
Submitted:
03 October 2024
Posted:
04 October 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: Short after the detection of the COVID virus in January 2020 the US Government introduced and enforced a series of restrictions to protect the elderly from a “deadly virus” and the “pandemic of the century”. Persons who disagreed were silenced and punished. Objective: In the 15th month of COVID epidemic (April 2021), we have access to sufficient statistical data and methods to better understand the nature, origin of the COVID pandemic. It is now possible to reliably evaluate the effectiveness of the restrictions and the human factors / driving forces behind this drastic limitations of our natural freedom in this country. Methods: Publicly available epidemiological and population parameters were collected and analyzed using the ‘political score’ and ‘restriction ranking’ of 50 states and evaluated by simple and usual statistical methods, mainly correlation analyses. Results: This study revealed, that 1) restrictions reduced the number of viral infections, but 2) they totally failed to reduce the number of supposedly COVID related deaths, 3) they increased (SIC!) the mortality of coronavirus. The grade of restrictions were/are strongly associated to the 4) left/right political ratio of the States, there States with more democrat citizens practiced more restrictions. It was found that race, religion and Medicare spending have significant influence on politic as well as on the grade of restriction orders. Factors moving States toward the political left and harder COVID restrictions have 5) larger ‘non-white’ population, 6) larger number of ‘non-protestant’ believers, 7) larger Jewish population, and 8) more generous Medicare spending. It was not possible to see any influence of the size of the 9) senior (65+) population [i.e. those who are allegedly the most vulnerable and are mostly in need of protective restrictions] neither on the States politic nor on the restrictions Conclusions: The conclusion is that COVID restrictions are primarily politically motivated, they are ineffective to reduce COVID related mortality and they provide no extra health benefit for the so called “vulnerable” minority (elderly).
Keywords:
COVID-19
; pandemic
; political
; mortality
; age
; aging
; co-morbidity
; underlying cause of death
; UCOD
; USA
; States
; restrictions
; political score
; restriction ranking
; religion
; ethnicity
Summary
Today, in the 15th month of COVID epidemic, we have now access to sufficient statistical data and methods to better understand the nature, origin and driving forces behind this pestilence. Introduction of ‘political score’ and ‘restriction ranking’ of 50 states and comparing the COVID data and the result of restrictions under different circumstances are very valuable sources of reliable information to see through the massive fog created by the occasionally dishonest media, sometimes fake scientists and the usually ignorant politicians.
This study revealed, that 1) restrictions reduced the number of viral infections, but 2) they totally failed to reduce the number of supposedly COVID related deaths, 3) they increased (SIC!) the mortality of coronavirus. The grade of restrictions were/are strongly associated to the 4) left/right political ratio of the States, there States with more democrat citizens practiced more restrictions. It was found that race, religion and Medicare spending have significant influence on politic as well as on the grade of restriction orders. Factors moving States toward the political left and harder COVID restrictions have 5) larger ‘non-white’ population, 6) larger number of ‘non-protestant’ believers, 7) larger Jewish population, and 8) more generous Medicare spending. It was not possible to see any influence of the size of the 9) senior (65+) population [i.e., those who are allegedly the most vulnerable and are mostly in need of protective restrictions] neither on the States politic nor on the restrictions.
The conclusion is that COVID restrictions are primarily politically motivated, they are ineffective to reduce COVID related mortality and they provide no extra health benefit for the so called “vulnerable” minority.
Methods
COVID statistical data was collected from public sources, like Center for Disease Control, CDC [1] and Worldometer [2].
The Political Score of the States (D/R) is the ratio of the proportion of citizens who self-identified as democrats or lean toward democratic party (D) divided by the proportion of citizens who self-identified as republican or lean toward republican party (R) in a given State [3]. The lowest Score (0.4) indicates a State with the lowest number of democrat oriented (D) or the highest number of republican oriented (R) citizens. The highest D/R score (max. 2.07) is obtained for a state with the highest number of D-oriented or the lowest number of R-oriented citizens. This tool turned out to be very useful to detect socio-political factors involved in the COVID syndemic [4,5].
The COVID Restriction Score of the States were adopted from a recent publication [6]. It ranks the states from 1-50, there 1 is the lowest number of restrictions and 50 is the highest number of restrictions applied by the States.
The results were evaluated by standard statistical methods.
Results
Left-oriented States and higher number of restrictions are associated with lower number of COVID cases (i.e., persons positive with viral tests). This is well in line with the purpose of the restrictions and might be interpreted as supporting argument for the democrat approach to the epidemic. (FIG. 1.)
The statistical results confirm the original observation by other investigators, only for some weeks ago [7] that COVID restrictions do NOT prevent statistically detectable number of deaths. (FIG. 2).
Reduced number of test positive cases and unchanged number of related deaths results in increase of mortality. (FIG. 3). This result doesn’t make any sense except if we assume, that the determination that COVID was the Underlying Cause of Death (UCOD) was not exclusively based on positive laboratory test (clinical evidence) but it was still diagnosed in the absence of test-confirmation – as it was done at the beginning of the epidemic for one year ago. The logical interpretation of the disappointing stagnation of COVID deaths may be that the strongly criticized “hearsay based diagnoses of COVID deaths” [8] is still in use in the restrictive/democrat States.
The determination of the UCOD is based on the assumption that the person was exposed to the virus, but it was never confirmed by specific laboratory test. We call it “hearsay diagnoses” because it is based on that was heard by one person about another and not on material evidence.
Possible Determinants of the State Politic and Degree of COVID Restrictions
“Save the vulnerable” (i.e., elderly) and those having chronical health conditions is the primary political motivation of all restrictions and the significant personal offerings of the younger generations. However there is no statistically detectable influence of elderly, neither on the states politics nor on the degree of restrictions. (FIG. 4)
‘White’ is the largest ethnical group in the USA (~ 60 % of all), therefore the simple white/non-white ratio was used. The proportion of ‘whites’ in the states reversely correlated with the democrat orientation and the number of restrictions in the states: more ‘whites’ indicates less democrats and less restrictions. (FIG. 5).
