
Submitted:
03 October 2024
Posted:
04 October 2024
You are already at the latest version
Abstract
Anaplastic thyroid cancer (ATC) is considered to be one of the most virulent, treatment refractory, malignancies. Recent molecular insights into the biology of thyroid cancer have transformed ATC management and BRAF/MEK targeted therapy is now incorporated into guideline based multidisciplinary care. We report visceral perforation in the setting of an extreme response to such therapy in a patient with a mixed papillary thyroid carcinoma and ATC. Molecularly targeted therapy afforded a dramatic, but life-threatening, response to treatment. This report highlights the complexities of care for the patient and treating clinicians.
Keywords:
Anaplastic thyroid carcinoma
; papillary thyroid carcinoma
; targeted therapy
; perforation
; complications
1. Introduction
Historically, a diagnosis of anaplastic thyroid cancer (ATC) carried a median overall survival of 3-6 months with a 1-year survival rate of 20%. [1,2] This prognosis was related to its invasive potential with local infiltration of vital neck structures and the rapid development of distant metastases. These characteristics were compounded by the refractoriness of ATCs to standard chemotherapy agents and radiotherapy. [3]
The V600E mutation in the BRAF (V-Raf murine sarcoma viral oncogene homolog B1) oncogene has been identified in melanoma and other solid tumor malignancies such as thyroid cancers. The mutation is reportedly found in 10-50% of ATC. [4,5] Initial successful use of BRAF V600E targeted therapies in melanoma has been followed by their combination with MEK (mitogen-activated protein kinase) inhibitors, and subsequent extension of their use in other cancer types, including rare tumours. [6] The use of BRAF and MEK targeting drugs in ATC is described in several basket studies, small single-arm studies, and case reports. [7,8,9,10]
These reports of activity in previously treated patients, has led to guideline integration into first line treatment of suitably selected patients, including as a bridging strategy in potentially resectable disease. [11] Cohort studies have demonstrated improved survival with such strategies.[12] In this report we review life-threatening complications of targeted therapy in a patient with newly diagnosed ATC.
2. Case Report
As outlined by the accompanying patient testimony (Table 1), a 65-year-old gentleman presented with a 6-week history of dysphagia. Computed tomography imaging (CT) of the thorax, abdomen and pelvis and magnetic resonance imaging (MRI) of the neck revealed a 7.2 centimeter (cm) mass centered in the left lobe of the thyroid. The mass involved the cervical esophagus and posterior tracheal wall leading to moderate cervical tracheal airway narrowing and invasion of both the prevertebral fascia and the posterior arch of the cricoid with metastatic right level 2, bilateral level 3 and bilateral level 4 neck nodes (shown in Figures 1 and 2). A 12 millimeter (mm) right hilar node and right paratracheal and subcarinal nodes of less than 10mm were suspicious for malignant involvement (Stage IVC). [13]
1A, 2A: Axial image at the level of the 2nd thoracic vertebra. .
1B, 2B: Axial image at the level of the 6th cervical vertebra.
Fine needle aspiration of bilateral level III neck masses in addition to a biopsy of the thyroid mass demonstrated malignant cytology, consistent with papillary thyroid carcinoma (PTC).
Further sectioning of a cell block found a small quantity of tumor (10%) demonstrating a BRAF V600E mutation. NRAS mutations were not detected. The patient underwent pan-endoscopy with rigid oesophagoscopy. Left tracheal biopsy demonstrated respiratory type mucosa with underlying infiltrative tumor which appeared highly pleomorphic, consistent with a poorly differentiated carcinoma and consistent with ATC (shown in Figure 3). Upper esophageal biopsy showed clusters of malignant cells with similar appearances to the tracheal biopsy. An incidental pulmonary embolism was detected and anticoagulation was initiated.
The case was discussed at the regional Head and Neck multidisciplinary team meeting (MDM) which advised of the presence of locally advanced PTC and ATC. The case was not amenable to surgery due to esophageal involvement and unreconstructable tracheal involvement. The patient commenced encorafenib 450 mg once daily and binimetinib 45 mg twice daily (EB) in a neoadjuvant approach. [14] A clinical response was noted by day 3 with improving dysphagia. On day 5 of EB treatment, while attending hospital, the patient collapsed with a large volume hematemesis. Gastroscopy (shown in Figure 4) and bronchoscopy revealed erosion of the esophagus with resultant hemorrhage and the presence of a tracheo-esophageal fistula. CT imaging 12 days post following initiation of EB therapy confirmed treatment response with decreasing left thyroid mass, but unchanged neck and mediastinal lymphadenopathy. Nasogastric feeding was implemented. The fistula was managed conservatively and following demonstration of clinical closure using barium swallow testing, oral light diet was resumed. Due to concerns regarding tumor flare, a decision was made to administer EB treatment orally with small mouthfuls of yogurt from day 12 post the episode of haematemesis. [10] This was tolerated by the patient without aspiration into the airway. Crushing the binimetinib and opening the encorafenib capsules was considered but the manufacturing company advised that there was insufficient evidence for its use in this manner at the time. [15] Subsequently the patient underwent percutaneous gastrostomy tube (PEG) insertion. Repeat endoscopy at the time of PEG insertion demonstrated fistula resolution.
MRI 4 weeks later demonstrated a sustained treatment response. Three weeks later an FDG-Positron Emission Tomography (PET) CT demonstrated uptake in the left lobe of the thyroid gland, bilateral cervical lymph nodes and superior mediastinal lymph nodes (shown in Figure 5) . Subsequent MDM discussion recommended radical thyroidectomy based on data from cohort studies showing improved outcomes. [16,17]
Total thyroidectomy, bilateral comprehensive neck dissection, and central and superior mediastinal nodal dissection was performed, with surgical impression of complete removal of all gross tumor and abnormal lymph nodes.
Pathological investigation demonstrated a 4.5cm papillary thyroid cancer with extrathyroidal extension and metastatic PTC in 36 of 100 resected lymph nodes with multilevel extranodal extension. A separate fibrotic plaque removed from the esophagus and trachea, corresponding with the area of previously grossly invasive cancer, was negative for tumor. There was no evidence of ATC within the resected tissue. Immunohistochemistry for BRAF V600E demonstrated positive staining confirming the presence of BRAF mutation in the well-differentiated PTC component (shown in Figure 6).
