
Submitted:
03 October 2024
Posted:
04 October 2024
You are already at the latest version
Abstract
Carcinoid syndrome (CS) is a rare condition associated with neuroendocrine tumors (NETs), particularly those originating in the gastrointestinal tract, which secrete bioactive substances like serotonin. The management of CS requires a multidisciplinary approach due to its complex clinical manifestations, including flushing, diarrhea, bronchospasm, and carcinoid heart disease. Optimal care involves collaboration between several professional figures like oncologists, endocrinolo-gists, gastroenterologists, surgeons, and dietitians. Currently, a wide range of treatments are available focused on both symptom control and tumor burden reduction. Somatostatin analogs (SSAs) are the first-line therapy for symptom relief. Still, in patients with progressive disease or refractory CS, other options include targeted therapies, peptide receptor radionuclide therapy (PRRT), liver-directed therapies, and surgical resection when feasible. Furthermore, management of complications related to prolonged serotonin release and malnutrition as a result of exocrine pancreatic insufficiency, post-surgical conditions, vitamin deficit, and chronic diarrhea often re-quires early detection to mitigate symptoms and improve the quality of life in these patients. The complexity of CS necessitates individualized care and continuous coordination among specialists to optimize outcomes and enhance patient well-being.
Keywords:
neuroendocrine tumor
; carcinoid syndrome
; cancer
; multidisciplinary team
1. Introduction
Heterogeneous biological behaviors with different clinical presentations and therapeutic approaches characterize neuroendocrine neoplasms (NENs). From a histological point of view, they can be distinguished based on the morphology of the tumor cells into well-differentiated forms, known as neuroendocrine tumors (NETs), and poorly differentiated forms, referred to as neuroendocrine carcinomas (NECs). From a clinical perspective, they can be categorized as functioning (when a specific tumor-related syndrome is present) or non-functioning (in cases where only generic, non-specific symptoms are observed).
One of the most representative clinical manifestations of functioning NETs is represented by carcinoid syndrome (CS), which is caused by tumoral secretion of multiple hormonal amines and peptides, mainly serotonin (5hydroxytryptamine, 5-HT) [1].
CS is predominantly described in about 20% of patients with well-differentiated small-intestine NETs, representing 50% of all gastro-entero-pancreatic neuroendocrine tumors (GEP-NETs) [2,3]. It is often diagnosed in the fifth and sixth decade of life, with a slightly higher incidence among females than males [4]. Since the liver has the function of deactivating tumor-released active hormones, generally, CS indicates the presence of a metastatic tumor outside of the portal venous drainage; however, in a small proportion of patients, CS may develop without liver metastases [5]. Patients with CS have an overall survival of 4.7 years compared with 7.1 years in patients without symptoms of CS, and tumor burden is described as one of the most relevant factors affecting CS-related mortality [2].
CS may occur with a vast and not-so-specific spectrum of symptomatology that is represented mainly by diarrhea and flushing because of the release of serotonin [1]. Moreover, CS in patients with NET is associated with worse quality of life (QoL), particularly compromised by increased diarrhea or flushing [6]. As the disease progresses slowly, long-term complications may arise, such as carcinoid heart disease (CHD), fibrotic small bowel obstruction, and, importantly, malnutrition. The condition can worsen to a life-threatening complication known as a carcinoid crisis characterized by bronchospasm, flushing, and significant hemodynamic instability (systolic blood pressure < 80 or >180 mmHg, heart rate > 120 bpm) [4,7].
2. Focus of the review
According to the latest scientific evidence, this review will focus on the diagnostic and therapeutic management of carcinoid syndrome in NETs. The intent is to provide clinicians with a broad and straightforward overview of the effective approach of CS, which requires a combination of biochemical, imaging, and therapeutic strategies to control both the tumor and the hormonal secretion. Through this focused approach, the review seeks to contribute valuable knowledge to enhance patient care and improve treatment outcomes in this patient population.
In this narrative review, we gathered data by conducting a comprehensive search of the MEDLINE database without imposing any date limitations. Our search criteria were conducted through specific keywords: “neuroendocrine tumors”, “carcinoid syndrome”, “diagnosis” and “treatment”. The scope of our inclusion was limited to articles pertinent to this review’s aims and composed in English. This research did not adhere to the systematic review protocol; instead, the articles were selected based on the authors’ subjective judgment.
3. Clinical Presentation
Clinical evaluation of patients with NET in whom there is suspicion of CS may be challenging. However, some signs and symptoms could guide therapeutic decisions.
CS is characterized frequently by diarrhea (60–80%) and flushing (90%) because 5-HT acts through mechanisms of vasoconstriction or vasodilation, increased gut motility, and increased secretion of water, sodium, chloride, and potassium [1].
- Diarrhea is defined in terms of alterations of stool frequency, consistency, volume, or weight, and it is typically secretory with patients complaining of at least three and up to 30 bowel movements in a day. To exclude other concomitant causes of diarrhea, personal and family history, previous surgery, home therapy, and other conditions NET-related (e.g., steatorrhea secondary to somatostatin analogs) must be investigated [4,8,9].
- Flushing is the most common sign of CS: the phenomenon may present as either an intermittent or persistent sensation of warmth accompanied by skin erythema, typically affecting the upper body region. (head, neck, upper chest) with eventual telangiectasia. In CS, flushing usually occurs as “dry,” reddish brown/bright red with short-lived episodes [5].
Recent reports indicate that gender-related disparities are observed in patients with CS associated with NET, highlighting significant variations in clinical presentation, risk factors, and outcomes between males and females. [10]. Women were found to experience more severe symptoms, including higher incidences of abdominal pain, tachycardia, and psychiatric disorders such as depression. At the same time, men showed a greater likelihood of lymph node metastases at diagnosis. Risk factor analysis indicated that men were more likely to be smokers and alcohol drinkers, which may contribute to these differences in disease manifestation. Despite these disparities in clinical presentation, the study found no significant differences in progression-free survival (PFS) or overall survival (OS) between genders, with both men and women responding similarly to treatments such as surgery and medical therapies. The data indicate that although CS occurs slightly more often in men, women might experience more severe symptomatology, highlighting the necessity for a gender-specific therapy strategy to enhance patient outcomes [10]. In the landscape of NET, women also tend to have better survival rates and treatment responses, but the disease impacts quality of life differently for both sexes. Despite known sex differences, they are primarily underestimated in clinical practice, and there is a lack of clinical trials addressing these disparities. More systematic studies on sex-related differences are needed to develop tailored treatment strategies that improve both prognosis and quality of life in patients with CS [11].
4. Diagnosis
Global assessment of CS results from a combination of appropriate clinical, biochemical, and radiological evaluations.
When CS is suspected, the most reliable initial assessment is the measurement of 24-h urinary 5-hydroxyindoleacetic acid (5-HIAA) levels (sensitivity 73–91%, specificity 100%), a metabolite of serotonin (>50 μmol, the cut-off to consider compatible with the diagnosis of CS) [12,13]. In selected cases, the assessment of plasma 5-HIAA can be used as a convenient alternative to the urinary 5-HIAA collection due to the similar sensitivity, the absence of influence by meals, and the advantage of a single determination in a day [5,14].
Recently, a close correlation between plasma and serum 5-HIAA has been demonstrated, with a sensitivity of 91.2% and specificity of 61.9% at a cut-off of 135 nmol/l compared to the urinary assay [15]. A statistically significant agreement was observed between plasma and serum 5-HIAA and the traditional urine assay in patients with nNETs (κ = 0.675, p < 0.001) and in healthy volunteers (κ = 0.967, p < 0.001), indicating that either plasma or serum can be reliably used for monitoring 5-HIAA. Based on these data, plasma measurement can be considered an alternative to urine testing. However, the latter remains more readily available in clinical practice and better standardized regarding result interpretation.Therefore, typical clinical symptoms, such as diarrhea and flushing, and the recognition of elevated serotonin metabolite 5-HIAA in a 24-h urine test establish the diagnosis of CS [16].