Protestants is the largest religious group in the USA (~ 43% of all), therefore the simple protestant/non-protestant ratio was used. The proportion of Protestants in the states reversely correlated with the democratic orientation and the number of restrictions in the states: more Protestants indicates less democrats and less restrictions. (FIG. 6)
The size of the Jewish population showed strong positive correlation with the democrat orientation and strict restrictions in the states. More Jewish citizens indicated more democrats and more restrictions in the State in question. (FIG. 7).
Increasing Medicaid spending [Federal money] correlates with the democrat excess and more restrictions. This tendency is less detectable regarding the total health spending of the respective states. (FIG. 8).
The ‘Big’ Picture
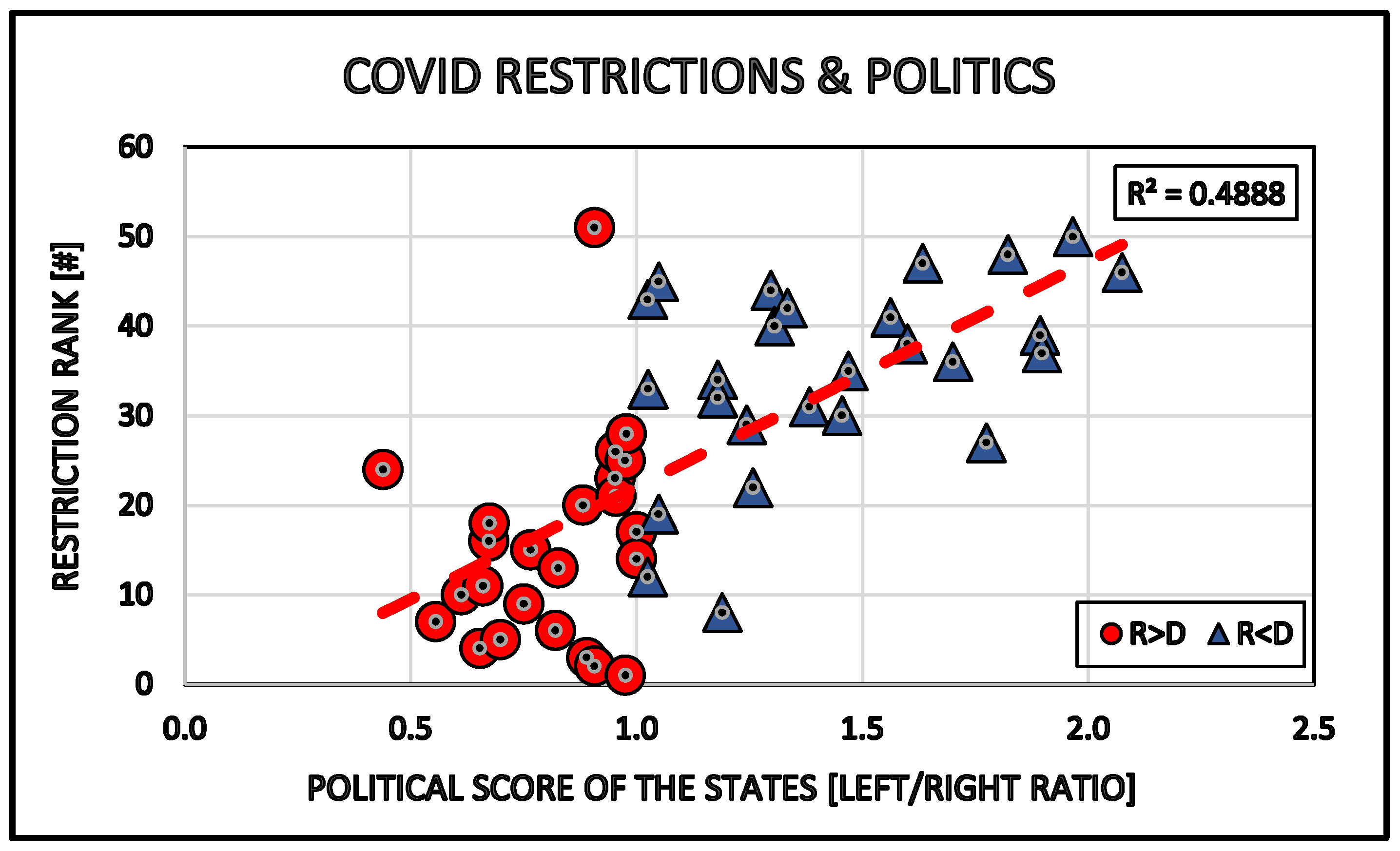
There is a strong positive correlation between the democrat bias of the States and the grade of restrictions in the respective states. More democrat affection in a State results in more restrictions in that State. (FIG. 9).
General Discussion and Suggested Conclusions
It was possible to observe, that significant differences exist between ‘red’ and ‘blue’ states regarding the involvement in the Covid epidemics. Democrat states were much harder effected by the virus, than republican States. The possible involvement of politic in the Covid response have been observed in the White House [President Trump]. We minted the term “Politi-Covid” in our earlier analyses. The Covid epidemic brutally interfered with the presidential election and resulted in very serious political complications.
The virus continued its political carrier end resulted in continued serious restrictions of our freedom and access to our normal work and regular social contacts. The theory behind the restrictions was, - that we all accepted, - that we have to save our elderly and other sick persons from Covid infection and the supposedly associated untimely death.
The introduction of qualitative statistical methods to the objective and non-partisan studies on the real results of the restrictions - and the driving forces behind - revealed that practically all of our restrictions were politically decided and enforced by the left oriented citizens. These restrictions (personal offerings by the citizens) didn’t result in any detectable reduction of the Covid mortality. The complete absence of any reduction of Covid deaths was observed first by other investigators and we could confirm it: Covid restrictions had no statistically detectable epidemiologic advantage for the “participating” Americans.