Following further discussion at both regional and national MDMs, indefinite BRAF/MEK inhibition therapy was recommended in conjunction with radioactive iodine (RAI) adjuvant therapy at a dose of 5.5 GBq (giga-becquerel). Unstimulated thyroglobulin levels were 222 mcg/L pre-therapy, anti-thyroglobulin levels <3 mU/L, with levels rising to 316 mcg/L with associated TSH levels of 192 mU/L due to the administration of recombinant human thyroid stimulating hormone. Nuclear medicine RAI isotope was 131. External beam radiotherapy was not recommended. Post therapeutic single-photon emission computerized tomography (SPECT) scan was clear of any residual disease. Ten months after initial therapy initiation, the patient remains in remission with no evidence of relapsed disease on surveillance CT imaging.
3. Discussion
This case describes an incident of extreme response to targeted therapy with life-threatening visceral perforation. The perforation was associated with a pathological complete response to targeted therapy in that ATC, which had initially infiltrated tissues concordant with its clinical notoriety, was not detected in the subsequent thyroidectomy and nodal dissection.
Treatment related perforations are commonly associated with some malignancies such as lymphoma, but are rarely reported in in solid tumor malignancies. [18,19] When present, perforations develop in treatment of lymphoma at a median of 46 days (range 2-298 days) after commencing systemic therapy with 44% occurring within 4 weeks as in the present case. [18]
Local complications following the use of targeted therapy in ATC have been documented. One case report describes the use of lenvatinib in recurrent ATC, post-surgical resection of stage IVC disease, in which the patient suffered a carotid artery aneurysmal rupture 19 days after commencing treatment. [20]
Staub and colleagues published a retrospective study analyzing the use of Lenvatinib in patients with thyroid cancer.[21] Sixteen patients, including 9 with PTC and 3 with ATC, were included. Most patients had previous curative surgical resections (13/16) or radio-iodine therapy (9/16) and some had previous external beam radiotherapy (6/16). Three patients suffered fistulae or a tumor bleed in response to treatment with Lenvatinib, 2 of these cases occurred in patients with ATC. The statistical analysis determined that ATC was a risk factor for developing such a complication (Odds Ratio 3.19; 95% CI: 1.61-1.98; p <0.033).
In the present case, the rapid onset of perforation was concordant with a response to therapy within days of starting treatment. To our knowledge, such a response is unique and has not been observed in case reports, case series or cohort studies reviewed for this manuscript. [7,10,15,16,19,20] Our patient was fortunately attending hospital for a routine follow up visit when he collapsed due to hemorrhage and associated perforation.
ATC derives from well-differentiated thyroid carcinomas (WDTC) such as papillary and follicular carcinomas.[22,23] Nikiforova and colleagues analyzed 320 thyroid tumors and nodules for BRAF mutations. They concluded that BRAF mutations arose only in PTC and poorly differentiated and anaplastic carcinomas deriving from BRAF mutant PTC. [24] In contrast to the pathological complete response observed in the ATC component in the present case, the PTC component showed little radiological, or pathological response, despite harboring an identical BRAF sensitizing mutation. Other studies have demonstrated poor response rates to BRAF/MEK targeted therapies in PTC, as in the present case. [25,26] Several investigators have demonstrated the accumulation of additional genetic abnormalities as PTC transforms to ATC. These include the development of “katageis” with focal hypermutability, and the alterations in cyclin kinase genes regulating the cell cycle. [3,27,28] It is possible that such changes sensitize the cell to targeted therapy. Comprehensive evaluation with whole genomic outlook and RNA sequencing, as was performed by these investigators, has not been performed in the present case.
The paradigm for the management of thyroid malignancies has evolved significantly in the past 2 decades. Food and Drug Administration approval for the use of BRAF/MEK inhibitor combinations in ATC was obtained based on results of an open-label, phase 2 clinical trial which enrolled 100 patients with BRAF V600E mutated malignancies to receive dabrafenib and trametinib (DT). [7] The overall response rate amongst the 16 ATC patients enrolled was 69% (11/16 patients; 95% CI: 41-89%) with 7 ongoing responses at the time of data cut-off. Although median progression free and overall survival rates were not reached at time of data cut-off, the 12-month estimates were 79% and 80%. Such figures contrast sharply with historical data. [1,2] Consequently, National Comprehensive Cancer Network (NCCN) guidelines for management of ATC recommend molecular testing to inform systemic therapy options and available clinical trials.[29] When systemic therapy is indicated, the NCCN recommends the use of targeted therapies. Systemic therapy options include larotrectinib or entrectinib for NTRK (Neurotrophic Tyrosine Receptor Kinase) gene fusion-positive tumors, selpercatinib for RET (Rearranged during transfection) fusion positive tumors, pembrolizumab for tumor mutational burden high tumors (>/= 10 mut/Mb) and BRAF targeted therapies. [30,31,32,33,34] In the present case, EB was prescribed as therapy based on it’s favorable toxicity profile and favorable prior institutional experience.
Current guidelines highlight the need for a multimodality approach to the management of ATC. [29] In recent years, clinicians have trialed short periods of targeted therapy in the neoadjuvant setting for ATC, to minimize the extent of surgery, or to achieve resectability in initially unresectable disease. [12,34] One case series described complete surgical resection following neoadjuvant DT in 6 patients with initially unresectable, BRAF V600E mutated ATC.[35] Three of the patients also received perioperative pembrolizumab. A complete surgical resection was achieved in all cases. OS at 6 months was 100% and OS at 1 year was 83% (5/6 patients). Pathological assessment of resected samples detected < 5% tumor viability in 83% of resected tumors. [35] This case series represented the first prospective demonstration of the feasibility and effectiveness of a neoadjuvant approach using DT, in patients with initially unresectable BRAF mutated ATC. Subsequently Maniakas and colleagues reported their 20-year experience in the treatment of 479 patients with ATC. [12] In this cohort of 479 patients, 23 received surgery following neoadjuvant treatment, 20 of these were BRAF targeted therapies, the other 3 patients received chemotherapy or a checkpoint/MEK-inhibitor combination. The 1-year survival rate of the 20 patients (8 of whom had presented with stage IVC disease) treated with neoadjuvant BRAF-directed therapies followed by surgery was 94%, compared to 52% in 35 patients treated with a BRAF/MEK inhibitor combination without tumor resection. These studies formed the basis for the decision to proceed to thyroidectomy in the present case.
