
Submitted:
29 September 2024
Posted:
30 September 2024
You are already at the latest version
Abstract
Diabetes mellitus is a prevalent disease with a rapidly increasing incidence projected worldwide, affecting both industrialized and developing regions. Effective diabetes management requires precise therapeutic strategies, primarily through self-monitoring of blood glucose levels to achieve tight glycemic control, thereby mitigating the risk of severe complications. In recent years, there have been significant advancements in non-invasive techniques for measuring blood glucose using photoacoustic spectroscopy (PAS) as it shows great promise for the detection of glucose using the Infrared region (e.g. MIR & NIR) of light. A critical aspect of this method is the detection of the photoacoustic signal generated from blood glucose, which needs to be amplified through a photoacoustic resonator (PAR). In this work, an overview of various types of PARs used for noninvasive glucose sensing is reviewed, highlighting their operating principle, design requirements, limitations, and potential improvements needed to enhance the analysis of photoacoustic signals. This analysis will be helpful for the basic understanding and achieving the highly sensitive PAR required for noninvasive glucose monitoring.
Keywords:
diabetes
; non-invasive glucose detection
; photoacoustic spectroscopy
; photoacoustic cell/resonator
; acoustic amplifier
; Q-factor
; frequency response
1. Introduction
Diabetes is one of the four major types of noncommunicable diseases (NCDs) leading to slow damage to the heart, blood vessels, eyes, kidneys, and nerves. The predominant form is type 2 diabetes, typically affecting adults, characterized by insulin resistance or insufficient insulin production. Over the last thirty years, there has been a substantial surge in the occurrence of type 2 diabetes across nations of varying economic statuses. Type 1 diabetes, previously known as juvenile diabetes or insulin-dependent diabetes, is a chronic condition characterized by little to no natural insulin production by the pancreas. About 422 million individuals globally are affected by diabetes, with a majority residing in low and middle-income nations, and an estimated 1.5 million deaths are directly linked to diabetes annually [1]. By the year 2045, International Diabetes Federation (IDF) forecasts indicate that one out of every eight adults, totaling approximately 783 million individuals, will be afflicted by diabetes, marking a surge of 46% [2]. The vast majority, exceeding 90%, of individuals grappling with diabetes are diagnosed with type 2 diabetes, a condition propelled by a combination of socio-economic, demographic, environmental, and genetic determinants. The primary factors contributing to the escalation of type 2 diabetes encompass urbanization, an aging populace, reduced levels of physical activity, and a growing prevalence of overweight and obesity[2]. According to data provided by the World Health Organization (WHO), the global prevalence of diabetes currently stands at approximately 450 million cases, with projections indicating a potential increase to 700 million cases by the year 2045 [3]. The population is projected to reach 39.7 million by the year 2030 and 60.6 million by 2060 in the United States exclusively [4]. Furthermore, alongside the substantial count of diagnosed individuals, there exists a notable portion of the populace who remain undiagnosed due to socioeconomic and various factors. Therefore, the emphasis on diabetes prevention has attracted increased attention internationally, especially in developed regions. Consequently, the identification and management of diabetes have evolved into a topic of considerable practical significance and economic advantages. Medical directives advocate for monitoring four times daily, with a rise to ten times per day during periods of illness or inadequate glycemic regulation control [5]. Regrettably, the matter of routinely monitoring blood glucose levels is often perceived as uncomfortable by the majority of individuals with diabetes. Traditional tools employed for glucose monitoring operate based on the principles of the electrochemical method [6]. Thus the creation of an effective non-invasive glucose measurement device would be transformative for millions of patients worldwide, enabling them to monitor their glucose levels with confidence and receive prompt treatment when needed [7]. In a greater sense, the overall blood glucose monitoring system can be classified into two categories: invasive and noninvasive. Figure 1 shows the general classification for blood glucose monitoring and the detailed methods are discussed in the following sections.
1.1. Invasive Blood Glucose Monitoring
Currently, the conventional method for blood glucose detection involves taking a blood sample or urine and analyzing it in vitro for glucose measurement. These methods are widely used in the laboratory. In hospitals, blood is collected from patients in the morning while fasting, and the blood glucose concentration is accurately measured using an automatic biochemical analyzer. Besides blood, glucose can also be determined using urine tests [8]. Urine test has both noninvasive and invasive collection methods as mentioned in the general classification above. Invasive urine collection is necessary for patients who are unable to cooperate, suffer from urinary incontinence, or have external urethral ulcerations that elevate the risk of contamination [9]. While these methods are accurate and valuable for diagnosing diabetes, they are not ideal for continuous monitoring of diabetics because they are time-consuming, require large blood samples, and are invasive. Self-monitoring of blood glucose (SMBG) is an alternative approach for checking blood glucose levels at specific times, typically using a home electronic glucometer. These devices commonly rely on glucose oxidase biosensors, collect a small blood sample from a finger prick using a disposable test strip, and measure glucose concentration through an electrochemical reaction.
The advantages of commercial glucose meters are their portability, affordability, simplicity, relatively accurate data, and the ability to monitor multiple times a day. However, these devices have some disadvantages, such as the need for frequent blood collection, which can lead to pain, stress, and increased risk of infection. Some common commercial glucose meter brands include Roche, Sano, Omron, Johnson and Johnson, Bayer, Abbott, Echeng, Ecco, and others [10].
1.2. Non-Invasive Blood Glucose Monitoring
Non-invasive blood glucose monitoring, as its name implies, involves identifying glucose levels in the bloodstream of individuals without causing harm to bodily tissues. Various techniques have been proposed and examined in recent decades. Significant effort has been invested in creating a non-invasive method for measuring glucose. Such a method would enhance the quality of life for diabetic patients and increase their adherence to regular glucose monitoring. To be considered for use in a glucose monitoring device, the method must meet the following criteria:
- Sensitivity: This denotes the minimum concentration that a sensor can detect. A blood glucose sensor should be capable of identifying glucose levels as low as 30 mg/dL [11].
- Stability: This pertains to the performance of a measurement device over an extended period. The device should exhibit high precision, ensuring that measurements remain consistent for the same concentration. Additionally, it should offer a high level of accuracy, meaning that measurements should not fluctuate over time.
- Selectivity: The measurement method must be able to distinguish the glucose signal from signals generated by other substances. Since glucose in the human body is present in aqueous solutions that also contain ions or proteins, which could produce interfering signals, the sensor must effectively isolate the glucose signal.
- Portability: The measurement device should be compact and convenient to carry.
Due to the difficulty of directly accessing blood for non-invasive glucose measurement, alternative biofluids such as urine [12], saliva [13], tears [14], and sweat [15] have been explored. However, glucose levels in these fluids often show a weak correlation with blood glucose levels [16] and experience a significant lag time [17], making them less viable. For instance, saliva glucose measurements can be influenced by pH changes after consuming acidic foods. A promising alternative is to measure glucose concentration from the interstitial fluid (ISF) in the epidermal layer of the skin because ISF constitutes the extracellular fluid that surrounds tissue cells and is comprised of numerous significant biomarkers(biomolecules present in blood, other bodily fluids, or tissues that indicates a normal or abnormal process, or a condition or disease[18]), exhibiting comparable medical diagnostic capabilities to that of blood. Minor molecular biomarkers undergo exchange between blood and ISF via the process of diffusion. Consequently, the relationship between ISF and blood may be employed to indirectly acquire health-related information about patients [10].
Non-invasive methods can be broadly classified as either optical or non-optical methods. There are several non-optical approaches mentioned as shown in Figure 1 such as impedance spectroscopy [19], electromagnetic [20], reverse iontophoresis [21], metabolic heat confirmation [22], and ultrasonic [23]. this methodology possesses the capability to modify the characteristics of the dermal layer and provoke phenomena such as blister formation, irritation, or erythema[19]. Furthermore, this technique necessitates meticulous instrumentation and rigorous calibration, which can be labor-intensive and challenging to execute. Optical spectroscopy is less likely to cause skin irritation compared to non-optical techniques and offers a high degree of specificity in detecting glucose, even in complex matrices such as blood [24]. Consequently, this literature emphasizes and discusses optical methods in detail. Some of them are fluorescence spectroscopy [25,26], optical coherence tomography [27], thermal spectroscopy[28,29], diffuse reflectance spectroscopy [30,31], polarimetry [32,33], absorption spectroscopy [34,35], and photoacoustic spectroscopy [36,37]. In recent years, Photo Acoustic Spectroscopy (PAS) has demonstrated effectiveness in non-invasive glucose detection due to its greater sensitivity compared to optical absorption spectroscopy [38,39,40]. The photoacoustic effect has shown promise in a range of applications for both gaseous and solid samples [41].
In the PAS process, infrared laser radiation is typically used to excite the vibrational states of molecules. Since the radiation is modulated, the heat released by the molecules is also modulated, leading to periodic pressure changes in the surrounding environment. These pressure fluctuations are detected as acoustic waves by a microphone or an acoustic transducer. The generated acoustic signal is typically weak and requires amplification before further processing. This can be accomplished by using an acoustic resonator, where exciting corresponding acoustic modes by the laser illumination. This approach significantly enhances the photoacoustic signal and improves the sensor’s overall detection sensitivity. To maximize signal amplification and neglect some of the environmental factors that deteriorate the actual signal, the resonator’s shape must be optimized.
