
Submitted:
01 October 2024
Posted:
02 October 2024
You are already at the latest version
Abstract
This scoping review aims to systematically examine and analyse the available literature on pure total talar dislocation, focusing on its epidemiology, clinical presentation, imaging techniques, surgical options, rehabilitation protocols, and complications. Following the PRISMA-ScR guidelines, a comprehensive search was conducted across PubMed, Web of Science, and Scopus databases. The search yielded 185 articles, from which 30 met the inclusion criteria, focusing on pure total talar dislocation without fractures. Data from each study were extracted, including patient demographics, injury characteristics, treatment methods, and outcomes. A total of 30 articles were included in this review after screening and quality assessment by five independent reviewers. The studies included case reports, case series, and reviews. Despite the heterogeneity of available studies, key findings suggested that early reduction, careful wound management, and soft tissue preservation are crucial in minimising complications such as avascular necrosis (AVN), post-traumatic arthritis, and infection. Long-term outcomes varied, and the risk of AVN remained high, particularly in cases with compromised blood supply to the talus. Pure total talar dislocation is a rare and challenging condition with no established management protocol. While talar reimplantation and joint fixation offer promising outcomes in preserving function, the risk of complications, particularly AVN, remains significant. Further research is needed to standardise treatment protocols and improve clinical outcomes for this rare but severe injury.
Keywords:
Total Talar Dislocation
; Pure Total Talar Dislocation
; Missing Talus
; Pantalar Dislocation
; Hawkin’s Sign
1. Introduction
Pantalar dislocations without an associated fracture, defined also as pure total talar dislocation, is a rare ankle lesion that accounts 0.06% of all dislocations and only 2% of all talar injuries [1]. In 1680, Fabricius von Hildanus the “father of German surgery” reported the first case of total talar dislocation without concomitant fracture [2].
Ankle injuries involving the talus can be severe. High-energy traumas can cause complete talus dislocation, affecting multiple joints. The talus, lacking muscular attachments, is prone to dislocation. This injury typically results from the ankle pointing downward and twisting outward [3].
Pantalar dislocation is usually an open injury involving nearby ligaments, capsular attachments, and bones (malleoli, navicular, or calcaneus). It also often leads to soft tissue damage, wound contamination, and disruption of the talar blood supply [4]. In particular, the missing talus is defined as a completely extruded talus lesion without remaining soft tissue attachments [5].
Pantalar dislocation is rare in orthopedic literature, making it challenging for surgeons to fully understand and treat. While there's no standard protocol, prompt treatment can reduce complications and improve outcomes. To preserve the blood supply of the talus, perform an early closed reduction. If this fails, do an open reduction [6,7].
Different methods can be used to stabilize the joint, depending on the surgeon's experience. In cases of missing talus, reattaching the native talus after thorough irrigation and debridement is recommended, despite the increased risk of complications such as avascular necrosis, infection, and posttraumatic arthritis, which may require secondary surgeries like primary talectomy and tibio-calcaneal arthrodesis [6,8].
This review aims to analyze all available literature on pure total talar dislocation, highlighting its epidemiological data, clinical and imaging characteristics, management, treatment, and outcomes.
2. Materials and Methods
2.1 Search Selection
This scoping review was completed following the PRISMA Extension for Scoping Reviews (PRISMA-ScR) recommendations.
The aim was to summarise the main features about pure pantalar dislocation, analysing all the available studies in literature and excluding articles that contained associated talar fractures. The presence of talus osteochondral defects did not represent an exclusion criterion.
The main electronic databases (Pubmed, Web of Science, Scopus) were explored by all the authors (M.D.C, E.D, M.A.M, S.P and A.S). The research keywords use were (("pantalar dislocation" OR "pantalar dislocations") OR ("total talar dislocation" OR "total talar dislocations" OR "total talar extrusion" OR "total talus dislocation")) NOT (fracture). MesSH terms were included. The study had no temporal limitation about studies publication. A total of n= 185 articles were found. Studies providing any level of evidence about pure total talar dislocation were considered eligible for this study.
