Submitted:
03 October 2024
Posted:
04 October 2024
You are already at the latest version
Abstract
The consumption of contaminated water contributes to the global burden of diarrhea and other water-borne diseases, especially among young children. While the decentralized solar water disinfection treatment system remains a viable option to have safe drinking water, our understanding of the effects of household water treatment before use on willingness to accept and adopt a decentralized solar water disinfection treatment system is limited. In this study, a complementary log-log regression analysis of the compositional and contextual factors that systematically vary with willingness to accept and adopt a decentralized solar water disinfection treatment system in the Sawla-Tuna-Kalba (STK) district of Ghana was carried out. Based on our findings, a greater proportion of households’ (97%) are willing to accept and adopt a decentralized solar water disinfection treatment system. Compositional and contextual factors such as age, marital status, education, religion, and geographical location significantly contribute to households’ willingness to accept and adopt a decentralized solar water disinfection treatment system in the STK district of Ghana. Households that treat their water before use (66%, P<0.05) are more likely to accept and adopt a solar water disinfection treatment system compared to those that do not treat their water before use. The findings therefore suggest that scaling up solar water disinfection systems in the STK district is sacrosanct, and highlight the necessity to analyze compositional and contextual factors influencing willingness to accept and adopt solar water disinfection systems. Our findings will inform policies and programs aimed at implementing solar water disinfection systems in the study area to improve the health of communities that must rely on poor quality drinking water sources.
Keywords:
SODIS
; Disinfection
; Willingness to accept
; Adoption
; Sawla-Tuna-Kalba district
; Complementary log-log regression
1. Introduction
Globally, one in four people lack access to continuous safe drinking water, hence posing a major health risk [1]. A significant proportion of rural populations still consume water from unimproved sources that are largely contaminated by feacal matter [2]. The World Health Organization (WHO) reported that about 115 million people live directly on untreated surface water such as lakes, ponds, rivers and streams [3]. In sub-Saharan Africa, nearly 58% of people lack clean water that is suitable for consumption or free from pathogenic microorganisms [4]. The consumption of water from unimproved sources contributes substantially to the global burden of diarrhea and other waterborne diseases especially among children below the age of five [5].
Improving household water quality to meet recommended standards for household use are currently being researched, developed and implemented among various communities across the world to determine whether alternative water supply systems are technologically viable, economically feasible, as well as socially acceptable within rural contexts [6,7,8]. In developed countries, particularly like Germany and Japan, local governments are addressing improved water access by building greater water infrastructure around centralized water treatment systems as well as encouraging household-level installations to harvest water [9,10,11]. Developing and transition countries on the other hand, largely rely on decentralized water treatment and on-site water storage and reuse systems as the most functional options [12,13].
Several rural areas in Sub-Saharan Africa still face limited access to improved water sources. As an intermediate solution to providing safer drinking water and reduce incidence of diseases, solar water disinfection treatment systems as well as household water treatment and safe storage (HWTS) are being proposed [14,15,16,17]. Solar water disinfection treatment systems scalability as an intervention for rural communities lacking clean water access remains an active policy debate and low rates of consistent patronage have been observed [18,19,20,21].
Decentralized solar water disinfection treatment systems are recognized worldwide approaches to improving water quality before use [4,22]. These approaches have the advantage of preventing diarrhea and other waterborne diseases. Therefore, it is becoming apparent that decentralized solar water disinfection treatment systems can be of critical importance in addressing improved water access in rural communities because of their ability to provide water to individual homes, small groups of houses, and large-scale housing developments in a simple and economically feasible way [16,22,23]. However, the use of these systems is also directly influenced by community attitudes due to the immediacy of responsibility in managing decentralized water supplies [7]. Furthermore, the need to understand factors influencing households to accept and adopt alternative water systems is crucial to the successful implementation of these strategies. That is, although decentralized solar water disinfection systems may improve clean water access, there is no guarantee that the general public will willingly accept or adopt them. Unfortunately, very little is known about factors at household levels facilitating and hindering social acceptance and adoption of solar water disinfection treatment systems.
In this study, we investigate the predictors of willingness to accept and adopt a solar water disinfection treatment system as well as how household water treatment before use influence household willingness to accept and adopt a solar water disinfection treatment system while controlling for relevant compositional and contextual factors.
2. Materials and Methods
2.1. Study district
This study was carried out in the Sawla-Tuna-Kalba (STK) district of the Savannah Region of Ghana. Figure 1 represents the study district and the selected communities.
The district shares boundaries with Wa West district to the North, Bole District to the South, West Gonja District to the East and Cote D’Ivoire to the West at the Black Volta [24]. The district is estimated to have a total land area of 4,226.9 square kilometers with a population of 112,664 as at 2021 [25].
Figure 1.
Map of the study area.