Radioiodine (Iodine –131) therapy is the treatment of choice following resection of intermediate and high-risk WDTC. [29] BRAF mutant PTC and poorly differentiated thyroid carcinomas demonstrate poor response rates to standard radioiodine treatment. [36] However, it has been demonstrated that BRAF/MEK inhibitor treatment can stimulate radioiodine uptake in these cancer cells and restore the therapeutic benefit of radioiodine therapy. [37] For this reason the patient is being referred for adjuvant RAI therapy.
This case report contributes to the limited published data demonstrating life-threatening complications following response to targeted therapy in ATCs. The patient’s subsequent favorable outcome has been transformative as he outlines in this report. Further studies are needed to discern treatment paradigms for patients with BRAF/MEK refractory or unresponsive disease in order to extend the benefits of this transformative therapy to all patients with ATC.
Author Contributions
Concept: Simon Barry and Seamus O’Reilly; Data Collection: All Authors; Manuscript writing: All Authors.
Funding
UCC Cancer Trials Group is supported by the Health Research Board.
Institutional Review Board Statement
Independent ethical committee approval was not required given the nature of this single patient case report.
Informed Consent Statement
Written informed consent has been obtained from the patient for publication of the case report and accompanying images.
Acknowledgments
We are grateful to the patient for agreeing to provide a testimony.
Conflicts of Interest
None relevant to declare.
References
- Wächter, S.; Vorländer, C.; Schabram, J.; et al. Anaplastic thyroid carcinoma: changing trends of treatment strategies and associated overall survival. Eur Arch Oto-Rhino-Laryngol 2020, 277, 1507–14. [Google Scholar] [CrossRef] [PubMed]
- Smallridge, R.C.; Copland, J.A. Anaplastic thyroid carcinoma: pathogenesis and emerging therapies. Clin Oncol 2010, 22, 486–97. [Google Scholar] [CrossRef] [PubMed]
- Stenman, A.; Juhlin, C.C. Novel Insights in the Genomics of Anaplastic Thyroid Carcinoma: A Role for Cyclin-Dependent Kinase Inhibition? Cancers (Basel) 2023, 15, 4621. [Google Scholar] [CrossRef] [PubMed]
- Cabanillas, M.E.; Ryder, M.; Jimenez, C. Targeted Therapy for Advanced Thyroid Cancer: Kinase Inhibitors and Beyond. Endocr Rev 2019, 40, 1573–604. [Google Scholar] [CrossRef] [PubMed]
- Kebebew, E.; Weng, J.; Bauer, J.; et al. The Prevalence and Prognostic Value of BRAF Mutation in Thyroid Cancer. Ann Surg 2007, 246, 466–71. [Google Scholar] [CrossRef]
- Sidaway, P. BRAF plus MEK inhibition effective in papillary craniopharyngioma. Nat Rev Clin Oncol 2023, 20, 661. [Google Scholar] [CrossRef]
- Subbiah, V.; Kreitman, R.J.; Wainberg, Z.A.; et al. Dabrafenib and Trametinib Treatment in Patients with Locally Advanced or Metastatic BRAF V600–Mutant Anaplastic Thyroid Cancer. J Clin Oncol 2018, 36, 7–13. [Google Scholar] [CrossRef]
- Hyman, D.M.; Puzanov, I.; Subbiah, V.; et al. Vemurafenib in Multiple Nonmelanoma Cancers with BRAF V600 Mutations. N Eng J Med 2015, 373, 726–36. [Google Scholar] [CrossRef]
- Subbiah, V.; Kreitman, R.J.; Wainberg, Z.A.; et al. Dabrafenib plus trametinib in BRAF V600E-mutated rare cancers: the phase 2 ROAR trial. Nat Med 2023, 1103–1112. [Google Scholar] [CrossRef]
- Agarwal, R.; Wang, J.; Wilson, K.; et al. Response to Targeted Therapy in BRAF Mutant Anaplastic Thyroid Cancer. J Natl Compr Canc Netw 2016, 14, 1203–1207. [Google Scholar] [CrossRef]
- Bible, K.C.; Kebebew, E.; Brierley, J.; et al. American Thyroid Association Guidelines for Management of Patients with Anaplastic Thyroid Cancer. Thyroid 2021, 31, 337–386. [Google Scholar] [CrossRef] [PubMed]
- Maniakas, A.; Dadu, R.; Busaidy, N.L.; et al. Evaluation of Overall Survival in Patients with Anaplastic Thyroid Carcinoma, 2000-2019. JAMA Oncol 2020, 6, 1397. [Google Scholar] [CrossRef]
- Tuttle, R.M.; Haugen, B.; Perrier, N.D. Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer (Eighth Edition): What Changed and Why? Thyroid 2017, 27, 751–6. [Google Scholar] [CrossRef] [PubMed]
- Tahara, M.; Kiyota, N.; Imai, H.; Takahashi, S.; Nishiyama, A.; Tamura, S.; Shimizu, Y.; Kadowaki, S.; Ito, K.I.; Toyoshima, M.; Hirashima, Y.; Ueno, S.; Sugitani, I. A Phase 2 Study of Encorafenib in Combination with Binimetinib in Patients with Metastatic BRAF-Mutated Thyroid Cancer in Japan. Thyroid. 2024, 34, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Jang, C.; Lau, S.C.; Velcheti, V. To crush or not to crush: Administering dabrafenib and trametinib through a nasogastric tube in a critically ill patient with non small cell lung cancer – a case report and review of literature of targeted therapies given through enteral feeding tubes. In Clinical Lung Cancer; 2023. [Google Scholar] [CrossRef]
- Wu, S.S.; Lamarre, E.D.; Yalamanchali, A.; et al. Association of Treatment Strategies and Tumor Characteristics With Overall Survival Among Patients With Anaplastic Thyroid Cancer: A Single-Institution 21-Year Experience. JAMA Otolaryngol Head Neck Surg 2023, 149, 300–309. [Google Scholar] [CrossRef]
- Zhao, X.; Wang, J.R.; Dadu, R.; et al. Surgery After BRAF-Directed Therapy Is Associated with Improved Survival in BRAF V600E Mutant Anaplastic Thyroid Cancer: A Single-Center Retrospective Cohort Study. Thyroid 2023, 33, 484–491. [Google Scholar] [CrossRef]
