
Submitted:
29 September 2024
Posted:
30 September 2024
You are already at the latest version
Abstract
Objective: This study aims to construct an early risk warning model to predict the risk of treatment failure in patients undergoing sequential High-Flow Nasal Cannula (HFNC) oxygen therapy following mechanical ventilation weaning. Methods: A retrospective analysis was conducted on clinical data from 145 patients who received HFNC treatment in the Emergency Intensive Care Unit of the Third People's Hospital of Bengbu City from June 2018 to June 2023. A wide range of indicators including general information, comorbidities, laboratory test results, vital signs, disease-related scores, and oxygenation data were collected. Data analysis was performed using R software, starting with the Lasso regression to filter features related to treatment outcomes. Patients were divided into a training set (70%) and a validation set (30%) using random grouping software. The Random Forest algorithm was then employed to evaluate and rank the important features related to outcome indicators. The predictive efficiency and stability of the model were assessed through the Receiver Operating Characteristic (ROC) curve, calibration curve, and decision curve analysis, culminating in the construction of an early risk warning nomogram. Results: The study found that the Random Forest model exhibited high predictive accuracy in the training set (AUC=0.98) and good stability in the validation set (AUC=0.84). Key feature variables identified by the model, such as APACHE II score, BNP, NLR, mROX, and SOFA, were found to significantly impact the prediction of HFNC treatment failure. Based on these variables, an early warning nomogram was further developed, providing clinicians with a convenient and effective risk assessment tool. Conclusion: This study has constructed an early risk warning model based on the Random Forest algorithm, capable of effectively predicting the risk of HFNC treatment failure. The model's high predictive efficiency and stability offer strong support for clinical decision-making, contributing to personalized treatment and improved patient outcomes. Future research should aim to expand the sample size, perform multicenter validation, and explore the integration of the model into Clinical Decision Support Systems for real-time risk assessment and intervention.
Keywords:
Acute Respiratory Failure
; High-Flow Nasal Cannula oxygen therapy
; Random Forest
; Early Risk Warning
Introduction
Acute Respiratory Failure (ARF) is a clinical syndrome caused by various etiologies, resulting in significant impairments in patients’ ventilation and lung function. In this condition, patients are unable to perform effective spontaneous gas exchange, leading to a series of physiological and metabolic disorders [1]. The current clinical treatment primarily relies on mechanical ventilation, which effectively restores patients’ ventilation, improves gas exchange, and maintains the required arterial oxygen levels [2]. As patients’ respiratory function gradually recovers, a transition to weaning and subsequent treatment becomes necessary. In this process, High-Flow Nasal Cannula (HFNC) oxygen therapy has become a crucial sequential therapy following mechanical ventilation globally [3].
HFNC offers several advantages in the treatment of critically ill patients with acute respiratory failure. Its heating system improves ciliary function, promoting sputum clearance; the low-level positive airway pressure generated by high oxygen flow reduces respiratory rate and inspiratory resistance, while providing constant oxygen concentration to improve oxygenation. Additionally, it preserves patients’ ability to cough, reduces the risk of aspiration, and decreases complications such as ventilator-associated pneumonia, barotrauma, or secondary infections. HFNC can deliver heated and humidified oxygen at rates of 30-60 L/min, offering good comfort and tolerability, effectively relieving respiratory distress and improving oxygenation [4,5,6]. In recent years, this technology has been widely applied and promoted domestically.
However, despite the significant success of HFNC in respiratory support, its application in sequential therapy following mechanical ventilation weaning still faces many challenges. Mechanical ventilation weaning is a critical step in the treatment of respiratory failure, requiring precise care and close monitoring to ensure a smooth transition to spontaneous breathing [7]. Currently, there is still insufficient understanding regarding the optimal application of HFNC during this stage and how to predict and manage potential complications after weaning. If treatment failure occurs, it significantly impacts patient prognosis, with high-flow oxygen therapy failure typically defined as requiring a switch to invasive ventilation or resulting in death during HFNC. Studies have shown that mortality rates among patients who fail high-flow oxygen therapy can reach 28% to 48% [8]. Therefore, assessing and predicting the effectiveness of high-flow oxygen therapy in critically ill patients to avoid reintubation remains a major challenge for clinical staff.
To address this issue, this study aims to develop an early warning model using the Random Forest (RF) algorithm developed by Leo Breiman and Adele Cutler [9] to assist clinicians in identifying patients at high risk of high-flow oxygen therapy failure. The Random Forest algorithm is a powerful machine learning tool that combines multiple decision trees to improve predictive accuracy and reliability. Compared to traditional logistic regression models, Random Forest demonstrates significant advantages in reducing the risk of overfitting, offering greater flexibility, and facilitating the identification of important features [10]. By constructing a Random Forest-based risk prediction model, this study aims to accurately predict which patients receiving high-flow oxygen therapy after mechanical ventilation weaning are at higher risk of treatment failure. This will provide clinicians with more precise decision-making support, help improve treatment outcomes, reduce unnecessary medical interventions, and ultimately enhance patients’ quality of life and prognosis.
