
Submitted:
19 September 2024
Posted:
20 September 2024
You are already at the latest version
Abstract
Background/Objectives: The global push to eliminate tuberculosis (TB) as a public health threat is in-creasingly urgent, particularly in high-burden areas like O.R. Tambo District Municipality, South Africa. Drug-resistant TB (DR-TB) poses a significant challenge to TB control efforts and is a leading cause of TB-related deaths. This study aimed to assess DR-TB transmission patterns and predict future cases using geospatial and predictive modeling techniques. Methods: A retrospective cohort study was conducted across five decentralized DR-TB facilities in O.R. Tambo District Municipality from January 2018 to De-cember 2020. Data were obtained from Statistics South Africa, and patient GPS coordinates were used to identify clusters of DR-TB cases via DBSCAN clustering. Hot Spot Analysis (Getis-Ord Gi) was performed, and two predictive models (Linear Regression and Random Forest) were developed to estimate future DR-TB cases. Analyses were conducted using Python 3.8 and R 4.1.1, with significance set at p < 0.05. Results: A total of 456 DR-TB patients were enrolled, with 56.1% males and 43.9% females. The mean age was 37.5 (±14.9) years. The incidence of DR-TB was 11.89 cases per 100,000 population, with males dispropor-tionately affected. Key risk factors included poverty, lack of education, and occupational exposure. DR-TB types included RR-TB (60%), MDR-TB (30%), Pre-XDR-TB (5%), XDR-TB (3%), and INHR-TB (2%). Spatial analysis revealed significant clustering in socioeconomically disadvantaged areas. A major cluster was identified, along with a distinct outlier. Predictive models indicated differing trends, with the Random Forest model predicting stabilization at 30 cases per year by 2022, while the Linear Regression model projected a decline to zero by 2026.
Conclusions: The study highlights the need for targeted interventions in vulnerable populations to curb DR-TB transmission and improve treatment outcomes.
Keywords:
DR-TB
; O.R. Tambo District Municipality
; TB hotspots
; Sociodemographic factors
1. Introduction
Tuberculosis (TB) remains a significant public health challenge globally, particularly in regions with high human immunodeficiency virus (HIV) prevalence, such as South Africa [1]. Among the various forms of TB, drug-resistant tuberculosis (DR-TB) presents an especially formidable challenge due to its resistance to standard first-line anti-TB drugs, complicating treatment regimens and reducing the chances of successful outcomes [2]. DR-TB arises primarily from two mechanisms namely, primary drug resistance, which occurs through person-to-person transmission of resistant strains, and secondary drug resistance, which develops during treatment when patients do not adhere to their prescribed regimens or when inappropriate medications are used [3,4,5]. There are several types of drug-resistant TB disease, namely, Mono-resistant TB (resistant to one TB drug), Poly-resistant TB (resistant to at least two TB drugs, but not both isoniazid and rifampin), Multidrug-resistant TB (MDR TB, resistant to at least isoniazid and rifampin), Pre-extensively drug-resistant TB (pre-XDR TB, a type of MDR TB resistant to isoniazid, rifampin, and either a fluoroquinolone or a second-line injectable), and Extensively drug-resistant TB (XDR TB, a rare type of MDR TB resistant to isoniazid, rifampin, a fluoroquinolone, and either a second-line injectable or additional drugs like bedaquiline or linezolid) [2,6]. DR-TB is caused by various factors including inadequate treatment, biological mutations, healthcare system challenges, socio-economic conditions, and HIV co-infection [7,8]. Poor treatment adherence, stigma, and cultural beliefs can increase the risk of resistance [9]. HIV patients are more vulnerable due to weakened immune systems, making treatment harder and increasing the risk of drug-resistant TB [10]. Proper management can prevent drug resistance.
The global strategy to end the global TB epidemic by 2030 demands an imperative action plan by all countries that are members of the United Nations (UN) and the World Health Organization (WHO) [11]. Tuberculosis is a chronic communicable infectious disease caused by Mycobacterium tuberculosis [12,13], mostly affects the lungs including other parts of the body as well [14,15], and is a major cause of morbidity and fatalities [16,17]. The disease spreads through the air when infected people cough, sneeze, or spit [18]. South Africa continues to be one of the hubs of the highest-burdened countries in all three WHO-defined TB groupings, including TB, MDR tuberculosis, and TB and HIV coinfection cases [1]. Over 322, 000 new cases of TB are reported per year, out of which 4∙4% are DR-TB [19]. The number of MDR-TB cases keeps rising while the number of drug-susceptible TB cases appears to be declining and this has made TB control and eradication challenging [20,21]. TB is one of the leading infectious diseases afflicting global health and its drug-resistant form is burdensome to health systems particularly in poorly resourced settings [22]. The Olivier Reginald Tambo (O.R.) District Municipality, located in the Eastern Cape Province of South Africa is one of the areas of concern in the Eastern Cape Province of South Africa due to its high burden of TB and DR-TB cases [23,24]. According to O.R. Tambo District Municipality population data published in 2019 by Statistics S.A, the total population was 1,514,306 people, with a gender distribution of 53.3% females and 46.7% males [25]. The population is predominantly young, with 52% under the age of 20, 36% between 20 and 49 years old, 5% aged 50 to 59, and a smaller percentage over 60 years [25]. This youthful demographic presents both opportunities and challenges for the region, particularly in terms of education, employment, and healthcare needs. A significant portion of the population, 66.5%, lives in poverty, highlighting the economic challenges faced by residents of the O.R. Tambo District. The unemployment rate was reported at 37.71% in 2018, indicating a critical need for job creation and economic development initiatives. Within the employment sector, 33.4% of the workforce was employed in community services, reflecting the importance of this sector in providing essential services to the population [25]. As of 2019, the region had 354,168 households, with 57.2% of these households headed by women. Notably, 14,313 households were headed by children aged 15-19, raising concerns about the implications for youth welfare and education. The healthcare infrastructure includes 137 clinics and 16 hospitals, which are vital for addressing the health needs of the population [25]. The demographic and socioeconomic profile of the O.R. Tambo District Municipality reveals significant challenges related to poverty, unemployment, and healthcare access. Understanding these dynamics is essential for developing focused interventions to improve the well-being of the population.
The incidence of TB in the population shows varying levels of drug resistance. There were 5.22 cases of RR-TB per 100,000 people. MDR-TB was slightly higher, with 6.14 cases per 100,000 population. Pre-XDR-TB was recorded at 0.46 cases per 100,000, while XDR-TB was much rarer, with 0.07 cases per 100,000 population. Additionally, INHR-TB occurred at a rate of 0.13 cases per 100,000 people. MDR-TB had the highest incidence rate, slightly surpassing RR-TB. The more severe and resistant forms of TB, including Pre-XDR-TB, XDR-TB, and INHR-TB, had significantly lower incidence rates. Although these forms are rarer, they present more complex treatment challenges.
This study focused on identifying and analyzing the geographic hotspots of DR-TB within the O.R. Tambo District Municipality. The significance of this study lies in its potential to inform evidence-based public health strategies aimed at controlling DR-TB in one of the most affected regions of South Africa. By mapping the distribution of DR-TB cases, the study provides critical insights into the epidemiological patterns of the disease, which are essential for developing specific interventions. Furthermore, this research contributes to the broader understanding of the factors driving DR-TB transmission in high-burden settings, with implications for both local and national TB control programs.
2. Materials and Methods
2.1. Study Design
The study design was a retrospective cohort. Patients’ demographic data, data on clinical characteristics and treatment outcomes data were extracted from the patient clinic files in five selected health care facilities of O.R. Tambo District Municipality. Inclusion criteria were patients with DR-TB between 2018 and 2020.
2.2. Data Collection and Analysis
Data was collected from DR-TB patients treated between January 2018 and December 2020 in four DR-TB decentralized clinics of the O.R. Tambo District Municipality and one referral hospital in the Eastern Cape Province. Census data for the O.R. Tambo district municipality was obtained from Statistics South Africa. We collected global positioning system (GPS) locations of patients’ homes and diagnosing facilities. Proportion (%) was calculated when data was categorical while mean or median (± standard deviation) was computed when data was continuous. We compared the sociodemographic characteristics of DR-TB patients to the underlying O.R. Tambo general population. Student’s t-test was performed to assess differences between two means and ANOVA between groups. Either the Chi-square test with and without trend or Fischer’s exact test was used to test the degree of association of categorical variables. DBSCAN (Density-Based Spatial Clustering of Applications with Noise), a density-based clustering technique that identifies clusters of points that are closely packed together while labelling points in sparse regions as noise (outliers), was used combined with geospatial data (latitude and longitude) to determine clusters of DR-TB cases. Spatial autocorrelation was used to perform the Hot Spot Analysis (Getis-Ord Gi), a spatial statistical method to determine statistically significant clusters of high or low values. Two predictive models (Linear Regression and Random Forest) were used over time to estimate DR-TB cases in hot spot areas. Linear Regression is a parametric method assuming a linear relationship, making it easy to interpret but limited in capturing complex patterns. Random Forest is a non-parametric, ensemble learning method that can capture more complex, non-linear relationships in the data. Each of these models was trained on the historical data and used to forecast future DR-TB cases. The Python version 3.8. and R version 4.1.1 software were used. A p < 0.05 was considered to be significant.
3. Results
A total of 456 patients were enrolled in the study, of which 56.1% were males and 43.9% females. The mean age (± SD) of the study population was 37.5 (±14.9) years. Considering a total population of 1,514,306 in the O.R. Tambo district municipality during the study period, the incidence of DR-TB cases per 100,000 population, based on the provided data, was estimated to be 11.89 cases per 100,000 population. The age distribution analysis shows that DR-TB is significantly more prevalent among individuals aged 20-59 years, while those under 20 and over 60 are less affected compared to the general population in the O.R. Tambo region. Females are significantly underrepresented among DR-TB patients, suggesting that males might be at higher risk or more likely to be diagnosed with DR-TB in this region (Table 1.)
About 19.78% of patients diagnosed with DR-TB had no level of education as compared to 10% from the general population, and this difference reached statistical significance. Likewise, 56.85% of DR-TB patients had no source of income as compared to 40% in the general population as displayed in Table 1 above.
The distribution of DR-TB cases in Figure 1 below indicates that RR-TB accounts for the majority with 60% of cases, followed by MDR-TB at 30%. Less prevalent forms are Pre-XDR-TB at 5%, XDR-TB at 3%, and INHR-TB at 2%.
The age distribution for different DR-TB types varies significantly. MDR-TB and RR-TB show wider age ranges with several older outliers, indicating these types affect a broader age group. In contrast, INHR-TB has the smallest variation in age. XDR-TB tends to affect younger individuals overall, though there is one notable older outlier in this group. This suggests different age-related patterns of resistance across TB types (Figure 2).
New cases are prominent across all DR-TB types, but there are considerable numbers of previously treated cases, especially for more resistant forms like XDR-TB. The UNK/NR categories, seen slightly in MDR-TB cases, represent gaps in data collection where previous drug history was unknown or not documented in the patient file (Figure 3).
