
Submitted:
26 September 2024
Posted:
26 September 2024
You are already at the latest version
Abstract
Background: Echovirus 11 (EV-11) is a notable enterovirus linked to severe infections in neonates, often resulting in significant morbidity and mortality. In April 2019, an EV-11 outbreak occurred in the sick neonate room at a teaching hospital in Taichung, Taiwan, posing a serious threat to the vulnerable infants in this setting. Objectives: This study aimed to identify the source and transmission dynamics of the EV-11 outbreak in the neonatal unit and evaluate the effectiveness of the infection control measures implemented to contain the outbreak. Methods: Patient records, epidemiological data, and laboratory findings were reviewed. For all cases, confirmatory tests were performed using virus isolated from cerebrospinal fluid. Rapid quarantine measures were employed. The hospital’s nosocomial infection surveillance system was used to track confirmed cases and exposed individuals to facilitate effective management and monitoring; Results: Five neonates were confirmed to have EV-11 during the outbreak. Surveillance of 10 contacts and 11 newly admitted cases yielded negative results. All infected infants eventually recovered. The cohort comprised three males and two females, with a birth weight range of 2472–4224 grams. Their gestational ages range of 34 3/7 weeks to 39 weeks; including two premature and three full-term infants. Symptoms began between 6 and 27 days of life, with fever being the consistent clinical manifestation. Strict infection control measures, including isolation of infected cases, suspension of rooming-in, and rigorous disinfection protocols, successfully halted viral spread. The outbreak was contained within 39 days, with no additional cases reported post-intervention; Conclusions: The prompt and effective response, including robust infection control protocols, was crucial for managing and containing the EV-11 outbreak in the neonatal unit. These cases underscore the significance of immediate action, stringent infection control measures, and ongoing monitoring for addressing enterovirus outbreaks in neonatal care settings.
Keywords:
Echovirus 11
; outbreak control
; neonatal infection
; sick neonate room
; infection control
; enterovirus
; epidemiology
; hospital outbreak
1. Introduction
Enterovirus infections have been linked to various clinical syndromes in newborns, ranging from mildly febrile illnesses with or without rash, herpangina, hand, foot, and mouth disease, conjunctivitis, respiratory and gastrointestinal tract diseases, to more severe, sometimes life-threatening conditions such as aseptic meningitis, encephalitis, polio-like paralysis, myopericarditis, and chronic enterovirus infections in immunocompromised individuals[1].
Echoviruses (Enteric Cytopathgenic Human Orphan viruses), 30μm in diameter, are non-enveloped viruses with a positive -sense single-stranded RNA genome with 30 serotypes, and are members of the genus Enterovirus from the family Picornaviridae[2]., and are classified in the species of human Enterovirus B[3]. Since its initial isolation and description in the 1950s[4], Echovirus are known to be a common cause of human diseases, including an acute nonspecific febrile illness with or without rash, and aseptic meningitis[5].Echovirus infections, especially in neonates, are usually mild and self-limited, however, there have been several outbreaks of severe illness with occasional fatal outcomes[6,7]. Echovirus 11, (EV-11), is the most commonly identified serotype that is typically associated with mild gastrointestinal and respiratory infections, hand foot mouth disease, and uveitis[8-10], however, it can escalate to more serious conditions, such as myocarditis, meningitis, encephalitis, and sepsis, in vulnerable populations, including neonates[3,11,12]. Immature immune systems and increased vulnerability to viral infections and inadequate inflammatory reactions in neonates may be two of the causes[13,14] .
During a 2018 outbreak in Taiwan, 181 cases were confirmed nationwide via viral culture surveillance by Taiwan Centers for Disease Control (CDC), with neonates comprising 19% (35 cases), and the mortality rate is 3.8% (7 cases) of the cases; nursery epidemics of EV-11 are common, with frequent reports of outbreaks [15]. A local study retrospectively analyzed 60 patients with EV-11 infection and found that 35% of infants with younger than 3 months old had positive virus culture from CSF specimens and 13% of severe hepatitis, and only one case died due to myocarditis and severe sepsis[13]. Another retrospective analysis targeted 10 infants with confirmed EV-11 infection found that 50% of infants (5 cases) with aseptic meningitis, and one case with fulminant hepatitis [16]. All highlight the vulnerability of newborns to EV-11 and underscores the importance of effective outbreak management.
In April 2019, a teaching hospital in Taichung, Taiwan experienced a significant EV-11 outbreak in the sick neonate room (SN), which is a nursery that provides nursing care to those infants convalescing or those sick infants not requiring intensive care. This outbreak presented a severe challenge to the hospital’s infection control practices, as the SN housed a particularly vulnerable group of neonates, many of whom were already in a fragile state due to their underlying conditions. The emergence of EV-11 in this setting prompted an urgent investigation to understand the source of the outbreak and the mechanisms of viral transmission.
This investigation aimed to identify the root causes of the outbreak and to implement effective control measures to prevent further spread of EV-11. Given the high risk of severe illness due to EV-11 in neonates, it is crucial to respond swiftly and efficiently to mitigate the impact of outbreaks. This study provides insights into the successful control of EV-11 outbreaks in neonatal settings and highlights the importance of robust infection control practices and timely interventions.
2. Materials and Methods
2.1. Study Population
This retrospective study was conducted at a teaching hospital in Taichung, Taiwan and focused on patients admitted to the SN, which accommodates up to 20 infants (Figure 1). The study spanned April to June 2019 and was approved by the Institutional Review Board of Tungs’ Taichung Metro Harbor Hospital (IRB approval No.:112054). The study included infants with symptoms suggestive of EV-11 infection, confirmed through viral isolation.