Reduction of total Covid cases will be positively interpreted by the supporters of further restrictions, however the value of this result is strongly questionable in the complete absence of reduction of the Covid associated death-rate.
It is of course valuable to see the same driving forces behind restrictions and politics, namely the preferential effect of the a) Judeo-Catholic (non-protestant) population, b) the non-white ethnical groups as well as the c) health-economic interest.
The protected elderly (65+) had no detectable effect neither on the politics nor the restrictions. It might be surprising for a politically naive observer.
The general suggestion (conclusion) of our statistical study is that the main difficulty to end the epidemic is not the virus itself, but the politically strongly biased population of America (radical ‘left’) in combination with the economic interest (medical/pharmaceutical industry) generated by the situation.
There remains - of course - a big question to answer: can a vaccine cure the infected soul of the great American Federation?
References
- CDC:, U.S. Center for Disease Control and Prevention - https://www.cdc.gov/ - accessed on 2021.
- Worldometer: https://www.worldometers.info/coronavirus/.
- Gallup tracking and 2018 Gallup Poll Social Series surveys. – State Party Identification and Leaning, 2018 - Politics, Feb.22, 2019 - https://news.gallup.com/poll/247025/democratic-states-exceed-republican-states-four-2018.aspx - Accessed. 2020.05.
- Biro, J.C. The “Politi-COVID (USA)” Epidemic in the “Pre-Election” America, 2020 and 2024. Preprints 2024, 2024092298. [Google Scholar] [CrossRef]
- 5 BIRO, J. C. Face Off: The Socio-Political Background of the COVID-19 Syndemic in USA. Preprints 2024, 2024091160. [Google Scholar] [CrossRef]
- Adam McCann, States with the Fewest Coronavirus Restrictions - Financial Writer, WalletHub, Mar 2, 2021- https://wallethub.com/edu/states-coronavirus-restrictions/73818.
- Adam McCann: States with the Fewest Coronavirus Restrictions – WalletHub, Apr 6, 2021 - https://wallethub.com/edu/states-coronavirus-restrictions/73818.
- BIRO, JC.-. Research Gate (preprint). https://www.researchgate.net/publication/384116200_FUNDAMENTAL_FLAWS_IN_COLLECTING_AND_INTERPRETING_COVID_DATA_%27COVIDISATION%27_OF_REGULAR_DEATHS_IN_USA?chan nel=doi&linkId=66eb99636b101f6fa4f0c598&showFulltext=true.
Figure 1.
Effects of politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) on the COVID case number in the States of the USA.
Figure 1.
Effects of politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) on the COVID case number in the States of the USA.
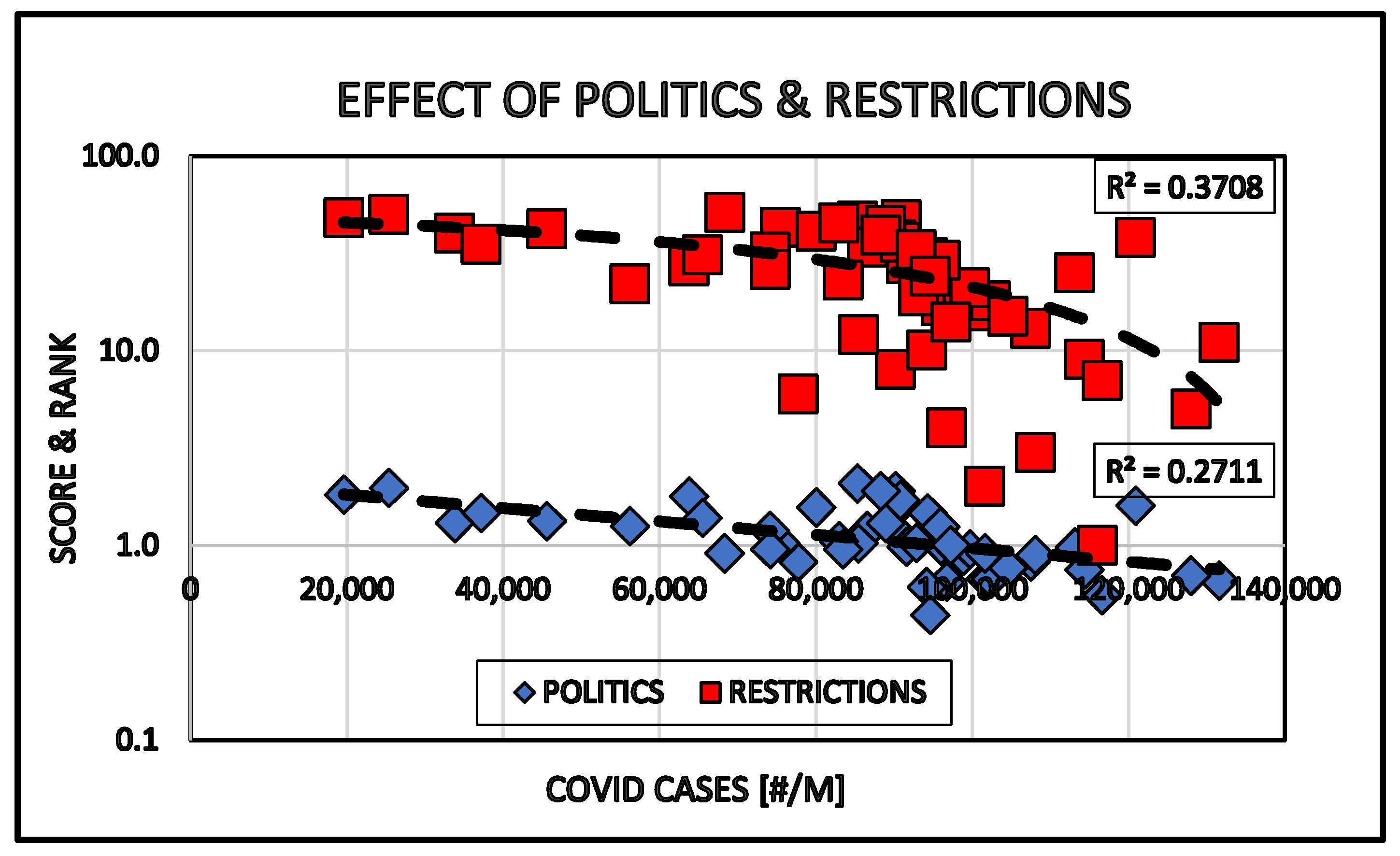
Figure 2.