- Yang, K.M.; Jeong, M.J.; Yoon, K.H.; et al. Oncologic outcome of colon cancer with perforation and obstruction. BMC Gastroenterol 2022, 22, 247. [Google Scholar] [CrossRef]
- Vaidya, R.; Habermann, T.M.; Donohue, J.H.; et al. Bowel perforation in intestinal lymphoma: Incidence and clinical features. Ann Oncol 2013, 24, 2439–43. [Google Scholar] [CrossRef]
- Obata, K.; Sugitani, I.; Ebina, A.; et al. Common carotid artery rupture during treatment with Lenvatinib for anaplastic thyroid cancer. Int Cancer Conf J 2016, 5, 197–201. [Google Scholar] [CrossRef]
- Staub, Y.; Nishiyama, A.; Suga, Y.; et al. Clinical Characteristics Associated with Lenvatinib-induced Fistula and Tumor-related Bleeding in Patients with Thyroid Cancer. Anticancer Res 2019, 39, 3871–8. [Google Scholar] [CrossRef]
- Wreesmann, V.B.; et al. Genome-wide appraisal of thyroid cancer progression. The Am J Pathol 2002, 161, 1549–1556. [Google Scholar] [CrossRef] [PubMed]
- Sheffield, E.A.; Rosai, J.; Carcangiu, M.; et al. Tumors of the thyroid gland. J Pathol 1992, 171, 247–248. [Google Scholar] [CrossRef]
- Nikiforova, M.N.; Kimura, E.T.; Gandhi, M.; et al. BRAF mutations in thyroid tumors are restricted to papillary carcinomas and anaplastic or poorly differentiated carcinomas arising from papillary carcinomas. J Clin Endocrinol Metab 2003, 88, 5399–404. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.B.; et al. Clinical responses to Vemurafenib in patients with metastatic papillary thyroid cancer harboring BRAFv600emutation. Thyroid 2013, 23, 1277–1283. [Google Scholar] [CrossRef] [PubMed]
- Brose, M.S.; et al. ‘Vemurafenib in patients with BRAF v600e-positive metastatic or unresectable papillary thyroid cancer refractory to radioactive iodine: A non-randomised, multicentre, open-label, phase 2 trial’. Lancet Oncol 2016, 17, 1272–1282. [Google Scholar] [CrossRef]
- Rubino, S.; Oliver, D.E.; Tran, N.D.; et al. Improving Brain Metastases Outcomes Through Therapeutic Synergy Between Stereotactic Radiosurgery and Targeted Cancer Therapies. Front Oncol 2022, 12, 854402. [Google Scholar] [CrossRef]
- Landa, I.; Ibrahimpasic, T.; Boucai, L.; et al. Genomic and transcriptomic hallmarks of poorly differentiated and anaplastic thyroid cancers. J Clin Invest 2016, 126, 1052–66. [Google Scholar] [CrossRef]
- Haddad, R.I.; Bischoff, L.; Ball, D.; et al. NCCN Clinical Practice Guidelines in Oncology: Thyroid Carcinoma Version 2.2022. Available at: NCCN.org. Accessed December 1, 2023.
- Drilon, A.; Laetsch, T.W.; Kummar, S.; et al. Efficacy of Larotrectinib in TRK Fusion–Positive Cancers in Adults and Children. N Eng J Med 2018, 378, 731–9. [Google Scholar] [CrossRef]
- Doebele, R.C.; Drilon, A.; Paz-Ares, L.; et al. Entrectinib in patients with advanced or metastatic NTRK fusion-positive solid tumours: integrated analysis of three phase 1–2 trials. Lancet Oncol 2020, 21, 271–82. [Google Scholar] [CrossRef]
- Hong, D.S.; Bauer, T.M.; Lee, J.J.; et al. Larotrectinib in adult patients with solid tumours: a multi-centre, open-label, phase I dose-escalation study. Ann Oncol. 2019, 30, 325–31. [Google Scholar] [CrossRef]
- Capdevila, J.; Wirth, L.J.; Ernst, T.; et al. PD-1 Blockade in Anaplastic Thyroid Carcinoma. J Clin Oncol 2020, 38, 2620–7. [Google Scholar] [CrossRef] [PubMed]
- Marabelle, A.; Fakih, M.; Lopez, J.; et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol 2020, 21, 1353–65. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.R.; Zafereo, M.E.; Dadu, R.; et al. Complete Surgical Resection Following Neoadjuvant Dabrafenib Plus Trametinib in BRAF V600E -Mutated Anaplastic Thyroid Carcinoma. Thyroid 2019, 29, 1036–43. [Google Scholar] [CrossRef] [PubMed]
- Riesco-Eizaguirre, G.; Rodríguez, I.; De la Vieja, A.; et al. The BRAFV600E oncogene induces transforming growth factor beta secretion leading to sodium iodide symporter repression and increased malignancy in thyroid cancer. Cancer Res 2009, 69, 8317–8325. [Google Scholar] [CrossRef]
- Rothenberg, S.M.; et al. Redifferentiation of iodine-refractory BRAF V600E-mutant metastatic papillary thyroid cancer with Dabrafenib. Clin Cancer Res 2015, 21, 1028–1035. [Google Scholar] [CrossRef]
Figure 1 and 2.
Pre-treatment CT imaging demonstrated a heterogeneous mass centered in the left thyroid with enhancing, calcified and hypo-enhancing components invading the esophagus and trachea with enhancing neck adenopathy (Figures 1A and1B). Follow-up CT Neck and Thorax performed 12 days later demonstrated a significant decrease in the hypo-enhancing (likely anaplastic) component of the mass with residual enhancing mass and adenopathy (likely papillary component) (Figures 2A and 2B).
Figure 1 and 2.
Pre-treatment CT imaging demonstrated a heterogeneous mass centered in the left thyroid with enhancing, calcified and hypo-enhancing components invading the esophagus and trachea with enhancing neck adenopathy (Figures 1A and1B). Follow-up CT Neck and Thorax performed 12 days later demonstrated a significant decrease in the hypo-enhancing (likely anaplastic) component of the mass with residual enhancing mass and adenopathy (likely papillary component) (Figures 2A and 2B).