1. Methods
1.1. Study Subjects
The study included patients who received High-Flow Nasal Cannula (HFNC) sequential therapy after mechanical ventilation weaning in the Intensive Care Unit (ICU) of our hospital between June 2018 and June 2023. The inclusion criteria were: (1) age ≥18 years; (2) dependence on mechanical ventilation for assisted ventilation; (3) intubation via oral endotracheal tube; (4) weaning method using T-tube; (5) duration of mechanical ventilation >48 hours; and (6) patients meeting the weaning criteria. Respiratory criteria: oxygenation index >150-200 mmHg (1 mmHg = 0.133 kPa) under conditions of fraction of inspired oxygen (FiO2) ≤50% and positive end-expiratory pressure (PEEP) ≤8 cm H2O, with normal or baseline arterial partial pressure of carbon dioxide (PaCO2), and the patient able to trigger inspiration. Cardiovascular criteria: no evidence of myocardial ischemia, heart rate not exceeding 140 beats per minute, and stable blood pressure with or without minimal use of vasopressors. Neurological status: Glasgow Coma Scale (GCS) score ≥10 points [11]. Complications resolved: no fever or significant electrolyte disturbances. Exclusion criteria: (1) pregnant or postpartum women; (2) patients after cardiopulmonary resuscitation, with severe chest or abdominal inflammation causing abdominal hypertension or affecting diaphragm movement; (3) patients with unilateral lung ventilation; (4) incomplete clinical or laboratory data; (5) patients unable to cooperate with sequential therapy.
1.2. Study Content
1.2.1. HFNC Sequential Therapy Protocol
The appropriate large-bore nasal cannula size was selected based on the size of the patient’s nostrils, with an initial flow rate set at 50 L/min (adjusted based on patient comfort and tolerance). The heated and humidified mixed gas was delivered through RT200 tubing via MR850, with FiO2 adjusted to maintain oxygen saturation (SpO2) between 90% and 94%. If the patient tolerated HFNC, continuous therapy was administered, with intermittent use based on the clinical situation. During HFNC pauses, oxygen was delivered via nasal cannula, with FiO2 adjusted to maintain SpO2 between 88% and 92%. If the patient’s respiratory rate (RR) was <25 breaths/min, there was no significant respiratory distress or need for accessory respiratory muscles, and arterial blood gas analysis indicated either baseline levels or a reduction in PaCO2 of more than 20 mmHg from pre-treatment levels, HFNC was discontinued. If clinically necessary, HFNC therapy could be resumed. Successful treatment was defined as no need for noninvasive ventilation (NIV), HFNC, or invasive mechanical ventilation within 72 hours after HFNC discontinuation.
The indications for reintubation and mechanical ventilation were: (1) pH ≤7.20 with a progressive increase in PaCO2 during treatment; (2) refractory hypoxemia (arterial oxygen partial pressure (PaO2) <50 mmHg under adequate oxygen therapy); (3) impaired consciousness, such as lethargy, coma, or delirium; (4) respiratory or cardiac arrest; (5) respiratory suppression (respiratory rate <8 breaths/min) or severe respiratory distress (respiratory rate >40 breaths/min).
1.2.2. Data Collection
Collected data included general information [gender, age, body mass index (BMI)], comorbidities [such as hypertension, diabetes, chronic obstructive pulmonary disease (COPD)], laboratory indicators [such as white blood cell count (WBC), C-reactive protein (CRP), albumin, procalcitonin (PCT), brain natriuretic peptide (BNP), neutrophil-to-lymphocyte ratio (NLR)], vital signs [such as respiratory rate, pulse rate (PR), oxygen saturation], disease-related scores [Sequential Organ Failure Assessment (SOFA) [12], Acute Physiology and Chronic Health Evaluation (APACHE II) [13], Glasgow Coma Scale, and Modified Respiratory Rate Oxygenation Index (mROX) [14]], oxygenation data [duration of mechanical ventilation (hours), FiO2], and outcome indicators [treatment success, failure (reintubation, death)].
1.3. Statistical Analysis
Data were analyzed using R software version 4.3.2 (https://www.r-project.org/). Continuous variables were compared using the t-test, and categorical variables were compared using the chi-square test. The Least Absolute Shrinkage and Selection Operator (Lasso) method was first used to select the features most strongly associated with treatment outcomes. The Random Forest algorithm was then used to rank the importance of outcome-related features and construct the Random Forest prediction model. Model stability and predictive performance were evaluated in both the training and validation sets using the area under the receiver operating characteristic curve (AUC), calibration curve, and decision curve analysis (DCA). The top 5 ranked features were included in a Logistic regression model to construct the early warning model. The following R packages were used in this study: “readxl, glmnet, randomForest, DALEX, rms, ggDCA, finalfit, flextable.”
2. Results
2.1. General Information of the Included Patients
A total of 145 patients were included in this study, with 126 cases of treatment success and 19 cases of treatment failure. The average age of the success group was 56.50 years, while the failure group averaged 59.32 years. In the success group, 66 patients were male, accounting for 52.38%, and in the failure group, 10 patients were male, accounting for 52.63%. There were statistically significant differences between the two groups in terms of BNP, mROX score, APACHE II score, and SOFA score, while no significant differences were found in other indicators. Specific details are shown in Table 1.