Effects of politic (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) on the number of COVID related deaths in the States of the USA.
Figure 2.
Effects of politic (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) on the number of COVID related deaths in the States of the USA.
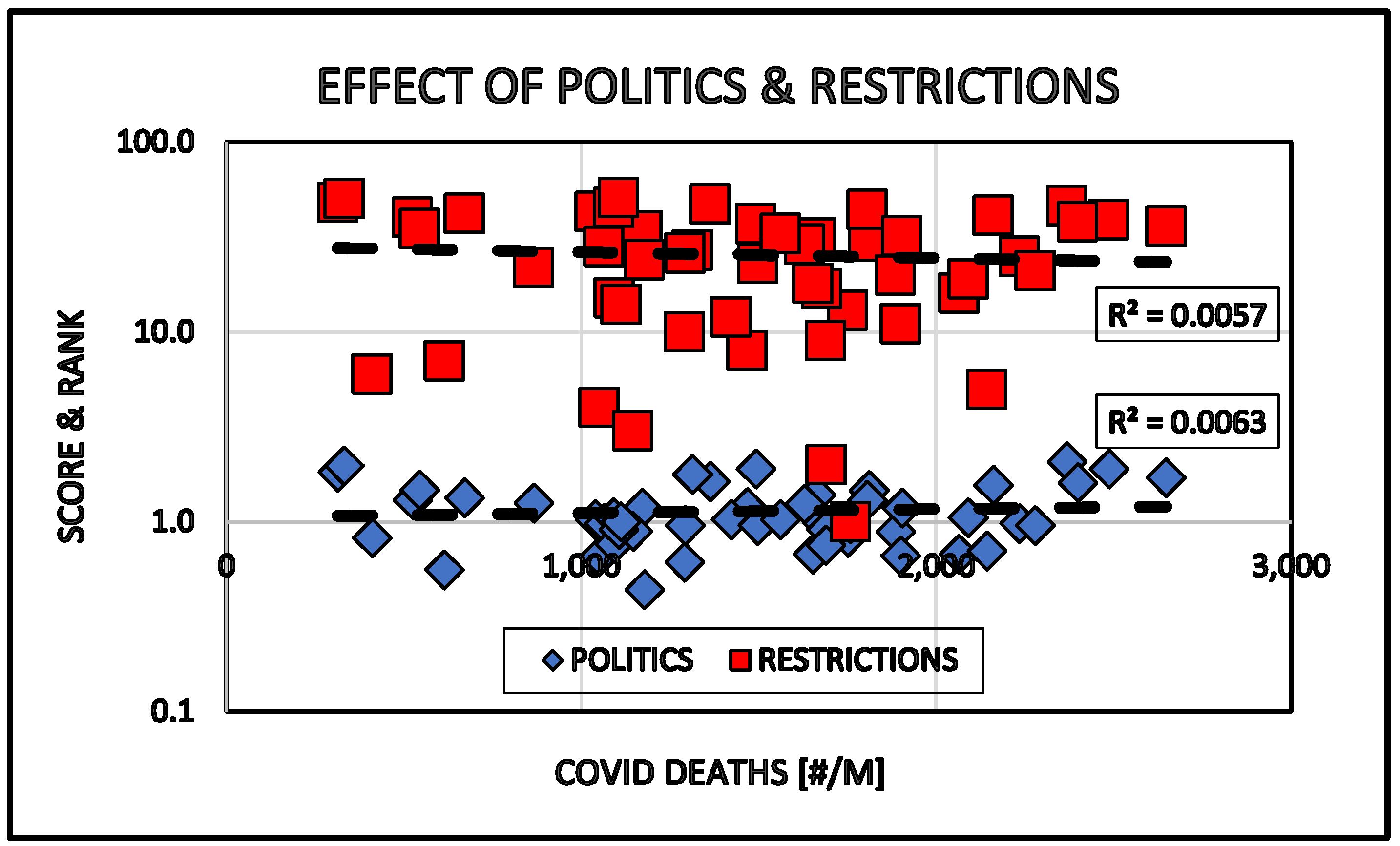
Figure 3.
Effect of politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) on the COVID mortality in the States of the USA.
Figure 3.
Effect of politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) on the COVID mortality in the States of the USA.