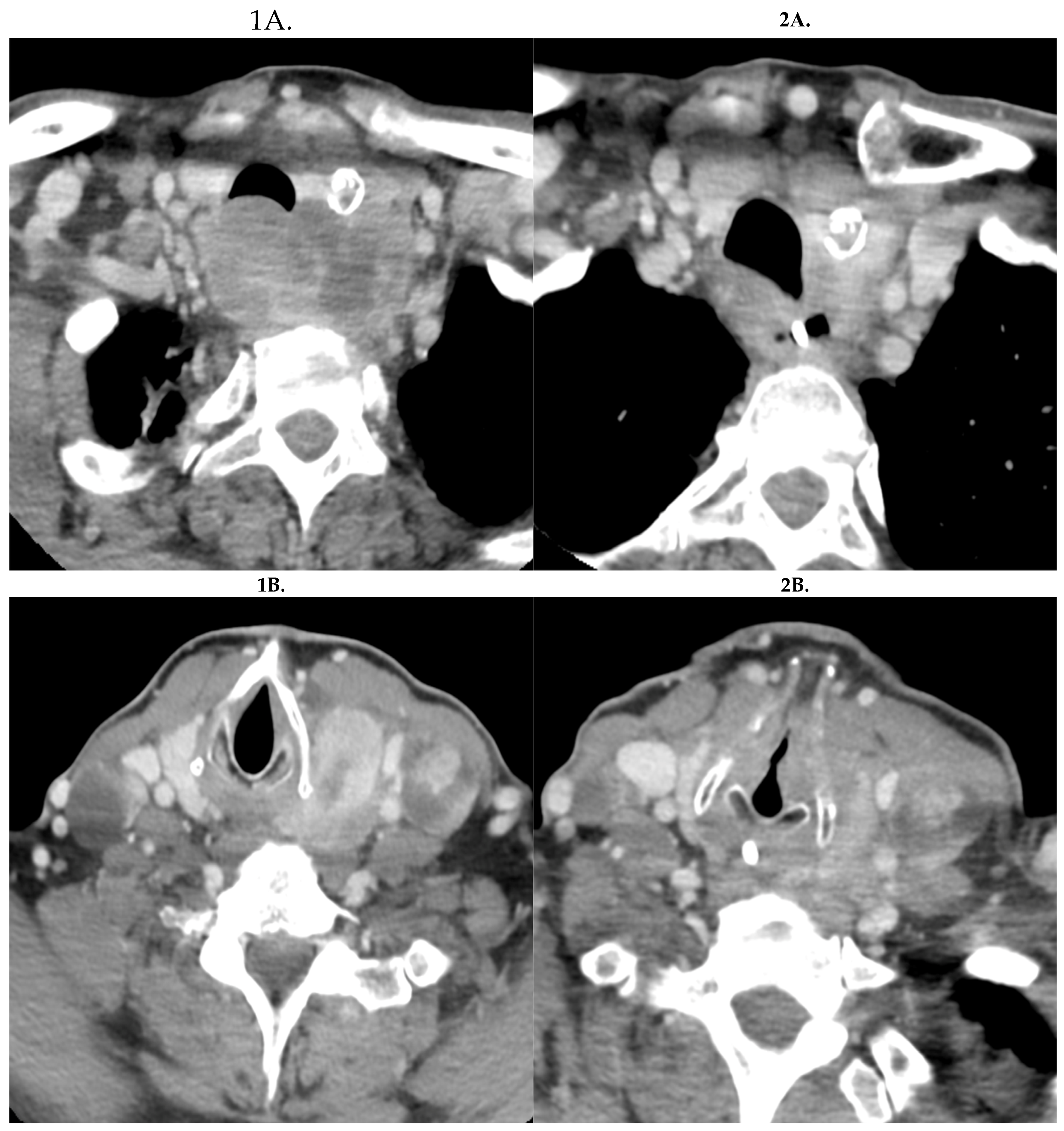
Figure 3.
Hematoxylin and Eosin (H&E) stain shows anaplastic thyroid carcinoma involving the trachea, with respiratory epithelium on the surface (10x magnification) (A). PAX8 (B) and TTF1 (C) immunohistochemical stains support the thyroid origin of the anaplastic tumor (10x magnification). H&E stain of the esophageal biopsy demonstrates superficial fragment of squamous mucosa with necro-inflammatory debris and separate fragment of tumor (10x magnification) (D).
Figure 3.
Hematoxylin and Eosin (H&E) stain shows anaplastic thyroid carcinoma involving the trachea, with respiratory epithelium on the surface (10x magnification) (A). PAX8 (B) and TTF1 (C) immunohistochemical stains support the thyroid origin of the anaplastic tumor (10x magnification). H&E stain of the esophageal biopsy demonstrates superficial fragment of squamous mucosa with necro-inflammatory debris and separate fragment of tumor (10x magnification) (D).