2.2. Inclusion and Exclusion Criteria
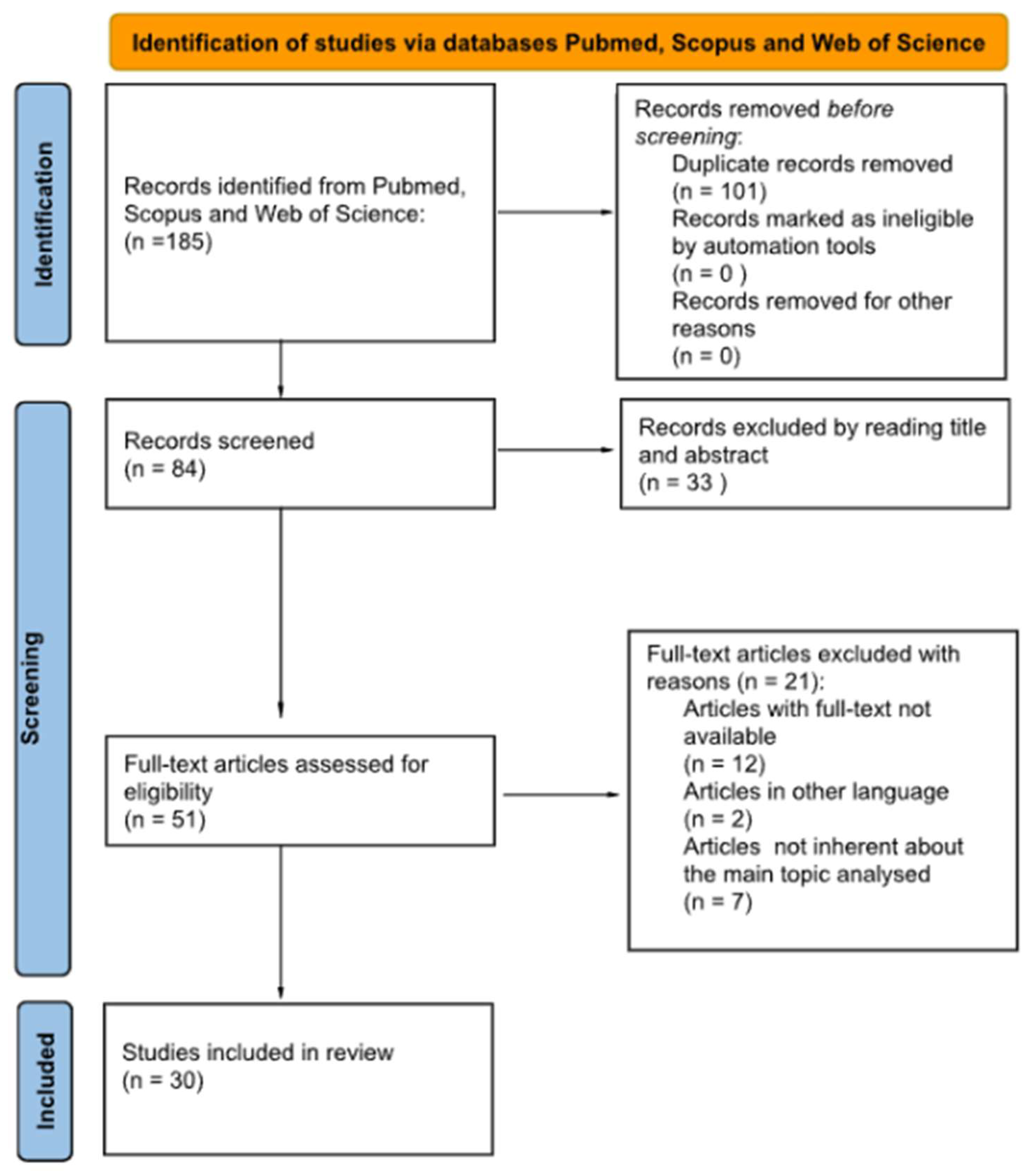
In the identification phase, a total of 185 articles were found. Out of these, 101 studies were excluded because they were reported more than once. After the first preliminary screening, 33 articles were removed because their titles or abstracts were not consistent with the main topic.
2.3. Data Extraction
The main parameters in each article were collected including the epidemiology, clinical and radiological presentation, treatment, rehabilitation and complications.
2.4. Quality Assessment
Five authors (M.D.C, E.D, M.A.M, S.P and A.S) individually read the selected articles, evaluating and discussing their quality. The senior author (V.P.) with his experience intervened in doubt cases.
3. Results
After conducting an initial screening, five authors (M.D.C, E.D, M.A.M, S.P, and A.S) selected 51 articles for full-text reading. In the second screening phase, they excluded articles with unavailable full text, non-English articles, and those not related to the main topic, resulting in 30 eligible articles based on inclusion criteria. Any uncertainties during the selection process were resolved with the help of the senior author. All authors collectively re-evaluated their choices to ensure accuracy, and the PRISM flow-chart is depicted in Figure 1.
The reference lists in the chosen articles were examined. The selected articles are summarized in Table 1.
| Author | Year | Title | Type of Study | N° of patients | Open/Closed dislocation | Reduction | Treatment | Follow-up (Months) |
| AlMaeen | 2020 | Complete Revascularization of Reimplanted Talus After Isolated Total Talar Extrusion: A Case Report | Case report | 1 | Open | Open | Cast | 12 |
| Apostle | 2010 | Reimplantation of a Totally Extruded Talus | Case report | 1 | Open (Missing talus) | - | K-wires fixation | 60 |
| Boden | 2017 | Complications and Functional Outcomes After Pantalar Dislocation | Case report | 19 | 14 Open, 5 Closed | 17 Open, 2 Closed | External fixator (9), K-wires fixation (4), K-wires + External fixator (3), Transtibial amputation (1) | 41 (3-157) |
| Breccia | 2014 | Treatment and outcome of Open dislocation of the ankle with complete talar extrusion: a case report | Case report | 1 | Open | Open | External fixator | 18 |
| Bugallo | 2021 | Closed posteromedial total talus and fibula dislocation without fracture. | Case report | 1 | Closed | Open | Cast | 2 |
| Burston | 2010 | Open total talus dislocation: clinical and functional outcomes: a case series | Case series + Literature review | 8 | Open (1 Missing talus) | Open | Cast (3), External fixator (2), Temporary External fixator (1), K-wires+ Screws fixation (1), Screws fixation (1) | 42 (13-72) |
| Eda | 2021 | Closed total talar dislocation without fracture in a rare college athlete case | Case report | 1 | Closed | Closed | Cast | 18 |
| Fleming | 2009 | Total talar extrusion: a case report | Case report | 1 | Open | Open | External fixator followed by Cast | 12 |
| Genena | 2020 | A Case Report of an Open Pan-Talar Dislocation | Case report | 1 | Open | Open | Steinmann pin | 12 |
| Gopisankar | 2012 | A rare case of Closed pantalar dislocation combined with Lisfranc's injury--The unusual complex | Case report | 1 | Closed | Closed | K-wires fixation + Cast | 12 |
| Gursu | 2013 | Closed total dislocation of talus without any accompanying fractures | Case report | 1 | Closed | Open | Cast | 24 |
| Karampinas | 2014 | Open talar dislocations without associated fractures | Retrospective | 9 | Open | Open | Steinmann pins + External fixator | 19-23 |
| Khan | 2022 | Pantalar dislocation: a rare presentation with review of treatment method | Case report + Literature review | 1 | Closed | Open | K-wires fixation + Splint | 6 |
| Kumar | 2014 | Closed Talar Dislocation without Associated Fracture a Very Rare Injury, a Case Report | Case report | 1 | Closed | Closed | K-wires fixation + Cast | 12 |
| Kwak | 2017 | Six-year survival of reimplanted talus after isolated total talar extrusion: a case report | Case report | 1 | Open | Open | K-wires fixation + External fixator | 72 |
