Submitted:
06 October 2024
Posted:
07 October 2024
You are already at the latest version
Abstract
Diffuse lipomatosis of the thyroid (DLT) is a rare condition characterized by the infiltration of thyroid parenchyma with mature adipose cells, replacing normal follicular structure. Though uncommon, it often presents as neck swelling or compression symptoms such as dyspnea, dysphagia, and hoarseness, complicating diagnosis. This case study details a 61-year-old female patient with DLT, who presented with a multinodular goiter and progressive neck swelling, and reviews 53 additional cases from the literature. The review reveals that DLT is often misdiagnosed due to its overlapping features with other thyroid pathologies. The exact pathophysiological mechanism remains unclear, but hypotheses include tissue hypoxia, embryological malformations, or lipid metabolism disturbances. Surgical excision is the most common treatment, particularly for symptomatic patients, yielding positive long-term results. Future research should focus on clarifying DLT’s exact etiology and improving diagnostic accuracy, especially in differentiating it from other fat-infiltrated thyroid lesions such as amyloid goiter and adenolipomas. Enhanced understanding will guide better management strategies and improve patient outcomes in this rare yet significant thyroid disorder.
Keywords:
diffuse lipomatosis
; thyroid
; amyloid goiter
; case report
; review
1. Introduction
Diffuse lipomatosis of the thyroid or DLT is characterized by infiltration of the parenchyma of the gland and replacement of the otherwise typical anatomical structure with mature adipose cells. It is not commonly found among other pathological conditions of the thyroid but nonetheless presents an interesting phenomenon. Although the thyroid is closely connected to other mesodermal structures during embryogenesis, contributing to fat deposition in areas around the cervical blood vessels in the subcapsular region of the anterior thyroid region, the presence of significant amounts of adipocytes within the thyroid stroma is rare [1,2,3,4]. Diffuse adipose tissue causing enlargement is often found in the thymus, parathyroid glands, pancreas and salivary glands, as a result of atrophy-related parenchymal fatty metaplasia, whereas thyrolipoma is the most common condition in the thyroid [5,6,7]. Adenolipomas of the thyroid or thyrolipomas are well-circumscribed admixtures of adipose and follicular cells surrounded by a fibrous capsule consisting of a mixed neoplasm that is, mesenchymo-epithelial [4]. Both thyrolipomas and diffuse lipomatosis are benign lesions of the gland, with the latter being more frequently associated with escalating growth clinically manifesting with compression symptoms from nearby organs such as dyspnea, hoarseness, dysphagia, and overall swelling. The enlargement observed in acquired and congenital goiters may also be caused by fat invasion rather than follicular proliferation [8,9]. The exact pathophysiological mechanism responsible for the diffuse nature of the fatty infiltration of the thyroid remains unclear. Here, we present an indigenous case and review the literature on DLT.
2. Case Report
Our case involves a 61-year-old woman who was referred to our department for a total thyroidectomy. She had been diagnosed with a substernal multinodular goiter two years ago and in the last six months she gradually developed neck swelling, dyspnea, and dysphagia. Her medical history showed that she had chronic renal failure of unknown etiology and had been undergoing hemodialysis for the last year. She was also diagnosed with hypertension, diabetes mellitus and obesity [BMI(Body mass index): 37]. Her thyroid function was normal [TSH (Thyroid Stimulating Hormone): 0.46 pmol/l, FT4 (Free Thyroxine): 20.09 pmol/l, FT3 (Free Triiodothyronine): 3.1 pmol/l)] and she tested negative for serum thyroperoxidase (anti-TPO) and thyroglobulin antibodies (anti-TG). Ultrasonography findings indicated a heterogeneous intrathoracic diffuse goiter and in accordance the CT (Computed Tomography) confirmed the presence of an enlarged gland showing low attenuation and septations. Computed tomography revealed that the thyroid had invaded the entire cervical area and the upper mediastinum compressing the surrounding tissue (Figure 1). Thyroid scintigraphy with Tc99m (Technetium-99m) revealed a low uptake of radioactivity and cold nodules in the lower lobes suggesting the possibility of subacute thyroiditis. The patient underwent total thyroidectomy. The operation lasted for 2 hours and proved to be an arduous challenge. Intraoperatively the thyroid was friable at touch, its capsule was very thin, and the gland was soft-fatty in texture, similar to a lipoma (Figure 2). Following surgery, the patient experienced no complications and was released two days later. Histopathological examination revealed fatty infiltration of the thyroid gland and degeneration of follicles. Immunohistochemical staining for thyroglobulin (TG) and thyroid transcription factor-1 (TTF1) verified the existence of a few colloid-filled thyroid follicles, whereas positive S100 staining demonstrated the preponderance of adipose tissue within the gland. (Figure 3). Therefore, the patient was diagnosed with diffuse thyroid lipomatosis. Two years after surgical treatment, the patient died because of complications associated with kidney failure.
3. Review
The first description of DLT in medical literature was by Dhayagude [10] in 1942. Since then, we have identified another 53 cases of thyroid lipomatosis including our own. Based on our criteria, we identified common characteristics among the above reports including sex, age, symptoms, thyroid function, renal status, initial diagnosis, treatment, histopathological features and follow-up. Nine of the patients (16%) were described by Ge [1], two in 2016 by Bell [11], and more recently 3 cases by Celik [8]. The average age was 50 years (range, 11 - 78 years), and there was no significant sex predilection between male (47%) and female (53%). The most significant clinical feature was local compression (60%), which involved dysphagia, dysphonia/hoarseness, dyspnea, and neck swelling (46.7%), whereas one-third of the patients did not show any symptoms. Thyroid function was uncompromised in most patients (66%), and only a few patients had hypothyroidism (12.7%) or hyperthyroidism (21.3%). What appeared to be of notice was the fact that 40% of patients suffered from renal failure with most of them being affected by secondary amyloidosis. Amyloid goiter is found more frequently in secondary amyloidosis than in primary amyloidosis and is commonly misdiagnosed as a thyroid carcinoma [12]. Many patients were initially diagnosed with goiter (64.6%) either diffuse or multinodular, and one patient reported an amyloid goiter (2.1%), while a diagnosis of DLT was recently proposed in eight reports (16.7%). Among the reports that mentioned a treatment method, total thyroidectomy was the predominant choice (47.9%). Only one patient with a preliminary diagnosis of DLT was discharged without treatment, and partial thyroidectomy was an alternative, especially in patients with unilateral nodular disease. The average thyroid weight was 232.16 grams (range 15-700 g). All cases revealed that the thyroid was almost entirely composed of mature adipose cells, and in cases of amyloid infiltration, the confirmation consisted of positive Congo red or thioflavin staining. Fat deposits that vary in amount are frequently found in amyloid goiter [7]. Amyloid infiltration was observed in almost half of patients (44.8%). We only included reports in which the gland was almost completely or in most parts infiltrated by fat tissue regardless of amyloid deposition, fibrosis, or lymphocyte aggregates. Only a minority of reports (43.4%) included follow-up information, and most (78.3%) had an uncomplicated post-operative course ranging from 1 day to 12 months. One patient reported respiratory difficulty 3 years after the first evaluation, three others died of complications, two pertaining to renal insufficiency and the other after developing metastases in the residual thyroid lobe. Finally, a DLT case with concurrent secondary amyloidosis was revealed via the patient’s autopsy. Table 1 summarizes the characteristics of the DLT in these patients (Table 1).
