Submitted:
25 September 2024
Posted:
25 September 2024
You are already at the latest version
Abstract
Botulinum toxin (BoNT) is recognized as one of the most potent neurotoxins, with a lethal dose as low as 2 ng/kg, but it has also demonstrated significant therapeutic potential in controlled doses. Produced by the gram-positive anaerobic bacterium Clostridium botulinum, BoNT exists in eight distinct serotypes (A, B, C1, C2, D, E, F, and G) that disrupt neuronal transmission by targeting the soluble N-ethylmaleimide-sensitive factor attachment protein receptors (SNARE) complex at the neuromuscular junction, inhibiting the release of acetylcholine and inducing flaccid paralysis. While BoNT is notorious for its toxicity, it has been repurposed for medical use across various clinical indications. Following their approval by the Food and Drug Administration (FDA), these toxins have been associated with significant improvements in patient outcomes, particularly for individuals with specific neuromuscular disorders such as spasticity, dystonia, and cerebral palsy, as well as non-neuromuscular conditions like hyperhidrosis and cosmetic concerns. This broad spectrum of therapeutic applications that botulinum neurotoxins offer has made them an integral part of contemporary healthcare. Considering their growing importance, a detailed evaluation of their pharmacological properties, available formulations, and clinical uses is crucial. This review provides a comprehensive analysis of BoNT's molecular structure, mechanism of action, and therapeutic applications, with a particular emphasis on the most widely used BoNT-A formulations: OnabotulinumtoxinA (Botox), AbobotulinumtoxinA (Dysport), and IncobotulinumtoxinA (Xeomin). We examine their clinical efficacy, safety profiles, and differences in pharmacological properties to guide healthcare providers in selecting the most appropriate treatment for various conditions. Additionally, the review explores the challenges of BoNT therapy, such as immunogenicity and dosing considerations, while highlighting its evolving role in neurorehabilitation and conservative treatment strategies.
Keywords:
Botulinum Toxins
; Botulinum Toxins Type A
; Botox
INTRODUCTION
The botulinum toxin (BoNT) is a neurotoxic protein that has been identified as one of the most poisonous naturally occurring substances in the world with a lethal dose of 2 ng/kg [1]. If ingested, the onset of cranial nerve palsies, bulbar symptoms, and symmetric descending muscle weakness can develop within hours to days, depending on dose, source, and individual patient factors such as age and immunity status [2].
It is derived from the gram-positive, anaerobic bacilli Clostridium botulinum capable of germinating spores across favorable mediums and contaminating soil, seafood, fruits, vegetables, and honey. Historically, foodborne botulism has been known as the predominant form of entry. However, the toxin can also gain access through contact with open wounds or inhalation of aerosolized spores, although historically, inhalation of the toxin was largely due to bioterrorism [2,3]. Thus, with increased surveillance and heightened security measures, aerosolization of botulinum only constitutes a small fraction of total cases. Nonetheless, knowledge of its transmissibility has led to widespread precautions in handling preservatives and improperly canned foods.
Through purification techniques, scientists have been able to isolate eight serologically and antigenically distinct isoforms, termed BoNT types A, B, C1, C2, D, E, F, and G [4]. While different, experimental data has demonstrated a common theme across all serotypes: their ability to disrupt neuronal transmission at the neuromuscular junction (NMJ) via cleavage of the (soluble N-ethylmaleimide-sensitive factor attachment protein receptors) SNARE complex at different target sites. Upon ingestion and release into the bloodstream, these toxins migrate to presynaptic nerve terminals at the NMJ and act to inhibit the release of acetylcholine (ACh), which is responsible for propagating action potentials in skeletal muscle. As a result, interruption of ACh transmission diminishes muscle contraction which can progress to a state of flaccid paralysis [5].
Though botulinum toxins seem fraught with danger, there is great therapeutic potential when administered in calculated doses. Its efficacy has been well-established and documented for a broad range of indications characterized by neural hyperactivity, including cerebrovascular-related spasticity, cerebral palsy, dystonia, dyskinesia, sialorrhea, hyperhidrosis, nonspecific hypertonia, various cosmetic conditions, detrusor dysfunction, and anal fissures [6]. It should be noted that BoNT is clinically advised as an adjunctive therapy to neurorehabilitation or conservative measures rightfully earning its name as the “miracle poison” [7].
The purpose of this review is to provide a comprehensive analysis of botulinum toxin's molecular structure, mechanism of action, and its diverse therapeutic applications, particularly in neuromuscular disorders. By examining the different serotypes and formulations of BoNT, this review aims to highlight their clinical efficacy, safety profiles, and the considerations necessary for optimal use in medical practice.
DISCUSSION
Molecular Characterization and Mechanism of Action
Botulinum neurotoxin’s molecular components and active features are just as important to recognize as its therapeutic effects. The composite protein is a 150 kDa two-chain polypeptide complex that can be subdivided into two fragments: a 100 kDa heavy chain (H-chain) and a 50 kDa light chain (L-chain) [8]. The two chains are connected via covalent disulfide crosslinks, thereby stabilizing tertiary structure as shown in Figure 1.
Across the different isoforms, botulinum toxin type A (BoNT/A) appears to predominate in neuromuscular therapy and its clinical outcomes are the most proven. Mechanisms mediating BoNT/A migration to cholinergic nerve terminals may be explained through ganglioside (PSG) and synaptic vesicle protein (SV2) binding, particularly for BoNT/A. It is postulated that FGFR3 receptors may also play a role in attachment by inducing dimerization in motor neurons, but additional experimentation is admittedly needed to elaborate further on this mechanism [9].
