
Submitted:
06 October 2024
Posted:
07 October 2024
You are already at the latest version
Abstract
The incidence of non-palpable breast cancer is increasing due to widespread screening and neoadjuvant therapies. Among the available tumor localization techniques, radio-guided occult lesion localization (ROLL) has largely replaced wire-guided localization (WGL). This study aimed to compare ROLL and WGL techniques in terms of the effectiveness of isotopic marking of axillary sentinel lymph nodes and to assess patient perspectives along with surgeon and radiologist preferences. A single-center, prospective randomized study enrolled 110 patients with non-palpable breast lesions (56 ROLL, 54 WGL). Breast type, tumor volume, location, histological and radiological features, and localization/surgical duration were evaluated in the context of sentinel lymph node marking using isotope (Technetium-99m labelled human serum albumin) and blue dye. Statistical analysis was performed with significance set at p<0.05 and strong significance at p<0.01. Both techniques were successful in localizing non-palpable lesions (100%). However, patients reported WGL as more painful. A notable difference was observed in axillary lymph node marking, with subareolar isotope injection (used in WGL) showing better results compared to ROLL. While ROLL provided advantages in terms of patient comfort, and logistical simplicity, WGL was superior for axillary sentinel lymph node marking, particularly in inner quadrant tumors, suggesting WGL may be preferred for these cases.
Keywords:
breast cancer
; ROLL
; wire guided localization
; sentinel lymph node marking
1. Introduction
About one in eight women will get invasive breast cancer in their lifetime. This is the most commonly diagnosed cancer among women, accounting for 11.7% of all cancers in 2020 [1]. Advances in screening and effective neoadjuvant treatments have increased the detection of non-palpable breast tumors, necessitating accurate preoperative localization to ensure timely safe resection [2,3,4]. Wire-guided localization (WGL), introduced in 1965, was the first method for localizing non-palpable tumors [5]. While WGL is cost-effective and widely accessible, it has several limitations, including difficulty in wire placement and the potential for excessive excision of healthy tissue [6,7]. Despite these drawbacks, WGL remains in use, particularly when sentinel lymph node marking is not required or when multiple isotope markings are necessary.
Radio-guided occult lesion localization (ROLL), introduced in 1998 [8], uses radioactive colloid for tumor and same session sentinel lymph node marking [9]. ROLL reduces excision volume, improves cosmetic results, and enhances lesion centricity [10,11,12].
Despite these benefits, studies have shown no significant difference between ROLL and WGL in successfully localizing non-palpable breast lesions [13]. However, a key methodological difference exists in sentinel lymph node marking: ROLL does not use peri-areolar isotope injection; instead, the sentinel node is marked with a single isotope injection at the tumor site within the breast. To date, no randomized studies have directly compared the effectiveness of these two classic methods in the context of sentinel lymph node marking.
Finding the proper place of new, emerging technologies such as magnetic, radioactive, radar, or radiofrequency location methods [13], commands the scrupulous evaluation of our own present practice with the most affordable modalities in order to proceed to the next, more advanced stages.
2. Aims
The primary objective of the study was to compare the efficacy of ROLL and WGL techniques in achieving feasible isotopic marking of axillary sentinel lymph nodes.
The secondary objective was to evaluate the accuracy, efficiency, and ergonomics of ROLL compared to WGL by examining radiological and pathological outcomes. Subjective factors such as patient pain perception and surgeon and radiologist preference were also assessed with questionnaires.
3. Materials and Methods
3.1. Study Design
This single-site, prospective, randomized, non-blinded comparative intervention study was conducted at our high-volume cancer-center university hospital. All surgical procedures were performed by the same surgeon (AD) who also attended personally all marking procedures.
3.2. Patient Selection and Randomization
A total of 110 female patients, aged between 36 and 80 years, with non-palpable breast lesions were included in the study. Patients were randomized into two groups: the ROLL group (n=56) and the WGL group (n=54). Randomization was carried out using a random number generator after obtaining informed consent (and basic anthropometric data) from all participants. Primary tumor detection mammography screening and complete clinical regression to neoadjuvant therapy ratio among the ROLL and WGL groups were 43/13 vs 44/10 respectively.
43 patients (77%) in the ROLL group, and 44 patients (79%) in the WGL group had a non-palpable tumor due to early detection with cancer screening. Neoadjuvant therapy caused regress of primary tumor to non-palpable size in 13 patients (23%) in the ROLL group and in 10 patients (18%) in the WGL group. There is no significant difference between the two groups regarding cancer screening and neoadjuvant therapy proportions (p=0.5449).
3.3. Breast and Tumor Characterization
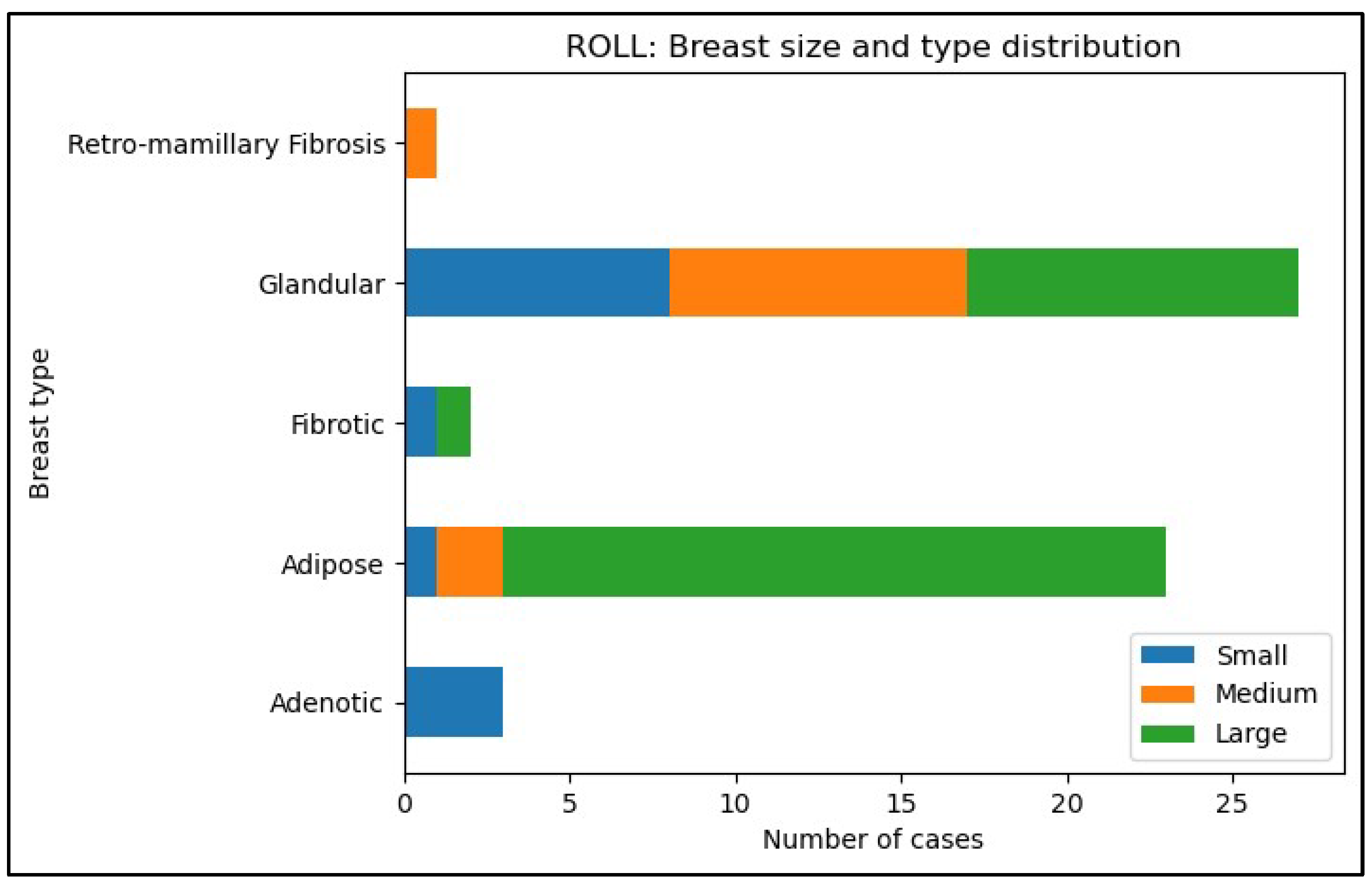
Breast size was classified based on brassiere size into three categories: A (small), B and C (medium), and D or larger (large). The breast tissue type was determined by a radiologist using mammography images and categorized into five distinct types: glandular (1), adipose (2), retro-mamillary fibrosis (3), adenotic (4), and fibrotic (5) (Table 2. and Table 3, and Figure 5., and Figure 6. in Appendix A).
The distance of the tumor from anatomical landmarks such as the nipple, skin surface, and pectoral fascia was measured using ultrasound. Tumor localization within the breast was documented in terms of four quadrants—upper-inner, upper-outer, lower-inner, and lower-outer—as well as the central area. Tumor localization distribution is shown in Table 4.
All patients underwent preoperative triple assessment, which included physical examination, mammography, breast ultrasonography and ultrasound-guided core biopsies. This approach enabled the classification of lesions according to the Breast Imaging-Reporting and Data System (Bi-RADS) and facilitated the subsequent histopathological diagnosis.
3.4. Tumor Marking Procedures
Tumor marking was performed under ultrasound guidance in 50 cases (93%) within the WGL group and in 52 cases (93%) within the ROLL group. For four patients in each group (7% and 7% respectively), stereotactic guidance was utilized for tumor marking, based on the tumor’s radiological characteristics. The duration and difficulty of the marking procedures were recorded by the radiologist and rated on a Visual Analog Scale (VAS) from 1 (easy) to 5 (difficult) [14]. In the WGL group, tumor marking was followed by surgery on the same day, while in the ROLL group, surgery was performed the following day, 16–32 hours after isotope injection.
3.5. Lymph Node Marking
All patients underwent dual lymphatic pathway marking. This included the isotope injection 16–32 hours before surgery and the injection of patent blue dye approximately 10 minutes before sentinel lymph node surgery.
3.6. Procedural Assessment
The procedural assessment involved gathering feedback from surgeons, radiologists, and patients. Surgeons completed a standardized questionnaire that documented patient demographics, the duration of the localization procedures, and the perceived difficulty of lesion localization during excision, rated on a VAS scale from 1 (very easy) to 5 (very difficult). Radiologists also filled out a questionnaire evaluating the complexity of marking non-palpable tumors. Patients were asked to rate their pain during the marking procedure on a VAS scale from 0 (no pain) to 10 (worst possible pain).
3.7. Post-Marking Procedures
Following the preoperative marking, resection of the primary tumor and axillary sentinel lymph node was performed for all patients, regardless of whether ROLL or WGL was used, by the same surgeon. The resected specimens were prepared for pathological examination using the Specimen Plate system, as described in our previous publication [15]. This system, along with precise orientation techniques, allowed for accurate in situ localization of the tumor and surrounding tissues, ensuring comprehensive pathological evaluation. Additionally, the weight of the resected specimens was recorded.
3.8. Histopathological and Imaging Analysis
Mammography images and histopathological findings were analyzed to determine the adequacy of resection, ensuring radiologically and pathologically clear margins. Data on these outcomes were systematically recorded and evaluated.
3.9. Statistical Analysis
Statistical analysis was performed using Python 3.11.5 with packages such as Pandas 2.0.3, SciPy 1.11.1, Seaborn 0.12.2, and Matplotlib 3.7.2.
Mann-Whitney test was used to evaluate differences between ROLL versus WGL. A p-value of <0.05 was considered statistically significant, strong statistical significance was proven if p<0.01.