4. Discussion
Numerous attempts have been made to explain the etiology of fatty infiltration in the thyroid gland. According to Dhayagude,[10] fat deposits in colloid goiters may arise from the degeneration of follicular tissue due to damage such as hemorrhage, fibrosis, infarction, calcification, or cystic degeneration. Willis [13] in his textbook “The borderland of Embryology and Pathology” describes an adenolipoma explaining that its presence could be a result of the metaplastic formation of fat. In amyloid goiters, it is presumed that adipose tissue is formed from stromal metaplasia of fibroblasts as a result of senile involution or tissue hypoxia [14]. Trites [15] hypothesized that some factor may have affected the primitive foregut during embryogenesis causing the formation of mixed embryonic tumors explaining fatty infiltration in congenital goiters. In various lipomas it has been suggested that a disturbance in lipid metabolism could promote the accumulation of fat tissue [16], whereas others have argued that fat accumulation does not seem to depend on general factors such as obesity [17]. Chevsky et al [18], proposed that adipose tissue might be incorporated into the thyroid during embryogenesis along with striated muscle; before the gland capsule is formed. Schroder [4] postulates that DLT is associated with “displaced nests of embryonic structures, calling the entity “choristomatous adiposity”. A recent theory that attempts to explain the pathophysiology of the disease suggests that somatic mutations leading to the loss of succinate dehydrogenase-subunit B (SDHB) expression may play a role. Immunohistological staining revealed the loss of this protein in cells from DLT tissue resulting in the deregulation of the mitochondrial respiration process and interference with lipid metabolism. This could result in a decrease in fatty acid oxidation, explaining the attenuation of fat in the gland and the replacement of normal follicles [6]. All of these theories could be plausible because they explain different aspects of infiltration, either regarding its diffuse presence in congenital and acquired goiters or the limitation of fatty deposition in certain regions of the gland.
Imaging techniques are a common diagnostic tool in the investigation of diffuse goiter and are the presumed initial diagnosis in most cases. After extensive investigation, only nine reports assumed that the gland was infiltrated by fat tissue. Ultrasonographic findings most commonly indicate parenchymal heterogeneity [19], gland enlargement and cystic or solid nodules with septations [20,21,22]. Computed tomography (CT) and fine-needle aspiration (FNA) biopsy are the gold standard for the early diagnosis of disease [20]. The tomographic findings consisted of an enlarged gland with low attenuation (-30 to -70 Hounsfield units) and heterogeneity of the parenchyma with a few areas showing hyperattenuation probably indicating the presence of normal thyroid tissue [20,22,23,24,25]. In cases where compressing symptoms were present, invasion of the retropharyngeal space, expansion to the thoracic inlet and compression of nearby organs such as the trachea or esophagus, were found [11,22]. Overall, almost all reports noted a low tomographic density of the thyroid stoma, but it was not low enough to be certain of fatty infiltration [11,24]. MRI (Magnetic Resonance Imaging) is occasionally used to confirm findings of low density in the stroma and increased signals with fat suppression in T1 and T2 sequences [26,27]. Scintigraphy with Tc99m or I123 (Iodine-123) showed heterogeneity in radioactive uptake, occasionally indicating the presence of cold nodules [19,28]. Finally, FNA cytology or biopsy was performed in ambivalent cases expressing infiltration of the gland with fatty tissue, either in the background or predominantly. However, clear guidelines for the definitive diagnosis of thyroid lipomatosis are eclipsed, and almost none of the above cases reached a diagnosis until after pathological findings were released [21]. A definitive diagnosis can be achieved after thyroidectomy if the pathological report describes diffuse gland infiltration [11].
The differential diagnoses include non-neoplastic fat-containing lesions such as adenolipoma, DLT, amyloid goiter, lymphocytic thyroiditis, heterotopic nests of adipose cells, parathyroid lipoma, or intrathyroid thymic tissue, and neoplastic lesions such as lipid-rich cell adenoma, liposarcoma, or encapsulated papillary carcinoma. Adenolipoma can be easily differentiated from diffuse lipomatosis by its well-defined, encapsulated appearance along with the simultaneous admixture with proliferated thyroid follicles [19,20,27]. Amyloid goiter is usually found in systemic amyloidosis, either primary or secondary and its pathognomonic characteristic of positive Congo red or crystal violet staining, makes the diagnosis relatively straightforward [5,19]. However, there are cases where both amyloid and fat cell depositions were found in equal amounts or amyloid deposits were scarce amidst a thyroid stroma mainly comprised of fat cells [19]. As there is no certainty regarding the criteria for the differential diagnosis of amyloid goiters with fatty infiltration from thyroid lipomatosis, we only considered cases where there was a clear predominance of fat tissue over amyloid proteins. Accumulation of various amounts of fat cells is a common finding in amyloid goiters because tissue hypoxia caused by a gradual increase in amyloid could drive fibroblasts to differentiate into fat cells as previously stated [29]. Lymphocytic thyroiditis is associated with extensive infiltration of the stroma by lymphocytes, whereas heterotopic nests can be only found in the subcapsular regions of the gland [3,17,20]. The intimate embryologic origin of the thyroid with the parathyroid glands and thymus may be the cause of parathyroid lipomas, with characteristic cytoplasmic glycogen deposits, and ectopic thymic tissue [1,5]. Lipid-rich follicular adenomas can be distinguished by the presence of follicles with aggravated intracytoplasmic lipid formation, circular nuclei, and vesicular morphology [3,30]. Liposarcoma is a rare, aggressive neoplasm that usually expands rapidly beyond the thyroid capsule. Finally, there have been a few cases in which papillary carcinoma was found within diffusely enlarged goiters infiltrated with fat. The histopathological features and immunohistochemical profile of the tumor were evident, and adipose cells were occasionally found in small amounts within the stroma [23].
A distinguishing feature of diffuse thyroid lipomatosis is the infiltration and replacement of what would be an otherwise normal thyroid stroma by mature adipose cells [31]. Macroscopically, the gland has a pale yellow-brown color and a soft, and friable texture. In most cases, the gland size exceeded the normal weight (10-20 g), the lobes were enlarged, and when cut, they had a lobular appearance [5,11,23]. Schroder et al [4] noted that the gland may resemble a congenital goiter because of its progressive growth during the first decade of life. Microscopic analysis revealed that mature adipocytes lacking encapsulation had replaced normal thyroid follicles [5,11,14,32]. The fat tissue is lobulated by strands of fibrous tissue. The remaining indigenous cells were clustered in random amounts and were scattered throughout the fatty stroma [14]. The follicles were lined with cuboidal epithelium and exhibited colloid accumulation [23]. Infiltration of fat with scarce lymphocytes was observed in a few cases, whereas deposition of pink unshaped material was found around the remnants of the follicular tissue [5,11]. Only in instances of systemic amyloidosis was this discovery described; in these cases, the amyloid A protein was identified through immunohistochemical staining and validated by apple-green birefringence during polarized microscopy using Congo red staining [11]. Papillary carcinoma coincided with DLT in three cases and was described as a localized group of follicles; surrounded by fat, with oval cells and enlarged ground glass nuclei. Immunohistochemical positivity for thyroglobulin and TTF-1 confirmed the diagnosis [3,33].