This study provides an overview of the photoacoustic resonators (PARs) that are used in PAS for noninvasive blood glucose detection. Here, we describe the basic principle of PAS with an emphasis on the PAR for acoustic signal amplification, where the amplification mechanism and performance in the context of noninvasive glucose monitoring are thoroughly highlighted that are published in the literature from 2012 to 2023. This work is presented in the following manner: Section 2 covers the fundamental principles and physics of conventional Photoacoustic Spectroscopy (PAS). It also explains how Photoacoustic Resonance (PAR) amplifies signals, along with the design and modeling techniques involved, as well as the factors that affect quality. In Section 3, a brief history of the use of photoacoustic cells for noninvasive glucose detection from 2012 to 2023 is provided, along with a review of the key literature published during that period. Lastly, Section 4 discusses potential future developments in the use of PAR for noninvasive glucose detection.
2. Principle of Photoacoustic Spectroscopy for Noninvasive Glucose Detection
2.1. Basic Interaction of IR Light with Human Skin/Tissue
Figure 2 (a) exhibits the schematic of typical human skin, which starts with the layer named stratum corneum (the outmost layer of epidermis). The skin consists of mainly three layers: epidermis, dermis, and subcutaneous tissue [43]. As the PAS combines optical spectroscopy and ultrasound tomography, an optical source needs to be selected that is sensitive to glucose molecules. Mostly, Infrared (IR) spectroscopy examines the interaction between tissue and infrared radiation, with wavelengths ranging from 700 nm to 25000 nm in the electromagnetic spectrum. This technique is rooted in vibrational spectroscopy and provides a quick method for both qualitative and quantitative analyses through direct measurement. For improved analytical capabilities, the IR spectrum is divided into three regions: near-infrared (NIR) from 700 to 2500 nm, mid-infrared (MIR) from 2500 to 25000 nm, and far-infrared (FIR) from 25000 to 1000000 nm [44].
NIR and MIR light sources are generally explored as excitation sources due to the strong glucose signature in these regions. Figure 3 (a) shows the absorption spectra of aqueous glucose in the MIR region, with water absorption subtracted from the spectra. Glucose absorption peaks are identified at approximately 920 cm-1, 1150 cm-1, 1365 cm-1, and 1435 cm-1 [17,45]. On the other hand, Figure 3 (b) represents the absorption spectrum of glucose for the NIR region ranging from 5550 cm-1 to 7400 cm-1. NIR measurements examine harmonic overtones of glucose vibrations [45], resulting in relatively weak glucose absorption compared to the background water absorption. The accuracy of these measurements is hindered by significant interference from tissue and other blood components with similar absorption spectra [46,47]. Additionally, NIR measurements are influenced by strong tissue scattering, unlike mid-infrared light. Glucose molecules strongly absorb MIR light in the 8–10 µm wavelength range due to their fundamental vibrational resonances [24,48]. The acoustic signal that is generated can go through the human tissue with minimal scattering and be detected by a microphone/transducer. Thus, the glucose information in the interstitial fluid (ISF) can be correlated to the acoustic signal in IR-based PAS [49]. The ISF is a layer of biological fluid located between cells, composed of water, solvents, and blood vessels. It contains various substances, including sugars, fats, amino acids, hormones, coenzymes, white blood cells, and cellular waste products. Glucose diffuses from the blood into the ISF with a delay of 5 to 15 minutes [50,51].
2.2. Principle of Generating and Detecting Photoacoustic Signals
Figure 4 shows the simplified schematic representation of the basic experimental setup of PAS for the detection of noninvasive blood glucose. The concept of PAS entails the initiation of acoustical waves via a pulsed electromagnetic source (e.g., IR lasers). The biological entity absorbs these electromagnetic waves, inducing thermal expansion or pressure, thereby giving rise to the generation of acoustical waves [53]. The signal generated by the photoacoustic effect is typically weak and requires amplification before further processing. This can be accomplished by adapting a Photoacoustic Resonator (PAR) in the setup, where modulating the electromagnetic radiation at the PAR’s acoustic eigenfrequency, thereby exciting the corresponding acoustic mode. This approach significantly enhances the photoacoustic signal and improves the sensor’s detection sensitivity. Optimizing the resonator’s design parameters can further maximize the amplification of the photoacoustic signal. Subsequently, sensitive ultrasonic microphones or piezoelectric transducers are capable of capturing the amplified waves, which are fed to a lock-in-amplifier allowing for noise reduction and further processing. Furthermore, the attributes of the modulated light source, such as modulation amplitude and duty cycle, exert a notable influence on the production of acoustical waves. The characteristics of human skin play a vital role in the process of wave generation. The pressure resulting from the photoacoustic phenomenon can be mathematically described by the following wave equation incorporating spatial heat distribution H (r, t), following the principles of thermodynamics [53]
where, p(r,t) represents spatial pressure distribution at time t, v is the acoustic velocity, Cp is the heat capacity, and β is the thermal expansion coefficient.
The equation below can be used to represent the peak pressure (P) for a medium that absorbs light weakly:
The system constant, denoted as k, is present in this context, alongside representing the incident laser pulse energy, and n, a constant falling within the range of 1 to 2, based on the specific experimental setup. At times, the combination of experimental variables may result in a heightened photoacoustic signal in contrast to conventional spectroscopic approaches. It is crucial to highlight that the response generated by glucose lacks the requisite level of signal amplification for detection purposes, necessitating the utilization of a PAR to amplify the signal.
2.3. Amplification Mechanism of Photoacoustic Resonator (PAR)
The signal generated by the photoacoustic effect tends to be relatively weak and necessitates amplification. This amplification can be accomplished by modulating the electromagnetic waves at an acoustic resonant frequency of a photoacoustic resonator, thereby stimulating the corresponding acoustic mode. “Acoustic modes” are the specific patterns of pressure variations or sound waves that resonate within a confined space, like a resonator, at certain frequencies. These modes are influenced by the resonator’s size, shape, and the properties of the medium inside it (such as air). Each mode corresponds to a particular frequency, known as the eigenfrequency or resonant frequency, where the resonator naturally enhances sound waves. Exciting these acoustic modes can significantly boost the signal strength of effects like the photoacoustic effect, thereby improving detection sensitivity in various applications [54]. Figure 5 (a) shows a schematic representation of a typical T-type PAR, where two cells are combined: absorption and resonant. In absorption cell
The quality factor is considered to be the performance-indicating parameters of an acoustic resonator and can be defined as the ratio of the resonance frequency to the bandwidth of the resonance peak. A higher quality factor (Q) implies a sharper resonance peak and can be represented as follows:
where f denotes the resonance frequency while is the difference in frequencies at which the value of the pressure amplitude has decreased to half of the resonance value. Enhancing the shape of the resonator can further optimize the amplification of the photoacoustic signal, as it enhances the quality factor by decreasing
2.4. Design and Modeling of Photoacoustic Resonator
In general, the modeling of a PAR can be done in various ways: experimental modeling and numerical modeling [54], Quantitative modeling [55], Optoacoustic inversion modeling [56], structural and functional modeling [57], Finite element method [58], etc. When conducting a purely experimental study, it becomes necessary to experiment with various resonator configurations as determining the most suitable geometry for maximal signal enhancement is not straightforward. This undertaking could prove to be exceedingly laborious and costly. Consequently, computational simulation techniques are the preferred approach [59,60,61]. El-Busaidy et al. [54] described two simulation models named VT (viscothermal) and AME (amplitude mode expansion) model. The VT model is widely regarded as the most precise numerical method for simulating photoacoustic signals in a PAR due to its ability to accurately represent loss effects at the resonator surfaces, which are the primary loss mechanisms in PARs [60]. However, the VT model is computationally demanding, requiring substantial memory and simulation time. For this reason, they explored the AME model, which is faster and less computationally intensive, within a closed T-cell resonator [61]. They extended the investigation of the AME model by simulating the photoacoustic signal of a macroscopic T-cell across a wide frequency range, from 8 kHz to 62 kHz. Their focus was on the photoacoustic signal generated by a solid sample, rather than a gaseous one. The solid sample was placed at one of the resonator’s openings, and the resonator was filled with air rather than a gaseous absorbing sample. Measurements of the photoacoustic signal from the simulated resonator were conducted and then compared to the simulated results [54].
Figure 6.
The frequency responses of the amplitude mode expansion (AME) model, and the viscothermal (VT) model [54].
Figure 6.
The frequency responses of the amplitude mode expansion (AME) model, and the viscothermal (VT) model [54].
