
Submitted:
23 September 2024
Posted:
24 September 2024
You are already at the latest version
Abstract
Background: Anterior cervical discectomy and fusion (ACDF) is a common procedure for cervical radiculopathy and myelopathy. Severe obesity (BMI ≥40 or BMI ≥35 with comorbidities) is associ-ated with increased perioperative risks. This study examines the impact of severe obesity on out-comes in patients undergoing single-level ACDF.
Methods :Data from the Nationwide Inpatient Sample (2016-2019) were analyzed, including 85,585 patients who underwent single-level ACDF. Patients were classified as severely obese (n = 4,935) or non-obese (n = 80,650). Outcomes such as length of stay, complications, and in-hospital mortali-ty were compared using SPSS and MATLAB, with a significance level of p < 0.05.
Results: Severely obese patients were younger (54 vs. 55.7 years, p < 0.001) and had more comor-bidities like type 2 diabetes (38% vs. 17.8%, p < 0.001) and obstructive sleep apnea (31.1% vs. 9.5%, p < 0.001). They experienced longer hospital stays (1.92 vs. 1.65 days, p < 0.001) but similar in-hospital mortality (0.1%, p = 0.506). Severe obesity was linked to higher odds of complications, the risk of developing dehiscence was 8.2 times higher in severely obese patients. Respiratory failure had an odds ratio of 6.5, while myocardial infarction showed an odds ratio of 5.5. Horner syn-drome was 4.7 times more likely to occur, and pulmonary edema had an odds ratio of 4.5. Dural tear risk was also significantly elevated, with an odds ratio of 4.1.The risk of developing acute kid-ney injury were 2.6 times higher, while the risk of pulmonary embolism was 2.5 times higher. Dysphonia was also more common in severely obese patients, with an odds ratio of 2.2.
Conclusion:
Severe obesity is associated with higher complication rates and longer hospital stays following ACDF. Tailored perioperative management is essential to mitigate risks and improve outcomes in this high-risk population.
Keywords:
Anterior Cervical Discectomy
; Severe Obesity
; BMI
; Postoperative Complications
; ACDF
1. Introduction
Anterior cervical discectomy and fusion (ACDF) remains the definitive treatment for cervical radiculopathy and myelopathy, particularly in patients with cervical spondylosis (1-3). With the global population aging rapidly, the incidence of spondylosis—and the corresponding need for ACDF—is expected to surge. ACDF is primarily indicated when conservative management fails to alleviate symptoms in degenerative cervical spine disorders, including spondylosis, disc herniations, fractures, and spinal tumors. Its high efficacy and favorable safety profile have cemented it as one of the most frequently performed procedures in addressing cervical spine degeneration.
Body mass index (BMI) is a well-established risk factor for increased complications and suboptimal outcomes after ACDF (4,5). Patients with elevated BMI, coupled with characteristics such as larger neck circumference and shorter neck length, are prone to longer operative times, greater blood loss, and a heightened likelihood of postoperative complications (6). These anatomical and physiological challenges further complicate the procedure, impacting both intraoperative management and postoperative recovery. In patients with severe obesity, however, ACDF poses specific challenges. The increased subcutaneous fat deposition and broader anatomical corridors introduce greater complexity in accessing the cervical spine. This often necessitates more forceful and prolonged retraction of adjacent structures such as the longus colli muscles, esophagus, and trachea, which can elevate the risk of complications. These include localized edema, tissue ischemia, longer operative durations, and increased intraoperative blood loss.
Obesity has been consistently associated with higher rates of perioperative complications and poorer outcomes in surgical procedures, including ACDF (7-10). According to WHO, obesity is categorized by BMI of ≥30.0, with further classifications as class I (30.0–34.9), class II (35.0–39.9), and class III (≥40.0). The prevalence of obesity in the United States continues to rise, placing this population at a significantly greater risk of developing degenerative spinal disorders across all levels of the spine, in comparison to individuals with a healthy BMI (11). Patients with a BMI over 30 have been identified as being at a heightened risk for developing complications such as dysphagia, neurological issues, respiratory complications, hematologic disorders, pulmonary embolism (PE), and durotomy.
A deeper insight into the impact of obesity on inpatient complications after ACDF could enhance patient selection, preoperative risk stratification, and patient counseling, potentially mitigating avoidable perioperative complications. This study seeks to evaluate the prevalence of obesity among ACDF patients and to assess its influence on postoperative inpatient outcomes, with the goal of improving clinical management strategies for this high-risk population.