Total thyroidectomy via a transverse horizontal cervical incision appears to be an appropriate therapeutic option for patients with symptomatic swelling [30]. Caution should be exercised in view of the softness and friability of the thyroid gland to avoid extensive intra-operative bleeding. Mobilization of the gland should be performed meticulously; with minimal traction during detachment and identification of the adjacent laryngeal nerves and parathyroid glands [20]. Left hemithyroidectomy was performed under FNA guidance. Subsequent histopathological evaluation confirmed a diagnosis of diffuse thyroid lipomatosis. Biopsy samples may have been obtained from areas with scarce or no fat content [32]. Our review summarizes that there should be a surgical attempt to assuage the patient only in cases in which compression symptoms are present. If the patient is asymptomatic and DLT is confirmed via imaging techniques or biopsy, the patient should be discharged, and follow-up will be advised in the next few months to re-estimate the extent of the disease [27]. Owing to the underlying pathophysiological mechanisms of the disease, in cases where DLT is confirmed before or during surgery, the potential presence of ectopic thyroid tissue should be investigated [34]. Finally in cases with thyroid swelling and hyperactivity indicated from scintigraphy, a CT scan should be ordered to examine the consistency of the gland and in view of a possible DLT diagnosis, radioiodine ablation therapy can be dismissed altogether and replaced directly by total thyroidectomy [24].
5. Conclusions
Diffuse lipomatosis of the thyroid gland is a rare but fascinating condition that involves replacement of normal thyroid tissue with fatty infiltration. Our review of the literature and presentation of a case report highlight the clinical features, diagnostic challenges, and treatment options associated with this condition. Our results indicate that surgical intervention should be considered in symptomatic patients as it has been shown to lead to positive long-term results in most cases. Further research is needed to better understand the underlying mechanisms of DLT, which will enable the development of more accurate diagnostic and therapeutic approaches and improve patient outcomes.
Author Contributions
Angeliki Emmanouilidou 1, 2 (Medical Student): Methodology(equal), formal analysis(lead), investigation(lead), writing -original draft(lead), writing -review and editing(equal). Michael Karanikas 2 (MD: PhD, MSc): Resources(equal), writing-review and editing(equal), project administration(supporting). Kalliopi Pazaitou-Panayiotou 3 (MD): Resources(equal), supervision(supporting), writing - review and editing(equal). Nikolaos Michalopoulos 2 (MD, PhD): Conceptualization(lead), methodology(equal), supervision(lead), writing-review and editing(equal), project administration(lead).
Funding
This study did not receive any funding.
Author Disclosure Statement
Angeliki Emmanouilidou: no conflict of interest; Michael Karanikas: no conflict of interest; Kalliopi Pazaitou-Panayiotou: no conflict of interest; Nikolaos Michalopoulos: no conflict of interest.
Data Availability
All relevant data are within the paper and its supporting information files.
References
- Ge, Y.; Luna, M.A.; Cowan, D.F.; Truong, L.D.; Ayala, A.G. Thyrolipoma and thyrolipomatosis: 5 case reports and historical review of the literature. Ann Diagn Pathol. 2009, 13, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Sanuvada, R.; Chowhan, A.; Rukmangadha, N.; Patnayak, R.; Yootla, M.; Amancharla, L. Thyrolipomatosis: an inquisitive rare entity. Gland Surgery . 2014, 3, E6–E9. [Google Scholar] [CrossRef] [PubMed]
- Nandyala, H.S.; Madapuram, S.; Yadav, M.; Katamala, S.K. Diffuse lipomatosis of the thyroid gland with papillary microcarcinoma: Report of a rare entity. Indian J Pathol Microbiol. 2015, 58, 348–350. [Google Scholar] [CrossRef] [PubMed]
- Schroder, S.; Bocker, W.; Hiisselmann, H.; Dralle, H. Hrchows Archiv A Case Report Adenolipoma (Thyrolipoma) of the Thyroid Gland Report of Two Cases and Review of Literature. Vol 404.; 1984.
- Dombale, V.D.; jaValgi, A.P. Symmetric Diffuse Lipomatosis of the Thyroid Gland. Journal of Clinical and Diagnostic Research. 2011, 5, 867–868 wwwjcdrnet. [Google Scholar]
- Lau, E.; Freitas, P.; Costa, J.; et al. Loss of mitochondrial SDHB expression: What is its role in diffuse thyroid lipomatosis? Hormone and Metabolic Research. 2015, 47, 165–167. [Google Scholar] [CrossRef]
- Daboin, K.P.; Ochoa-Perez, V.; Luna, M.A. Adenolipomas of the head and neck: analysis of 6 cases. Ann Diagn Pathol. 2006, 10, 72–76. [Google Scholar] [CrossRef]
- Çelik, Z.E. Mature Fat Containing Thyroid Lesions. European Journal of General Medicine. 2015, 12, 353–355. [Google Scholar] [CrossRef]
- Citgez, B.; Uludag, M.; Yetkin, G.; et al. Amyloid goiter with diffuse lipomatosis. World Journal of Endocrine Surgery. 2011, 3, 97–99. [Google Scholar] [CrossRef]
- Dhayagude, R.G. Case report: massive fatty infiltration in a colloid goiter. Arch Pathol (Chic) 1942, 33, 357–360. [Google Scholar]
- Bell, S.; Sosa, G.A.; del Valle Jaen, A.; Russo Picasso, M.F. Thyroid lipomatosis in a 36-year-old patient with rheumatoid arthritis and a kidney transplant. Endocrinol Diabetes Metab Case Rep. 2016, 2016. [Google Scholar] [CrossRef]
- Munzinger, U. Amyloid Goiter. Vol 104.; 1974.
- Willis, RA. The Borderland of Embryology and Pathology. Butterworth & Co.; 1958.
- Schroder, S.; Boeker, W. Lipomatous Lesions of the Thyroid Gland: A Review. Appl Pathol 1985, 3, 140–149. [Google Scholar] [PubMed]
- Trites, A.E.W. Thyrolipoma Thyrolipoma, Thymolipoma and Pharyngeal Lipoma: A Syndrome. Canad Med Ass J. 1966, 95, 1254–1259. [Google Scholar] [PubMed]
- Gellhorn, A.; Marks, P.A. The composition and biosynthesis of lipids in human adipose tissues. J Clin Invest 1961, 40, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Derienzo D, Truong L. Thyroid Neoplasms Containing Mature Fat: A Report of Two Cases and Review of the Literature. Vol 2.; 1969.