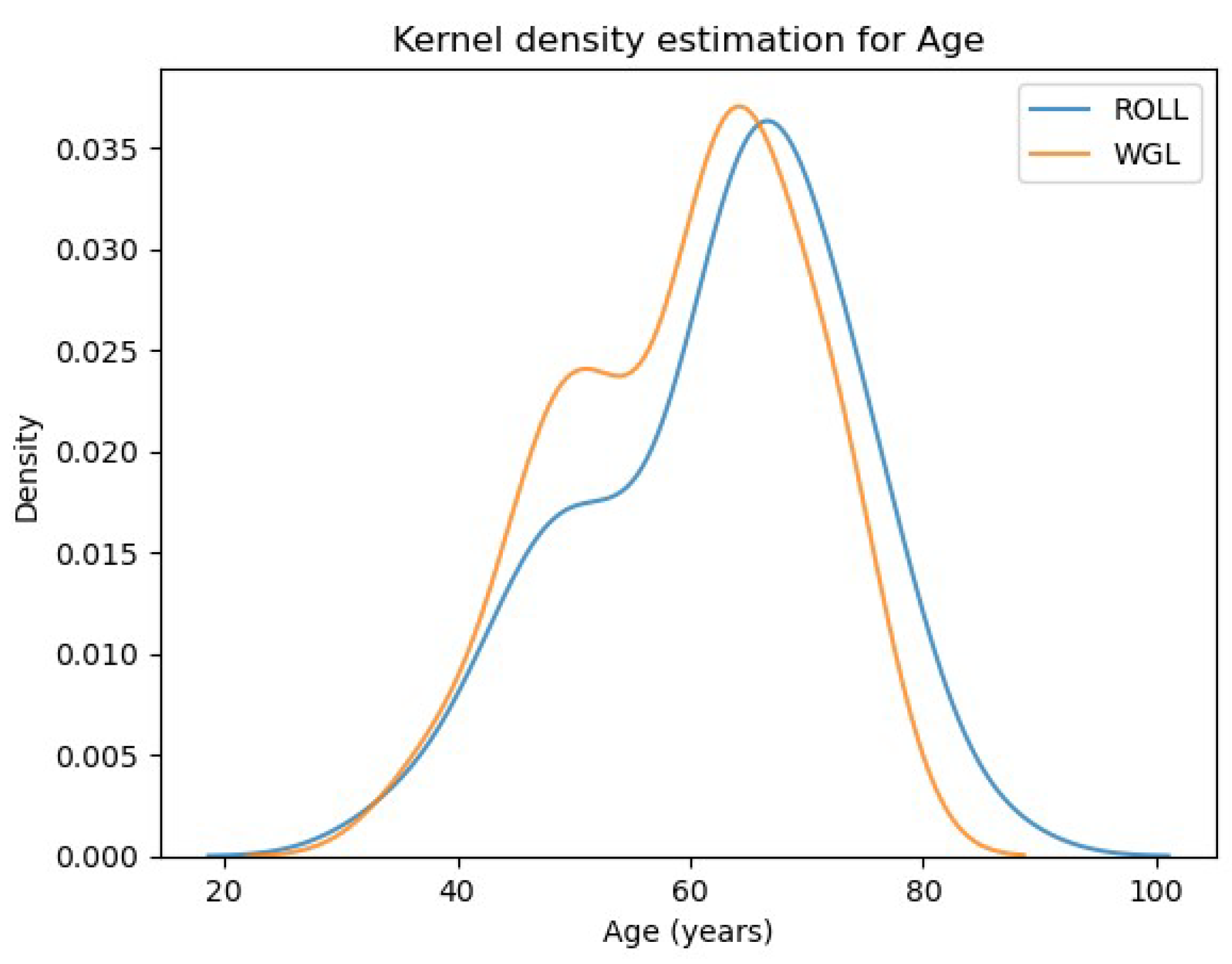
The mean age of patients was 62.4 ± 11.31 years in the ROLL group and 59.56 ± 10.1 years in the WGL group, with 95% confidence intervals of (59.37, 65.43) and (56.8, 62.32), respectively. Mean BMI was 26.24 ± 3.61 kg/m² in the ROLL group and 25.89 ± 3.19 kg/m² in the WGL group, with 95% confidence intervals of (25.27, 27.2) and (25.01, 26.76), respectively. No significant differences were found between the groups regarding age or BMI distributions.
The Kolmogorov-Smirnov test showed no significant differences in BMI (p = 0.9339) or age (p = 0.1177) distributions between the groups. Similar results were observed with the Mann-Whitney and Cramer-von Mises tests. One-way ANOVA also indicated no significant differences in mean BMI (p = 0.5932) or age (p = 0.1681) between the groups. (See statistical result figures in Appendix A)
4. Results
Difficulty of preoperative lesion marking from the radiologist’s perspective (VAS scale from 1 to 5) was 1.75 ±0.96 in the ROLL group and 2.31 ±0.97 in the WGL group, with a strong significant benefit of the ROLL technique (p=0.00022)
Preoperative marking took 2.93 ±3.71 minutes in the ROLL group and 3.92 ±3.16 minutes in the WGL group showing strong significant superiority of the ROLL technique (p=0.001).
Patients’ subjective pain (VAS 0-10) during preoperative marking also showed strong significant advantage of ROLL (1.41 ±1.42) versus WGL (3.78 ±2.03) p=0.0000000007)
Surgeon’s subjective perspective of operative difficulty of lesion localization also makes ROLL significantly superior to WGL technique. (VAS scale 1.91 ±0.96 versus 2.29 ±1.04 respectively, p=0.0197).
Skin-to-skin operation time was similar in the ROLL (71.05 ±18.92 minutes) and in the WGL group (69.26 ±14.51 minutes) (p=0.9593)
Removed breast tissue weight (pathology specimen) was 88.48 ±45.25 grams for ROLL patients and 72.43 ±33.55 grams in the WGL group. Multiple statistical tests were carried out due to inconsistent significance. Mann-Whitney (p=0.019) and Cramer- von Mises (p=0.0162) tests show significantly lower amount of resected tissue in WGL patients, while the conservative Kolmogorov-Smirnov test reached no significance (p=0.0637).
All 110 patients underwent successful operations with clear and safe resection margins following either ROLL or WGL marking. The figures presenting the detailed results can be found in Appendix A.
4.1. Sentinel Lymph Node Marking Results
We compared the percentage of sentinel lymph node isotope marking failures across different tumor quadrants for both techniques. The ROLL technique demonstrated a significantly higher failure rate in sentinel lymph node marking with radioisotope, compared to WGL combined with peri-areolar radiotracer injection. Specifically, for tumors in the lower-inner quadrant, the failure rate for ROLL was four times greater (67%) than for WGL (14%) (p=0.0265). Similarly, this increased failure rate was observed in the upper-inner quadrant as well (40% versus 10% respectively, p=0.0607).
Study limitations: Due to the small sample size, we cannot exclude the possibility that some differences may lack statistical significance.
Full details of the statistical comparisons, including p-values, are summarized in Table 7, and Table 8, and in Appendix B. Statistically significant differences are marked with *, and strong significance with **, with all significant results favoring WGL.
In the majority of cases, patients with non-detectable sentinel lymph nodes using the ROLL technique were characterized by large breast size and fatty involution.
In the WGL group, SLN isotope identification failure was not so common than in the ROLL group. Even in large breasts with fatty involution.
Peri-areolar radioisotope injection associated with wire-guided marking had a lesser adverse impact on the axillary sentinel lymph node marking, even in cases with large breast size and fatty involution.
The distribution of non-palpable tumors according to the TNM classification (Tumor size, Node involvement, and Metastasis) is shown in the following figure, based on their size and characteristics observed during histopathological processing. The distribution of tumor sizes is similar between the two examined groups.
5. Discussion
Although non-palpable breast tumors confer better prognosis, their treatment poses challenges on several fronts. Foremost is the necessity for preoperative radiologically guided localization techniques, and more intricate surgical procedures.
Neoadjuvant chemotherapy also decreases the chance of axillary sentinel lymph node marking even after peri-areolar isotope injection [16]. In cases of tumor regression, where the tumor becomes non-palpable and a ROLL procedure is performed, there is a increased risk that the sentinel lymph node may not be marked with isotope. Therefore, the likelihood of unsuccessful axillary lymph node staging increases.
Several clinical studies and meta-analyses support the preference for the ROLL technique as a simple and convenient technique [17]. According to some studies ROLL allows a cosmetically superior and faster excision and simplifies concurrent sentinel lymph node marking [11,12,[18],]. Since both the tumor and the axillary lymph node are marked with one single injection, patients subjectively perceive the procedure less painful than a wire placement and a peri-areolar radioisotope injection.
Nevertheless, the wire localization method remains a valid alternative as lesion identification and clear margin rates do not differ significantly from ROLL technique. [13] According to the latest international recommendations WGL is primarily suggested for cases involving extensive microcalcifications, radial scar, and complex sclerosing lesions when concurrent sentinel lymph node biopsy is not necessary [19], [20], [21].
According to both the literature and our observations, wire-guided localization (WGL) may offer advantages in certain other cases.
When sentinel lymph node marking is not required, WGL provides a way to avoid unnecessary exposure to radioactivity. Additionally, more successful sentinel lymph node visualization was achieved with peri-areolar subdermal injection of the radioisotope, particularly in cases where the tumor became non-palpable after neoadjuvant chemotherapy. In contrast, the ROLL technique, when used without peri-areolar radiotracer injection, is more likely to result in unmarked axillary sentinel lymph nodes [22]. This outcome is influenced by factors such as the tumor’s intra-mammary location, breast size, and breast density.
In situations where the sentinel lymph node fails to be identified with nuclide injection, additional intraoperative blue dye can be used that is also injected into the subareolar lymphatic plexus [23]. If sentinel node marking proves unsuccessful, surgeons are compelled to contemplate axillary lymph node dissection for nodal staging.
Our randomized study shows the ROLL technique is superior to WGL, being less painful for patients and more ergonomic for the medical team. The process was faster, consistent with existing literature, but the difference in procedure time, though statistically significant, lacks clinical relevance as it’s just a few minutes. No significant differences were seen in surgical times or specimen size, though results for resected tissue size were mixed, with some tests showing significance and others not.
However, the subjective ease of localizing non-palpable breast tumors is facilitated during the ROLL technique, it can be affirmed that the WGL technique with sub-areolar injection of the radiocolloid is more successful in terms of visualizing the sentinel lymph node [24,25,26,27].
In order to avoid the morbidity associated with extensive axillary surgery, achieving a high rate of accurate sentinel lymph node identification is crucial. Hence, it becomes imperative for physicians to identify the elevated risk for a failure of sentinel lymph node marking.
Therefore, it is needed to determine in which cases should be ROLL avoided / substituted with another localization technique that involves peri-areolar radioisotope injection.
Our results demonstrate that in large, adipose breasts, particularly when the tumor is located in the inner quadrants, especially the inner-lower quadrant, ROLL technique’s isotope tracking failed to mark sentinel lymph nodes four times more often than peri-areolar isotope injection used with WGL (67% vs 14%).
While case number limited statistical power of the analysis, there seems to be strong clinical relevance of our observation with reference to the application of in inner quadrant lesions.
Accurate sentinel lymph node identification is crucial to avoid extensive axillary surgery morbidity. Physicians must recognize cases with a higher risk of sentinel lymph node marking failure and consider alternative localization techniques involving peri-areolar radioisotope injection. This consideration is particularly important for large, adipose breasts with tumors in the inner quadrants, as demonstrated by our results.
The preference for ROLL due to its simplicity, patient comfort, and cosmetic outcomes is well-supported by the literature. However, the study also appropriately acknowledges the continued relevance of wire localization, especially in specific clinical scenarios.
The analysis of sentinel lymph node marking failures highlights an important area of concern and suggests a tailored approach based on individual patient characteristics, such as breast size, density, and tumor location.
5.1. Suggested Protocol for Non-Palpable Breast Tumor Localization
Given the variability in effectiveness between ROLL and WGL, this protocol emphasizes a patient-tailored approach to optimize sentinel lymph node (SLN) identification and minimize unnecessary axillary surgeries:
5.1.1. Patient Assessment
- Evaluate breast size, density, and tumor location (with special attention to inner quadrant tumors).
- Prioritize WGL or other non-palpable breast tumor localization method that uses peri-areolar radiocolloid injection for tumors located in the inner quadrants, especially in large, adipose breasts, where ROLL is less likely to achieve adequate SLN marking.
5.1.2. Preferred Technique
- ROLL: Use as the primary localization method for non-palpable tumors, given its advantages in patient comfort, procedural simplicity, and cosmetic outcomes.
- WGL: Prefer for patients with tumors in the inner quadrants, particularly those who have undergone neoadjuvant chemotherapy, as WGL demonstrates superior SLN identification in these cases.
5.1.3. Intraoperative Contingency Plan
- If SLN marking fails using ROLL, intraoperative blue dye injection into the subareolar plexus should be employed.
- Surgeons should be prepared to perform axillary lymph node dissection if SLN identification remains unsuccessful.
5.1.4. Post-Chemotherapy Considerations
- For patients with tumor regression after neoadjuvant chemotherapy, consider avoiding ROLL when SLN identification is critical, as its success rate is lower without peri-areolar isotope injection in such cases compared to WGL. Especially in adipose involution of large breasts.