The H-chain initiates a cascade of molecular events after its C-terminus selectively, but reversibly, latches onto receptors at the presynaptic axon terminal with a strong binding affinity. Live-cell imaging and electron microscopy studies have demonstrated that concurrent binding of the H-chain to PSG and SV2 receptors as shown in Figure 2], forming a tripartite nanocluster, is required for energy-dependent endocytosis [7,10]. Once terminal attachment via glycoprotein docking and subsequent internalization occur, there are a series of environmental changes including endosomal acidification and disulfide bond reduction that enable the separation of chains at the cleavage site [11]. After disengaging, the H-chain acts as a molecular chaperone to facilitate translocation and channeling of the L-chain into the cytoplasmic space [12]. It then navigates to the postsynaptic membrane where it proteolyzes components SNARE complex, particularly SNAP-25 and syntaxin, through its zinc-endopeptidase as shown in Figure 2, which possesses intrinsic metalloprotease activity [13]. After proteolytic cleavage is completed, the SNARE complex can no longer serve as a functional docking and fusion site for vesicular exocytosis and subsequent release of acetylcholine.
Under normal circumstances, neurotransmitters, predominately acetylcholine, are packaged into vesicles and directed to the postsynaptic membrane. Embedded within the vesicle membrane are v-SNARE proteins, which include synaptotagmin, acting as a Ca2+ sensor, and VAMP, alternatively known as synaptobrevin. Lying at the cytoplasmic interface of the terminal membrane are t-SNARE proteins, which include SNAP-25 and syntaxin as displayed in Figure 3 [14].
Increased calcium concentrations in the interneuronal space are transported inside the cytoplasmic space through voltage-gated calcium channels (VGCCs) and are ultimately recognized by synaptotagmin, commencing SNARE assembly. Although not well documented, Munc18 appears to play a role in interacting with syntaxin as the second step in this process. Thereafter, the Munc-18-syntaxin binary complex engages with SNAP-25 and VAMP/synaptobrevin, mobilizing the vesicle to the postsynaptic membrane [15,16]. The bridging of vesicle and transmembrane proteins creates a helically wound complete SNARE complex, coined the “zipper” hypothesis. The resultant configuration is inherently stable from torsional support. Chemical contents are exocytosed into the synaptic cleft through either spontaneous release or stimuli produced by Munc18 and other proteins, including complexins, known to be key regulators in presynaptic fusion [17].
Depending on BoNT isoform, there are different molecular targets of the SNARE complex as shown in Figure 4 [18]. As these targets may underlie varied clinical outcomes, it is important to establish a basis for this signaling. Serotypes A, E, and C target and truncate SNAP-25 whereas serotypes B, D, F, and G target and cleave VAMP/synaptobrevin [19]. While there are distinct sites of action based on serotype, the ultimate inhibition of transmembrane vesicle fusion and thus blockage of neurotransmitter release at motor nerve endings is shared.
Therapeutic Uses in Neuromuscular Disorders.
While comparative literature across different botulinum toxin subtypes is limited, it is clear that the therapeutic formulations of BoNT-A and BoNT-B constitute the overwhelming majority in managing movement disorders. Supported by clinically documented results, indications for botulinum toxins encompass a broad range of neuromuscular disorders, which include strabismus, blepharospasm, hemifacial spasm, focal dystonias, tics, tremors, and more. Treatment primarily revolves around improving muscular resistance, slowing hyperkinetic activity, normalizing autonomic dysfunction, and restoring hypertonia [20]. Food and Drug Administration (FDA) approvals and additional uses are constantly evolving so attention to updated guidelines and indications is encouraged.
On average, BoNT has an onset of action between 12-72 hours, achieving peak effect in approximately 1-3 weeks. Duration varies with individual patient factors but typically lasts 1-2 months and the effect begins to wane 2 to 3 months after. Hence, re-administration at 3-month intervals has commonly been used as a clinical standard [21].
With the wide-ranging applications of BTX, identification of the criteria and guidelines for healthcare utilization is warranted. There are three pharmaceutically distinct, commercially available formulations of the botulinum toxin type A that predominate in the sphere of neuromuscular disorders: IncobotulinumtoxinA (Xeomin), OnabotulinumtoxinA (Botox), AbobotulinumtoxinA (Dysport) [22]. A comprehensive list of neuromuscular and non-neuromuscular indications and applications for BoNT-A is illustrated in Table 1, Table 2, Table 3 and Table 4.
Safety Profile Considerations Between Different BoNT Formulations
Products of botulinum toxin A including Botox (approved in 2002), Dysport (approved in 2009), and Xeomin (approved in 2011), have a well-established presence in clinical practice. However, their administration must adhere to FDA guidelines to ensure patient safety and efficacy. Extensive research has established the lethal dosages and potentially harmful quantities of these agents, with particular emphasis on LD50 values and the minimum effective dose.
In contrast to many induced immunological responses that occur with medically administered injections (e.g. vaccines), only a minority of patients will develop toxin-blocking antibodies that can bind to and neutralize or inactivate the toxin. The degree of immunogenicity of different BoNT isoforms is relatively well known as BoNT-B boasts far greater immunogenic potential and autonomic adverse effects than its counterpart, BoNT-A [23]. The risk of blocking antibody formation must be considered to avoid diminishing the therapeutic effects. If no response is observed after a meaningful initial response, then one should examine the possibility of antibody-induced BoNT therapy failure. It is important to note that deviations from longer durations of action in other patients should be considered normal as each patient’s physiology is different and may yield varying results [24].
The potencies of botulinum toxin formulations also differ significantly, necessitating careful clinical judgment in selecting the appropriate product and dosing based on factors such as the dose-effect correlation, dose-duration correlation, impending muscle atrophy, and dilution effects [25]. Proper reconstitution and dosing are critical for optimal outcomes.