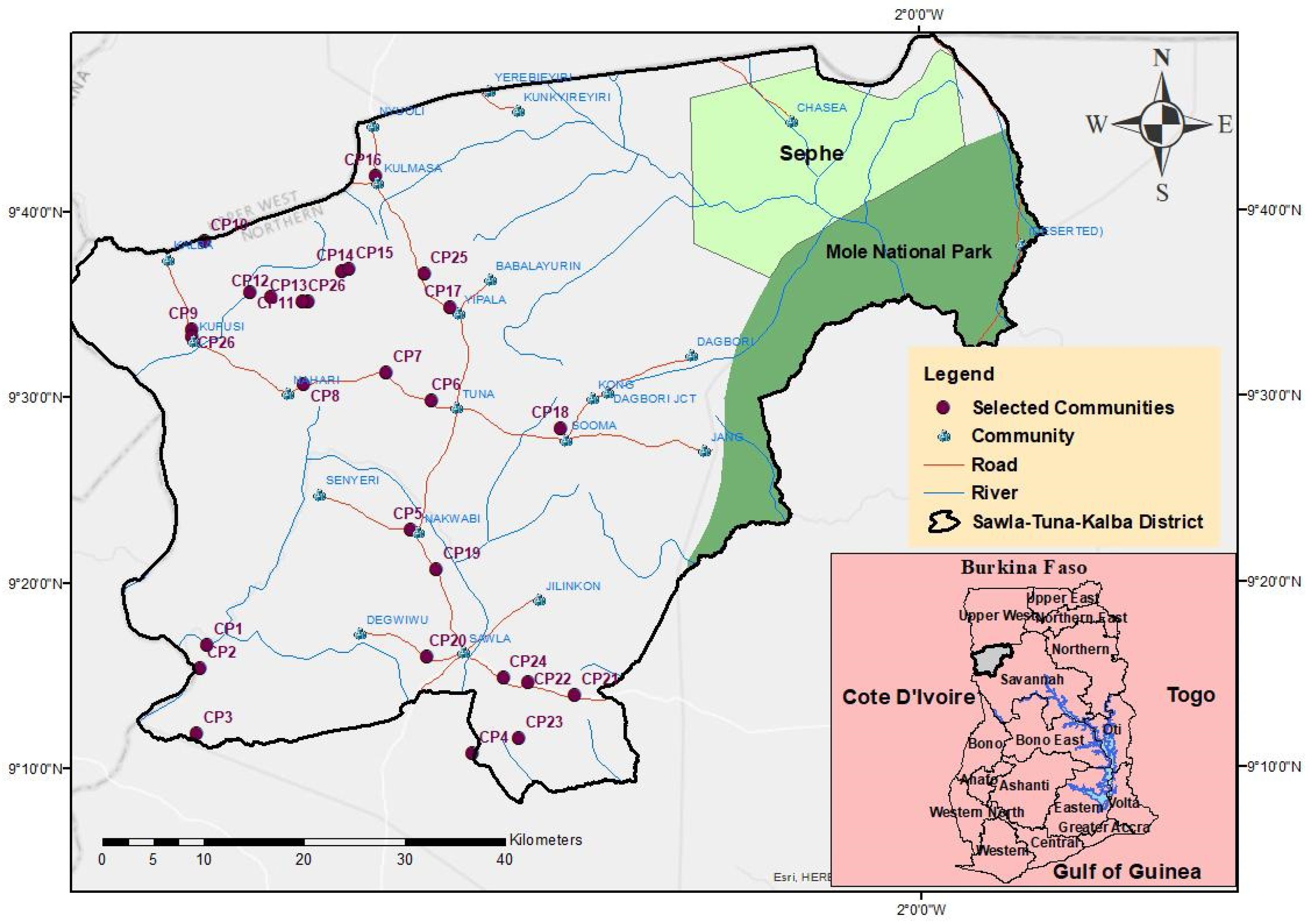
The study largely focused on rural communities. The rural population in the STK district is estimated to be around 90,133 [25] with an estimated household population of 90,068 [25]. Communities included in this study were selected based on the following selection criteria. The community must (i) be rural with household population less than 500. (ii) be part/located in the STK district. (iii) use an unimproved water source either as a primary or secondary water source. Unimproved water source in this context refers to water sources that are not protected from outside contamination especially faecal matter. Such water sources include unprotected wells, unprotected springs, rivers, dams, and lakes. Improved water sources on the other hand refers to water sources that are protected from outside contamination especially faecal matter. These water sources include household connections, standpipes, boreholes, protected dug wells and protected springs.
Twenty-seven (27) communities met the inclusion criteria defined and were therefore included in the study. The selected communities are shown in Table 1. A total of 1155 households were interviewed. A household in this study refers to a person or group of persons that have the same water arrangement or drink from the same water storage system and recognizes one as a head.
2.2. Data collection and sampling procedure
A survey instrument of 65 items was deployed on a kobo tool box and administered to households in the selected 27 communities of the STK district. Data were collected electronically using tablets. All households’ heads present during the survey period were recruited into the study as participants. Data cleaning and analyses resulted in a total sample size of 1155 households heads collected between the period of 4th May, 2024 and 9th July, 2024.
Before the administration of the survey, a pilot study was done in the Bole district that has similar attributes of the study communities. This helped identify the understandability of terminologies, identify questions that may reflect any form of bias, consistency of terms, check logical order of relevant open-ended questions, and enrich the content of the survey instrument.
2.3. Measures
A questionnaire was designed for the cross-sectional study consisting of five (5) measuring dimensions: background information including socio-demographic variables, water quality, water practice, water treatment system and barriers to the implementation of water treatment systems. The questionnaire consisted of sixty-five (65) questions in total. Cronbach’s alpha was used to measure the internal consistency and reliability of the data collated. A value of α = 0.903 was obtained.
2.4. Response variable
The response variable used in this study was willingness to accept and adopt a solar water disinfection treatment system for improving water quality for household use (coded as Willingness). Household purposes in the context of this study refers to processes such as drinking, bathing, washing of clothes and other home chores. Similarly, a solar water disinfection treatment system refers to a water system that relies on solar energy (UVA range, 315-400 nm) to disinfect water to meet the Ghana Water Company drinking water requirements and uses sunlight as its source of energy. The response variable (Willingness) was a dichotomous variable requiring a no or yes response from the respondents (household heads). These responses to this variable were coded 0 (no) and 1 (yes).
2.5. Key predictor/Explanatory variables
The key predictor variable (treatment of household water from main source before use) and all other variables were selected based on literature, parsimony, model fit, practical significance and theoretical relevance. Treatment of household water from main source before use (hereafter treatment of water) was represented as a dichotomous variable requiring respondents to answer “no = 0” or “yes = 1”.
2.6. Compositional and contextual factors
The compositional factors considered in this study were age in years (below 25, 25-30,31-37,38-44, 45-54, above 54), gender (male, female), household income (low, high) marital status (single, married, divorced, widow/widower), highest educational attainment (no formal education, primary, secondary, higher), household size (low, medium, high), and religion (Christian, muslim, traditionalist). Compositional factors consist of biosocial and sociocultural attributes of a population and whereas biosocial traits have an underlying biological or physical component, sociocultural attributes are attributes acquired by one’s position in the social system. Except individual ethnicity, all biosocial factors are rooted in biology. Biosocial factors include gender, age, race, and ethnicity. Sociocultural factors include customs, beliefs, lifestyles, income, education, occupation, and values [26,27,28].
Contextual factors simply are geographical location and or environmental conditions. For this study, contextual factors considered are communities’ zones (Sawla, Gindabuo, Kalba, Tuna/Sanyeri). For parsimony and to establish sufficient cases in each sub-group, some of the variables observed, such as Marital status (divorced and widow/widower combined), education (secondary and higher combined), were combined and recoded. Household income was measured as a continuous variable, however, for purposes of analyses it was grouped into two distinct categories using World Bank criteria, thus Low income (earn <1.9USD a day), high income (earn >1.9 USD a day) [29]. A conversion rate of 1 USD = 15 Ghana Cedis was used to extrapolate the equivalent monthly income of households from the collated data into the two distinct sub-groups (Low and high income). Household size was measured as a continuous variable but for the purposes of analysis, it was grouped into low household size (0-5 members), medium household size (6-10 members), and high household size (above 10 members). Communities zones were derived by grouping the 27 communities into four distinct zones based on their locations (Table 2).