Research Questions
Our goal is to investigate the correlation between severe obesity (BMI ≥40 or BMI ≥35 with obesity-related comorbidities) and the outcomes of patients undergoing single-level ACDF
2. Methods
Research Questions
This study utilized a comprehensive dataset extracted from the Nationwide Inpatient Sample (NIS), the largest publicly available all-payer inpatient care database in the United States. The dataset included a total of 85,585 patients who underwent single-level Anterior Cervical Discectomy and Fusion (ACDF) between 2016 and 2019.
Study Period and Data Source
The study period spanned from January 1st, 2016, to December 31st, 2019. The NIS, a core component of the Healthcare Cost and Utilization Project (HCUP), captures 20% of inpatient stays from HCUP-associated hospitals, amounting to approximately seven million unweighted enrollments annually.
Patient Identification and Obesity Definition
Patients undergoing single-level ACDF were identified using specific ICD-10 codes. Severe obesity was defined by the ICD-10 code E66.01, indicating patients with a body mass index (BMI) of 40 or higher, or a BMI of 35 or higher with obesity-related health conditions (e.g., diabetes, hypertension). In total, 4,935 patients were identified as having severe obesity, while 80,650 patients were classified as non-severe or non-obese.
Statistical Analyses
Statistical analyses were performed using SPSS 26 and MATLAB 2024. Crosstabs and independent sample t-tests were conducted to compare outcomes between severely obese and non-obese patients undergoing single-level ACDF. A significance level of p < 0.05 was applied..
Comorbidity and Outcome Identification
Comorbidities were identified using ICD-10 codes and included conditions such as diabetes, hypertension, and chronic respiratory disease. Clinical outcomes were also extracted using ICD-10 codes and included in-hospital mortality, length of stay, complications, and overall hospitalization costs. Complications analyzed included dysphagia, blood loss anemia, cervical spinal cord injury, urinary tract infection (UTI), acute renal failure, pneumonia, blood transfusion requirement, venous thromboembolism, pulmonary edema, ileus, sepsis, and pulmonary embolism.
Ethical Considerations
The study was conducted under exempt status granted by the institutional review board due to the de-identified nature of the data. No informed consent was required.
3. Results
Comparison of Key Demographic and Hospital Characteristics
Table 1 presents the demographic and hospital characteristics of patients undergoing single-level ACDF surgery, comparing those with and without severe obesity.
Severely obese patients were younger (54 vs. 55.7 years, p<0.001) and had a higher percentage of females (57.1% vs. 51.3%, p<0.001). Medicare coverage was more common among severely obese patients (35% vs. 33.8%, p<0.001). A greater proportion of surgeries for severely obese patients occurred in rural hospitals (75.6% vs. 72.9%, p<0.001).
Comparison of Comorbidities Between Severely Obese and Non-Obese Patients
Table 2 shows the comorbidities associated with patients undergoing single-level ACDF surgery, comparing those with and without severe obesity.Severely obese patients were significantly more likely to have type 2 diabetes mellitus (38% vs. 17.8%, p<0.001), obstructive sleep apnea (31.1% vs. 9.5%, p<0.001), and chronic kidney disease (6.4% vs. 3.6%, p<0.001). They also had a higher prevalence of mental disorders (45.7% vs. 40.4%, p<0.001) and thyroid disorders (15.4% vs. 11.7%, p<0.001). However, they were less likely to have hypertension (43.7% vs. 56.3%, p<0.001) and dyslipidemia (30% vs. 70%, p<0.001). Other notable differences include higher rates of chronic lung disease (11.4% vs. 7.8%, p<0.001) and chronic anemia (3.5% vs. 2.3%, p<0.001) in severely obese patients.
Comparison of Hospitalization Outcomes Between Severely Obese and Non-Obese Patients
Table 3 shows the hospitalization outcomes for patients undergoing single-level ACDF surgery. There was no significant difference in in-hospital mortality between severely obese and non-obese patients (both 0.1%, p=0.506). However, the length of stay was significantly longer for severely obese patients (1.92 days vs. 1.65 days, p<0.001). Total hospital charges were similar between the two groups, with no significant difference ($66,655 vs. $66,913, p=0.702).
Postoperative Complications in Severely Obese vs. Non-Obese Patients
Table 4 highlights the postoperative complications that did not differ significantly between severely obese and non-obese patients undergoing single-level ACDF surgery. The rates of venous thromboembolism (0.1% vs. 0.1%, p=0.452), pneumonia (0.3% vs. 0.2%, p=0.446), and dysphagia (4.9% vs. 5.1%, p=0.383) were similar between the two groups. Other complications such as cardiac arrhythmias, urinary tract infections, and cerebrospinal fluid leaks also showed no statistically significant differences.
