
Submitted:
02 October 2024
Posted:
04 October 2024
You are already at the latest version
Abstract
Mild traumatic brain injury mTBI is a common occurrence around the world, associated with a variety of blunt force and torsion injuries affecting all age groups. Most never reach medical attention, and identification of acute injury and later clearance to return to usual activities is relegated to clinical evaluation particularly in sports injuries. Advanced structural imaging is rarely performed due to the usual absence of associated acute anatomic/hemorrhagic changes. This review targets physiologic imaging techniques available to identify subtle blood brain barrier dysfunction and white matter tract shear injury, and their association with chronic traumatic encephalopathy. These techniques provide needed objective measures to assure recovery from injury in those patients with persistent cognitive/emotional symptoms and in the face of repetitive mTBI.
Keywords:
Mild traumatic brain injury
; Chronic traumatic encephalopathy
; Blood brain barrier dysfunction
; Shear white matter injury
; Arterial spin labeling MRI
; Diffusion tensor imaging MRI
; 18-fluorodeoxyglucose positron emission tomography
; Dynamic contrast-enhanced (DCE) MR perfusion
1. Introduction
Mild traumatic brain injury (mTBI) is a pervasive problem worldwide and typically managed without hospitalization thus unreported. The estimated prevalence rate of 369 per 100,000 individuals underestimates the scope of the problem as a result [1,2,3]. Most head injuries are mild (90%) defined by clinical functionality scales such as the Glasgow Coma scale where a score of 13-15/15 is defined as mild [4]. The scale includes basic tests of level of consciousness as defined by verbal, eye opening and motor responses to commands or noxious stimuli. It is an invaluable tool for assessing aTBI and follow up of moderate or severe TBI. More subtle brain injury however is not captured by this scale, as it is meant as a simple stratification tool for rapid assessment and prognosis of more serious head trauma [4].
The assessment of mTBI is currently the sole prevue of clinical assessment to categorize acute cognitive or other subtle neurologic deficit, along with behavioral/emotional effects [5]. Likewise, return to normal learning or sport activities are based on these measures [6]. Since anatomic imaging studies in mTBI are almost invariable normal, they are often not employed [9,10]. However, developing a noninvasive physiologic measure of acute injury and subsequent recovery would provide a critical objective assessment of safe return to sport/usual activities.
1.1. Background
1.1.1. Minor Closed Head Injury
Mild traumatic brain injury (mTBI) is defined as traumatic brain injury resulting in brief if any loss of consciousness with associated transient cognitive (thinking, memory, general confusion), neurologic (vertigo, delayed reaction times), and/or behavioral (depression, aggression) dysfunctions, and often headache [11]. Most frequent causes include contact sport, blast, and acceleration-deceleration injuries. Sports injuries are acutely assessed on the field acutely or within 72 hours using validated clinical testing instruments such as Sport concussion Assessment Tool (SKAT 6), Glascow coma scale, Vestibular Ocular Motor Screening (VOMS) [5,12,13]. Along with inclusion of the testing measures cognitive function (orientation, immediate and delayed memory recall, concentration, emotionality, depression, anxiety, speech, and task specific processing, as well as coordination, balance, eye movements, and headache [14]. A more comprehensive version for office use, SCOAT 6, has also been validated for use within 72 hours of injury. In addition to testing SKAT 6 items, it catalogues prior head injuries, cognitive and emotional history, current medications, and a detailed neurologic examination. Further it includes recommended strategies for return to learning and return to sport activities [15,16]. Currently corroborating physiologic testing is not commonly employed.
To that end, the physiologic consequences of mTBI will be reviewed, and methods to identify those changes using imaging modalities will be discussed. The potential combined use of both clinical and physiologic testing may improve the accuracy of diagnosis and readiness to return to usual activities and predict persistent physiologic dysfunction. The latter when associated with prior mTBIs may potentially lead to chronic progressive disease -chronic traumatic encephalopathy (CTE) years later, as seen in professional contact sports athletes.
1.1.2. Pathophysiology
Given the brain is a soft delicate organ contained within a closed box, sudden applied blunt trauma and inertial forces of acceleration, deceleration, or rotational trauma, dictates the severity and location of cortical, white matter tract, and vasculature injury. Unlike moderate or severe TBI, mTBI injury is associated with minimal or no disruption of these structures in most cases, but not all [17,18]. That said physiologic consequences of disrupted electrolyte pumps and blood flow acutely post head injury have been well delineated with acute impairment of electrolyte (sodium potassium, calcium, and magnesium) distribution notably mitochondrial calcium sequestration with altered metabolism in neurons and astroglia and reduced local blood flow [19,20,21]. This results in an acute glycolysis hypermetabolism to restore normal electrolyte balance [21]. Disruption of the blood brain barrier (BBB) even in mild Traumatic Brain injury (mTBI) is reflective of this acute phase of injury [22,23]. The duration of this varies, dependent upon location and severity of injury leading to hypometabolism in the affected regions which can persist for weeks or longer [22]. The chronic phase of injury is largely thought to be related to persistent physiologic alterations from persistent activated microglia and its effect on the neurovascular unit [24,25]. The focus of this article principally addresses the BBB dysfunction and identifying imaging techniques. Additionally, techniques demonstrating shear force white matter tract injury will be discussed.
1.1.3. Shear Injury in TBI
The most troublesome and unfortunately permanent sequelae of TBI is the result of shear injury to white matter tracts [18,26,27]. The extent and severity of damage escalates proportional to force and location of impact with compiled additional effects from edema mass effect and inflammatory upregulation. In mTBI, the general assumption is absence of substantive anatomic injury [17,18]. This however belies subtle changes in personality, and emotionality, particularly in adolescence, from damage to developing limbic connections [26,27,28,29].
The underpinnings of shear injury are quite understandable with sudden mechanical deformation of the brain tearing apart connections [26,30,31]. The longer-term damage though is caused by subsequent mass effect from edema, hemorrhage, or later from inflammation [22,32,33,34]. To understand the latter influences, animal models have been employed using a variety of species, most commonly rodents and rarely large animals [35]. Translatability from rodent to human physiology is problematic given vast differences in brain structure and physiologic responses to injury [36,37].
Current medical state of the art possesses no means of restoring shear tract injury. Prevention of delayed injury by reducing mass effect and swelling preserve life and may reduce secondary shear injury [27,29,30,31,32]. But knowledge of how to best limit the secondary tract damage will require additional mechanistic study in higher animals (swine or primates) with closer anatomic affiliation to the human brain [36,37].
Too often the die is cast for potential clinical recovery based on the initial extent of shear force injury. That said identifying the severity of tract injury has potential importance in prognostic discussions with the patient and family.
1.1.4. Blood Brain Barrier Dysfunction in TBI Acute And Chronic
In mTBI, the microcirculation (capillary system) BBB is disrupted acutely causing reduced mean capillary transit time (cMTT) and reduced glymphatic flow (GF) in the region(s) of impact both coup and contrecoup with limited or no white matter tract injury [39,40]. The effect of this disruption is leak and trapping of normally restricted substances into the brain and thus reduced clearance out of the brain. This results in measurable reduction in clearance rate of intraparenchymal fluid which can be identified by imaging techniques (see below). In animal studies, BBB disruption and leak of IGG locally persisted for up to a month following moderate TBI with associated delayed microhemorrhages at those sites [18,32].
A brief summary of the complexity of BBB structure and function is presented here. Details of the cellular interactions, signaling mechanisms, and what is known of the basic biology are beyond the scope of this review but referenced [40,41,42,43,44,45].
The blood brain barrier is dependent on a complex interplay of cells within the neurovascular unit (NVU), including the endothelial cells, pericytes, and astrocyte end feet [33,46,47]. Signalling within this triad in homeostasis allows for transport of needed electrolyte, glucose, and specific lipids and proteins while excluding common blood constituents that are toxic to the complex interstitial environment [48,49,50,51,52,53,54]. The interaction and communication among elements of the NVU, extracellular matrix (ECM) and microglia dictate the presence, expression, and integrity of the various tight junction (TJ) proteins [45,55,56,57]. Presence of specific inflammatory cytokines may result in either a proinflammatory milieux or counterintuitively, a restorative one [24,37,44,45]. For example, Endothelial cell derived IL1 β acutely downregulates TJ protein ZO-1/occludin thus increasing BBB permeability, but by promoting expression of Pentraxin 3 later enhances its restoration [58]. The relative balance of local microglial proinflammatory versus homeostatic regulatory influences also determines the BBB integrity [59,60,61]. That balance is dictated by neuronal and astrocyte signaling which is influenced by presence of cell injury and local inflammation [61].
Fundamental questions remain regarding defining the restorative pathways post injury, and long-term consequences of persistent leak [62,63]. In TBI BBB leak is caused by proinflammatory microglial-endothelial signaling and to shear forces disrupting endothelial glycocalyx, the latter allowing leak of IGG and upregulation of inflammatory cytokines causing local conversion of microglia to proinflammatory state [58,59,60,61]. Activated microglia express complement (C3a) fragment which in turn upregulates C3aR in capillary endothelial cells altering its phenotype to a proinflammatory/immune cell attractant state with associated disruption of intercellular tight junctions thus triggering additional BBB leak [64]. In the chronic phase of injury presence of activated microglia induces BBB dysfunction, local chronic inflammatory changes, and neuronal dysfunction [23,39,65]. The persistence of this especially with multiple mTBI result in perivascular accumulation of pTau within astroglia and neurons in the sulcal depths, the hallmark of CTE [65,66,67,68].
Restoration of normal BBB integrity following mTBI generally occurs quickly in youth, however in some persistence of activated microglia can persist for months or longer resulting in reduction in threshold for additional mTBI related pathology with clinical accompaniment [67,68,69]. With advancing age, recovery is less complete and progression of both inflammation with BBB leak with cognitive decline following TBI is more likely [70]. Further, the lower threshold and persistence of mTBI in young women is well recognized and postulated to be influenced by sex hormones, and reduced muscle mass compared to their male counterparts [71]. The mechanisms of the BBB repair process in humans remain incompletely delineated, and in particular the specifics of the pathways active in youth but lost in the circumstances of repetitive TBI or in the normal aging process [72].