- Chesky, V.E.; Dreese, W.C.; Hellwig, C.A. Adenolipomatosis of the thyroid: a new type of goiter. Surgery 1953, 34, 38–45. [Google Scholar]
- Gonulalan, G.; Esen, H.; Mehmet, E.; Cakir, M. Thyroid Lipomatosis. Internal Medicine. 2012, 51, 3383–3385. [Google Scholar] [CrossRef]
- Pradeep, P.V.; Kumar, R.; Ragavan, M.; Ramakrishna, B.A. Diffuse lipomatosis of thyroid with hyperthyroidism. J Postgrad Med. 2010, 56, 35–36. [Google Scholar] [CrossRef]
- Cavaco, D.R.; Alves Rafael, A.; Cabrera, R.; Vilar, H.; Leite, V. Case Report: A Rare Association of Diffuse Thyroid Lipomatosis with Amyloid Deposition. Eur Thyroid J. 2021, 10, 528–532. [Google Scholar] [CrossRef]
- Lo, R.; Donaldson, C. Diffuse Lipomatosis of the Thyroid Gland. Ultrasound Q. 2013, 29, 253–254 wwwultrasound. [Google Scholar] [CrossRef]
- Ben Gamra, O.; Romdhane, N.; Nefzaoui, S.; et al. Diffuse lipomatosis of the thyroid gland. Egyptian Journal of Ear, Nose, Throat and Allied Sciences. 2016, 17, 167–169. [Google Scholar] [CrossRef]
- Harisankar, C.N.B. A Rare Case of Thyrolipomatosis Presenting with Latent Hyperthyroidism. Indian J Nucl Med. 2018, 33, 237–238. [Google Scholar] [CrossRef]
- Ravinder, K.; Abhishek, B.; Gagan, J. Thyrolipomatosis: A Rare Fat Containing Lesion diffusely Infiltrating Throughout the Thyroid Gland. Journal of the Association of Physicians of India. 2019, 67, 77. [Google Scholar]
- Campion, T.; Maity, A.; Ali, S.; Richards, P.; Adams, A. Concurrent thyrolipomatosis and thymolipoma in a patient with myasthenia gravis: A case report and review of the literature. Ann R Coll Surg Engl. 2021, 103, 212–215. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Goyal, A.; Kandasamy, D. Diffuse Thyroid Lipomatosis - a Rare Image. Indian Journal of Surgery. 2020, 82, 1310–1311. [Google Scholar] [CrossRef]
- Ahmed, J.; Amine REl Bouziane, C. Diffuse Lipomatosis of Thyroid—Case Report. Surg Sci. 2018, 09, 469–473. [Google Scholar] [CrossRef]
- Himmetoglu, C.; Yamak, S.; Tezel, G.G. Diffuse fatty infiltration in amyloid goiter. Pathol Int. 2007, 57, 449–453. [Google Scholar] [CrossRef]
- Hijazi, D.M.; Addas, F.A.; Alghanmi, N.M.; Marzouki, H.Z.; Merdad, M.A. An enlarged goiter presenting with a rare diffuse lipomatosis of the thyroid gland. American Journal of Case Reports 2018, 19, 808–811. [Google Scholar] [CrossRef]
- Ishida, M.; Kashu, I.; Morisaki, T.; et al. Thyrolipomatosis: A case report with review of the literature. Mol Clin Oncol. 2017, 6, 893–895. [Google Scholar] [CrossRef]
- Martí-Fernández, R.; Cassinello-Fernández, N.; Palomares-Casasús, S.; Gómez-Adrián, J.C.; Ferrández-Izquierdo, A. Diffuse Lipomatosis of the Thyroid Gland. American Surgeon. Published online 2021. [CrossRef]
- Kuk, M.; Kuo, C.J.; Nguyen, V.H.; Chen, C.C. Synchronous thyrolipoma and papillary thyroid carcinoma: A rare but significant event. Diagnostics. 2021, 11(8). [CrossRef]
- Kesici, U.; Karatepe, Y.K.; Isceviren, B. Concurrence of Thyrolipoma-tosis with Hyperthyroidism and Ectopic Thyroid Tissue. Journal of the College of Physicians and Surgeons Pakistan. 2022, 32, 1231–1232. [Google Scholar] [CrossRef]
- Simard, L.C. Une nouvelle forme de goître: la scléro-lympho-lipomatose thyroidiènne. Union Med Can 1945, 74, 884–991. [Google Scholar]
- Bielicki, F.; Dawiskiba, E.; Kasprzak, A.; Kawecki, K.; Zagrobelny, Z. [Struma lipomatosa]. Pol Tyg Lek (Wars). 1968, 23, 2018–2019. [Google Scholar]
- Dalforno, S.; Donna, A. Lipomatosi diffusa della tiroide (Struma lipomatose). Cancro 1959, 22, 613–617. [Google Scholar]
- Asirwatham, J.E.; Barcos, M.; Shimaoka, K. Hamartomatous adiposity of thyroid gland. J Med. 1979, 10, 197–206. [Google Scholar] [PubMed]
- Simha, M.R.; Doctor, V.M. Adenolipomatosis of the thyroid gland. Indian J Cancer. 1983, 20, 215–217. [Google Scholar]
- Téllez, R.; Le Cerf, P.; Araos, F.; Michaud, P. Diffuse fatty infiltration of the thyroid gland associated to amyloidosis in a patient with chronic renal failure. Rev Med Chil. 1996, 124, 1251–1255. [Google Scholar]
- Paoletti, H.; Tourrette, J.; Terrier, J.; et al. [Diffuse thyroid lipomatosis]. J Radiol. 1997, 78, 1291–1294. [Google Scholar]
- Arslan, A.; Lent Alíç, B.; Kemal Uzunlar, A.; Seyin Büyü, H.; Sarí, I. Diffuse lipomatosis of thyroid gland. Auris Nasus Larynx, 1999; 26, 213–215. [Google Scholar]
- Di Scioscio, V.; Loffreda, V.; Feraco, P.; et al. Diffuse lipomatosis of thyroid gland. Journal of Clinical Endocrinology and Metabolism. 2008, 93, 8–9. [Google Scholar] [CrossRef]
- Gupta, R.; Arora, R.; Sharma, A.; Dinda, A. Diffuse lipomatosis of the thyroid gland: A pathologic curiosity. Indian J Pathol Microbiol. 2009, 52, 215. [Google Scholar] [CrossRef]
- Jacques, T.A.; Stearns, M.P. Diffuse lipomatosis of the thyroid with amyloid deposition. Journal of Laryngology and Otology. 2013, 127, 426–428. [Google Scholar] [CrossRef]
- Costa, J.; Pardal, J.; Máximo, V.; Gonçalves, F.; Eloy, C. Diffuse lipomatosis of thyroid: A case report. Virchows Archiv. 2013, 463, 155. [Google Scholar]
- Liyanaarachchi, N.; Lim, A.; Donaldson, E. Diffuse lipomatosis and amyloid deposition of the thyroid gland associated with poorly differentiated/insular carcinoma of the thyroid: report of a rare entity. Pathology. 2016, 48(81).