Postoperative Complications with Significantly Higher Odds in Severely Obese Patients
Figure 1 presents the odds ratios (OR) and confidence intervals (CI) for various postoperative complications in severely obese patients after single-level ACDF surgery. The OR provides a measure of the likelihood that a complication occurs in severely obese patients compared to non-obese patients. An OR greater than 1 indicates a higher risk of complication in the severely obese group.
- Dehiscence had the highest OR at 8.2 (95% CI: 2.8–23.9, p<0.001.
- Respiratory failure had an OR of 6.5 (95% CI: 3.1–13.6, p<0.001), showing a significantly increased risk for severely obese patients.
- Myocardial infarction had an OR of 5.5 (95% CI: 2.0–15.0, p<0.001), indicating a markedly higher risk in the severely obese group.
- Horner syndrome had an OR of 4.7 (95% CI: 2.3–9.5, p<0.001).
- Pulmonary edema had an OR of 4.5 (95% CI: 2.5–7.9, p<0.001).
- Dural tear had an OR of 4.1 (95% CI: 2.0–8.2, p<0.001).
- Acute kidney injury had an OR of 2.6 (95% CI: 2.0–3.3, p<0.001).
- Pulmonary embolism had an OR of 2.5 (95% CI: 1.3–4.9, p=0.005).
- Dysphonia had an OR of 2.2 (95% CI: 1.6–3.1, p<0.001).
These findings indicate that severely obese patients are at significantly higher risk for multiple complications following single-level ACDF surgery compared to non-obese patients.
4. Discussion
ACDF is the most commonly performed procedure on the cervical spine, with its incidence tripling over the past two decades. Despite its reputation as a safe and effective intervention, ACDF is not without risks, and significant complications can still arise (1,2,12,14-16). Advances in surgical techniques and innovations in interbody fusion devices and plating systems have contributed to reducing postoperative morbidity. However, surgeons must remain vigilant, recognizing potential complications, fully informing patients of the associated risks, and implementing appropriate management strategies. ACDF remains the gold standard for addressing cervical radiculopathy and myelopathy, particularly when dealing with focal anterior compression of the nerve roots and/or spinal cord, often caused by cervical spondylosis.
Impact of BMI on ACDF Outcomes
BMI is a recognized risk factor for increased complications and poorer clinical outcomes following ACDF. Elevated BMI, often associated with anatomical challenges such as increased neck circumference and reduced neck length, predisposes patients to longer operative times, greater intraoperative blood loss, and a significantly higher rate of postoperative complications. (1,4,12)
Study Findings: Demographics
Severely obese patients were generally younger and more likely to be female compared to non-obese patients. Interestingly, a larger proportion of surgeries for severely obese patients were performed in rural hospitals. This finding could reflect a geographic disparity in the distribution of obesity or surgical access in certain populations. Other studies, such as those by Roberto et al. (2), have similarly observed a higher prevalence of female patients among obese individuals, particularly those from lower socioeconomic backgrounds. These demographic differences suggest that gender, socioeconomic status, and geographic location may influence surgical outcomes differently across populations.
Study Findings: Comorbidities:
Severely obese patients in our study exhibited higher rates of significant comorbidities, including type 2 diabetes, obstructive sleep apnea, chronic kidney disease, and mental health disorders. However, we found surprisingly lower rates of hypertension and dyslipidemia in this population. The increased prevalence of conditions like diabetes and sleep apnea in severely obese patients aligns with findings from previous studies, which have linked higher BMI with a greater burden of metabolic and respiratory disorders (1,2). The presence of these comorbidities can complicate both the surgical procedure and the postoperative recovery process, underscoring the importance of thorough preoperative assessment and planning.
Study Findings: Postoperative Complications:
Severely obese patients were found to have significantly longer hospital stays compared to non-obese patients (1.92 days vs. 1.65 days), reflecting more complex postoperative courses. However, no significant differences were observed in in-hospital mortality rates or total hospital costs between the two groups. Interestingly, while conditions like venous thromboembolism, pneumonia, and dysphagia showed similar rates across BMI categories, severely obese patients had a markedly higher risk of certain serious complications, including wound dehiscence, respiratory failure, myocardial infarction, Horner syndrome, and pulmonary edema. In some cases, the odds ratios (ORs) indicated up to an 8-fold increased risk for these complications.