| Lee | 2014 | Total talar extrusion without soft tissue attachments | Case series | 2 | Open (Missing talus) | - | External fixator with Antibiotic cement spacer followed by Ilizarov External fixator and Bone graft Arthrodesis (1), Reimplantation and Subtalar Fusion with Screws (1) | 24-96 |
| Leonetti | 2023 | Total Talar Prosthesis, Learning from Experience, Two Reports of Total Talar Prosthesis after Talar Extrusion and Literature Review | Case series + Literature review | 2 | Open (Missing talus) | - | External fixator with Antibiotic cement spacer followed by Reimplantation and Arthrodesis, Total Talar Replacement and final Triple Arthrodesis (1), external fixator with antibiotic cement spacer followed Total Talar Replacement and final Total Ankle Prosthesis (1) | 60 |
| Mohindra | 2014 | Early reimplantation for Open total talar extrusion | Retrospective | 7 | Open | Open | K-wires + External fixator (5), Tension Band Wiring + Splint (2) | 32 (24-46) |
| Nanjayan | 2014 | Total dislocation of the talus: a case report. Foot Ankle | Case report | 1 | Closed | Closed | Cast | 24 |
| Papanikolaou | 2002 | Successful treatment of total talar dislocation with Closed reduction: A case report | Case report | 1 | Closed | Closed | Steinmann pin | 30 |
| Ranalli | 2016 | Rehabilitation Following a Traumatic Dislocation of the Talus: A Case Study | Case study | 1 | Open | Open | Splint | 6 |
| Ritsema | 1988 | Total talar dislocation | Retrospective | 5 | Closed | Open | ----- | 48 (36-72) |
| Ruatti | 2017 | Replacement after Talar Extrusion | Case report | 1 | Open | Open | Antibiotic cement spacer followed by Total Ankle Prosthesis | 24 |
| Sié | 2014 | Delayed debridement of an Open total talar dislocation reimplanted in the emergency room | Case report | 1 | Open | Open | Splint | 12 |
| Steinmetz | 2017 | Isolated Open Total Talar Dislocation: A Case Report and Literature Review | Case report | 1 | Open | Open | External fixator | 18 |
| Taymaz | 2005 | Complete dislocation of the talus unaccompanied by fracture | Case report | 1 | Closed | Closed | Cast | 48 |
| Vaienti | 2011 | Therapeutic management of complicated talar extrusion: Literature review and case report | Case report | 1 | Open (Missing talus) | / | External fixator with Antibiotic cement spacer followed by Talar Reimplantation and Arthrodesis | |
| Wagner | 2004 | Talar dislocations | Retrospective | 6 | 2 Open, 4 Closed | Open | Secondary Arthrodesis (4), K-wires fixation (1), External fixator (1), | 76 (9-204) |
| Weston | 2015 | Systematic Review of Total Dislocation of the Talus | Systematic review | 29*/86 (no fractures of the talus or adjacent bones) |
21 Open, 8 Closed | 27 Open, 2 Closed | Internal fixation (10), K-wires fixation (4), Screws (3), Pins (1) - External fixation (10), Arthrodesis (8) |
32 |
| Yapici | 2019 | Open reduction of a total talar dislocation: A case report and review of the literature | Case report + Literature review | 1 | Closed | Open | K-wires fixation + Cast | 36 |
4. Discussion
4.1. Definition and History
The talus bone has a rich history, being used in divination, gambling, and early forms of gaming. It was made into dice-like objects and used in rituals and entertainment. In Ancient Greek, the word "astragalos" referred to both the bone itself and the game played with it. In Latin, the bone was called "talus" (plural "tali"), a term that also referred to both the bone and the dice crafted from it.
The role of the talus in trauma medicine, particularly in cases of dislocation, is also compelling. In the modern era, Fabricius von Hildanus, the “father of German surgery,” made the first account of a talus fracture in 1608. The same Hildanus reported the first case of talar dislocation treated by telectomy in 1680 in the opera called observationum et curationum medico-chirurgicarum, quae exstant omnia [2].
In 1853, Broca described this type of trauma as a severe injury, which can lead to the expulsion of the talus from all its ligamentous connections, and used the term "enucleation" to drastically define this condition [9].
“Aviator's talus” was a term related to war. Anderson mentioned it in 1919 [10], and, in 1952, Coltart adopted this term to describe talar dislocations and fracture-dislocations, as these injuries were often observed in airplane crashes [11].