2.2. Lasso Regression Analysis for Feature Selection Related to Outcomes
Through Lasso analysis, the study identified feature variables associated with outcome indicators. Figure 1A shows the cross-validation curve for Lasso regression, yielding two fitted equations, with LogLambda_min = -4.073 representing the best model, which includes 10 feature variables (WBC, NLR, CRP, BNP, mROX, APACHE II, SOFA, hypertension, diabetes, and chronic heart failure). Figure 1B illustrates the path of regression coefficients for the feature variables. As the parameter LogLambda increases, the y-axis (regression coefficients) progressively converges, eventually to zero. At LogLambda = -4.073, 10 non-zero regression coefficients remained.
2.3. Random Forest Analysis to Identify Important Features Related to Outcomes
Based on the results of the Lasso analysis, the study retained the above 10 feature variables for further Random Forest analysis. The data were first randomly split based on outcome indicators into a training set (70%, 101 cases) and a validation set (30%, 44 cases). Table 2 compares the feature variables between the training and validation sets, showing no significant statistical differences between the two groups. Figure 2A displays the important features from the Random Forest analysis of the training set, ranked in the following order of importance: APACHE II, BNP, NLR, mROX, SOFA, WBC, and CRP. Figure 2B illustrates the SHAP distribution values for each feature variable from the Random Forest analysis. SHAP (Shapley Additive Explanations) is an advanced method of interpretable machine learning that shows the weight of each feature variable in the analysis. The results intuitively demonstrate how each feature influences the treatment outcome. The study further assessed the predictive performance and stability of the Random Forest analysis results. The results showed that the training set had an AUC of 0.98 (0.94-1.00), while the validation set had an AUC of 0.84 (0.62-0.93) (Figure 3A). The calibration curve (Figure 3B) and decision curve (Figure 3C) indicated that the model has good stability and clinical applicability.
2.4. Construction of an Early Warning Model Nomogram
Based on the results of the Random Forest analysis, this study further constructed a nomogram for an early warning model. The top 5 ranked feature variables from the Random Forest analysis were included in a Logistic regression to build the early warning model. Figure 4A presents the nomogram of the model, where the probability of treatment success or failure can be derived based on the values of each variable, assisting clinicians in making early interventions. Figure 4B shows the forest plot of the predictive model, displaying the odds ratio (OR) for each feature variable, with APACHE II at 1.59, BNP at 1.01, NLR at 1.04, mROX at 0.71, and SOFA at 1.26.
Discussion
This study used the Random Forest algorithm to construct an early risk warning model aimed at predicting the risk of failure in sequential High-Flow Nasal Cannula (HFNC) therapy after mechanical ventilation weaning. Through the analysis of data from 145 patients, the study found that the warning model demonstrated high predictive accuracy, with an AUC of 0.98 in the training set and 0.84 in the validation set. The calibration curve and decision curve showed that the model has good stability and clinical applicability. Based on the Random Forest algorithm, this study further developed a nomogram for the early warning model, providing a convenient and effective tool for clinical use, facilitating the early identification of high-risk patients and enabling more precise treatment decisions.
The Random Forest algorithm is widely recognized for its efficiency in handling large datasets and its ability to process complex data structures. The Random Forest (RF) algorithm is now extensively used for risk factor screening and prediction model construction. For example, Giri J et al. [15] used RF to construct a model for predicting early mortality risk in critically ill patients, while Daiquan Gao et al. [16] combined Lasso analysis with RF to develop a model predicting poor functional outcomes in patients with cerebral hemorrhage, both demonstrating good predictive performance.
In this study, Random Forest analysis showed that APACHE II, BNP, NLR, mROX, and SOFA had significant impacts on predicting HFNC treatment failure. Particularly, the APACHE II score, the most important feature, was significantly associated with treatment failure risk. APACHE II is a widely used scoring system in critical care that considers both physiological abnormalities and chronic health conditions to assess the severity of a patient’s illness and predict in-hospital mortality. Wei Lu et al. [17] found that the APACHE II score was significantly positively correlated with mechanical ventilation pressure parameters in patients with Acute Respiratory Distress Syndrome (ARDS) and had high diagnostic value for the prognosis of ARDS patients. Similarly, a meta-analysis by Wenrui Li et al. [18] involving 22,304 patients assessed the risk factors for reintubation in mechanically ventilated patients and found that a high APACHE II score was a significant risk factor for reintubation. In this study, the APACHE II score was the most critical feature, and higher scores were associated with an increased risk of HFNC treatment failure. This may be because patients with higher APACHE II scores are physiologically more vulnerable and less tolerant and responsive to treatment, increasing the likelihood of HFNC failure.
BNP is a biomarker released during cardiac stress, commonly used to diagnose and assess heart failure. Elevated BNP levels reflect the extent of cardiac dysfunction [19]. In this study, BNP was one of the feature variables, and its elevation was associated with an increased risk of HFNC treatment failure. This suggests that cardiac insufficiency is an important factor contributing to HFNC failure, possibly because patients with poor cardiac function may be less able to tolerate the potential cardiac load increase induced by high-flow oxygen therapy, thus increasing the risk of treatment failure [20].