These findings emphasize the need for increased vigilance and tailored preoperative strategies for severely obese patients. It is essential to implement a multidisciplinary approach, involving anesthesiologists, nutritionists, and physical therapists, to optimize patient outcomes and mitigate the risks associated with obesity.
Limitations
While our study provides valuable insights, several limitations should be acknowledged due to the nature of database-driven research.
The NIS relies on administrative billing codes, which lack detailed clinical information such as comorbidity severity, preoperative status, or disc displacement. These missing variables are important for surgical decision-making and may affect the accuracy of the findings. Additionally, the retrospective nature of the NIS introduces potential inaccuracies and underreporting of complications (22-25).The study does not include detailed information on operative techniques or surgeon expertise, both of which can significantly impact outcomes. Without this data, it is difficult to fully assess the differences between patient groups based on surgical approach or skill. The lack of Patient-Reported Outcomes limits our understanding of long-term recovery and quality of life, as they provide essential information about postoperative satisfaction and functional outcomes. Future studies should incorporate PROs for a more complete evaluation of patient recovery.
5. Conclusions:
Severely obese patients were younger, predominantly female, and had higher rates of comorbidities, such as type 2 diabetes and sleep apnea. They also faced increased risks of complications like respiratory failure and myocardial infarction, though hospital costs remained similar to non-obese patients. The study's limitations include reliance on retrospective coding and lack of patient-reported outcomes. Despite this, it offers important insights into managing high-risk ACDF patients.
Funding
None.
Informed consent
Irrelevant.
Acknowledgments
Irrelevant.
Conflicts of Interest
None.
Ethical approval
The study was conducted under exempt status granted by the institutional review board, and the requirement for informed consent was waived due to the de-identified nature of the NIS dataset.
References
- Shao Jin Teo, William Yeo, Marcus Zhixing Ling, Poh Ling Fong, Chang Ming Guo, John Li Tat Chen, and Reuben Chee Cheong Soh. The Effect of Body Mass Index on Long-Term Patient-Reported Outcome Scores after Anterior Cervical Discectomy and Fusion in an Asian Population: A 2-Year Study. Asian Spine J. 2020 Sep 22. 15(4): 512–522. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8377209/. [CrossRef] [PubMed]
- Roberto, J. Perez-Roman, David McCarthy, Evan M. Luther, Julian G. Lugo-Pico, Roberto Leon-Correa, Wendy Gaztanaga, Karthik Madhavan, and Steven Vanni1. Effects of Body Mass Index on Perioperative Outcomes in Patients Undergoing Anterior Cervical Discectomy and Fusion Surgery. Neurospine. 2020 Nov 17. 18(1): 79–86. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8021846/. [PubMed]
- Kyung-Jin Song and Byeong-Yeol Choi. Current Concepts of Anterior Cervical Discectomy and Fusion: A Review of Literature. Asian Spine J. 2014 Aug 19. 8(4): 531–539. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4150000/. [CrossRef] [PubMed]
- Elliot, D.K. Cha, Conor P. Lynch, James M. Parrish, Nathaniel W. Jenkins, Shruthi Mohan, Cara E. Geoghegan, Caroline N. Jadczak, and Kern Singh. Recovery of Physical Function Based on Body Mass Index Following Anterior Cervical Discectomy and Fusion. Int J Spine Surg. 2022 Jan 25. 15(6): 1123–1132. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9469024/. [CrossRef] [PubMed]
- Qi, Min MD; Xu, Chen MD; Cao, Peng MD; Tian, Ye MD; Chen, Huajiang MD; Liu, Yang MD; Yuan, Wen MD. Does Obesity Affect Outcomes of Multilevel ACDF as a Treatment for Multilevel Cervical Spondylosis? Clinical Spine Surgery. December 2020. 33(10):p E460-E465. Available online: https://journals.lww.com/jspinaldisorders/abstract/2020/12000/does_obesity_affect_outcomes_of_multilevel_acdf_as.10.aspx. [CrossRef]