Talar dislocations can be categorized based on their involvement in different joints. They are classified as mono-articular dislocations (occurring within the talocrural joint), bi-articular dislocations (affecting both the talocalcaneal and talonavicular joints), or tri-articular dislocations (involving the talocrural, talocalcaneal, and talonavicular joints), which are also known as luxatio tali totalis [12].
4.2. Epidemiology
Total talar dislocation is defined as the dislocation of the talus from the tibiotalar, talocalcaneal, and talonavicular joints, and it could be referred to as "floating foot" [13].
It accounts for only 3.4% of talar injuries, with a total extrusion without concomitant fracture being even rarer, being only 0.06% of all dislocations and 2% of talar injuries [14]. However, it appears that as trauma kinetics have changed over time, total dislocation is becoming more frequent [15].
The usual mechanism of talus dislocation involves a combination of plantar flexion with either supination or pronation of the foot [16]. Despite the lack of muscular or tendinous attachments on the talus, which theoretically increases its own vulnerability to dislocation, this injury is rare due to the talus’s deep position within the tibio-peroneal mortise [17].
The talus's position is primarily maintained by its ligamentous support, including the anterior/posterior tibiotalar deltoid ligaments medially, the anterior/posterior talofibular ligaments laterally, and the talocalcaneal interosseous ligament [1].
Talar dislocations can be categorised as either subtalar or pantalar. Subtalar dislocations involve the talocalcaneal and talonavicular joints, while pantalar dislocations additionally include the tibiotalar joint. Pantalar dislocations can present as anterolateral (most common), posteromedial, or posterior. Despite the frequency of open and anterolateral talar dislocations (more than 50% of cases) [18], anteromedial and posteromedial dislocations are less common, with the latter being extremely rare [19].
In cases of extrusion, the talus may either remain attached via capsular attachments or be totally expelled through the skin and absent at the time of initial presentation [20]. Such high-energy trauma is often associated with events like falls from heights or motor vehicle accidents [14].
Leitner described a three-stage mechanism for anterolateral dislocation, considering talar extrusion as the final stage of combined subtalar supination and tibiotalar plantarflexion, which pulls the talus out of the ankle mortise [3]. Talar dislocation typically occurs in axial trauma, where plantar flexion combines with excessive inversion or eversion of the subtalar joint, leading to lateral dislocation in inversion cases or medial dislocation in eversion cases.
In a typical presentation, a fall with the ankle in a pointed-down and inward position can cause injury to the heel bone. The twisting of the joint in the foot can lead to the dislocation of the talus bone and damage to the ankle's inner structures. The force of the injury can also harm the front and side capsules of the ankle, the ligament connecting the tibia and fibula in the front, and the membrane between the two lower leg bones. The absence of a fibula fracture could be due to the dissipation of energy across two main injury points—the talus dislocation and ankle injury [21].
4.3. Clinical Presentation
Upon arrival at the emergency department, it is evident from the initial physical examination that the patient has pantalar dislocations. This is characterized by the patient being unable to walk on the injured foot and complaining of severe pain. In most cases, the extreme forces that cause the dislocation result in the talar extrusion through an open wound. [1]. Skin appears to be lacerated more often along the lateral or anterolateral aspect of the ankle and the talus results partially extruded from its articulation, sometimes just held to the hindfoot just by a few soft tissues or even completely enucleated - this rare and peculiar injury takes the name of “missing talus”) [5,22,23].
After road-traffic accidents, the extruded talus may be found hours later at the scene of trauma [24].
The wound, the subcutaneous tissues and the bone itself could be macroscopically contaminated and at high risk of infection [22,25].
In less frequent closed dislocations, the lower extremity is visibly deformed with ankle joint and foot swelling and very tense skin due to the prominence of the underlying talar head [26]. Possible superficial abrasions or even blisters could be seen [27,28]. The foot is usually plantarflexed and pronounced with lateral displacement or supinated with medial displacement according to the dislocation mechanism and direction [29].
The neurovascular status of the extremity could be compromised: tibialis posterior and dorsalis pedis pulses are not always palpable and possible motor or sensory deficit could be detected. When impaired, the neurovascular status can be restored after the dislocation reduction [30].
4.4. Imaging
The diagnosis of this injury is typically confirmed through an X-ray evaluation [1].
A 3D CT scan is recommended to check for additional fractures or injuries not visible on X-ray. CT images of the original talus or 3D mirroring of the opposite talus are often used as references for creating prostheses [25].
Avascular necrosis (AVN), which typically appears six months to two years after the injury, is one of the most worrisome consequences [18]. Imaging helps identify early signs of revascularization, with the Hawkins' sign being the only early predictor on conventional radiographs. This sign is observed six to eight weeks post-injury as a subchondral radiolucency in the talar dome, indicating early subchondral atrophy [31]. However, MRI continues to be the most specific and sensitive technique for detecting early AVN development in the postoperative phase, and it is essential to allow the patient to bear weight [18].
4.5. Surgical Techniques
Total talar dislocation is rare, and the best approach for managing complete talus dislocation remains controversial.[32]. However, generally, basic principles of correct management for talus injuries include early reduction, joint fixation if unstable, careful soft tissue handling and a thorough wound care, if open dislocation [32,33].
Historically, primary talectomy and tibio-calcaneal arthrodesis were recommended to manage pantalar dislocation and reduce complications. However, primary talectomy leads to leg-length discrepancy and hinders hindfoot functionality, limiting future reconstructive options.[6,34,35]. Recent literature suggests that accurate removal of damaged tissue, reinsertion of the talus, and temporary fixation of the affected joints have shown satisfactory clinical outcomes by preserving bone stock and restoring talar height[22,30,35].