The cumulative effects of multiple mTBI events causes ongoing inflammatory upregulation resulting in both permanent microvascular changes and persistent upregulation of inflammation within the neuropil [67]. This induces altered synthesis, degradation, accumulation and transsynaptic spread of toxic misfolded proteins predominantly hyperphosphorylated Tau (pTau), but also Lewey body proteins, TDP-43 and to a delayed and minor degree β amyloid [69,74]. The consequence is the well described high incidence of chronic traumatic encephalopathy (CTE) in professional contact sport athletes [75]. The clinical correlates include aggression, depression, suicide ideation, impulsivity, cognitive decline, parkinsonian features [66,75,76]. To reduce the likelihood of progressive dementia from cumulative brain injury, the addition of objective physiologic testing in mTBI should prove invaluable in conjunction with clinical assessment to identify the early chronic inflammatory conversion.
Given the importance of maintaining BBB integrity, there is likely more than one pathway regulating restoration post injury [62,63]. That said, duration and speed of clinical recovery are correlated with patient’s age, location and magnitude of force, and prior head injuries [60,61]. The inverse correlation of severity of head injury and restoration of BBB integrity are understandable related to anatomic and vascular disruption [77]. The caveat to this general rule in adolescence has shown clinical evidence of emotional dysfunction even in mTBI which can be persistent suggesting limbic system tract injury [66].
Of particular interest is why do these mechanisms rapidly repair the BBB leaks in youth with a single mTBI but flags in the aging brain even without injury? The answer may lie in the long-term presence of proinflammatory microglia and ECM constituent protein alterations which increase local BBB permeability [78]. Alternatively, upregulation of inflammatory cytokines related to other unrelated health issues may contribute [79,80,81,82]. Conversely, is it a failure of normal restorative signaling pathways lost in the aging process that are root cause? Or perhaps a combination all three mechanisms? This question has profound implications for treatment of the underpinnings of other diseases such as neurogenerative diseases where loss of BBB integrity is the nexus of their development [63,79,80,81,82]. Further, of the two pathologic features of traumatic brain injury, restoration of BBB integrity as opposed to shear injury appears to be the most amenable to intervention.
To assess presence of BBB leak, physiologic imaging methods are required. Likewise, assessment of future treatment modalities to monitor outcomes of clinical treatment trials addressing BBB repair requires the same [63,83]. In the next sections, current most usable and clinically available methods of anatomic and physiologic imaging will be discussed and their roles in identifying specific pathologic features of head injury.
1.2. Structural Imaging in mTBI
Although anatomic imaging in singular mTBI is infrequently done and if performed is almost invariably normal. It clearly has a place in evaluation of patients with multiple mTBI and of course more severe injury. In moderate or severe acute brain injury, CT head is the study of choice for evaluation of bleeding or mass effect [18,83,84]. Evaluating subacute or chronic injury the benefit of MRI capabilities for defining atrophy with T1sequences, white matter lesions with fluid attenuated inversion recovery (FLAIR), and prior micro or macro hemorrhages with Susceptibility Weighted Images (SWI) are the gold standards [83,84].
1.3. Physiologic Imaging
Assessment of TBI potentially takes three forms: anatomic, clinical cognitive/neurologic examination, and physiologic testing. In mTBI, structural evaluation with CT or MRI is nearly always normal, whereas the clinical cognitive assessments are far more revealing. However subtle changes in processing, memory, personality, and emotional stability may miss subclinical physiologic injuries. Current clinically available methodologies for assessing the physiologic change in BBB function include Dynamic Contrast Enhanced MRI (DCE-MRI) and arterial spin labeling (ASL) MRI [85]. Evaluation of WM tract shear injury can be assessed directly with MRI tractography- Diffusion Tensor Imaging (DTI)., Positron Emission Tomography (PET), assesses reduction in glucose utilization reflective of regional loss of normal metabolic function [85] . Indirect means include Functional MRI imaging (not discussed further as it is not commonly used clinically). Pros and cons of each method will be discussed below.
1.3.1. Diffusion Tensor Imaging
Diffusion Tensor Imaging is a non-invasive method of investigating white matter tract integrity, which leverages imaging of water movement within the brain [86,87]. Water in the absence of obstruction will move randomly in all directions ((isotropy). In normal brain however water is forced to move parallel to white matter tract obstructions (anisotropy). With shearing force injury these neat pathways are interrupted and hence water present in those locations moves more isotopically. Diffusion imaging techniques can identify that disruption (Figure 1). Technical improvement to this methodology is under development. Current methods available lack sensitivity and are hampered by long scan times [85]. Nonetheless, as methods ameliorating persistent BBB leak develop, knowledge of the extent of untreatable shear injury is of value in prognosticating ultimate neurologic recovery.
1.3.2. Dynamic Contrast Enhanced (DCE) MRI
Dynamic Contrast Enhanced (DCE) MRI directly measures leak of contrast agent into the neuropil in excess of its natural infusibility. Given gadolinium contrast agents are mostly excluded from passage through the BBB normally, their passage increases with its disruption. The technique assesses plasma volume, interstitial space and can calculate a volumetric transfer constant from vascular to interstitial space [88,89,90]. Excess accumulation of contrast in the interstitial space beyond the calculated diffusion amount is indicative of BBB leak. This method allows direct visualization of BBB leak but is invasive (requires gadolinium contrast injection) and thus is not suitable for serial measurements over time, given the concern of retained gadolinium contrast within the CNS [91,92,93] (Figure 2). Specific software to sort out normal contrast diffusion through the BBB from that related to excess leak is also required [89]. Depending on patient circumstances though its use as a diagnostic one-off study when coupled with DTI may prove helpful in prognosticating recovery in those slow to do so. The combination would reveal the extent of BBB leak and white matter tract injury.
Figure 2.
Individual subject examples from a representative control (A) and subacute TBI subject (B). The TBI nonlesional patient shows similar mild elevations in Ktrans and NPI in the anterior frontal white matter (yellow arrows), and additional small areas of Ktrans elevation in the occipital lobes (blue arrow).
Figure 2.
Individual subject examples from a representative control (A) and subacute TBI subject (B). The TBI nonlesional patient shows similar mild elevations in Ktrans and NPI in the anterior frontal white matter (yellow arrows), and additional small areas of Ktrans elevation in the occipital lobes (blue arrow).

Ware, Jeffrey B., Saurabh Sinha, Justin Morrison, Alexa E. Walter, James J. Gugger, Andrea LC Schneider, Cian Dabrowski et al. "Dynamic contrast enhanced MRI for characterization of blood-brain-barrier dysfunction after traumatic brain injury." NeuroImage: Clinical 36 (2022): 103236. [123]
2213-1582/©2022 The Authors. Published by Elsevier Inc. This is an open access article under the CCBY-NC-ND license (http://creativecommons.org/licenses/bync-nd/4.0/).
1.3.3 18-Fluorodeoxyglucose Positron Emission Tomography (FDG-PET)
Utilizing radioactively labeled fluorodeoxyglucose (18FDG) and measuring cellular uptake thereof via positron emission tomography (PET) indirectly measures metabolic activity [94,95]. With less metabolic activity there is reduced uptake of labeled glucose as occurs in acute mTBI [96,97]. In the acute phase of severe injury there is increased uptake of 18FDG corresponding to the increased glycolysis required to reestablish electrolyte balance [98,99]. In the chronic phase of injury, there is reduced uptake of glucose corresponding to reduced local activity [99,100,101,102,103]. When overlayed on CT or MRI brain images localization of abnormalities is enhanced (Figure 3). Sensitivity, specificity, cost, and scan times limit its utility.
Morgan, Richard, Jordon Prosapio, Sam Kara, Sreepadma Sonty, Pamela Youssef, and Kester Nedd. "Preliminary clinical diagnostic criteria for chronic traumatic encephalopathy: A case report and literature review." Interdisciplinary Neurosurgery 26 (2021): 101290. [124]
Published by Elsevier B.V. This is an open access article under the CC BY-NC-ND license
Application of tau PET scan will not be discussed here as they would not be employed in mTBI but in cases of repetitive TBI when the question of CTE arises. The reader is referred to excellent reviews of these techniques [94,104,105,106,107,108,109,110,111,112,113,114].
1.3.4. Arterial Spin Labeling MRI
Another method to indirectly determine BBB leak utilizes the clearance rate of magnetically labelled protons using 3D ASL MRI technology. This technique leverages the physiologic effects of altered perfusion with delayed capillary mean transit time (cMTT) and reduced glymphatic outflow in the late phase of the perfusion cycle, correlating with the location of BBB leak [115] (Figure 4). It is a non-invasive method using blood protons magnetically spin labeled in the neck and after specified post labeling delay (PLD), residual signal averages are sampled in desired cortical regions.
T1 times (63% signal decay) of major signal contributors indicated by the colored dots.
Magenta dot = 800-850 msec T1 of white matter.
Orange dot = 1650 msec T1 of blood.
Green dot = 1700 msec T1 of gray matter (all values are for 3T)
Dk blue dot = 3800 msec T1 of water (CSF fluid); (all values are for 3T)
BAT = bolus arrival time; aaTT =artery-artery arrival time; τ = peak capillary arrival time
Adapted with publisher permission (Wiley) from reference [125].
By using multiple sequential PLD’s in the late phase of the perfusion cycle linear analysis can be employed to determine rate of clearance (slope of the line) [115,116] . In regions of BBB leak there are localized changes in blood flow that correlate with diminished clearance rates. Since the signal measured is largely from trapped labeled water protons in the late phase of perfusion, it is much more sensitive determining minor BBB leaks than gadolinium (large molecule) based DCE [117].