Comparative Compositional Analysis of BonT-A Formulations
Botox was the first neuromodulator to gain FDA approval, making its clinical debut on the market, and continues to dominate the industry in neuromuscular and cosmetic applications, comprising up to 85% of total BoNT usage [21]. So, it naturally follows that its research-backed results tower over its other two competitors, Dysport and Xeomin. Purified through repeated precipitation and re-dissolution, Botox contains trace amounts of albumin and sodium chloride and carries a full complement of protective proteins along with an accessory protein to enhance its delivery. Through ELISA testing, it is determined that Botox supplies up to 60% more neurotoxin protein, serving as the crudest and most denatured form of the therapeutically available BoNT-A formulations [22]. It is important to note that once the product is reconstituted, the contents of the vial begin to diminish, as does the potency. Hence, it is wise for providers to schedule groups of patients on the same day to minimize wasted product [1].
Dysport, arriving several years later into the market, shared much of the profile as Botox except its purification techniques, more widespread delivery, and greatest proportionally active neurotoxin activity. In contrast to Botox, Dysport is purified by way of column separation. This injectable has a quicker onset of action compared to its counterparts, offering an alternative for patients wishing to see more rapid results. Dysport has also shown the ability to have more diffusion or drifting effect, offering suitability for larger surface areas that would normally call for multiple injections [26].
Xeomin, making its entrance not long after Dysport, hoped to create a safer alternative that minimized the risk of patient rejection and anaphylactic reactions to the additives or preservatives in its counterparts. Experts claim Xeomin to be “naked” or the “purest” of the three injectables as it contains fewer foreign substances and is free of superfluous complexing proteins, thus mitigating the risk of sensitization [23]. For this reason, Xeomin rarely induces antibody formation, even at high doses, allowing for more frequent, repeated administration as needed [1]. Ironically, Xeomin appears to boast the highest specific neurotoxin activity, arising from its unbounded, free-form state [27].
CONCLUSION
Botulinum toxin, despite its infamous status as one of the most potent naturally occurring toxins, has proven to be a versatile and valuable therapeutic agent when harnessed in controlled doses. They block acetylcholine release at the neuromuscular junction, suppressing action potential and reducing hyperactive muscle contraction, has been repurposed to address a wide spectrum of medical conditions ranging from neuromuscular disorders to cosmetic applications. Additionally, with proper reconstitution, these minuscule doses have shown to provide long-lasting pain relief. The different BoNT serotypes and formulations, such as BoNT-A and BoNT-B, each offer unique properties, efficacy, and safety profiles, which enable tailored treatment strategies. However, physicians should use this treatment judiciously to prevent adverse reactions and minimize antibody formation. Patients should be well-advised about the risks, benefits, and realistic expectations of BoNT injections.
ACKNOWLEDGEMENT
None to declare
References
- Nigam, P.K.; Nigam, A. Botulinum toxin. Indian J Dermatol 2010, 55, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Jeffery IA, Karim S. “Botulism.,” StatPearls. Treasure Island (FL): StatPearls Publishing (2024) http://www.ncbi.nlm.nih.gov/books/NBK459273/ [Accessed September 23, 2024].
- Tiwari A, Nagalli S. “Clostridium botulinum Infection.,” StatPearls. Treasure Island (FL): StatPearls Publishing (2024) http://www.ncbi.nlm.nih.gov/books/NBK553081/ [Accessed September 24, 2024].
- Pirazzini, M.; Rossetto, O.; Eleopra, R.; Montecucco, C. Botulinum Neurotoxins: Biology, Pharmacology, and Toxicology. Pharmacol Rev 2017, 69, 200–235. [Google Scholar] [CrossRef] [PubMed]
- Whitemarsh, R.C.M.; Tepp, W.H.; Bradshaw, M.; Lin, G.; Pier, C.L.; Scherf, J.M.; Johnson, E.A.; Pellett, S. Characterization of botulinum neurotoxin A subtypes 1 through 5 by investigation of activities in mice, in neuronal cell cultures, and in vitro. Infect Immun 2013, 81, 3894–3902. [Google Scholar] [CrossRef] [PubMed]
- Intiso, D. Therapeutic Use of Botulinum Toxin in Neurorehabilitation. J Toxicol 2012, 2012, 802893. [Google Scholar] [CrossRef]
- Park, M.Y.; Ahn, K.Y. Scientific review of the aesthetic uses of botulinum toxin type A. Arch Craniofac Surg 2021, 22, 1–10. [Google Scholar] [CrossRef]
- Tehran, D.A.; Pirazzini, M. Novel Botulinum Neurotoxins: Exploring Underneath the Iceberg Tip. Toxins 2018, 10, 190. [Google Scholar] [CrossRef]
- Brin, M.F.; Burstein, R. Botox (onabotulinumtoxinA) mechanism of action. Medicine (Baltimore) 2023, 102, e32372. [Google Scholar] [CrossRef]
- Jiang, Y.-H.; Liao, C.-H.; Kuo, H.-C. Current and potential urological applications of botulinum toxin A. Nat Rev Urol 2015, 12, 519–533. [Google Scholar] [CrossRef]
- Ayyar, B.V.; Aoki, K.R.; Atassi, M.Z. The C-terminal heavy-chain domain of botulinum neurotoxin a is not the only site that binds neurons, as the N-terminal heavy-chain domain also plays a very active role in toxin-cell binding and interactions. Infect Immun 2015, 83, 1465–1476. [Google Scholar] [CrossRef]
- M; M Translocation of botulinum neurotoxin light chain protease by the heavy chain protein-conducting channel. Toxicon : official journal of the International Society on Toxinology 2009, 54. [CrossRef]
- Fj, L.; Rz, C.; U, M.; R, S.; Br, S.; M, A. The zinc-dependent protease activity of the botulinum neurotoxins. Toxins 2010, 2. [Google Scholar] [CrossRef] [PubMed]