This protocol aims to optimize SLN marking success and reduce axillary surgery morbidity by selecting the appropriate technique based on individual tumor and breast characteristics.
6. Conclusions
Patients report experiencing less pain with the ROLL procedure compared to wire placement. From both radiological and surgical perspectives, tumor localization is technically simpler with ROLL. Although ROLL demonstrates advantages in several aspects, there was no significant difference in overall tumor localization accuracy. However, axillary sentinel lymph node marking is more frequently inadequate with peritumoral (ROLL) marking, particularly for tumors located in the inner quadrants. In these situations, the wire-guided technique or alternative approaches utilizing peri-areolar isotope injection are recommended to ensure more accurate sentinel lymph node identification and reduce the risk of unnecessary axillary surgery.
Informed Consent Statement:
Informed consent was obtained from all subjects involved in the study.
Author Contributions
“Conceptualization: AD, TFM.; methodology: AD, TFM; validation: AD, LD, formal analysis: AD, TFM; investigation: AD, LD; resources: AD, DK; data curation: IAH, KSZ; LD, AD, writing—original draft preparation: DA, TFM, DK; writing—review and editing: DA, TFM, DK, visualization: AD, DK, TFM, IAH, KSZ, supervision: TFM, IAH, project administration: AD. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study protocol was approved by the Scientific Ethics Committee of Petz Aladár University Teaching Hospital, Hungary (Ethical approval number reference: 76-1-25/2019).
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A. Statistical Results
Figure 5.
Breast size and type distribution in the WGL group.
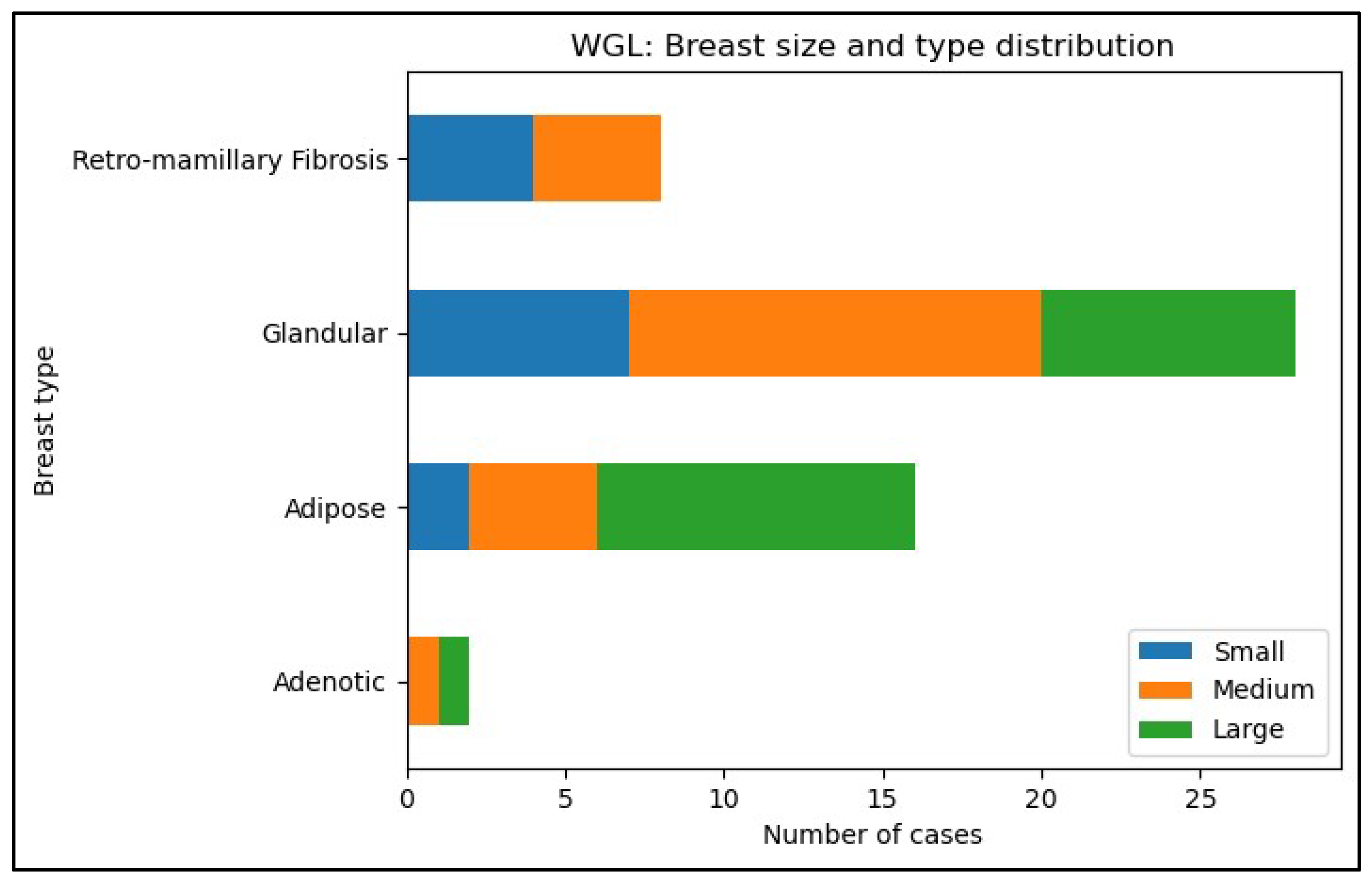
Figure 6.
Breast size and type distribution in the ROLL group.
- 1.
- Ages of patients in the two examined groups
Figure 7.
Ages of patients in the examined groups at the time of the operation. The mean age of patients was 62.4 ± 11.31 years in the ROLL group and 59.56 ± 10.1 years in the WGL group, with 95% confidence intervals of (59.37, 65.43) and (56.8, 62.32), respectively.
Figure 7.
Ages of patients in the examined groups at the time of the operation. The mean age of patients was 62.4 ± 11.31 years in the ROLL group and 59.56 ± 10.1 years in the WGL group, with 95% confidence intervals of (59.37, 65.43) and (56.8, 62.32), respectively.
- 2.
- BMI of patients in the two examined groups
Mean BMI 25.5±4.2 in the ROLL group and 26,5±4.1 in the WGL group (P value: 0.5932).
Figure 8.
BMI of patients at the time of the operation.
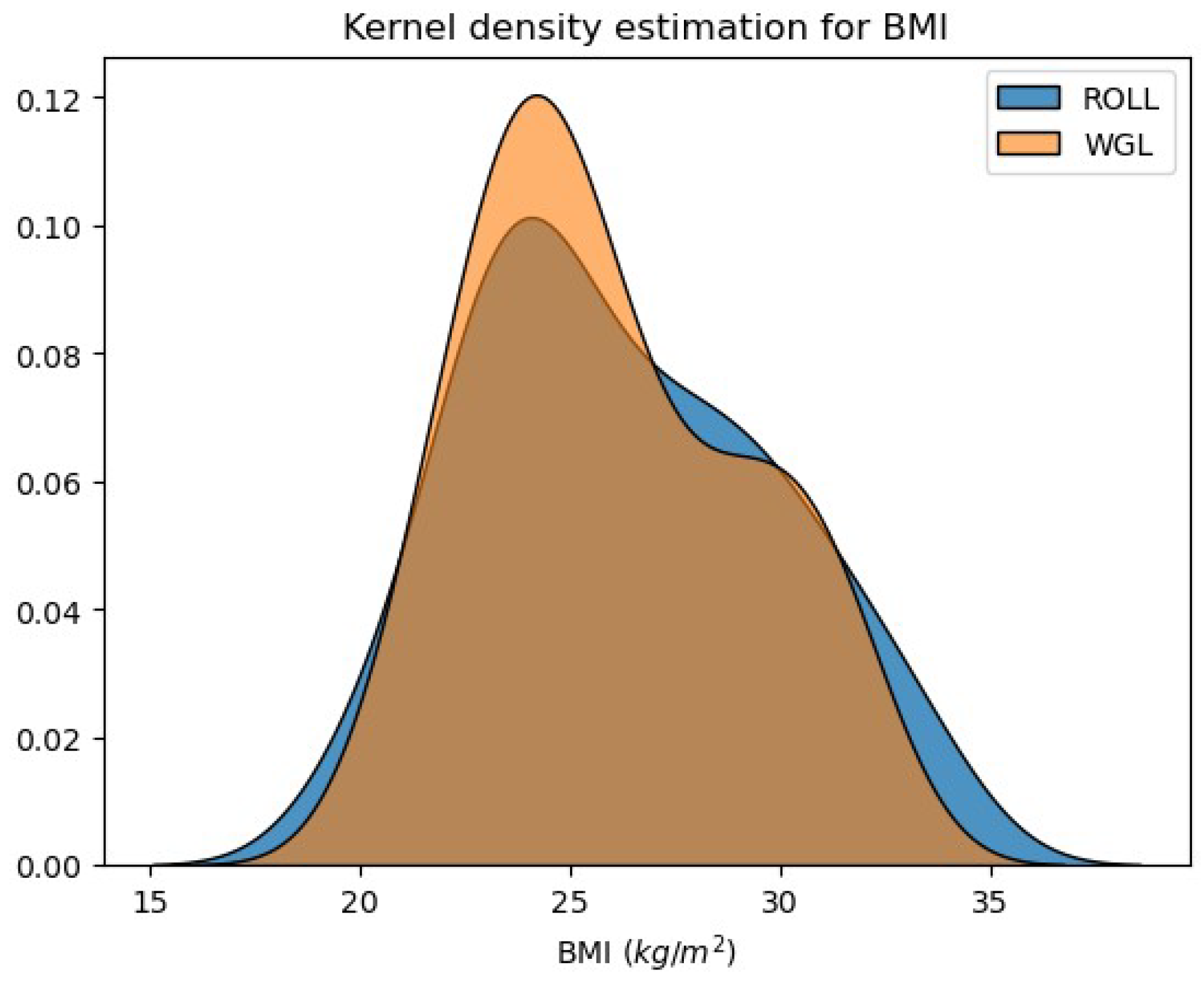
Mean BMI was 26.24 ± 3.61 kg/m² in the ROLL group and 25.89 ± 3.19 kg/m² in the WGL group, with 95% confidence intervals of (25.27, 27.2) and (25.01, 26.76), respectively. No significant differences were found between the groups regarding age or BMI distributions.
- 3.
- Pre-operative difficulty of non-palpable breast lesion marking with each procedure - Radiologists’ perspective
Figure 9.
Pre-operative difficulty of non-palpable breast lesion marking.