Recent literature suggests that accurate exposure debridement of soft tissues, talus reimplantation, and temporary fixation of involved joints have demonstrated satisfying clinical outcomes, preserving bone stock and restoring talar height. [22,30,35].
Furthermore, recent case series of open pantalar dislocation have proved that risks of osteomyelitis and AVN are intimately associated with time to reimplantation, with the best prognosis when it is performed within three hours and poorest one when treated over 24 hours, making secondary tibiocalcaneal arthrodesis essential [5,33,36].
Overall, most authors suggest restricted use of primary talectomy and tibio-calcaneal arthrodesis for cases of severe and gross contamination not liable for a satisfactory debridement and likely evolving to complications, or when time of reimplantation is delayed [5,30,34,36]. The same approach is generally considered the main choice when facing complications such as infection, early post-traumatic arthrosis or AVN [5,30,34].
Some information arising from recent literature could help orthopaedic surgeons facing a pantalar dislocation. Firstly, in case of closed pantalar dislocation, an early closed reduction manoeuvre, first described by Mitchell, is warranted to prevent pressure necrosis of the overlying skin [27,32,37,38]; nevertheless, most authors suggest only few attempts because of their side effects on talar vascularity. If closed reduction is attainable, the results are usually good [6,7]; however, it is predominantly not achievable [1,22] due mainly to trapping of talar neck between flexor tendons, buttonholing of head of talus between the tendons of tibialis posterior and flexor digitorum longus and nondisplaced medial malleolus [6]. If all attempts of closed reduction fail, open reduction must be performed, usually exploiting an antero-lateral approach to talus, eventually combining a medial approach that allows a complete view of dislocated joint or engaged talus [6,7,32,39]. This management can be largely applied, even for open dislocation, using the wound as a surgical approach. In that case, authors suggest a single surgical debridement with primary closure to minimise the risk of infection [22].
Debridement is an important step in cases of open dislocations because it could reduce infection risks. A plentiful irrigation with sterile normal saline [22], eventually adding antibiotics, such as cefazoline or gentamicin/clindamycin, or 5 to 10 % povidone iodine [8,23,30,33,34,35], thorough debridement and trimming and excision of the contused subcutaneous tissues [22,34,36,40] should be generally performed, together with appropriate antibiotics protocol and tetanus immune globulin booster [23,35].
In case of pantalar dislocation without talar fractures, Boden KA et al suggest reducing firstly the talonavicular joint then reduction of other joints should be attempted [22]. Conversely, Bugallo et al recommend reducing tibiotalar joint to make other reduction easier [21]. Other authors do not suggest settled order reducing talar dislocation. Different case series reported temporary Schanz pin or K-wire as a support for talar manipulation [8].
After achieving complete reduction, it's important to confirm joint stability. The talus usually has good stability in its original position due to surrounding ligaments and articular surface congruence. Some authors suggest internal fixation isn't needed unless there's a burst-type open wound or an accompanying fracture [7]. On the other hand, many authors usually apply 1 or 2 K-Wire or Schanz pin to increase articular stability, directly associating a below-the-knee cast splint. External fixation is an effective solution for ankle stabilisation and contemporary a handy option for management of daily wound medication [30]. It is not clearly defined which stabilisation system is the best, and the choice is left to the personal surgeon’s experience and local clinical issue.
4.6 Rehabilitation
After total talar dislocation, the rehabilitation protocol aims to restore ankle range of motion and walking ability. Following surgery or closed reduction, the foot is immobilized, and the patient is kept non-weight-bearing on the injured limb for 6-8 weeks.[23,33,37]. Following this, physical rehabilitation can begin with active and passive exercises to improve ankle range of motion and muscle strength. Manual techniques and elastic taping can help reduce swelling and soft tissue adhesions. Partial weight-bearing using crutches may be allowed, gradually increasing alongside gait training exercises focusing on proprioception, balance, and resistance [41]. Before proceeding ahead and allowing full weight-bearing, radiographs revealing no Hawkins sign or magnetic resonance imaging confirming no signs of talus AVN may be required [18,31,42].
Usually after 4-6 postoperative months, the patient is able to walk full-weight-bearing without aids [33,36].
The rehabilitation protocol should continue to focus on restoring function, such as improving tolerance for walking on uneven ground, climbing and descending stairs, and avoiding obstacles.[41]. The goal of a rehabilitation protocol is to help the patient return to their previous level of function, including normal daily activities and high-impact recreational activities, despite mild or moderate impairment, within about a year. [38,41,43].
Some of the parameters used to assess the recovery of foot and ankle are degree of movement in plantar flexion, dorsiflexion, pronation and supination , and specific scores as the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Score [8,25,28,43,44], The Foot Function Index (FFI) and Musculoskeletal Function Assessment (MFA) [22], the Manchester-Oxford Foot Questionnaire-Index (MOXFQ-Index) or the Short Form Health Survey 36 (sf 36) [40].
4.7. Complications
A total closed or open talar dislocation is often a severe injury that could cause a disabling ankle [1]. The severity of ankle injury and the treatment chosen to reimplant the talus into the mortise are two factors strongly associated with the risk to develop the three main complications: avascular necrosis (AVN), post-traumatic arthrosis [45] and infections.