- Silky Chotai, J. Alex Sielatycki, Scott L. Parker, Ahilan Sivaganesan, Harrison L. Kay, David P. Stonko, Joseph B. Wick, Matthew J. McGirt, Clinton J. Devin. Effect of obesity on cost per quality-adjusted life years gained following anterior cervical discectomy and fusion in elective degenerative pathology. the spine journal. July 6, 2016. Available online: https://www.thespinejournalonline.com/article/S1529-9430(16)30281-9/abstract. [CrossRef]
- Evan, G. Gross, Nicholas M.B. Laskay, James Mooney, M. Chandler McLeod, Travis J. Atchley, Dagoberto Estevez-Ordonez, Jakub Godzik. Morbid Obesity Increases Length of Surgery in Elective Anterior Cervical Discectomy and Fusion Procedures but Not Readmission or Reoperation Rates: A Cohort Study. Orld neurosurgery. 2023 Mar 11 173:e830-e837. Available online: https://pubmed.ncbi.nlm.nih.gov/36914028/. [CrossRef] [PubMed]
- George THOMAS, Puneet GUPTA, Taimur CHAUDHRY, Neil D ALMEIDA, William WOODALL, John THOMAS, Bennett R. LEVY, Nyle C. ALMEIDA, Jonathan H SHERMAN. Impact of Obesity on Anterior Cervical Discectomy and Fusion (ACDF): Postoperative Morbidity and Mortality. Turk Neurosurg. 25.09.2023. Available online: https://pubmed.ncbi.nlm.nih.gov/37846533/. [CrossRef] [PubMed]
- Andrew, B. Andrew B. Koo , Aladine A. Elsamadicy , Margot Sarkozy , Wyatt B. David , Benjamin C. Reeves , Christopher S. Hong , Arianne Boylan , Maxwell Laurans , Luis Kolb. Independent Association of Obesity and Nonroutine Discharge Disposition After Elective Anterior Cervical Discectomy and Fusion for Cervical Spondylotic Myelopathy. World neurosurgery. 2021 May 18. 151:e950-e960. Available online: https://pubmed.ncbi.nlm.nih.gov/34020060/. [CrossRef] [PubMed]
- Eric Tecce, Advith Sarikonda, Adam Leibold, Daniyal Mansoor Ali, Sara Thalheimer, Ashmal Sami, Joshua Heller, Srinivas Prasad, Ashwini Sharan, James Harrop, Alexander Vaccaro, Ahilan Sivaganesan. Does Body Mass Index Influence Intraoperative Costs and Operative Times for Anterior Cervical Discectomy and Fusion? A Time-Driven Activity-Based Costing Analysis. World Neurosurg. 2024 Feb 19. 185:e563-e571. Available online: https://pubmed.ncbi.nlm.nih.gov/38382758/. [CrossRef] [PubMed]
- Taylor, D. Ottesen, Rohil Malpani, Anoop R. Galivanche, Cheryl K. Zogg, Arya G. Varthi, and Jonathan N. Grauer. Underweight patients are at just as much risk as super morbidly obese patients when undergoing anterior cervical spine surgery. Spine J. 2020 Mar 16. 20(7): 1085–1095. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7380546/. [CrossRef] [PubMed]
- Bryce A Basques, Jannat M Khan, Philip K Louie, Jeremy Mormol, Steven Heidt, Arya Varthi, Justin C Paul, Edward J Goldberg, Howard S An. Obesity does not impact clinical outcome but affects cervical sagittal alignment and adjacent segment degeneration in short term follow-up after an anterior cervical decompression and fusion. Spine J. 2019 Mar 23. 19(7):1146-1153. Available online: https://pubmed.ncbi.nlm.nih.gov/30914278/. [CrossRef] [PubMed]
- Shyam J Kurian, Waseem Wahood, Yagiz Ugur Yolcu, Elena Blaginykh, Anshit Goyal, Arjun S Sebastian, Mohamad Bydon. Risk Factors for Unplanned Readmissions Following Anterior Cervical Discectomy and Fusion and Posterior Lumbar Fusion Procedures: Comparison of Two National Databases. World Neurosurg. 2020 Aug 8. 143:e613-e630. Available online: https://pubmed.ncbi.nlm.nih.gov/32781151/. [CrossRef] [PubMed]
- Alba Scerrati, Antonino Germano', Nicola Montano, Jacopo Visani, Fabio Cacciola, Giovanni Raffa,Ilaria Ghetti,Fabrizio Pignotti, Michele Alessandro Cavallo, Alessandro Olivi, and Pasquale de Bonis. Factors affecting functional outcome after anterior cervical discectomy and fusion: A multicenter study. J Craniovertebr Junction Spine. 2021 Jun 10. 12(2): 144–148. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8214232/. [CrossRef] [PubMed]