2.2. The Outbreak
The outbreak led to the retrospective identification of five cases potentially linked to the incident in the SN. Case 1, a premature and inborn infant, presented fever, poor activity, acrocyanosis, apnea, and bradycardia on her seventh day of life. All symptoms spontaneously resolved after five days of fluid and empirical antibiotic treatment. However, EV-11 was isolated from her CSF on the 23rd day of life. Case 2 was admitted to the SN for his prematurity and shortness of breath. His vital signs remained stable until the sixth day, when he developed fever, tachypnea, and poor activity. Laboratory results indicated anemia, thrombocytopenia, hepatitis, elevated troponin I, and BNP. Initially, clinicians contributed his symptoms to herpes virus infection. As his fever persisted after three days of acyclovir (30 mg/kg/day) administration, clinicians contributed his fever to herpes virus intractable to acyclovir. After a trial of administered immunoglobulin (IVIG; 1 g/kg/dose) on day six, his fever subsided and activity significantly improved by day eight. EV-11 was isolated from his CSF on day 20..Case 3, an outborn neonate, was stable at a postpartum care center until presenting with fever, poor feeding, poor activity, and skin rash on the ninth day of life. She was subsequently admitted to the SN. 1 g/kg/dose of IVIG was given on day ten due to her persistent fever, attributed to herpes virus infection despite two days of acyclovir treatment. Her symptoms drastically improved by day 12. Her EV-11 meningitis was confirmed with virus isolation in her CSF on day 33. Case 4 (the index case), an outborn neonate, exhibited fever and skin rash at a postpartum care center on the 26th day of life. He was admitted to the SN and recovered without complications after receiving fluids and empirical antibiotics. EV-11 was isolated from his CSF on day 47. Cases 1 and 2 were cared for in close proximity to Case 4 during the outbreak (see Figure. 1A). Case 5 was admitted to a postpartum care center, where he exhibited fever, poor feeding, and skin rash on the ninth day of life. He was transferred to the SN for further evaluation. 1 g/kg/dose of IVIG was administered on day ten for his persistent fever, suspected to be due to herpes virus infection despite two days of acyclovir treatment. All symptoms resolved without complications, and EV-11 meningitis was confirmed with virus isolation in his CSF on day 33. Before the action of investigation, the Cases 3 to 5 were studied for viral infections upon admission, but not isolated, contributing to the spread of the virus within the SN. Notably, Cases 3 to 5 were born at the same clinic and had no prior connections within the community before their hospital admission. Detailed patient data are presented in Table 1 and Table 2.
2.3. Clinical Investigation and Intervention
After an on-site inspection on the 4th of May 2019, a designated isolation zone was established in the isolation area of the SN to manage suspected and confirmed cases (Figure 1B). A bundle of infection control measures was enforced, including strict hand hygiene protocols involving water, 75% alcohol, and 0.5% chlorhexidine gluconate-based hand rubs disinfection process. Healthcare workers and visitors were required to use gloves and isolation gowns. Access to the SN was limited to one visitor per patient, and individuals with signs of any infectious diseases were barred from entry. Patient transfers were restricted to the same floor, and infection control practitioners closely monitored hand hygiene practices, providing feedback to ensure adherence to outbreak control measures. Environmental cleaning was intensified, with daily disinfection using a 1:50 dilution of sodium hypochlorite (1000 ppm) for at least 10 minutes. Pacifiers and baby bottles used by confirmed cases were sterilized and were not shared with others. Quarantine measures were implemented, and clinical presentations associated with EV-11 were educated to patients’ family to monitor all contacts. During April and June 2019, only five cases were identified. After the infection control interventions, no further cases have been identified or linked to this hospital setting following the outbreak. The epidemiologic curve, illustrating the dates of admission, onset of echovirus 11 infections, and intervention dates, is shown in Figure 2.
2.4. Laboratory Investigations
Specimens of the cerebrospinal fluid (CSF) from the SN patients were sent to a medical center for analysis. The virus was isolated following established protocols. After five additional infants had fever, the outbreak was reported to the infection control committee on the 4th of May. The committee soon activated a hospital emergency response team for epidemiological investigations, implementation of infection control measures, and reconstruction of the SN infrastructure to contain the outbreak.
3. Results
3.1. Descriptive Epidemiology
The demographic and epidemiological characteristics of the five neonates diagnosed with EV-11 infection are summarized in Table 1. The cohort consisted of three males and two females, with birth weights ranging from 2472 grams to 4224 grams. Two infants were premature. The age at symptom onset varied, ranging from 6th to 27th day. The age at the laboratory confirmation of EV-11 infection ranged from 20th day to 47th day of life, indicating variability in the time to diagnosis. All infants developed a fever as the primary clinical manifestation, highlighting it as a consistent symptom of EV-11 infection in this cohort. Despite variations in the timing of symptom onset and diagnosis, the presence of fever was a clinical feature common to all cases, suggesting that early fever in neonates may be a critical indicator of EV-11 infection.

Table 1.
Demographic and Clinical Data of Neonatal Patients with EV-11 meningitis.
| Case | Clinical manifestations | Outborn | Birth weight (g)/ gender | Gestational age(weeks) | Age at onset (d) | Age at Lab confirm (d) |
| Case 1 | fever, poor activity, acrocyanosis, apnea, bradycardia | - | 4224/F | 36 2/7 | 7 | 23 |
| Case 2 | fever, tachypnea, poor activity | - | 2472/M | 34 3/7 | 6 | 20 |
| Case 3 | fever, poor feeding, poor activity, skin rash | + | 3670/F | 39 | 9 | 23 |
| Case 4 | fever, skin rash | + | 3035/M | 38 3/7 | 27 | 47 |
| Case 5 | fever, poor feeding, skin rash | + | 3040/M | 39 | 9 | 39 |
This table provides detailed demographic and clinical characteristics of the five neonates diagnosed with Echovirus 11 (EV-11) infection during the outbreak. The variables include primary symptoms, outborn or inborn, gestational age, gender, birth weight, age at symptom onset, and age at EV-11 isolated from CSF.
3.2. Laboratory Investigations
The laboratory investigations provided comprehensive data on the hematological, biochemical, and CSF parameters of the infected infants (Table 2). White blood cell (WBC) counts varied significantly among the infants and ranged from 5000 cells/µL to 26,400 cells/µL. Differential counts showed a predominance of segmented neutrophils, which ranged from 53.3% to 88%, with corresponding lymphocyte percentages varying between 7.6% and 38%. Platelet counts varied significantly among the infants and ranged from 60,000 platelets/µL to 11,300 platelets/µL. The variation in these parameters indicates differing immune response levels among the infants, possibly reflecting the severity of the infection.
Liver enzyme levels, including glutamic oxaloacetic transaminase (GOT) and glutamic pyruvic transaminase (GPT), were elevated in Case 2, who had significantly high GOT and GPT levels of 8879 IU/L and 549 IU/L, respectively. These elevated liver enzymes suggest hepatic involvement, a common feature in viral infections, particularly those caused by EV-11[4, 14–15].