- Kumar, R.; Bhargava, A.; Jaiswal, G. A Case Report on Radiologic Findings of Thyrolipomatosis: a Rare Fat Containing Lesion diffusely Infiltrating throughout the Thyroid Gland. Journal of Kathmandu Medical College. 2016, 5, 71–73. [Google Scholar] [CrossRef]
- López-Muñoz, B.; Greco Bermúdez, L.; Marín-Jiménez, D.; et al. An Unusual Amyloid Goiter in a 48-Year-Old Woman with Rheumatoid Arthritis, Secondary Amyloidosis and Renal Failure. Case Rep Endocrinol. 2019, 2019. [Google Scholar] [CrossRef] [PubMed]
- Stanaway, A.; Lam, T. Consecutive cases of thyrolipomatosis and thymolipoma: a case report. ANZ J Surg. 2019, 89, 614–616. [Google Scholar] [CrossRef] [PubMed]
- Ayadi, S.; Hammami, B.; Boudaouara, O.; Boudawara, T.; Kallel, S.; Charfeddine, I. [Association of thyrolipoma and thyrolipomatosis: A case report]. Ann Pathol. 2021, 41, 326–329. [Google Scholar] [CrossRef]
- Xhemalaj, D.; Xhardo, E.; Gradica, F.; Lisha, L. Diffuse Lipomatosis of Thyroid Gland. Case Report and Review of Literature. Diagn Pathol. 2022, 7, 285. [Google Scholar] [CrossRef]
- Morado da Silva, E.M.; Ferreira RA da, C.; Lozada, A.R.C.; Duarte, J.M.S. A 54-Year-Old Woman with Papillary Thyroid Carcinoma Associated with Secondary Amyloid Goiter and Thyroid Lipomatosis. American Journal of Case Reports. 2022, 23, 1–4. [Google Scholar] [CrossRef]
- Kawai, C.; Miyao, M.; Kotani, H.; et al. Systemic amyloidosis with amyloid goiter: An autopsy report. Leg Med. 2023, 60(102167). [CrossRef]
- Paz-Ibarra, J.; Concepción-Zavaleta, M.; Mendoza-Quispe, D.; et al. Coexistence of thyrolipomatosis and tongue squamous cell carcinoma: A case report. touchREVIEWS in Endocrinology. 2023, 19, 103–107. [Google Scholar] [CrossRef]
- Alenezi, S.; Saleem, A.; Alhajri, O.; Alozairi, O. Thyrolipoma presentation as a huge multinodular goiter; A case report of an extremely rare entity. Int J Surg Case Rep. 2023, 112(108936). [CrossRef]
- Gonzalez-Gil, A.M.; Ruiz-Santillan, M.A.; Force, B.K.; Gaba, R. A Case of Diffuse Thyroid Lipomatosis With Amyloid Deposits Presenting With Thyrotoxicosis. JCEM Case Reports. 2024, 2, 1–5. [Google Scholar] [CrossRef]
- George, D.M.; Shah, S.N. Diffuse Thyroid Lipomatosis and Amyloid Goiter With Incidental Papillary Thyroid Carcinoma: A Rare Case Report. Cureus. Published online April 9, 2024. [CrossRef]
| 1 | School of Medicine, Aristotle University of Thessaloniki, 54124, Thessaloniki, Greece |
| 2 | Advancer Center of Endocrine Surgery, Genesis Hospital, 54301, Thessaloniki, Greece |
| 3 | Division of Endocrinology, European Interbalkan Medical Center, 55535, Thessaloniki, Greece |
Figure 1.
A: Ultrasonography of thyroid showing heterogeneity of parenchyma. B, C: CT findings indicating a diffusely enlarged thyroid with hypodense areas and intrathoracic extensions. D: Tc99m scintigraphy showing heterogeneous uptake of the isotope and cold areas in the lower parts of the gland.
Figure 1.
A: Ultrasonography of thyroid showing heterogeneity of parenchyma. B, C: CT findings indicating a diffusely enlarged thyroid with hypodense areas and intrathoracic extensions. D: Tc99m scintigraphy showing heterogeneous uptake of the isotope and cold areas in the lower parts of the gland.
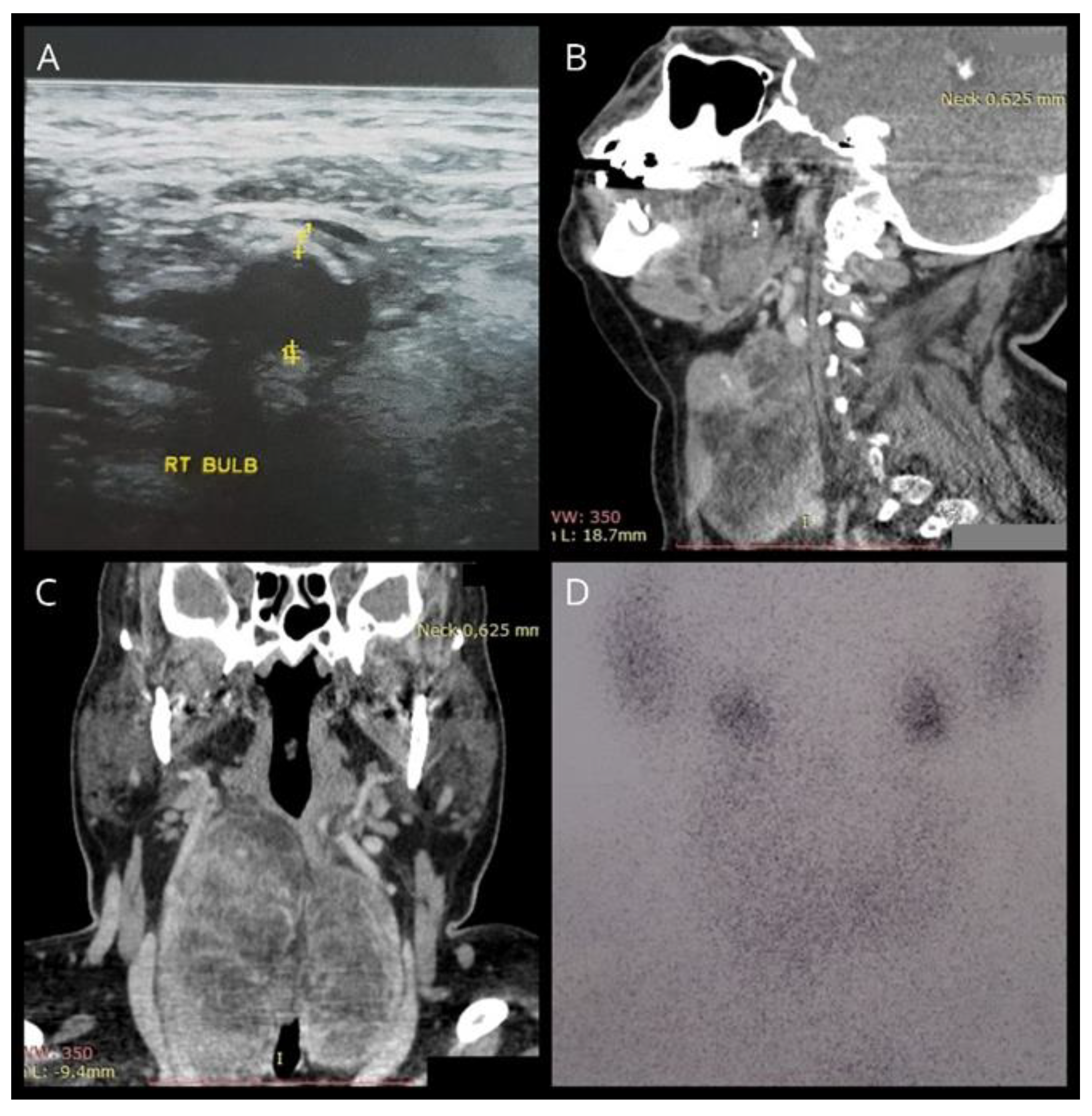
Figure 2.
Thyroid specimen after total thyroidectomy.
