
Submitted:
29 September 2024
Posted:
30 September 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Introduction: Variants of COVID-19 are responsible for 700 million infections and 7 million deaths worldwide. Vaccinations have high efficiency in preventing infection and secondary benefits of reducing COVID-19 hospital admissions, attenuating disease severity and duration of illness. Conflicting reports were published regarding COVID-19 among PLWH. Objective: The aim of this study was to evaluate COVID-19 morbidity, hospitalization and the magnitude of immunological response to sequential BNT 162b2 mRNA vaccines in PLWH regarding demographic and clinical factors. Results: Our retrospective study included 784 PLWH who had at least one anti- SARS-CoV-2 antibody test between March 2021 and October 2021. Half of our patients (392) had CD4 cells count above 500 cells/µl, 40.2% (315) had 200<CD4<500 cells/µL and only 9.8% (77) had CD4 <200 cells/µL at their last laboratory workup. The mean age was 50.2±12.2 years. About 90% of our patients were given at least two doses of the BNT 1626b2 Pfizer vaccines, about 60% received three doses of the vaccine. About a quarter of our patients (27.3%) had COVID-19 infection. Only 6 patients required hospital admission. All six patients recovered from COVID-19 infection. Titers of COVID-19 antibodies were lower for patients with CD4 cells count of less than 200 cells/ µL in the first, second and third serological tests with statistical significance. In a multinomial logistic regression the influence of other factors such as age, sex, previous COVID-19 infection on first COVID-19 antibodies titers was not significant. Conclusions: PLWH are responsive to COVID-19 vaccines. As was expected, patients with higher CD4 cells count have higher titers of COVID-19 antibodies and less severe illness. Age, sex and previous COVID-19 infection did not significantly affect antibodies titers according to our study. Larger prospective studies with control groups are needed to further characterize immunologic response to COVID-19 vaccination among PLWH.
Keywords:
HIV
; AIDS
; COVID-19
; COVID-19 mRNA Vaccine
; Vaccination response
Introduction
First cases of corona virus disease 2019 (COVID-19) emerged in Wuhan, China in December 2019. The disease, caused by the severe acute respiratory syndrome coronavirus 2 (SARS- CoV-2), spread rapidly worldwide and was announced as a global pandemic by the world health organization (WHO) in March 2020. As of July 2023, the different variants of COVID-19 are responsible for 700 million infections and 7 million deaths. At the end of 2020 two mRNA COVID-19 vaccines were authorized by the FDA. Large, randomized, controlled phase 3 trials proved the two dose BNT 1626b2 Pfizer vaccine to confer 95% protection against COVID-19 infection [1]. Vaccination in real world conditions reconfirmed the high efficiency in preventing infection and demonstrated secondary benefits of the vaccine in reducing COVID-19 hospital admissions, attenuating disease severity and duration of illness [2].
Patients living with HIV (PLWH) were assumed to have an increased risk for COVID-19 infection and to have more severe illness. Conflicting reports were published. Initial studies found no increased risk for infection or more severe COVID-19 illness among PLWH. Yet, later studies demonstrated an increased risk for severe COVID-19 among PLWH [3]. PLWH are often less responsive to vaccines, with lower efficacy. Even successfully treated HIV patients, show specific defects in memory follicular T helper cells that lead to reduced B cell response and antibodies production [4,5,6]. Data regarding COVID-19 vaccination in PLWH and the clinical characteristics of their serologic response was sparse [7,8,9,10]. The aim of this study was to evaluate the magnitude of immunological response to sequential BNT 162b2 mRNA vaccines in PLWH regarding demographic and clinical factors including CD4 status, viral load, COVID-19 morbidity, and hospitalization.
Methods
Patients
PLWH treated at the "Neve Or" HIV clinic were offered an anti- SARS-CoV-2 antibody test to be added to their routine laboratory workup. Testing for anti- SARS-CoV-2 antibody started on March 1st 2021. Patients with a COVID -19 serology test between 01/03/2021 and 30/10/2021 were included in the current retrospective cohort.