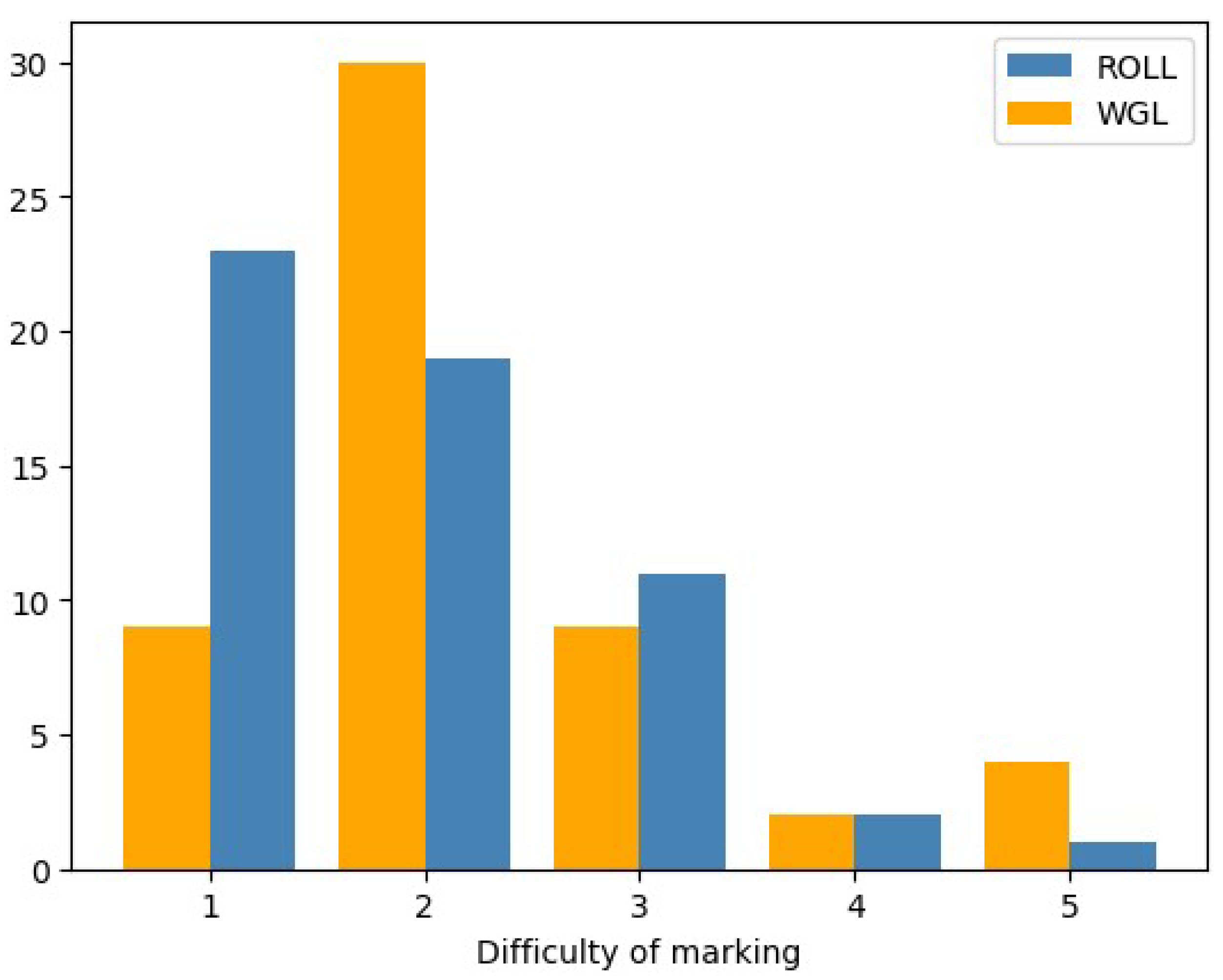
ROLL: min: 1, mean: 1.75, median: 1.5, max: 5, standard deviation: 0.96
WGL: min: 1, mean: 2.31, median: 2, max: 5, standard deviation: 0.97
The pre-operative difficulty of lesion marking in case of ROLL is significantly lower than in the case of WGL (Mann-Whitney, p-value:0.00022).
- 4.
- Time duration of marking procedures
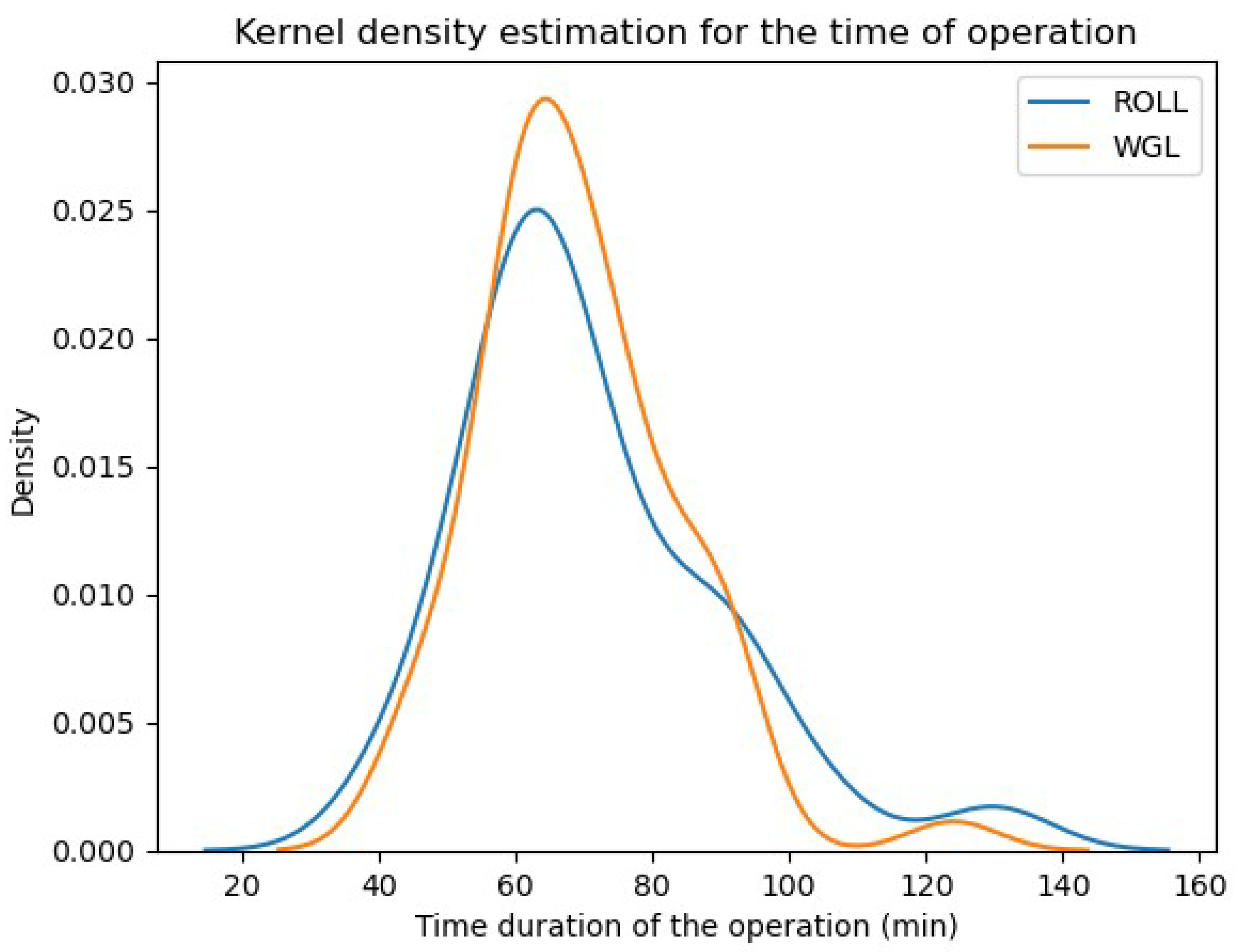
Figure 10.
Time duration of marking the non-palpable tumors.
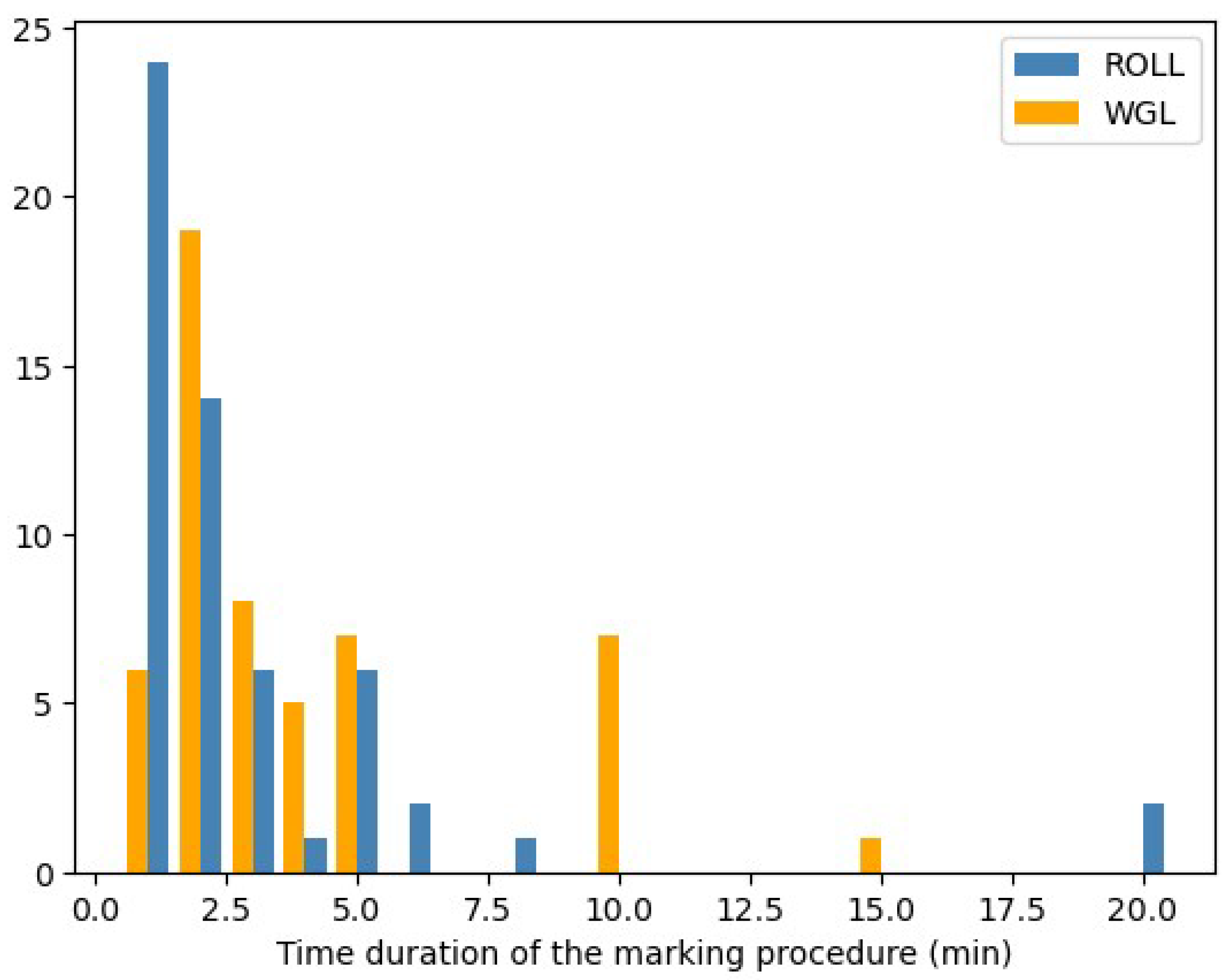
ROLL: mean: 2.93 minutes, std: 3.71
WGL: mean: 3.92 minutes, std: 3.16
The Time duration of localization in case of ROLL is significantly lower than in the case of WGL (Mann-Whitney, p-value:0.001).
- 5.
- The pain of tumor marking with each technique – Patients’ perspective
Figure 11.
Pain of the tumor marking procedures.
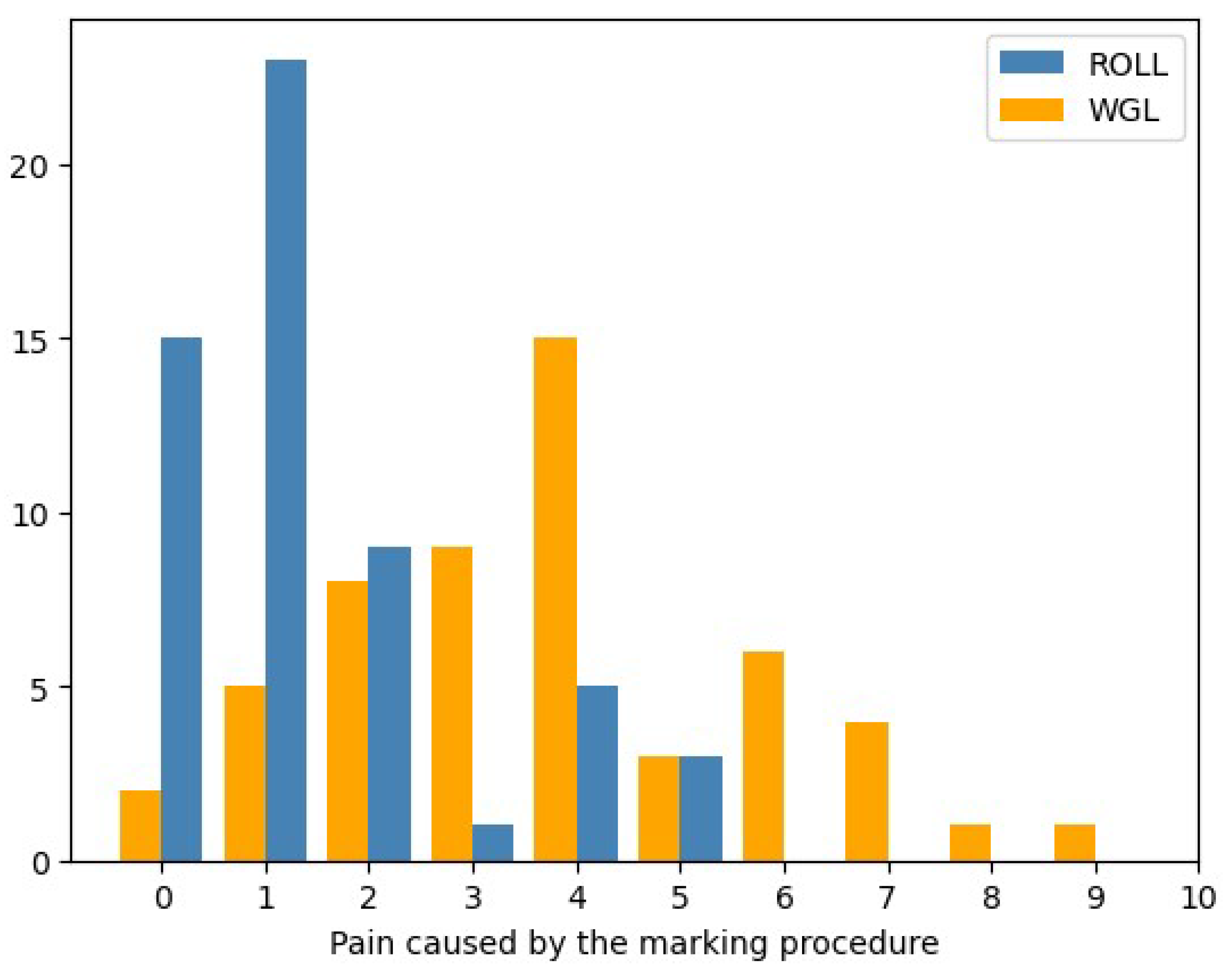
The pain of tumor marking with each technique – Patients’ perspective
Pain was assessed by the patients themselves using the Wong-Baker scale [[1]] from 0 (no pain=no hurt)-10 (maximum pain=hurts worst).