Imaging studies (CT scan, MRI, and PET Gallium DOTATOC) are taking a key role in the whole assessment of the patients with NET associated with CS to determine global tumor burden and liver metastasis, somatostatin receptor status and to evaluate tumor growth rate and eventual locoregional therapies [17].
Despite CS usually arises when NENs, primarily from the small intestine, secrete serotonin and other vasoactive substances that bypass liver metabolism, often due to hepatic metastases, allowing these products to enter the systemic circulation and cause characteristic symptoms, it may occur even in the absence of liver metastases. The study by Halperin et al. confirms that CS is commonly associated with advanced disease but unexpectedly found a high incidence of the syndrome in patients with localized (19%) and regional (37%) disease, particularly in those with small-bowel NET. This suggests that unrecognized hepatic metastases or CS in locoregional disease might be more prevalent. The study indicates an unexpectedly high prevalence of CS in individuals with colorectal NETs, perhaps attributable to the extensive categorization of these tumors, encompassing both midgut and hindgut origins. Lung NETs exhibited a very low incidence of CS, potentially attributable to unusual manifestations that allow released substances to bypass hepatic clearance [2].
5. Treatment
Carcinoid syndrome presents a significant challenge in clinical management due to its debilitating symptoms. Currently, several therapeutic options are available for alleviating these symptoms, which can significantly impact the quality of life for affected patients. The primary treatment modality involves somatostatin analogs, such as octreotide and lanreotide, which have been shown to provide substantial symptom relief in many cases. However, for patients who experience refractory symptoms, additional treatment options exist, including telotristat ethyl, which explicitly targets serotonin production, and everolimus, an mTOR inhibitor that can help control tumor growth. Furthermore, liver-directed therapies and chemotherapy may be considered depending on the extent of the disease and patient-specific factors. This multifaceted approach underscores the importance of effective personalized treatment plans in managing carcinoid syndrome (Figure 1).
- Medical therapy
First-line treatment for controlling the symptoms of CS is represented by long-acting release somatostatin analogs (SSAs), such as octreotide (30 mg/4 weeks) and lanreotide (60 mg, 90 mg, and 120 mg/4 weeks), which provide substantial symptom relief in CS. A meta-analysis summarized the treatment of CS patients with both analogs, reporting achievement of CS symptom control in 66–70% of patients and a decrease in 5-HIAA levels in 45–46% of CS patients [18]. These agents also have an antiproliferative effect on tumor growth (directly with cycle arrest and apoptosis, indirectly by inhibition of angiogenesis and immunomodulation), prolonging PFS, as reported by phase-3 randomized controlled trials [19,20,21]. SSAs are safe and well-tolerated drugs, with only 15% of patients experiencing adverse events (AEs) which could be short-term AEs (usually mild/moderate) such as pain at injection site, nausea (76%), constipation (85%), diarrhea (16–78%), abdominal cramps (50%), and hyperglycemia and long-term AEs including cholelithiasis (5–60%) and exocrine pancreatic insufficiency (20–24%) [9].
However, in about 30–76% of cases, patients with NET associated with CS may experience a condition called refractory CS (RCS), namely recurrence/persistence of CS symptoms and increase/persistence of high urinary 5-HIAA levels despite the use of maximum label doses of SSA. This condition might result from the progression of symptoms, which is more often caused by tumor growth than by the development of tachyphylaxis to the administered doses of SSA [5,16]. Nevertheless, several other medical therapeutic strategies can come to aid clinicians.
The first therapeutic step in patients with RCS is to evaluate the possibility of SSA dose escalation, decreasing the interval time of SSA administration. In this regard, several studies have reported favorable clinical, biochemical, and tumor response results. Strosberg et al. reported that on 239 patients receiving above-standard doses of SSA due to CS (62%) or tumor progression (28%), the most common dose changes were escalation to 40 mg every four weeks (71%) and to 60 mg every four weeks (18%). Of 90 patients with flushing before the first dose escalation, 73 (81%) were reported to have experienced improvement or resolution of their symptoms following the dose escalation. Of 107 patients who complained of diarrhea before the first dose escalation, 85 (79%) were reported to have experienced improvement or resolution after the first dose escalation [22]. Indeed, a small phase II study showed that increasing the frequency of administration of SSA to every 21 days led to complete and partial control of clinical symptoms in 40% and 60% of cases, respectively [23]. ENETS guidelines also suggested that administration of the long-acting SSA should be combined with (100 μg to 500 μg every 6–8 h), for up to 2 weeks or as a rescue therapy when CS is not controlled [5].
Analyzing the data from the available studies is not straightforward due to various influencing factors. They show variability in the effectiveness of octreotide LAR for managing CS symptoms, with efficacy rates ranging from 25% to 70% [16]. This variation is likely attributed to differences in study designs and inclusion criteria, including symptom severity, tumor burden, and SSA dosing schedules. Additionally, when reporting adverse AEs, it is crucial to consider potential confounding factors, such as differing toxicity assessment methods. Symptoms of CS, like abdominal pain and diarrhea, can be challenging to differentiate from those caused by SSA.
Pasireotide is a SSA with a higher affinity to somatostatin receptors 1, 3, and 5 when compared with octreotide and lanreotide. It has been shown to be effective, especially in managing diarrhea and flushing symptoms in most patients suffering from RCS [4]. A phase III study compared long-acting pasireotide 60 mg to octreotide LAR 40 mg every 28 days was performed in 110 patients with RCS symptoms on previous SSA. The treatment with long-acting pasireotide reduced diarrhea by 25% and flushing by 42% at six months compared with baseline. The most frequent AE registered was hyperglycemia (pasireotide 28.3% vs. octreotide 5.3%) [24]. Pasireotide LAR showed a trend toward a higher tumor control rate at month 6, even with no statistical significance. However, the study was discontinued prematurely due to a low likelihood of demonstrating that long-acting pasireotide was superior to an increased dose of long-acting octreotide [25].
Interferon alpha (IFN-α) is an ancient drug that may be considered in patients with RCS due to anti-proliferative efficacy through cytotoxic, anti-angiogenic, and immunomodulatory effects. Still, its low safety profile has limited its use (e.g., flu-like symptoms, chronic fatigue, liver, and bone marrow toxicity) [26]. Even though an age-old study reported improvement in 50% of patients treated with IFN after the failure of SSA in controlling CS, prospective randomized trials did not confirm any benefit of the addition of IFN to SSA in controlling tumor growth and improving the survival of patients compared to SSA monotherapy [16].
Telotristat ethyl is an oral inhibitor of tryptophan hydroxylase, the limiting enzyme of serotonin synthesis. The recommended dose is 250 mg three times a day [5]. The most recent studies that evaluated telotristat for CS control refractory to somatostatin analogs are two phase III studies (TELESTAR and TELECAST), using 250 mg and 500 mg three times a day. These trials described similar results regarding a decrease in bowel movement frequency ranging from 26% to 43% and a significant reduction of urinary 5-HIAA value [27,28]. As the results of the TELEPATH study described, the main AEs registered due to telotristat administration included liver-related AEs, depression, and gastrointestinal AEs (e.g., nausea and abdominal pain). The occurrence of AEs was not related to dosage or duration of therapy. Most AEs were mild to moderate in severity, and no deaths were related to telotristat ethyl [29].
Everolimus is an mTOR inhibitor, which blocks the mammalian target of the rapamycin (mTOR) pathway, which plays a key role in regulating cell growth, proliferation, metabolism, and survival.