C-reactive protein (CRP), a marker of inflammation, was notably elevated in several cases, particularly in Case 1 at 7.79 mg/dL. This increase is indicative of a strong inflammatory response, which is consistent with the acute phase of EV-11 infection. The troponin I level is a marker of cardiac injury[17]. B type natriuretic peptide (brain natriuretic peptide; BNP) a hormone is produced by the ventricular muscle in human hearts [18]. Both showed a significant elevation in case 2 (troponin I: 0.292ng/mL; BNP: 717 pg/mL), and the ejection fraction calculated with a cardioechogram was 82%, which was not compatible with the criteria of myocarditis. CSF analysis yielded significant findings: glucose levels ranging from 51 mg/dL to 73 mg/dL and protein levels between 43 mg/dL and 229 mg/dL. WBC counts in the CSF varied, with Case 3 showing a particularly high count of 56 cells/µL, and the presence of RBCs (56,000 cells/µL ) in the CSF suggested a robust inflammatory response in the central nervous system, or a traumatic tapping. The presence of RBCs in the CSF was also noted, although in low quantities, indicating mild hemorrhagic involvement in some cases.
Overall, the laboratory investigations highlighted the systemic nature of EV-11 infection, which affected multiple organ systems including the liver, blood cells, and central nervous system. The variability in laboratory parameters among the infants underscores the diverse clinical presentations and the need for comprehensive monitoring and management of neonates with suspected or confirmed EV-11 infection.
Table 2.
Laboratory Investigations of Neonatal Patients with EV-11 meningitis.
| Case | Blood | CSF | ||||||||||||
| WBC (X1000) |
N/L | PLT (X1000) |
Hb | GOT /GPT |
BUN /Cr |
CPK | CRP | TPNI | BNP | Glu | Glu | Protein | WBC /RBC | |
| Case 1 | 19.6 | 88.2/7.6 | 225 | 17 | 56 /8 |
11 /0.52 |
308 | 7.79 | 0.017 | 198 | 59 | 57 | 71 | 2/1 |
| Case 2 | 26.4 | 74/10 | 60 | 11.7 | 8879 /549 |
19 |
||||||||
This table highlights the hematological, biochemical, and cerebrospinal fluid (CSF) parameters for the neonates infected with EV-11. The variables include white blood cell count (WBC), platelet count, hemoglobin (Hb), liver enzyme levels (GOT/GPT: glutamic-oxaloacetic transaminase/ glutamic-pyruvic transaminase), kidney function levels (BUN/Cr: blood urea nitrogen/ creatinine), muscle enzyme levels (CPK: Creatine phosphokinase); CRP (C-reactive protein), TPNI ( Troponin I), BNP (B-type natriuretic peptide), Glu (Glucose), and cerebrospinal fluid analysis results.
3.3. Further Interventions
During the outbreak, new patient admissions were suspended until designated quarantine areas were established. To prevent community infections, additional beds were allocated in general wards for non-critical outborn neonates. Critical patients were admitted and quarantined within an isolation zone in the SN. Throat and rectal swabs from all new cases underwent viral isolation surveillance; negative results permitted release from quarantine, while cases exhibiting EV-11-related symptoms required further viral isolation and testing and remained quarantined until their symptoms were free.
3.4. Hospital Information System and Control Measures
During the outbreak, confirmed cases and exposed patients from April to June 2019 were recorded as EV-11 contacts in the hospital information system for tracking by the emergency and outpatient departments. Follow-up was conducted one week post-discharge, and healthcare workers were promptly notified of new EV-11 infection results via text messages and the hospital information system. To prevent the vertical transmission of EV-11 from mothers, infection control measures were implemented in the delivery room and nursery, allowing only one designated visitor during hospitalization. Disinfection procedures mirrored those of isolation zones, breastfeeding and rooming-in were prohibited, and electronic and paper-posters were displayed to raise awareness. Symptomatic neonates were promptly transferred to quarantined areas.
Figure 1.
Layout of the Sick Neonatal Room and Isolation Zones.
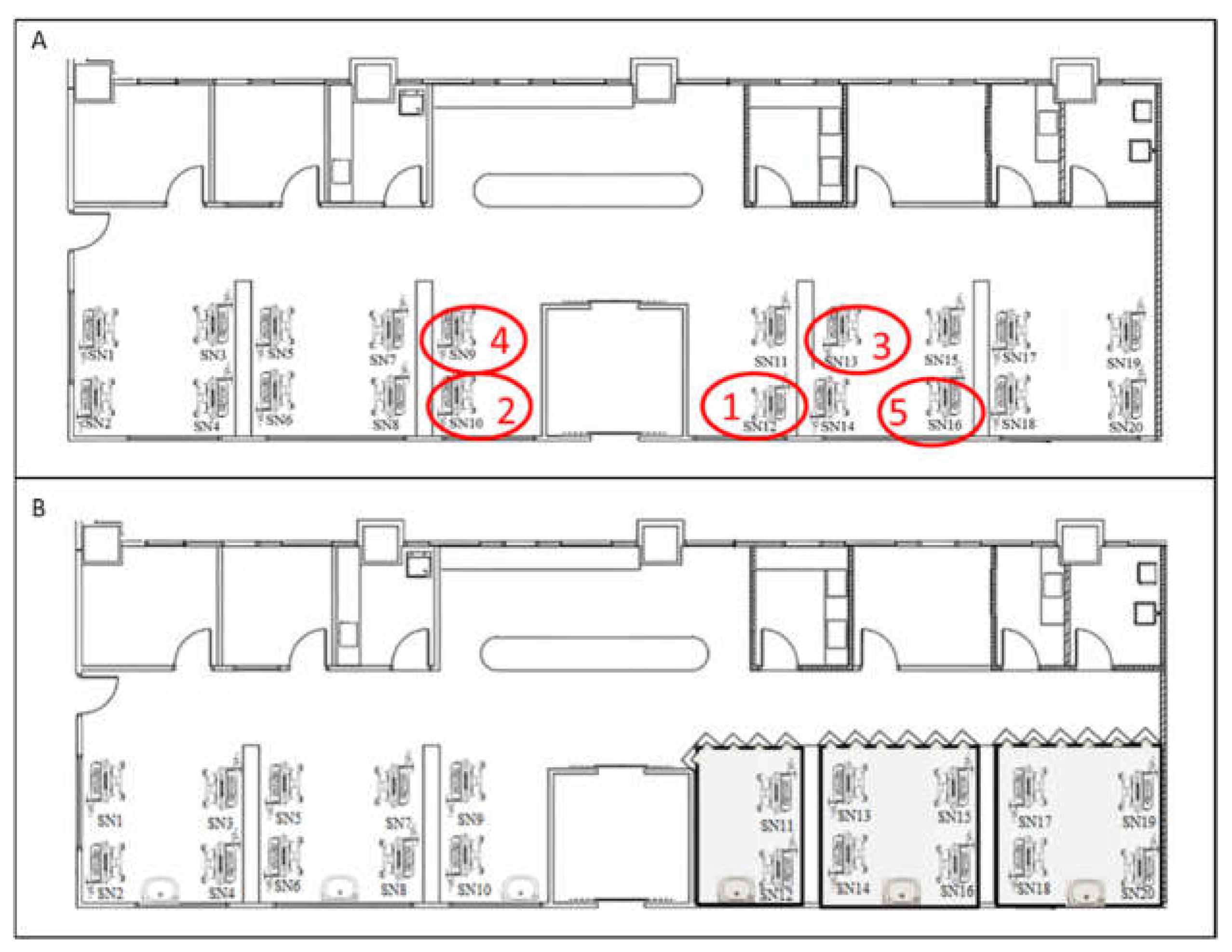
This figure illustrates the floor plan of the SN before (A) and after (B) the implementation of infection control measures. The positions of case 1 to case 5 were demonstrated in red circles. The case 1, case 2 and case 4 shared . The implementation of of infection control measures including setting up isolation zones (grey color) ;  : basin;
: basin;  : insulation board; and
: insulation board; and  :curtains. Soap, 75% alcohol, and 0.5% Chlorhexidine gluconate gluconate-based hand rubs were all available nearby any basins and incubators.