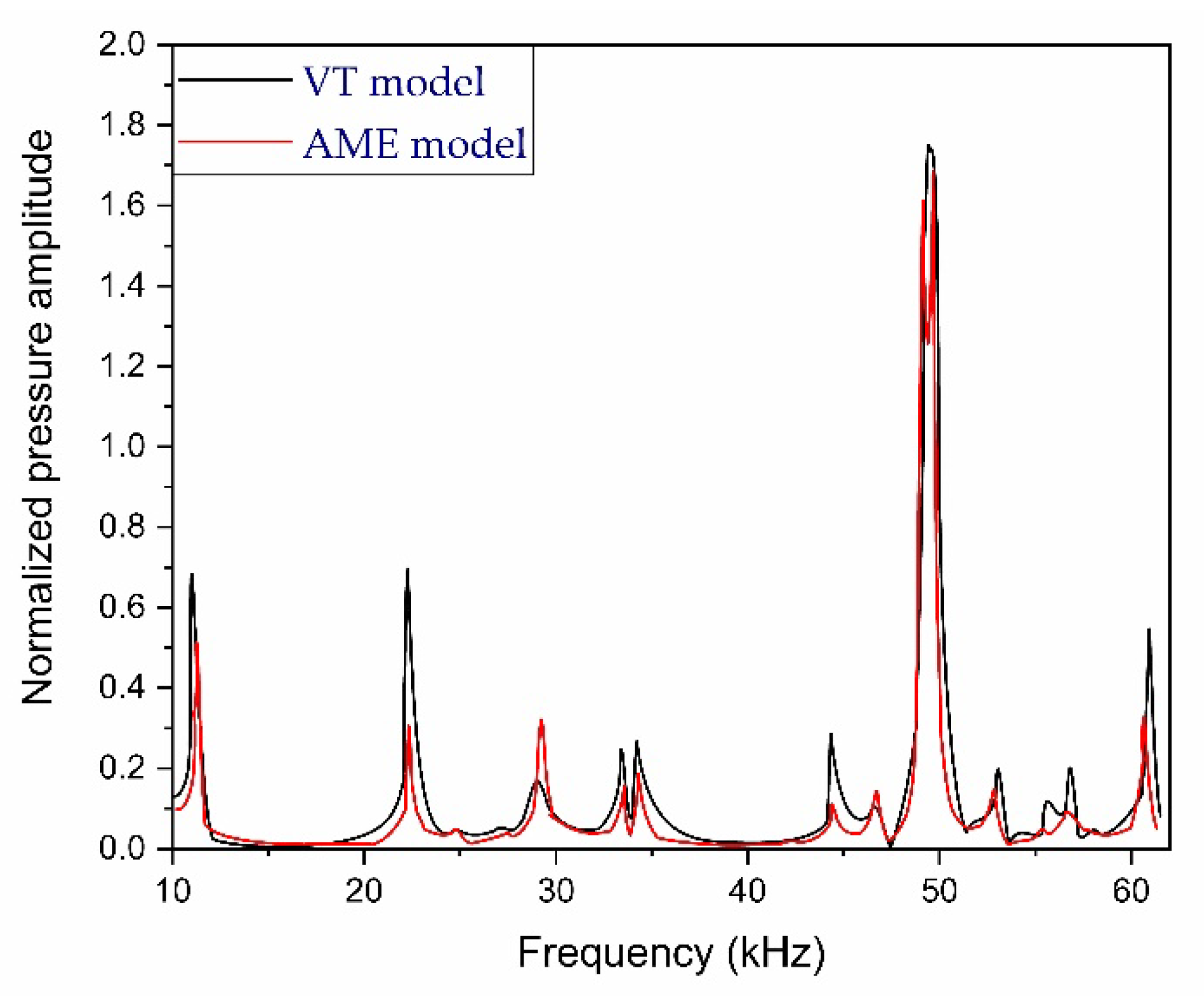
Figure 5 shows two simulated frequency response curves between 10 kHz to 62 kHz using VT and AME simulation models. The AME model measurement results were compared to the VT model, which is regarded as the most accurate simulation method. The resonance frequencies from the measurements showed good accordance with the VT simulations, with a relative difference in peak resonance frequency of not more than 1.1% compared to the VT model values. It should be noted that the temperature of the air inside the resonator was not monitored during the measurements. Temperature variations could contribute to deviations, as the speed of sound and, consequently, the resonance frequencies are dependent on the air temperature [54].
2.5. Requirements of PAR for Noninvasive Glucose Detection
The key aspects to consider when developing a PAR system for noninvasive glucose detection include [58]:
- Humidity issue:
One of the ends is left unsealed to prevent an increase of humidity within the resonator that is caused by skin transpiration [62], that’s why photoacoustic measurements of blood glucose levels are performed using open T-shaped resonators [62,63]. Furthermore, the opening enhances the stability of the measurement by reducing the temperature fluctuations [62].
- Volume and surface loss:
If the thermal conductivity of the fluid (i.e., air inside the cell) is negligible, there is no heat transfer between adjacent pressure maxima and minima. However, if this heat transfer cannot be ignored, the fluctuations in energy density will diminish, leading to the dissipation of the sound wave.
- Location and position of light source & cylinders:
The location of LASER beams in the T cell and the position of the resonance cylinder and the microphones also define the performance of PAR. The additional loss is due to leakage of the PA signal from the resonator end sealed with the microphone [64].
3. History of PA Cells Used in PAS for Noninvasive Blood Glucose Detection
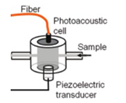
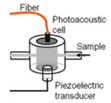
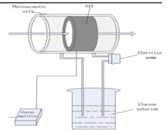
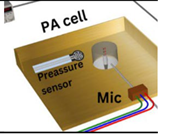
Camou et al. [65] designed a detection photoacoustic (PA) cell in 2012 that is made of brass and provides a sufficient acoustic impedance mismatch with water so that acoustic energy remains confined within the inner volume of the cell. Here, they used a piezoelectric transducer which is set perpendicular to the optical fiber so that the light beam cannot directly strike the sensitive surface of the transducer. This cylindrical-shaped fiber-coupled PA cell’s working frequency range is 300-500 kHz, where they used aqueous glucose solutions whose concentration ranges from 0 to 15 g/dL. In 2013, the same research group [66] proposed a fabrication method that consists of patterning three PMMA plates with a laser cutter to ensure fast prototyping and flexibility in the design. They used the same frequency range of 300-500 kHz and glucose solution concentration levels ranged from 0 to 10 g/dL.
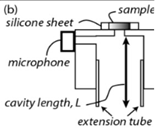
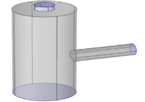
Pleitez et al. [67] designed a T-shaped PA cell for in-vivo measurement of blood glucose. This combination facilitates a quantitative measurement for concentrations of skin glucose in the range from <50 mg/dL to >300mg/dL. This range is relevant for glucose monitoring in diabetes patients. In a T-shaped resonator, there exist two cylindrical cavities perpendicularly connected, which are the absorption and resonance cavities. An anti-reflection coated ZnSe window was used for antireflection purposes. This T-shaped PA cell has a working frequency range of 50-54 kHz with a quality (Q) factor of 102. Later on, they [68] showed the application of a novel open, windowless cell in 2013 for the photoacoustic IR spectroscopy of human skin. The windowless cavity is tuned for optimum performance in the ultrasound range between 50-60 kHz. Here, they used open cells to prevent an increase in humidity inside the acoustic resonator due to skin transpiration. The frequency response of the open cell is dominated by two resonance peaks at 51.7 kHz and 53.8 kHz having a quality factor of 45 and 32, respectively. Finally, they observed that the Q factor for the same windowless PA cell is about 50% lower than the Q factor for the same PA cell geometry in the closed configuration.
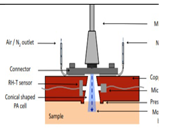
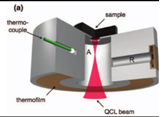
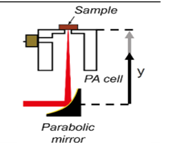
Kottmann et al. [39] introduced the first MIR fiber-coupled photoacoustic sensor designed to study condensed samples within the MIR fingerprint region. The photoacoustic chamber features a conical shape that aligns with the beam emitted from the fiber, effectively minimizing the volume of the cell. This setup yields a detection limit of 57mg/dL with SNR = 1. This falls within the physiological range (i.e., 30-500 mg/dL), but improvements are necessary for non-invasive in vivo glucose measurements to become viable in the future. This research group [69] in 2016 presented a new study based on MIR spectroscopy and PA detection. Here, they employed two setups. One is a fiber-coupled PA cell with a tunable QCL(quantum cascade laser) and the other is two QCLs at different wavelengths combined with PA detection. Finally, they conducted a performance test with an OGTT (oral glucose tolerance test). Here, the PA cell is conically shaped and the range of concentration of used glucose was 0-440 mg/dL.
In 2015 [70] Wadamori et al. showed a configuration of PA cells that were used in conjunction with the sample reservoir to monitor time-dependent concentration changes of glucose dissolved in distilled water. Each PA signal was obtained by averaging (1000 times) the PA signal at the modulation frequency 5.05 kHz, which is a resonance frequency for the cell. The resonator was T-shaped and the glucose concentration was measured for the range of 30-500 mg/dL.
In 2016, Sim et al. [71] illustrated a method for enhancing the sensitivity of the PAS system by aligning a resonance peak of their PA cell with a microphone. Their T-shaped cell, made up of two intersecting cylinders, enables the independent optimization of key parameters to maximize signal strength. The resonance frequency of their designed cell was 51 kHz, and the glucose concentration used was 1000 mg/dL. The same research group in 2018 [72] exhibited a T-shaped PA cell having a resonant frequency of 47.5 kHz. They introduced a method to address the challenges of MIR photoacoustic spectroscopy by capturing microscopic spatial information of the skin during the measurement. This approach allows for the selective targeting of skin areas where the IR spectra are unaffected by skin conditions, facilitating a reliable prediction of glucose levels from the PAS signal.
Zhao et al. [73] during the year 2017 demonstrated the theory of liquid photoacoustic resonance by giving a rigorous mathematical expression. A signal processing method was simultaneously demonstrated under liquid PA resonance conditions. Its feasibility and validity were confirmed through experiments using various concentrations of glucose solution. This method addresses the challenges of low sensitivity and inaccurate detection in non-resonant scenarios, yielding accurate results. The cylindrical-shaped PA cell has an excitation wavelength of 1064 nm and the transducer which is used has a peak resonant frequency of 310 kHz and the range of glucose concentration used here was 0-440mg/dL.
El-Busaidy et al. [74] represented two new approaches for simulating the PA signal in a PA open resonator using finite elements. The methods used included the amplitude mode expansion model and the viscothermal model. They validated the simulation results by comparing them with PA measurements. These approaches offer a solid foundation for designing and optimizing open resonators with enhanced sensitivity.