The main study was the RADIANT-2, a double-blind, placebo-controlled phase III trial of 429 patients with advanced NET and history of symptomatic carcinoid syndrome investigating the efficacy of everolimus 10 mg daily in combination with long-acting octreotide 30 mg every 28 days. Although the primary endpoint was progression-free survival, a significant reduction in urinary 5-HIAA in the everolimus arm was also reported compared to the other arm (61% versus 36%) [30]. The control of symptoms associated with carcinoid syndrome was not assessed, but they are properly derived from case reports and case series. Control of carcinoid syndrome with everolimus [31]. The most frequent AEs registered from RADIANT-2 were stomatitis, rash, and fatigue.
Peptide receptor radionuclide therapy (PRRT) with 177Lu-DOTATATE represents an efficient and safe systemic option among the wide possibilities to treat NET patients with positive somatostatin receptor imaging and to improve symptoms in progressive disease.
The NETTER-1 phase III trial randomized 229 patients with advanced well-differentiated G1 or G2 progressing midgut NET in two arms (Lutetium177 Dotatate plus octreotide LAR 30 mg vs. octreotide LAR 60 mg) [32]. As regards CS diarrhea (present almost equally in both treatment arms) improved equivalently in 48% and 43% of the patients in the 177Lu-DOTATATE + octreotide LAR 30 mg arm versus octreotide LAR 60 mg arm alone, respectively; however, considering diarrhea, quality of life after PRRT is significantly better than in the control arm in terms of time to deterioration. Unfortunately, there was no difference in control of other symptoms, including flushing [33]. The study by Bongiovanni et al. showed significant improvements in symptoms of diarrhea and flushing among patients with functioning NENs treated with 177Lu-DOTATATE. Of the 68 patients, 62 (91.1%) reported diarrhea and flushing as primary symptoms. After treatment, 88.1% experienced a syndromic response, substantially reducing these symptoms. Specifically, bowel movements were reduced by 30% or more over 12 weeks, while flushing episodes significantly decreased. These improvements in diarrhea and flushing contributed to an enhanced quality of life for the patients receiving 177Lu-DOTATATE [34].
Regarding the RCS, a recent study included 22 patients with a metastatic midgut NET, elevated urinary 5-HIAA acid excretion, and flushing and/or diarrhea despite treatment with SSA without documented disease progression. PRRT with 177Lu-DOTATATE with a primary aim to reduce symptoms. After PRRT, bowel movement frequency decreased more than 30% in 47% of patients, and flushing decreased more than 50% of daily flushing in 67% of patients. A significant decrease in urinary 5-HIAA was reported in 56% of patients [35].
Concerns have been raised regarding the potential worsening of symptoms that may occur in patients with carcinoid syndrome undergoing PRRT. The study by Rico et al. highlights that although carcinoid crises, including severe diarrhea and flushing, are rare during PRRT, high-risk patients—especially those with a history of carcinoid crisis, large tumor burdens, or liver metastases—are vulnerable. Prophylactic use of octreotide and corticosteroids, in most cases, reduced the severity of symptoms. Despite these measures, some patients still experienced symptom flares, underscoring the need for tailored pre- and post-PRRT management protocols. The findings suggest that identifying high-risk patients early and implementing standardized prophylactic interventions can significantly improve outcomes and reduce the incidence of severe carcinoid crises [36].
Chemotherapy is rarely applied in clinical practice because of its limited role in CS symptom control. Most data available are old and scarce, not descriptive of CS-specific outcomes, but, unfortunately, they are restricted to the biochemical response [5]. The reported 5-HIAA response rates after chemotherapy regimens, which include combinations of streptozotocin, cyclophosphamide, platinum derivatives, or 5-fluorouracil, are 31% on average across 111 patients (ranging from 0% to 71%). Clinical response data are limited to cisplatin (0%), cyclophosphamide combined with methotrexate (6.7%), and lomustine with 5-fluorouracil [18].
- b.
- Locoregional treatment: liver-directed therapies
Locoregional therapies play a significant role in the management of CS in patients with NET, especially for controlling larger or multifocal lesions in oligometastatic patients or for hormonal symptom relief, as international guidelines suggested [3,37]. Since most of all NET patients with CS present liver metastasis, liver-directed therapies are particularly effective in controlling this syndrome. Multiple liver-directed interventions have been assessed, including radiofrequency ablation (RFA), selective internal radiotherapy (SIRT), and hepatic arterial embolization (HAE) or chemotherapy (TACE). The size, number, and distribution of liver metastases are important factors affecting survival and choice of treatment strategies, often considered for CS patients with inoperable liver metastases [38].
Prospective clinical studies evaluating the symptomatic benefits of these locoregional techniques in patients with carcinoid syndrome are scarce.
The analysis of 479 patients from 25 studies showed that liver-directed interventions result in an 82% overall symptomatic response rate and a 61% reduction in serotonin-related biochemical markers, particularly 5-HIAA. This is significant since serotonin plays a key role in causing symptoms like diarrhea and flushing in carcinoid syndrome. The interventions primarily include methods that selectively reduce blood supply to liver tumors, such as embolization techniques, which block the blood flow and reduce the tumor’s ability to secrete hormones [18].
Embolization methods, including bland embolization, chemoembolization (which combines embolization with direct chemotherapy directly delivered to liver tumors), and radioembolization (using radioactive particles), were shown to provide high efficacy in controlling symptoms. These treatments were effective even in patients who had previously received SSAs, a common first-line therapy for managing hormone secretion. Despite the effectiveness, many studies were retrospective and lacked controls, raising concerns about potential bias.
Liver-directed therapies offer a crucial option for patients whose symptoms persist despite medical management. However, there is a clear need for prospective, high-quality trials to understand the long-term outcomes better and optimize treatment protocols [18].
One significant complication is post-embolisation syndrome, which occurs in approximately 40% of patients undergoing TAE or TACE [39]. This syndrome typically presents with symptoms such as right-sided abdominal pain, nausea, vomiting, fever, leucocytosis, and transient liver function abnormalities. While these symptoms are usually temporary, they can cause considerable discomfort.
More serious complications are less common but noteworthy. These include liver abscesses, gallbladder necrosis, intestinal ischemia, and liver insufficiency. A high incidence of biliary injury has been reported in phase 2 studies of drug-eluting bead TACE, with complications such as biloma and hepatic abscess being observed. Certain conditions, such as portal vein thrombosis, biliary stasis, and poor liver function, are considered contraindications for TAE and TACE.
Selective embolization is always advisable to reduce ischemic complications.
Radioembolization, also known as SIRT, has gained traction over the past decade due to its promising results in tumor reduction and manageable toxicity profiles. The procedure involves the intra-arterial delivery of radioactive beads to deliver high doses of radiation directly to liver tumors. Recent studies indicate that radioembolization yields objective response rates ranging from 36% to 54%, with disease control rates between 69% and 94% [40]. Factors such as tumor grading and extrahepatic disease can influence the treatment’s effectiveness. Data from various studies indicate that the incidence of serious complications is relatively low. For instance, radioembolization-induced liver disease occurs in only about 0.6% to 2% of patients, showcasing its safety in terms of liver function preservation [40]. Furthermore, the overall complication rates associated with this procedure are generally reported to be manageable, with most patients experiencing only mild to moderate side effects. Serious complications such as radiation pneumonitis or gastrointestinal ulcers due to extrahepatic deposition of radioactivity are rare but can occur. The risk of lung shunting, where radioactive particles inadvertently travel to the lungs, is a critical concern; however, thorough pre-treatment imaging and planning can mitigate this risk effectively.
- c.