- Scott C Robertson, Mason R Ashley. Complications of Anterior Cervical Discectomy and Fusion. Acta Neurochir Suppl. 2023:130:169-178. Available online: https://pubmed.ncbi.nlm.nih.gov/37548736/. [CrossRef] [PubMed]
- Kimia Khalatbari Kani, Felix S Chew. Anterior cervical discectomy and fusion: review and update for radiologists. Skeletal Radiol. 2017 Oct 23. 47(1):7-17. Available online: https://pubmed.ncbi.nlm.nih.gov/29058045/. [CrossRef] [PubMed]
- John A Sielatycki, Silky Chotai, Harrison Kay, David Stonko, Matthew McGirt, Clinton J Devin. Does Obesity Correlate With Worse Patient-Reported Outcomes Following Elective Anterior Cervical Discectomy and Fusion? Neurosurgery. 2016 Jul;79(1):69-74. Available online: https://pubmed.ncbi.nlm.nih.gov/27166659/. [CrossRef] [PubMed]
- Peter Y Joo, Justin R Zhu, Christopher Wilhelm, Kevin Tang, Wesley Day, Jay Moran, Jonathan N Grauer. Anterior Cervical Discectomy and Fusion Outcomes in Patients With and Without Bariatric Surgery-Weight Loss Does Make a Difference. Spine (Phila Pa 1976). 2023 Jan 24.2023 Mar 15;48(6):400-406. Available online: https://pubmed.ncbi.nlm.nih.gov/36735637/. [CrossRef] [PubMed]
- Tangyiheng Chen, Yujie Wang, Hong Zhou, Cheng Lin, Xuefeng Li, Huilin Yang, Yijie Liu, Weimin Jiang. Comparison of anterior cervical discectomy and fusion versus anterior cervical corpectomy and fusion in the treatment of localized ossification of the posterior longitudinal ligament. J Orthop Surg (Hong Kong). 2023 Jan-Apr;31(1):10225536231167704. Available online: https://pubmed.ncbi.nlm.nih.gov/36972216/. [CrossRef] [PubMed]
- Ankur S Narain, Fady Y Hijji, Brittany E Haws, Krishna T Kudaravalli, Kelly H Yom, Jothan Markowitz, Kern Singh. Impact of body mass index on surgical outcomes, narcotics consumption, and hospital costs following anterior cervical discectomy and fusion. J Neurosurg Spine. 2017 Dec 1. 28(2):160-166. Available online: https://pubmed.ncbi.nlm.nih.gov/29192877/. [CrossRef] [PubMed]
- Vladimir Katuch, Jan Banoci, Veronika Magocova, Martin Cmorej, Jana Katuchova, Kleanthia Efthymiou, Veronika Roskovicova. Postoperative complications associated with anterior cervical discectomy and three years follow-up. Bratisl Lek Listy. 2024;125(3):183-188. Available online: https://pubmed.ncbi.nlm.nih.gov/38385545/. [CrossRef] [PubMed]
- Maman, D.; Mahamid, A.; Finkel, B.; Gan-Or, H.; Fournier, L.; Berkovich, Y.; Behrbalk, E. Comparative evaluation of postoperative outcomes and expenditure between robotic and conventional single-level lumbar fusion surgery: A comprehensive analysis of nationwide inpatient sample data. Eur. Spine J. 2024, 33, 2637–2645. [Google Scholar] [CrossRef] [PubMed]
- Maman, D.; Laver, L.; Becker, R.; Mahamid, A.; Berkovich, Y. Robotic-assisted total knee arthroplasty reduces postoperative complications and length of stay without increased cost compared to navigation-guided techniques: A national analysis. Knee Surg. Sports Traumatol. Arthrosc.
- Maman, D.; Laver, L.; Becker, R.; Takrori, L.A.; Mahamid, A.; Finkel, B.; Gan-Or, H.; Yonai, Y.; Berkovich, Y. Trends and Epidemiology in Robotic-Assisted Total Knee Arthroplasty: Reduced Complications and Shorter Hospital Stays. Knee Surg. Sports Traumatol. Arthrosc.
- Maman, D.; Mahamid, A.; Yonai, Y.; Berkovich, Y. Comparing Complication Rates, Costs, and Length of Stay between Unicompartmental and Total Knee Arthroplasty: Insights from a Big Data Analysis Using the National Inpatient Sample Dataset. J. Clin. Med. 2024, 13, 3888. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Odds Ratios (OR) of Postoperative Complications in Severely Obese Patients Undergoing Single-Level ACDF Surgery compared to patients without severe obesity.
Figure 1.
Odds Ratios (OR) of Postoperative Complications in Severely Obese Patients Undergoing Single-Level ACDF Surgery compared to patients without severe obesity.