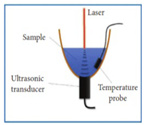
Yang et al. [75] in 2022 designed a bowl-shaped PA cell structure, which used a focused ultrasonic transducer to receive signals. In their configuration, the ultrasonic transducer was submerged in the liquid, allowing the PA signal to be generated and transmitted directly within it. The attenuation of the ultrasonic signal in liquid was minimal compared to air, enabling the device to maintain high signal accuracy.
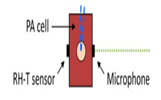
Aloraynan et al. [76] in 2023 developed a dual single wavelength QCL-based system using photoacoustic spectroscopy for noninvasive glucose measurement. They developed biomedical skin phantoms which possess quite similar properties to human skin. The detection sensitivity of their developed system was 12.5mg/dL. And finally, they developed a machine-learning model for further analysis. There used PA cell was T shaped and the range of used glucose concentration was 100-275 mg/dL.

Table 2.
A detailed summary of the recent progress of non-invasive glucose sensing using MIR-based PAS. PAC: photoacoustic cell; QCL: quantum cascade laser; PA: photoacoustic; EC: external cavity.
Table 2.
A detailed summary of the recent progress of non-invasive glucose sensing using MIR-based PAS. PAC: photoacoustic cell; QCL: quantum cascade laser; PA: photoacoustic; EC: external cavity.
| Year of Publication |
Excitation Wavelength (nm) |
Type of PA Cell | Frequency Range (kHz) |
Q-factor | Investigated Sample | Glucose level (mg/dL) |
Schematic of PA cell |
|---|---|---|---|---|---|---|---|
| 2012 [65] | 1382 & 1610 | Cylindrical shaped Fiber-coupled |
300-500 | ----- | Acquous Glucose solution |
50,100,150 |
 |
| 2012 [67] | 8196 to 10000 | T shaped | 50-54 | 102 | Fingertips of healthy&diabetes affected volunteers | <50, and <300 |  |
| 2013 [66] | 1382 to 1610 | Cylindrical shaped Fiber-coupled |
300-500 | ------ | Aqueous Glucose solution |
0-100 |
 |
| 2013 [39] | 9090 to 9132 | Conically shaped | ------ | ------- | Both in aqueous glucose soln and different body sites of human |
30–500 |
 |
| 2013 [68] | 8032 to 10000 | T shaped |
50-60 | ------ | Fingertips of healthy&diabetes affected volunteers |
30-500 |
 |
| 2015 [70] | 1550 | T shaped |
5.05 (resonance frequency of PA cell) |
------ | Aqueous Glucose solution |
30-500 |
 |
| 2016 [71] | 8064 to 11111 | T shaped |
51 (resonance frequency of PA cell) |
------ | Carbon black tape As reference sample |
1000 |
 |
| 2016 [69] | 8032 to 10000 | conically-shaped | ------- | ------- | Both in aqueous glucose solution and fingertips of human |
0–440 |
 |
| 2017 [73] | 1064 | Cylindrical shaped |
310 (resonant peak of PZT) |
------ | Aqueous Glucose solution |
20-100 |
 |
| 2018 [72] | 8000 to 11111 | T shaped | 47.5 (resonant Peak of PA cell) |
------ | Index fingertip |
------ |
 |
| 2020 [74] | ----- | T shaped | 10-60 | ----- | ------ |
----- |
 |
| 2022 [75] | 1535 | bowl-shaped structure |
0-5 ( for bandpass signal processing) |
------ | Aqueous Glucose solution |
30 to 500 |
 |
| 2023 [76] | 9250 | T shaped |
10 to 40 (With a frequency step of 0.15 kHz) |
------ | Biomedical skin phantom |
100 to 275 |
 |
4. Prospects of PAR for Noninvasive Glucose Detection
The strength of the photoacoustic signal is highly influenced by resonance amplification, and numerous studies have focused on optimizing PA sensors. Building on these insights, further improvements are necessary to achieve optimal performance. The following factors could be considered for designing highly sensitive PAR for noninvasive glucose detection.
- Finding proper geometry:
Detection sensitivity is significantly influenced by the geometric shape of the resonator. For example, in this paper [77], the authors demonstrated that the intensity of the generated PA signal is inversely proportional to the volume of a non-resonant cell. High detection sensitivity can be achieved by using a small-sized Helmholtz resonant cell. In contrast, conventional straight-type resonant cells, which have a large dead volume, result in lower detection sensitivity [78]. It is also suggested in Ref. [82] that the sensitivity of the PA system increases when the resonance peak is matched with that of the microphone used to collect the acoustic signal. Thus, to achieve an effective design, the appropriate geometry should be selected, taking into account the factors mentioned above.
To accurately determine the geometry of the PAR, the topology optimization model, integrated with pressure acoustics in the finite element method, was employed to design the PA cell and achieve the optimal structure [81]. For example, Haouari R. et al. [83] achieved an acoustic gain almost twice that of the conventional design by using a 3D topology optimization method to develop a “potato-shaped” PA cell for trace gas detection.
- Identifying proper resonant frequency of cell:
The resonant frequency of the cell should be determined through numerical acoustic analysis, employing methods such as the finite element method. Since the resonant frequency of the resonator is the most sensitive and provides the greatest amplification, it is crucial to account for acoustic losses, including viscosity and heat exchange within the cell, to ensure proper functioning [78].
- Observation of detection sensitivity and signal-to-noise ratio(SNR):
Since tissues contain various fluids, primarily water which creates background noise, so a designer needs to focus on calculating the signal-to-noise ratio (SNR) that can be achieved with the resonator. For instance, the SNR of a small-sized Helmholtz-type resonant cell was found to be approximately 69 dB, compared to 62 dB [78] for a conventional straight-type resonant cell. Both of these values are significantly higher than the required SNR of 50 dB [79,80].
- Importance of Manufacturing Accuracy:
When the PA cell is implemented, the resonant frequency can deviate significantly from the calculated and simulated values. This deviation occurs due to changes in the internal volume caused by dimensional errors introduced during the manufacturing process [78].
5. Conclusion
In this review, we concentrated on the recent advancements in the development of photoacoustic resonators, which are crucial for non-invasive glucose measurement using photoacoustic spectroscopy (PAS) in the infrared (IR) spectrum, particularly in the mid-infrared (MIR) and near-infrared (NIR) regions. PAS shows significant promise for future non-invasive techniques. The photoacoustic resonator is essential for amplifying specific modes, as the signals generated by the photoacoustic effect are inherently weak and require appropriate amplification. This work investigates and reviews optimal resonator geometries and their performance. We also discussed the primary limitations and identified the main sources of losses in resonators. Among various simulation models, we focused on the viscothermal model and the amplitude mode expansion model, as discussed in the existing literature. Finally, we highlighted the potential of IR-based PAS for non-invasive blood glucose detection, emphasizing that using a well-designed resonator could lead to more desirable outcomes. This review serves as a key reference for future research on the development of optimal photoacoustic resonators, contributing to the accurate and reliable detection of glucose.
Author Contributions
Conceptualization, M.R.K. and T.M.Z.; data curation, M.R.K. and T.M.Z.; formal analysis, M.R.K.; funding acquisition, D.B.; investigation, M.R.K., T.M.Z., ZW and S.R.; methodology, M.R.K. and T.M.Z.; project administration, D.B.; resources, D.B.; supervision, D.B.; validation, M.R.K.; visualization, M.R.K.; writing—original draft, M.R.K. and T.M.Z.; writing—review and editing, M.R.K., T.M.Z., ZW, and S.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
This work was supported by the Natural Science and Engineering Research Council (NSERC), Ontario Centre of Excellence (OCE), Mitacs and University of Waterloo, AIH Technologies Inc.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- “Diabetes.” Accessed: Jul. 25, 2024. [Online]. Available: https://www.who.int/health-topics/diabetes?gad_source=1#tab=tab_1.
- “Diabetes Facts and Figures | International Diabetes Federation.” Accessed: Jul. 25, 2024. [Online]. Available: https://idf.org/about-diabetes/diabetes-facts-figures/.
- N. H. Cho et al., “IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045,” Diabetes Res. Clin. Pract., vol. 138, pp. 271–281, Apr. 2018. [CrossRef]
- J. Lin et al., “Projection of the future diabetes burden in the United States through 2060,” Popul. Health Metr., vol. 16, no. 1, p. 9, Dec. 2018. [CrossRef]
- “Standards of Medical Care in Diabetes—2010,” Diabetes Care, vol. 33, no. Supplement_1, pp. S11–S61, Jan. 2010. [CrossRef]
- L. C. Clark and C. Lyons, “ELECTRODE SYSTEMS FOR CONTINUOUS MONITORING IN CARDIOVASCULAR SURGERY,” Ann. N. Y. Acad. Sci., vol. 102, no. 1, pp. 29–45, Oct. 1962. [CrossRef]
- W. Villena Gonzales, A. W. Villena Gonzales, A. Mobashsher, and A. Abbosh, “The Progress of Glucose Monitoring—A Review of Invasive to Minimally and Non-Invasive Techniques, Devices and Sensors,” Sensors, vol. 19, no. 4, p. 800, Feb. 2019. [CrossRef]
- “Phenobarbital - Health Encyclopedia - University of Rochester Medical Center.” 2017. Accessed: Jul. 29, 2024. [Online]. Available: https://www.urmc.rochester.edu/encyclopedia/content.aspx?ContentTypeID=167&ContentID=glucose_urine.