- Surgery
Debulking surgery for liver disease should be considered a recommendable palliative option in patients with symptoms related to carcinoid syndrome refractory to medical therapy or in whom there is evidence of clinical or radiologic progression disease, as guidelines suggested [3]. When liver metastases are potentially resectable, surgery can offer long-term disease-free survival and relief from CS symptoms. However, patients with CS often have extensive liver involvement, making complete surgical resection rarely feasible [26].
For a very select group of young patients (less than 1%) with liver-only metastases, stable, and a resected primary tumor, liver transplantation could be considered, as studies report a 5-year recurrence-free survival rate of 20–30% [41].
A recent study evaluated the effectiveness of surgical cytoreduction in patients with small intestinal NETs that have metastasized to the liver and peritoneum [42]. Conducted over a 20-year period, the study analyzed 261 patients who underwent cytoreductive surgery, comparing outcomes between those with isolated liver metastases and those with both liver and peritoneal metastases. The findings reveal that complete cytoreduction was achieved in 78% of patients with isolated liver metastases compared to 56% of those with both types of metastases. Despite these differences, median overall survival after complete cytoreduction was similar for both groups, approximately 11.5 years for isolated liver metastases and 11.2 years for those with both liver and peritoneal metastases. Notably, the study found that 97% of patients experienced relief from carcinoid syndrome symptoms post-surgery. This data highlights that aggressive surgical approaches can lead to favorable outcomes even in patients with peritoneal metastases, suggesting that the presence of such metastases should not automatically exclude patients from surgical intervention [42].
The study by Chan et al. examined outcomes of cytoreductive surgery for 55 patients with low-grade NETs and extrahepatic metastases. The procedure resulted in significant hormonal and symptomatic control, with 70% of patients achieving hormonal response and 75% experiencing symptomatic improvement. Postoperative morbidity and mortality were low at 18% and 3.6%, respectively. Long-term outcomes were favorable, with a 5-year progression-free survival of 51% and a 5-year overall survival of 77%. The findings suggest cytoreductive surgery can be safely performed in patients with extrahepatic NET metastases, providing effective symptom control and favorable long-term outcomes [43].
6. Complications
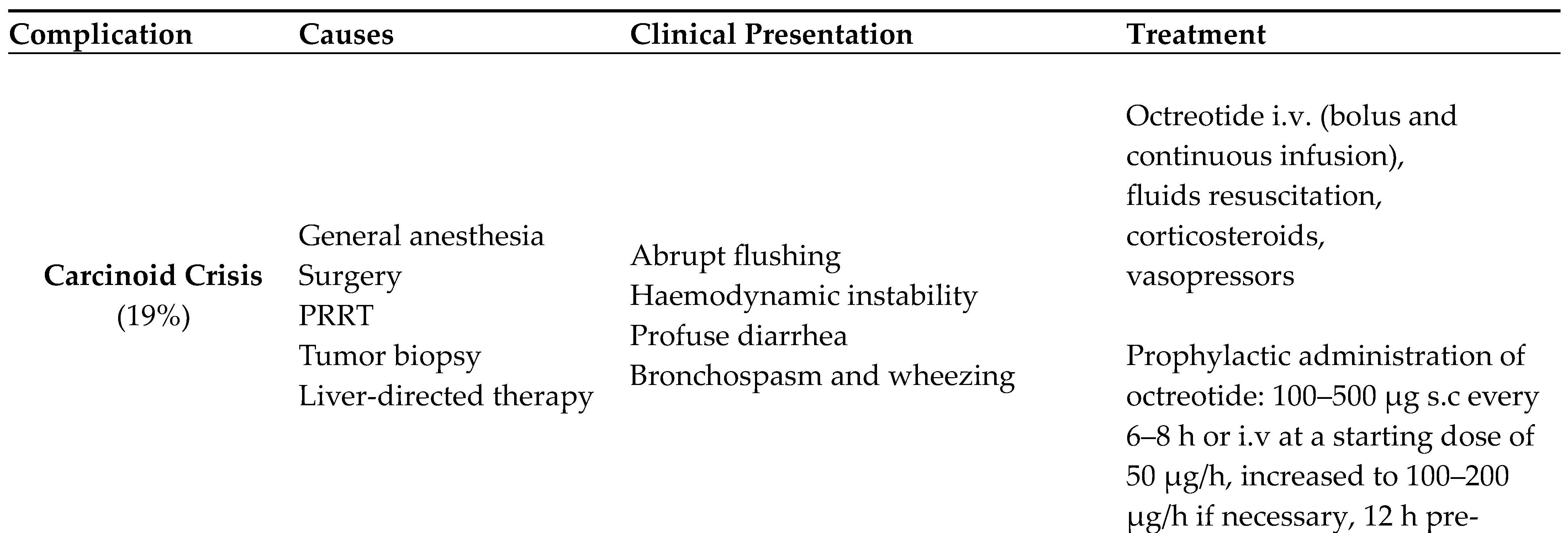
Complications of CS (Table 1) arise primarily through direct pathways from the prolonged and excessive release of hormonal amines and peptides, mostly serotonin, into the circulation, affecting multiple organ systems and also through indirect pathways due to surgical resection or drug administration.
- Carcinoid Crisis
The most serious complication of CS is Carcinoid Crisis (CC), a potentially life-threatening condition in which the sudden release of high levels of vasoactive hormones can result in hemodynamic instability because of distributive shock [5].
The symptoms can be dramatic, with the rapid onset of abrupt flushing, severe shifts in blood pressure, profuse diarrhea, and distressing bronchospasm with wheezing.
The exact incidence of CC is unknown, mainly because a standard definition has not been established, so the reported rates vary widely between groups [44]. The diagnosis is predominantly clinical, depending on an unexpected onset of the aforementioned symptoms in individuals with confirmed or suspected NET.
Although the pathophysiology of CC is hypothesized to be attributable to a sudden, massive release of vasoactive hormones, a prospective study conducted by Condron et al. didn’t find a statistically significant increase of serotonin, histamine, kallikrein, or bradykinin during the crises, suggesting that CC could be an entirely separate pathophysiologic entity from CS, rather than the extreme end of a spectrum of CS [45].
Common triggers of CC include general anesthesia as well as procedures that result in tumor manipulation, like surgery, PRRT, tumor biopsy, or liver-directed therapy [46].
A systematic review and meta-analysis by Xu A. et al. conducted on surgical patients with midgut NETs and/or neuroendocrine liver metastasis found that CC is relatively common, occurring in 1 in 5 patients (incidence = 19%) in the pooled data [47]. In that review, the risk of CC increased in patients with liver metastases and decreased in males. Interestingly, other characteristics traditionally considered risk factors, including CS and carcinoid heart disease were not significantly associated with an increased risk of CC.
Given the severity and difficulty of managing this condition, which can require an intensive care setting, preventing CC rather than treating it once it is established is important.
International guidelines suggest administering SSA in patients with functional NETs as a peri-operative preparation to prevent CC [5,48]. Specifically, the latest ENETS guidelines recommend prophylactic administration of octreotide with a precise dose scheme: 100–500 μg subcutaneously every 6–8 h or infused at a starting dose of 50 μg/h, increased to 100–
200 μg/h if necessary, 12 h pre-operatively and before anesthesia, continuously throughout the procedure, and post-operatively until the patient is clinically stable [5]. However, CC is not entirely preventable, so prompt recognition is crucial since it can result in serious postoperative complications and, finally, death. Once established, an aggressive treatment, including intravenous fluids, corticosteroids, and vasopressors, is needed [5].
- b.
- Mesenteric Fibrosis
Mesenteric Fibrosis (MF) is a significant and common complication in patients with CS, occurring because of prolonged release of serotonin and other bioactive substances.
Serotonin has been classically considered the main mediator of MF since it exerts both mitogenic and fibrogenic effects in fibroblasts, smooth muscle cells, and endothelial cells.