Demographic Clinical and Laboratory Data
Data were collected from patients' electronic files. Demographic characteristics included gender, age and way of HIV acquisition. Clinical characteristic included CD4, nadir of CD4, time since HIV diagnosis (in years), viral suppression, COVID-19 morbidity, hospital admissions for COVID-19 infection and outcomes, number and dates of COVID-19 vaccination and antibodies titers.
The BNT 1626b2 Pfizer vaccine was used for all vaccinated patients and subsequent second and third booster immunizations if taken. Abbott's© SARS-CoV-2 IgG II quant assay was used to determine the qualitative measure of IgG antibodies against spike receptor binding domain (RBD). This test detects a positive antibody responses from both infected and vaccinated individuals. A titer of less than 50 reflects no immunization, titers between 50 and 40,000 are considered immune and results higher than 40,000 are regarded highly immune. RBD IgG levels were recorded in relation to the time (measured in days) from each vaccine taken.
Patients were divided to three groups according to their CD4 cell count; less than 200 cells/µl, CD4 cells count between 200-500 cells/µl and above 500 cells/ µl. viral load was considered undetectable for participants with less than 200 copies/µl.
Statistical Analysis
Data are presented as means ± standard deviations. Continuous variables between the study groups were tested for normality by Shapiro- Wilk test and when abnormal distribution was found, non-parametric tests were performed. The Kruskal-Wallis H groups was performed to compare the three groups. A repeated measures analysis of variance was used to determine any significant differences between variability over time. Initial multivariable logistic regression models were built including variables with statistical significance at univariate analysis. P value <0.05 was considered statistically significant. Data were analyzed using SPSS 25.
Results
Demographic and Clinical Characteristics
Our retrospective study included 784 PLWH who had at least one anti- SARS-CoV-2 antibody test between the first of March 2021 and the end of October 2021. Demographic and clinical data for these patients are presented at Table 1. Half of our patients (392) had CD4 cells count above 500 cells/µl, 40.2% (315) had 200<CD4<500 cells/µL and only 9.8% (77) had CD4 <200 cells/µL at their last laboratory workup. The mean age of the patients was 50.2±12.2 years; patients with CD4 cell counts of less than 200 cells/µL were older with statistical significance; P=0.0001. Most of our patients (55.6%) were males; higher rate of males were in the group of patients with low CD4 cells counts, with statistical significance. Most of our HIV positive patients (60.2%) were immigrants from endemic country. The mean duration of HIV infection was 16.5±7.8 years. The CD4 nadir was lower for patients with lower CD4, with statistical significance (Table 1). 93.9% of our patients had HIV viral suppression at their last laboratory workup; lower rate of viral suppression was observed in the group of patients with lower CD4 cell counts.
COVID-19 Vaccination and Infection
As can be seen in Table 2, about 90% of our patients were given at least two doses of the BNT 1626b2 Pfizer vaccines and about 60% received three doses of the vaccine. About a quarter of our patients (27.3%) had COVID-19 infection, with no correlation to their CD4 cell count. Only 6 patients (0.76%) required hospital admission for their COVID-19 infection: one patient with CD4 cells count of less than 200 cells/µL, five patients with CD4 cells count of 200-500 and none with CD4 cells count above 500 cells/µL; P=0.047. All six patients recovered from COVID-19 infection. None of our patient died of COVID-19. Titers of COVID-19 antibodies were lower for patients with CD4 cells count of less than 200 cells/ µL in the first, second and third serological tests with statistical significance; P= 0.0001 for the first titer (Table 2).
Antibodies Titer over Time
As was expected repeated measurements revealed an increase in the qualitative measure of IgG antibodies against spike receptor binding domain (RBD) over time, with statistical significance; p<0.001 (Figure 1). 78.8% of our patients had normal or high titer of COVID-19 antibodies at the first measurement (618/784), 88.8% of our patients had normal or high titer of COVID-19 antibodies at their second measurement (493/555). The third measurement revealed that 93.4% of our patients had normal or high titers of COVID-19 antibodies, but the group was small (43/46).