- D. G. Ross, “Urinalysis,” in Imaging and Technology in Urology, Cham: Springer International Publishing, 2023, pp. 171–175. [CrossRef]
- L. Tang, S. J. L. Tang, S. J. Chang, C.-J. Chen, and J.-T. Liu, “Non-Invasive Blood Glucose Monitoring Technology: A Review,” Sensors, vol. 20, no. 23, p. 6925, Dec. 2020. [CrossRef]
- H. von Lilienfeld-Toal, M. H. von Lilienfeld-Toal, M. Weidenmüller, A. Xhelaj, and W. Mäntele, “A novel approach to non-invasive glucose measurement by mid-infrared spectroscopy: The combination of quantum cascade lasers (QCL) and photoacoustic detection,” Vib. Spectrosc., vol. 38, no. 1–2, pp. 209–215, Jul. 2005. [CrossRef]
- H. D. Park, K. J. Lee, H. R. Yoon, and H. H. Nam, “Design of a portable urine glucose monitoring system for health care,” Comput. Biol. Med., vol. 35, no. 4, pp. 275–286, May 2005. [CrossRef]
- S. Panchbhai, “Correlation of Salivary Glucose Level with Blood Glucose Level in Diabetes Mellitus,” J. Oral Maxillofac. Res., vol. 3, no. 3, Jul. 2012. [CrossRef]
- S. Iguchi et al., “A flexible and wearable biosensor for tear glucose measurement,” Biomed. Microdevices, vol. 9, no. 4, pp. 603–609, Jul. 2007. [CrossRef]
- J. Moyer, D. Wilson, I. Finkelshtein, B. Wong, and R. Potts, “Correlation Between Sweat Glucose and Blood Glucose in Subjects with Diabetes,” Diabetes Technol. Ther., vol. 14, no. 5, pp. 398–402, May 2012. [CrossRef]
- S. Delbeck, T. S. Delbeck, T. Vahlsing, S. Leonhardt, G. Steiner, and H. M. Heise, “Non-invasive monitoring of blood glucose using optical methods for skin spectroscopy—opportunities and recent advances,” Anal. Bioanal. Chem., vol. 411, no. 1, pp. 63–77, Jan. 2019. [CrossRef]
- M. Pleitez, H. M. Pleitez, H. von Lilienfeld-Toal, and W. Mäntele, “Infrared spectroscopic analysis of human interstitial fluid in vitro and in vivo using FT-IR spectroscopy and pulsed quantum cascade lasers (QCL): Establishing a new approach to non invasive glucose measurement,” Spectrochim. Acta Part A Mol. Biomol. Spectrosc., vol. 85, no. 1, pp. 61–65, Jan. 2012. [CrossRef]
- “Definition of biomarker - NCI Dictionary of Cancer Terms - NCI.” Accessed: Aug. 19, 2024. [Online]. Available: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/biomarker.
- J. Huang, Y. J. Huang, Y. Zhang, and J. Wu, “Review of non-invasive continuous glucose monitoring based on impedance spectroscopy,” Sensors Actuators A Phys., vol. 311, p. 112103, Aug. 2020. [CrossRef]
- L. A. Buehler et al., “Noninvasive Glucose Monitor Using Dielectric Spectroscopy,” Endocr. Pract., vol. 28, no. 2, pp. 142–147, Feb. 2022. [CrossRef]
- Sieg, R. H. Guy, and M. B. Delgado-Charro, “Noninvasive Glucose Monitoring by Reverse Iontophoresis in Vivo: Application of the Internal Standard Concept,” Clin. Chem., vol. 50, no. 8, pp. 1383–1390, Aug. 2004. [CrossRef]
- F. Tang, X. Wang, D. Wang, and J. Li, “Non-Invasive Glucose Measurement by Use of Metabolic Heat Conformation Method,” Sensors, vol. 8, no. 5, pp. 3335–3344, May 2008. [CrossRef]
- J. Kost, “Ultrasound-Assisted Insulin Delivery and Noninvasive Glucose Sensing,” Diabetes Technol. Ther., vol. 4, no. 4, pp. 489–497, Aug. 2002. [CrossRef]
- M. R. Kaysir, J. M. R. Kaysir, J. Song, S. Rassel, A. Aloraynan, and D. Ban, “Progress and Perspectives of Mid-Infrared Photoacoustic Spectroscopy for Non-Invasive Glucose Detection,” Biosensors, vol. 13, no. 7, p. 716, Jul. 2023. [CrossRef]
- R. Ballerstadt, C. R. Ballerstadt, C. Evans, A. Gowda, and R. McNichols, “In Vivo Performance Evaluation of a Transdermal Near- Infrared Fluorescence Resonance Energy Transfer Affinity Sensor for Continuous Glucose Monitoring,” Diabetes Technol. Ther., vol. 8, no. 3, pp. 296–311, Jun. 2006. [CrossRef]
- W. March, D. W. March, D. Lazzaro, and S. Rastogi, “Fluorescent Measurement in the Non-Invasive Contact Lens Glucose Sensor,” Diabetes Technol. Ther., vol. 8, no. 3, pp. 312–317, Jun. 2006. [CrossRef]
- R. O. Esenaliev, K. V. R. O. Esenaliev, K. V. Larin, I. V. Larina, and M. Motamedi, “Noninvasive monitoring of glucose concentration with optical coherence tomography,” Opt. Lett., vol. 26, no. 13, p. 992, Jul. 2001. [CrossRef]
- M. K. Enejder et al., “Raman spectroscopy for noninvasive glucose measurements,” J. Biomed. Opt., vol. 10, no. 3, p. 031114, 2005. [CrossRef]
- J. L. Lambert, C. C. J. L. Lambert, C. C. Pelletier, and M. Borchert, “Glucose determination in human aqueous humor with Raman spectroscopy,” J. Biomed. Opt., vol. 10, no. 3, p. 031110, 2005. [CrossRef]
- K. Maruo, M. K. Maruo, M. Tsurugi, M. Tamura, and Y. Ozaki, “In Vivo Noninvasive Measurement of Blood Glucose by Near-Infrared Diffuse-Reflectance Spectroscopy,” Appl. Spectrosc., vol. 57, no. 10, pp. 1236–1244, Oct. 2003. [CrossRef]
- R. Marbach, T. R. Marbach, T. Koschinsky, F. A. Gries, and H. M. Heise, “Noninvasive Blood Glucose Assay by Near-Infrared Diffuse Reflectance Spectroscopy of the Human Inner Lip,” Appl. Spectrosc., vol. 47, no. 7, pp. 875–881, Jul. 1993. [CrossRef]
- H. Malik and G. L. Coté, “Real-time, closed-loop dual-wavelength optical polarimetry for glucose monitoring,” J. Biomed. Opt., vol. 15, no. 1, p. 017002, 2010. [CrossRef]
- G. Purvinis, B. D. G. Purvinis, B. D. Cameron, and D. M. Altrogge, “Noninvasive Polarimetric-Based Glucose Monitoring: An in Vivo Study,” J. Diabetes Sci. Technol., vol. 5, no. 2, pp. 380–387, Mar. 2011. [CrossRef]
- Vrančić et al., “Continuous glucose monitoring by means of mid-infrared transmission laser spectroscopy in vitro,” Analyst, vol. 136, no. 6, p. 1192, 2011. https://doi.org/10.1039/c0an00537a. [CrossRef]
- G. Spanner and R. Nie�ner, “New concept for the non-invasive determination of physiological glucose concentrations using modulated laser diodes,” Anal. Bioanal. Chem., vol. 354, no. 3, pp. 306–310, Jan. 1996. [CrossRef]
- J. Kottmann, J. M. J. Kottmann, J. M. Rey, and M. W. Sigrist, “New photoacoustic cell design for studying aqueous solutions and gels,” Rev. Sci. Instrum., vol. 82, no. 8, Aug. 2011. [CrossRef]
- G. Spanner and R. Niessner, “Noninvasive determination of blood constituents using an array of modulated laser diodes and a photoacoustic sensor head,” Anal. Bioanal. Chem., vol. 355, no. 3–4, pp. 327–328, Jun. 1996. [CrossRef]
- P. P. Pai, P. K. Sanki, and S. Banerjee, “A photoacoustics based continuous non-invasive blood glucose monitoring system,” in 2015 IEEE International Symposium on Medical Measurements and Applications (MeMeA) Proceedings, IEEE, May 2015, pp. 106–111. [CrossRef]
- J. Kottmann, U. J. Kottmann, U. Grob, J. Rey, and M. Sigrist, “Mid-Infrared Fiber-Coupled Photoacoustic Sensor for Biomedical Applications,” Sensors, vol. 13, no. 1, pp. 535–549, Jan. 2013. [CrossRef]
- M. A. Pleitez, T. M. A. Pleitez, T. Lieblein, A. Bauer, O. Hertzberg, H. von Lilienfeld-Toal, and W. Mäntele, “In Vivo Noninvasive Monitoring of Glucose Concentration in Human Epidermis by Mid-Infrared Pulsed Photoacoustic Spectroscopy,” Anal. Chem., vol. 85, no. 2, pp. 1013–1020, 2013. [CrossRef]
- P. Beard, “Biomedical photoacoustic imaging,” Interface Focus, vol. 1, no. 4, pp. 602–631, Aug. 2011. [CrossRef]
- J. Kottmann, J. J. Kottmann, J. Rey, and M. Sigrist, “Mid-Infrared Photoacoustic Detection of Glucose in Human Skin: Towards Non-Invasive Diagnostics,” Sensors, vol. 16, no. 10, p. 1663, Oct. 2016. [CrossRef]
- G. B. Christison and H. A. MacKenzie, “Laser photoacoustic determination of physiological glucose concentrations in human whole blood,” Med. Biol. Eng. Comput., vol. 31, no. 3, pp. 284–290, May 1993. [CrossRef]
- R. Fakhlaei et al., “Application, challenges and future prospects of recent nondestructive techniques based on the electromagnetic spectrum in food quality and safety,” Food Chem., vol. 441, p. 138402, May 2024. [CrossRef]