- Schjeide, B.-M. Entwicklung und Charakterisierung des MoN-Light BoNT-Tests zur Bestimmung der Toxizität von Botulinum-Neurotoxin in Motorneuronen, die aus CRISPR-modifizierten induzierten pluripotenten Stammzellen differenziert wurdenDevelopment and characterization of the MoN-Light BoNT assay to determine the toxicity of botulinum neurotoxin in motor neurons differentiated from CRISPR-modified induced pluripotent stem cells, Universität Potsdam, 2021. [CrossRef]
- J, M.; J, W.; M, S.; Jo, D. TNFα induces co-trafficking of TRPV1/TRPA1 in VAMP1-containing vesicles to the plasmalemma via Munc18-1/syntaxin1/SNAP-25 mediated fusion. Scientific reports 2016, 6. [Google Scholar] [CrossRef]
- Lu, B. The destructive effect of botulinum neurotoxins on the SNARE protein: SNAP-25 and synaptic membrane fusion. PeerJ 2015, 3, e1065. [Google Scholar] [CrossRef]
- Rizo, J. Mechanism of neurotransmitter release coming into focus. Protein Sci 2018, 27, 1364–1391. [Google Scholar] [CrossRef] [PubMed]
- Arnon, S.S.; Schechter, R.; Inglesby, T.V.; Henderson, D.A.; Bartlett, J.G.; Ascher, M.S.; Eitzen, E.; Fine, A.D.; Hauer, J.; Layton, M.; et al. Botulinum toxin as a biological weapon: medical and public health management. JAMA 2001, 285, 1059–1070. [Google Scholar] [CrossRef]
- Brideau-Andersen, A.; Dolly, J.O.; Brin, M.F. Botulinum neurotoxins: Future innovations. Medicine (Baltimore) 2023, 102, e32378. [Google Scholar] [CrossRef]
- Chf, C.; Hag, T. Use of botulinum toxin for movement disorders. Drugs in context 2019, 8. [Google Scholar] [CrossRef]
- Tilton, A.H. Injectable neuromuscular blockade in the treatment of spasticity and movement disorders. J Child Neurol 2003, 18 Suppl 1, S50–66. [Google Scholar] [CrossRef]
- Choudhury, S.; Baker, M.R.; Chatterjee, S.; Kumar, H. Botulinum Toxin: An Update on Pharmacology and Newer Products in Development. Toxins (Basel) 2021, 13, 58. [Google Scholar] [CrossRef]
- Bentivoglio, A.R.; Del Grande, A.; Petracca, M.; Ialongo, T.; Ricciardi, L. Clinical differences between botulinum neurotoxin type A and B. Toxicon 2015, 107, 77–84. [Google Scholar] [CrossRef]
- Dressler, D. Clinical presentation and management of antibody-induced failure of botulinum toxin therapy. Mov Disord 2004, 19 Suppl 8, S92–S100. [Google Scholar] [CrossRef]
- D, D.; F, A.S. Botulinum toxin: mechanisms of action. European neurology 2005, 53. [Google Scholar] [CrossRef]
- Walker, T.J.; Dayan, S.H. Comparison and overview of currently available neurotoxins. J Clin Aesthet Dermatol 2014, 7, 31–39. [Google Scholar] [PubMed]
- Frevert, J. Content of Botulinum Neurotoxin in Botox®/Vistabel®, Dysport®/Azzalure®, and Xeomin®/Bocouture®. Drugs R D 2010, 10, 67–73. [Google Scholar] [CrossRef]
- Field, M.; Splevins, A.; Picaut, P.; van der Schans, M.; Langenberg, J.; Noort, D.; Foster, K. AbobotulinumtoxinA (Dysport®), OnabotulinumtoxinA (Botox®), and IncobotulinumtoxinA (Xeomin®) Neurotoxin Content and Potential Implications for Duration of Response in Patients. Toxins (Basel) 2018, 10, 535. [Google Scholar] [CrossRef]
- Scaglione, F. Conversion Ratio between Botox®, Dysport®, and Xeomin® in Clinical Practice. Toxins (Basel) 2016, 8, 65. [Google Scholar] [CrossRef]
- Thomas, A.J.; Larson, M.O.; Braden, S.; Cannon, R.B.; Ward, P.D. Effect of 3 Commercially Available Botulinum Toxin Neuromodulators on Facial Synkinesis. JAMA Facial Plast Surg 2018, 20, 141–147. [Google Scholar] [CrossRef]
- Pasricha, P.J.; Rai, R.; Ravich, W.J.; Hendrix, T.R.; Kalloo, A.N. Botulinum toxin for achalasia: long-term outcome and predictors of response. Gastroenterology 1996, 110, 1410–1415. [Google Scholar] [CrossRef] [PubMed]
- Campanati A, Martina E, Gregoriou S, Kontochristopoulos G, Paolinelli M, Diotallevi F, Radi G, Bobyr I, Marconi B, Gualdi G, et al. Botulinum Toxin Type A for Treatment of Forehead Hyperhidrosis: Multicenter Clinical Experience and Review from Literature. Toxins (Basel) 2022, 14, 372. [Google Scholar] [CrossRef]
- Chow, P.-M.; Kuo, H.-C. Botulinum Toxin A Injection for Autonomic Dysreflexia—Detrusor Injection or Urethral Sphincter Injection? Toxins (Basel) 2023, 15, 108. [Google Scholar] [CrossRef]
- Romanov A, Pokushalov E, Ponomarev D, Bayramova S, Shabanov V, Losik D, Stenin I, Elesin D, Mikheenko I, Strelnikov A, et al. Long-term suppression of atrial fibrillation by botulinum toxin injection into epicardial fat pads in patients undergoing cardiac surgery: Three-year follow-up of a randomized study. Heart Rhythm 2019, 16, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Carroll, I.; Clark, J.D.; Mackey, S. Sympathetic Block with Botulinum Toxin to Treat Complex Regional Pain Syndrome. Ann Neurol 2009, 65, 348–351. [Google Scholar] [CrossRef] [PubMed]
- Lawson, O.; Sisti, A.; Konofaos, P. The Use of Botulinum Toxin in Raynaud Phenomenon: A Comprehensive Literature Review. Ann Plast Surg 2023, 91, 159–186. [Google Scholar] [CrossRef]
- Geoghegan, L.; Rodrigues, R.; Harrison, C.J.; Rodrigues, J.N. The Use of Botulinum Toxin in the Management of Hidradenitis Suppurativa: A Systematic Review. Plast Reconstr Surg Glob Open 2022, 10, e4660. [Google Scholar] [CrossRef]
- Zhang, H.; Tang, K.; Wang, Y.; Fang, R.; Sun, Q. Use of Botulinum Toxin in Treating Rosacea: A Systematic Review. Clin Cosmet Investig Dermatol 2021, 14, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Brisinda, G.; Chiarello, M.M.; Crocco, A.; Bentivoglio, A.R.; Cariati, M.; Vanella, S. Botulinum toxin injection for the treatment of chronic anal fissure: uni- and multivariate analysis of the factors that promote healing. Int J Colorectal Dis 2022, 37, 693–700. [Google Scholar] [CrossRef]
- González, C.; Franco, M.; Londoño, A.; Valenzuela, F. Breaking paradigms in the treatment of psoriasis: Use of botulinum toxin for the treatment of plaque psoriasis. Dermatol Ther 2020, 33, e14319. [Google Scholar] [CrossRef]
Figure 1.