ROLL: min.: 0, mean: 1.41, median: 1, max: 5, standard deviation: 1.42
WGL: min: 0, mean: 3.78, median: 4, max: 9, standard deviation: 2.03
The pain caused in ROLL marking is significantly lower, than during WGL (Mann-Whitney test p-value: 0.0000000007).
- 6.
- Operative difficulty of lesion localization – Surgeons’ perspective
Figure 12.
Operative difficulty of lesion localization.
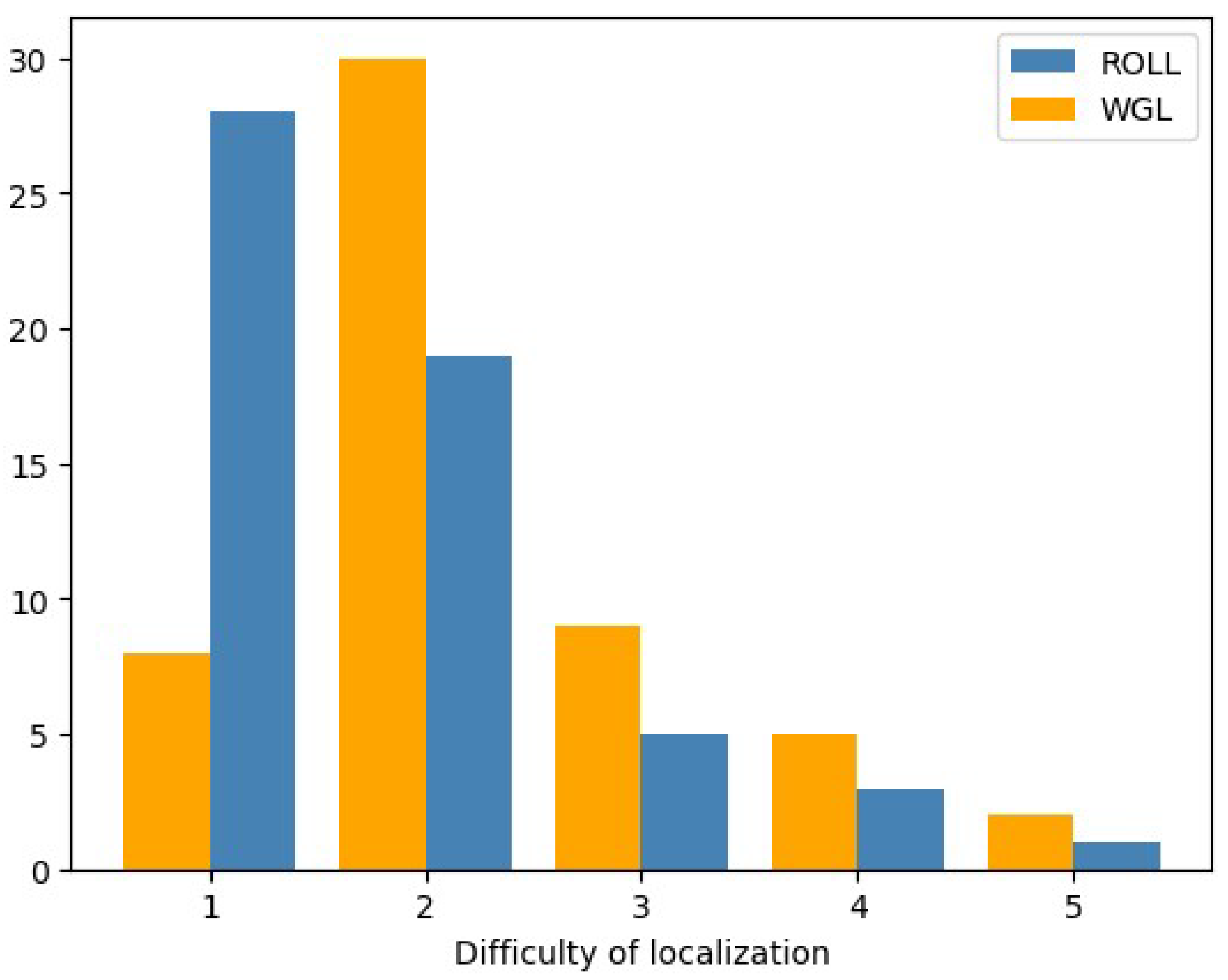
ROLL: min: 1, mean: 1.91, median: 2, max: 5, standard deviation: 0.96
WGL: min 1, mean: 2.29, median: 2, max: 5, standard deviation: 1.04
The Operative difficulty of lesion localization in case of ROLL is significantly lower than in the case of WGL (Mann-Whitney, p-value:0.0197).
- 7.
- Time (duration) of operation (min):
Figure 13.
Time duration of the operations in each group.
ROLL: mean: 71.05 minutes, std: 18.92
WGL: mean: 69.26 minutes, std: 14.51
The 95% confidence intervals for the mean time are (65.99, 76.12) and (65.3 , 73.22), respectively.
There is no significant difference between the distributions of the duration of operation (p-value: 0.9593), there is no significant difference between the mean time (According to Kolmogorov-Smirnov test and two sample t-test, Welch’s version, p-value: 0.5771).
- 8.
- Weight of the specimen:
Figure 14.
Weight of specimens in the two groups.
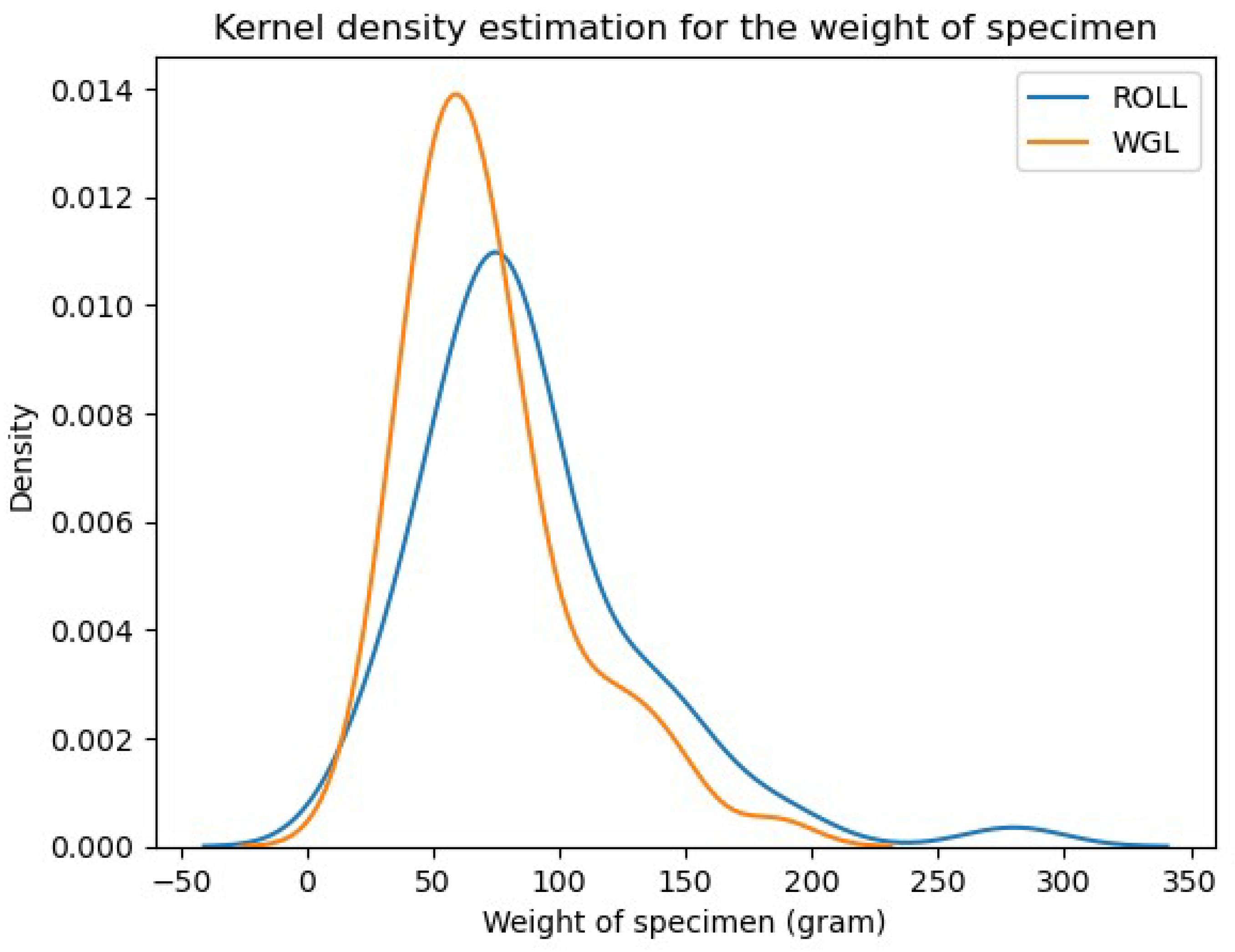
ROLL: mean: 88.48 grams, standard deviation: 45.25
WGL: mean: 72.43 grams, standard deviation: 33.55
The 95% confidence intervals for the mean weight are (76.36, 100.6) and (63.27, 81.58), respectively.
Volume of the removed tissue, represented by its weight was not different in the two groups, based on the Kolmogorov-Smirnov test. However, while there is no significant difference between the weight distributions (p-value: 0.0637) this p-value is quite close to the margin (0.05), moreover, the Kolmogorov-Smirnov test is conservative. Thus, we applied other tests: based on the Cramer - von Mises test (p-value: 0.0162) or on the Mann-Whitney test (p-value: 0.019) there is significant difference between the distributions, meaning that average specimen weigh was bigger in the ROLL group. Moreover, the mean value of WGL is significantly smaller (p-value: 0.0183).
Appendix B
For clarity, we provide a summary of the statistical comparisons presented in the Table 5, and Table 6. ‘No difference’ indicates no statistically significant difference at the 5% level, while ‘better’ refers to a lower failure rate. Additionally, the corresponding p-values are provided.

Table 9.