- J. Yadav, A. J. Yadav, A. Rani, V. Singh, and B. M. Murari, “Prospects and limitations of non-invasive blood glucose monitoring using near-infrared spectroscopy,” Biomed. Signal Process. Control, vol. 18, pp. 214–227, Apr. 2015. [CrossRef]
- J. J. Burmeister and M. A. Arnold, “Evaluation of Measurement Sites for Noninvasive Blood Glucose Sensing with Near-Infrared Transmission Spectroscopy,” Clin. Chem., vol. 45, no. 9, pp. 1621–1627, Sep. 1999. [CrossRef]
- J. T. Olesberg, M. A. J. T. Olesberg, M. A. Arnold, C. Mermelstein, J. Schmitz, and J. Wagner, “Tunable Laser Diode System for Noninvasive Blood Glucose Measurements,” Appl. Spectrosc., vol. 59, no. 12, pp. 1480–1484, Dec. 2005. [CrossRef]
- V. V. Tuchin, Ed., Handbook of Optical Sensing of Glucose in Biological Fluids and Tissues. CRC Press, 2008. [CrossRef]
- S. N. Thennadil, J. L. S. N. Thennadil, J. L. Rennert, B. J. Wenzel, K. H. Hazen, T. L. Ruchti, and M. B. Block, “Comparison of Glucose Concentration in Interstitial Fluid, and Capillary and Venous Blood During Rapid Changes in Blood Glucose Levels,” Diabetes Technol. Ther., vol. 3, no. 3, pp. 357–365, Sep. 2001. [CrossRef]
- S. Liakat, K. A. S. Liakat, K. A. Bors, T.-Y. Huang, A. P. M. Michel, E. Zanghi, and C. F. Gmachl, “In vitro measurements of physiological glucose concentrations in biological fluids using mid-infrared light,” Biomed. Opt. Express, vol. 4, no. 7, p. 1083, Jul. 2013. [CrossRef]
- Rosencwaig, “Photoacoustic Spectroscopy of Biological Materials,” Science (80-. )., vol. 181, no. 4100, pp. 657–658, Aug. 1973. [CrossRef]
- K. Maruo and Y. Yamada, “Near-infrared noninvasive blood glucose prediction without using multivariate analyses: introduction of imaginary spectra due to scattering change in the skin,” J. Biomed. Opt., vol. 20, no. 4, p. 047003, 2015. [CrossRef]
- H. A. MacKenzie et al., “Advances in Photoacoustic Noninvasive Glucose Testing,” Clin. Chem., vol. 45, no. 9, pp. 1587–1595, Sep. 1999. [CrossRef]
- S. El-Busaidy, B. S. El-Busaidy, B. Baumann, M. Wolff, L. Duggen, and H. Bruhns, “Experimental and Numerical Investigation of a Photoacoustic Resonator for Solid Samples: Towards a Non-Invasive Glucose Sensor,” Sensors, vol. 19, no. 13, p. 2889, Jun. 2019. [CrossRef]
- Cox, J. G. Laufer, S. R. Arridge, and P. C. Beard, “Quantitative spectroscopic photoacoustic imaging: a review,” J. Biomed. Opt., vol. 17, no. 6, p. 061202, 2012. [CrossRef]
- Rosenthal, V. Ntziachristos, and D. Razansky, “Model-based optoacoustic inversion with arbitrary-shape detectors,” Med. Phys., vol. 38, no. 7, pp. 4285–4295, Jul. 2011. [CrossRef]
- L. Nie and X. Chen, “Structural and functional photoacoustic molecular tomography aided by emerging contrast agents,” Chem. Soc. Rev., vol. 43, no. 20, pp. 7132–7170, 2014. [CrossRef]
- Baumann, B. Kost, M. Wolff, and H. Groning, “Modeling and Numerical Investigation of Photoacoustic Resonators,” Model. Simul., 2008. [CrossRef]
- L. Duggen, N. L. Duggen, N. Lopes, M. Willatzen, and H.-G. Rubahn, “Finite Element Simulation of Photoacoustic Pressure in a Resonant Photoacoustic Cell Using Lossy Boundary Conditions,” Int. J. Thermophys., vol. 32, no. 4, pp. 774–785, Apr. 2011. [CrossRef]
- Glière, J. Rouxel, M. Brun, B. Parvitte, V. Zéninari, and S. Nicoletti, “Challenges in the Design and Fabrication of a Lab-on-a-Chip Photoacoustic Gas Sensor,” Sensors, vol. 14, no. 1, pp. 957–974, Jan. 2014. [CrossRef]
- Baumann, M. Wolff, B. Kost, and H. Groninga, “Finite element calculation of photoacoustic signals,” Appl. Opt., vol. 46, no. 7, p. 1120, Mar. 2007. [CrossRef]
- M. A. Pleitez, T. M. A. Pleitez, T. Lieblein, A. Bauer, O. Hertzberg, H. von Lilienfeld-Toal, and W. Mäntele, “Windowless ultrasound photoacoustic cell for in vivo mid-IR spectroscopy of human epidermis: Low interference by changes of air pressure, temperature, and humidity caused by skin contact opens the possibility for a non-invasive monitoring of glucose in th,” Rev. Sci. Instrum., vol. 84, no. 8, Aug. 2013. [CrossRef]
- J. Y. Sim, C.-G. J. Y. Sim, C.-G. Ahn, E.-J. Jeong, and B. K. Kim, “In vivo Microscopic Photoacoustic Spectroscopy for Non-Invasive Glucose Monitoring Invulnerable to Skin Secretion Products,” Sci. Rep., vol. 8, no. 1, p. 1059, Jan. 2018. [CrossRef]
- S. El-Busaidy, B. S. El-Busaidy, B. Baumann, M. Wolff, and L. Duggen, “Shape optimization of an open photoacoustic resonator,” Appl. Sci., vol. 11, no. 6, pp. 1–11, 2021. [CrossRef]
- S. Camou, T. S. Camou, T. Haga, T. Tajima, and E. Tamechika, “Detection of aqueous glucose based on a cavity size- and optical-wavelength-independent continuous-wave photoacoustic technique,” Anal. Chem., vol. 84, no. 11, pp. 4718–4724, 2012. [CrossRef]
- Sensors Council, Annual IEEE Computer Conference, M. IEEE Sensors Conference 12 2013.11.03-06 Baltimore, and M. IEEE Sensors Conference 12 2013.11.04-06 Baltimore, IEEE sensors, 2013 3-6 Nov. 2013, Baltimore, Maryland, USA ; proceedings ; the 12th IEEE Sensors Conference.
- M. A. Pleitez, T. M. A. Pleitez, T. Lieblein, A. Bauer, O. Hertzberg, H. von Lilienfeld-Toal, and W. Mäntele, “In Vivo Noninvasive Monitoring of Glucose Concentration in Human Epidermis by Mid-Infrared Pulsed Photoacoustic Spectroscopy,” Anal. Chem., vol. 85, no. 2, pp. 1013–1020, Jan. 2013. [CrossRef]
- M. A. Pleitez, T. M. A. Pleitez, T. Lieblein, A. Bauer, O. Hertzberg, H. Von Lilienfeld-Toal, and W. Mäntele, “Windowless ultrasound photoacoustic cell for in vivo mid-IR spectroscopy of human epidermis: Low interference by changes of air pressure, temperature, and humidity caused by skin contact opens the possibility for a non-invasive monitoring of glucose in th,” Rev. Sci. Instrum., vol. 84, no. 8, 2013. [CrossRef]
- J. Kottmann, J. M. J. Kottmann, J. M. Rey, and M. W. Sigrist, “Mid-infrared photoacoustic detection of glucose in human skin: Towards non-invasive diagnostics,” Sensors (Switzerland), vol. 16, no. 10, Oct. 2016. [CrossRef]
- N. Wadamori, “Behavior of long-period measurements using a small-sized photoacoustic cell for aqueous glucose monitoring,” in 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), IEEE, Aug. 2015, pp. 1267–1270. [CrossRef]
- J. Y. Sim, C.-G. J. Y. Sim, C.-G. Ahn, E. Jeong, and B. K. Kim, “Photoacoustic spectroscopy that uses a resonant characteristic of a microphone for in vitro measurements of glucose concentration,” in 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), IEEE, Aug. 2016, pp. 4861–4864. [CrossRef]
- J. Y. Sim, C. G. J. Y. Sim, C. G. Ahn, E. J. Jeong, and B. K. Kim, “In vivo Microscopic Photoacoustic Spectroscopy for Non-Invasive Glucose Monitoring Invulnerable to Skin Secretion Products,” Sci. Rep., vol. 8, no. 1, pp. 1–11, 2018. [CrossRef]
- S. Zhao, W. S. Zhao, W. Tao, Q. He, H. Zhao, and H. Yang, “Glucose solution determination based on liquid photoacoustic resonance,” Appl. Opt., vol. 56, no. 2, p. 193, 2017. [CrossRef]
- S. A. S. El-Busaidy, B. Baumann, M. Wolff, and L. Duggen, “Modelling of open photoacoustic resonators,” Photoacoustics, vol. 18, no. December 2019, 2020. [CrossRef]
- L. Yang, C. L. Yang, C. Chen, Z. Zhang, and X. Wei, “Glucose Determination by a Single 1535 nm Pulsed Photoacoustic Technique: A Multiple Calibration for the External Factors,” J. Healthc. Eng., vol. 2022, pp. 1–10, Sep. 2022. [CrossRef]
- Aloraynan, S. Rassel, M. R. Kaysir, and D. Ban, “Dual quantum cascade lasers for noninvasive glucose detection using photoacoustic spectroscopy,” Sci. Rep., vol. 13, no. 1, pp. 1–9, 2023. [CrossRef]
- Y. ISHIHARA and N. WADAMORI, “A Study on Enhancement of Sensitivity of a PhotoAcoustic Detector Cell for Non-invasive Measurements Based on Finite Element Method Analysis(Symposium on Biomedical Engineering 2007),” Trans. Japanese Soc. Med. Biol. Eng. BME, vol. 46, no. 2, pp. 238–245, 2008.