AVN is the most common long-term complication estimated at 26% [1] even if this percentual could be underestimated because of the short follow up of studies [22]. Post traumatic talar AVN develops after interruption or compromission of anastomoses from anterior tibial, posterior tibial and perforating peroneal arteries that guarantee blood supply network to the entire talar bone [5,46]. For this reason, it is essential to preserve the remaining blood supply to ensure a good perfusion of the bone whatever treatment that will undertake [20]. According to several studies, the risk of AVN is higher in addition to vascular compromission when no soft tissues remain attached to the talus [5]. Schiffer et al. supported that the onset of AVN may be avoided if the deltoid ligament or the posterior tibial artery that branch off the posterior process are preserved [14]. The risk of post traumatic talar AVN is over 90% during the first year [47] and remains high until the second-year post injury. It's important to diagnose AVN as soon as possible. However, Hawkin’s sign, an indirect sign of vascularization, may only appear on an X-ray 6-8 weeks after the trauma. A positive Hawkin’s sign shows good vascularization, while a negative sign indicates osteonecrosis. MRI is more effective than X-ray in observing Hawkin’s sign, but it's not cost-effective for screening [18,48]. To reduce the risk of AVN, Eda et al. recommend: (I) to avoid surgery when possible, opt for closed reduction to preserve soft tissues and blood supply; (II) to start early rehabilitation; (III) to allow weight bearing after detecting a positive Hawkin’s sign on X-ray [38].
The second prevalent complication is post-traumatic arthrosis [49]. In literature it is reported a rate of 22% for radiographic osteoarthritis and a rate of 16% for clinical osteoarthritis [1]. These percentual could be underestimated for short follow up of the studies in literature [22]. Arthrosis could involve one of tibiotalar, subtalar and talonavicular or more than one joint altogether. Anyway, in absence of talar fracture is difficult to predict post traumatic arthrosis [20].
The third most common complication is infection, associated with poor clinical and functional outcomes. It is correlated with open fractures or extrusions. Nowadays, the incidence of infection has decreased to a range of 25-38%, compared to the past rate of 89%, due to improved antibiotic therapy protocols and soft tissue handling. [45,50]. The integrity of the soft tissue works as a barrier against microorganism and a good bloody supply simplifies the arrival of antibiotics [46]. Timing for reimplanting the talus into the mortise is crucial to prevent infection. Delayed re-implantation increases infection risk. In cases of total talar extrusion, prompt wound debridement and reimplantation are necessary [50]. These procedures are supported by administering oral antibiotics, and in cases of massive contamination, intravenous antibiotics are used. Primary talectomy and/or arthrodesis are not the initial procedures to perform; these surgeries are reserved for patients with deep infections [5]. Ely et al. reported a case of below the knee amputation after resistant infection in a patient with open total talar dislocation [51].
At last, the complex regional pain syndrome type 1 is a rare complication associated with delayed reduction or partial analgesia [52] after direct injury of tibial nerve.
4.8. Limitations
The study has limitations due to the rarity of the condition, leading to unreliable conclusions. The collected studies were heterogeneous, with varying follow-up timing and duration, making it difficult to assess long-term outcomes and detect complications.
5. Conclusions
Pure total talar dislocation is a rare and complex injury. Early and accurate diagnosis is crucial for effective management to prevent complications such as avascular necrosis, infection, and post-traumatic arthritis. While there's no consensus on the best management approach, principles include early reduction, stabilisation with an external fixator for unstable joints, and accurate wound debridement for open dislocations. Rehabilitation is important for restoring function. Continued documentation of cases is essential for refining protocols and improving outcomes. Future studies should focus on developing standardized treatment guidelines for this complex injury.
Author Contributions
Conceptualization, E.D.; methodology, M.S.; software, M.D.C; validation, G.T.; formal analysis, M.A.M.; investigation, S.P.; resources, A.S.; data curation, E.D.; writing—original draft preparation, E.D.; writing—review and editing, G.T.; visualization, M.S.; supervision, G.T.; project administration, V.P.; funding acquisition, V.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- J. T. Weston, X. Liu, M. E. Wandtke, J. Liu, e N. E. Ebraheim, «A Systematic Review of Total Dislocation of the Talus», Orthop. Surg., vol. 7, fasc. 2, pp. 97–101, mag. 2015. [CrossRef]
- Hildanus FG, «Opera observationum et curationum medico-chirurgicarum, quae exstant omnia», 1682.
- B. Leitner, «The mechanism of total dislocation of the talus», J. Bone Joint Surg. Am., vol. 37-A, fasc. 1, pp. 89–95, gen. 1955. [CrossRef]
- Y. Turhan, H. Cift, K. Ozkan, A. Ozkut, e A. Eren, «Closed Total Talar Extrusion After Ankle Sprain», Foot Ankle Spec., vol. 5, fasc. 1, pp. 51–53, feb. 2012. [CrossRef]
- Y. Hiraizumi, T. Hara, M. Takahashi, e S. Mayehiyo, «Open Total Dislocation of the Talus with Extrusion (Missing Talus): Report of Two Cases», Foot Ankle, vol. 13, fasc. 8, pp. 473–477, ott. 1992. [CrossRef]
- Khan M.J, «Pantalar dislocation: a rare presentation with review of treatment methods».