2.7. Data and statistical analyses
The data was subjected to both univariate/descriptive (Pearson’s chi square and Cramer’s V statistics) and multivariate analyses (Complementary log-log regression) to evaluate the associations and proportions between predictor variables and households’ willingness to accept and adopt a solar water disinfection treatment system for improving household water quality before use. Additionally, the analyses assess how households’ choice of treating water from main source before use predicts their willingness to accept and adopt a solar water disinfection treatment system while controlling for theoretically relevant biosocial, sociocultural and contextual factors. All data coding, cleaning and analyses were performed using Stata 15 (StataCorp, College Station, TX, USA) SE software.
2.8. Multivariate regression
Generalized linear models (GLMs) - (complementary log-log regression models)- were run at the multivariate level to assess the relationship between households’ willingness to accept and adopt a solar water disinfection treatment system and the key predictor variable (treatment of water before use). The complementary log-log regression model is appropriate for a dependent binary response variable (no=0, yes=1) if the responses are asymmetric in the (0, 1) interval for which the affirmative is more than 55% [27,30]. Ninety-seven percent (97%) of the respondents responded “yes” to accept and adopt a solar water disinfection treatment system for improving household water quality before use. The complementary log-log regression model which requires the affirmative should be more likely, gives a better representation and was used for the analysis. The model estimations were reported as exponential coefficients- odds ratios (ORs). An OR >1 means the predictor is associated with higher odds of households’ willingness to accept and adopt a solar water disinfection treatment system; an OR=1 means that the predictor does not affect the odd of households’ willingness to accept and adopt a solar water disinfection treatment system; an OR <1 means that the predictor is associated with lower odds of households’ willingness to accept and adopt a solar water disinfection treatment system. The study employed a statistical significance level (P value) set at 0.05 with a 95% confidence interval (CI). Three models were run. Model 1 include treatment of water before use and biosocial factors, sociocultural factors (model 2), and contextual factors (model 3).
2.9. Ethical statement
The purpose of the research work was disclosed to the communities’ authorities and participants. Oral consent was obtained from each participant before the research commenced and all respondents willingly took part in the study without coercion. Local authorities and participants were made to understand how important their information could help improve continuous access to clean water.
3. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
3.1. Descriptive statistics
The distribution of households’ willingness to accept and adopt a solar water disinfection treatment system and independent variables are presented in the contingency table (Table 1). Generally, households’ willingness to accept and adopt a solar water disinfection treatment system was 97%. The results show that 99% of households that treat their water at home before use are willing to accept and adopt a solar water disinfection system while households that do not treat their water before use reported 96% willing to accept and adopt a solar water disinfection system. Households with high income and low income reported 98% and 96% willingness to accept and adopt a solar water disinfection treatment system respectively. Females and males’ proportions of willingness to accept and adopt a solar water disinfection treatment system were respectively 96% and 98%.
3.1.1. Measures of association
The observed differences in households’ willingness to accept and adopt a solar water disinfection treatment system, treatment of water before use, as well as compositional and contextual factors were evaluated using Pearson chi-square (χ2) and Cramer’s V statistic.
The Pearson chi-square statistic results (Table 3) reveals that treatment of household water before use (χ2 = 8.8863, P = 0.003), age of household head (χ2 = 19.6873, P = 0.001), marital status (χ2 = 6.0191, P = 0.049), religion (χ2 = 12.9472, P = 0.002) were all significant, signifying there is a relationship between these variables and willingness to accept and adopt a solar water disinfection treatment system. These associations however, are all weak associations as revealed by the Cramer’s V statistics (Table 3). Gender, household income, household size, highest educational attainment, community zones were not statistically significant.
3.2. Multivariate statistical analyses
Three (3) models were run at the multivariate level (Table 4). Treatment of household water before use and biosocial factors (model 1), socio-cultural factors (model 2), and contextual factors (model 3) were performed to assess their relationship with households’ willingness to accept and adopt a solar water disinfection system for improving household water quality before use. The complementary log-log regression model output (Table 4) shows the OR, robust standard error (SE), probability values, and CIs in the models.
Model 1 results indicated that households that treat their water before use are 68% more likely to accept and adopt a solar water disinfection treatment system compared to their counterparts that do not treat their water before use (OR=1.682, P<0.05). Additionally, the model revealed that household heads in the age group 38-44 (OR=0.584, P<0.05) and older (> 54 years) (OR=0.460, P<0.05) are respectively 42% and 54% less likely to accept and adopt a solar water disinfection treatment system compared to the reference group (less than 25 years).
Socio-cultural factors were controlled for in model 2. The relationship between treatment of household water before use and households’ willingness to accept and adopt a solar water disinfection treatment system remained robust. Households that treat their water before use (66%, P<0.05) are more likely to accept and adopt a solar water disinfection treatment system compared to the reference group (no treatment of water before use). The results output shows that household heads in the age categories 31-37 (59%, P<0.05), 38-44 (66%, P<0.05), 45-54 (58%, P<0.05), and Above 54 years (66%, P<0.05) were all less likely to accept and adopt a solar water disinfection treatment system compared to the reference group (<25 years). The model results equally show that married household heads (97%, P<0.05) are more likely to accept and adopt a solar water disinfection treatment system compared to their counterparts that are single. Highest educational attainment was equally controlled for in model 2. The results show that household heads that attained higher education (1.654, P<0.05) are 65% more likely to accept and adopt a solar water disinfection treatment system compared to their counterparts that had no formal education. The results also revealed that Muslim households (0.754, P<0.05) are less likely to accept and adopt a solar water disinfection treatment system compared to the reference group (Christians). Gender of household head and household size were not significant predictors of households’ willingness to accept and adopt a decentralized solar water disinfection treatment system in model 2 (Table 4).