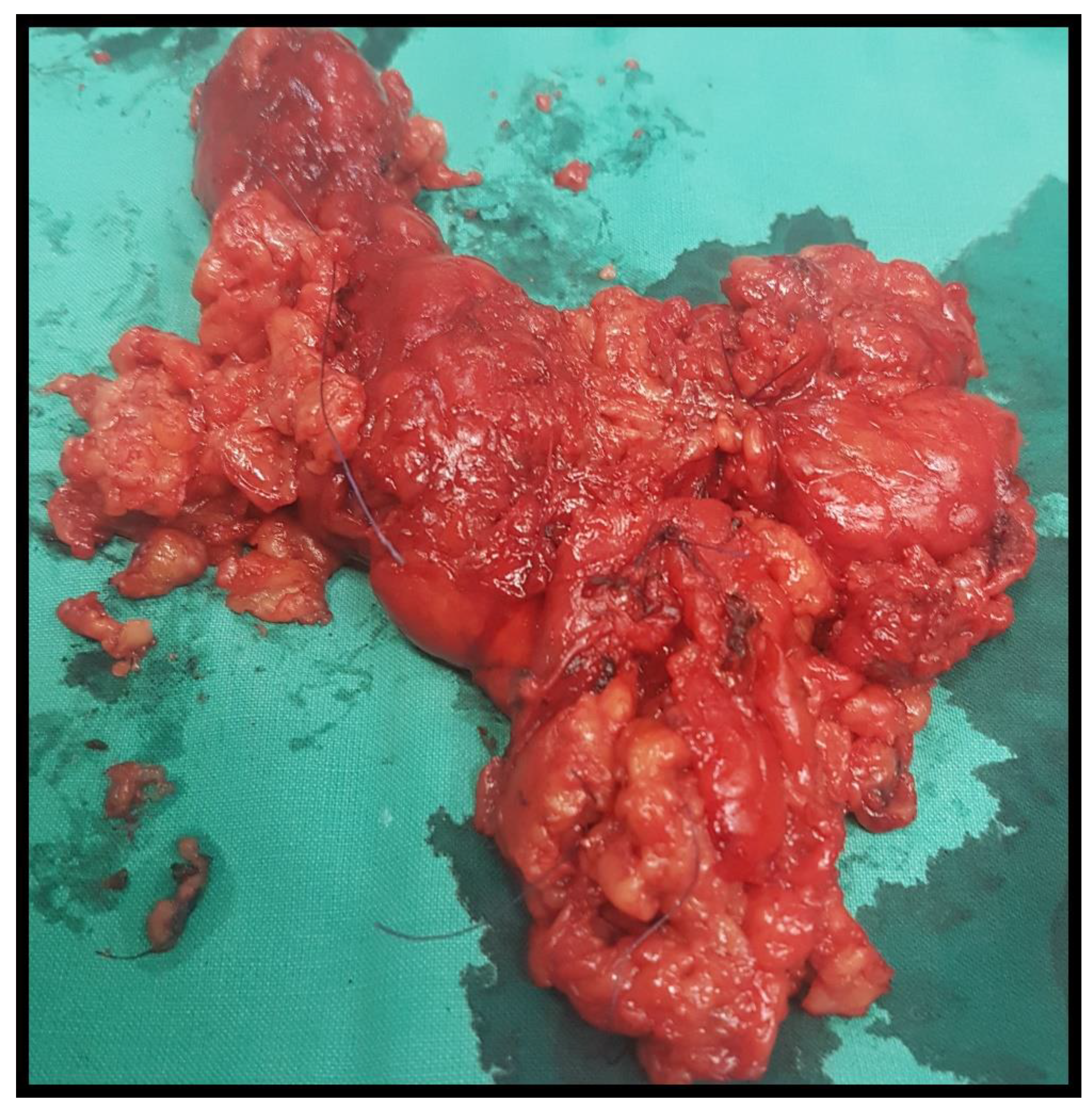
Figure 3.
A: Staining with hematoxylin-eosin (H&E) (magnification, x10), B: Staining with hematoxylin-eosin (H&E) (magnification, x40), C: Staining with hematoxylin-eosin (H&E) (magnification, x100), D: TTF-1 staining.
Figure 3.
A: Staining with hematoxylin-eosin (H&E) (magnification, x10), B: Staining with hematoxylin-eosin (H&E) (magnification, x40), C: Staining with hematoxylin-eosin (H&E) (magnification, x100), D: TTF-1 staining.
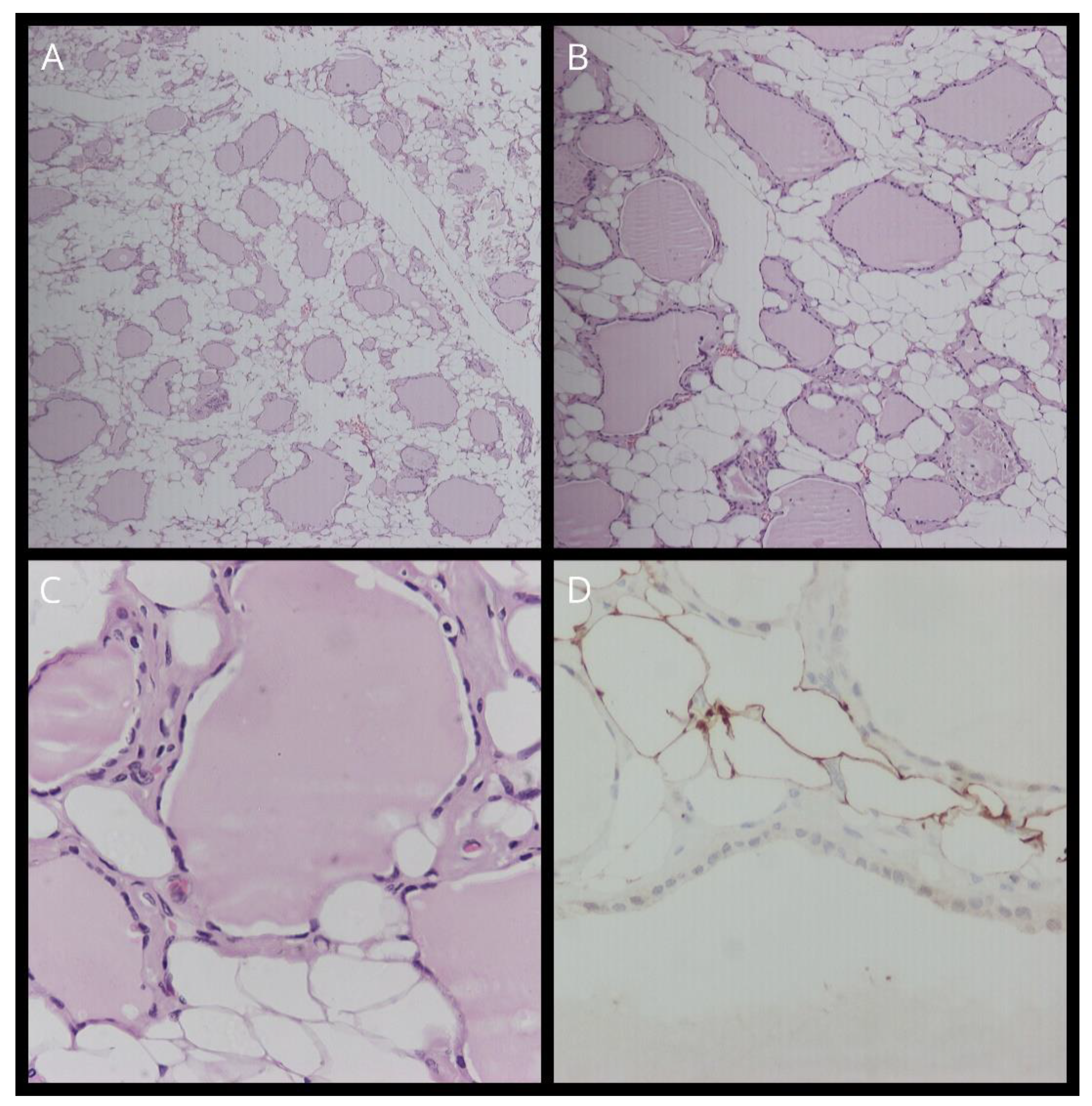

Table 1.