- Gursu S., «Closed Total Dislocation of Talus Without Any Accompanying Fractures», J. Am. Podiatr. Med. Assoc., vol. 103, fasc. 1, pp. 73–75, gen. 2013. [CrossRef]
- M. Mohindra, P. Gogna, A. Thora, A. Tiwari, R. Singla, e P. Mahindra, «Early Reimplantation for Open Total Talar Extrusion», J. Orthop. Surg., vol. 22, fasc. 3, pp. 304–308, dic. 2014. [CrossRef]
- Broca P, «Dissertation on Subtalar Dislocations. Bulletins et mémoires de la Société de chirurgie de Paris», 1853.
- Anderson HG, «The medical and surgical aspects of aviation. Chapter VII: The Surgery of Aviation.», 1919. [CrossRef]
- W. D. Coltart, «AVIATOR’S ASTRAGALUS», J. Bone Joint Surg. Br., vol. 34-B, fasc. 4, pp. 545–566, nov. 1952. [CrossRef]
- R. Wagner, T. R. Blattert, e A. Weckbach, «Talar dislocations», Injury, vol. 35, fasc. 2, pp. 36–45, set. 2004. [CrossRef]
- Hendin e H. Rosenberg, «The floating foot: a case of total talar dislocation», CJEM, vol. 19, fasc. 2, pp. 154–155, mar. 2017. [CrossRef]
- H. Hosny, «Open Complete Medial Talar Dislocation without Fracture of the Talus or the Malleoli: A Case Report», JBJS Case Connect., vol. 4, fasc. 4, p. e117, dic. 2014. [CrossRef]
- T. Karachalios, M. Pearse, P. Sarangi, e R. Atkins, «Dislocation of the intact fibula with fracture of the medial malleolus», J. Bone Joint Surg. Br., vol. 75-B, fasc. 5, pp. 833–834, set. 1993. [CrossRef]
- J. L. Marsh, C. L. Saltzman, M. Iverson, e D. S. Shapiro, «Major Open Injuries of the Talus»:, J. Orthop. Trauma, vol. 9, fasc. 5, pp. 371–376, ott. 1995. [CrossRef]
- N. T. Brewster e N. Maffulli, «Reimplantation of the Totally Extruded Talus»:, J. Orthop. Trauma, vol. 11, fasc. 1, pp. 42–45, gen. 1997. [CrossRef]
- N. Van Opstal e G. Vandeputte, «Traumatic talus extrusion: case reports and literature review», Acta Orthop. Belg., vol. 75, fasc. 5, pp. 699–704, ott. 2009.
- P. Ramesh, A. Avadhani, J. Dheenadhayalan, e S. Rajasekaran, «Reimplantation of total talar extrusions», Inj. Extra, vol. 41, fasc. 5, pp. 53–57, mag. 2010. [CrossRef]
- A. Taymaz e I. Gunal, «Complete dislocation of the talus unaccompanied by fracture», J. Foot Ankle Surg., vol. 44, fasc. 2, pp. 156–158, mar. 2005. [CrossRef]
- F. G. Bugallo, J. Bridger, C. Chiarella, S. Garbarini, e M. Vergara, «Closed posteromedial total talus and fibula dislocation without fracture», Trauma Case Rep., vol. 34, p. 100504, ago. 2021. [CrossRef]
- K. A. Boden, D. S. Weinberg, e H. A. Vallier, «Complications and Functional Outcomes After Pantalar Dislocation», J. Bone Jt. Surg., vol. 99, fasc. 8, pp. 666–675, apr. 2017. [CrossRef]
- E. J. B. Sié, A. Traoré, A. K. Sy, K. Soumaro, e Y. Lambin, «Delayed debridement of an open total talar dislocation reimplanted in the emergency room», J. Clin. Orthop. Trauma, vol. 5, fasc. 3, pp. 176–180, set. 2014. [CrossRef]
- H. S. Lee, H. W. Chung, e J. S. Suh, «Total Talar Extrusion without Soft Tissue Attachments», Clin. Orthop. Surg., vol. 6, fasc. 2, p. 236, 2014. [CrossRef]
- D. Leonetti, G. C. Basile, G. Giuca, E. Corso, D. Fenga, e I. Sanzarello, «Total Talar Prosthesis, Learning from Experience, Two Reports of Total Talar Prosthesis after Talar Extrusion and Literature Review», Medicina (Mex.), vol. 59, fasc. 8, p. 1498, ago. 2023. [CrossRef]
- El Ibrahimi, M. Shimi, M. Elidrissi, A. Daoudi, e A. Elmrini, «A case of closed total dislocation of talus and literature review», Am. J. Emerg. Med., vol. 29, fasc. 4, p. 475.e1-475.e3, mag. 2011. [CrossRef]
- Kumar C, «Closed Talar Dislocation without Associated Fracture a Very Rare Injury, a Case Report».
- G. Gopisankar Balaji, S. V. Arockiaraj Justin, e A. C. Roy, «A rare case of closed pantalar dislocation combined with Lisfranc’s injury—The unusual complex», Foot Ankle Surg., vol. 18, fasc. 3, pp. e21–e24, set. 2012. [CrossRef]
- T. Bas, V. Vicent, P. Alcántara, e A. J. Llabrés, «Complete dislocation of the talus: a report of 5 cases», The Foot, vol. 4, fasc. 2, pp. 102–105, giu. 1994. [CrossRef]
- M. Breccia, M. Peruzzi, L. Cerbarano, e M. Galli, «Treatment and outcome of open dislocation of the ankle with complete talar extrusion: A case report», The Foot, vol. 24, fasc. 2, pp. 89–93, giu. 2014. [CrossRef]
- P. T. Fortin e J. E. Balazsy, «Talus Fractures: Evaluation and Treatment»:, J. Am. Acad. Orthop. Surg., vol. 9, fasc. 2, pp. 114–127, mar. 2001. [CrossRef]
- M. F. Githens e J. Tangtiphaiboontana, «Pantalar Dislocation», in Fractures and Dislocations of the Talus and Calcaneus, M. R. Adams e S. K. Benirschke, A c. di, Cham: Springer International Publishing, 2020, pp. 141–159. [CrossRef]
- J. L. Burston, P. Isenegger, e R. Zellweger, «Open Total Talus Dislocation: Clinical and Functional Outcomes: A Case Series», J. Trauma Inj. Infect. Crit. Care, vol. 68, fasc. 6, pp. 1453–1458, giu. 2010. [CrossRef]
- Apostle K.L, «Reimplantation of a Totally Extruded Talus: A Case Report».