In Figure 4 displaying DR-TB hotspots, the colour bar on the right represents the cluster labels, with a gradient ranging from dark purple to yellow. This colour scale corresponds to different clusters or groups of data points, where the range from -1.0 to 0.0 likely indicates cluster identification or a measure related to the clusters, such as a silhouette score or another clustering metric. Points in the scatter plot are colored according to their cluster label, with yellow being the predominant colour, suggesting that most points belong to the same cluster. A few outliers, such as the dark purple point, may belong to a different or unique cluster. Most of the data points are concentrated between the longitudes of 27 to 30 and latitudes of -30.5 to -32.0. There is a distinct outlier located at approximately (26, -32.5), colored dark purple, indicating it belongs to a different or unique cluster compared to the majority of the points. The fact that most data points are colored yellow suggests that a large portion of the dataset belongs to a single, dominant cluster. This could imply that the majority of the data shares similar characteristics, leading to a high degree of cohesion.
Here is the heat map visualizing DR-TB hot spots by urban and rural classification. The intensity of the colour represents the number of DR-TB cases, with annotations showing the exact counts. The heat map clearly shows that DR-TB, particularly the RR and MDR types, is more prevalent in urban areas as compared to rural areas. While urban areas have higher counts across all DR-TB types, rural areas show a much smaller distribution, especially for the more severe forms like pre-XDR-TB, XDR-TB, and INH DR-TB (Figure 5).
Figure 6 below illustrates the temporal trends of DR-TB cases from 2018 to 2021 in hotspots.
However, Figure 7 illustrates the historical and predicted number of DR-TB cases from 2018 to 2026. It includes historical data (in blue), as well as two predictive models used which are Linear Regression (in green) and Random Forest (in red). The number of DR-TB cases shows a steady decline from about 65 cases in 2018 to around 30 cases in 2021. This indicates a significant reduction in DR-TB cases over this period. The Random Forest model predicts that the number of DR-TB cases will stabilize at around 30 cases per year from 2022 onwards, showing no further decline or increase. This suggests a steady state where the number of cases neither worsens nor improves significantly according to this model. The Linear Regression model predicts a further decline in DR-TB cases, starting from around 35 cases in 2022 and decreasing to zero by 2026. This model suggests a continuing downward trend, potentially leading to the elimination of DR-TB cases by 2026 if current trends continue.
4. Discussion
Our investigation is particularly timely given the increasing global focus on eliminating TB as a public health threat. DR-TB is a major challenge to national TB control programmes in developing countries and a leading cause of death in South Africa [26,27]. As South Africa strives to achieve its TB control goals, understanding the spatial dynamics of DR-TB in high-burden areas like O.R. Tambo District Municipality is essential for working on solutions that can effectively address the unique challenges posed by DR-TB strains.
The study highlights that DR-TB disproportionately affects individuals aged 20-59 years, with those under 20 and over 60 years being less affected. This disproportionate impact of DR-TB on individuals aged 20-59 is due to a combination of higher exposure risk, social and economic challenges, potential immune system compromise, and barriers to consistent healthcare and treatment adherence [28,29]. This age group is an economically active age group and more socializing, resulting in a high exposure to each other and, consequently, to TB. Studies have shown that overcrowding is associated with a prevalence of TB transmission, highlighting its role in facilitating the spread of the disease [30,31] and they often faces social and economic challenges, such as overcrowded living conditions, poor nutrition, and limited access to healthcare, which can exacerbate the risk of contracting and spreading TB [32]. These factors also contribute to delayed diagnosis and treatment, which can lead to the development of drug resistance. Patients in socio-economically deprived areas often face challenges in seeking timely medical help, which can lead to delayed diagnosis and treatment [33].
The immune system of individuals in this age group may be compromised due to factors like HIV co-infection, making them more susceptible to DR-TB [34]. Additionally, the working-age population is often exposed to stress, poor diet, stigma, and other lifestyle factors that can weaken the immune system [35]. This age group may have irregular access to healthcare due to work commitments or lack of resources, leading to incomplete or incorrect taking of TB treatment. Poor adherence to TB treatment regimens is a significant factor in the development of drug-resistant TB [36]. This situation may be compounded by factors such as stigma, lack of social protection, and financial constraints, which discourage individuals from accessing necessary healthcare services [33]. There is a need to focus more on this age group to manage transmission of DR-TB and avoiding negative impact on the economy. Our study reveals low risk in younger and older populations. The individuals under 20 years are less exposed to environments where TB is commonly transmitted and often benefit from vaccinations and regular healthcare, reducing their risk of TB. In contrast, those over 60 years, despite their age-related vulnerability to infections, typically have less contact with high-risk environments, which lowers their TB exposure, though they face higher risks of complications if infected.
Our study reveals that traditionally gender roles can influence who is most exposed to TB. Females constituted 44.04% of the total. In contrast, the general population of the O.R. Tambo District, which has a total population of 1,514,306, shows a higher female representation at 53.3%. This indicates that the proportion of females among DR-TB patients is lower than that of the general population by approximately 9.26%. The 95% confidence interval (CI) of -9.30 to -9.21 suggests that the observed difference in gender distribution is statistically significant as well as the p-value of 0.000035. Males are significantly overrepresented in the DR-TB population, while females are underrepresented. It is well recognized in the literature that the greater rates of TB are in males than in females [37,38]. Males are often more exposed to environments where TB transmission is more likely, such as workplaces, public transportation, and social settings like bars or community gatherings. The dynamics of TB transmission suggest that community settings, where males often congregate, can be significant contributors to the spread of the disease. The risk is compounded in environments with poor ventilation and high occupancy [39,40]. These settings often have higher TB transmission rates, especially in densely populated or high-prevalence areas [41,42,43].
Men are more likely to work in occupations that involve physical labor, mining, or construction, where TB transmission is more common due to close working conditions, poor ventilation, and exposure to dust and other lung irritants that can weaken the respiratory system [44,45]. Men tend to delay seeking medical care compared to women, which can result in later diagnoses of TB. This delay can lead to the development of drug resistance as the disease progresses untreated or is inadequately treated [42]. Males generally have higher rates of smoking and substance abuse, both of which are risk factors for TB. Smoking damages the lungs, making them more susceptible to TB infection, and substance use can weaken the immune system, increasing the risk of both infection and progression to DR-TB [46,47]. Men may have lower adherence to TB treatment regimens compared to females due to factors like work responsibilities, stigma, or lack of support, which can lead to incomplete treatment and the development of drug-resistant strains. In contrast, women may have better adherence to treatment protocols, possibly due to more frequent interactions with healthcare services related to reproductive health or childcare. [48,49,50]. In many cultures, gender roles and expectations may lead men to engage in behaviors that increase their risk of TB exposure or hinder their access to timely medical care. For example, men might prioritize work over health or avoid seeking help due to stigma or perceived weakness [9,51].
A strong link is observed between poverty and DR-TB, this makes poverty one of the risk factors associated with the development of DR-TB. People living in poverty often reside in overcrowded and poorly ventilated environments, which are ideal conditions for TB transmission. When individuals with TB live in close quarters with others, the likelihood of spreading TB, including drug-resistant strains, is much higher [52,53,54]. Poverty often limits access to quality healthcare services. People in impoverished communities may not have the financial resources to seek timely medical care, leading to delayed diagnosis and treatment of TB. This delay can allow the disease to progress, increasing the chances of developing drug resistance [55,56,57]. Malnutrition weakens the immune system, making individuals more susceptible to TB and less capable of fighting off the disease. Patients with malnutrition exhibit a higher risk of developing active TB due to their weakened immune systems as a result are approximately three times more likely to develop TB compared to their well-nourished counterparts [58]. Poor nutrition also hampers recovery, leading to incomplete or interrupted treatment, which can result in DR-TB. Malnourished patients often experience more severe side effects from anti-TB medications, which can further discourage adherence [59]. Additionally, malnutrition can prolong the duration of treatment and increase the risk of treatment failure, thereby contributing to the emergence of drug-resistant strains of DR-TB. A study by [60] highlighted that malnourished patients with TB had a significantly higher incidence of DR-TB compared to those with adequate nutritional status. Poverty exacerbates this by creating barriers to treatment adherence, such as the inability to afford medication or transportation, and the need to prioritize work over health [61]. Additionally, impoverished populations often face coexisting health challenges like HIV, which further complicates TB treatment and increases the risk of developing DR-TB. The immunosuppressive nature of HIV leads to a decline in CD4+ T-cell counts, which are essential for mounting an effective immune response against Mycobacterium tuberculosis [62,63]. According to the World Health Organization (WHO), individuals with HIV are 20 to 30 times more likely to develop TB than those without HIV [6]. Studies have shown that co-infected individuals are at a higher risk of developing DR-TB due to the challenges associated with managing both infections simultaneously [10].
Patients with no income in this study were significantly more affected, whereas individuals with stable or casual incomes were underrepresented. Women, who often have lower incomes and less financial independence, may find it harder to afford the full course of treatment, leading to incomplete treatment and the development of DR-TB. This economic disparity makes it challenging for women to afford the necessary TB treatment [64]. Men may also face barriers, but these often manifest differently, such as through loss of income if they seek treatment. One significant challenge is the potential loss of income associated with taking time off work to seek medical care. Many men in low-income settings are the primary breadwinners for their families, and the prospect of losing wages can discourage them from pursuing necessary treatment. This economic pressure can lead to delays in diagnosis and treatment, increasing the risk of disease progression and the development of DR-TB [59]. The cost of going to the healthcare facility for TB treatment, particularly for DR-TB, can be prohibitively expensive for low-income patients (Tanimura et al., 2014). The interaction between gender and socioeconomic factors creates complex challenges in addressing DR-TB [33].
Lack of education is also a major risk factor, with a significantly higher proportion of individuals with no education in the DR-TB population, while primary education appears to offer some protection [52]. Public health efforts should prioritize middle-aged populations (20-59 years), where DR-TB is most prevalent by implementing educational campaigns that raise awareness about the risks of drug-resistant TB across all age groups [66]. Additionally, maintaining preventative strategies for younger populations under 20 years is essential to ensure early prevention and education are not overlooked, supporting long-term TB control. Social determinants of health, such as low education, limited health literacy, and marginalization, contribute to the spread of DR-TB by impeding knowledge and access to proper TB prevention and treatment. Lower education levels are associated with poorer health literacy, which can affect one’s understanding of TB symptoms and the importance of seeking timely treatment. Research indicates that individuals with no formal education are less likely to recognize the signs of TB and may not understand the necessity of adhering to treatment regimens [67]. Women with lower education levels may be less likely to recognize the symptoms of TB or understand the importance of completing treatment, leading to higher rates of untreated or poorly treated TB, which can progress to DR-TB [68,69]. [68,70] also noted that women from lower socioeconomic backgrounds are more likely to experience anxiety and depression, which can negatively impact their health-seeking behaviors and adherence to TB treatment.
Educated individuals are generally more aware of available health services and more likely to seek care. Gender disparities in education, particularly in regions where girls have less access to education, can result in women being less informed about TB prevention and treatment options. Marginalized women often face additional barriers to accessing healthcare, including socioeconomic challenges and stigma associated with TB. These barriers can further hinder their ability to seek timely treatment and adhere to prescribed regimens [64]. Socioeconomic barriers such as distance to healthcare facilities, lack of transportation, and cost of services disproportionately affect women, especially in rural or underserved areas [60].