Summary of Thyroid Lipomatosis Case Reports.
| Reference | Sex/Age | Clinical Features | Thyroid Function | Renal Failure | Initial Diagnosis | Treatment | Thyroid size/weight | Pathology | Amyloid deposition | Follow-up |
|---|---|---|---|---|---|---|---|---|---|---|
| 10 | M/32 | Local compression | NS (Not Stated) |
No | Diffuse goiter | Excision | 10 x 8 x 5.5 cm (R), 8 x 6 x 5.5cm (L)/ 500g | Diffuse infiltration of fibrous-fatty tissue, anomalous follicles, focal fibrosis |
NS | NS |
| 35 | F/11 | No | BMR (Basic metabolic rate) +3% (hyperthyroidism) | No | Diffuse goiter (since birth) | Excision | x5 normal thyroid size | Diffuse fat infiltration alongside small thyroid follicles and lobules with fibrous septa |
NS | NS |
| 18 | M/15 | No | Normal | No | Diffuse goiter (since birth) | Excision | 12 x 7 x 4 cm (R), 8 x 5 x 2.5cm (L)/ 253g | Diffuse fat infiltration, small and medium thyroid follicles, stromal edema |
NS | NS |
| 36 | M/58 | Local compression | Hyperthyroidism | No | Diffuse goiter | Excision | NS | Diffuse fat infiltration surrounding normal follicles, stromal fibrosis, lymphocyte aggregation |
NS | NS |
| 37 | F/51 | No | Normal | No | Diffuse goiter | Excision | NS | Diffuse fat infiltration surrounding normal follicles, stromal fibrosis |
NS | NS |
| 38 | F/73 | No | Normal | No | Diffuse goiter | Excision | NS/120g | Diffuse fat infiltration around normal follicles, lymphocyte aggregation |
NS | NS |
| 39 | M/12 | No | Normal | No | Right neck mass | Excision | 13 x 8 x 6.5cm (R)/415g | Diffuse fat infiltration surrounding normal thyroid follicles, presence of lymphocytes and fibrous tissue |
NS | NS |
| 40 | M/26 | Neck swelling, hoarseness, dysphagia | Normal | Yes | Cervical mass | Total thyroidectomy | NS | Diffuse infiltration of thyroid by fat | Yes | NS |
| 41 | F/77 | No | Normal | No | Cervical mass | Excision | NS/700g | Thyroid follicles surrounded by adipose cells | NS | NS |
| 42 | M/38 | Neck swelling | Normal | No | Diffuse enlargement of thyroid | Excision | 4 x 3 x 2cm (I), 13 x 7 x 3cm (R), 15 x 9 x 5cm (L)/465g | Mature adipose tissue surrounded the different sized but otherwise normal follicles of the thyroid | No | Well -post-operatively |
| 29 | F/58 | Neck swelling, dysphagia, hoarseness, hyperthermia | Hypothyroidism | Yes | Diffuse goiter | Total thyroidectomy | 9.5 x 7 x 5cm (R), 8 x 6 x 3.5cm (L)/230g | Diffuse fatty infiltration, loss of most thyroid follicles, eosinophilic substance deposition in the hyalinized stroma, lymphocytic thyroiditis | Yes | NS |
| 43 | M/64 | Enlarged thyroid, dyspnea |
Normal | Yes | Diffuse goiter | NS | NS | NS | NS | NS |
| 44 | M/45 | Neck swelling, respiratory distress | Normal | No | Diffuse thyroid enlargement | Subtotal thyroidectomy | 2 x 1.5 x 1cm (I), 9 x 7 x 4cm (R), 9 x 5 x 3.5cm (L), 4 x 3 x 2 (P)/225g | Colloid filled thyroid follicles, fatty infiltration of interfollicular stroma | No | NS |
| 1 | F/67 | Dysphagia | Normal | Yes | Enlarged nodular left thyroid lobe | Left thyroidectomy | 7 x 3.5 x 2cm (L)/41g | Thyroid follicles separated by fat, adipose tissue density varied from 30%-90% of total tissue, fat infiltration in adenomatous nodules | No | Well- 2 years after |
| 1 | F/59 | No | Hypothyroidism | No | Right thyroid mass | Right thyroid lobectomy and isthmusectomy/ left thyroidectomy | 7 x 4 x 1.2cm (R+I), 6 x 3 x 1.2cm (L)/56g | Nodular and diffuse pattern of fatty infiltration, presence of a 0.8cm papillary carcinoma | No | Well -6 years after |
| 20 | F/40 | No | Hyperthyroidism | No | Multinodular goiter | Excision | NS | Colloid filled thyroid follicles of various sizes, replacement of stroma by mature adipose tissue | No | Well -post-operatively |
| 9 | M/37 | Neck swelling, dyspnea | Normal | Yes | Diffuse thyroid enlargement | Total thyroidectomy | NS/304g | Widespread deposition of eosinophilic material with scarcity of thyroid follicles, diffuse lipomatosis and amyloidosis (secondary) | Yes | Well -3rd post-operative day |
| 5 | M/62 | Neck swelling, dyspnea | Normal | No | Nodular goiter | Near total thyroidectomy | 12 x 10 x 6cm (R), 15 x 8 x 6cm(L)/285g | Colloid filled thyroid follicles, diffuse infiltration of stroma with mature adipose tissue, scarce lymphocytic infiltration | No | NS |
| 19 | M/43 | Neck swelling, dyspnea | Normal | Yes | Enlarged thyroid | Total thyroidectomy | 6 x 2 x 1cm (I), 7.5 x 6 x 4.5cm (R), 6.5×4.5×2 (L)/160g | Scattered thyroid follicles in a dense mature fat stroma | Yes | NS |
| 45 | M/55 | Neck swelling, cough | Normal | Yes | Diffuse goiter | Total thyroidectomy | 4 x 2 x 1cm (I), 9 x 6 x 4cm (R), 7 x 5 x 2.5cm (L)/ 148g | Infiltration of thyroid by adipose tissue, small amounts of colloid filled follicles remained | Yes | Well post-operatively |
| 22 | F/52 | No | Normal | NS | Diffuse lipomatosis | NS | NS | NS | NS | Difficulty breathing – 3 years later |
| 46 | M/46 | NS | Hypothyroidism | No | Cervical mass | Partial thyroidectomy (same procedure at 3 years of age) | NS | Infiltration of thyroid by mature adipocytes. Same results as 43 years before | No | NS |
| 2 | F/32 | Neck swelling | Hyperthyroidism | No | Toxic multinodular goiter | Total thyroidectomy | 11 x 5 x 2cm(total)/88g | Thyroid follicles filled with colloid, diffuse fatty infiltration of stroma | No | NS |
| 3 | M/37 | Neck swelling | NS | No | Nodular goiter | Total thyroidectomy | 5 x 11 x 15 cm (total)/NS | Thyroid tissue replaced by mature adipocytes, papillary thyroid carcinoma | NS | NS |
| 6 | M/47 | NS | Hypothyroidism | No | Fatty infiltration of thyroid | Excision | 16.5 x 8 x 5.5cm (total)/250g | Atrophic follicles of thyroid alongside mature adipose tissue infiltration, SDHB loss of expression (follicular or adipose cells) | No | NS |
| 8 | M/25 | NS | Hypothyroidism | NS | NS | NS | NS | Various sizes of thyroid follicles, abundant distribution of mature fat around thyroid tissue | NS | NS |