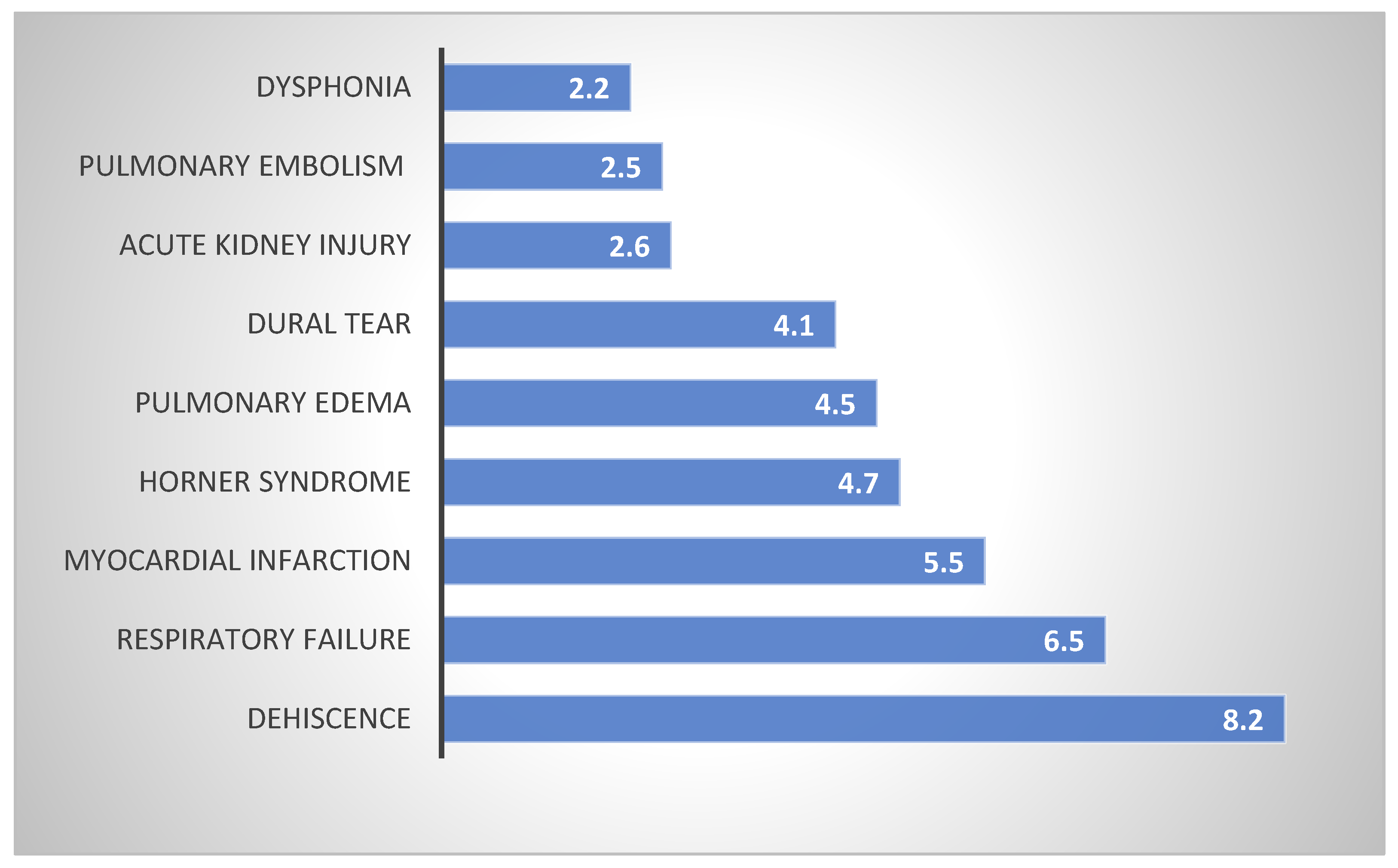

Table 1.
Demographic and Hospital Characteristics of Patients Undergoing Single-Level ACDF Surgery Stratified by Severe Obesity Status.
Table 1.