Molecular Architecture of Botulinum Neurotoxins. Legends: Courtesy: Tehran and Pirazzini (8). L: light chain; HN: heavy chain translocation domain; HC-C: heavy chain C (carboxy-) terminus receptor binding subdomain; HC-N: heavy chain N (amino-) terminus receptor binding subdomain; belt: represents a 50-residue strip encircling the light chain serving as a pseudosubstrate to inhibit premature endopeptidase activity.
Figure 1.
Molecular Architecture of Botulinum Neurotoxins. Legends: Courtesy: Tehran and Pirazzini (8). L: light chain; HN: heavy chain translocation domain; HC-C: heavy chain C (carboxy-) terminus receptor binding subdomain; HC-N: heavy chain N (amino-) terminus receptor binding subdomain; belt: represents a 50-residue strip encircling the light chain serving as a pseudosubstrate to inhibit premature endopeptidase activity.
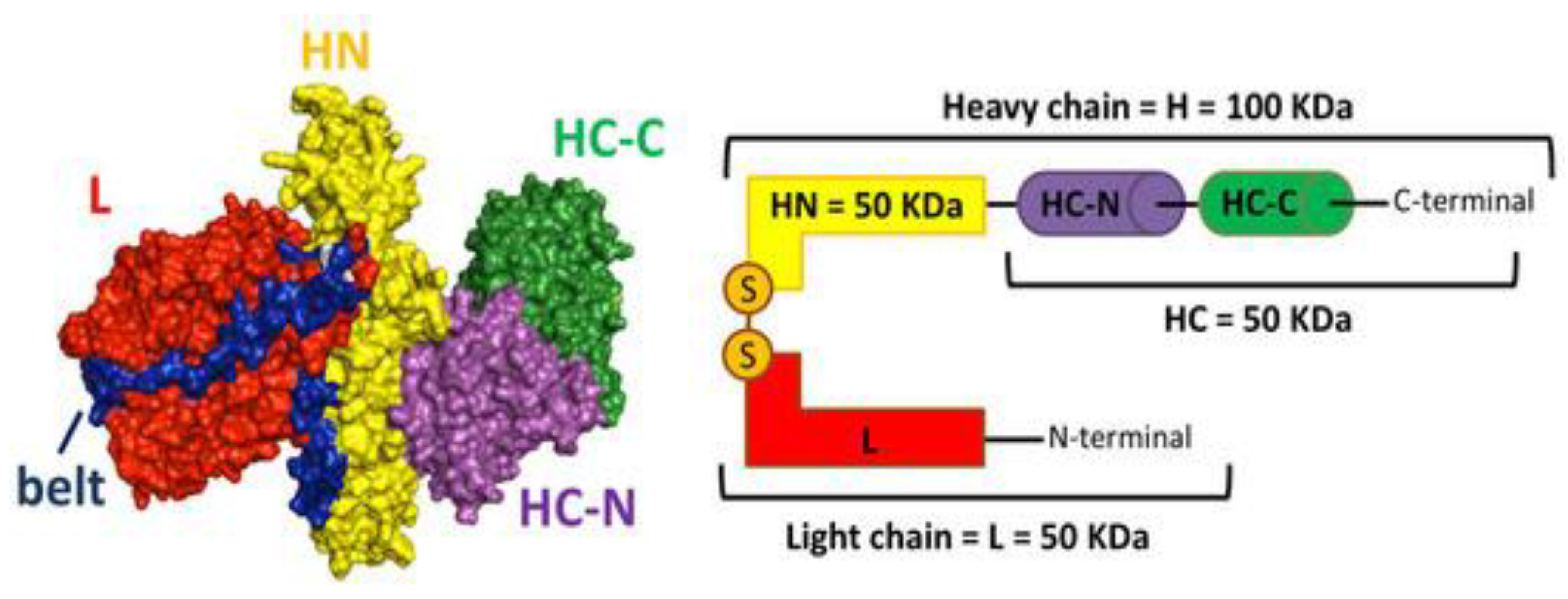
Figure 2.