Apart from serotonin, many other mediators have been studied as potentially responsible for MS, such as Transforming Growth Factor-α and -β (TGF-α, TGF-β), Connective Tissue Growth Factor (CTGF), Platelet-Derived Growth Factor (PDGF), Insulin-Like Growth Factor 1 (IGF-1) and Epidermal Growth Factor (EGF) [49]. At least some signs of MF occur in approximately 50% of CS patients, resulting from a fibrotic and desmoplastic reaction around metastatic mesenteric lymph nodes [50]. MF causes contraction and tightening of the adjacent bowel loop, potentially leading to acute complications such as intestinal obstruction, intussusception, and/or intestinal ischemia because of impaired blood supply to the intestines. Nevertheless, MF can cause chronic conditions such as postprandial abdominal pain, thus influencing patients’ food intake and resulting in malnutrition and weight loss in the long term. Another rare complication of MF is diffuse retroperitoneal fibrosis, which happens when tumor secretory products drain directly into the systemic circulation through retroperitoneal lymphatic spread. This may lead to urinary system obstruction and renal failure late in the disease clinical course [51].
A retrospective cohort study found that advanced MF associated with intestinal ischemia is a poor prognostic factor for OS [52].
MF can be radiologically identified by calcified mesenteric mass, fibrotic radiating strands showing a stellate pattern, and adjacent bowel-wall thickening [17]. A retrospective study by Pantograg-Brown L. et al. proposed a classification for the radiological severity of MS based on the number and thickness of radiating strands on CT images; however, this classification showed no correlation with any kind of clinical aspects such as symptoms or prognosis [53].
The management of MF is mainly surgical and aimed at providing symptomatic relief. However, locoregional surgical resection has to be carefully considered since it is technically challenging and carries risks due to vascular involvement and the extensive nature of fibrosis.
- c.
- Malnutrition
Malnutrition is a common condition in oncological diseases and is associated with poorer response to treatment, increased rates of complications, and decreased quality of life. Maasberg et al. demonstrated malnutrition’s existence and potential prevalence in people with a GEP NET, assessing that malnutrition was diagnosed in 25% of patients. Patients with Grade 3 disease had a significantly higher prevalence of malnutrition than patients with Grade 1 or 2 disease (57.9 and 22.1%, respectively, p = 0.002). Lastly, it is reported that malnourished patients had significantly shorter overall survival (19.94 vs. 31.17 months, p < 0.001) and significantly longer length of stay than well-nourished patients (8.8 vs. 4.0 days, respectively, p < 0.001) [54].
Patients with GEP NETs, particularly those associated with CS, may have a nutrition and metabolic asset altered due to multifactorial causes: excessive hormones and peptide release, signs and symptoms related to the eventual progression of the disease, vitamin deficiency, and treatments administered. However, there is limited information and clinical awareness about nutrition issues in these patients.
Chronic diarrhea is one of the burdensome signs that characterized CS clinical presentation and affected NET patients’ quality of life, especially in those who experienced ≥ 4 bowel movements per day [55]. It could be mainly caused by tumoral excessive serotonin release and surgical intestinal resection, which could be responsible for reduced absorption of bile acid and cobalamin (B12 vitamin) and reduced bowel motility. Chronic diarrhea can lead to loss of appetite, electrolyte imbalances, dehydration, and short gut syndrome or bacterial overgrowth in case of surgical intestinal resection [56]. Antidiarrheal agents, such as loperamide, may be useful [5].
As mentioned above, the main therapeutic approach in CS consists of SSA administration. Considering the inhibitory effect of SSAs on pancreatic exocrine function, long-term SSA administration could lead to reduced secretion of digestive enzymes, causing symptoms like steatorrhea, weight loss, and malabsorption of lipids and liposoluble vitamins (A, D, E, and K). This clinical and biochemical presentation describes a condition of exocrine pancreatic insufficiency (EPI) with a prevalence rate of approximately 20–24% in patients receiving long-term SSA treatment [9,57]. The dosage of fecal elastase (FE-1 < 200 µg/g, diagnostic cut-off) represents one of the indirect tests, non-invasive, with high sensitivity and specificity for the detection of EPI [58]. Therapeutic management of EPI includes treatment with pancreatic enzyme replacement therapy (PERT) at the minimum dosage of at least 40,000 USP units of lipase during each meal. Indicators of successful treatment with PERT include reduced steatorrhea and related gastrointestinal symptoms, weight gain, increased muscle mass and function, as well as improved levels of fat-soluble vitamins [59]. Naturally, primitive pancreatic resection is another cause that can result in EPI. It depends on the type and the extension of resection; indeed, the post-operative EPI incidence is 56–98% in pancreaticoduodenectomy and 12–80% following distal and central pancreatectomy [60].
Moreover, another characteristic risk factor in NET patients with CS may be supported by malnutrition due to elevated serotonin levels or its precursor (5-hydroxytryptophan). Under normal conditions, only a small portion of tryptophan metabolism is dedicated to serotonin production, with the majority following a pathway that partially converts it to niacin (B3 vitamin). However, the increased shift of tryptophan toward serotonin synthesis in CS patients may lead to varying degrees of niacin deficiency [61]. The prevalence of biochemical or “sub-clinical niacin deficiency” may be as high as 30–45% [56]. The most reliable and sensitive test to define niacin status is urinary excretion of N1-methyl nicotinamide and its derivative N1-methyl-2-pyridone-5-carboxyamide, as Bouma et al. utilized in a recent study to assess the niacin status before and after supplementation in patients with serotonin-producing NET [61,62]. Knowing eventual niacin deficiency has a relevant clinical role in the management of CS patients because of the risk of developing pellagra. The clinical manifestations of pellagra are scaly skin, glossitis, stomatitis, and confusion. Violent behavior and language deficits are also associated with niacin deficiency. In isolated cases, this condition could lead to death [4].
For this reason, searching for conditions of sub-clinical niacin deficiency and contributing to niacin supplementation is a crucial clinical aim. Current evidence suggests that it would be appropriate to recommend proactive niacin supplementation of at least 40 mg per day for patients with CS and at least 100 mg per day (200–250 mg) for those with confirmed niacin deficiency [5,56].
Furthermore, some studies focused on the role of sarcopenia in NET patients as another factor in the malnutrition overview. A recent retrospective study included 30 patients with advanced gastrointestinal well-differentiated G1 and G2 NET and, through CT scan evaluation with calculation of skeletal muscle index, it was found that 66% of patients both at the time of diagnosis and follow-up presented a sarcopenia status with statistical significance in the group of patients with carcinoid syndrome (p = 0.0178), EPI (p = 0.0018), and weight loss (p = 0.0001) [63].
Therefore, in light of the above, it is crucial to increase clinical awareness about the nutritional status of NET patients, particularly associated with CS. Physicians should evaluate clinical signs (e.g., bowel movements frequency, weight, skin evaluation), nutritional and metabolic assets (liposoluble vitamins, niacin, B12 vitamin, anemia, blood glucose, cholesterol, albumin), exocrine pancreatic function (fecal elastase) and suggest nutritional counseling to the patient.
- d.
- Carcinoid Heart Disease
Carcinoid heart disease (CHD) is a complex cardiac complication that mainly involves the right-sided heart valves, eventually leading to right heart failure (RHF).
CHD is present in approximately 20%–50% of CS patients and significantly affects prognosis, with reduced overall survival at three years of 31% in patients with CHD, compared to 69% in patients without CHD [5,64].
The right heart is mainly affected due to its direct exposure to the bloodstream from the systemic venous circulation and to the hormones and bioactive substances produced by the neuroendocrine tumor.