Multi Variant Analysis
Multinomial logistic regression was done to examine the influence of other factors such as age, sex, previous COVID-19 infection and last CD4 value on COVID-19 antibodies titers. The first titer of antibodies correlated to CD4 at the last laboratory workup. Low CD4 cells count (<200 cells/µl) reduced the chances of normal and high titers of COVID-19 antibodies with an odds ratio of 0.27; p<0.01 for normal antibodies response and odds ratio of 0.304 for high antibodies response; P= 0.001. Age, sex and previous infection with COVID-19 did not have significant influence on first COVID-19 antibodies titers. Multinomial logistic regression of the second titer of antibodies revealed that low CD4 cells counts (<200 cells/µl) were strongly associated with low COVID-19 antibodies titers, odds ratio of 0.261; P=0.002. Older age was associated with higher antibodies titer with an odds ratio of 1.025 for every year; P=0.04.
Discussion
In this study, which examined 784 people living with HIV (PLWH) in Israel, we observed a high rate of COVID-19 vaccination, with about 90% of the participants receiving at least two doses of the BNT 162b2 mRNA vaccine. The high vaccination rate against COVID-19 observed in our cohort is particularly noteworthy when compared to other studies in different regions. For instance, a cross-sectional study in South Africa reported that only 57% of PLWH were willing to accept future vaccination [11], and a study from New York City found that 28% of PLWH had not received any COVID-19 vaccination by March 2022 [12]. The rate of COVID-19 vaccination among our HIV patients was higher compared to the rate of vaccination among the general population in Israel, which was 84.3% in March 2022 [13]. The higher vaccination rates in our study may reflect the stronger engagement of PLWH to healthcare compared to the general population.
The demographic characteristics of our patients represents HIV infected patients in a "real world" setting. Our cohort included a unique patient population with relatively high proportion of women and individuals of African descent, mainly Ethiopian, which may differ from other studies that predominantly feature male participants [12]. Additionally, our study followed large number of HIV patients during a long period of the COVID-19 pandemic, reflecting the surge of different variants waves including the beta, delta, omicron BA1/2 and even for some extent omicron BA4/5. This broad temporal coverage adds robustness to our findings, suggesting that the immune response observed is consistent across different variants of the virus.
In Oct 2021, the cumulative COVID-19 infection rate of our HIV patients was 27.6%, higher than the infection rate of the entire Israeli population at the same time point [14]. Despite the higher rates of infection, hospitalization rate due to COVID-19 was not higher than the rate of hospitalization in the entire Israeli population [14]. Only six patients required hospitalization, all of them recovered. A study from the USA from the beginning of the COVID-19 pandemic reported that people living with diagnosed HIV experienced poorer COVID-related outcomes relative to persons living without diagnosed HIV [15]. Later study, from the UK found an adjusted hazard ratio of 0.49 for invasive mechanical ventilation/death of hospitalized PLWH compared to HIV negative hospitalized population [16]. This encouraging finding suggests COVID-19 vaccination provides substantial protection against severe disease in PLWH, even among those with lower CD4 counts. The absence of COVID-19-related mortality in our cohort further supports the effectiveness of vaccination in this population.
In line with other studies, our research confirms that PLWH with higher CD4 cell counts exhibit better immunologic responses to COVID-19 vaccines [17,18]. Specifically, patients with CD4 counts below 200 cells/µL had significantly lower antibody titers after vaccination [19,20]. Notably, our findings align with those from other studies, such as an Israeli study that reported 136 PLWH having a humoral immune response comparable with that of health care workers (without HIV) to 2 doses of BNT 162b2 mRNA vaccine. PLWH with CD4 cell counts less than 300 cells/µl had lower antibody titers than those with higher CD4 cell count [10].
Interestingly, while age, sex, and previous COVID-19 infection did not significantly impact the first antibody titer in our cohort, older age was associated with higher antibody titers in subsequent measurements. This finding contrasts with some reports that suggest older individuals might have a diminished response to vaccination [21]. The reasons for this discrepancy could be multifactorial and warrant further investigation. It is possible that the older participants in our study had more consistent healthcare access or that other unmeasured factors contributed to this outcome.