:curtains. Soap, 75% alcohol, and 0.5% Chlorhexidine gluconate gluconate-based hand rubs were all available nearby any basins and incubators.
: basin; : insulation board; and :curtains. Soap, 75% alcohol, and 0.5% Chlorhexidine gluconate gluconate-based hand rubs were all available nearby any basins and incubators. Figure 2.
Epidemiological Curve of the EV-11 Outbreak.
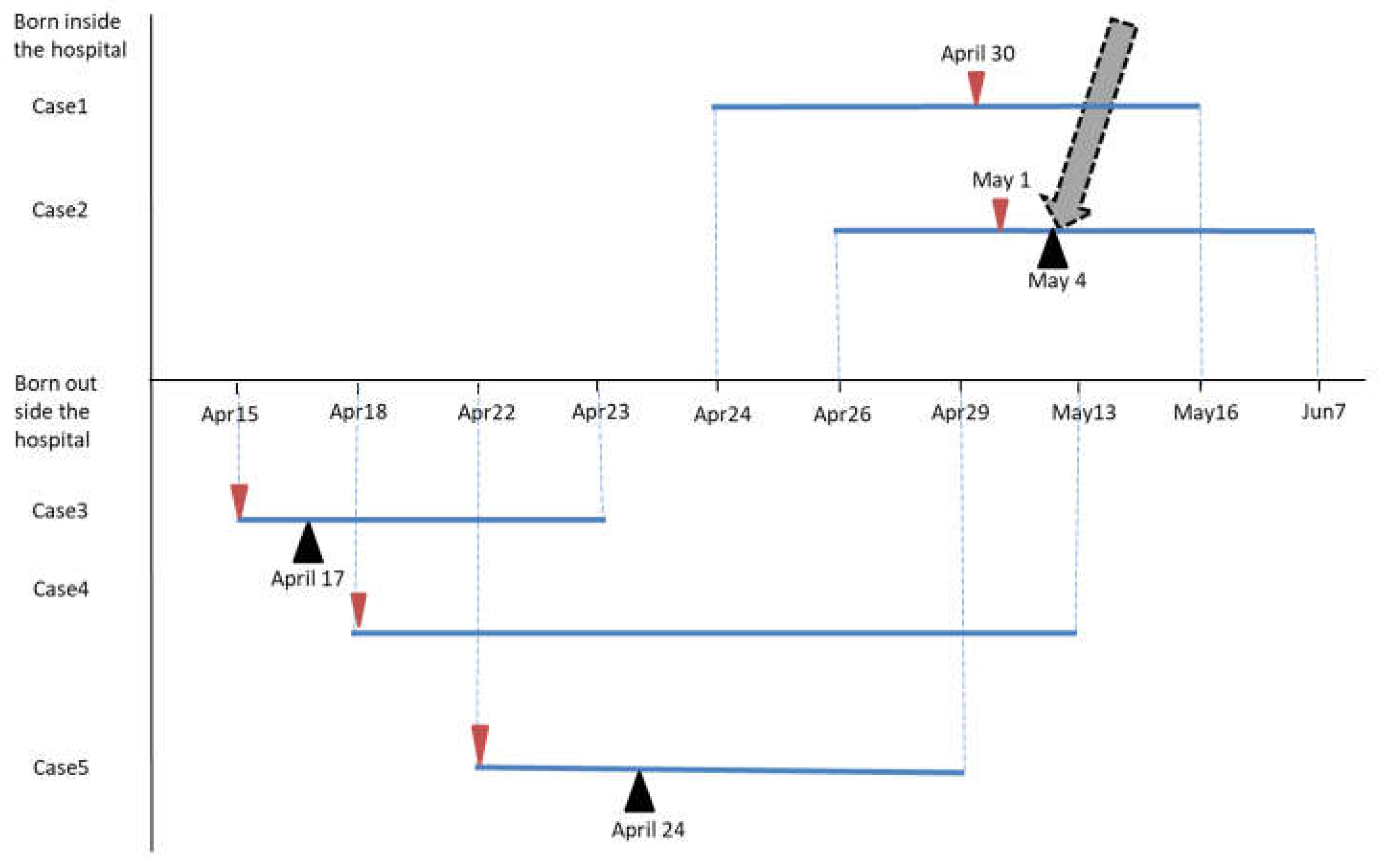
The epidemiological curve shows the timeline of symptom onset, hospital admissions, and infection control interventions during the EV-11 outbreak. It maps the dates on which patients exhibited symptoms, received diagnoses, and when containment measures were put in place. Blue line: The period of admission to the SN.  : Date at symptom onset.
: Date at symptom onset.  : Date at IVIG administered.