Since this is a non-invasive technique, it is suitable for sequential studies without risk of exogenous contrast. Currently when combined with FLAIR and Susceptibility Weighted Images (SWI), scan time is about 18 1/2 minutes [116]. ASL MRI requires a 3 Tesla magnet and is limited reduced S/N. The latter can be circumvented by measuring a large field of view and obtaining multiple PLDs. Using 3D data acquisition allows for multiple regions of the brain to be investigated in one study. For example, our usage in mTBI acquired clearance rates from 6 brain regions, homologous temporal, frontal, and parietal regions [115]. Newer ASL MRI sequences allow for acquiring multiple PLDs in one sequence, reducing scan times to under 5 minutes [118]. This technique has significant potential in following the progress of BBB repair or alternatively persistent leak. In our pilot study of mTBI in college age athletes, both reduced glymphatic clearance post-acute injury and restoration of BBB integrity as measured by this technique correlated with high sensitivity with clinical recovery [116]. Future studies evaluating more serious head injury sequentially may shed light on those patients with persistent dysfunction which sets the stage for progressive dementia (CTE). In addition, this objective measure could help determine when and if an injured athlete or soldier could safely return to their sport or active duty. Limitations of this technique include the indirect method of determination (results are graphic in nature post analysis as opposed specific images of leak) and low S/N ratio. The latter is compensated for by analyzing multiple data points and acquiring signal from a large FOV. Given the test is noninvasive as well as, time and cost efficient, this method is suitable for serial studies post TBI in the assessment of BBB dysfunction [63,119].
1.3.6 Summary of techniques
Table 1 below summarizes the imaging target, relative advantages, and disadvantages of the four physiologic imaging techniques presented in evaluating mTBI. They provide objective information regarding the state of brain and vascular function at the time they are employed post head injury. The techniques will continue to improve and become more widely available providing both prognostic information. They also will be essential as outcome measures of future treatment trials.
Table 1 summarizes the DTI in identifying shear tract injury, which if present, correlates with persistence of neurologic deficit and recovery depending on its extent. DCE, and ASL MRI identify loss of BBB integrity the former directly and the latter indirectly. 18FDG-PET measures metabolic activity and thus could be negatively influenced by either shear tract injury or BBB leak.
2. Conclusion
With the mounting evidence of severe late life repercussions (CTE) related to repetitive mTBI among professional athletes in contact sports, there is a need to evaluate the physiology leveraging the loss of BBB integrity post injury, that if persistent, correlates with the progressive changes in CTE [39,60,79,85,120,121]. By adopting physiologic testing measures, safe return to the sport could be more accurately predicted in mTBI. Since the potential of both subtle white matter tact shear injury and persistent BBB leak occur simultaneously assessment of damage requires attention to both which translates into white matter tract imaging as well as evaluation of BBB integrity. Further as we uncover the mechanisms of BBB repair going forward and can leverage that knowledge therapeutically, identifying and assessing outcomes of future treatments will be possible. The benefits of identifying BBB dysfunction spill over from TBI to preclinical stages of neurodegenerative disease (NG), where loss of its integrity is at the nexus of development and prime target for early intervention.
Acronyms Dictionary
| TBI- mild traumatic brain injury |
| TJ protein ZO-1-tight junction protein Zona Occludens 1 |
| C3a- complement C3a protein |
| C3aR- complement C3a receptor protein |
| pTau- hyperphosphorylated Tau |
| TDP-43- Transactive response DNA binding protein- 43 |
| FLAIR- fluid attenuated inversion recovery |
| SWI- Susceptibility Weighted Images |
| ASL MRI-Arterial Spin Labeling MRI |
| PLD- Post labeling delay |
| DTI MRI- Diffusion Tensor Imaging |
| DCE MRI- Dynamic Contrast Enhanced MRI |
| PET- Positron Emission Tomography |
| S/N- Signal to Noise |
| SKAT 6- Sport concussion Assessment Tool |
| VOMS- Vestibular Ocular Motor Screening |
| SCOAT 6- Sports Concussion Office Assessment Tool |
| CTE- chronic traumatic encephalopathy |
| cMTT- mean capillary transit time |
| GF- glymphatic flow |
| BBB- Blood brain barrier |
| IGG- Immunoglobulin G |
| NVU- the neurovascular unit |
| ECM- extracellular matrix |
| IL1 β- interleukin 1 beta |
Acknowledgments
The author wants to thank Liberty University for funding this publication, in addition to students and faculty colleagues who were instrumental in the ASL MRI clinical research projects referred to in this article.
Conflicts of Interest
The author has no competing issues or conflicts of interest in the writing of this manuscript. The author is solely responsible for the content of this article.
References
- Maas, A.I.R.; Menon, D.K.; Manley, G.T.; Abrams, M.; Åkerlund, C.; Andelic, N.; Aries, M.; Bashford, T.; Bell, M.J.; Bodien, Y.G.; et al. Traumatic brain injury: progress and challenges in prevention, clinical care, and research. Lancet Neurol. 2022, 21, 1004–1060. [Google Scholar] [CrossRef]
- Forrest, R.H.J.; Henry, J.D.; McGarry, P.J.; Marshall, R.N. Mild traumatic brain injury in New Zealand: factors influencing post-concussion symptom recovery time in a specialised concussion service. J. Prim. Heal. Care 2018, 10, 159–166. [Google Scholar] [CrossRef]
- Traumatic Brain Injury in the United States: Epidemiology and Rehabilitation. CDC NIH Rep to Congr 1–74.
- Reith, Florence CM, Hester F. Lingams, Belinda J. Gabe, Fiona E. Lecky, Ian Roberts, and Andrew IR Maas. "Differential effects of the Glasgow Coma Scale Score and its Components: An analysis of 54,069 patients with traumatic brain injury." Injury 48, no. 9 (2017): 1932-1943. [CrossRef]
- Dessy, A.M.; Yuk, F.J.; Maniya, A.Y.; Gometz, A.; Rasouli, J.J.; Lovell, M.R.; Choudhri, T.F. Review of Assessment Scales for Diagnosing and Monitoring Sports-related Concussion. Cureus 2017, 9, e1922. [Google Scholar] [CrossRef]
- Polinder, S.; Cnossen, M.C.; Real, R.G.L.; Covic, A.; Gorbunova, A.; Voormolen, D.C.; Master, C.L.; Haagsma, J.A.; Diaz-Arrastia, R.; Von Steinbuechel, N. A Multidimensional Approach to Post-concussion Symptoms in Mild Traumatic Brain Injury. Front. Neurol. 2018, 9, 1113. [Google Scholar] [CrossRef]
- Williams, R.M.; Puetz, T.W.; Giza, C.C.; Broglio, S.P. Concussion Recovery Time Among High School and Collegiate Athletes: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 893–903. [Google Scholar] [CrossRef]
- Williams, R.M.; Puetz, T.W.; Giza, C.C.; Broglio, S.P. Concussion Recovery Time Among High School and Collegiate Athletes: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 893–903. [Google Scholar] [CrossRef]
- Wintermark, M.; Sanelli, P.C.; Anzai, Y.; Tsiouris, A.J.; Whitlow, C.T.; Druzgal, T.J.; Gean, A.D.; Lui, Y.W.; Norbash, A.M.; Raji, C.; et al. Imaging Evidence and Recommendations for Traumatic Brain Injury: Conventional Neuroimaging Techniques. J. Am. Coll. Radiol. 2015, 12, e1–e14. [Google Scholar] [CrossRef]
- Eierud, C.; Craddock, R.C.; Fletcher, S.; Aulakh, M.; King-Casas, B.; Kuehl, D.; LaConte, S.M. Neuroimaging after mild traumatic brain injury: Review and meta-analysis. NeuroImage: Clin. 2014, 4, 283–294. [Google Scholar] [CrossRef]
- Roberts, M.A.; Manshadi, F.F.; Bushnell, D.L.; Hines, M.E. Neurobehavioural dysfunction following mild traumatic brain injury in childhood: A case report with positive findings on positron emission tomography (PET). Brain Inj. 1995, 9, 427–436. [Google Scholar] [CrossRef]
- Echemendia, R.J.; Brett, B.L.; Broglio, S.; A Davis, G.; Giza, C.C.; Guskiewicz, K.M.; Harmon, K.G.; Herring, S.; Howell, D.R.; Master, C.L.; et al. Introducing the Sport Concussion Assessment Tool 6 (SCAT6). Br. J. Sports Med. 2023, 57, 619–621. [Google Scholar] [CrossRef]
- Patricios, Jon, Geoff M. Schneider, Jacqueline van Ierssel, Laura K. Purcell, Gavin A. Davis, Ruben J. Echemendia, Pierre Frémont et al. "Sport concussion office assessment tool 6." British journal of sports medicine 57, no. 11 (2023): 651-667. [CrossRef]
- Polinder, S.; Cnossen, M.C.; Real, R.G.L.; Covic, A.; Gorbunova, A.; Voormolen, D.C.; Master, C.L.; Haagsma, J.A.; Diaz-Arrastia, R.; Von Steinbuechel, N. A Multidimensional Approach to Post-concussion Symptoms in Mild Traumatic Brain Injury. Front. Neurol. 2018, 9, 1113. [Google Scholar] [CrossRef]
- Meier, T.B.; Bellgowan, P.S.F.; Singh, R.; Kuplicki, R.; Polanski, D.W.; Mayer, A.R. Recovery of Cerebral Blood Flow Following Sports-Related Concussion. JAMA Neurol. 2015, 72, 530–538. [Google Scholar] [CrossRef]
- Roberts, M.A.; Manshadi, F.F.; Bushnell, D.L.; Hines, M.E. Neurobehavioural dysfunction following mild traumatic brain injury in childhood: A case report with positive findings on positron emission tomography (PET). Brain Inj. 1995, 9, 427–436. [Google Scholar] [CrossRef]
- Ilvesmäki, T.; Luoto, T.M.; Hakulinen, U.; Brander, A.; Ryymin, P.; Eskola, H.; Iverson, G.L.; Öhman, J. Acute mild traumatic brain injury is not associated with white matter change on diffusion tensor imaging. Brain 2014, 137, 1876–1882. [Google Scholar] [CrossRef]
- Lee, H.; Wintermark, M.; Gean, A.D.; Ghajar, J.; Manley, G.T.; Mukherjee, P. Focal Lesions in Acute Mild Traumatic Brain Injury and Neurocognitive Outcome: CT versus 3T MRI. J. Neurotrauma 2008, 25, 1049–1056. [Google Scholar] [CrossRef]
- Hiebert, J.B.; Shen, Q.; Thimmesch, A.R.; Pierce, J.D. Traumatic Brain Injury and Mitochondrial Dysfunction. Am. J. Med Sci. 2015, 350, 132–138. [Google Scholar] [CrossRef]
- Vagnozzi R, Tavazzi B, Signoretti S, Amorini AM, Belli A, Cimatti M, et al. Temporal window of metabolic brain vulnerability to concussions: mitochondrial-related impairment part I. Neurosurgery. 2007; 61:379–89. [CrossRef]
- Bergsneider, M.; Hovda, D.A.; Shalmon, E.; Kelly, D.F.; Vespa, P.M.; Martin, N.A.; Phelps, M.E.; McArthur, D.L.; Caron, M.J.; Kraus, J.F.; et al. Cerebral hyperglycolysis following severe traumatic brain injury in humans: a positron emission tomography study. J. Neurosurg. 1997, 86, 241–251. [Google Scholar] [CrossRef]
- Hay, Jennifer R., Victoria E. Johnson, Adam MH Young, Douglas H. Smith, and William Stewart. "Blood-brain barrier disruption is an early event that may persist for many years after traumatic brain injury in humans." Journal of neuropathology and experimental neurology 74, no. 1: 12 (2015), 2015. [CrossRef]
- Johnson, V.E.; Stewart, J.E.; Begbie, F.D.; Trojanowski, J.Q.; Smith, D.H.; Stewart, W. Inflammation and white matter degeneration persist for years after a single traumatic brain injury. Brain 2013, 136, 28–42. [Google Scholar] [CrossRef]
- Thurgur, H.; Pinteaux, E. Microglia in the Neurovascular Unit: Blood-Brain Barrier-microglia Interactions After Central Nervous System Disorders. Neuroscience 2019, 405, 55–67. [Google Scholar] [CrossRef]
- Christman, C.W.; Grady, M.S.; Walker, S.A.; Holloway, K.L.; Povlishock, J.T. Ultrastructural Studies of Diffuse Axonal Injury in Humans. J. Neurotrauma 1994, 11, 173–186. [Google Scholar] [CrossRef]
- El Sayed, Tamer, Alejandro Mota, Fernando Fraternali, and Michael Ortiz. "Biomechanics of traumatic brain injury." Computer Methods in Applied Mechanics and Engineering 197, no. 51-52 (2008): 4692-4701.
