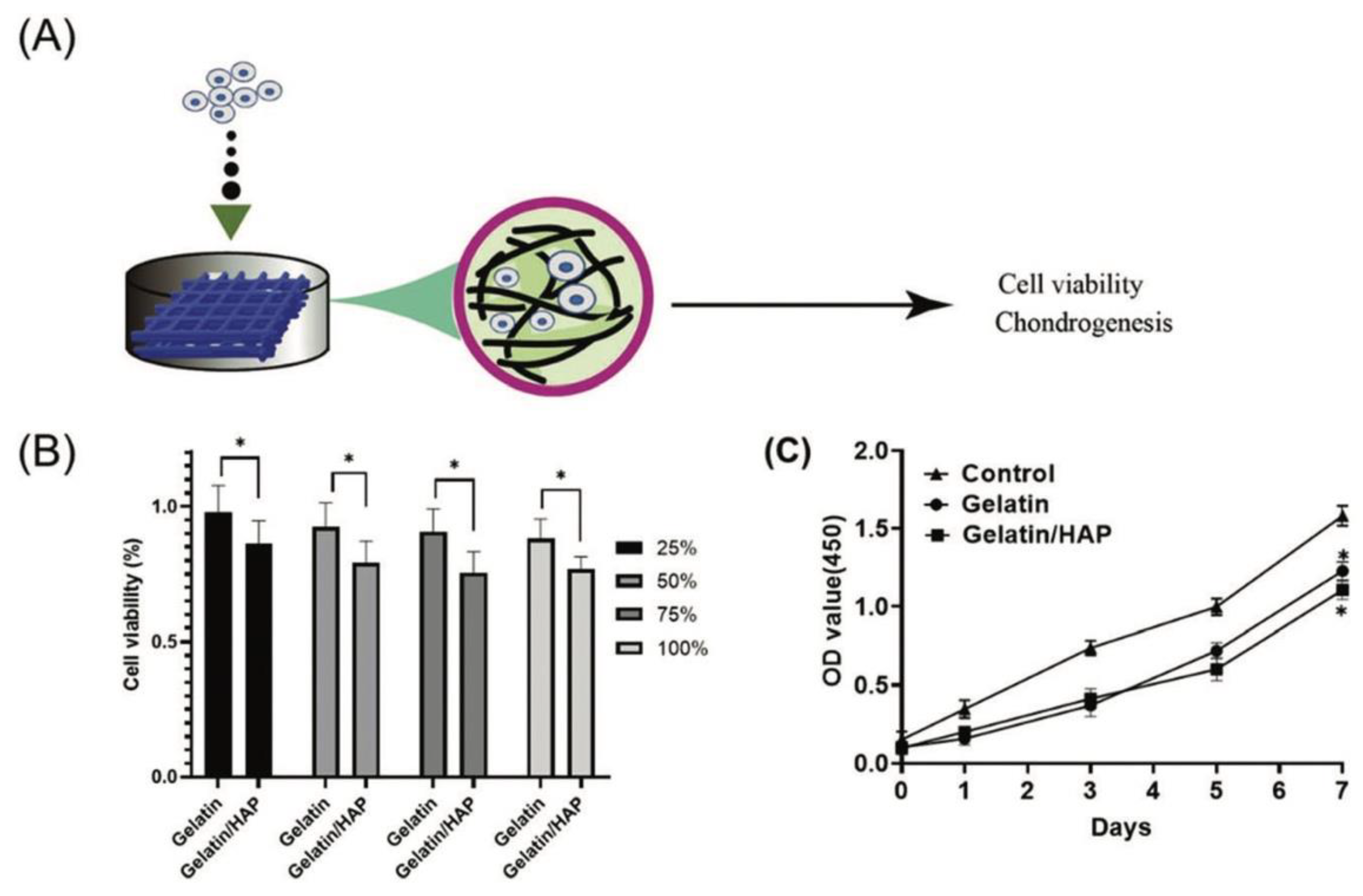
Figure 8.