CHD is characterized by plaque-like deposition of fibrous tissue on valvular cusps leaflets, papillary muscles, chordae, ventricular walls, and occasionally on the intima of pulmonary arteries [65]. Fibrosis causes valve thickening, restricting valve mobility and resulting in regurgitation, stenosis, or both. The tricuspid valve is typically most affected, with tricuspid regurgitation being a common consequence, while the pulmonary valve may also exhibit regurgitation or stenosis.
Left heart valves are usually spared because the vasoactive substances responsible for CHD are enzymatically inactivated in the lung vasculature, preventing transport to the left heart. However, the left-sided disease can occur in <10% of patients in the presence of a patent foramen ovale (which causes a right-to-left atrial shunt), in the presence of a functioning lung NET, or the presence of high serotonin levels due to poorly controlled carcinoid syndrome overwhelming the hepatic and pulmonary degradative capacity [66].
All patients with CS should be questioned and examined for symptoms and physical signs of CHD, which include fatigue, dyspnoea, peripheral edema, and/or ascites.
A recent systematic review and meta-analysis, including 36 articles, showed that N-terminal pro-brain natriuretic peptide (NTproBNP) and 5-HIAA levels were higher in patients with CHD than those without CHD [67]. Therefore, ENETS guidelines recommend the evaluation of NT-proBNP as a valid screening tool for identifying patients with high suspicion of CHD in the context of CS at baseline and follow-up [5].
Moreover, since transthoracic echocardiography (TTE) is the key investigation for CHD diagnosis and monitoring, the same guidelines recommend performing a TTE every 6–12 months in any patient with CS and/or high 5-HIAA level with CHD symptoms and/or NT-proBNP > 260 pg/mL. TTE should be ideally undertaken by an experienced professional in CHD.
Instead, the North American Neuroendocrine Tumor Society recommends annual TTE for patients with a urinary 5-HIAA level > five times the upper limit of normal [37].
Factors associated with the development and progression of CHD are challenging to identify, as the main publications have analyzed them with varying definitions. Several flushing episodes per day, 5-HIAA urinary level, and high liver burden disease have been postulated as possible factors [68].
No treatment has been reported to induce regression of the fibrous-plaque deposits, and CHD-related valve disease is currently considered irreversible. Treatment of CHD is complex and relies on control of CS and surgical valve replacement in cases of severe CHD. A multidisciplinary approach between NET oncologists, cardiologists, cardiac surgeons, and anaesthesiologists is needed since the timing of surgery is the most crucial point of CHD management and has to be decided on a case-by-case basis. Surgical intervention should be considered early, before a disease progression to a point at which surgery would be too high risk and with at least 12 months of anticipated post-operative survival from their NET disease [5].
7. Conclusion
At the heart of effective management of CS lies the indispensable role of a multidisciplinary team [69]. This collaborative approach is not merely beneficial but essential in addressing the multifaceted nature of carcinoid syndrome. The team should ideally include Gastroenterologists, Endocrinologists, Radiologists, Oncologists, Nuclear Medicine Physicians, Surgeons, Cardiologists, and Nutritionists. Each specialist brings unique expertise, allowing for a holistic approach to patient care. This interdisciplinary collaboration is vital in addressing all pathological aspects of the condition, formulating the most appropriate therapeutic strategy tailored to each patient, and implementing early interventions to improve overall quality of life.
The synergy created by this multidisciplinary approach ensures that patients receive comprehensive care that addresses the primary symptoms, potential complications, and comorbidities. By leveraging various specialists’ collective knowledge and skills, healthcare providers can offer more nuanced, personalized treatment plans that significantly enhance clinical outcomes and the overall well-being of CS patients.
Author Contributions
Conceptualization, M.M. and F.P.; methodology, F.P.; writing—original draft preparation, M.M. and E.R; writing—review and editing: all authors; visualization, M.M.; supervision, F.P.; project administration, F.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Clement D, Ramage J et al. Update on Pathophysiology, Treatment, and Complications of Carcinoid Syndrome. J Oncol. 2020, 2020, 8341426. [CrossRef]
- Halperin DM, Shen C et al. Frequency of carcinoid syndrome at neuroendocrine tumour diagnosis: a population-based study. Lancet Oncol. 2017 Apr;18, 525–534.
- Pavel M, Öberg K et al. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020 Jul;31, 844–860. [CrossRef]
- Magi, L.; Rinzivillo, M.; Panzuto, F. What Gastroenterologists Should Know about Carcinoid Syndrome. Gastroenterol. Insights 2022, 13, 127-138. [CrossRef]
- Grozinsky-Glasberg S, Davar J et al. European Neuroendocrine Tumor Society (ENETS) 2022 Guidance Paper for Carcinoid Syndrome and Carcinoid Heart Disease. J Neuroendocrinol. 2022 Jul;34, e13146. [CrossRef]
- Beaumont JL, Cella D et al. Comparison of health-related quality of life in patients with neuroendocrine tumors with quality of life in the general US population. Pancreas. 2012 Apr;41, 461-6. [CrossRef]
- Condron ME, Pommier SJ et al. Pommier RF. Continuous infusion of octreotide combined with perioperative octreotide bolus does not prevent intraoperative carcinoid crisis. Surgery. 2016 Jan;159, 358-65. [CrossRef]
- Arasaradnam RP, Brown S et al. Guidelines for the investigation of chronic diarrhoea in adults: British Society of Gastroenterology, 3rd edition. Gut. 2018 Aug;67, 1380-1399. [CrossRef]
- Marasco M, Dell’Unto E et al. Gastrointestinal side effects of somatostatin analogs in neuroendocrine tumors: a focused review. J Gastroenterol Hepatol. 2024 May 23. [CrossRef]
- Ruggeri RM, Altieri B et al. Gender-related differences in patients with carcinoid syndrome: new insights from an Italian multicenter cohort study. J Endocrinol Invest. 2024 Apr;47, 959-971. [CrossRef]
- Ruggeri RM, Altieri B et al. Sex differences in carcinoid syndrome: A gap to be closed. Rev Endocr Metab Disord. 2022 Jun;23, 659-669. [CrossRef]
- Ito T, Lee L et al. Carcinoid-syndrome: recent advances, current status and controversies. Curr Opin Endocrinol Diabetes Obes. 2018 Feb;25, 22-35.
- Fanciulli G, Ruggeri RM et al. Serotonin pathway in carcinoid syndrome: Clinical, diagnostic, prognostic and therapeutic implications. Rev Endocr Metab Disord. 2020 Dec;21, 599-612.
- Adaway JE, Dobson R et al. Serum and plasma 5-hydroxyindoleacetic acid as an alternative to 24-h urine 5-hydroxyindoleacetic acid measurement. Ann Clin Biochem. 2016 Sep;53(Pt 5):554-60.
- Ewang-Emukowhate M, Subramaniam K et al. Plasma or serum 5-hydroxyindoleacetic acid can be used interchangeably in patients with neuroendocrine tumours. Scand J Clin Lab Invest. 2023 Dec;83, 576-581. [CrossRef]
- Koumarianou A, Daskalakis K et al. Efficacy, safety and unmet needs of evolving medical treatments for carcinoid syndrome. J Neuroendocrinol. 2022 Jul;34, e13174. [CrossRef]
- Sundin A, Arnold R et al. ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: Radiological, Nuclear Medicine & Hybrid Imaging. Neuroendocrinology. 2017;105, 212-244.
- Hofland J, Herrera-Martínez AD et al. Management of carcinoid syndrome: a systematic review and meta-analysis. Endocr Relat Cancer. 2019 Mar;26, R145-R156.
- Bousquet C, Lasfargues C et al. Clinical review: Current scientific rationale for the use of somatostatin analogs and mTOR inhibitors in neuroendocrine tumor therapy. J Clin Endocrinol Metab. 2012 Mar;97, 727-37.