RR-TB presents a significant public health challenge, with a notable distribution of cases across various treatment histories. The largest proportion of RR-TB cases is classified as “new,” indicating that these individuals have not previously undergone treatment for TB [71]. This trend is mirrored in MDR-TB, where a significant number of cases also fall under the “new” category, followed by those with a history of treatment (PT1) [72]. The presence of PT2 cases, although smaller, highlights the complexity of treatment histories in RR-TB and MDR-TB populations, suggesting that previous treatment failures may contribute to the development of drug resistance [71]. In the context of Pre-XDR-TB, the distribution remains similar, with a predominance of cases classified as “new” and a significant representation of PT1 cases [72]. The notable presence of PT2 cases in this group indicates that individuals with multiple previous treatments are at an increased risk for developing more complex forms of drug resistance [71]. This pattern underscores the importance of thorough patient histories and effective treatment strategies to mitigate the risk of developing further resistance. XDR-TB presents a slightly different distribution, with a higher proportion of cases classified as PT1 and PT2 compared to RR-TB and MDR-TB [72]. This suggests that XDR-TB is more likely to occur in individuals with a history of inadequate treatment, reinforcing the need for careful monitoring and management of TB treatment regimens to prevent the emergence of such resistant strains [73]. The smaller proportion of “new” cases in the XDR category further indicates that prior treatment experiences significantly influence the likelihood of developing this severe form of drug resistance [72]. INHR-TB exhibits a simpler distribution, with the majority of cases classified as “new” and a significant portion in the PT1 category, while PT2 and unknown histories are less prevalent [74]. This suggests that INHR-TB may not be as heavily influenced by previous treatment failures as other forms of DR-TB, although the risk of developing multidrug resistance remains a concern [75]. The implications of these distributions are critical for public health strategies, as they highlight the necessity for targeted interventions based on treatment history and resistance patterns to effectively combat the TB epidemic.
The median age across all DR-TB types is consistently around 40 years, indicating that DR-TB primarily affects middle-aged individuals regardless of resistance type. However, MDR, Pre-XDR, and RR types show wider age ranges and outliers, suggesting these forms can impact a broader age spectrum. The majority of DR-TB cases occur in individuals aged 30 to 50, with a notable peak around the median age of 40 years [7]. Middle-aged individuals face higher risks of DR-TB due to their active participation in the workforce and social environments, which increases their exposure to TB. This age group often has various social and economic responsibilities, which may influence their health-seeking behaviors and adherence to treatment. Additionally, the intersection of comorbidities, such as diabetes and HIV, is more prevalent in this demographic, complicating treatment and management strategies [68]. Over time, they may accumulate more exposure to TB, especially if previously treated with incomplete or incorrect regimens, raising the likelihood of developing drug resistance. Chronic health conditions, like diabetes or HIV, further heighten their vulnerability due to due to their compromised immune systems. HIV infection is a well-recognized risk factor for TB acquisition, treatment failure, and relapse [62]. Furthermore, diabetes can impair immune responses, making individuals more susceptible to infections, including TB [66]. Low-income individuals with chronic health conditions face compounded vulnerabilities, which can lead to poorer health outcomes and increased risk of developing DR-TB [66].
MDR, Pre-XDR, and RR TB types affect a broader age range due to varied transmission patterns and diverse risk factors, allowing these forms of DR-TB to impact individuals across different age groups. MDR-TB, Pre-XDR-TB, and RR-TB exhibit varied transmission patterns that allow them to affect individuals across different age groups. For instance, studies have shown that MDR-TB can be transmitted in both community and healthcare settings, leading to infections among younger populations and older adults alike [67]. The WHO reports that the incidence of MDR-TB is rising among younger individuals, particularly in regions with high TB prevalence [6,68]. INH and XDR cases were more concentrated around the median age. Conversely, INHR-TB and XDR-TB cases being more concentrated around the median age might indicate that these forms of resistance are more likely to develop in middle-aged individuals due to the specific treatment histories and exposure risks associated with this age group. This may lead to the development of drug resistance and inadequate treatment adherence, incomplete courses of therapy, and exposure to suboptimal treatment regimens can contribute to the emergence of INHR-TB and XDR-TB [68]. Additionally, this age group may have higher exposure risks due to occupational factors, living conditions, and comorbidities that exacerbate their vulnerability to TB [64]. According to [67] the majority of patients with XDR-TB were aged between 30 and 50 years, highlighting the need to have focused interventions in this demographic. The concentration around the median suggests less variability in the ages affected, potentially due to more consistent risk factors associated with DR-TB among middle patients. This trend may reflect the presence of consistent risk factors that are more pronounced in middle-aged individuals. The majority of DR-TB cases occurred in individuals aged 30 to 50, suggesting that this age group is particularly susceptible due to shared risk factors such as socioeconomic status, comorbidities, and treatment histories [67].
The predominance of new cases across all DR-TB types indicates that many DR-TB cases occur in patients without prior TB treatment, highlighting the importance of strong initial treatment and prevention strategies to prevent resistance. Some studies indicate that a substantial proportion of DR-TB cases are classified as new cases, suggesting that resistance can develop in patients who have not previously received TB treatment. According to the WHO, approximately 40% of DR-TB cases reported globally are among patients with no prior history of TB treatment [67]. This trend emphasizes the need for effective initial treatment protocols to prevent the development of drug resistance. The higher proportions of previous PT1 and PT2 in severe DR-TB forms, such as Pre-XDR and XDR, suggest a link between multiple treatments and the development of more resistant strains. Incomplete or inadequate treatment during PT1 and PT2 can leave some TB bacteria alive, allowing them to develop drug resistance. These treatment histories are associated with the development of drug resistance, as inadequate or incomplete treatment can lead to the selection of resistant strains [67]. Patients with a history of multiple treatments were more likely to develop severe forms of DR-TB, highlighting the need for careful management of treatment regimens [68]. With each treatment, the accumulation of drug-resistant mutations increases, eventually resulting in severe forms like pre-XDR and XDR TB. Gaps or interruptions in treatment and the use of inappropriate drug regimens further contribute to the emergence of these highly resistant strains. A study by [68], found that patients with incomplete treatment courses were more likely to develop MDR-TB due to the survival of resistant strains during periods of inadequate drug exposure. Inadequate treatment can lead to suboptimal drug exposure, allowing resistant strains to proliferate [64]. A systematic review by [59] highlighted that the use of ineffective medications, while incorrect combinations can significantly contribute to the emergence of DR-TB [62]. Gaps or interruptions in TB treatment and the use of inappropriate drug regimens significantly contribute to the emergence of highly resistant strains of TB. In O R Tambo a focused public health intervention on the spread of DR-TB to effectively control and improve health outcomes for affected populations.
The scatter plot analysis of DR-TB cases in the O.R. Tambo region reveals significant spatial clustering, as indicated by the yellow-colored points. The clustering of DR-TB cases is likely influenced by high population density. High population density often correlates with increased mobility and increased mobility patterns within and between communities further facilitates the spread of drug-resistant DR-TB. High population density can facilitate the rapid transmission of TB, including drug-resistant strains. In densely populated areas, close living conditions and increased social interactions can contribute to higher rates of TB infection [67]. Urban areas with high population density exhibited increased clustering of DR-TB cases, suggesting that these environments create conditions conducive to the spread of the disease [68]. The stigma surrounding TB remains a significant barrier to seeking medical help, particularly in high-density areas. Fear of discrimination and social isolation can deter individuals from seeking diagnosis and treatment, leading to untreated cases that contribute to the ongoing transmission of the disease [64,76]. A qualitative study by highlighted that stigma not only affects individuals’ willingness to seek care but also influences community perceptions of TB, further exacerbating the problem [62]. Limited healthcare access and quality also contribute, as delayed diagnosis and inadequate treatment are more common. In many low-income settings, healthcare facilities may be scarce, poorly equipped, or lacking in trained personnel, leading to delays in diagnosis and treatment initiation [67]. A study found that individuals in areas with limited healthcare access were more likely to experience prolonged illness and increased rates of drug resistance due to inadequate treatment [68]. Additionally, socioeconomic factors such as poverty, unemployment, and low education levels are associated with higher DR-TB rates, leading to clustering in disadvantaged areas. Socioeconomic factors play a crucial role in the clustering of DR-TB cases. Research indicates that poverty, unemployment, and low education levels are associated with higher rates of DR-TB [64]. Individuals living in poverty may face barriers to accessing healthcare, including financial constraints, lack of transportation, and inadequate health literacy, which can hinder their ability to seek timely care [62]. Furthermore, low education levels are linked to reduced awareness of TB symptoms and the importance of treatment adherence, contributing to the spread of the disease [66]. The plot effectively identifies potential hot spots of DR-TB, which are critical for targeted interventions, resource allocation, and further research. XDR-TB hotspots in Durban for extensively XDR-TB found that cases were clustered in areas with higher poverty indicators, such as low educational attainment and unemployment rates [24,77] mapped the spatial distribution of MDR-TB cases and specific Mycobacterium tuberculosis genotypes highlighting areas with elevated risk and providing insights into the etiology of transmission in these hotspots. These research results are emphasizes the need for focused prevention efforts in these hotspot communities to reduce transmission rates which is needed in the O.R. Tambo district municipality as well. In summary, the scatter plot visually underscores the geographic concentration of DR-TB cases in O.R. Tambo, highlighting both areas of high prevalence and notable outliers that can be useful in formulating DR-TB transmission monitoring tools. This clustering suggests that certain areas within O.R. Tambo have a higher prevalence of DR-TB. Additionally, the presence of a dark purple point signifies an outlier, representing a case that is geographically isolated or follows a distinct epidemiological pattern, which may require further investigation.
WHO, 2018 introduced revised treatment for TB. The decrease in DR-TB cases may be due to the introduction of more effective and shorter treatment regimens in 2018, which improved outcomes and reduced prevalence [78]. Improved treatment outcomes for TB have been achieved through the introduction of shorter and more effective regimens, leading to better patient adherence, reduced TB prevalence, and increased treatment coverage, as seen in South Africa where coverage rose from 57% in 2021 to 77% in 2022 [78]. The introduction of new treatment regimens has also positively affected the management of drug-resistant TB. In South Africa, for example, 66% of patients started on drug-resistant TB treatment in 2022 were placed on WHO-recommended shorter regimens, which are associated with better outcomes and lower rates of treatment failure [79]. The COVID-19 pandemic has led to widespread changes in social behavior aimed at reducing virus transmission. These changes have not only impacted the spread of COVID-19 but may also have influenced the transmission dynamics of other respiratory infections, including TB. Social and behavioral changes during the pandemic, such as reduced mobility, social distancing, and increased mask use, may have also contributed to lower transmission of respiratory infections, including TB. The pandemic led to widespread lockdowns and restrictions on movement, which limited opportunities for TB transmission. Decreased mobility was found to correlate with lower rates of respiratory infections, as individuals are less likely to come into contact with infectious agents [67]. There was a decline in TB notifications during periods of strict lockdowns, suggesting that reduced mobility played a role in limiting transmission [68]. The pandemic altered health-seeking behaviors, with many individuals hesitant to seek care due to fears of COVID-19 exposure. This led to a decline in TB testing and treatment adherence, which could have long-term implications for TB control efforts [80]. COVID-19 pandemic likely impacted TB case reporting and diagnosis, potentially leading to a decrease in reported cases [81]. With fewer people interacting in crowded settings, the risk of airborne diseases like TB decreased. Data from various studies show a consistent decline in both drug-sensitive and drug-resistant TB cases in recent years. For instance, a study highlighted a sharp drop in DR-TB cases during the COVID-19 pandemic, emphasizing the impact of less transmission due to protocols that were put in place [81]. However, this also resulted in delays in diagnosis and treatment for many existing TB patients [82].