Our findings contribute to the growing body of evidence that suggests PLWH, particularly those with well-managed HIV, exhibit a robust immunologic response to COVID-19 vaccination [22]. An Israeli prospective study with 143 PLWH found the BNT 162b2 mRNA vaccine to be immunogenic in PLWH that were taking antiretroviral treatment, with unsuppressed CD4 cell counts and suppressed viral load [7]. A retrospective analysis of 665 PLWH from Germany/Munich found a strong immune response to standard vaccination with a high antibody concentration associated with being female and having high CD4 cell counts [9]. Our study found that a significant majority (78.8%) of participants had normal or high titers of COVID-19 antibodies after the first serological measurement, and this proportion increased with subsequent measurements.
Despite these positive outcomes, it is important to acknowledge the limitations of our study. As a retrospective analysis, our study is subject to the inherent biases associated with this study design, including selection bias and the potential for missing data. Moreover, our cohort is relatively unique, with a high rate of viral suppression and a specific demographic composition, which may limit the generalizability of our findings to other PLWH populations.
In conclusion, our study provides valuable insights into the immunologic response to COVID-19 vaccination in PLWH, highlighting the importance of vaccination in this population. The findings underscore the need for continued efforts to vaccinate PLWH, particularly those with lower CD4 counts, to ensure broad protection against COVID-19. Further research, particularly prospective studies with control groups, is needed to fully understand the long-term immunologic outcomes and the potential need for additional booster doses in this population.

Table 3.
Multinomial logistic regression of age, sex, previous COVID-19 infection and last CD4 value of first and second titer of COVID-19 antibodies.
Table 3.
Multinomial logistic regression of age, sex, previous COVID-19 infection and last CD4 value of first and second titer of COVID-19 antibodies.
| First titer of COVID-19 antibodies (784 patients) | Second titer of COVID-19 antibodies (555 patients) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Wald (df=1) | Exp(B) | 95% Confidence Interval | B | Std. Error | Wald | Exp(B) | 95% Confidence Interval | |
| Age | 0.016 | 0.009 | 3.471 | 1.016 | 0.999-1.034 | 0.024 | 0.012 | 4.224* | 1.025 | 1.001-1.049 |
| Sex | 0.232 | 0.214 | 1.169 | 1.261 | 0.828-1.918 | 0.555 | 0.286 | 3.767 | 1.742 | 0.995-3.05 |
| COVID-19 infection | 0.214 | 0.244 | 0.769 | 1.238 | 0.768-1.996 | -0.220 | 0.318 | 0.479 | 0.803 | 0.431-1.496 |
| CD4 | -1.189 | 0.349 | 11.609* | 0.304 | 0.154-0.603 | -1.344 | 0.432 | 9.704** | 0.261 | 0.112-0.607 |
*P<0.05; **P<0.01.
References
- Fernando P Polack 1, Stephen J Thomas 1, Nicholas Kitchin 1, Judith Absalon 1, Alejandra Gurtman 1, Stephen Lockhart et al. Clinical Trial Group. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Engl J Med 2020 Dec 31;383(27):2603-2615. [CrossRef]
- Thompson MG, Burgess JL, Naleway AL, Tyner H, Yoon SK, Meece J et al. Prevention and Attenuation of Covid-19 with the BNT162b2 and mRNA-1273 Vaccines. N Engl J Med. 2021 Jul 22;385(4):320-329. [CrossRef]
- Barbera LK, Kamis KF, Rowan SE, Davis AJ, Shehata S, Carlson JJ et al. HIV and COVID-19: review of clinical course and outcomes. HIV Res Clin Pract. 2021 Aug;22(4):102-118. [CrossRef]
- Lacey CJ. HPV vaccination in HIV infection. Papillomavirus Res. 2019 Dec;8:100174. [CrossRef]
- E. Irungu, N. Mugo, K. Ngure, R. Njuguna, C. Celum, C. Farquhar, et al. Immune response to hepatitis B virus vaccination among HIV-1 infected and uninfected adults in Kenya. J. Infect. Dis., 207 (2013), pp. 402-410. [CrossRef]
- R. Cubas, J. van Grevenynghe, S. Wills, L. Kardava, B.H. Santich, C.M. Buckner, et al. Reversible reprogramming of circulating memory T follicular helper cell function during chronic HIV infection. J. Immunol., 195 (2015), pp. 5625-5636. [CrossRef]
- Levy I, Wieder-Finesod A, Litchevsky V, Biber A, Indenbaum V, Olmer L et al.. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in people living with HIV-1. Clin Microbiol Infect. 2021 Dec;27(12):1851-1855. [CrossRef]
- Liu Y, Han J, Li X, Chen D, Zhao X, Qiu Y et al. COVID-19 Vaccination in People Living with HIV (PLWH) in China: A Cross Sectional Study of Vaccine Hesitancy, Safety, and Immunogenicity. Vaccines (Basel). 2021 Dec 9;9(12):1458. [CrossRef]
- Noe S, Ochana N, Wiese C, Schabaz F, Von Krosigk A, Heldwein S et al. Humoral response to SARS-CoV-2 vaccines in people living with HIV. Infection 2022 Jun;50(3):617-623. [CrossRef]
- Tau L, Turner D, Adler A, Marom R, Ahsanov S, Matus N, Levi I et al. SARS-CoV-2 Humoral and Cellular Immune Responses of Patients With HIV After Vaccination With BNT162b2 mRNA COVID-19 Vaccine in the Tel-Aviv Medical Center. Open Forum Infect Dis. 2022 Feb 23;9(4).