When the contextual factor was accounted for in model 3, the odds observed in model 2 for the relationship between treatment of water before use and willingness to accept and adopt a solar water disinfection treatment system became more robust. Households that treat their water before use (66%, P<0.05) are more likely to accept and adopt a solar water disinfection treatment system compared to the reference group (no treatment of water). Households heads aged 31-37 (63%, P<0.05), 38-44 (69%, P<0.05), 45-54 (62%, P<0.05), and Above 54 years (69%, P<0.05) were all less likely to accept and adopt a solar water disinfection treatment system compared to those below 25 years category. The model output equally shows that household heads that are married (2.048, P<0.05) are more likely to accept and adopt a solar water disinfection treatment system compared to the reference group (single). Household heads with highest educational attainment (63%, P<0.05) are more likely to accept and adopt a solar water disinfection treatment system compared to the reference category (no formal education). The results also revealed that Muslim households (26%, P<0.05) are less likely to accept and adopt a solar water disinfection treatment system compared to the reference group (Christians). Gender of household head and household size were not significant predictors of households’ willingness to accept and adopt a solar water disinfection system just as observed in model 2. Households in the Kalba zone (72%, P<0.05) are more likely to accept and adopt a solar water disinfection system compared to those in the Sawla zone.
4. Discussion
This study assessed the effect of household water treatment before use on willingness to accept and adopt a decentralized solar water disinfection treatment system in selected communities in the STK district of Ghana while controlling for relevant compositional and contextual factors. There is evidence from various settings that socio-cultural factors influence the choice of drinking water and more particularly water from a solar disinfection treatment system [31,32,33,34]. Generally, households’ willingness to accept and adopt a solar water disinfection treatment system was high (97%). Different studies highlight the importance of achieving a critical 50% proportion of willingness to accept a solar water disinfection treatment system to achieve a sustained adoption [35]. Our results underscore that pre-assessments of the compositional and contextual factors that predict willingness to accept and adopt a decentralized solar water disinfection treatment system in setting-specific dimensions where no central water purification options can be provided.
As described in the studies of Luzi et al., [36] solar water disinfection treatment systems have the potential to gain acceptance of many water users worldwide who decide to apply the method for its advantages in terms of effectiveness, low cost, as well as availability and affordability of required materials. The acceptance and adoption of a particular technology for water treatment in a population is largely influenced by the receptiveness of potential adopters, characteristics of the new technology, and government policy, among others [37]. However, our findings contradict with the works of Nuño Martínez et al., [33] who reported that solar water disinfection treatment system is not desirable in rural Andean Bolivia despite its local public image as a simple, safe, low-cost means of preparing safe drinking water. The authors added that participants of the study still consume “raw” water even after asserting to the fact that “raw” water may contain pathogenic microorganisms that could cause diseases.
In Bolivia, other studies reported taste as a predictor of current and intended use of a solar water disinfection system [38,39]. Also, studies by Halperin et al., [40] in Peru believed that water from a solar water disinfection treatment system caused stomach-aches compared to piped water. A study carried out in Indonesia revealed that although solar water disinfection system was considered to provide larger economical and time-saving benefits, negative perceptions of its taste and odour hinder its adoption [41]. These differences could be as a result of some cultural norms and values that the population could be attached to.
Different acceptance and adoption proportions of solar water disinfection treatment system are reported in the literature that fall below the 97% found in this study. These differences could be attributed to several factors including the geographical location and the terminologies used in the various studies during the study periods and more importantly the availability of other improved water infrastructure. Lack of potable water in rural communities where centralized systems cannot be provided, coupled with diseases incidence are good reasons for them to accept a technology that will improve their household water quality. It is also obvious that many households in rural areas are aware of the poor quality of their water source hence, resort to treating their household water before use [21,42].
We found that household level characteristics such as treatment of household water before use, age of household head, marital status, educational attainment and religion are significant predictors of willingness to accept and adopt a solar water disinfection treatment system in the STK district of Ghana. Our findings confirm the works of Moser and Mosler [35] that found that existing knowledge about the need to treat drinking water predicted early solar water disinfection system adoption.
Older Households (greater than 25 years) heads were all less likely to accept and adopt a solar water disinfection treatment system compared to those below 25 years category. Older people are more tied to their beliefs and custom values. They turn to argue about the feasibility of emerging technologies and the health impacts, therefore do not readily accept new technologies compared to younger individuals.
Married household heads are more likely to accept and adopt a solar water disinfection treatment system compared to their counterparts that are single. Married individuals in Ghana and more particularly the study district have larger household sizes compared with single household heads [43]. The higher household size means a greater demand for water to meet the needs of the household members. This implies that, treatment of household water before use at the household level will require greater efforts and resources compared to single households. Christen et al., [44] in their study found that households that were more likely to use solar water disinfection system were those that included women.
Household heads with highest educational attainment have higher odds of accepting and adopting a solar water disinfection treatment system compared to their counterparts with no formal education. This may be attributed to the fact that educated people appreciate the benefits and cost of using improved household water. Nonetheless, highly educated people are more hesitant to accept that solar water disinfection could provide drinking water free of microbial contaminants and hence, needed to be convinced with examples from field demonstrations in different settings [16]. These findings align with the work by Meierhofer and Landolt, [45]. The authors reported that more highly educated people, such as teachers, health workers or village leaders, were more difficult to convince that solar water disinfection system can efficiently treat drinking water. Solar water disinfection demonstrations in Bolivia and Nepal as well as a project evaluation in Kenya reported that once doubts on disinfection efficiency are dispelled, people with higher education and economic statuses are more likely to adopt a solar disinfection treatment system [45,46]. A field study by Altherr et al., [47] in Nicaragua, revealed that the intention to use a solar disinfection system and the actual use of a solar disinfection system are mainly dependent on the overall positive attitude and ability to inspire confidence in the new technology.
Our results suggest that there are substantial geographical inequalities in willingness to accept and adopt a solar water disinfection treatment system across the STK district. This probably could be influenced by the differences in economic growth, infrastructure development, government and nongovernmental organizations interventions etc. in the district [34,48]. As communities in the Sawla zone see more improved water infrastructure like pipe and boreholes in the district capital (Sawla) they would preferably wish for similar water infrastructure in their communities. Additionally, several communities lacking improved water sources are being promised of boreholes or other improved water sources by political parties (respondents assert). Promises of political parties for power to rule the district are unfulfilled and therefore makes some communities to prefer one water treatment technology to another. This is not different in the STK district. It is therefore clear that, communities in the Sawla zone have other alternative improved water sources compared to those in the Kalba zone. Studies have shown that governments and relevant stakeholders needs to deliberately adopt strategies that target deprived areas and population groups in order to achieve universal improved water coverage [48,49]. It is therefore important that government and other organisations which are into the provision of potable water can consider decentralized solar water disinfection treatment systems.