- Meier, T.B.; Bellgowan, P.S.F.; Singh, R.; Kuplicki, R.; Polanski, D.W.; Mayer, A.R. Recovery of Cerebral Blood Flow Following Sports-Related Concussion. JAMA Neurol. 2015, 72, 530–538. [Google Scholar] [CrossRef]
- Roberts, M.A.; Manshadi, F.F.; Bushnell, D.L.; Hines, M.E. Neurobehavioural dysfunction following mild traumatic brain injury in childhood: A case report with positive findings on positron emission tomography (PET). Brain Inj. 1995, 9, 427–436. [Google Scholar] [CrossRef]
- Meaney, D.F.; Smith, D.H. Biomechanics of Concussion. Clin. Sports Med. 2011, 30, 19–31. [Google Scholar] [CrossRef]
- Donat, C.K.; Lopez, M.Y.; Sastre, M.; Baxan, N.; Goldfinger, M.; Seeamber, R.; Müller, F.; Davies, P.; Hellyer, P.; Siegkas, P.; et al. From biomechanics to pathology: predicting axonal injury from patterns of strain after traumatic brain injury. Brain 2021, 144, 70–91. [Google Scholar] [CrossRef]
- Glushakova, Olena Y., Danny Johnson, and Ronald L. Hayes. "Delayed increases in microvascular pathology after experimental traumatic brain injury are associated with prolonged inflammation, blood–brain barrier disruption, and progressive white matter damage." Journal of neurotrauma 31, no. 13 (2014): 1180-1193. [CrossRef]
- Thurgur, H.; Pinteaux, E. Microglia in the Neurovascular Unit: Blood-Brain Barrier-microglia Interactions After Central Nervous System Disorders. Neuroscience 2019, 405, 55–67. [Google Scholar] [CrossRef]
- Haider, M.N.; Leddy, J.J.; Hinds, A.L.; Aronoff, N.; Rein, D.; Poulsen, D.; Willer, B.S. Intracranial pressure changes after mild traumatic brain injury: a systematic review. Brain Inj. 2018, 32, 809–815. [Google Scholar] [CrossRef]
- Barzó, P.; Marmarou, A.; Fatouros, P.; Corwin, F.; Dunbar, J. Magnetic resonance imaging—monitored acute blood-brain barrier changes in experimental traumatic brain injury. J. Neurosurg. 1996, 85, 1113–1121. [Google Scholar] [CrossRef]
- Morganti-Kossmann, Maria Cristina, E. Yan, and Nicole Bye. "Animal models of traumatic brain injury: is there an optimal model to reproduce human brain injury in the laboratory?" Injury 41 (2010): S10-S13. [CrossRef]
- Johnson, Victoria E., David F. Meaney, D. Kacy Cullen, and Douglas H. Smith. "Animal models of traumatic brain injury." Handbook of clinical neurology 127 (2015): 115-128. [CrossRef]
- Morganti-Kossmann MC, Rancan M, Otto VI, Stahel PF, Kossmann T. Role of cerebral inflammation after traumatic brain injury: a revisited concept. Shock (Augusta, Ga). 001; 16:165–77. [CrossRef]
- Doherty, C.P.; O’keefe, E.; Wallace, E.; Loftus, T.; Keaney, J.; Kealy, J.; Humphries, M.M.; Molloy, M.G.; Meaney, J.F.; Farrell, M.; et al. Blood–Brain Barrier Dysfunction as a Hallmark Pathology in Chronic Traumatic Encephalopathy. J. Neuropathol. Exp. Neurol. 2016, 75, 656–662. [Google Scholar] [CrossRef]
- Hattori, N.; Huang, S.-C.; Wu, H.-M.; Liao, W.; Glenn, T.C.; Vespa, P.M.; E Phelps, M.; A Hovda, D.; Bergsneider, M. Acute changes in regional cerebral (18)F-FDG kinetics in patients with traumatic brain injury. . 2004, 45, 775–83. [Google Scholar]
- Ziebell, J.M.; Morganti-Kossmann, M.C. Involvement of Pro- and Anti-Inflammatory Cytokines and Chemokines in the Pathophysiology of Traumatic Brain Injury. Neurotherapeutics 2010, 7, 22–30. [Google Scholar] [CrossRef]
- Woodcock T, Morganti-Kossmann C. The role of markers of inflammation in traumatic brain injury. Front Neurol. 2013; 4:18. [CrossRef]
- Ziebell, J.M.; Morganti-Kossmann, M.C. Involvement of Pro- and Anti-Inflammatory Cytokines and Chemokines in the Pathophysiology of Traumatic Brain Injury. Neurotherapeutics 2010, 7, 22–30. [Google Scholar] [CrossRef]
- Woodcock T, Morganti-Kossmann C. The role of markers of inflammation in traumatic brain injury. Front Neurol. 2013; 4:18. [CrossRef]
- Engelhardt, B.; Liebner, S. Novel insights into the development and maintenance of the blood–brain barrier. Cell Tissue Res. 2014, 355, 687–699. [Google Scholar] [CrossRef]
- Iadecola, C. The Neurovascular Unit Coming of Age: A Journey through Neurovascular Coupling in Health and Disease. Neuron 2017, 96, 17–42. [Google Scholar] [CrossRef]
- Bhowmick, S.; D'Mello, V.; Caruso, D.; Wallerstein, A.; Abdul-Muneer, P. Impairment of pericyte-endothelium crosstalk leads to blood-brain barrier dysfunction following traumatic brain injury. Exp. Neurol. 2019, 317, 260–270. [Google Scholar] [CrossRef]
- Sweeney, M.D.; Kisler, K.; Montagne, A.; Toga, A.W.; Zlokovic, B.V. The role of brain vasculature in neurodegenerative disorders. Nat. Neurosci. 2018, 21, 1318–1331. [Google Scholar] [CrossRef]
- Sweeney, M.D.; Zhao, Z.; Montagne, A.; Nelson, A.R.; Zlokovic, B.V. Blood-Brain Barrier: From Physiology to Disease and Back. Physiol. Rev. 2019, 99, 21–78. [Google Scholar] [CrossRef]
- Andjelkovic, Anuska V., et al. "Blood-brain barrier dysfunction in normal aging and neurodegeneration: mechanisms, impact, and treatments." Stroke 54.3 (2023): 661-672. [CrossRef]
- Kadry, Hossam, Behnam Noorani, and Luca Cucullo. "A blood–brain barrier overview on structure, function, impairment, and biomarkers of integrity." Fluids and Barriers of the CNS 17. 1: (2020), 2020. [CrossRef]
- Zhao, L.; Tannenbaum, A.; Bakker, E.N.T.P.; Benveniste, H. Physiology of Glymphatic Solute Transport and Waste Clearance from the Brain. Physiology 2022, 37, 349–362. [Google Scholar] [CrossRef]
- Preston, Jane E., N. Joan Abbott, and David J. Begley. "Transcytosis of macromolecules at the blood–brain barrier." Advances in pharmacology 71 (2014): 147-163. [CrossRef]
- van Leeuwen, E.; Hampton, M.B.; Smyth, L.C. Redox signalling and regulation of the blood-brain barrier. Int. J. Biochem. Cell Biol. 2020, 125, 105794. [Google Scholar] [CrossRef]
- Baeten KM, Akassoglou K (2011) Extracellular matrix and matrix receptors in blood–brain barrier formation and stroke. Dev Neurobiol 71:1018–1039. [CrossRef]
- Lochhead, J.J.; Yang, J.; Ronaldson, P.T.; Davis, T.P. Structure, Function, and Regulation of the Blood-Brain Barrier Tight Junction in Central Nervous System Disorders. Front. Physiol. 2020, 11, 914. [Google Scholar] [CrossRef]
- Hudson, Natalie, and Matthew Campbell. "Tight junctions of the neurovascular unit. 7: Frontiers in Molecular Neuroscience 14 (2021), 2021. [CrossRef]
- Sun, X.-C.; Cheng, C.-J.; Zhou, C.; Chen, H.; Zheng, J.-F.; Guo, Z.-D.; Huang, Z.-J.; Wu, Y.; Zhong, J.-J. Pentraxin 3 contributes to neurogenesis after traumatic brain injury in mice. Neural Regen. Res. 2020, 15, 2318–2326. [Google Scholar] [CrossRef]
- Shabab, T.; Khanabdali, R.; Moghadamtousi, S.Z.; Kadir, H.A.; Mohan, G. Neuroinflammation pathways: a general review. Int. J. Neurosci. 2016, 127, 624–633. [Google Scholar] [CrossRef]
- Zhang J, Puvenna V, Janigro D. Biomarkers of traumatic brain injury and their relationship to pathology. Translational research in traumatic brain injury: CRC Press/Taylor and Francis Group; 2016.