NLR is a simple biomarker of inflammation and immune status. An inflammatory response can trigger an increase in circulating neutrophils and a decrease in lymphocytes, leading to elevated NLR levels. The NLR index has significant prognostic value for various conditions, including inflammation, cancer, and autoimmune diseases [21,22,23]. Elevated NLR is typically associated with enhanced inflammatory response, increased risk of infection, and suppressed immune function. In this study, NLR was identified as a feature variable predicting HFNC failure, reflecting patients’ inflammatory status and infection risk, both of which can affect the outcome of HFNC treatment.
The ROX index, derived from SpO2, FiO2, and RR, has previously been reported to have predictive value for HFNC outcomes in patients with pneumonia-induced respiratory failure [24]. However, a meta-analysis by Xiaoyang Zhou et al. [25] pointed out that the ROX index has limitations in early prediction of HFNC failure, including low sensitivity and specificity and a delayed time window. Compared to ROX, the modified ROX (mROX) index, which uses PaO2 instead of SpO2, was included in this study. A lower mROX value indicates poorer oxygenation and higher respiratory load. Roca O et al. [26] evaluated the predictive value of ROX-related indices in HFNC outcomes, showing that the mROX index had a stronger association with HFNC failure in elderly patients with respiratory failure. In this study, the inclusion of the mROX index in the comprehensive analysis showed that its decrease was associated with HFNC failure risk, consistent with previous research.
The SOFA score is a scoring system used to assess organ dysfunction in critically ill patients. Higher SOFA scores indicate more severe organ dysfunction [27]. In this study, SOFA was one of the feature variables, and higher SOFA scores were associated with HFNC failure risk. Patients with severe organ dysfunction are less tolerant and responsive to most treatments, and organ failure may lead to HFNC treatment failure.
The findings of this study are consistent with existing literature, indicating that patients who fail high-flow oxygen therapy tend to have higher levels of inflammation and poorer physiological function. The results align with the majority of previous research, but this study differs by applying machine learning techniques, offering a more precise and personalized risk assessment tool, which aids clinicians in making more targeted decisions during the weaning process. This innovation is rarely seen in prior studies. The methods and findings of this study provide new directions and ideas for future related research.
However, this study has some limitations. First, the sample size is relatively small, which may affect the generalizability and predictive accuracy of the model. Second, the study was conducted at a single center, which may introduce center-specific bias. Future studies need to validate the model in multicenter and diverse populations. Additionally, the model construction relies on clinical and laboratory indicators, and future research should consider incorporating more physiological signals and biomarkers to further improve the predictive performance of the model.
Conclusion
This study used the Random Forest algorithm to construct an early risk warning model for predicting the risk of HFNC sequential therapy failure after mechanical ventilation weaning. The model demonstrated good predictive performance and clinical applicability in both the training and validation sets. The key feature variables included APACHE II, BNP, NLR, mROX, and SOFA, all of which were closely related to HFNC failure risk, providing strong support for clinical decision-making. Despite the limitations in sample size and center specificity, this study utilized machine learning algorithms to offer a precise risk assessment tool, helping clinicians make more targeted decisions during HFNC therapy. Future research should focus on expanding the sample size, conducting multicenter validation, and integrating the model into clinical decision support systems to enable real-time risk assessment and intervention, thereby improving the success rate of HFNC therapy and patient prognosis.
References
- Rochwerg, B.; Brochard, L.; Elliott, M.W.; et al. Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J. 2017, 50, 1602426. [Google Scholar] [CrossRef] [PubMed]
- Piraino, T. Noninvasive Respiratory Support in Acute Hypoxemic Respiratory Failure. Respir Care. 2019, 64, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Rochwerg, B.; Granton, D.; Wang, D.X.; et al. High flow nasal cannula compared with conventional oxygen therapy for acute hypoxemic respiratory failure: a systematic review and meta-analysis. Intensive Care Med. 2019, 45, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.; Gu, S.; Lei, W.; et al. High-flow nasal cannula versus conventional oxygen therapy in acute COPD exacerbation with mild hypercapnia: a multicenter randomized controlled trial. Crit Care. 2022, 26, 109 Published 2022 Apr 15. [Google Scholar] [CrossRef]