- Rinke A, Müller HH et al. Placebo-Controlled, Double-Blind, Prospective, Randomized Study on the Effect of Octreotide LAR in the Control of Tumor Growth in Patients with Metastatic Neuroendocrine Midgut Tumors: A Report from the PROMID Study Group. Journal of Clinical Oncology 2009, 27 (28), 4656–4663. [CrossRef]
- Caplin ME, Pavel M et al. CLARINET Investigators. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N Engl J Med. 2014 Jul 17;371, 224-33.
- Strosberg JR, Benson AB et al. Clinical benefits of above-standard dose of octreotide LAR in patients with neuroendocrine tumors for control of carcinoid syndrome symptoms: a multicenter retrospective chart review study. Oncologist. 2014 Sep;19, 930-6.
- Ferolla P, Faggiano A et al. Shortened interval of long-acting octreotide administration is effective in patients with well-differentiated neuroendocrine carcinomas in progression on standard doses. J Endocrinol Invest. 2012 Mar;35, 326-31. [CrossRef]
- Wolin EM, Jarzab B et al. Phase III study of pasireotide long-acting release in patients with metastatic neuroendocrine tumors and carcinoid symptoms refractory to available somatostatin analogues. Drug Des Devel Ther. 2015 Sep 3;9:5075-86. [CrossRef]
- Wolin EM, Benson Iii AB. Systemic Treatment Options for Carcinoid Syndrome: A Systematic Review. Oncology. 2019;96, 273-289.
- Oleinikov K, Avniel-Polak S et al. Carcinoid Syndrome: Updates and Review of Current Therapy. Curr Treat Options Oncol. 2019 Jul 9;20, 70.
- Kulke MH, Hörsch D et al. Telotristat Ethyl, a Tryptophan Hydroxylase Inhibitor for the Treatment of Carcinoid Syndrome. J Clin Oncol. 2017 Jan;35, 14-23.
- Pavel M, Gross DJ et al. Telotristat ethyl in carcinoid syndrome: safety and efficacy in the TELECAST phase 3 trial. Endocr Relat Cancer. 2018 Mar;25, 309-322. [CrossRef]
- Hörsch D, Anthony L et al. Long-Term Treatment with Telotristat Ethyl in Patients with Carcinoid Syndrome Symptoms: Results from the TELEPATH Study. Neuroendocrinology. 2022;112, 298-310. [CrossRef]
- Pavel ME, Hainsworth JD et al. RADIANT-2 Study Group. Everolimus plus octreotide long-acting repeatable for the treatment of advanced neuroendocrine tumours associated with carcinoid syndrome (RADIANT-2): a randomised, placebo-controlled, phase 3 study. Lancet. 2011 Dec 10;378, 2005-2012.
- Capdevila J, Díez Miranda I et al. Control of carcinoid syndrome with everolimus. Ann Oncol. 2011 Jan;22, 237-239.
- Strosberg J, El-Haddad G et al. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N Engl J Med. 2017 Jan 12;376, 125-135. [CrossRef]
- Strosberg J, Wolin E et al. Health-Related Quality of Life in Patients With Progressive Midgut Neuroendocrine Tumors Treated With 177Lu-Dotatate in the Phase III NETTER-1 Trial. J Clin Oncol. 2018 Sep 1;36, 2578-2584. [CrossRef]
- Bongiovanni A, Nicolini S et al. 177Lu-DOTATATE Efficacy and Safety in Functioning Neuroendocrine Tumors: A Joint Analysis of Phase II Prospective Clinical Trials. Cancers (Basel). 2022 Dec 7;14, 6022.
- Zandee WT, Brabander T et al. Peptide Receptor Radionuclide Therapy With 177Lu-DOTATATE for Symptomatic Control of Refractory Carcinoid Syndrome. J Clin Endocrinol Metab. 2021 Aug 18;106, e3665-e3672.
- Tapia Rico G, Li M et al. Prevention and management of carcinoid crises in patients with high-risk neuroendocrine tumours undergoing peptide receptor radionuclide therapy (PRRT): Literature review and case series from two Australian tertiary medical institutions. Cancer Treat Rev. 2018 May;66:1-6.
- Strosberg JR, Halfdanarson TR et al. The North American Neuroendocrine Tumor Society Consensus Guidelines for Surveillance and Medical Management of Midgut Neuroendocrine Tumors. Pancreas. 2017 Jul;46, 707-714.
- Basuroy R, Srirajaskanthan R et al. Neuroendocrine Tumors. Gastroenterol Clin North Am. 2016 Sep;45, 487-507.
- Clift AK, Frilling A. Liver-Directed Therapies for Neuroendocrine Neoplasms. Curr Oncol Rep. 2021 Mar 15;23, 44. [CrossRef]
- Ramdhani K, Braat AJAT. The Evolving Role of Radioembolization in the Treatment of Neuroendocrine Liver Metastases. Cancers 2022 Jul 14;14, 3415. [CrossRef]
- Pavel M, Baudin E et al. ENETS Consensus Guidelines for the management of patients with liver and other distant metastases from neuroendocrine neoplasms of foregut, midgut, hindgut, and unknown primary. Neuroendocrinology. 2012;95, 157-76.
- Gudmundsdottir H, Fogliati A et al. Value of Surgical Cytoreduction in Patients with Small Intestinal Neuroendocrine Tumors Metastatic to the Liver and Peritoneum. Ann Surg Oncol. 2024 Aug;31, 5370-5376.
- Chan DL, Dixon M et al. Outcomes of Cytoreductive Surgery for Metastatic Low-Grade Neuroendocrine Tumors in the Setting of Extrahepatic Metastases. Ann Surg Oncol. 2018 Jun;25, 1768-1774.
- Maxwell JE, Naraev B et al. Shifting Paradigms in the Pathophysiology and Treatment of Carcinoid Crisis. Ann Surg Oncol. 2022 May;29, 3072-3084. [CrossRef]
- Condron ME, Jameson NE et al. A prospective study of the pathophysiology of carcinoid crisis. Surgery. 2019 Jan;165, 158-165. [CrossRef]
- Kwon DH, Paciorek A et al. Periprocedural Management of Patients Undergoing Liver Resection or Embolotherapy for Neuroendocrine Tumor Metastases. Pancreas. 2019 Apr;48, 496-503.
- Xu A, Suz P et al. Perioperative Carcinoid Crisis: A Systematic Review and Meta-Analysis. Cancers (Basel). 2022 Jun 16;14, 2966.
- Howe JR, Merchant NB et al. The North American Neuroendocrine Tumor Society Consensus Paper on the Surgical Management of Pancreatic Neuroendocrine Tumors. Pancreas. 2020 Jan;49, 1-33.
- Koumarianou A, Alexandraki KI et al. Pathogenesis and Clinical Management of Mesenteric Fibrosis in Small Intestinal Neuroendocine Neoplasms: A Systematic Review. J Clin Med. 2020 Jun 8;9, 1777.
- Druce MR, Bharwani N et al. Intra-abdominal fibrosis in a recent cohort of patients with neuroendocrine (‘carcinoid’) tumours of the small bowel. QJM. 2010 Mar;103, 177-85. [CrossRef]
- Druce M, Rockall A et al. Fibrosis and carcinoid syndrome: from causation to future therapy. Nat Rev Endocrinol. 2009 May;5, 276-83. [CrossRef]
- Daskalakis K, Karakatsanis A et al. Clinical signs of fibrosis in small intestinal neuroendocrine tumours. Br J Surg. 2017 Jan;104, 69-75. [CrossRef]
- Pantongrag-Brown L, Buetow PC et al. Calcification and fibrosis in mesenteric carcinoid tumor: CT findings and pathologic correlation. AJR Am J Roentgenol. 1995 Feb;164, 387-91.