5. Limitations of the study
In this study, we identified some compositional and contextual predictors of adoption and acceptance of decentralized solar water disinfection treatment system in the STK district applying quantitative methods. The design of this study did not allow making any inference to governmental supports and legal frameworks as well as characteristics of the new technology. Different authors heighted other factors that are associated with implementation and adoption of a solar water disinfection treatment system [37]. Adopting a multi-level perspective when studying the acceptance and adoption of a solar water disinfection treatment system, such as the analysis of enabling environments and other system factors, economic opportunities, and drivers of behaviour change is critical [33]. To holistically assess the willingness to accept and adopt a solar water treatment system to possibly lead to the implementation of such systems in communities lacking potable water, the barriers and enabling factors need to be assessed. Future research designs in the same study district focusing on the barriers and enabling factors to implementing a solar water disinfection treatment system would provide better evidence for in-depth conclusions to be drawn on implementation and adoption of solar water treatment systems in the STK district.
6. Conclusions
This current study examined the effects of household water treatment before use on willingness to accept and adopt a decentralized solar water disinfection treatment system in selected communities in the STK district of Ghana. Based on our findings, a greater proportion of households’ (97%) are willing to accept and adopt a decentralized solar water disinfection treatment system. Compositional and contextual factors such as age, marital status, education, religion, geographical location significantly contribute to households’ willingness to accept and adopt a decentralized solar water disinfection treatment system in the STK district of Ghana. Households that treat their water before use are more likely to accept and adopt a solar water disinfection treatment system compared to their counterparts that do not treat their household water before use. Older Households heads were all less likely to accept and adopt a solar water disinfection treatment system compared to those below 25 years category. Married household heads are more likely to accept and adopt a solar water disinfection treatment system compared to their counterparts that are single. Household heads with highest educational attainment are more likely to accept and adopt a solar water disinfection treatment system compared to the reference category (no formal education). Households in the Kalba zone are more likely to accept and adopt a solar water disinfection system compared to those in the Sawla zone. The findings in this study reveals that scaling up solar water disinfection systems in the STK district is sacrosanct, and highlight the necessity to analyze compositional and contextual factors influencing willingness to accept and adopt solar water disinfection systems. Our findings will inform policies and programs aimed at implementing solar water disinfection systems in the study area to improve the health of communities that must rely on poor quality drinking water sources. We recommend that future research designs in the same study district should focus on the barriers and enabling factors to implementing a solar water disinfection treatment system to provide better evidence for in-depth conclusions to be drawn on implementation and adoption of solar water treatment systems in the STK district.
Author Contributions
Conceptualization, Abdul-Rahaman Afitiri.; methodology, Abdul-Rahaman Afitiri.; Ernest Kofi Amankwa Afrifa; software, Abdul-Rahaman Afitiri.; validation, Abdul-Rahaman Afitiri., Ernest Kofi Amankwa Afrifa; formal analysis, Abdul-Rahaman Afitiri.; investigation, Abdul-Rahaman Afitiri.; resources, Abdul-Rahaman Afitiri and Ernest Kofi Amankwa Afrifa.; data curation, Abdul-Rahaman Afitiri; writing—original draft preparation, Abdul-Rahaman Afitiri and Ernest Kofi Amankwa Afrifa; writing—review and editing, Abdul-Rahaman Afitiri and Ernest Kofi Amankwa Afrifa; visualization, Abdul-Rahaman Afitiri.; supervision, Ernest Kofi Amankwa Afrifa; project administration, Abdul-Rahaman Afitiri. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data that support the findings of this study are available on request from the corresponding author.
Acknowledgments
The authors are grateful to the Field Assistants- Dery Kelvin, Iddrisu Abubakari Afitiri, Seidu Issah, and Seidu Haruna for supporting in the data collection process. Abdul-Rahaman Afitiri expresses his gratitude to the Graduate Research School (GRS) of the Brandenburg University of Technology and Deutscher Akademischer Austauschdienst (DAAD) for the financial support for his PhD and fieldwork.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- H. Ritchie, F. Spooner, and M. Roser, “Clean water,” Our World Data, Jan. 2024, Accessed: Aug. 09, 2024. [Online]. Available: https://ourworldindata.org/clean-water.
- D. L. Crispim, M. F. Progênio, and L. L. Fernandes, “Proposal for a tool for assessing access to water in rural communities: a case study in the brazilian semi-arid,” Environ. Manage., vol. 69, no. 3, pp. 529–542, Mar. 2022. [CrossRef]
- WHO, “Drinking-water.” Accessed: Aug. 09, 2024. [Online]. Available: https://www.who.int/news-room/fact-sheets/detail/drinking-water.