- Frat, J.P.; Marie, D.; Thille, A.W. Acute respiratory failure: nonintubation assist methods for the acutely deteriorating patient. Curr Opin Crit Care. 2019, 25, 591–596. [Google Scholar] [CrossRef]
- Oczkowski, S.; Ergan, B.; Bos, L.; et al. ERS clinical practice guidelines: high-flow nasal cannula in acute respiratory failure. Eur Respir J. 2022, 59, 2101574. [Google Scholar] [CrossRef]
- Hernández, G.; Paredes, I.; Moran, F.; et al. Effect of postextubation noninvasive ventilation with active humidification vs high-flow nasal cannula on reintubation in patients at very high risk for extubation failure: a randomized trial [published correction appears in Intensive Care Med. 2023 Mar;49, 385]. Intensive Care Med. 2022, 48, 1751–1759. [Google Scholar]
- Frat, J.P.; Thille, A.W.; Mercat, A.; et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med. 2015, 372, 2185–2196. [Google Scholar] [CrossRef]
- Liu, X.; Song, M.; Tao, D.; et al. Random forest construction with robust semisupervised node splitting. IEEE Trans Image Process. 2015, 24, 471–483. [Google Scholar] [CrossRef]
- Wallace, M.L.; Mentch, L.; Wheeler, B.J.; et al. Use and misuse of random forest variable importance metrics in medicine: demonstrations through incident stroke prediction. BMC Med Res Methodol. 2023, 23, 144. [Google Scholar] [CrossRef]
- Middleton, P.M. Practical use of the Glasgow Coma Scale; a comprehensive narrative review of GCS methodology. Australas Emerg Nurs J. 2012, 15, 170–83. [Google Scholar] [CrossRef] [PubMed]
- Lambden, S.; Laterre, P.F.; Levy, M.M.; Francois, B. The SOFA score-development, utility and challenges of accurate assessment in clinical trials. Crit Care. 2019, 23, 374. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Jin, Z.; Deng, J.; She, Y.; Zhong, Y.; Sun, W.; Ren, Y.; Cao, N.; Chen, C. Development and validation of a deep learning model to predict the survival of patients in ICU. J Am Med Inform Assoc. 2022, 29, 1567–1576. [Google Scholar] [CrossRef] [PubMed]
- Ai, T.; Zhang, Z.; Tan, Z.; Shi, Z.; Li, H.; Zhang, S.; Zhao, X.; Yao, Y.; Li, W.; Gao, Y.; Zhu, M. Modified Respiratory Rate Oxygenation Index: An Early Warning Index for the Need of Intubation in COVID-19 Patients with High-Flow Nasal Cannula Therapy. J Emerg Med. 2023, 65, e93–e100. [Google Scholar] [CrossRef]
- Giri, J.; Al-Lohedan, H.A.; Mohammad, F.; et al. A Comparative Study on Predication of Appropriate Mechanical Ventilation Mode through Machine Learning Approach. Bioengineering 2023, 10, 418. [Google Scholar] [CrossRef]
- Gao, D.; Feng, W.; Qiao, Y.; Jiang, X.; Zhang, Y. Development and validation of a random forest model to predict functional outcome in patients with intracerebral hemorrhage. Neurol Sci. 2023, 44, 3615–3627. [Google Scholar] [CrossRef]
- Lu, W.; Zhang, J.; Qiu, Y.; Fei, N.; Yin, L. Correlations between APACHE-II score and pressure parameters of mechanical ventilation in patients with ARDS and their value in prognostic evaluation. Pak J Med Sci. 2023, 39, 1584–1588. [Google Scholar] [CrossRef]
- Li, W.; Zhang, Y.; Wang, Z.; Jia, D.; Zhang, C.; Ma, X.; Han, X.; Zhao, T.; Zhang, Z. The risk factors of reintubation in intensive care unit patients on mechanical ventilation: A systematic review and meta-analysis. Intensive Crit Care Nurs. 2023, 74, 103340. [Google Scholar] [CrossRef]
- González, A.; Schelbert, E.B.; Díez, J.; Butler, J. Myocardial Interstitial Fibrosis in Heart Failure: Biological and Translational Perspectives. J Am Coll Cardiol. 2018, 71, 1696–1706. [Google Scholar] [CrossRef]
- Cortegiani, A.; Longhini, F.; Carlucci, A.; Scala, R.; Groff, P.; Bruni, A.; Garofalo, E.; Taliani, M.R.; Maccari, U.; Vetrugno, L.; Lupia, E.; Misseri, G.; Comellini, V.; Giarratano, A.; Nava, S.; Navalesi, P.; Gregoretti, C. High-flow nasal therapy versus noninvasive ventilation in COPD patients with mild-to-moderate hypercapnic acute respiratory failure: study protocol for a noninferiority randomized clinical trial. Trials. 2019, 20, 450. [Google Scholar] [CrossRef]
- Capone, M.; Giannarelli, D.; Mallardo, D.; et al. Baseline neutrophil-to-lymphocyte ratio (NLR) and derived NLR could predict overall survival in patients with advanced melanoma treated with nivolumab. J Immunother Cancer. 2018, 6, 74. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Xie, T.; Chen, Y.; Zhou, Y.; Han, X. The Effects of Bivalirudin and Ordinary Heparin on the Incidence of Bleeding Events and the Level of Inflammation after Interventional Therapy for Acute Myocardial Infarction. Altern Ther Health Med. Published online May 24, 2024.
- VIKAS,GUPTA, VIKRAM,CHAUDHARI, SHAILESH V.,SHRIKHANDE, et al. Does Preoperative Serum Neutrophil to Lymphocyte Ratio (NLR), Platelet to Lymphocyte Ratio (PLR), and Lymphocyte to Monocyte Ratio (LMR) Predict Prognosis Following Radical Surgery for Pancreatic Adenocarcinomas? Results of a Retrospective Study. Journal of gastrointestinal cancer 2022, 53, 641–648.