- Maasberg S, Knappe-Drzikova B et al. Malnutrition Predicts Clinical Outcome in Patients with Neuroendocrine Neoplasia. Neuroendocrinology. 2017;104, 11-25. [CrossRef]
- Pearman TP, Beaumont JL et al. Health-related quality of life in patients with neuroendocrine tumors: an investigation of treatment type, disease status, and symptom burden. Support Care Cancer. 2016 Sep;24, 3695-703. [CrossRef]
- Laing E, Kiss N et al. Nutritional Complications and the Management of Patients with Gastroenteropancreatic Neuroendocrine Tumors. Neuroendocrinology. 2020;110, 430-442.
- Rinzivillo M, De Felice I et al. Occurrence of exocrine pancreatic insufficiency in patients with advanced neuroendocrine tumors treated with somatostatin analogs. Pancreatology. 2020 Jul;20, 875-879.
- Vanga RR, Tansel A et al. Diagnostic Performance of Measurement of Fecal Elastase-1 in Detection of Exocrine Pancreatic Insufficiency: Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2018 Aug;16, 1220-1228.e4.
- Whitcomb DC, Buchner AM et al. AGA Clinical Practice Update on the Epidemiology, Evaluation, and Management of Exocrine Pancreatic Insufficiency: Expert Review. Gastroenterology. 2023 Nov;165, 1292-1301. [CrossRef]
- Phillips ME. Pancreatic exocrine insufficiency following pancreatic resection. Pancreatology. 2015 Sep-Oct;15, 449-455. [CrossRef]
- Shah GM, Shah RG et al. Biochemical assessment of niacin deficiency among carcinoid cancer patients. Am J Gastroenterol. 2005 Oct;100, 2307-14.
- Bouma G, van Faassen M et al. Niacin (Vitamin B3) Supplementation in Patients with Serotonin-Producing Neuroendocrine Tumor. Neuroendocrinology. 2016;103, 489-94.
- Romano E, Polici M et al. Sarcopenia in Patients with Advanced Gastrointestinal Well-Differentiated Neuroendocrine Tumors. Nutrients. 2024 Jul 11;16, 2224.
- Davar J, Connolly HM et al. Diagnosing and Managing Carcinoid Heart Disease in Patients With Neuroendocrine Tumors: An Expert Statement. J Am Coll Cardiol. 2017 Mar 14;69, 1288-1304.
- Jin C, Sharma AN et al. Carcinoid Heart Disease: Pathophysiology, Pathology, Clinical Manifestations, and Management. Cardiology. 2021;146, 65-73.
- Connolly HM, Schaff HV et al. Surgical management of left-sided carcinoid heart disease. Circulation. 2001 Sep 18;104(12 Suppl 1):I36-40.
- Namkoong J, Andraweera PH et al. A systematic review and meta-analysis of the diagnosis and surgical management of carcinoid heart disease. Front Cardiovasc Med. 2024 Mar 20;11:1353612. [CrossRef]
- Delhomme C, Walter T et al. Carcinoid heart disease in patients with midgut neuroendocrine tumours. J Neuroendocrinol. 2023 Apr;35, e13262. [CrossRef]
- Magi L, Mazzuca F et al. Multidisciplinary Management of Neuroendocrine Neoplasia: A Real-World Experience from a Referral Center. J Clin Med. 2019 Jun 25;8, 910. [CrossRef]
Figure 1.
Diagnostic and therapeutic management of carcinoid syndrome.
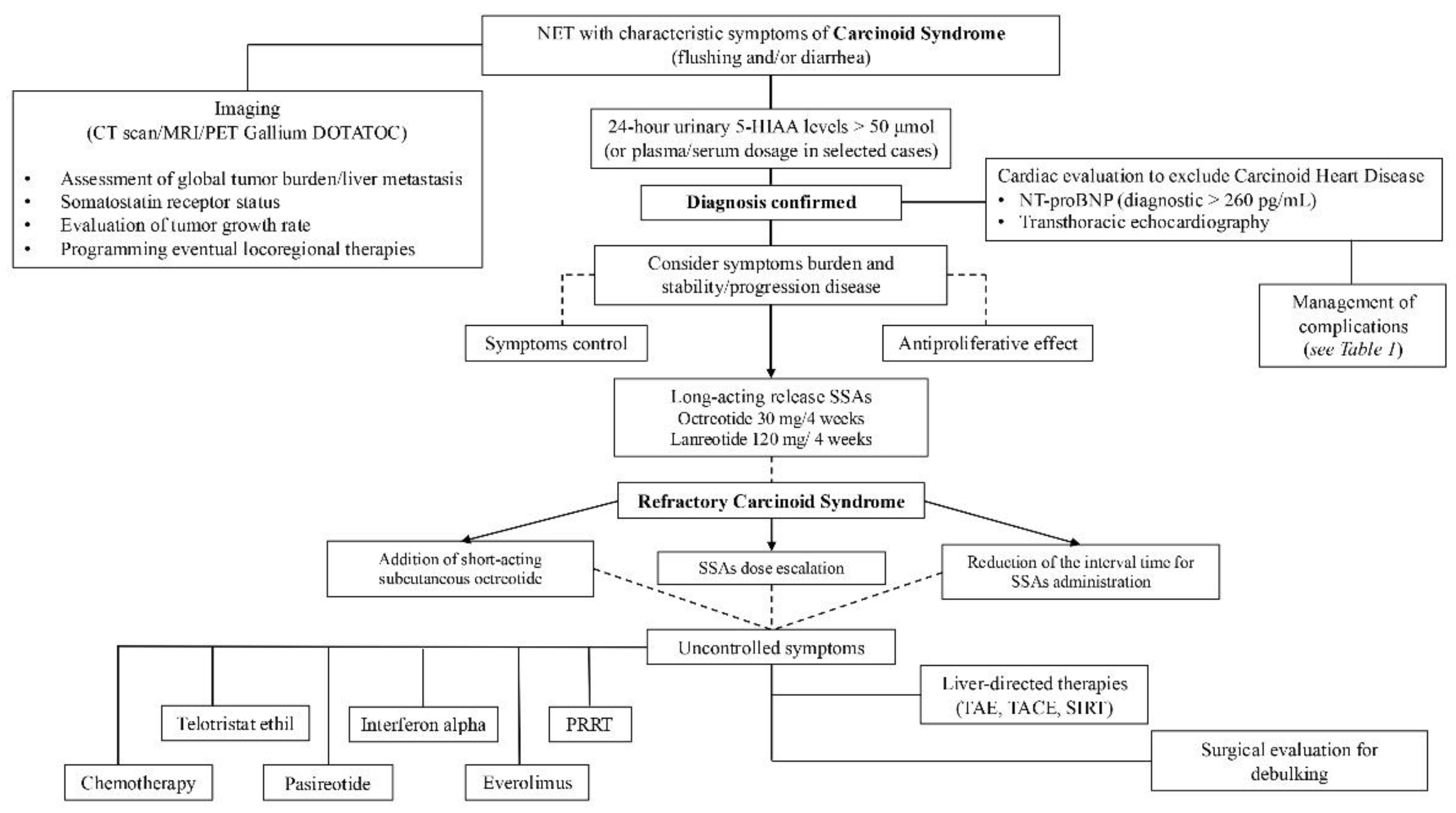

Table 1.
Complications management in patients with carcinoid syndrome.

PRRT: peptide Receptor Radionuclide Therapy, EPI: exocrine pancreatic insufficiency, PERT: pancreatic enzyme replacement therapy, TTE: transthoracic echocardiography.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