Comparison of sentinel lymph node marking failure.
| Localization | Isotope marking failure | Patent blue marking failure |
| Lower-inner q. | WGL better (0.0265) | no difference (0.0847) |
| Upper-inner q. | no difference (0.0607) | WGL better (0.0017) |
| Central | - | - |
| Lower-outer q. | WGL better (0.0451) | no difference (0.1812) |
| Upper-outer q. | WGL better (0.0155) | no difference (0.1169) |
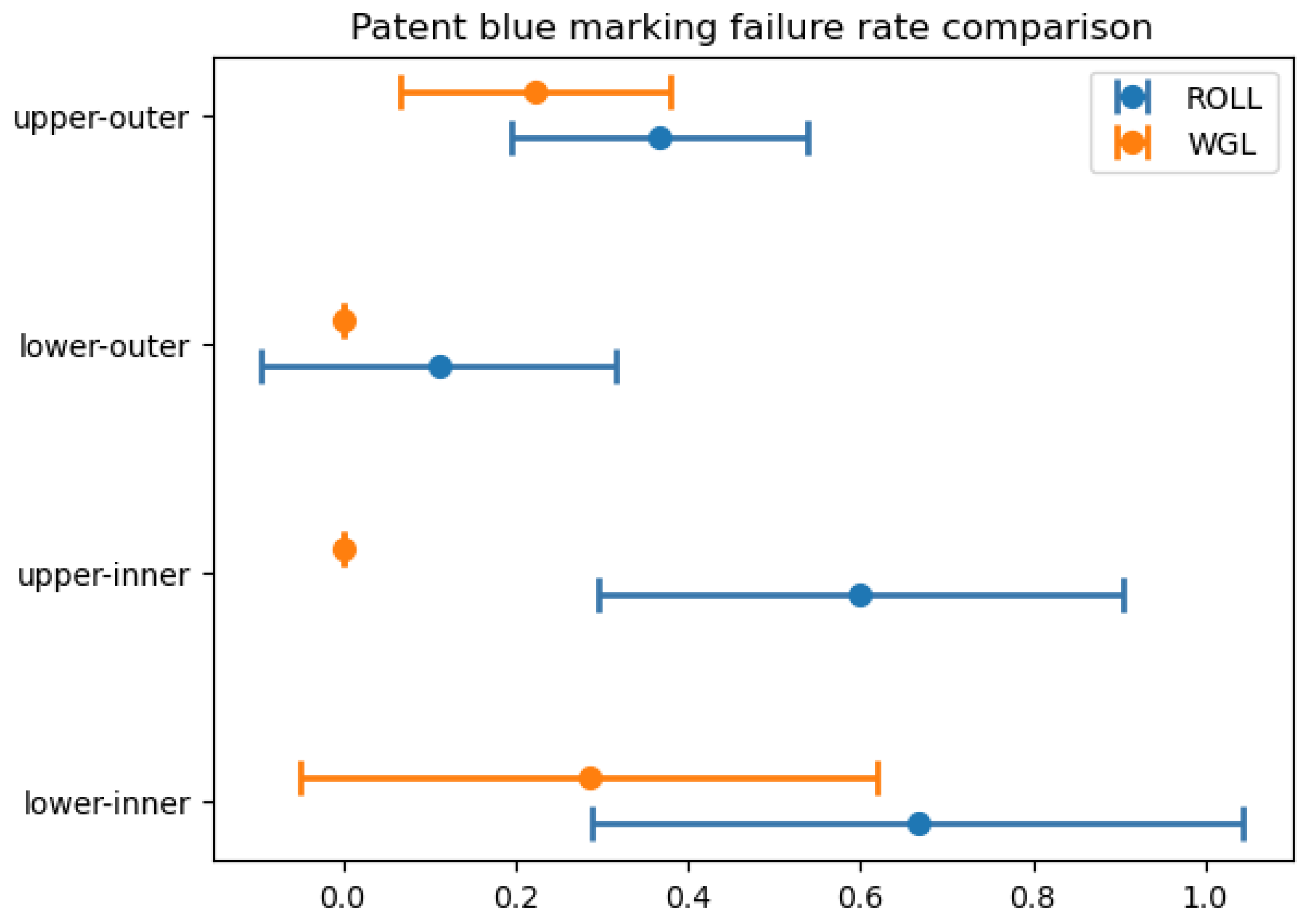
For clear visualization of the situation, we constructed confidence intervals for the failure rates (using Wald estimation). Graphically, if the mean (middle point of the interval) is included in the other interval, then there is no significant difference at a level of 5%. Note that Wald estimation provides narrower intervals than Student (t) estimation.
Figure 15.
Confidence intervals for comparison of WGL and ROLL isotope marking failure rates.
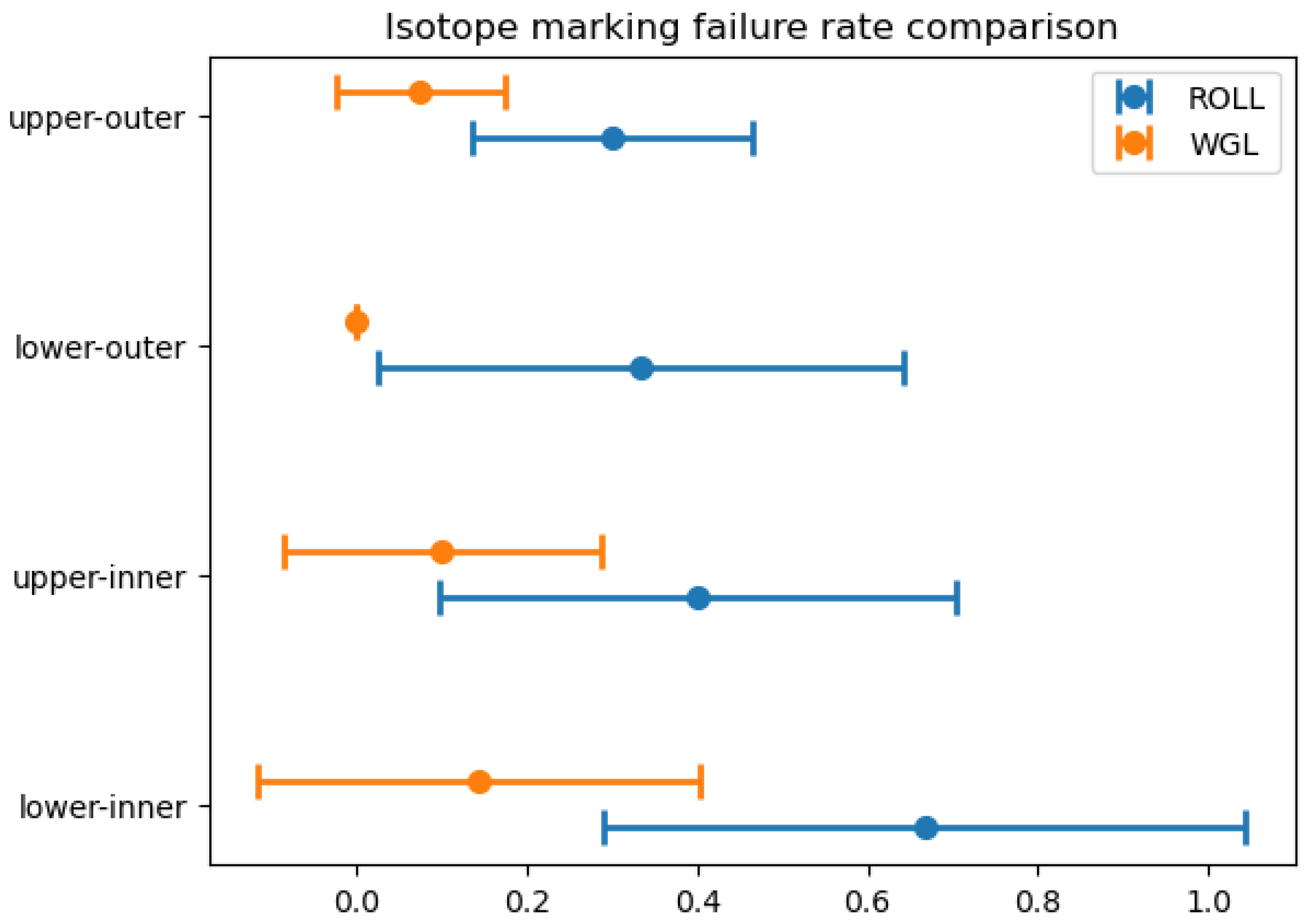
Figure 16.
Confidence intervals for comparison of WGL and ROLL patent blue marking failure rates.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Plevritis, S.K.; Munoz, D.; Kurian, A.W.; Stout, N.K.; Alagoz, O.; Near, A.M.; Lee, S.J.; Broek, J.J.v.D.; Huang, X.; Schechter, C.B.; et al. Association of Screening and Treatment With Breast Cancer Mortality by Molecular Subtype in US Women, 2000-2012. JAMA 2018, 319, 154–164. [Google Scholar] [CrossRef]
- Massat, N.J.; Dibden, A.; Parmar, D.; Cuzick, J.; Sasieni, P.D.; Duffy, S.W. Impact of Screening on Breast Cancer Mortality: The UK Program 20 Years On. Cancer Epidemiology Biomarkers Prev. 2016, 25, 455–462. [Google Scholar] [CrossRef]
- Beriwal, S.; Schwartz, G.F.; Komarnicky, L.; Garcia-Young, J.A. Breast-Conserving Therapy after Neoadjuvant Chemotherapy: Long-term Results. Breast J. 2006, 12, 159–164. [Google Scholar] [CrossRef]
- Kopans, D.B.; DeLuca, S. A modified needle-hookwire technique to simplify preoperative localization of occult breast lesions. Radiology 1980, 134, 781. [Google Scholar] [CrossRef]
- Elzohery, Y.H.; Gomaa, M.M.; Mohamed, G.; Fadlalla, W.M.; Taha, S.N.; Ibraheem, M.H. Comparison of wire-guided localization (WGL) and radio-guided occult lesion localization (ROLL) in localization of non-palpable breast lesions. World J. Surg. Oncol. 2023, 21, 1–10. [Google Scholar] [CrossRef]
- the ROLL study group. Postma, E.L.; Verkooijen, H.M.; van Esser, S.; Hobbelink, M.G.; van der Schelling, G.P.; Koelemij, R.; Witkamp, A.J.; Contant, C.; van Diest, P.J.; et al. Efficacy of ‘radioguided occult lesion localisation’ (ROLL) versus ‘wire-guided localisation’ (WGL) in breast conserving surgery for non-palpable breast cancer: a randomised controlled multicentre trial. Breast Cancer Res. Treat. 2012, 136, 469–478. [Google Scholar] [CrossRef]
- A, L.; S, Z.; V, G.; G, P. Correspondence. Eur. J. Cancer 1998, 34, 204–205. [Google Scholar] [CrossRef]
- Feggi, L.; Basaglia, E.; Corcione, S.; Querzoli, P.; Soliani, G.; Ascanelli, S.; Prandini, N.; Bergossi, L.; Carcoforo, P. An original approach in the diagnosis of early breast cancer: use of the same radiopharmaceutical for both non-palpable lesions and sentinel node localisation. Eur. J. Nucl. Med. 2001, 28, 1589–1596. [Google Scholar] [CrossRef]
- Takács, T.; Paszt, A.; Simonka, Z.; Ábrahám, S.; Borda, B.; Ottlakán, A.; Ormándi, K.; Lázár, M.; Vörös, A.; Kahán, Z.; et al. Radioguided Occult Lesion Localisation Versus Wire-Guided Lumpectomy in the Treatment of Non-Palpable Breast Lesions. Pathol. Oncol. Res. 2013, 19, 267–273. [Google Scholar] [CrossRef]
- Hawkins, S.; Brown, I.; King, P.; El-Gammal, M.; Stepp, K.; Widdison, S.; Barta, M.; Jackson, N.; English, R.; Ahmad, S.; et al. Time to go wireless? A 15-year single institution experience of radioisotope occult lesion localisation (ROLL) for impalpable breast lesions. Eur. J. Surg. Oncol. (EJSO) 2016, 43, 62–67. [Google Scholar] [CrossRef]
- Lovrics, P.J.; Cornacchi, S.D.; Vora, R.; Goldsmith, C.H.; Kahnamoui, K. Systematic review of radioguided surgery for non-palpable breast cancer. Eur. J. Surg. Oncol. (EJSO) 2011, 37, 388–397. [Google Scholar] [CrossRef]
- Banys-Paluchowski, M.; Kühn, T.; Masannat, Y.; Rubio, I.; de Boniface, J.; Ditsch, N.; Cakmak, G.K.; Karakatsanis, A.; Dave, R.; Hahn, M.; et al. Localization Techniques for Non-Palpable Breast Lesions: Current Status, Knowledge Gaps, and Rationale for the MELODY Study (EUBREAST-4/iBRA-NET, NCT 05559411). Cancers 2023, 15, 1173. [Google Scholar] [CrossRef]
- Kane, R.L.; Bershadsky, B.; Rockwood, T.; Saleh, K.; Islam, N.C. Visual Analog Scale pain reporting was standardized. J. Clin. Epidemiology 2005, 58, 618–623. [Google Scholar] [CrossRef]
- Drozgyik, A.; Szabó, T.; Kovács, G.; Kollár, D.; Molnár, T.F. A New Approach to Breast Specimen Orientation: Avoiding Pitfalls with the Specimen Plate Concept. Curr. Oncol. 2024, 31, 4589–4598. [Google Scholar] [CrossRef]
- Schrenk, P.; Hochreiner, G.; Fridrik, M.; Wayand, W. Sentinel Node Biopsy Performed Before Preoperative Chemotherapy for Axillary Lymph Node Staging in Breast Cancer. Breast J. 2003, 9, 282–287. [Google Scholar] [CrossRef]
- McGhan, L.J.; McKeever, S.C.; Pockaj, B.A.; Wasif, N.; Giurescu, M.E.; Walton, H.A.; Gray, R.J. Radioactive Seed Localization for Nonpalpable Breast Lesions: Review of 1,000 Consecutive Procedures at a Single Institution. Ann. Surg. Oncol. 2011, 18, 3096–3101. [Google Scholar] [CrossRef]
- Ahmed, M.; Douek, M. ROLL versus RSL: toss of a coin? Breast Cancer Res. Treat. 2013, 140, 213–217. [Google Scholar] [CrossRef]
- Lázár G, Kelemen P, Kósa C, et al. IV. Emlőrák Konszenzus Konferencia – Az Emlőrák Korszerű Sebészi Kezelése [Modern Surgical Treatment of Breast Cancer. 4th Breast Cancer Consensus Conference]. Magy Onkol. 2020;64(4):329-346.