Coarse-grained molecular structures of individual components of long-chain ceramides (CER), cholesterol (CHOL), and free fatty acids (FFA) of skin lipid matrix, water and thiol-coated AuNPs of different sizes were used in the simulation. Reproduced from Ref. [142]. This work is licensed under a Creative Commons Attribution 4.0 International License, http://creativecommons.org/licenses/by/4.0/.
Figure 8.
Coarse-grained molecular structures of individual components of long-chain ceramides (CER), cholesterol (CHOL), and free fatty acids (FFA) of skin lipid matrix, water and thiol-coated AuNPs of different sizes were used in the simulation. Reproduced from Ref. [142]. This work is licensed under a Creative Commons Attribution 4.0 International License, http://creativecommons.org/licenses/by/4.0/.
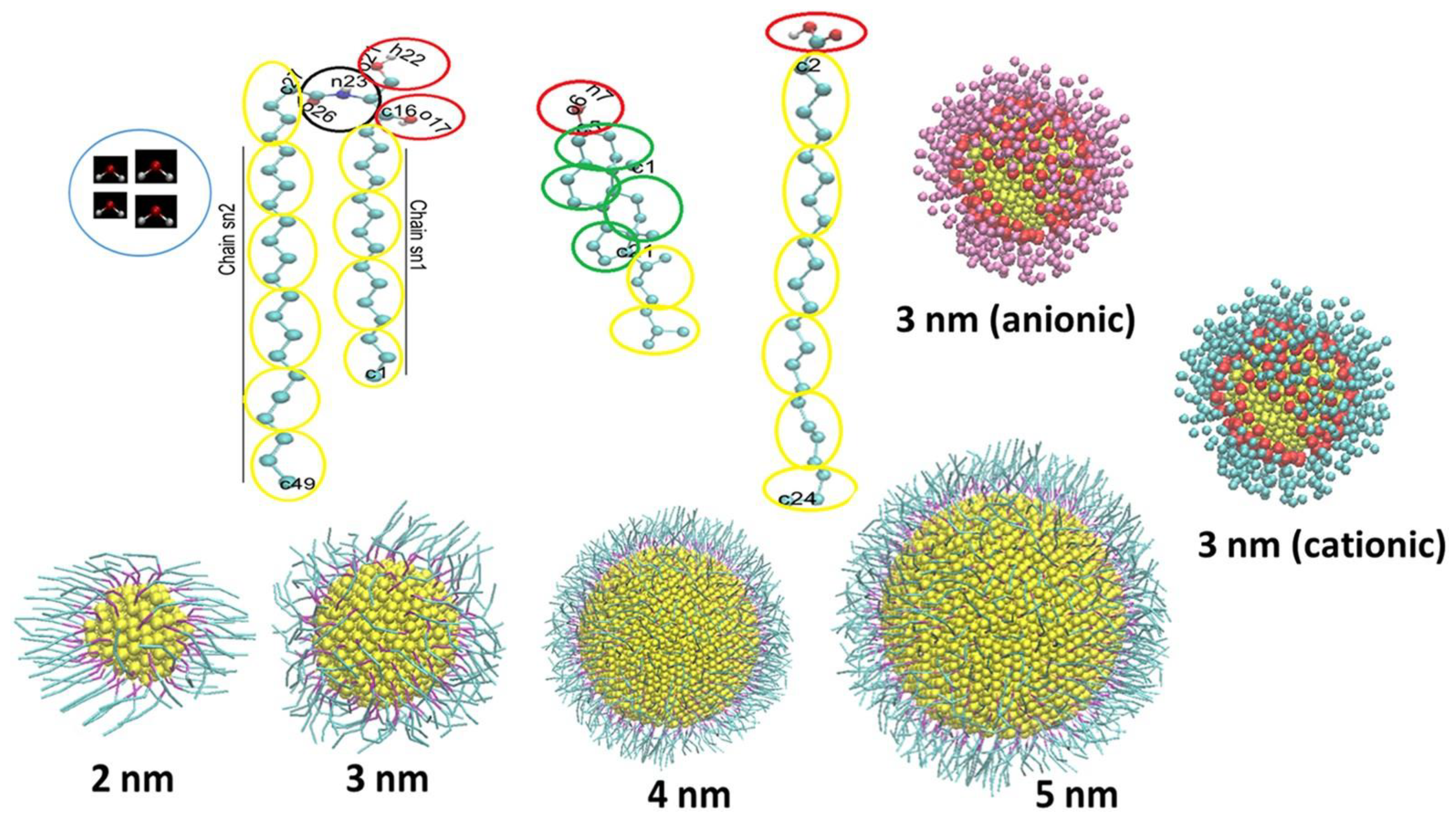
Figure 9.