Effects of BoNT-A on detrusor smooth muscle contraction. Legends: Courtesy: Jiang et al. (10). PSG: polysialoganglioside; SV2: synaptic vesicle glycoprotein 2; VGSC: voltage-gated sodium channel; VGCC: voltage-gated calcium channel.
Figure 2.
Effects of BoNT-A on detrusor smooth muscle contraction. Legends: Courtesy: Jiang et al. (10). PSG: polysialoganglioside; SV2: synaptic vesicle glycoprotein 2; VGSC: voltage-gated sodium channel; VGCC: voltage-gated calcium channel.
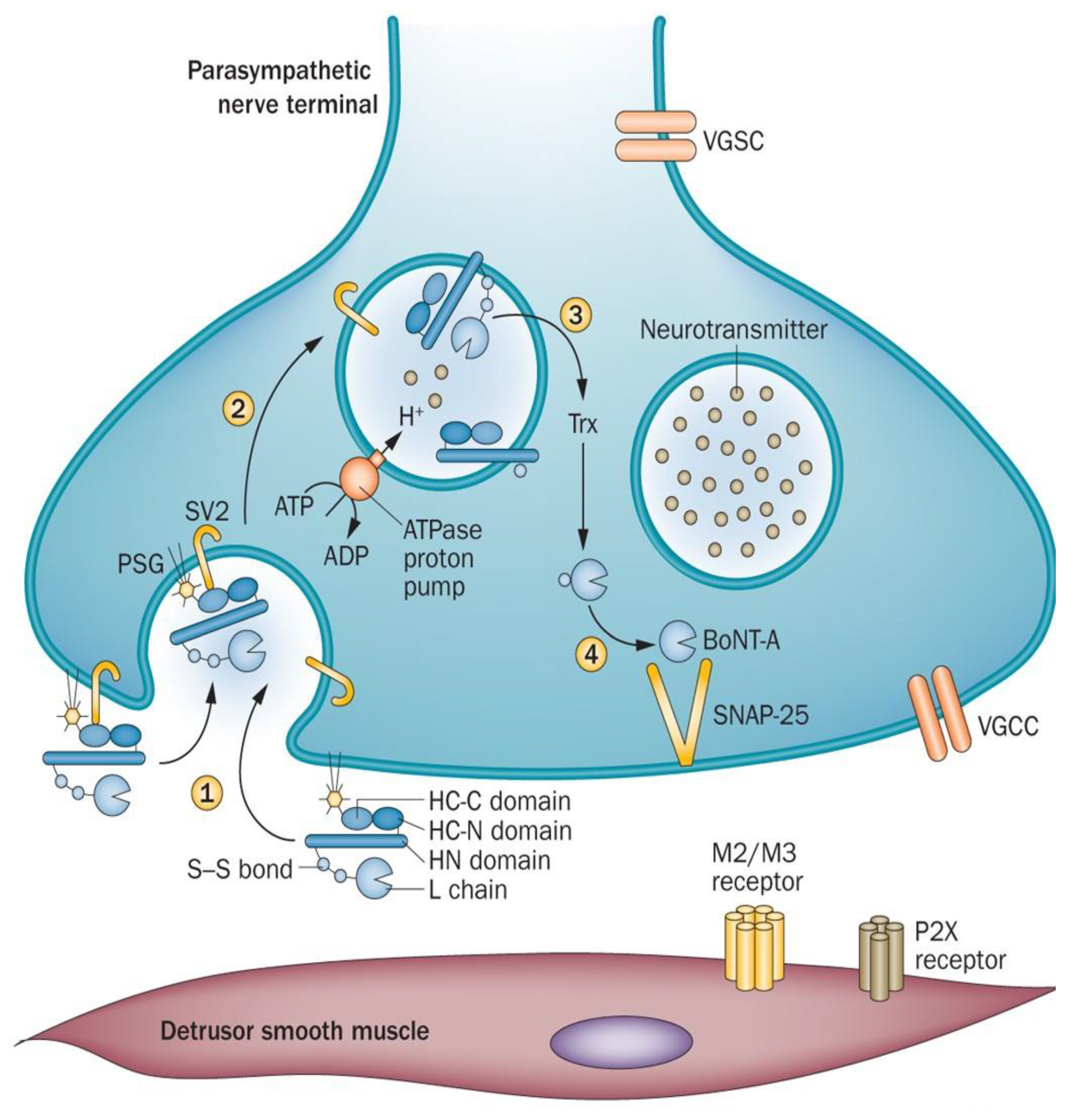
Figure 3.
Simplified Schematic of SNARE Complex-mediated Vesicle. Legends: Courtesy: Schjeide et al. (14).
Figure 3.
Simplified Schematic of SNARE Complex-mediated Vesicle. Legends: Courtesy: Schjeide et al. (14).