- B. D. Bitew, Y. K. Gete, G. A. Biks, and T. T. Adafrie, “Barriers and Enabling Factors Associated with the Implementation of Household Solar Water Disinfection: A Qualitative Study in Northwest Ethiopia,” Am. J. Trop. Med. Hyg., vol. 102, no. 2, pp. 458–467, Feb. 2020. [CrossRef]
- S. L. McGuinness et al., “Household water storage management, hygiene practices, and associated drinking water quality in rural India,” Environ. Sci. Technol., vol. 54, no. 8, pp. 4963–4973, Apr. 2020. [CrossRef]
- A. Q. Jones et al., “Public perceptions of drinking water: a postal survey of residents with private water supplies,” BMC Public Health, vol. 6, no. 1, p. 94, Apr. 2006. [CrossRef]
- A. Mankad and S. Tapsuwan, “Review of socio-economic drivers of community acceptance and adoption of decentralised water systems,” J. Environ. Manage., vol. 92, no. 3, pp. 380–391, 2011. [CrossRef]
- M. A. Massoud, A. Tarhini, and J. A. Nasr, “Decentralized approaches to wastewater treatment and management: Applicability in developing countries,” J. Environ. Manage., vol. 90, no. 1, pp. 652–659, Jan. 2009. [CrossRef]
- E. Ghisi and S. Mengotti de Oliveira, “Potential for potable water savings by combining the use of rainwater and greywater in houses in southern Brazil,” Build. Environ., vol. 42, no. 4, pp. 1731–1742, Apr. 2007. [CrossRef]
- J. Mwenge Kahinda, A. E. Taigbenu, and J. R. Boroto, “Domestic rainwater harvesting to improve water supply in rural South Africa,” Phys. Chem. Earth Parts ABC, vol. 32, no. 15, pp. 1050–1057, Jan. 2007. [CrossRef]
- E. Nolde, “Possibilities of rainwater utilisation in densely populated areas including precipitation runoffs from traffic surfaces,” Desalination, vol. 215, no. 1, pp. 1–11, Sep. 2007. [CrossRef]
- R. Chen and X. C. Wang, “Cost–benefit evaluation of a decentralized water system for wastewater reuse and environmental protection,” Water Sci. Technol., vol. 59, no. 8, pp. 1515–1522, Apr. 2009. [CrossRef]
- D. Zhang, R. M. Gersberg, C. Wilhelm, and M. Voigt, “Decentralized water management: rainwater harvesting and greywater reuse in an urban area of Beijing, China,” Urban Water J., vol. 6, no. 5, pp. 375–385, Nov. 2009. [CrossRef]
- A.-R. Afitiri, S. Appah Aram, and M. Martienssen, “Systematic review of the effects of advanced oxidation processes integration with solar water disinfection for improved drinking water production,” Waste Manag. Bull., vol. 1, no. 4, pp. 52–59, Mar. 2024. [CrossRef]
- Z. Burt et al., “User preferences and willingness to pay for safe drinking water: Experimental evidence from rural Tanzania,” Soc. Sci. Med., vol. 173, pp. 63–71, Jan. 2017. [CrossRef]
- C. Hendrickson et al., “Decentralized solar-powered drinking water ozonation in Western Kenya: an evaluation of disinfection efficacy,” Gates Open Res., vol. 4, p. 56, 2020. [CrossRef]
- J. Wolf et al., “Systematic review: Assessing the impact of drinking water and sanitation on diarrhoeal disease in low- and middle-income settings: systematic review and meta-regression,” Trop. Med. Int. Health, vol. 19, no. 8, pp. 928–942, 2014. [CrossRef]
- J. Brown, S. Proum, and M. D. Sobsey, “Sustained use of a household-scale water filtration device in rural Cambodia,” J. Water Health, vol. 7, no. 3, pp. 404–412, May 2009. [CrossRef]
- S. P. Luby, C. Mendoza, B. H. Keswick, T. M. Chiller, and R. M. Hoekstra, “Difficulties in bringing point-of-use water treatment to scale in rural Guatemala,” Am. J. Trop. Med. Hyg., vol. 78, no. 3, pp. 382–387, 2008.
- W.-P. Schmidt, “The elusive effect of water and sanitation on the global burden of disease,” Tropical Medicine & International Health, vol. 19, no. 5. pp. 522–527, 2014. Accessed: Aug. 21, 2024. [Online]. Available: https://fr.ircwash.org/sites/default/files/elusive-2014-schmidt.pdf.
- W.-P. Schmidt and S. Cairncross, “Household water treatment in poor populations: is there enough evidence for scaling up now?,” Environ. Sci. Technol., vol. 43, no. 4, pp. 986–992, Feb. 2009. [CrossRef]
- B. J. M. Chaúque and M. B. Rott, “Solar disinfection (SODIS) technologies as alternative for large-scale public drinking water supply: Advances and challenges,” Chemosphere, vol. 281, p. 130754, Oct. 2021. [CrossRef]
- S. Cook, G. Tjandraatmadja, A. Ho, and A. Sharma, Definition of decentralised systems in the South East Queensland context. Urban Water Security Research Alliance Brisbane, Australia, 2008. Accessed: Aug. 20, 2024. [Online]. Available: https://sswm.info/sites/default/files/reference_attachments/COOK%20et%20al%202009%20Definition%20of%20Decentralised%20Systems%20in%20the%20South%20East%20Queensland%20Context.pdf.
- G. S. S. GSS, 2010 Population & Housing Census: Demographic, Social, Economic & Housing Characteristics. Ghana Statistical Service, 2013.
- GSS, “Ghana 2021 population and housing census general report volume 3A.” 2021. [Online]. Available: https://statsghana.gov.gh/gssmain/fileUpload/pressrelease/2021%20PHC%20General%20Report%20Vol%203A_Population%20of%20Regions%20and%20Districts_181121.pdf.
- D. F. Ahadzi, A.-R. Afitiri, and E. Ahadzi, “Organizational safety culture perceptions of healthcare workers in Ghana: A cross-sectional interview study,” Int. J. Nurs. Stud. Adv., vol. 3, p. 100020, Nov. 2021. [CrossRef]
- F. A. Armah, B. Ekumah, D. O. Yawson, J. O. Odoi, A.-R. Afitiri, and F. E. Nyieku, “Access to improved water and sanitation in sub-Saharan Africa in a quarter century,” Heliyon, vol. 4, no. 11, p. e00931, Nov. 2018. [CrossRef]
- L. G. Pol and R. K. Thomas, The demography of health and health care. Springer Science & Business Media, 2001.
- World Bank, Monitoring Global Poverty: Report of the Commission on Global Poverty. The World Bank, 2016. [CrossRef]
- I. M. Bryant and A.-R. Afitiri, “Household willingness to adopt a single-stage solar-supported hyper-thermophilic anaerobic biogas digester in Ghana,” Energy Sustain. Soc., vol. 11, no. 1, p. 16, May 2021. [CrossRef]
- M. de França Doria, “Factors influencing public perception of drinking water quality,” Water Policy, vol. 12, no. 1, pp. 1–19, Nov. 2009. [CrossRef]
- M. Kaplan, “Lonely drinking fountains and comforting coolers: Paradoxes of water value and ironies of water use,” Cult. Anthropol., vol. 26, no. 4, pp. 514–541, 2011. [CrossRef]
- N. Nuño Martínez et al., “The meanings of water: socio-cultural perceptions of solar disinfected (SODIS) drinking water in Bolivia and implications for its uptake,” Water, vol. 12, no. 2, Art. no. 2, Feb. 2020. [CrossRef]
- A. Yasar, N. Y. Khan, A. Batool, A. B. Tabinda, R. Mehmood, and A. Iqbal, “Women perception of water quality and its impacts on health in Gangapur, Pakistan,” Pak. J. Nutr., vol. 10, no. 7, pp. 702–706, Jun. 2011. [CrossRef]
- S. Moser and H.-J. Mosler, “Differences in influence patterns between groups predicting the adoption of a solar disinfection technology for drinking water in Bolivia,” Soc. Sci. Med., vol. 67, no. 4, pp. 497–504, 2008. [CrossRef]
- S. Luzi, P. Gurung, R. Meierhofer, and M. Wegelin, “User acceptance: the key to evaluating SODIS and other methods for household water treatment and safe storage,” 2009, Accessed: Jul. 29, 2024. [Online]. Available: https://repository.lboro.ac.uk/articles/User_acceptance_the_key_to_evaluating_SODIS_and_other_methods_for_household_water_treatment_and_safe_storage/9585584/files/17224250.pdf.