| 8 | F/19 | NS | Hypothyroidism | NS | NS | NS | NS | Various sizes of thyroid follicles, abundant distribution of mature fat around thyroid tissue | NS | NS |
| 8 | M/63 | NS | Normal | NS | NS | NS | NS | Preservation of a few thyroid follicles, abundant distribution of mature fat around follicles | NS | NS |
| 47 | M/69 | Hoarseness, exertional dyspnea | NS | Yes | Diffuse fatty conversion and solid/cystic nodule of thyroid | Right hemithyroidectomy /completion thyroidectomy | NS | Diffuse infiltration of thyroid stroma by mature fat, insular carcinoma | Yes | NS |
| 23 | F/67 | Neck swelling, respiratory distress | Hyperthyroidism | Yes | Diffuse goiter | Total thyroidectomy | 2 x 2cm (I), 12 x 6 x 3.5cm (R), 10 x 5 x 2.5cm (L)/215g | Infiltration of thyroid by mature fat, scarcity of colloid follicles | No | Well- post-operatively |
| 11 | F/36 | Dyspnea | Normal | Yes | Multinodular goiter | Excision | 9.8 x 9.5 x 4.5cm (total)/144g | Replacement of normal thyroid tissue by mature adipocytes except from small remnants of normal colloid filled follicles | Yes | NS |
| 48 | M/73 | Neck swelling, dyspnea, hoarseness | Normal | No | Thyrolipomatosis | Near Total thyroidectomy | NS | Thyrolipomatosis | NS | NS |
| Present Study | F/61 | Neck swelling, dyspnea, dysphagia | Normal | Yes | Diffuse Goiter | Total thyroidectomy | NS | Fatty infiltration of thyroid, degeneration of follicles | NS | Dead – after 3 years (due to kidney failure) |
| 31 | F/68 | NS | Normal | No | Diffuse goiter | Total thyroidectomy | NS | Fatty infiltration of thyroid, hyperplastic follicles alongside stromal sclerosis and calcification | No | Well- after 3 months |
| 24 | F/49 | Neck swelling | Subclinical hyperthyroidism | No | Diffuse goiter | Radioiodine ablation (RAI)/ total thyroidectomy | NS | Infiltration of thyroid stroma by fat | NS | Well – post-operatively |
| 30 | F/53 | Local compression, dysphagia | Normal | Yes | Non-toxic diffuse multinodular goiter | Total thyroidectomy | 2.5 x 2 x 1.5cm (I), 5 x 2.5 x 2cm (R), 11 x 7 x 3.5cm (L)/415g | Admixture of adipocytes with follicular cells | NS | NS |
| 28 | F/55 | Neck swelling, hoarseness | Normal | No | Diffuse goiter | Total thyroidectomy | 1.5 x 1cm (I), 5.5 x 3.5 x 3cm (R), 4 x 2.5 x 2.2cm (L)/NS |
Replacement of thyroid tissue by mature fat , few distended thyroid follicles | No | Well- post-operatively |
| 49 | F/48 | Dysphagia | Subclinical hyperthyroidism | Yes | Amyloid Goiter | Total Thyroidectomy | 13.5 x 4.5, 6.5 x 3.5 3.5 x 2.5 cm/NS | Adipose metaplasia of thyroid stroma | Yes | Well- post-operatively |
| 50 | M/20 | Dysphagia | Normal | No | Follicular nodule | Left hemithyroidectomy | NS | Diffuse fatty infiltration of thyroid | NS | NS |
| 25 | M/73 | Neck swelling, dyspnea, hoarseness | Normal | No | Diffuse lipomatosis of thyroid | Total thyroidectomy | NS | Diffuse presence of fat cells in the thyroid | No | NS |
| 27 | M/72 | No | NS | Yes | Diffuse lipomatosis of thyroid | No | NS | NS | NS | NS |
| 21 | M/46 | Dyspnea, hoarseness, dysphagia | Normal | No | Diffuse goiter | Total thyroidectomy | 10.5 x 6.5 x 4.3 (R), 11.1 x 4 x 2.6cm (L)/237g | Normal follicular architecture, fat infiltration of stroma | Yes | Well- post-operatively |
| 32 | F/52 | No | Normal | No | Goiter/suspicious nodule | Left hemithyroidectomy | 6 x 4 x 2cm (L)/26g | Fatty infiltration of stroma, predominance of adipocytes in most regions | NS | Well – after 6 months |
| 51 | M/48 | Neck swelling | Normal | Yes | Multinodular goiter | Total thyroidectomy | NS | Diffuse and nodular infiltration of thyroid by adipose cells, scarce thyroid follicles | No | Well- after 12 months |
| 26 | M/40 | Neck swelling | Normal | No | Thyrolipoma and thymolipoma | Total thyroidectomy | NS | Thyroid follicular cells surrounded by mature adipocytes | No | Well – after 2 weeks |
| 52 | F/69 | Neck swelling, dyspnea, dysphagia, hoarseness | Normal | No | Multinodular goiter | Total thyroidectomy | 1.5 x 1 x 1cm (I), 6.5 x 5 x 3cm (R), 5 x 3 x 2.5cm (L)/NS | Diffuse infiltration of adipocytes and replacement of normal thyroid follicles | NS | Well – post-operatively |
| 53 | F/54 | Neck swelling, hoarseness, dysphagia | Normal | Yes | Diffuse lipomatosis of thyroid and follicular neoplasm | Total thyroidectomy | 2.6 x 4.5 x 2cm (I), 4.5 x 7.5 x 3.4cm (R), 3.2 x 6.7 x 2.8cm (L)/81g | Papillary thyroid carcinoma, admixture of thyroid follicles with mature adipose tissue | Yes | Dead – after 5 months (urinary tract infection -sepsis) |
| 34 | F/57 | Dyspnea, dysphagia, local compression | Hyperthyroidism | No | NS | Total thyroidectomy | NS | NS | NS | NS |
| 54 | F/60 | NS | Hyperthyroidism | Yes | NS | Autopsy | NS | Replacement of normal thyroid follicles by diffuse fat deposits | Yes | Deceased |
| 55 | F/44 | Tongue mass, dysphagia, weight loss | NS | No | Multinodular goiter | Right hemithyroidectomy | 6 x 3.5 x 2cm (R)/15g | Diffuse fat metaplasia of stromal thyroid tissue indicative of thyrolipomatosis | No | Dead – after 5 months (septic shock after metastasis of squamous cell carcinoma of the tongue to the remaining left thyroid lobe) |
| 56 | F/78 | Neck swelling, dysphagia, hoarseness | Normal | Yes | Multinodular goiter | Total thyroidectomy | 22.4 x 8.5 x 5cm/ 300g | Infiltration of the gland by mature adipocytes, a few extended thyroid follicles and a stroma filled with adipocytes and fibrotic tissue | NS | Well – post-operatively |
| 57 | F/64 | Weight loss, fatigue, enlarged thyroid | Hyperthyroidism | Yes | Diffuse Thyroid Lipomatosis | Methimazole | NS | Benign adipose tissue with entrapped thyroid follicles (biopsy) | Yes | NS |
| 58 | F/51 | NS | NS | Yes | Multinodular goiter | Total thyroidectomy | 9.4 x 6.6 x 5.7cm (R), 8.5 x 5.2 x 4.7cm (L), 2.2 x 1.2 x 1cm (I)/ NS | Lobules of adipocytes with few areas of atrophic thyroid follicles, papillary carcinoma | Yes | Well – after 6 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