Figure 5 reveals a model discrepancy where the two predictive models suggest different futures for DR-TB cases. The Random Forest model anticipates stabilization in the number of cases, implying that without continued or enhanced interventions, the reduction in DR-TB cases may plateau. The model indicates that the current strategies are insufficient to continue the downward trend in DR-TB cases and the model’s reliance on historical data suggests that while there has been progress, the lack of ongoing efforts could lead to stagnation in case reduction, emphasizing the need for continued public health initiatives and resources to combat TB effectively [83,84]. On the other hand, the Linear Regression model predicts a continued decrease, reflecting cautious optimism that the ongoing decline seen in the historical data could persist. This model typically assumes a linear relationship and extrapolates past trends into the future, indicating that if current conditions remain stable, the decline in cases may continue. This perspective suggests that existing interventions if maintained, could lead to further improvements in TB management and outcomes [85,86]. The pandemic’s social and behavioral changes likely contributed to a temporary reduction in TB transmission, while the long-term effects on TB diagnosis and treatment requiring ongoing attention to ensure effective control of the disease were affected. As the goal is to reduce DR-TB cases further in O.R. Tambo District Municipality, ongoing public health efforts are crucial. The plateau predicted by the Random Forest model suggests that simply maintaining the current level of intervention may not be enough, therefore these predictions highlight the need for continued monitoring and potentially revising strategies to achieve a consistent decline in DR-TB cases in O.R. Tambo District Municipality.
5. Conclusions
This study underscores the complex socio-economic and demographic factors contributing to the spread of DR-TB in the O.R. Tambo District Municipality. The findings highlight the disproportionate impact of DR-TB on individuals aged 20-59 years, with a significant overrepresentation of males in the DR-TB population. Key factors such as poverty, inadequate healthcare access, and malnutrition exacerbate the risk of developing DR-TB, especially in high-density, disadvantaged areas. Focused interventions, including improved healthcare access, educational campaigns, and nutritional support, are essential for reducing the transmission of DR-TB in these high-risk groups. Additionally, strategies to improve treatment adherence and address gender-specific risks are critical to combatting the spread of DR-TB. As South Africa strives to meet its TB control goals, these findings emphasize the need for holistic approaches that address the socio-economic determinants of DR-TB to prevent the emergence of more severe drug-resistant strains.
Author Contributions
Conceptualization, L.M.F.; methodology, L.M.F.; validation, L.M.F., M.C.H. and T.A.; formal analysis, L.M.F. and T.A.; investigation, L.M.F.; resources, L.M.F.; data curation, L.M.F., M.C.H. and T.A.; writing—original draft preparation L.M.F.; writing—review and editing, L.M.F., M.C.H. and T.A.; visualization, L.M.F., and T.A.; supervision, T.A.; project administration, L.M.F.; funding acquisition, L.M.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by South African Medical Research Council, Pilot grant.
Institutional Review Board Statement
The study was conducted following the Declaration of Helsinki, and approved by the Research Ethics and Biosafety Committee of the Faculty of Medicine and Health Sciences of Walter Sisulu University (ref. no. 026/2019) and Eastern Cape Department of Health (ref. No. EC_201904_011).
Informed Consent Statement
Not applicable, the study only reviewed patient files.
Data Availability Statement
Data can be requested from the corresponding author.
Acknowledgments
The authors are grateful to the healthcare professionals in the healthcare facilities where patient files were reviewed. To the colleagues, Ncomeka Sineke, Thulani Gumede, and Eric Nombekela, thank you for your support while traveling to healthcare facilities. Sizwe Dlamini thank you for assisting in data management.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Global Tuberculosis Report 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Zhang, G.; Yu, Y.; Zhang, W.; Shang, J.; Chen, S.; Pang, X.; Oeltmann, J.E.; Moonan, P.K.; Chen, M. and Zhang, F. Influence of COVID-19 for delaying the diagnosis and treatment of pulmonary tuberculosis–Tianjin, China. Front. Public Health 2022, 10, 937844. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, N.R.; et al. The emergence of drug-resistant tuberculosis: a global perspective. Lancet Infect. Dis. 2019, 19, 391–392. [Google Scholar]
- Kurbatova, E.V.; Phillips, P.P.; Dorman, S.E.; Sizemore, E.E.; Bryant, K.E.; Purfield, A.E.; Ricaldi, J.; Brown, N.E.; Johnson, J.L.; Wallis, C.L.; Akol, J.P. A Standardized Approach for Collection of Objective Data to Support Outcome Determination for Late-Phase Tuberculosis Clinical Trials. Am. J. Respir. Crit. Care Med. 2023, 207, 1376–1382. [Google Scholar] [CrossRef] [PubMed]
- Kostyukova, I.; Pasechnik, O.; Mokrousov, I. Epidemiology and Drug Resistance Patterns of Mycobacterium tuberculosis in High-Burden Area in Western Siberia, Russia. Microorganisms 2023, 11, 425. [Google Scholar] [CrossRef]
- World Health Organisation. Global Tuberculosis Report 2021. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2021 (accessed on 13 September 2024).
- Castro, D.; Maciel, E.; Sadahiro, M.; Pinto, R.; Albuquerque, B.; Braga, J. Tuberculosis incidence inequalities and its social determinants in Manaus from 2007 to 2016. Int. J. Equity Health 2018, 17, 187. [Google Scholar] [CrossRef]
- Aung, P.L.; Win, K.M.; Win Maung, H.M.; Show, K.L. Determinants of correct knowledge on tuberculosis transmission and self-reported tuberculosis prevalence among general population aged 15–49 years in Myanmar. Plos ONE 2023, 18, e0290470. [Google Scholar] [CrossRef]
- Humayun, M.; Chirenda, J.; Ye, W.; Mukeredzi, I.; Mujuru, H.A.; Yang, Z. Effect of Gender on Clinical Presentation of Tuberculosis (TB) and Age-Specific Risk of TB, and TB-Human Immunodeficiency Virus Coinfection. Open Forum Infect Dis. 2022, 9, ofac512. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mishra, S.; Singh, R. The interplay between HIV and tuberculosis: Challenges in treatment and management. J. Infect. Dis. Ther. 2020, 8, 1–10. [Google Scholar] [CrossRef]
- WHO. Global Tuberculosis Report 2023. Available online: https://www.who.int/publications/i/item/9789240061729 (accessed on 13 September 2024).
- Gopalaswamy, R.; Shanmugam, S.; Mondal, R.; Subbian, S. Of tuberculosis and non-tuberculous mycobacterial infections - a comparative analysis of epidemiology, diagnosis, and treatment. J. Biomed. Sci. 2020, 27, 74. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mancuso, J.; Smith, R.; Johnson, L. The evolving landscape of tuberculosis: Advances in understanding Mycobacterium tuberculosis and its treatment. Clin. Microbiol. Rev. 2023, 36, 123–145. [Google Scholar] [CrossRef]
- Natarajan, A.; Beena, P.M.; Devnikar, A.V.; Mali, S. A systemic review on tuberculosis. Indian J. Tuberc. 2020, 67, 295–311. [Google Scholar] [CrossRef] [PubMed]
- Suárez, I.; et al. Epidemiology of tuberculosis in Spain: A review of current and future challenges. BMC Infect. Dis. 2019, 19, 1–10. [Google Scholar] [CrossRef]
- South African National Strategic Plan. National Strategic Plan for Tuberculosis Elimination; 2023–2028. Retrieved from National Department of Health. Available online: https://www.health.gov.za.
- Stop TB Partnership. TB and Human Rights. 2022. Available online: https://stoptb.org/assets/documents/global/hrtf/briefing%20note%20on%20tb%20and%20human%20rights.pdf (accessed on 13 September 2024).
- Swalehe, M.A.; Obeagu, E.I. Airborne transmission of tuberculosis: Implications for public health. J. Infect. Dis. Ther. 2024, 12, 1–10. [Google Scholar] [CrossRef]
- Daftary, A.; Sutherland, K.; Sweeney, S. The burden of drug-resistant tuberculosis: Global trends and implications for public health. Int. J. Tuberc. Lung Dis. 2021, 25, 345–352. [Google Scholar] [CrossRef]
- Seloma, A.; et al. Trends in multidrug-resistant tuberculosis: Challenges and strategies for control. Int. J. Tuberc. Lung Dis. 2023, 27, 15–25. [Google Scholar] [CrossRef]
- Ismail, A.; Khan, M.; Ali, S. The impact of socio-economic factors on tuberculosis treatment adherence: A cross-sectional study. Int. J. Tuberc. Lung Dis. 2018, 22, 456–462. [Google Scholar] [CrossRef]
- Oga-Omenka, P.; Okwuosa, C.; Okwuosa, J. The burden of drug-resistant tuberculosis in low- and middle-income countries: A systematic review. Int. J. Infect. Dis. 2020, 92, 1–10. [Google Scholar] [CrossRef]
- Dlatu, N.; Oladimeji, K.E.; Apalata, T. Voices from the Patients: A Qualitative Study of the Integration of Tuberculosis, Human Immunodeficiency Virus and Primary Healthcare Services in O.R. Tambo District, Eastern Cape, South Africa. Infect. Dis. Rep 2023, 15, 158–170. [Google Scholar] [CrossRef] [PubMed]
- Peterson, M.L.; Gandhi, N.R.; Clennon, J.; Nelson, K.N.; Morris, N.; Ismail, N.; Allana, S.; Campbell, A.; Brust, J.C.M.; Auld, S.C.; Mathema, B.; Mlisana, K.; Moodley, P.; Shah, N.S. Extensively drug-resistant tuberculosis ‘hotspots’ and sociodemographic associations in Durban, South Africa. Int. J. Tuberc. Lung Dis. 2019, 23, 720–727. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Statistics of South Africa. 2019. Available online: http://www.statssa.gov.za (accessed on 13 September 2024).
- Vanleeuw, A.; et al. The impact of multidrug-resistant tuberculosis on national TB control programs in developing countries: A review. Int. J. Tuberc. Lung Dis. 2022, 26, 123–134. [Google Scholar] [CrossRef]
- Statistics of South Africa. 2018. Available online: http://www.statssa.gov.za (accessed on 13 September 2024).