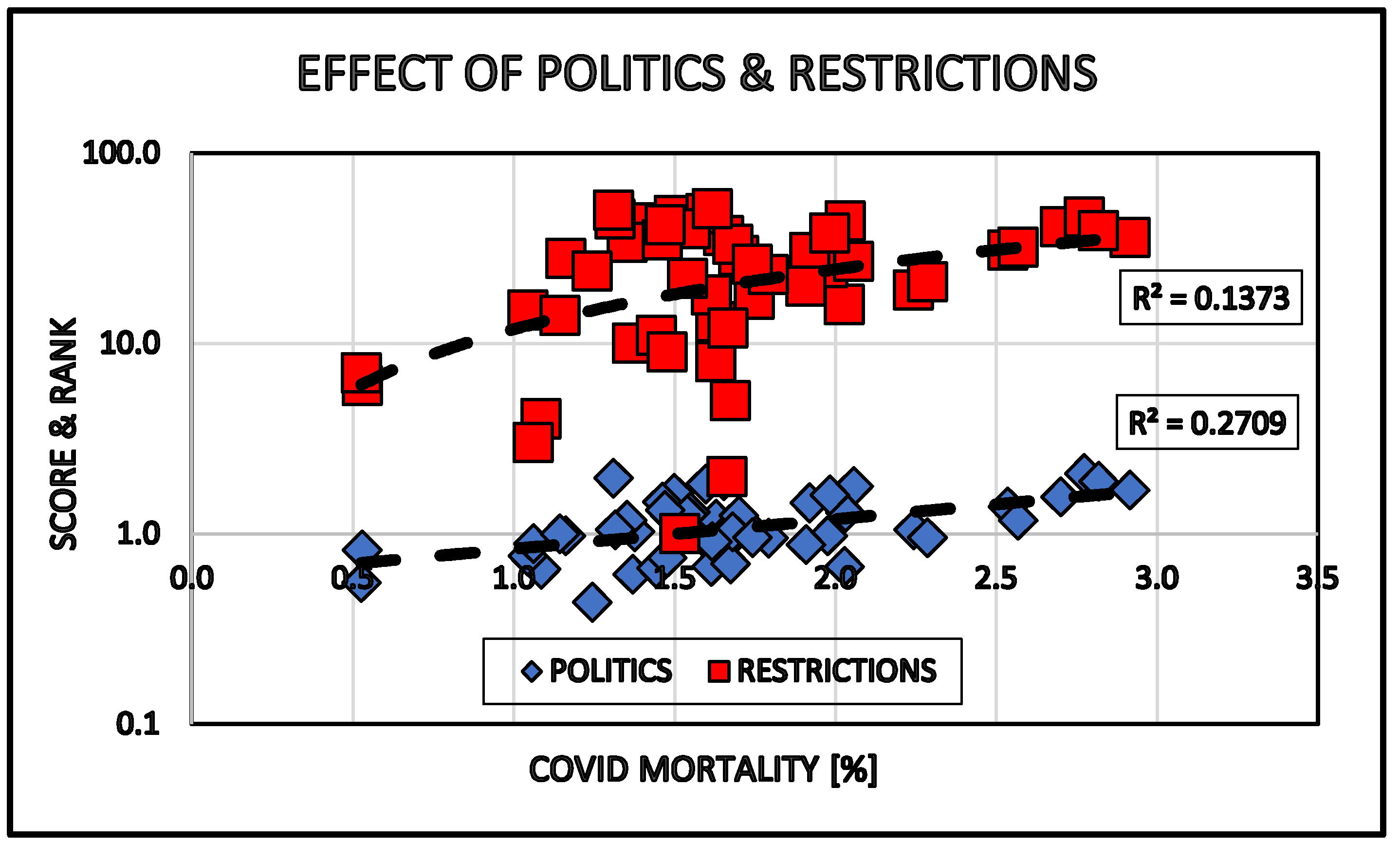
Figure 4.
Effect of the size of the senior population (65+) in the States on the politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) of that State.
Figure 4.
Effect of the size of the senior population (65+) in the States on the politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) of that State.
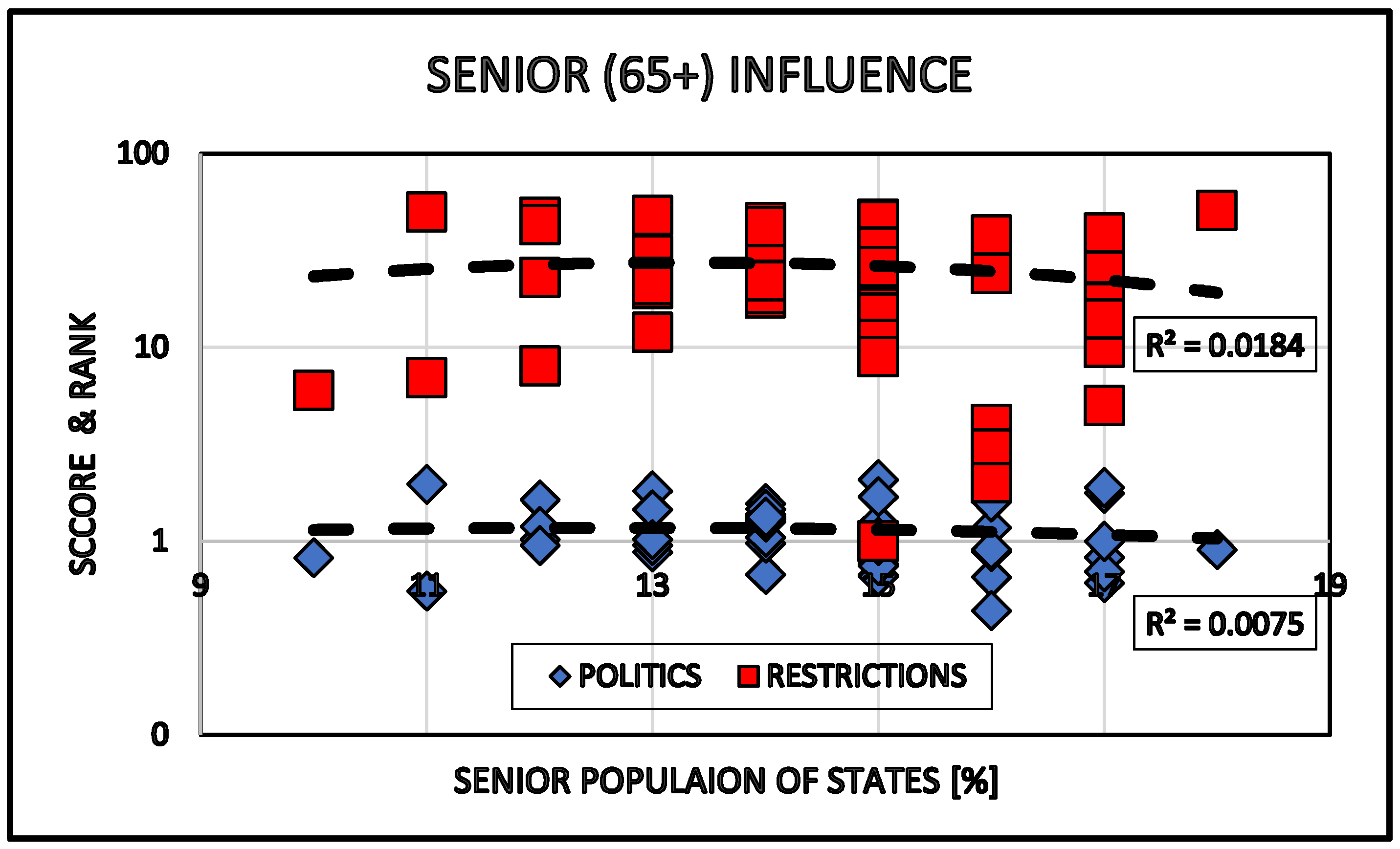
Figure 5.