- Ramlackhansingh, A.F.; Brooks, D.J.; Greenwood, R.J.; Bose, S.K.; Turkheimer, F.E.; Kinnunen, K.M.; Gentleman, S.; Heckemann, R.A.; Gunanayagam, K.; Gelosa, G.; et al. Inflammation after trauma: Microglial activation and traumatic brain injury. Ann. Neurol. 2011, 70, 374–383. [Google Scholar] [CrossRef]
- Profaci, C.P.; Munji, R.N.; Pulido, R.S.; Daneman, R. The blood–brain barrier in health and disease: Important unanswered questions. J. Exp. Med. 2020, 217. [Google Scholar] [CrossRef]
- Joseph, C.R. Progressive Age-Associated Blood–Brain Barrier Leak/Dysfunction-Nexus of Neurodegenerative Disease Using MRI Markers to Identify Preclinical Disease and Potential New Targets for Future Treatments. Diagnostics 2024, 14, 726. [Google Scholar] [CrossRef]
- Propson, N.E.; Roy, E.R.; Litvinchuk, A.; Köhl, J.; Zheng, H. Endothelial C3a receptor mediates vascular inflammation and blood-brain barrier permeability during aging. J. Clin. Investig. 2021, 131. [Google Scholar] [CrossRef]
- Nakajima, Y.; Horiuchi, Y.; Kamata, H.; Yukawa, M.; Kuwabara, M.; Tsubokawa, T. Distinct Time Courses of Secondary Brain Damage in the Hippocampus Following Brain Concussion and Contusion in Rats. Tohoku J. Exp. Med. 2010, 221, 229–235. [Google Scholar] [CrossRef]
- Ryan LM, Warden DL. Post concussion syndrome. Int Rev Psychiatry. 2003; 15:310–6.
- Prins, M.L.; Alexander, D.; Giza, C.C.; Hovda, D.A. Repeated Mild Traumatic Brain Injury: Mechanisms of Cerebral Vulnerability. J. Neurotrauma 2013, 30, 30–38. [Google Scholar] [CrossRef]
- Laurer HL, Bareyre FM, Lee VM, Trojanowski JQ, Longhi L, Hoover R, et al. Mild head injury increasing the brain's vulnerability to a second concussive impact. J Neurosurg. 2001; 95:859–70. [CrossRef]
- Sorby-Adams, A.J.; Marcoionni, A.M.; Dempsey, E.R.; Woenig, J.A.; Turner, R.J. The Role of Neurogenic Inflammation in Blood-Brain Barrier Disruption and Development of Cerebral Oedema Following Acute Central Nervous System (CNS) Injury. Int. J. Mol. Sci. 2017, 18, 1788. [Google Scholar] [CrossRef]
- Andjelkovic, Anuska V., et al. "Blood-brain barrier dysfunction in normal aging and neurodegeneration: mechanisms, impact, and treatments." Stroke 54.3 (2023): 661-672. [CrossRef]
- Farace E, Alves WM. Do women fare worse? A metanalysis of gender differences in outcome after traumatic brain injury. Neurosurg Focus. 2000; 8:1–8.
- Bennett ER, Reuter-Rice K, Laskowitz DT. Genetic influences in traumatic brain injury. Transl Res Traumatic Brain Inj. 2016.
- McKee, A.C.; Stein, T.D.; Nowinski, C.J.; Stern, R.A.; Daneshvar, D.H.; Alvarez, V.E.; Lee, H.-S.; Hall, G.; Wojtowicz, S.M.; Baugh, C.M.; et al. The spectrum of disease in chronic traumatic encephalopathy. Brain 2012, 136, 43–64. [Google Scholar] [CrossRef]
- Ayubcha, Cyrus, Mona-Elisabeth Revheim, Andrew Newberg, Mateen Moghbel, Chaitanya Rojulpote, Thomas J. Werner, and Abass Alavi. "A critical review of radiotracers in the positron emission tomography imaging of traumatic brain injury: FDG, tau, and amyloid imaging in mild traumatic brain injury and chronic traumatic encephalopathy." European Journal of Nuclear Medicine and Molecular Imaging 48 (2021): 623-641.
- Mez, J.; Daneshvar, D.H.; Kiernan, P.T.; Abdolmohammadi, B.; Alvarez, V.E.; Huber, B.R.; Alosco, M.L.; Solomon, T.M.; Nowinski, C.J.; McHale, L.; et al. Clinicopathological Evaluation of Chronic Traumatic Encephalopathy in Players of American Football. JAMA 2017, 318, 360–370. [Google Scholar] [CrossRef]
- Lenihan, M.W.; Jordan, B.D. The Clinical Presentation of Chronic Traumatic Encephalopathy. Curr. Neurol. Neurosci. Rep. 2015, 15, 1–8. [Google Scholar] [CrossRef]
- Karton, Clara, and T. Blaine Hoshizaki. "Concussive and subconcussive brain trauma: the complexity of impact biomechanics and injury risk in contact sport." Handbook of clinical neurology 158 (2018): 39-49.78.
- Bang SA, Song YS, Moon BS, Lee BC, Lee H-y, Kim J-M, et al. Neuropsychological, metabolic, and GABAA receptor studies in subjects with repetitive traumatic brain injury. J Neurotrauma. 2016; 33:1005–14. [CrossRef]
- Wooten, D.W.; Ortiz-Terán, L.; Zubcevik, N.; Zhang, X.; Huang, C.; Sepulcre, J.; Atassi, N.; Johnson, K.A.; Zafonte, R.D.; El Fakhri, G. Multi-Modal Signatures of Tau Pathology, Neuronal Fiber Integrity, and Functional Connectivity in Traumatic Brain Injury. J. Neurotrauma 2019, 36, 3233–3243. [Google Scholar] [CrossRef]
- Knox, E.G.; Aburto, M.R.; Clarke, G.; Cryan, J.F.; O’driscoll, C.M. The blood-brain barrier in aging and neurodegeneration. Mol. Psychiatry 2022, 27, 2659–2673. [Google Scholar] [CrossRef]
- Lendahl, U.; Nilsson, P.; Betsholtz, C. Emerging links between cerebrovascular and neurodegenerative diseases—a special role for pericytes. Embo Rep. 2019, 20, e48070. [Google Scholar] [CrossRef]
- Searson, Peter Charles, et al. "The influence of physiological and pathological perturbations on blood-brain barrier function." Frontiers in Neuroscience 17 (2023): 1289894. [CrossRef]
- Elschot, E.P.M.; Backes, W.H.; Postma, A.A.; van Oostenbrugge, R.J.; Staals, J.; Rouhl, R.P.; Jansen, J.F. A Comprehensive View on MRI Techniques for Imaging Blood-Brain Barrier Integrity. Investig. Radiol. 2020, 56, 10–19. [Google Scholar] [CrossRef]
- Eierud, C.; Craddock, R.C.; Fletcher, S.; Aulakh, M.; King-Casas, B.; Kuehl, D.; LaConte, S.M. Neuroimaging after mild traumatic brain injury: Review and meta-analysis. NeuroImage: Clin. 2014, 4, 283–294. [Google Scholar] [CrossRef]
- Sparks, P.; Lawrence, T.; Hinze, S. Neuroimaging in the Diagnosis of Chronic Traumatic Encephalopathy: A Systematic Review. Am. J. Ther. 2020, 30, S1–S10. [Google Scholar] [CrossRef]
- Ranzenberger LR, Das JM, Snyder T. Diffusion Tensor Imaging. 2023 Nov 12. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. [PubMed]
- Kim, E.; Yoo, R.-E.; Seong, M.Y.; Oh, B.-M. A systematic review and data synthesis of longitudinal changes in white matter integrity after mild traumatic brain injury assessed by diffusion tensor imaging in adults. Eur. J. Radiol. 2021, 147, 110117. [Google Scholar] [CrossRef]
- Yoen, H.; Yoo, R.-E.; Choi, S.H.; Kim, E.; Oh, B.-M.; Yang, D.; Hwang, I.; Kang, K.M.; Yun, T.J.; Kim, J.-H.; et al. Blood-Brain Barrier Disruption in Mild Traumatic Brain Injury Patients with Post-Concussion Syndrome: Evaluation with Region-Based Quantification of Dynamic Contrast-Enhanced MR Imaging Parameters Using Automatic Whole-Brain Segmentation. Korean J. Radiol. 2021, 22, 118–130. [Google Scholar] [CrossRef]
- Ware, J.B.; Sinha, S.; Morrison, J.; Walter, A.E.; Gugger, J.J.; Schneider, A.L.; Dabrowski, C.; Zamore, H.; Wesley, L.; Magdamo, B.; et al. Dynamic contrast enhanced MRI for characterization of blood-brain-barrier dysfunction after traumatic brain injury. NeuroImage: Clin. 2022, 36, 103236. [Google Scholar] [CrossRef]
- Oh, Sung Suk, Eun-Hee Lee, Jong-Hoon Kim, Young Beom Seo, Yoo Jin Choo, Juyoung Park, and Min Cheol Chang. "The use of dynamic contrast-enhanced magnetic resonance imaging for the evaluation of blood-brain barrier disruption in traumatic brain injury: what is the evidence?" Brain Sciences 11, no. 6 (2021): 775. [CrossRef]
- Iyad, N.; S. Ahmad, M.; Alkhatib, S.G.; Hjouj, M. Gadolinium contrast agents- challenges and opportunities of a multidisciplinary approach: Literature review. Eur. J. Radiol. Open 2023, 11, 100503. [Google Scholar] [CrossRef]
- Rasschaert, Marlène, Roy O. Weller, Josef A. Schroeder, Christoph Brochhausen, and Jean-Marc Idée. "Retention of gadolinium in brain parenchyma: pathways for speciation, access, and distribution. A critical review." Journal of Magnetic Resonance Imaging 52, no. 5 (2020): 1293-1305. [CrossRef]
- Stanescu, A.L.; Shaw, D.W.; Murata, N.; Murata, K.; Rutledge, J.C.; Maloney, E.; Maravilla, K.R. Brain tissue gadolinium retention in pediatric patients after contrast-enhanced magnetic resonance exams: pathological confirmation. Pediatr. Radiol. 2020, 50, 388–396. [Google Scholar] [CrossRef]
- Byrnes, K.R.; Wilson, C.M.; Brabazon, F.; von Leden, R.; Jurgens, J.S.; Oakes, T.R.; Selwyn, R.G. FDG-PET imaging in mild traumatic brain injury: a critical review. Front. Neuroenergetics 2014, 5, 13. [Google Scholar] [CrossRef]
- Gandy, S.; DeKosky, S.T. [18F]-T807 tauopathy PET imaging in chronic traumatic encephalopathy. F1000Research 2014, 3, 229. [Google Scholar] [CrossRef]