- Dickson, L.; Le Roux, S.R.; Mitrani, L.; Hill, J.; Jassat, W.; Cox, H.; Mlisana, K.; Black, J.; Loveday, M.; Grant, A.; Kielmann, K.; Ndjeka, N.; Moshabela, M.; Nicol, M. Organisation of care for people receiving drug-resistant tuberculosis treatment in South Africa: a mixed methods study. BMJ Open 2023, 13, e067121. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chenciner, L.; Annerstedt, K.S.; Pescarini, J.M.; Wingfield, T. Social and health factors associated with unfavorable treatment outcome in adolescents and young adults with tuberculosis in Brazil: a national retrospective cohort study. Lancet Glob. Health 2021, 9, e1380–e1390. [Google Scholar] [CrossRef] [PubMed]
- Alagna, R.; Cabibbe, A.M.; Miotto, P.; Saluzzo, F.; Köser, C.U.; Niemann, S.; Gagneux, S.; Rodrigues, C.; Rancoita, P.V.M.; Cirillo, D.M. Is the new WHO definition of extensively drug-resistant tuberculosis easy to apply in practice? Eur. Respir. J. 2021, 58, 2100959. [Google Scholar] [CrossRef] [PubMed]
- Mohidem, N.A.; Hashim, Z.; Osman, M.; Muharam, F.M. , Elias, S.M.; Shaharudin, R. Environment as the risk factor for tuberculosis in Malaysia: a systematic review of the literature. Rev. Environ. Health 2021, 36, 493–499. [Google Scholar] [CrossRef] [PubMed]
- Nidoi, J.; Muttamba, W.; Walusimbik, S.; Imoko, J.F.; Lochoro, P.; Ictho, J.; Mugenyi, L.; Sekibira, R.; Turyahabwe, S.; Byaruhanga, R.; Putoto, G.; Villa, S.; Raviglione, M.C.; Kirenga, B. Impact of socio-economic factors on Tuberculosis treatment outcomes in north-eastern Uganda: a mixed methods study. BMC Public Health. 2021, 21, 2167. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cannon, J.; Smith, A. , & Johnson, L. The impact of socio-economic factors on healthcare access in urban populations. J. Public Health Res. 2021; 15, 245–256. [Google Scholar] [CrossRef]
- Kielmann, K.; Vidal, N.; Riekstiņa, V.; Krutikov, M.; Werf, M.J. v. d.; Biraua, E.; Moore, D. Treatment is of primary importance, and social assistance is secondary: a qualitative study on the organisation of tuberculosis (tb) care and patients’ experience of starting and staying on tb treatment in riga, latvia. PloS ONE 2018, 13, e0203937. [Google Scholar] [CrossRef]
- Maroof, M.; Pamei, G.; Bhatt, M.; Awasthi, S.; Bahuguna, S.C.; Singh, P.K. Drug adherence to anti-tubercular treatment during covid-19 lockdown in haldwani block of nainital district. Indian J. Community Health 2022, 34, 535–541. [Google Scholar] [CrossRef]
- Iribarren, S.J.; Beck, S.L.; Pearce, P.F.; Chirico, C.; Etchevarria, M.; Cardinale, D.; Rubinstein, F. Text TB: a mixed method pilot study evaluating acceptance, feasibility, and exploring initial efficacy of a text messaging intervention to support TB treatment adherence. Tuberc. Res. Treat. 2013, 1–12. [Google Scholar] [CrossRef]
- Imam, F.; Sharma, M.; Obaid Al-Harbi, N.; Rashid Khan, M.; Qamar, W.; Iqbal, M.; Daud Ali, M.; Ali, N.; Khalid Anwar, M. The possible impact of socioeconomic, income, and educational status on adverse effects of drug and their therapeutic episodes in patients targeted with a combination of tuberculosis interventions. Saudi J Biol Sci. 2021, 28, 2041–2048. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- World Health Organization. Global Tuberculosis Report, 2018. Available online: https://www.who.int/publications/i/item/9789240062006.
- Nardell, E.A. Transmission and Institutional Infection Control of Tuberculosis. Cold Spring Harb Perspect Med. 2015, 6, a018192. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Coleman, M.; Martinez, L.; Theron, G. ; Wood; R.; Marais, B. Mycobacterium tuberculosis Transmission in High-Incidence Settings-New Paradigms and Insights. Pathogens, 2022; 11, 1228. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.P.; Oeltmann, J.E.; Hill, A.N.; Tobias, J.L.; Boyd, R.; Click, E.S.; Finlay, A.; Mondongo, C.; Zetola, N.M.; Moonan, P.K. Characterizing tuberculosis transmission dynamics in high-burden urban and rural settings. Sci Rep. 2022, 12, 6780. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Verver, S.; Warren, R.M.; Munch, Z.; Vynnycky, E.; van Helden, P.D.; Richardsonl, M.; van der Spuy, G.D.; Enarsonk, D.A.; Borgdorff, M.W.; Behr, M.A.; Beyers, N. Transmission of tuberculosis in a high incidence urban community in South Africa. Int J Epidemiol. 2004, 33, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Patterson, B.; Morrow, C.D.; Kohls, D.; Deignan, C.; Ginsburg, S.; Wood, R. Mapping sites of high TB transmission risk: integrating the shared air and social behaviour of TB cases and adolescents in a South African township. Sci. Total Environ. 2017, 583, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Kootbodien, T.; Monyane, M.; Mothibe, N. The impact of socio-economic factors on tuberculosis treatment outcomes in South Africa: A retrospective cohort study. BMC Public Health 2018, 18, 1234. [Google Scholar] [CrossRef]
- Youakin, A.; Smith, J.; Johnson, L. The impact of socio-economic factors on tuberculosis treatment outcomes: A systematic review. Int. J. Tuberc. Lung Dis. 2016, 20, 567–574. [Google Scholar] [CrossRef]
- Soh, A.Z.; Chee, C.B.E.; Wang, Y.T.; et al. Alcohol drinking and cigarette smoking in relation to risk of active tuberculosis: prospective cohort study. BMJ Open Resp Res 2017, 4, e000247. [Google Scholar] [CrossRef]
- Alavi-Naini, R.; Sharifi-Mood, B.; Metanat, M. Association between tuberculosis and smoking. Int. J. High Risk Behav. Addict. 2012, 1, 71. [Google Scholar] [CrossRef]
- Mukherjee, A.; Saha, I.; Sarkar, A.; Chowdhury, R. Gender differences in notification rates, clinical forms and treatment outcome of tuberculosis patients under the RNTCP. Lung India 2012, 29, 120–122. [Google Scholar] [CrossRef]
- Deshmukh, S.; Sane, M.; Gaikwad, S.; Sahasrabudhe, T.; Barthwal, M.; Lokhande, R.; Raskar, S.; Kagal, A.; Dharmshale, S.; Pradhan, N.; Gupte, A.; Alfarisi, O.; Gupta, A.; Dooley, K.E.; Gupte, N.; Golub, J.E.; Mave, V. Sex Differences in TB Clinical Presentation, Drug Exposure, and Treatment Outcomes in India. Chest. 2023, 163, 778–789. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Murphy, M.E.; Wills, G.H.; Murthy, S.; et al. Gender differences in tuberculosis treatment outcomes: a post hoc analysis of the REMoxTB study. BMC Med. 2018, 16, 189. [Google Scholar] [CrossRef]
- Msoka, E.F.; Orina, F.; Sanga, E.S.; Miheso, B.; Mwanyonga, S.; Meme, H.; Kiula, K.; Liyoyo, A.; Mwebaza, I.; Aturinde, A.; Joloba, M.; Mmbaga, B.; Amukoye, E.; Ntinginya, N.E.; Gillespie, S.H.; Sabiitim, W. Qualitative assessment of the impact of socioeconomic and cultural barriers on uptake and utilisation of tuberculosis diagnostic and treatment tools in East Africa: a cross-sectional study. BMJ Open 2021, 11, e050911. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Baker, M.A.; et al. The role of education in the prevention of tuberculosis: a systematic review. Int. J. Tuberc. Lung Dis. 2018, 22, 1–10. [Google Scholar]
- Lönnroth, K.; Raviglione, M. Global tuberculosis control: The need for new metrics. Lancet 2016, 387, 1127–1129. [Google Scholar] [CrossRef]
- World Health Organization. Global Tuberculosis Report, 2022. Available online: https://www.who.int/publications/i/item/9789240062006.
- Harrisson, L.; Smith, J. Socio-economic determinants of tuberculosis treatment outcomes: A systematic review. Int. J. Tuberc. Lung Dis. 2020, 24, 600–610. [Google Scholar] [CrossRef]
- Osei, D.; et al. Barriers to tuberculosis treatment adherence in low-income communities: A qualitative study. BMC Public Health 2019, 19, 1234. [Google Scholar] [CrossRef]
- Menzies, D.; et al. The impact of poverty on tuberculosis treatment outcomes: A systematic review. Int. J. Tuberc. Lung Dis. 2012, 16, 367–374. [Google Scholar] [CrossRef]
- Morshed, M.; et al. The impact of malnutrition on tuberculosis susceptibility: A systematic review. J. Infect. Dis. 2020, 221, 456–467. [Google Scholar] [CrossRef]
- Khan, M.; Ali, S.; Rahman, A. Socio-economic determinants of tuberculosis treatment adherence: A cross-sectional study in urban settings. Int. J. Tuberc. Lung Dis. 2021, 25, 567–574. [Google Scholar] [CrossRef]
- Dhedhi, S.; Kumar, A.; Sharma, R. Nutritional status and its impact on drug-resistant tuberculosis: A study from a tertiary care center. J. Clin. Tuberc. Other Mycobact. Dis. 2022, 25, 100–110. [Google Scholar] [CrossRef]
- O’Donnell, M.; et al. The impact of socio-economic factors on tuberculosis treatment adherence: A systematic review. Int. J. Tuberc. Lung Dis. 2016, 20, 1–10. [Google Scholar] [CrossRef]
- Chin, A.; Rylance, J.; Makumbirofa, S.; Meffert, S.M.; Vu, T.A.; Clayton, J.M.; Metcalfe, J. Chronic lung disease in adult recurrent tuberculosis survivors in Zimbabwe: a cohort study. Int. J. Tuberc. Lung Dis. 2019, 23, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Havir, E.; Smith, J.; Johnson, L. The impact of socio-economic factors on tuberculosis treatment outcomes: A systematic review. J. Infect. Dis. 2019, 220, 345–356. [Google Scholar] [CrossRef]
- Hassan, A.R.; Mousnad, M.A. Systematic review of the impact of food provision on adherence to the tuberculosis treatment. Health Prim. Care 2019, 3. [Google Scholar] [CrossRef]
- WHO Treatment Guidelines for Isoniazid-Resistant Tuberculosis: Supplement to the WHO Treatment Guidelines for Drug-Resistant Tuberculosis; World Health Organization: Geneva, Switzerland, 2018.