: Date at IVIG administered.  : date at infection control interventions.
: date at infection control interventions.
: Date at symptom onset. : Date at IVIG administered. : date at infection control interventions.4. Discussion
EV-11 can cause severe illnesses in neonates and infants, often leading to high morbidity and mortality rates. During the 2018 outbreak in Taiwan, 7 out of 8 severe cases resulted in death[13]. In May 2019, a nosocomial EV-11 infection in Guangzhou City, Guangdong Province, caused the deaths of five infants suffering from neonatal pneumonia and other underlying conditions [19]. Between July 2022 and April 2023, seven out of nine infants with severe EV-11 infection died in France [6]. Even though no mortality was recorded, the EV-11 outbreak discussed in this study presented a significant challenge, particularly given the vulnerability of neonates to severe complications from enterovirus infections. This study assesses the management of the outbreak, compares findings with previous research, and highlights the critical importance of stringent infection control measures in neonatal care settings.
The outbreak was initiated by Case 1, and Case 2 admitted to the SN, both of whom were neonates born inside the hospital presenting fever and EV-11 was isolated from their CSF. A further investigation found that Case 3, Case4, and Case 5 were born outside the hospital, and presented fever and later transferred without adequate isolation measures. Case 1 and Case 2 were highly possible to be infected by the Case 4, because hospitalization periods of those three cases showed overlapped. Additionally, Case1, Case 2 and Case 4 were cared by the same caregivers during the same shifts. Some caregivers may underestimate the danger of outbreak and not follow stricter isolation and control measures. This led to rapid intrahospital transmission, highlighting a significant lapse in infection control. The response of the hospital involved immediate establishment of a designated isolation zone, suspension of new patient admissions, and strict quarantine measures in controlling further spread.
Previous studies have underscored the high transmissibility of EV-11 in neonatal units[13,16,20,21]. For instance, Ho et al. documented a similar EV-11 outbreak in a NICU, where inadequate isolation practices contributed to widespread transmission. They reported that, of the 10 confirmed cases, three were likely community-acquired infections, while seven were healthcare-associated. The initial cases were not properly isolated, leading to the spread of EV-11 to seven others, likely transmitted by healthcare workers during the same shift[16]. The prompt identification and containment measures taken during the outbreak discussed in this study reflect lessons learned from previous such incidents, in which early intervention was the key to controlling viral spread.
Ho et al. highlighted the broad clinical spectrum of neonatal echovirus infections, ranging from mild febrile illness to severe multi-organ involvement [16]. Fang et al. also emphasized the role of multi-organ involvement in neonates, which contributes to the severity of enteroviral infections and the need for vigilant monitoring[22]. In this study, EV-11 symptoms included fever (5 cases); poor activity (3 cases); skin rash (3 cases); poor feeing (2 cases); hepatitis (1 case); thrombocytopenia (1 case). The clinical manifestations of EV-11 in infants primarily included fever, consistent with previous reports on neonatal enteroviral infections[16,19,23]. Skin rash associated with EV-11 was reported to be unique as vesicular skin lesions[24]. However, due to the limitation of this retrospective study, we could not make this conclusion. Moreover, skin rash was only found four out of sixty patients with EV-11 [13].
Non-specific symptoms such as poor feeding, and poor activity were also noted in this study, as reported in the literature[13,16,25]. A report analyzing genotypes of EV-11 in China from 1994 to 2017 collected specimens from patients with acute flaccid paralysis, and hand-foot-mouth disease. Interestingly, EV-11 could be detected in healthy individuals[26], and this could explain subjects with EV-11 show no symptoms.
Laboratory findings showed significantly elevated WBC counts and CRP, indicating systemic inflammation related to EV-11[13]. While echovirus types 6, 9, 14, 19, 21, 30, and 11 have been associated with hepatitis, particularly severe and fatal cases involving EV-11[13,16,27], only one case (Case 2) in this study showed elevated GOT and GPT levels. This suggests that the link between hepatitis and EV-11 infections may not be as consistent as previously thought. Although enterovirus infections, especially EV-9[28] and EV-30[29], are known to cause rhabdomyolysis with high CPK levels [30,31], CPK levels in these five EV-11 cases were normal, indicating that muscle tissue may not be involved in EV-11 infections in infants.
Myocarditis is a serious and potentially fatal complication of EV-11 infection, though its incidence was low in the studies by Ho et al.[16] (1/10) and Chen et al.[13] (1/37). Although Case 2 had elevated troponin I and BNP levels, his ejection fraction of 82% did not meet the criteria for myocarditis, and none of the infants in this study showed signs of myocarditis, suggesting that the incidence of myocarditis in EV-11-infected infants is uncommon.
Meningitis is a common and serious complication of EV-11 infection, and the incidence in the studies by Ho et al.[16] (5/10), Chen et al.[13] (10/37), Bina Rai et al. [32](2/11), and Grapin et al.[6] (5/9). All five cases were found EV-11 positive in the CSF specimens in this study, suggesting that EV-11 is prone to spread and enter the CNS in this local area.
The pathophysiology of echovirus 11 (EV-11) is not yet fully understood. As EV-11 initiates infection by targeting host cells using the cell surface protein decay-accelerating factor (DAF or CD55) [33] and β2-microglobulin[34]. Once attached, the virus enters the host cells through various endocytic pathways, including clathrin-mediated endocytosis, caveolin-mediated endocytosis, and macropinocytosis[35-37]. Upon entry, EV-11-containing vesicles are transported through the cytoplasm along microtubules or actin filaments to the endosome, where the virus undergoes uncoating. After uncoating, the viral genome is released into the cytoplasm and viral genome replication occurs within double-membrane vesicles in the cytoplasm, and new virions are ultimately released from the host cell through lysis[38]. Through those steps, EV-11 can disseminate from the gastrointestinal tract to the bloodstream, leading to systemic infections[39]. EV-11 causing severe complications such as myocarditis, encephalitis, and sepsis in neonates may attribute to their immature immune systems and increased vulnerability[13]. Recent research suggests that EV-11 can efficiently infect liver cells and macrophages through triggering inflammatory responses and pyroptosis, a form of programmed cell death associated with inflammation[14]. Future research should focus on evaluating multi-organ involvement in a larger cohort, which was not fully explored in this study. Understanding the full spectrum of the clinical impact of EV-11 is essential for improving neonatal care and outcomes.