- P. O’Callaghan, G. Daigger, L. Adapa, and C. Buisman, “Development and application of a model to study water technology adoption,” Water Environ. Res., vol. 90, no. 6, pp. 563–574, 2018. [CrossRef]
- S. Heri and H.-J. Mosler, “Factors affecting the diffusion of solar water disinfection: a field study in Bolivia,” Health Educ. Behav. Off. Publ. Soc. Public Health Educ., vol. 35, no. 4, pp. 541–560, Aug. 2008. [CrossRef]
- A. Tamas and H.-J. Mosler, “Why do people stop treating contaminated drinking water with Solar Water Disinfection (SODIS)?,” Health Educ. Behav. Off. Publ. Soc. Public Health Educ., vol. 38, no. 4, pp. 357–366, Aug. 2011. [CrossRef]
- M. Halperin, V. A. Paz-Soldán, V. Quispe, A. Paxton, and R. H. Gilman, “Sustainability of solar disinfection to provide safe drinking water in rural Peru,” Public Health Rep. Wash. DC 1974, vol. 126, no. 5, pp. 762–768, Oct. 2011. [CrossRef]
- E. Roma, T. Bond, and P. Jeffrey, “Factors involved in sustained use of point-of-use water disinfection methods: a field study from Flores Island, Indonesia,” J. Water Health, vol. 12, no. 3, pp. 573–583, Feb. 2014. [CrossRef]
- A. A. Azamzam et al., “Insights into solar disinfection enhancements for drinking water treatment applications,” Sustainability, vol. 13, no. 19, Art. no. 19, Jan. 2021. [CrossRef]
- M. Kpessa-Whyte, “Aging and demographic transition in Ghana: State of the elderly and emerging issues,” The Gerontologist, vol. 58, no. 3, pp. 403–408, May 2018. [CrossRef]
- A. Christen et al., “Factors associated with compliance among users of solar water disinfection in rural Bolivia,” BMC Public Health, vol. 11, p. 210, Apr. 2011. [CrossRef]
- R. Meierhofer and G. Landolt, “Factors supporting the sustained use of solar water disinfection — Experiences from a global promotion and dissemination programme,” Desalination, vol. 248, no. 1, pp. 144–151, Nov. 2009. [CrossRef]
- R. C. Rainey and A. K. Harding, “Drinking water quality and solar disinfection: effectiveness in peri-urban households in Nepal,” J. Water Health, vol. 3, no. 3, pp. 239–248, Sep. 2005. [CrossRef]
- A.-M. Altherr, H.-J. Mosler, R. Tobias, and F. Butera, “Attitudinal and relational factors predicting the use of solar water disinfection: a field study in Nicaragua,” Health Educ. Behav., vol. 35, no. 2, pp. 207–220, Apr. 2008. [CrossRef]
- R. L. Pullan, M. C. Freeman, P. W. Gething, and S. J. Brooker, “Geographical Inequalities in Use of Improved Drinking Water Supply and Sanitation across Sub-Saharan Africa: Mapping and Spatial Analysis of Cross-sectional Survey Data,” PLoS Med., vol. 11, no. 4, p. e1001626, Apr. 2014. [CrossRef]
- T. T. Tuyet-Hanh et al., “Household trends in access to improved water sources and sanitation facilities in Vietnam and associated factors: findings from the Multiple Indicator Cluster Surveys, 2000–2011,” Glob. Health Action, vol. 9, no. 1, p. 29434, Dec. 2016. [CrossRef]

Table 1.
Selected communities in the STK district.
| ID | Community | ID | Community | ID | Community |
| CP 1 | Liimetey | CP 11 | Vomgbe | CP 21 | Nasoyiri |
| CP 2 | Jambar | CP 12 | Jingo | CP 22 | Jobriyiri |
| CP 3 | Tuonbo | CP 13 | Paradori | CP 23 | Nyangekura |
| CP 4 | Konkrompe | CP 14 | Negber | CP 24 | Nyange |
| CP 5 | Nakwabi | CP 15 | Kancheng | CP 25 | Neon |
| CP 6 | Naafa | CP 16 | Kulmasa | CP 26 | Vondiel |
| CP 7 | Nahari | CP 17 | Yipala | CP 27 | Kalba |
| CP 8 | Kunfunsi | CP 18 | Soma | ||
| CP 9 | Jokolpo | CP 19 | Blema | ||
| CP 10 | Jieyiri | CP 20 | Digzie |
Table 2.
Communities zones.
| Zone | Community |
| Sawla | Blema, Digzie, Jambar, Jobriyiri, Konkrompe, Liimetey, Nyange, Nyage kura |
| Gindabuo | Jokokura, Vomgbe, Paradore, Negber, Kancheng, Ne-on, Vondiel |
| Kalba | Nasoyiri, Tuonbo, Kunfunsi, Jeiyiri, Jingo, Kalba |
| Tuna/Sanyeri | Nafaa, Nakwabi, Nahare, Yipala, Soma, Jokolpo |
Table 3.
Percentage distribution of households’ willingness to accept and adopt a solar water disinfection system by predictor values (n=1155).
Table 3.