- Govere-Hwenje S, Jarolimova J, Yan J, Khumalo A, Zondi G, Ngcobo et al. Willingness to accept COVID-19 vaccination among people living with HIV in a high HIV prevalence community. BMC Public Health. 2022 Jun 22;22(1):1239. [CrossRef] [PubMed] [PubMed Central]
- Rosenthal EM, Patterson W, Chicoine J, Dorabawila V, Adamashvili N, Rajulu DT, Rosenberg ES, Tesoriero JM. COVID-19 Vaccination and Hospitalization Among Persons Living With Diagnosed HIV in New York State. J Acquir Immune Defic Syndr. 2023 Jun 1;93(2):92-100. [CrossRef]
- Shkalim Zemer V, Grossman Z, Cohen HA, Hoshen M, Gerstein M, Yosef N et al. Acceptance Rates of COVID-19 Vaccine Highlight the Need for Targeted Public Health Interventions. Vaccines (Basel). 2022 Jul 22;10(8):1167. [CrossRef]
- Israeli ministry of health. Corona virus in Israel - Data (in Hebrew). Available online: https://datadashboard.health.gov.il/portal/dashboard/health/%7Cdashboard.
- Tesoriero JM, Swain CE, Pierce JL, Zamboni L, Wu M, Holtgrave DR et al. COVID-19 Outcomes Among Persons Living With or Without Diagnosed HIV Infection in New York State. JAMA Netw Open. 2021 Feb 1;4(2):e2037069. [CrossRef]
- Geretti AM, Stockdale AJ, Kelly SH, Cevik M, Collins S, Waters L, et al. Outcomes of Coronavirus Disease 2019 (COVID-19) Related Hospitalization Among People With Human Immunodeficiency Virus (HIV) in the ISARIC World Health Organization (WHO) Clinical Characterization Protocol (UK): A Prospective Observational Study. Clin Infect Dis. 2021 Oct 5;73(7):e2095-e2106. [CrossRef]
- Coburn SB, Humes E, Lang R, Stewart C, Hogan BC, Gebo KA, et al. Analysis of postvaccination breakthrough COVID-19 infections among adults with HIV in the United States. JAMA Netw Open. 2022;5:e2215934. [CrossRef]
- Zhou Q, Liu Y, Zeng F, Meng Y, Liu H, Deng G. Correlation between CD4 T-Cell Counts and Seroconversion among COVID-19 Vaccinated Patients with HIV: A Meta-Analysis. Vaccines (Basel). 2023 Apr 4;11(4):789. [CrossRef]
- Antinori A, Cicalini S, Meschi S, Bordoni V, Lorenzini P, Vergori A, et al. Humoral and Cellular Immune Response Elicited by mRNA Vaccination Against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in People Living With Human Immunodeficiency Virus Receiving Antiretroviral Therapy Based on Current CD4 T-Lymphocyte Count. Clin Infect Dis. 2022 Aug 24;75(1):e552-e563. [CrossRef] [PubMed] [PubMed Central]
- Hassold N, Brichler S, Ouedraogo E, Leclerc D, Carroue S, Gater Y et al. Impaired antibody response to COVID-19 vaccination in advanced HIV infection. AIDS. 2022 Mar 15;36(4):F1-F5. [CrossRef] [PubMed]
- Romero-Olmedo, A.J., Schulz, A.R., Hochstätter, S. et al. Induction of robust cellular and humoral immunity against SARS-CoV-2 after a third dose of BNT162b2 vaccine in previously unresponsive older adults. Nat Microbiol 7, 195–199 (2022). [CrossRef]
- Brumme ZL, Mwimanzi F, Lapointe HR, Cheung P, Sang Y, Duncan MC, et al. Humoral immune responses to COVID-19 vaccination in people living with HIV receiving suppressive antiretroviral therapy. Update in: NPJ Vaccines. 2022 Feb 28;7(1):28. [CrossRef]
Figure 1.