- Roca, O.; Messika, J.; Caralt, B.; García-de-Acilu, M.; Sztrymf, B.; Ricard, J.D.; Masclans, J.R. Predicting success of high-flow nasal cannula in pneumonia patients with hypoxemic respiratory failure: The utility of the ROX index. J Crit Care. 2016, 35, 200–5. [Google Scholar] [CrossRef]
- Zhou, X.; Liu, J.; Pan, J.; Xu, Z.; Xu, J. The ROX index as a predictor of high-flow nasal cannula outcome in pneumonia patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis. BMC Pulm Med. 2022, 22, 121. [Google Scholar] [CrossRef]
- Roca, O.; Messika, J.; Caralt, B.; et al. Predicting success of high-flow nasal cannula in pneumonia patients with hypoxemic respiratory failure: The utility of the ROX index. J Crit Care. 2016, 35, 200–205. [Google Scholar] [CrossRef]
- incent, J.L.; de Mendonça, A.; Cantraine, F.; et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef]
Figure 1.
Lasso Regression Analysis Results (A: Cross-validation Curve of Lasso Regression; B: Regression Coefficient Path Diagram of Each Feature Variable).
Figure 1.
Lasso Regression Analysis Results (A: Cross-validation Curve of Lasso Regression; B: Regression Coefficient Path Diagram of Each Feature Variable).
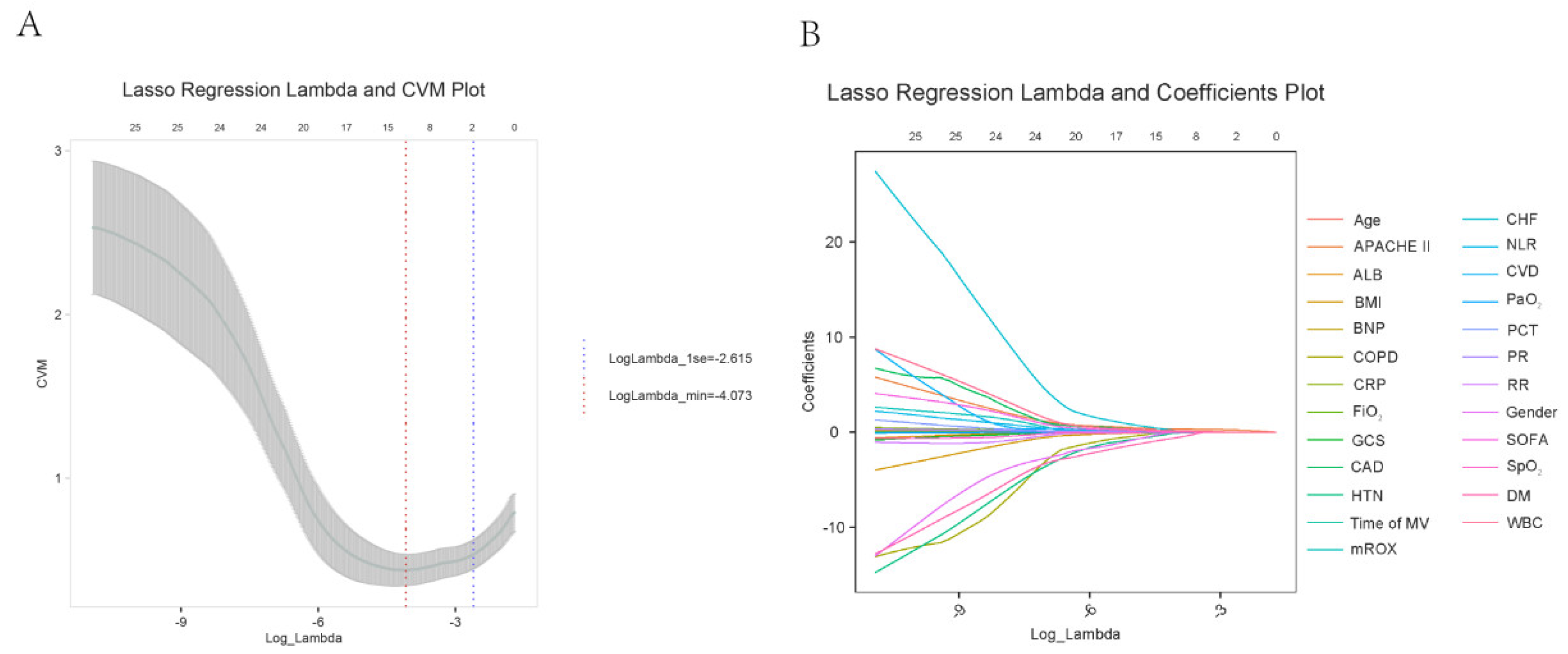
Figure 2.
Feature Importance in Random Forest Analysis of the Training Set (A: Feature Importance Ranking; B: Feature SHAP Value Beehive Plot).
Figure 2.
Feature Importance in Random Forest Analysis of the Training Set (A: Feature Importance Ranking; B: Feature SHAP Value Beehive Plot).