The transmission of EV-11 is respiratory and fecal–oral spread. Although the source of the outbreak had not been identified, the infected inborn infants (Case 1 and 2) could have acquired the virus from infected asymptomatic caregivers through hand contacts, or through baby-to-baby transmission. The infection control measures taken during the EV-11 outbreak were comprehensive and proved effective in stopping viral transmission. Key actions included the establishment of a designated isolation zone, enforcement of strict hand hygiene protocols, and use of protective equipment. As EV-11 was reported to widespread circulation and increasing prevalence in local sewage[19], environmental cleaning protocols, particularly the use of sodium hypochlorite for surface disinfection, were implemented based on evidence from previous outbreaks. The efficacy of ethanol against echoviruses is rather good. Study shows that ethanol at 92.4% are effective against EV-11[40,41]. Although studies indicate that enteroviruses are resistant to most commercial alcohol-based disinfectants and require either a minimum of 95% ethanol to be effectively inactivated[42-44], however Chang et al. admitted that 95% ethanol still cannot fully inactivate EV71 and may be impractical for use in many instances[42]. Our findings align with those of previous studies that underscored the importance of hand-washing with soap and water, the use of gloves, 75% alcohol, and 0.5% Chlorhexidine gluconate gluconate-based hand rubs enhances compliance and effectiveness of infection control.
Ho et al. and Chen et al. highlighted that rigorous infection control practices, including the use of isolation rooms and strict hand hygiene, are crucial for controlling EV-11 outbreaks in NICUs[13,16] . The success of the outbreak management described in this study can be credited to the hospital’s swift implementation of these measures. In addition, the hospital’s decision to prohibit breastfeeding and rooming-in during the outbreak was essential for minimizing the risk of vertical transmission. This approach, although challenging, was supported by Chang et al.’s and Maus et al.’s , which showed that enteroviruses could be transmitted from mother to infant during delivery or through breastfeeding[45,46]. By enforcing these restrictions, the hospital significantly reduced the risk of mother-to-infant transmission, a critical factor in managing neonatal outbreaks.
Despite the successful containment of the outbreak, several limitations are noted. The study was conducted in a single hospital setting, which may limit the generalizability of the findings to other healthcare institutions. The small sample size of infected neonates also constrains the ability to draw broader conclusions about the epidemiology and clinical outcomes of EV-11 infections. In addition, the emotional and psychological impact on families due to the restrictions on breastfeeding and rooming-in was not assessed, which is an important consideration in managing such outbreaks. Lastly, while the infection control measures were effective, the long-term outcomes of the infected infants were not monitored, leaving gaps in the understanding of the full impact of the outbreak.
The successful control of this EV-11 outbreak provides several important lessons for managing future outbreaks in neonatal and pediatric settings. First, the importance of early detection cannot be overstated. The rapid identification of the index cases and the prompt implementation of isolation and quarantine measures were critical in preventing widespread transmission. The initial lapse in isolating the index case (Case 4) upon admission allowed the virus to spread, illustrating the need for stringent infection control protocols to be in place at all times. This includes the use of protective equipment, rigorous hand hygiene, and environmental cleaning, as well as clear protocols for managing suspected infectious cases.
Finally, this study underscores the value of public health education for managing infectious diseases. By educating healthcare workers and the public about the risks of enteroviral infections and the necessary precautions, the hospital was able to enhance compliance with infection control measures and prevent further transmission. This approach is consistent with the recommendations of the World Health Organization, which emphasize the role of public health education in controlling infectious disease outbreaks
5. Conclusions
The investigation and successful control of the EV-11 outbreak highlight the critical importance of rapid response, stringent infection control measures, and effective public health education in managing enteroviral outbreaks in neonatal settings. The proactive implementation of isolation protocols, continuous surveillance, and strict hygiene practices were key factors in preventing further spread and ensuring the safety of vulnerable neonates. However, the limitations of this study highlight the need for broader research and consideration of long-term effects on affected families and infants. The lessons learned from this outbreak, particularly the emphasis on the need for early detection, comprehensive infection control, and continuous public health education, can inform the management of future outbreaks. By applying these principles, healthcare institutions can effectively manage and control infectious disease outbreaks and protect vulnerable populations, such as neonates, from severe complications.
Author Contributions
Conceptualization, H. –C. F.; methodology, H.-C. C., H. –C. Y., K. –T. Y., and B. –C. S.; software, H.-C. C., H. –C. Y., K. –T. Y., and B. –C. S.; validation, K. –T. Y., and B. –C. S.; formal analysis, H.-C. C., and H. –C. Y.; investigation, M. –C. T.; resources, M. –C. T.; data curation, K. –T. Y., and B. –C. S.; writing—original draft preparation, H. –C. F.; writing—review and editing, H. –C. F., and M. –C. T.; visualization, H. –C. F.; supervision, M. –C. T.; project administration, H. –C. F.; funding acquisition, M. –C. T.. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by grants from the Tungs’ MetroHarbor Hospital (grant number: TTMHH-R1130039).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Tungs' Taichung Metro Harbor Hospital, No. 699, Sec. 8, Taiwan Blvd., Taichung City, 435, Taiwan (protocol code 112054 and date of approval:10t, January, 2024 ).
Informed Consent Statement
Because of the anonymized nature of the dataset, the need for informed consent was waived.
Data Availability Statement
The data are not publicly available due to privacy.
Acknowledgments
We would like to express our sincere gratitude to Kai-Ping Chang (Division of Pediatric Neurology, Department of Pediatrics, Taipei Veterans General Hospital, Taipei, Taiwan; Department of Pediatrics, Wei-Gong Memorial Hospital, Miaoli, Taiwan), Shyi-Jou Chen (Department of Pediatrics, Tri-Service General Hospital, Taipei, Taiwan), and Ching-Shiang Chi (Department of Pediatrics, Taichung Veterans General Hospital) for their helpful suggestions and comments.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of this study; in the collection, analysis, or interpretation of the data; in the writing of this manuscript; or in the decision to publish the results.