- Burstein, H.J.; Curigliano, G.; Loibl, S.; Dubsky, P.; Gnant, M.; Poortmans, P.; Colleoni, M.; Denkert, C.; Piccart-Gebhart, M.; Regan, M.; et al. Estimating the benefits of therapy for early-stage breast cancer: the St. Gallen International Consensus Guidelines for the primary therapy of early breast cancer 2019. Ann. Oncol. 2019, 30, 1541–1557. [Google Scholar] [CrossRef]
- Balic, M.; Thomssen, C.; Würstlein, R.; Gnant, M.; Harbeck, N. St. Gallen/Vienna 2019: A Brief Summary of the Consensus Discussion on the Optimal Primary Breast Cancer Treatment. Breast Care 2019, 14, 103–110. [Google Scholar] [CrossRef]
- Hellingman, D.; Wan, O.Y.; Veen, B.J.d.W.-V.d.; van der Ploeg, I.M.; Elkhuizen, P.H.; Rutgers, E.J.; Stokkel, M.P.; Hellingman, D.; Wan, O.Y.; Veen, B.J.d.W.-V.d.; et al. Predictive risk factors for sentinel lymph node nonvisualization on planar lymphoscintigraphy using an intratumoral injection in patients with primary breast cancer. Nucl. Med. Commun. 2019, 40, 317–324. [Google Scholar] [CrossRef]
- Borgstein, P.J.; Meijer, S.; Pijpers, R.J.; van Diest, P.J. Functional Lymphatic Anatomy for Sentinel Node Biopsy in Breast Cancer. Ann. Surg. 2000, 232, 81–89. [Google Scholar] [CrossRef]
- Klimberg, V.S.; Rubio, I.T.; Henry, R.; Cowan, C.; Colvert, M.; Korourian, S. Subareolar Versus Peritumoral Injection for Location of the Sentinel Lymph Node. Ann. Surg. 1999, 229, 860–860. [Google Scholar] [CrossRef]
- Smith, L.F.; Cross, M.J.; Klimberg, V. Subareolar injection is a better technique for sentinel lymph node biopsy. Am. J. Surg. 2000, 180, 434–438. [Google Scholar] [CrossRef]
Figure 1.
SLN isotope marking failure in the different quadrants and the proportion of large breasts in fatty involution - ROLL group.
Figure 1.
SLN isotope marking failure in the different quadrants and the proportion of large breasts in fatty involution - ROLL group.
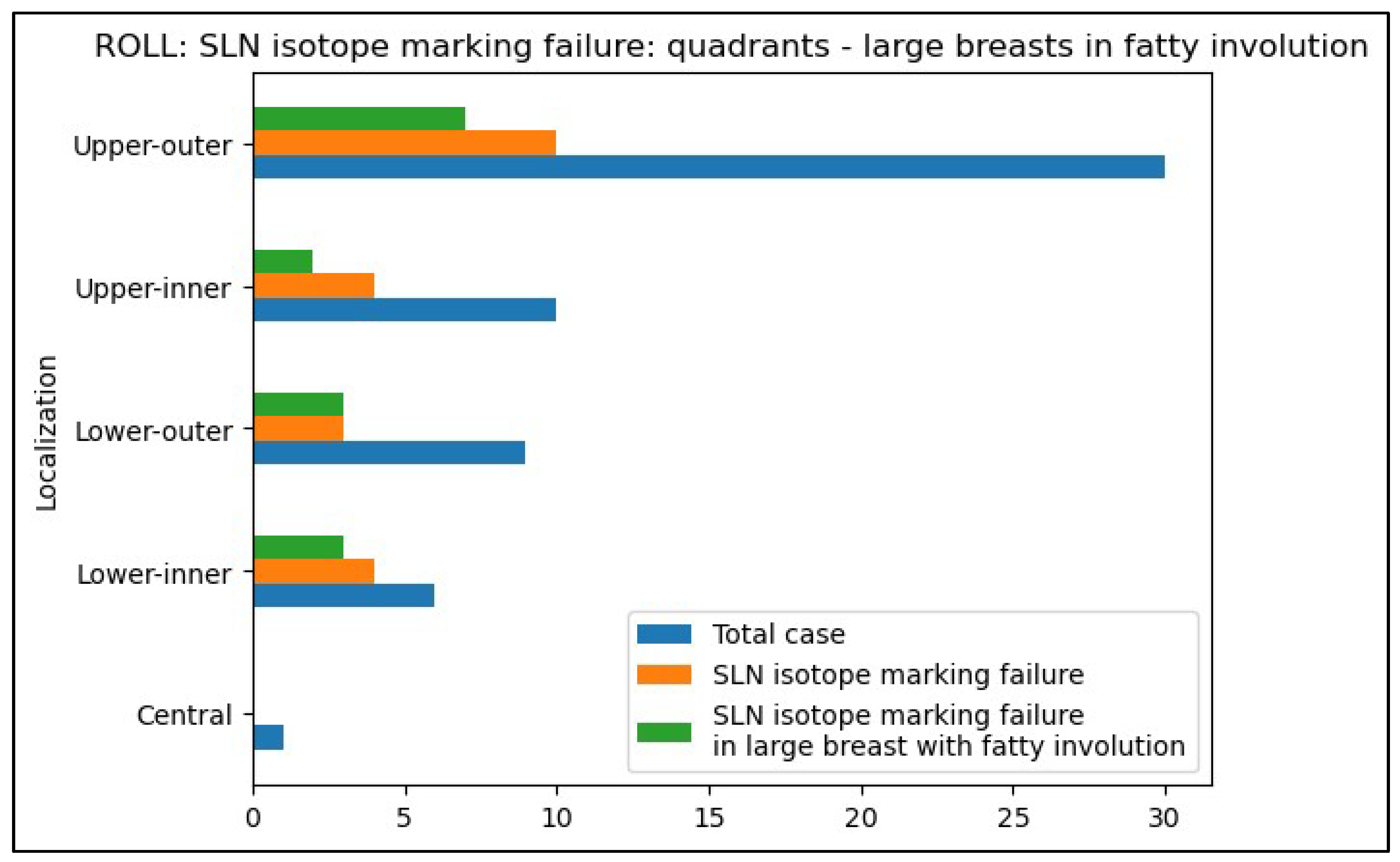
Figure 2.
SLN isotope marking failure in the different quadrants and the proportion of large breasts in fatty involution - WGL group.
Figure 2.
SLN isotope marking failure in the different quadrants and the proportion of large breasts in fatty involution - WGL group.
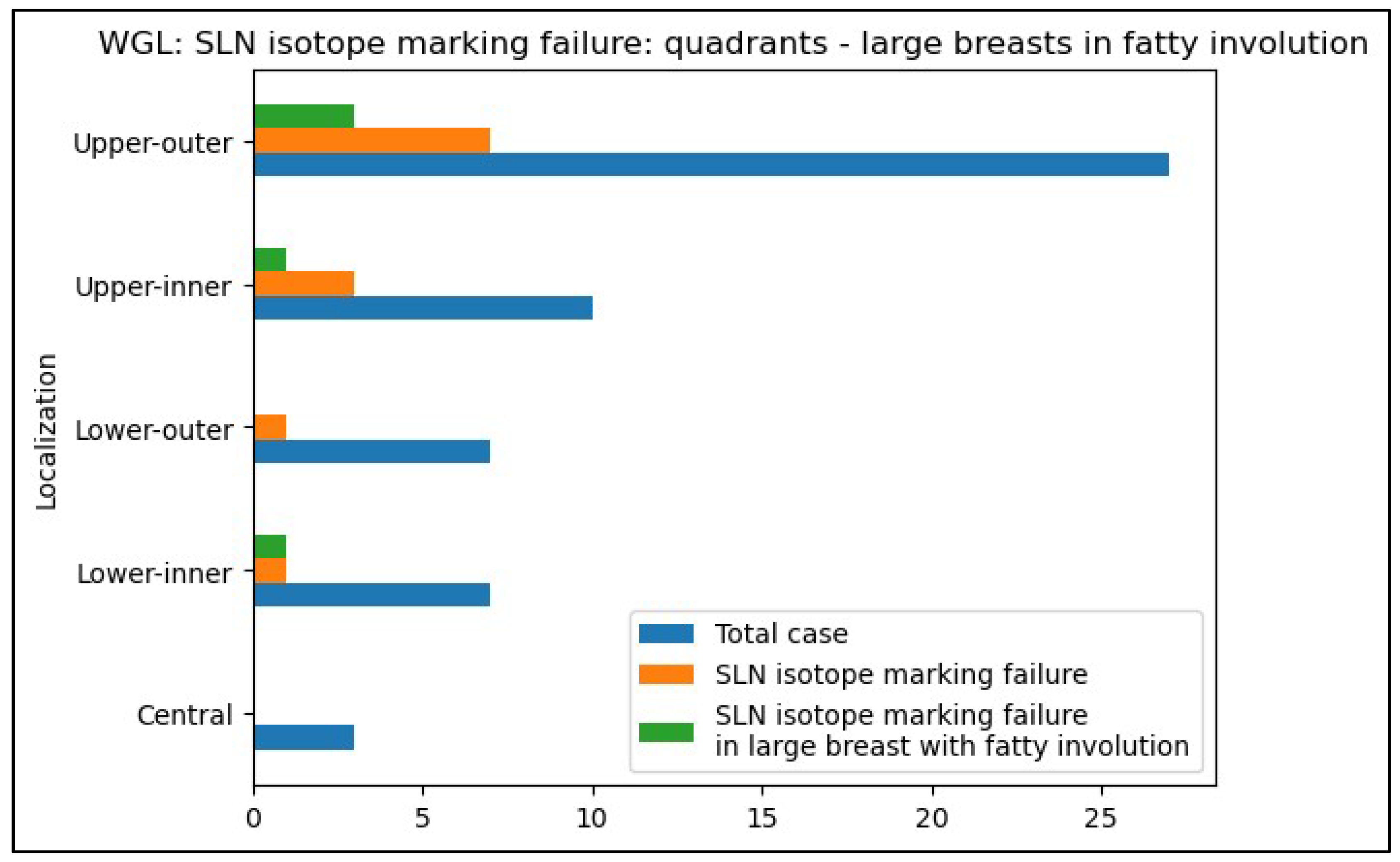
Figure 3.
The primary tumor size distribution based on postoperative histopathological examination of the excised specimen in the ROLL group.
Figure 3.
The primary tumor size distribution based on postoperative histopathological examination of the excised specimen in the ROLL group.