- A. Genena e A. Abouelela, «A Case Report of an Open Pan-Talar Dislocation», Cureus, lug. 2020. [CrossRef]
- N. AlMaeen, I. S. ElMaghrby, M. K. AlNour, T. A. Alrefeidi, e S. M. Abu Adas, «Complete Revascularization of Reimplanted Talus After Isolated Total Talar Extrusion: A Case Report», Cureus, mag. 2020. [CrossRef]
- S. K. Nanjayan, J. Broomfield, B. Johnson, A. Patel, S. Srivastava, e A. Sinha, «Total Dislocation of the Talus: A Case Report», Foot Ankle Spec., vol. 7, fasc. 1, pp. 71–73, feb. 2014. [CrossRef]
- Y. Eda, Y. Yanagisawa, Y. Matsumoto, T. Mori, e M. Yamazaki, «Closed total talar dislocation without fracture in a rare college athlete case», Trauma Case Rep., vol. 35, p. 100519, ott. 2021. [CrossRef]
- P. Korovessis, P. Spastris, P. Sidiropoulos, T. Katsardis, e P. Spyropoulos, «Complete lateral dislocation of the talus without fracture», J. Orthop. Trauma, vol. 6, fasc. 1, pp. 125–128, 1992.
- S. Ruatti et al., «Total Talar Prosthesis Replacement after Talar Extrusion», J. Foot Ankle Surg., vol. 56, fasc. 4, pp. 905–909, lug. 2017. [CrossRef]
- K. C. Ranalli, «Rehabilitation Following a Traumatic Dislocation of the Talus: A Case Study», Int. J. Athl. Ther. Train., vol. 21, fasc. 3, pp. 28–31, mag. 2016. [CrossRef]
- F. Yapici, M. Coskun, M. C. Arslan, E. Ulu, e Y. E. Akman, «Open reduction of a total talar dislocation: A case report and review of the literature», World J. Clin. Cases, vol. 7, fasc. 14, pp. 1850–1856, lug. 2019. [CrossRef]
- S. Steinmetz, N. Rotigliano, e P. Zermatten, «Isolated open total talar dislocation: A case report and literature review», Arch. Trauma Res., vol. 6, fasc. 3, p. 49, 2017. [CrossRef]
- P. K. Karampinas, E. Kavroudakis, V. Polyzois, J. Vlamis, e Sp. Pneumaticos, «Open talar dislocations without associated fractures», Foot Ankle Surg., vol. 20, fasc. 2, pp. 100–104, giu. 2014. [CrossRef]
- L. C. Detenbeck e P. J. Kelly, «Total dislocation of the talus», J. Bone Joint Surg. Am., vol. 51, fasc. 2, pp. 283–288, mar. 1969. [CrossRef]
- J. M. Palomo-Traver, E. Cruz-Renovell, V. Granell-Beltran, e J. Monzonís-García, «Open Total Talus Dislocation: Case Report and Review of the Literature»:, J. Orthop. Trauma, vol. 11, fasc. 1, pp. 45–49, gen. 1997. [CrossRef]
- J. M. Sarabia Condes, E. De Casas Fernández, e E. J. Salmerón Martı́nez, «Subtotal talus dislocation», Foot Ankle Surg., vol. 9, fasc. 1, pp. 45–49, gen. 2003. [CrossRef]
- M. Tezval, C. Dumont, e K. M. Stürmer, «Prognostic Reliability of the Hawkins Sign in Fractures of the Talus», J. Orthop. Trauma, vol. 21, fasc. 8, pp. 538–543, set. 2007. [CrossRef]
- M. Assal e R. Stern, «TOTAL EXTRUSION OF THE TALUS: A CASE REPORT», J. Bone Jt. Surg.-Am. Vol., vol. 86, fasc. 12, pp. 2726–2731, dic. 2004. [CrossRef]
- C. S. Smith, S. E. Nork, e B. J. Sangeorzan, «The Extruded Talus: Results of Reimplantation», J. Bone Jt. Surg., vol. 88, fasc. 11, pp. 2418–2424, nov. 2006. [CrossRef]
- E. E. Ely, E. K. Konstantakos, R. T. Laughlin, R. M. Johnson, e J. C. Binski, «Total Dislocation of the Talus and the Navicular: A Case Report», J. Orthop. Trauma, vol. 23, fasc. 7, pp. 546–549, ago. 2009. [CrossRef]
- E. C. R. Merchan, «Subtalar dislocations: long-term follow-up of 39 cases», Injury, vol. 23, fasc. 2, pp. 97–100, gen. 1992. [CrossRef]
Figure 1.
Identification of studies.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