- Wu, S.; Litvinjenko, S.; Magwood, O.; Wei, X. Defining tuberculosis vulnerability based on an adapted social determinants of health framework: a narrative review. Global Public Health 2023, 18, 2221729. [Google Scholar] [CrossRef] [PubMed]
- Castro, D.; Maciel, E.; Sadahiro, M.; Pinto, R.; Albuquerque, B.; Braga, J. Tuberculosis incidence inequalities and its social determinants in manaus from 2007 to 2016. Int. J. Equity Health 2018, 17, 187. [Google Scholar] [CrossRef] [PubMed]
- Putra, K.; Toonsiri, C. Factors related to the successful treatment of tuberculosis: a literature review. Belitung Nurs. J. 2019, 5, 136–146. [Google Scholar] [CrossRef]
- Munro, S.A.; Lewin, S.A.; Smith, H.J.; Engel, M.E.; Fretheim, A.; Volmink, J. Patient adherence to tuberculosis treatment: a systematic review of qualitative research. PLoS Med. 2007, 4, e238. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hussain, H.; Mori, A.T.; Khan, A.J.; et al. The cost-effectiveness of incentive-based active case finding for tuberculosis (TB) control in the private sector Karachi, Pakistan. BMC Health Serv. Res. 2019, 19, 690. [Google Scholar] [CrossRef]
- Jaleta, K.; Gizachew, M.; Gelaw, B.; Tesfa, H.; Getaneh, A.; Biadgo, B. Rifampicin-resistant <em>mycobacterium tuberculosis</em> among tuberculosis-presumptive cases at university of gondar hospital, northwest ethiopia. Infect. Drug Resist. 2017, 10, 185–192. [Google Scholar] [CrossRef]
- Sharma, A.; Hill, A.; Kurbatova, E.; Walt, M.; Kvasnovsky, C.; Tupasi, T.; Cegielski, P. Estimating the future burden of multidrug-resistant and extensively drug-resistant tuberculosis in india, the philippines, russia, and south africa: a mathematical modelling study. Lancet Infect. Dis. 2017, 17, 707–715. [Google Scholar] [CrossRef]
- Misyatin, D.; Soeroto, A.; Ferdian, F. Distribution of rifampicin-resistant tuberculosis patients based on presumptive drug-resistant tuberculosis criteria at dr. hasan sadikin hospital 2016–2019. Althea Med. J. 2022, 9. [Google Scholar] [CrossRef]
- Baéz-Saldaña, R.; Delgado-Sánchez, G.; García-García, L.; Cruz-Hervert, L.; Montesinos-Castillo, M.; Ferreyra-Reyes, L.; Ponce-de-León, A. Isoniazid mono-resistant tuberculosis: impact on treatment outcome and survival of pulmonary tuberculosis patients in Southern Mexico 1995-2010. Plos One 2016, 11, e0168955. [Google Scholar] [CrossRef] [PubMed]
- Edwards, B.; Edwards, J.; Cooper, R.; Kunimoto, D.; Somayaji, R.; Fisher, D. Incidence, treatment, and outcomes of isoniazid mono-resistant mycobacterium tuberculosis infections in alberta, canada from 2007-2017. Plos One 2020, 15, e0229691. [Google Scholar] [CrossRef] [PubMed]
- Senbeto, M.; Tadesse, S.; Tadesse, T.; et al. Appropriate health-seeking behavior and associated factors among people who had cough for at least two weeks in northwest Ethiopia: a population-based cross-sectional study. BMC Public Health 2013, 13, 1222. [Google Scholar] [CrossRef] [PubMed]
- Zelner, J.L.; Murray, M.B.; Becerra, M.C.; Galea, J.; Lecca, L.; Calderon, R.; Yataco, R.; Contreras, C.; Zhang, Z.; Manjourides, J.; Grenfell, B.T.; Cohen, T. Identifying Hotspots of Multidrug-Resistant Tuberculosis Transmission Using Spatial and Molecular Genetic Data. J. Infect. Dis. 2016, 213, 287–94. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- MacNeil, A.; Glaziou, P.; Sismanidis, C.; Date, A.; Maloney, S.; Floyd, K. Global Epidemiology of Tuberculosis and Progress Toward Meeting Global Targets—Worldwide, 2018. MMWR Morb Mortal Wkly Rep 2018, 69, 281–285. [Google Scholar] [CrossRef]
- Ndjeka, N.; Campbell, J.R.; Meintjes, G.; Maartens, G.; Schaaf, H.S.; Hughes, J.; Padanilam, X.; Reuter, A.; Romero, R.; Ismail, F.; Enwerem, M.; Ferreira, H.; Conradie, F.; Naidoo, K.; Menzies, D. Treatment outcomes 24 months after initiating short, all-oral bedaquiline-containing or injectable-containing rifampicin-resistant tuberculosis treatment regimens in South Africa: a retrospective cohort study. Lancet Infect Dis. 2022, 22, 1042–1051. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cioboata, R.; Biciusca, V.; Olteanu, M.; Vasile, C.M. COVID-19 and Tuberculosis: Unveiling the Dual Threat and Shared Solutions Perspective. J Clin Med. 2023, 12, 4784. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Muhammad Dayyab, F.; Iliyasu, G.; Garba Ahmad, B.; Aliyu Umar, I.; Musa Shuaib, N.; Bajehson, M.; Muhammad Daiyab, I.; Akpala, O.; Remilekun, O.; Garba Habib, A. For Kano TB Concilium Experts: Emerging threat of drug-resistant tuberculosis and trends in the era of COVID-19: A descriptive study from northwestern Nigeria. J Clin Tuberc Other Mycobact Dis 2022, 28, 100319. [Google Scholar] [CrossRef] [PubMed]
- Aznar, M.L.; Espinosa-Pereiro, J.; Saborit, N.; Jové, N.; Martinez, F.S.; Pérez-Recio, S.; Vitoria, A.; Sanjoaquin, I.; Gallardo, E.; Llenas-García, J.; Pomar, V. Impact of the COVID-19 pandemic on tuberculosis management in Spain. Int. J. Infect. Dis. 2021, 108, 300–305. [Google Scholar] [CrossRef]
- Zhu, Q.; Liu, J. A united model for diagnosing pulmonary tuberculosis with random forest and artificial neural network. Front. Genet. 2023, 14, 1094099. [Google Scholar] [CrossRef] [PubMed]
- Kouchaki, S.; Yang, Y.; Lachapelle, A.; Walker, T.M.; Walker, A.S.; CRyPTIC Consortium; Peto TEA.; Crook, D.W.; Clifton, D.A. Multi-Label Random Forest Model for Tuberculosis Drug Resistance Classification and Mutation Ranking. Front. Microbiol. 2020, 11, 667. 2020, 11, 667. [CrossRef] [PubMed]
- Bedaso, M.H.; Kalil, F.S. Trends of Drug Resistance Tuberculosis from 2014 to 2018, Bale Zone, Oromia Region, Ethiopia. Infect Drug Resist. 2021, 14, 2073–2078. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rodrigues, M.M.S.; Barreto-Duarte, B.; Vinhaes, C.L.; Araújo-Pereira, M.; Fukutani, E.R.; Bergamaschi, K.B.; Kristki, A.; Cordeiro-Santos, M.; Rolla, V.C.; Sterling, T.R.; Queiroz, A.T.L.; Andrade, B.B. Machine learning algorithms using national registry data to predict loss to follow- up during tuberculosis treatment. BMC Public Health. 2024, 24, 1385. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Proportions of DR-TB types within total DR-TB cases.
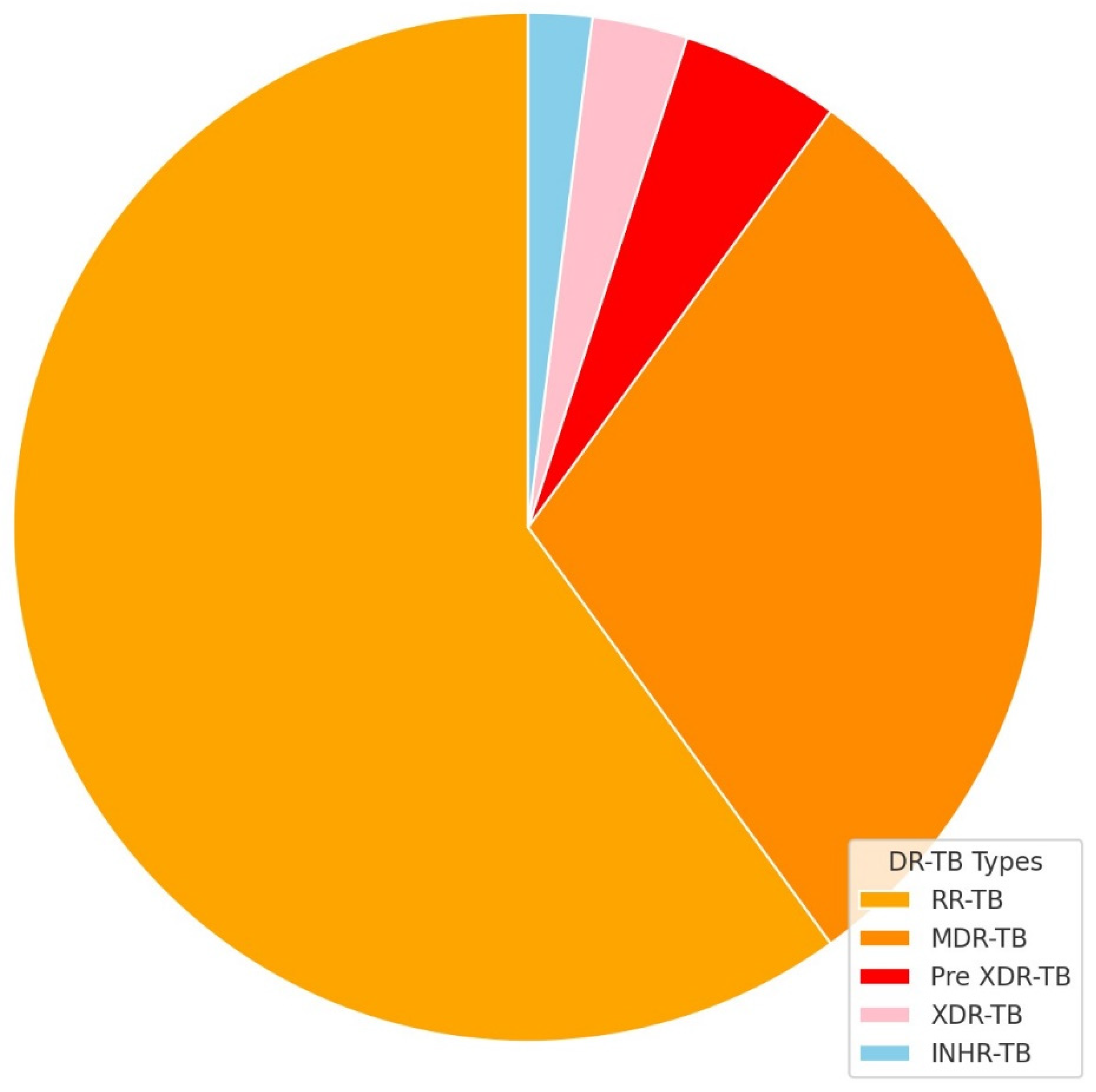
Figure 2.
Age distribution by DR-TB type.
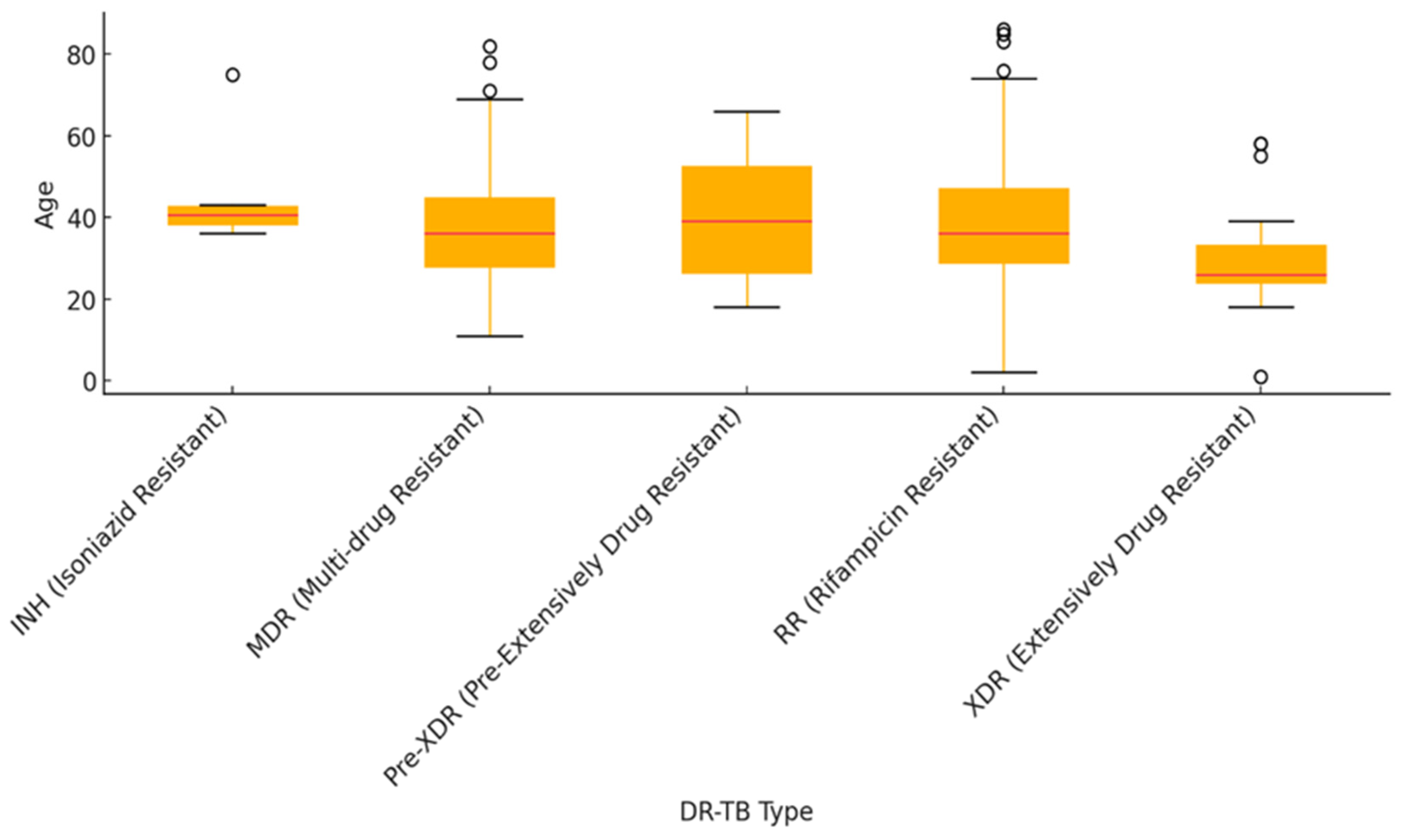
Figure 3.