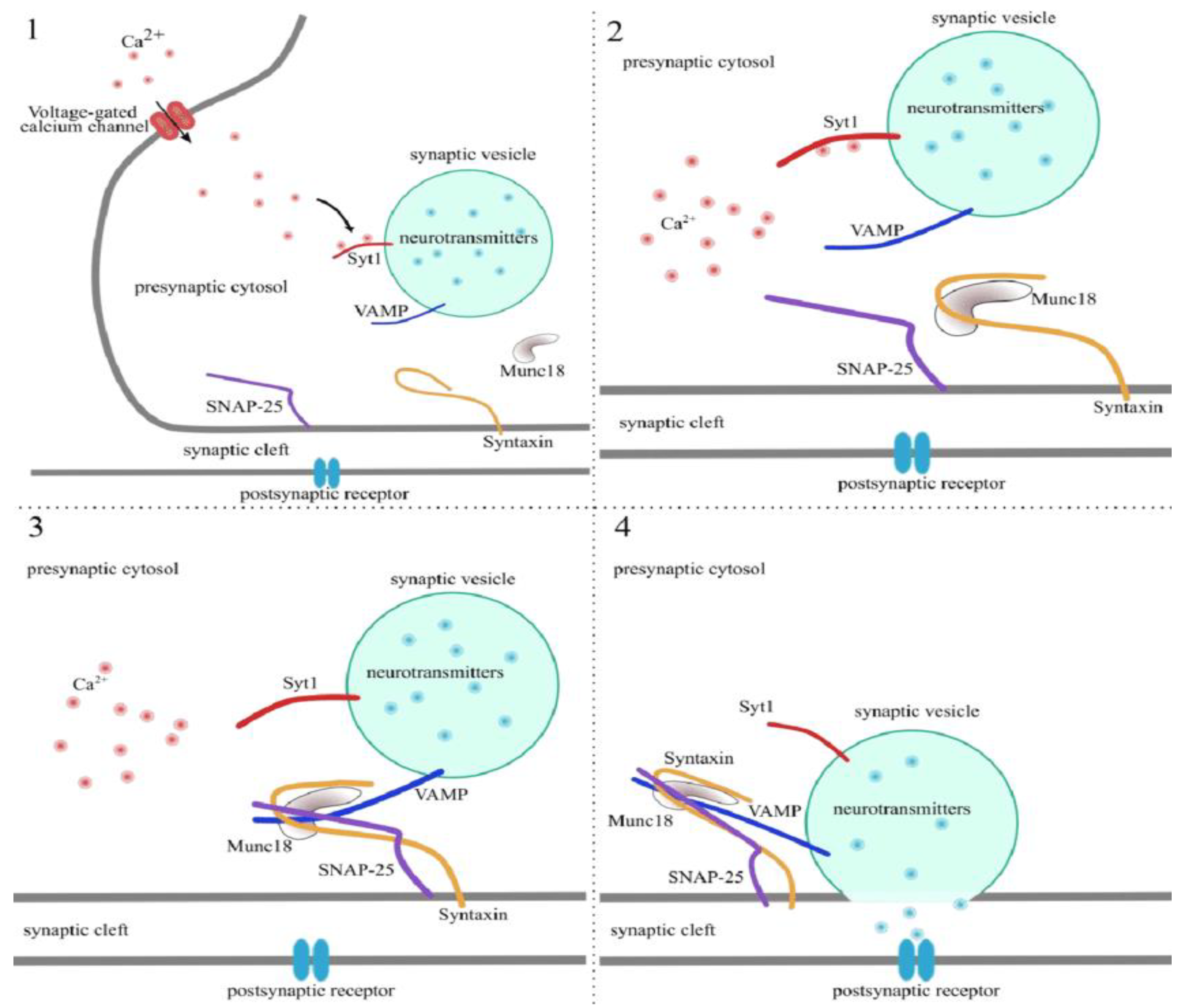
Figure 4.
Mechanism of Action of Botulinum Toxin. Legends: Courtesy: Arnon et al. (18).
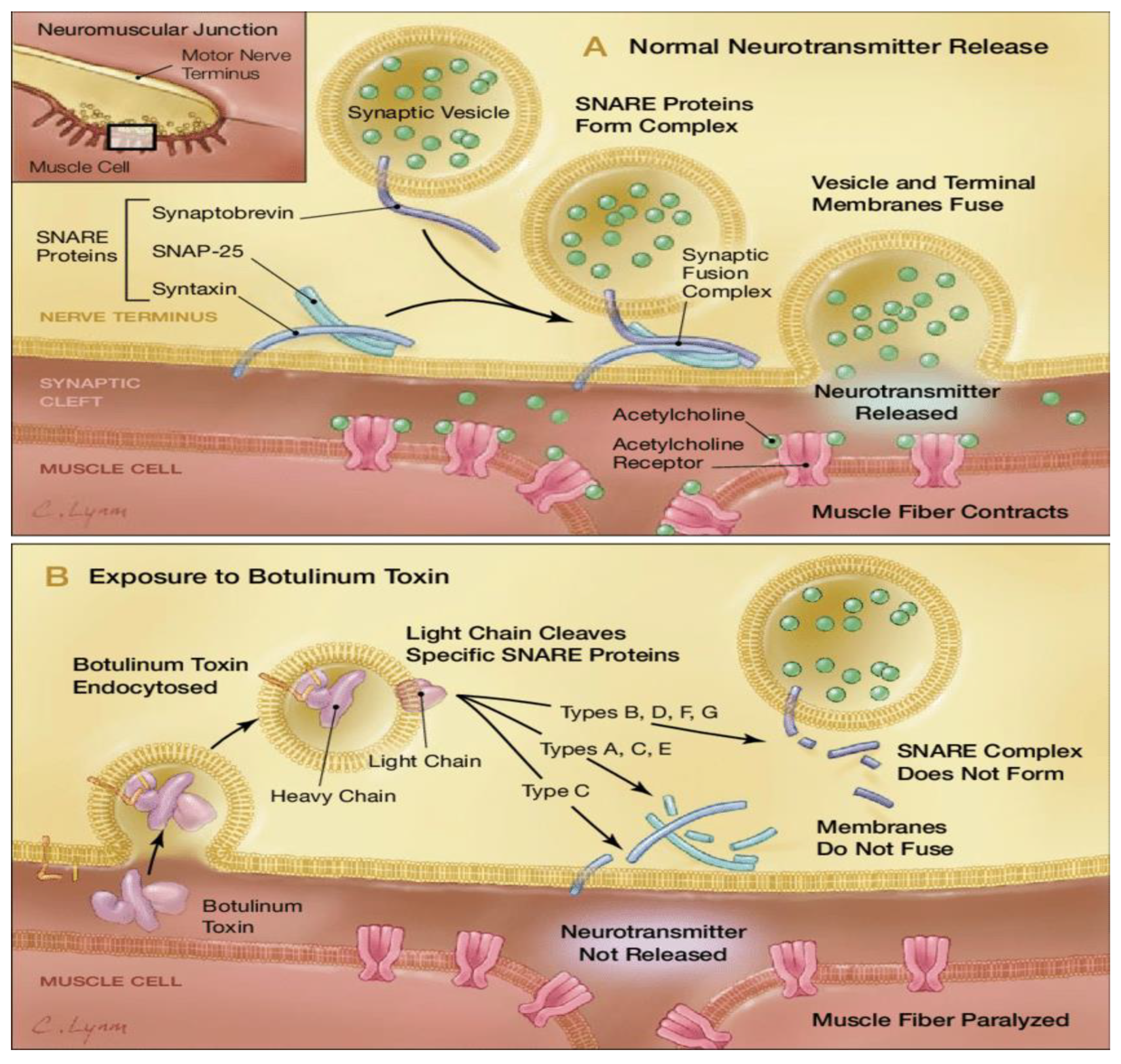

Table 1.