The cell viability and ROS generation of MSCs with different concentrations of AuNPs. (A) The cell viability of MSCs treated with AuNPs indicated that AuNP 1.25 and 2.5 ppm treatments enhanced MSCs proliferation at 48 and 72 h, while the AuNP 5 and 10 ppm treatments had significantly lower cell viability. (B, C) Intracellular ROS generation in MSCs was detected using the FACS method after 24 and 48 hrs of treatment. AuNP 1.25 and 2.5 ppm induced lower ROS production at both time points. The results are displayed as mean ± SD (n = 3). *p < 0.05, **p < 0.01, ***p < 0.001: compared to the control group (TCPS). Reproduced from Ref. [140]. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Figure 9.
The cell viability and ROS generation of MSCs with different concentrations of AuNPs. (A) The cell viability of MSCs treated with AuNPs indicated that AuNP 1.25 and 2.5 ppm treatments enhanced MSCs proliferation at 48 and 72 h, while the AuNP 5 and 10 ppm treatments had significantly lower cell viability. (B, C) Intracellular ROS generation in MSCs was detected using the FACS method after 24 and 48 hrs of treatment. AuNP 1.25 and 2.5 ppm induced lower ROS production at both time points. The results are displayed as mean ± SD (n = 3). *p < 0.05, **p < 0.01, ***p < 0.001: compared to the control group (TCPS). Reproduced from Ref. [140]. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
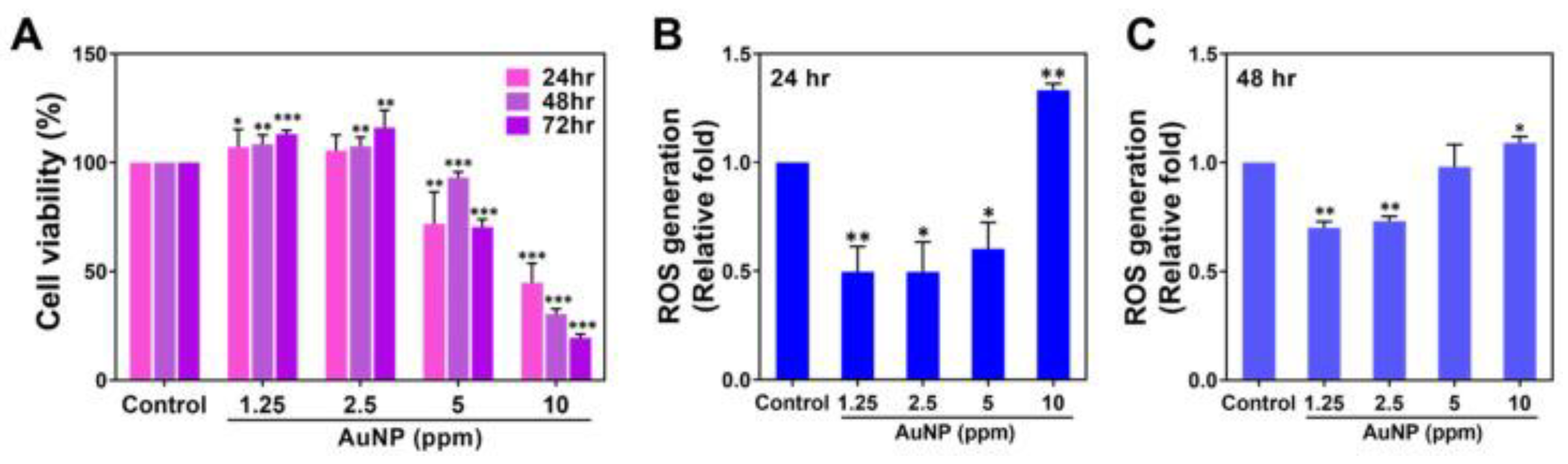
Figure 10.