Stratified previous drug history by DR-TB type. PT1 (previously treated once), PT2 (previously treated twice), UNK (unknown), NR (not written).
Figure 3.
Stratified previous drug history by DR-TB type. PT1 (previously treated once), PT2 (previously treated twice), UNK (unknown), NR (not written).
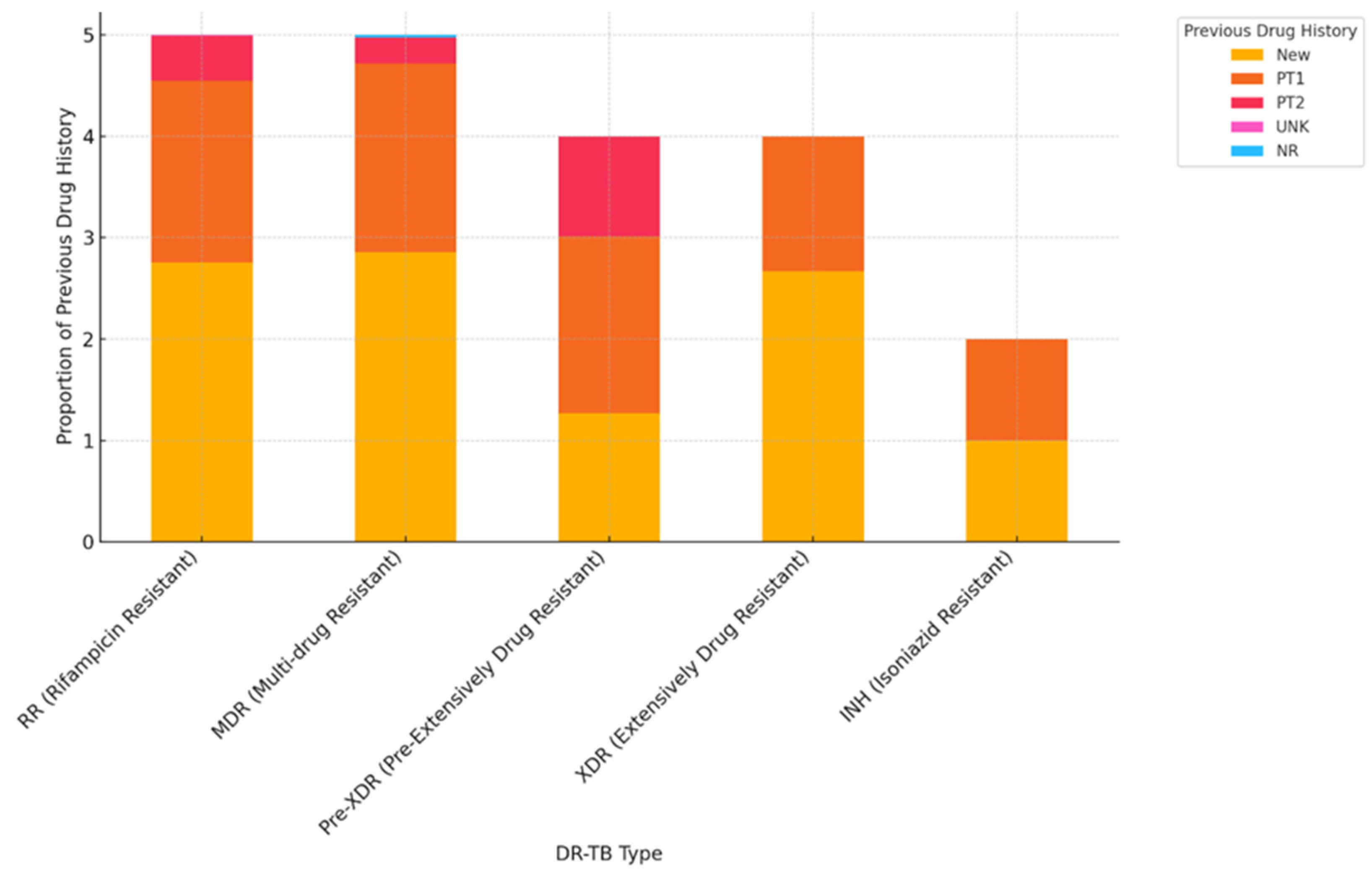
Figure 4.
DR-TB hot spots in O.R. Tambo District Municipality.
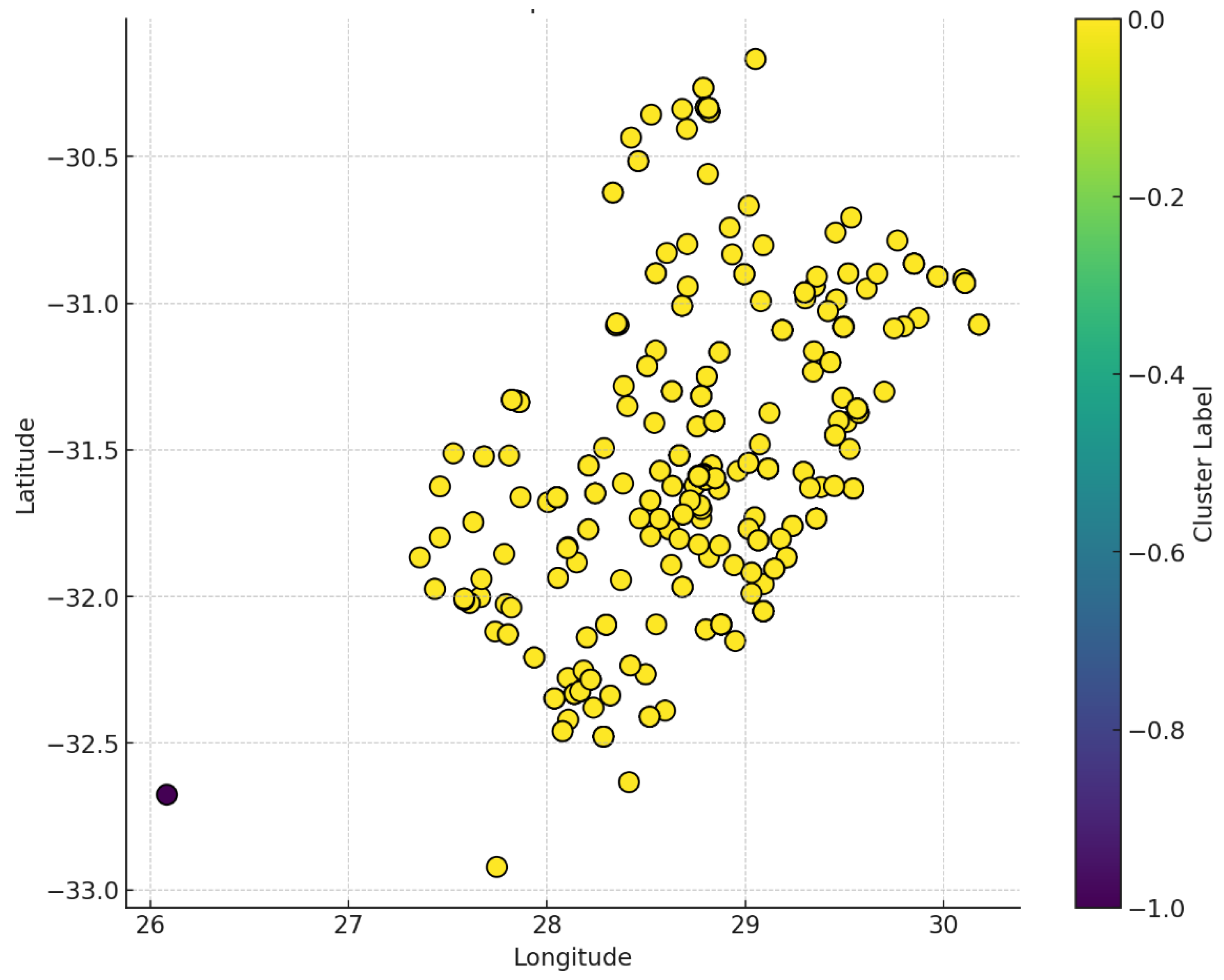
Figure 5.
Heat map of DR-TB hot spots by urban and rural classification.
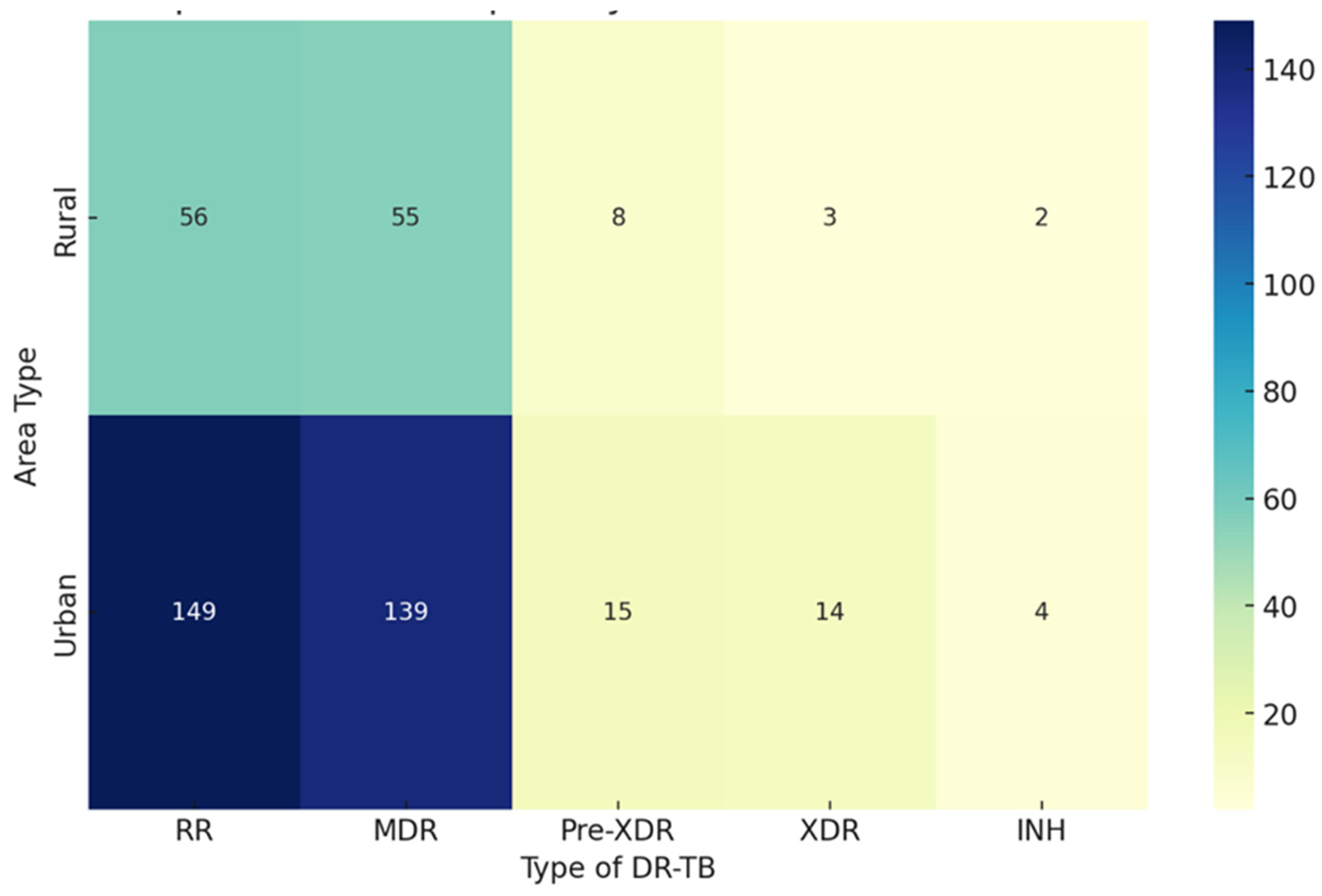
Figure 6.