Effect of ethnicity in the States on the politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) of that State.
Figure 5.
Effect of ethnicity in the States on the politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) of that State.
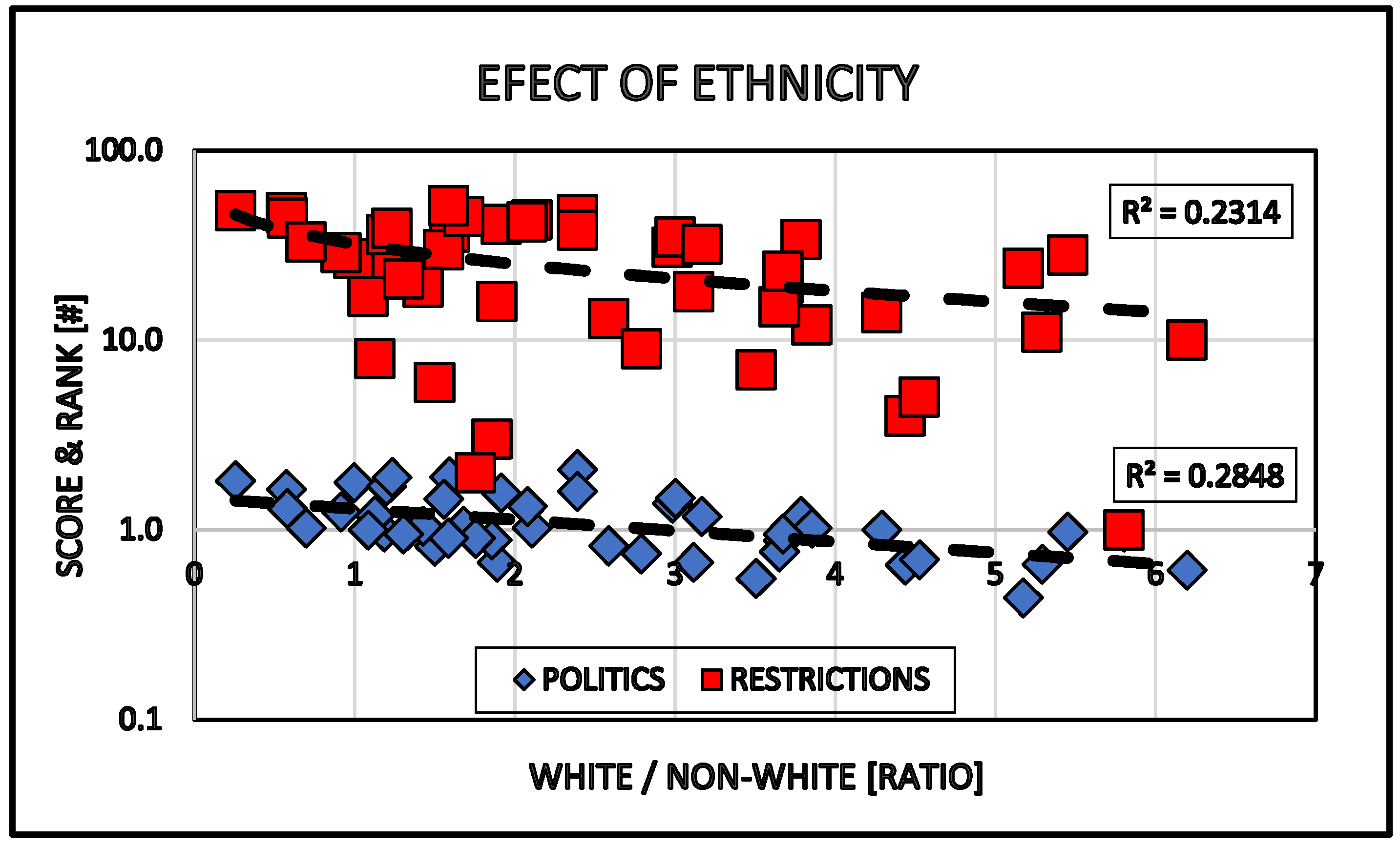
Figure 6.
Effect of religious affiliation in the States on the politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) of that State.
Figure 6.
Effect of religious affiliation in the States on the politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) of that State.