Antibodies titers over time for 46 patients with three measurements. *P<0.001.
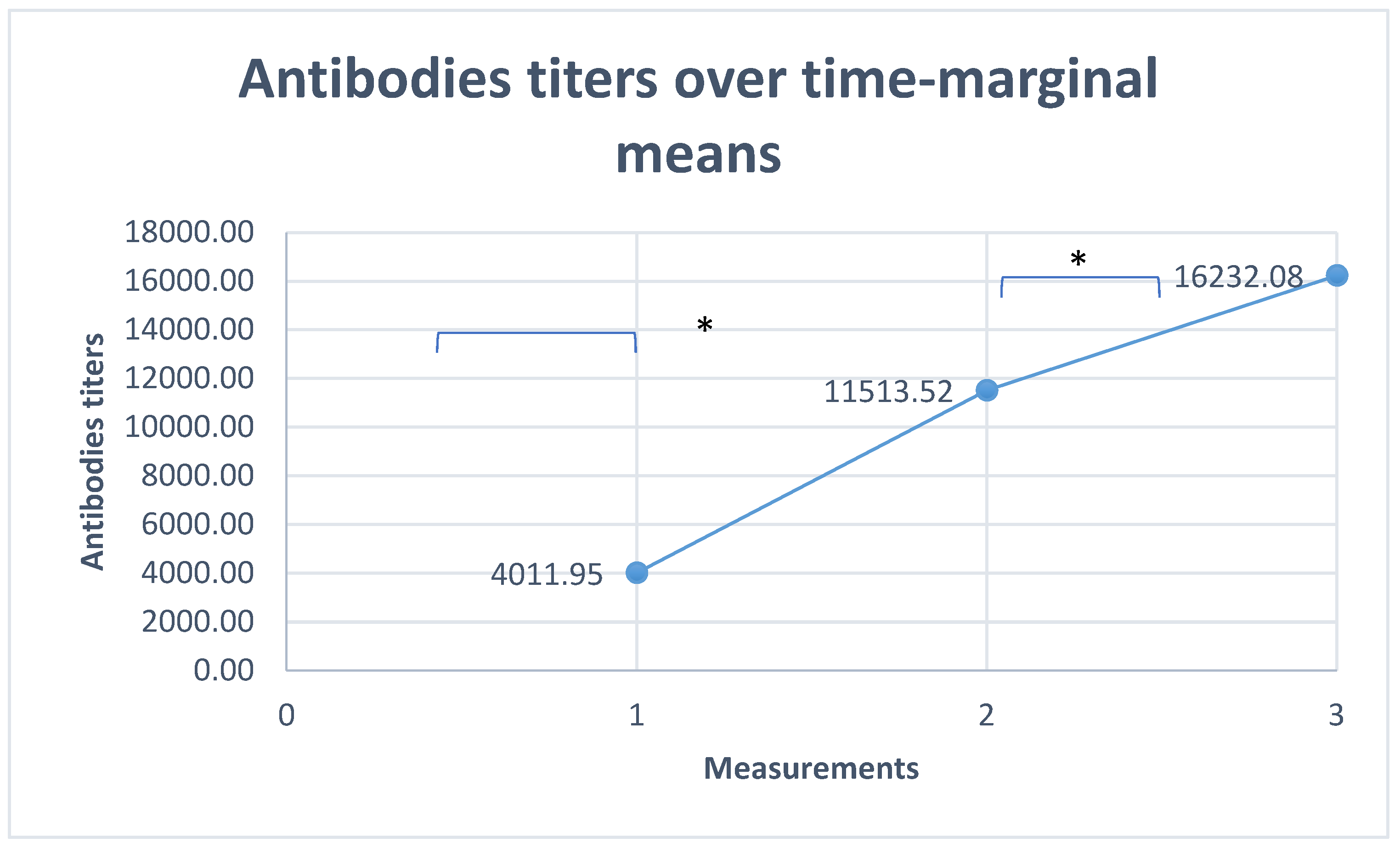
Table 1.