- K. Tachibana, K. K. Tachibana, K. Okada, R. Kobayashi, and Y. Ishihara, “Development of a high-sensitivity and portable cell using Helmholtz resonance for noninvasive blood glucose-level measurement based on photoacoustic spectroscopy,” Proc. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. EMBS, vol. 2016-October, pp. 6477–6480, 2016. [CrossRef]
- R. Takamoto, R. R. Takamoto, R. Namba, M. Matsuoka, and T. Sawada, “Human in vivo percutaneous absorptiometry using the laser-photoacoustic method,” Anal. Chem., vol. 64, no. 21, pp. 2661–2663, Nov. 1992. [CrossRef]
- R. Takamoto, S. R. Takamoto, S. Yamamoto, R. Namba, T. Takamatsu, M. Matsuoka, and T. Sawada, “In vivo Percutaneous Absorptiometry by a Laser Photoacoustic Method Using a Novel Open-Ended Cell Combined with Light Guide,” Anal. Chem., vol. 66, no. 14, pp. 2267–2271, Jul. 1994. [CrossRef]
- Tang Z, Ni W, Li Z, Hou J, Chen S, Shum PP, Yang C. Performance Enhancement of Opened Resonance Photoacoustic Cells Based on Three Dimensional Topology Optimization. Photonics. 2021; 8(9):380. [CrossRef]
- J. Y. Sim, C. J. Y. Sim, C. -G. Ahn, E. Jeong and B. K. Kim, “Photoacoustic spectroscopy that uses a resonant characteristic of a microphone for in vitro measurements of glucose concentration,” 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 2016, pp. 4861-4864. [CrossRef]
- Haouari, R.; Rochus, V.; Lagae, L.; Rottenberg, X. Topology Optimization of an Acoustical Cell for Gaseous Photoacoustic Spectroscopy using COMSOL Multiphysics. In Proceedings of the 2017 COMSOL Conference in Rotterdam, Rotherdam, UK, 16 November 2017.
Figure 1.
General classification of overall glucose measurement techniques covering both invasive and noninvasive methods.
Figure 1.
General classification of overall glucose measurement techniques covering both invasive and noninvasive methods.
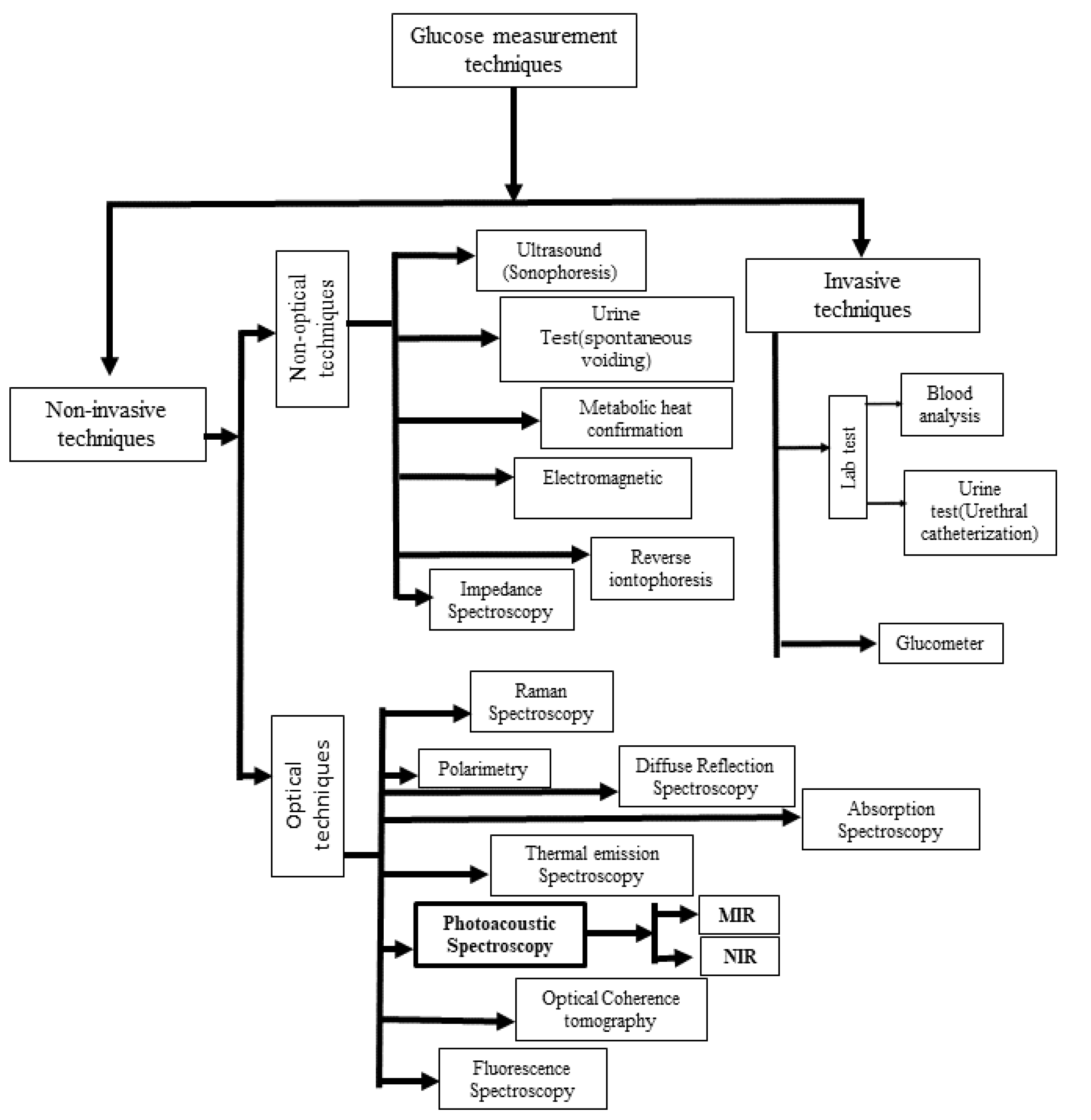
Figure 2.
(a) Schematic representation of the components of human skin [42].
Figure 2.
(a) Schematic representation of the components of human skin [42].
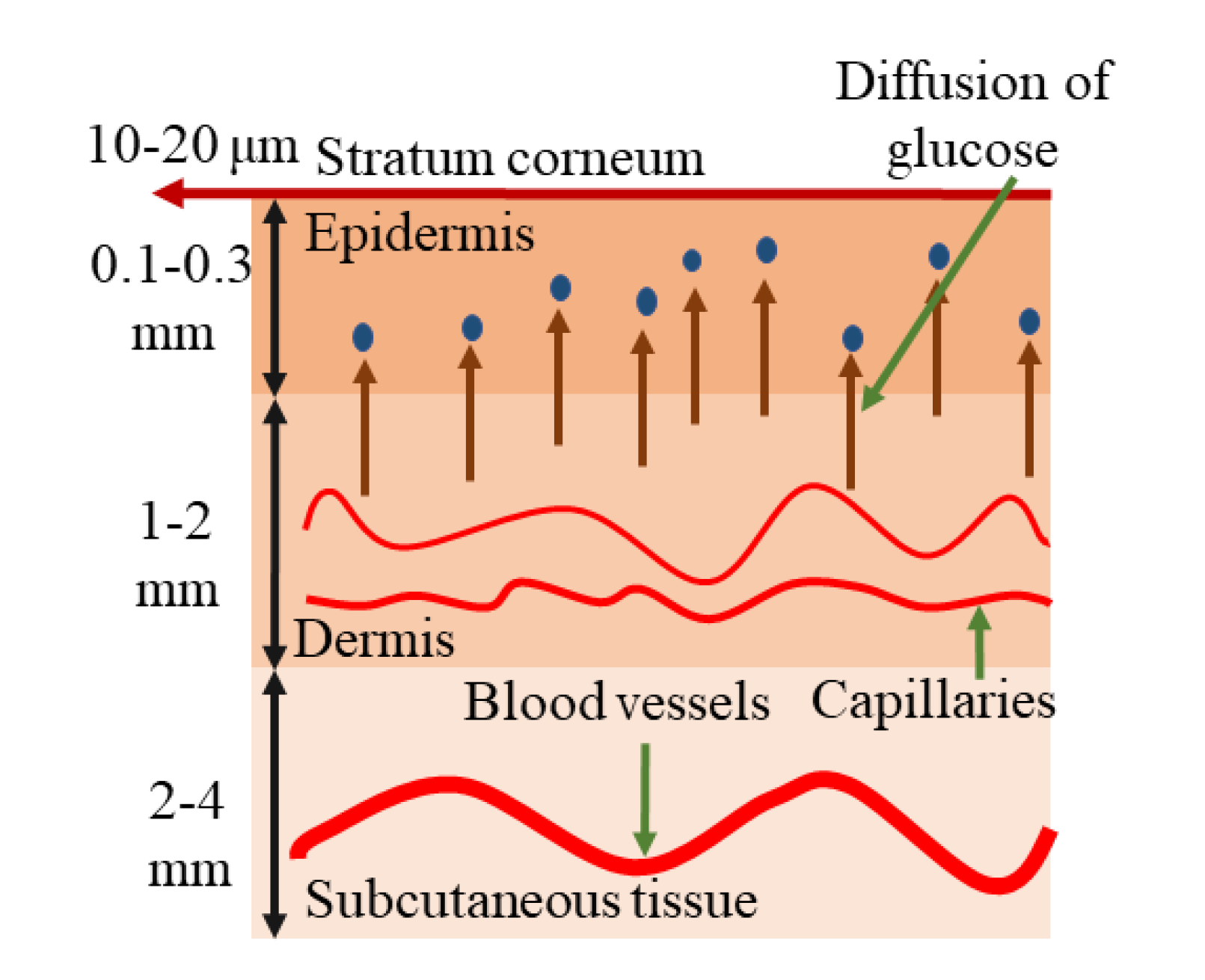
Figure 3.