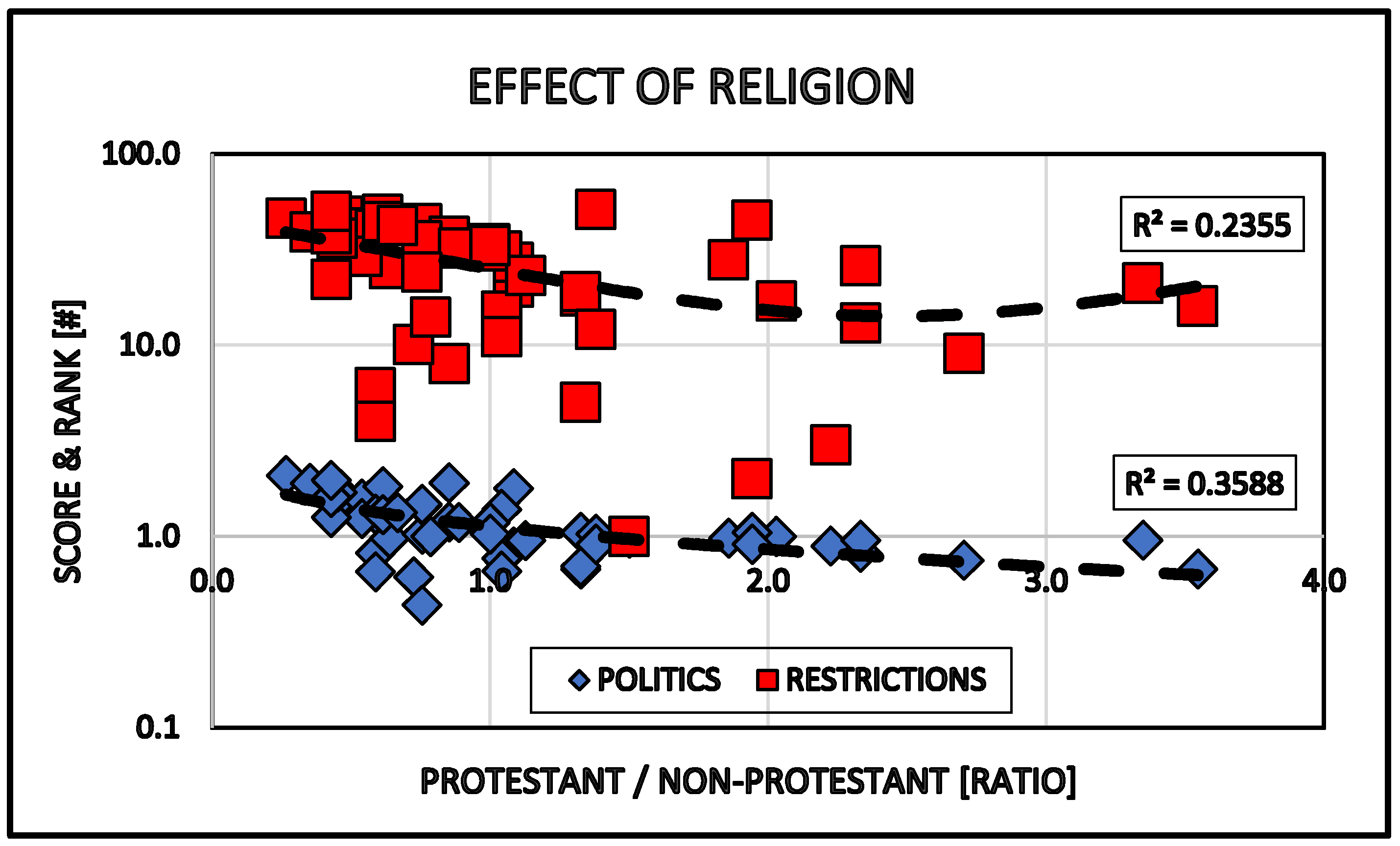
Figure 7.
Effect of Jewish population in the States on the politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) of that State.
Figure 7.
Effect of Jewish population in the States on the politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) of that State.
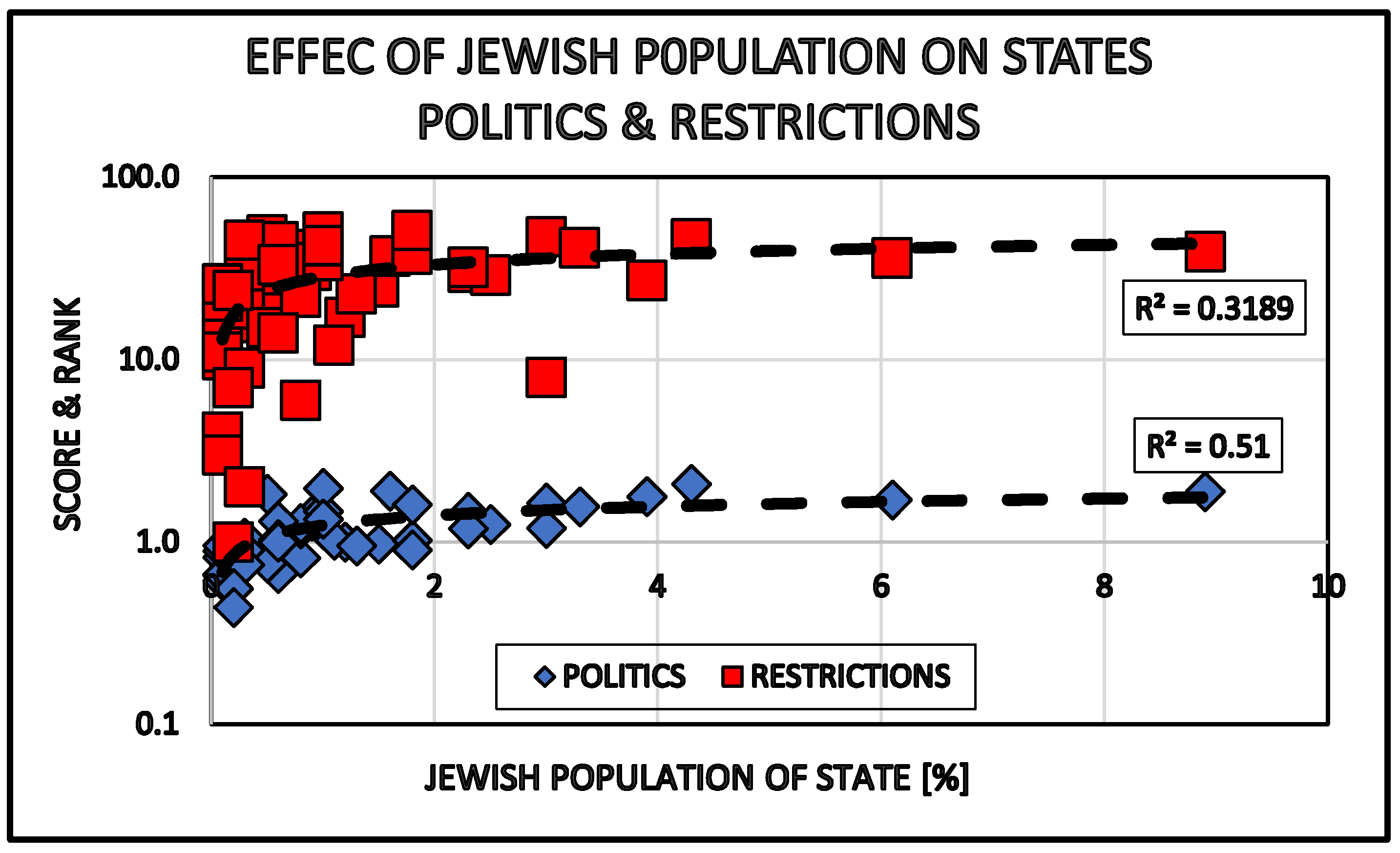
Figure 8.