- Selwyn, R.; Hockenbury, N.; Jaiswal, S.; Mathur, S.; Armstrong, R.C.; Byrnes, K.R. Mild Traumatic Brain Injury Results in Depressed Cerebral Glucose Uptake: An 18FDG PET Study. J. Neurotrauma 2013, 30, 1943–1953. [Google Scholar] [CrossRef]
- Wu, H.-M.; Huang, S.-C.; Hattori, N.; Glenn, T.C.; Vespa, P.M.; Yu, C.-L.; Hovda, D.A.; Phelps, M.E.; Bergsneider, M. Selective Metabolic Reduction in Gray Matter Acutely following Human Traumatic Brain Injury. J. Neurotrauma 2004, 21, 149–161. [Google Scholar] [CrossRef]
- Hattori, N.; Huang, S.-C.; Wu, H.-M.; Liao, W.; Glenn, T.C.; Vespa, P.M.; E Phelps, M.; A Hovda, D.; Bergsneider, M. Acute changes in regional cerebral (18)F-FDG kinetics in patients with traumatic brain injury. . 2004, 45, 775–83. [Google Scholar]
- Bergsneider, M.; Hovda, D.A.; Shalmon, E.; Kelly, D.F.; Vespa, P.M.; Martin, N.A.; Phelps, M.E.; McArthur, D.L.; Caron, M.J.; Kraus, J.F.; et al. Cerebral hyperglycolysis following severe traumatic brain injury in humans: a positron emission tomography study. J. Neurosurg. 1997, 86, 241–251. [Google Scholar] [CrossRef]
- Worley, G.; Hoffman, J.M.; Paine, S.S.; Kalman, S.L.; Claerhout, S.J.; Boyko, O.B.; Kandt, R.S.; Santos, C.C.; Hanson, M.W.; Oakes, W.J.; et al. 18-FLUORODEOXYGLUCOSE POSITRON EMISSION TOMOGRAPHY IN CHILDREN AND ADOLESCENTS WITH TRAUMATIC BRAIN INJURY. Dev. Med. Child Neurol. 1995, 37, 213–220. [Google Scholar] [CrossRef]
- Bergsneider, M.; Hovda, D.A.; Lee, S.M.; Kelly, D.F.; McARTHUR, D.L.; Vespa, P.M.; Lee, J.H.; Huang, S.-C.; Martin, N.A.; Phelps, M.E.; et al. Dissociation of Cerebral Glucose Metabolism and Level of Consciousness During the Period of Metabolic Depression Following Human Traumatic Brain Injury. J. Neurotrauma 2000, 17, 389–401. [Google Scholar] [CrossRef]
- level of consciousness during the period of metabolic depression following human traumatic brain injury. J Neurotrauma. 2000; 17:389–401.
- Buchsbaum MS, Simmons AN, DeCastro A, Farid N, Matthews SC. Clusters of low 18F-fluorodeoxyglucose uptake voxels in combat veterans with traumatic brain injury and post-traumatic stress disorder. J Neurotrauma. 2015; 32:1736–50. [CrossRef]
- Komura, A.; Kawasaki, T.; Yamada, Y.; Uzuyama, S.; Asano, Y.; Shinoda, J. Cerebral Glucose Metabolism in Patients with Chronic Mental and Cognitive Sequelae after a Single Blunt Mild Traumatic Brain Injury without Visible Brain Lesions. J. Neurotrauma 2019, 36, 641–649. [Google Scholar] [CrossRef]
- Leuzy, A.; Chiotis, K.; Lemoine, L.; Gillberg, P.-G.; Almkvist, O.; Rodriguez-Vieitez, E.; Nordberg, A. Tau PET imaging in neurodegenerative tauopathies—still a challenge. Mol. Psychiatry 2019, 24, 1112–1134. [Google Scholar] [CrossRef]
- Shivamurthy, V.K.N.; Tahari, A.K.; Marcus, C.; Subramaniam, R.M. Brain FDG PET and the Diagnosis of Dementia. Am. J. Roentgenol. 2015, 204, W76–W85. [Google Scholar] [CrossRef]
- Moghbel MC, Saboury B, Basu S, Metzler SD, Torigian DA, Långström B, et al. Amyloid-β imaging with PET in Alzheimer’s disease: is it feasible with current radiotracers and technologies? Springer; 2012.
- Leuzy, A.; Chiotis, K.; Lemoine, L.; Gillberg, P.-G.; Almkvist, O.; Rodriguez-Vieitez, E.; Nordberg, A. Tau PET imaging in neurodegenerative tauopathies—still a challenge. Mol. Psychiatry 2019, 24, 1112–1134. [Google Scholar] [CrossRef]
- Barrio JR, Small GW, Wong K-P, Huang S-C, Liu J, Merrill DA, et al. In vivo characterization of chronic traumatic encephalopathy using [F-18] FDDNP PET brain imaging. Proc Natl Acad Sci. E: 2015;112, 2015. [CrossRef]
- Harada, R.; Okamura, N.; Furumoto, S.; Tago, T.; Yanai, K.; Arai, H.; Kudo, Y. Characteristics of Tau and Its Ligands in PET Imaging. Biomolecules 2016, 6, 7. [Google Scholar] [CrossRef]
- Choi SR, Schneider JA, Bennett DA, Beach TG, Bedell BJ, Zehntner SP, et al. Correlation of amyloid PET ligand florbetapir F 18 binding with Aβ aggregation and neuritic plaque deposition in postmortem brain tissue. Alzheimer Dis Assoc Disord.2012;26:8–16. [CrossRef]
- Lister-James, J.; Pontecorvo, M.J.; Clark, C.; Joshi, A.D.; Mintun, M.A.; Zhang, W.; Lim, N.; Zhuang, Z.; Golding, G.; Choi, S.R.; et al. Florbetapir F-18: A Histopathologically Validated Beta-Amyloid Positron Emission Tomography Imaging Agent. Semin. Nucl. Med. 2011, 41, 300–304. [Google Scholar] [CrossRef]
- Baker, S.L.; Harrison, T.M.; Maass, A.; La Joie, R.; Jagust, W.J. Effect of Off-Target Binding on 18F-Flortaucipir Variability in Healthy Controls Across the Life Span. J. Nucl. Med. 2019, 60, 1444–1451. [Google Scholar] [CrossRef]
- Dani, M.; Brooks, D.J.; Edison, P. Tau imaging in neurodegenerative diseases. Eur. J. Nucl. Med. 2015, 43, 1139–1150. [Google Scholar] [CrossRef]
- Kantarci K, Lowe VJ, Boeve BF, Senjem ML, Tosakulwong N, Lesnick TG, et al. AV-1451 tau and β-amyloid positron emission tomography imaging in dementia with Lewy bodies. Ann Neurol. 2017; 81:58–67. [CrossRef]
- Joseph, C.R.; Benhatzel, C.M.; Stern, L.J.; Hopper, O.M.; Lockwood, M.D. Pilot study utilizing MRI 3D TGSE PASL (arterial spin labeling) differentiating clearance rates of labeled protons in the CNS of patients with early Alzheimer disease from normal subjects. Magma: Magn. Reson. Mater. Physics, Biol. Med. 2020, 33, 559–568. [Google Scholar] [CrossRef]
- Joseph, C.R.; Lim, J.K.; Grohol, B.N.; Zivcevska, M.; Lencke, J.; Rich, E.D.; Arrasmith, C.J.; Dorman, I.S.; Clark, B.W.; Love, K.; et al. Identifying delay in glymphatic clearance of labeled protons post-acute head trauma utilizing 3D ASL MRI (arterial spin labeling): a pilot study. Sci. Rep. 2024, 14, 1–10. [Google Scholar] [CrossRef]
- Zhao, Moss Y., Audrey P. Fan, David Yen-Ting Chen, Magdalena J. Sokolska, Jia Guo, Yosuke Ishii, David D. Shin et al. "Cerebrovascular reactivity measurements using simultaneous 15O-water PET and ASL MRI: Impacts of arterial transit time, labeling efficiency, and hematocrit." Neuroimage 233 (2021): 117955. [CrossRef]
- Elschot, E.P.M.; Backes, W.H.; Postma, A.A.; van Oostenbrugge, R.J.; Staals, J.; Rouhl, R.P.; Jansen, J.F. A Comprehensive View on MRI Techniques for Imaging Blood-Brain Barrier Integrity. Investig. Radiol. 2020, 56, 10–19. [Google Scholar] [CrossRef]
- Joseph, C.R.; Kreilach, A.; Reyna, V.A.; Kepler, T.A.; Taylor, B.V.; Kang, J.; McCorkle, D.; Rider, N.L. Utilizing Reduced Labeled Proton Clearance to Identify Preclinical Alzheimer Disease with 3D ASL MRI. Case Rep. Neurol. 2023, 15, 177–186. [Google Scholar] [CrossRef]
- Takahata, K.; Kimura, Y.; Sahara, N.; Koga, S.; Shimada, H.; Ichise, M.; Saito, F.; Moriguchi, S.; Kitamura, S.; Kubota, M.; et al. PET-detectable tau pathology correlates with long-term neuropsychiatric outcomes in patients with traumatic brain injury. Brain 2019, 142, 3265–3279. [Google Scholar] [CrossRef]
- Gorgoraptis, N.; Li, L.M.; Whittington, A.; Zimmerman, K.A.; Maclean, L.M.; McLeod, C.; Ross, E.; Heslegrave, A.; Zetterberg, H.; Passchier, J.; et al. In vivo detection of cerebral tau pathology in long-term survivors of traumatic brain injury. Sci. Transl. Med. 2019, 11. [Google Scholar] [CrossRef]
- Gandy, Sam, Milos D. Ikonomovic, Effie Mitsis, Gregory Elder, Stephen T. Ahlers, Jeffrey Barth, James R. Stone, and Steven T.DeKosky. "Chronic traumatic encephalopathy: clinical biomarker correlations and current concepts in pathogenesis." Molecular neurodegeneration 9 (2014): 1-22. [CrossRef]
- Ware, Jeffrey B., Saurabh Sinha, Justin Morrison, Alexa E. Walter, James J. Gugger, Andrea LC Schneider, Cian Dabrowski et al. "Dynamic contrast enhanced MRI for characterization of blood-brain-barrier dysfunction after traumatic brain injury." NeuroImage: Clinical 36 (2022): 103236. [CrossRef]
- Morgan, Richard, Jordon Prosapio, Sam Kara, Sreepadma Sonty, Pamela Youssef, and Kester Nedd. "Preliminary clinical diagnostic criteria for chronic traumatic encephalopathy: A case report and literature review." Interdisciplinary Neurosurgery 26 (2021): 101290. [CrossRef]
- Li, Ka-loh, Xiaoping Zhu, Nola Hylton, Geon-Ho Jahng, Michael W. Weiner, and Norbert Schuff. "Four-phase single-capillary stepwise model for kinetics in arterial spin labeling MRI." Magnetic Resonance in Medicine: An Official Journal of the International Society for Magnetic Resonance in Medicine 53, no. 3 (2005): 511-518. [CrossRef]
Figure 1.