Indications of OnabotulinumtoxinA (Botox).
| Serial No. | Disorder Specification | Symptoms Experienced (27–30) |
|---|---|---|
| 1. | Upper Limb Spasticity | Muscles in the arms become stiff, flexed, & painful. |
| 2. | Lower Limb Spasticity | Muscles in the legs become stiff, flexed, & painful. |
| 3. | Cervical Dystonia | Abnormalities in head and neck posture with severe pain. |
| 4. | Chronic Migraine Prophylaxis | Recurring throbbing and pulsating sensations that impair daily activity. |
| 5. | Blepharospasm and Strabismus | Uncontrolled, spasmodic facial or eye muscle movement. |
| 6. | Bladder (detrusor) Dysfunction | Hyperactivity leading to increased urinary incontinence, urgency, and frequency. |
| 7. | Primary Axillary Hyperhidrosis | Over-stimulation of sweat glands that causes excessive perspiration. |
| 8. | Cosmetics | Glabellar/frown lines - vertical wrinkles from corrugator and procerus overactivity Crow’s Feet - lateral canthal lines from orbicularis oculi overactivity Forehead lines - horizontal wrinkles from frontalis overactivity. |
Table 2.
Indications for IncobotulinumtoxinA (Dysport).
| Serial No. | Disorder Specification | Symptoms Experienced (27–30) |
|---|---|---|
| 1. | Cervical Dystonia | Abnormalities in head and neck posture with severe pain. |
| 2. | Upper Limb Spasticity | Muscles in the arms become stiff, flexed, & painful. |
| 3. | Lower Limb Spasticity | Muscles in the legs become stiff, flexed, & painful. |
| 4. | Glabellar/Frown Lines | Moderate-severe vertical wrinkles from corrugator and procerus overactivity. |
Table 3.
Indications for AbobotulinumtoxinA (Xeomin).
| Serial No. | Disorder Specification | Symptoms Experienced (27–30) |
|---|---|---|
| 1. | Cervical Dystonia | Abnormalities in head and neck posture with severe pain. |
| 2. | Upper Limb Spasticity | Muscles in the arms become stiff, flexed, & painful. |
| 3. | Blepharospasm | Abnormal contractions that cause squeezing and twitching of the eyelid muscles. |
| 4. | Chronic Sialorrhea | Excessive drooling or salivation from poor orofacial muscle control. |
| 5. | Glabellar Lines | Moderate-severe vertical wrinkles from corrugator and procerus overactivity. |
Table 4.
Off-label uses of botulinum toxin.
| Serial No. | Disorder Specification | Mechanism of action | Symptoms Experienced |
|---|---|---|---|
| 1. | Achalasia | Relieves chronically contracted LES | Motor disorder of distal esophageal sphincter involving degeneration of inhibitory NO-producing neurons with resultant aperistalsis and hypertonia causing dysphagia to liquids and solids (31). |
| 2. | Palmar/Craniofacial Hyperhidrosis | Interrupt neural transmission of nicotinic and muscarinic receptors destined for eccrine and apocrine sweat glands. | Idiopathic excessive sweat production in other than axillary areas (32). |
| 3. | Autonomic Dysreflexia | Blunts reflexive sympathetic spinal responses. | Autonomic dysregulation often arising from spinal cord injury, leading to sympathetic control imbalances (33). |
| 4. | Atrial Fibrillation | Injection into epicardial fat pads suppresses ectopy. | Electrical abnormalities within the cardiac circuit that do not terminate spontaneously (34). |
| 5. | Complex Regional Pain Syndrome | Blockade of cholinergic preganglionic fibers with sympathetic ganglion block. | Disrupted relationship between sympathetic nervous system and nociceptive transmission (35). |
| 6. | Raynaud’s Phenomenon | Restoration of arterial flow through vasodilation. | Exaggerated vasoregulatory constriction of distal extremities in response to certain stressors (36). |
| 7. | Hidradenitis Suppurativa | Suppresses release of follicular contents into dermis. | Persistent, painful nodules, abscesses, and fistulas in the skin folds of the axilla, groin, gluteal, and perineal regions (37). |
| 8. | Rosacea | Modulation of Ach, substance P, CGRP, and VIP. | Erythema, telangiectasia, papules and pustules in and around the face, forehead, nose, cheeks, and chin (38). |
| 9. | Anal Fissures | Relieves painful spasms of internal anal sphincter and regulates autonomic control. | Tears in the epithelial lining of the anal canal distal to dentate line, sensitizing somatic nerve fibers (39). |
| 10. | Plaque Psoriasis | Intradermal injection demonstrates complete remission from targeted lesional eruption. | Erythematous, scaly papules and thick plaques typically on the scalp, trunk, elbows, knees, and gluteal folds (40). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