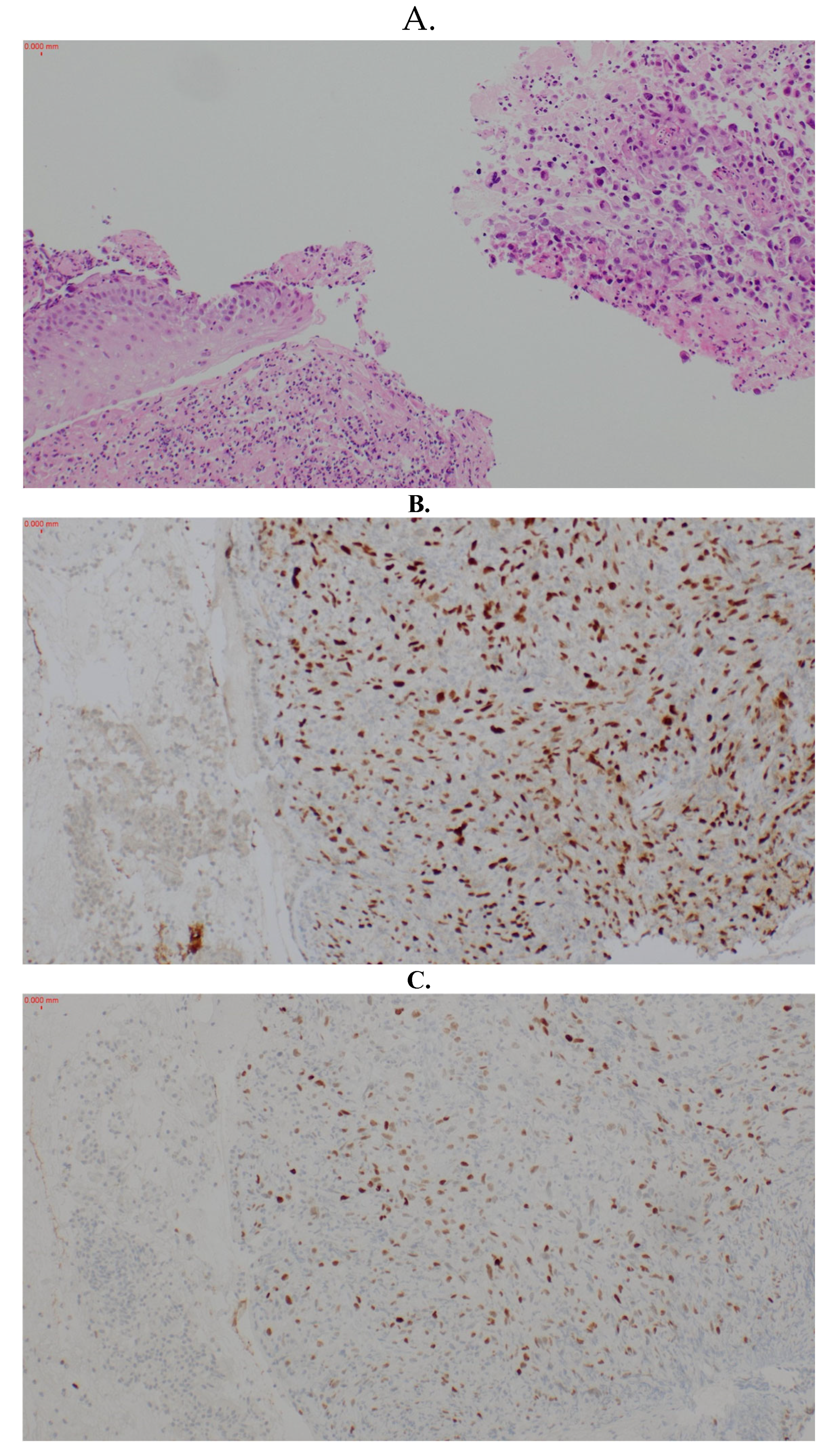
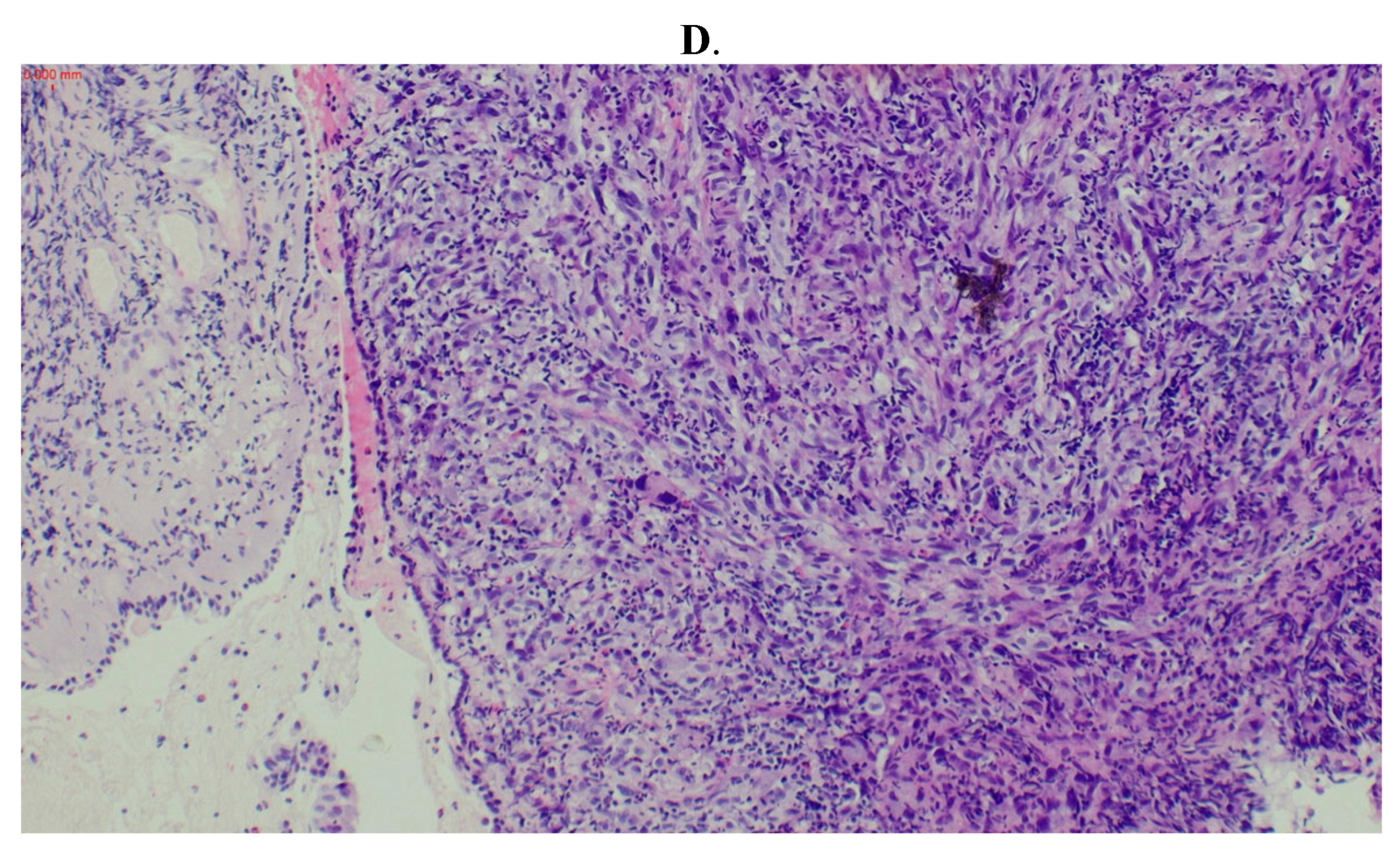
Figure 4.
Gastroscopy demonstrated necrotic debris at the site of fistulation with overlying clot (A). The clot was removed using suction. Fistulation was confirmed by passing an endotracheal tube and passing air bubbles via gastroscopy (not pictured). Bubbling was then noted on bronchoscopy thus demonstrating the passage between the two viscera. Bronchoscopy demonstrated adherent clot over the site of fistulation (B).
Figure 4.
Gastroscopy demonstrated necrotic debris at the site of fistulation with overlying clot (A). The clot was removed using suction. Fistulation was confirmed by passing an endotracheal tube and passing air bubbles via gastroscopy (not pictured). Bubbling was then noted on bronchoscopy thus demonstrating the passage between the two viscera. Bronchoscopy demonstrated adherent clot over the site of fistulation (B).