Relative cell viability of HSF cells treated with (a) AuNPs and (b) Collagen-I@AuNPs. The asterisk indicates a significant difference in cell viability compared to untreated HSF cells (control; P < 0.05). Statistical analysis was performed using Turkey-Kramer (n ≥ 7). Reprinted with permission from Ref. [147] from Elsevier.
Figure 10.
Relative cell viability of HSF cells treated with (a) AuNPs and (b) Collagen-I@AuNPs. The asterisk indicates a significant difference in cell viability compared to untreated HSF cells (control; P < 0.05). Statistical analysis was performed using Turkey-Kramer (n ≥ 7). Reprinted with permission from Ref. [147] from Elsevier.
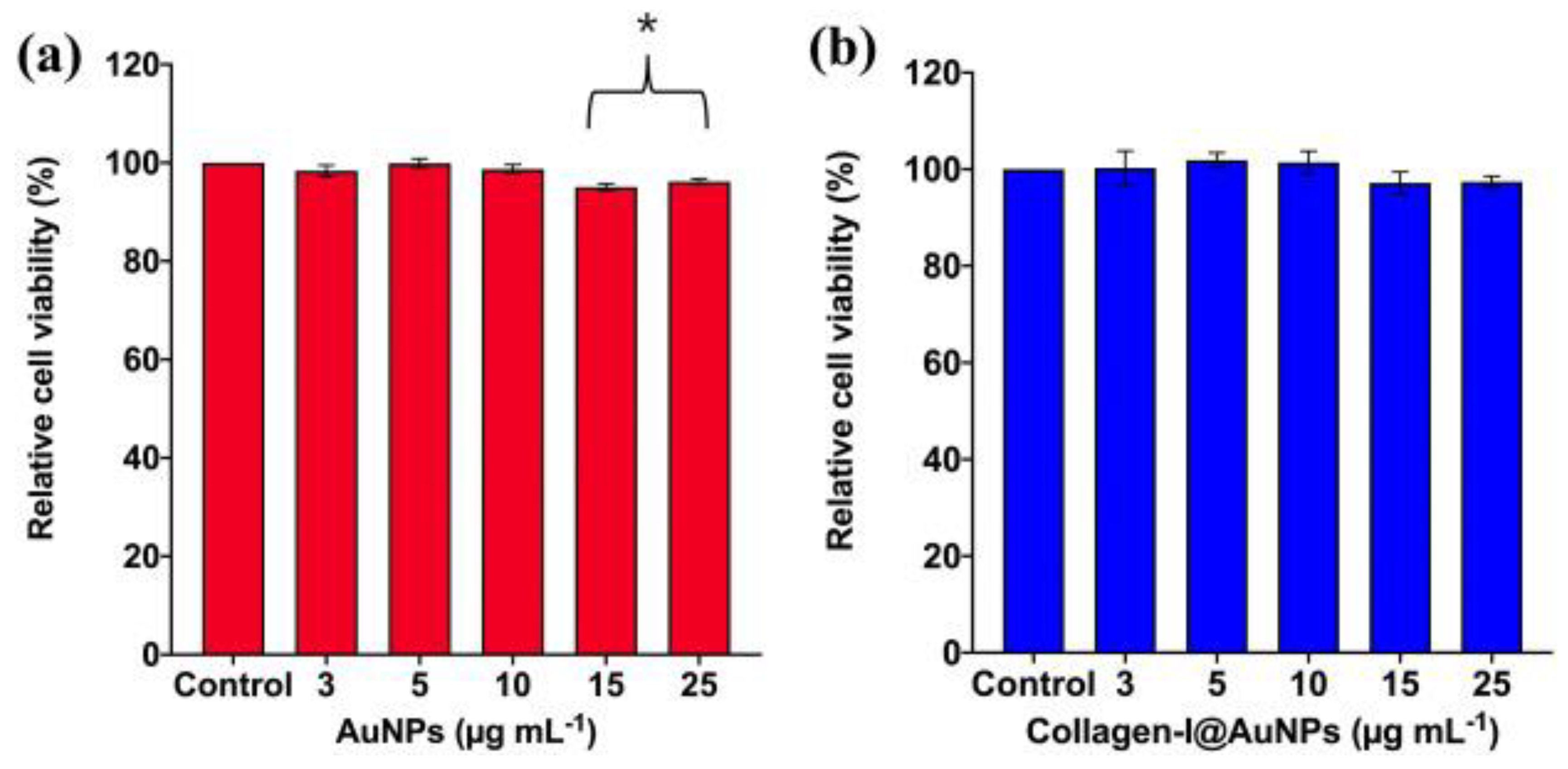
Figure 11.
(a) Percentage of wound closure of scratched HSF cells treated with 3 μg mL−1 AuNPs and Collagen-I@AuNPs for 24, 48, and 72 h. *Significant difference in wound closure percentage at P < 0.05 compared with control cells (untreated HSF cells) at 24 and 48 h, respectively. #Significant difference in wound closure percentage of HSF cells treated with AuNPs and Collagen-I@AuNPs for 24 h, at P < 0.05. Statistical analysis was performed using the Turkey-Kramer test (n ≥ 11). (b) Cell migration images of scratched HSF cells treated with 3 μg mL−1AuNPs and Collagen-I@AuNPs for 24 h, 48 h, and 72 h. The figure and caption are reprinted with permission from Ref. [147] from Elsevier.
Figure 11.
(a) Percentage of wound closure of scratched HSF cells treated with 3 μg mL−1 AuNPs and Collagen-I@AuNPs for 24, 48, and 72 h. *Significant difference in wound closure percentage at P < 0.05 compared with control cells (untreated HSF cells) at 24 and 48 h, respectively. #Significant difference in wound closure percentage of HSF cells treated with AuNPs and Collagen-I@AuNPs for 24 h, at P < 0.05. Statistical analysis was performed using the Turkey-Kramer test (n ≥ 11). (b) Cell migration images of scratched HSF cells treated with 3 μg mL−1AuNPs and Collagen-I@AuNPs for 24 h, 48 h, and 72 h. The figure and caption are reprinted with permission from Ref. [147] from Elsevier.