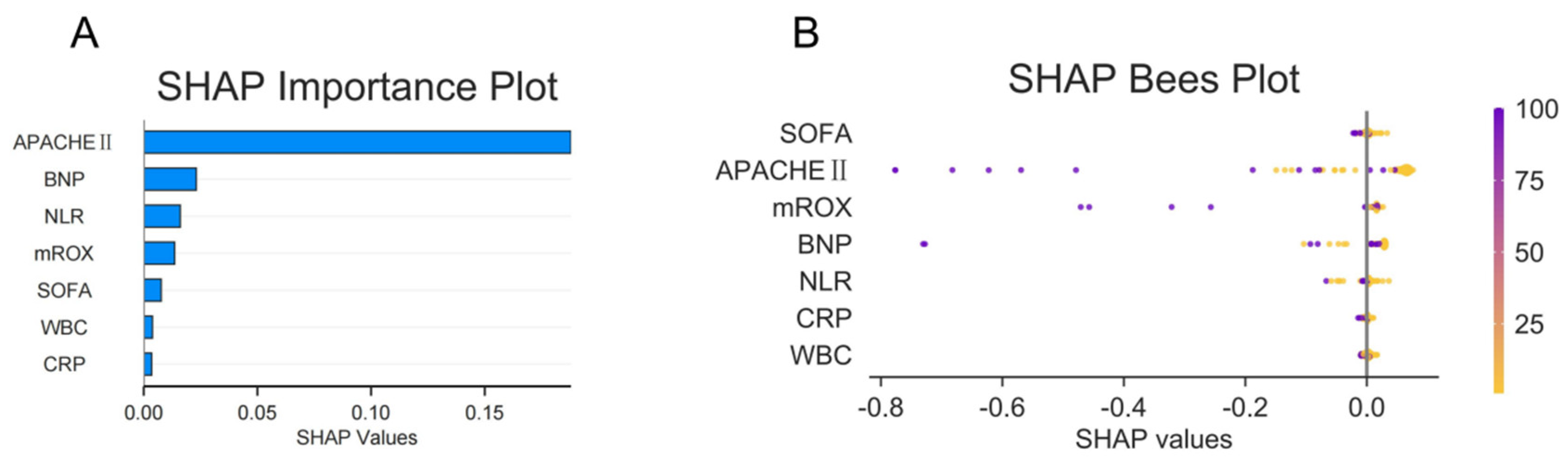
Figure 3.
Random Forest Analysis ROC Curve (A); Calibration Curve (B); Decision Curve (C).
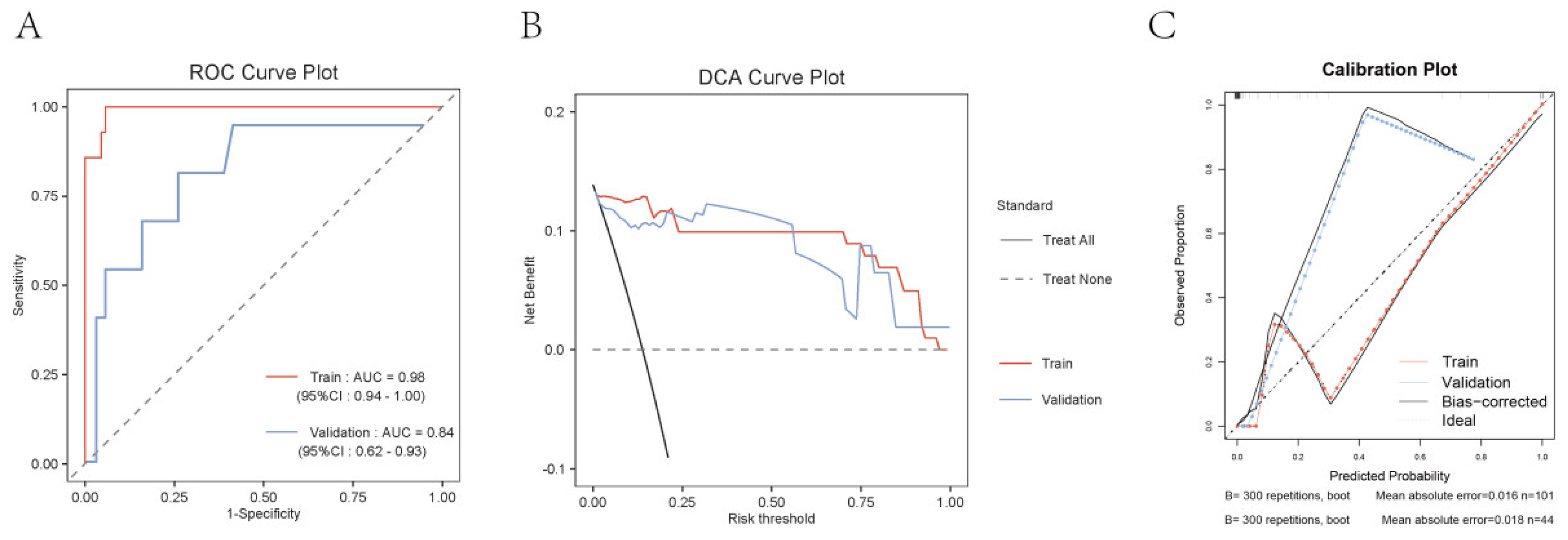

Table 1.