Demographic and Hospital Characteristics of Patients Undergoing Single-Level ACDF Surgery Stratified by Severe Obesity Status.
| Parameter | Without Severe Obesity (%) | Severe Obesity (%) | Significance |
|---|---|---|---|
| Total Surgeries | 80650 | 4935 | - |
| Average Age (y) | 55.7 | 54 | P<0.001 |
| Female (%) | 51.3 | 57.1 | P<0.001 |
| Primary expected payer - Medicare (%) | 33.8 | 35 | P<0.001 |
| Primary expected payer - Medicaid (%) | 10.6 | 12.2 | |
| Primary expected payer - private including HMO (%) | 44.5 | 44.8 | |
| Primary expected payer - self-pay (%) | 1.2 | 1.1 | |
| Primary expected payer - no charge (%) | 0.1 | 0.1 | |
| Primary expected payer - other (%) | 9.8 | 6.9 | |
| Status of hospital (STRATA) - Rural (%) | 72.9 | 75.6 | P<0.001 |
| Status of hospital (STRATA) - Urban nonteaching (%) | 23.3 | 20.7 | |
| Status of hospital (STRATA) - Urban teaching (%) | 3.8 | 3.7 |
Table 2.
Comorbidities in Patients Undergoing Single-Level ACDF Surgery by Severe Obesity Status.
| Prameter | Without Severe Obesity (%) | Severe Obesity (%) | Significance |
|---|---|---|---|
| Type 2 Diabetes Mellitus | 17.8 | 38 | P<0.001 |
| Diabetes Mellitus | 19.5 | 38.5 | P<0.001 |
| Mental Disorders | 40.4 | 45.7 | P<0.001 |
| Hypertension | 56.3 | 43.7 | P<0.001 |
| Dyslipidemia | 70 | 30 | P<0.001 |
| Obstructive Sleep Apnea | 9.5 | 31.1 | P<0.001 |
| Chronic Kidney Disease | 3.6 | 6.4 | P<0.001 |
| Chronic Lung Disease | 7.8 | 11.4 | P<0.001 |
| Thyroid Disorder | 11.7 | 15.4 | P<0.001 |
| Chronic Anemia | 2.3 | 3.5 | P<0.001 |
| Heart Failure | 0.1 | 0.3 | P<0.001 |
| Connective Tissue Disorder | 0.1 | 0.1 | P=0.621 |
| History of Myocardial Infarction | 2.9 | 3.1 | P=0.372 |
| Peripheral Vascular Disease | 1.3 | 1.4 | P=0.559 |
| Dementia | 0.2 | 0.2 | P=0.002 |
| Peptic Ulcer Disease | 0.3 | 0.3 | P=0.623 |
| IBD (Inflammatory Bowel Disease) | 0.5 | 0.3 | P=0.038 |
| Hemiplegia | 0.2 | 0.1 | P=0.085 |
| Neoplasms | 0.8 | 0.9 | P=0.576 |
| Neoplasms of Lymphoid/Hematopoietic | 0.3 | 0.3 | P=0.664 |
| Fibromyalgia | 3.8 | 4.4 | P=0.041 |
| Smoking | 1.2 | 0.7 | P=0.001 |
| Alcohol Abuse | 1.2 | 1 | P=0.279 |
| Osteoporosis | 2.3 | 2 | P=0.137 |
| Parkinson Disease | 0.5 | 0.3 | P=0.103 |
| Alzheimer Disease | 0.1 | 0.1 | P=0.097 |
Table 3.
Hospitalization Outcomes for Single-Level ACDF Surgery by Severe Obesity Status.
| Parameter | Without Severe Obesity (%) | Severe Obesity (%) | Significance |
|---|---|---|---|
| Died During Hospitalization (%) | 0.1 | 0.1 | P=0.506 |
| Length of stay (Days) | 1.65 | 1.92 | P<0.001 |
| Total charges ($) | 66913 | 66655 | P=0.702 |
Table 4.
Postoperative Complications with No Significant Difference Between Severe and Non-Severe Obesity Groups Following Single-Level ACDF Surgery.
Table 4.
Postoperative Complications with No Significant Difference Between Severe and Non-Severe Obesity Groups Following Single-Level ACDF Surgery.
| Parameter | Without Severe Obesity (%) | Severe Obesity (%) | Significance |
|---|---|---|---|
| Venous Thromboembolism | 0.1 | 0.1 | P=0.452 |
| Cardiac Arrhythmias | 2 | 2.3 | P=0.092 |
| Pneumonia | 0.2 | 0.3 | P=0.446 |
| Urinary Tract Infection (UTI) | 0.6 | 0.8 | P=0.059 |
| Blood Transfusion | 0.2 | 0.1 | P=0.347 |
| Blood Loss Anemia | 1.6 | 1.6 | P=0.907 |
| Dysphagia | 5.1 | 4.9 | P=0.383 |
| Brachial Plexus Injury | 0 | 0 | P=0.338 |
| Cerebrospinal Fluid Leak | 0.3 | 0.2 | P=0.483 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