Sparse canonical correlation analysis (SCCA) of T1-weighted MP-RAGE and 30-direction diffusion tensor images (DTI) datasets are used to quantify traumatically induced disruption of WM and cortical networks. The cohort includes 17 controls and 16 patients with TBI (age and gender matched). Each patient had a history of non-penetrating TBI of at least moderate severity. White matter integrity is assessed by DTI and fractional anisotropy (FA) maps are generated. Separately, probabilistic segmentation of the T1-weighted imaging is performed to assess gray matter integrity. Variation in brain shape across subjects is normalized by diffeomorphically mapping these data into a population- specific template space. Image processing steps rely on the Camino and ANTs (Advanced Normalization Tools) neuroimage analysis open-source toolkits. SCCA demonstrates significant differences between the control and patient groups in both the FA (p < 0.002) and gray matter (p < 0.01) that are widespread but largely focus on thalamocortical networks related to the limbic system. Using SCCA identified regions, a strong correlation is identified between degree of injury in WM and GM within the patient group. Figure courtesy of James R. Stone. Gandy, Sam, Milos D. Ikonomovic, Effie Mitsis, Gregory Elder, Stephen T. Ahlers, Jeffrey Barth, James R. Stone, and Steven T.DeKosky. "Chronic traumatic encephalopathy: clinical biomarker correlations and current concepts in pathogenesis." Molecular neurodegeneration 9 (2014): 1-22. [122].
Figure 1.
Sparse canonical correlation analysis (SCCA) of T1-weighted MP-RAGE and 30-direction diffusion tensor images (DTI) datasets are used to quantify traumatically induced disruption of WM and cortical networks. The cohort includes 17 controls and 16 patients with TBI (age and gender matched). Each patient had a history of non-penetrating TBI of at least moderate severity. White matter integrity is assessed by DTI and fractional anisotropy (FA) maps are generated. Separately, probabilistic segmentation of the T1-weighted imaging is performed to assess gray matter integrity. Variation in brain shape across subjects is normalized by diffeomorphically mapping these data into a population- specific template space. Image processing steps rely on the Camino and ANTs (Advanced Normalization Tools) neuroimage analysis open-source toolkits. SCCA demonstrates significant differences between the control and patient groups in both the FA (p < 0.002) and gray matter (p < 0.01) that are widespread but largely focus on thalamocortical networks related to the limbic system. Using SCCA identified regions, a strong correlation is identified between degree of injury in WM and GM within the patient group. Figure courtesy of James R. Stone. Gandy, Sam, Milos D. Ikonomovic, Effie Mitsis, Gregory Elder, Stephen T. Ahlers, Jeffrey Barth, James R. Stone, and Steven T.DeKosky. "Chronic traumatic encephalopathy: clinical biomarker correlations and current concepts in pathogenesis." Molecular neurodegeneration 9 (2014): 1-22. [122].
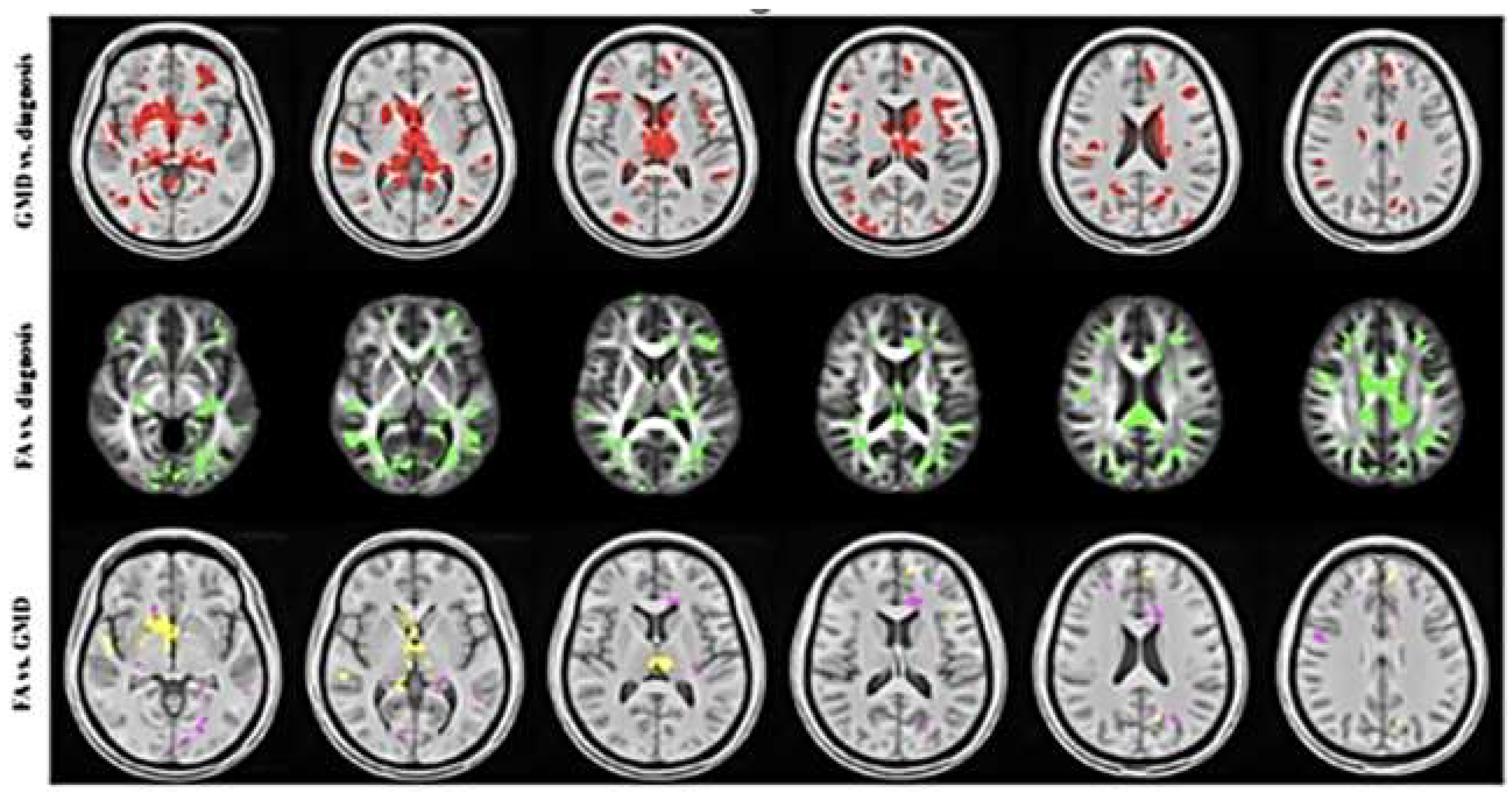
Figure 3.
FDG-PET scan of the brain. (Top) Sagittal views (Left to right) illustrate hypometabolism in the bilateral posterior parietotemporal regions, posterior_cingulate and precuneus (Middle) Coronal views (Posterior to anterior) show decreased uptake in the medial_temporal_lobes (Bottom) Axial views (Inferior to superior) demonstrate hypometabolism in the frontal_lobe and anterior temporal poles.
Figure 3.
FDG-PET scan of the brain. (Top) Sagittal views (Left to right) illustrate hypometabolism in the bilateral posterior parietotemporal regions, posterior_cingulate and precuneus (Middle) Coronal views (Posterior to anterior) show decreased uptake in the medial_temporal_lobes (Bottom) Axial views (Inferior to superior) demonstrate hypometabolism in the frontal_lobe and anterior temporal poles.