Comparative Analysis of General Information of Patients Included in the Study.
| Succeed(n=126) | Failure(n=19) | t/χ² | P | |
| Age | 56.50±14.94 | 59.32±13.24 | -0.78 | 0.439 |
| BMI(kg/m2) | 24.06±3.25 | 23.63±3.45 | 0.53 | 0.6 |
| Time of MV(h) | 218.47±64.01 | 208.58±63.76 | 0.63 | 0.531 |
| WBC(10^9/L) | 13.89±2.51 | 15.68±1.92 | -3.64 | 0.001 |
| NLR | 7.61±4.42 | 9.37±3.68 | -1.65 | 0.101 |
| CRP(mg/L) | 39.94±22.72 | 58.68±38.93 | -2.05 | 0.054 |
| Alb(g/L) | 33.40±7.53 | 34.16±8.61 | -0.4 | 0.688 |
| PCT(ng/mL) | 7.49±3.92 | 7.63±4.02 | -0.14 | 0.886 |
| BNP(pg/mL) | 148.45±109.65 | 291.26±140.73 | -5.09 | <.001 |
| RR | 21.75±3.55 | 21.05±3.39 | 0.8 | 0.426 |
| PR | 93.44±12.76 | 94.63±11.28 | -0.38 | 0.702 |
| SpO2 (%) | 93.73±2.21 | 94.16±2.46 | -0.78 | 0.439 |
| PaO2(mmHg) | 77.23±20.09 | 72.26±19.42 | 1.01 | 0.315 |
| FiO2 | 0.77±0.20 | 0.72±0.19 | 1.01 | 0.315 |
| mROX | 5.16±1.33 | 3.95±1.50 | 3.64 | <.001 |
| APACHEⅡ | 13.07±3.47 | 19.47±3.12 | -7.59 | <.001 |
| GCS | 10.69±3.86 | 11.54±4.59 | 1.9 | 0.16 |
| SOFA | 9.56±3.73 | 12.21±2.76 | -3.7 | <.001 |
| Gender,n(%) | 0 | 0.984 | ||
| Male | 66(52.38) | 10(52.63) | ||
| Female | 60(47.62) | 9(47.37) | ||
| HTN,n(%) | 0.03 | 0.855 | ||
| No | 99(78.57) | 14(73.68) | ||
| Yes | 27(21.43) | 5(26.32) | ||
| DM,n(%) | 0.75 | 0.388 | ||
| No | 101(80.16) | 13(68.42) | ||
| Yes | 25(19.84) | 6(31.58) | ||
| CAD,n(%) | 0.49 | 0.483 | ||
| No | 105(83.33) | 14(73.68) | ||
| Yes | 21(16.67) | 5(26.32) | ||
| CHF,n(%) | 0.37 | 0.543 | ||
| No | 104(82.54) | 14(73.68) | ||
| Yes | 22(17.46) | 5(26.32) | ||
| COPD,n(%) | 0.03 | 0.87 | ||
| No | 82(65.08) | 12(63.16) | ||
| Yes | 44(34.92) | 7(36.84) | ||
| CVD,n(%) | 2.43 | 0.119 | ||
| No | 108(85.71) | 13(68.42) | ||
| Yes | 18(14.29) | 6(31.58) |
Table 2.
Comparative Analysis between Training Set and Validation Set.
| Train set(n=101) | Validation set(n=44) | t/χ² | P | |
| WBC(10^9/L) | 13.97±2.37 | 14.81±2.51 | -1.60 | 0.112 |
| NLR | 7.13±4.04 | 8.42±4.33 | -1.45 | 0.151 |
| CRP(mg/L) | 44.39±28.82 | 46.81±23.05 | -0.41 | 0.681 |
| BNP(pg/mL) | 181.50±124.84 | 170.94±131.88 | 0.39 | 0.701 |
| mROX | 4.93±1.31 | 5.17±1.62 | -0.81 | 0.419 |
| APACHEⅡ | 13.80±4.05 | 13.52±4.46 | 0.32 | 0.754 |
| SOFA | 10.39±3.93 | 10.00±3.45 | 0.47 | 0.638 |
| HTN,n(%) | 0.10 | 0.757 | ||
| No | 78(77.23) | 35(79.55) | ||
| Yes | 23(22.77) | 9(20.45) | ||
| DM,n(%) | 0.03 | 0.858 | ||
| No | 79(78.22) | 35(79.55) | ||
| Yes | 22(21.78) | 9(20.45) | ||
| CHF,n(%) | 0.14 | 0.708 | ||
| No | 83(82.18) | 35(79.55) | ||
| Yes | 18(17.82) | 9(20.45) | ||
| Outcome,n(%) | 1.89 | 0.169 | ||
| Succeed | 63(90.00) | 24(77.42) | ||
| Failure | 7(10.00) | 7(22.58) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