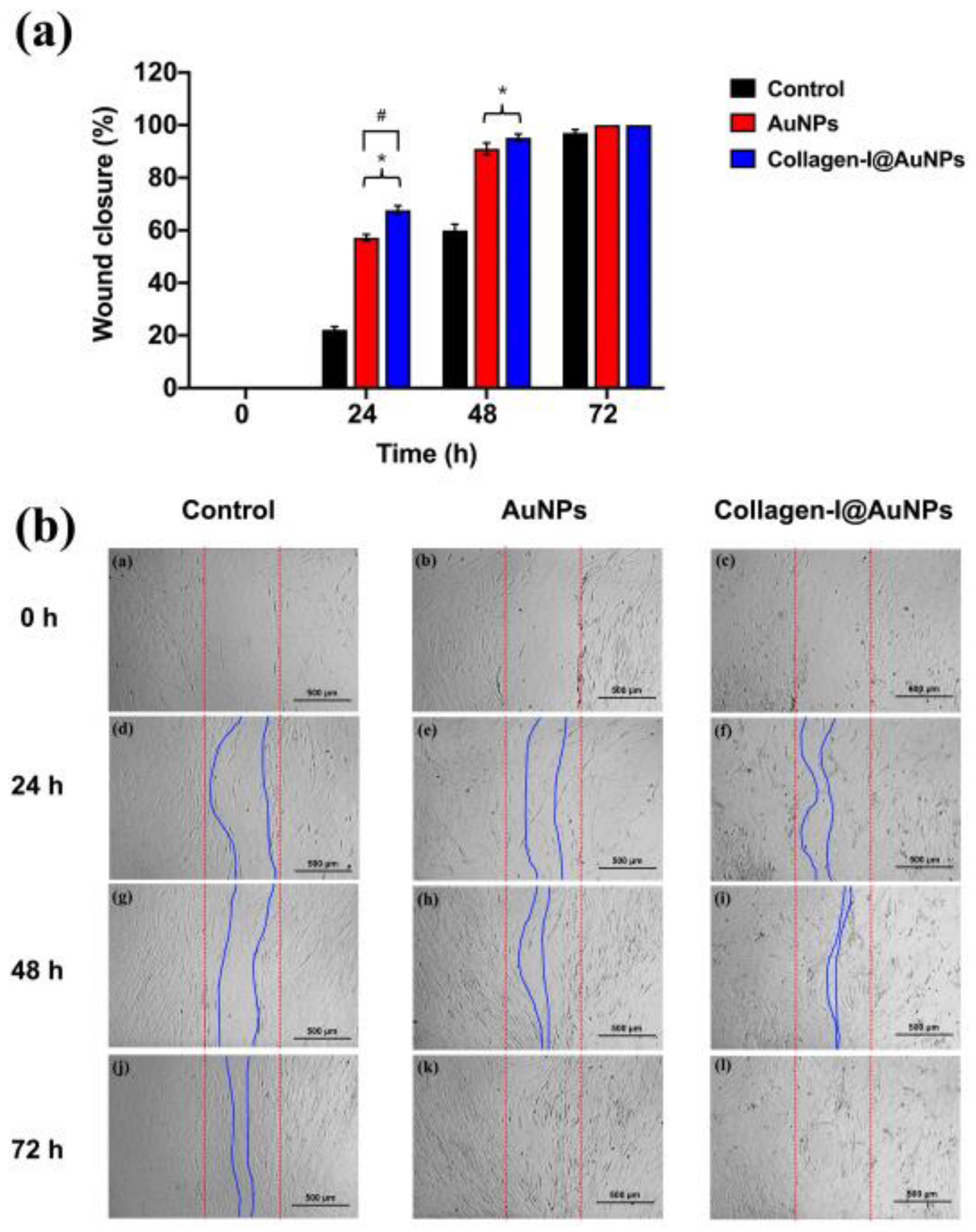
Figure 12.
The innovative strategies involved in the rational design of biomimetic natural biomaterials that can mimic the ECM of tissues. Reproduced from Ref. [148]. This article is licensed under a Creative Commons Attribution 4.0 International License, http://creativecommons.org/licenses/by/4.0/.
Figure 12.
The innovative strategies involved in the rational design of biomimetic natural biomaterials that can mimic the ECM of tissues. Reproduced from Ref. [148]. This article is licensed under a Creative Commons Attribution 4.0 International License, http://creativecommons.org/licenses/by/4.0/.