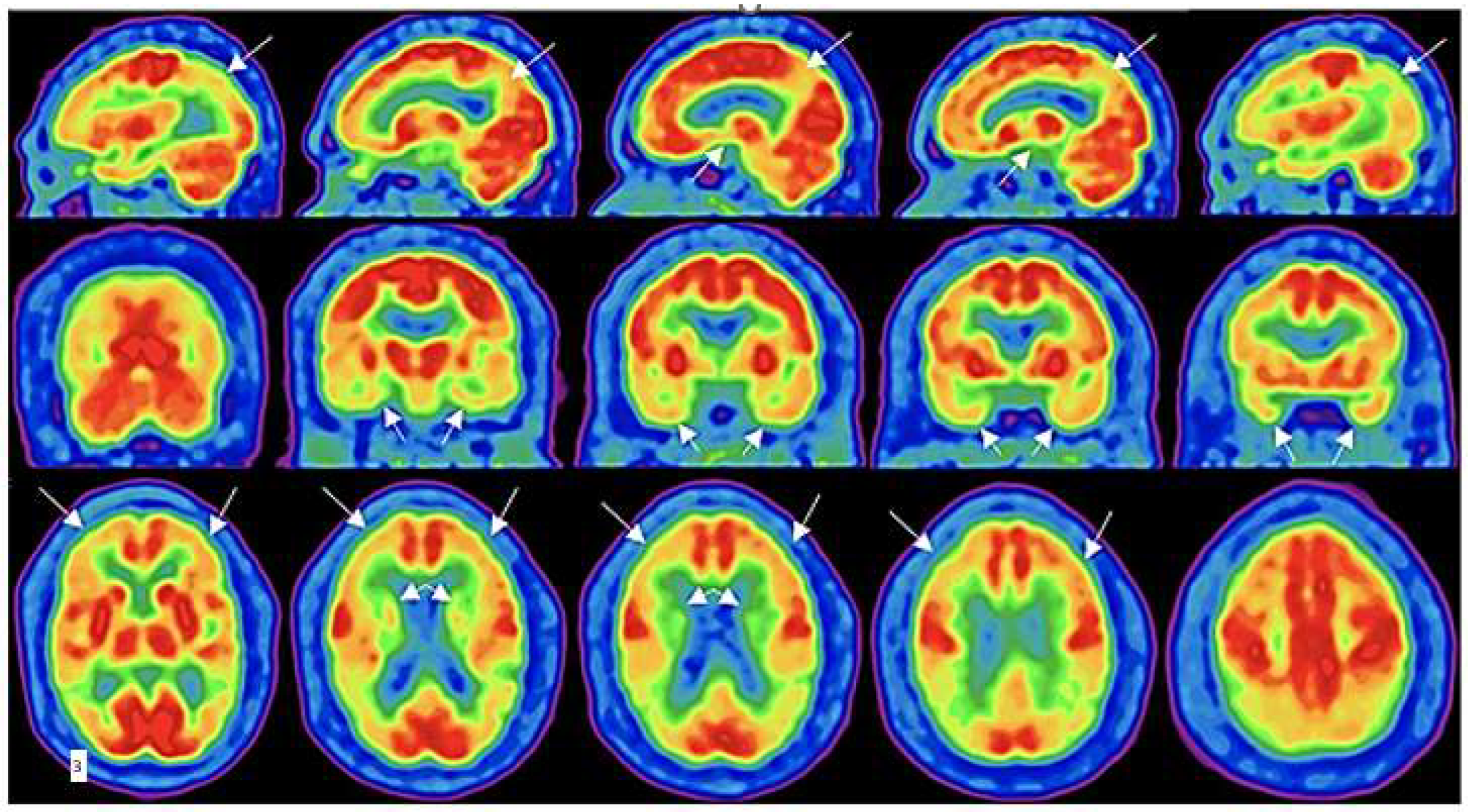
Figure 4.
Composition of the ASL signal/time into its various components: arterial (dotted line), capillary (dot and dash line, and extra capillary (dashed line) spaces. TI (acquisition) times utilized in this study are between the red arrow limits. Note the signal composition is nearly completely extravascular (interstitial) water, which is normally cleared by the glymphatic system. Red bars and arrows = our post labeling delay acquisition times; Lt blue dot = 800-850 msec T1 of white matter; Orange dot = 1700ms T1 of gray matter (all values are for 3T); Green dot = 1650 msec T1 (63% signal decay) of blood; Dk Blue dot = 3800ms T1 of water (CSF fluid)
Figure 4.
Composition of the ASL signal/time into its various components: arterial (dotted line), capillary (dot and dash line, and extra capillary (dashed line) spaces. TI (acquisition) times utilized in this study are between the red arrow limits. Note the signal composition is nearly completely extravascular (interstitial) water, which is normally cleared by the glymphatic system. Red bars and arrows = our post labeling delay acquisition times; Lt blue dot = 800-850 msec T1 of white matter; Orange dot = 1700ms T1 of gray matter (all values are for 3T); Green dot = 1650 msec T1 (63% signal decay) of blood; Dk Blue dot = 3800ms T1 of water (CSF fluid)
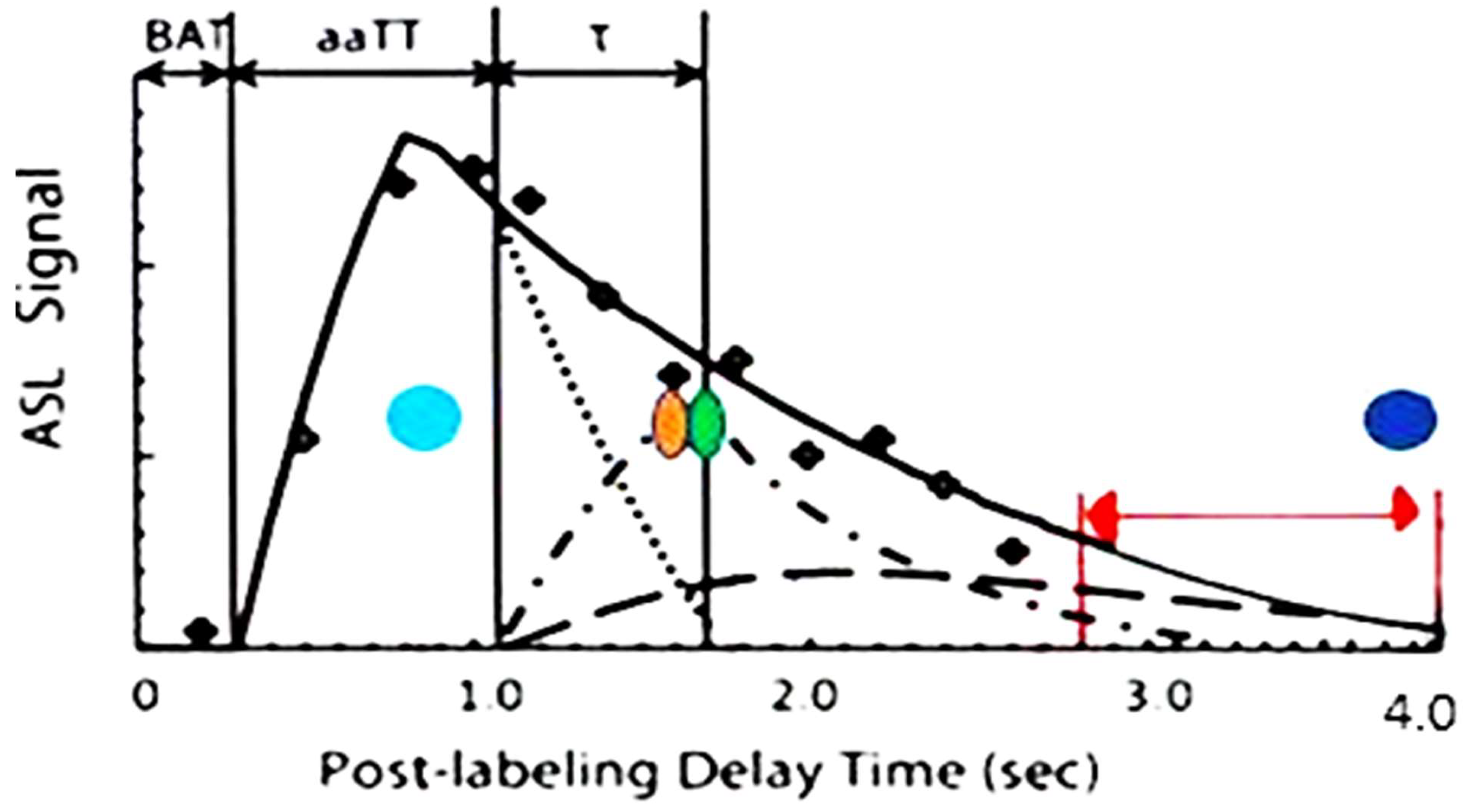

Table 1.
Methods of BBB and shear injury imaging modalities and limitations.
| Imaging procedure. | Target | Sensitivity | Limitations |
|---|---|---|---|
| Diffusion Tensor Imaging (DTI) MRI | Diffusion of water -white matter tracts | Not clear, older techniques problematic. New techniques in development | Technique specific sensitivity, scan time |
| Dynamic Contrast Enhanced (DCE) MRI | BBB leak of contrast | Sensitive for BBB leak | Requires gadolinium contrast, long scan times, not suitable for serial studies due to cerebral accumulation of GD+ |
| 18FDG-PET | Glucose utilization metabolic activity | Can identify the brief hypermetabolism acutely (animal studies) and chronic hypometabolism (human) chronically across severity spectrum | Cost, long scan times, availability of technology, |
| 3D ASL MRI | Perfusion/Diffusion of labeled protons | Highly sensitive in a small clinical trial in mTBI determining altered cMTT/BBB leak with delayed BBB clearance/recovery | Requires a 3T or greater field strength, Low signal, hand drawn ROI, requires a larger series for confirmation of sensitivity. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