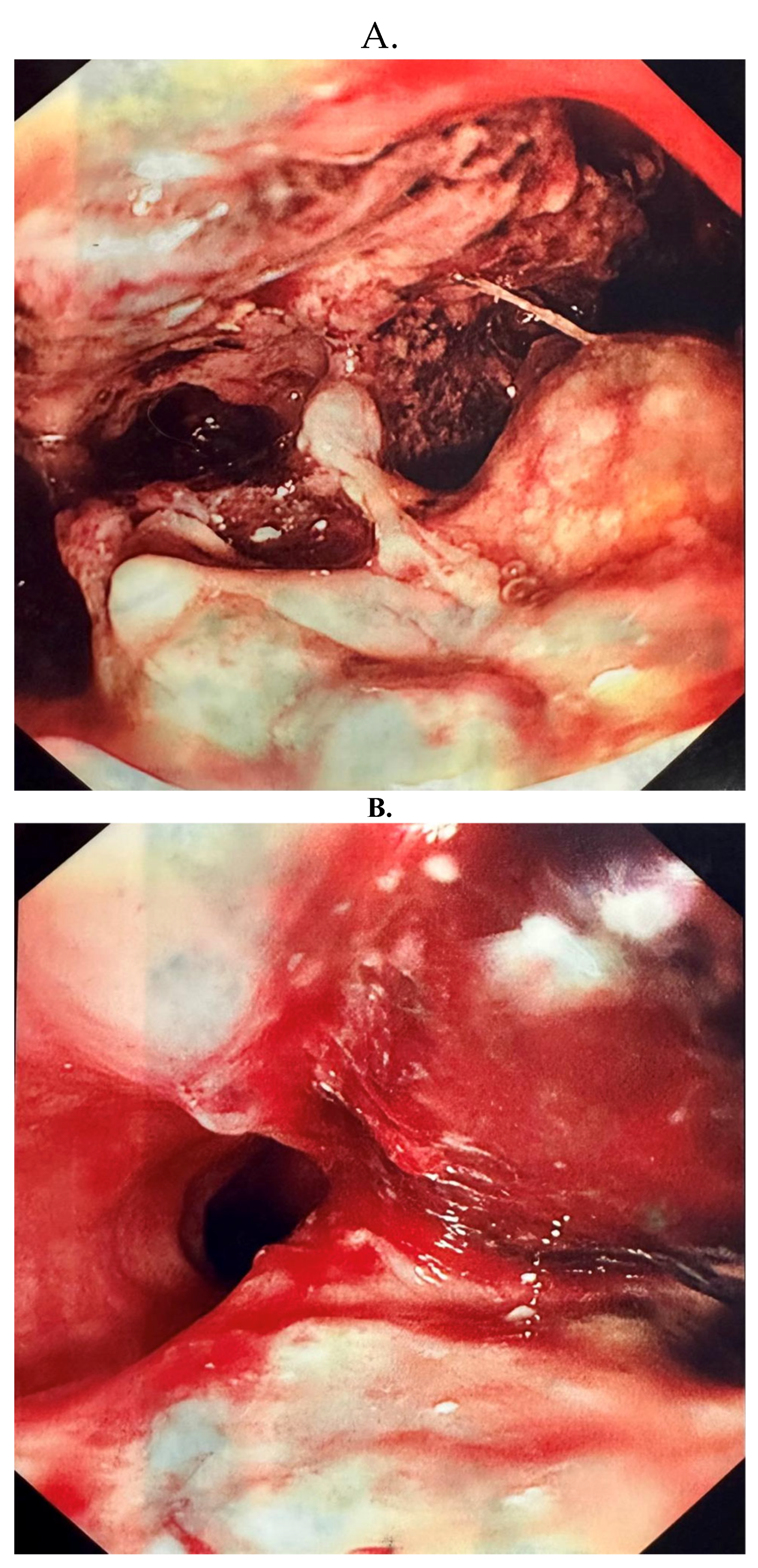
Figure 5.
(A and B): Pre-operative PET CT demonstrated uptake within the residual component of the left thyroid mass and the bilateral neck adenopathy but no distant metastatic disease.
Figure 5.
(A and B): Pre-operative PET CT demonstrated uptake within the residual component of the left thyroid mass and the bilateral neck adenopathy but no distant metastatic disease.
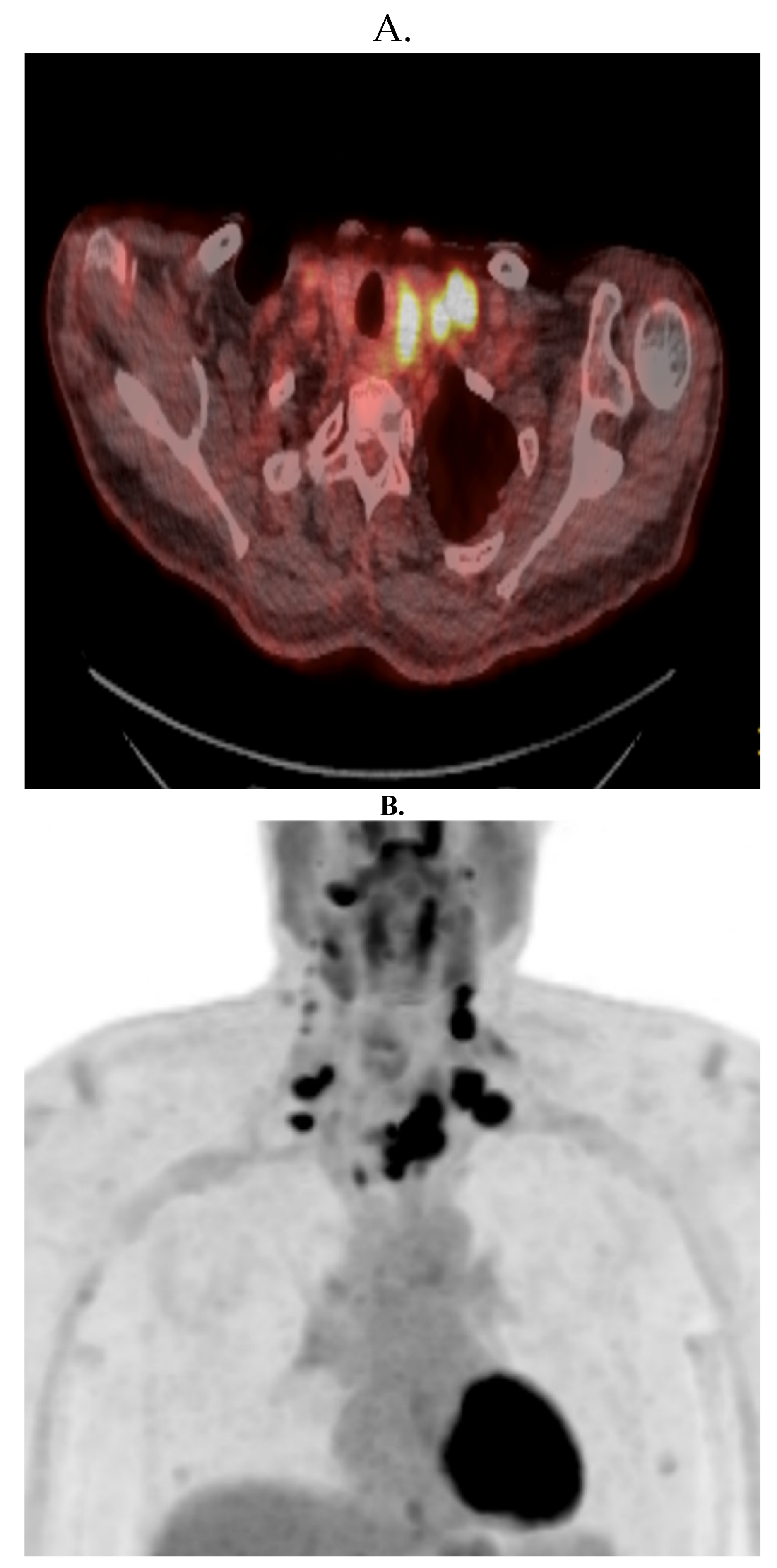
Figure 6.