References
- Xie, Z.; Khamrin, P.; Maneekarn, N.; Kumthip, K. Epidemiology of Enterovirus Genotypes in Association with Human Diseases. Viruses 2024, 16. [CrossRef]
- Joki-Korpela, P.; Hyypia, T. Parechoviruses, a novel group of human picornaviruses. Ann Med 2001, 33, 466-471. [CrossRef]
- Gong, Y.N.; Yang, S.L.; Chen, Y.C.; Liu, Y.C.; Huang, Y.C.; Tsao, K.C. Novel intertypic recombination of Echovirus 11 in the Enterovirus species B. J Med Virol 2024, 96, e29323. [CrossRef]
- Philipson, L.; Rosen, L. Identification of a cytopathogenic agent called U-virus recovered from patients with non-diphtheritic croup and from day-nursery children. Arch Gesamte Virusforsch 1959, 9, 25-30. [CrossRef]
- Dahllund, L.; Nissinen, L.; Pulli, T.; Hyttinen, V.P.; Stanway, G.; Hyypia, T. The genome of echovirus 11. Virus Res 1995, 35, 215-222. [CrossRef]
- Grapin, M.; Mirand, A.; Pinquier, D.; Basset, A.; Bendavid, M.; Bisseux, M.; Jeannoel, M.; Kireche, B.; Kossorotoff, M.; L'Honneur, A.S.; et al. Severe and fatal neonatal infections linked to a new variant of echovirus 11, France, July 2022 to April 2023. Euro Surveill 2023, 28. [CrossRef]
- Wang, P.; Xu, Y.; Liu, M.; Li, H.; Wang, H.; Liu, Y.; Wang, B.; Xia, S.; Su, H.; Wei, M.; et al. Risk factors and early markers for echovirus type 11 associated haemorrhage-hepatitis syndrome in neonates, a retrospective cohort study. Front Pediatr 2023, 11, 1063558. [CrossRef]
- Modlin, J.F. Perinatal echovirus infection: insights from a literature review of 61 cases of serious infection and 16 outbreaks in nurseries. Rev Infect Dis 1986, 8, 918-926. [CrossRef]
- Lukashev, A.N.; Lashkevich, V.A.; Koroleva, G.A.; Ilonen, J.; Hinkkanen, A.E. Recombination in uveitis-causing enterovirus strains. J Gen Virol 2004, 85, 463-470. [CrossRef]
- Laassri, M.; Zagorodnyaya, T.; Hassin-Baer, S.; Handsher, R.; Sofer, D.; Weil, M.; Karagiannis, K.; Simonyan, V.; Chumakov, K.; Shulman, L. Evolution of echovirus 11 in a chronically infected immunodeficient patient. PLoS Pathog 2018, 14, e1006943. [CrossRef]
- Khetsuriani, N.; Lamonte, A.; Oberste, M.S.; Pallansch, M. Neonatal enterovirus infections reported to the national enterovirus surveillance system in the United States, 1983-2003. Pediatr Infect Dis J 2006, 25, 889-893. [CrossRef]
- Loconsole, D.; Centrone, F.; Sallustio, A.; Casulli, D.; Zagaria, R.; Sacco, D.; Colella, V.; Albano, N.; Caselli, D.; Cardinale, F.; et al. Echovirus 11 lineage I and other enteroviruses in hospitalized children with acute respiratory infection in Southern Italy, 2022- 2023. Int J Infect Dis 2024, 146, 107091. [CrossRef]
- Chen, Y.C.; Yang, S.L.; Yang, H.; Lin, T.Y.; Hsieh, Y.C.; Huang, K.A.; Kuo, C.Y.; Chiu, C.H.; Huang, Y.C.; Chu, S.M.; et al. Clinical characteristics of echovirus 11 and coxsackievirus B5 infections in Taiwanese children requiring hospitalization. J Microbiol Immunol Infect 2021, 54, 581-587. [CrossRef]
- Wang, C.; Yang, R.; Yang, F.; Han, Y.; Ren, Y.; Xiong, X.; Wang, X.; Bi, Y.; Li, L.; Qiu, Y.; et al. Echovirus 11 infection induces pyroptotic cell death by facilitating NLRP3 inflammasome activation. PLoS Pathog 2022, 18, e1010787. [CrossRef]
- Lai, S.K.C., C.M.; Kuo, H.W.; Liu, D.P. Neonatal enterovirus infection caused by echovirus 11 in Taiwan, 2018. Taiwan Epidemiol Bull 2018, 34, 336-340.
- Ho, S.Y.; Chiu, C.H.; Huang, Y.C.; Chen, C.J.; Lien, R.; Chu, S.M.; Huang, C.G.; Tsao, K.C.; Shih, S.R.; Hsu, J.F. Investigation and successful control of an echovirus 11 outbreak in neonatal intensive care units. Pediatr Neonatol 2020, 61, 180-187. [CrossRef]
- Potter, J.M.; Hickman, P.E.; Cullen, L. Troponins in myocardial infarction and injury. Aust Prescr 2022, 45, 53-57. [CrossRef]
- Law, Y.M.; Hoyer, A.W.; Reller, M.D.; Silberbach, M. Accuracy of plasma B-type natriuretic peptide to diagnose significant cardiovascular disease in children: the Better Not Pout Children! Study. J Am Coll Cardiol 2009, 54, 1467-1475. [CrossRef]
- Lu, J.; Kang, M.; Zeng, H.; Zhong, Y.; Fang, L.; Zheng, X.; Liu, L.; Yi, L.; Lin, H.; Peng, J.; et al. Tracking echovirus eleven outbreaks in Guangdong, China: a metatranscriptomic, phylogenetic, and epidemiological study. Virus Evol 2020, 6, veaa029. [CrossRef]
- Chen, J.H.; Chiu, N.C.; Chang, J.H.; Huang, F.Y.; Wu, K.B.; Lin, T.L. A neonatal echovirus 11 outbreak in an obstetric clinic. J Microbiol Immunol Infect 2005, 38, 332-337.
- Groneck, P.; Jahn, P.; Schuler-Luttmann, S.; Beyrer, K. [Neonatal enterovirus meningitis: transmission via parents during rooming-in and current epidemiology in Germany]. Z Geburtshilfe Neonatol 2011, 215, 1-5. [CrossRef]
- Fang, C.Z., X.; Huang, X.; Xu, F.; Zhao, D. Epidemiology and control measures of an outbreak of neonatal echovirus 11 infections in Guangdong, China: A retrospective analysis. Biosafety and Health 2023, 5, 227-232.