(a) Absorption spectrum for aqueous glucose in the MIR region extending from 800 cm-1 to 1600 cm-1 [45], and (b) Absorption spectrum of glucose for NIR region from 5550 cm-1 to 7400 cm-1 [52].
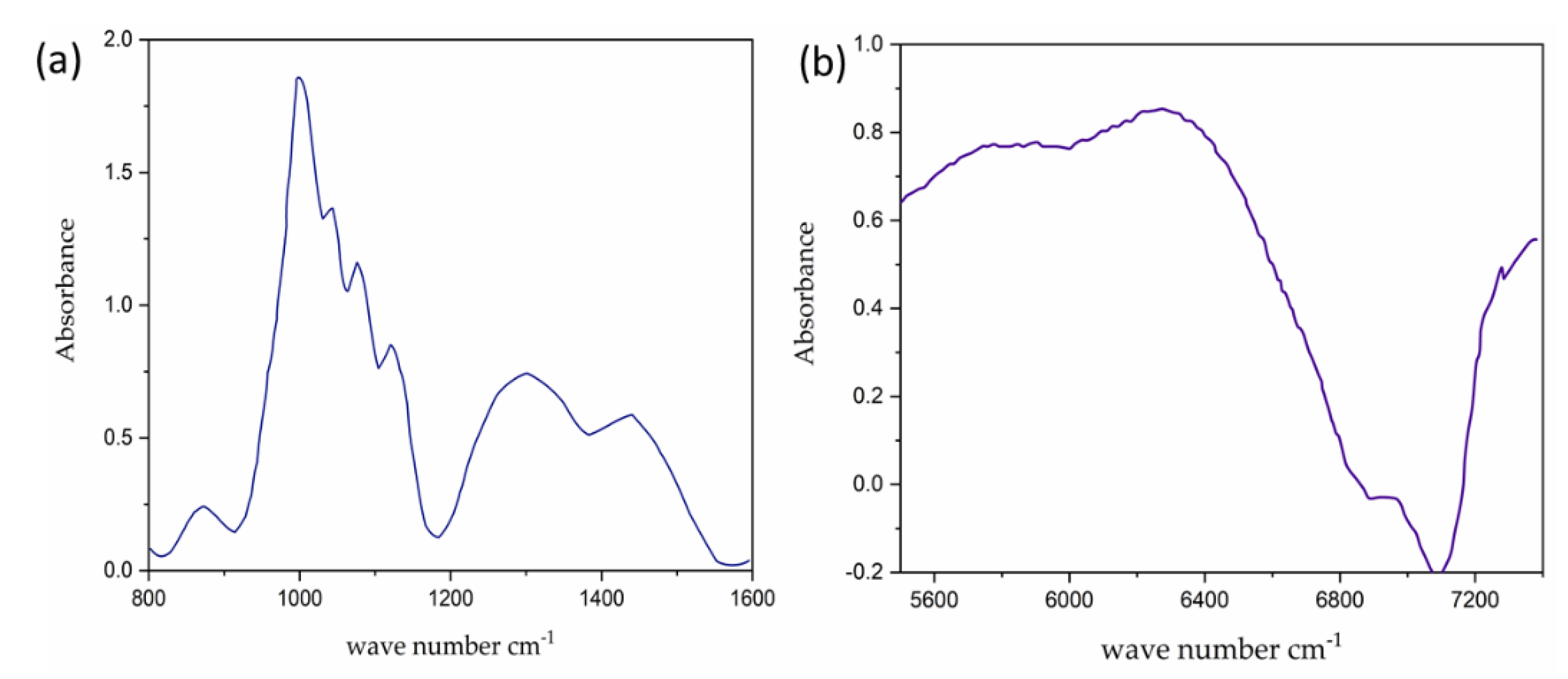
Figure 4.
The basic experimental setup for the generation and detection of acoustic signal used in PAS [MIC: Microphone, PAR: Photoacoustic Resonator].
Figure 4.
The basic experimental setup for the generation and detection of acoustic signal used in PAS [MIC: Microphone, PAR: Photoacoustic Resonator].
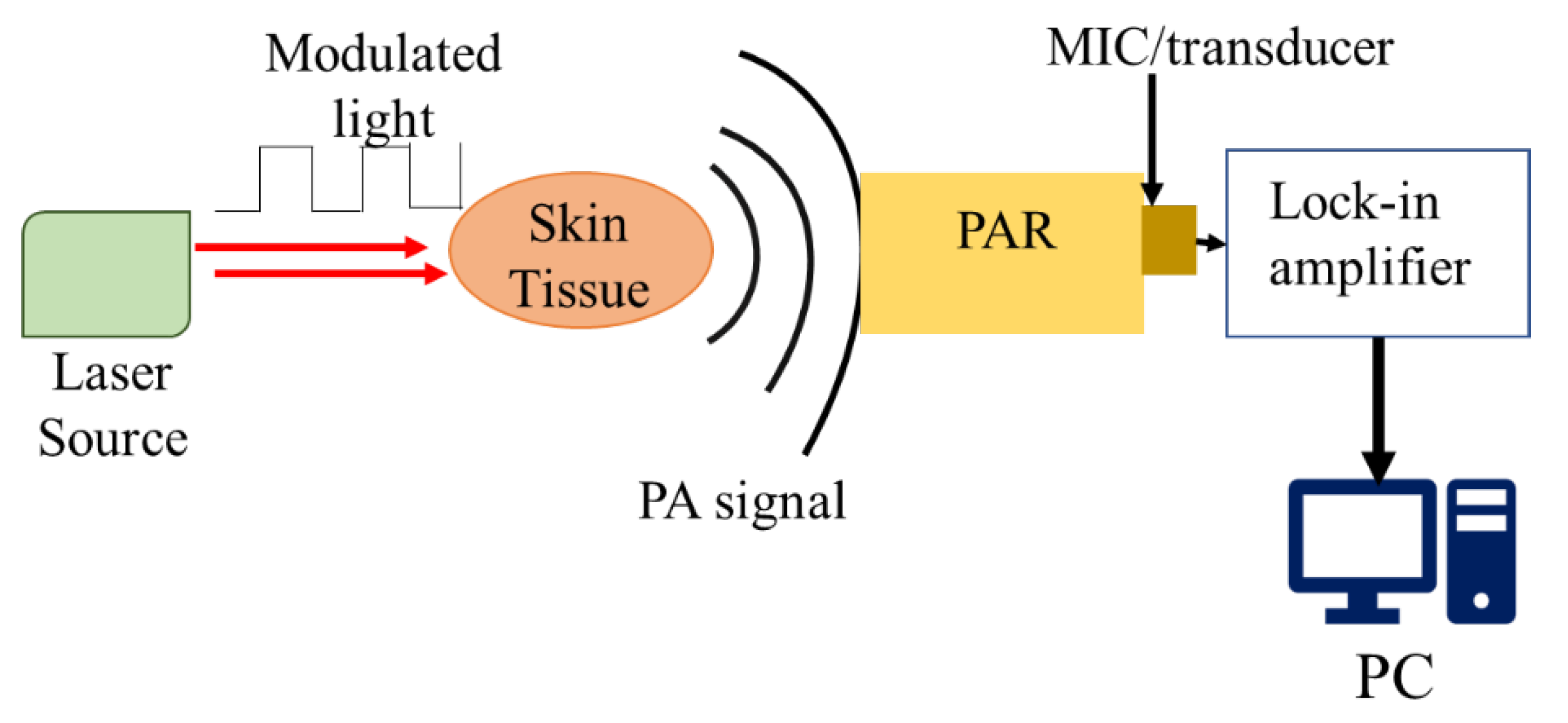
Figure 5.
(a) Schematic representation of a typical T-type PAR, and (b) The frequency response of a PAR, (c, d) Profile of acoustic mode at the peak frequencies at 49.5 kHz and 22.2 kHz, respectively corresponding to Fig. (b) [54].
Figure 5.
(a) Schematic representation of a typical T-type PAR, and (b) The frequency response of a PAR, (c, d) Profile of acoustic mode at the peak frequencies at 49.5 kHz and 22.2 kHz, respectively corresponding to Fig. (b) [54].

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