(A-C): Hematoxylin and Eosin (H&E) stain of the resected papillary thyroid carcinoma (A = H&E at 4x magnification; B = H&E at 20x magnification; C = BRAF Immunostain at 10x magnification.).
Figure 6.
(A-C): Hematoxylin and Eosin (H&E) stain of the resected papillary thyroid carcinoma (A = H&E at 4x magnification; B = H&E at 20x magnification; C = BRAF Immunostain at 10x magnification.).
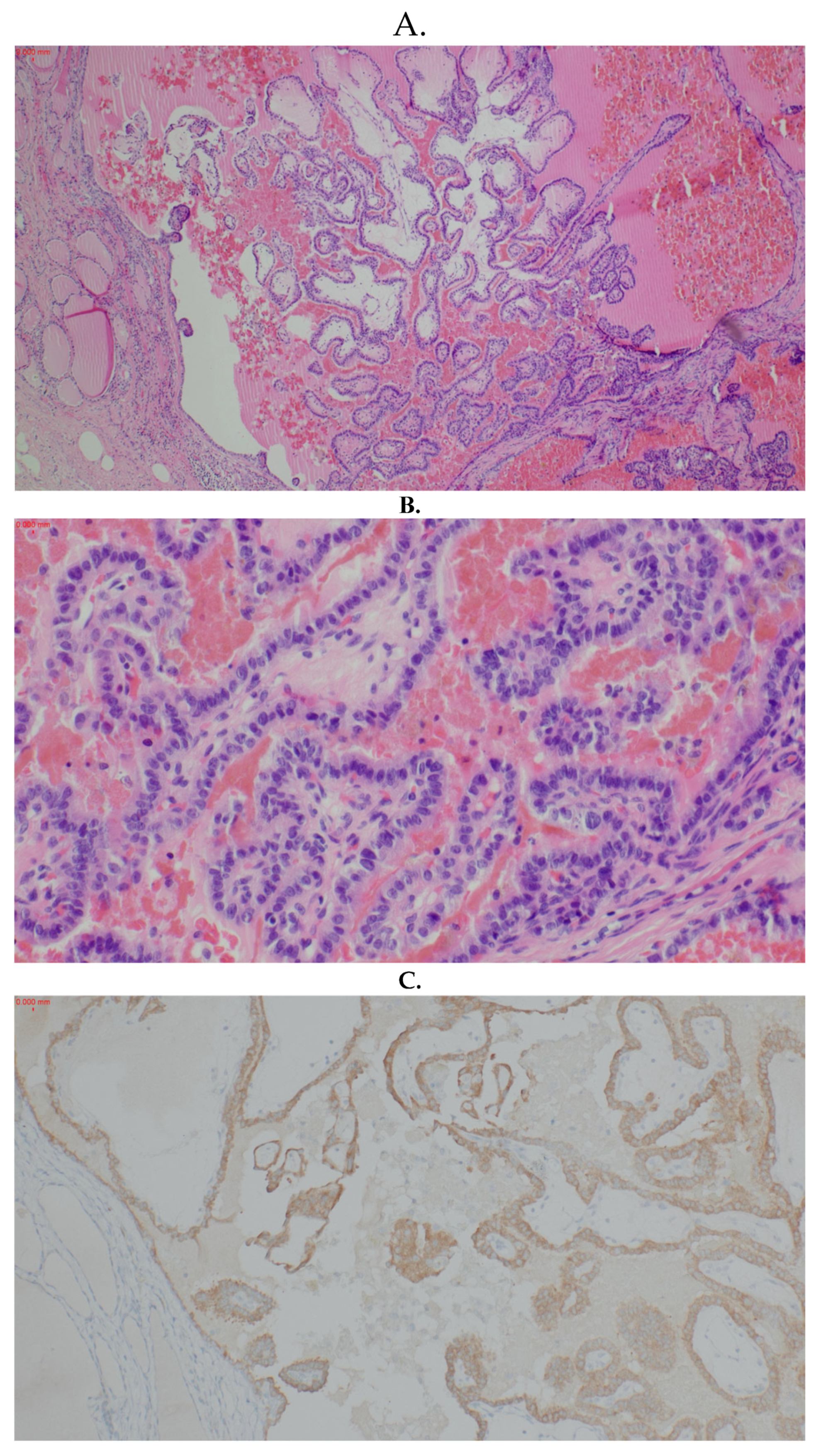

Table 1.
Patient Testimony.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