- Mostoufizadeh, M.; Lack, E.E.; Gang, D.L.; Perez-Atayde, A.R.; Driscoll, S.G. Postmortem manifestations of echovirus 11 sepsis in five newborn infants. Hum Pathol 1983, 14, 818-823. [CrossRef]
- Deseda-Tous, J.; Byatt, P.H.; Cherry, J.D. Vesicular lesions in adults due to echovirus 11 infections. Arch Dermatol 1977, 113, 1705-1706.
- Bose, C.L.; Gooch, W.M., 3rd; Sanders, G.O.; Bucciarelli, R.L. Dissimilar manifestations of intrauterine infection with echovirus 11 in premature twins. Arch Pathol Lab Med 1983, 107, 361-363.
- Li, J.; Yan, D.; Chen, L.; Zhang, Y.; Song, Y.; Zhu, S.; Ji, T.; Zhou, W.; Gan, F.; Wang, X.; et al. Multiple genotypes of Echovirus 11 circulated in mainland China between 1994 and 2017. Sci Rep 2019, 9, 10583. [CrossRef]
- Lefterova, M.I.; Rivetta, C.; George, T.I.; Pinsky, B.A. Severe hepatitis associated with an echovirus 18 infection in an immune-compromised adult. J Clin Microbiol 2013, 51, 684-687. [CrossRef]
- Tanaka, T.; Takada, T.; Takagi, D.; Takeyama, N.; Kitazawa, Y. Acute renal failure due to rhabdomyolysis associated with echovirus 9 infection: a case report and review of literature. Jpn J Med 1989, 28, 237-242. [CrossRef]
- Sousa, I.P., Jr.; Burlandy, F.M.; Lima, S.T.S.; Maximo, A.C.B.; Figueiredo, M.A.A.; Maia, Z.; da Silva, E.E. Echovirus 30 detection in an outbreak of acute myalgia and rhabdomyolysis, Brazil 2016-2017. Clin Microbiol Infect 2019, 25, 252 e255-252 e258. [CrossRef]
- Nazir, H.F.; Al Yazidi, L. Disseminated Enterovirus Infection Complicated by Rhabdomyolysis in a Child with Acute Lymphoblastic Leukemia. Oman Med J 2024, 39, e617. [CrossRef]
- Soliman, A.; Bisht, S.; Jeyamurugan, K.; Balasundaram, P.; Basak, R. Severe Rhabdomyolysis in a Pediatric Patient after Coxsackie B Virus Infection without Acute Renal Failure: A Case Report. Cureus 2020, 12, e7126. [CrossRef]
- Bina Rai, S.; Wan Mansor, H.; Vasantha, T.; Norizah, I.; Chua, K.B. An outbreak of echovirus 11 amongst neonates in a confinement home in Penang, Malaysia. Med J Malaysia 2007, 62, 223-226.
- Bergelson, J.M.; Chan, M.; Solomon, K.R.; St John, N.F.; Lin, H.; Finberg, R.W. Decay-accelerating factor (CD55), a glycosylphosphatidylinositol-anchored complement regulatory protein, is a receptor for several echoviruses. Proc Natl Acad Sci U S A 1994, 91, 6245-6248. [CrossRef]
- Ward, T.; Powell, R.M.; Pipkin, P.A.; Evans, D.J.; Minor, P.D.; Almond, J.W. Role for beta2-microglobulin in echovirus infection of rhabdomyosarcoma cells. J Virol 1998, 72, 5360-5365. [CrossRef]
- Kim, C.; Bergelson, J.M. Echovirus 7 entry into polarized intestinal epithelial cells requires clathrin and Rab7. mBio 2012, 3. [CrossRef]
- Krieger, S.E.; Kim, C.; Zhang, L.; Marjomaki, V.; Bergelson, J.M. Echovirus 1 entry into polarized Caco-2 cells depends on dynamin, cholesterol, and cellular factors associated with macropinocytosis. J Virol 2013, 87, 8884-8895. [CrossRef]
- Xing, L.; Huhtala, M.; Pietiainen, V.; Kapyla, J.; Vuorinen, K.; Marjomaki, V.; Heino, J.; Johnson, M.S.; Hyypia, T.; Cheng, R.H. Structural and functional analysis of integrin alpha2I domain interaction with echovirus 1. J Biol Chem 2004, 279, 11632-11638. [CrossRef]
- Robinson, M.; Schor, S.; Barouch-Bentov, R.; Einav, S. Viral journeys on the intracellular highways. Cell Mol Life Sci 2018, 75, 3693-3714. [CrossRef]
- Zhong, Q.; Carratala, A.; Shim, H.; Bachmann, V.; Jensen, J.D.; Kohn, T. Resistance of Echovirus 11 to ClO(2) Is Associated with Enhanced Host Receptor Use, Altered Entry Routes, and High Fitness. Environ Sci Technol 2017, 51, 10746-10755. [CrossRef]
- Drulak, M.; Wallbank, A.M.; Lebtag, I. The relative effectiveness of commonly used disinfectants in inactivation of echovirus 11. J Hyg (Lond) 1978, 81, 77-87. [CrossRef]
- Kurtz, J.B. Virucidal effect of alcohols against echovirus 11. Lancet 1979, 1, 496-497. [CrossRef]
- Chang, S.C.; Li, W.C.; Huang, K.Y.; Huang, Y.C.; Chiu, C.H.; Chen, C.J.; Hsieh, Y.C.; Kuo, C.Y.; Shih, S.R.; Lin, T.Y. Efficacy of alcohols and alcohol-based hand disinfectants against human enterovirus 71. J Hosp Infect 2013, 83, 288-293. [CrossRef]
- Kampf, G. Efficacy of ethanol against viruses in hand disinfection. J Hosp Infect 2018, 98, 331-338. [CrossRef]
- Steinmann, J.; Nehrkorn, R.; Meyer, A.; Becker, K. Two in-vivo protocols for testing virucidal efficacy of handwashing and hand disinfection. Zentralbl Hyg Umweltmed 1995, 196, 425-436.
- Chang, M.L.; Tsao, K.C.; Huang, C.C.; Yen, M.H.; Huang, C.G.; Lin, T.Y. Coxsackievirus B3 in human milk. Pediatr Infect Dis J 2006, 25, 955-957. [CrossRef]
- Maus, M.V.; Posencheg, M.A.; Geddes, K.; Elkan, M.; Penaranda, S.; Oberste, M.S.; Hodinka, R.L. Detection of echovirus 18 in human breast milk. J Clin Microbiol 2008, 46, 1137-1140. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