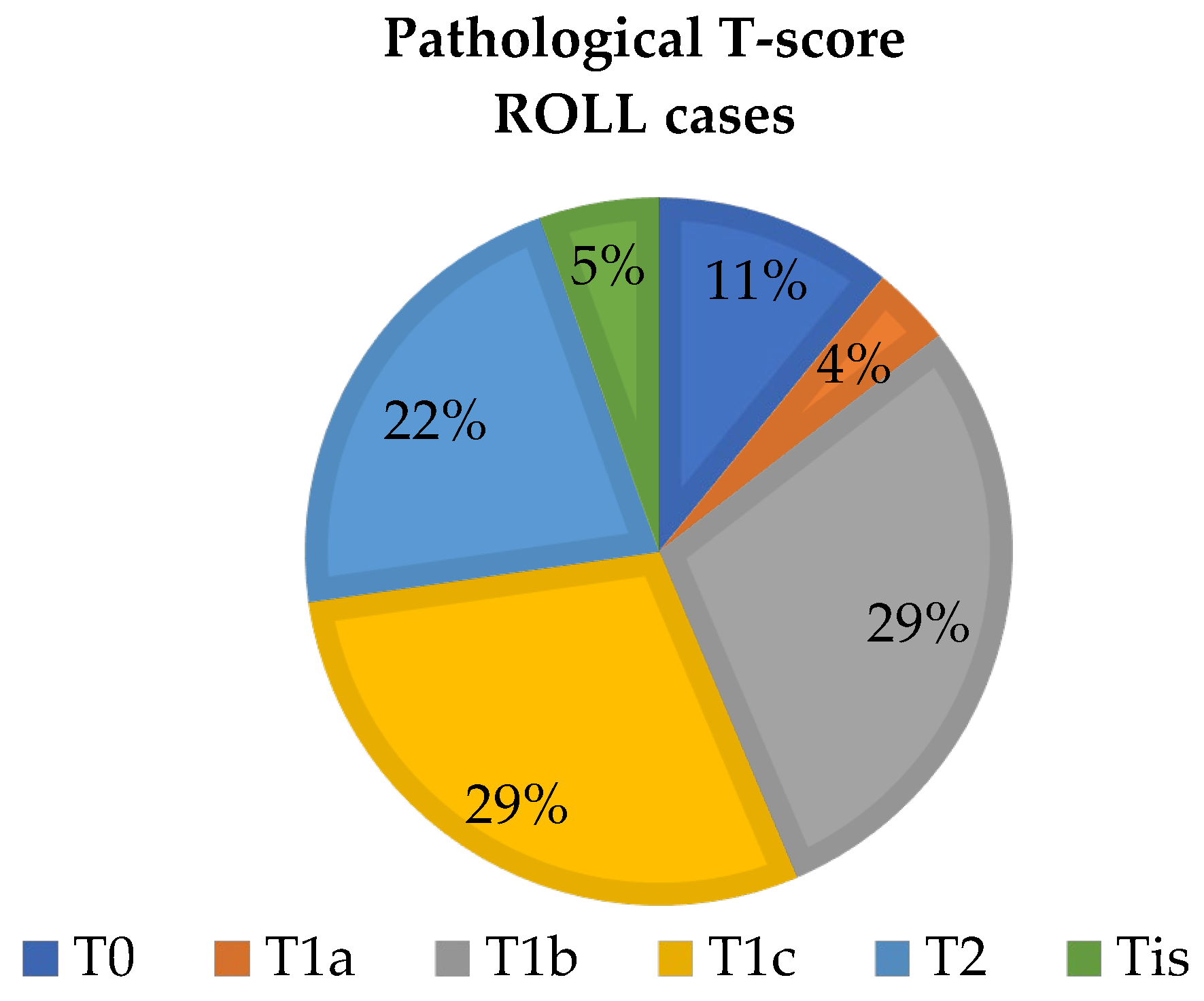
Figure 4.
The primary tumor size distribution based on postoperative histopathological examination of the excised specimen in the WGL group.
Figure 4.
The primary tumor size distribution based on postoperative histopathological examination of the excised specimen in the WGL group.
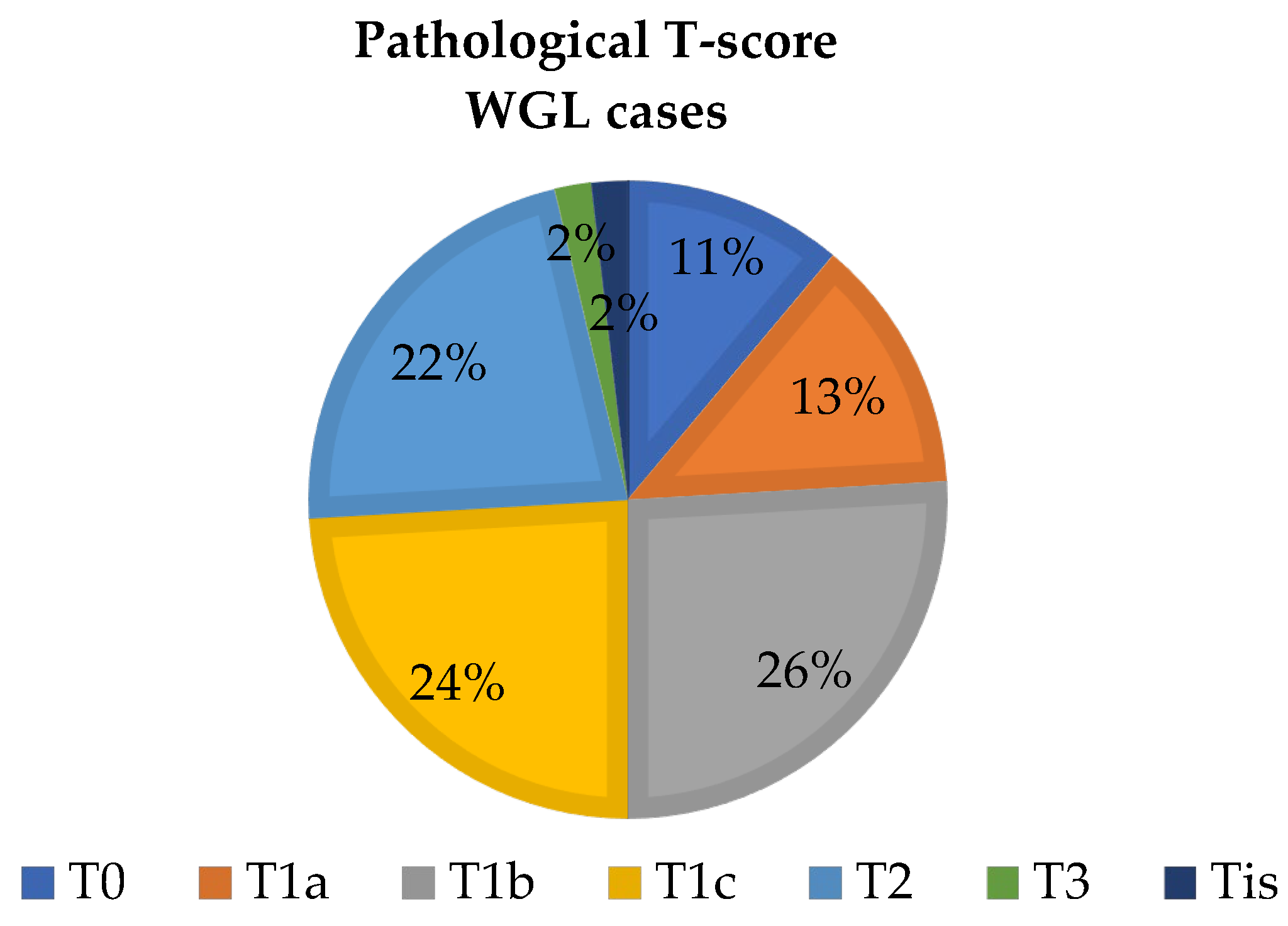
Table 1.
The ratio of cases for non-palpable lesions of primary surgeries and operations after neoadjuvant treatments.
Table 1.
The ratio of cases for non-palpable lesions of primary surgeries and operations after neoadjuvant treatments.
| ROLL/WGL group | Cancer screening | Neoadjuvant therapy |
| ROLL group | 43 (77%) | 13 (23%) |
| WGL group | 44 (79%) | 10 (18%) |
Table 2.
Breast Size and Type Distribution in the ROLL group (n=56).
| Type- and size of breast in the ROLL group (n=56) | Glandular | Adipose | Retro-mamillary Fibrosis | Adenotic | Fibrotic | Total |
| Small | 8(14%) | 1(2%) | 0 | 3(5%) | 1(2%) | 13(23%) |
| Medium | 9(16%) | 2(4%) | 1(2%) | 0 | 0 | 12(21%) |
| Large | 10(18%) | 20(36%) | 0 | 0 | 1(2%) | 31(55%) |
Table 3.
Breast Size and Type Distribution in the WGL Group (n=54).
| Type- and size of breast in the WGL group (n=56) | Glandular | Adipose | Retro-mamillary Fibrosis | Adenotic | Fibrotic | Total |
| Small | 7(13%) | 2(4%) | 4(7%) | 0 | 0 | 13(24%) |
| Medium | 13(24%) | 4(7%) | 4(7%) | 1(2%) | 0 | 22(40%) |
| Large | 8(15%) | 10(19%) | 0 | 1(2%) | 0 | 19(35%) |
Table 4.
Distribution of Tumor Localization in Breast Quadrants.
| Localization* | ROLL(n=56) | WGL (n=54) | ||||
| Laterality | Number of cases | Laterality | Number of cases | |||
| Left | Right | Left | Right | |||
| Lower-inner q. | 3 (5%) | 3 (5%) | 6 (11%) | 4 (7%) | 3 (5%) | 7 (13%) |
| Upper-inner q. | 8 (14%) | 2 (4%) | 10 (18%) | 8 (14%) | 2 (4%) | 10 (18%) |
| Central | 1 (2%) | 0 | 1 (2%) | 1 (2%) | 2 (4%) | 3 (5%) |
| Lower-outer q. | 1 (2%) | 8 (14%) | 9 (16%) | 2 (4%) | 5 (9%) | 7 (13%) |
| Upper-outer q. | 14 (25%) | 16 (29%) | 30 (54%) | 11 (20%) | 16 (29%) | 27 (48%) |
*Provides detailed data on the distribution of tumors across different quadrants of the breast in both the ROLL and WGL groups, considering both the left and right sides. The majority of tumors were located in the upper-outer quadrant for both groups, reflecting a common site for breast tumors.
Table 5.
Sentinel lymph node marking failure.
| ROLL (n=56) | WGL (n=54) | |||
| Localization | Isotope marking failure | Patent blue marking failure | Isotope marking failure | Patent blue marking failure |
| Lower-inner q. | 4 (67%) | 4 (67%) | 1 (14%) | 2 (29%) |
| Upper-inner q. | 4 (40%) | 6 (60%) | 1 (10%) | 0 |
| Central | 0 | 0 | 0 | 1 (33%) |
| Lower-outer q. | 3 (33%) | 1 (11%) | 0 | 0 |
| Upper-outer q. | 9 (30%) | 11 (37%) | 2 (7%) | 6 (22%) |
Table 6.
Comparison of sentinel lymph node marking failure rates.
| Localization | Isotope marking failure | Patent blue marking failure |
| Lower-inner quadrant | 0.0265* | 0.0847 |
| Upper-inner quadrant | 0.0607 | 0.0017** |
| Central | - | - |
| Lower-outer quadrant | 0.0451* | 0.1812 |
| Upper-outer quadrant | 0.0155* | 0.1169 |
P values: * p<0.05, ** p<0.01.
Table 7.
Rate and percentage of SLN isotope marking depending on the Breast Size and Type Distribution in the ROLL group (n=56).
Table 7.
Rate and percentage of SLN isotope marking depending on the Breast Size and Type Distribution in the ROLL group (n=56).
| Type- and size of breast in the ROLL group (n=56) | Glandular | Adipose | Retro-mamillary Fibrosis | Adenotic | Fibrotic | Total |
| Small | 8/8(100%) | 1/1(1) | 0/0(0) | 3/3(1) | 1/1(1) | 13/13(1) |
| Medium | 9/8(89%) | 2/1(50%) | 1/1(100%) | 0/0 | 0/0(0) | 12/10(83%) |
| Large | 10/6(60%) | 20/5(25%) | 0/0 | 0/0 | 1/1(100%) | 31/12(39%) |
Table 8.
Rate and percentage of isotope marking depending on the Breast Size and Type in the WGL Group (n=54).
Table 8.
Rate and percentage of isotope marking depending on the Breast Size and Type in the WGL Group (n=54).
| Type- and size of breast in the WGL group (n=54) | Glandular | Adipose | Retro-mamillary Fibrosis | Adenotic | Fibrotic | Total |
| Small | 7/7(100%) | 2/2(100%) | 4/3(75%) | 0/0 | 0/0 | 13/12(92%) |
| Medium | 13/9(69%) | 4/4(100%) | 4/4(100%) | 1/1(100%) | 0/0 | 22/18(82%) |
| Large | 8/6(75%) | 10/5(50%) | 0/0 | 1/1(100%) | 0/0 | 19/12(63%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