Temporal trends of DR-TB cases in hot spot.
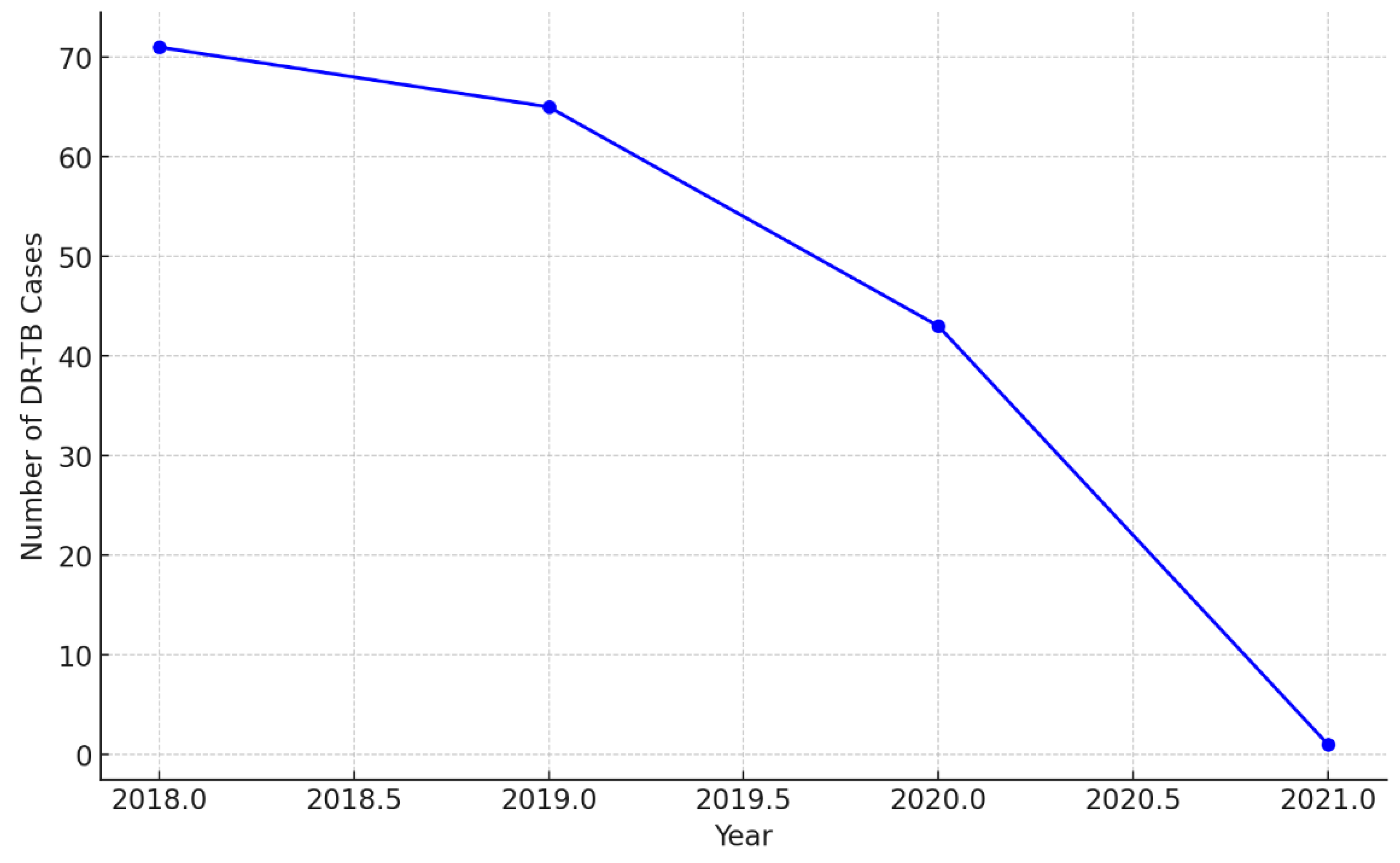
Figure 7.
Predicted future DR-TB trends in hot spot areas.
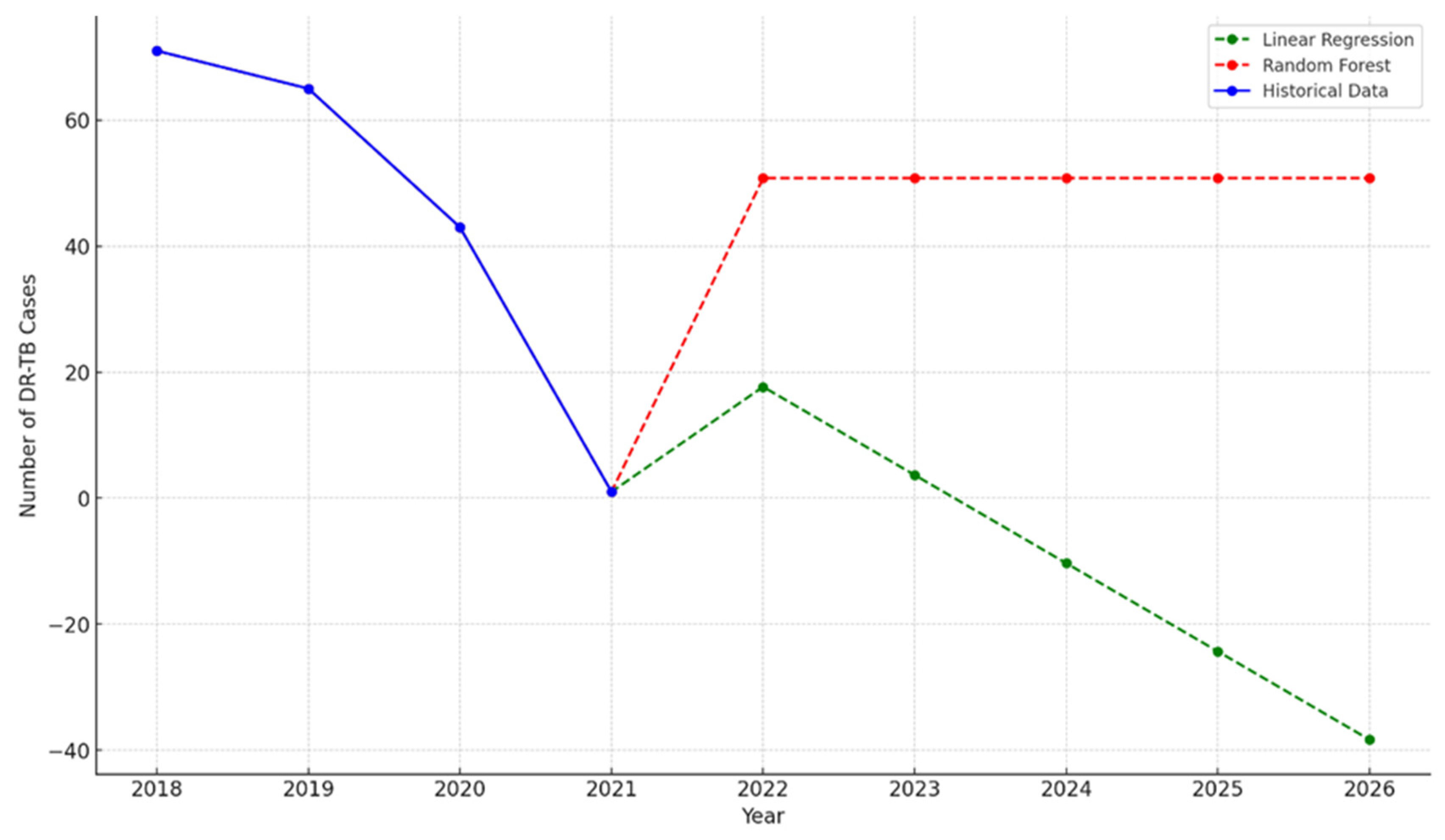

Table 1.
Baseline characteristics of DR-TB patients in O.R. Tambo district compared to underlying general population characteristics.
Table 1.
Baseline characteristics of DR-TB patients in O.R. Tambo district compared to underlying general population characteristics.
| Characteristics of Interest |
Enrolled DR-TB Patients (n=456) (%) |
O.R. Tambo population (n=1 514 306) % | Difference % | [95% CI] | P-value |
|---|---|---|---|---|---|
| Demographic characteristics |
|||||
|
Age (years) <20 20-49 50-59 >60 |
30.0 50.0 15.0 5.0 |
52.0 36.0 5.0 7.0 |
-22.0 14.0 10.0 -2.0 |
[-22.04; -21.96] [13.96; 14.04] [9.97; 10.03] [-2.02; -1.98] |
<0.0001 <0.0001 <0.0001 0.0597 |
|
Gender Female |
44.04 |
53.3 |
-9.26 |
[-9.30; -9.21] |
0.000035 |
|
Level of education No Education Primary Education Secondary Education Tertiary Education |
19.78 22.92 47.87 9.21 |
10 30 50 10 |
+9.78 -7.08 -2.13 -0.79 |
[9.75%, 9.81%] [-7.12%, -7.04%] [-2.17%, -2.09%] [-0.82%, -0.76%] |
<0.0001 0.00033 0.3407 0.5488 |
|
Income category No Income Salary or Wages Casual UIF Disability Grant |
56.85 19.15 15.96 1.54 3.08 |
40 25 20 5 5 |
+16.85 -5.85 -4.04 -3.46 -1.92 |
[16.81%, 16.89%] [-5.89%, -5.81%] [-4.07%, -4.01%] [-3.48%, -3.44%] [-1.94%, -1.90%] |
<0.0001 0.0016 0.0187 0.00036 0.0292 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