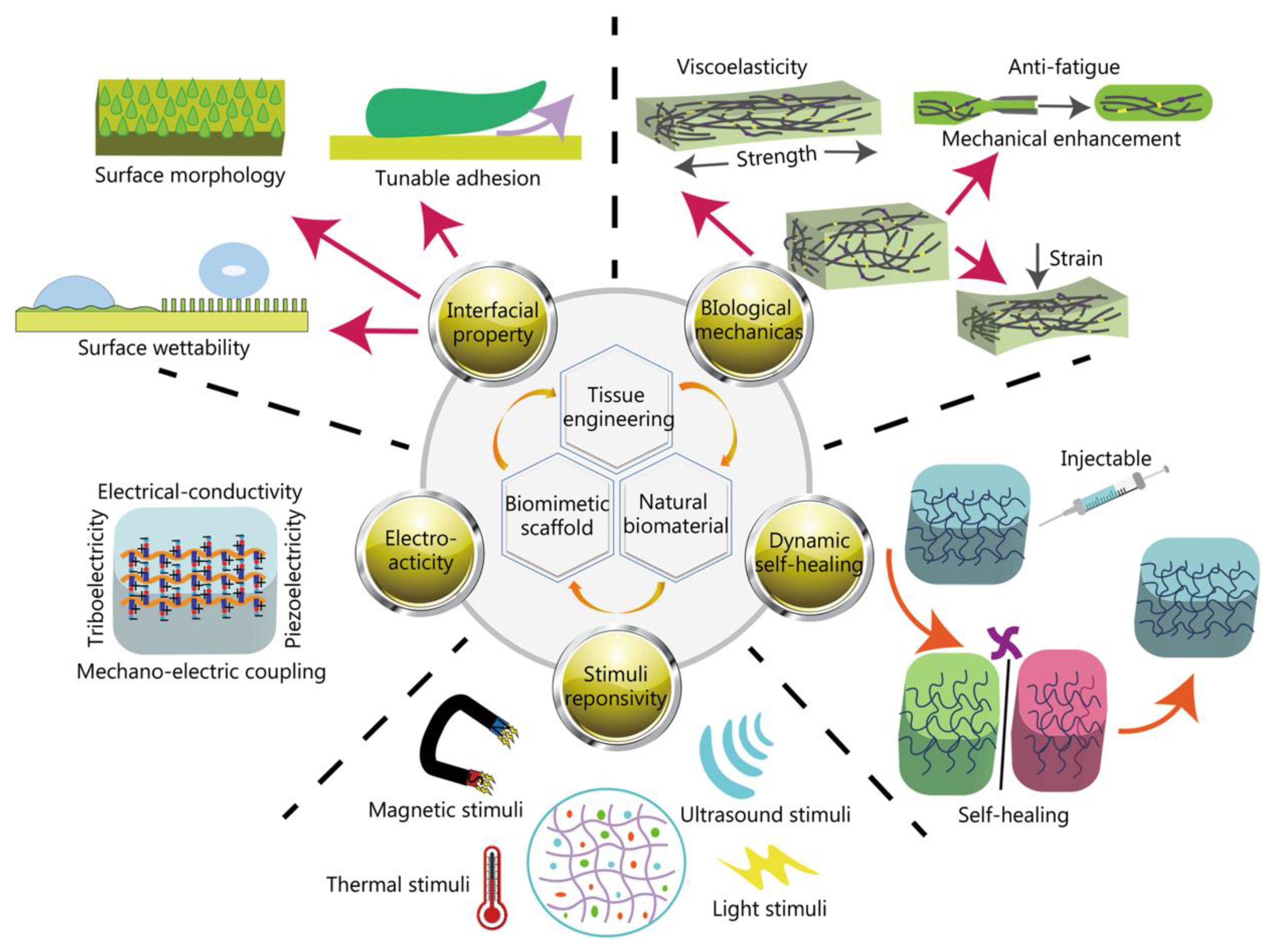
Figure 13.
Clinical trials involving biomaterials in diseases and various target tissues. (A) The in vivo application of biomaterial in diseases and target tissues. The distribution of clinical trials involving biomaterials in (B) disease categories and (C) various target tissues. (D) The distribution of clinical trials involving nanobiomaterials in different target tissues. Reproduced from Ref. [154]. This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial license, https://creativecommons.org/licenses/by-nc/4.0/.
Figure 13.
Clinical trials involving biomaterials in diseases and various target tissues. (A) The in vivo application of biomaterial in diseases and target tissues. The distribution of clinical trials involving biomaterials in (B) disease categories and (C) various target tissues. (D) The distribution of clinical trials involving nanobiomaterials in different target tissues. Reproduced from Ref. [154]. This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial license, https://creativecommons.org/licenses/by-nc/4.0/.