Correlation between healthcare spending (all & Medicaid) in the States and the politics (Political Score – Democrat/Republican Ratio) as well as the restrictions (Restriction Rank) of that State.
Figure 8.
Correlation between healthcare spending (all & Medicaid) in the States and the politics (Political Score – Democrat/Republican Ratio) as well as the restrictions (Restriction Rank) of that State.
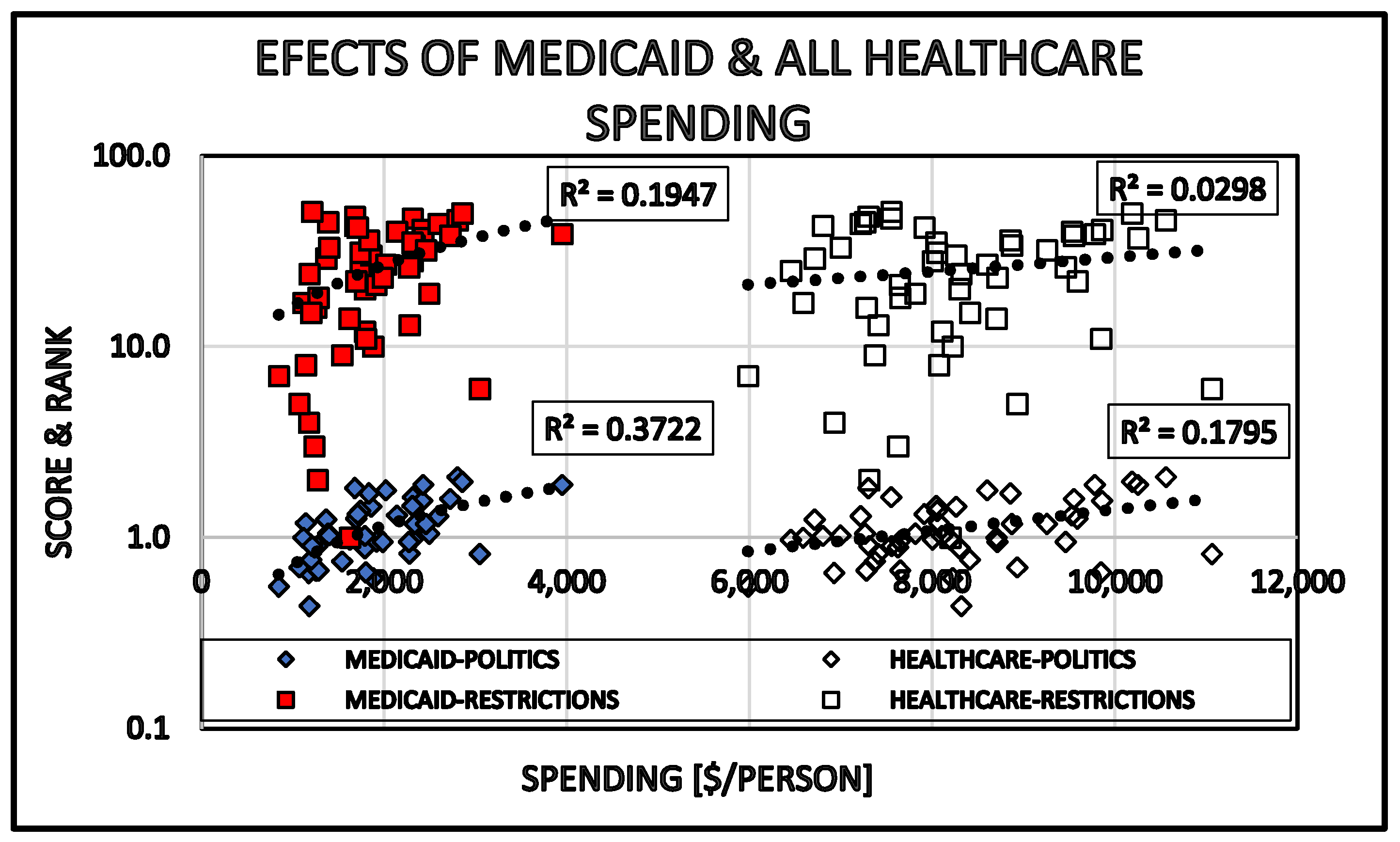
Figure 9.
Correlation between politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) of the States.
Figure 9.
Correlation between politics (Political Score: Democrat/Republican Ratio) and restrictions (Restriction Rank) of the States.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