Demographic and clinical characteristics of the patients enrolled in our study .
| Demographic and clinical characteristics | Total number of PLVWH | PLVWH with CD4 <200 | PLVWH with 200<CD4 <500 | PLVWH with CD4≥500 | P value |
|---|---|---|---|---|---|
| Total number of PLWH (%) | 784 (100) | 77 (9.8) | 315 (40.2) | 392 (50) | |
| Females (%) | 348 (48.9) | 27 (35.1) | 127 (40.3) | 194 (49.4) | P=0.011 |
| Males (%) | 436 (55.6) | 50 (64.9) | 188 (59.7) | 198 (50.5) | |
| Mean age ±SD ( range), years | 50.2±12.2 (18-89) | 53.2±12.9 (22-89) | 51.7±13.1 (18-85) | 48.4±11.1 (20-89) | P=0.0001 |
| Years since HIV diagnosis | 16.5±7.8 | 17.4±8 | 16.2±7.7 | 16.6±7.8 | P=0.388 |
| Nadir of CD4 cells/µL | 187.8±170 | 79.4±100.6 | 136.8±98.1 | 249.9±199.7 | P=0.001 |
| Viral load suppression (%) | 736 (93.9) | 61 (79.2) | 293 (93) | 382 (97.4) | P=0.0001 |
Table 2.
COVID-19 infections, hospital admissions and antibodies titer.
| Clinical and laboratory data | Total number of PLVWH | PLVWH with CD4 <200 | PLVWH with 200<CD4 <500 | PLVWH with CD4≥500 | P value | |||
|---|---|---|---|---|---|---|---|---|
| COVID-19 vaccination (at least two doses) (%) | 708 (90.3) | 68 (88.3) | 281(89.2) | 359 (91.5) | ||||
| COVID-19 infection (%) | 217 (27.6) | 19 (24.6) | 88 (27.9) | 110 (28.1) | P=0.824 | |||
| Patients hospitalized for COVID-19 infection (%) | 6 (0.8) | 1 (1.3) | 5 (1.68) | 0 (0) | P=0.047 | |||
| Patients with first Antibodies titer for Covid-19 | Low titer | 784 | 166 (21.2) | 32 (41.6) | 62 (19.7) | 72 (18.3) | P=0.0001 | |
| Normal titer | 403 (51.4) | 29 (37.6) | 158 (50.2) | 216 (55.1) | ||||
| High titer | 215 (27.4) | 16 (20.7) | 95 (30.2) | 104 (26.5) | ||||
| Patients with second antibodies titer for Covid-19 | Low titer | 555 | 62 (11.2) | 11 (25.5) | 25 (10.9) | 26 (9.5) | P=0.041 | |
| Normal titer | 159 (28.6) | 18 (41.8) | 71 (31) | 70 (25.6) | ||||
| High titer | 334 (60.2) | 24 (55.8) | 133 (58.1) | 177 (64.8) | ||||
| Patients with third antibodies titer for Covid-19 | Low titer | 46 | 3 (6.5) | 2 (28.6) | 1 (5.2) | 0 (0) | P=0.038 | |
| Normal titer | 12 (26.1) | 3 ( 42.8) | 3 (15.7) | 6 (30) | ||||
| High titer | 31 (67.4) | 2 (28.6) | 15 (78.9) | 14 (70) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