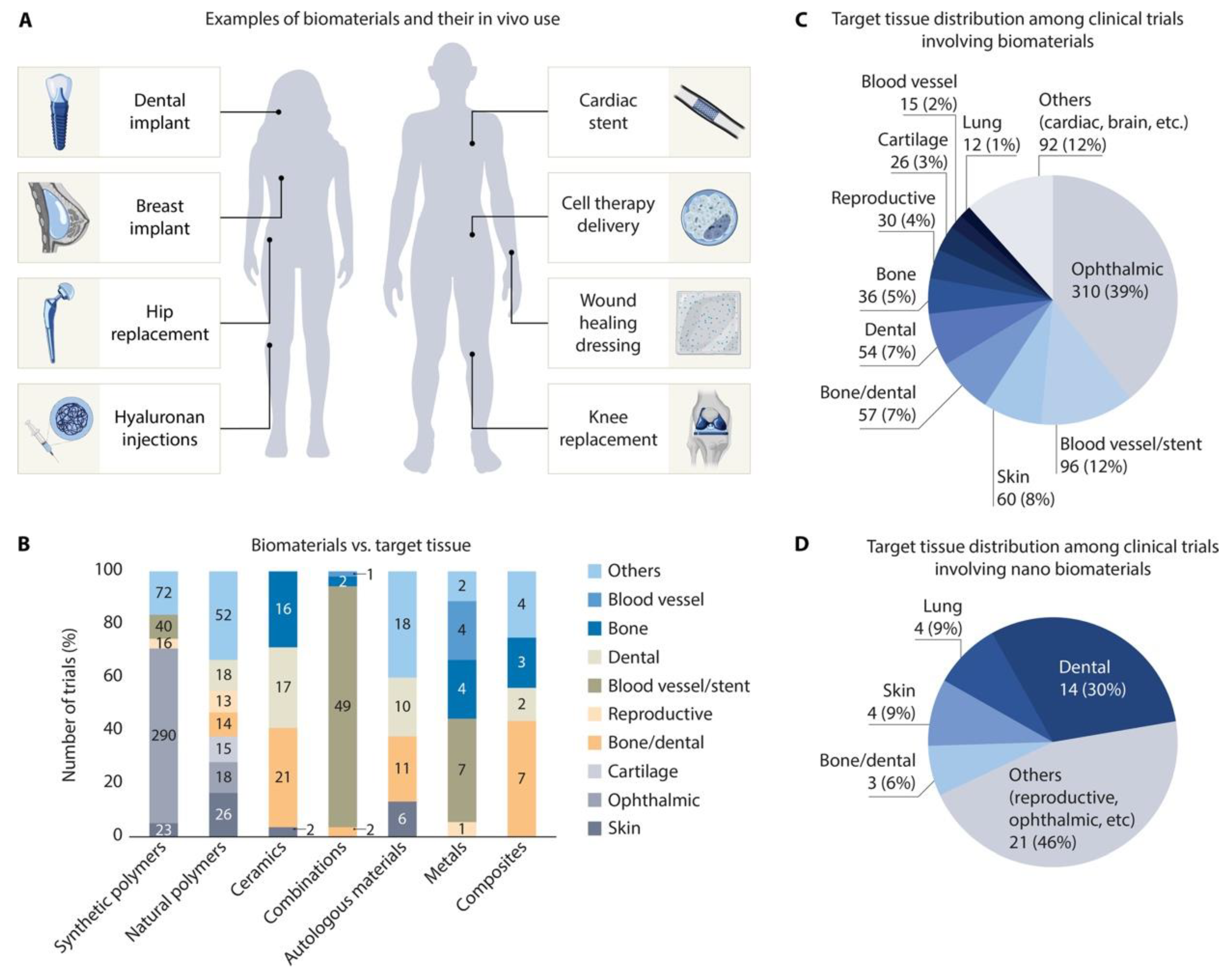
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