Percentage distribution of households’ willingness to accept and adopt a solar water disinfection system by predictor values (n=1155).
| Variable | Households willingness to accept and adopt a solar water disinfection system | ||
|---|---|---|---|
| No (%) | Yes (%) | Inferential Statistics | |
| Treatment of water from main source | |||
| No | 4 | 96 | Pearson chi2 = 8.8863 (Pr=0.003; Cramér's V =0.0877) |
| Yes | 1 | 99 | |
| Household income | |||
| Low | 4 | 96 | Pearson chi2 = 3.8081 (Pr=0.051; Cramér's V =0.0574) |
| High | 2 | 98 | |
| Sex | |||
| Male | 2 | 98 | Pearson chi2 = 3.5575 (Pr = 0.059; Cramér's V =-0.0555) |
| Female | 4 | 96 | |
| Age group (years) | |||
| 24 and below | 1 | 99 | Pearson chi2 = 19.6873 (Pr = 0.001; Cramér's V =0.1306) |
| 25-30 | 1 | 99 | |
| 31-37 | 2 | 98 | |
| 38-44 | 5 | 95 | |
| 45-54 | 3 | 97 | |
| 55 and above | 10 | 90 | |
| Highest educational attainment | |||
| No education | 4 | 96 | Pearson chi2 = 97.4883 (Pr = 0.000; Cramér's V = 0.0785) |
| Primary | 4 | 96 | |
| Secondary | 0 | 100 | |
| Higher | 1 | 99 | |
| Marital status | |||
| Single | 1 | 99 | Pearson chi2 = 6.0191 (Pr = 0.049; Cramér's V =0.0722) |
| Maried | 3 | 97 | |
| Divorced/Widow/Widower | 8 | 92 | |
| Household size | |||
| Small (0-5) | 2 | 98 | Pearson chi2 = 1.9855 (Pr = 0.371; Cramér's V =0.0417) |
| Medium (6-10) | 4 | 96 | |
| Large (>11) | 4 | 96 | |
| Religion | |||
| Christian | 2 | 98 | Pearson chi2 = 12.9472 (Pr = 0.002; Cramér's V =0.1059) |
| Muslim | 5 | 95 | |
| Traditional | 12 | 88 | |
| Community zones | |||
| Sawla | 3 | 97 | Pearson chi2 = 3.5461 (Pr=0.315; Cramér's V =0.0554) |
| Gindabuo | 3 | 97 | |
| Kalba | 1 | 99 | |
| Tuna/Sanyeri | 4 | 96 | |
| n | 1155 | ||
Table 4.
Complementary log-log regression model showing the relationship between households’ willingness to accept and adopt a solar water disinfection system and household characteristics.
Table 4.
Complementary log-log regression model showing the relationship between households’ willingness to accept and adopt a solar water disinfection system and household characteristics.
| Variable | Treatment of water before use + Biosocial factors | + Socio-cultural factors | + Contextual factors | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | SE | P value | Conf. Interval | OR | SE | P value | Conf. Interval | OR | SE | P value | Conf. Interval | ||||
| Model 1 | MODEL 2 | MODEL 3 | |||||||||||||
| Treat household water before usage (ref: No) | |||||||||||||||
| Yes | 1.682 | 0.326 | 0.007 | 1.151 | 2.4584 | 1.663 | 0.305 | 0.006 | 1.161 | 2.383 | 1.662 | 0.289 | 0.003 | 1.182 | 2.337 |
| Sex (ref: Male) | |||||||||||||||
| Female | 0.826 | 0.089 | 0.076 | 0.669 | 1.0201 | 0.846 | 0.101 | 0.163 | 0.669 | 1.070 | 0.802 | 0.097 | 0.068 | 0.633 | 1.017 |
| Age group (ref: <25 years) | |||||||||||||||
| 25-30 | 1.0496 | 0.3042 | 0.867 | 0.595 | 1.852 | 0.837 | 0.321 | 0.642 | 0.394 | 1.776 | 0.799 | 0.313 | 0.567 | 0.370 | 1.722 |
| 31-37 | 0.7286 | 0.1776 | 0.194 | 0.452 | 1.175 | 0.410 | 0.155 | 0.019 | 0.195 | 0.861 | 0.374 | 0.149 | 0.014 | 0.171 | 0.817 |
| 38-44 | 0.5836 | 0.1369 | 0.022 | 0.369 | 0.924 | 0.343 | 0.133 | 0.006 | 0.160 | 0.733 | 0.308 | 0.124 | 0.004 | 0.140 | 0.680 |
| 45-54 | 0.6989 | 0.1716 | 0.145 | 0.432 | 1.131 | 0.424 | 0.171 | 0.034 | 0.192 | 0.936 | 0.380 | 0.160 | 0.022 | 0.166 | 0.869 |
| >54 | 0.4601 | 0.1386 | 0.010 | 0.255 | 0.830 | 0.342 | 0.153 | 0.016 | 0.142 | 0.822 | 0.306 | 0.143 | 0.011 | 0.123 | 0.764 |
| Household income (ref: Low) | |||||||||||||||
| High | 1.113 | 0.140 | 0.394 | 0.870 | 1.424 | 1.171 | 0.155 | 0.231 | 0.904 | 1.517 | |||||
| Marital status (ref: Single) | |||||||||||||||
| Married | 1.996 | 0.521 | 0.008 | 1.197 | 3.330 | 2.048 | 0.558 | 0.009 | 1.200 | 3.493 | |||||
| Divorced/Widow/Widower | 1.702 | 0.562 | 0.107 | 0.891 | 3.252 | 1.791 | 0.625 | 0.095 | 0.904 | 3.548 | |||||
| Highest Educational (ref: No formal education) | |||||||||||||||
| Primary | 0.874 | 0.140 | 0.401 | 0.638 | 1.197 | 0.803 | 0.133 | 0.185 | 0.581 | 1.111 | |||||
| Higher | 1.654 | 0.307 | 0.007 | 1.150 | 2.379 | 1.633 | 0.327 | 0.014 | 1.102 | 2.418 | |||||
| Household size (ref: Low (0-5)) | |||||||||||||||
| Medium (6-10) | 0.948 | 0.118 | 0.667 | 0.743 | 1.209 | 0.919 | 0.118 | 0.509 | 0.715 | 1.181 | |||||
| High (>11) | 0.962 | 0.171 | 0.827 | 0.679 | 1.363 | 0.960 | 0.172 | 0.818 | 0.675 | 1.363 | |||||
| Religion (ref: Christian) | |||||||||||||||
| Muslim | 0.754 | 0.106 | 0.044 | 0.573 | 0.992 | 0.736 | 0.109 | 0.039 | 0.550 | 0.985 | |||||
| Traditional | 0.654 | 0.170 | 0.102 | 0.393 | 1.089 | 0.675 | 0.172 | 0.124 | 0.409 | 1.113 | |||||
| Communities zones (ref: Sawla) | |||||||||||||||
| Gindabuo | 1.043 | 0.159 | 0.784 | 0.773 | 1.406 | ||||||||||
| Kalba | 1.715 | 0.311 | 0.003 | 1.203 | 2.446 | ||||||||||
| Tuna/Sanyeri | 0.996 | 0.132 | 0.976 | 0.769 | 1.291 | ||||||||||
| n | 1155 | 1155 | 1155 | ||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



